ABCs of Shock
67
ABCs of Shock Pediatric Critical Care Medicine Emory University Children’s Healthcare of Atlanta
-
Upload
carter-morse -
Category
Documents
-
view
104 -
download
1
description
ABCs of Shock. Pediatric Critical Care Medicine Emory University Children’s Healthcare of Atlanta. Objectives. Review basic physiology of shock states in pediatrics Classification and recognition of clinical shock states Review initial management of shock. Definition. Shock?. Shock?. - PowerPoint PPT Presentation
Transcript of ABCs of Shock

ABCs of Shock
Pediatric Critical Care MedicineEmory University
Children’s Healthcare of Atlanta

2
Objectives• Review basic physiology of shock states in
pediatrics• Classification and recognition of clinical
shock states• Review initial management of shock

Definition
3

Shock?
4

Shock?
5

6
Definition• Failure of delivery oxygen and substrates to meet
the metabolic demands of the tissue beds
SUPPLY < DEMAND
Oxygen delivery < Oxygen Consumption DO2 < VO2
• Failure to remove metabolic end-products• Result of inadequate blood flow and/or oxygen
delivery

7
Definition• Common pathway
– Failure to deliver substrates conversion to anaerobic metabolism
• Reversible if recognized early • Irreversible organ damage at the late stage
– Progressive acidosis and eventually cell death
• Early recognition is key

8
Epidemiology• Incidence: not clear
– Shock is not commonly listed as the diagnosis in ER visits
• Estimated that more children die from sepsis than cancer each year
• Common causes: hypovolemia, sepsis & trauma– Worldwide: diarrhea– Developed countries: trauma

9
Pathophysiology• Children
– Higher % body water – Higher resting metabolic rate– Higher insensible losses– Lower renal concentrating ability– Subtle signs/symptoms
• Higher risk for organ hypo-perfusion

10
Pathophysiology
O2 supply < O2 demand
O2 delivery < O2 consumption
DO2 < VO2

11
Oxygen delivery (DO2)• DO2 = CO x CaO2
– DO2 : oxygen delivery
– CO : Cardiac output
– CaO2: arterial oxygen content
• CO = HR x SV– HR: heart rate– SV: stroke volume
• CaO2 = HgB x SaO2 x 1.34 + (0.003 x PaO2)– Oxygen content = oxygen carried by HgB + dissolved
oxygen

Oxygen delivery (DO2)DO2 = CO x CaO2
12
Critical DO2: consumption depends on delivery

Oxygen delivery DO2 = CO x CaO2
13

Oxygen delivery DO2 = CO x CaO2
• CO = HR x SV• HR is independent
– Neonates depend on HR (can’t increase SV)
• SV depends on – Pre-load: volume of blood– After-load: resistance to contraction– Contractility: force
14

Oxygen delivery DO2 = CO x CaO2
• CaO2 = HgB x SaO2 x 1.34 + (0.003 x PaO2)
• Normal circumstance: CaO2 is closely associated with SaO2
• Severe anemia or in the presence of abnormal HgB (i.e. CO poisoning) - CaO2 is strongly affected by PaO2
15

16
Hypo-perfusion• Poor perfusion of a vital organs leads to organ
dysfunction– Decreased urine output– Altered mental status
– Elevated LFTs, bilirubin• Switches to anaerobic metabolism Lactate• Activates inflammatory cascade
– Activates neutrophils, releases cytokines
• Increases adrenergic stress response– Increases lipolysis/glycogenolysis (also increases
lactate)– Releases catecholamine and corticosteroid

Classification of ShockStages vs. Types
17

18
Stages of Shock• Compensated
– Maintains end organ perfusion– BP is maintained usually by ↑ HR
• Uncompensated– Decreases micro-vascular perfusion– Sign/symptoms of end organ dysfunction– Hypotensive
• Irreversible – Progressive end-organ dysfunction– Cellular acidosis results in cell death

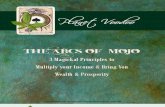
Blood Pressure and Volume
% blood loss
% BP
25% Normal
50% 60% o
19
•BP drops quickly after reaching 50% blood loss•CO follows BP closely

20
Systemic Inflammatory Response Syndrome (SIRS)
• Widespread inflammation due to infection, trauma, burns, etc.
• Criteria – requires 2 of the followings– Core temp >38.5˚C or <36˚C– Tachycardia (or bradycardia in infants)– Tachypnea– Elevated or depressed WBC or >10% bands

21
Types of Shock• Hypovolemic• Distributive• Cardiogenic• Septic

Types of Shock
Type Pathophysiology Signs & Symptoms
Hypovolemic ↓ PRELOAD: ↓CO, ↑ SVR, intravascular volume loss
↑HR, ↓ pulses, delayed cap refill, dry skin, sunken eyes, oliguria
Distributive ↓ AFTERLOAD (SVR)
Anaphylactic ↑ CO, ↓ SVR Angioedema, low BP, wheezing, resp. distress
Spinal Normal CO, ↓ SVR Low BP without tachycardia; paralysis, h/o trauma
Cardiogenic ↓ CO, variable SVR Normal to ↑ HR, ↓ pulses, delayed CR, JVD, murmur or gallop, hepatomegaly
Septic Variable More to come

23
Hypovolemic Shock• Most common type in children • #1 cause of death worldwide
– Hemorrhagic: developed countries – GI bleed, trauma (liver/spleen injuries, long bone fractures), intracranial hemorrhage
– Non-hemorrhagic: vomiting/diarrhea, heat stroke, burns, DKA
• Pathophysiology: – Loss of intravascular volume ↓ PRELOAD

24
Hypovolemic Shock• Clinical symptoms
– Sunken fontanel/eyes– Dry mucous membrane– Poor skin turgor– Delayed capillary refill– Cool extremities
• Tachycardia = compensated shock!– Normal BP until volume loss >30-40%

25
Distributive Shock• Loss of SVR (AFTERLOAD) results in abnormal
distribution of blood flow• Increased CO and HR
– Often hyper dynamic contractility, bounding pulses, flash CR
• Loss of vascular tone eventually leads to loss of PRELOAD– Blood volume pools in the periphery

26
Distributive Shock• Anaphylaxis is IgE mediated hypersensitive
response– Massive release of cytokines from activated mast cells– Associated with respiratory distress, angioedema,
vascular tone collapse
• Neurogenic: unusual and mostly transient– Follows acute CNS injury (brain or spinal cord)– Loss of sympathetic and autonomic tone– Unique presentation: hypotension with normal heart
rate

27
Distributive Shock
Vasodilation Venous pooling
Decrease after-load
Mal-distribution of regional blood flow

28
Cardiogenic Shock• Impaired CONTRACTILITY (pump failure)• 3 categories
– Cardiomyopathy– Arrhythmia– Obstruction

29
Cardiogenic Shock• Cardiomyopathy
– Infectious – post viral infection (coxsakie)– Infiltrative – storage disease– Ischemia – cardiac arrest or bypass– Sepsis – late stage

30
Cardiogenic Shock• Arrhythmia
– Ventricular fibrillation & pulseless ventricular tachycardia abolish cardiac output
– Prolonged or recurrent SVT– Brady-arrhythmias or heart block seen in neonatal SLE

31
Cardiogenic Shock• Obstructive
– Physical obstruction – tension pneumothorax, tamponade, pulmonary embolus
– Congenital - coartation of the aorta, hypoplastic left heart, critical aortic stenosis
» Usually present in shock with closing of the ductus arteriosus

Septic Shock
32

33
Septic Shock• 20% presentation – classic warm shock
– High CO, low SVR
• 60% presentation – cold shock– Low CO, high SVR
• Small % presentation with mixed pictures

34
Septic Shock• Highest in infants (particularly in newborns)• Risks
– Structural heard disease– Neutropenia– Neurodevelopmental disorders– Invasive devices

Evaluation & Treatment
35

36
Initial Assessment• Goals
– Immediate identification of life-threatening conditions– Rapid recognition of circulatory compromise– Early classification of the type and cause of shock

37
Initial Assessment• Airway
– Mental status: can the patient maintain the airway
• Breathing – ?impending respiratory failure
• Circulation– Heart rate, pulses, blood pressure– Capillary refills - perfusion
• Dextrose

Treatment
38
Increase O2 contentsIncrease cardiac outputIncrease blood pressure
Early intubationSedationAnalgesia


40
Surviving sepsis
Campaign 2008

PALS Shock Algorithm

42
History & Physical Exam• Brief medical history
– Preceding events, recent illness or trauma– PMH– Allergies & exposure
• Focused physical examination– Neuro – mental status– CV – HR/perfusion/CR, ?gallop/murmur– Resp – crackles, wheezing– GI - ?HSM

43
Early Goal-Directed Therapy
• Goal – in the first 6 hours of presentation - improvement of indicators of perfusion and vital organ function
• Physiologic targets– BP >5th percentile for age– Quality of central & peripheral pulses– Normal perfusion– Mental status– UOP > 1 ml/kg/hr

44
Fluid Resuscitation• Isotonic crystalloids – availability
– 20cc/kg reassess (overload vs. third spacing)
• Rapid infusion – 5 - 10 min
• NO upper limit– Pressor if > 60ml/kg– May need up to 100-200 ml/kg during the first few hours

Volume
45
LR NS
pH 6.0-7.5 4.5-7.0
Na+ 130 154
K+ 4 0
Ca++ 3 0
Cl- 109 154
Lactate 28 0
Calorie 9 0
Osmolarity
273 308

46
Treatment: Volume
• Volume resuscitation optimize preload• >60 ml/kg during 1st hr associated with increase
survival• Titrate volume to improve CO, normal HR, BP;
improve perfusion/cap refill; improve UOP, MS
– Carcillo JA, Fields AI. Clinical practice parameters for hemodynamic support of pediatric and neonatal patients in septic shock. Crit. Care Med. 2002; 30:1365-1378

47
Treatment: Volume
• Retrospective review of 34 pts with septic shock & hypovolemia with 1st hr fluid resuscitation– Group 1: up to 20ml/kg– Group 2: 20-40ml/kg– Group 3: >40mg/kg
• No different in rate of ARDS
– Carcillo JA, Davis AL, Zaritsky A, Role of early fluid resuscitation in pediatric septic shock. JAMA. 1991; 266:1242-1245

48
Treatment: Volume
• Colloids – blood products – Trauma or DIC in septic shock– PRBC to help with oxygen carrying and delivery

PALS Shock Algorithm

Vasopressors
50

51
Adrenergic Receptors• α – subtype-1: vascular smooth muscle
– Increase SVR, afterload
• β – Myocardium, bronchial smooth muscle & vessels– β -1: increase HR & contractility– β -2: bronchodilation, peripheral vasodilation
• Dopaminergic – renal, coronary, cerebral beds

52
Adrenergic Receptors
Alpha Dopamine Beta
Epinephrine
Norepinephrine DobutaminePhenylephrine
???Milrinone

53
Dopamine• Readily available, pre-mixed• PIV up to 10 mcg/kg/min• Start at 5 mcg/kg/min, titrate to effects• Receptors
– 2-5 mcg/kg/min (renal) – D receptors– 5-15 mcg/kg/min – β activity
– >15 mcg/kg/min – α activity

54
Dopamine• No evidence to support low-dose (“renal” dose)• Evidence that suggests dopamine inhibits
secretion of prolactin– Could increase lymphocyte apoptosis– Impairment of immune response to sepsis

55
Norepinephrine• Mostly α, minimum to no β activity increase
SVR and after-load• Start at 0.05 – 0.1 mcg/kg/min (max 1
mcg/kg/min)• “Warm” septic shock• Avoid in myocardial dysfunction

56
Epinephrine• Mostly β with some α activity• Start at 0.05 – 0.1 mcg/kg/min (max 1
mcg/kg/min)• “Cold” septic shock
– Improves contractility + vasoconstriction– Best drug for myocardial dysfunction

57
Phenylephrine• Pure α activity• Significantly increases SVR
– May have reflex bradycardia
• Spinal shock

58
Dobutamine• Mainly β-1; little β-2 and α activity• Increases contractility & HR increases
myocardial oxygen consumption• Uses in cardiac patients

59
Milrinone• Phosphodiesterase-3 inhibitor• Increases intracellular Ca++
– Improves contractility– Decreases afterload– No increase in myocardial oxygen demand– Lusotropic: diastolic relaxation improve SV
• Start 0.3 – 0.5 mcg/kg/min• Side effect: hypotension

60
Vasopressin
• V-2 receptor: – Vasoconstriction mainly in the capillaries and small
arterioles– Direct stimulation to pituitary gland ACTH production – Restores catecholamine sensitivity
• Uses in catecholamine-resistant vasodilatory shock
• 0.01 – 0.04 U/min

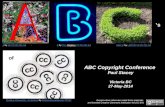
Treatment: Inotropes
61
AgentAgent Site of ActionSite of Action DoseDose
Mcg/kg/minMcg/kg/minEffectsEffects
DopamineDopamine DopaminergicDopaminergic
BetaBeta
Alpha > BetaAlpha > Beta
1-31-3
5-105-10
11-2011-20
Renal vasodilationRenal vasodilation
Inotrope/vasoconstrictionInotrope/vasoconstriction
Increase perip. Vasc. Increase perip. Vasc. resistanceresistance
DobutamineDobutamine Beta 1 & 2Beta 1 & 2 1-201-20 InotropeInotrope
VasodilationVasodilation
EpineprhineEpineprhine Beta > alphaBeta > alpha 0.05 – 1.00.05 – 1.0 Inotrope, vasoconstrictionInotrope, vasoconstriction
TachycardiaTachycardia
NorepinephNorepinephrinerine
Alpha > betaAlpha > beta 0.05 – 1.00.05 – 1.0 Profound vasoconstrictionProfound vasoconstriction
inotropeinotrope
MilranoneMilranone PhosphodiesteraPhosphodiesterase inhibitorse inhibitor
0.5 – 0.750.5 – 0.75 InotropeInotrope
vasodilationvasodilation

PALS Shock Algorithm

63
Therapy Monitoring
• Central venous pressure– Intravascular volume– Goal 6 mmgHg (nl 4-8 mmHg)
• Mixed venous saturation (SvO2)– Goal >70% (nl 65-70%)– Indicate oxygen extraction by the tissues– Best obtained from CVL: SC or IJ
• Lactate clearance: indication of anaerobic metabolism– >10% – Follow trends

64
Adrenal Insufficiency• Common occurrence in sepsis
– Use of Etomidate for intubation– Chronic steroid use
• 2 forms of insufficiency– Absolute: random cortisol <10– Relative: ∆ <9
• Tx: Hydrocortisone– Load: 100mg/m2
– Maintenance: 25mg/m2 Q6 x 7 days

65
Treatment: Steroids
• No pediatric study• Adult studies – hydrocortisone controversy over
28-day mortality• International guidelines for management of
severe sepsis & septic shock: Surviving Sepsis Campaign
• http://www.learnicu.org/SiteCollectionDocuments/GuidelineHemodynamicSupport.pdf

66
Summary• Shock is a dynamic & unstable physiologic state
that results in inadequate tissue perfusion– High morbidity and mortality
• Tachycardia is the early sign• Hypotension is a very late sign• Early & aggressive treatment during the “golden
hour” improves outcomes

References1. Fleegler, E. and M. Kleinman. Guidelines for pediatric advanced life support.
Uptodate.com, last updated Oct 14, 2009.2. Carcillo, JA et al. Goal-directed management of pediatric shock in the
emergency department. Clinical Pediatric Emergency Medicine: Vol 8; 3; 165-175.
3. Dellinger, RP et al. Surviving Sepsis Campaign: international guidelines for management of severe sepsis and septic shock: 2008. Intensive Care Medicine: Vol 34; 1; 17-60.
4. Han, YY et al. Early reversal of pediatric-neonatal septic shock by community physicians is associated with improved outcome. Pediatrics: Vol 112; 4; 793-799.
5. McKiernan, CA and SA Lieberman. Circulatory Shock in Children. Pediatrics in Review 2005; 26; 451-460.
6. Pomerantz, W. and M. Roback. Physiology and classification of shock in children. Uptodate.com, last updated Aug 21, 2007.
7. Waltzman, M. Initial management of shock in children. Uptodate.com, last updated May 11, 2010.