
Abbreviations - Brands Delmar - Cengage Learning · Abbreviations A ABN Advance Beneficiary Notice...
21
Abbreviations A ABN Advance Beneficiary Notice ADA American Disabilities Act AFDC Aid to Families with Dependent Children AHA American Hospital Association AHIMA American Health Information Management Association AHFS American Hospital Formulary Service AMA American Medical Association APC Ambulatory payment classification ASC Ambulatory Surgical Center B BC Blue Cross BCAC Beneficiary Counseling and Assistance Coordinator BCBS Blue Cross/Blue Shield BCBSA Blue Cross and Blue Shield Association BRAC Base Realignment and Closure BS Blue Shield BSR Beneficiary Services Representative C Ca Cancer or carcinoma CAT Computerized axial tomography CCI Correct Coding Initiative CCS Certified Coding Specialist CF Conversion factor CHAMPVA Civilian Health and Medical Program of Veterans Affairs CIM Coverage Issues Manual CLIA Clinical Laboratory Improvement Act CMP Competitive medical plan CMS Centers for Medicare and Medicaid Services CMS-1500 Insurance claim, developed by the National Uniform Claims Committee (NUCC), for use by noninstitutional providers and suppliers to bill third-party payers CMS-1450 also known as the UB-92; insurance claim, developed by the National Uniform Billing Committee (NUBC), for use by institutional and other selected providers to bill third- party payers COB Coordination of benefits COBRA Consolidated Omnibus Budget Reconciliation Act of 1985 CPC Certified professional coder CPT Current Procedural Terminology CRI CHAMPUS Reform Initiative CT Computed tomography D DEERS Defense Enrollment Eligibility Reporting System DME Durable medical equipment DMEPOS Durable Medical Equipment, Prosthetic and Orthotic Supplies DMERC Durable Medical Equipment Regional Carriers DoD Department of Defense DRG Diagnosis Related Groups E EDI Electronic data interchange EGHP Employer Group Health Plan E/M Evaluation and Management EMC Electronic media claim EOB Explanation of benefits EPO Exclusive provider organization EPSDT Early and Periodic Screening, Diagnoses, and Treatment ERISA Employee Retirement Income Security Act of 1974 ESRD End-stage renal disease F FECA Federal Employment Compensation Act FEHBP Federal Employee Health Benefits Program FELA Federal Employment Liability Act FEP Federal Employee Program FI Fiscal intermediary FMAP Federal Medical Assistance Percentage FPL Federal poverty level FR Federal Register G GEP General Enrollment Period GPCI Geographic practice cost index
Transcript of Abbreviations - Brands Delmar - Cengage Learning · Abbreviations A ABN Advance Beneficiary Notice...
AbbreviationsAABN Advance Beneficiary NoticeADA American Disabilities ActAFDC Aid to Families with Dependent ChildrenAHA American Hospital Association AHIMA American Health Information Management
AssociationAHFS American Hospital Formulary ServiceAMA American Medical AssociationAPC Ambulatory payment classificationASC Ambulatory Surgical Center
BBC Blue Cross BCAC Beneficiary Counseling and Assistance
CoordinatorBCBS Blue Cross/Blue Shield BCBSA Blue Cross and Blue Shield Association BRAC Base Realignment and ClosureBS Blue ShieldBSR Beneficiary Services Representative
CCa Cancer or carcinomaCAT Computerized axial tomographyCCI Correct Coding InitiativeCCS Certified Coding SpecialistCF Conversion factorCHAMPVA Civilian Health and Medical Program of
Veterans AffairsCIM Coverage Issues ManualCLIA Clinical Laboratory Improvement ActCMP Competitive medical planCMS Centers for Medicare and Medicaid ServicesCMS-1500 Insurance claim, developed by the National
Uniform Claims Committee (NUCC), for useby noninstitutional providers and suppliers tobill third-party payers
CMS-1450 also known as the UB-92; insurance claim,developed by the National Uniform BillingCommittee (NUBC), for use by institutionaland other selected providers to bill third-party payers
COB Coordination of benefits
COBRA Consolidated Omnibus Budget ReconciliationAct of 1985
CPC Certified professional coderCPT Current Procedural TerminologyCRI CHAMPUS Reform InitiativeCT Computed tomography
DDEERS Defense Enrollment Eligibility Reporting
SystemDME Durable medical equipmentDMEPOS Durable Medical Equipment, Prosthetic and
Orthotic SuppliesDMERC Durable Medical Equipment Regional
CarriersDoD Department of DefenseDRG Diagnosis Related Groups
EEDI Electronic data interchangeEGHP Employer Group Health PlanE/M Evaluation and ManagementEMC Electronic media claimEOB Explanation of benefitsEPO Exclusive provider organizationEPSDT Early and Periodic Screening, Diagnoses,
and Treatment ERISA Employee Retirement Income Security Act
of 1974ESRD End-stage renal disease
FFECA Federal Employment Compensation Act FEHBP Federal Employee Health Benefits Program FELA Federal Employment Liability Act FEP Federal Employee ProgramFI Fiscal intermediaryFMAP Federal Medical Assistance PercentageFPL Federal poverty levelFR Federal Register
GGEP General Enrollment PeriodGPCI Geographic practice cost index

GPWW Group practice without wallsGRP# Group practice identification number
HHA Health Affairs HCF Health Care FinderHCFA Health Care Financing AdministrationHCPCS Healthcare Common Procedure Coding
SystemHEDIS Health Plan Employer Data and Information
SetHIPAA Health Insurance Portability and
Accountability Act of 1996HMO Health Maintenance OrganizationHMO Act Health Maintenance Organization
of 1973 Assistance Act of 1973HPSA Health Personnel Shortage Area
IICD International Classification of DiseasesICD-9-CM International Classification of Diseases–9th
Revision–Clinical ModificationIEP Initial Enrollment PeriodIPA Individual practice associationIPA Independent practice associationIPO Integrated provider organization
JJCAHO Joint Commission on Accreditation of
Healthcare Organizations
LLA Lead AgentLC Limiting chargeLHWCA Longshore and Harbor Workers’
Compensation ActLLC Limited license practitionersLMC Local Medicare Carrier
MMCM Medicare Carriers ManualMCO Managed Care OrganizationMFN Most favored nationMHSS Military Health Services SystemMM Major MedicalMN Medically needy MRI Magnetic resonance imagingMSA Medical savings accountMSDS Material Safety Data SheetMSN Medicare Summary NoticeMSO Management service organizationMSP Medicare Supplemental Plan MTF Military treatment facility
NNAS Nonavailability statementNCHS National Center for Health StatisticsNCQA National Committee for Quality Assurance NEC Not elsewhere classifiableNMOP National Mail Order PharmacyNonPAR Nonparticipating providerNP Nurse PractitionerNPI National Provider Identifier
OOBRA Omnibus Budget Reconciliation Act of 1981OCR Optical character reader
OHI Other health insuranceOMP Office of Personnel ManagementOPAP Outpatient Pretreatment Authorization Plan ORIF Open reduction with internal fixationOSHA Occupational Safety and Health
Administration
PPA Physician AssistantPAR Participating providerPAYERID Payer identification number (now known
as PlanID)PCM Primary care managerPCP Primary care providerPFFS Private fee-for-service planPFPWD Program for Persons with Disabilities PFS Physician Fee SchedulePIN Provider identification numberPlanID National health plan identification numberPMO Program Management OrganizationPOS Place of servicePOS Point-of-service planPPA Preferred provider arrangementPPN Preferred provider networkPPO Preferred provider organizationPSO Provider-sponsored organization
QQDWI Qualified Disabled and Working Individual QI Qualifying IndividualQMB Qualified Medicare Beneficiary
RRBRVS Resource-Based Relative Value Scale RVU Relative value units
SSCHIP State Children’s Health Insurance Program SLMB Specified Low-income Medicare
BeneficiarySOAP Subjective, Objective, Assessment, PlanSSA Social Security AdministrationSSI Supplemental Security IncomeSSN Social Security NumberSSO Second surgical opinion
TTANF Temporary Assistance for Needy Families TEFRA Tax Equity and Fiscal Responsibility Act of
1982TMA TRICARE Management ActivityTOS Type of serviceTPA Third-party administrator TPR TRICARE Prime RemoteTSC TRICARE Service Center
UUCR Usual, Customary, and ReasonableUPIN Unique Provider Identification Number
VVA Veterans Administration

Common Medical TerminologyPrefixes, Suffixes, and
Combining Formsa-, an- no; notab- away fromabdomin- abdomenacr- extremities; top ad- toward -ad toward adip- fat -al pertaining to angi- vessel ankyl- crooked; bent anti- against arthr- joint -asis, -esis, -iasis, condition
-isis, -sisbi- two blephar- eyelid brachy- short brady- slow bronch- bronchial tube cardi- heart cephal- head cervic- neck; cervix colp-, kolp- vagina contra- against; oppositecrani- skull cry- cold cyan- blue dacry- tear dactyl- fingers; toes de- lack of; down demi- half derm-, dermat- skin
dextr- right di- two dis- separation -dynia pain dys- bad; painful-ectomy excision; removal -emesis vomiting-emia blood condition en- in; within end-, endo- in; within epi- above; upon erythr- red -esis condition -esthesia nervous sensationeti- cause ex- out; away from extra- outside fibr- fiber fore- before galact-, lact- milk gaster-, gastr- stomach genit- genitals gloss- tonguegluc-, glyc- sugar, glucose -gram record -graph instrument for reading -graphy process of recording gyn-, gyne-, gynec- women; female hem-, hema-, hemat- blood hemi- half hepat- liver hyp-, hyph- below; under

hyper- above; excessive hyster- uterus; womb-ia, -iasis condition -ic pertaining to ileo- ileum (small intestine)ilio- ilium (hip bone)in- in; into; not infra- within; into inter- between intra-, intro- within; into ipsi- same -isis condition -itis inflammation juxta- near laryng- larynx (voice box)later- side leuk- white lingu- tongue lip- fat; lipid -lith stone -lysis breakdownmal- bad -mania obsessive preoccupation med-, medi- middle mega-, megal- large melan- black meta- change; beyond metr-, metra- uterus; measure mon- one; single musculo-, my- muscle myel- spinal cord; bone marrownas- nose necr- death neo- new nephr-, nephra- kidney non- not; nonorm- rule; orderob- obstetricsoculo-, optico-, opto- eye-oma tumor; massomphal- umbilicus (navel) onych- nail oo-, ovi-, ovo- egg oophor-, oophoron- ovary -osis condition—usually abnormaloste- bone-ostomosis, -ostomy, new opening
-stomosis, -stomyot- ear-otomy incision-ous pertaining topach-, pachy- heavy; thickpan- allpara-, -para near; besidespath-, -pathic, -pathy diseaseper- through
peri- surrounding-pexy fixationpharyng- throat (pharynx)phleb- vein-phobia fear-plegia paralysispleur- pleurapneum-, pneumat- lung; air-poiesis, -poietic formationpoly- many; muchpost- after; behindposter- back; behindpro- before; forwardpseud- falsepsych- mindpyelo- renal pelvisre- back; againren- kidneyretr- behind; backrhe-, -rrhea flowrhin- nose-rrhage, -rhagia bursting forth of blood-rrhaphy suturesalping- fallopian tube; auditory tubescirrh- hard-sclerosis hardening-scope instrument for visual
examination-scopy visual examinationsemi- halfsoma-, somat- bodysphygm- pulsesplen- spleenspondyl- vertebrasten- narrownesssteth- chestsub- belowsuper- above, superiorsupra- above, uppertachy- fasttel-, tele- completetend-, ten- tendonthorac-, thoraci- chest; pleural cavitythromb- clot-tomy process of cuttingtrans- acrosstrich-, trichi- hairtympan- tympanic membraneultra- beyond; excessuni- oneureter- ureterurethr- urethra-uria urinationvas- vessel; ductven- veinvesic- urinary bladder

Web Sites
C H A P T E R 1
CMS http://cms.hhs.govAAMA http://www.aama-ntl.orgAHIMA http://www.ahima.orgAAPC http://www.aapcnatl.orgACAP http://www.claims.org
C H A P T E R 2
Disability insurance http://www.edd.ca.gov
C H A P T E R 3
Kaiser Permanente http://www.kaiserpermanente.orgMedical Data International http://www.medicaldata.comNCQA–Report Card http://hprc.ncqa.orgHealthEast IDS http://www.healtheast.orgNCQA http://www.ncqa.orgJCAHO http://www.jcaho.org
C H A P T E R 4
Government regulators http://www.ambest.com
C H A P T E R 5
Federal Register http://www.archives.govCMS press releases http://cms.hhs.govTrailblazer Health Enterprises http://www.trailblazerhealth.com
CodeCorrect http://www.codecorrect.comState departments of health http://www.cdc.govCMS listservs http://www.cms.hhs.gov/medlearn/listserv.aspMedicare Part-B listserv http://lyris.ucg.com/cgi-bin/listserv/listserv.pl/partb-lMedicare training http://www.cms.hhs.gov/medlearnCMS/HIPAA http://www.cms.gov/hipaaOIG Fraud Prevention & Detection http://oig.hhs.govCCI Edits Manual from NTIS http://www.ntis.govAdminaStar Federal, Inc. http://www.adminastar.comMedicare’s National CCI Edits http://www.cms.hhs.gov/medlearn/ncci.aspCCI edits (private vendor software) http://www.codecorrect.comEncoderPro software http://www.ingenixonline.comANSI ASC X12N 837 implementation
guides http://www.wpc-edi.com/hipaa/Retail pharmacy standards http://www.ncpdp.orgCMS Standard EDI Enrollment Form http://cms.hhs.govAdministrative Simplification (HIPAA) http://aspe.hhs.govHHS Office for Civil Rights http://www.hhs.gov/ocr/hipaaBusiness associate contract provisions http://www.hss.gov/ocr/hipaa/contractprov.html
C H A P T E R 6
Delmar Learning http://www.delmarhealthcare.comICD-9-CM Updates http://www.cdc.gov/nchs/icd9.htmICD-9-CM on CD-ROM http://bookstore.gpo.govNational Uniform Claim Committee http://www.nucc.orgNational Uniform Billing Committee http://www.nubc.orgASC X12 (HIPAA Administrative
Simplification) http://www.x12.orgFederal Register http://www.archives.govICD-9-CM and ICD-10-CM
development (NCHS) http://www.cdc.gov/nchs/icd9.htmICD-10-PCS development (NCVHS) http://www.cms.hhs.gov/paymentsystems/icd9/
icd10.aspICD-10 development (WHO) http://www.who.intCoding Updates (Medicode) http://www.ingenixonline.com
C H A P T E R 7
CPT Coding Manual (Delmar Learning) http://www.delmarhealthcare.comCPT Coding Manual (AMA) http://www.ama-assn.orgE/M Documentation Guidelines http://cms.hhs.gov/medicareSpecialty exam scoresheets http://www.hgsa.comE/M Coding Tools http://www.donself.comFamily Practice Management newsletter http://www.aafp.org

C H A P T E R 8
HCPCS information http://cms.hhs.gov/medicare/hcpcs/default.aspMedicare Carrier Manual (MCM) http://cms.hhs.gov/manuals
C H A P T E R 9
Coverage Issues Manual (CIM) and Medicare Carriers Manual (MCM) http://cms.hhs.gov/manuals/
C H A P T E R 1 0
No Web sites
C H A P T E R 1 1
No Web sites
C H A P T E R 1 2
No Web sites
C H A P T E R 1 3
BCBS health care news http://www.bcbshealthissues.com
C H A P T E R 1 4
Medicare physician fee schedules http://cms.hhs.gov/physicians/pfs/RBRVS information http://www.rbrvs.comMedicare consumer information http://www.medicare.govMedicare downloadable files http://cms.hhs.gov/medicareIntermediary-Carrier Directory http://cms.hhs.gov/manuals/
C H A P T E R 1 5
Medicaid publications http://cms.hhs.gov/publicationsState Medicaid toll-free numbers http://cms.hhs.gov/medicaid/tollfree.asp
C H A P T E R 1 6
TRICARE manuals http://www.tricare.osd.milCHAMPVA http://www.va.gov/hacTRICARE Dental Program http://www.ucci.comTRICARE Pharmacy Program http://www.tricare.osd.mil/pharmacyTRICARE Supplemental Plan http://www.tricare.osd.mil/supplementalinsurance/
plans.cfm

C H A P T E R 1 7
US Federal Mine Safety laws http://www.msha.govOSHA http://www.osha.govFederal workers’ compensation programs http://www.dol.gov/dol/topic/workcomp/index.htmState workers’ compensation Web sites http://www.dol.gov/esa/regs/compliance/owcp/wc.htm
UB-92
I N T R O D U C T I O N
This appendix provides an introduction to the use of the UB-92 (UniformBill, implemented in 1992) claim for institutional services (e.g., hospitalsand skilled nursing facilities).
U B - 9 2
The UB-92 claim contains data entry blocks called form locators (FLs) thatare similar to the CMS-1500 claim blocks used to input information aboutprocedures or services provided to a patient. While some institutions actu-ally complete the UB-92 claim (Figure IX-1) and submit it to third-party pay-ers for reimbursement, most perform data entry of UB-92 information usingcommercial software (Figure IX-2). What this means is most institutions donot actually complete a UB-92 claim for submission to a payer (unlikeproviders who usually complete the CMS-1500 claim either manually or on-screen using a software package). Instead, personnel who render servicesto institutional patients (e.g., nursing, laboratory or radiology) enter UB-92data into the commercial software product. The data resides in the patient’scomputerized account, and upon discharge of the patient from the institu-tion, the data is verified by billing office personnel and transmitted elec-tronically either directly to the third-party payer or (more likely) to a clear-inghouse that processes electronic claims by editing and validating them toensure that they are error-free, reformatting them to the specifications of thepayer, and submitting them electronically to the appropriate payer.
EXAMPLE: During an inpatient admission, the attending physicianwrites an order in the patient’s record for a blood glucose level to be per-formed by the laboratory. The patient’s nurse processes the order by con-tacting the laboratory (e.g., telephone or computer message), which sendsa technician to the patient’s room to perform a venipuncture (blood draw,or withdrawing blood from the patient’s arm using a syringe). The bloodspecimen is transported to the laboratory by the technician where the blood
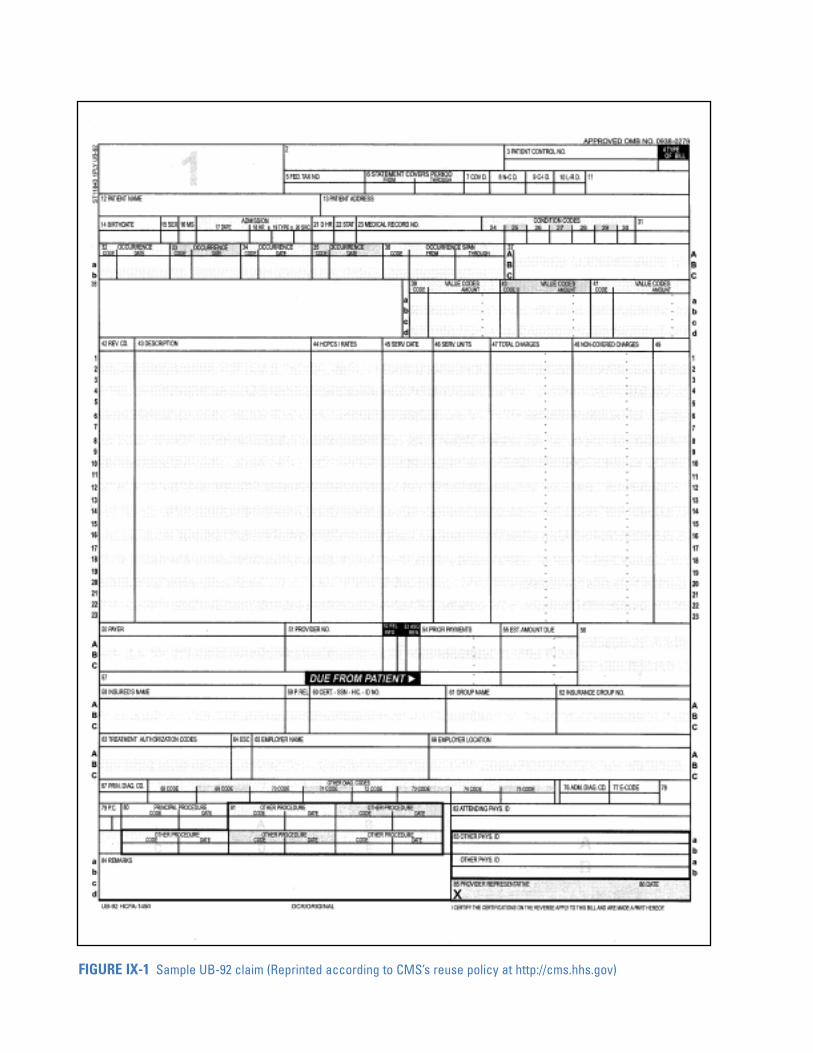
FIGURE IX-1 Sample UB-92 claim (Reprinted according to CMS’s reuse policy at http://cms.hhs.gov)

glucose test is completed. The technician entersthe results into the patient record information tech-nology (IT) system using a computer terminal. Atthe same time, the UB-92 data elements are inputinto the patient account IT system using a comput-er terminal. This data resides in the patient’s com-puterized account until it is verified by the billingoffice (at patient discharge) and is then transmittedto a clearinghouse that processes the claim andsubmits it to the third-party payer. The clearing-house also uses the network to send an acknowl-edgment to the institution upon receipt of the sub-mitted claim. ●
UB-92 Claim Developmentand Implementation
Institutional and other selected providers submitUB-92 (CMS-1450) claim data (Figure IX-2) to pay-
ers for reimbursement of patient services. TheNational Uniform Billing Committee (NUBC) isresponsible for developing data elements reportedon the UB-92 in cooperation with State UniformBilling Committees (SUBCs).
NOTE: UB-92 claim data for Medicare Part Areimbursement is submitted to fiscal intermedi-aries (FIs), which are private insurance companiescontracted by CMS to serve as the financial agentbetween providers and the federal government forthe purpose of handling Medicare Part A reim-bursement. The FI processes payments for hospi-tals, skilled nursing facilities, home health and hos-pice agencies, dialysis facilities, rehabilitation facil-ities, and rural health clinics. ●
HINT: The role of the FI is similar to that ofthe Medicare carrier associated with MedicarePart B claims processing. ●
FIGURE IX-2 Sample data entry screen using UB-92 electronic data interchange software (Permission to reprintgranted by Remora Software, Inc.)

N a t i o n a l U n i f o r m B i l l i n gC o m m i t t e e ( N U B C )
Like the role of the National Uniform ClaimsCommittee (NUCC) in the development of the CMS-1500 claim, the National Uniform BillingCommittee (NUBC) is responsible for identifyingand revising data elements (information enteredinto UB-92 form locators or submitted by institu-tions using electronic data interchange), and it orig-inally designed the first uniform bill (called theUB-82 because of its 1982 implementation date).The current claim is called the UB-92 because itwas implemented in 1992.
The NUBC was created by the AmericanHospital Association (AHA) in 1975 and is repre-sented by major national provider (e.g., AHA StateHospital Association Representatives) and payer(e.g., Blue Cross and Blue Shield Association)organizations. The intent was to develop a singlebilling form and standard data set that could beused by all institutional providers and payers forhealth care claims processing. In 1982, the NUBCvoted to accept the UB-82 and its data set (a com-pilation of data elements that are reported on theuniform bill) for implementation as a national uni-form bill. Once the UB-82 was adopted, the focusof the NUBC shifted to the state level, and a StateUniform Billing Committee (SUBC) was created ineach state to handle implementation and distribu-tion of state-specific UB-82 manuals (that con-tained national guidelines along with unique statebilling requirements).
When the NUBC established the UB-82 dataset design and specifications, it also implementedan evaluation process through 1990 to determinewhether the UB-82 data set was appropriate forthird-party payer claims processing. The NUBCsurveyed SUBCs to obtain suggestions for improv-ing the design of the UB-82, and the UB-92 wasimplemented in 1992 to incorporate the best of theUB-82 with data set design improvements (e.g.,providers no longer need to include as manyattachments to UB-92 claims submitted).
Data Specifications for the UB-92
When reviewing data specifications for the UB-92,the NUBC balances the payers’ need to collect
information against the burden of providers toreport that information. In addition, the adminis-trative simplification principles required of theHealth Insurance Portability and AccountabilityAct of 1996 (HIPAA) are applied when developingdata elements. Each data element required forreporting purposes is assigned to a unique UB-92form locator (FL), which is the designated spaceon the claim identified by a unique number andtitle, such as the patient name in FL12 (Refer toFigure IX-1).
UB-92 Claim Submission
Whether completed manually (Figure IX-1) orusing on-screen software (Figure IX-2), the UB-92claim contains 86 form locators (Table IX-1). Thedata is entered according to third-party payerguidelines that contain instructions for completingthe UB-92.
Providers that submit the UB-92 claim (orUB-92 data elements in EDI format) include:
● ambulance companies.
● ambulatory surgery centers (ASC).
● home health care agencies (HHA).
● hospice organizations.
● hospitals (emergency department, inpatient,and outpatient services).
● psychiatric drug/alcohol treatment facilities(inpatient and outpatient services).
● skilled nursing facilities (SNFs).
● subacute facilities.
● stand-alone clinical/laboratory facilities.
● walk-in clinics.
The UB-92 (CMS-1450) and its data elementsserve the needs of many third-party payers, andwhile some payers do not collect certain data ele-ments, it is important to capture all NUBC-approved data elements for audit trail purposes. Inaddition, NUBC-approved data elements arereported by facilities that have established coordi-nation of benefits agreements with the payers.
NOTE: All Medicare claims are currently sub-mitted either manually on the UB-92 paper claim,or processed according to electronic data inter-change (EDI) guidelines. Form locator definitions

TABLE IX-1 UB-92 form locators and brief description of information to be entered
FORM BRIEF DESCRIPTION OF FORM BRIEF DESCRIPTION OF LOCATOR INFORMATION TO BE LOCATOR INFORMATION TO BE
ENTERED ON THE UB-92 ENTERED ON THE UB-92
1 Provider Name, Address & Telephone # 46 Units of Service
2 Unlabeled Field - State Use 47 Total Charges (by Revenue Code Category)
3 Patient Control Number (Account Number) 48 Non-Covered Charges
4 Type of Bill 49 Unlabeled Field - National Use
5 Federal Tax Number 50A-C Payer Identification
6 Statement Covers Period 51A-C Provider Number
7 Covered Days 52A-C Release of Information Certification Indicator
8 Non-Covered Days 53A-C Assignment of Benefits Certification Indicator
9 Coinsurance Days 54A-C, P Prior Payments - Payers and Patient
10 Lifetime Reserve Days 55A-C, P Estimated Amount Due
11 Unlabeled Field - State Use 56 DRG Number and Grouper ID
12 Patient Name 57 Unlabeled Field - National Use
13 Patient Address 58A-C Insured’s Name
14 Patient Birthdate 59A-C Patient’s Relationship to Insured
15 Patient Sex 60A-C Health Insurance Claim Identification Number
16 Patient Marital Status 61A-C Insured Group Name
17 Admission Date 62A-C Insurance Group Number
18 Admission Hour 63A-C Treatment Authorization Code
19 Type of Admission 64A-C Employment Status Code
20 Source of Admission 65A-C Employer Name
21 Discharge Hour 66A-C Employer Location
22 Patient Status 67 Principal Diagnosis Code
23 Medical/Health Record Number 68-75 Other Diagnosis Codes
24-30 Condition Codes 76 Admitting Diagnosis
31 Unlabeled Field - National Use 77 External Cause of Injury Code (E-Code)
32-35a,b Occurrence Codes and Dates 78 Principal Diagnosis Code
36a,b Occurrence Span Codes and Dates 79 Procedure Coding Method Used
37 Internal Control Number (ICN) 80 Principal Procedure Code and Date
38 Responsible Party Name and Address 81A-E Other Procedure Codes and Dates
39-41a-d Value Codes and Amounts 82a-b Attending Physician ID
42 Revenue Code 83a-b Other Physician ID
43 Revenue Description 84 Remarks
44 HCPCS/Rates 85 Provider Representative Signature
45 Service Date 86 Date Bill Submitted (Reprinted according to content reuse policy at http://cms.hhs.gov)
are identical and in some situations, the electronicclaim contains more characters than the corre-sponding item on the paper form. ●
U B - 0 2
The National Uniform Billing Committee (NUBC)is working on the proposed UB-02, which isscheduled to replace the UB-92. (The implementa-tion date has not yet been announced.) Revisions
will emphasize clarification of definitions for dataelements and codes to eliminate amibiguity and tocreate consistency. The UB-02 will also addressemergency department (ED) coding and data col-lection issues to respond to state public healthreporting systems. The NUBC continues to empha-size the need to stay involved so that data sourcescan continue to support public health data report-ing needs.

Dental Claims Processing
I N T R O D U C T I O N
Dental benefits programs offer a variety of options in the form of either fee-for-service or managed care plans that reimburse a portion of a patient’sdental expenses and may exclude certain treatments (e.g., dental sealants).It is, therefore, important for the insurance specialist to become familiarwith the specifics of dental plans in which the dental professional partici-pates. It is equally important to become familiar with dental terminology(Table X-1).
D E N TA L C L A I M S P R O C E S S I N G
Dental claims are submitted on the American Dental Association (ADA)approved claim and instructions (Table X-2) should be carefully followed.Dental offices also have the option of submitting electronic claims accord-ing to HIPAA’s electronic transaction standard, ASC Xl2N 837v.4010–Health Care Claim: Dental.
Dental treatment is reported using codes assigned from the CurrentDental Terminology, 4th Edition (CDT-4). CDT-4 is published by theAmerican Dental Association (ADA), which ensures that codes are:
● created according to a standard format.
● at an appropriate level of specificity.
● uniformly applied to dental treatment.
● used to report dental procedures.
The American Dental Association periodically reviews and revises CDT-4 toupdate codes according to recognized changes in dental procedures.Published revisions are implemented biannually, at the beginning of odd-numbered years. (CDT-4 codes were reported effective January 1, 2003.)CDT-4 contains the following features:
● codes and descriptions
● a section on implant-supported prosthetics

● glossaries of dental and dental benefit termi-nology
● the new ADA claim
● an introduction to the SystematizedNomenclature of Dentistry (SNODENT).SNODENT contains standard terms to
describe dental disease, captures clinicaldetail and patient characteristics, and allowsfor the analysis of patient care services andoutcomes.
NOTE: CDT-5 is being developed for imple-mentation in 2004. ●
TABLE X-1 Glossary of common dental terms
DENTAL TERM DEFINITION
American Academy of Periodontology (AAP) dedicated to advancing the art and science of periodontics andimproving the periodontal health of the public
American Academy of Pediatric Dentistry dedicated to improving and maintaining the oral health of infants, (AAPD) children, adolescents, and persons with special health care needs
Alliance for the Best Clinical organization that encourages development of evidence-based Practices in Dentistry (ABCPD) prevention and treatment protocols through the process of organ-
izing focused seminars
abscess acute or chronic, localized inflammation associated with tissuedestruction
American Dental Association (ADA) promotes public health through commitment of member dentists toprovide high quality oral health care and promotes accessible oralhealth care
Academy of General Dentistry (AGD) serves needs and represents interests of general dentists
amalgam alloy used in direct dental restorations; also called a silver filling
attrition normal wearing away of the surface of a tooth from chewing
baby bottle tooth decay severe decay in baby teeth due to sleeping with a bottle of milk orjuice; natural sugars from drinks combine with bacteria in themouth to produce acid that decays teeth
bitewing radiograph X-rays of top and bottom molars and premolars
bruxism involuntary clenching or grinding of teeth
calculus hard deposit of mineralized material that adheres to teeth; alsocalled tarter or calcified plaque
caries tooth decay
crown artificial covering of a tooth with metal, porcelain, or porcelainfused to metal
deciduous teeth baby teeth or primary teeth
endentulous having no teeth
(continues)

TABLE X-1 (continued)
DENTAL TERM DEFINITION
endodontics dental specialty concerned with treatment of the root and nerve ofa tooth
fluoride chemical compound that prevents cavities and makes tooth sur-face stronger
gingivitis inflammation of gums surrounding teeth, caused by buildup ofplaque or food
gum disease see periodontitis
halitosis bad breath
malocclusion improper alignment of biting or chewing surfaces of upper andlower teeth
orthodontics dental specialty concerned with straightening or moving mis-aligned teeth and/or jaws with braces and/or surgery
Prevent Abuse and Neglect through educational program that educates oral health professionals about Dental Awareness (PANDA) child abuse and helps them learn how to diagnose and report
potential abuse situations to appropriate authorities
panoramic radiograph single, large X-ray of jaws taken by a machine that rotates aroundthe head
pedodontics dental specialty concerned with treatment of children; also calledpediatric dentistry
periodontics dental specialty concerned with treatment of gums, tissue, andbone that supports the teeth
periodontitis inflammation and loss of connective tissue of the supporting orsurrounding structure of the teeth; also called gum disease
plaque bacteria containing substance that collects on the surface ofteeth, which can cause decay and gum irritation when notremoved by daily brushing and flossing
prophylaxis professional cleaning to remove plaque, calculus, and stains
prosthodontics dental specialty concerned with restoration and/or replacement ofmissing teeth with artificial materials
radiograph X-ray
scaling removal of plaque, calculus, and stains from teeth
sealant thin plastic material used to cover biting surface of a child's tooth
supernumerary tooth extra tooth
tarter see calculus

TABLE X-2 Instructions for completing ADA Dental Claim, 2002
BLOCK INSTRUCTIONS
Header Information
Block 1 Enter an X in the appropriate box.Select the Statement of Actual Services to obtain reimbursement for services provided. Select
the Request for Predetermination/ Preauthorization to obtain preapproval of dental services. Select the EPSDT/Title XIX if the patient is covered by Medicaid’s Early and Periodic Screening, Diagnosis, and Treatment program for persons under age 21.
Block 2 Enter the predetermination or preauthorization number assigned by the payer, if applicable. Otherwise, leave blank.
Primary Payer Information
Block 3 Enter the primary payer’s name, address, city, state, and zip code.
Other Coverage NOTE: Always complete Block 4. Complete Blocks 5-11 only if the patient has a secondary dental plan. ●
Block 4 Enter an X in the NO box if the patient is not covered by another dental insurance plan, and go to Block 12. Enter an X in the YES box if the patient is covered by another dental insurance plan, and complete Blocks 5-11.
Remember! Complete Blocks 5-11 only if the patient has a secondary dental plan. Otherwise, leave Blocks 5-11 blank.
Block 5 If the patient has secondary dental plan coverage, enter the complete name (last, first, middle initial, suffix) of the individual named as policyholder on the secondary plan.
Block 6 If the patient has secondary dental plan coverage, enter the secondary policyholder’s date of birth as MMDDYYYY (without spaces).
Block 7 If the patient has secondary dental plan coverage, enter an X in the appropriate box to indicate the secondary policyholder’s gender.
Block 8 If the patient has secondary dental plan coverage, enter the secondary policyholder’s social se-curity number (SSN) or dental plan identification number, whichever appears on the dental plan card.
Block 9 If the patient has secondary dental plan coverage, enter the secondary policyholder’s dental plan number and group number (e.g., 123456 001).
Block 10 If the patient has secondary dental plan coverage, enter an X in the appropriate box to indicate the relationship of the primary policyholder to the secondary policyholder.
Block 11 If the patient has secondary dental plan coverage, enter the dental plan’s name, address, city, state, and zip code.
Primary Subscriber Information
Block 12 Enter the primary policyholder’s complete name, address, city, state, and zip code.
Block 13 Enter the primary policyholder’s date of birth as MMDDYYYY (without spaces).
Block 14 Enter an X in the appropriate box to indicate the primary policyholder’s gender.
Block 15 Enter the primary policyholder’s social security number (SSN) or dental plan identification number, whichever appears on the dental plan card.
(continues)
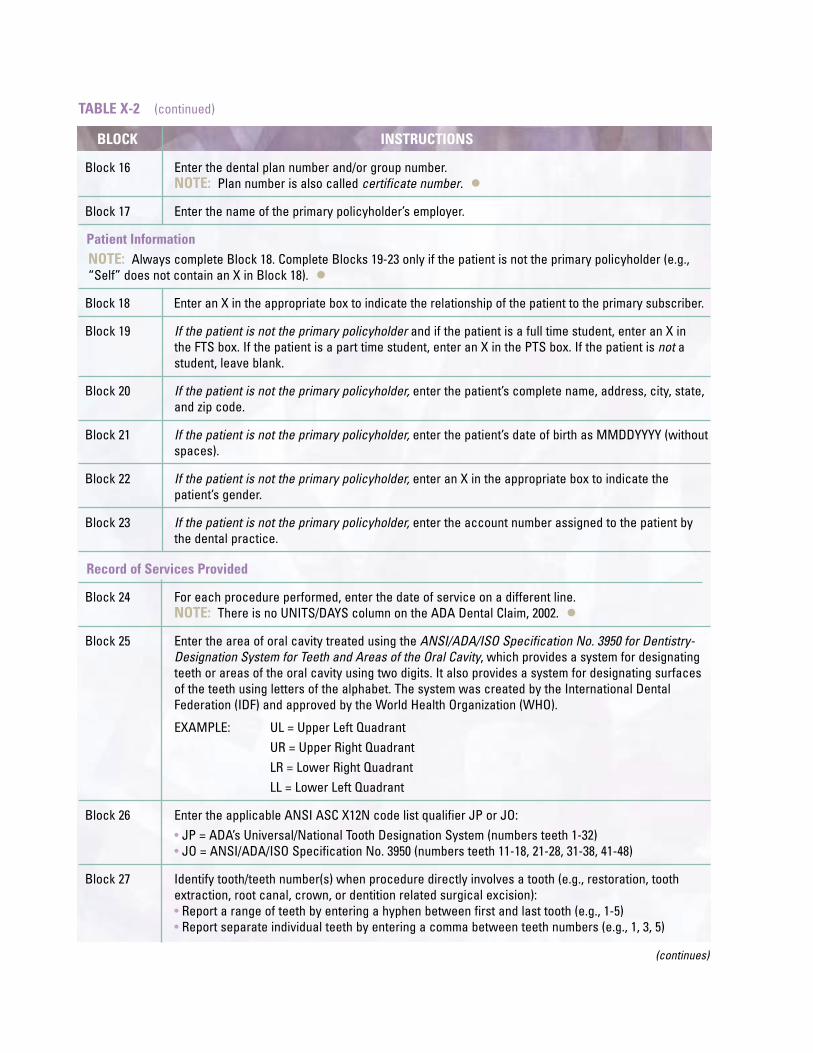
TABLE X-2 (continued)
BLOCK INSTRUCTIONS
Block 16 Enter the dental plan number and/or group number.NOTE: Plan number is also called certificate number. ●
Block 17 Enter the name of the primary policyholder’s employer.
Patient InformationNOTE: Always complete Block 18. Complete Blocks 19-23 only if the patient is not the primary policyholder (e.g., “Self” does not contain an X in Block 18). ●
Block 18 Enter an X in the appropriate box to indicate the relationship of the patient to the primary subscriber.
Block 19 If the patient is not the primary policyholder and if the patient is a full time student, enter an X in the FTS box. If the patient is a part time student, enter an X in the PTS box. If the patient is not astudent, leave blank.
Block 20 If the patient is not the primary policyholder, enter the patient’s complete name, address, city, state, and zip code.
Block 21 If the patient is not the primary policyholder, enter the patient’s date of birth as MMDDYYYY (without spaces).
Block 22 If the patient is not the primary policyholder, enter an X in the appropriate box to indicate the patient’s gender.
Block 23 If the patient is not the primary policyholder, enter the account number assigned to the patient by the dental practice.
Record of Services Provided
Block 24 For each procedure performed, enter the date of service on a different line.NOTE: There is no UNITS/DAYS column on the ADA Dental Claim, 2002. ●
Block 25 Enter the area of oral cavity treated using the ANSI/ADA/ISO Specification No. 3950 for Dentistry-Designation System for Teeth and Areas of the Oral Cavity, which provides a system for designatingteeth or areas of the oral cavity using two digits. It also provides a system for designating surfaces of the teeth using letters of the alphabet. The system was created by the International Dental Federation (IDF) and approved by the World Health Organization (WHO).
EXAMPLE: UL = Upper Left QuadrantUR = Upper Right QuadrantLR = Lower Right QuadrantLL = Lower Left Quadrant
Block 26 Enter the applicable ANSI ASC X12N code list qualifier JP or JO:• JP = ADA’s Universal/National Tooth Designation System (numbers teeth 1-32)• JO = ANSI/ADA/ISO Specification No. 3950 (numbers teeth 11-18, 21-28, 31-38, 41-48)
Block 27 Identify tooth/teeth number(s) when procedure directly involves a tooth (e.g., restoration, tooth extraction, root canal, crown, or dentition related surgical excision):• Report a range of teeth by entering a hyphen between first and last tooth (e.g., 1-5)• Report separate individual teeth by entering a comma between teeth numbers (e.g., 1, 3, 5)
(continues)

TABLE X-2 (continued)
BLOCK INSTRUCTIONS
NOTE: Use numerical identification (1-32) for permanent teeth and capital letter identification (A-T) for primary teeth. Leave blank if treatment of a specific tooth (e.g., oral examination) is not performed. For supernumerary tooth numbering, contact the dental plan. ●
Block 28 When procedure(s) directly involve one or more tooth surface(s), enter up to five of the following codes (without spaces):B = Buccal F = Facial M = MesialD = Distal L = Lingual O = Occlusal
Block 29 Enter the CDT procedure code for dental treatment provided.
Block 30 Enter terminology to describe the service provided.NOTE: If service is for a supernumerary tooth, enter the word “supernumerary” and includeinformation to identify the closest numbered tooth. ●
Block 31 Enter the fee charged for the procedure.
Block 32 Enter other fees (e.g., state taxes where applicable, fees imposed by regulatory agencies).
Block 33 Enter the total of all fees reported on the claim.
Missing Teeth Information
Block 34 Enter an X on each number that corresponds to a missing tooth.
Block 35 Enter additional applicable information (e.g., multiple supernumerary teeth).
Authorizations
Block 36 Obtain patient/guardian signature and date, which authorizes payment and release of information to dental plan.
Block 37 Obtain policyholder’s signature and date, which authorizes the dental plan to make payment directly to the provider (e.g., dentist).
Ancillary Claim/Treatment Information
Block 38 Enter an X in the appropriate box to indicate place of treatment.NOTE: ECF refers to extended care facility (e.g., nursing facility). ●
Block 39 Enter an X in the appropriate box if the claim has attached radiograph(s), oral image(s), and/or model(s). If nothing is attached to the claim, leave blank.
Block 40 Enter an X in the NO box if treatment is not for orthodontics, and go to Block 43. Enter an X in the YES box if treatment is for orthodontics, and complete Blocks 41 and 42.
Block 41 Enter the date appliance (e.g., braces) were placed as MMDDYYYY (without spaces). Leave blank if an X was entered in the NO box in Block 40.
Block 42 Enter a number that represents the remaining months of treatment (e.g., 26). Leave blank if an X was entered in the NO box in Block 40.
(continues)

TABLE X-2 (continued)
BLOCK INSTRUCTIONS
Block 43 Enter an X in the NO box if treatment is not for replacement of prosthesis, and go to Block 45. Enter an X in the YES box if treatment is for replacement of prosthesis, and complete Block 44.
Block 44 Enter the date the prior prosthesis was placed as MMDDYYYY (without spaces). Leave blank if an X was entered in the NO box in Block 43.
Block 45 Enter an X in the appropriate box, if applicable, and complete Blocks 46 and 47. Otherwise, leave blank.
Block 46 If an X was entered in a box in Block 47, enter the date of accident as MMDDYYYY (without spaces). Otherwise, leave blank.
Block 47 If an X was entered in the AUTO ACCIDENT box in Block 47, enter the state in which the accident occurred. Otherwise, leave blank.
Billing Dentist or Dental Entity
Remember! Complete Blocks 48-52 only if the provider is submitting a claim on behalf of the patient or policyholder.
Block 48 If the provider is submitting a claim on behalf of the patient or policyholder, enter the provider’s name, address, city, state, and zip code.
Block 49 If the provider is submitting a claim on behalf of the patient or policyholder, enter the provider’s identification number.NOTE: This is not the provider’s social security number or tax identification number. ●
Block 50 If the provider is submitting a claim on behalf of the patient or policyholder, enter the provider’s license number.
Block 51 If the provider is submitting a claim on behalf of the patient or policyholder, enter the provider’s social security number or tax identification number.
Block 52 If the provider is submitting a claim on behalf of the patient or policyholder, enter the provider’s telephone number.
Treating Dentist and Treatment Location Information
Block 53 Have the treating dentist provider sign and date the completed claim.NOTE: Check with the dental plan to determine if the signature can be typed or stamped, instead of signed by the provider. ●
Block 54 Enter the treating dentist’s identification number.
Block 55 Enter the treating dentist’s license number.
Block 56 Enter the treating dentist’s address, city, state, and zip code.
Block 57 Enter the treating dentist’s telephone number.
Block 58 Enter the code from the HIPAA Health Care EDI Provider Taxonomy Codes list that corresponds to the treating dentist’s specialty.NOTE: Go to http://www.wpc-edi.com/codes/codes.asp to obtain the current HIPAA Health Care EDI Provider Taxonomy Codes list (e.g., 1223G0001X General Practice). ●


















