
AAGLaagl.org/2012syllabus/PG105.pdf · PG 105 . Fundamentals of Laparoscopic & Robotic...
72
AAGL acknowledges that it has received support in part by educational grants and equipment (in-kind) from the following companies: Applied Medical Sponsored by AAGL Advancing Minimally Invasive Gynecology Worldwide Fundamentals of Laparoscopic & Robotic Hysterectomy: From Simple to Complex (Didactic) PROGRAM CHAIR Arnold P. Advincula, MD Ted Teh Min Lee, MD Richard B. Rosenfield, MD Stacey A. Schieb, MD
Transcript of AAGLaagl.org/2012syllabus/PG105.pdf · PG 105 . Fundamentals of Laparoscopic & Robotic...

AAGL acknowledges that it has received support in part by educational grants and equipment (in-kind) from the following companies:
Applied Medical
Sponsored by
AAGLAdvancing Minimally Invasive Gynecology Worldwide
Fundamentals of Laparoscopic & Robotic
Hysterectomy: From Simple to Complex
(Didactic)
PROGRAM CHAIR
Arnold P. Advincula, MD
Ted Teh Min Lee, MD Richard B. Rosenfi eld, MD Stacey A. Schieb, MD

Professional Education Information Target Audience Educational activities are developed to meet the needs of surgical gynecologists in practice and in training, as well as, other allied healthcare professionals in the field of gynecology. Accreditation AAGL is accredited by the Accreditation Council for Continuing Medical Education to provide continuing medical education for physicians. The AAGL designates this live activity for a maximum of 3.75 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity. DISCLOSURE OF RELEVANT FINANCIAL RELATIONSHIPS As a provider accredited by the Accreditation Council for Continuing Medical Education, AAGL must ensure balance, independence, and objectivity in all CME activities to promote improvements in health care and not proprietary interests of a commercial interest. The provider controls all decisions related to identification of CME needs, determination of educational objectives, selection and presentation of content, selection of all persons and organizations that will be in a position to control the content, selection of educational methods, and evaluation of the activity. Course chairs, planning committee members, presenters, authors, moderators, panel members, and others in a position to control the content of this activity are required to disclose relevant financial relationships with commercial interests related to the subject matter of this educational activity. Learners are able to assess the potential for commercial bias in information when complete disclosure, resolution of conflicts of interest, and acknowledgment of commercial support are provided prior to the activity. Informed learners are the final safeguards in assuring that a CME activity is independent from commercial support. We believe this mechanism contributes to the transparency and accountability of CME.
Table of Contents
Course Description ........................................................................................................................................ 1 Disclosure ...................................................................................................................................................... 3 Maximizing Outcomes and Minimizing Complications with Monopolar, Bipolar and Ultrasonic Devices A.P. Advincula .............................................................................................................................................. 5 A Primer on Pelvic and Retroperitoneal Anatomy: the Gynecologist’s Achilles Heel T. Lee ......................................................................................................................................................... 18 A Practical Surgical Approach to Laparoscopic Hysterectomy R.B. Rosenfield ........................................................................................................................................... 28 Utilizing Reduced and Single Port Techniques for Conventional Laparoscopic and Robotic Hysterectomy S.A. Scheib .................................................................................................................................................. 35 Surgical Roadmaps for the Complex Laparoscopic Hysterectomy T. Lee ......................................................................................................................................................... 40 Robotic Hysterectomy: a Systematic Approach in 3‐D A.P. Advincula ............................................................................................................................................ 47 Tips and Tricks for Tackling the Large Uterus during Laparoscopic Hysterectomy R.B. Rosenfield ........................................................................................................................................... 57 Dealing with Difficult Peritoneal Access, Obesity and Vaginal Cuff Issues S.A. Scheib .................................................................................................................................................. 61 Cultural and Linguistics Competency ......................................................................................................... 69

PG 105 Fundamentals of Laparoscopic & Robotic Hysterectomy:
from Simple to Complex (Didactic)
Arnold P. Advincula, Chair Faculty: Ted Teh Min Lee, Richard B. Rosenfield, Stacey A. Scheib
Course Description
This interactive surgical video-based course is designed for individuals interested in incorporating laparoscopic hysterectomy into their minimally invasive surgical armamentarium. Basic and advanced techniques will be discussed in order to allow novice as well as experienced gynecologic surgeons to tackle simple and complex hysterectomies. Both conventional and robot-assisted laparoscopic approaches will be discussed in the setting of traditional multi-port peritoneal access as well as reduced and single port laparoscopy. An emphasis on proper energy device usage, optimization of uterine manipulation, proper retroperitoneal dissection, and management of complications will be made. Tips and tricks for the large uterus as well as navigating pelvic adhesive disease will also be discussed.
Course Objectives At the conclusion of this activity, the participant will be able to: 1) Distinguish between optimal and suboptimal performance of colpotomy and vaginal cuff closure; 2) apply safe and efficient strategies for managing large uteri laparoscopically; 3) demonstrate proper dissection techniques for retroperitoneal exploration and ureterolysis; 4) analyze and compare various energy sources used in laparoscopic hysterectomy; 5) distinguish between conventional laparoscopic and robotic hysterectomy; and 6) apply multi-port as well as reduced and single port strategies for peritoneal access.
Course Outline 8:00 Welcome, Introductions and Course Overview A.P. Advincula 8:05 Maximizing Outcomes and Minimizing Complications with Monopolar, Bipolar
and Ultrasonic Devices A.P. Advincula 8:30 A Primer on Pelvic and Retroperitoneal Anatomy: the Gynecologist’s Achilles Heel T. Lee 8:55 A Practical Surgical Approach to Laparoscopic Hysterectomy R.B. Rosenfield 9:20 Utilizing Reduced and Single Port Techniques for Conventional Laparoscopic and
Robotic Hysterectomy S.A. Scheib 9:45 Questions & Answers All Faculty 9:55 Break 10:10 Surgical Roadmaps for the Complex Laparoscopic Hysterectomy T. Lee
1

10:35 Robotic Hysterectomy: a Systematic Approach in 3-D A.P. Advincula 11:00 Tips and Tricks for Tackling the Large Uterus during Laparoscopic Hysterectomy R.B. Rosenfield 11:25 Dealing with Difficult Peritoneal Access, Obesity and Vaginal Cuff Issues S.A. Scheib 11:50 Questions & Answers All Faculty 12:00 Course Evaluation
2

PLANNER DISCLOSURE The following members of AAGL have been involved in the educational planning of this workshop and have no conflict of interest to disclose (in alphabetical order by last name). Art Arellano, Professional Education Manager, AAGL* Viviane F. Connor Consultant: Conceptus Incorporated Frank D. Loffer, Executive Vice President/Medical Director, AAGL* Linda Michels, Executive Director, AAGL* Jonathan Solnik Other: Lecturer - Olympus, Lecturer - Karl Storz Endoscopy-America SCIENTIFIC PROGRAM COMMITTEE Arnold P. Advincula Consultant: CooperSurgical, Ethicon Women's Health & Urology, Intuitve Surgical Other: Royalties - CooperSurgical Linda Bradley Grants/Research Support: Elsevier Consultant: Bayer Healthcare Corp., Conceptus Incorporated, Ferring Pharmaceuticals Speaker's Bureau: Bayer Healthcare Corp., Conceptus Incorporated, Ferring Pharm Keith Isaacson Consultant: Karl Storz Endoscopy Rosanne M. Kho Other: Honorarium - Ethicon Endo-Surgery C.Y. Liu* Javier Magrina* Ceana H. Nezhat Consultant: Intuitve Surgical, Lumenis, Karl Storz Endoscopy-America Speaker's Bureau: Conceptus Incorporated, Ethicon Women's Health & Urology William H. Parker Grants/Research Support: Ethicon Women's Health & Urology Consultant: Ethicon Women's Health & Urology Craig J. Sobolewski Consultant: Covidien, CareFusion, TransEnterix Stock Shareholder: TransEnterix Speaker's Bureau: Covidien, Abbott Laboratories Other: Proctor - Intuitve Surgical FACULTY DISCLOSURE The following have agreed to provide verbal disclosure of their relationships prior to their presentations. They have also agreed to support their presentations and clinical recommendations with the “best available evidence” from medical literature (in alphabetical order by last name). Arnold P. Advincula Consultant: CooperSurgical, Ethicon Women's Health & Urology, Intuitve Surgical Other: Royalties – CooperSurgical Ted Lee Grants/Research Support: Ethicon Endo-Surgery Consultant: Ethicon Endo-Surgery, Gyrus ACMI (Olympus)
3

Richard B. Rosenfield Other: Cofounder - Surgiview Stacey A. Scheib Grants/Research Support: Intuitve Surgical Consultant: Covidien Nash S. Moawad* Asterisk (*) denotes no financial relationships to disclose.
4

Maximizing Outcomes & Minimizing Complications with Monopolar, Bipolar and Ultrasonic Devices
Arnold P. Advincula, MD, FACOG, FACS
Professor of Obstetrics & Gynecology
University of Central Florida College of Medicine
Director, Center for Specialized Gynecology
Director, Celebration Health Endometriosis Center
Director, AAGL/SRS MIS Fellowship
Florida Hospital ‐ Celebration Health
Disclosure
• Consultant: CooperSurgical, Ethicon Women's Health & Urology, IntuitveSurgical
• Other: Royalties CooperSurgical• Other: Royalties - CooperSurgical
Learning Objectives
• Understand the basic principles involved in today’s electrosurgery platforms.
• Discuss the issues & risks surrounding the use of monopolar and bipolar electrosurgical devices in p p gminimally invasive surgery.
• Review the rationale behind & evolution of both advanced bipolar thermal tissue fusion devices.
Thermocautery
5,000 year old technique.
Use of Energy to Heat a Metal Object
Properties of Electricity
• Atoms are the basic building blocks of all matter.
• Atoms are composed of – Neutrons,
– Protons (+) and
– Electrons (-)
Properties of Electricity
• Current flow occurs when electrons flow from one atom to the orbit of an adjacent atom.V lt i th f• Voltage is the force or push that provides electrons with the ability to travel from atom to atom.
• If electrons encounter resistance (impedance), heat can be produced.
• A completed circuitmust be present in order for electrons to flow.
5
Properties of Electricity
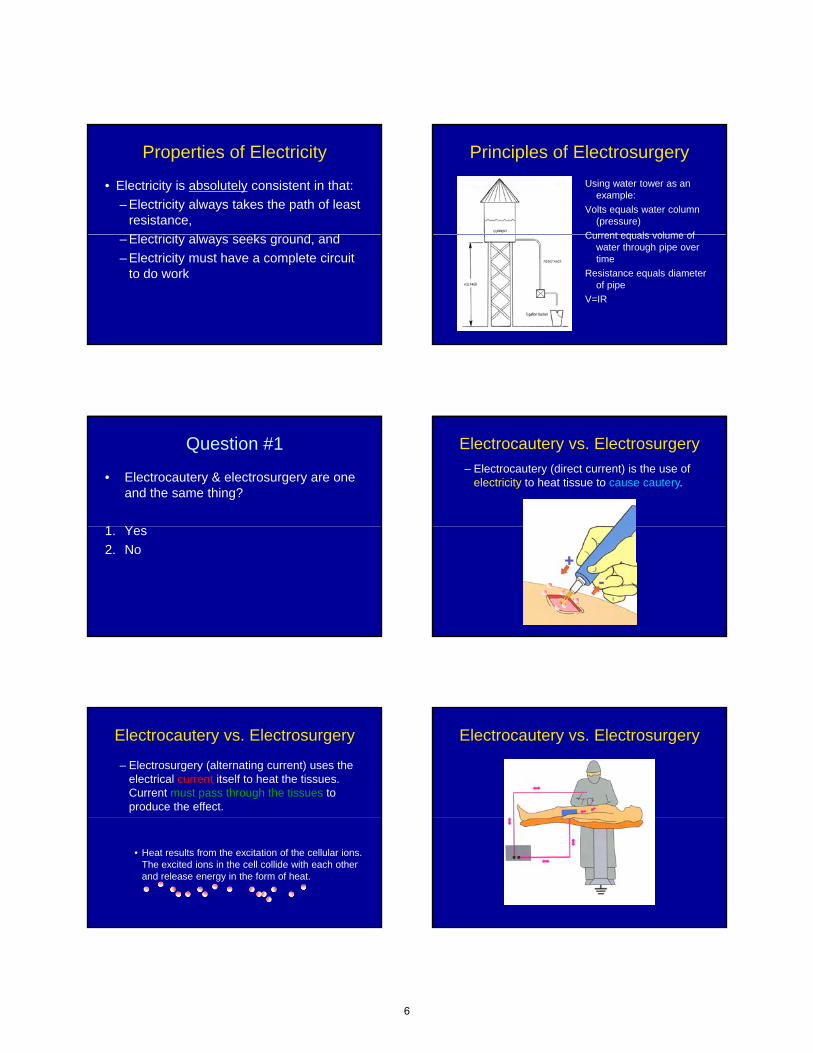
• Electricity is absolutely consistent in that:
– Electricity always takes the path of least resistance,
El t i it l k d d– Electricity always seeks ground, and
– Electricity must have a complete circuit to do work
Principles of Electrosurgery
Using water tower as an example:
Volts equals water column (pressure)
Current equals volume ofCurrent equals volume of water through pipe over time
Resistance equals diameter of pipe
V=IR
Question #1
• Electrocautery & electrosurgery are one and the same thing?
1 Y1. Yes
2. No
Electrocautery vs. Electrosurgery
– Electrocautery (direct current) is the use of electricity to heat tissue to cause cautery.
Electrocautery vs. Electrosurgery
– Electrosurgery (alternating current) uses the electrical current itself to heat the tissues. Current must pass through the tissues to produce the effect.
• Heat results from the excitation of the cellular ions. The excited ions in the cell collide with each other and release energy in the form of heat.
Electrocautery vs. Electrosurgery
6

Question #2
• Electrosurgical current used in the operating room runs at ?
1 60 H1. 60 Hz
2. 200 kHz – 3.3 MHz
3. 54 – 880 MHz
4. None of the above
How can you introduce electricity into the body without causing electrocution?
ElectrosurgeryPower Delivery
RF Generator
RFG “pushes”the current (voltage)
Current seeks
groundCurrent flows throughpatient
Ohm’s Lawin action
RF Generator
RFG “pushes”the current (Voltage)
Ohm's law: Voltage = Current x Resistance
Current
Impeded by Resistanceprovided by
instrument and patient.
Electrosurgical Effect on Cells
Radiofrequency current transfers energy to intracellular ions. Sine waveform results in oscillation of ions, imparting heat to intracellular water causing cell to burst
Question #3
• The following are electrosurgical clinical effects?
1 C t1. Cut
2. Fulguration
3. Dessication
4. All of the above
7

Effect of Waveform on Tissue
Cutting• Sine wave• Low voltage (1000
volts at 50 Watts power)p )
• Current arcs to tissue across steam envelope
• Less heating of tissue/thermal spread than coagulation waveform
Effect of Waveform on Tissue
Fulguration
(non-contact coagulation)
• Uses spark gap current
• High voltage (5000 volts• High voltage (5000 volts at 50 watts)
• Current arcs to tissue
• Causes heating and necrosis of tissue; greater thermal spread
Effect of Waveform on Tissue
Dessication
• Uses spark gap current
• High voltage (5000• High voltage (5000 volts at 50 watts)
• Direct contact to tissue
• Causes heating and necrosis of tissue
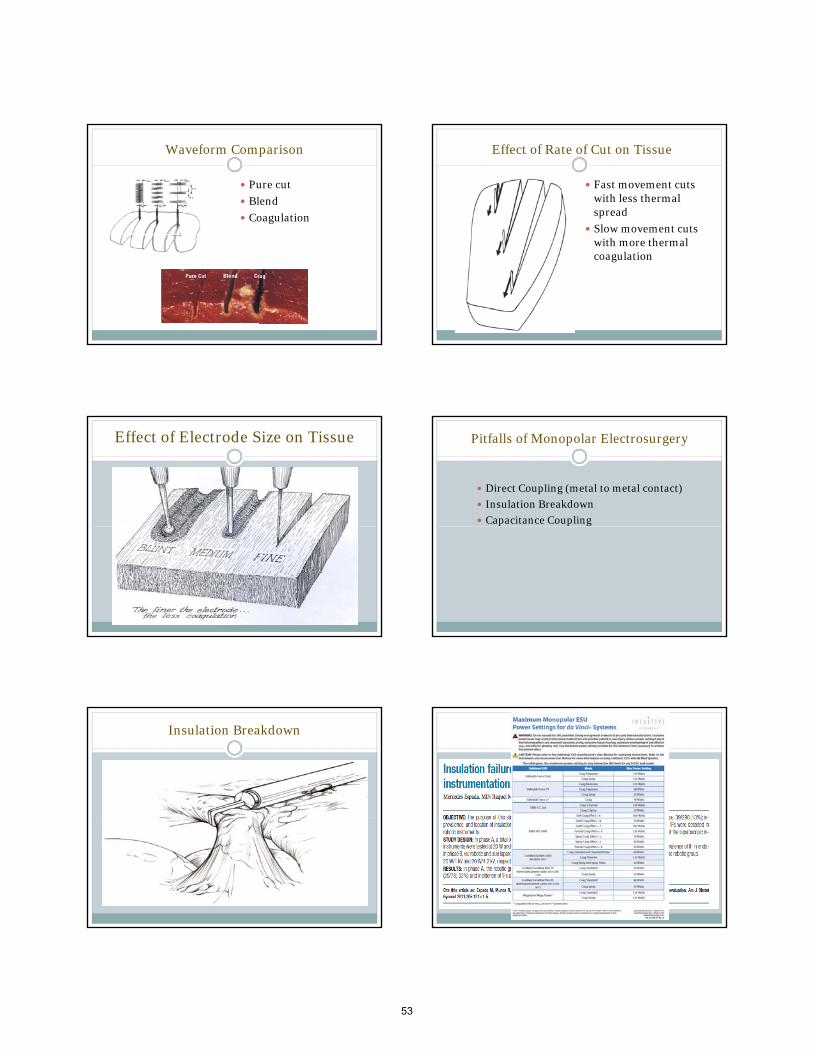
Waveform Comparison
• Pure cut
• Blend
• Coagulation
Effect of Rate of Cut on Tissue
• Fast movement cuts with less thermal spread
• Slow movement cuts with more thermal coagulation
Effect of Electrode Size on Tissue
8

Power FlowCurrent
• Monopolar RF
Generator
RFG “pushes”the current (voltage)
Current seeks ground
Ground Pad
Resistanceresults from medium
through which current flows
Question #4
• The following can be a hazard of monopolar current?
1 Di t li1. Direct coupling
2. Insulation breakdown
3. Capacitance coupling
4. All of the above
Pitfalls of Monopolar Electrosurgery
• Direct Coupling (metal to metal contact)
• Insulation Breakdown
• Capacitance Coupling
Direct Coupling
Insulation Breakdown Insulation Breakdown
9

Insulation Breakdown Capacitance Coupling
Capacitance Coupling
• Occurs when energy is transferred to an adjacent metal structure through an insulator
• Can cause injury remote from instrument tip
Capacitance Injury
Capacitance Injury Bipolar Electrosurgery
• Safer than monopolar electrosurgery
• Current flow: electrode-tissue-electrode
• Current precisely applied to target tissue
• No need for return pad
10

Power Delivery
• Bipolar RF
Generator
No Ground Pad
Required
Return path in jaws of instrument
Pitfalls of Bipolar Electrosurgery
• Power may be insufficient to coagulate large vessels
• Cutting may be inadequate
Th l h ti f i t t• Thermal heating of instrument
• Thermal spread increases with continued instrument activation
Bipolar ElectrosurgeryFlow of energy is Through tissue between jaws
Requires moisture in tissueFor conductivity.
Desiccated tissue is no longer conductive.
Resistance!
Question #5
• Ultrasonic devices?
1. Blend monopolar & bipolar current
2. Run at 200 kHz – 3.3 MHz
3. Utilize a radiofrequency of 50 kHz
4. Incorporate mechanical motion
5. Numbers 1 & 3
Ultrasonic (Mechanical) Energy
• Utilizes mechanical motion instead of RF
• Instruments oscillate at 55 KHz
• Mechanical energy transmission heats ti i ll l itissue, causing cell lysis
• Can be used for cutting and small vessel coagulation (cannot coagulate without cutting)
• Technique sensitive
11

Ultrasonic DevicesFlow of energy is Surface to Surface
Vibrating Member
Causes heating by friction in tissue No temperature control Instrument tip remains hot after application
Ultrasonic Devices
• Harmonic Ace (Ethicon Endo-Surgery)
• Sonicision (Covidien)
• SonoSurg (Olympus)
Laparoscopic Left Salpingectomy with Ultrasonic Scalpel
Evolution of Electrosurgical Vessel Sealing
LigaSure
Gyrus
EnSeal
Evolution of Electrosurgery
Monopolar• Current passes from active electrode, into the tissue, through the
patient, to the dispersive pad to the ESU
Conventional bipolar• Current passes from one electrode through tissue and returns to the
ESU via the second electrode of the instrument. No grounding pad.g g p
Advanced bipolar• Current passes from one electrode through tissue and returns to the
ESU via the second electrode of the instrument. No grounding pad.• Consistent hemostasis without sticking or thermal heating• Vessel sealing • Bipolar cutting• Concept of ““tensiontension--free sealing and transectionfree sealing and transection”” is very
important
Ligasure
• Permanently fuses vessels up to and including 7 mm in diameter and tissue bundles without dissection or isolation
• Seals withstand 3x normal systolic blood pressuresystolic blood pressure
• Provides a unique combination of pressure and energy to create vessel fusion
• Measures tissue impedance/resistance at the electrode site (feedback-controlled response system)
• Minimal sticking or charring
• Reduces thermal spread
12

Gyrus System
• PlasmaKinetic Vapor Pulse Coagulation (PK VPC):bipolar energy delivered as a series of pulses– Minimizes thermal spread– Minimizes tissue sticking– Minimizes heating of instrumentMinimizes heating of instrument– Minimizes surgical plume
• Multiple instruments, each has a unique default setting which determines the pulse on/off cycle and wattage– Output load curve customized for each instrument– Pulse rate tailored to maximize performance
PlasmaKinetic Vapor Pulse CoagulationOverview
• Vapor Pulse Coagulation: The End Point– Pulses are repeated until the tissue cannot absorb the high
energy pulses (visual of tissue swelling and release of steam with each pulse)
– Tissue cannot absorb the high energy current when it is fully and uniformly coagulatedy g
– The audible and visual impedance monitor provides a reference for endpoint desiccation
Conventional bipolar may cause sticking, thermal spread, and excess heating of instrument, due to constant power being delivered to the targeted tissue
PlasmaKinetic - VP Outputs PlasmaKinetic - VP Outputs
Gyrus Plasmakinetic Bipolar Cutting Forceps
First GenerationOf Electrosurgery
Devices
Physician Control
13

Second GenerationOf Electrosurgery
Devices
Smart Generator Control
Third GenerationOf Electrosurgery
Devices
(EnSeal)
Smart Electrode Control
EnSeal System Arteries have coiled Arteries have coiled elastin centrally located elastin centrally located
(inner layer)(inner layer)
vessel wall fusion can be achieved using RF energy to denature collagen & elastin in vessel
walls to reform into a permanent seal
Veins have elastin distributed throughoutVeins have elastin distributed throughout
Electrosurgical Vessel Welding
Hydrothermal
rupture of hydrogen
Cooling & renaturation of entangledCooling & renaturation of entangledunwound collagen strandsunwound collagen strands
rupture of hydrogen
cross-links by
elevating to 60-95oC
Electrosurgical Vessel Welding
High uniform mechanical compression High uniform mechanical compression increases entanglement and increases entanglement and
rere--crosslinking upon thermal relaxationcrosslinking upon thermal relaxationrere crosslinking upon thermal relaxationcrosslinking upon thermal relaxation
High tensile strength with High tensile strength with substantial elasticitysubstantial elasticity
14

Conventional Closing Mechanism
EnSeal Closing Mechanism
EnSeal Proprietary Technology
Cutting I Beam
Mechanical incision by I-beam as tissue
is progressively squeezed
Smart Electrode TechnologySmart Electrode TechnologyReturn electrode
TissueParticles already disconnected fromconductive path-temperature of tissue is abovetarget
RF source
Active electrode
Current conductivepath-temperatureof tissue is belowtarget
EnSealself-controlled electrode-network
amorphous
Temp coefficient matrixTemp coefficient matrix
0 5120oC
118oC
crystalline
Temperature sensitive, high Temperature sensitive, high density polyethylenedensity polyethylene with with embedded nanometerembedded nanometer--size size
conductive carbon conductive carbon spherulesspherules
1000
0.5
Nano-conductor Temperature sensitivematerial
Fatty tissueLess conductive
Vascular tissueMore conductive
15

Internal Electrode
Electrode with Nano-ParticleEnergy and Temperature ControlEnergy and Temperature Control
Spark-Control IntermediaryLayer
EnSeal TRIO
Clinical Obstetrics and Gynecology, 2010
Where do we go next?
ALTRUS (ConMed)Thermal Tissue Fusion
ALTRUS “seal line”
16

Altrus – Advantages
• Visually: minimal lateral thermal spread, smoke plume & instrument sticking
• A pure thermal-based system (NO RFA pure thermal based system (NO RF CURRENT) eliminates:
– Direct coupling
– Capacitance coupling
What will surgeons ask?
• Will patient outcomes improve?
• Will my ability to render care improve?
• Generalizability & reproducibility to the ?
4 Basic Questions
masses?
• Costs?
Conclusion
• There is no perfect energy device, yet.
• Understanding device characteristics will optimize tissue effect outcomes.
A l “l i ft b t” ith• As a rule, “less is often best”, with energy sources.
?’s
17

Ted T.M. Lee,M.D., FACOG
Director, Minimally Invasive Gynecologic Surgery
Magee Womens Hospital
UPMC
Disclosure
Grants/Research Support: Ethicon Endo-Surgery
Consultant: Ethicon Endo-Surgery, Gyrus ACMI (Olympus)Gyrus ACMI (Olympus)
The mother of surgery is anatomy, the father is exposure.y p
John Mikuta, M.D.
If you know your anatomy, know how to provide exposure, know how to dissect know how know how to dissect, know how to suture, you will become__________
Objectives
Promote understanding of pelvic retroperitoneal surgical anatomy using dissection techniques based on actual surgical procedureson actual surgical procedures (Different from the approach used in Gross Anatomy in Med School)
Special focus on pelvic sidewall anatomy
Gateway to the Retroperitoneum
Kadar, N
18

Gateway to Retroperitoneum Gateway to Retroperitoneum
Gateway to Retroperitoneum Gateway to Retroperitoneum
Gateway to Retroperitoneum Gateway to Retroperitoneum
19

Kadar, N
Relevance of Retropubic Space Anatomy
Pubovaginal sling, TVT
Burch
Paravaginal defect repair
Retropubic Space Entry
20

Relevence of Rectovaginal and Medial Pararectal Space
Rectovaginal endometriosis
Rectal resection
Sacrocolpoperineopexy
21

Important Structure in Medial Pararectal Space:
Middle Rectal Artery
Relevence of Presacral/retrorectal Space Anatomy
Presacral neurectomy
Sacrocolpopexy
Rectosigmoid Resection
22

23

Presacral Anatomy
Pelvic Sidewall Anatomy
Ureteral identification
Uterine artery ligation
Pelvic nodes
Pelvic Sidewall
Bladder
PV PV
MUL MUL
UterusUA UA
Hypogastric/Int Illiac Hypogastric/Int Illi
Ureter Ureter
PRPR
PV
24

Utility of Uterine Artery Ligation
Patholgy which make the ascending branch of uterine artery inaccessible. (Large fibroid, cervical fibroid, broad ligament fibroid, retroperitoneal g , pfibrosis/endometriosis involving the parametrium, ovarian remnant, ovary densely adherent to the parametrium.
25

Uterine Artery Ligation using Medial Umbilical Ligament
Uterine Artery Ligation by Developing Pararectal Space If you know your anatomy,
know how to provide exposure, know how to dissect know how know how to dissect, know how to suture, you will become__________
26

New Spokespeople for
Holiday Inn Express
27

LSH and TLH A Practical Approach
A Practical Surgical Approach to Laparoscopic
Hysterectomy
AAGL - PG 105
Presented by Richard B Rosenfield, MD
Director of GynecologyppStaying Out of Trouble
Richard Rosenfield MD
Medical Director, Pearl Women’s Center
Portland OR
Pearl Women’s Center / Pearl SurgicenterPortland, OR, USA
Disclosure
• Co-Founder, Chief Medical Officer of SURGiVIEW
Learning Objectives
• Review of hysterectomy statistics in the US
• Review the differences in terminology for laparoscopic hysterectomylaparoscopic hysterectomy
• Identify Benefits of Laparoscopic Hysterectomy when compared to traditional approaches
Basic Statistics
• 600,000 Hysterectomies per year in USA– Majority by Invasive Techniques
– Minimally Invasive Approaches• TVH
• LAVH
• LSH
• TLH
• TRH
LSH and TLH
• Is there a contraindication for laparoscopy ?• Size of uterus, size of patient, previousSize of uterus, size of patient, previous
surgery ?• Cancer ?
Why Laparoscopy ?
• Better Visualization
• Less Tissue Trauma
• Fast Recovery• Fast Recovery
• Cosmesis
• Outpatient Potential
28

Laparoscopic Entry
• Be Safe and Consistent
• Use trocars you are familiar with to avoid loss of pneumo slippage unplanned traumaloss of pneumo, slippage, unplanned trauma
• Consider towel clips for elevation of anterior abdominal wall
• Consider LUQ entry if concern of adhesions
How to get from point A to Point B
LSH Pearls- the room
• Operating Room Table- height and tilt
• Proper Positioning- Arms and Legs
• Dual Monitors• Dual Monitors
• Camera Resolution and Scope Quality
• Uterine Positioning
LSH Pearls- the surgeon
• Visualization is everything
• Maintain hemostasis to ensure visualization
• Slow and steady beats fast and sloppy• Slow and steady beats fast and sloppy
• 30 Degree Laparoscope imperative for complex advanced laparoscopy
LSH Pearls- the surgeon
• Seal vessels prior to transection
• Ablate endocervical canal for reduced cyclic bleeding (up to 5% in literature)cyclic bleeding (up to 5% in literature)
• Morcellation– Several vendors- Gynecare, Lina, Wolf, Storz
– Run the outside of specimen
– Calcified fibroids may dull blade
Ergonomic Morcellation
29

LSH Pearls- the assistant
• Help with visualization, because…
• Help with uterine manipulationCornua or Fimbria– Cornua or Fimbria
• Lean Technique
• Morcellator stays in position and blade is in mid-view; 5 mm scope from low lateral port
BMI 59- too big ?
Standardize Your Approach TLH- Why ?
• Dysplasia
• Cervical Bleeding
• Deep Dyspareunia Pelvic Pain• Deep Dyspareunia, Pelvic Pain
• Need for Intact endometrium
TLH errors
• Uterine vessel laceration at cuff– Solution: Reverse Horseshoe on TLH vessels
• Loss of Pnemoperitoneum at colpotomy• Loss of Pnemoperitoneum at colpotomy– Solution: occluder with infant bulb, assist to
pull up on cup
• Suturing– Large bites, mucosa, uterosacrals, barbed suture
TLH Pearls
• Mastery of LSH prior to TLH
• Use of Colpotomizer- drop ureters, visualize colpotomy targetvisualize colpotomy target
• Suturing- practice with Lap Trainer
• Ranfac Knot Pusher or V Loc
• BEWARE of magnification
30

TLH Pearls
• Use of Bipolar or Harmonic Device to reduce smoke for anterior and posterior Colpotomyp y
• Use Bipolar at 3 and 9 o’clock for uterine branches
• Maintain pneumoperitoneum with uterus in vagina, Bulb (or gloved Raytec)
TLH Pearls
• Retrograde fill the bladder if not absolutelycertain of reflection
• Use GOOD NEEDLE DRIVERSUse GOOD NEEDLE DRIVERS– Surgeon preference varies
– Self righting can be a problem at cuff
Why do we have complications ?
• Surgeon or Environment ?
• What variables can we control ?
Surgeons are victims of their surroundings
• How low does the table go ?
• What is max degree of trendelenberg ?
• Do you know the crew ?• Do you know the crew ?
• Have you selected the tools in the laparoscopy set ?
Is this safe ? I Have a Choice ?
31

Controlling Variables
If you take control of your surgical environment, you
minimize the opportunity for avoidable error
Anesthesia
• Preemptive management of pain and nausea
• “Balanced Anesthetic”R idl l d di ti– Rapidly cleared medications
– Local Anesthetic Injection
– Toradol, Decadron, Reglan, Zofran, Propofol, Versed (the magic 5)
Anesthesia
• There is noone named, “Anesthesia”
• Ok to change table position to help both you and your anesthetic providerand your anesthetic provider
• Proper airway selection for outpatient cases
Anesthesia
• Preop- no magic; consider NSAIDs
• Intraop- rapidly cleared meds
• Postop AVOID use of LONGACTING• Postop- AVOID use of LONGACTING NARCOTICS and NAUSEA POTENTIATORS
(Scopolamine Patch in cases of proven nausea)
Nursing and OR staff
• Crew understands roles and goals
• In Surgicenter, this is easy- Nurses understand how to mobilize patientsunderstand how to mobilize patients
• Verbal encouragement for discharge (gentle but firm motivation)
• Foley removed in Operating Room
32

The 9 Step Program
1. Learn to walk before you run
2 Begin at the Beginning2. Begin at the Beginning
3. Happy preop patients become happy postop patients
The 9 Step Program
4. Find Your Paintbrush and Canvas
5 Surround yourself with competence and5. Surround yourself with competence and minimize risk
6. Become friends with your anesthesia team
The 9 Step Program
7. Gentle Forcefulness Transitions Patients
8 The Art of Early Discharge Assurance8. The Art of Early Discharge- Assurance, Reassurance, Availability
9. Track Your Data
Where we were, 1929
Where we are… Where are we going ?
33

Technology… Is Changing….
You must keep up !
Thank you
Videos
• Stepwise approach to Laparoscopic Hysterectomy
34

Utilizing Reduced and Single Port Techniques for Conventional Laparoscopic and Robotic Hysterectomy
Stacey A. Scheib, MD, FACOG
Director of Minimally Invasive GynecologyJohns Hopkins Hospital
• Grants/Research Support: Intuitive Surgical
• Consultant: Covidien
• Explain the theory and rationale behind single port and reduced port laparoscopy
• Identify the limitations of single port and reduced port hysterectomyreduced port hysterectomy
• Apply single incision and reduced port laparoscopy to hysterectomy
Background• Gynecology has been at the forefront of single site
surgery starting almost 40 years ago. – The offset operating laparoscope used for
laparoscopic tubal ligations,1-2
– The first complex procedure, a hysterectomy and bilateral salpingo-oophorectomy was performed by P l i d P l i i 1991 ith t dditi l t h 3Pelosi and Pelosi in 1991, without additional trochars.3
Despite these early efforts, single site surgery did not become a standard surgical technique in gynecologic surgery for several reasons and is now only taken off due to advances in technology.
Why Bother?
Morbidity
• Each additional port used potentially increases morbidity
• Bleeding
• Port site hernia• Port-site hernia
• Internal organ injury
• Vascular injury
• Post-operative wound infection
• Decreases cosmetic outcome
2 weeks postop
35

Pain
• Potential decrease in postoperative pain and need for postoperative pain medications, which might be due to avoidance of multiple muscle‐splitting incisions 4‐7muscle splitting incisions.
Gynecology and Single Incision
• Anatomy of the Pelvis
• Ease of Specimen Removal
Disadvantages
• Restricted by a surgeon’s experience with advanced laparoscopy.
– Loss of triangulation
– Special instrumentation
– Learning curve
Single Incision Hysterectomy:Let’s break it down
Just Remember
• Follow standard laparoscopic fundamentals(LESS and reduced port laparoscopy is an ACCESS technique…NOT a new procedure)
• Includes using all normal precautionary steps such as identifying and isolating ureters, bladder, and bowel
What will you need to get started?
• Port
• Laparoscope – Angled or Flexible Tip
• Instruments – Traditional Straights
• Energy – Anything but ultrasonic technology
• Uterine Manipulator
• Morcellator
36

Abdominal Entry: Hasson Technique
1.Skin Incision
• 2-3cm
• Omega or Vertical Incision
2. Identify fascia.
3.The fascia is grasped and elevated with a pair of Allis or g p pKocher clamps.
4.Adherent subcutaneous tissue is gently dissected free.
5. Incision made in fascia
• At least 1-2 finger breaths
6.Peritoneum entered bluntly or sharply
Putting in the Port
• This will vary slightly based on the port selected
Where is the surgeon?
• Stand by the patient’s head
M d t• May need to move the OR table away from anesthesia
Cross Over Technique• Grasper goes in contralateral
trochar from the direction of retraction
• If you are clashing instruments, t lik l i t t i thmost likely instruments are in the
wrong trochars…pull everything out and reassess
• Set yourself up to be successful…camera, then grasper, and finally energy
Cross Over Technique
• Internal and external video
Cross Energy Above or Below the Grasper?
ABOVE• Round ligament• Bladder flap• Colpotomy• Cervical amputationBELOW• Infundibulopelvic ligament• Utero-ovarian ligament• Fallopian tube• Round Ligament• Uterine artery• Colpotomy• Cervical amputation
37

Morcellation• Video
• When using a morcellator, must visualize tip at all ptimes…Patient Safety First!
• Keep in the midline
Cuff Closure• Vaginal closure
• Laparoscopic suturing device with an articulating laparoscopic grasperg p p g p
• Vertical laparoscopic closure with a “puppet string” at 12 o’clock (advanced single incision laparoscopic technique)
Worst Case Scenario
Add another trochar!!!
Closure
• Close the fascia
• May need to stitch base of umbilicus down to fascia
• Place several buried interrupted to space out tension• Place several buried interrupted to space out tension
• Subcutaneous stitch to reapproximate skin
• Discourage use of skin glue
Single Incision Robotic Assisted Hysterectomy
• Limitations with current system
• Need a 30 degree “UP” scope (8mm if il bl )available)
• Will need up to a 4 cm facial incision
Port Configuration
FEET
HEAD
38

Take Home
• Anticipate the need for “cross-over” of instruments
• Expect every step to take more thought and concentration
• Utilize a bariatric and/or articulating scope to remove g pclutter from the immediate operating field
• Be aware of a tendency to accept less anatomic visualization than conventional laparoscopic and don’t accept this…Patient Safety First!
• If it is necessary, place an additional trochar
Your turn…
1. Wheeless CR. A rapid, inexpensive and effective method of surgical sterilization by laparoscopy. Journal of Reproductive Medicine. 1969; 3: 65-9.
2. Wheeless CR, Thompson BH. Laparoscopic sterilization: review of 3600 cases. Obstetrics and Gynecology. 1973; 42: 751-8.
3. Pelosi MA, Pelosi MA. Laparoscopic hysterectomy with bilateral salpingo-oophorectomy using a single umbilical puncture. New England Journal of Medicine. 1991; 88: 721–6.
4. Fader AN, Escobar PF. Laparoscopic single-site surgery (LESS) in gynecologic oncology: Technique and initial report. Gynecologic Oncology. 2009; 114: 157-61.
5. Kim TJ et al. Single-port-access laparoscopic-assisted vaginal hysterectomy versus conventional laparoscopic-assisted vaginal hysterectomy: a comparison of perioperative outcomes. Surg Endosc. 2010 Sep;24(9):2248-52.
6. Yim GW et al. Transumbilical single-port access versus conventional total laparoscopic hysterectomy: surgical outcomes Am J Obstet Gynecol 2010 Jul; 203(1):outcomes. Am J Obstet Gynecol. 2010 Jul; 203(1): 26.e1-6.
7. Yim GW et al. Is Single-Port Access Laparoscopy Less Painful Than Conventional Laparoscopy for Adnexal Surgery? A Comparison of Postoperative Pain and Surgical Outcomes. Surg Innov. 2012 Mar 12. [Epubahead of print]
39

Ted Lee, M.D.
Director, Minimally Invasive Gynecologic Surgery
Magee Womens Hospital
UPMC
Disclosure
Grants/Research Support: Ethicon Endo-Surgery
Consultant: Ethicon Endo-Surgery, Gyrus ACMI (Olympus)Gyrus ACMI (Olympus)
Objectives
Facilitate the understanding of strategies and techniques for difficult hysterectomy based on sound surgical principles and knowledge of p p gretroperitoneal pelvic anatomy.
Situations which distort pelvic anatomy
Fibroid uterus Endometriosis with obliteration of cul de sac. Severe uterine adhesions to the bladder and
anterior abdominal (c-section, myomectomy). Dense ovarian adhesion to the ovarian fossa
and parametrium with or without retroperitoneal fibrosis.
Obesity. Increased retroperitoneal adioposity.
Helpful Tools in Difficult Hysterectomy
Angeled scope (30 or 45 degree) or flexible scope
Ureteral stents Use the uterine manipulator with a well
fit obturator. Powerful morcelator Reliable vessel sealer
40

Anterior Abdominal Wall Adhesions45 Degree Scope
Ureter at Risk
Not knowing the location of ureter halts the progression of surgery for the careful and invites disaster for the careless.
Ureteral stents let you know the course of the ureter so you can zip along when you are away from the ureter and refine your dissection as you get closer
41

Ureteral Stent General Strategies for Hysterectomy
Always Take the Easier Pedicles Do not tackle the hard pedicle without
securing the easier pediclessecuring the easier pedicles Can always take the uterovarian and go back
for the IP. Can always take one IP (sacrifice one ovary)
if uterovarian is difficult
Uterine Artery Ligation-Four Ways
Conventional
Anterior approach (ascending branch)
Posterior approach (ascending branch)
Lateral Approach-at its origin from internal iliac.
Anterior Approach Ligation of the ascending branch uterine
artery without opening the posterior broad ligament.
Good for uterus with large fibroid uterus with Good for uterus with large fibroid uterus with poor access to the cul de sac and posterior broad ligament, Large fibroid uterus not maneuverable by the manipulator
Not good for patients with fibrosis in the parametrium from endometriosis or dense bladder adhesions from c-sec.
42

43

Posterior Approach
Ligation of ascending branch of uterine artery without developing bladder flap.
Excellent in patients with extensive and d t i dh i t th bl dd ddense uterine adhesions to the bladder and anterior abdominal wall.
Technique usually not available during open surgery, unique to laparoscopic approach.
44

Lateral Approach
Commonly done in radical hysterectomy for cervical cancer.
Good for retroperitoneal fibrosis in the parametrium seen in severe endometriosisparametrium seen in severe endometriosis.
Ovarian remnant. Large fibroid uterus. Maybe difficult to visualize without angled
scope in broad fibroid uterus.
45

Know Your Anatomy like the Cab Driver Knows the Streets in any Big City
Need to know more than one way to get from point A to point B so if you get in the jam you know the alternate route.
Try the alternative route when there is no traffic/pressure.
Know the freeway as well as the side streets
46

Robotic Hysterectomy: A Systematic Approach in 3‐D
Arnold P. Advincula, MD, FACOG, FACS
Professor of Obstetrics & Gynecology
University of Central Florida College of Medicine
Director, Center for Specialized Gynecology
Director, Celebration Health Endometriosis Center
Director, AAGL/SRS Accredited MIS Fellowship
Florida Hospital ‐ Celebration Health
A Systematic Approach in 3‐D
Disclosure
Consultant: CooperSurgical, Ethicon Women's Health & Urology, Intuitve Surgical
Other: Royalties - CooperSurgical
OBJECTIVES
Review the rationale behind considering a standardized approach to the simple hysterectomy (from instrumentation to technique).
Discuss the potential implications stemming from improper patient positioning peritoneal access port improper patient positioning, peritoneal access, port placement, and uterine manipulation.
Demonstrate principles and techniques of robot-assisted laparoscopic dissection & suturing.
Review the key steps leading up to and involved in optimal colpotomy & vaginal cuff management.
TLHTLHVHVH
Robotic HystRobotic Hyst
LSHLSH
LAVHLAVH
TAHTAH
Instrument Tray Standardization
47

Top Tray•Robotic instruments
Middle Tray•Cords•Laparoscopic instruments•Laparoscopic instruments•Open instruments
Bottom Tray•Vaginal instruments•Dilators•Speculum
MonopolarCurved Scissors
Mega SuturecutNeedle Driver
PrograspForceps
Cobra Grasper
PK Dissecting
Forceps
Mega Needle Driver
Long Tip Forceps
TenaculumForceps
Back Table Vaginal Mayo Stand
Roving Instrument Cart Key Technical Steps
Patient positioning Peritoneal access & strategic trocar placement Uterine manipulation Docking (center, L/R)
f i fi ld (“ f h ”) Survey of operative field (“a game of chess”) Adnexal management Round ligament & entry into broad ligament Vesico-uterine reflection Identification of ureters Skeletonization & ligation of uterine vasculature
48

Key Technical Steps
Retention or removal of cervix
Management of vaginal cuff Colpotomy
Closure
Specimen extraction Mechanical morcellation
Dorsal lithotomy
Arms padded and tucked at sides
Steep Trendelenburg
B l P ??? Bowel Prep???
Decompress stomach & bladder
Collaborate with Anesthesia team
Low lithotomy position: abdominal or laparoscopic approach
15Barnett et al. 2007
Hip abduction
16 Barnett et al. 2007
Optimal Patient Positioning OR Bed Setup
49

OR Bed Setup Egg Crate Foam Mattress Technique
20
Port Placement:“standard rules but individualized”
3-Arm 4-Arm
Measurements should be made after insufflation!
Center-docking
Side-docking 3-Arm (Left)
50

4-Arm (Left) Uterine Manipulation Method
ZUMI
Apple Obturators
RUMI colpotomizer system
VCARE
Colpotomizer
RUMI II handle with Koh Efficient
colpotomizer system
V-Care
Advincula Arch with Koh Efficient Colpotomizer System
Colpotomy RingUreter #1 Ureter #2
“Size Matters”
“Choose Proper Koh Colpotomizer Cup Size”
“Size Matters”
Choose Appropriate RUMI Tips
Impacts uterine maneuverability!
51

“Inflate Pneumo-occluder Balloon Prior to Colpotomy” Adnexal Management
Retain adnexa or remove after hysterectomy for improved exposure (“preservation of triangle”)
Immediate removal
Vesico-Uterine Reflection/Bladder Flap
Efficient Colpotomy
Energy source does not matter; what matters is the way the energy source is handled
Upward tension on colpotomizer
Tolerate some bleeding (vaginal cuff should not look like charcoal)
OPTIMIZATION OF ELECTROSURGERY
USAGE
52
Waveform Comparison
Pure cut
Blend
Coagulation
Effect of Rate of Cut on Tissue
Fast movement cuts with less thermal spread
Slow movement cuts with more thermal coagulation
Effect of Electrode Size on Tissue Pitfalls of Monopolar Electrosurgery
Direct Coupling (metal to metal contact)
Insulation Breakdown
Capacitance Coupling
Insulation Breakdown Insulation Failure
53

Properties of Electricity
Electricity is absolutely consistent in that:
Electricity always takes the path of least resistanceresistance,
Electricity always seeks ground, and
Electricity must have a complete circuit to do work
Direct Coupling
Capacitance Coupling EndoWrist® One™ Vessel Sealer
Designed to seal & cut up to 7 mm diameter vessels
Single use disposable
8 mm diameter instrument
Compact snake wristp
Product has received FDA clearance
Key Concept #4: Adequate Suturing
Conventional & robot-assisted laparoscopic suturing rely heavily on the principles of: Adequate bites of tissue beyond the cut electrosurgical edge
(do not suture through devitalized tissue)
Incorporation of both vaginal epithelium and fascia Incorporation of both vaginal epithelium and fascia
Barbed Suture:QuillV-Loc
54

Cut suture flush with tissue!Tissue Extraction: Morcellation
Efficiency/Safety Strategies
• Undock patient side-cart if robotic case• Place morcellator at camera port site• Use 5 mm laparoscope placed in one of the lower quadrant trocarsreduced to 5 mm• Chip management•Benign Endometrial Sampling
Final Steps
Irrigate operative field “Low pressure check”
Cystoscopy with Indigo Carmine or Pyridium
Inspect vaginal cuff with speculum
Post-operative care/precautions
Post-Operative Care
Pelvic rest for 8 weeks
No STDs Sex
Tampons
hi Douching
Vaginal cuff inspection at 8 weeks post-op
TLH 4.93%TVH 0.29%TAH 0.12%
Overall 0.14% in 7039 ptsover 6 years
RaTLH 4.1%in 510 pts
55

TLH 1.35%
Conclusion
Success with the simple (complex) minimally invasive hysterectomy relies heavily on a well thought strategy from start to finish.
Conclusion
Prevention of vaginal cuff complications is multi-factorial (not an issue of absent haptic feedback) Colpotomizer
Bladder flap development
Efficient use of energy source during colpotomy (energy source Efficient use of energy source during colpotomy (energy source does not matter)
Adequate suturing (suture type does not matter)
Pelvic rest (8 weeks)
?’s? s
56

LSH and TLH A Practical Approach
Tips and Tricks for Tackling the Large Uterus during
Laparoscopic Hysterectomy
AAGL - PG 105
Presented by Richard B Rosenfield, MDppStaying Out of Trouble
Richard Rosenfield MD
Medical Director, Pearl Women’s Center
Portland OR
Presented by Richard B Rosenfield, MD
Director of Gynecology
Pearl Women’s Center / Pearl SurgicenterPortland, OR, USA
Disclosure
• Co-Founder, Chief Medical Officer of SURGiVIEW
Learning Objectives
• Define Large Uterus
• Review Anatomical Changes and Relationships with a Large UterusRelationships with a Large Uterus
• Video Session Reviewing Parallel Port Technique for Hysterectomy with Large Uterus
So, What Defines LARGE
• According to CMS, and our CPT codes
• 250 grams
• What about 500 grams
• 1000 grams
• 3000 grams
Is there a size limit for LSH / TLH
• “In my experience, and with my training, I feel that this surgery would best be g yapproached…”
• What’s the downfall of trying ?
Big PATIENT
57

Big UTERUS SURGICAL APPROACH
5 Trocar Approach Why ?
• 750 Consecutive Cases
• 100% Success
• 0% Conversion to Laparotomy• 0% Conversion to Laparotomy
• Uteri as Large as 2000 grams in outpatient center with same day discharge home
Anatomical Consideration
• Uterine Size
• Patient Size
• Patient Pelvis• Patient Pelvis
• Number of Fibroids
• Location of Fibroids
• Relation of Fibroids to Pelvis, Ureters, and other confounding variables
Energy Source
• Can you secure large vessels ?
• Can you seal vessels without cutting them ?
• Do you measure blood vessel diameter ?• Do you measure blood vessel diameter ?
• Endoclips, suture ligation, retroperitoneal dissection to origin of uterine artery
58

Uterine Manipulation
• Acorn Cannula is a cervical manipulator
• Intrauterine placement optimal
• Intraperitoneal options (tenaculum lean• Intraperitoneal options (tenaculum, lean technique)
Morcellation
• Single Use versus Multi-use
• Blade dulling can be problematic
• Arm fatigue• Arm fatigue
• Scatter of Tissue
Laparoscopic Entry
• Umbilical versus LUQ
• Use trocars you are familiar with to avoid loss of pneumo slippage unplanned traumaloss of pneumo, slippage, unplanned trauma
• Consider towel clips for elevation of anterior abdominal wall
• Move everything CEPHALAD
How to get from point A to Point B
Stepwise Approach
• Easy Side FIRST if possible
• Anterior Approach
• Enucleate Fibroids• Enucleate Fibroids
• Caution with ureters
• Once uterines are secure, so are you !
Pearls
• Seal vessels prior to transection
• Try LEAN technique over grasping to avoid bleedingbleeding
• Discuss EACH STEP with assistant
• Use OR Table as a tool
• Morcellation
59

LSH Pearls- the assistant
• Help with visualization
• Help with uterine manipulationCornua or Fimbria– Cornua or Fimbria
• Lean Technique
• Morcellator stays in position and blade is in mid-view; 5 mm scope from low lateral port
Videos
• Stepwise approach to Laparoscopic Hysterectomy
60

Dealing with Difficult Peritoneal Access, Obesity,
and Vaginal Cuff Issues
Stacey A. Scheib, MD, FACOG
Director of Minimally Invasive GynecologyJohns Hopkins Hospital
• Grants/Research Support: Intuitive Surgical
• Consultant: Covidien
• Identify when to use non-umbilical entries
• Employ safe practice to laparoscopic entry
• Implement preoperative, perioperative, t ti t f th bpostoperative management for the obese
patient
• Apply safe practice to minimize cuff complications
Peritoneal Access
• “Mini-laparotomy” entry
• A cannula with a cone-like sleeve is inserted. The peritoneal edge and fascia are tagged and attached to the cannula.
Open or Hasson Technique1 Closed Techniques• Direct Entry +/- Optical Trochar
– Trochar is inserted without pneumoperitoneum
• Veress Needle
– Involves the insertion of a Veress Needle (a needle equipped with a spring‐loaded obturator) into theequipped with a spring loaded obturator) into the peritoneal cavity, followed by gas insufflation then insertion of a trocar
– The use of the Veress Needle was associated with an increased incidence of failed entry, extraperitoneal insufflation and omental injury2
61

Candidates for Non-Umbilical Entry
• Obesity
• Suspected Adhesive Disease
• Prior ventral hernia repair
• Extreme thinness
• Pregnancy
• Abdominal wall laxity
• Large pelvic mass
Upper Abdomen
• Palmer’s point3
• Left 9th or 10th Intercostal space4-6
• Supraumbilical
• Need an naso- or oro-gastric tube
• Contraindications: hepatosplenomegaly, portal hypertention, gastropancreatic masses, prior gastric bypass
Trans-Uterine Entry
• Patient in Trendelenberg and uterus is anteverted prior to long Veress insertion7-11
• Helpful for obese women and those with contraindications to umbilical and left upper quadrant entry
• Contraindications: fibroids, infertility work up
Wolfe WM, Pasic R. Obstet Gynecol, 1990.
Trans-Vaginal Entry• Inserted in the midline of a taut
posterior fornix approx 1.75cm with long Veress12, 13
• Helpful for obese women and those with contraindications tothose with contraindications to umbilical and left upper quadrant entry
• Contraindications: fixed retroverted uterus, prior pelvic infection
Good Practice• The angle of the Veress/trochar at the
umbilicus should vary according to the BMI of the patient14
Hurd et al. Obstet Gynecol, 1992.
Good Practice
Insertion with patient flatInsertion with patient in Trendelenberg
62

Good Practice
• An opening intraperitoneal pressure ≤ 10mm Hg15-21
U lt ti t h i ft 3 f il d• Use an alternative technique after 3 failed Veress attempts15,16
Obesity
Obesity Definitions and Trends
• Morbid Obesity, Super Obese and Super-Super Obese
• The prevalence in these groups is increase much faster than the prevalence of obesity.22-24
• Treating the morbid and super obese will NOT be rare event anymore.
Percentage increase in BMI categories since 1986 (source: Behavioral Risk Factor Surveillance Survey)
Sturm R. Arch Intern Med, 2003.
Routine Assessment
• Higher incidence of co-morbidities due to their weight, which implies greater overall operative risk25
• A comprehensive medical history and physical examination including questions about her exercise tolerance and OSH screening questions26
• Labs: CBC, Glucose, BUN, Cr, coagulation studies
• Chest X-ray
• EKG27
• Tailor any addition other studies based on the patient’s risk factors and not the degree of obesity28,29
DVT Prophylaxis
• The American College of Chest Physicians guidelines that bariatric surgery patients have a high risk VTE and have recommended routine pharmacologic prophylaxis combined with mechanical prophylaxis.30
• The American Association of Clinical Endocrinologists• The American Association of Clinical Endocrinologists (AACE)/The Obesity Society (TOS)/the American Society for Metabolic and Bariatric Surgery (ASMBS) guidelines have recommended the insertion of preoperative IVC filters in bariatric surgery patients who have a particularly high risk of VTE31,32
Positioning the Patient• Risk of the pressure sores and nerve injuries is very high
in these patients.33-37
– Risk depends on the amount of compressive force applied and the duration of the compression35-37
– Compression for a duration for 6-8 hours or more can lt i t t l d t th 36 37result in structural damage to the nerve36-37
– Most common are ulnar and sciatic nerves
• Allot extra time for positioning
• Trial of Trendelenberg
63

Laparoscopy in the Obese Patient• Can be accomplished safely without an increase in
complications38
• Why bother?
– ↓ postoperative pain, ↓ impairment of postoperative ↓ p p p , ↓ p p ppulmonary function, ↓ length of hospital stay, ↓ time to return to work and routine activities, and↓ rate/severity of infections when compared to open gastric bypass39
– ↓ in the rate of incisional hernia (about 7 to 1) and infection rates (10.5 vs. 1.3% )40
Technical Implications• ↓respiratory function41-44
• ↑ intra-abdominal pressure
• Weight of chest
• ↓ total compliance and functional reserve capacity
• ↑ intra-abdominal pressure↑ intra abdominal pressure
• hepatic steatosis, thickened transverse colon, and ample visceral fat
• ↓ visualization and require longer trocars with the concomitant need for ↑ torque and ↑ operator fatigue38
Making Adjustments
• Can avoid with appropriate changes in ventilation by anesthesia
• Less Trendelenberg
• Decreasing pneumoperitoneum pressure
M h i ll lli i id t f l i• Mechanically pulling sigmoid out of pelvis
• Mechanically lifting the pannus
LaparoscopicPannus Retraction Techniques
• Video
Postoperative Management
• Extended DVT prophylaxis for 3-4 weeks postoperative for high risk patients32, 45-49
• Covalence in the semi-recumbent position postop50, 51
• Aggressive pulmonary toilet with incentive spirometry and chest physical therapyand chest physical therapy
• Early institution of CPAP
• Early ambulation
• Respiratory distress or failure to wean from ventilatory support should raise suspicion and prompt an evaluation for acute postoperative complications31
Postoperative Management
• Urinary output of 30mL/hr
• Avoiding volume overload
• Use of short acting opioids
• LOW THRESHOLD for keeping in house
64
Closing the Vaginal Cuff
Difficult Laparoscopic Cuff Closures
• Vaginal closure
• Use of “puppet strings”
• Barbed suture
Vaginal Cuff Complications
• Dehiscence52‐55
– Energy
– Size of the bites
– Laparoscopic SuturingLaparoscopic Suturing
• Abscess
– Presence of bacterial vaginosis
• Fistula
– Sutures in the bladder
Looking at Cuff Closure
• Use the lowest settings possible for colpotomy
• Minimize use of electrosurgery
• Take good bites of the cuff: at least 5 mm b d h d d dbeyond the edge and spaced 5 mm apart
• Role of 2 layer closure and barbed suture53,55
• Cystoscopy
1. Hasson HM. A modified instrument and method for laparoscopy. Am J Obstet Gynecol, 1971; 1110: 886-7.
2. Ahmad G et al. Laparoscopic entry techniques. Cochrane Database Syst Rev. 2012 Feb 15;2:CD006583.
3 Palmer R Safety in laparoscopy J Reprod Med 1974;3. Palmer R. Safety in laparoscopy. J Reprod Med. 1974; 13:1-5.
4. Lam KW, Pun TL. Left upper quadrant approach in gynecologic laparoscopic surgery with reusable instruments. J Am Assoc Gynecol Laparosc, 2002; 9: 199-203.
5. Agarwala N. Liu CY. Safe entry technique during laparoscopy: left upper quadrant entry using the ninth intercostal space: a review of 918 procedures. J Minim Invasive Gynecol, 2005; 12:55-61.
6. Reich H et al. Establishment of pneumoperitoneum through the left ninth intercostal space. Gynaecol Endosc, 1995; 4: 141-3.
7. Sanders RR, Filshie GM. Transfundal induction of pneumoperitoneum prior to laparoscopy. J Obstet Gynaecol Br Cmwlth, 1994; 107: 316-7.
8. Morgan HR. Laparoscopy: induction of pneumoperitoneum via transfundal puncture. Obste Gynecol, 1979; 54: 260-1.
65

9. Wolfe WM, Pasic R. Transuterine insertion of Veress needle in laparoscopy. Obstet Gynecol, 1990; 75: 456-7.
10.Pasic R et al. Laparoscopy inmorbidly obese patients. J Am Assoc Gynecol, 1999; 6: 307-12.
11.Santala M et al. Transfundal insertion of a Veress 11.Santala M et al. Transfundal insertion of a Veress needle in laparoscopy of obese subjects: a practical alternative. Hum Reprod, 1999; 14: 2277-8.
12.Neeley MR et al. Laparoscopy: routine pneumoperitoneum via the posterior fornix. Obstet Gynecol, 1975; 45: 459-60.
13.Van Lith DA et al. Cul-de-sac insufflation: an easy alternative route for safely inducing pneumoperitoneum. Int J Gynaecol Obstet, 1980; 17: 375-8.
14.Hurd WW et al. The relationship of the umbilicus to the aortic bifurcation: implications for laparoscopic technique. Obstet Gynecol, 1992; 80(1):48-51.
15.Teoh B et al. An evaluation of four tests used to ascertain Veres needle placement at closed laparoscopy. J Minim Invasive Gynecol, 2005; 12:152-8.
16.Richardson RF, Sutton CJG. Complications of first entry for laparoscopy: a prospective laparoscopic audit. Gynaecol Endosc, 1999; 8: 327-34.
17.Garry R. Complications of laparoscopic entry [editorial review]. Gynaecol Endocsc,1997; 6: 319-29
18.Dubuisson JB et al. ‘Classic’ laparoscopic entry in a university hospital: a series of 8324 cases. Gynaecol Endosc, 1999; 8: 349-52.
19.Ricci M, Aboolian A. Needle Pneumoperitoneum. An alternaltive technique. Surg Endosc, 1999 Jun; 13(6):629.
20.Vilos GA, Vilos AG. Safe laparoscopic entry guided by Veress needle CO2 insufflation pressure. J Am Assoc Gynecol Laparosc, 2003; 10: 415-20.
21.Vilos AG et al. Effect of body habitus on the initial Veres intraperitoneal (VIP) CO2 insufflation pressure during laparoscopic access in women. J Minim Invasive Gynecol, 2006; 13(2): 108-13.
22.Sturm R. Increases in morbid obesity in the USA: 2000-2005. Public Health, 2007; 121 (7): 492-6.
23 Sturm R Increases in clinically severe obesity in the23.Sturm R. Increases in clinically severe obesity in the United States, 1986-2000. Arch Intern Med. 2003 Oct 13;163(18):2146-8.
24.Ogden Cl et al. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA, 2006 Apr;295(13):1549-55.
25.Kral JG. Morbid obesity and related health risks. Ann Intern Med, 1985;103(6 (Pt 2)):1043-7.
26.Livingston EH, Langert J. The impact of age and Medicare status on bariatric surgical outcomes. Arch Surg, 2006;141(11):1115-20; discussion 21.
27.Poirier P et al. Cardiovascular evaluation and o e et a Ca d o ascu a e a uat o a dmanagement of severely obese patients undergoing surgery: a science advisory from the American Heart Association. Circulation, 2009;120(1):86-95.
28.Ramaswamy A, Gonzalez R, Smith CD. Extensive preoperative testing is not necessary in morbidly obese patients undergoing gastric bypass. J Gastrointest Surg2004;8(2):159-64; discussion 64-5.
29.Schumann R, Jones SB, Ortiz VE, Connor K, Pulai I, Ozawa ET, et al. Best practice recommendations for anesthetic perioperative care and pain management inanesthetic perioperative care and pain management in weight loss surgery. Obes Res, 2005;13(2):254-66.
30.Geerts WH et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest, 2008;133(6 Suppl):381S-453S.
66

31.Mechanick JI et al. Executive summary of the recommendations of the American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery medical guidelines for clinical practice for the perioperative nutritional, metabolic, and nonsurgical
f h b i i i E d Psupport of the bariatric surgery patient. Endocr Pract, 2008;14(3):318-36.
32.Agarwal R et al. Venous thromboembolism prophylaxis for patients undergoing bariatric surgery: a systematic review. Surg Obes Relat Dis, 2010; 6: 213-20
33.Mathews PV et al. Compartment syndrome of the well leg as a result of the hemilithotomy position: a report of two cases and review of literature. J Orthop Trauma, 2001;15(8):580-3.
34.Freedman JM et al. Transient neurologic symptoms after spinal anesthesia: an epidemiologic study of 1,863 patients. Anesthesiology, 1998;89(3):633-41.
35.Lundborg G, Dahlin LB. Anatomy, function, and pathophysiology of peripheral nerves and nerve compression. Hand Clin, 1996;12(2):185-93.
36.Berhane L et al. Lower extremity paralysis after operative laparoscopy from conversion disorder. A case report. J Reprod Med,1998;43(9):831-5.
37.Massey EW, Pleet AB. Compression injury of the sciatic nerve during a prolonged surgical procedure in a diabetic patient. J Am Geriatr Soc,1980;28(4):188-9.
38.Artuso D et al. Extremely high body mass index is not a contraindication to laparoscopic gastric bypass. Obes Surg, 2004;14(6):750-4.
39.Gould JC et al. Laparoscopic gastric bypass: risks vs. p p g ypbenefits up to two years following surgery in super-super obese patients. Surgery, 2006;140(4):524-9; discussion 9-31.
40.Puzziferri N et al. Three-year follow-up of a prospective randomized trial comparing laparoscopic versus open gastric bypass. Ann Surg, 2006;243(2):181-8. 138.
41.van Gemert WG et al. Quality of life assessment of morbidly obese patients: effect of weight-reducing surgery. Am J Clin Nutr, 1998;67(2):197-201.
42.Ogden CL et al. Prevalence of overweight and obesity in the United States, 1999-2004. JAMA, 2006;5;295(13):1549-55.
43.Flegal KM et al. Prevalence and trends in obesity among US adults, 1999-2000. JAMA, 2002;288(14):1723-7.
44.Sugerman HJ et al. Gastric surgery for respiratory insufficiency of obesity. Chest, 1986;90(1):81-6.
45.Abou-Nukta F et al. Clinical pulmonary embolus after gastric bypass surgery. Surg Obes Relat Dis, 2006;2(1):24-8; discuss 9.
46.Hamad GG, Bergqvist D. Venous thromboembolism in bariatric surgery patients: an update of risk and prevention. Surg Obes Relat Dis, 2007;3(1):97-102.
47.Scholten DJ et al. A comparison of two different prophylactic dose regimens of low molecular weightprophylactic dose regimens of low molecular weight heparin in bariatric surgery. Obes Surg, 2002;12(1):19-24.
48.Miller MT, Rovito PF. An approach to venous thromboembolism prophylaxis in laparoscopic Roux-en-Y gastric bypass surgery. Obes Surg, 2004;14(6):731-7.
49.Cotter SA et al. Efficacy of venous thromboembolism prophylaxis in morbidly obese patients undergoing gastric bypass surgery. Obes Surg, 2005;15(9):1316-20.
50.Vaughan RW, Wise L. Postoperative arterial blood gas measurement in obese patients: effect of position on gas exchange. Ann Surg, 1975; 182(6):705-9.
51.Vaughan RW et al. Effect of position (semirecumbent versus supine) on postoperative oxygenation inversus supine) on postoperative oxygenation in markedly obese subjects. Anesth Analg, 1976; 55(1):37-41.
52.Hur HC et al. Incidence and patient characteristics of vaginal cuff dehiscence after different modes of hysterectomies. J Minim Invasive Gynecol, 2007;14(3):311.
67

53.Cronin B et al. Vaginal cuff dehiscence: risk factors and management. Am J Obstet Gynecol, 2012;206(4):284-8.
54.Kho RM et al. Incidence and characteristics of patients with vaginal cuff dehiscence after robotic procedures. Obstet Gynecol, 2009;114(2 Pt 1):231-5.
55.Uccella S et al. Vaginal cuff dehiscence in a series of 12 398 hysterectomies: effect of different types of12,398 hysterectomies: effect of different types of colpotomy and vaginal closure. Obstet Gynecol,2012;120(3):516-23.
56.Siedhoff MT et al. Decreased incidence of vaginal cuff dehiscence after laparoscopic closure with bidirectional barbed suture. J Minim Invasive Gynecol, 2011; 18:218.
68

CULTURAL AND LINGUISTIC COMPETENCY Governor Arnold Schwarzenegger signed into law AB 1195 (eff. 7/1/06) requiring local CME providers, such as
the AAGL, to assist in enhancing the cultural and linguistic competency of California’s physicians
(researchers and doctors without patient contact are exempt). This mandate follows the federal Civil Rights Act of 1964, Executive Order 13166 (2000) and the Dymally-Alatorre Bilingual Services Act (1973), all of which
recognize, as confirmed by the US Census Bureau, that substantial numbers of patients possess limited English proficiency (LEP).
California Business & Professions Code §2190.1(c)(3) requires a review and explanation of the laws
identified above so as to fulfill AAGL’s obligations pursuant to California law. Additional guidance is provided by the Institute for Medical Quality at http://www.imq.org
Title VI of the Civil Rights Act of 1964 prohibits recipients of federal financial assistance from
discriminating against or otherwise excluding individuals on the basis of race, color, or national origin in any of their activities. In 1974, the US Supreme Court recognized LEP individuals as potential victims of national
origin discrimination. In all situations, federal agencies are required to assess the number or proportion of LEP individuals in the eligible service population, the frequency with which they come into contact with the
program, the importance of the services, and the resources available to the recipient, including the mix of oral
and written language services. Additional details may be found in the Department of Justice Policy Guidance Document: Enforcement of Title VI of the Civil Rights Act of 1964 http://www.usdoj.gov/crt/cor/pubs.htm.
Executive Order 13166,”Improving Access to Services for Persons with Limited English
Proficiency”, signed by the President on August 11, 2000 http://www.usdoj.gov/crt/cor/13166.htm was the genesis of the Guidance Document mentioned above. The Executive Order requires all federal agencies,
including those which provide federal financial assistance, to examine the services they provide, identify any
need for services to LEP individuals, and develop and implement a system to provide those services so LEP persons can have meaningful access.
Dymally-Alatorre Bilingual Services Act (California Government Code §7290 et seq.) requires every
California state agency which either provides information to, or has contact with, the public to provide bilingual
interpreters as well as translated materials explaining those services whenever the local agency serves LEP members of a group whose numbers exceed 5% of the general population.
~
If you add staff to assist with LEP patients, confirm their translation skills, not just their language skills.
A 2007 Northern California study from Sutter Health confirmed that being bilingual does not guarantee competence as a medical interpreter. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2078538.
US Population
Language Spoken at Home
English
Spanish
AsianOther
Indo-Euro
California
Language Spoken at Home
Spanish
English
OtherAsianIndo-Euro
19.7% of the US Population speaks a language other than English at home In California, this number is 42.5%
69


















