AACE/ACE Conference Proceedings - American Association of ... · and Internal Medicine Universidad...
27
AACE/ACE Conference Proceedings TRANSCULTURALIZATION RECOMMENDA TIONS FOR DEVELOPING LATIN AMERICAN CLINICAL PRACTICE ALGORITHMS IN ENDOCRINOLOGY—PROCEEDINGS OF THE 2015 PAN-AMERICAN WORKSHOP BY THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS AND AMERICAN COLLEGE OF ENDOCRINOLOGY Jeffrey I. Mechanick, MD, FACP, FACE, FACN, ECNU, Chair 1 ; R. Mack Harrell, MD, FACP, FACE, ECNU 2 ; Myriam Z. Allende-Vigo, MD, MBA, FACP, FACE 3 ; Carlos Alvayero, MD 4 ; Onix Arita-Melzer MD 5 ; Pablo Aschner, MD, MSc 6 ; Pauline M. Camacho, MD, FACE 7 ; Rogelio Zacarias Castillo, MD 8 ; Sonia Cerdas, MD 9 ; Walmir F. Coutinho, MD, PhD 10 ; Jaime A. Davidson, MD, FACP, MACE 11 ; Jeffrey R. Garber, MD, FACP, FACE 12 ; W. Timothy Garvey, MD, FACE 13 ; Fernando Javier Lavalle González, MD 14 ; Denis O. Granados, MD 15 ; Osama Hamdy, MBBch, PhD 16 ; Yehuda Handelsman, MD, FACP, FACE, FNLA 17 ; Manuel Francisco Jiménez-Navarrete, MD 18 ; Mark A. Lupo, MD, FACE, ECNU 19 ; Enrique J. Mendoza, MD, MSc, FACP 20 ; José G. Jiménez-Montero, MD, FACE 21 ; Farhad Zangeneh, MD, FACP, FACE 22 From the 1 Clinical Professor of Medicine Director, Metabolic Support Division of Endocrinology, Diabetes, and Bone Disease Icahn School of Medicine at Mount Sinai, New York, NY; 2 Co-Director Memorial Center for Integrative Endocrine Surgery Hollywood, FL; 3 Professor of Medicine University of Puerto Rico School of Medicine, Director Endocrinology Section University Hospital San Juan Puerto Rico, President AACE Puerto Rico Chapter, San Juan, Puerto Rico; 4 Medical Director, Instituto Salvadoreño del Corazón, Unidad Diagnóstica de Osteoporosis, San Salvador, El Salvador; 5 Internal Medicine and Endocrinology, Education Program Director in Diabetes and Risk Factors, Thyroid and Diabetes Clinical Management Director, Hospital Bendaña, Honduras, CA; 6 Scientific Director, Colombian Diabetes Association, Professor Endocrinology and Clinical Epidemiology, Javeriana University and San Ignacio University Hospital, Bogotá, Colombia; 7 Professor of Medicine, Loyola University Medical Center, Director, Loyola University Osteoporosis and Metabolic Bone Disease Center, Maywood, IL; 8 Clinical Professor of Internal, Medicine Division of Internal Medicine, Hospital General “Dr. Manuel Gea González” México City, Mexico; 9 Division of Endocrinology, Hospital Cima Director of San Agustin Research Center San José, Costa Rica; 10 Catholic University of Rio de Janeiro, State Institute of Diabetes and Endocrinology; 11 Clinical Professor of Medicine, Touchstone Diabetes Center, The University of Texas Southwestern Medical Center Dallas. TX; 12 Endocrine Division, Harvard Vanguard Medical Associates, Division of Endocrinology, Beth Israel Deaconess Medical Center Boston, MA; 13 Department of Nutrition Sciences and the UAB Diabetes Research Center, University of Alabama at Birmingham, and The Birmingham Veterans Affairs Medical Center Birmingham, AL; 14 Professor, Faculty of Medicine, UANL: Nutrition, Endocrinology, Internal Medicine, Education Coordinator Endocrinology Service, Hospital Universitario, UANL, Head of the Diabetes Clinic of the Hospital Universitario “Dr. José E. González” UANL, Regional Hospital endocrinologist ISSSTE Monterrey, Policy Coordinating Group for Treatment of Diabetes in the Official Mexican Standar State Program Coordinator for Healthy Eating and Physical Activity Monterrey, Nuevo Leon, Mexico; 15 Internal Medicine and Endocrinology Hospital Alemán Nicaraguense Hospital Metropolitano Vivian Pellas, Professor Endocrinology and Internal Medicine Universidad Nacional Autónoma de Nicaragua Managua, Nicaragua; 16 Medical Director, Obesity Clinical Program, Director of Inpatient Diabetes Program, Joslin Diabetes Center, Harvard Medical School Boston, MA; 17 Medical Director & Principal Investigator, Metabolic Institute of America Tarzana, CA; 18 President Costa Rican Association of Endocrinologists (ANPEDEM), Professor Endocrinology and Internal Medicine, University of Costa Rica Coordinator Endocrinology Department, Hospital San Vicente de Paul, Costa Rica; 19 Medical Director, Thyroid & Endocrine Center of Florida Assistant Clinical Professor, Florida State University College of Medicine Sarasota, FL; 20 Full Professor of Biochemistry and Nutrition. Dean School of Medicine, University of Panama, Panama; 21 Professor of Medicine, Dean Post Graduate Studies, Universidad de Ciencias Médicas Head of the Division of Endocrinology Hospital CIMA, Escasu, San Jose, Costa Rica; 22 Consultant in Endocrinology Medical Director, Endocrine, Diabetes & Osteoporosis Clinic (EDOC) Sterling, VA. Address correspondence to American Association of Clinical Endocrinologists, 245 Riverside Avenue, Suite 200, Jacksonville, FL 32202. E-mail: [email protected]. DOI: 10.4158/EP161229.GL To purchase reprints of this article, please visit: www.aace.com/reprints. Copyright © 2016 AACE. 476 ENDOCRINE PRACTICE Vol 22 No. 4 April 2016
-
Upload
phungtuyen -
Category
Documents
-
view
218 -
download
0
Transcript of AACE/ACE Conference Proceedings - American Association of ... · and Internal Medicine Universidad...

AACE/ACE Conference Proceedings
TRANSCULTURALIZATION RECOMMENDATIONS
FOR DEVELOPING LATIN AMERICAN CLINICAL PRACTICE
ALGORITHMS IN ENDOCRINOLOGY—PROCEEDINGS OF
THE 2015 PAN-AMERICAN WORKSHOP BY
THE AMERICAN ASSOCIATION OF CLINICAL ENDOCRINOLOGISTS
AND AMERICAN COLLEGE OF ENDOCRINOLOGY
Jeffrey I. Mechanick, MD, FACP, FACE, FACN, ECNU, Chair1; R. Mack Harrell, MD, FACP, FACE, ECNU2; Myriam Z. Allende-Vigo, MD, MBA, FACP, FACE3;
Carlos Alvayero, MD4; Onix Arita-Melzer MD5; Pablo Aschner, MD, MSc6; Pauline M. Camacho, MD, FACE7; Rogelio Zacarias Castillo, MD8;
Sonia Cerdas, MD9; Walmir F. Coutinho, MD, PhD10; Jaime A. Davidson, MD, FACP, MACE11; Jeffrey R. Garber, MD, FACP, FACE12; W. Timothy Garvey, MD, FACE13;
Fernando Javier Lavalle González, MD14; Denis O. Granados, MD15; Osama Hamdy, MBBch, PhD16; Yehuda Handelsman, MD, FACP, FACE, FNLA17; Manuel Francisco Jiménez-Navarrete, MD18; Mark A. Lupo, MD, FACE, ECNU19; Enrique J. Mendoza, MD, MSc, FACP20; José G. Jiménez-Montero, MD, FACE21;
Farhad Zangeneh, MD, FACP, FACE22
From the 1Clinical Professor of Medicine Director, Metabolic Support Division of Endocrinology, Diabetes, and Bone Disease Icahn School of Medicine at Mount
Sinai, New York, NY; 2Co-Director Memorial Center for Integrative Endocrine Surgery Hollywood, FL; 3Professor of Medicine University of Puerto Rico School
of Medicine, Director Endocrinology Section University Hospital San Juan Puerto Rico, President AACE Puerto Rico Chapter, San Juan, Puerto Rico; 4Medical
Director, Instituto Salvadoreño del Corazón, Unidad Diagnóstica de Osteoporosis, San Salvador, El Salvador; 5Internal Medicine and Endocrinology, Education
Program Director in Diabetes and Risk Factors, Thyroid and Diabetes Clinical Management Director, Hospital Bendaña, Honduras, CA; 6Scientific Director,
Colombian Diabetes Association, Professor Endocrinology and Clinical Epidemiology, Javeriana University and San Ignacio University Hospital, Bogotá,
Colombia; 7Professor of Medicine, Loyola University Medical Center, Director, Loyola University Osteoporosis and Metabolic Bone Disease Center, Maywood,
IL; 8Clinical Professor of Internal, Medicine Division of Internal Medicine, Hospital General “Dr. Manuel Gea González” México City, Mexico; 9Division of
Endocrinology, Hospital Cima Director of San Agustin Research Center San José, Costa Rica; 10Catholic University of Rio de Janeiro, State Institute of Diabetes
and Endocrinology; 11Clinical Professor of Medicine, Touchstone Diabetes Center, The University of Texas Southwestern Medical Center Dallas. TX; 12Endocrine
Division, Harvard Vanguard Medical Associates, Division of Endocrinology, Beth Israel Deaconess Medical Center Boston, MA; 13Department of Nutrition
Sciences and the UAB Diabetes Research Center, University of Alabama at Birmingham, and The Birmingham Veterans Affairs Medical Center Birmingham, AL; 14Professor, Faculty of Medicine, UANL: Nutrition, Endocrinology, Internal Medicine, Education Coordinator Endocrinology Service, Hospital Universitario,
UANL, Head of the Diabetes Clinic of the Hospital Universitario “Dr. José E. González” UANL, Regional Hospital endocrinologist ISSSTE Monterrey, Policy
Coordinating Group for Treatment of Diabetes in the Official Mexican Standar State Program Coordinator for Healthy Eating and Physical Activity Monterrey,
Nuevo Leon, Mexico; 15Internal Medicine and Endocrinology Hospital Alemán Nicaraguense Hospital Metropolitano Vivian Pellas, Professor Endocrinology
and Internal Medicine Universidad Nacional Autónoma de Nicaragua Managua, Nicaragua; 16Medical Director, Obesity Clinical Program, Director of Inpatient
Diabetes Program, Joslin Diabetes Center, Harvard Medical School Boston, MA; 17Medical Director & Principal Investigator, Metabolic Institute of America
Tarzana, CA; 18President Costa Rican Association of Endocrinologists (ANPEDEM), Professor Endocrinology and Internal Medicine, University of Costa Rica
Coordinator Endocrinology Department, Hospital San Vicente de Paul, Costa Rica; 19Medical Director, Thyroid & Endocrine Center of Florida Assistant Clinical
Professor, Florida State University College of Medicine Sarasota, FL; 20Full Professor of Biochemistry and Nutrition. Dean School of Medicine, University of
Panama, Panama; 21Professor of Medicine, Dean Post Graduate Studies, Universidad de Ciencias Médicas Head of the Division of Endocrinology Hospital
CIMA, Escasu, San Jose, Costa Rica; 22Consultant in Endocrinology Medical Director, Endocrine, Diabetes & Osteoporosis Clinic (EDOC) Sterling, VA.
Address correspondence to American Association of Clinical Endocrinologists, 245 Riverside Avenue, Suite 200, Jacksonville, FL 32202.
E-mail: [email protected]. DOI: 10.4158/EP161229.GL
To purchase reprints of this article, please visit: www.aace.com/reprints.
Copyright © 2016 AACE.
476 ENDOCRINE PRACTICE Vol 22 No. 4 April 2016


Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 477
ABSTRACT
The American Association of Clinical Endocrinologists
(AACE) and American College of Endocrinology (ACE)
convened their first Workshop for recommendations to
optimize Clinical Practice Algorithm (CPA) development
for Latin America (LA) in diabetes (focusing on glycemic
control), obesity (focusing on weight loss), thyroid (focus-
ing on thyroid nodule diagnostics), and bone (focusing
on postmenopausal osteoporosis) on February 28, 2015,
in San Jose, Costa Rica. A standardized methodology is
presented incorporating various transculturalization fac-
tors: resource availability (including imaging equipment
and approved pharmaceuticals), health care professional
and patient preferences, lifestyle variables, socio-eco-
nomic parameters, web-based global accessibility, elec-
tronic implementation, and need for validation protocols.
A standardized CPA template with node-specific recom-
mendations to assist the local transculturalization process
is provided. Participants unanimously agreed on the fol-
lowing five overarching principles for LA: (1) there is only
one level of optimal endocrine care, (2) hemoglobin A1C
should be utilized at every level of diabetes care, (3) nutri-
tion education and increased pharmaceutical options are
necessary to optimize the obesity care model, (4) quality
neck ultrasound must be part of an optimal thyroid nodule
care model, and (5) more scientific evidence is needed on
osteoporosis prevalence and cost to justify intervention by
governmental health care authorities. This 2015 AACE/
ACE Workshop marks the beginning of a structured activ-
ity that assists local experts in creating culturally sensitive,
evidence-based, and easy-to-implement tools for opti-
mizing endocrine care on a global scale. (Endocr Pract.
2016;22:476-501)
Abbreviations:
A1C = glycated hemoglobin; AACE = American
Association of Clinical Endocrinologists; ACE =
American College of Endocrinology; BG = blood glu-
cose; BMI = body mass index; CPA = Clinical Practice
Algorithm; CPG = Clinical Practice Guideline; CVD
= cardiovascular disease; DXA = dual X-ray absorpti-
ometry; EDC = endocrine-disrupting compound; FBG
= fasting blood glucose; FNA = fine-needle aspiration;
HCP = health care professional; LA = Latin America;
PAACE = Pan-American AACE; SU = sulfonylurea;
T2D = type 2 diabetes; tDNA = transcultural Diabetes
Nutrition Algorithm; TSH = thyroid-stimulating hor-
mone; WC = waist circumference; WHO = World
Health Organization
INTRODUCTION
Evidence-based medicine has generated many philo-
sophical and pragmatic challenges to clinical care (1,2).
Chief among these challenges is how to deliver culturally
appropriate individualized endocrine care while adhering
with evidence-based guidelines and algorithms developed
for large heterogeneous populations. Management strate-
gies must therefore be adapted for individual patients within
single regions harboring different cultures (e.g., Mexican-
Americans and Asian-Americans in California), individual
patients in different regions harboring a common culture
(e.g., Latinos in Mexico and Latinos in the Dominican
Republic), or individual patients in different regions har-
boring many cultures (e.g., Asian Indians in India who are
Muslim, Hindu, Jain, or Sikh; urban or rural residents in
Mexico; or immigrant workers versus Emirati citizens in
the United Arab Emirates). Unfortunately, this challenge
has been largely ignored in clinical medicine, particularly
with respect to white papers (an authoritative report by [a]
specific organization[s] on a complex topic) that are prof-
fered for wide acceptance and anticipated implementation.
This white paper specifically addresses this challenge with
specific application to Latin America (LA).
To date, white papers in clinical medicine have not pro-
duced the high impact on quality of care that was expected,
even with formal implementation, validation efforts, and
the noblest of intentions. Potential reasons for this failure
range from burdensome time commitments for health care
professionals (HCPs) to lack of validation for different tar-
get populations. Another key factor in adapting evidence to
the individualized patient is context recognition—a critical
part of patient-centered decision-making (3,4). More spe-
cifically, virtually all white papers lack depth and relevance
in the way they relate to a multitude of different cultures,
both within and outside a target region. Indeed, virtually
any urban area in the U.S. contains a medley of cultures
that constitute a significant portion of any local American
medical practice.
Many experts and organizations define “culture” in
different ways, but a common thread is the clustering of
primarily nonphysical attributes distinguishing categories
of people (Table 1) (5-14). The clustering of only physi-
cal or genetic attributes common to a category of people
is more characteristic of “race,” whereas clustering that
incorporates not only culture and race, but also an empha-
sis on genealogy, ancestry, geography (region), linguistics,
and political ideology is characteristic of “ethnicity.” There
are obviously overlaps among culture, race, and ethnicity,
so for the purpose of clarity, culture will be referred to
in this document as the main classifier that distinguishes
different people around the world. Once culture is under-
stood, there are other related terms that should be defined.
Transculturalization describes the process of adapting
concepts from one culture to another, without changing
either culture. This is different than acculturation (changes
in culture that occur when two or more cultures interact),
deculturation (losing a previous culture), neoculturation
(creating a new culture), and transculturation (creation of
a new culture when two or more cultures merge). Thus,

478 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Table 1
Definitions of Culturea
Definition (paraphrased) Source
Symbolic, ideational, and intangible aspects of human societies Banks et al (5)
Shared patterns of behaviors and interactions, cognitive constructs, and affective
understanding learned through socialization
Center for Advanced Research on
Language Acquisition (6)
Learned and shared human patterns or models for living – a primary adaptive mechanism Damen et al (7)
Collective programming of the mind, which distinguishes members of one category of
people from another
Hofstede (8)
Historically created designs for living, explicit and implicit, rational, irrational, and
nonrational
Kluckholm et al (9)
Patterns, explicit and implicit, of and for behavior acquired and transmitted by symbols,
constituting the distinctive achievements of human groups
Kroeber et al (10)
Shared knowledge and schemes created by a set of people for perceiving, interpreting,
expressing, and responding to the social realities around them
Lederach et al (11)
Configuration of learned behaviors and results of behavior whose component elements are
shared and transmitted by a particular society
Linton et al (12)
Patterns relative to behavior and the products of human action, which may be inherited …
independent of the biological genes
Parson et al (13)
Learned and shared behavior of a community of interacting human beings Useem et al (14)
a Culture therefore incorporates socio-economic, knowledge and practice patterns, and politics.
the process of transculturalizing an evidence-based white
paper entails adaptation of rationale and generalized rec-
ommendations by accounting for cultural differences
between a document’s original source and the target region,
as well as differences among various cultures within the
target region. Additionally, the transculturalization process
does not pass judgment on a society’s culture or customs—
namely, there is no “right” or “wrong” since there is no
universal standard of morality (this concept is referred to
as “cultural relativism”) (15).
Cultural factors that affect health care include, among
others, gender roles, language barriers, personal space
orientations, attitudes toward food, nutrition, and physi-
cal activity, exposures to toxins and endocrine disruptors,
and socio-economics. For example, poverty—a socio-
economic descriptor—is associated with fatalism, need
for governmental aid, drug and alcohol abuse, dysfunc-
tional family life, low self-esteem, and community disen-
gagement. This can translate into increased risk for dis-
ease, more disease complications, longer recovery times,
impaired postillness function, and decreased access to
health care. Thus, culture here will query the multitudinous
layers of ethnic and regional factors in the context of opti-
mizing health care delivery, and more specifically, endo-
crine health. Even though the effect of cultural factors is
relatively easy to understand with respect to lifestyle modi-
fication, the consideration of region-specific political and
regulatory factors is much more complex and carries pro-
found implications with respect to technology deployment,
pharmaceutical development, and health care accessibility.
Latin culture is found in many of the Spanish-speaking
nations and has been adopted by many different ethnic
groups (Table 2) (16). The term “Latino” refers to those
of Latin American origin or ancestry, including Brazilians.
LA generally refers to South and Central America, as well
as Mexico, where the dominant language is Spanish or
Portuguese. Parenthetically, in some Central American
countries, such as Guatemala, a number of aboriginal
tongues are spoken, and in the Caribbean, African sub-
cultural and ethnic ancestries predominate, collectively
increasing population diversity. The term “Hispanic” is
an official U.S. census category and refers to those from
Spain and Spanish-speaking LA, but excludes Brazilians.
The term Hispanic therefore describes a culture, indepen-
dent of race, and a population smaller than Latinos (since
the population of Spain is smaller than the population of
Brazil). However, from a practical standpoint in the U.S.,
colloquial use of both Latino and Hispanic terms refer to
the same population.
The Latin culture is influenced by pre-Colombian,
European colonial, and later immigrant African and Asian
cultures. Primary components of the Latin culture include
the Spanish and Portuguese languages, Christian religion,
elements of the Constructivist Movement and Muralism in

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 479
art, various literary movements, positivism, diverse musi-
cal genres, experimental cinematography, traditional and
highly energetic dance styles, theater with historical con-
text, and a cuisine with typical foods (Table 3). Overall,
the diversity of the LA population imposes a challenge for
the development of a generalized approach to prevent and
treat chronic conditions, such as obesity and type 2 diabe-
tes (T2D). This concern has been successfully addressed
by integrating education, group support, and case manage-
ment for Hispanics with T2D (17,18), with notable success
when implemented in the workplace (19).
Biological drivers are not descriptors of culture per se.
However, there are several pathophysiologic mechanisms
that link certain cultures with higher risks for specific
chronic diseases and therefore deserve consideration when
transculturalizing clinical recommendations. For example,
one of these mechanisms is based on the mitochondrial
paradigm, championed by Wallace (20). In this paradigm,
the rapid mutational rate of mitochondrial DNA allows
energetics to quickly adapt to a changing environment.
This is exemplified by ancestral human migration from
Africa, through Europe and Asia, and subsequently into
colder (Northern) climes crossing the Bering Strait land
bridge into the Americas (20). The adaptive effect of colder
climes on mitochondrial regulation of energetics may now
be manifested by American aboriginal racial differences
Table 2
Latin American Socio-Economic and Ethnic Attributes by Countrya
Country
Pop.
(mill.)
LEB
(years)
GNI
($U.S.)
Urban
(%)
Illiteracy
(%)
Ethnicity
%C %N %M %B %O
Argentina 37 73 7,550 89 3 97 1 1 – 1
Bolivia 8 62 990 62 14 24 45 31 – –
Brazil 171 70 4,350 76 10 53 1 39 6 1
Chile 15 75 4,630 85 4 2 6 92 – –
Colombia 42 70 2,170 73 9 20 1 61 18 –
Costa Rica 4 76 3,570 47 5 33 1 60 3 3
Cuba 11 78 NA 77 4 37 – 51 1 1
Dominican Rep. 8 70 1,920 64 17 15 – 75 10 –
Ecuador 13 70 1,360 64 9 4 52 40 4 –
El Salvador 6 69 1,920 46 22 1 5 94 – –
Guatemala 11 64 1,680 39 32 8 45 45 1 1
Haiti 8 54 460 35 39 5 – – 95 –
Honduras 6 69 760 51 26 1 7 90 2 –
Mexico 99 72 4,440 74 9 10 10 80 – –
Nicaragua 5 68 410 55 32 17 9 69 5 –
Panama 3 74 3,080 56 8 10 8 66 10 6
Paraguay 5 69 1,560 55 7 3 2 95 – –
Peru 26 69 2,130 75 16 13 45 37 2 3
Uruguay 3 73 6,220 91 2 90 – 10 – –
Venezuela 24 73 3,680 86 8 20 1 61 18 –
Abbreviations: B = Black; C = Caucasian; GNI = gross national income in U.S. dollars per inhabitant; LEB = life expectancy at birth; M = Mestizo (combined European and Amerindian descent); N = Native American; NA = not available; O = Other; Pop. = population. a Countries in bold type were represented at the PAACE Workshop in 2015. Population figures are from 2000 and are provided for context at time when other information was collected (16).

480 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Table 3
Some Typical Foods in the Latin Culturea
Food Examples
Maize-based tortillas, tamales, pupusas
Salsas guacamole, pico de gallo, mole
Spices canela, epazote, cilantro, comino, laurel, tomillo
Fruits papaya, tuna (prickly pear; cactus fruit)
Root jicama
Meats carnitas, barbacoa, birria, cecina, suadero
mixiote, pibil, tortas (pan con carne)
Beverages mate, pisco sour, horchata, chichi, atole, cacao, posol, aguas frescas
a This is an incomplete list. Typical foods may have different names, preferences, preparation techniques, and nutritional values according to the specific Latin American country and region.
in glycemic status, adiposity and body composition, lipid
metabolism, and consequent cardiovascular disease (CVD)
risk (20). Thus, identification of mitochondrial haplotypes
in specific cultures and subcultures (distinct groups within
a culture) in LA could theoretically assist with disease risk
assessment and targeted therapy (an example of “precision
medicine”). Another underrecognized driver of chronic
disease in LA, especially metabolic disorders such as T2D
and obesity, are the genotoxic and molecular effects of
endocrine-disrupting compounds (EDCs) (21) and pollut-
ants (22,23), including artificial sweeteners, which can act
through taste receptors in the intestine that modulate the
microbiome, entero-insular axis, and appetite (24). Lastly,
an allostatic load model of stress and physiologic dys-
regulation may be an attractive hypothesis for a metabolic
disease driver in LA, though Gersten et al (25) analyzed
cross-sectional survey data and were unable to identify sta-
tistically significant associations among life stressors and
neuroendocrine biomarkers.
In 2010, the transcultural Diabetes Nutrition Algorithm
(tDNA) program was initiated to address a specific need:
to provide evidence-based and detailed nutritional infor-
mation for the HCP caring for patients with T2D on a
global scale, based on the premise that diverse cultures
contributed to different disease expressions. This was in
response to the growing global diabetes and obesity epi-
demics and a lack of accessible and/or implemented evi-
dence-based nutritional information for T2D, particularly
in the most heavily affected regions, such as LA, India,
Southeast Asia, and the Persian Gulf. The Clinical Practice
Algorithm (CPA; 26) format was favored in the tDNA pro-
gram over other lengthy and text-heavy Clinical Practice
Guideline (CPG) formats in order to improve the likeli-
hood of acceptance and implementation in diverse cultural
settings. Following a sequence of multiple tDNA summits
with didactic lectures and small breakout sessions, conven-
ing key opinion leaders in LA, North America, Europe, the
Persian Gulf, India, China, and Southeast Asia, a series of
papers was published from 5 diverse regions (27-33), as
well as a methods description (34) and a content validation
(35).
To provide context for the imperative to globalize
key medical recommendations, the following chronology
is offered. In 2006, the General Assembly of the United
Nations adopted resolution A/RES/61/225, which recog-
nized diabetes as a chronic, debilitating, and costly disease
and established World Diabetes Day (36). In 2011, the
General Assembly of the United Nations adopted resolu-
tion A/RES/66/2, a political declaration bringing the global
health problem on noncommunicable diseases, including
diabetes and obesity, into sharp focus (37). The immedi-
ate ramifications of this latter declaration were calls for
policy reform and scalability to address high-need areas,
especially in lower socio-economic regions (38), as well
as ethnic minorities in higher socio-economic regions (39).
Most recently, in September 2015, the issue of noncom-
municable diseases was included in the United Nations
Sustainable Development Summit, further advancing a
global commitment to diabetes care (40).
In 2014, the American Association of Clinical
Endocrinologists (AACE) and American College of
Endocrinology (ACE) began planning a Pan-American
AACE (PAACE) Conference. A Workshop was appended
to the PAACE conference in San Jose, Costa Rica, to iden-
tify transcultural attributes and challenges for local devel-
opment of 4 LA CPAs consistent with existing AACE/
ACE white papers (CPG, CPA, and other position papers
and conference proceedings). In early 2015, AACE/ACE
initiated efforts to promote the development, distribution,
and validation of current and future transculturalizations
of white papers on endocrine disease management. The
goal of these activities is to assist experts and professional
societies from both within and outside the U.S. to develop
white papers that are culturally sensitive and applicable to
the broad cultural array of patients found in their clinical
practices.
Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 481
This document represents the results of the 2015
AACE/ACE workshop in which culturally and region-
ally sensitive recommendations are provided for subse-
quent local LA CPA production. These recommendations
incorporate nuance- and evidence-based suggestions for
enhancement of patient care oriented to individual nodes
in a CPA. Furthermore, these results provide content for
education, hypothesis generation for research, and local
LA CPA production in local markets.
METHODS
Preworkshop Development
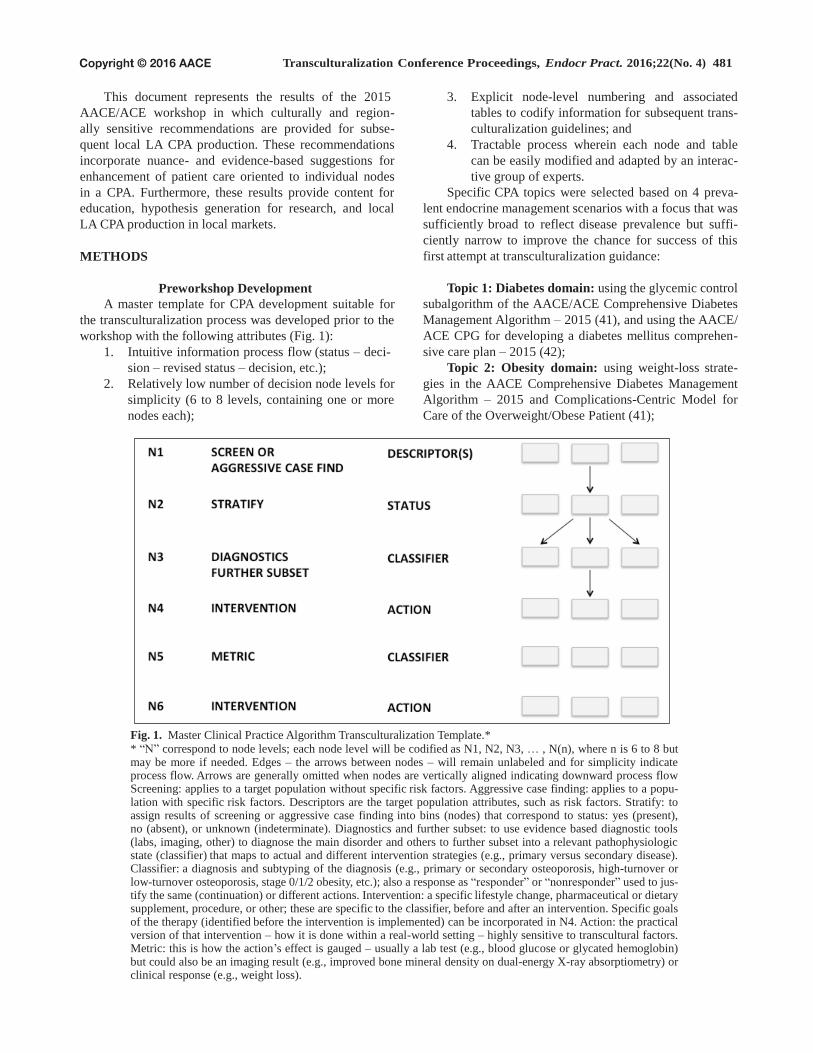
A master template for CPA development suitable for
the transculturalization process was developed prior to the
workshop with the following attributes (Fig. 1):
1. Intuitive information process flow (status – deci-
sion – revised status – decision, etc.);
2. Relatively low number of decision node levels for
simplicity (6 to 8 levels, containing one or more
nodes each);
3. Explicit node-level numbering and associated
tables to codify information for subsequent trans-
culturalization guidelines; and
4. Tractable process wherein each node and table
can be easily modified and adapted by an interac-
tive group of experts.
Specific CPA topics were selected based on 4 preva-
lent endocrine management scenarios with a focus that was
sufficiently broad to reflect disease prevalence but suffi-
ciently narrow to improve the chance for success of this
first attempt at transculturalization guidance:
Topic 1: Diabetes domain: using the glycemic control
subalgorithm of the AACE/ACE Comprehensive Diabetes
Management Algorithm – 2015 (41), and using the AACE/
ACE CPG for developing a diabetes mellitus comprehen-
sive care plan – 2015 (42);
Topic 2: Obesity domain: using weight-loss strate-
gies in the AACE Comprehensive Diabetes Management
Algorithm – 2015 and Complications-Centric Model for
Care of the Overweight/Obese Patient (41);
Fig. 1. Master Clinical Practice Algorithm Transculturalization Template.*
* “N” correspond to node levels; each node level will be codified as N1, N2, N3, … , N(n), where n is 6 to 8 but may be more if needed. Edges – the arrows between nodes – will remain unlabeled and for simplicity indicate process flow. Arrows are generally omitted when nodes are vertically aligned indicating downward process flow Screening: applies to a target population without specific risk factors. Aggressive case finding: applies to a popu- lation with specific risk factors. Descriptors are the target population attributes, such as risk factors. Stratify: to assign results of screening or aggressive case finding into bins (nodes) that correspond to status: yes (present), no (absent), or unknown (indeterminate). Diagnostics and further subset: to use evidence based diagnostic tools (labs, imaging, other) to diagnose the main disorder and others to further subset into a relevant pathophysiologic state (classifier) that maps to actual and different intervention strategies (e.g., primary versus secondary disease). Classifier: a diagnosis and subtyping of the diagnosis (e.g., primary or secondary osteoporosis, high-turnover or low-turnover osteoporosis, stage 0/1/2 obesity, etc.); also a response as “responder” or “nonresponder” used to jus- tify the same (continuation) or different actions. Intervention: a specific lifestyle change, pharmaceutical or dietary supplement, procedure, or other; these are specific to the classifier, before and after an intervention. Specific goals of the therapy (identified before the intervention is implemented) can be incorporated in N4. Action: the practical version of that intervention – how it is done within a real-world setting – highly sensitive to transcultural factors. Metric: this is how the action’s effect is gauged – usually a lab test (e.g., blood glucose or glycated hemoglobin) but could also be an imaging result (e.g., improved bone mineral density on dual-energy X-ray absorptiometry) or clinical response (e.g., weight loss).

482 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Topic 3: Thyroid domain: using the AACE thyroid
nodule algorithm for electronic implementation (43); and
Topic 4: Bone domain: using the most recent post-
menopausal osteoporosis clinical practice guideline (44).
AACE Scientific Committees provided updated scien-
tific materials. Preliminary disease-specific CPA templates
(Fig. 2 through 5) were developed in adherence with the
master CPA template. The templates were then distributed
to AACE/ACE workshop participants with instructions to
provide their thoughts regarding transculturalizing each
node and table for use among those patients residing in LA.
Following receipt of these vetted algorithms from work-
shop participants, a preworkshop syllabus and PowerPoint
presentation were created and distributed for on-site use
during the AACE/ACE workshop. Iterative preworkshop
revisions were performed based on participant feedback for
each CPA domain until a general consensus was reached
(modified Delphi method; 45).
2015 Workshop Proceedings
The purpose of the 2015 AACE/ACE workshop was
to allow an opportunity for face-to-face discussion of
culturally and regionally sensitive node-specific recom-
mendations to assist local transculturalization efforts. The
Workshop was conducted on Saturday, February 28, 2015,
from 7 am to 1 pm at The Intercontinental Hotel in San Jose,
Costa Rica. Following introductions of participants (Table
4), J.M. presented introductory material on transcultural
endocrinology and then the CPA templates. Next, each of
the specific endocrine disease management CPAs was pre-
sented: diabetes (Y.H.), obesity (J.M.), thyroid (R.M.H.),
and bone (P.C.).
The Workshop participants reached consensus on 5
overarching principles during the CPA discussions.
1. There is only one level of optimal endocrine care
for LA: the participants rejected the notion that
there should be separate private and public levels
of care for high and low socio-economic classes,
respectively. Realistically, the one target level of
care is viewed as “excellent,” but within the con-
text of feasibility.
2. All patients with suspected prediabetes or dia-
betes should have a glycated hemoglobin (A1C)
measurement as part of the initial evaluation
and, if the diagnosis is confirmed, to have A1C
measurements with follow-up: the participants
recognized that there are problems with accessi-
bility and affordability of a reliable A1C assay but
agreed that this test was an absolutely necessary
part of an optimal diabetes care plan.
Table 4
Participants at the 2015 AACE/ACE Workshop
Name Country
Jeffrey I. Mechanick, MD (J.M.) USA (Chairperson)
Carlos Alvayero, MD (C.A.) El Salvador
Onix Arita-Melzer, MD (O.A.) Honduras
Pablo Aschner Montoya, MD (P.A.M.) Colombia
Myriam Z. Allende-Vigo, MD (M.A.V.) USA
Ruth Báez, MD (R.B.) Dominican Republic
Pauline M. Camacho, MD (P.C.) USA
Sonia Cerdas Perez, MD (S.C.P.) Costa Rica
Manuel Cigarruista, MD (M.C.) Panama
Walmir F. Coutinho, MD (W.C.) Brazil
Jaime A. Davidson, MD (J.D.) USA
Felix Escano, MD (F.E.) Dominican Republic
Yehuda Handelsman, MD (Y.H.) USA
R. Mack Harrell, MD (R.M.H.) USA
Manuel Jiménez, MD (M.J.) Costa Rica
Jose G. Jimenez-Montero, MD (J.J.M.) Costa Rica
Fernando Javier Lavalle González, MD (F.L.G.) Mexico
Denis Granados, MD (D.G.) Nicaragua
Mark Lupo, MD (M.L.) USA
Enrique Jorge Mendoza, MD (E.J.M.) Panama
Jorge Hector Mestman, MD (J.H.M.) USA
Rogelio Zacarias Castillo, MD (R.Z.C.) Mexico
Farhad Zangeneh, MD (F.Z.) USA

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 483
3. Nutritional education and more pharmacologic
options are necessary to optimize the obesity care
model: the participants recognized that inertia in
creating a successful comprehensive obesity care
model was due to a conspicuous lack of effective
nutritional education and pharmacologic options.
4. Optimal thyroid nodule evaluation and manage-
ment must employ neck ultrasound: although
the participants recognized the low availability of
neck ultrasound in many LA regions, this tech-
nology, at a sufficiently high level of quality, was
deemed necessary for early and accurate diagno-
sis and follow-up of thyroid nodule pathology.
5. More scientific data on bone loss in LA is needed
to prompt governmental policy supporting the
highest standard of osteoporosis care: the partic-
ipants agreed that there is a paucity of evidence,
particularly from LA, on bone loss, the use of
dual X-ray absorptiometry (DXA), biochemical
testing, lifestyle, and pharmacologic intervention,
and in addition, that presentation of this evidence
could lead to governmental actions to raise the
level of osteoporosis screening and care.
The proceedings were translated (Spanish to English;
English to Spanish) in real-time for all participants, and
then translated transcripts were provided for document
preparation. In addition, at the conclusion of the workshop,
each participant provided his or her handwritten notes and
feedback for translation and document preparation.
Postworkshop Development
Following the 2015 AACE/ACE workshop, all com-
ments were reviewed and incorporated into a revised
document with further writing and reviewing assignments
sent to participant teams. A final document was produced
after several iterations of review/revision by primary
writers, expert reviewers, and the ACE Transcultural
Endocrinology Task Force and then approvals by the
AACE Executive Committee, AACE Board of Directors,
and ACE Board of Trustees. This document will be ini-
tially published in English with the intent to translate into
Spanish and is available free of charge through LA AACE
chapters as well as by posting on the AACE website (www.
aace.com). This plan is designed to maximize dissemina-
tion of information.
The objective for this effort is to provide recommen-
dations for local experts to subsequently develop their own
local, culturally and regionally sensitive, evidence-based
CPAs, consistent with existing AACE/ACE white papers.
General Recommendations
AACE/ACE white papers, and CPAs in particular,
must conform to the following rules, which are also rec-
ommended for the production of local LA CPAs:
1. Experts must have scientific credibility in the
topic being addressed;
2. Disclosures of multiplicities of interest must
be preliminarily obtained, with the intention of
including experts without a true conflict of inter-
est that could mitigate objective participation (as
evaluated by the writing committee Chair and
appropriate AACE/ACE committees);
3. There is no industry involvement with produc-
tion, including but not limited to, funding, con-
sulting, review, and commentary;
4. Full commitment of the writing committee to
complete assignments on time and in conformity
with the Chair’s instructions is essential;
5. Writing must be completed in a reasonable time
(less than 6 to 12 months);
6. Information is constrained to a specific and rel-
evant clinical question or problem;
7. Commitment to an evidence-based methodology
is imperative, with
a. Transparency;
b. Middle-range literature searching
(between overly generalized reviews and
overly specific case reports);
c. Incorporation of subjective factors;
d. Incorporation of patient-oriented evi-
dence that matters (“POEM;” i.e., clini-
cally relevant, instead of exclusively dis-
ease-oriented evidence); and
e. Recommendation cascades are the pre-
ferred outputs (providing alternatives for
diagnostics and therapeutics);
8. A formal multi-level review process is used (writ-
ers, reviewers, committees, boards, etc.); and
9. CPAs are created with development of electronic
implementation, performance metrics, and valida-
tion studies in mind (1,2,26).
Specific Node-Specific Recommendations
There are broad categories of LA transculturalization
factors (31-33) that can be used in node-by-node analyses
of Figures 2 through 5:
• anthropometrics;
• food sourcing and accessibility, culinary styles,
and eating patterns;
• physical activity,
• tobacco and alcohol use;
• psychological stress and personal behavior;
• use of dietary supplements and nutraceuticals;
• exposure to EDCs and pollutants;
• local health care practices and attitudes;
• public advocacy programs;
• medical school curricula and clinical research
methodologies;
• structure and financing of health care systems;
484 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
• family and community engagement;
• accessibility to health care (with or without the
use of technology);
• governmental policy and politics; and
• socio-economic factors.
General information is provided for each endocrine
domain (Fig. 2 through 5). Core recommendations are pro-
vided for each endocrine domain and node level (N1, N2,
N3, … , N6-8).
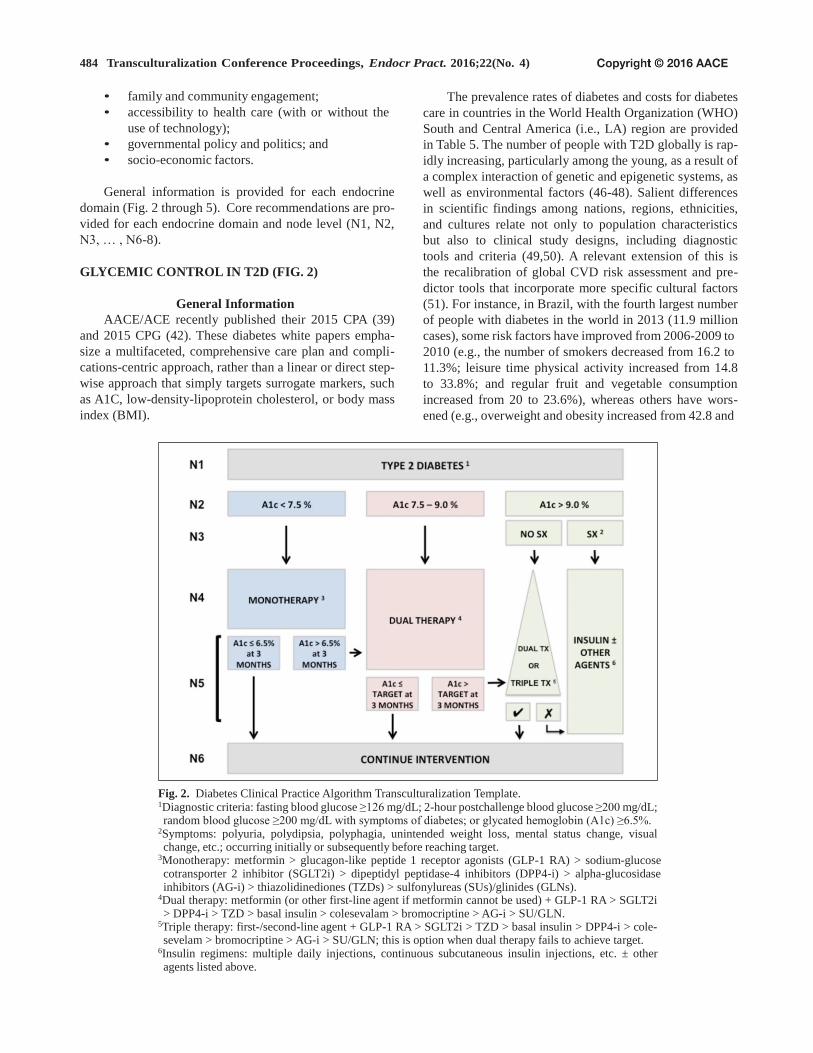
GLYCEMIC CONTROL IN T2D (FIG. 2)
General Information
AACE/ACE recently published their 2015 CPA (39)
and 2015 CPG (42). These diabetes white papers empha-
size a multifaceted, comprehensive care plan and compli-
cations-centric approach, rather than a linear or direct step-
wise approach that simply targets surrogate markers, such
as A1C, low-density-lipoprotein cholesterol, or body mass
index (BMI).
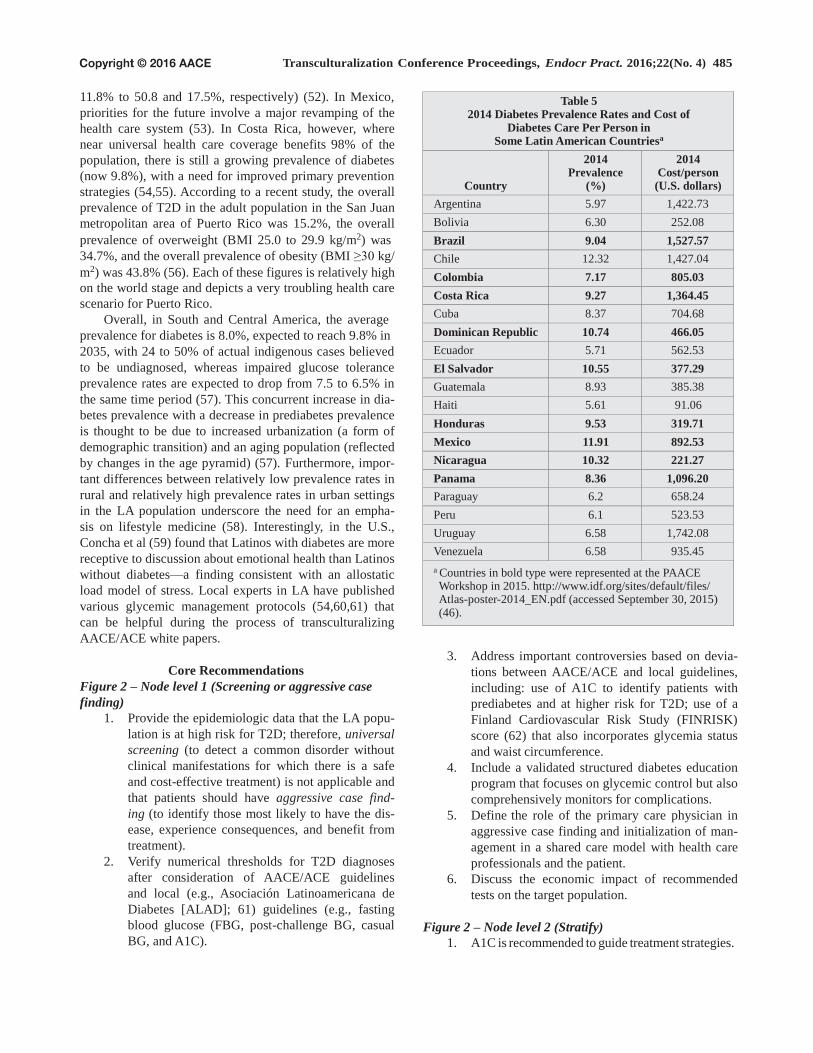
The prevalence rates of diabetes and costs for diabetes
care in countries in the World Health Organization (WHO)
South and Central America (i.e., LA) region are provided
in Table 5. The number of people with T2D globally is rap-
idly increasing, particularly among the young, as a result of
a complex interaction of genetic and epigenetic systems, as
well as environmental factors (46-48). Salient differences
in scientific findings among nations, regions, ethnicities,
and cultures relate not only to population characteristics
but also to clinical study designs, including diagnostic
tools and criteria (49,50). A relevant extension of this is
the recalibration of global CVD risk assessment and pre-
dictor tools that incorporate more specific cultural factors
(51). For instance, in Brazil, with the fourth largest number
of people with diabetes in the world in 2013 (11.9 million
cases), some risk factors have improved from 2006-2009 to
2010 (e.g., the number of smokers decreased from 16.2 to
11.3%; leisure time physical activity increased from 14.8
to 33.8%; and regular fruit and vegetable consumption
increased from 20 to 23.6%), whereas others have wors-
ened (e.g., overweight and obesity increased from 42.8 and
Fig. 2. Diabetes Clinical Practice Algorithm Transculturalization Template. 1Diagnostic criteria: fasting blood glucose ≥126 mg/dL; 2-hour postchallenge blood glucose ≥200 mg/dL; random blood glucose ≥200 mg/dL with symptoms of diabetes; or glycated hemoglobin (A1c) ≥6.5%.
2Symptoms: polyuria, polydipsia, polyphagia, unintended weight loss, mental status change, visual change, etc.; occurring initially or subsequently before reaching target.
3Monotherapy: metformin > glucagon-like peptide 1 receptor agonists (GLP-1 RA) > sodium-glucose cotransporter 2 inhibitor (SGLT2i) > dipeptidyl peptidase-4 inhibitors (DPP4-i) > alpha-glucosidase inhibitors (AG-i) > thiazolidinediones (TZDs) > sulfonylureas (SUs)/glinides (GLNs).
4Dual therapy: metformin (or other first-line agent if metformin cannot be used) + GLP-1 RA > SGLT2i > DPP4-i > TZD > basal insulin > colesevalam > bromocriptine > AG-i > SU/GLN.
5Triple therapy: first-/second-line agent + GLP-1 RA > SGLT2i > TZD > basal insulin > DPP4-i > cole- sevelam > bromocriptine > AG-i > SU/GLN; this is option when dual therapy fails to achieve target.
6Insulin regimens: multiple daily injections, continuous subcutaneous insulin injections, etc. ± other agents listed above.
Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 485
11.8% to 50.8 and 17.5%, respectively) (52). In Mexico,
priorities for the future involve a major revamping of the
health care system (53). In Costa Rica, however, where
near universal health care coverage benefits 98% of the
population, there is still a growing prevalence of diabetes
(now 9.8%), with a need for improved primary prevention
strategies (54,55). According to a recent study, the overall
prevalence of T2D in the adult population in the San Juan
metropolitan area of Puerto Rico was 15.2%, the overall
prevalence of overweight (BMI 25.0 to 29.9 kg/m2) was
34.7%, and the overall prevalence of obesity (BMI ≥30 kg/
m2) was 43.8% (56). Each of these figures is relatively high
on the world stage and depicts a very troubling health care
scenario for Puerto Rico.
Overall, in South and Central America, the average
prevalence for diabetes is 8.0%, expected to reach 9.8% in
2035, with 24 to 50% of actual indigenous cases believed
to be undiagnosed, whereas impaired glucose tolerance
prevalence rates are expected to drop from 7.5 to 6.5% in
the same time period (57). This concurrent increase in dia-
betes prevalence with a decrease in prediabetes prevalence
is thought to be due to increased urbanization (a form of
demographic transition) and an aging population (reflected
by changes in the age pyramid) (57). Furthermore, impor-
tant differences between relatively low prevalence rates in
rural and relatively high prevalence rates in urban settings
in the LA population underscore the need for an empha-
sis on lifestyle medicine (58). Interestingly, in the U.S.,
Concha et al (59) found that Latinos with diabetes are more
receptive to discussion about emotional health than Latinos
without diabetes—a finding consistent with an allostatic
load model of stress. Local experts in LA have published
various glycemic management protocols (54,60,61) that
can be helpful during the process of transculturalizing
AACE/ACE white papers.
Core Recommendations
Figure 2 – Node level 1 (Screening or aggressive case
finding)
1. Provide the epidemiologic data that the LA popu-
lation is at high risk for T2D; therefore, universal
screening (to detect a common disorder without
clinical manifestations for which there is a safe
and cost-effective treatment) is not applicable and
that patients should have aggressive case find-
ing (to identify those most likely to have the dis-
ease, experience consequences, and benefit from
treatment).
2. Verify numerical thresholds for T2D diagnoses
after consideration of AACE/ACE guidelines
and local (e.g., Asociación Latinoamericana de
Diabetes [ALAD]; 61) guidelines (e.g., fasting
blood glucose (FBG, post-challenge BG, casual
BG, and A1C).
Table 5 2014 Diabetes Prevalence Rates and Cost of
Diabetes Care Per Person in Some Latin American Countriesa
Country
2014 Prevalence
(%)
2014 Cost/person
(U.S. dollars)
Argentina 5.97 1,422.73
Bolivia 6.30 252.08
Brazil 9.04 1,527.57
Chile 12.32 1,427.04
Colombia 7.17 805.03
Costa Rica 9.27 1,364.45
Cuba 8.37 704.68
Dominican Republic 10.74 466.05
Ecuador 5.71 562.53
El Salvador 10.55 377.29
Guatemala 8.93 385.38
Haiti 5.61 91.06
Honduras 9.53 319.71
Mexico 11.91 892.53
Nicaragua 10.32 221.27
Panama 8.36 1,096.20
Paraguay 6.2 658.24
Peru 6.1 523.53
Uruguay 6.58 1,742.08
Venezuela 6.58 935.45
a Countries in bold type were represented at the PAACE Workshop in 2015. http://www.idf.org/sites/default/files/ Atlas-poster-2014_EN.pdf (accessed September 30, 2015) (46).
3. Address important controversies based on devia-
tions between AACE/ACE and local guidelines,
including: use of A1C to identify patients with
prediabetes and at higher risk for T2D; use of a
Finland Cardiovascular Risk Study (FINRISK)
score (62) that also incorporates glycemia status
and waist circumference.
4. Include a validated structured diabetes education
program that focuses on glycemic control but also
comprehensively monitors for complications.
5. Define the role of the primary care physician in
aggressive case finding and initialization of man-
agement in a shared care model with health care
professionals and the patient.
6. Discuss the economic impact of recommended
tests on the target population.
Figure 2 – Node level 2 (Stratify)
1. A1C is recommended to guide treatment strategies.
486 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
2. Consider other A1C cutoffs (e.g., 7 to 8%) sup-
ported by local epidemiologic evidence that cor-
relates with complication risk (61).
3. If unable to check A1C due to cost, availability, or
reliability, management can be indexed to a BG
metric (e.g., BG <140 mg/dL; 141 to 250 mg/dL;
and >250 mg/dL) as long as supportive data can
be provided.
Figure 2 – Node level 3 (Diagnostics and further subset
classification)
1. Recognize that A1C is not an absolute criterion
to start insulin and that the presence or absence
of symptoms may be a better indicator to start
insulin.
2. If an A1C is not available, then a very elevated
BG (e.g., >250 mg/dL; fasting, postprandial, or
random) and the presence of symptoms may be a
suitable indicator to start insulin.
3. Consider a more specific process for individu-
alization of risk stratification based on other
lifestyle or biological factors associated with
increased risk of diabetes-related complications.
Figure 2 – Node level 4 (Intervention)
1. Initiate lifestyle interventions for all patients:
this may be provided by the primary care physi-
cian, diabetes educator alone or in group sessions,
and/or the endocrinologist and should emphasize
caloric reduction if overweight/obese, as well
behavioral medicine and emotional health.
2. Provide recommendations for culturally sensitive
foods, meal planning, and healthy eating (Table
6).
3. Provide recommendations for culturally sensitive
physical activity and sports.
4. Where appropriate, discuss and provide evi-
dence for siesta breaks (short afternoon nap-
ping) in the framework of healthy sleep hygiene,
healthy eating, and synchronization with diabetes
medications.
5. Emphasize the use of diabetes educators.
6. Monotherapy is with metformin (unless contra-
indicated or poor tolerance anticipated); if not
metformin, then incretin-based or sodium-glu-
cose cotransporter 2 agents.
7. Do not recommend adding a sulfonylurea (SU) to
metformin unless there are no other options avail-
able and/or cost issues, and if SUs are added, (1)
educate regarding hypoglycemia, and (2) specify
which SUs are recommended and the reasons.
8. Triple therapy is generally not recommended
initially.
9. Insulinization is reserved for patients who are
poorly controlled and symptomatic despite
attempts to control with appropriate noninsulin
therapies; however, insulinization may need to
be introduced earlier if no other add-on therapy is
available or affordable.
10. Consider elements of ALAD guidelines (61).
11. Include a listing of available medications and cost
analysis for pharmacotherapy options.
12. Provide a detailed insulin management protocol
using available insulin preparations and consis-
tent with current guidelines (41,42).
Figure 2 – Node level 5 (Metric)
1. Specify LA A1C targets, and if they are different
from the <6.5% (or at least <7%) range by 3 to 6
months, provide the reasons and evidence.
2. Specify weight loss targets if overweight/obese.
3. Specify any other targets relevant to glycemic
control.
Figure 2 – Node level 6 (Follow-up intervention)
1. Continue to follow flow from monotherapy to
dual therapy to triple therapy and insulin add-ons,
as needed, depending on initial risk stratifica-
tion, response to therapy, and whether the target
is achieved. Acceleration of management should
not be longer than every 3 months.
2. Provide individualized glycemic targets, interven-
tions, and strategies incorporating comprehensive
management plans.
WEIGHT LOSS IN OVERWEIGHT AND
OBESITY (FIG. 3)
General Information
Overweight and obesity are risk factors and patho-
physiologic drivers for the development of T2D and CVD.
With global obesity prevalence rates failing to decline and
actually worsening in certain groups, such as children, eth-
nic minorities, lower socio-economic classes, and more
severely obese, among others, new paradigms of anti-obe-
sity management must be considered. In 2012, AACE pub-
lished a position paper on Obesity and Obesity Medicine
calling for greater collaboration among stakeholders (63),
authored and successfully advocated for the passage of
the 2013 American Medical Association resolution 420
“Resolution of Obesity as a Disease” (64), organized a
2014 Consensus Conference on Obesity to build an evi-
dence base (65), and produced a 2014 advanced framework
for a new diagnosis of obesity based on a complications-
centric chronic disease model (66). However, similar to
the above AACE/ACE diabetes white papers, there were
minimal culturally sensitive specific recommendations.
This needs to be addressed, not only for Latinos in their
native countries, but also for optimal management of the
U.S. Latino population (67,68).

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 487
According to the WHO, as of January 2015, the global
obesity prevalence rate has doubled since 1980, and most
people live in areas of the world where mortality rates
from overweight/obesity exceed those from undernutrition
(69). The highest obesity prevalence rates are in Tonga,
Nauru, and the Cook islands (>60%), with China and the
U.S. harboring the greatest increased rates, followed by
Brazil and Mexico (70). The greatest increase in obesity
among women is in South and Central America (LA) and
also Oceania (70). Moreover, in low- and middle-income
countries, many of which are represented in LA, waist cir-
cumference (WC) has increased roughly 2 to 4 cm since
the early 1990s at the same BMI (>25 kg/m2), suggesting
even further increased cardiometabolic risk (71).
In a 2006 study, the prevalence of increased WC in
Mexico ranged from 42.7 to 74.2% depending on the
definition by ATPIII, AHA/NHLBI, or the International
Diabetes Federation (72), with an overall prevalence of
overweight/obesity based on a BMI ≥25 kg/m2 of 71.2%
(73). In another study from 2011, the WC cutoffs that cor-
relate with visceral adipose tissue in LA are comparable to
those for europids (European Caucasians; 94 cm for men;
90 to 92 cm for women) and effectively identify individu-
als with a strong genetic predisposition for insulin resis-
tance (74). Pediatric overweight/obesity is also an iden-
tifiable driver for adult overweight/obesity in LA, with a
prevalence rate of 18.9 to 36.9% in children age 5 to 11
years and 16.6 to 35.8% in adolescents age 12 to 19 years
(75). A summary of obesity/overweight prevalence rates in
Latin American countries is provided in Table 7 (76,77).
Among the set of WHO global targets to combat non-
communicable diseases, the rise in diabetes and obesity
must be halted (78). In fact, decreasing the obesity preva-
lence rate by as little as 1% in Brazil—where it is estimated
Table 6
Healthy Eating Recommendations for Type 2 Diabetesa
Topic Recommendation
General eating habits
Eat regular meals and snacks; avoid fasting to lose weight
Consume plant-based diet (high in fiber, low calories/glycemic index, and high in
phytochemicals/antioxidants)
Understand Nutrition Facts Label information
Incorporate beliefs and culture into discussions
Use mild cooking techniques instead of high-heat cooking
Use meal and/or snack replacements as needed
Keep physician-patient discussions informal
Carbohydrate
Explain the 3 types of carbohydrates—sugars, starch, and fiber—and the effects on
health for each type
Specify healthful carbohydrates (fresh fruits and vegetables, legumes, whole grains);
target 7-10 servings per day
Lower-glycemic index foods may facilitate glycemic control (glycemic index score
<55 out of 100: multigrain bread, pumpernickel bread, whole oats, legumes, apple,
lentils, chickpeas, mango, yams, brown rice), but there is insufficient evidence
to support a formal recommendation to educate patients that sugars have either
positive and negative health effects
Fat
Specify healthful fats (low mercury/contaminant-containing nuts, avocado, certain
plant oils [e.g., olive oil], fish)
Limit saturated fats (butter, fatty red meats, tropical plant oils [e.g., coconut and palm
oils], fast foods) and trans fat; choose fat-free or low-fat dairy products
Protein
Consume protein in foods with low saturated fats (fish, egg whites, beans); there is no
need to avoid animal protein
Avoid or limit processed meats
Micronutrients
Routine supplementation is not necessary; a healthful eating meal plan can generally
provide sufficient micronutrients
Specifically, chromium; vanadium; magnesium; vitamins A, C, and E; and CoQ10 are
not recommended for glycemic control
Vitamin supplements should be recommended to patients at risk of insufficiency or
deficiency
a See reference 42.

488 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Fig. 3. Obesity Clinical Practice Algorithm Transculturalization Template. Refer to AACE/ACE advanced framework for comprehensive overweight/obesity management (66). BMI = body mass index; WRC = weight-related complication.
that by 2050, 95% of males will be overweight or obese—
will reduce the prevalence of CVD, stroke, hypertension,
cancer, osteoarthritis, and/or T2D by 800 per 100,000 and
reduce projected 2050 health care costs from $330 billion
to $302 billion (79).
There are many dimensions to the obesity problem in
LA other than clinical health, wellness, and disease pre-
vention. Although there is considerable heterogeneity in
lifestyle among the various LA regions and cultures, the
impact of food insecurity (lack of access to sufficient food
for an active healthy life; 80), double-burden of under-
and overnutrition (81), and nutrition transition (changes
in eating patterns [e.g., more refined high-calorie foods;
less fresh fruits, vegetables, and grains]; 82) is significant.
Moreover, the obesity problem not only affects the health
of the LA population, it also increases the economic burden
due to health care costs (83) and potentially compromises
national security (84) due to diminished health and cardio-
metabolic risk in recruits.
In an effort to gain insight into the motivation for
anti-obesity legislation to rein in these manifold problems,
Gomez (85) performed a nested analysis and found that
in the case of Brazil, there are different drivers for obe-
sity at the national, urban, and rural levels that involve
complex interactions among international, historical, and
social factors. This made it difficult to draw meaningful
conclusions when examining cross-national statistical
evidence. This is consistent with an earlier conclusion
reached by Trivedi et al (86), who explained the lack of
direct correlation between state-by-state anti-obesity leg-
islation in the U.S. and the concavity (or acceleration) of
obesity prevalence growth rates as an insufficient effect
on emergent and complex drivers, particularly those in the
built environment (the human-made space: food availabil-
ity and presentation, areas for physical activity, media and
advertising, etc.).
Is the road to optimizing obesity care one that involves
more anti-obesity legislation? The legal, social, and eco-
nomic framework for this decision-making in Argentina
and Brazil was recently reviewed by Arbex et al (87), once
again supporting the hypothesis that cultural factors are
part of the LA obesity problem. A potential tool to untan-
gle the intricacies of obesity care in LA uses Census Tract
data, as in the case for Rio de Janeiro city, Brazil, and a
combinatorial spatial microsimulation model (88). Here,
obesity ranged from 8 to 25% without socio-economic or
gender differences at small local scales, with significant
correlations with sugared-soda consumption (88). In Chile,
where rapid societal changes have reduced undernutrition,
an unintended consequence is overnutrition. As a result,
an effective regulatory framework has been established to
combat overweight/obesity in Chile through improved and
iterative monitoring of lifestyle and appropriate actions,
again in a local context (89).

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 489
Table 7 Age-Standardized Prevalence Rates of Obesity in Latin America by Gender and Countrya
2013 Prevalence rates (%) Men Women
Chile
El Salvador
Honduras 30–40
20–29
15–19
10–14
5–9
Mexico
Nicaragua
Paraguay
Argentina Argentina Cuba
Chile Bolivia Dominican Republic
Mexico Brazil Peru
Paraguay Colombia Uruguay
Uruguay Costa Rica Venezuela
Costa Rica Ecuador
Cuba Guatemala
Panama
Bolivia Haiti
Brazil
Colombia
Dominican Republic
Nicaragua
Panama
Venezuela
Ecuador
El Salvador
Guatemala
Honduras
Peru
<5 Haiti
a Countries in bold type were represented at the PAACE Workshop in 2015. Adapted from data presented in reference 77.
The role of government and national surveys to
establish data-driven behavioral and specific food-based
recommendations is also important. For example, a cam-
paign that popularizes a healthy plate of LA foods would
be highly effective. The plate would reflect a clinically
effective and evidence-based healthy meal plan, similar to
the plant-based Dietary Approaches to Stop Hypertension
(DASH) diet, which is higher in fiber (fruits and greens),
with adequate protein (lean meats and low-fat dairy) and
relatively low starch (primarily found in staples: corn,
plantain, beans, etc.).
Within the U.S., culturally sensitive interventions
for obesity among the Latino population should address
healthy eating, physical activity, behavior, environmental
change, policy reformation, economic considerations,
school- and community-based interventions, and the use of
bilingual/bicultural HCPs (67,68).
Core Recommendations
Figure 3 – Node level 1 (Screening or aggressive case
finding)
1. Use BMI and determine if other anthropomet-
rics are appropriate (e.g., WC cutoffs based on
local epidemiologic data) to identify patients with
excess adiposity as either overweight or obese—
a necessary step to initialize overweight/obesity
weight-loss management programs.

490 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Table 8 Weight-Related Complicationsa
Disability/immobility
Dyslipidemia
Gastro-esophageal reflux disease
Hypertension
Metabolic syndrome
Nonalcoholic fatty liver disease
Obstructive sleep apnea
Osteoarthritis
Polycystic ovary syndrome
Psychological disorder and/or stigmatization
Prediabetes
Type 2 diabetes
Urinary stress incontinence
a See reference 66.
Figure 3 – Node level 2 (Stratify)
1. Assign appropriate terminology in the native lan-
guage for best communication with people with
overweight/obesity (health care literacy and nutri-
tional messaging).
2. Determine appropriate risk categories based on
local correlative epidemiologic data.
Figure 3 – Node level 3 (Diagnostics and further sub-
sets)
1. Evaluate patients with overweight/obesity for the
presence and severity of weight-related complica-
tions, such as metabolic syndrome, prediabetes,
T2D, hypertension, dyslipidemia, nonalcoholic
fatty liver disease, sleep apnea, osteoarthritis, etc.
(Table 8) (66). These and other weight-related
complications, and their relative priorities, should
be evaluated based on local evidence.
2. Include additional evidence-based anthropomet-
ric classifiers and their cutoffs, as needed (e.g.,
WC, waist-to-hip ratio, intra-abdominal fat by
computed tomography, and body composition by
DXA).
3. Include evidence-based and locally validated
complications-centric composite scoring systems,
such as the Edmonton Obesity Staging System
(90) and the Cardiometabolic Disease Staging
System (91).
Figure 3 – Node level 4 (Intervention)
1. All patients should be treated with lifestyle
interventions.
2. Provide culturally sensitive foods and meal-plan-
ning recommendations that also accommodate
individual preferences.
3. Provide culturally sensitive physical activity and
sports recommendations that also accommodate
individual preferences.
4. Discuss and provide evidence, where appropri-
ate, on the beneficial and harmful effects of siesta
breaks (short afternoon napping) on healthy sleep
hygiene and healthy eating. Provide specific rec-
ommendations regarding siesta breaks to opti-
mize lifestyle.
5. Organize interventions based on a preventive care
model:
a. primary—to decrease risk of disease;
b. secondary—to prevent disease progres-
sion and the emergence of complica-
tions; and
c. tertiary—to treat complications and
minimize morbidity and mortality in late
symptomatic disease.
6. Consider patients with more severe weight-
related complications for more aggressive weight
loss approaches that could include intensification
of the lifestyle interventions, use of weight-loss
medications, and/or bariatric surgery or other
available and approved nonsurgical procedures.
7. Take inventory of available weight-loss medica-
tions and include safety and efficacy in local clini-
cal trials (if any), cost, and cost-effectiveness (if
possible).
8. Take inventory of available bariatric surgical and
nonsurgical procedures and include safety and
efficacy in local clinical trials (if any), cost, and
cost-effectiveness (if possible)
9. Consider providing a listing of surgical centers
with established excellence in bariatric proce-
dures (surgical and nonsurgical).
10. Recommend more education for HCPs regarding
lifestyle interventions, pharmacotherapy, and bar-
iatric procedures (surgical and nonsurgical).
11. Address obesity medicine availability and afford-
ability issues.
12. Recommend standards of excellence and training
for procedural (surgical and nonsurgical) inter-
ventions for obesity that minimize adverse events
and optimize clinical outcomes.
13. Specifically recommend expert pre- and post-
operative nonsurgical management of patients
undergoing bariatric surgery, consistent with the
AACE/ACE CPG (92).
14. Consider specific therapeutic approaches to vita-
min D undernutrition.
15. Engage government and policy-makers in effect-
ing beneficial changes to the built environment,
education, research, and ability for HCPs to pro-
vide optimal comprehensive obesity care.
Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 491
Figure 3 – Node level 5 (Metrics)
1. Individualize and prioritize weight-loss goals
based on targeted weight-related complications,
specific patient attributes, patient/physician pref-
erences, etc.
Figure 3 – Node level 6 (Follow-up intervention)
1. Following the period of weight loss, patients will
need ongoing interaction with the HCP team and
a plan designed to maintain the weight loss over
the long term.
2. Give special attention to whether the weight
loss has adequately improved weight-related
complications.
3. If not, treatment should be initiated or intensi-
fied that specifically targets the weight-related
complication.
4. Provide evidence-based individualized ongoing
strategies.
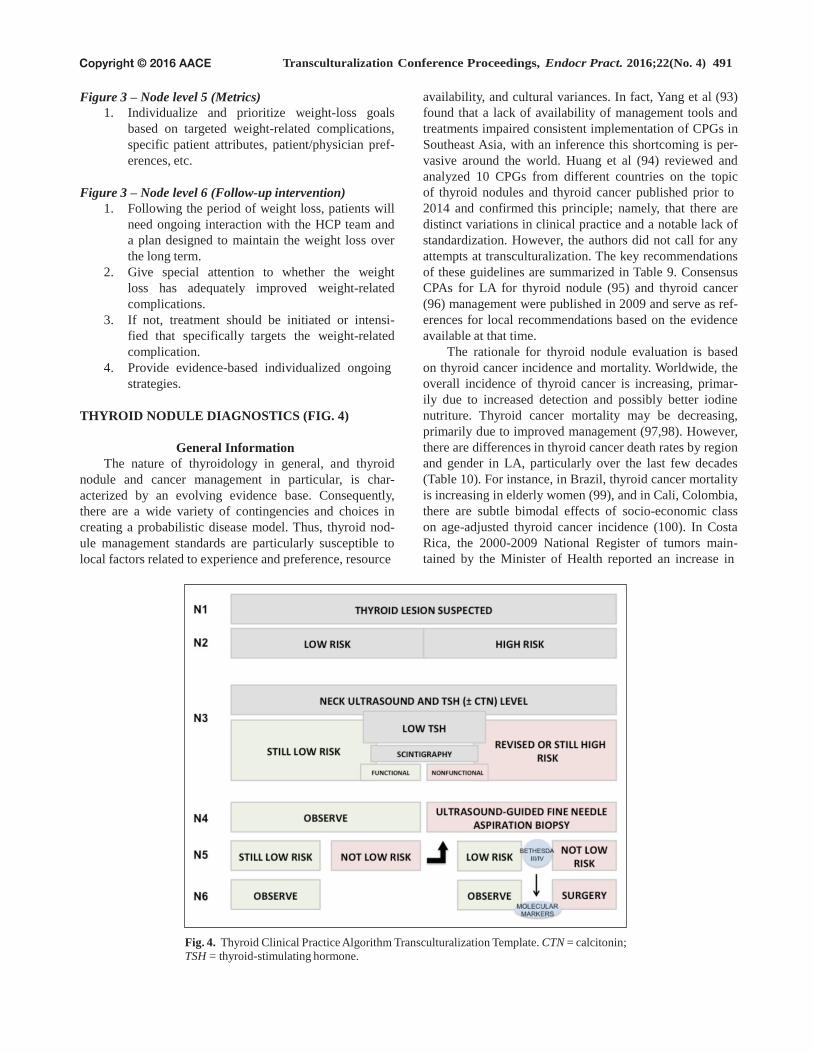
THYROID NODULE DIAGNOSTICS (FIG. 4)
General Information
The nature of thyroidology in general, and thyroid
nodule and cancer management in particular, is char-
acterized by an evolving evidence base. Consequently,
there are a wide variety of contingencies and choices in
creating a probabilistic disease model. Thus, thyroid nod-
ule management standards are particularly susceptible to
local factors related to experience and preference, resource
availability, and cultural variances. In fact, Yang et al (93)
found that a lack of availability of management tools and
treatments impaired consistent implementation of CPGs in
Southeast Asia, with an inference this shortcoming is per-
vasive around the world. Huang et al (94) reviewed and
analyzed 10 CPGs from different countries on the topic
of thyroid nodules and thyroid cancer published prior to
2014 and confirmed this principle; namely, that there are
distinct variations in clinical practice and a notable lack of
standardization. However, the authors did not call for any
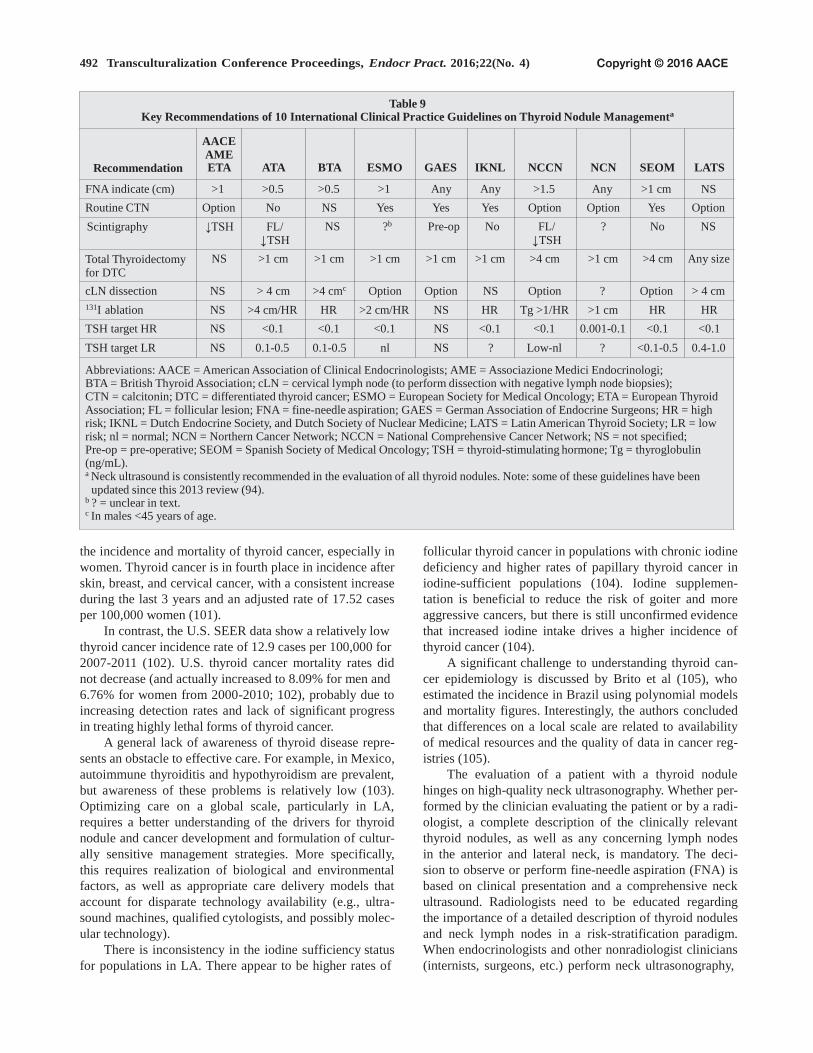
attempts at transculturalization. The key recommendations
of these guidelines are summarized in Table 9. Consensus
CPAs for LA for thyroid nodule (95) and thyroid cancer
(96) management were published in 2009 and serve as ref-
erences for local recommendations based on the evidence
available at that time.
The rationale for thyroid nodule evaluation is based
on thyroid cancer incidence and mortality. Worldwide, the
overall incidence of thyroid cancer is increasing, primar-
ily due to increased detection and possibly better iodine
nutriture. Thyroid cancer mortality may be decreasing,
primarily due to improved management (97,98). However,
there are differences in thyroid cancer death rates by region
and gender in LA, particularly over the last few decades
(Table 10). For instance, in Brazil, thyroid cancer mortality
is increasing in elderly women (99), and in Cali, Colombia,
there are subtle bimodal effects of socio-economic class
on age-adjusted thyroid cancer incidence (100). In Costa
Rica, the 2000-2009 National Register of tumors main-
tained by the Minister of Health reported an increase in
Fig. 4. Thyroid Clinical Practice Algorithm Transculturalization Template. CTN = calcitonin;
TSH = thyroid-stimulating hormone.
492 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Table 9
Key Recommendations of 10 International Clinical Practice Guidelines on Thyroid Nodule Managementa
Recommendation
AACE
AME ETA ATA BTA ESMO GAES IKNL NCCN NCN SEOM LATS
FNA indicate (cm) >1 >0.5 >0.5 >1 Any Any >1.5 Any >1 cm NS
Routine CTN Option No NS Yes Yes Yes Option Option Yes Option
Scintigraphy ↓TSH FL/ ↓TSH
NS ?b Pre-op No FL/
↓TSH
? No NS
Total Thyroidectomy for DTC
NS >1 cm >1 cm >1 cm >1 cm >1 cm >4 cm >1 cm >4 cm Any size
cLN dissection NS > 4 cm >4 cmc Option Option NS Option ? Option > 4 cm
131I ablation NS >4 cm/HR HR >2 cm/HR NS HR Tg >1/HR >1 cm HR HR
TSH target HR NS <0.1 <0.1 <0.1 NS <0.1 <0.1 0.001-0.1 <0.1 <0.1
TSH target LR NS 0.1-0.5 0.1-0.5 nl NS ? Low-nl ? <0.1-0.5 0.4-1.0
Abbreviations: AACE = American Association of Clinical Endocrinologists; AME = Associazione Medici Endocrinologi; BTA = British Thyroid Association; cLN = cervical lymph node (to perform dissection with negative lymph node biopsies); CTN = calcitonin; DTC = differentiated thyroid cancer; ESMO = European Society for Medical Oncology; ETA = European Thyroid Association; FL = follicular lesion; FNA = fine-needle aspiration; GAES = German Association of Endocrine Surgeons; HR = high risk; IKNL = Dutch Endocrine Society, and Dutch Society of Nuclear Medicine; LATS = Latin American Thyroid Society; LR = low risk; nl = normal; NCN = Northern Cancer Network; NCCN = National Comprehensive Cancer Network; NS = not specified; Pre-op = pre-operative; SEOM = Spanish Society of Medical Oncology; TSH = thyroid-stimulating hormone; Tg = thyroglobulin (ng/mL). a Neck ultrasound is consistently recommended in the evaluation of all thyroid nodules. Note: some of these guidelines have been
updated since this 2013 review (94). b ? = unclear in text. c In males <45 years of age.
the incidence and mortality of thyroid cancer, especially in
women. Thyroid cancer is in fourth place in incidence after
skin, breast, and cervical cancer, with a consistent increase
during the last 3 years and an adjusted rate of 17.52 cases
per 100,000 women (101).
In contrast, the U.S. SEER data show a relatively low
thyroid cancer incidence rate of 12.9 cases per 100,000 for
2007-2011 (102). U.S. thyroid cancer mortality rates did
not decrease (and actually increased to 8.09% for men and
6.76% for women from 2000-2010; 102), probably due to
increasing detection rates and lack of significant progress
in treating highly lethal forms of thyroid cancer.
A general lack of awareness of thyroid disease repre-
sents an obstacle to effective care. For example, in Mexico,
autoimmune thyroiditis and hypothyroidism are prevalent,
but awareness of these problems is relatively low (103).
Optimizing care on a global scale, particularly in LA,
requires a better understanding of the drivers for thyroid
nodule and cancer development and formulation of cultur-
ally sensitive management strategies. More specifically,
this requires realization of biological and environmental
factors, as well as appropriate care delivery models that
account for disparate technology availability (e.g., ultra-
sound machines, qualified cytologists, and possibly molec-
ular technology).
There is inconsistency in the iodine sufficiency status
for populations in LA. There appear to be higher rates of
follicular thyroid cancer in populations with chronic iodine
deficiency and higher rates of papillary thyroid cancer in
iodine-sufficient populations (104). Iodine supplemen-
tation is beneficial to reduce the risk of goiter and more
aggressive cancers, but there is still unconfirmed evidence
that increased iodine intake drives a higher incidence of
thyroid cancer (104).
A significant challenge to understanding thyroid can-
cer epidemiology is discussed by Brito et al (105), who
estimated the incidence in Brazil using polynomial models
and mortality figures. Interestingly, the authors concluded
that differences on a local scale are related to availability
of medical resources and the quality of data in cancer reg-
istries (105).
The evaluation of a patient with a thyroid nodule
hinges on high-quality neck ultrasonography. Whether per-
formed by the clinician evaluating the patient or by a radi-
ologist, a complete description of the clinically relevant
thyroid nodules, as well as any concerning lymph nodes
in the anterior and lateral neck, is mandatory. The deci-
sion to observe or perform fine-needle aspiration (FNA) is
based on clinical presentation and a comprehensive neck
ultrasound. Radiologists need to be educated regarding
the importance of a detailed description of thyroid nodules
and neck lymph nodes in a risk-stratification paradigm.
When endocrinologists and other nonradiologist clinicians
(internists, surgeons, etc.) perform neck ultrasonography,

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 493
Table 10
Age-Adjusted Death Rates and Corresponding Percentage Changes for
Thyroid Cancer From Around 2000 (1998-2002) to Around 2010 (2008-2012) in Some Latin American Countriesa
Country 2000 Death rate 2010 Death rate Change (%)
Argentina 0.25 0.23 −8.46
Bolivia – – –
Brazil 0.19 0.20 +4.42
Chile 0.33 0.24 −28.25
Colombia 0.34 0.32 −7.42
Costa Rica 0.15 0.24 +66.89
Cuba 0.19 0.20 +4.73
Dominican Republic – – –
Ecuador 0.27 0.37 +36.34
El Salvador – – –
Guatemala – – –
Haiti – – –
Honduras – – –
Mexico 0.32 0.33 +2.23
Nicaragua – – –
Panama – – –
Paraguay – – –
Peru – – –
Uruguay 0.24 0.36 +47.94
Venezuela 0.25 0.23 −5.05
a Countries in bold type were represented at the PAACE Workshop in 2015. Adapted from data in reference 97. Age-standardized rates derived by direct method using world standard population (98). For comparison, in the U.S., the 2000 and 2010 death rates were 0.23 and 0.25, respectively, corresponding to an increase of 8.09%.
training and certification programs must be established to
ensure quality. The cytologist interpreting the FNA should
provide a detailed description of the findings as well as
the Bethesda cytologic classification (106,107). The trans-
culturalized LA algorithm should utilize patient historic
data, physical examination findings, ultrasound findings,
and cytologic findings (preferably using the Bethesda sys-
tem), as well patient preferences, when determining which
nodules to observe and which nodules to resect. Entry of
patient demographics, risk factors, and thyroid nodule
characteristics into widely utilized patient registries would
be optimal.
Core Recommendations
Figure 4 – Node level 1 (Screening or aggressive case
finding)
1. To specify how the algorithm is initiated: pres-
ence of risk factors, incidental discovery of a thy-
roid lesion, palpation of a thyroid nodule on rou-
tine examination, etc.
2. To review and modify the following list of spe-
cific high-risk descriptors based on epidemiologic
data in LA: progressive local symptoms, affected
first-degree relative, family member with medul-
lary thyroid cancer, familial syndrome with papil-
lary or follicular thyroid cancer, prior head/neck
irradiation, growing/fixed/hard/irregular thyroid
mass or large/immobile/hard cervical lymph node
on exam, or an elevated calcitonin level.
3. To incorporate additional clinical scenarios and
risk factors substantiated by relevant epidemio-
logic data.
Figure 4 – Node level 2 (Stratify)
1. Initial risk stratification status can be based on
a composite risk score validated in the local LA
region/culture (108).
2. Consider analyzing existing LA regional thyroid
cancer registries to guide selection of appropriate risk
scores and stratification protocols.

494 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Figure 4 – Node level 3 (Diagnostics and further
subset)
1. Review and incorporate published white
papers for neck ultrasound methodologies and
interpretations.
2. Incorporate the Thyroid Image Reporting and
Data System (TIRADS) or other local classifica-
tion systems for neck ultrasonography use (109).
3. Stipulate the need for high-quality neck ultrasound
machines, and if not readily available, mecha-
nisms must be described to access this essential
resource, including finding off-site locations and
providing logistics for purchase or lease.
4. Emphasize the need for expertise in performing
diagnostic neck ultrasound, and if not available,
to establish mechanisms for training, certifica-
tion, and continuing education, such as the AACE
Endocrine Certification in Neck Ultrasound
(ECNU) program.
5. Provide detail for logistics and acquisition of sup-
plies for high-quality neck ultrasonography.
6. Incorporate current and locally validated strate-
gies for neck ultrasonography, thyroid-stimulat-
ing hormone (TSH), and thyroid scintigraphy in
the routine evaluation of thyroid nodules, coupled
with aforementioned Node 2 risk factors, to estab-
lish an overall risk class to guide management.
Figure 4 – Node level 4 (Intervention)
1. Stipulate the need for expertise in performing
ultrasound-guided FNA for the routine evaluation
of higher-risk thyroid nodules, and if not avail-
able, to establish mechanisms for training, cer-
tification, and continuing education, such as the
AACE ECNU program.
2. Provide pathways for logistics, education, and
acquisition of supplies for high-quality ultra-
sound-guided FNA.
3. Recognize that the quality of ultrasound machine
technology and user skill/experience in perform-
ing neck ultrasound for FNA guidance in Node 4
does not need to be as high as in Node 3 for neck
diagnostics.
4. Create access to sensitive and accurate TSH
assays, preferably an ultrasensitive, or third-gen-
eration, TSH assay.
5. Ensure availability of high-quality thyroid scin-
tigraphy for clinical use when the TSH is low;
this includes not only access to the technology
but also access to well-trained endocrinologists,
radiologists, or nuclear medicine specialists for
interpretation.
Figure 4 – Node level 5 (Metric)
1. Focus on neck ultrasonography findings that
are associated with higher risk (e.g., growing,
irregular margins, microcalcifications, intrano-
dular hypervascularity, associated with abnormal
lymph nodes, etc.).
2. Employ the Bethesda classification system for
cytology interpretation, with particular focus on
protocols to further manage Bethesda III and IV
(specifying if Hürthle cell [oncocytic] type) clas-
sifications, with or without availability of molecu-
lar markers.
3. Develop protocols for the use of molecular mark-
ers (for indeterminate cytologic results, such as
Bethesda III and IV) based on currently published
CPGs as well as any locally developed CPGs. If
this technology is available, to provide as much
detail as possible regarding logistics and per-
formance, particularly if there are different tests
available.
Figure 4 – Node level 6 (Follow-up intervention)
1. Provide protocols for observation, time inter-
vals for re-evaluation, and need for surgery or
other interventions, all supported by scientific
substantiation.
2. Use registries to enhance uniform application of
CPA-driven care.
POSTMENOPAUSAL OSTEOPOROSIS (FIG. 5)
General Information
Culturally sensitive influences on fracture risk among
postmenopausal women on a global scale can be con-
sidered in 3 broad categories. The first relates to genetic
and epigenetic system interactions, the second to lifestyle
variables (eating patterns, physical activity, smoking, alco-
hol use, exposure to EDCs, etc.), and the third to health
care accessibility, variances in practice standards, HCP
experience, and availability of technology. Prevention of
bone loss is a key to improving osteoporosis prevalence
rates and the direct and indirect costs associated with this
chronic disease.
The first population-based study of vertebral fractures
in LA found an 11.18% prevalence rate of radiographically
ascertained vertebral fractures in a random sample of 1,922
women aged 50 to 80 years from cities within 4 different
countries (Argentina, Brazil, Colombia, Mexico) and in
Puerto Rico (106). The prevalence of asymptomatic ver-
tebral fractures steadily increased from age 50 to 59 years
to over 80 years without regional variations. However,
patient age and history of fractures were associated with
vertebral fractures in this population (110). Sen et al (111)
described a risk assessment tool for LA (Osteorisk), which
incorporates age, weight, country, estrogen use, and history
of fracture, with 91% sensitivity and 47% specificity.
The burden of disease, represented as disability-
adjusted life years for osteoporotic fractures, is interme-
diate among various chronic diseases, with osteoporotic

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 495
A
Fig. 5. Bone Clinical Practice
Algorithm Transculturalization
Template. BMD = bone mineral
density; DR = distal 33% radius;
DXA = dual-energy X-ray
absorptiometry; FN = femoral neck;
LS = lumbar spine; LSC = least
significant change (least amount
of BMD change that is statistically
significant); TH = total hip.
1 FRAX scores (120). 2 Indicators of fracture risk: age,
frailty, prior fractures,
glucocorticoids, FRAX components,
others (Table 11). 3 Includes intact parathyroid hormone,
25-hydroxyvitamin D, and 24-hour
urinary calcium excretion. Markers
of bone turnover (e.g., N-telopeptide,
C-telopeptide, bone-specific alkaline
phosphatase, and osteocalcin) are not
included in current AACE CPG. 4 For example, kidney, liver, adrenal,
thyroid, parathyroid, hematologic/
oncologic diseases. 5 Oral antiresorptive agents –
alendronate and risedronate;
injectable antiresorptive agents
– zoledronic acid and denosumab;
alternative agents – ibandronate,
raloxifene, and teriparatide. 6 See oral and injectable antiresorptive
agents above; alternative agents
– alendronate, risedronate,
ibandronate, and raloxifene.
B
C

496 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
fracture rates ranging from only 0.8% in Africa to 34.8% in
Europe (the rate is 15.7% in the Americas) (112). Costs of
fragility fractures for all persons 40 years of age and over
in Mexico exceeded $250 million in 2010, in the context
of prevalence rates of 32.8% for osteopenia and 8% for
osteoporosis (113). Overall expenditures related to bone
loss were over $400 million in 2010 and are expected to
rise by 19.2% in 2015 and 41.7% by 2020 (113). In Brazil,
the prevalence of osteoporosis (determined by measuring
bone mineral density) among clinical series of women over
40 years of age ranges from 25 to 33% (114). In another
study, Morales-Torres et al (16) found that in the expand-
ing elderly population of LA, 12 to 18% of women over 50
years of age have vertebral osteoporosis and 8 to 22% have
proximal femur osteoporosis. Vertebral and femoral neck
bone mineral densities decline comparably over the lifes-
pan in women among 6 LA countries studied: Argentina,
Mexico, Brazil, Colombia, Cuba, and Chile (16).
In a review by Prentice (115), with the exception of
calcium and vitamin D, there is only weak to no evidence
to support the inclusion or exclusion of specific dietary
components for bone health. However, in a study compar-
ing attitudes toward dietary supplements for osteoporosis,
Mexican respondents reported taking their calcium but not
their vitamin D (116). In fact, there is a linear association
of calcium intake and hip fracture incidence for 15 differ-
ent countries from around the world (115). Furthermore,
various dietary factors have possible positive (vitamin D,
calcium, fruits and vegetables, and moderate alcohol con-
sumption), neutral (phosphate), negative (low body weight,
high alcohol consumption, and sodium), and unclear (pro-
tein) associations with fracture risk (115). In a study by
Copês et al (117) of postmenopausal women in Brazil, obe-
sity was not associated with fracture.
In Brazil, expenditures for osteoporosis in 2008-
2010 exceeded $288 million, with most resources directed
toward women (118). Most of the osteoporosis-related
procedures were outpatient, but most of the expenses were
inpatient (118). There are no demonstrable associations of
fracture risk among men and women in Brazil with social
class, but among women, there is a higher incidence of
fractures in metropolitan areas compared with rural areas
(119).
Core Recommendations
Figure 5 – Node level 1 (Screening or aggressive case
finding)
1. Emphasize that all postmenopausal women are at
increased risk for bone loss and fragility fracture,
and therefore, DXA serves as a tool for aggressive
case finding in this setting and not for screening
per se.
2. Provide accurate DXA T-scores for lumbar spine,
total hip, femoral neck, and distal third of the
forearm, where bone loss can occur.
3. Use region-specific, validated fracture risk assess-
ment tool scores to quantify risk (120).
Figure 5 – Node level 2 (Stratify)
1. Emphasize that the main classifier is whether a
patient has disease (osteoporosis) or not.
2. Define the osteoporosis state for the postmeno-
pausal woman with a culturally specific context
that helps with patient-physician communication
and health literacy.
Figure 5 – Node level 3 (Diagnostics and further
subset)
1. Clarify the meaning of osteopenia as a non–dis-
ease state that is associated with higher risk for
disease (osteoporosis) and therefore requires
some degree of intervention, ranging from life-
style intervention alone (physical activity and
nutritional recommendations) to pharmacother-
apy in higher-risk categories.
2. Emphasize the relevance of prior fragility frac-
tures in further risk assessment for future frac-
tures and need for intervention.
3. Evaluate the validity of other factors associated
with fracture risk within the context of a specific
LA region or culture (see Table 11).
4. Provide an assessment for each biochemical test
recommended based on cost, cost-effectiveness,
performance, availability, and logistics for use.
5. Validate and standardize each test for the target
LA population.
6. Provide context and evidence-based recommen-
dations for the issue of vitamin D undernutrition,
sunlight exposure, and use of sunscreens.
7. Screening for other secondary causes should be
guided by region-specific prevalence rates and/or
risk factors.
8. Currently, bone turnover markers are not used
in AACE CPGs for stratification purposes or to
direct specific interventions.
Figure 5 – Node level 4 (Intervention)
1. Recognize the different protocols for treating
those with only moderate risk versus those with
high risk.
2. Provide a pragmatic listing of available interven-
tions with evidence for safety and efficacy, as well
as costs and logistics.
3. Emphasize the role of culturally sensitive lifestyle
interventions for all patients with any degree of
bone loss, including low-impact, weight-bearing
physical activity, nutritional (including increased
fruits and vegetables), tobacco cessation, modera-
tion of alcohol consumption, and prevention of
falls.

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 497
Table 11
Risk Factors for Fracture in Postmenopausea
Increased age
Alcohol >3 drinks/day
Body mass index
Current tobacco smoking
Femoral neck BMD
Frailty
Neuropathy, instability, and falls
Glucocorticoids
Parent with fractured hip
Prior fracture
Rheumatoid arthritis
Other causes for secondary osteoporosis
Abbreviation: BMD = bone mineral density (determined using dual X-ray absorptiometry). a See http://www.shef.ac.uk/FRAX/tool.jsp for World Health
Organization Fracture Risk Assessment tool (FRAX) (120).
4. Include a statement about medications associated
with bone loss and the need for the HCP to discuss
these issues with the patient.
5. Consider the transformative nature of these
CPGs, especially where resources are limited or
constrained.
6. Validate and standardize these tests for the target
Latin American population.
7. Comment about the need for further research
and data collection that is region- and culturally
specific.
Figure 5 – Node level 5 (Metric)
1. Define responder classifications based on locally
validated evidence, if available.
2. Specifically mention the threshold for magnitude
of response needed as well as the time interval for
interrogation to determine whether an adequate
response has occurred.
Figure 5 – Node levels 6-8 (Follow-up interventions and
metrics)
1. Present iterations of interrogation and action that
are based on scientific evidence.
2. Explain the concept of a “drug holiday” in a way
that the target population understands it as a pause
in treatment with the intent to minimize adverse
effects of prolonged therapy and to then re-evalu-
ate after a specified period of time.
3. Emphasize the message that osteoporosis is a
chronic disease that will require management for
a potentially long period of time, spanning years.
CONCLUSION
The 2015 AACE/ACE CPA node-specific analysis and
portfolio of recommendations is designed to optimize endo-
crine care on a global scale by facilitating the local CPA
transculturalization process. This methodology is tractable
and designed for easy reproducibility by a wide range of
professional medical organizations. Transculturalization is
mandatory for the translation of scientifically substantiated
clinical practice white papers into meaningful and success-
ful implementation strategies on a global scale, as well
as a regional/national scale wherein multiple cultures co-
exist. In other words, transculturalization offers the means
to effectively address epidemiologic trends in health care,
which have previously demonstrated recalcitrance to con-
ventional white paper development and implementation
strategies. Notwithstanding, this aspiration of enhanced
relevance of transculturalized CPAs requires additional
formalization.
One aspect of formalization is the creation of elec-
tronic products that, in contrast with printed narrative
documents, are more accessible, easier to publish, and less
costly to modify over time. Moreover, electronic versions
are suitable not only for domestic use in modernized clini-
cal practice settings but also accessible through a global
Internet application. In this latter construct, the user would,
in theory, be able to designate their location on a world
map, input information about their region, culture, and
personal medical status, and then query specific areas of
interest, for example, a healthy eating pattern for a young
adult male in Mexico who is overweight and has T2D.The
output could consist of updated scientifically substantiated
nutritional recommendations tailored for the particular
query. All input and output information would lack per-
sonal identifiers to protect privacy, but depersonalized
inputs could be collected in a registry. This would allow
for further data mining, research, and discovery of emer-
gent information and should enable well-designed valida-
tion protocols based on longitudinal data input. Financing
this enhancement of the current transculturalization project
and other derivative activities would be challenging, albeit
solvable, and part of the enduring mission of AACE/ACE.
DISCLOSURE
Dr. Jeffrey Mechanick has received honoraria from
Abbott Nutrition International for lectures and for the
tDNA program development.
Dr. Pauline Camacho has received research grants
from Amgen and Eli Lilly and has served on the advisory
board for Amgen.
Dr. Walmir Coutinho has received honoraria from
Abbott Diabetes Care, ACHE, AstraZeneca, Janssen, and
Novo Nordisk.

498 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
Dr. Pablo Aschner has served on advisory boards for 8. Hofstede G. National cultures and corporate cultures. In:
AstraZeneca, Eli Lilly & Co, GlaxoSmithKline, Janssen,
Merck, Novartis, Sanofi, and Sharpe & Dohme. He has also
been on the speakers’ bureau for AstraZeneca, Boehringer
Ingelheim, Eli Lilly & Co, Merck, Novartis, Sanofi, and
Sharpe & Dohme.
Dr. W. Timothy Garvey has received consultant
fees from Boehringer Ingelheim, Daiichi-Sankyo, Eisai,
Janssen, Liposcience, Novo Nordisk, and Vivus, Inc. He
was principal investigator for contracted research for
Amylin, AstraZeneca, Eisai, Elcelyx, Lexicon, Merck,
Novo Nordisk, Pfizer, Sanofi, and Weight Watchers and is
a stockholder for Bristol-Myers Squibb, ISIS, Lilly, Merck,
Novartis, and Pfizer.
Dr. Osama Hamdy has received research support from
Metagenics, Inc and the USDA Dairy Council and has
served on the advisory board for AstraZeneca and Novo
Nordisk.
Dr. Yehuda Handelsman has received research grant
support, been a consultant for, and received speaker hono-
raria from Amarin, Amgen, AstraZeneca, Bristol-Myers
Squibb, Boehringer Ingelheim, Eisai, Essperion, Frifolis,
GlaxoSmithKline, Hamni, Intarcia, Janssen, Lexicon, Eli
Lilly & Co, Merck, Novo Nordisk, Pfizer, Regeneron,
Sanofi, Takeda, and Vivus, Inc. He is also the Immediate
Past President of the American College of Endocrinology.
The other authors have no multiplicity of interest to
disclose.
REFERENCES
1. Mechanick JI, Bergman DA, Braithwaite SS, Palumbo
PJ; American Association of Clinical Endocrinologists Ad Hoc Task Force for Standardized Production of
Clinical Practice Guidelines. American Association of Clinical Endocrinologists protocol for standardized pro- duction of clinical practice guidelines. Endocr Pract. 2004;10:353-361.
2. Mechanick JI, Camacho PM, Cobin RH, et al. American Association of Clinical Endocrinologists protocol for stan- dardized production of clinical practice guidelines--2010 update. Endocr Pract. 2010;16:270-283.
3. Weiner SJ, Schwartz A, Weaver F, et al. Contextual errors and failures in individualizing patient care: a multi- center study. Ann Intern Med. 2010;153:69-75.
4. Weiner SJ, Schwartz A, Sharma G, et al. Patient- centered decision making and health care outcomes: an observational study. Ann Intern Med. 2013;158:573-579.
5. University of Minnesota, Center for Advanced Research
on Language Acquisition. What is culture? Available at: http://www.carla.umn.edu/culture/ definitions.html. Accessed January 26, 2015.
6. Banks JA, McGee Banks CA, eds. Multicultural Education: Issues and Perspectives. 2nd ed. Boston, MA: Allyn & Bacon; 1989.
7. Damen L. Culture Learning: The Fifth Dimension in the Language Classroom. Reading, MA: Addison Wesley Publishing Company; 1987.
Samovar LA, Porter RE, eds. Communication Between Cultures. Belmont, CA: Wadsworth; 1984: 51.
9. Kluckhohn C, Kelly WH. The concept of culture. In: Linton R, ed. The Science of Man in the World Culture. New York, NY: Columbia University Press; 1945: 78-105.
10. Kroeber AL, Kluckhohn C. Culture: a critical review of concepts and definitions. Papers. Peabody Museum of American Archeology and Ethnology, Harvard University. 1952;47.
11. Lederach JP. Preparing for Peace: Conflict Transformation Across Cultures. Syracuse, NY: Syracuse University Press; 1995.
12. Linton R. The Cultural Background of Personality. New York, NY: Appleton-Century; 1945.
13. Parsons T. Essays in Sociological Theory. Glencoe, IL: Free Press; 1949.
14. Useem J, Useem R, Donoghue J. Men in the middle of the third culture: the roles of American and Non-Western peo- ple in cross-cultural administration. Human Organization. Fall 1963;22:169-179.
15. Texas A&M University. Culture. Available at: http:// www.tamu.edu/faculty/choudhury/culture.html. Accessed January 26, 2015.
16. Morales-Torres J, Gutiérrez-Ureña S; Osteoporosis Committee of Pan-American League of Associations
for Rheumatology. The burden of osteoporosis in Latin America. Osteoporos Int. 2004;15:625-632.
17. Brown SA, García AA, Winter M, Silva L, Brown A,
Hanis CL. Integrating education, group support, and case management for diabetic Hispanics. Ethn Dis. 2011;21: 20-26.
18. Chary A, Greiner M, Bowers C, Rohloff P. Determining adult type 2 diabetes-related health care needs in an indigenous population from rural Guatemala: a mixed- methods preliminary study. BMC Health Serv Res. 2012; 12:476.
19. Brown SA, García AA, Steinhardt MA, et al. Culturally tailored diabetes prevention in the workplace: focus group interviews with Hispanic employees. Diabetes Educ. 2015; 41:175-183.
20. Wallace DC. A mitochondrial paradigm of metabolic and degenerative diseases, aging, and cancer: a dawn for evo- lutionary medicine. Annu Rev Genet. 2005;39:359-407.
21. Sánchez-Guerra M, Pérez-Herrera N, Quintanilla-Vega B. Organophosphorous pesticides research in Mexico: epi- demiological and experimental approaches. Toxicol Mech Methods. 2011;21:681-691.
22. Schell LM, Burnitz KK, Lathrop PW. Pollution and human biology. Ann Hum Biol. 2010;37:347-366.
23. Villarreal-Calderón A, Acuña H, Villarreal-Calderón
J, et al. Assessment of physical education time and after- school outdoor time in elementary and middle school stu- dents in south Mexico City: the dilemma between physical fitness and the adverse health effects of outdoor pollutant exposure. Arch Environ Health. 2002;57:450-460.
24. Lange FT, Scheurer M, Brauch HJ. Artificial sweeten- ers--a recently recognized class of emerging environmen- tal contaminants: a review. Anal Bioanal Chem. 2012;403: 2503-2518.
25. Gersten O, Dow WH, Rosero-Bixby L. Stressors over the life course and neuroendocrine system dysregulation in Costa Rica. J Aging Health. 2010;22:748-771.
Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 499
26. Mechanick JI, Camacho PM, Garber AJ, et al. American Association of Clinical Endocrinologists and American College of Endocrinology protocol for standard- ized production of clinical practice guidelines, algorithms, and checklists – 2014 update and the AACE G4G program. Endocr Pract. 2014;20:692-702.
27. Su HY, Tsang MW, Huang SY, Mechanick JI, Sheu
WH, Marchetti A. Transculturalization of a diabetes- specific nutrition algorithm: Asian application. Curr Diab Rep. 2012;12:213-219.
28. Joshi SR, Mohan V, Joshi SS, Mechanick JI, Marchetti A. Transcultural diabetes nutrition therapy algorithm: the Asian Indian application. Curr Diab Rep. 2012;12:204-212.
29. Hussein Z, Hamdy O, Chin Chia Y, et al. Transcultural diabetes nutrition algorithm: a Malaysian application. Int J Endocrinol. 2013;2013:679396.
30. Gougeon R, Sievenpiper JL, Jenkins D, et al. The trans- cultural diabetes nutrition algorithm: a Canadian perspec- tive. Int J Endocrinol. 2014;2014:151068.
31. Nieto-Martínez R, Hamdy O, Marante D, et al. Transcultural diabetes nutrition algorithm (tDNA): Venezuelan application. Nutrients. 2014;6:1333-1363.
32. Bolio-Galvis A, Hamdy O, Escalante-Pulido M, et al. Transcultural diabetes nutrition algorithm: the Mexican Application. J Diabetes Metab. 2014;5:423.
33. Moura F, Salles J, Hamdy O, et al. Transcultural diabetes nutrition algorithm: Brazilian application. Nutrients. 2015; 7:7358-7380.
34. Mechanick JI, Marchetti AE, Apovian C, et al. Diabetes- specific nutrition algorithm: a transcultural program to optimize diabetes and prediabetes care. Curr Diab Rep. 2012;12:180-194.
35. Hamdy O, Marchetti A, Hegazi RA, Mechanick JI. The transcultural diabetes nutrition algorithm toolkit: survey and content validation in the United States, Mexico, and Taiwan. Diabetes Technol Ther. 2014;16:378-384.
36. United Nations General Assembly. Document A/ RES/61/225: World Diabetes Day. Available at: http:// www.un.org/ga/search/viewm_doc.asp?symbol=A/ RES/61/225. Accessed November 23, 2015.
37. United Nations General Assembly. Document A/66/L.1: Political Declaration of the High-Level Meeting of the General Assembly on the Prevention and Control of Non- communicable Diseases. Available at: http://www.un.org/ ga/search/view_doc.asp?symbol=A/66/L.1. Accessed February 5, 2016.
38. Mendis S, Chestnov O. Policy reform to realize the com- mitments of the political declaration on noncommunicable diseases. Br Med Bull. 2013;105:7-27.
39. Lirussi F. The global challenge of type 2 diabetes and the strategies for response in ethnic minority groups. Diabetes Metab Res Rev. 2010;26:421-432.
40. United Nations. Time for Global Action 2015. Available at: http://www.un.org/sustainabledevelopment/blog/2015/02/ time-for-global-action-2015/. Accessed September 28, 2015.
41. Garber AJ, Abrahamson MJ, Barzilay JI, et al. AACE/ ACE comprehensive diabetes management algorithm 2015. Endocr Pract. 2015;21:438-447.
42. Handelsman Y, Bloomgarden ZT, Grunberger G, et al. American Association of Clinical Endocrinologists and American College of Endocrinology – clinical practice guidelines for developing a diabetes mellitus comprehen- sive care plan – 2015. Endocr Pract. 2015;21 (suppl 1): 1-87.
43. Peleg M, Fox J, Patkar V, et al. A computer-interpretable version of the AACE, AME, ETA medical guidelines for clinical practice for the diagnosis and management of thy- roid nodules. Endocr Pract. 2014;20:352-359.
44. Watts NB, Bilezikian JP, Camacho PM, et al. American Association of Clinical Endocrinologists medical guide- lines for clinical practice for the diagnosis and treatment of postmenopausal osteoporosis. Endocr Pract. 2010;16 (suppl 3):1-37.
45. Hsu CC, Sandford BA. The Delphi technique: making sense of consensus. Available at: http://www.pareonline. net/getvn.asp?v=12&n=10. Accessed October 2, 2015.
46. International Diabetes Federation. IDF Diabetes Atlas 2014, 6th ed. Available at: http://www.idf.org/sites/default/ files/Atlas-poster-2014_EN.pdf. Accessed September 30, 2015.
47. Chen L, Magliano DJ, Zimmet PZ. The worldwide epi- demiology of type 2 diabetes mellitus--present and future perspectives. Nat Rev Endocrinol. 2011;8:228-236.
48. Danaei G, Finucane MM, Lu Y, et al. National, regional, and global trends in fasting plasma glucose and diabe- tes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011; 378:31-40.
49. Fazeli Farsani S, van der Aa MP, van der Vorst MM,
Knibbe CA, de Boer A. Global trends in the incidence and prevalence of type 2 diabetes in children and ado- lescents: a systematic review and evaluation of meth- odological approaches. Diabetologia. 2013;56:1471- 1488.
50. Mudaliar U, Kim WC, Kirk K, Rouse C, Narayan KM,
Ali M. Are recommended standards for diabetes care met in Central and South America? A systematic review. Diabetes Res Clin Pract. 2013;100:306-329.
51. Echouffo-Tcheugui JB, Kengne AP. On the importance of global cardiovascular risk assessment in people with type 2 diabetes. Prim Care Diabetes. 2013;7:95-102.
52. de Almeida-Pititto B, Dias ML, de Moraes AC, Ferreira SR, Franco DR, Eliaschewitz FG. Type 2 diabetes in Brazil: epidemiology and management. Diabetes Metab Syndr Obes. 2015;8:17-28.
53. Barquera S, Campos-Nonato I, Aguilar-Salinas C,
Lopez-Ridaura R, Arredondo A, Rivera-Dommarco J. Diabetes in Mexico: cost and management of diabetes and its complications and challenges for health policy. Global Health. 2013;9:3.
54. Cerdas M. Epidemiology and control of hypertension and diabetes in Costa Rica. Ren Fail. 2006;28:693-696.
55. Barcelo A, Gregg EW, Gerzoff RB, et al. Prevalence of diabetes and intermediate hyperglycemia among adults from the first multinational study of noncommunicable diseases in six Central American countries: the Central America Diabetes Initiative (CAMDI). Diabetes Care. 2012;35:738-740.
56. Allende-Vigo MZ, Pérez CM, Hernández JJ, et al. Unequal burden of diabetes and hypertension in the adult population of the San Juan metropolitan area of Puerto Rico. J Diabetes Metab. 2013;4:261.
57. Aschner P, Aguilar-Salinas C, Aguirre L, et al. Diabetes in South and Central America: an update. Diabetes Res Clin Pract. 2014;103:238-243.
58. Aschner P. Diabetes trends in Latin America. Diabetes Metab Res Rev. 2002;18(suppl 3):S27-S31.

500 Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4)
59. Concha JB, Mezuk B, Duran B. Culture-centered overweight and obesity in Latin America: a systematic
approaches: the relevance of assessing emotional health for Latinos with type 2 diabetes. BMJ Open Diabetes Res Care. 2015;3:e000064.
60. Escalante M, Gagliardino JJ, Guzmán JR, Tschiedel B. Call-to-action: timely and appropriate treatment for people with type 2 diabetes in Latin America. Diabetes Res Clin Pract. 2014;104:343-352.
61. Guzmán JR, Lyra R, Aguilar-Salinas CA, et al. Treatment of type 2 diabetes in Latin America: a con- sensus statement by the medical associations of 17 Latin American countries. Latin American Diabetes Association. Rev Panam Salud Publica. 2010;28:463-471.
62. Lahti-Koski M, Pietinen P, Heliövaara M, Vartiainen E. Associations of body mass index and obesity with phys- ical activity, food choices, alcohol intake, and smoking in the 1982-1997 FINRISK studies. Am J Clin Nutr. 2002; 75:809-817.
63. Mechanick JI, Garber AJ, Handelsman Y, Garvey WT. American Association of Clinical Endocrinologists’ posi- tion statement on obesity and obesity medicine. Endocr Pract. 2012;18:642-648.
64. American Medical Association House of Delegates. Resolution 420 (A-13). Available at: http://www.npr. org/documents/2013/jun/ama-resolution-obesity.pdf. Accessed January 31, 2015.
65. Garvey WT, Garber AJ, Mechanick JI, et al. American Association of Clinical Endocrinologists and American College of Endocrinology consensus conference on obe- sity: building an evidence base for comprehensive action. Endocr Pract. 2014;20:956-976.
66. Garvey WT, Garber AJ, Mechanick JI, et al. American Association of Clinical Endocrinologists and American College of Endocrinology position statement on the 2014 advanced framework for a new diagnosis of obesity as a chronic disease. Endocr Pract. 2014;20:977-989.
67. Perez LG, Arredondo EM, Elder JP, Barquera S, Nagle B, Holub CK. Evidence-based obesity treatment interven- tions for Latino adults in the U.S.: a systematic review. Am J Prev Med. 2013;44:550-560.
68. Holub CK, Elder JP, Arrendondo EM, et al. Obesity control in Latin American and U.S. Latinos: a systematic review. Am J Prev Med. 2013;44:529-537.
69. World Health Organization. Obesity and overweight. Fact sheet No. 311. Available at: http://www.who.int/medi- acentre/factsheets/fs311/en/. Accessed January 31, 2015.
70. Pérez Rodrigo C. Current mapping of obesity. Nutr Hosp. 2013;28(suppl 5):21-31.
71. Popkin BM, Slining MM. New dynamics in global obe- sity facing low- and middle-income countries. Obes Rev. 2013;14(suppl 2):11-20.
72. Rojas R, Aguilar-Salinas CA, Jiménez-Corona A, et al. Metabolic syndrome in Mexican adults: results from the National Health and Nutrition Survey 2006. Salud Publica Mex. 2010;52(suppl 1);S11-S18.
73. Barquera S, Campos-Nonato I, Hernández-Barrera L, Pedroza A, Rivera-Dommarco JA. Prevalence of obesity in Mexican adults 2000-2012 [in Spanish]. Salud Publica Mex. 2013;55(suppl 2):S151-S160.
74. Aschner P, Buendía R, Brajkovich I, et al. Determination of the cutoff point for waist circumference that establishes the presence of abdominal obesity in Latin American men and women. Diabetes Res Clin Pract. 2011;93:243-247.
75. Rivera JÁ, de Cossío TG, Pedraza LS, Aburto TC, Sánchez TG, Martorell R. Childhood and adolescent
review. Lancet Diabetes Endocrinol. 2014;2:321-332. 76. Cuevas A, Alvarez V, Olivos C. The emerging obesity
problem in Latin America. Expert Rev Cardiovasc Ther. 2009;7:281-288.
77. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in chil- dren and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384:766-781.
78. World Health Organization. Global status report on non- communicable diseases, 2014. Available at: http://apps. who.int/iris/bitstream/10665/148114/1/9789241564854_ eng.pdf?ua=1. Accessed February 5, 2016.
79. Rtveladze K, Marsh T, Webber L, et al. Health and economic burden of obesity in Brazil. PLoS One. 2013;8:e68785.
80. Pérez-Escamilla R, Villalpando S, Shamah-Levy T,
Méndez-Gómez Humarán I. Household food insecurity, diabetes and hypertension among Mexican adults: results from Ensanut 2012. Salud Publica Mex. 2014;56(suppl 1):S62-S70.
81. Kroker-Lobos MF, Pedroza-Tobías A, Pedraza LS,
Rivera JA. The double burden of undernutrition and excess body weight in Mexico. Am J Clin Nutr. 2014;100: 1652S-1658S.
82. Bermudez OI, Tucker KL. Trends in dietary patterns of Latin American populations. Cad Saude Publica. 2003;19(suppl 1):S87-S99.
83. Rtveladze K, Marsh T, Barquera S, et al. Obesity preva- lence in Mexico: impact on health and economic burden. Public Health Nutr. 2014;17:233-239.
84. Popkin BM. Is the obesity epidemic a national security issue around the globe? Curr Opin Endocrinol Diabetes Obes. 2011;18:328-331.
85. Gómez EJ. Responding to obesity in Brazil: understand- ing the international and domestic politics of policy reform through a nested analytic approach to comparative analysis. J Health Polit Policy Law. 2015;40:73-99.
86. Trivedi NJ, Fields J, Mechanick CH, Klein M, Mechanick JI. Lack of correlation between antiobesity policy and obesity growth rates: review and analysis. Endocr Pract. 2012;18:737-744.
87. Arbex AK, Rocha DR, Aizenberg M, Ciruzzi MS. Obesity epidemic in Brazil and Argentina: a public health concern. J Health Popul Nutr. 2014;32:327-334.
88. Cataife G. Small area estimation of obesity prevalence and dietary patterns: a model applied to Rio de Janeiro city, Brazil. Health Place. 2014;26:47-52.
89. Garmendia ML, Corvalan C, Uauy R. Addressing mal- nutrition while avoiding obesity: minding the balance. Eur J Clin Nutr. 2013;67:513-517.
90. Sharma AM, Kushner RF. A proposed clinical staging system for obesity. Int J Obes (Lond). 2009;33:289-295.
91. Guo F, Moellering DR, Garvey WT. The progression of cardiometabolic disease: validation of a new cardiometa- bolic disease staging system applicable to obesity. Obesity (Silver Spring). 2014;22:110-118.
92. Mechanick JI, Youdim A, Jones DB, et al. Clinical practice guidelines for the perioperative nutritional, metabolic, and nonsurgical support of the bariatric sur- gery patient--2013 update: cosponsored by American Association of Clinical Endocrinologists, the Obesity Society, and American Society for Metabolic & Bariatric Surgery. Endocr Pract. 2013;19:337-372.

Transculturalization Conference Proceedings, Endocr Pract. 2016;22(No. 4) 501
93. Yang SP, Ying LS, Saw S, Tuttle RM, Venkataraman K,
Su-Ynn C. Practical barriers to implementation of thyroid cancer guidelines in the Asia-Pacific region. Endocr Pract. 2015;21:1255-1268.
94. Huang TW, Lai JH, Wu MY, Chen SL, Wu CH, Tam
KW. Systematic review of clinical practice guidelines in the diagnosis and management of thyroid nodules and can- cer. BMC Med. 2013;11:191.
95. Camargo R, Corigliano S, Friguglietti C, et al. Latin American Thyroid Society recommendations for the man- agement of thyroid nodules. Arq Bras Endocrinol Metabol. 2009;53:1167-1175.
96. Pitoia F, Ward L, Wohllk N, et al. Recommendations of the Latin American Thyroid Society on diagnosis and management of differentiated thyroid cancer. Arq Bras Endocrinol Metabol. 2009;53:884-887.
97. La Vecchia C, Malvezzi M, Bosetti C, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer. 2015;136:2187-2195.
98. Doll R, Peto R. The causes of cancer: quantitative esti- mates of avoidable risks of cancer in the United States today. J Natl Cancer Inst. 1981;66:1191-1308.
99. Guimarães RM, Muzi CD, Parreira VG, Santos RD, Sampaio JR. Evolution of thyroid cancer mortality in adults in Brazil. Arq Bras Endocrinol Metabol. 2013;57: 538-544.
100. Cuello C, Correa P, Haenszel W. Socio-economic class differences in cancer incidence in Cali, Colombia. Int J Cancer. 1982;29:637-643.
101. Ministerio de Salud. EstadÃ-stica de CÃncer - Registro Nacional Tumores. Available at: www.ministeriodesalud. go.cr/index.php/vigilancia-de-la-salud/estadisticas-y- bases-de-datos/estadisticas/estadistica-de-cancer-registro- nacional-tumores. Accessed April 4, 2015.
102. Veiga LH, Neta G, Aschebrook-Kilfoy B, Ron E, Devesa SS. Thyroid cancer incidence patterns in Sao Paulo, Brazil, and the U.S. SEER Program, 1997-2008. Thyroid. 2013;23:748-757.
103. Robles-Osorio ML, Zacarías-Rangel V, García-Solís P, Hernández-Montiel HL, Solís JC, Sabath E. Prevalence of thyroid function test abnormalities and anti-thyroid antibodies in an open population in Central Mexico. Rev Invest Clin. 2014;66:113-120.
104. Zimmermann MB, Boelaert K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015;3: 286-295.
105. Brito Ados S, Coeli CM, Barbosa Fdos S, Caetano R,
Santos Mde O, Vaisman M. Estimates of thyroid cancer incidence in Brazil: an approach using polynomial models. Cad Saude Publica. 2011;27:1441-1444.
106. Baloch ZW, Cibas ES, Clark DP, et al. The National Cancer Institute Thyroid Fine Needle Aspiration State of the Science Conference: a summation. Cytojournal. 2008;5:6.
107. Bongiovanni M, Spitale A, Faquin WC, Mazzucchelli L,
Baloch ZW. The Bethesda System for Reporting Thyroid Cytopathology: a meta-analysis. Acta Cytol. 2012;56: 333-339.
108. Rodríguez-Cuevas S, Labastida-Almendaro S,
Cortés-Arroyo H, López-Garza J, Barroso-Bravo S. Multifactorial analysis of survival and recurrences in differ- entiated thyroid cancer. Comparative evaluation of useful- ness of AGES, MACIS, and risk group scores in Mexican population. J Exp Clin Cancer Res. 2002;21:79-86.
109. Radiopaedia.org. Thyroid image reporting and data system (TIRADS). Available at: http://radiopaedia.org/ articles/thyroid-image-reporting-and-data-system-tirads. Accessed October 4, 2015.
110. Clark P, Cons-Molina F, Deleze M, et al. The preva- lence of radiographic vertebral fractures in Latin American countries: the Latin American Vertebral Osteoporosis Study (LAVOS). Osteoporos Int. 2009;20:275-282.
111. Sen SS, Rives VP, Messina OD, et al. A risk assessment tool (OsteoRisk) for identifying Latin American women with osteoporosis. J Gen Intern Med. 2005;20:245-250.
112. World Health Organization. WHO Scientific Group on the Assessment of Osteoporosis at Primary Health Care Level: Summary Meeting Report, Brussels, Belgium, 5-7 May 2004. Available at: http://www.who.int/chp/topics/ Osteoporosis.pdf. Accessed February 5, 2016.
113. Carlos F, Clark P, Galindo-Suárez RM, Chico-Barba LG. Health care costs of osteopenia, osteoporosis, and fra- gility fractures in Mexico. Arch Osteoporos. 2013;8:125.
114. Marinho BC, Guerra LP, Drummond JB, Silva BC, Soares MM. The burden of osteoporosis in Brazil. Arq Bras Endocrinol Metabol. 2014;58:434-443.
115. Prentice A. Diet, nutrition and the prevention of osteopo- rosis. Public Health Nutr. 2004;7:227-243.
116. Resch H, Walliser J, Phillips S, Wehren LE, Sen SS. Physician and patient perceptions on the use of vitamin D and calcium in osteoporosis treatment: a European and Latin American perspective. Curr Med Res Opin. 2007;23: 1227-1237.
117. Copês RM, Comim FV, Langer FW, et al. Obesity and fractures in postmenopausal women: a primary-care cross- sectional study at Santa Maria, Brazil. J Clin Densitom. 2015;18:165-171.
118. Moraes LF, Silva EN, Silva DA, Paula AP. Expenditures on the treatment of osteoporosis in the elderly in Brazil (2008-2010): analysis of associated factors [in English, Portuguese]. Rev Bras Epidemiol. 2014;17:719-734.
119. Pinheiro MM, Ciconelli RM, Jacques Nde O, Genaro PS, Martini LA, Ferraz MB. The burden of osteoporosis in Brazil: regional data from fractures in adult men and women--the Brazilian Osteoporosis Study (BRAZOS). Rev Bras Reumatol. 2010;50:113-127.
120. World Health Organization. WHO Fracture Risk Assessment Tool. Available at: http://www.shef.ac.uk/ FRAX/tool.jsp?locationValue=9. Accessed September 30, 2015.


















