Pharmaceutical Benefits Under State Medical Assistance Programs, 2007

©2017 MFMER | slide-1
AAA Bedside Assistance: Pharmaceutical Management of Abdominal Aortic AneurysmsJanelle O. Poyant, PharmD, BCPSPGY2 Critical Care Pharmacy Resident
Pharmacy Grand RoundsJanuary 31, 2017

©2017 MFMER | slide-2
Presentation Objectives• Review the pathophysiology of abdominal aortic
aneurysms• Discuss the optimal hemodynamic goals in the
management of acute abdominal aortic aneurysms
• Describe the pharmaceutical management approach for both acute and chronic abdominal aortic aneurysms

©2017 MFMER | slide-3
Kent KC, Solomon CG. N Engl J Med 371.22(2014): 2101-108
Higher aortic wall
stress
Decreased aortic wall strength
Progressive aortic
expansionAortic
dilation
AAA Pathophysiology
Immune response
Oxidative stressThrombosis
Inflammation

©2017 MFMER | slide-4
Risk Factors
Development• Advanced age • Male gender• Caucasian race• Smoking• Family history• Other aneurysms• Atherosclerosis• Genetics
Expansion• Size >5.5 cm• Rate >0.5 cm in 6
months• Female gender• HTN• Elevated wall stress• Recent surgery• Smoker
Aggarwal S, et al. Exp Clin Cardiol;2011:16(10):11-15HTN: hypertension

©2017 MFMER | slide-5
Aortic Arch
Descending Aorta
Suprarenal
Infrarenal
Pararenal
Diaphragm
Ascending Aorta
Aortic Root
AAA Pathophysiology
≥3 cm

©2017 MFMER | slide-6
Aortic Dissection
Acute AD Subacute AD Chronic AD<14 days 15-90 days >90 days
Erbel R, et al. Eur Heart J 2014;35(41):2873-2926Image: http://www.mayoclinic.org/diseases-conditions
• Intramural bleeding• Separation of aortic
wall layers• Intimal layer tears
• Propagation of dissection
• High mortality if untreated

©2017 MFMER | slide-7
Classification Systems of Aortic Dissection
Erbel R, et al. Eur Heart J 2014;35(41):2873-2926Thrumurthy SG, et al. BMJ 2011;344:d8290
StanfordA: Ascending aorta affectedB: Ascending aorta not affected
DeBakeyI: Originates in ascending aortaII: Originates in and is confined to ascending aortaIII: Originates in descending aorta and extends distally

©2017 MFMER | slide-8
The pathophysiology of aortic aneurysms is characterized by mechanisms leading to higher aortic wall stress
A. TrueB. False

©2017 MFMER | slide-9
Patient JL• 54 year old male with sudden onset of pain and
numbness of his legs
• HTN• No home medicationsPMH
• One ppd cigarettes• One case of beer per daySH
PMH: past medical historySH: social historyPPD: pack per dayBP: blood pressureHR: heart rate
BP HR Respiratory Rate Temperature Saturation218/166 mmHg 118 bpm 22 bpm 37.2°F 97% RA

©2017 MFMER | slide-10
Erbel R, et al. Eur Heart J 2014;35(41):2873-2926Golledge J, Eagle KA. Lancet 2008;372:55-66
Clinical Presentation
Acute AD
Chest pain
Radiation to the back and/or abdomen
Chronic AAAPain and tenderness
on palpitation
Incidental finding

©2017 MFMER | slide-11
• Aortic regurgitation• Cardiac tamponade• Malperfusion of:
• Brain• Coronary artery
• Malperfusion of:• Spinal cord• Legs• Liver• Bowel• Kidneys
Image adapted from: Golledge J, Eagle KA. Lancet 2008;372:55-66
Clinical Presentation of Aortic Dissection

©2017 MFMER | slide-12
Patient JL
• Hypertensive emergency
CTA Chest/AbdomenStanford type B aortic dissection extends from just distal to the origin of the left subclavian artery through the abdominal aorta and iliac arteries bilaterally
HR 118218/166 mmHg
First-line intervention
HR 70166/100 mmHg
Second-line intervention
CTA: computed tomography angiogram
GOAL
©2017 MFMER | slide-13
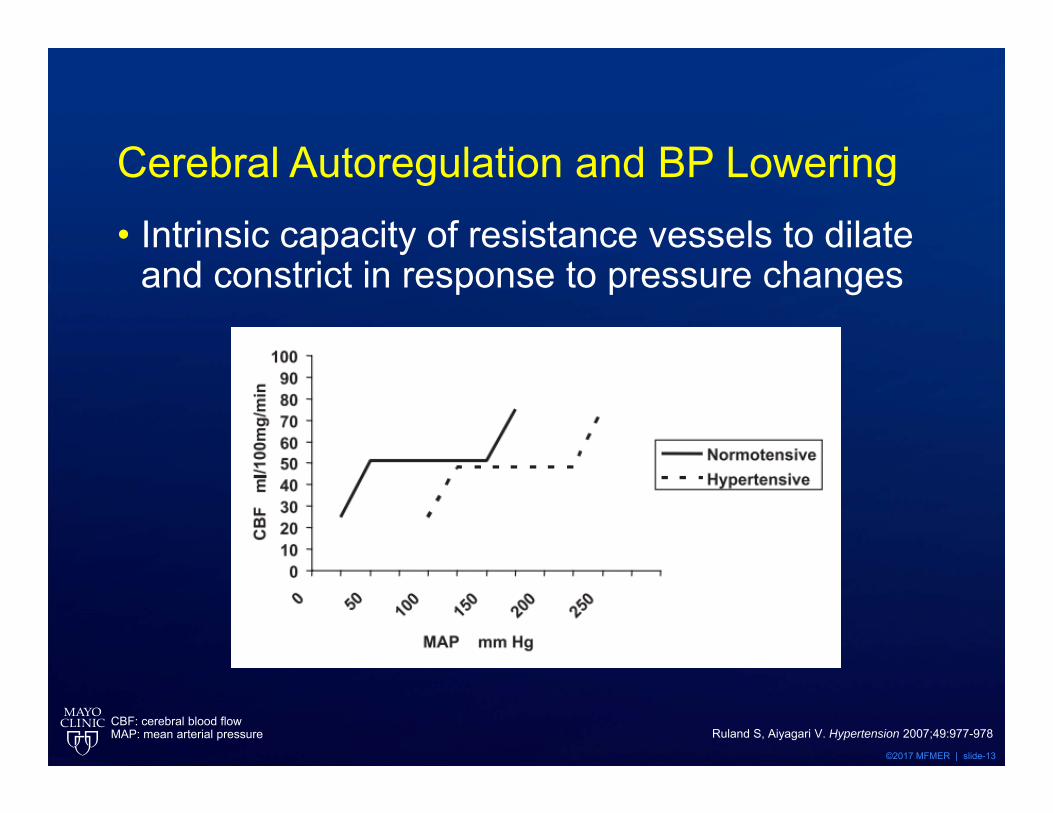
Cerebral Autoregulation and BP Lowering• Intrinsic capacity of resistance vessels to dilate
and constrict in response to pressure changes
Ruland S, Aiyagari V. Hypertension 2007;49:977-978CBF: cerebral blood flowMAP: mean arterial pressure

©2017 MFMER | slide-14
Acute AD: Medical Management
Marik PE, Varon J. Chest 2007;131;1949-1962Stayer et al. Current Cardiology Revi
• Decrease aortic wall stress then SBP• A vasodilator alone is not ideal
Shear stress SBPdp
dtHR

©2017 MFMER | slide-15
Acute AD: Medical Management
HR 60-70 bpm
SBP 110-120 mmHg
MAP 60-80 mmHg
Marik PE, Varon J. Chest 2007;131;1949-1962
• Control of pain and anxiety • Hydromorphone, fentanyl

©2017 MFMER | slide-16
Ideal Pharmaceutical Agent• Short-acting• Continuous infusion• Titratable • Avoid
• Oral• Sublingual• Intramuscular
Marik PE, Varon J. Chest 2007;131;1949-1962
©2017 MFMER | slide-17
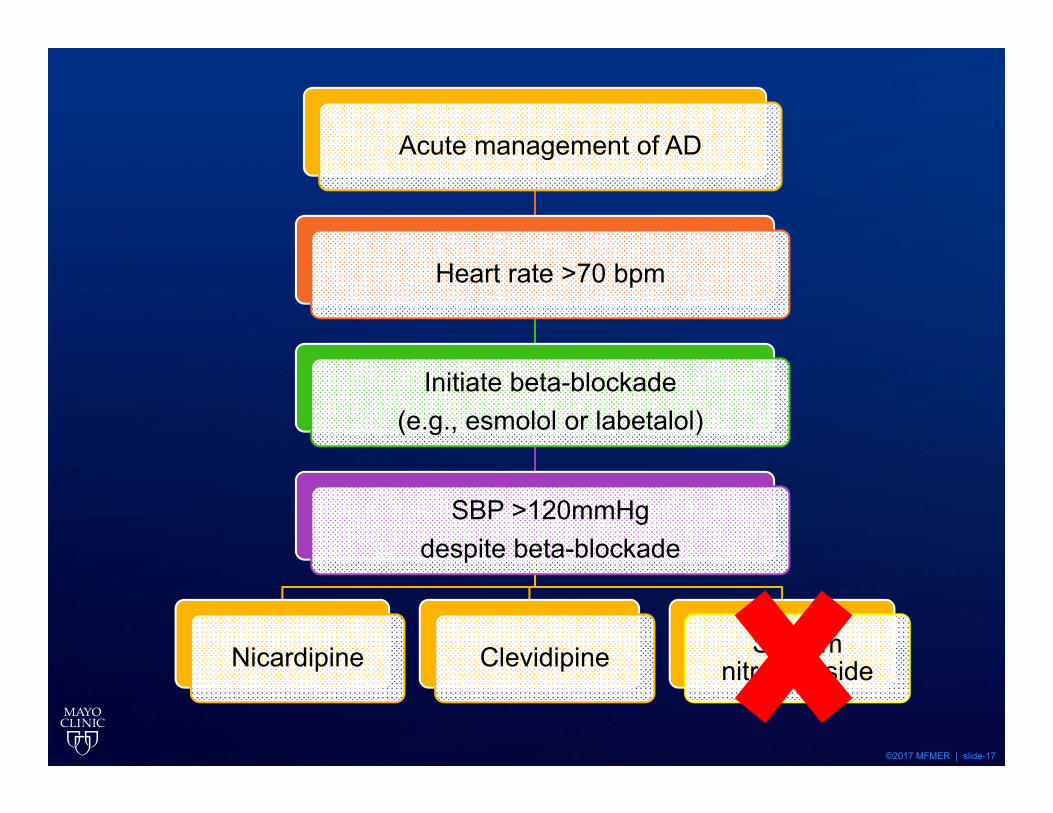
Acute management of AD
Heart rate >70 bpm
Initiate beta-blockade (e.g., esmolol or labetalol)
SBP >120mmHg despite beta-blockade
Nicardipine Clevidipine Sodium nitroprusside

©2017 MFMER | slide-18
Clevidipine • Third generation dihydropyridine CCB• Reduces afterload without
• affecting cardiac filling pressures • causing reflex tachycardia
• Rapid onset and offset of action
Rhoney D, Peacock WF AJHP 2009;66:1343-52Marik PE, Varon J. Chest 2007;131;1949-1962
No bolusInfusion
1-2 mg/hrMaximum 21 mg/hr
CCB: calcium channel blocker

©2017 MFMER | slide-19
Agents to Avoid in Initial Management• Nitroglycerin
• Reflex tachycardia• Reduction in preload and cardiac output
• Hydralazine• Prolonged and unpredictable
antihypertensive effects• Inability to titrate
Rhoney D, Peacock WF AJHP 2009;66:1343-52Marik PE, Varon J. Chest 2007;131;1949-1962

©2017 MFMER | slide-20
JL presents with a BP of 218/166 mmHg with HRs in110s. A Type B AAA is found on CT. JL has a PMH of HTN, HL and DM. What is the best method to optimize JL’s hemodynamics at this time?
A. Reduce DBP by 10-15% over 30-60 minutesB. Reduce DBP to ~110 mmHg over 30-60
minutesC. Reduce HR to <60 then reduce SBP to <120
mmHg as quickly as possibleD. Reduce SBP to <180 mmHg over <20
minutes while reducing HR to <80HL: hyperlipidemiaDM: diabetes mellitus

©2017 MFMER | slide-21
What do you recommend for JL’s initial pharmacologic therapy?
A. NicardipineB. NitroprussideC. ClevidipineD. Esmolol

©2017 MFMER | slide-22
Postoperative Pearls• Spinal drains
• Reduce the rate of paraplegia• Continued 72 hours postoperatively
• Increased MAP goals• 80-90 mmHg
• ATN• Reinitiation of thromboembolism prophylaxis is
surgeon-dependent
Erbel R, et al. Eur Heart J 2014;35(41):2873-2926Bethel SA. J Vasc Nurs 1999;17(3):53-58
Crawford ES, et al. J Vasc Surg 1986;3:389-404CSF: cerebrospinal fluidATN: acute tubular necrosis

©2017 MFMER | slide-23
Transitioning to Oral Agents
• Overlap IV therapy with oral• Utilize higher doses and multiple mechanisms
HR 60-70 bpm
SBP 110-120 mmHg
MAP 60-80 mmHg

©2017 MFMER | slide-24
Chronic AAA: Medical Management • Open repair versus surveillance
• No statistically significant effect of intervention on survival
• Surgery reserved for complicated AAAs• International Registry of Aortic Dissection (IRAD)
• 73% managed medically• Survival at ten years is ~40-45%
• Options for pharmaceutical stabilization?
Suzuki T, et al. Circulation 2003;108(S1):II312-7Tsai Ttet al. Circulation.2005;112:3802–13
Doroghazi RM, et al. J Am Coll Cardiol. 1984;3:1026 –1034Filardo G. Mayo Clin Proc 2013;88(9):910-919

©2017 MFMER | slide-25
Role of β-Blockers
Leach SD, et al. Arch Surg 1988;123:606-9Gadowski GR, et al. J Vasc Surg 1994;19(4):727-31
AAA Expansion Rate: Effect of Size and β–adrenergic Blockade
Design Prospective, observational, cohort studyPrimary endpoint AAA expansion rateInclusion criteria Patient with AAA <5 cm or contraindications to surgery
Demographics β-blocker (n=83)
No β-blocker (n=38) p-value
Age* (years) 67 ± 10 68 ± 8 0.56Male 74% 71% 0.97Initial size* (cm) 4.0 ± 0.8 4.0 ± 0.7 1.0SBP* (mmHg) 154 ± 18 151 ± 20 0.43
*mean ± SD

©2017 MFMER | slide-26
Role of β-Blockers
Gadowski GR, et al. J Vasc Surg 1994;19(4):727-31
Result β-blocker No β-blocker p-valueExpansion rate* 0.38 ± 0.44**Expansion rate* 0.30 ± 0.3** 0.44 ± 0.42** NSLarge AAA expansion rate* 0.36 ± 0.20** 0.68 ± 0.64** < 0.02Rupture rate 5% 13% NS
• Significantly faster expansion with aneurysms >5.0 cm without β-blockers
00.10.20.30.40.50.60.7
3.0-3.9 4.0-4.9 ≥5
Gro
wth
Rat
e (c
m/y
r)
Aneurysm Diameter (cm)
β-blockerNo β-blocker
p<0.05
p<0.02
*mean ± SD**cm/year

©2017 MFMER | slide-27
Role of β-Blockers: Application to Practice• β-blockers reduce wall shear stress and
subsequently reduce AAA growth • Potential benefit in cohort studies• Not confirmed in three RCTs
• Pooled growth rate difference: -0.005 cm/yr, 95% CI -0.016 to 0.005
Erbel R, et al. Eur Heart J 2014;35(41):2873-2926Guessous I, et al. PLoS One 2008;3:e1895
Rughani G, et al. Cochrane Database Syst Rev 2012;9:CD009536
It is reasonable to reduce BP with β-blockers to the lowest point patients can
tolerate without AE
AE: adverse effects

©2017 MFMER | slide-28
Role of ACE-I• Suggested benefit
• Case control study for rupture prevention (OR 0.82; 95% CI 0.74-0.90)
• Possible harm• Prospective cohort study indicating
significant increase in aneurysm growth rate • Guidelines
• Conflicting and moderate quality evidence
Hackem DJ. Lancet 2006;368:659-65Sweeting MJ. J Vasc Surg 2010;52:1-4ACE-I: angiotensin-converting-enzyme inhibitor

©2017 MFMER | slide-29
Role of ACE-I
Aortic aneurysmal regression of dilation: value of ACE-inhibition on risk (AARDVARK)
Design Multicenter, single-blind, randomized, three arm, placebo-controlled
Primary endpoint Aneurysm growth rate
Intervention Perindopril 10mg, amlodipine 5mg or placebo
Population
Inclusion: Patients ≥55 years, AAA diameter 3.0-5.4 cm and SBP <150 mmHg
Exclusion: ACE-I, ARB, known renal artery stenosis , SCr > 2, unable to complete 3–6 monthly surveillance
SCr: serum creatinine Bicknell CD. Eur Heart Jour 2016;37:3213-3221

©2017 MFMER | slide-30
Role of ACE-I
• Perindopril and amlodipine effectively lowered SBP but did not affect AAA growth
• Perindopril did not affect the overall growth rate of AAAs during 2 years of follow up
Comparison Difference in average growth rate p-value
Perindopril vs. Placebo 0.8 cm NSAmlodipine vs. Placebo 1.2 cm NS
Bicknell CD. Eur Heart Jour 2016;37:3213-3221

©2017 MFMER | slide-31
ACE-I Application to Practice• Excellent follow-up• Drug compliance assessed (and excellent)• Limitations
• Lack of generalizability • Intra- and inter-observer variability
It is reasonable to reduce BP with ACE-I to the lowest point patients
can tolerate without AEBicknell CD. Eur Heart Jour 2016;37:3213-3221

©2017 MFMER | slide-32
Role of Statins• Chronic AAA
• May inhibit expansion of aneurysms• Small observational studies
• Post-AAA repair• Association with improved survival
• 3x reduction in the risk of CV death• The use of statins may be considered to reduce
aortic complications in patients with small AAAs
Erbel R, et al. Eur Heart J 2014;35(41):2873-2926Jovin IS, et al. Am J Cardiol 2012;109:1050-54Stein LH, et al. Am J Cardiol 2013;112:1240-45De Bruin, et al. J Vasc Surg 2014;59:p39-44e1
CV: cardiovascular

©2017 MFMER | slide-33
Other Potential OptionsDrug Pathologic Target Outcome Result
DoxycyclineMatrix metalloproteinases and inflammation
AAA growth Faster in intervention group
Pemirolast Mast cell inhibitor AAA growth NSAmlodipine HTN AAA growth NS
Cyclosporine A Inflammation, matrixremodelling AAA growth Recruiting
Ticagrelor AAA thrombus, inflammation AAA growth Ongoing
ValsartanAngiotensin II, inflammation, matrix remodelling
AAA growth Ongoing
Golledge, et al. J Vasc Surg 2017;65:225-35Clinicaltrials.gov/NCT02225756Clinicaltrials.gov/NCT02070653Clinicaltrials.gov/NCT01904981

©2017 MFMER | slide-34
Chronic Management• Stringent control of risk factors
• Smoking cessation• Moderate physical activity
• Optimization of comorbid conditions• Strict BP and HR control
• 110-120 mmHg• 60-70 bpm
• Serial imaging
Erbel R, et al. Eur Heart J 2014;35(41):2873-2926Aggarwal S, et al Exp Clin Cardiol 2011;16(1):11-15
Tsai Ttet al. Circulation.2005;112:3802–13

©2017 MFMER | slide-35
Acute AD
HR 60-70 bpm and
SBP 110-120 mmHg
Surgical intervention
IV β-blocker then IV
vasodilator
Chronic AAA
Chronic Medical
Management
HR 60-70 bpm and
SBP 110-120 mmHg
β-blocker, ACE-inhibitor
Thrumurthy SG, et al. BMJ 2011;344:d8290Erbel R, et al. Eur Heart J 2014;35(41):2873-2926

©2017 MFMER | slide-36
Conclusion• Mechanisms leading to aortic aneurysms
surround higher wall stress• No RCTs have been reported to guide acute
management of acute AD• Acute management should be focused on
HR control then BP lowering• Pharmaceutical stabilization of AAA is an unmet
medical need

©2017 MFMER | slide-38
Esmolol• β1-adrenergic antagonist• Rapid onset with a short duration of action• Caution in decompensated heart failure and
reactive airway disease
Rhoney D, Peacock WF AJHP 2009;66:1343-52Marik PE, Varon J. Chest 2007;131;1949-1962
Bolus 500 mcg/kg
Infusion50 mcg/kg/min
Maximum300 mcg/kg/min

©2017 MFMER | slide-39
Labetalol• α1- and nonselective β-adrenergic antagonist• Increased β receptor activity in IV formulation• Quick onset with short duration of action• Caution in reactive airway disease, COPD, HF,
and second or third decree AV block
Rhoney D, Peacock WF AJHP 2009;66:1343-52Kitiyakara C, et al. J Am Soc Nephrol 1998;9:133-42
Marik PE, Varon J. Chest 2007;131;1949-1962
Bolus 20 mg
Incremental20-80 mg
Infusion0.5-4 mg/min
COPD: chronic obstructive pulmonary diseaseHF: heart failureAV: atrioventricular

©2017 MFMER | slide-40
Nicardipine• Second generation dihydropyridine CCB• Quick onset with moderate duration of action• Dosage is independent of weight• Reduces cardiac and cerebral ischemia
Rhoney D, Peacock WF AJHP 2009;66:1343-52Marik PE, Varon J. Chest 2007;131;1949-1962
No bolus Starting rate
5 mg/hrInfusion
5-15 mg/hr
CCB: calcium channel blocker

©2017 MFMER | slide-41
Nitroprusside• Arterial and venous vasodilator• Coronary steal• Contains 44% cyanide by weight
• Adequate liver and renal function required• Limit duration and dosage
Marik PE, Varon J. Chest 2007;131;1949-1962
No bolusInfusion
0.5-2 mcg/kg/minMaximum
2 mcg/kg/min