A YRBS Survey of Youth Risk Behaviors at Alternative High Schools and Mainstream High Schools in...
5
A YRBS Survey of Youth Risk Behaviors at Alternative High Schools and Mainstream High Schools in Hong Kong Albert Lee, Clement K. K. Tsang, Shiu-hung Lee, Cho-yee To ABSTRACT: In Hong Kong, prevocaiional schools serve as an aliemiive to mainsiream schools to provide educaiion wiih more emphasis on praciical and iechnical subjecis. In this paper, health-risk behaviors of prevocaiional school (PVS)siudenis were idenii- fied, and comparisons of healih-risk behaviors wiih or wiihoui adjusting ihe demographicfaciors from prevocaiional schools and mainsiream schools were made. The PVS students were at higher risk for most caiegories of healih-risk behaviors such as uninien- iional and inieniional injuries, smoking. alcohol drinking, glue sniflng, inadequaie physical aciiviiy, insuficieni consumption of fresh fruits and vegetables, and early sexual activity wiih muliiple pariners. Female siudenis of PVS reporied higher prevalence of emoiional problems and substance abuse. Findings suggesi ihai ihe school environment is an influenrial factor on ihe lifesiyle behav- ior of students. Comprehensive healih educaiion and inierveniion programs are needed for youih in Hong Kong prevocaiional schools. (J Sch Health. 2001;71(9):443-447) pproximately 5% of all secondary school (equivalent to A US high school) students enroll in prevocational schools (PVS) in Hong Kong.' The PVS serve as an alterna- tive to mainstream schools to provide education with more emphasis on practical and technical subjects rather than academic subjects. The PVS prepare students to enter apprenticeships so students with lower academic ability can complete their secondary education rather than drop- ping out. Studies show that low-achieving students experience more extreme negative effects of school transition from primary to secondary s c h o o l ~ . ~ ~ ~ Several investigators suggested that the transition to junior high school may contribute to the emergence of social, emotional, and behavioral problems that undermine healthy youth develop- ment.J~5 Students attending PVS have different levels of academic background, so they might have a higher risk of adopting risky health behavior. Currently, few local data are available to describe the health risks.6 In Hong Kong, the leading causes of morbidity and mortality relate to health behaviors such as smoking and alcohol, unhealthy dietary behavior, physical inactivity, and injuries.'-" Coronary heart disease, cancer, and stroke were the top three leading causes of death in Hong Kong for the past decade.' The changing pattern of disease from predom- inately infectious disease to chronic illnesses occurred mainly from unhealthy lifestyles. Lifestyle development starts early in life and continues throughout the learning process at schools. Research indicates that the experiences of children gained at school help determine their health behaviors during adolescence and beyond,'* and risk behav- iors for chronic disease among adolescents relate Albert Lee, MB, BS, MPH, (alee9cuhk.edu. hk), Associaie Professor, Communiiy and Family Medicine, and Director, Centre for Healih Educaiion and Healih Promoiion, School of Public Healih, The Chinese Universiiy of Hong Kong; Clement K. K. Tsang, MD, Leciurer, Community and Family Medicine, and Depuiy Director, Healthy Schools Program, The Chinese Universiiy of Hong Kong; Shiu-hung Lee, MB, BS, MD. Direcior, School of Public Healih. The Chinese University of Hong Kong; and Cho-yee To, MA, PhD. Professor, Educaiion, The Chinese University of Hong Kong: Depi. of Communiiy and Family Medicine, The Chinese Universiiy of Hong Kong, 4th poor, School of Public Healih Bldg.. Prince of Wales Hospiial, Shatin, N.T., Hong Kong. This study was supported in pari by the Qualiiy Educaiion Fund of the Hong Kong Government, Special Adminisiraiive Region. This article was submitted November 2, 2000, and revised and accepted for publication March 26,2001. commonly and inversely to socioeconomic status.13 Therefore, one would hypothesize that students not study- ing in mainstream schools would face higher risk of adopt- ing unhealthy lifestyles. This paper provides a comparative analysis of health-risk behaviors between students of PVS and students of mainstream schools to test the hypothesis. The results are of interest in Hong Kong and other devel- oped countries because many Asian countries face similar changing disease patterns as Hong Kong. Asians from well- developed countries also represent one of the major ethnic groups in North America and Europe. SURVEY PLANNING A cross-sectional study, the Youth Risk Behavior Survey (YRBS), was conducted by the Centre for Health Education and Health Promotion at The Chinese University of Hong Kong in 1999 as part of the Health Promoting School Programme.14The survey was administered to adolescent students aged 10-19 (from secondary grades 1 to 7) at secondary schools from a long-established school organiza- tion in Hong Kong. That organization manages schools of different academic levels, including PVS, in different geographical areas throughout the territory, so the sample population included a variety of students with different academic attainments. Profiles of the schools and the chil- dren suggest a reasonably representative sample was obtained. The self-administered YRBS covered six health behavior categories: unintentional and intentional injuries; tobacco use; alcohol use and other drug use; sexual behavior; unhealthy dietary behavior; and physical activity.IS The questionnaire also included demographic and morbidity data. Questions were translated into Chinese, then back translated into English. Questionnaire content was validated by face validity. The questionnaire was pilot-tested with students from different schools and different age groups. To ensure the quality of data collected, the research team visited each participating school to brief the teachers on details and objectives of the study. Letters also were sent to parents explaining the study objectives and to obtain permission for their children to participate voluntarily. Students were briefed about the purpose of the study, with strong emphasis on voluntary participation and anonymity of responses. The detailed methodology has been described elsewhere. l6 Journal of School Health November 2001, Vol. 71, No. 9 443
-
Upload
albert-lee -
Category
Documents
-
view
213 -
download
0
Transcript of A YRBS Survey of Youth Risk Behaviors at Alternative High Schools and Mainstream High Schools in...

A YRBS Survey of Youth Risk Behaviors at Alternative High Schools and Mainstream High Schools in Hong Kong Albert Lee, Clement K. K. Tsang, Shiu-hung Lee, Cho-yee To
ABSTRACT: In Hong Kong, prevocaiional schools serve as an aliemiive to mainsiream schools to provide educaiion wiih more emphasis on praciical and iechnical subjecis. In this paper, health-risk behaviors of prevocaiional school (PVS) siudenis were idenii- fied, and comparisons of healih-risk behaviors wiih or wiihoui adjusting ihe demographic faciors from prevocaiional schools and mainsiream schools were made. The PVS students were at higher risk for most caiegories of healih-risk behaviors such as uninien- iional and inieniional injuries, smoking. alcohol drinking, glue sniflng, inadequaie physical aciiviiy, insuficieni consumption of fresh fruits and vegetables, and early sexual activity wiih muliiple pariners. Female siudenis of PVS reporied higher prevalence of emoiional problems and substance abuse. Findings suggesi ihai ihe school environment is an influenrial factor on ihe lifesiyle behav- ior of students. Comprehensive healih educaiion and inierveniion programs are needed for youih in Hong Kong prevocaiional schools. (J Sch Health. 2001;71(9):443-447)
pproximately 5% of all secondary school (equivalent to A US high school) students enroll in prevocational schools (PVS) in Hong Kong.' The PVS serve as an alterna- tive to mainstream schools to provide education with more emphasis on practical and technical subjects rather than academic subjects. The PVS prepare students to enter apprenticeships so students with lower academic ability can complete their secondary education rather than drop- ping out.
Studies show that low-achieving students experience more extreme negative effects of school transition from primary to secondary s c h o o l ~ . ~ ~ ~ Several investigators suggested that the transition to junior high school may contribute to the emergence of social, emotional, and behavioral problems that undermine healthy youth develop- ment.J~5 Students attending PVS have different levels of academic background, so they might have a higher risk of adopting risky health behavior. Currently, few local data are available to describe the health risks.6
In Hong Kong, the leading causes of morbidity and mortality relate to health behaviors such as smoking and alcohol, unhealthy dietary behavior, physical inactivity, and injuries.'-" Coronary heart disease, cancer, and stroke were the top three leading causes of death in Hong Kong for the past decade.' The changing pattern of disease from predom- inately infectious disease to chronic illnesses occurred mainly from unhealthy lifestyles. Lifestyle development starts early in life and continues throughout the learning process at schools. Research indicates that the experiences of children gained at school help determine their health behaviors during adolescence and beyond,'* and risk behav- iors for chronic disease among adolescents relate
Albert Lee, MB, BS, MPH, (alee9cuhk.edu. hk), Associaie Professor, Communiiy and Family Medicine, and Director, Centre for Healih Educaiion and Healih Promoiion, School of Public Healih, The Chinese Universiiy of Hong Kong; Clement K . K. Tsang, M D , Leciurer, Community and Family Medicine, and Depuiy Director, Healthy Schools Program, The Chinese Universiiy of Hong Kong; Shiu-hung Lee, MB, BS, MD. Direcior, School of Public Healih. The Chinese University of Hong Kong; and Cho-yee To, MA, PhD. Professor, Educaiion, The Chinese University of Hong Kong: Depi. of Communiiy and Family Medicine, The Chinese Universiiy of Hong Kong, 4th poor, School of Public Healih Bldg.. Prince of Wales Hospiial, Shatin, N.T., Hong Kong. This study was supported in pari by the Qualiiy Educaiion Fund of the Hong Kong Government, Special Adminisiraiive Region. This article was submitted November 2, 2000, and revised and accepted for publication March 26,2001.
commonly and inversely to socioeconomic status.13 Therefore, one would hypothesize that students not study- ing in mainstream schools would face higher risk of adopt- ing unhealthy lifestyles. This paper provides a comparative analysis of health-risk behaviors between students of PVS and students of mainstream schools to test the hypothesis. The results are of interest in Hong Kong and other devel- oped countries because many Asian countries face similar changing disease patterns as Hong Kong. Asians from well- developed countries also represent one of the major ethnic groups in North America and Europe.
SURVEY PLANNING A cross-sectional study, the Youth Risk Behavior Survey
(YRBS), was conducted by the Centre for Health Education and Health Promotion at The Chinese University of Hong Kong in 1999 as part of the Health Promoting School Programme.14 The survey was administered to adolescent students aged 10-19 (from secondary grades 1 to 7) at secondary schools from a long-established school organiza- tion in Hong Kong. That organization manages schools of different academic levels, including PVS, in different geographical areas throughout the territory, so the sample population included a variety of students with different academic attainments. Profiles of the schools and the chil- dren suggest a reasonably representative sample was obtained.
The self-administered YRBS covered six health behavior categories: unintentional and intentional injuries; tobacco use; alcohol use and other drug use; sexual behavior; unhealthy dietary behavior; and physical activity.IS The questionnaire also included demographic and morbidity data. Questions were translated into Chinese, then back translated into English. Questionnaire content was validated by face validity. The questionnaire was pilot-tested with students from different schools and different age groups. To ensure the quality of data collected, the research team visited each participating school to brief the teachers on details and objectives of the study. Letters also were sent to parents explaining the study objectives and to obtain permission for their children to participate voluntarily. Students were briefed about the purpose of the study, with strong emphasis on voluntary participation and anonymity of responses. The detailed methodology has been described elsewhere. l6
Journal of School Health November 2001, Vol. 71, No. 9 443

Data Analysis Data analysis was conducted using the SPSS package.
The study included 21 mainstream secondary schools and 3 prevocational schools. Data were tabulated on risk behav- iors at the two different school types with or without adjust- ing for demographic factors such as age group, gender, and parents’ education and occupation. Educational background of parents was classified in two categories: secondary education or above and other. Occupation of parents was classified in two categories: skilled and other. The chi- square test of independence between the risk behavior of students of prevocational schools and mainstream school was conducted at the 5% and 1% levels of significance.
SURVEY RESULTS Of 17,673 questionnaires distributed, 15,448 (87.4%)
valid questionnaires were returned. The response rate of the prevocational schools was higher (94.9% vs. 74.3%) The general profile of respondents was compared with the total Hong Kong population in terms of age and gender distribu- tion. Mean age of the sample was similar to the Hong Kong population. Mean ages of respondents versus the general population were 14 and 13.1 years for secondary grades one to three, and 16.4 and 16.1 years for secondary grades four to seven. Gender distribution of the sample also was similar to the Hong Kong population. Female students versus male students in the survey, were 50.7% and 49.3%, respectively. In Hong Kong, the proportion was 49.4% and 50.6%, respectively.
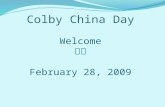
Table 1 shows overall risk behavior patterns of students from PVS compared with mainstream schools. A higher proportion of PVS students did not wear seatbelts or helmets, and they were involved or injured in physical fights. A higher proportion of PVS students was current or frequent smokers, current or episodic heavy drinkers, and glue sniffers. A higher proportion of PVS students had sexual intercourse, were currently sexually active, and had more multiple sexual partners. The greater proportion of PVS students did not consume fresh fruits and vegetables. In mainstream schools, a higher proportion of students ate desserts or fried fruits four times or more in a week. Mainstream school students also were less likely to partici- pate in vigorous physical activities or to participate in strengthening exercises.
Results were analyzed with parents’ education back- ground and occupation justified (Table 2). Parents’ educa- tion level or occupation had no noticeable effect on the difference in risk behavior between students of PVS and mainstream schools.
Results were analyzed with age of students classified in two age groups: ages 10 to 14 and ages 15 to 19. The pattern was similar to the overall pattern with students of PVS having a higher prevalence of many risk behaviors except for lifetime alcohol users. Among this group there was a higher prevalence for PVS students aged 10 to 14 (50.7% vs. 45.4%), but reverse for those aged 15 to 19 (56.5% vs. 58.2%). For frequent consumption of fried food, only the older age group showed a higher prevalence among students of mainstream schools (36.8% vs. 32.9%).
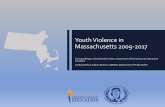
Results were analyzed by gender (Table 3). A higher proportion of female PVS students were involved in physi- cal fights whereas no statistical significance was found for male students. Results also showed that a statistically
significant proportion of female PVS students had made suicide plans, were current substance abusers, and were current alcohol users. For exercise patterns, female students of mainstream schools were more likely to participate in exercise, especially strengthening exercise. However, the pattern reversed for males and, a higher proportion of male PVS students were involved in vigorous activities.
SURVEY IMPLICATIONS Schools were not randomly selected, but the study
subjects were similar in age and gender distribution to the total school population as a whole, and they came from different districts of Hong Kong. The large sample helped yield a more precise estimate of the proportion of students reporting a particular behavior. Assuming the proportion of a sample reporting a given behavior was 1%, to achieve a level of 0.1 % with 95% confidence, a sample size of 9,900 was required (n= p(1-p)/s.e.2 where n is sample size, p is proportion of sample reporting given behavior, and s.e. is standard error or precision level). Data were collected by self-reported health behaviors. The nonresponse rate was low; about 80% of students responded.
For most categories of health-risk behavior such as unin- tentional and intentional injuries, smoking, alcohol drink- ing, glue sniffing, inadequate physical activity, insufficient consumption of fresh fruits and vegetables, early sexual
Table 1 Prevalence of Risk Behaviors
from Prevocational School and Mainstream School with Chi-square Test
Risk Behavior
Prevocational Mainstream School School
Rarely or never wore bicycle helmets I+ Rarely or never wore seat belts I+ In a physical fight (HI
Injured in a physical fight I+ Attempted suicide I+ Lifetime cigarette use I+ Current cigarette use I+ Frequent cigarette use .cI Current alcohol use I+ Episodic heavy drinking I+ Lifetime sniffed glue * Ever had sexual intercourse I+ First sexual intercourse before age 13 I+ Four or more sexual partners during the lifetime I+ Current sexually active I+ No consumption of fruit I+ No consumption of vegetable I+ Participated in vigorous physical activities * Participated in strengthening exercise *
68.4% 63.8%
36.3% 31.7% 13.4% 10.1% 2.4% 1.4% 5.9% 4.2%
35.1 % 21.2% 10.5% 5.0% 6.7% 2.5%
16.0% 11.3% 7.7% 4.0% 2.5% 1.8% 6.5% 2.9%
2.1 % 0.8%
1.3% 0.4% 4.1% 1.7%
1 1.4% 7.7% 4.7% 2.6%
30.9% 24.7%
21.4% 19.5%
* statistically significant as p .= 0.05 I+ statistically significant as p .= 0.01
444 Journal of School Health November 2001, Vol. 71, No. 9

activity and multiple sexual partner; the PVS students were at higher risk. A previous study showed that a higher proportion of students from alternative high schools reported being involved in a physical fight the past year,
having smoked at least one cigarette the past month, having drunk five or more drinks at least once the past month, having smoked marijuana at least once the past month, having used cocaine at least once the past month, and
Table 2 Chi-square Test Between Risk Behaviors (Row Variables) and Column Variables
School Types School Types (2 categories: (2 categories:
Mainstream School) Mainstream School) Prevocational School and Prevocational School and
Risk Behavior Fixed Factor: Parent Education
Rarely or never wore bicycle helmets
In a physical fight
Attempted suicide
Current cigarette use
Frequent cigarette use
Episodic heavy drinking
Current sniffed glue
Ever had sexual intercourse
First sexual intercourse before age 13
Four or more sexual partners during the lifetime
Current sexually active
No consumption of fruit
No consumption of vegetables
Participated in vigorous physical activities
Secondary or Higher
71.8% vs. 62.6%
19.3% vs. 9.1 %
6.5% vs. 4.1 %
10.6% vs. 3.9%
8.8% vs. 2.2%
11.6% vs. 3.9%
3.0% vs. 1 .O%
6.7% vs. 2.4%
2.1 % vs. 0.7%
H
H
*
H
**
x
H
H
H
0.5% vs. 0.3%
2.9% vs. 1.4%
11.5% vs. 5.9%
4.6% vs. 1.7%
33.8% vs. 26.2%
x
**
x
x
H
Other
67.3% vs. 65.2%
10.9% vs. 9.6%
5.7% vs. 4.0%
9.4% vs. 5.5%
5.4% vs. 2.4%
6.5% vs. 3.7%
1.8% vs. 0.9%
7.0% vs. 3.2%
1.9% vs. 0.9%
0.9% vs. 0.4%
4.7% vs. 2.0%
10.8% vs. 8.2%
3.5% vs. 2.4%
28.9% vs. 23.4%
H
*
H
H
H
*
H
xx
H
x
H
x
x
Fixed Factor: Parent Occupation
Skilled
70.1% vs. 61.2%
19.3% vs. 9.3%
7.8% vs. 4.3%
11.4% vs. 4.1 %
10.9% vs. 2.0%
11.4% vs. 3.7%
2.3% vs. 1.2%
9.9% vs. 2.8%
4.1 % vs. 0.9%
4.1 % vs. 0.3%
4.7% vs. 1.5%
13.5% vs. 6.5%
5.7% vs. 2.4%
*
H
*
H
H
H
H
H
H
w
H
H
35.0% vs. 25.7% H
Other
68.3% vs. 64.9%
11.3% vs. 10.2%
5.5% vs. 4.2%
10.2% vs. 5.1 %
6.2% vs. 2.6%
6.9% vs. 3.8%
1.7% vs. 0.9%
5.4% vs. 2.6%
1.8% vs. 0.8%
1.3% vs. 0.4%
3.6% vs. 1.6%
11.4% vs. 8.1 %
4.8% vs. 2.8%
30.1 % vs. 23.6%
H
*
H
x
H
*
H
H
H
x
II
x
H
* statistically significant as p c 0.05 ** statistically significant as p c 0.01
Journal of School Health November 2001, Vol. 71, No. 9 445

having ever had sexual interco~rse.~’ Though a higher proportion of PVS students reported substance abuse behavior, the difference was not statistically significant, perhaps due to the small number of students with substance abuse behavior compared to the United States.
The effect was similar after parents’ education back- ground and occupation were stratified. Though the likeli- hood of engaging in health-risk behaviors among adolescents relates inversely to socioeconomic status,13 findings from this survey suggested that school environ- ment would exert a significant influence on lifestyle behav- ior of the students. Education may impart knowledge of healthy behavior patterns along with positive social, psychological, and economic skills and assets. Such skills and assets may include positive attitudes about health, higher self-esteem and self-efficacy, and membership in peer groups that promote adoption or continuation of posi- tive health The PVS students were less likely to possess those skills and assets. Among the adolescents, perceived academic and social competence were predictive of high self-esteem.21 The PVS students were less likely to develop high self-esteem due to their academic problems. Low self-esteem also might lead to an increase in health- risk behavior.
In Chinese culture, parents have great expectations for their children in academic achievement. Few students view PVS as a viable alternative for their education. Therefore, few students are psychologically prepared for PVS, thus leading to greater problems in behavior and positive think- ing. Moreover, PVS teachers tend to concentrate more on practical and technical training and not spending time in meeting the psychological needs of students. This fact might explain why female PVS students were more likely to be involved in a physical fight, planning suicide, being current alcohol users, and engaging in substance abuse behaviors. Female students seem more vulnerable to stress during adolescent development. If they do not receive appropriate support in the school environment, they may turn to risk behaviors as a coping mechanism.zz
Lack of space for facilities in prevocational schools explains why a lesser proportion of PVS students engaged in exercise. However, a high proportion of male PVS students reported a higher level of vigorous activities than did mainstream schools. A higher proportion of students in mainstream schools consumed fried food and desserts. The pattern was similar after stratification of parents’ back- ground, perhaps due to the fact that students in mainstream schools tend to follow the eating habits of an affluent society .
For the risk behavior of smoking, the prevalence of frequent smokers among PVS students was higher than rates from a local study in 1993.23 The higher prevalence of lifetime alcohol use among students of PVS at younger ages suggests that students of PVS use alcohol as a coping strategy.
CONCLUSION A need exists for comprehensive health education and
intervention programs to address the needs of youth in prevocational schools. Children and adolescents need preventive measures before their unhealthy behaviors are fully established. One study demonstrated evidence of early consolidation and tracking of physical activity and food
preferences among a cohort of adole~cents.~~ A number of risk factors for chronic disease track from childhood.25 This paper illustrated the importance of interaction with the immediate social environment and peer influence. This approach supports social learning theory focusing on both individual determinants of behavior such as knowledge and motivation, and on external determinants including physical and social cues for behavior, and reinforcers of behavior.
The concept of “Health Promoting Schools” seeks to involve a wide sector of the community to enhance and sustain positive health behavior.z6 The concept is of particu- lar importance for prevocational training schools because a study by Nutbeam et all2 showed a strong and progressive relationship between indicators of “alienation” from school and health promoting behaviors.
References 1. Hong Kong Government. Hong Kong 1997. Information Services
Department of the Hong Kong S A R Government, 1997. 2. Midgley C, Feldlaufer H, Eccles JS. Studentkeacher relations and
attitudes toward mathematics before and after the transition to junior high school. Child Dev. 1988;60:375-395.
Table 3 Chi-square Test Between Risk Behaviors
(Row Variables) and Column Variables
School Types (2 categories:
Prevocational School and Mainstream School)
Fixed Factor: Risk Behavior Gender
In a physical fight
Current alcohol use
Lifetime sniffed glue
Current sniffed glue
Lifetime cough syrups use
Current cough syrups use
Participated in vigorous physical activities
Participated in strengthening exercise
Female
6.8% vs. 3.5%
14.1 % vs. Icc
8.4%
1 .a%
0.8%
H
3.1 % vs.
Icc
2.4% vs.
Icc
1.2% vs. 0.6%
0.9% vs. 0.3% vs. H
14.6% vs. 14.7%
9.3% vs. 11 .a% *
Male
19% vs. 18.0%
17.5% vs. 14.6%
1.9% vs. 1 .a%
1 .O% vs. 1 .O%
0.9% vs. 0.7%
0.3% vs. 0.4%
44.4% vs. 36.7% Icc
3 1 . 3 % ~ ~ . 29.0%
* statistically significant as p < 0.05 ** statistically significant as p < 0.01
446 Journal of School Health November 2001, Vol. 71, No. 9

3. Midgley C, Feldlaufer H, Eccles JS. Change in teacher efficacy and student self- and task-related beliefs during the transition to junior high
4. Eccles J , Midgley C, Buchanan CM, Wigfield A, Reuman D, MacIver D. Developmental during adolescents: the impact of stage/envi- ronment fit. Am Psychol. 1993;48:90-101.
5. Simmons RG, Blyth DA. Moving into Adolescence: The Impact of Pubertal Change and School Context. Hawthorn, NY: Aldine de Gruyter; 1987.
6. Grunbaum JA, Kann L, Kinchen SA, et al. Youth Risk Behabior Surveillance: National Alternative High School Youth Risk Behavior Survey, United States, 1998. JSch Health. 2000,70(1):5-17.
7. Department of Health. Annual Report, 1997/98. Department of Health, Hong Kong SAR Government; 1998.
8. Hospital Authority. Annual Report, 1998199. Hong Kong: Hospital Authority.
9. Office of Population Census & Survey, Royal College of General Practitioners, Department of Health. Morbidity Statistics from General Practice. London, England: Fourth National Study 1991-92 Hh4SO; 1995.
10. Van der Velden J, De Baker DH, Claessens AAMC, Schelleuis FG. Morbidity in General Practice: Dutch National Survey of General Practice. Netherland Institute of Primary Care; 1992.
11. Lee A, Chan K, Wun YT, Ma PL, Li L, Siu PC. A morbidity survey in Hong Kong, 1994. Hong Kong Pract. 1995;17(6);246-255.
12. Nutbeam D, Smith C, Moore L, Baurman A. Warning! Schools can damage your health alternation from school and its impact on health behavior. J Paediatr Child Health. 1993;29(Suppl l):S25-30.
13. Lowry R, Kann L, Collins J, Kolbe LJ. The effect of socio- economic status on chronic disease risk behaviors among US adolescents.
14. Lee A. Youth health promotion and Health Promoting Schools: What should be the aims? Asia Pacif ic J Public Heal th.
15. Kolbe LJ, Kann L, Collins JL. Overview of the Youth Risk Behavior Surveillance System. Public Health Rep. 1993;108
School. J Educ Psychol. 1989;81:247-258.
JAMA. 1996;276( 10):792-797.
2000; 12(suppI):S55-57.
(suppl 1) :2-10.
16. Lee A, Tsang KK, Lee SH, To CY, Healthy School Research Support Group older school children are not necessarily healthier: analysis of medical consultation pattern of school children from a territory wide School Health Surveillance. Public Health. 2000,115:30-33.
17. Grunbaum JA, Basen-Engquist K. Comparision of health risk behaviors between students in a regular high school and students in an alternative high school. J Sch Health. 1993;63( 10):421-425.
18. Winkley MA, Jatulis DE, Frnak E, Fortmann SP. Socioeconomic status and health: how education, income, and occupation contribute to risk factors for cardiovascular disease. Am J Public Health. 1992;82:
19. Winkleby MA, Fortmann SP, Barrett DC. Social class disparities in risk factors for disease: eight-year prevalence patterns by level of education. Prev Med. 199O;l-12.
20. Bunker JP, Gomby DS, Preface. In: Bunker JP, Gomby DS, Kehrer BH, eds. Pathways to Health: The Role of Social Factors. Menlo Park, Calif Henry J. Kaiser Foundation; 1989: 15.
21. Harter S. Developmental differences in the nature of self-represen- tations: implications for the understanding, assessment, and treatment of maladaptive behavior. Cog Ther Res. 1990;14113-142.
22. Eccles J, Midgely C. Stage/environment fit: eevelopmentally appropriate classrooms for early adolescents. In: Ames RE, Ames C, eds. The Development of Achievement Motivation. Greenwich, Conn: JAI Press; 1989:283-331.
23. Wong R, Chan P, Ngai A, Pang PY, Chan C, Yuen A. Youth Trends in Hong Kong 1999. Hong Kong Federation of Youth Study Group; 1999.
24. Kelder SH, Perry CL, Kleep KI, Lytle LL. Longitudinal tracking of adolescent smoking, physical activity, and food choice behaviors. Am J Public Health. 1994;84:1121-1126.
25. Webber LS, Srinivasan SR, Wattigney WA, Berenson GS. Tracking of serum lipids and lipoproteins from childhood to adulthood: the Bogalusa Heart study. Am JEpidemiology. 1991; 133: 884-899.
26. Lee A, Tsang KK, Lee SH, To CY. ‘Healthy Schools Program’ in Hong Kong: Enhancing Positive Health Behavior for School Children and Teachers. Special joint issue of Educ Health, and Ann Behav Sci Med
8 16-820.
Educ 2000; 13(3):399-403.
A S H A P A R T N E R S President’s Diamond Endowment Partner + + McGovem Fund for the Behavioral Sciences, 221 1 Norfolk, Suite 900, Houston, TX 77098-4044
Merck & Co., Inc., 770 Sumneytown Pike, West Point, PA 19486-0004
Gold Endowment Partner + + + American Cancer Society, 1599 Clifton Road, NE, Atlanta, GA 30329 Bayer Consumer Care Division, 16 West 22nd St., New York,NY 10010 Tampax Health Education, 1500 Front St., Yorktown Heights, NY 10598
Silver Endowment Partner + + + Dept. of Applied Health Science, Indiana University, Bloomington, IN 47405 Dept. of Health Science Education, University of Florida, Gainesville, FL 3261 1-8210 Division of Health and Safety, Texas A&M University, College Station, TX 77843-4243
Sustaining Partner
Century Partner
+ National Fire Protection Association, 1 Batterymarch Park, Quincy, MA 02269-9101
+ + + + +
Center for Cross-Cultural Pediatric Behavioral Health, University of North Texas, P.O. Box 3 1 1280, Denton, TX 76203 Center for Mental Health in Schools, UCLA, P.O. Box 951563, Los Angeles, CA 90095-1563 Center for School Mental Health Assistance (CSMHA), University of Maryland School of Medicine, Baltimore, MD 2 120 1 - 1570 The Children’s Health Market, P.O. Box 7294, Wilton, CT 06897 William V. MacGill 6r Co., 720 Annoreno Drive, Addison, IL 60101
Journal of School Health November 2001, Vol. 71, No. 9 447