I. Amputations and Limb Prostheses - Rehabilitation Research

Aweb-basedinterventionforupperlimbrehabilitationfollowingstroke
JaneBurridgeProf.ofRestorativeNeuroscienceUniversityofSouthamptonUKjhb1@soton.ac.uk

ThispresentationpresentsindependentresearchfundedbytheNationalInstituteforHealthResearch(NIHR)underitsResearchforPatientBenefit(RfPB)(Grant
Reference#PB-PG-0909-20145).Theviewsexpressedarethoseoftheauthorsandnotnecessarilythoseofthe
NHS,theNIHRortheDepartmentofHealth.

Howcantheinternetincreaseintensityofpractice?

Whatthistalkisabout
• Thewaystrokerehabilitationismoving(intheUK…)• Evidenceforintensityofpractice• Rationaleandpotentialbenefitsofrehabilitationtechnologies
• Anexamplefromourcurrentresearch:– Web-basedsupportprogrammeforhome-basedupperlimbrehabilitation
Futuremodelofstrokerehabilitation
• Driveforcost-effectiverehabilitation• Targetingrecovery• Changeinattitudesfromdependencetoindependence
• EarlySupportedDischarge(ESD)• Rehabilitationathome• Improvingassessment
Intensity
• Agameoftennis:– 5strokes/point– 10points/game– 10games/set– 3 sets/match
• =750strokes/match• Howmanyrepetitionsinatherapysession?
• In(human)strokerehabilitationthetypicalnumberofrepetitionsinasessionis30(Langetal,2009)
• Inanimals,changesinprimarymotorcortexsynapticdensityoccurafter400(butnot60)reaches(Remple etal,2001)
• Mighttherebea‘threshold’abovewhichULuseimprovesandbelowwhichitdecreases(Schweighofer etal,2009)
• Canthenumberbeincreasedbyprovidingothersupporttoenablemovementorgivingmotivatingfeedback?
Isthereevidencetosupport‘increaseddose’?

ThedoseofULtreatmentafterstrokeisunacceptablylow
• Patientsdoverylittleinhospital
• JulieBernhardtreportedthatpatientsareonlyactive13%oftheday.AndALONE60%oftheday
• Notthebestenvironmenttopromoteneuroplasticity
• Animalstudies- need400-600repsofreachtasks
• Onaveragepatientsachieve32repsinatherapysession
• Strongevidencethathighdoseoftherapyiseffective
• Incorporatinghighintensityofrepetitivetaskpractice
• Variedandgoalorientated

Is More Better? Using Metadata to Explore Dose–Response Relationships in Stroke Rehabilitation
Keith R. Lohse, PhD; Catherine E. Lang, PT, PhD; Lara A. Boyd, PT, PhD
• Usedregressionmodelstopredictimprovementoffunction
• 30studies1750participants• Increasedtimescheduledwasapredictorofclinicallymeaningfulimprovement
• Irrespectiveoftimepost-stroke
Stroke2014;45:2053-2058

…...Buthowcanweachievetherequiredintensityinroutineclinicalpractice?
Withinthenext10yearsrehabilitationtechnologieswillusedroutinelyinclinicalpractice

Rationalefortechnologies

Whatourpatientstellus..
‘Recoveringfromstrokeislikewatchingpaintdry– itsdifficulttokeepmotivatedwhenyoudon’tseemtobeimproving’
Whatarethekeydeterminantsofaneffectivemotortrainingprogram?
• Intensity?• Repetition?• Taskspecificfunctionaltraining?• Providingfeedbacktopatient?• Alternating/changingtasks?


Constraint-InducedMovementTherapy
(CIMT)

LifeGuidePlatform• DevelopedinSouthampton- fundedbytheUKResearchCouncil• Tomotivateandsupportbehavioralchangee.g.drugaddiction,
obesity• Softwaretocreateweb-basedinteractivetherapiesthat:– Givepersonalizedadviceandguidancebasedontheuser'sanswerstoquestions
– Supportuserstoplan,chartandchecktheirprogress– Sendsupportingmessagestousersintheformofpersonalizedemailsortexts
– Storeandtransmitdatasecurely
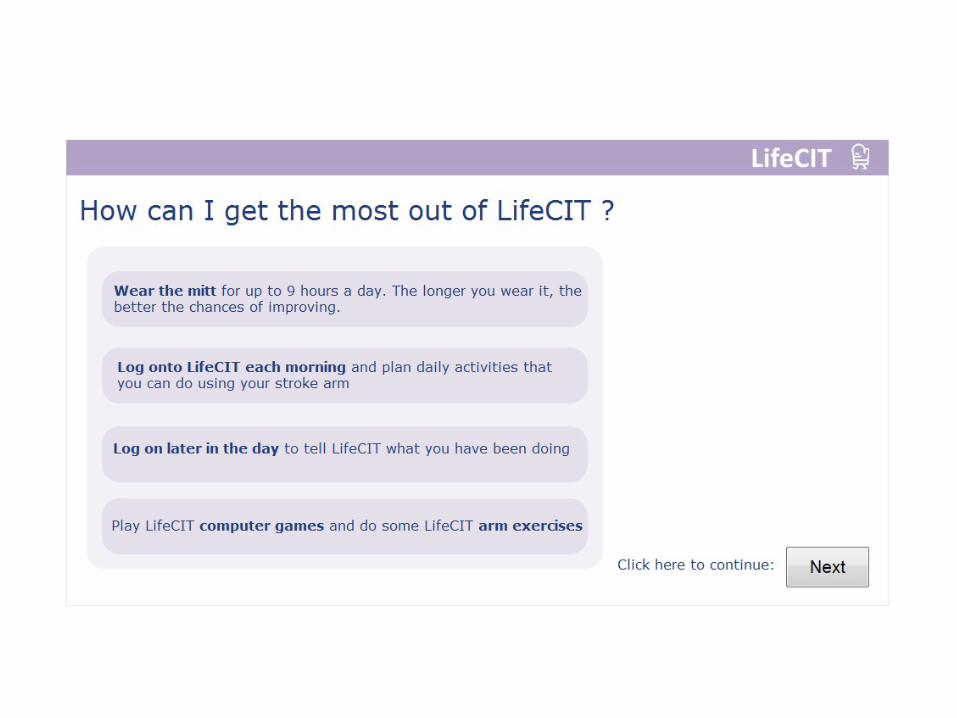
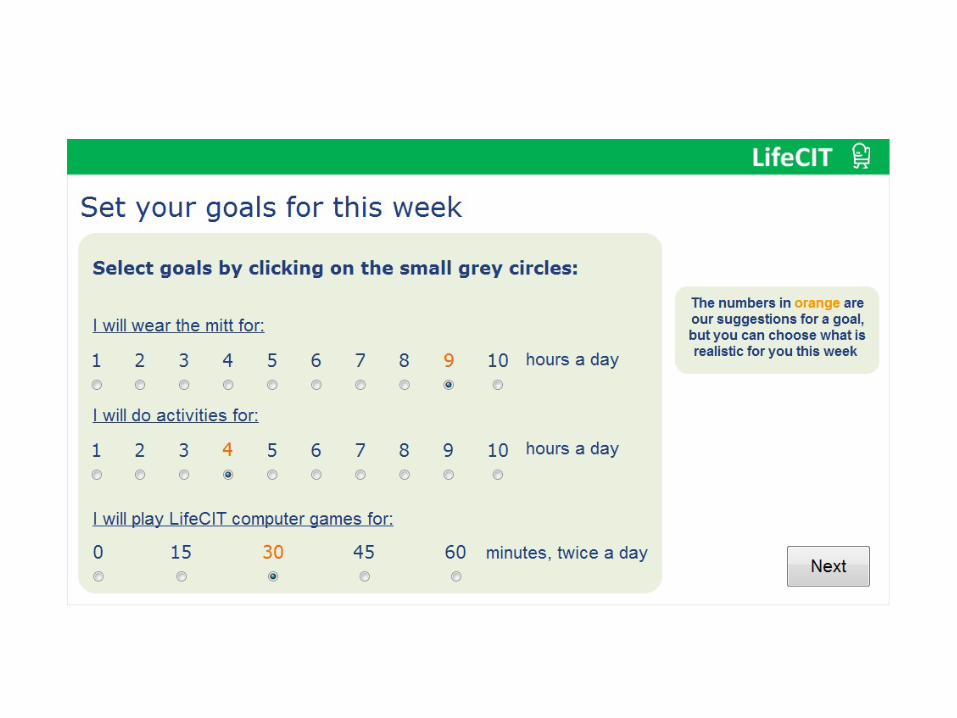
LifeCIT- RationaleandAims
• CIThasasoundneurophysiologybase• HasbeenshowntobeeffectiveBUT• Iscostlyintermsofcontacttime• Evidenceforefficacyasahome-basedintervention• Butfeedbackhasshownpotentialproblemswithadherenceand
motivation• LifeCITsupportshome-basedCIT
LifeCITMethodology
• STAGE1:Co-designwithpatients,carersandtherapistsinaclinical/homeenvironment– Webpagesincludingdesigningaprogrammeofassessment,activities,
games,feedbackandsupport– Interaction,communicationandfeedbacksupportfromtherapists,
friendsandfamily• STAGE2:PragmaticRCT(n=30)withstrokepatientsfollowingdischargefrom
hospitalto:– Testfeasibilityandidentifyproblems– Assesseffectonupperlimbfunctionandqualityoflife– Estimateeffectsizecomparedwithusualcare– Monitoradherence

LifeCIT:Philosophy
• NOT:‘Thisiswhatyouneedtodo….’ Givinginstructions– thetherapistisincharge
• BUT: ‘Whatdoyouwanttobeabletodo?’Thepatienttakesthelead– thesystem(LifeCIT)supportsandguides
• Usingthisapproachweaimtoencourageself-efficacyandindependenceratherthancomplianceanddependence

Phase1:DevelopmentofPrototype1
• Meetingswiththerapists(6siteseachn=1-6)usingpower-pointslidesillustratingmock-upsoftheproposedwebsite– Therapistsmadesuggestionsaboutcontentofthewebsitee.g.exercises,games,activitiesatdifferentlevels
– Reviewedcurrentlyusedexercisesheetsforpatientsofdifferentlevelsofability
– Discussedcommunicationbetweentherapists,patientsandcarers
• DesignedandbuiltfirstprototypeLifeCITwebsite

Phase1:Prototype2.Developedviathink-aloudstudieswith12sub-acute(<12weeks)patientsinhospitalandathome

Developmentsbasedonobservedpatients’behaviornavigatingthewebsiteandsimultaneousoralfeedback
• Websitenavigation:– avoidmultiplemenuoptions- linearprogressionthroughthepages
– noscrolling– allinformationononepage
• Clarityofinstructions:– minimaltextandavoidingambiguity– motivationallanguageandillustrationse.g.‘congratulations’‘useitorloseit’
– Instructionsviavideowithavoice-overratherthantext
• Simplifiedcomputergames

FinalVersionoftheWebsite
https://pips.ecs.soton.ac.uk/player/play/LifeCIT_demo
EnterauserID:2numbersand2lettersPW:anythingyoulike!


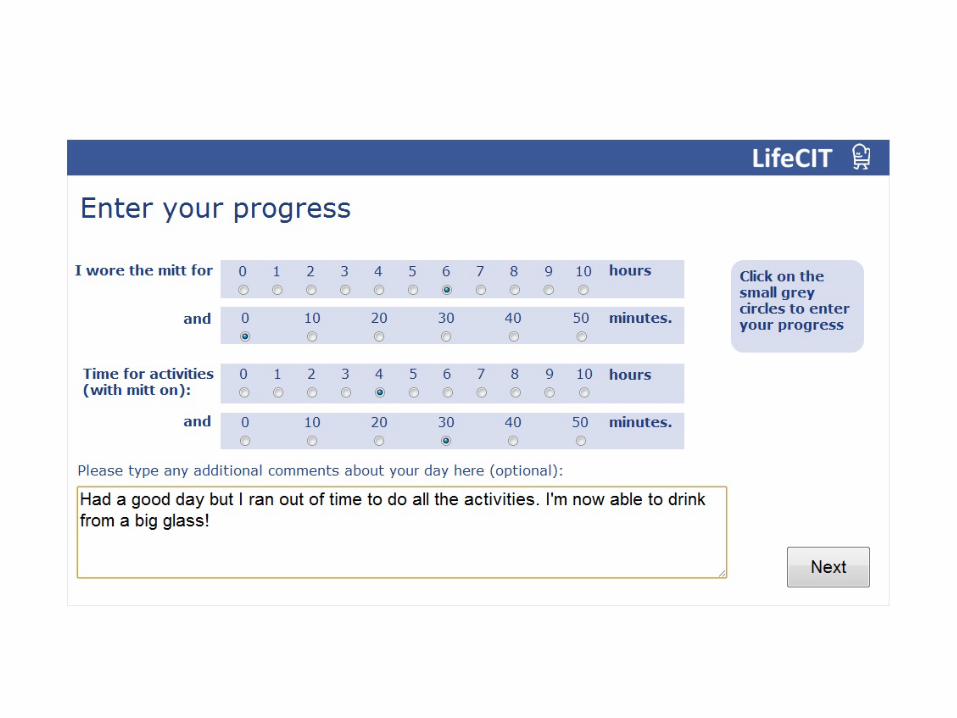
UsingtheMotorActivityLog(MAL)
• Personalized:acriticalfactorinmotivationandadherence
• Activitiesthatinteresttheindividual• Relatetopersonalobjectives• Attherightlevelofability• TheMALisusedtoassesswhatthepatient‘cando’andthedataisthenusedtopersonalizethewebpages

Choosingactivities



Laterintheday…..


Doesa3-weekLifeCITinterventionimproveupperlimbfunctionandmaintainedatsix-monthfollow-up?
• Feasibilitystudy- PragmaticpilotRCT• Patientsrecruitedondischargefromhospital7daysto3
monthspoststrokeandasecondcohortpost16weeks• SelectioncriteriaincludedsafetyusingCITathome,>10°
wristmovementand>2.4ontheMAL• Mainoutcomemeasures:WMFTandMAL(Baseline,post
interventionandsix-monthfollowup)• PosttreatmentinterviewswiththepatientswhousedLifeCIT
Results
Participants• Screened:N=83(60didnotmeetinginclusioncriteria4 declined(3couldnotuseacomputer)
• Recruited:ControlN=8TreatmentN=11
• Drop-outs:1 duringtheintervention(secondstroke),2 missed6-monthassessment(1frozenshoulderand1unabletocontact)
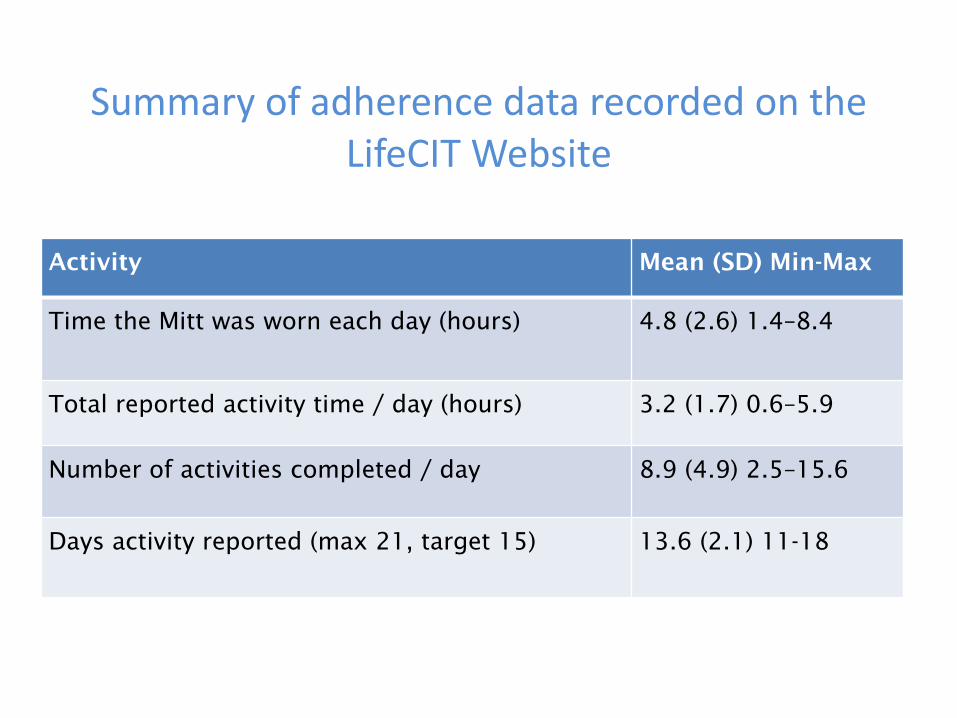
SummaryofadherencedatarecordedontheLifeCITWebsite
Activity Mean (SD) Min-Max
Time the Mitt was worn each day (hours) 4.8 (2.6) 1.4–8.4
Total reported activity time / day (hours) 3.2 (1.7) 0.6–5.9
Number of activities completed / day 8.9 (4.9) 2.5–15.6
Days activity reported (max 21, target 15) 13.6 (2.1) 11-18

BetweenGroupdifferencesformainoutcomemeasures
OutcomeMeasure Meandifferencebetweengroups
ANCOVAP-Value(95%CI)
MAL/AOUBaselinetoendoftreatmentScore- 0-5
1.00* <0.003**(0.43-1.57)
MAL/AOUBaselinetofollow-up 0.25 0.64(0.95-1.44)
MAL/QOUBaselinetoendoftreatmentScore0-5
0.89* <0.003**(0.36-1.40)
MAL/QOUBaselinetofollow-up 0.46 0.42(0.80-1.71)
WMFT(FAS)BaselinetoendoftreatmentScore0-5
0.45* <0.001**(0.24-0.65)
WMFT(FAS)Baselinetofollow-up 0.50* 0.15(-0.24-1.24)
*MinimumClinicallyImportantDifferences(MCID):**betweengroupsigP<0.05MAL:10%(i.e.0.5)(VanderLeeStroke2003) - acutestrokeWMFT(FAS)0.2-0.4(Keh-chung NNR2009)

Whattheparticipantshadtosay…

Keyfactorsthatchangedbehaviourwere:
• Usingtheonlinesystem• UsingtheC-MIT• Componentsofthetherapy:Activitiesofdailyliving/functionalgoalswerekeyforeveryone
• AdaptingovertimetofrustrationsofwearingtheC-Mitt
• Seeingfunctionalgain• FamilySupportandsocialencouragement

Summary
• UseofLifeCITathomeisfeasibleandwellacceptedbyusers(100%retentionduringthetrial).
• Upperextremityfunctioninsub-acuteandchronicstrokepatientsimprovedfollowingathree-weekinterventionandatasix-monthfollow-up.
• Only1 participantdeclinedtotakepartbecausetheydidnot/couldnotuseacomputer
• Excellentadherence• Positivefeedback
Development• LifeCIThasnowbeendevelopedtobeusefulforlowerfunctioningpatientswhowouldnotbesuitableforusingCIT
• Web-basedInteractiveSupportforrecoveryofthearmandhandafterStrokE (WISE)
• PhaseIIImulti-centretrialStrokeWISE withstandardcare(HTA)

Conclusions• Technologies,especiallythoseexploitingtele-healtharelikelytobecomenormalpractice
• Toaugmentconventionalpractice• Toimprovecost-effectiveness• Currentlythereisalackofevidence• Motivation,selfmanagementandindependencearekeyfactorsinrehabilitation
• Co-designwithALLusersiskeytoacceptance– itmustbeverysimpleforpatients

Acknowledgements• Co-applicants:Ann-MarieHughes,LucyYardley,MarkWeal,
DamianJenkinson,MarkMullee• Healtheconomist:JeremyJones• Researchers:ClaireMeagher,SeanEwings,SebastienPollet,
CarolinaGonclaves andClaudiaAlt• FreddieNashandTomLeese,6th FormComputerScience
studentsfromBishopWordsworthSchool,Salisbury• Patientsandcarers• TrialSteeringCommittee– chairedbyDr TobyBlack

Thankyou
Questions?