A tumour in the cerebellopontine angle region
6
A TUMOUR IN THE CEREBELLOPONTINE ANGLE REGION AN UNUSUAL CASE A.J.E.M. Fischer*, E.H.M.A. Marres* and H. O.M. Thijssen** SUMMARY This paper describes a nearly 60-year old patient with unilateral hearing loss, developed in one year, and complaints of tinnitus and dizziness. Additional findings were unilateral peripheral facial paresis and a diminished corneal reflex. The cause was found to be a metastasis of an anaplastic carcinoma, localized at the site of the internal acoustic porus. INTRODUCTION Tumours localized, entirely or partly, in the internal acoustic meatus or porus can produce symptoms based on damage to the vestibular, cochlear and facial nerves, because these nerves are localized in the internal acoustic meatus. The most common type of tumour in this region is an acoustic neurinoma~ but other ex- panding processes can also, if only rarely, be present at this site. The following case history illustrates this. CASE HISTORY In May 1976 a nearly 60-year old male teacher was examined in our department in view of a one-year history of rapidly progressive leftsided hearing loss. Subjective hearing on the right was normal. Tinnitus had developed in the last six months and in the last two months he had been light-headed for a few seconds, whenever he executed certain movements of the head, which could not be precisely defined. There were no vegetative symptoms. There was no history of otitis. The patient felt healthy despite of a chronic bronchitis. Other anamnestic data: cholecystectomy for cholelithiasis in 1965; shortly after (likewise in 1965) hemicolectomy with end-to- end anastomosis between ileum and transverse colon after extirpation of an ana- plastic adenocarcinoma from the ascending colon and caecum; prostatectomy in 1973, on which no details were available. FINDINGS The first preliminary ENT examination revealed no anomalies. No lymph nodes * Department of Otorhinolaryngology, St. Radboud Hospital. University of Nijmegen, The Netherlands. ** Department of Radiology St. Radboud Hospital, University of Nijmegen. The Netherlands. Clin. Neurol. Neurosurg., Vol. 80-3
Transcript of A tumour in the cerebellopontine angle region

A T U M O U R IN THE CEREBELLOPONTINE A N G L E REGION
AN UNUSUAL CASE
A.J.E.M. Fischer*, E.H.M.A. Marres* and H. O.M. Thijssen**
SUMMARY
This paper describes a nearly 60-year old patient with unilateral hearing loss, developed in one year, and complaints of tinnitus and dizziness. Additional findings were unilateral peripheral facial paresis and a diminished corneal reflex. The cause was found to be a metastasis of an anaplastic carcinoma, localized at the site of the internal acoustic porus.
INTRODUCTION
Tumours localized, entirely or partly, in the internal acoustic meatus or porus can produce symptoms based on damage to the vestibular, cochlear and facial nerves, because these nerves are localized in the internal acoustic meatus. The most common type of tumour in this region is an acoustic neurinoma~ but other ex- panding processes can also, if only rarely, be present at this site. The following case history illustrates this.
CASE HISTORY
In May 1976 a nearly 60-year old male teacher was examined in our department in view of a one-year history of rapidly progressive leftsided hearing loss. Subjective hearing on the right was normal. Tinnitus had developed in the last six months and in the last two months he had been light-headed for a few seconds, whenever he executed certain movements of the head, which could not be precisely defined. There were no vegetative symptoms. There was no history of otitis. The patient felt healthy despite of a chronic bronchitis. Other anamnestic data: cholecystectomy for cholelithiasis in 1965; shortly after (likewise in 1965) hemicolectomy with end-to- end anastomosis between ileum and transverse colon after extirpation of an ana- plastic adenocarcinoma from the ascending colon and caecum; prostatectomy in 1973, on which no details were available.
FINDINGS
The first preliminary ENT examination revealed no anomalies. No lymph nodes
* Department of Otorhinolaryngology, St. Radboud Hospital. University of Nijmegen, The Netherlands. ** Department of Radiology St. Radboud Hospital, University of Nijmegen. The Netherlands.
Clin. Neurol. Neurosurg., Vol. 80-3

190
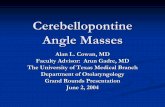
Fig. 1. Normal right temporal bone as dis- closed by STENVERS view.
Fig. 2. STENVERS view of the left temporal bone. The destruction of the left petrous apex is shown in part. The cranial wall of the internal meatus is ab- sent as well as the bony part of the pos- terior canal.

191
were palpable in the cervical region. Slight peripheral facial paresis on the left, of which the patient was unaware. The left corneal reflex was unmistakable diminished. No paresis of the abducens nerve. Audiometric examination disclosed only incipient presbyacusis on the right, but on the left side there was a almost complete loss of hearing, In view of these preliminary findings, the patient was hospitalized for an extensive otological, vestibular, general internal, neurological and radiological study.
General internal examination revealed no anomalies. Specifically, urogenital and digestive tracts were normal; thyroid function and thyroid scan were likewise normal.
Radiological examination of the heart, lungs, stomach, oesophagus and kidneys failed to reveal an anomaly.
Additional audiometric examination showed, that no stapedius muscle reflexes were measurable. Determination of recruitment and a tone decay test on the left, in order to differentiate between a cochlear and a retrocochlear process, were impos- sible because hearing was too poor. A left-sided electrocochleogram provided in- conclusive information.
In the vestibular study, the Babinkski-Weil walking test and Unterberger's marking-time test were decidedly disturbed, rotation being clockwise and counter- clockwise. The Romberg test was negative and finger-pointing tests were normal, as was diadochokinesis. There was no spontaneous or positional nystagmus. A calorization study with the aid of electronystagmography revealed marked patho- logical diminution of the exitability of the left labyrinth. Optokinetic stimulation produced an asymmetrical response with nystagmus preference to the left.
Neurological examination revealed, in addition to left-sided facial paresis, loss of hearing and a negative corneal reflex, some slight asymmetry in the function of the 9th, 10th and 12th cranial nerves with, surprisingly, disadvantage of the right side. The ocular fundi and fields of vision were normal. Gnostic sensibility was intact and there were no indications of pyramidal tract pathology. The EEG disclosed a slight disturbance of brainstem function and electromyographic examination of the musculture of the left facial nerve revealed indications of an old neurogenic lesion. The total protein content of the CSF was increased (523 mg/1) and the protein pattern was normal.
In the otoradiological and neuroradiological study aimed projections of the left petrosal bone and tomograms showed bone destruction around the left labyrinth. This destruction was observed in the superior and posterior aspects of the petrosal bones. The roof of the internal acoustic meatus was absent as far as the fundus, as was the environment of the posterior vertical semicircular canal. Mastoid process, middle ear structures and antral cells were intact (Figs. 1 and 2). Carotid and vertebral angiography showed no demonstrable extension ofa tumour in the middle and posterior cranial fossae; this, however, does not exclude such an extension with certainty. At meatocisternography the presence of an expanding process in the left cerebellopontine anglewasdemonstrable (Fig.3). This osteolytic process, localized in the left petrosal bone at the site of the cranial and dorsal delimitation of the inner

192
Fig. 3. Contrast meatography of the left cerebellopontine cistern. About I ml of contrastmaterial (Durolio- paque R) has been used. The absence of this material on the lateral side of the porus indicated the evidence of an obstruction.
ear with extension into the left cerebellopontine angle, was most probably (in view of type and localization) a tumour, which primarily arose from the meninges (VALVASSORI, 1974). Type and localization of the lesion strongly suggest a primary (conginital, primitive) cholesteatoma (DULAC, 1974).
On radiological grounds, an alternative possibility was a metastasis. An acoustic neurinoma or arachnoidal cyst were less plausible in view of the destruction on the cranial side of the petrosal bone. A meningeoma was unlikely in view of the absence of sclerosis around the internal acoustic porus.
The above clinical and radiological findings are conclusive of an expanding process on the cranial and occipital side of the left petrosal bone. In view of this localization and the destructive nature of the lesion, the considered alternatives were: primary cholesteatoma, a metastasis (although a primary tumour study dur- ing the period in hospital revealed no pertinent indications) and although less probable an acoustic neurinoma. A decision, therefore was made in favour of surgical exploration.
The localization of the process made a translabyrinthine approach undesirable. Therefore a cerebellar trephination was performed by the neurosurgeon. A tumour with a diameter of about 25 mm was found attached to the petrosal bone at the site of the internal acoustic porus, extending about 10 mm into the posterior cranial fossa. A frozen section from a biopsy specimen from the tumour was examined and yielded the diagnosis: malignant tumour, probably a metastasis of a carcinoma. Total extirpation was not practicable. The postoperative course was uneventful.
In summary, this study showed that a newly made chest X-ray revealed a slightly enlarged left hilus; tomography and bronchographic examination of this area disclosed in the upper pole of the left hilus a density for which could be suggestive

193
for a tumour. Bronchography did not reveal bronchial occlusions. Bronchoscopy with cytological examination of the secretion from the apicoposterior segment of the left upper lobe strongly suggested malignancy. These findings, although not entirely conclusive, were highly indicative of a primary bronchial carcinoma with an intra- cranial metastasis. In 1965, the patient had undergone hemicolectomy for anaplastic adenocarcinoma in another hospital, but radiological examination revealed no signs of tumour recurrence and the patient had been free from abdominal symptoms since 1965; specifically, the pattern of defaecation was undisturbed. Nevertheless, the sections of the specimen resected in 1965 were requested and compared with the sections through the intracranial metastasis. The pathologist concluded that the two tumours had identical features and it was therefore plausible, that the former was a metastasis of the latter. It therefore seemed certain, that the patient was suffering from a metastasis of a primary carcinoma of the colon which had developed in the meninges and subsequently invaded the left petrosal bone as well as the hilus of the left lung. However, it remained possible, that a primary bronchial carcinoma had developed separately from the intracranial metastasis of a primary carcinoma of the colon. After consultation, the patient was presented to a radiotherapist for irradiation of the left petrosal bone and the left lung hilus.
DISCUSSION
So-called cerebellopontine neoplasms account for 10% of all intracranial tumours. The term 'cerebellopontine angle tumour' is still in use as a collective name; a proportion of the tumours-so-referred are localized entirely or partly in the internal acoustic meatus (BERENDES et al., 1965). Acoustic neurinomas, which are the most common intracranial tumours after gliomas and meningiomas (RADEMAKERS, 1973) and account for 9% of all intracranial tumours (VAPARELLA, 1973) are the most frequently observed cerebellopontine angle tumours (mTSELBERGER and HOUSE, 1964). They are regarded as the cerebellopontine angle tumours par excellence. Of course other processes occur in this region and histological examination has made it possible to differentiate between the various expanding processes which occur in the cerebellopontine angle. After unilateral acoustic neurinomas, meningiomas were found to be the most common tumours. They are believed to account for 6.3% of all cerebellopontine angle tumours versus 71% accounted for acoustic neurinomas (PORTMANN et al., 1975); they are followed by epidermoids (otherwise known as primary cholesteatomas), which account for 5% of all expanding processes in the cerebellopontine angle (HITSELBERGER and HOUSE, 1971). In decreasing frequency, the literature ranks the bilateral acoustic neurinomas, most often found in association with Von Recklinghausen's disease (PORTMANN et al., 1975), arachnoidal cysts (THIJSSEN et al., 1976) and metastatic processes.
Neoplasms which produce brain metastases account for 3.5% of all brain tumours (MUMENTHALER, 1970). They are usually multiple growths in one or both hemi- spheres but occasionally they are confined to the posterior cranial fossa, sometimes near the internal acoustic meatus. As the above case history shows, there may be a

194
surprisingly long interval (5-15 years) between extirpation of the primary tumour and the onset of intracranial symptoms.
If, in view of the radiological findings the described tumour, is regarded as a meningeal metastasis, then the primary tumour can, above all, be expected in the digestive tract, the breast or the lungs in accordance with Biemond's diagram on relations between primary tumour and metastasis (BIEMOND, 1972). In our patient, this relation was in fact established after comparison of the histological material.
In the differential diagnosis with reference to primary tumour localization, not only the above mentioned organs should be considered but evidently also organs known to be capable of producing intracranial metastases: prostate, thyroid and kidneys (hypernephroma). The possibility of a metastasis is by no means always evident from the history and the symptomatology but, although it is rare, it should be taken into account in the examination of patients presenting with cerebellopon- tine angle pathology.
ACKNOWLEDGEMENTS
The authors are grateful to Dr. E. Meijer, Nijmegen, who performed the neurosur- gical operation, and to Dr. J. Slooff, Nijmegen, who examined the pathological material.
REFERENCES
BERENDES, J. (1965) HNO-Heilkunde (Band III, Teil I) Thieme Verlag, Stuttgart, BIEMOND, A. (1972) Hersenziekten. De Erven F. Bohn, Haarlem. DULAC, G.L. (1974) Les tumeurs du temporal Trait6 de radiodiagnostic. 279, Paris Masson. HITSELBERGER, W.E. and W.F. HOUSE (1964) Tumors of the cerebellopontine angle. Arch.Otolaryng. 80, 720. HITSELBERGER, W.E. and W.F. HOUSE (1971) Diagnosis and management of acoustic tumors. In: Maloney
W. (ed.): Otolaryngology Vol. II, Harper and Row, New York. MUMENTHALER, M. (1970) Neurologie fi~r ,~rtze und Studenten. Thieme Verlag Stuttgart. PaPARELLA, M.M. and D.A. SHUMRICK (1973) Otolaryngology, Vol. 111. Saunders Philadelphia. Pa. PORTMAN~, M.,R. LINK, S. Z~JLLNER(1975) The Internal Auditory Meatus.Churchill Livingstone, Edinburgh. RADEMAKERS, F.A.a.M. (1973) Acusticusneurinoom. Proefschrift Amsterdam. TmJSSEN, H.O.M., E.H.M.A. MARRES. J.L. SLOOFF (1976) Arachnoid cyst simulating intrameatal acoustic
neuroma. Neuroradiology I I, 205. VaLVASSORt, G.E. (1974) Benign tumors of the temporal bone. Radiol. Clin. N.A. XII-3, 533.