A Tale of two dogs: Meningoencephalitis of unknown etiology ... · Meningoencephalitis •...
61
A TALE OF TWO DOGS: MENINGOENCEPHALITIS OF UNKNOWN ETIOLOGY (MUE) Sarah Trub, DVM (Resident in Neurology & Neurosurgery)
-
Upload
truongdiep -
Category
Documents
-
view
215 -
download
0
Transcript of A Tale of two dogs: Meningoencephalitis of unknown etiology ... · Meningoencephalitis •...
A TALE OF TWO DOGS: MENINGOENCEPHALITIS OF UNKNOWN ETIOLOGY (MUE)
Sarah Trub, DVM (Resident in Neurology & Neurosurgery)
Meningoencephalitis
• Inflammation of the brain and leptomeninges • Meningoencephalomyelitis if spinal cord is also
involved
2
Two groups of etiologies
• Infectious • Immune-mediated
Common infectious etiologies
• Protozoal • Toxoplasma • Neospora
• Viral • Distemper
4
• Rickettsial diseases • E. canis • Anaplasma spp • R. rickettsii (RMSF)
• Fungal • Cryptococcus spp • Coccidioides immitis
• Bacterial
Meningoencephalitis of Unknown Etiology • Encompasses all clinically diagnosed cases of
noninfectious inflammatory CNS disease • Does not include diseases without overt CNS
involvement (i.e. SRMA) • Histopathology is necessary for definitive
diagnosis of subtype
5
Granulomatous meningoencephalitis (GME) • T-cell mediated delayed-type hypersensitivity
reaction with organ-specific autoimmune disease
• Young adults (1-6 yrs), females and small breeds
6
GME: Distributions • Disseminated
• White matter of the cerebrum, caudal brainstem, cerebellum and cervical spinal cord
• +/- gray matter, leptomeninges, choroid plexus • Multifocal signs • Acute onset and rapid progression
• Focal • Solitary granuloma • Most common in cerebral white matter • More insidious progression
• Ocular • Retinal or post-retinal portions of the optic nerve • Acute visual dysfunction
7
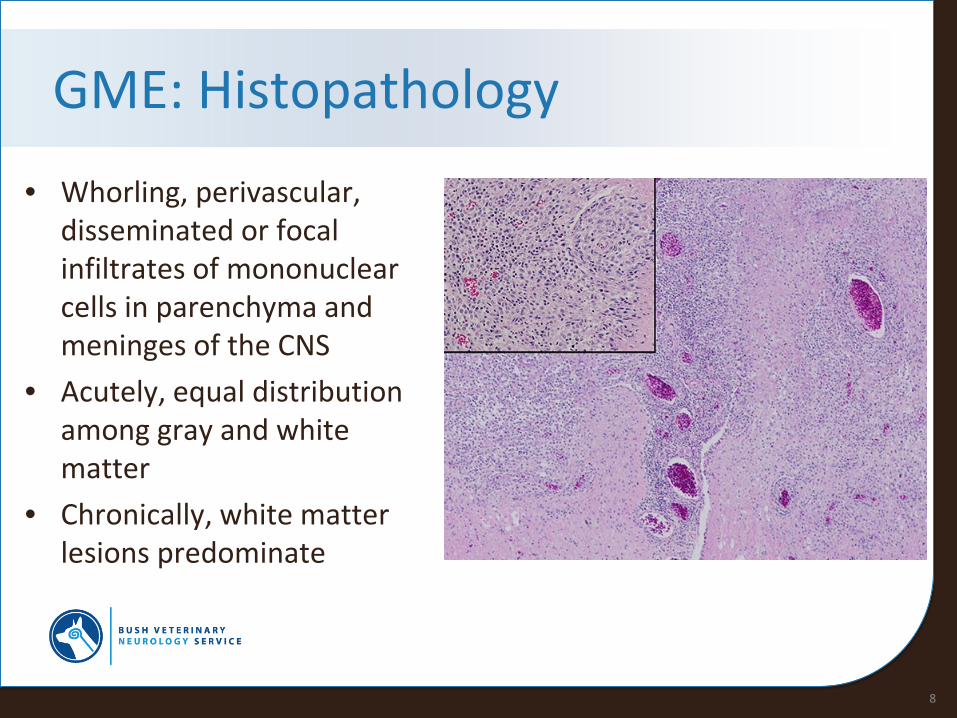
GME: Histopathology
• Whorling, perivascular, disseminated or focal infiltrates of mononuclear cells in parenchyma and meninges of the CNS
• Acutely, equal distribution among gray and white matter
• Chronically, white matter lesions predominate
8
Necrotizing Encephalitis (NE)
• Necrotic lesions in cerebral white or gray matter
• Rapidly progressive neurologic signs • 6 mo - 7 yr, mean age 2.5 yr • Two subtypes: NME, NLE
9
Necrotizing meningoencephalitis (NME) • Young, small breeds • Pugs overrepresented
• Familial inheritance
10
NME: Distribution
• Most often affects the cerebrum and/or thalamus
• Lesions most often located at the junction between the gray and white matter
11
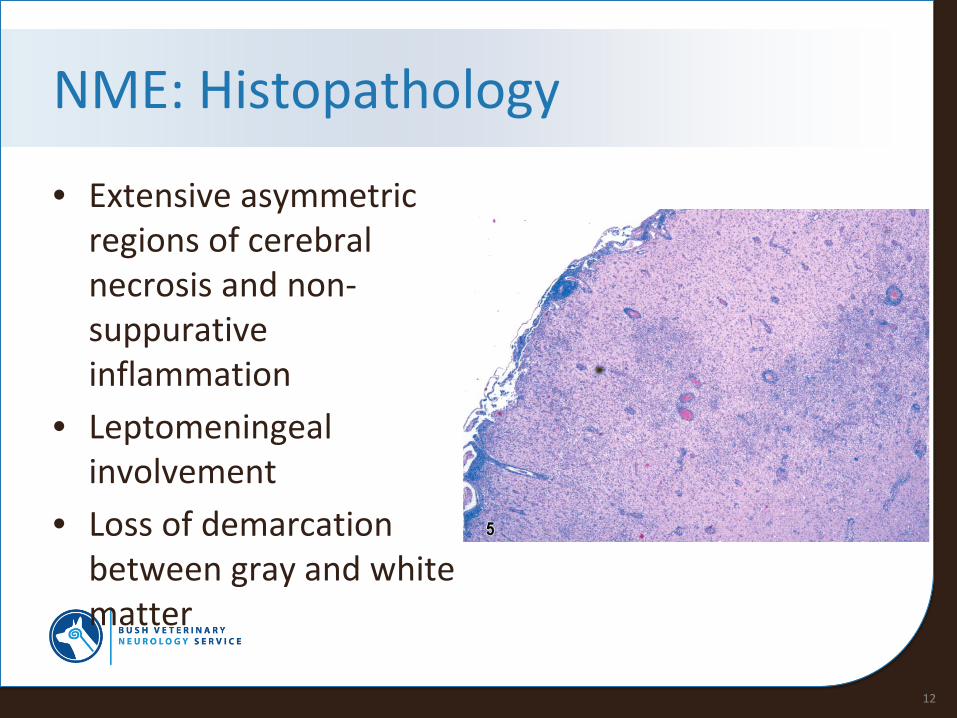
NME: Histopathology
• Extensive asymmetric regions of cerebral necrosis and non-suppurative inflammation
• Leptomeningeal involvement
• Loss of demarcation between gray and white matter
12
Necrotizing leukoencephalitis (NLE)
• Yorkshire Terrier • French bulldog
13
NLE: Distribution
• Forebrain • Brainstem
14
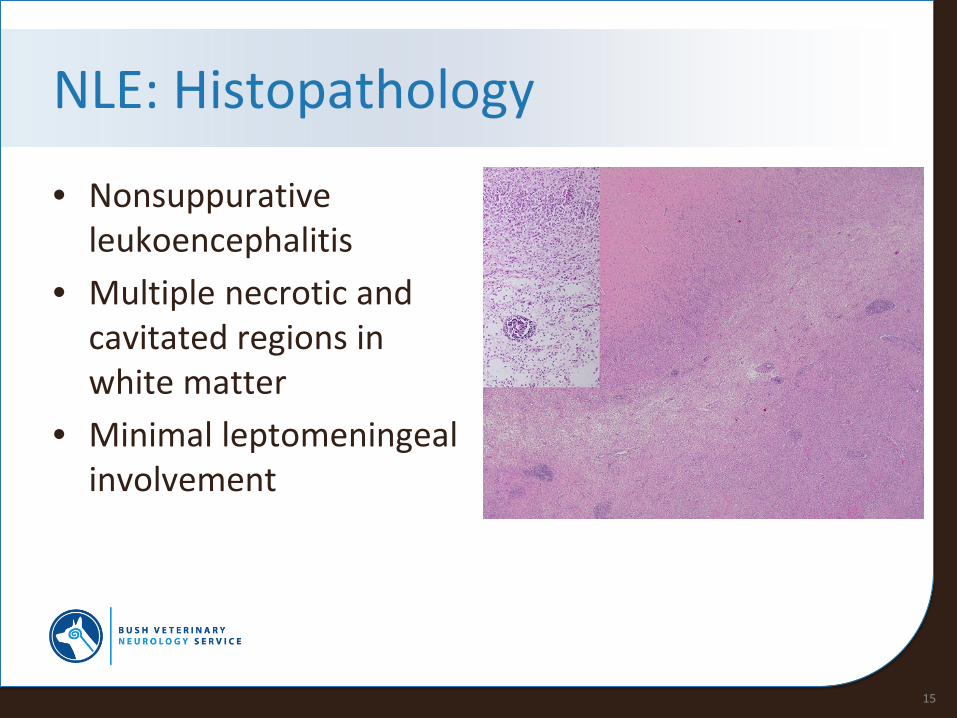
NLE: Histopathology
• Nonsuppurative leukoencephalitis
• Multiple necrotic and cavitated regions in white matter
• Minimal leptomeningeal involvement
15
Clinical presentation
• Varies based on lesion distribution
• Typically, fever is not present
16
Diagnostics: CBC/Chem
• Typically normal
17
Diagnostics: MRI
• Multifocal, single, or diffuse, ill-defined, intra-axial variably contrast-enhancing lesions, hyperintense on T2w and FLAIR
• +/- Leptomeningeal enhancement (NME) • +/- Perilesional edema • +/- Mass effect suggesting elevated ICP • +/- Ventriculomegaly • +/- Cavitary lesions (NE) • Normal (25%)
18
Diagnostics: CSF
• Mononuclear pleocytosis most common • Other pleocytoses possible
• Elevated protein concentration • Due to BBB disruption or intrathecal IgG
production • Nonspecific indicator of CNS disease
• Normal
19
Diagnostics: Rule out infection
• Toxoplasma IgG/IgM • Neospora IFA • Distemper PCR or serology • Tick PCR panel • Cryptococcus PCR or fungal profile • +/- CSF culture and sensitivity
20
Diagnostics: Biopsy (101)
• 82-100% accurate • Methods
• Stereotactic • Ultrasound-guided • Endoscopic-guided • CT-guided
• 6-29% mortality and morbidity • Not commonly performed
21
Treatment: Goal
• Achieve remission • Minimize adverse effects
22
Treatment: Treat the Cause • Empiric antibiotic therapy
• Clindamycin • Doxycycline or minocycline
• Immunosuppressive therapy • Corticosteroid therapy • Cytosine arabinoside • Cyclosporine • Procarbazine • Lomustine
23
Treatment: Treat the Symptoms • Anticonvulsant therapy • Maropitant, meclizine • Pain medications • IV fluids • Nutrition
24
Prognosis • MST
• Multimodal tx: 240-590 d
• Corticosteroid +/- lomustine: 28-357 d
• 56% die within 2 months of diagnosis • 31% (70% of those who live >2 m) have good to excellent long-term
outcomes • Patients that survive 3 months tend to live • Relapses are common (65%) • Most will require life-long therapy • Some may achieve remission and be able to be weaned off all medications
25
Prognosis
• Repeat diagnostics are helpful • MR + CSF more sensitive for predicting relapse • Discontinuing tx before resolution of MR lesions
always resulted in relapse • Abnormal CSF at 3 mo associated with increased risk
of relapse
26
Sophie • 5 yo FS Yorkshire Terrier • Presents for circling
27
History
• 1 week prior, unwilling to navigate stairs and would lose balance/tumble when attempted
• Progressed to worsened incoordination, leaning to the right, head tilt, lethargy, shaking, excessive panting, vomiting
• 1 day prior began circling tightly to the right
28
Examination Findings • Alert and appropriate, excitable
• Moderate head tilt (predominantly right-sided), undulating head and neck movements, intermittent predominantly right-sided head turn
• Ambulatory, moderate vestibulocerebellar ataxia with circling both tightly and widely in both directions (predominantly to the left), hypermetria x4
• Inconsistently slow placing and hopping on the left side
• Inconsistent menace OU (OD>OS)
• Decreased palpebral OD
• Intermittent spontaneous horizontal nystagmus (FFL) and positional vertical nystagmus
• Head pain
• T 103.1 F
29
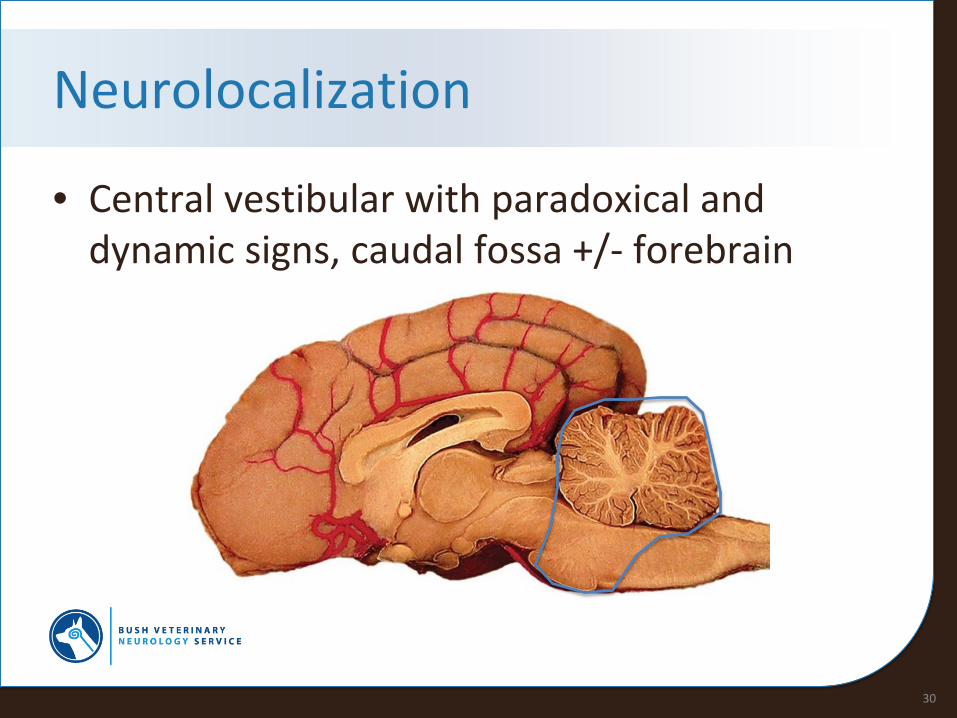
Neurolocalization
• Central vestibular with paradoxical and dynamic signs, caudal fossa +/- forebrain
30
Differentials
• Meningoencephalitis • Congenital malformation • Neoplasia
31
Diagnostics: Preliminary
• CBC: Hct 59.51%, rbc 8.97, Hgb 18.2 g/dL • Chem: BUN 26 mg/dL, Glu 153 mg/dL • BP: 100 mmHg
32
Diagnostics: MRI
33
34
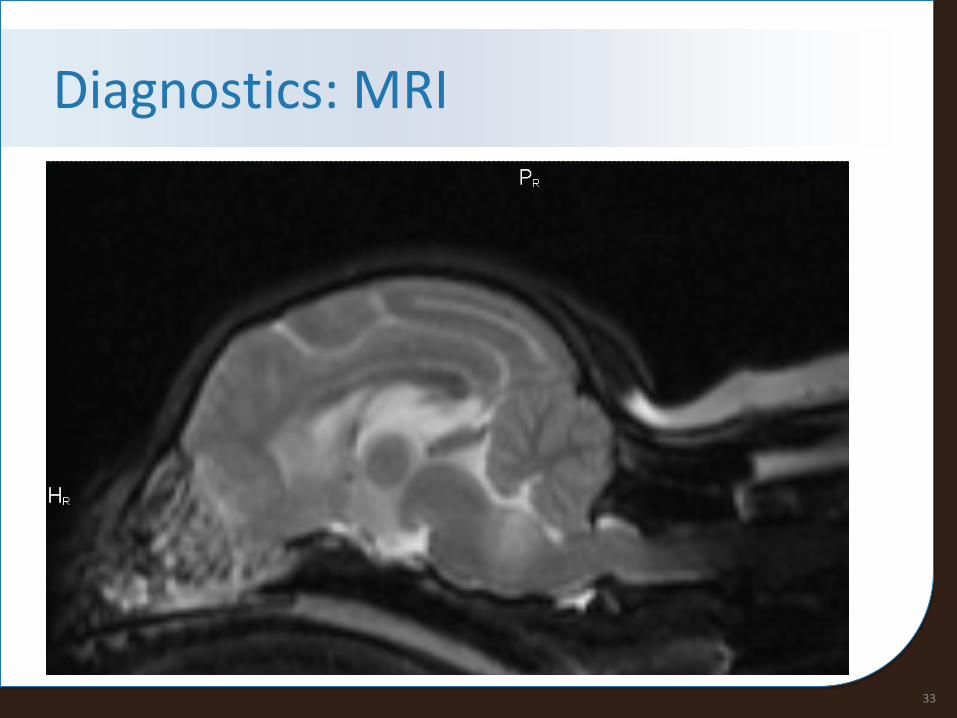
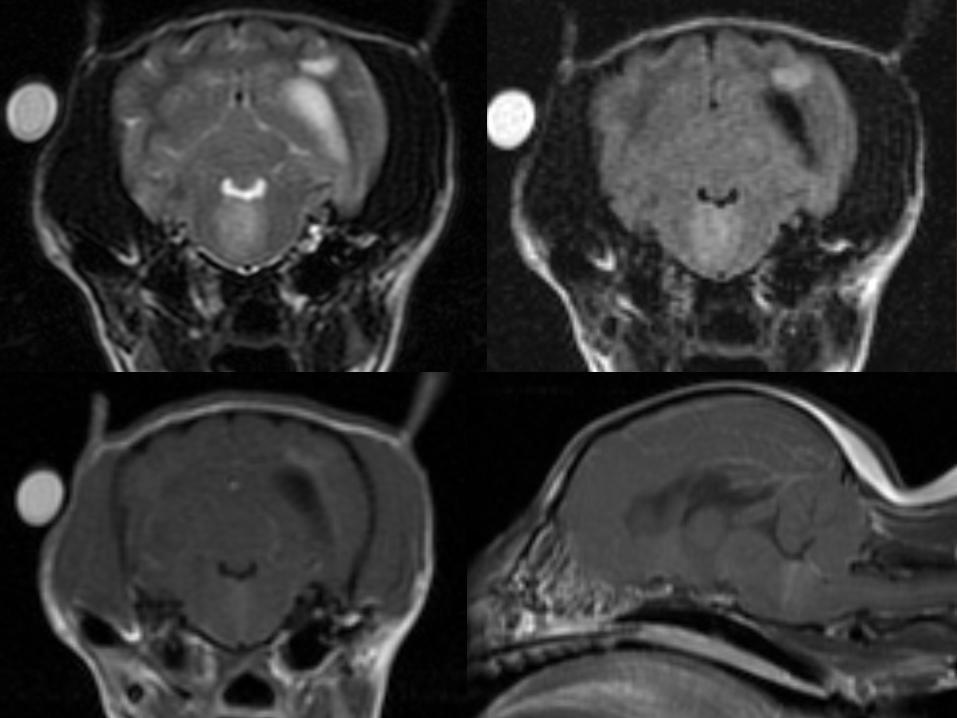
Diagnostics: MRI • Multifocal, ill-defined lesions involving the right frontal lobe, left
occipital lobe and pons, hyper intense on T2w and FLAIR images, moderately contrast-enhancing; most suggestive of inflammatory or neoplastic disease
• Meninges contrast-enhance • Mass effect with leftward shift of the medulla and mild FMH • Mild to moderate COMS, likely exacerbated by suspected inflammatory
disease • Hyperintense signal on T2w images within the cervical spine, likely pre-
syrinx formation or extension of inflammatory disease • Moderate hydrocephalus, likely congenital
35
Diagnostics: CSF
• Not performed due to mass effect and considerable brainstem disease
36
Diagnostics: Infectious Diseases
• Cryptococcus Ag: neg • Toxoplasma IgM/IgG: neg • Neospora IFA: neg
37
Treatment
• Cytosar CRI • Corticosteroid therapy • Doxycycline • Clindamycin
38
• IV fluids • Maropitant • Gabapentin • Famotidine
Progress • Gradual improvement • At discharge 48 hr later
• Mild, slow positional nystagmus (horizontal, FFL) • Circles widely to the left • Hypermetric • Right-sided head tilt and turn • Mildly decreased palpebral and menace OD
• 5d post-discharge • Near normal at home
39
Progress • 12d post-discharge
• Recurrance of vomiting, trouble jumping, lethargy, hugging walls, rubbing face on furniture
• Recheck exam: circling widely in both directions, tightly towards the left, mild positional ventral strabismus OS
• Added in cyclosporine • Gradual return to normal, still doing well today!
40
41
Ralphie
• 4 yo MN Chihuahua • Presented for fever and
head bobbing
42
History • 1 month ago fever and diffuse spinal pain, improved on
gabapentin and meloxicam • Signs recurred once meloxicam was discontinued, started
prednisone and improved • With tapering of prednisone, lethargic, inappetent, staring
off, coughing, febrile, head bobbing • Restarted prednisone, started doxycycline and clindamycin • Yesterday, tachypnic and hacking cough • Previous CBC, chem, 4DX, AUS and rads wnl
43
Examination Findings
• Hypersalivation • Ambulatory, occasionally lifts up LTL • Inconsistent menace OU (OD>OS) • Head and cervical pain
44
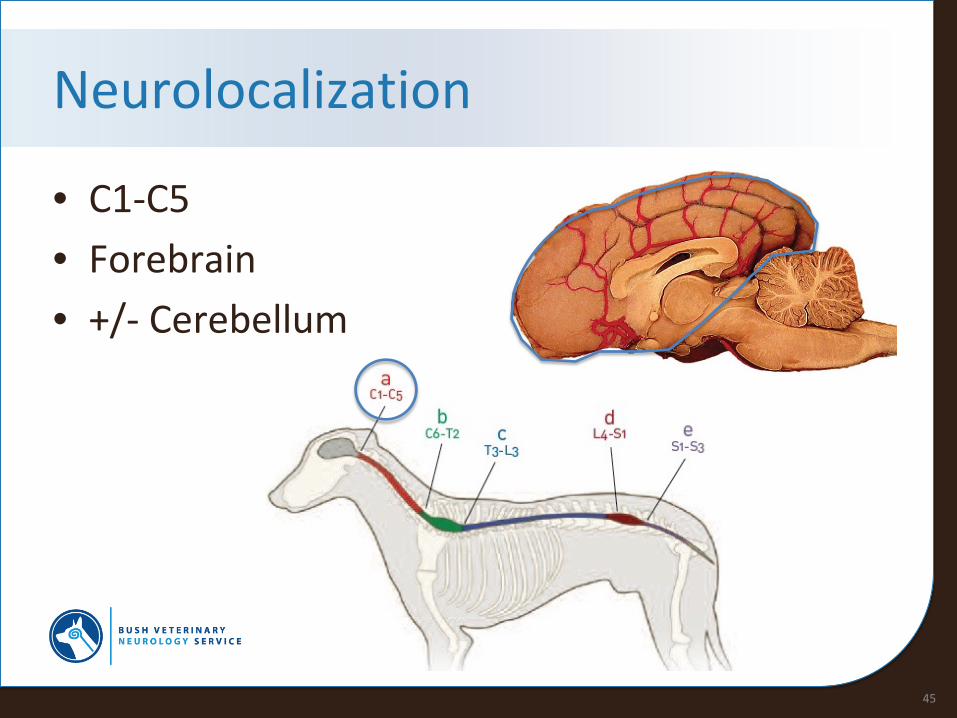
Neurolocalization
• C1-C5 • Forebrain • +/- Cerebellum
45
Differentials
• MUE • Neoplasia • Congenital malformation • Metabolic
46
Diagnostics: Preliminary
• CBC: wnl • Chem: ALT 483 U/L, Glu 131 mg/dL
47
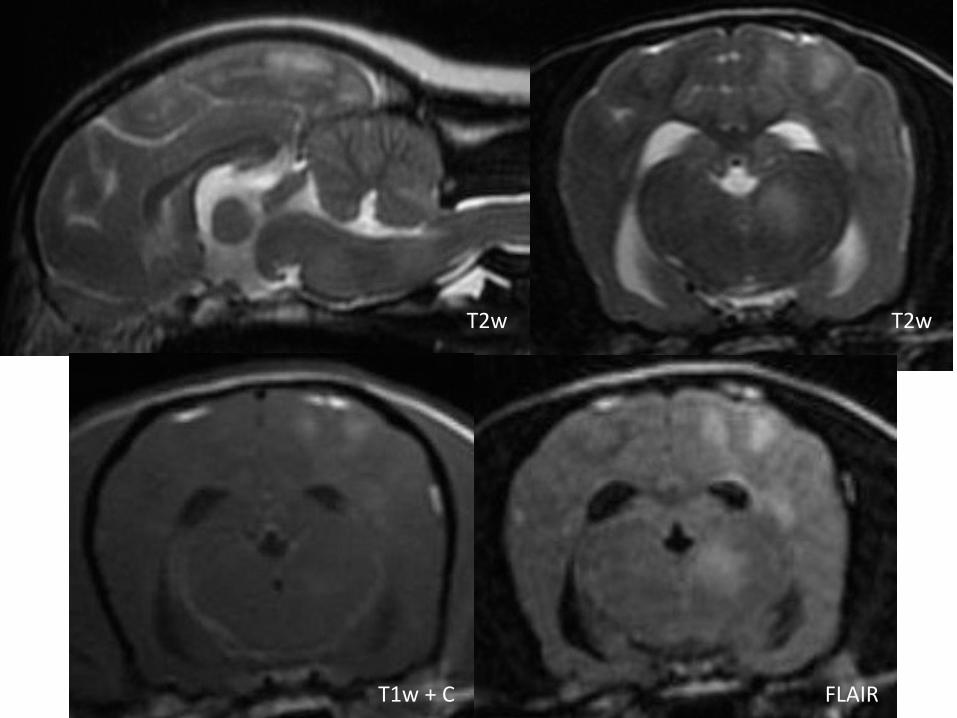
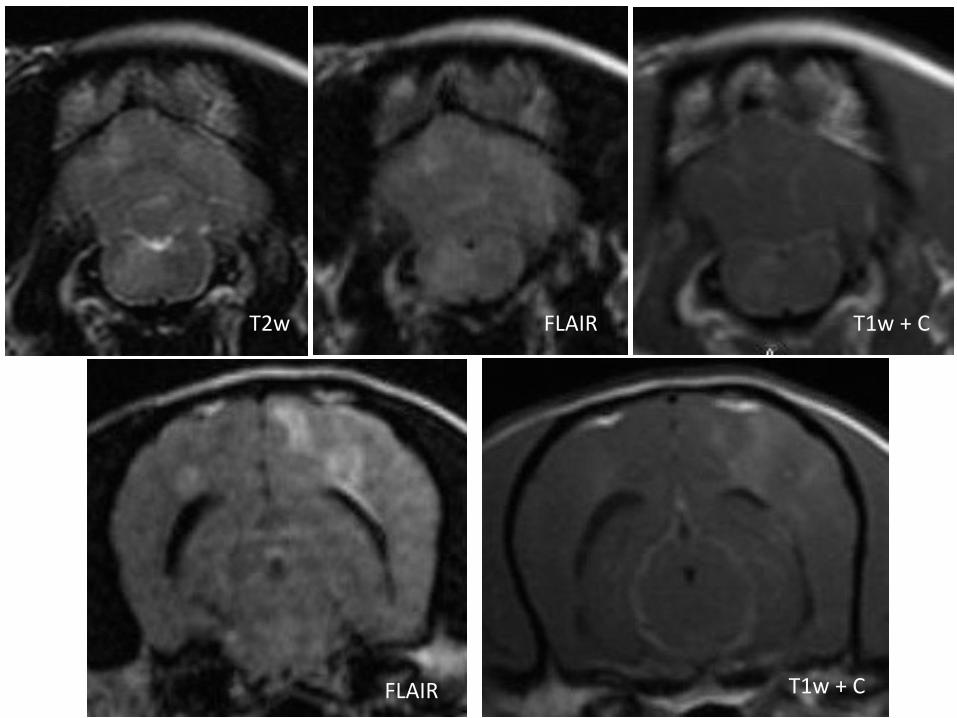
Diagnostics: MRI
• Multifocal contrast-enhancing lesions throughout white matter of all regions of the brain, hyperintense on T2w and FLAIR images
48
FLAIR
T2w T2w
T1w + C
FLAIR
FLAIR T2w T1w + C
T1w + C
Diagnostics: CSF
• Protein: 300 mg/dL • Cell count: 2376 wbc/uL • Cytology: 44% lymphocytes, 30% neutrophils,
26% monocytes • Mixed/mononuclear pleocytosis
51
Diagnostics: Infectious Diseases
• Cryptococcus Ag: neg • Distemper PCR: neg
52
Treatment
• Cytosar CRI • Prednisone • Cyclosporine • Clindamycin • Doxycycline
53
• IV fluids • Gabapentin • Famotidine
Progress
• Signs waxed and waned for the next couple of months
• In general, steady decline • Persistent cough • Vestibular ataxia • Decreased gag • Dull • CP deficits
54
Progress
• Repeat CXR wnl • Repeat MRI
55

T2w T2w
FLAIR T1w + C
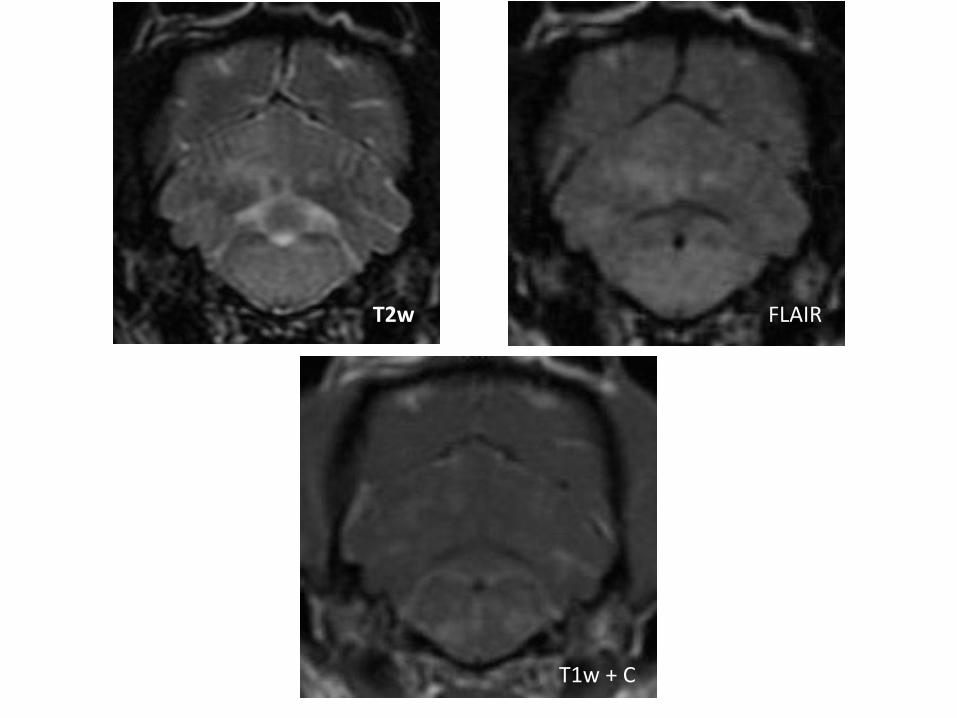
T2w FLAIR
T1w + C
Outcome
• Ralphie was euthanized
58
References • Adamo P, Adams W and Steinberg H. Granulomatous meningoencephalitis in dogs.
Compendium 2007;29(11):678-90.
• Coates J and Jeffery N. Perspectives on meningoencephalitis of unknown origin. Veterinary Clinics of North America: Small Animal Practice 2014;44(6),1157-1185.
• Flegel T, Boettcher IC, Matiasek K, et al. Comparison of oral administration of lomustine and prednisolone or prednisolone alone as treatment for granulomatous meningoencephalomyelitis or necrotizing encephalitis in dogs. J Am Vet Med Assoc 2011;238:337-45.
• Higginbotham M, Kent M and Glass E. Noninfectious inflammatory central nervous system diseases in dogs. Compendium 2007;29(8):488-97.
• Lamb CR, Croson PJ, Cappellow R, et al. Magnetic resonance imaging findings in 25 dogs with inflammatory cerebrospinal fluid. Vet Radiol Ultrasound 2005;46:17-22.
• Lowrie M, Smith PM, Garosi L. Meningoencephalitis of unknown origin: investigation of prognostic factors and outcome using a standard treatment protocol. Vet Rec 2013;172:527-34.
59
Acknowledgements
• Dr. David Brewer • Sophie and Ralphie’s committed owners
60