A systematic review and meta-analysis comparing immediate ... · place is generally based on custom...
10
ORIGINAL ARTICLE A systematic review and meta-analysis comparing immediate and delayed catheter removal following uncomplicated hysterectomy Peng Zhang & Wan-Li Hu & Bei Cheng & Long Cheng & Xiao-Kan Xiong & Yang-Jun Zeng Received: 27 August 2014 /Accepted: 18 October 2014 /Published online: 15 November 2014 # The International Urogynecological Association 2014 Abstract Background The use of an indwelling catheter after uncom- plicated hysterectomy is common, but remains controversial because of the occurrence of catheter-associated urinary tract infections (UTIs) and discomfort. Objective To examine the evidence on the benefits and harm from the use of an indwelling catheter after uncomplicated hysterectomy. Design Systematic review and meta-analysis of randomized controlled trials (RCTs). Data sources Electronic databases including PubMed, Embase, the Cochrane Library, and Science Citation Index up to July 2014 were searched for relevant RCTs and the reference lists of the included studies were also searched manually. Review methods Included studies were RCTs comparing im- mediate and delayed catheter removal following uncomplicat- ed hysterectomy without concomitant pelvic floor surgery. Two independent reviewers identified relevant RCTs, assessed their methodological quality and extracted data. Mantel-Haenszel estimates were calculated and pooled using a fixed or random effects model data are expressed as relative risks (RRs) and 95 % confidence intervals (CIs). Results Ten RCTs with a total of 1,188 patients that met the inclusion criteria were analysed. Early catheter removal was associated with a reduced risk of positive urine culture (RR 0.60, 95 % CI 0.40 to 0.88) and symptomatic UTI (RR 0.23, 95 % CI 0.10 to 0.52). However, the incidence of recatheterization was lower among patients with delayed cath- eter removal (RR 3.32, 95 % CI 1.48 to 7.46). There was no significant difference in febrile morbidity associated with UTI between the two approaches (RR 0.38, 95 % CI 0.11 to 1.36). In addition, delayed catheter removal was asso- ciated with a longer time to first ambulation (standard mean difference -2.73, 95 % CI -4.00 to -1.47]. Conclusions The existing evidence from RCTs suggests that delayed catheter removal following uncomplicated hysterectomy increases the incidence of postoperative bac- teriuria and symptomatic UTI but reduces the risk of recatheterization. Keywords Catheter . Hysterectomy . Urinary tract infection . Urinary retention Abbreviations RCT randomized controlled trial. RR relative risk. SMD standard mean difference. CI confidence intervals. UTI urinary tract infection. PRISMA the Preferred Reporting Items for Systematic Reviews and Meta-Analysis. Electronic supplementary material The online version of this article (doi:10.1007/s00192-014-2561-0) contains supplementary material, which is available to authorized users. P. Zhang : W.<L. Hu (*) : L. Cheng : Y.<J. Zeng Department of Urology, Zhongnan Hospital, Wuhan University, 115 Donghu load, Wuchang district, Wuhan 430071, Hubei, China e-mail: [email protected] B. Cheng School of Basic Medicine, Department of Medicine, Wuhan University, Wuhan, Hubei 430071, People’ s Republic of China X.<K. Xiong Department of Endocrinology, Zhongnan Hospital, Wuhan University, Wuhan, Hubei 430071, People’ s Republic of China Int Urogynecol J (2015) 26:665–674 DOI 10.1007/s00192-014-2561-0
Transcript of A systematic review and meta-analysis comparing immediate ... · place is generally based on custom...

ORIGINAL ARTICLE
A systematic review and meta-analysis comparing immediateand delayed catheter removal following uncomplicatedhysterectomy
Peng Zhang & Wan-Li Hu & Bei Cheng & Long Cheng &
Xiao-Kan Xiong & Yang-Jun Zeng
Received: 27 August 2014 /Accepted: 18 October 2014 /Published online: 15 November 2014# The International Urogynecological Association 2014
AbstractBackground The use of an indwelling catheter after uncom-plicated hysterectomy is common, but remains controversialbecause of the occurrence of catheter-associated urinary tractinfections (UTIs) and discomfort.Objective To examine the evidence on the benefits and harmfrom the use of an indwelling catheter after uncomplicatedhysterectomy.Design Systematic review and meta-analysis of randomizedcontrolled trials (RCTs).Data sources Electronic databases including PubMed,Embase, the Cochrane Library, and Science Citation Indexup to July 2014 were searched for relevant RCTs and thereference lists of the included studies were also searchedmanually.Review methods Included studies were RCTs comparing im-mediate and delayed catheter removal following uncomplicat-ed hysterectomy without concomitant pelvic floor surgery.
Two independent reviewers identified relevant RCTs,assessed their methodological quality and extracted data.Mantel-Haenszel estimates were calculated and pooled usinga fixed or random effects model data are expressed as relativerisks (RRs) and 95 % confidence intervals (CIs).Results Ten RCTs with a total of 1,188 patients that met theinclusion criteria were analysed. Early catheter removal wasassociated with a reduced risk of positive urine culture (RR0.60, 95 % CI 0.40 to 0.88) and symptomatic UTI (RR 0.23,95 % CI 0.10 to 0.52). However, the incidence ofrecatheterization was lower among patients with delayed cath-eter removal (RR 3.32, 95 % CI 1.48 to 7.46). There was nosignificant difference in febrile morbidity associated withUTI between the two approaches (RR 0.38, 95 % CI 0.11to 1.36). In addition, delayed catheter removal was asso-ciated with a longer time to first ambulation (standardmean difference −2.73, 95 % CI −4.00 to −1.47].Conclusions The existing evidence from RCTs suggeststhat delayed catheter removal following uncomplicatedhysterectomy increases the incidence of postoperative bac-teriuria and symptomatic UTI but reduces the risk ofrecatheterization.
Keywords Catheter . Hysterectomy . Urinary tract infection .
Urinary retention
AbbreviationsRCT randomized controlled trial.RR relative risk.SMD standard mean difference.CI confidence intervals.UTI urinary tract infection.PRISMA the Preferred Reporting Items for Systematic
Reviews and Meta-Analysis.
Electronic supplementary material The online version of this article(doi:10.1007/s00192-014-2561-0) contains supplementary material,which is available to authorized users.
P. Zhang :W.<L. Hu (*) : L. Cheng :Y.<J. ZengDepartment of Urology, Zhongnan Hospital,Wuhan University,115 Donghu load, Wuchang district, Wuhan 430071, Hubei, Chinae-mail: [email protected]
B. ChengSchool of Basic Medicine, Department of Medicine,Wuhan University,Wuhan, Hubei 430071, People’s Republic of China
X.<K. XiongDepartment of Endocrinology, Zhongnan Hospital,Wuhan University,Wuhan, Hubei 430071, People’s Republic of China
Int Urogynecol J (2015) 26:665–674DOI 10.1007/s00192-014-2561-0

Introduction
Hysterectomy for noncancerous conditions is the most com-mon major gynaecological operation performed. Women inthe US and UK have a high chance of hysterectomy by the ageof 55 years [1–3]. To prevent iatrogenic injury to the bladderand postoperative urinary retention, the placement of an in-dwelling urinary catheter is a standard procedure in womenundergoing hysterectomy [4]. The indwelling catheter is re-moved 24 h or more after surgery to assess urinary output andto prevent postoperative urinary retention because patientswith abdominal wounds are less able to increase the intra-abdominal pressure to aid voiding [5].
However, the placement of an indwelling catheter follow-ing uncomplicated hysterectomy remains controversial.Indwelling urinary catheterization is associated with an in-creased white cell count, a higher rate of positive urine culture,and even symptomatic urinary tract infection (UTI) [6, 7].Furthermore, UTI can also result in an increase in morbidity,length of hospital stay, and overall healthcare cost [7, 8].Evidence-based international clinical practice guidelines forprocedures and strategies to reduce the risks of catheter-associated asymptomatic bacteriuria and UTIs wereestablished by the expert panel of the Infectious DiseasesSociety of America [9]. They support the recommendationthat indwelling catheters should be removed once they areno longer required for reducing the risks of bacteriuria andUTI [9].
The time a postoperative indwelling catheter should be inplace is generally based on custom rather than strong pub-lished evidence and consequently varies considerably [10,11]. Summitt et al. concluded that short-term catheter drainageafter uncomplicated vaginal hysterectomy is unnecessary[12]. However, Dobbs et al. found that short-term indwellingurinary catheterization carried a low risk of patient morbiditycompared to “in–out” urinary catheterization [13]. Dunn et al.in a prospective randomized controlled trial (RCT) in 250women found that immediate catheter removal followinghysterectomy was not associated with an increase in adverseoutcomes and was associated with less pain [14].Postoperative fever, UTI and recatheterization were not sig-nificantly different in their study between immediate anddelayed catheter removal (at 24 hours) [14]. They suggestedthat immediate removal of the catheter might be beneficial topatients in the early postoperative period [14]. Chai and Punfound that there were no significant differences in the inci-dence of positive urine culture, symptomatic UTI and urethralpain between immediate and delayed catheter removal (at24 hours) following total abdominal hysterectomy [5].
We performed a systematic review and meta-analysis com-paring immediate and delayed catheter removal followinghysterectomy to identify the benefits and harm from the useof an indwelling catheter after uncomplicated hysterectomy.
Materials and methods
Before the systematic review and meta-analysis was conduct-ed, we registered the protocol on the PROSPERO database(www.crd.york.ac.uk/PROSPERO) and the protocol(CRD42014013081) was published on the website.Subsequently, our systematic review and meta-analysis wasperformed based on the methodology recommended by theCochrane Collaboration and according to the PreferredReporting Items for Systematic Reviews and Meta-Analysis(PRISMA) statement [15].
Eligibility criteria
Studies were included if they met the following criteria: (1)study participants were women undergoing total hysterectomyfor benign conditions, and were excluded if they had positivepreoperative urine culture or any urinary symptom or otherillnesses possibly interfering with the outcomes of studies; (2)RCTs with designs involving immediate and delayed catheterremoval following hysterectomy as the control and interven-tion arms, respectively; (3) at least one of two key outcomesreported including UTI diagnosed on urine culture or othermethods and urinary retention or recatheterization.
Search strategy
We searched PubMed (1966 to August 2014), Embase (1974to August 2014), the Cochrane Library (issue 8, August 2014)and Science Citation Index (1974 to August 2014) to obtainparallel RCTs meeting the inclusion criteria. The search strat-egy is summarized in Appendix S1.We searched the referencelists of the included studies by hand to further identify relevantstudies, and unpublished studies not found by the searchstrategy. No limits based on language were imposed.
Study selection and data extraction
The titles and abstracts were screened independently by tworeviewers (Long Cheng and Xiao-Kan Xiong). They indepen-dently assessed the titles and abstracts of all identified trials toconfirm whether the inclusion criteria were met. Data wereextracted independently by two authors using standard dataextraction forms including study characteristics (title, publi-cation time, and sample size), detailed information included inthe PICOS approach (participant, intervention, comparison,outcomes, and study design), and other characteristics. Whenthe study design involved catheter removal at multiple timepoints after surgery in patients with delayed catheter removal,we used a delay of 24 hours or more than or close to 24 hours.Disagreements were resolved in consultation with an arbitra-tor (Bei Cheng). We also contacted the authors of the originalstudies for missing information where necessary.
666 Int Urogynecol J (2015) 26:665–674
Methodological quality assessment
We used the Cochrane Collaboration tool for assessing risk ofbias to evaluate the methodological quality of each includedRCT [16]. For assessing bias, the tool provides seven items:random sequence generation (selection bias), allocation con-cealment (selection bias), blinding of participants and person-nel (performance bias), blinding of outcome assessment (de-tection bias), incomplete outcome data (attrition bias), selec-tive reporting (reporting bias) and other bias [17]. Each itemwas categorized as low risk of bias, “unclear” (either lack ofinformation or uncertainty over the potential for bias), andhigh risk of bias following the guidance in the CochraneHandbook [17].
Data synthesis and analysis
The meta-analysis was performed with Stata 12.0 softwareaccording to the PRISMA guidelines. Heterogeneity wasassessed by examining the clinical characteristics of the in-cluded studies as well as by formal statistical testing with χ2
and I2. For binary outcomes, we used Mantel-Haenszel esti-mates with a fixed-effect analytical model to calculate relative
risks (RRs) and their 95 % confidence intervals (CIs) unlessthere was significant heterogeneity among the studies (I2
values of more than 40 %), in which case a random effectsstatistical model was used [17]. For continuous outcomes, weused inverse variance estimates in a random effects model tocalculate standard mean differences (SMDs) and their 95 %CIs when there was significant between-trial heterogeneitybased on I2 values of more than 40 % [17]. When there arefewer than ten studies in a meta-analysis, the funnel plotmethods of Begg and Egger are known to be unreliable andwe could not apply these methods [17, 18].We also performedsensitivity analyses according to methodological qualityparameters.
Results
Characteristics of the included studies
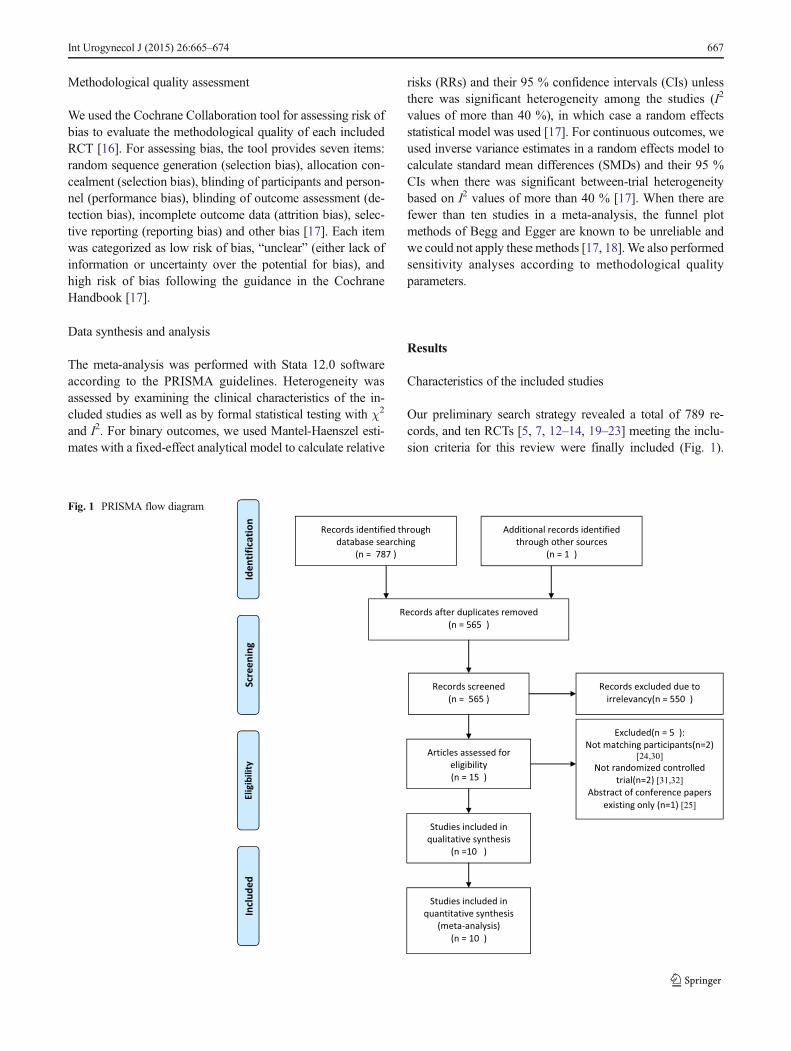
Our preliminary search strategy revealed a total of 789 re-cords, and ten RCTs [5, 7, 12–14, 19–23] meeting the inclu-sion criteria for this review were finally included (Fig. 1).
Fig. 1 PRISMA flow diagram
Int Urogynecol J (2015) 26:665–674 667
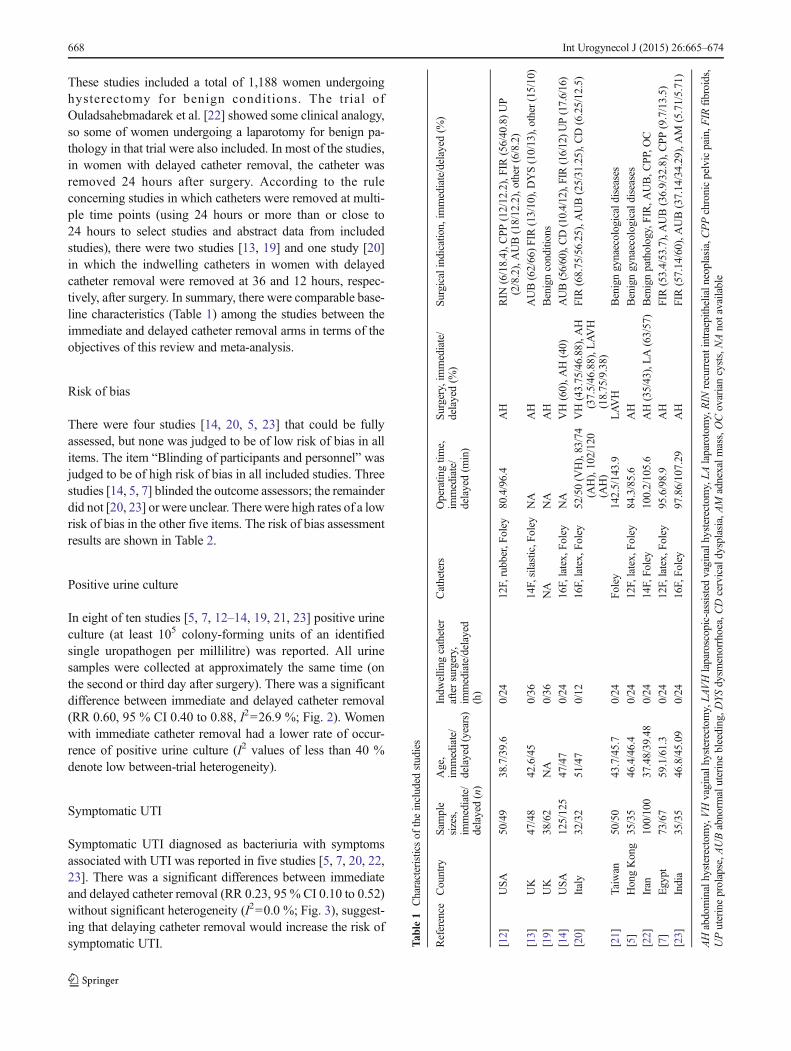
These studies included a total of 1,188 women undergoinghysterectomy for benign conditions. The trial ofOuladsahebmadarek et al. [22] showed some clinical analogy,so some of women undergoing a laparotomy for benign pa-thology in that trial were also included. In most of the studies,in women with delayed catheter removal, the catheter wasremoved 24 hours after surgery. According to the ruleconcerning studies in which catheters were removed at multi-ple time points (using 24 hours or more than or close to24 hours to select studies and abstract data from includedstudies), there were two studies [13, 19] and one study [20]in which the indwelling catheters in women with delayedcatheter removal were removed at 36 and 12 hours, respec-tively, after surgery. In summary, there were comparable base-line characteristics (Table 1) among the studies between theimmediate and delayed catheter removal arms in terms of theobjectives of this review and meta-analysis.
Risk of bias
There were four studies [14, 20, 5, 23] that could be fullyassessed, but none was judged to be of low risk of bias in allitems. The item “Blinding of participants and personnel” wasjudged to be of high risk of bias in all included studies. Threestudies [14, 5, 7] blinded the outcome assessors; the remainderdid not [20, 23] or were unclear. There were high rates of a lowrisk of bias in the other five items. The risk of bias assessmentresults are shown in Table 2.
Positive urine culture
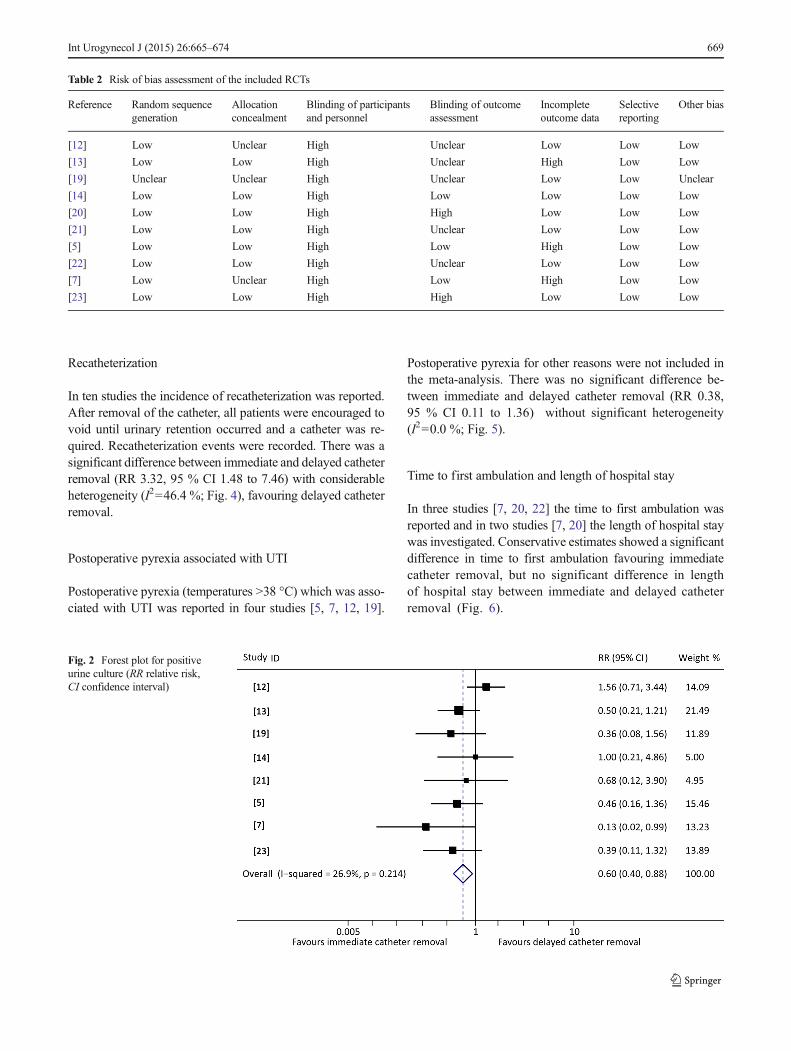
In eight of ten studies [5, 7, 12–14, 19, 21, 23] positive urineculture (at least 105 colony-forming units of an identifiedsingle uropathogen per millilitre) was reported. All urinesamples were collected at approximately the same time (onthe second or third day after surgery). There was a significantdifference between immediate and delayed catheter removal(RR 0.60, 95 % CI 0.40 to 0.88, I2=26.9 %; Fig. 2). Womenwith immediate catheter removal had a lower rate of occur-rence of positive urine culture (I2 values of less than 40 %denote low between-trial heterogeneity).
Symptomatic UTI
Symptomatic UTI diagnosed as bacteriuria with symptomsassociated with UTI was reported in five studies [5, 7, 20, 22,23]. There was a significant differences between immediateand delayed catheter removal (RR 0.23, 95 % CI 0.10 to 0.52)without significant heterogeneity (I2=0.0 %; Fig. 3), suggest-ing that delaying catheter removal would increase the risk ofsymptomatic UTI. T
able1
Characteristicsof
theincluded
studies
Reference
Country
Sample
sizes,
immediate/
delayed(n)
Age,
immediate/
delayed(years)
Indw
ellin
gcatheter
aftersurgery,
immediate/delayed
(h)
Catheters
Operatin
gtim
e,im
mediate/
delayed(m
in)
Surgery,immediate/
delayed(%
)Su
rgicalindicatio
n,im
mediate/delayed
(%)
[12]
USA
50/49
38.7/39.6
0/24
12F,rubber,F
oley
80.4/96.4
AH
RIN
(6/18.4),C
PP(12/12.2),FIR(56/40.8)UP
(2/8.2),AUB(18/12.2),other(6/8.2)
[13]
UK
47/48
42.6/45
0/36
14F,silastic,F
oley
NA
AH
AUB(62/66)FIR(13/10),DYS(10/13),other(15/10)
[19]
UK
38/62
NA
0/36
NA
NA
AH
Benignconditions
[14]
USA
125/125
47/47
0/24
16F,latex,Foley
NA
VH(60),A
H(40)
AUB(56/60),CD(10.4/12),FIR(16/12)UP(17.6/16)
[20]
Italy
32/32
51/47
0/12
16F,latex,Foley
52/50(V
H),83/74
(AH),102/120
(AH)
VH(43.75/46.88),AH
(37.5/46.88),L
AVH
(18.75/9.38)
FIR(68.75/56.25),AUB(25/31.25),C
D(6.25/12.5)
[21]
Taiwan
50/50
43.7/45.7
0/24
Foley
142.5/143.9
LAVH
Benigngynaecologicaldiseases
[5]
HongKong
35/35
46.4/46.4
0/24
12F,latex,Foley
84.3/85.6
AH
Benigngynaecologicaldiseases
[22]
Iran
100/100
37.48/39.48
0/24
14F,Fo
ley
100.2/105.6
AH(35/43),LA(63/57)
Benignpathology,FIR,A
UB,C
PP,O
C
[7]
Egypt
73/67
59.1/61.3
0/24
12F,latex,Foley
95.6/98.9
AH
FIR(53.4/53.7),AUB(36.9/32.8),CPP
(9.7/13.5)
[23]
India
35/35
46.8/45.09
0/24
16F,Fo
ley
97.86/107.29
AH
FIR(57.14/60),A
UB(37.14/34.29),AM
(5.71/5.71)
AHabdominalhysterectomy,VHvaginalh
ysterectom
y,LA
VHlaparoscopic-assistedvaginalh
ysterectom
y,LAlaparotomy,RIN
recurrentintraepith
elialn
eoplasia,C
PPchronicpelvicpain,F
IRfibroids,
UPuterineprolapse,A
UBabnorm
aluterinebleeding,D
YSdysm
enorrhoea,CDcervicaldysplasia,AM
adnexalm
ass,OCovariancysts,NAnotavailable
668 Int Urogynecol J (2015) 26:665–674
Recatheterization
In ten studies the incidence of recatheterization was reported.After removal of the catheter, all patients were encouraged tovoid until urinary retention occurred and a catheter was re-quired. Recatheterization events were recorded. There was asignificant difference between immediate and delayed catheterremoval (RR 3.32, 95 % CI 1.48 to 7.46) with considerableheterogeneity (I2=46.4 %; Fig. 4), favouring delayed catheterremoval.
Postoperative pyrexia associated with UTI
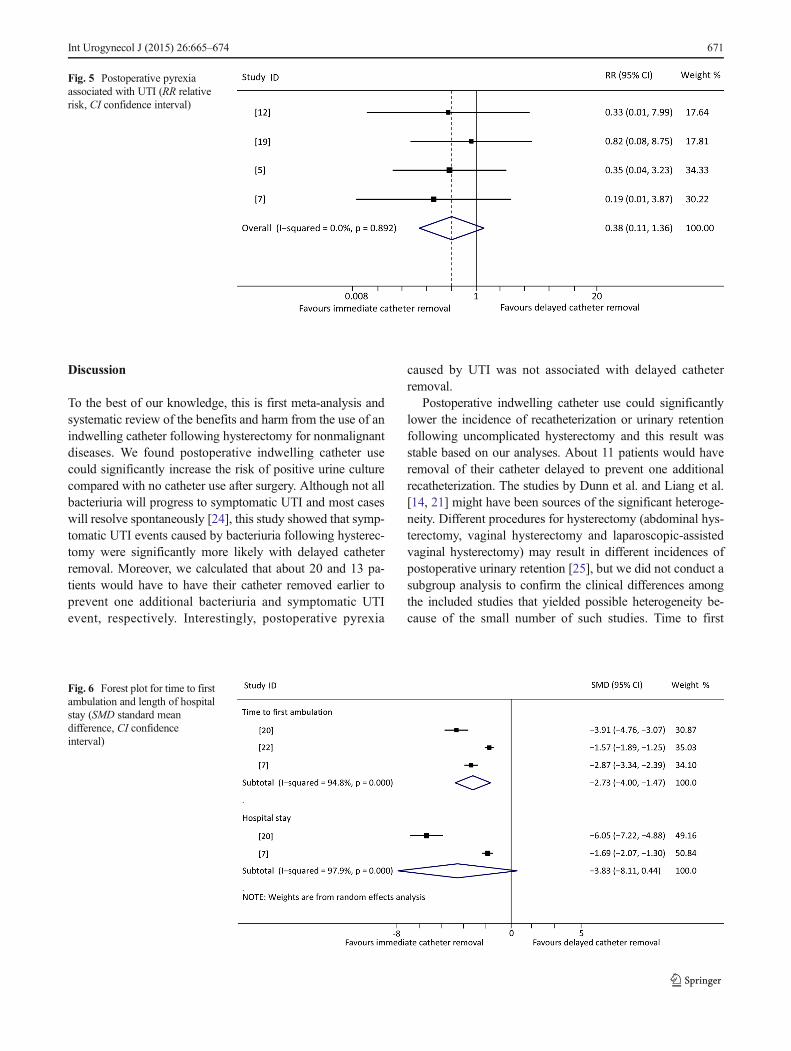
Postoperative pyrexia (temperatures >38 °C) which was asso-ciated with UTI was reported in four studies [5, 7, 12, 19].
Postoperative pyrexia for other reasons were not included inthe meta-analysis. There was no significant difference be-tween immediate and delayed catheter removal (RR 0.38,95 % CI 0.11 to 1.36) without significant heterogeneity(I2=0.0 %; Fig. 5).
Time to first ambulation and length of hospital stay
In three studies [7, 20, 22] the time to first ambulation wasreported and in two studies [7, 20] the length of hospital staywas investigated. Conservative estimates showed a significantdifference in time to first ambulation favouring immediatecatheter removal, but no significant difference in lengthof hospital stay between immediate and delayed catheterremoval (Fig. 6).
Table 2 Risk of bias assessment of the included RCTs
Reference Random sequencegeneration
Allocationconcealment
Blinding of participantsand personnel
Blinding of outcomeassessment
Incompleteoutcome data
Selectivereporting
Other bias
[12] Low Unclear High Unclear Low Low Low
[13] Low Low High Unclear High Low Low
[19] Unclear Unclear High Unclear Low Low Unclear
[14] Low Low High Low Low Low Low
[20] Low Low High High Low Low Low
[21] Low Low High Unclear Low Low Low
[5] Low Low High Low High Low Low
[22] Low Low High Unclear Low Low Low
[7] Low Unclear High Low High Low Low
[23] Low Low High High Low Low Low
Fig. 2 Forest plot for positiveurine culture (RR relative risk,CI confidence interval)
Int Urogynecol J (2015) 26:665–674 669

Catheter-associated discomfort
Because different outcome measures were applied to as-sess catheter-associated discomfort such as vesical or ure-thral pain and relevant urinary symptoms (dysuria, fre-quency, urgency, etc.), these outcomes were not pooled(Table 3). In five studies [5, 12, 14, 22, 23] catheter-associated pain was reported and two of these five studies[14, 22] suggested that immediate catheter removal isassociated with significantly less urethral or vesical pain.Catheter-related lower urinary symptoms were reported inthree studies [7, 13, 21] and two studies of the three [7,13] showed significant differences favouring immediatecatheter removal.
Publication bias and sensitivity analysis
There was no obvious publication bias in the included studiesthat reported the incidence of recatheterization (Fig. 7, Begg’sfunnel plot). Figure 8 shows sensitivity analysis forrecatheterization (Fig. 8a) and positive urine culture (Fig. 8b).There were still significant differences when included studieswere omitted from the pooled analyses. Furthermore, when thestudies by Dunn et al. and Liang et al. [14, 21] were omittedfrom the meta-analysis for recatheterization, the results wereclearly different from those when other studies were omitted.When the study by Summitt et al. [12] was omitted from themeta-analysis for positive urine culture, the results were clearlydifferent from those when other studies were omitted.
Fig. 3 Forest plot forsymptomatic UTI (RR relativerisk, CI confidence interval)
Fig. 4 Forest plot forrecatheterization (RR relative risk,CI confidence interval)
670 Int Urogynecol J (2015) 26:665–674
Discussion
To the best of our knowledge, this is first meta-analysis andsystematic review of the benefits and harm from the use of anindwelling catheter following hysterectomy for nonmalignantdiseases. We found postoperative indwelling catheter usecould significantly increase the risk of positive urine culturecompared with no catheter use after surgery. Although not allbacteriuria will progress to symptomatic UTI and most caseswill resolve spontaneously [24], this study showed that symp-tomatic UTI events caused by bacteriuria following hysterec-tomy were significantly more likely with delayed catheterremoval. Moreover, we calculated that about 20 and 13 pa-tients would have to have their catheter removed earlier toprevent one additional bacteriuria and symptomatic UTIevent, respectively. Interestingly, postoperative pyrexia
caused by UTI was not associated with delayed catheterremoval.
Postoperative indwelling catheter use could significantlylower the incidence of recatheterization or urinary retentionfollowing uncomplicated hysterectomy and this result wasstable based on our analyses. About 11 patients would haveremoval of their catheter delayed to prevent one additionalrecatheterization. The studies by Dunn et al. and Liang et al.[14, 21] might have been sources of the significant heteroge-neity. Different procedures for hysterectomy (abdominal hys-terectomy, vaginal hysterectomy and laparoscopic-assistedvaginal hysterectomy) may result in different incidences ofpostoperative urinary retention [25], but we did not conduct asubgroup analysis to confirm the clinical differences amongthe included studies that yielded possible heterogeneity be-cause of the small number of such studies. Time to first
Fig. 5 Postoperative pyrexiaassociated with UTI (RR relativerisk, CI confidence interval)
Fig. 6 Forest plot for time to firstambulation and length of hospitalstay (SMD standard meandifference, CI confidenceinterval)
Int Urogynecol J (2015) 26:665–674 671

ambulation was clearly longer with delayed catheter removal.This result was meaningful because it is known that routineearly ambulation can decrease the incidence of deep venousthrombosis [26]. However, the meta-analysis showed thatthere was no significant difference between immediateand delayed catheter removal in the length of hospitalstay although there were statistically significant differ-ences in two studies separately [7, 13].
We did not include catheter-associated discomfort in themeta-analysis, but a descriptive review showed that the resultsof some studies supported the logical view that patients withan indwelling catheter suffer more vesical or urethral pain andrelevant urinary symptoms after surgery.
Catheter-associated UTI is the second most common causeof hospital-acquired infection around the world, and usuallyoccurs in patients with an indwelling catheter that drains urineduring and after surgery or illness [27]. As a result of de-
afferentiation of the bladder wall or bladder neck associatedwith nonradical hysterectomy, partial or complete sensorydenervation of the bladder can lead to loss of bladder-fillingsensation, augmenting bladder capacity and urinary retention[28]. However, abnormal bladder function is usually tempo-rary [29]. In our study, we found that delayed indwellingcatheter removal could reduce the incidence of postoperativerecatheterization for urinary retention, and this might be areason for indwelling catheter use after uncomplicatedhysterectomy.
Before we searched the electronic databases, we publishedthe protocol (CRD42014013081) on the PROSPEROwebsite. Our systematic review included ten RCTs and wewere able to analyse a larger sample than has been analysed inany previous study. Low-quality studies were distinguishedfrom the studies included using the Cochrane collaboration’stool for assessing risk of bias. In addition, we performed
Table 3 Discomfort associated with indwelling catheters comparing immediate and delayed catheter removal following hysterectomy
Study Discomfort Assessment method, immediate/delayed (%) P value Significance
[12] Pain from Foley catheter Arbitrary scale 0 – 3 (0 no discomfort, 3severe discomfort)
Not availablea –
[14] Pain in bladder or urethra Wong scale and Self-report scale 0.0001 Favouring immediate removal
[5] Urethral pain Visual analogue scale 0 – 100 1.00 Not significant
[22] Urethral pain Incidence (4/14), visual analogue scale NA/0.002 Favouring immediate removal
[23] Pain in bladder or urethra Pictorial questionnaire 0.567 Not significant
[13] Urinary symptoms Incidence (15/23) <0.1 Favouring immediate removal
[21] Urinary symptoms SF-36, IIQ-7, and UDI-6 scores at 3 and 6 months 0.26/0.773 Not significant
[7] Urinary symptoms Dysuria (0/22.4), frequency (1.4/26.9), urgency(1.4/25.4), loin pain (0/2.9) 1 week after surgery
0.001/0.002/0.001/0.09 Favouring immediate removal
a Only 10.6 % of the women with delayed catheter removal complained of moderate to severe pain and pain in the women with immediate catheterremoval was not recorded
Fig. 7 Funnel plot of includedstudies evaluating the incidenceof recatheterization
672 Int Urogynecol J (2015) 26:665–674
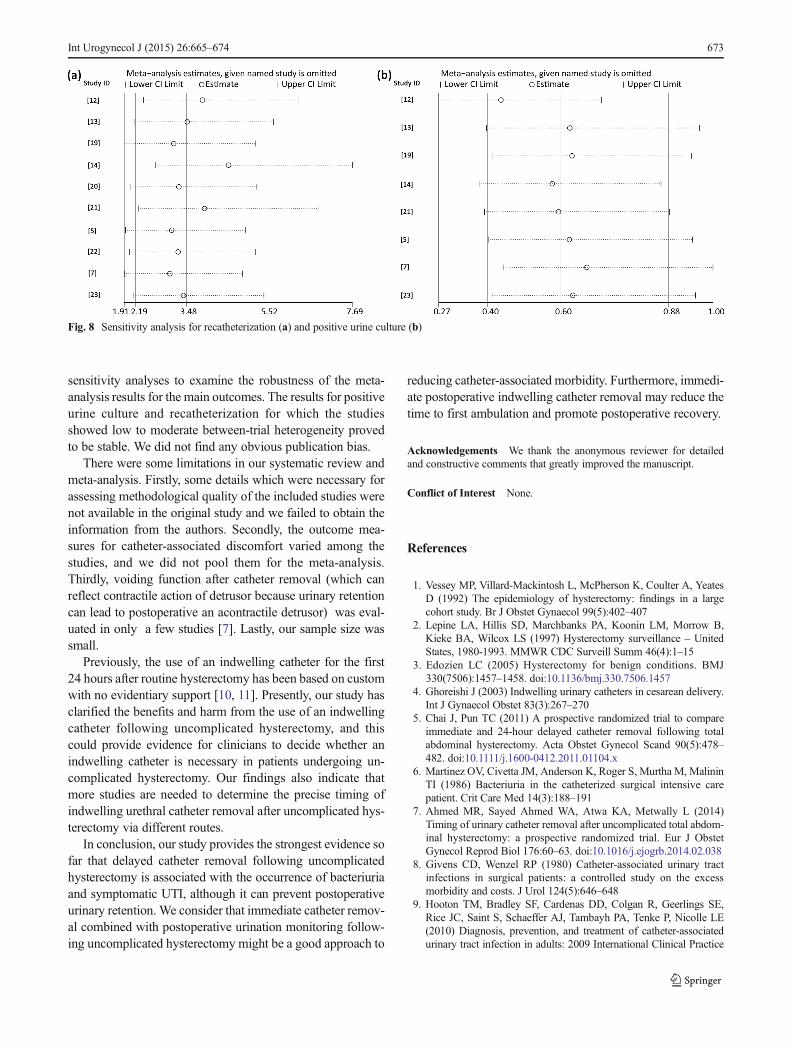
sensitivity analyses to examine the robustness of the meta-analysis results for the main outcomes. The results for positiveurine culture and recatheterization for which the studiesshowed low to moderate between-trial heterogeneity provedto be stable. We did not find any obvious publication bias.
There were some limitations in our systematic review andmeta-analysis. Firstly, some details which were necessary forassessing methodological quality of the included studies werenot available in the original study and we failed to obtain theinformation from the authors. Secondly, the outcome mea-sures for catheter-associated discomfort varied among thestudies, and we did not pool them for the meta-analysis.Thirdly, voiding function after catheter removal (which canreflect contractile action of detrusor because urinary retentioncan lead to postoperative an acontractile detrusor) was eval-uated in only a few studies [7]. Lastly, our sample size wassmall.
Previously, the use of an indwelling catheter for the first24 hours after routine hysterectomy has been based on customwith no evidentiary support [10, 11]. Presently, our study hasclarified the benefits and harm from the use of an indwellingcatheter following uncomplicated hysterectomy, and thiscould provide evidence for clinicians to decide whether anindwelling catheter is necessary in patients undergoing un-complicated hysterectomy. Our findings also indicate thatmore studies are needed to determine the precise timing ofindwelling urethral catheter removal after uncomplicated hys-terectomy via different routes.
In conclusion, our study provides the strongest evidence sofar that delayed catheter removal following uncomplicatedhysterectomy is associated with the occurrence of bacteriuriaand symptomatic UTI, although it can prevent postoperativeurinary retention. We consider that immediate catheter remov-al combined with postoperative urination monitoring follow-ing uncomplicated hysterectomy might be a good approach to
reducing catheter-associated morbidity. Furthermore, immedi-ate postoperative indwelling catheter removal may reduce thetime to first ambulation and promote postoperative recovery.
Acknowledgements We thank the anonymous reviewer for detailedand constructive comments that greatly improved the manuscript.
Conflict of Interest None.
References
1. Vessey MP, Villard-Mackintosh L, McPherson K, Coulter A, YeatesD (1992) The epidemiology of hysterectomy: findings in a largecohort study. Br J Obstet Gynaecol 99(5):402–407
2. Lepine LA, Hillis SD, Marchbanks PA, Koonin LM, Morrow B,Kieke BA, Wilcox LS (1997) Hysterectomy surveillance – UnitedStates, 1980-1993. MMWR CDC Surveill Summ 46(4):1–15
3. Edozien LC (2005) Hysterectomy for benign conditions. BMJ330(7506):1457–1458. doi:10.1136/bmj.330.7506.1457
4. Ghoreishi J (2003) Indwelling urinary catheters in cesarean delivery.Int J Gynaecol Obstet 83(3):267–270
5. Chai J, Pun TC (2011) A prospective randomized trial to compareimmediate and 24-hour delayed catheter removal following totalabdominal hysterectomy. Acta Obstet Gynecol Scand 90(5):478–482. doi:10.1111/j.1600-0412.2011.01104.x
6. Martinez OV, Civetta JM, Anderson K, Roger S, Murtha M, MalininTI (1986) Bacteriuria in the catheterized surgical intensive carepatient. Crit Care Med 14(3):188–191
7. Ahmed MR, Sayed Ahmed WA, Atwa KA, Metwally L (2014)Timing of urinary catheter removal after uncomplicated total abdom-inal hysterectomy: a prospective randomized trial. Eur J ObstetGynecol Reprod Biol 176:60–63. doi:10.1016/j.ejogrb.2014.02.038
8. Givens CD, Wenzel RP (1980) Catheter-associated urinary tractinfections in surgical patients: a controlled study on the excessmorbidity and costs. J Urol 124(5):646–648
9. Hooton TM, Bradley SF, Cardenas DD, Colgan R, Geerlings SE,Rice JC, Saint S, Schaeffer AJ, Tambayh PA, Tenke P, Nicolle LE(2010) Diagnosis, prevention, and treatment of catheter-associatedurinary tract infection in adults: 2009 International Clinical Practice
Fig. 8 Sensitivity analysis for recatheterization (a) and positive urine culture (b)
Int Urogynecol J (2015) 26:665–674 673
Guidelines from the Infectious Diseases Society of America. ClinInfect Dis 50(5):625–663. doi:10.1086/650482
10. Hilton P (1988) Bladder drainage: a survey of practices amonggynaecologists in the British Isles. Br J Obstet Gynaecol 95(11):1178–1189
11. Schiotz HA (1991) Catheterization routines after gynecologic surgeryin Norway. Tidsskr Nor Laegeforen 111(7):841–843
12. Summitt RL Jr, Stovall TG, Bran DF (1994) Prospective comparisonof indwelling bladder catheter drainage versus no catheter aftervaginal hysterectomy. Am J Obstet Gynecol 170(6):1815–1818,discussion 1818–1821
13. Dobbs SP, Jackson SR,Wilson AM,Maplethorpe RP, Hammond RH(1997) A prospective, randomized trial comparing continuous blad-der drainage with catheterization at abdominal hysterectomy. Br JUrol 80(4):554–556
14. Dunn TS, Shlay J, Forshner D (2003) Are in-dwelling cathetersnecessary for 24 hours after hysterectomy? Am J Obstet Gynecol189(2):435–437
15. Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009)Preferred reporting items for systematic reviews and meta-analyses:the PRISMA statement. PLoS Med 6(7):e1000097. doi:10.1371/journal.pmed.1000097
16. Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD,Savovic J, Schulz KF, Weeks L, Sterne JA; Cochrane Bias MethodsGroup; Cochrane Statistical Methods Group (2011) The CochraneCollaboration's tool for assessing risk of bias in randomised trials.BMJ 343:d5928. doi:10.1136/bmj.d5928
17. Higgins JPT, Green S (eds) (2011) Cochrane handbook for system-atic reviews of interventions version 5.1.0 [updated March 2011].The Cochrane Collaboration. Available from www.cochrane-handbook.org
18. Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias inmeta-analysis detected by a simple, graphical test. BMJ 315(7109):629–634
19. Roy S, Sau M, Watson AJ (2001) Bladder care after abdominalhysterectomy: a comparison of in-and-out versus continuous drain-age. J Obstet Gynaecol 21(6):630. doi:10.1080/01443610120085654
20. Alessandri F, Mistrangelo E, Lijoi D, Ferrero S, Ragni N(2006) A prospective, randomized trial comparing immediateversus delayed catheter removal following hysterectomy. ActaObstet Gynecol Scand 85(6):716–720. doi :10.1080/00016340600606976
21. Liang CC, Lee CL, Chang TC, Chang YL, Wang CJ, Soong YK(2009) Postoperative urinary outcomes in catheterized and non-
catheterized patients undergoing laparoscopic-assisted vaginal hys-terectomy – a randomized controlled trial. Int Urogynecol J PelvicFloor Dysfunct 20(3):295–300. doi:10.1007/s00192-008-0769-6
22. Ouladsahebmadarek E, Sayyah-Melli M, Jafari-Shobeiri M (2012) Arandomized clinical trial to compare immediate versus delayed re-moval of foley catheter following abdominal hysterectomy and lap-arotomy. Pak J Med Sci 28(3):380–383
23. Joshi B, Aggarwal N, Chopra S, Taneja N (2014) A prospectiverandomized controlled comparison of immediate versus late removalof urinary catheter after abdominal hysterectomy. J Midlife Health5(2):68–71. doi:10.4103/0976-7800.133990
24. Schiotz HA, Tanbo TG (2006) Postoperative voiding, bacteriuria andurinary tract infection with Foley catheterization after gynecologicalsurgery. Acta Obstet Gynecol Scand 85(4):476–481. doi:10.1080/00016340500409877
25. Arava UM, Roberts M (2013) Is an indwelling catheter needed aftertotal laparoscopic hysterectomy? BJOG 120:404–405
26. Davis JD (2001) Prevention, diagnosis, and treatment of venousthromboembolic complications of gynecologic surgery. Am JObstet Gynecol 184(4):759–775. doi:10.1067/mob.2001.110957
27. Weber DJ, Sickbert-Bennett EE, Gould CV, Brown VM, Huslage K,Rutala WA (2011) Incidence of catheter-associated and non-catheter-associated urinary tract infections in a healthcare system. InfectControl Hosp Epidemiol 32(8):822–823. doi:10.1086/661107
28. Everaert K, De Muynck M, Rimbaut S, Weyers S (2003) Urinaryretention after hysterectomy for benign disease: extended diagnosticevaluation and treatment with sacral nerve stimulation. BJU Int91(6):497–501
29. Weber AM, Walters MD, Schover LR, Church JM, Piedmonte MR(1999) Functional outcomes and satisfaction after abdominal hyster-ectomy. Am J Obstet Gynecol 181(3):530–535
30. Kamilya G, Seal SL, Mukherji J, Bhattacharyya SK, Hazra A (2010)A randomized controlled trial comparing short versus long-termcatheterization after uncomplicated vaginal prolapse surgery. JObstet Gynaecol Res 36(1):154–158. doi:10.1111/j.1447-0756.2009.01096.x
31. Ghezzi F, Cromi A, Uccella S, Colombo G, Salvatore S, Tomera S,Bolis P (2007) Immediate Foley removal after laparoscopic andvaginal hysterectomy: determinants of postoperative urinary reten-tion. J Minim Invasive Gynecol 14(6):706–711
32. Griffiths R, Fernandez R (2007) Strategies for the removal of short-term indwelling urethral catheters in adults. Cochrane Database ofSystematic Reviews, issue 2. Art. no.: CD004011. doi:10.1002/14651858.CD004011.pub3
674 Int Urogynecol J (2015) 26:665–674


![META [DADOS] / META [DATA]](https://static.fdocuments.us/doc/165x107/5790780b1a28ab6874c09b8f/meta-dados-meta-data.jpg)