A Subset of Metastatic Human Colon Cancers Expresses ... · A Subset of Metastatic Human Colon...
9
Vol. 7. 497-504, June 1998 Cancer Epidemiology, Biomarkers & Prevention 497 3 The abbreviation used is: TGF. transforming growth factor. A Subset of Metastatic Human Colon Cancers Expresses Elevated Levels of Transforming Growth Factor 3 11 Antonio Picon, Leslie I. Gold, Jingping Wang, Alfred Cohen, and Eileen Friedman2 Departments of Surgery. Memorial Sloan-Kettering Cancer Center. New York, New York 10021 IA. P., A. Cl; Department of Pathology, New York University Medical Center. New York. New York 10016 [L. I. G.l; and Department of Pathology, SUNY Health Science Center, Syracuse, New York 13210 IJ.W..E.FI Abstract Although transforming growth factor (TGF)431 is a potent growth inhibitor of normal epithelial cells including colonocytes, TGF-fJl has also been implicated as an enhancer of colon cancer metastasis. Decreasing TGF-31 protein levels in the metastatic U9 colon cancer cell line by antisense methodology decreased both U9 cell metastasis to the liver and s.c. tumor formation in a nude mouse system, and the tumors that did arise had regained TGF-31 expression (F. Huang et a!., Cell Growth Differ., 6: 1635-1642, 1995). In addition, in a clinical immunohistochemistry study, colon cancers with elevated TGF-1 protein levels were found to be 18 times more likely to recur as distant metastases than colon cancers expressing low TGF-fil levels, after resection of the primary tumor (E. Friedman et aL, Cancer Epidemiol. Biomark. Prey., 4: 549-554, 1995). Because both studies implicated TGF-j31 in colon cancer metastasis, we wished to know whether a selection bias for TGF-1 was maintained in metastatic cells or was only a property of the primary site tumors that were likely to metastasize. TGF-1 levels were measured using two different antibodies in paired primary site cancers and their metastases by immunohistochemistry and, in selected cases, by Western blot analysis. In 16 of 21 cases (76%) with antibody G and 23 of 31 cases (74%) with antibody P, higher expression of TGF-1 was found in colon cancer cells invading local lymph nodes compared with primary site colon cancer cells, or (2 and 6 cases, respectively) high TGF-1 expression in the primary site cancer was maintained in invasive cells. Analysis by Western blotting using both antibodies also demonstrated that higher levels of TGF-fil protein were found in metastases compared with the primary site tumor or normal tissue. Additional cases of paired primary site Received 5/20/97: revised I 2/8/97: accepted 3/I 6/98. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be hereby marked advertisenvent in accordance with 18 U.S.C. Section 1734 solely to indicate this fact. Supported by NCI ROI CA75708 (to E. F.) and National Cancer Institute ROI CA49507 (to L. I. G.. 2 To whom requests for reprints should be addressed, at Department of Pathology, SUNY Health Science Center at Syracuse. 750 East Adams Street, Syracuse. NY 13210. Phone: (315)464-7148: Fax: (315)464-8419. colon cancer, local lymph node metastases, and cancer cells metastasizing to distant sites were examined. In six of eight such cases (75%), TGF-1 levels were increased in both invasive cell populations compared with the primary site cancer (five cases), or high levels in the primary site cancer were maintained in the metastatic cells (one case). These data suggest that TGF-fil plays a role in promoting colon cancer metastasis throughout the metastatic process in roughly 75% of cases. TGF-1 may increase metastasis by paracrine mechanisms, such as suppression of local immune response or increased angiogenesis, as was seen with the U9 cell line. In those cancers with nonmutated TGF4J receptors and non- mutated smad proteins like U9 cells, TGF-fJl could also act in an autocrine manner to increase invasion by increasing cell motility (Hsu et aL, Cell Growth Differ., 5: 267-275, 1994). Introduction The TGF3- family of growth factors includes three highly homologous isoforms in mammals, TGF-f31, TGF-32, and TGF-f33, whose mature forms exhibit nearly 80% identity. All three isoforms are synthesized as a single-chain pre-pro latent molecule. The C’ terminal region is cleaved to form a I 12- amino acid monomer, which subsequently dimerizes to an active Mr 25,000 form (I). As growth factors, TGF- isoforms are unique because they inhibit the growth of normal epithelial cells. TGF-f3l inhibits the growth of normal intestinal epithelial cells in vivo, where it decreases both villus and crypt cell height and cellularity (2). Although TGF-/31 inhibits the growth of some less aggressive colon carcinoma cell lines in vitro, this growth-inhibitory response is lost with tumor progression. In -20% of cases, TGF-/3 response is lost because of inactivating mutations in the TGF-3 type II signaling receptor (3) or mac- tivating mutations in the TGF- signaling molecules smad4 (4) and smad2 (5). No mutations were found in the other sinad genes in colon cancers (6). Our previous studies have indicated that after loss of a growth-inhibitory response to TGF-l , some malignant epithelial cells use TGF-f31 to stimulate their inva- sion (7). These aggressive colon cancers retain functional TGF-j3 receptors, but TGF- signaling was associated with a new pattern of induction of immediate-early genes (7). Consti- tutive expression of a TGF-f31 antisense construct in these aggressive cells blocked tumor cell invasion and decreased the capacity of these cells to metastasize (8). Supporting these results in an experimental system, a strong correlation was shown in a clinical study between high expression of TGF-l protein in the primary site colorectal cancer and progression to metastases, suggesting that TGF-f3l produced by colon cancer cells promotes their metastasis (9). In the present study, we on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from
Transcript of A Subset of Metastatic Human Colon Cancers Expresses ... · A Subset of Metastatic Human Colon...

Vol. 7. 497-504, June 1998 Cancer Epidemiology, Biomarkers & Prevention 497
3 The abbreviation used is: TGF. transforming growth factor.
A Subset of Metastatic Human Colon Cancers Expresses Elevated
Levels of Transforming Growth Factor �3 11
Antonio Picon, Leslie I. Gold, Jingping Wang,Alfred Cohen, and Eileen Friedman2
Departments of Surgery. Memorial Sloan-Kettering Cancer Center. New York,
New York 10021 IA. P., A. Cl; Department of Pathology, New York
University Medical Center. New York. New York 10016 [L. I. G.l; andDepartment of Pathology, SUNY Health Science Center, Syracuse, New York
13210 IJ.W..E.FI
Abstract
Although transforming growth factor (TGF)431 is apotent growth inhibitor of normal epithelial cellsincluding colonocytes, TGF-fJl has also been implicated
as an enhancer of colon cancer metastasis. DecreasingTGF-�31 protein levels in the metastatic U9 colon cancer
cell line by antisense methodology decreased both U9 cellmetastasis to the liver and s.c. tumor formation in a nudemouse system, and the tumors that did arise hadregained TGF-�31 expression (F. Huang et a!., CellGrowth Differ., 6: 1635-1642, 1995). In addition, in aclinical immunohistochemistry study, colon cancers withelevated TGF-�1 protein levels were found to be 18 timesmore likely to recur as distant metastases than coloncancers expressing low TGF-fil levels, after resection ofthe primary tumor (E. Friedman et aL, CancerEpidemiol. Biomark. Prey., 4: 549-554, 1995). Becauseboth studies implicated TGF-j31 in colon cancermetastasis, we wished to know whether a selection biasfor TGF-�1 was maintained in metastatic cells or was
only a property of the primary site tumors that werelikely to metastasize. TGF-�1 levels were measured usingtwo different antibodies in paired primary site cancersand their metastases by immunohistochemistry and, inselected cases, by Western blot analysis. In 16 of 21 cases(76%) with antibody G and 23 of 31 cases (74%) withantibody P, higher expression of TGF-�1 was found incolon cancer cells invading local lymph nodes comparedwith primary site colon cancer cells, or (2 and 6 cases,respectively) high TGF-�1 expression in the primary sitecancer was maintained in invasive cells. Analysis byWestern blotting using both antibodies also demonstrated
that higher levels of TGF-fil protein were found inmetastases compared with the primary site tumor ornormal tissue. Additional cases of paired primary site
Received 5/20/97: revised I 2/8/97: accepted 3/I 6/98.
The costs of publication of this article were defrayed in part by the payment of
page charges. This article must therefore be hereby marked advertisenvent in
accordance with 18 U.S.C. Section 1734 solely to indicate this fact.� Supported by NCI ROI CA75708 (to E. F.) and National Cancer Institute ROI
CA49507 (to L. I. G..
2 To whom requests for reprints should be addressed, at Department of Pathology,
SUNY Health Science Center at Syracuse. 750 East Adams Street, Syracuse. NY
13210. Phone: (315)464-7148: Fax: (315)464-8419.
colon cancer, local lymph node metastases, and cancer
cells metastasizing to distant sites were examined. In sixof eight such cases (75%), TGF-�1 levels were increasedin both invasive cell populations compared with theprimary site cancer (five cases), or high levels in theprimary site cancer were maintained in the metastaticcells (one case). These data suggest that TGF-fil plays arole in promoting colon cancer metastasis throughout themetastatic process in roughly 75% of cases. TGF-�1 mayincrease metastasis by paracrine mechanisms, such assuppression of local immune response or increasedangiogenesis, as was seen with the U9 cell line. In thosecancers with nonmutated TGF4J receptors and non-mutated smad proteins like U9 cells, TGF-fJl could alsoact in an autocrine manner to increase invasion byincreasing cell motility (Hsu et aL, Cell Growth Differ., 5:267-275, 1994).
Introduction
The TGF3-� family of growth factors includes three highlyhomologous isoforms in mammals, TGF-f31, TGF-�32, andTGF-f33, whose mature forms exhibit nearly 80% identity. Allthree isoforms are synthesized as a single-chain pre-pro latentmolecule. The C’ terminal region is cleaved to form a I 12-amino acid monomer, which subsequently dimerizes to an
active Mr 25,000 form (I). As growth factors, TGF-� isoformsare unique because they inhibit the growth of normal epithelial
cells. TGF-f3l inhibits the growth of normal intestinal epithelialcells in vivo, where it decreases both villus and crypt cell height
and cellularity (2). Although TGF-/31 inhibits the growth ofsome less aggressive colon carcinoma cell lines in vitro, thisgrowth-inhibitory response is lost with tumor progression. In-20% of cases, TGF-/3 response is lost because of inactivating
mutations in the TGF-�3 type II signaling receptor (3) or mac-tivating mutations in the TGF-� signaling molecules smad4 (4)
and smad2 (5). No mutations were found in the other sinad
genes in colon cancers (6). Our previous studies have indicated
that after loss of a growth-inhibitory response to TGF-�l , somemalignant epithelial cells use TGF-f31 to stimulate their inva-sion (7). These aggressive colon cancers retain functional
TGF-j3 receptors, but TGF-� signaling was associated with anew pattern of induction of immediate-early genes (7). Consti-
tutive expression of a TGF-f31 antisense construct in theseaggressive cells blocked tumor cell invasion and decreased thecapacity of these cells to metastasize (8). Supporting theseresults in an experimental system, a strong correlation wasshown in a clinical study between high expression of TGF-�lprotein in the primary site colorectal cancer and progression tometastases, suggesting that TGF-f3l produced by colon cancercells promotes their metastasis (9). In the present study, we
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

498 Elevated TGF.�J1 Expression in Meta.static Colon Cancers
have asked whether a selection bias for TGF-�1 was main-tamed in metastatic cells or whether it was a property only ofthe primary site tumor.
Materials and Methods
Materials. ‘ 2�I-Labeled protein A was obtained from DuPont-New England Nuclear, polyvinylidene difluoride transfer paper
lmmobulin-P from Millipore, and the Vectastain Elite ABC kitfrom Vector Laboratories (Burlingame, CA). For antisera G,rabbit polyclonal antisera to TGF-�l was developed by immu-
nization with peptides representing amino acid residues 4-19of the mature processed forms of TGF-�l . The specificity of
this antibody was established by immunoblotting intact nativeand recombinant human TGF-fJl and by blocking immunore-activity with the peptide used as immunogen (10). This antiseradid not show cross-reactivity with TGF-�2 or TGF-�3 isoformsby Western blot analysis using recombinant TGF-�3 and por-cine TGF-f32 (10). Antisera P (Promega Corp.) was raised inrabbits against acid-activated TGF-f3l (I 1) from platelets. This
antisera showed no cross-reactivity with recombinant TGF-f32and TGF-J33 by immunoblotting. All other reagents were pur-
chased from Sigma Chemical Co.
Cell Culture. U4 human colon carcinoma cells were main-tamed in 7% fetal bovine serum supplemented with DMEM.
Western Blotting. Tissue specimens were homogenized using
a Dounce homogenizer in 1 .0 ml of RIPA buffer [137 m�i NaC1,20 m�i Tris-HC1 (pH 8.0), 10% glycerol, 1% NP4O, 0.1% SDS,
and 0. 1% sodium deoxycholate] containing 3 msi EDTA, I mt�iphenylmethylsulfonyl fluoride, 20 ,LM leupeptin, 5 mr�i NaVO4,and 0. 15 unitlml aprotinin. Extracts were adjusted to equalprotein concentrations in SDS-sample buffer, heated for 5 mmat 100#{176}C,then electrophoresed in 15% acrylamide-SDS gels.Proteins separated in the gel were transferred by electrophoresisto a polyvinylindene difluoride membrane exactly as detailed(12). Proteins were detected using either 2 �g/ml of antisera P
or 0.5 p�g/ml antisera G, followed by ‘251-labeled protein A andautoradiography. For U4 cell line studies, lysates were preparedidentically. Fifty �g of cell lysate in SDS-sample buffer were
heated for 5 mm at 100#{176}C,then electrophoresed in 15% acryl-
amide-SDS gels. Western blotting was as above. Densitometricscanning was performed for quantitation.
Tissues. Colon cancer tissue from the periphery of the tumor,normal colon mucosa dissected free of the muscle layer, livermetastases from the edge of the tumor, and fragments of normalliver were obtained at surgery and immediately frozen in liquid
N,. Liver metastases were obtained from patients with synchro-nous or metachronous lesions. Patients were admitted for elec-tive or emergency resection of colorectal cancer. For immuno-
cytochemistry, sections from resected colon cancers wereobtained from the Memorial Hospital pathology archives. All
sections had been fixed in buffered formalin and stored inparaffin blocks. Patients’ slides were number coded, reactedwith the TGF-f3l isoform-specific antisera, processed for im-munocytochemistry, scored by three independent observers(see sections below), and then uncoded. The entrance criteriafor each patient were then reviewed by a Surgery Departmentdata manager for accuracy.
Immunocytochemistry. For antisera G, number-coded tissuesections were deparaffinized in xylene, rehydrated in TBS,incubated with 1 mg/ml hyaluronidase in 0. 1 M sodium acetate
buffer, blocked with normal goat serum, and incubated with theprimary antibody at 2.5 �g/ml in blocking solution for 16 h at4#{176}C,as detailed (9). Following the use of reagents of the
Vectastain Elite ABC kit, the antibody reaction was detectedwith diaminobendizine. Slides were reacted with each antiseraat 4#{176}Covernight in one lot using sections of the human coloncarcinoma U4H cell line grown as a s.c. tumor in a nude mouse
as the positive control and normal rabbit serum as the negativecontrol. For antisera P. anti-human TGF-f3l polyclonal antiserawas purchased from Promega and used at 13 �g/ml at 4#{176}Covernight. Sections were incubated with 0. 1% Pronase E (Sig-
ma) for 8 mm at room temperature before application of anti-sera. The degree of intensity of immunostaining was detected as
above.
Scoring. Scoring was performed independently by three ob-servers on number-coded slides on a scale of 1-4 using sections
of the human colon carcinoma U4H cell line grown as a s.c.tumor in a nude mouse as the positive control at 1 . Data wereobtained by chart review, and patient data were verified by aSurgery Department data manager after the scoring of the slideswas complete.
Results
Two Antibodies to TGF-�31 Identify Different TGF-g31Species in Colon Carcinoma Cells by Western Blotting.TGF-�l had been implicated as an enhancer of colon cancermetastasis in two ways: (a) decreasing expression of TGF-j31
protein levels in metastatic U9 colon cancer cells by an anti-sense expression plasmid decreased liver metastasis and s.c.tumor formation in a nude mouse system, and tumors that didarise had regained TGF-j31 expression (8); and (b) in a series ofcolorectal cancer specimens from patients whose disease recur-rence or lack of recurrence had been documented, a strong
correlation was shown between high expression of TGF-�31protein in the primary site colorectal cancer and progression to
metastases, suggesting TGF-j3l produced by colon cancer cellspromotes their metastasis (9). In the present study, we haveasked whether a selection bias for TGF-31 was maintained in
metastatic cells. The level of TGF-�3l protein in metastatic
human colon cancer cells and their originating primary sitecancer were compared by both Western blotting and immuno-
cytochemistry.Two TGF-f31 antibodies were used for this study. Anti-
body P was raised against the entire molecule of acid-activatednatural TGF-131 and therefore would be expected to recognize
additional epitopes to those detected by an anti-peptide anti-
body such as antibody 0. Treatment of U4 colon carcinoma
cells with a differentiating agent such as sodium butyrate hasbeen shown to increase TGF-f31 mRNA and active peptidelevels (13). Treatment of U4 cells with 0.5-10 mM sodium
butyrate for 24 h resulted in an increase in the abundance of theMr 25,000 TGFfJ1 dimer, the biologically active form (Fig.1A). No other TGF-(31 species were identified. Similar datawere seen when U4 cells were treated with other TGF-�l -
inducing agents, sodium propionate and sodium isovalerate(data not shown). Nonnecrotic portions of five primary site
colon cancers were resected by one of us within a 3-weekperiod, were frozen in the operating room (see “Materials andMethods”), and were then used for immunoblotting for TGF-f31
species in human colon tumors. In marked contrast to the cellline studies, antibody P detected a Mr 1 10,000 protein complexin each of the five colon cancer lysates (Fig. 1B, 1 10 kDacomplex seen in lysate #1 with longer exposure, data notshown) and a low abundance of the monomeric Mr 12,500
TGF-f31 chain in tumor 4. The Mr 25,000 form was not ob-served. A Mr 95,000� 10,000 complex immunoreactive withTGF-/3l antisera has been detected in cell lysates by others in
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

25 kDaTGFB1dimer->
25 kDaTGFB1 dimer
Cancer Epidemiology, Biomarkers & Prevention 499
A. Induction of TGFBI in U4 Colon CarcinomaLine with Sodium Butyrate
0 0.1 0.5 1 3 5 10mM..�
9’
... . . 25kDa
- . TGFO1� � �Nm� � � � <- dimer
D. Antibody G Detection of TGFB1 Dimers
In 5 Human Colon Carcinomas
M 1 2 3 4 5
B. Antibody P Detection of TGFBI Complexesin 5 Human Colon Carcinomas
1 2 3 4 5 2freeze-thaw12.5kDa->-1IOkDaTGFOI TGFB1 �monomer
.55 kDa latentproTGFB1
E. Antibody G Detection of TGFBI Dimersin Colon carcinoma Metastases
C. TGFB1 Complexes in Colon CarcinomaMetastases Detected by Antibody P
-12.5kDa TGFB1 15M 15L 18M 181 18T 18NTGFB1 dimer-> _____________________________ -
monomer -..�
-110 kDa TGFO1Complex
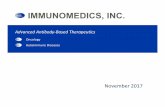
Fig. I. Characterization of TGF-fJl species in colon carcinomas identified by antibodies P (A-C) and G (D and E) by Westem blotting under nonreducing conditions.
A. increasing abundance of TGF-j3l M, 25,000 dimer induced by 24-h treatment of U4 human colon carcinoma cells with a range of concentrations from 0. I to 10 msi
of the differentiation agent sodium butyrate. Dashes on right, molecular weight markers of Mr 18,000 and M, 29,000 (in thousands). B, detection of TGF-�3l species in
colon cancer lysates using antibody P. One hundred fifty jzg of protein were analyzed per lane from specimens of five resected colon carcinomas, Lam’s 1-5, fresh-frozen
in liquid nitrogen in the operating room. The M, I 10,000 TGF-f31 complex is detected in all lysates, with lysate I requiring more exposure of the autoradiogram (data not
shown). Lysate 2 was rerun after freeze-thawing disrupted most of the M, I 10,000 TGF-)31 complex into constituent mature M, 25,000 TGF-f31 dimer and the latent
proTGF-f3l of Mr 55.000 (rigltunost lane). C, elevated abundance of Mr I 10,000 TGF�3l complex in liver metastases. Samples of normal liver (L). primary site cancer
(1), and liver metastases (M), fresh-frozen in liquid nitrogen immediately after surgery. are shown. Dashes on left, molecular weight markers of M, 68.000 and M� 97,000.D. mature TGF-�I dimer of M, 25,000 detected by antibody G in the same five samples of human colon cancers analyzed in B. Reduced recombinant single-chain TGF-�l
of M, 12,500 was run in the molecular weight marker Lane M. E. elevated abundance of TGF-�l M, 25,000 dimer in colon cancer meta.stases detected by antibody G.Samples of normal liver (L), primary site cancer (7). liver metastases (M). and normal colon mucosa (N) fresh-frozen in liquid nitrogen immediately after surgery are shown.
These are identical samples to those analyzed in C with antibody P.
earlier studies (1 1, 14) and found to contain mature TGF-�lcovalently linked by disulfide bonds to Mr 55,000 unprocessedpro-TGF-j31 and to the associated protein portion of the pre-cursor. To determine whether the large molecular weight corn-
plexes detected by antisera P contained known TGF-f31 species,lysate from carcinoma 2 was freeze-thawed and reanalyzed by
SDS-PAGE and Western blotting. Freeze-thawing released theMr 25,000 TGF-�l dimer and the Mr 55,000 unprocessedpro-TGF-�l from the Mr 1 10,000 complex (Fig. 1A, right, Lane
2R). We next assayed TGF-/31 levels in two cases of pairedmetastases and normal tissue (Fig. 1 C). In case I 8, an increasein TGF-�l levels was seen in liver metastases when comparedwith the primary site tumor or paired normal mucosa. In case15, an increase in TGF-f3l levels was seen in liver metastaseswhen compared with uninvolved liver. In both cases, the only
TGF-pl species identified by antibody P was the Mr 1 10,000TGF-f31 complex. Therefore, although antibody P could detect
the Mr 25,000 dirner form in established colon cancer cell lines,
the major TGF-/31 species it detected in human colon cancersresected from patients was a larger complex.
Antibody G was raised to a synthetic peptide correspond-
ing to residues 4-19 of mature TGF-�l . Antibody G has beenused extensively by several groups to quantitate TGF-/31 ex-pression within various tumor types and in mammalian devel-opment (15-18). This is an isotype-specific antibody that does
not cross-react with TGF-�32 or TGF-�33 and the reactivity ofwhich is blocked by the synthetic peptide used as immunogen
(10).Antibody G recognized both the monomeric Mr I 2,500
chain of recombinant TGF-�l used as a marker and the Mr
25,000 dirner form of mature TGF-(31 (Fig. ID) within each of
the five human colon cancer lysates blotted previously withantibody P (Fig. IB). No Mr I 10,000 TGF�l complex wasdetected by antibody G. The same two paired cases of colon
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

.-
a � ‘�‘ , .‘�
��S#{188}
.::�:��a � � : �.s�’�’
�, � t�\�:�i*.:.,.:
s.,,- ..
,�--
. P1
.,_4
“i.; ‘... I:�#{163}P� � -�-L-�1.
;� �
5(X) Elevated TGF43I Expression in Metastatic Colon Cancers
. . .-.s�., . .
: . .� � � � .:L. �
.. ,. .
S � �
�4mi
#.
�
.‘� �e._�p.u�i :���!ft; � �T-��’ �
� ‘3:�� “� �;�4;.
� �
��z;C � ‘P�� �
. C-’,,
. ‘W�j �
.�,
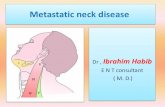
Fig. 2. Detection of TGF-f3l in sectioned colon carcinomacells by immunocytochemistry using antisera G. Upper panel
left, P4: primary colon cancer B. Upper pastel right. P4 met:
concurrent liver metastases from primary colon cancer P4.Losserpanel left, P1: primary colon. L�overpanel right, P1 LN:
regional lymph node resected concurrently with primary colon
cancer P1. Arrow, colon cancer cells arising around a vesselwithin the lymph node. X 109. No sections were counterstained:
therefore, the specimens in the negative control slides are not
shown (they did not develop any benzidine stain: no cellular
morphology could be seen).
cancer metastases and normal tissues tested previously with
antibody P (Fig. 1C) were then assayed by Western blottingwith antibody G (Fig. 1E). In both cases, the only TGF-�l
species identified by antibody G was the Mr 25,000 TGF�1
complex. In case 18, an increase in TGF-�3l protein levels wasseen in liver metastases when compared with the primary sitetumor, normal uninvolved liver, or paired normal mucosa. Incase 15, an increase in TGF-�l levels was seen in liver me-tastases when compared with uninvolved liver. Thus, colon
cancers with elevated expression of TGF-�l Mr 25,000 dimerdetected by antibody G also exhibited elevated expression ofthe Mr 1 10,000 TGF�l complex detected by antibody P. Both
antibodies gave the same results: enhanced levels of TGF-�1protein within metastases of tumors 15 and 18 compared withnormal tissues, and in case 18, the primary site tumor (Fig. 1,compare C and E). In addition, tumor 4, a mucinous tumor,exhibited the greatest abundance of TGF-� 1 species of the five
human primary site cancers compared by both antibodies (Fig.1. compare B and D). This result is consistent with a recentstudy ( 19) in which a mucinous colon cancer exhibited a
TGF-�3l mRNA level higher than colon cancers of other dif-
ferentiation classes. In addition, this study demonstrated that
high levels of TGF-f31 mRNA levels in colon cancers corre-
lated with disease progression (19).
Elevated Levels of TGF-�31 Were Found in Colon Cancer
Cells Invasive to Regional Lymph Nodes and to DistantMetastatic Sites in a Subset of Colon Cancers. These two
antibodies gave us a novel opportunity to compare expres-
sion of both TGF-�3l species, the Mr 25,000 biologically
active dimer and the Mr 1 10,000 complex, by immunocyto-chemistry in a series of fixed colon tumors. We first needed
to confirm that quantitation of TGF-/31 abundance in colon
cancer tissues by immunocytochemistry was valid. In par-
allel to the samples of tumors 1-5 used for immunoblotting
in Fig. 1, other samples were fixed by routine methods for
immunocytochemistry. TGF-f31 protein levels within each
tumor were then determined using both antibodies using
sections of the human colon carcinoma cell line U4H, which
has a known high level of expression of TGF-j31 protein
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

4.
3
2
I
A
UC
VC
.04
IL0I-
B
1 2 3 4 5 6 7 8
Colon Cancer Cases
0 prImary U node #{149}metastases
�, . - - .
0 5 10 15 20 25
Colon Cancer Cases
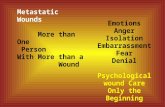
Fig. 4. TGF-)31 abundance assayed by immunocytochemistry with antisera P ineight cases of number-coded paired primary site colon cancers. regional lymph
4 nodes, and distant metastases.
their corresponding regional lymph nodes. All sections were
3 number-coded and scored by three reviewers without the
knowledge of the case number. Primary site cancer and nodeswere scored independently. A range from + to + + + + was
observed within each primary site colon cancer, whereas lymph
2 nodes scored from + + to + + + + compared with the U4Htumor positive control. With antibody G, the protein level ofTGF-f31 was higher in the cancer cells in the local lymph nodes
primary than in the primary site cancer in the same patient in 14 cases
I node (Fig. 3A). For example, colon cancer cells with high levels ofTGF-j3l were evident surrounding vessels within the regional
lymph nodes resected with tumor P1 (Fig. 2, arross’, lower right
panel tumor #1 LN). These invasive colon cancer cells exhib-0 ‘ ‘ . , . , . ‘ ited more TGF-/3l protein than the primary site colon cancer I
0 1 0 2 0 3 0 4 0 (Fig. 2, compare two lower panels). Only in four cases (19%)
was there a decrease in TGF-f31 levels in the cancer cells in the
Colon Cancer Cases lymph nodes compared with the primary site cancer. Our orig-inal observation (9) was that high levels of TGF-�l in a
Fig. 3. TGF-f3I abundance assayed by immunocytochemistry in number-ceded p�’�mary site colon cancer made the tumor more likely to recurpaired nodes and primary site colon cancers, 21 cases with antisera G (A) and 31 as distant metastases. High levels of TGF-�l, as judged bypaired cases with antisera P (B). immunocytochemistry compared with a positive control xeno-
graph known to synthesize TGF-�3l, were +31+4. In the cur-
rent study, two of the cases exhibited +3 or +4 TGF-j’31 levels(13), as the positive control and normal rabbit serum as the in both primary site and local lymph nodes (Fig. 3A). Thus in
negative control. Antibody binding was detected by the these two tumors, high levels of TGF-j31 in the primary werediaminobenzidine reaction without counterstaining; thus, the maintained in the metastatic cells. Therefore, in 16 of 21 cases
intensity of the color reflects the antibody binding and thus (76%), either increased TGF-/3l protein levels were found inthe abundance of TGF-/31 . Tumor 4, which had displayed the the invasive cells or high levels in the primary site cancer cells
highest level of TGF-�3l protein by Western blotting, also were maintained in the cells invading the local lymph nodes.exhibited the highest levels of TGF-/3l by immunohisto- The immunohistochemical survey was then repeated usingchemistry of the five cancers, clearly higher than tumor 1 antibody P on the same 21 cases shown in Fig. 3A and an(Fig. 2, antibody G sections shown; similar data for antibody additional 10 cases. Antisera P gave identical results to antiseraP). Because there was a correlation between the results G in the majority of cases (85%), when the results from both
obtained by Western blotting and those from immunohisto- antisera were uncoded and compared (data not shown). In 17
chemistry, quantitation of the level of TGF-f31 protein in cases, TGF-f3l protein expression was higher in the cancer cellscolon cancer specimens could be obtained by immunohisto- in the local lymph nodes than in the primary site cancer from
chemical methods. the same patient (Fig. 3B). In six cases, high levels of TGF-f3lTGF-/3l levels were measured by immunocytochemistry (+31+4) found in the original tumor were maintained in the
as above in a coded series of primary site colon carcinomas and lymph nodes. Only in five cases ( I 6%) did the invasive cancer
U
C
.DC
.0
4
U-0I-.
U
U
U.
0 prImary
. node
UC
VC
.04
IL0I-
Cancer Epidemiology, Biomarkers & Prevention 50/
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

P16 P16m#{149}t
.. .-
502 Elevated TGF.fiI Expression in Metastatic Colon Cancers
P16LN
.\
�-1’, . r , ‘ . .
: � -# I �
� :4 � *4Fig. 5. Detection of TGF-f31 in sectioned colon carcinoma cells by immunocytochemistry using antisera G. Left panel. P16: primary site colon cancer 16. Middle panel.
P16/N: regional lymph node from primary site colon cancer 6. with arrow indicating the cancer cells that bind the anttsera more avidly: Right panel. Pl#{243}mei: synchronousliver metastases arising from primary site colon cancer 16. with arrow indicating the cancer cells. This metastatic foci, like the cancer cells invading the lymph node. is
readily detected because of its higher expression of TGF-(31 compared with the normal cells in the surrounding tissue. X 109.
cells in the lymph nodes exhibit less TGF-�l than the primarysite cancer. Thus, in 23 of 31 cases (74%), the data supportedthe interpretation that elevated levels of TGF-� 1 were a selec-
tion criteria for metastatic colon cancer cells.We next determined whether the elevated expression of
TGF-�l protein found in many colon cancer cells invasive tolocal lymph nodes would he maintained when these cells dis-
seminated to distant metastatic sites. It was difficult to obtain
many cases for this study because the original resection tendedto be performed at a local hospital, whereas the metastases wereremoved at Memorial Hospital, a regional cancer center. Eightcases of paired primary site, local lymph nodes, and distant
metastases were examined for TGF-�l expression by immu-nocytochemistry (Fig. 4). In five cases (63%), the abundance ofTGF-�l protein was higher in lymph nodes than in the primarysite colon cancer. and this elevated level was maintained orincreased in distant metastases. For example in case P16, thecolon carcinoma cells within the lymph node (Fig. 5, PI6LN,
center) and within the liver could be clearly detected by theirabundant quantities of TGF-�l protein compared with thesurrounding tissues (Fig. 5, PlOmet, right: arross’s point to theinvading cancer cells detected with antisera G). In one case, the
primary site cancer exhibited high levels of TGF-�l, and this
high level was maintained in the cells invading the lymph nodesand those metastatic cells reaching distant sites. An example ofthe latter is colon cancer case 4, with synchronous liver me-tastases. The primary site cancer exhibited high levels of TGF-�l, and this high level was maintained in the metastases, asshown by immunohistochemistry (Fig. 2, compare upper pan-
els). Thus, the results of immunocytochemistry (Fig. 4) andWestern blotting gave similar results, elevated levels ofTGF-f3l protein within invasive and metastatic cells.
Discussion
In a prior study, we examined the expression of TGF-�l,TGF-�2, and TGF-f33 isoforms using immunocytochemistry in
a series of colorectal cancer specimens from patients whosedisease recurrence or lack of recurrence had been documented
(9). A strong correlation was shown between high expression of
TGF-f3l protein in the primary site colorectal cancer and pro-
gression to metastases, suggesting that TGF-f31 produced by
colon cancer cells promotes their metastasis (9). TGF-�3l alsowas found to be an independent prognostic marker for shorterpostoperative survival in a second study by another group of
investigators (20), confirming our observations. These studiessuggested that one selection criteria for invasive colon cancer
cells was their level of TGF-�l. In the current study, TGF-f3llevels were measured by immunocytochemistry in a number-
coded series of primary site colon carcinomas and their corre-sponding regional lymph nodes, and where possible, in metas-tases from the same patient. In roughly 75% ofcases, metastatic
cells either in local lymph nodes or at distant sites exhibited
elevated levels of TGF-J31 compared with the primary site
cancer, or in a few cases where the primary site cancer itself
exhibited high levels ofTGF-�3l, this high level was maintainedin the metastatic cells.
Three hypotheses, not mutually exclusive, may explain the
presence of high levels of TGF-�l within invasive colon
cancers:(a) We propose that high levels ofTGF-�3l within a colon
cancer may increase the likelihood of metastases by locallysuppressing immune function. In syngeneic mice with an intact
immune system, Meth A sarcoma cells overexpressing TGF-j31were more tumorigenic than transfectants expressing lower
levels of TGF-�l (21). Because Meth A sarcoma cell growthwas strongly inhibited by TGF-/3 in vitro in an autocrine man-
ner, tumorigenicity in viva may be enhanced by TGF-�31
through host immunosuppressive activities. Thus, the presenceofhigh levels ofTGF-�3l in cells that were proliferating to form
enlarging, invasive, and finally metastatic tumors in vivo is
inconsistent with the growth inhibition function of TGF-�l in
vitro. TGF-�3l generally functions as an immunosuppressive
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

Cancer Epidemiology, Biomarkers & Prevention 503
agent by affecting the function of various target immune cells.This includes inhibiting B-cell, thymocyte, T-lymphocyte, andlarge granular lymphocyte proliferation and inhibiting the gen-eration of CTLs and natural killer cells (22). In this way,increased expression and release ofTGF-�1 from a primary siteor metastatic colon cancer cell could impair a patient’s local
immune response, thereby promoting tumor growth.(b) A second hypothesis is that TGF-�l may have a
biphasic effect on tumor growth, becoming growth promotingat later stages in progression. Although TGF-�l was shown to
inhibit benign tumor formation, TGF-j31 enhanced progressionof skin tumors to invasive spindle carcinomas in carcinogen-
treated transgenic mice with keratinocyte-targeted expressionof TGF-f31 (23). TGF-f3l appeared to have a biphasic action
during colon tumor progression, acting on well-differentiatedcancers as a tumor suppressor and growth inhibitor, but at laterstages in tumor progression acting to enhance malignancy.TGF-�l is a growth inhibitor for normal epithelial cells and
certain highly differentiated colon cancers in vitro. However,
upon progression of colon cancer to more invasive phenotypes,colon cancer cells become autocrine growth stimulated byTGF-f31 , possibly because they use a different TGF-j3l signal
transduction pathway. Resected poorly differentiated colon
cancers and resected metastatic colon cancers in primary cul-ture were stimulated to proliferate by TGF-f31 and by hexam-
ethylene bisacetamide, which induced TGF-f3l . This increasein tumor growth was measured by cumulative [3H]thymidineincorporation and by direct cell counting (24, 25). These dataobtained from primary cultures of resected cancers were similarto those obtained from HT29 colon carcinoma sublines. Colon
carcinoma cell lines that respond to exogenous TGF-�l bygrowth stimulation are highly invasive in vitro and are highly
tumorigenic in athymic mice (7). These cells also synthesizeTGF-�l mRNA and secrete TGF-�l as a bioactive dimer.Neutralizing antibody to TGF-�3l and constitutive expression ofa TGF-j3l antisense construct blocked both cell growth and
invasion in vitro and growth in athymic mice, thereby demon-
strating the autocrine stimulating activity of TGF-�3l in highlyaggressive colon cancer cells (7, 26). Thus, elevated levels of
TGF-/31 may provide a selective advantage for aggressivecolon cancer cells by directly stimulating their growth andinvasiveness.
(c) A third function for elevated levels of TGF-f31 in colon
tumor cells is to increase the expression of PDGF-B chain ininvasive, undifferentiated colon carcinoma cells but not in
differentiated cells (27). There is evidence linking the produc-tion of PDGF-B in human colon cancers with increased angio-
genic potential. The PDGF-j3 receptor was found in microvas-cular pericytes, not in the epithelial cells, in each of a series of210 colorectal cancers by immunohistochemistry (28, 29). Co-
lon cancer cells that produce PDGF-B in response to TGF-�3lcould stimulate the growth or function of microvascular pen-cytes expressing PDGF-j3 receptors, leading to an increase intumor vascularization.
Evidence has accumulated that many carcinomas respondto TGF-f3l with disease progression. Examples are numerous.Increased expression of TGF-�l and to a lesser extent TGF-j32and TGF-f33 correlated with disease progression to complex
hyperplasia and adenocarcinoma of the endometrium (16). In-creased mRNA and protein expression of TGF-� isoforms inpancreatic cancer correlated with decreased survival (18). In-creased levels of TGF-�3l protein in breast carcinomas was
positively correlated with disease progression (17). Intenseimmunoreactivity for TGF-�l, not TGF-�2 or TGF-�3, in
tumor cells was statistically significant (P = 0.009) for recur-
rence or progression in breast cancer, independent of age, stage,nodal status, or estrogen receptor status ( I 7). The metastatic
potential of mammary adenocarcinoma cells was increased byin vitro treatment with TGF-f31 before injection into syngeneicrats. TGF-j31 pretreatment increased the number of metastases
at the surface of the lung 2-3-fold and increased in vitro
invasion 2-3-fold by increasing type IV collagenase andheparanase activities (30). In other studies, breast cancer cells
that overexpressed TGF-�l exhibited estrogen-independent tu-morigenicity in athymic mice (3 1). Moreover, elevated levels of
TGF-/31 protein have been found in prostate cancer (32).TGF-f3l has been shown to be a marker for malignancy in
astrocytomas because normal astrocytes do not express thisisoform (15). Thus, TGF-�l has been associated with increased
tumor progression in several human cancers in addition to coloncancer. Because elevated levels of TGF-f31 correlate with ag-gressive and metastatic behavior of tumor cells in a variety ofcancers, TGF-�l may also be considered a prognostic markerof malignant progression.
References
I . Kingsley. D. The TGF� superfamily: new members, new receptors. and new
genetic tests of function in different organisms. Genes Dcv., 8: 133-146. 1994.
2. Migdalska. A.. Molineux, G., Demuynck, H.. Evans. G., Ruscetti, F., and
Dexter, T. Growth inhibitory effects of TGF/31 in visa. Growth Factors, 4:
239-245. 1991.
3. Markowitz, S., Wang. J.. Myeroff. L.. Parsons. R., Sun, L., Lutterbaugh. J..
Fan, R.. Zborowska, E., Kinzler, K., Vogelstein, B.. Brattain. M.. and WilIson.J. Inactivation of the type II TGF� receptor in colon cancer cells with microsat-
ellite instability. Science (Washington DC). 268: 1336-1338. 1995.
4. Hahn, S., Schutte, M., Hoque, A. T. M. S., Moskaluk. C.. da Costa, L.,
Rozenblum, E., Weinstein, C., Fischer, A., Yeo, C., Hruban, R. H.. and Kem. S.
DPC4. a candidate tumor suppressor gene at human chromosome I 8qa2 I .I.
Science (Washington DC). 271: 350-353. 1996.
5. Riggins, G., Thagalingam. S., Rozenblum. E.. Weinstein, C., Kem. S.,
Hamilton, S., Willson, J., Markowitz, S., Kinzler, K., and Vogelstein. B. Mad-
related genes in the human. Nat. Genet., /3: 347-349, 1996.
6. Riggins, G., Kinzler, K.. Vogelstein. B.. and Thagalingam. S. Frequency of
Smad gene mutations in human cancers. Cancer Res.. 57: 2578-2580. 1997.
7. Hsu, S., Huang. F., Hafez. M., Winawer, S.. and Friedman. F. Colon carci-
noma cells switch their response to TGF�I with tumor progression. Cell Growth
Differ.. 5: 267-275. 1994.
8. Huang, F., Newman, E.. Kerbel, R.. and Friedman, E. TGF�I is an autocnnepositive regulator of colon carcinoma U9 cells in visa as shown by transfection
of a TGFI3I antisense expression plasmid. Cell Growth Differ., 6: 1635-1642,
I995.
9. Friedman, E.. Gold. L.. Klimstra, D.. Zeng. Z.. Winawer. S.. and Cohen. A.
High levels ofTGF�l correlate with disease progression in human colon cancer.
Cancer Epidemiol. Biomark. Prey.. 4: 549-554. 1995.
10. Pelton, R., Saxena, B., Jones, M.. Moses, H.. and Gold. L. Immunohisto-
chemical localization of TGFj3I. TGFI32 and TGFI33 in the mouse embryo:
expression patterns suggest multiple roles during embryonic development. J. Cell
Biol., 1/5: 1091-1105. 1991.
II. Purchio, A., Cooper. J.. Brunner. A., Lioubin. M., Gentry. L.. Kovacina, K.,Roth, R., and Marquardt, H. Identification of mannose-6-phosphate in two
asparagine-linked sugar groups of recombinant TGFI3 precursor. J. Biol. Chem..
263: 14211-14215. 1988.
12. Yan, Z., Hsu. S., Winawer, S.. and Friedman, E. TGF�I inhibits retinoblas-
toma gene expression but not pRB phosphorylation in TGF�l-growth-stimulated
colon carcinoma cells. Oncogene. 7: 801-805. 1992.
13. Hafez. M., Hsu, S., Yan. Z., Winawer, S., and Friedman, E. Two roles for
TGFI3I in colon enterocytic differentiation. Cell Growth Differ.. 3: 753-762.
I992.
14. Gentry, L., Lioubin. M., Purchio, A.. and Marquardt, H. Molecular events in
the processing of recombinant type I pre-pro-transforming growth factor �3 to the
mature polypeptide. Mol. Cell. Biol., 8: 4162-4168. 1988.
15. Jennings, M. T., Kaariainen, I. T., Gold, L., Maciunas. R. J., and Commers,
P. A. TFG beta I and TGF beta 2 are potential growth regulators for medullo-
blastomas, primitive neuroectodermal tumors. and ependymomas: evidence in
support of an autocrine hypothesis. Hum. Pathol., 25: 464-475. 1994.
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

504 Elevated TGF.fil Expression in Metastatic Colon Cancers
16. Gold. L., Saxena. B.. Mittalk. K.. Marmor, M., Goswami, S., Nactigal, L.,
Korc, M., and Demopoulos. R. Increased expression of transforming growth
factor �3 isoforms and basic fibroblast growth factor in complex hyperplasia and
adenocarcinoma of the endometrium: evidence for paracrine and autocrine action.
Cancer Res., 54: 2347-2358, 1994.
17. Gorsch. S., Memoli. V., Stukel, T., Gold, L., and Arrick, B. Inununohisto-
chemical staining for transforming growth factor 131 associates with disease
progression in human breast cancer. Cancer Res., 52: 6949-6952, 1992.
18. Freiss, H., Yamanaka, Y., Buehler, M., Ebert, M., Berger, H., Gold, L., andKorc, M. Enhanced expression of TGFf3 isoforms in pancreatic cancer correlates
with decreased survival. Gastroenterology. /05: 1846-1856, 1994.
19. Tsushima, H., Kawata, S., Tamura, S., Ito, N., Shirai, Y., Kiso, S., Imai, Y.,
Shimomukai, H., Normura, Y., Matsuda, Y., and Matsuzama, Y. High level of
TGF�I in patients with colorectal cancer: association with disease progression.
Gastroenterology. I 10: 375-382, 1996.
20. Robson, H., Anderson, E., James, R., and Schofield, P. TGFf31 expression in
human colorectal tumours: an independent prognostic marker in a subgroup of
poor prognosis patients. Br. J. Cancer. 74: 753-758. 1996.
21. Chang. H-L., Gillett, N., Figari, 1., Lopez. A., Palladino. M., and Derynck, R.
Increased transforming growth factor �3 expression inhibits cell proliferation inritro, yet increases tumorigenicity and tumor growth of Meth A sarcoma cells.
Cancer Res., 53: 4391-4398, 1993.
22. Ruscetti, F., and Palladino, M. TGFI3 and the immune system. Growth Factor
Res., 3: 159-175, 1991.
23. Cui, W., Fowlis, D., Bryson, S.. Duffie, E., Ireland, H., Balmain, A., and
Akhurst, R. TGFf3I inhibits the formation of benign skin tumors, but enhances
progression to invasive spindle carcinomas in transgenic mice. Cell, 86: 531-542,
I996.
24. Schroy, P., Carnright, K., Winawer, S., and Friedman, E. Heterogeneous
responses of human colon carcinomas to hexmethylene bisacetamide. Cancer
Res., 48: 5487-5484, 1988.
25. Schroy, P., Rifkin, J., Coffey, R., Winawer, S., and Friedman, E. Role of
TGFI3I in induction of colon carcinoma differentiation by hexamethylene bisac-
etamide. Cancer Res., 50: 261-265, 1990.
26. Huang, F., Hsu, S., Yan, Z., Winawer, S., and Friedman, E. The capacity for
growth stimulation by TGF�31 seen only in advanced colon cancers cannot beascribed to mutations in APC, DCC, p53 or ras. Oncogene, 9: 3701-3706, 1994.
27. Hsu, S., Huang, F., and Friedman, E. Paracrine PDGF-B increases colon
cancer growth in viva. J. Cell Physiol., 165: 239-245, 1995.
28. Lindmark, G., Sundberg, C., Glimelius, B., Pahlman, L., Rubin, K., and
Gerdin, B. Stromal expression of PDGFf3-receptor and PDGF B-chain in cob-
rectal cancer. Lab. Invest., 69: 682-689, 1993.
29. Sundberg, C., Ljungstrom. M., Lindmark, G., Gerdin, B., and Rubin, K.Microvascular pericytes express PDGFf3-receptors in human healing wounds and
colorectal adenocarcinoma. Am. J. Pathol., /43: 1377-1388, 1993.
30. Welch, D., Fabra, A., and Nakajima, M. TGF(3 stimulates mammary adeno-
carcinoma cell invasion and metastatic potential. Proc. Natl. Acad. Sci. USA, 87:
7678-7682, 1990.
31. Arteaga, C., Carty-Dugger, T., Moses, H., Hurd, S., and Pietenpol, J. TGF�I
can induce estrogen-independent tumorigenicity of human breast cancer cells in
athymic mice. Cell Growth Differ.. 4: 193-201, 1993.
32. Truong, L., Kadmon, D., McCune, B., Flanders, K., Scardino, P., and
Thompson, T. Association ofTGFj3l with prostate cancer. Hum. Pathol., 24: 4-9,
1993.
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from

1998;7:497-504. Cancer Epidemiol Biomarkers Prev A Picon, L I Gold, J Wang, et al. elevated levels of transforming growth factor beta1.A subset of metastatic human colon cancers expresses
Updated version
http://cebp.aacrjournals.org/content/7/6/497
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cebp.aacrjournals.org/content/7/6/497To request permission to re-use all or part of this article, use this link
on July 1, 2020. © 1998 American Association for Cancer Research. cebp.aacrjournals.org Downloaded from