A study on the magnetic resonance imaging (MRI)...
15
IOP PUBLISHING PHYSICS IN MEDICINE AND BIOLOGY Phys. Med. Biol. 53 (2008) 3579–3593 doi:10.1088/0031-9155/53/13/013 A study on the magnetic resonance imaging (MRI)-based radiation treatment planning of intracranial lesions T Stanescu 1,2 , H-S Jans 3 , N Pervez 1 , P Stavrev 3 and B G Fallone 1,2,3 1 Department of Oncology, University of Alberta, Cross Cancer Institute, Edmonton, Alberta, Canada 2 Department of Physics, University of Alberta, University of Alberta Cross Cancer Institute, Edmonton, Alberta, Canada 3 Department of Medical Physics, University of Alberta, University of Alberta Cross Cancer Institute, Edmonton, Alberta, Canada E-mail: [email protected] Received 5 December 2007, in final form 5 June 2008 Published 17 June 2008 Online at stacks.iop.org/PMB/53/3579 Abstract The aim of this study is to develop a magnetic resonance imaging (MRI)- based treatment planning procedure for intracranial lesions. The method relies on (a) distortion correction of raw magnetic resonance (MR) images by using an adaptive thresholding and iterative technique, (b) autosegmentation of head structures relevant to dosimetric calculations (scalp, bone and brain) using an atlas-based software and (c) conversion of MR images into computed tomography (CT)-like images by assigning bulk CT values to organ contours and dose calculations performed in Eclipse (Philips Medical Systems). Standard CT + MRI-based and MRI-only plans were compared by means of isodose distributions, dose volume histograms and several dosimetric parameters. The plans were also ranked by using a tumor control probability (TCP)-based technique for heterogeneous irradiation, which is independent of radiobiological parameters. For our 3 T Intera MRI scanner (Philips Medical Systems), we determined that the total maximum image distortion corresponding to a typical brain study was about 4 mm. The CT + MRI and MRI-only plans were found to be in good agreement for all patients investigated. Following our clinical criteria, the TCP-based ranking tool shows no significant difference between the two types of plans. This indicates that the proposed MRI-based treatment planning procedure is suitable for the radiotherapy of intracranial lesions. 1. Introduction In recent years there has been an increasing interest in developing new techniques for MRI simulation, i.e. radiation treatment planning (RTP) based solely on MRI data, aimed at 0031-9155/08/133579+15$30.00 © 2008 Institute of Physics and Engineering in Medicine Printed in the UK 3579
Transcript of A study on the magnetic resonance imaging (MRI)...

IOP PUBLISHING PHYSICS IN MEDICINE AND BIOLOGY
Phys. Med. Biol. 53 (2008) 3579–3593 doi:10.1088/0031-9155/53/13/013
A study on the magnetic resonance imaging(MRI)-based radiation treatment planning ofintracranial lesions
T Stanescu1,2, H-S Jans3, N Pervez1, P Stavrev3 and B G Fallone1,2,3
1 Department of Oncology, University of Alberta, Cross Cancer Institute, Edmonton, Alberta,Canada2 Department of Physics, University of Alberta, University of Alberta Cross Cancer Institute,Edmonton, Alberta, Canada3 Department of Medical Physics, University of Alberta, University of Alberta Cross CancerInstitute, Edmonton, Alberta, Canada
E-mail: [email protected]
Received 5 December 2007, in final form 5 June 2008Published 17 June 2008Online at stacks.iop.org/PMB/53/3579
AbstractThe aim of this study is to develop a magnetic resonance imaging (MRI)-based treatment planning procedure for intracranial lesions. The methodrelies on (a) distortion correction of raw magnetic resonance (MR) images byusing an adaptive thresholding and iterative technique, (b) autosegmentationof head structures relevant to dosimetric calculations (scalp, bone andbrain) using an atlas-based software and (c) conversion of MR images intocomputed tomography (CT)-like images by assigning bulk CT values toorgan contours and dose calculations performed in Eclipse (Philips MedicalSystems). Standard CT + MRI-based and MRI-only plans were compared bymeans of isodose distributions, dose volume histograms and several dosimetricparameters. The plans were also ranked by using a tumor control probability(TCP)-based technique for heterogeneous irradiation, which is independentof radiobiological parameters. For our 3 T Intera MRI scanner (PhilipsMedical Systems), we determined that the total maximum image distortioncorresponding to a typical brain study was about 4 mm. The CT + MRI andMRI-only plans were found to be in good agreement for all patients investigated.Following our clinical criteria, the TCP-based ranking tool shows no significantdifference between the two types of plans. This indicates that the proposedMRI-based treatment planning procedure is suitable for the radiotherapy ofintracranial lesions.
1. Introduction
In recent years there has been an increasing interest in developing new techniques for MRIsimulation, i.e. radiation treatment planning (RTP) based solely on MRI data, aimed at
0031-9155/08/133579+15$30.00 © 2008 Institute of Physics and Engineering in Medicine Printed in the UK 3579
3580 T Stanescu et al
improving the RTP process of brain (Stanescu et al 2006a, 2006b, 2007) and prostate (Chenet al 2004a, 2004b, Lee et al 2003) cancer. In particular for brain, the most common RTPprocedure consists of (a) image fusion of MRI and CT corresponding datasets, (b) contouringof the target and organs at risk on the MR images to take advantage of MRI’s superior soft-tissue contrast and transfer the volume contours on the CT images and (c) dose calculations onCT images based on their innate electron density information. A particular reason for imagefusion is that MR images are inherently prone to distortions that can alter the local topographytargeted by the radiation treatment. Imprecise localization of the target may lead to an overallreduction in treatment accuracy and efficiency. Replacing the current CT + MRI-based RTPprocedure with MRI simulation will eliminate the CT scanning sessions (no x-ray exposure)and consequently the image fusion process. Moreover, any incidental errors caused by patientinter-procedure positioning and image fusion would be eliminated. As a consequence, theimproved target localization is expected to lead to a higher local tumor control and reducednormal tissue complications.
For MRI simulation it is required that different electron density information (i.e. CTvalues) be correlated or assigned to MR images and the image distortions be addressed (Chenet al 2004b, Doran et al 2005, Stanescu et al 2006a, 2006c).
There is no apparent correlation between MR tissue signal intensity and CT numbersas different tissues may exhibit similar signal values, e.g. hard bone and air show as darkregions. To compensate for this limitation, MR images can be prepared for dose calculationsby assigning bulk CT values to the voxels corresponding to segmented volumes of interest(VOIs) (Chen et al 2004a, Stanescu et al 2006a). These VOIs represent certain tissue typesrelevant to dosimetric calculations such as bone, lung and soft tissue.
MR image distortions are caused by scanner-related and patient-induced effects. Thescanner-related distortions, inherent to any MRI scanner, are due to magnetic field (B0)inhomogeneities and gradient nonlinearities (Doran et al 2005, Stanescu et al 2006c). Incontrast, the patient-induced artifacts are rooted in susceptibility and chemical shift localvariations in the imaged volume (Bakker et al 1992, Chang and Fitzpatrick 1992). Themagnitude of distortions depends on the scanning parameters of the imaging sequence. AsRTP requires a spatial image resolution of less than 2 mm, the distortions need to be quantifiedand rectified before the images are used in the clinical process (Doran et al 2005, Stanescuet al 2006c).
There is little literature on brain MRI simulation techniques. In the late 1990s, Beaviset al (1998) reported on a method based on assigning a unique electron density value,i.e. water, to the entire head volume, thus neglecting the effects of inhomogeneities. Intheir study, the authors also assumed that the impact of the 3D image distortions werenegligible. The latter assumption was based on image distortion measurements performedwith a phantom object. However, this phantom, by its design, prevented an accuratedescription of the entire 3D distortion field. Namely, the reference points that sampledthe volume of interest were insufficient, i.e. limited to 17 points per image slice for a typicalhead field of view (FOV) of 20 cm diameter. A significantly larger number of referencepoints are required to precisely evaluate the local variations of the distortion field (Doranet al 2005). Furthermore, the slice warp distortion, i.e. distortion along the z-axis, wasnot addressed as the authors investigated the in-plane distortions only. Recent studies(Wang et al 2004, Stanescu et al 2006c) showed that the scanner-related distortion levels,corresponding to a brain scan, can be up to 6 mm depending on the scanner type andimaging sequence. These findings stress the importance of implementing techniques forcorrecting the MR images before using them in the RTP’s contouring and dose calculationprocesses.

A study on the MRI-based radiation treatment planning of intracranial lesions 3581
We propose an MRI-based treatment planning method for intracranial lesions that relieson (a) image distortion correction based on an adaptive thresholding and iterative method,(b) autosegmentation of organ structures relevant to dosimetric calculations (i.e. scalp, boneand brain) using an atlas-based non-rigid registration technique, (c) conversion of MR imagesinto CT-like images by assigning bulk electron density values to organ contours and dosecalculations performed with a treatment planning system (TPS) and (d) plan ranking based ona tumor control probability (TCP) method for heterogeneous irradiation that is independentof radiobiological parameters. To validate our procedure we compared MRI-only and CT +MRI-based plans.
2. Methods and materials
2.1. Data acquisition—CT and MRI scanning procedures
We used data from four glioblastoma multiforme (GBM) patients. Each individual wassubjected to two subsequent scanning sessions, namely CT and 3 T MRI, following a clinicalprotocol implemented at our institution. Firstly, data were acquired on a Piker PQ 5000 CTsimulator (Philips Medical Systems, Cleveland, OH) by means of a 480 mm FOV, matrix512 × 512 (pixel resolution 0.94 mm), 83 partitions with 2 mm thickness each and slice gapof 2.5 mm. Each patient was positioned on the scanner couch using a head immobilizationsystem consisting of a jig on which custom plastic shells were attached. Donut-shaped fiducialmarkers filled with a copper sulfate solution (IZI Medical Products, Inc.) were placed on theshells to mark the triangulation laser reference points.
A time interval of about half an hour is required to relocate the patients and to preparethem for the MRI scanning session performed on a 3 T Intera (Philips Medical Systems)unit. To mimic the setup used in the CT room (same system of reference), the subjects wererepositioned by using the scanner’s lasers, an in-house built flat bed and the same head insert,plastic shells and fiducial markers. The positioning devices were used inside a head coilas its aperture was sufficiently large to house them. The imaging protocol includes (a) astandard scout sequence to select the region containing the target, (b) a 3D T1 turbo field echo(TFE) sequence with contrast enhancement administered intravenously, i.e. 0.2 mmol kg−1
body weight Gd-DTPA, and (c) a 3D T2 turbo spin echo (TSE) sequence. The T1-weightedimage sequence was used for contouring the target and the organs at risk (i.e. eyes, eye lenses,optic nerves, optic chiasm, pituitary gland and brain stem). In contrast, the T2-weighteddatasets were required for visualization purposes only to better identify the tumor’s spread.The 3D T1 TFE sequence is characterized by a TE/TR/α of 4.1/8.8/8◦, 240 × 240 mm2 FOV,256 × 256 in-plane matrix (pixel resolution 0.9 mm) and 125 contiguous partitions of 1 mmeach. It is assumed that the inter-modality patient positioning can be achieved with an accuracyof 1–2 mm. After the scanning process, the image datasets were recorded and subsequentlytransferred via a local network to Eclipse TPS (Varian Medical Systems) for virtual treatmentplanning simulation.
2.2. MR image distortion correction
The patient datasets were rectified for the system-related image artifacts by using a phantom-based distortion correction method, which was presented elsewhere (Stanescu et al 2006c).Briefly, it relies on (a) an adaptive image thresholding analysis performed to accurately identifythe reference points required for the 3D distortion field mapping, and (b) an iterative processto determine the distortion along the main axes. Using this method the 3D distortion field was

3582 T Stanescu et al
determined for the 3D T1-weighted imaging sequence, which was used to scan all the GBMpatients. Once the system-related local distortions are mapped, they can be used to correctany subsequent clinical dataset as this type of distortions is not patient-dependent.
The maximum absolute distortion along the x, y and z axes are defined as
δx = max(|δxi |)δy = max(|δyi |), i = 1, N
δz = max(|δzi |)(1)
where δxi, δyi and δzi are the local distortion values, and N is the total number of referencepoints used to determine the 3D distortion field. The total maximum absolute distortion isgiven by
δt = max[√
(δxi)2 + (δyi)2 + (δzi)2], i = 1, N. (2)
Previous studies (Bhagwandien 1994, Moerland et al 1995, Sumanaweera et al 1994)showed that patient-induced distortions were noticeable, i.e. 2–4 mm, only in the sinuses’region at the air–tissue boundaries. In the radiation treatment planning-relevant volumes,e.g. brain, the distortions were found to be insignificant, i.e. within the image pixel size.We compared the contours of various head sub-structures segmented on the MR correctedimages (system-related distortions) with their corresponding CT representation. Specifically,following the CT-MR image fusion (see below), the MR contours were overlaid on the CTimages and Eclipse’s measuring tools were used to quantify the contours shift.
2.3. Structures segmentation
The head structures relevant to dosimetric calculations, i.e. brain, bone and scalp, weresegmented using a freely available library of image processing tools, i.e. FSL (AnalysisGroup, FMRIB, Oxford, UK) (Stephen et al 2004). Specifically, these structures can beautomatically extracted by using an atlas-based non-rigid registration technique. The outputconsists of binary image datasets corresponding to each structure of interest, namely theorgans, depicted as white regions on black background. The contours of these structures canbe easily obtained (e.g. in Matlab) and converted into RT structure files that are subsequentlyimported into Eclipse. Alternatively, the binary images can be directly imported into Eclipseand automatically outlined by setting a unique threshold value for the entire dataset (e.g.‘Search Body’ contouring tool). The accuracy of the autosegmentation method was inspectedvisually by overlaying the outlines on the images in Eclipse, and little manual adjustmentwas required to adjust the contours to match the anatomical structures within 1 mm. The airregions were not segmented as they were not relevant for dosimetric calculations.
The clinical target volume (CTV) and the organs at risk (i.e. eyes, eye lenses, opticnerves, optic chiasm, pituitary gland and brain stem) were contoured by a radiation oncologiston the T1-weighted uncorrected datasets by using typical contouring tools available in Eclipse.A 5 mm margin was uniformly added in all directions to the CTV to generate the planningtarget volume (PTV).
2.4. CT + MRI-based RTP
In our institution, the standard RTP procedure for GBM subjects relies on image fusion ofCT and MRI (uncorrected for distortion) datasets along with CT-based dose calculations onEclipse. To register the MRI and CT datasets, we used prominent bony landmarks locatedaround the brain (i.e. local protuberates of the parietal and occipital bones). At least five

A study on the MRI-based radiation treatment planning of intracranial lesions 3583
pairs of identical and non-coplanar bony landmarks were marked on both CT and MR images.As a preliminary step, to assess the accuracy of the registration process we used Eclipse’s‘Mean Error Indicator’. This metric is defined by the mean error between the displacementsof registration pairs of point identified in the CT and MR images. For all registrations weachieved an error of approximately 1.0–1.5 mm. Furthermore, three-dimensional manualrefining was performed to adjust the image registration according to brain tissue and thebone–brain interface. We avoided relying on fiducial markers or any bony landmarks locatednear the nasal sinuses as they are prone to artifacts due to susceptibility variations at themarker/tissue–air interfaces. The results were visually verified by overlaying the CT and MRimages. The tumor and organs at risk volumes were copied onto the CT datasets, which weresubsequently used for dose calculations.
For each patient, we generated IMRT plans based on an arrangement of five beams tomeet our clinical acceptance criteria; specifically 95% of the PTV has to receive the prescribeddose (Dref). In addition, the maximum dose to the target (Dmax) should not exceed 105% ofDref and the minimum dose to the target (Dmin) should not be lower than 95% of Dref unlessthe hot and cold spot areas, respectively, are smaller than 1 cm2. The plans were verified andapproved by a radiation oncologist.
2.5. MRI-based RTP
Firstly, the patient MR images were corrected for distortion. The next step was to generateimage binary masks for scalp, bone and brain using the FSL autosegmentation tool. Thecontours of these structures were recorded in Eclipse as separate volumes. For this study,instead of re-drawing the organs at risk on the corrected MR images it was easier to correctthe contours for distortion as follows:
(a) export from Eclipse the RT structure file containing the uncorrected volumes;(b) read in the RT structure file, extract and rectify for distortion the coordinates of all contour
points corresponding to each structure;(c) write back in the RT structure file the new coordinates of the contour points and(d) import in Eclipse the new RT structure file and record the corrected organ volumes.
Steps (b) and (c) were performed by using an in-house developed software tool written inMatlab. Besides being more practical to obtain the corrected organs at risk outlines, anotherimportant reason for using this method was to avoid intra-modality volume changes. Thisis important for an accurate evaluation of the MRI-based treatment planning procedure. Inpractice, for MRI-based RTPs the organs at risk volumes will be segmented directly on thecorrected datasets.
Once the images and all contours of interest are available, we need to assign bulk CTvalues to the voxels enclosed by the scalp, bone and brain volumes, to convert the MRimages into CT-like images. For scalp and brain we assigned 0 HU and for bone 1000 HU,respectively. In particular for brain, we performed on the CT datasets a uniformity check ofthe CT numbers. This was done by placing five regions of interest (ROIs) on each CT imageslice containing brain information. The CT numbers were averaged in each ROI and comparedfor the entire brain volume, i.e. same slice and slice-by-slice. We found that there was nosignificant variation from the CT numbers corresponding to water (within 2%). Therefore, abulk value (i.e. 0 HU) was assigned to the MRI brain volumes.
Each MRI-only plan was generated by applying its corresponding CT + MRI-based plan,i.e. by copying the beam arrangements and fluences. The plan transfer is done with regard tothe isocenter, which was set to be at the center of mass of the PTV. Before performing dose

3584 T Stanescu et al
calculations in Eclipse, each MRI dataset has to be associated with an imaging device, i.e. toassign a conversion table between HU values and relative electron densities.
2.6. Comparison and evaluation of CT + MRI- and MRI-based RTPs
To validate our MRI-based treatment planning method we generated and compared severaltreatment plans as follows.
(a) All MR contours including PTV, organs at risk and dosimetrically relevant structures (i.e.scalp, bone and brain) were transferred onto the CT images through image fusion. BulkCT values were assigned to scalp, bone and brain, thus neglecting the intrinsic CT valuesof the images. For convenience we will name this type of plan CT + MRI (MRI contoursdosimetry). This plan was compared to the standard CT + MRI-based plan in order toevaluate the accuracy of CT values assignation method.
(b) To investigate the effects of MR image distortions we compared MRI (uncorrected) toMRI (corrected)-only plans. Also, for the same purpose, we compared the CT + MRIplans based on the uncorrected and corrected PTV volumes, respectively.
(c) To determine the overall effect of image fusion, MR image distortions, segmentationof head sub-structures and CT values bulk assignation we compared the CT + MRI(uncorrected) to MRI (corrected)-only plans.
To compare the plans we used isodose distributions, dose volume histograms (DVHs) andseveral PTV dosimetric parameters, i.e. the dose at the isocenter (Diso), mean target dose(Dmean), Dmin and Dmax. The plans were ranked by using a TCP-based technique forheterogeneous irradiation (Stanescu et al 2006a). This technique does not require previousknowledge of exact parameter values (see the appendix). The corresponding TCP values forthe investigated CT + MRI and MRI-only plans were calculated and compared for parametervalues of the entire parametric space.
3. Results and discussion
3.1. MR image distortion
The system-related distortions were determined using our distortion correction technique forthe 3D T1-weighted sequence, which was used to scan all the patients. Figure 1(a) showsthe distortion values along the main axes and the total maximum distortion (see section 2.2),respectively, corresponding to spherical volumes with radii ranging from 20 to 130 mm. Thetotal maximum distortion relevant to a typical brain study, i.e. 10 cm radius, is approximately4 mm indicating that the MR brain images need to be rectified before being used in thetreatment planning process. Figure 1(b) shows an example of a brain image before andafter being corrected for distortions. Also, the difference between the two is displayed, whichshows the distribution of in-plane distortions, i.e. asymmetric light and dark areas. The residualgeometric distortions determined after applying the correction procedure are negligibly small,being within one pixel resolution, i.e. 0.94 × 0.94 mm2.
We also investigated the magnitude of patient-induced distortions by comparing thecontours of several structures delineated on both CT and MR corrected images (e.g. brain,scalp, organs at risk). We found that the local maximum shift between contours was about1.0–1.5 mm, hence being acceptable for RT planning purposes.

A study on the MRI-based radiation treatment planning of intracranial lesions 3585
(a)
(b)
Figure 1. (a) Maximum absolute distortions measured on the surface of a sphere with the sphere’sradius varying from 20 to 130 mm; (b) a typical example of a MR image before and after beingrectified for distortions and the difference map showing removed distortions.
3.2. MR image distortion impact on RTP
The MRI-based procedure suggested by Beavis et al (1998) considered the distortions in thebrain as being negligible. However, the authors used a 2D distortion correction techniquealong with a phantom object that prevented them from accurately determining the 3Ddistortion field. Considering the particular characteristics of our MR imaging protocol forGBM patients, namely a 3D TFE sequence acquired on a 3 T Intera scanner, MR imagedistortion correction is required as suggested by figure 1(a). In a previous study, Wang et al(2004) investigated in detail the distortion fields of several commercially available MRIscanners and found that the magnitude of distortions can be as high as 6 mm for a typicalbrain study FOV. These findings stress the importance of determining the 3D distortion field,which is unique to each MRI scanner, as a necessary step in the MRI-based treatment planningprocess. Also, patient images need to be rectified before being used for RTP purposes.This is crucial as local distortions affect both the volume size and the spatial location ofthe organs. Any error in identifying the target/organs will translate into a reduced accuracyin delivering the treatment and consequently in likely reduction of the probability of tumorcontrol.

3586 T Stanescu et al
Table 1. PTV volumes determined on the MRI uncorrected and corrected datasets along with theirpercent difference.
Patient Uncorrected Corrected Differencenumber (cm3) (cm3) (%)
1 102.69 103.58 0.92 96.58 96.12 0.53 85.47 84.56 1.14 47.34 47.21 0.3
Table 2. Distortion values corresponding to several structures of interest.
Patient PTV Body Bone Brainnumber (mm) (mm) (mm) (mm)
1 1.56 1.84 1.69 1.682 1.58 1.73 1.63 1.633 1.25 1.67 1.63 1.594 1.50 1.66 1.65 1.65
Table 3. Percent difference of dosimetric parameters calculated for the PTV uncorrected and PTVcorrected volumes on the CT + MRI-based plan.
Patient Dmean Dmin Dmax
number (%) (%) (%)
1 0.0 1.7 0.22 0.0 1.5 0.03 0.0 0.0 0.04 0.0 0.1 0.0
To assess the effect of image distortion on the accuracy of the RTP process we firstlycompared the effects of distortions on the PTV. Table 1 shows the PTV volumes correspondingto the corrected and uncorrected MR image datasets. For three out of four patients, byrectifying the images the PTVs became smaller. The maximum percent difference was1.1% corresponding to patient 3. Table 2 summarizes the maximum absolute distortioncorresponding to the PTV, body, bone and brain volume outlines. For all structures of interestthe distortion is less than 2 mm. In table 3 the percent difference of dosimetric parameterscalculated for the PTV uncorrected and PTV corrected structures are presented for the CT +MRI-based plan. There is practically no difference in Dmean and Dmax values and a maximumchange of < 2% in Dmin values. Table 4 compares the MRI (uncorrected)- and MRI (corrected)-based plans in terms of the percent difference of several dosimetric parameters such as Dmean,Dmin and Dmax. The differences in terms of Dmean and Dmax values between the two plansare negligible. The minimum target dose, i.e. Dmin, between the two plans agrees within1%. For the above plans, the isodose distributions are similar and the changes in the DVHs,corresponding to the organs at risk and target, are clinically insignificant.
Analyzing the available data, we found that image distortion had a negligible impact onthe RT plans’ outcome. This is apparently in disagreement with our earlier results, i.e. imagedistortion is important for brain studies (see figure 1(a)). However, this can be explained

A study on the MRI-based radiation treatment planning of intracranial lesions 3587
Table 4. Percent difference of dosimetric parameters calculated for the PTV corresponding to theMRI (uncorrected) and MRI (corrected)-based plans.
Patient Dmean Dmin Dmax
number (%) (%) (%)
1 0.1 0.4 0.42 0.1 1.0 0.23 0.0 0.3 0.24 0.0 0.1 0.0
Table 5. Percent difference of dosimetric parameters calculated for the CT + MRI and CT + MRI(MRI-contours dosimetry)-based plans.
Patient Diso Dmean Dmin Dmax
number (%) (%) (%) (%)
1 0.9 0.1 0.6 0.22 0.9 0.2 0.0 0.63 0.9 0.3 0.4 0.54 1.0 0.3 0.8 0.4
by considering that the clinical protocol at our institution considers the acquisition of 125contiguous MR image slices only, with a thickness of 1 mm each (see section 2.1). The dataare acquired in such a way that only the target area and its close vicinity are imaged and notthe entire head as in a standard CT scan (or MRI simulation). Furthermore, the datasets arecentered at the isocenter of the MRI scanner where the magnitude of distortion is significantlylower. As a consequence, all MRI datasets will have an extension along z. axis of about±6.25 cm only. In such a volume, the distortion level is roughly 2 mm, in agreement withdata shown in table 2.
3.3. Bulk CT values: effect on RTP
Brain studies (Ramsey and Oliver 1998, Stanescu et al 2006a) showed that the differencebetween turning on and off the inhomogeneity correction resulted in a dose difference of about2–3%. For the MRI-based plans, the inhomogeneities taken into account as the scalp, skulland brain outlines were automatically obtained with the FSL software library tools. UsingFSL, the structures’ segmentation becomes significantly faster than with the manual/semi-automatic techniques (Stanescu et al 2006a). Considering that (a) the MR image distortionswere negligible and (b) for the image fusion process we used anatomical landmarks that werenot affected by subject-induced image artifacts, the registration errors of the CT and MRdatasets were minimal, i.e. <1–2 mm.
Table 5 shows the comparison between the CT + MRI and CT + MRI (MRI contoursdosimetry)-based plans in terms of the percent difference calculated for Diso, Dmean, Dmin,and Dmax. The difference in maximum and minimum dose delivered to the target is < 1%.Similarly, for all subjects the Diso variation is approximately 1%. Dmean values change slightlyfrom one plan to another. There is no clinically relevant difference in the DVHs. Also, byusing the RT ranking tool we did not find any significant change between the plans. Thedosimetric parameters shown in table 5 suggest that the conversion process of MR images intoCT-like images was accurate enough for RTP purposes.

3588 T Stanescu et al
(a) (b)
Figure 2. Typical example showing a comparison of isodose distributions between (a) CT + MRI(uncorrected) plan and (b) MRI (corrected)-only plan.
(This figure is in colour only in the electronic version)
Table 6. Percent difference of dosimetric parameters calculated for the CT + MRI (uncorrected)and MRI (corrected)-only plans.
Patient Diso Dmean Dmin Dmax
number (%) (%) (%) (%)
1 1.0 0.2 5.5 0.52 1.8 0.3 12.5 0.43 1.2 0.3 4.7 0.54 1.2 0.3 6.3 0.5
3.4. CT + MRI (uncorrected) versus MRI (corrected)-only plans
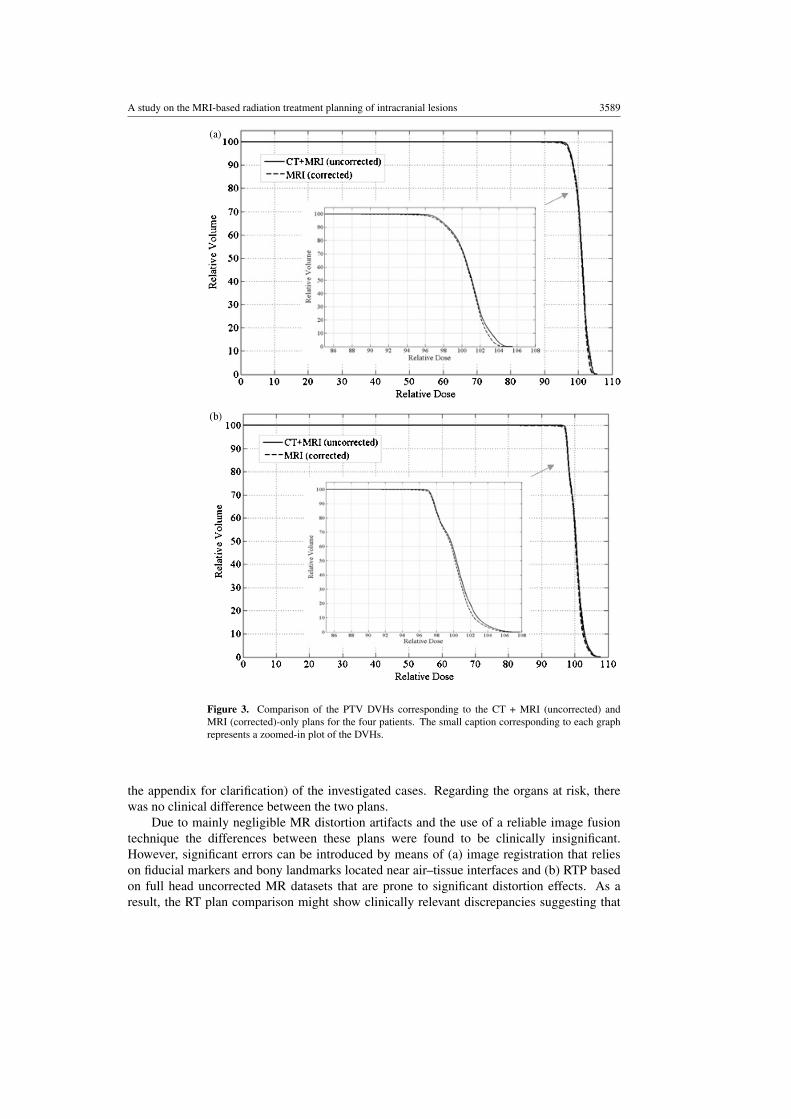
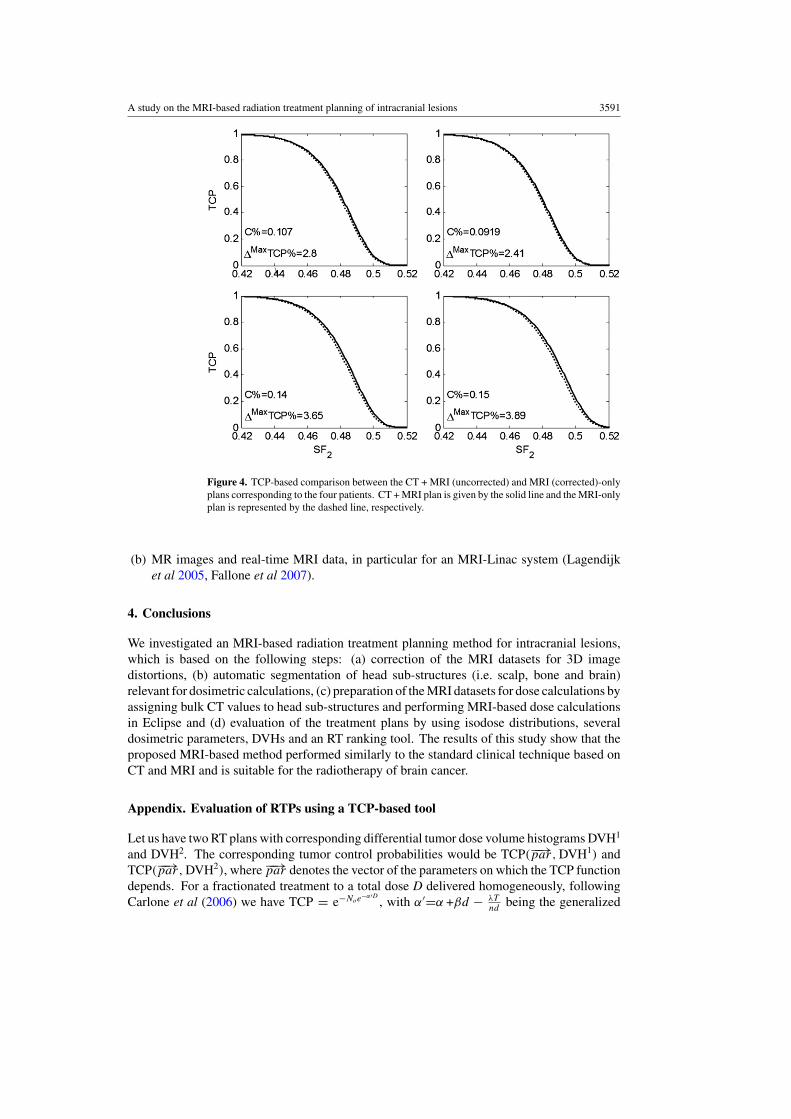
To determine the overall effect of image fusion, MR distortions, segmentation of head sub-structures and CT values bulk assignation we compared CT + MRI (uncorrected) to MRI(corrected)-only plans. Figure 2 compares the isodose distributions, corresponding to theisocenter slice, between a typical CT + MRI (uncorrected) and MRI (corrected)-only plans(patient number 1). The PTV is depicted as the red-colored area, and the isocenter is shown bythe yellow dot. In particular, in figure 2(a) the brain, bone and scalp contours are also displayed.The scalp outline mask coincides with the patient outline. The dose distributions of the twoplans are very similar, showing a complete coverage of the PTV by the 95% isodose line.Table 6 summarizes the dosimetric parameters used to compare the two plans. Specifically,the percent difference in the Dmean and Dmax values is <1%. The maximum variations in termsof Diso and Dmin are 1.8% and 12.5%, respectively. The DVHs corresponding to the PTVs areshown in figure 3. Comparing the two plans by means of the RT ranking tool, we found thatthe difference in TCPs between them was within 1%. The maximal TCP difference betweenboth plans, in all cases, is not greater than 4%. Figure 4 displays the TCP plan ranking (see
A study on the MRI-based radiation treatment planning of intracranial lesions 3589
Figure 3. Comparison of the PTV DVHs corresponding to the CT + MRI (uncorrected) andMRI (corrected)-only plans for the four patients. The small caption corresponding to each graphrepresents a zoomed-in plot of the DVHs.
the appendix for clarification) of the investigated cases. Regarding the organs at risk, therewas no clinical difference between the two plans.
Due to mainly negligible MR distortion artifacts and the use of a reliable image fusiontechnique the differences between these plans were found to be clinically insignificant.However, significant errors can be introduced by means of (a) image registration that relieson fiducial markers and bony landmarks located near air–tissue interfaces and (b) RTP basedon full head uncorrected MR datasets that are prone to significant distortion effects. As aresult, the RT plan comparison might show clinically relevant discrepancies suggesting that

3590 T Stanescu et al
Figure 3. (Continued.)
the MRI (corrected)-only plans are more accurate than the standard procedure CT + MRI(uncorrected).
Depending on the RT modality used in conjunction with the MRI-based treatment planningprocedure, the RT verification process can be performed based on the registration processbetween
(a) digitally reconstructed radiographs from MR images (MR-DRRs) and CT/MVCT imagesby segmenting the MR datasets into dosimetric relevant VOIs (e.g. bone and soft-tissue)and assigning to them bulk electron density information (Chen et al 2007, Ramsey et al1999, Yin et al 1998). In our case, the skull can be automatically segmented using FSL(see section 2.3) and electron density information can be assigned in Eclipse in order togenerate MR-DRRs and
A study on the MRI-based radiation treatment planning of intracranial lesions 3591
Figure 4. TCP-based comparison between the CT + MRI (uncorrected) and MRI (corrected)-onlyplans corresponding to the four patients. CT + MRI plan is given by the solid line and the MRI-onlyplan is represented by the dashed line, respectively.
(b) MR images and real-time MRI data, in particular for an MRI-Linac system (Lagendijket al 2005, Fallone et al 2007).
4. Conclusions
We investigated an MRI-based radiation treatment planning method for intracranial lesions,which is based on the following steps: (a) correction of the MRI datasets for 3D imagedistortions, (b) automatic segmentation of head sub-structures (i.e. scalp, bone and brain)relevant for dosimetric calculations, (c) preparation of the MRI datasets for dose calculations byassigning bulk CT values to head sub-structures and performing MRI-based dose calculationsin Eclipse and (d) evaluation of the treatment plans by using isodose distributions, severaldosimetric parameters, DVHs and an RT ranking tool. The results of this study show that theproposed MRI-based method performed similarly to the standard clinical technique based onCT and MRI and is suitable for the radiotherapy of brain cancer.
Appendix. Evaluation of RTPs using a TCP-based tool
Let us have two RT plans with corresponding differential tumor dose volume histograms DVH1
and DVH2. The corresponding tumor control probabilities would be TCP(−−→par, DVH1) andTCP(−−→par, DVH2), where −−→par denotes the vector of the parameters on which the TCP functiondepends. For a fractionated treatment to a total dose D delivered homogeneously, followingCarlone et al (2006) we have TCP = e−Noe
−α′D, with α′=α +βd − λT
ndbeing the generalized

3592 T Stanescu et al
radiosensitivity and No is the initial number of clonogens. In the case of heterogeneousirradiation one has
TCP = exp(−ρ
∑Vi e−α′Di
)= exp
(−ρ
∑ViSF
0.5Di
2
)(A.1)
where ρ is the cell density, {Vi, Di} represents the differential DVH using the absolute (notthe relative) tumor sub-volumes Vi irradiated to doses Di and SF2 is the tumor cell survivingfraction at a dose equal to 2 Gy and for the corresponding fractionation regime.
Essentially a plan resulting in higher TCP values, for any value of the parameter SF2,should be considered superior to the plan resulting in lower TCP values. Thus, if we plot theTCP curves as functions of the parameter SF2 – TCP(SF2|DVH1) and TCP(SF2|DVH2), theright curve will correspond to the better RT plan, producing higher TCPs for any value of SF2.
The following measures could be introduced for the estimation of the closeness in TCPterms of two RT plans:
C =∫ 1
0(TCP(SF2|DVH2) − TCP(SF2|DVH1)) dSF2 (A.2)
�max TCP = maxSF1
(TCP(SF2|DVH2) − TCP(SF2|DVH1)). (A.3)
The first measure C is defined in the interval [0, 1] and gives the area between the TCPcurves corresponding to the two plans under investigation. The second measure representsthe maximal expected TCP difference between the two plans. The sign of these two measuresnaturally indicates the better plan.
References
Bakker C, Moerland M A, Bhagwandien R and Beersma R 1992 Analysis of machine-dependant and object-inducedgeometric distortion in 2DDT MR imaging Magn. Reson. Imag. 10 597–608
Beavis A, Gibbs P, Dealey R A and Whitton V J 1998 Radiotherapy treatment planning of brain tumors using MRIalone Br. J. Rad. 71 544–8
Bhagwandien R 1994 Object induced geometry and intensity distortions in magnetic resonance imaging PhD ThesisUniversity of Utrecht, The Netherlands
Carlone M C, Warkentin B, Stavrev P and Fallone B G 2006 Fundamental form of the population TCP model in thelimit of large heterogeneity Med. Phys. 33 1634–42
Chang H and Fitzpatrick J M 1992 A technique for accurate magnetic resonance imaging in the presence of fieldinhomogeneities IEEE Trans. Med. Imag. 11 319–29
Chen L et al 2004a MRI-based treatment planning for radiotherapy: dosimetric verification for prostate IMRT Int. J.Radiat. Oncol. Biol. Phys. 60 636–47
Chen L et al 2004b Dosimetric evaluation of MRI-based treatment planning for prostate cancer Phys. Med. Biol.49 5157–70
Chen L, Thai-Binh N, Elan M S, Chen Z, Wei L, Lu W, Price R A, Pollack A and Ma C 2007 Magnetic resonance-based treatment planning for prostate intensity-modulated radiotherapy: creation of digitally reconstructedradiographs Int. J. Radiat. Oncol. Biol. Phys. 68 903–11
Doran S J, Charles-Edwards L, Reinsberg S A and Leach M O 2005 A complete distortion correction for MR images:I. Gradient warp correction Phys. Med. Biol. 50 1343–61
Fallone B, Carlone M, Murray B, Rathee S, Stanescu T, Steciw S, Wachowicz K and Kirkby C 2007 Development ofa Linac-MRI system for real-time ART Med. Phys. 34 2547
Lagendijk J et al 2005 In room magnetic resonance imaging guided radiotherapy (MRIgRT) Med. Phys. 32 2067Lee Y K et al 2003 Radiotherapy treatment planning of prostate cancer using magnetic resonance imaging alone
Radiother. Oncol. 66 203–16Moerland M, Beersma R, Bhagwandien R, Wijrdeman H K and Bakker C J G 1995 Analysis and correction of
geometric distortions in 1.5 T magnetic resonance images for use in radiotherapy treatment planning Phys. Med.Biol. 40 1651–64
Ramsey C, Arwood D, Scaperoth D and Oliver A L 1999 Clinical application of digitally reconstructed radiographsgenerated from magnetic resonance imaging for intracranial lesions Int. J. Radiat. Oncol. Biol. Phys. 45 797–802

A study on the MRI-based radiation treatment planning of intracranial lesions 3593
Ramsey C and Oliver A L 1998 Magnetic resonance imaging based digitally reconstructed radiographs, virtualsimulation, and three-dimensional treatment planning for brain neoplasms Med. Phys. 25 1928–34
Stanescu T, Jans H S, Stavrev P and Fallone B G 2006a 3T MR-based treatment planning for radiotherapy of brainlesions Radiol. Oncol. 40 125–32
Stanescu T, Jans H S, Stavrev P and Fallone B G 2006b A complete MR-based treatment planning procedure forradiotherapy of intracranial lesions Med. Phys. 33 2271
Stanescu T, Jans H and Fallone B G 2006c Investigation of a 3D MR distortion correction protocol Proc. 52nd Ann.Meeting of Canadian Organization of Medical Physicists (COMP) (Saskatoon, Canada) pp 36–8
Stanescu T, Jans H, Pervez N, Stavrev P and Fallone B G 2007 Developments in MRI simulation of intracraniallesions Radiother. Oncol. 84 S18
Stephen M et al 2004 Advances in functional and structural MR image analysis and implementation as FSLNeuroImage 23 208–19
Sumanaweera T et al 1994 Characterization of spatial distortion in magnetic resonance imaging and its implicationsfor stereotactic surgery Neurosurgery 35 696–704
Wang D, Strugnell W, Cowin G, Doddrell D M and Slaughter R 2004 Geometric distortion in clinical MRI systemspart 1: evaluation using a 3D phantom Mag. Res. Imag. 22 1211–21
Yin F et al 1998 MR image-guided portal verification for brain treatment field Int. J. Radiat. Oncol. Biol. Phys.40 703–11