A Study ofCongenital and Early Acquired Impairment ofHearing studyof congenital and early.pdf · A...
8
SCIENCE I ORIGINAL ARTICLE' A Study of Congenital and Early Acquired Impairment of Hearing Parmod Kalsotra*, S. Kumar*, P. Gosh*, N. K. Mishra**, I. C. Verma*** Abstract The present study included 261 patients (M:F=I.72: I) suffering from congenital and early acquired hearing loss. The aetiological breakup of the hearing loss was: genetic factors 47.5%. non-genetic factors 16.8%, congenital ear malfonnations 8.5% and cryptogenic factors in 27.2% cases. Autosomal recessive mode of inheritance was seen most commonly (62%) followed by autosomal dominant (20%) in the genetic group of hearing loss. Maternal Rubella was most common cause of prenatal group of hearing loss while perinataly birth anoxia and prematurity were common. Postnataly meningitis was most common aetiology of hearing loss. Linkage analysis on SLINK 2 point autosomal data yielded LOD score of more than 3 in an autosomal dominant family. KeyWords Congenital. Genetic. Non-genetic, Hearing loss. Introduction - ·d ). ,. ;1 :1 Impairment of hearing is one of the major disabilities occuring in India, affecting about 1.8% of ·the population. According to the National Sample Survey (I), the prevalence of hearing disability per 1000 population. were 5.53 in rural and 3.90 in urban areas. These rates are higher than those for disability due to loss of vision and locomotor problems. There is virtually no data regarding prevalence of congenital and early acquired hearing loss in India except few regional surveys. Kameswaran and Rajendra Kumar (lCMR) (2) reported 0.1 % of the population to be suffering from congenital sensorineural '. hearing loss and 0.02% of urban and rural population suffering from congenital conductive hearing loss in Tamil Nadu. Pat et. al. (3) reported 2 per 1000 children under 5 years and 4.2 per 1000 children under 15 years to have bilateral sensorineural hearing loss of worse than 60 dB. This study was undertaken to find out the prevalence of congenital and acquired hearing loss \\ 1111 analysis of various causes for the same. Material and Methods The present study was undertaken at ENT OPO, All India Institute of Medical Sciences, New Delhi to study the main aetiologcial factors causing congenital and early acquired hearing loss. '1 from the Deptls. of *ENT, **Ncuro-Radiology & ***Paediatrics. All India Institute of Medical Sciences, New Delhi, India. Correspondence to: Dr. Parmod Kalsotra, Lecturer, Department arENT, SMGS Hospital, Govt. Medical College. Jammu (J&K) India. 1'01. 4 No.3, July-September 2002 136
Transcript of A Study ofCongenital and Early Acquired Impairment ofHearing studyof congenital and early.pdf · A...
~~~~~~~~~ ~JK SCIENCE
IORIGINAL ARTICLE'
A Study of Congenital and Early AcquiredImpairment of Hearing
Parmod Kalsotra*, S. Kumar*, P. Gosh*, N. K. Mishra**, I. C. Verma***
Abstract
The present study included 261 patients (M:F=I.72: I) suffering from congenital and early acquiredhearing loss. The aetiological breakup of the hearing loss was: genetic factors 47.5%. non-geneticfactors 16.8%, congenital ear malfonnations 8.5% and cryptogenic factors in 27.2% cases. Autosomalrecessive mode of inheritance was seen most commonly (62%) followed by autosomal dominant(20%) in the genetic group of hearing loss. Maternal Rubella was most common cause of prenatalgroup of hearing loss while perinataly birth anoxia and prematurity were common. Postnatalymeningitis was most common aetiology ofhearing loss. Linkage analysis on SLINK 2 point autosomaldata yielded LOD score of more than 3 in an autosomal dominant family.
KeyWords
Congenital. Genetic. Non-genetic, Hearing loss.
Introduction
-
·d
).
,.;1
:1
Impairment of hearing is one of the major
disabilities occuring in India, affecting about 1.8%of ·the population. According to the National
Sample Survey (I), the prevalence of hearing
disability per 1000 population. were 5.53 in rural and
3.90 in urban areas. These rates are higher than those
for disability due to loss of vision and locomotor
problems.
There is virtually no data regarding prevalence
of congenital and early acquired hearing loss in
India except few regional surveys. Kameswaran and
Rajendra Kumar (lCMR) (2) reported 0.1 % of the
population to be suffering from congenital sensorineural'.
hearing loss and 0.02% of urban and rural population
suffering from congenital conductive hearing loss inTamil Nadu. Pat et. al. (3) reported 2 per 1000 children
under 5 years and 4.2 per 1000 children under 15 years
to have bilateral sensorineural hearing loss ofworse than
60 dB. This study was undertaken to find out the
prevalence ofcongenital and acquired hearing loss \\ 1111
analysis of various causes for the same.
Material and Methods
The present study was undertaken at ENT OPO, All
India Institute of Medical Sciences, New Delhi to study
the main aetiologcial factors causing congenital and early
acquired hearing loss.
'1
from the Deptls. of *ENT, **Ncuro-Radiology & ***Paediatrics. All India Institute of Medical Sciences, New Delhi, India.Correspondence to: Dr. Parmod Kalsotra, Lecturer, Department arENT, SMGS Hospital, Govt. Medical College. Jammu (J&K) India.
1'01. 4 No.3, July-September 2002 136
,______________~JK SCIE CE
I. Patient Selection
ta) InclUSion cntcna All those patients with
prelmgually 'mpaired hearing who have no history
of environmental factors to explain the hearing
loss dunng the pre lingual period were subjected'.
to further detailed work up.
Ib) ExclUSion cnteria The following cases were
excluded Irom the study.
(I) H,story of ear infections and trauma.
(il) IIlstory of Q!otoxic drug intake, mumps,
measles or men ingi tis after 6 months ofage.
(ill) Family history ofotospongiosis.
2. Work-up of an Individual Case
Detahed work-up of an mdividual case was carried
out mcludmg prenatal, perinatal and postnatal history to
find out vanous exog~nouscongenital causes.
Pedigree chart of the affected child was drawn at least
upto three generations and a detailed systemic
exammatlon of ophthalmology, cardiovascular system
and abdomen was performed to look for associated
anomahes. ENT examination with spec,al attenllon to
branchial arch system was performed. Mode of
IIlhentancc was ascertained whenever possible as per
the criteria used by RIJn and Cremers (4) for acceptance
ofherednary and acquired causes.
Spec,al l11\'esllgations were performed wherever
mdlcated and possible to establish the diagnosis. These
mcludcd :
I. Antibody tnres lor toxoplasmosis, rubella. CMY.
measles. mumps 111 cases when suspected and
feas,ble espcctally for Rubella within 4 years of
age (6) and CMY within 3 weeks of life (7).
2. EKG for suspcctcd Jervell and tange-Neilson
syndrome.
3. ERG for suspected Usher's syndrome.
4. Thyroid function test lor suspected pendred's
syndrome.
5. Mucopolysaccharide and amimo ac,ds screenmg
in the urine in suspected metabolic aetIOlogy.
6. Renal function test for Alport 's and other otorenal
syndromes.
7. Serum uric acid. pyrophosphates ctc to exclude
metabolic causes.
8. Chromosomal studies: In the presence of mul11ple
malformations in a case ""th heanng loss not
suspected to be due to a single gene d,sroder were
subjects for chromosomal studies.
3. Hearing Evaluation
Included the pure tone audiometry. free flllJd testlOg
(FFT) inpedence and acoustic reflex and bramstem
evoked response audiometry (BERA).
4. Radiology
High resolution CT Scan (1.5 mm sect,ons through
temporal bone in 30 degrees aXial plane) "as done In
selected cases particularly whcrc cochlear dysgenesIs
was suspected.
Results
The present study group included 261 cases 01
congenital and early acquired heanng Impalrmen
attending ENT outpatients department. All pat,enls wllh
a hearing loss conductive. mixed or senson-neural.
averaging 25 dB HL or more m the beller ear by at,conduction. within the frequency range of500-2000 HI
were included in the study.
Aetiology
The aetiology of 261 children stud'ed. was elassdied
into f<;lur main groups as shown in Table I. Congemla!
ear malformations were considered separately beeauM
they d,d not fall into any defill1tl\'e group (5).
Vol. 4 0.3. July-September ~

______________ ~I\~K SCIENCE~,,;-
TableNo. I
Aetiology of Hear"jog Loss
\ctiolog) No. or eases Percentage
Genetic 124 47.5
AuIOS0Il1.11 Recessive 77 29.5
Autosomal Dominant 26 10.0
X-Rcccssl\c 1 0.4
Multifactorial 15 5.7
Chromosomal 2 0.8
UnclasSified <ISS0Cialion 3 1.1
~ on-Genetic 44 16.8
Prenatal 6 2.3
Pennatal 12 4.6
Neonatal Jaundice 3 1.1
Smh anax l<l & prematurity 9· 3.5
Postnatal 26 99
MClllgltlS 18 6.9
OIOIO\; IClt) 5 1.8
Typhoid 2 0.8
Inf<Jlllilc Measles I 0.4
J. Cryptogenic 71 27.2
~ Congcnitltl Ear \Ialformation 22 85
External c::tr 1l1<llformatlon 19 7.3
Middle car malformation 3 1.2
Total 261 100.00
I. Non-genetic group (n=44) was further sub
classified into 3 main categories depending upon time
ofexogenous msult to auditory apparatus which may be
anlenata!. pennatal or Immediate post natal period
extending till 6 months of age.
la) Prenatal group (n=6) : This included 5 cases of
congenItal rubella and in one case, Ihe mother had
uncontrolled tuberculosis during pregnancy. Serology
lias possible 10 only two cases, while in resl of three
cases. no serology was advised due to late presentation.
'<0 case of congennal CMV could be diagnosed because
oflaler presentation of cases as serology in diagnostic
only," first 3 weeks of life (7).
Vol. 4 No.3. July-Seplember 2002
(b) Perinatal group (n= 12) : It mcluded three cases
of neonatal jaundice, nine cases of birth anOXia and
prematurity (Birth weight < 1500 gm.) BOlh the factors
i.e. birth anoxia and prematurity, were grouped logether
because of small sample and both are known to
supplement each other in causation of hcaring
impairment (8).
(c) Immediate postnatal causes (n=26) : This group
included cases ofpostnatal causes which were presumcd
to have acted upon during firsl 6 months of hfc. These
included one case of infan:ile measles. IwO cases of
typhoid fever. five cases of ototOXIC drug
(aminoglycosides) intake and remaming 18 cases with
history of neonatal meningitis. The causallve organIsm
was tubercular bacilli in t patient, pneumococcal 10 3
patients, while in remaining 14 pallents no defi11lte
causative organism was found.
2. Genetic factors (n=24) were further subclassi eied
as shown in Table I.
(a) Auto~omal dominant (n=26) : It mcluded 4 cases
ofnon-syndromal inheritance and 22 cases with specilic
syndromes. It included 7 cases or Waardenburg's
syndrome, 6 cases of Treacher-collms syndrome. 4 or
Alport's syndrome, 2 of Crollzon 's syndrome and one
with Apert's syndrome. Two patients had associated
malformations not fittmg mto any known syndrome. It
included one remale patient with associated upper limb
malfornlation and bilateral conductive heating loss. while
in another patient. bilateral conductive heaCing
Impairment was associated with OptiC atrophy and
velopharyngeaI incompetence, both showmg autosomal
dommant pattern of inheritance.
(b) Autosomal recessive (n=77) : It Included
two cases of Usher's Type I syndrome and rest 75 of
non-syndrome hearing loss. No case or Pendred's

" JK SCIENCE
syndrome or Jervell and Lange Nielson syndrome was
detected.
(c) X-linked inheritance (n=l) : The present study
included one case ofHunter's syndrome with moderately
severe mixed hearing impainnent.
(d) Multi Factorial inheritance (polygenic group)
(n=15) : It included II cases ofcraniofacial microsomia,
one ofCharge association and 3 patients ofKlippel-Feil
syndrome.
(e) Chromosomal group (n=2) : Included one case
of Turner's syndrome (moderately severe conductive
hearing impainnent) and one case ofDown's syndrome
with severe sensory hearing loss.
(I) Unclassified association (n=3) : It included two
female patients with associated congenital heart defects,
one had atrial septal defect and pulmonary stenosis with
moderate conductive bilateral hearing impainnent. The
other had ventricular septal defect with severe SNHL
and an epileptic focus on EEG. The third case had
associated microcephaly, syndactyly and mental
retardation with severe hearing impainnent.
3. Congenital Ear Malformations (n=22) :
It included 19 cases ofexternal ear malfonnation and
3 cases of isolated middle ear malfonnations. External
ear anomalies included 9 cases ';;ith bilateral and 10 with
unilateral involvement (7 with right side and 3 with left
side involvement). The 3 cases of isolated middle ear
malfonnation were taken up for middle ear exploration
and the findings were:
~ Body ankylosis of Malleus and Incus in first case.
- Absence oflong process of Incus withabsent stapes
suprastructure and narrow oval window niche in
the second case.
139
In third case, stapedius tendon was absent with
malfonned stapedial crura.
4. Unknown aetiology (crypotogenic group)
(n=71) :
There were 71 cases where the history. laboratory
and other evidence could not identify the precise
cause of the hearing impairment to any of the
preceding aetiological factors. In this group. 5 cases
which had more that two possible causes of hearing
impainnent, were included as per Rijn and Cremer's (4)
guidelines, while in rest 66, possible aetiology could be
ascribed.
Sex Ratio
The present study of 261 cases consisted of 165
males (63.2%) and 96 females (36.8%) with male
preponderance of 1.72 : I. Table 2 shows a marked
preponderance of males in the postnatal, Mendelian
single gene inheritance group and cryptogenic group
while preponderance of females in multifactorial and
chromosome abnonnalities group.
Audiological Assessment of the Study Group
Two hundred and ten children cooperated for pure
tone audiometry. Results from free-field tests
supplemented by BERA were available in 44 children.
In remaining 7 children: results were inconsistent and
till the tennination of our study, no consistent response
was found ever on BERA te.ting. Four patients had blank
audiograms (no response to any frequency). It included
3 cases ofgenetic deafness (Waardenberg' s syndrome =
I and craniofacial microsomia"" 2) and one case of
cryptogenic deafness.
Air conduction threshold of these patients were
categorised according to severity of hearing impairment
Vol. 4 No.3. July-September 2002

_____________~,JK SCIENCE
mto 5 groups as per Kemker's (9) criteria. The results
were as per Table 3. There was an overall male
preponderance in all categories of hearing loss.
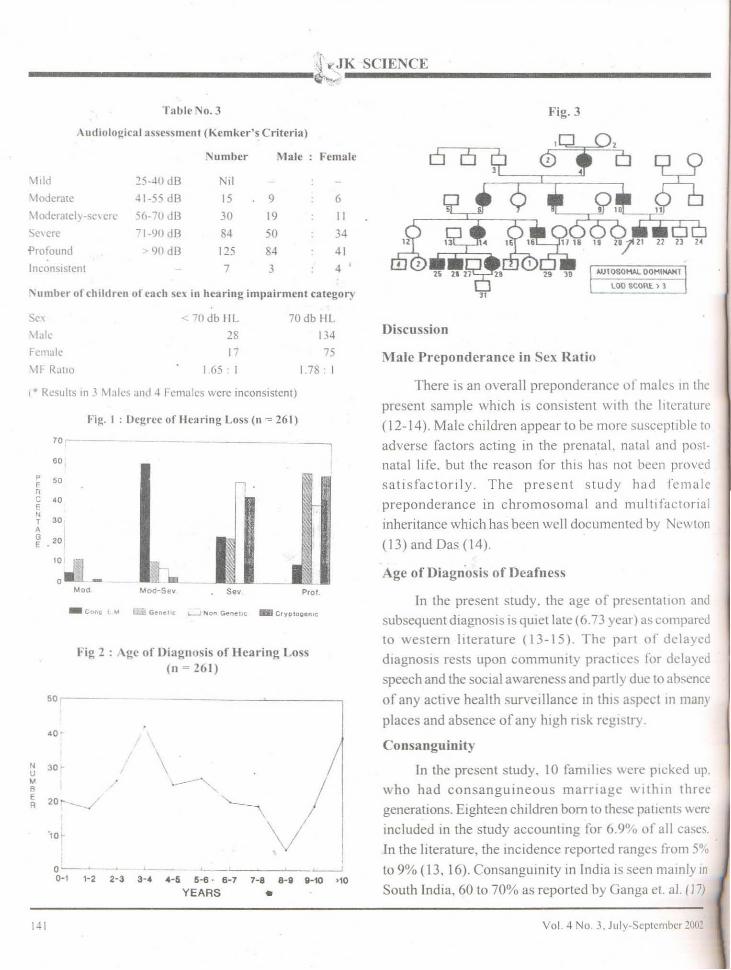
The degree of hearing impairment in each category
,elalive to the aetiology of hearing' impairment was.
observed as shown in Fig. I. With maximum number of
cryptogenic and genetic cases with severe to profound
,earing loss.
\ge of Diagnosis of Hearing impairment:
In the present study, the age of presentation
"d subsequent diagnosis was variable, the range
being from less than I month to 22 years (mean age =
6.73 years) as shown in Fig. 2. 40.5% of
cases presented before 4 years of age with peak at
fourth year (16%). The range of age group when the
parents suspected the hearing impairment was right from
birth due to presence of congeni)al external ear
malformations to as late as 16 years (mainly in females
of marriageable age desirous ofearly tTeatment). In 242
cases the mean was 2.54 years (insufficient data In
19 cases).
Linkage Analysis:
18 family pedigrees were studied out of which
four were selected for linkage analysis (3 of
autosomal recessive and one of autosomal
dominant inheritance). Only the pedigree of autosomal
dominant inheritance generated LOD (log of odds)
score of 3 or greater 72.8% of the times (Fig. 3)
while 3 autosomal recessive families were not
good enough to generate signi ficant linkage data.
This analysis was done at National Institue of
Deafness and other Communication Disroders
(NIH), USA on SLINK programme for Linkage
Analysis (10, II).
Table No. 2
Sex distribution in relation to aetiology of hearing impairment
Sex
\tale
Female
\1F Ratio
In Genetic Group:
Genetic
. 73
51
1.43 : 1
Non genetic Cryptogenic Congenital Earmalformations
29 45 t 8
15 26 4
1.93 : I 1.73: I 4.5 :
Sex
Male
Female
MF Ratio
AutosomalDominant
19
7
2.71 :
AutosomalRecessive
48
29
2,52: I
Multifactorial
4
11
0.36: 1
X-linked Chromosomal
2
Unknownassociation
2
0.5 : I
In non-genetic group:
\1alc
Female
MF Ratio
Prenatal
3
3
I: I
Perinatal
6
6
I: I
Postnatal
20
6
3.3 :
Vol. 4 No.3, July-September 2002 140
JdK SCIENCE---------~~~
Tablr No.3 Fig. 3
Audiologic:'lJ assessment (Kemker-'s Criteria)
Number Male Female
\111d 25--10 dB il\1odcralc ~1-55 dB 15 9 6
\ 1odcrarcl\-sc\ CIT 56-70 dB 30 19 IISC\ ere '1-90 dB 84 50 34
'Profound <)0 dB 125 84 41
Inconsistent 7 3 4 '
"umber of children of (':!ell sex in hearing impairment category 11
MJTOSOMAl OOMINAHl
LOO SCORE.) 1
50r,--
\* Results In J Males and ~ Females were inconsistent)
Discussion
In Ihe present study. the age of presentatIOn and
subsequent diagnosis is quiellate (6.73 yem) as comparedto western literature (13-15). The part of delayed
d,agnosls rests upon community practices lor dclayed
speech and the social awareness and partly due to absence
of any active health surveillance In th,s aspect In many
places and absence of any high risk reg'stry.
Consanguinity
In the present study, 10 families were plckcd up.
who had consanguineous marnage wlthll] three
generations. Eighteen children born to thesc pallcnts were
included in the study accounling for 6.9% of all cases.
In the literature, the incidence reported ranges from 5°'0
to 9% (13, 16). Consanguinity in India IS seen mainly In
South India, 60 to 70% as reported by Ganga el al. (J 7)
Age of Diagn·osis of Deafness
M ale Preponderance ill Sex Ratio
There is an overall preponderance of male, 10 the
present sample which is consistent with the literature
(12-14). Male children appear to be more suseepllble to
adverse factors acting in the prenatal. natal and posl
natal lifc. but the reason for this has not been proYcd
satisfactorily. The present study had female
preponderance in chromosomal and multi factorial
inheritance which has been well documented by Newton
(13) and Oas (14).
Prols••
• Gene'" ~ Non Genel"; _ C'Ylllooen,c
Fi~. I : Uegrec of IIcal"ing Loss (n -= 261)
Fig 2: \gc of Di~lgnosis of Hearing Loss(11~261)
70-
'0,
50FRC '0ENT 30A
201GE
10
0MOd
_ Con, I loA
'o-
N 30·UM
~ /BE
20___..../ ~R ,
V'lOt-
,0-- ~ -'---'0-' '-2 2-3 3-' .-. 6-6 . 6-7 7-8 a-. ,HO "0
YEARS •
Sex ~ 70db HL 70 db HL
\Ialc 28 134
Female 17 75
\IF- RJtlO I 65 I I. 78 I
I~ I Vol. 4 No, 3, July·Scptcmbcr 2011!

_____________.;~~K SCIENCE
and RajInder Kumar (18) and in Muslims. Our study
sample maInly had cases from North and West India
thereby It had relaltvely small sample ofconsanguinity.
Aetiology
(a) Genetic Group
The modcs of Inherited deafness in the present
study are comparable to the various studies in the
literature like Rijn and Cremers (4), Elango (7),
Felnmesser (16) and Fraser (19), all revealing
predomInance ofautosomal recessive inheritance except
studies by ParvIng (20) and Ruben and Ruzycki (21)
with significant autosomal dominant inheritance.
(b) :"on-Genetic Group (n=44)
I. Prenatal group (n=6) : There were five cases
ofcongcnital rubella in the present study. In the Western
literature, It vanes li-olll < 7% in non-epidemic years
( 19) lO about 60",,, 111 epidemic years (22).
2. Periuatal causes ('1=12): (a) Neonataljaundice
(n=3. 1.1'5%): The proportion of neonatal jaundice in
the present study "as very small as compared to the
western literature which varies from 4.5% to 15% (13,
14: 16.23.24).
(b) Birth anoxia and prematurity (n=9): There were
nme cases (3.5%) ofbirth anoxia and prematurity group.
In the literature. \'anous studies have shown different
tigures "arylng from 1'10 to IS"!., (5-7,16.25).
3. Postnatal causes (n=26) : The present study
re\t~aledmeningitis as 1110St common calise of postnatal
hearIng loss whIch IS well documented In the literature
by varIOUS authors (4.7. 12, 13. 15).
In the Iilerature the percentage of non-genelic
group vanes from 17 lYo to 75% (maximum studies have
quoted 30°,,, to 40%) (5. 13. 16. 26). 'In this study the
relaltvely few cascs of nongenetic congenital and early
acquIred group (16.8%) as compared to genetic and
cryplOgeolc group IS not m agreement with the literature.
ThIS may be due to 1I1cluSlon of the congemtal and early
acquired group (within 6 months postanatal) excluding
Vol. -l '\'0. 3. JlIly~Scplclllbcr 2002
all other acquired causes in this study. Also other possible
explanation in the referral system \\ here multiple
handicapped dcaf children are rcferrcd directly to
rehabilitation departments and special c1illlcs tor mentally
retarded. Also due lO lack of "High RIsk Registry", lh~
cases are not referred for subsequent screen1l1g and
. management. Due to lack of good Infrastructure at
peripheral level. increased mortality in acquired group
results in less number ofsurvivals to present subscquentl,
seeking advice for deafness. Also large number ofstud Ie,
in the literature havc included maInly the posllmgual
deafness and therefore the subsequcl1l Increase In the
percentage of nongenetlc acqll1red causes as compared
to the present study.
Cryptogenic Group (unknown cause) (n=71) (27.2'Yo,)
In various studies in literature. thc cryptogenic
group has been reported from as 10\\ as 10% 10 ahout
60% (average 400/0) whIch 15 well III accordance \\'Ith
the present study (5. 13. 15.26,27).
Congenital Ear Malformations
The present study included 22 (8.5"'0) cases 01
external ear malformations with 19 cases or ntemal
auditory canal atresia and thrce cases of lsolat~d
congenital middle ear pathology which IS driTerent li'om
the figures reported in literature Val) IIlg li'om 211II to -lu."
(19.23.28.29).
Conclusion
In this study. the mcan age 01' prcs~n,"llon and
diagnosis of hearing loss was 6.73 years. [hc ~encllc
aetiology was found to be most C0I111110n calise (-17.5 11n I
followed by cryptogcnic (27.2",,) and nOll-genctlc
(16.8%) of the congenital and early acqUired dcali,c".
Autosomal recessive mode of InhcrJlanCl' \\ a") ..... l'1'1l 1110 ..... 1
commonly (62%) followed by autosomal domll1ant (2()""j
in the gcnetic group. Maternal rubella lIlJectlnn \\as the
most common cause of prenatal de3fl1es~ \\-hllt'
perinatally birth anOXia and prematuntv \\cre common
Post natally the menlllgitis and OlOlO'IClt) '\ere morc
common.

______________~K SCIENCE
The pre,cnt siudy being a preliminary study
conducted at a tertiary centre. has its own bias. merits
and dement' bUI docs reflect the need of 'Higb risk'
registry mamtenance at alilhe peripheral hcalth centres
\\ nh active sun edlance and subsequent screening for
early detection ofheanng loss.
I~cfcrcnces
"'Jallonal Sample SlIt"\ey of Disabled persons in India. Censusof IndIu ( ll)~ I ), Registrar General. GO\t. of India. Ministry ofHome .\ fL.lll"s
2 IC\1R (19~31ColL.l.horatl\ c study In prevention and actlOlog)'of hcanng Imp.lIrmCllI Publ IndIan Council of MedIcalRcsc<.lrch and Dcp•.lr1ll1cm of SCIence and Technology, Nc\\Deihl
Pal J. I1hatw Ill .. Prasad BG. Dayal D, J,1I11 Pc. Deafnessamong [he UrhJll cornrlllllty An cpidcnllologlcal sur\'CY a1Lud,nO\\ (L PI /I/(( J .\/£'d Res 1974: 62 857-68.
~ R1JIl \ and Crcl11crs. Causes of childhood deafness at a Dutchschool for the heanng Impaired ·11111 {)Iol Rhmol Larmgol
199\ . 1110 903-0.
Fraser LJR Profound chddhood deafness. J Med CelleJ
191>4'.1 Ilb-151
6 ray lor IG. Illne \\ D. I3rasler VJ eJ al .A study of the causes
of heanng loss In J population of deaf children with speCial
reference to genetic factors. J Laryllgol 0101 1975 : 89
899-914
7 Elango S. Actlology of deafness III children from a school for
the deaf 111 \<1<1laY51'1. 1111.1 Pedwlr Olorhinolarl"llgol 1983 :17 21-17
0; Hall·Jonl:s J Congenital deufness. The aetiology and
management of 100 cases. .I 1.1I1TIIl!ol Orol 1970 . 84I () U':!(,
9 Kcmkcr I·J, ( ·lassll1cJtlon ofaudllory ImpalmlCnl. Orolan'l1xol
CIII/vo/" /11/ 1975.86 3·17.
1() 011 J Computcr sll11ulatlon methods in human lmkage analysis.l'meNClI! /('(/(!,';("/ (1.<.,'/1 1989: 86: 4175-78,
11 Weeks Dl:. Ott J. Lathrop G\1 SLINK A general stimulationprognllll for linkage analysls . .-Jm J HUIJI Gellel 1990.47 (3)A 2114 ISupp!. )
11. 'vtarlln JAM Aetlological factors relatlllg to childhood
deafness III the I--uropean community. Audiology. 1981: 21 .
149-58.
1.', Newton VE. Aetlologyofbllaler;J1 senson-neurul heanng loss
1Il young children..! Larl'lIgo! Olnl (.S'/IPP! ) ll)k~ . 10 : 1·57.
14 Das VK. AetIOlogy of bilateral sensormenml deafness In
children. J I.arn/gol 010! 1968 . 101 ( I I ) . 97S·!'\O
IS, Kankkunen A Pre·school children \\ lIh Impaired heanng In
Goteborg 1964-1980. l{"fa-OIOlarl'lI}!ol (Suppll (S(o{M,)
1982 : Suppl. 391
16, FelnmesserM. Tell L, Le\l H. EtIOlogy ofchildhood dearness
with reference to the group of unknown cause. IllIdlO!OJ:\
1986 : 25 . 65-69.
17 Ganga N, RaJOIgopal B, RanJendran S el III. Deafness In
children an analYSIS. Ind Pedlar/" 1991 . 18 27.~·7(1
18. RaJJnder Kumar PV A study on the inCidence and aCl1olog~
of deafness In a South Indian Population lIul JOwl 11)74
26.153-57
19 FraserGR. Causes of profound deafness In childhood A stud~
of 3535 indl\'lduals With se\ere heanng loss present at blrlhor of childhood onset John Hopkl1ls Unl\Crslt\ Pres~,
Baltimore. USA. 1976
:!O. Pan Ing A Epidemiology of heanng loss and aCllologlCadiagnOSIs of heanng Irnpalflnent III childhood !III.I P{,d,atr
OJorhlllolar.l'lIgol 1983 . 5 : 151 ·56
21. Ruben RJ and RozyckI DL. Clinical aspects of genetic
dcafness. AIIII Oro! Rhillo! Larrllgo! 1971 : SO 15:'-63
22. Gumpel SM. Hayes K. Congenllal perceptl\'c deafness. Roleof Intrauterme rubella. IJr Aled J 1971 ; 1. 300·04
23, Fowler EP ~ JR and Sasck \i1 Causes of deafness In young
chlldrcn. Arch Ololarl'lIgoll954. S9: 476-84
24, Holten A and Parvmg A. ACllology of hearing dIsorders In
children III Ihe school for the deaf. !lIr ./ Pedillir
Olorhillolan'IIKol 1985 ; 10: 229-36
25 Gra} RF Causes ofdeafness III schools ronhe deaf In \ladras
1111 J PedlOtr Otorhlllolarrngo! 1989 • 18 97-106
26 Pabla liS. Me Cormick B, Glbbln KP !m.l P{,dlU(r
OforlllllolarJ'lIgol1991 : 12,161-165.
17 Parvmg A. AetlOloglcal dIagnOSIs m heanng Impmred chlldren
clinical value and application of a modern exar11lnal1on
programme. 1111 .J I'('diarr OlOr!lIlIolal'l'lIgo! 19847; 29-38.
18 l30rdely JE and Hardy WG The cllology or deafnessyoung children. Acta Ola!aryngol (Slock) 1951 40 -2--1)
29 Zondermon B. The preschool nerve deaf chJld. 1.llntl,..,CfJ!-.w;)"
1959 ; 69 54-89.
Vol. 4 1\0 J. Jllly-Scplcmbcr ~(~