A “special protocol” for the local treatment of full-thickness burns. Author :Anemona-Madalina...
20
A “special protocol” for the local treatment of full-thickness burns. Author :Anemona-Madalina Stana Coordinator: Adrian Botan MD, PhD, Senior Consultant Plastic Surgeon & Chief, The Burn Centre & Plastic Surgery Department of Targu-Mures County Hospital.
-
Upload
gilbert-dickerson -
Category
Documents
-
view
214 -
download
0
Transcript of A “special protocol” for the local treatment of full-thickness burns. Author :Anemona-Madalina...

A “special protocol” for the local treatment of full-thickness burns.
Author :Anemona-Madalina StanaCoordinator: Adrian Botan MD, PhD, Senior
Consultant Plastic Surgeon & Chief, The Burn Centre & Plastic Surgery Department of
Targu-Mures County Hospital.

INTRODUCTION
Thermal burns are produced by open fire, electric flames, boillings liquids or the contact with hot objects. Full-thickness burns are those lesions involving all skin structures. Skin layers transform into a leathery, dry eschar, so the only adequate treatment is the excision of the eschar as soon as possible and skin grafting of the
remaining defect.

MATERIAL AND METHOD
This paper presents only 2 cases with full-
thickness burns selected from the period between 2011-2013; the other 15 cases with deep burns admitted in the above mentioned period have been treated by the same protocol, so any statistic analysis is difficult.
In the Burn Centre of Targu Mures (due to the ‘local conditions‘ in this medical unit) in the last 15 years has been used a ‘special protocol’ which is a mixture of early sharp debridement combined with autolytic debridement that remove the burn eschar and obtain an
adequate granulation for skin grafting.

CASE NR. 1
60 year old male patient with full-thickness burn of the posterior trunk and arm. Initial aspect on the admission in The Burn Centre.

Figure nr. 2
Early tangential excision of the burn eschar using a manual dermatome.

Figure nr. 3
A thin layer of the full-thickness eschar still remains attached to the substrate thus preventing unnecessary excision of healthy tissue and possible brisk bleeding.

Figure nr.4
This remaining eschar is removed step by step using different synthetic dressings (such as Ligasano PUR-foam dressings) which stimulate the natural autolytic debridement.

Figure nr. 5
One can see that on behalf of synthetic dressings, sloughs, fibrin, deposit and exudate are slowly removed.

Figure nr. 6
2 to 3 weeks later a very good granulation bed is obtain.
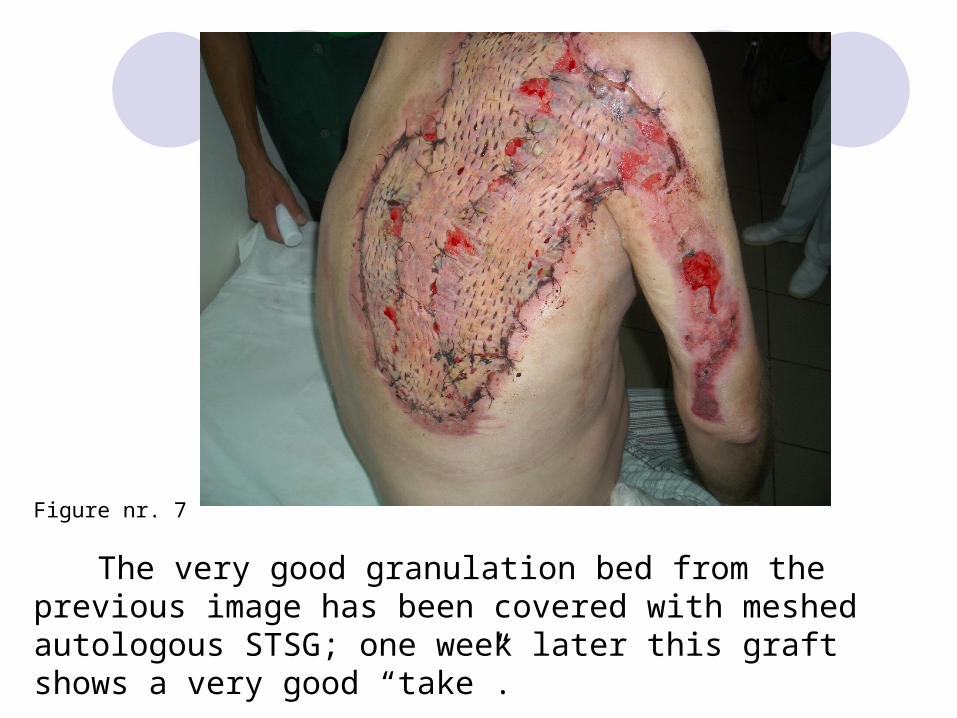
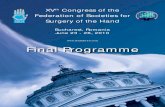
Figure nr. 7
The very good granulation bed from the previous image has been covered with meshed autologous STSG; one week later this graft shows a very good “take”.

Figure nr. 8
One month later the full-thickness burn is completely healed with no morbidity on the donor site. This patient had a follow-up for about 3 months and he has no more come for routine control.

CASE NR. 2
19 years male patient with a full-thickness flame burn of the posterior trunk and buttocks.
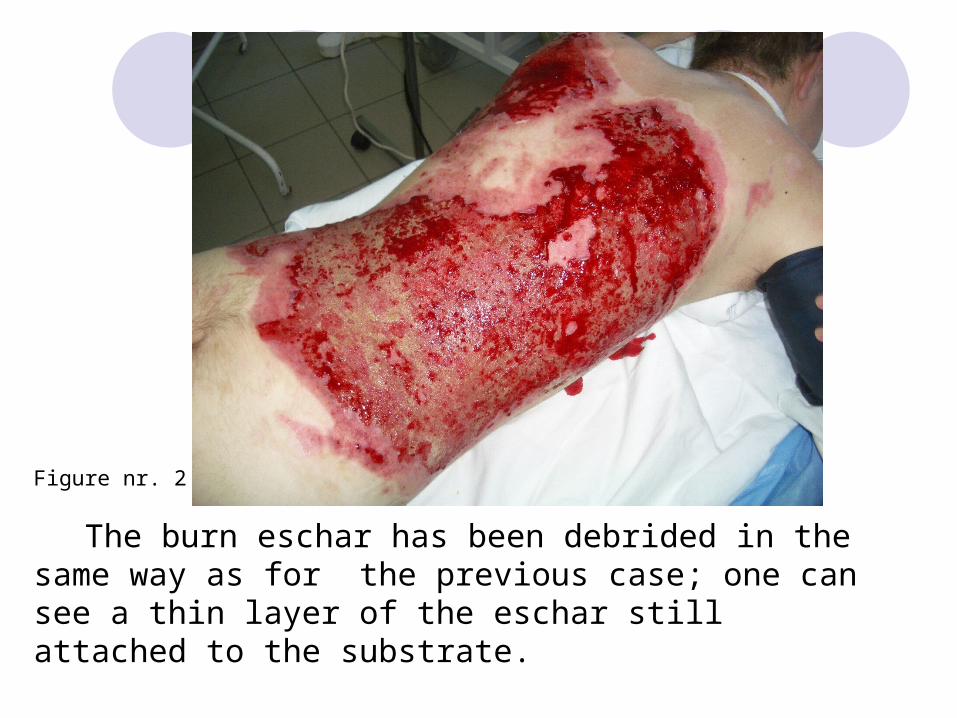
Figure nr. 2
The burn eschar has been debrided in the same way as for the previous case; one can see a thin layer of the eschar still attached to the substrate.
Figure nr. 3
The large defect of the posterior trunk has been eventually covered with meshed autologous STSG harvested for the posterior aspect of the lower limbs.

Figure nr. 4
Close intra-operative aspect during grafting showing the perforations into the graft sheets, allowing blood and exudate to drain from the space between the graft and the granulation bed thus improving early graft revascularization.
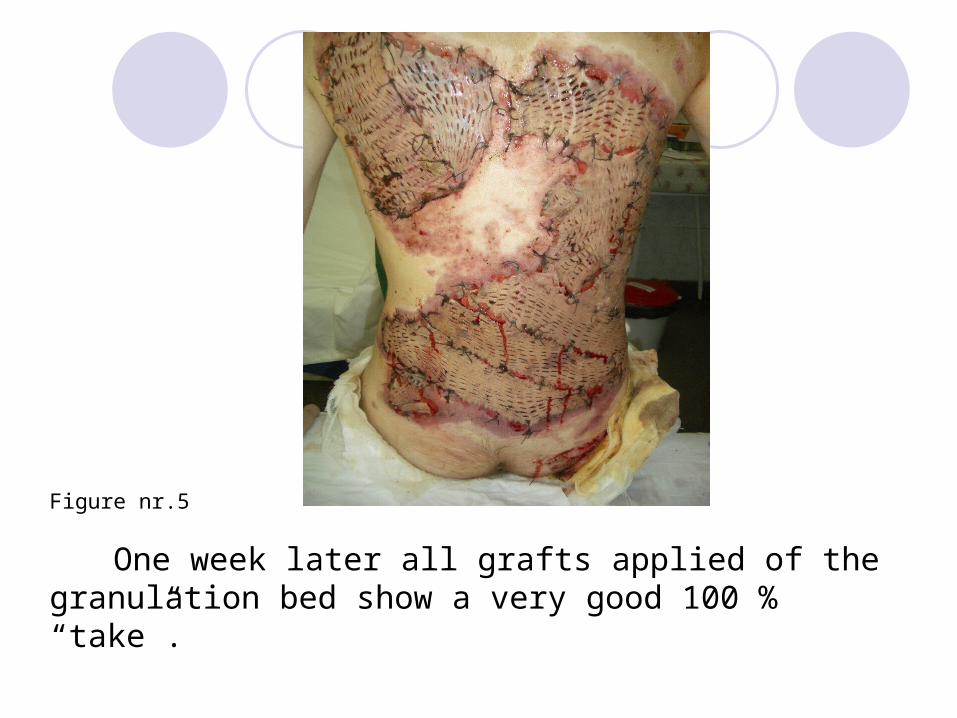
Figure nr.5
One week later all grafts applied of the granulation bed show a very good 100 % “take”.
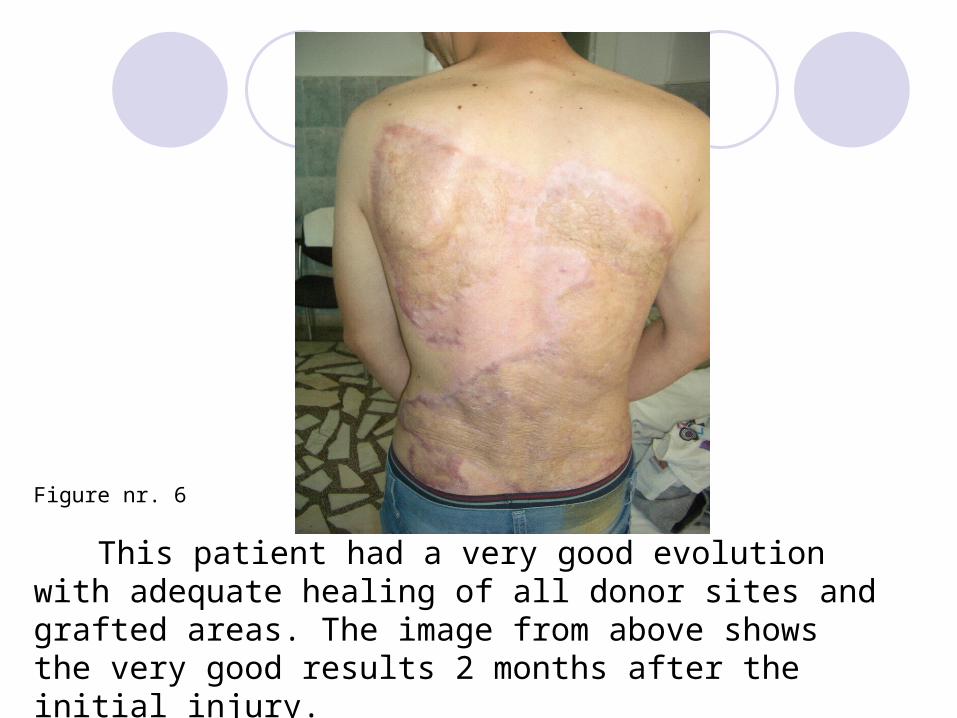
Figure nr. 6
This patient had a very good evolution with adequate healing of all donor sites and grafted areas. The image from above shows the very good results 2 months after the initial injury.

RESULTS AND DISCUSSIONS
This incomplete tangential excision of the burn eschar gave very good results. The thin layer of eschar remaining at the end of the sharp debridement prevents the accidental removal of healthy tissue avoiding the brisk bleeding requiring blood transfusion. Complete removal of the burn eschar and adequate wound bed preparation followed by early cover with STSG is the only way to prevent early and late complications of full-thickness burns.

CONCLUSIONS
The surgical procedure mentioned above is a
cheap, safe and easy way to achieve the goals mentioned at the beginning of this paper, thus avoiding all major early and late complications which could follow more aggressive surgery.

THANK YOU FOR YOUR ATTENTION !