A SingHealth Newsletter for Medical Practitioners MCI (P ... · In short, early reper - fusion can...
11
OCT-DEC 14 www.singhealth.com.sg SingHealth Academic Healthcare Cluster • Singapore General Hospital • KK Women’s and Children’s Hospital • Sengkang Health • National Cancer Centre Singapore • National Dental Centre of Singapore • National Heart Centre Singapore • National Neuroscience Institute • Singapore National Eye Centre • SingHealth Polyclinics • Bright Vision Hospital A SingHealth Newsletter for Medical Practitioners MCI (P) 057/11/2014 Time is Brain Mechanical Clot Retrieval for Acute Ischaemic Stroke Parkinson Disease and Related Disorders Pituitary Tumours Focus: Neurology
Transcript of A SingHealth Newsletter for Medical Practitioners MCI (P ... · In short, early reper - fusion can...

Oct-Dec 14 www.singhealth.com.sg
SingHealth Academic Healthcare Cluster• Singapore General Hospital • KK Women’s and Children’s Hospital • Sengkang Health • National Cancer Centre Singapore • National Dental Centre of Singapore
• National Heart Centre Singapore • National Neuroscience Institute • Singapore National Eye Centre • SingHealth Polyclinics • Bright Vision Hospital
A SingHealth Newsletter for Medical Practitioners MCI (P) 057/11/2014
Time is BrainMechanical Clot Retrieval for Acute Ischaemic Stroke
Parkinson Disease and Related Disorders
Pituitary Tumours
Focus: Neurology

32
Oct-Dec 2014
thrombolytic therapy. It offers the ad-vantages of ‘getting directly at the clot’ and at the same time not delaying clot dissolving therapy and importantly not compromising the risk of haemorrhage.
At the National Neuroscience Institute (NNI), in line with the national effort to minimise the impact of stroke disability and mortality, mechanical thrombec-tomy for acute clot retrieval was made available as an adjunct to medical intravenous/intra-arterial lytic therapy since 2007.
Over the years, the experience with mechanical methods of clot retrieval has matured and NNI has grown to be the largest cen-tre to offer this service in Singa-pore.
How iS iT DoNe?Retrieving an acute clot in the brain vessel is like clearing a blocked pipe. Various mechanical approaches have been used alone or in combination with adjuvant intravenous or intra-arte-rial rTPA (recombinant tissue plasmino-gen activator).
Time is BrainMechanical Clot Retrieval for Acute Ischaemic Stroke
Dr Wickly Lee, Senior Consultant, Department of Neuroradiology, National Neuroscience Institute
wHaT iS iScHaemic STRoke?To put it simply, ischaemic stroke is caused by a sudden critical reduction in blood supply to the brain, resulting in brain tissue death. Following the oc-clusion of an artery, the brain tissue, supplied by that artery, begins a pro-cess of cell death within minutes. This starts with an inner ‘core’ of infarcted tissue and is surrounded by tissue that is initially only functionally impaired.
If blood supply can be restored early, the functionally impaired tissue can be ‘rescued’, thereby minimising the eventual damage. In short, early reper-fusion can salvage those cells at risk from critical hypo perfusion.
wHY mecHaNical TReaTmeNT aPPRoacH?Mechanical treatment methods for acute ischaemic stroke result in fast and efficient reperfusion with short procedure times and high recanalisa-tion rates, thereby extending the treat-ment window.
Mechanical clot retrieval devices have, in recent years, played a greater role in the treatment of acute ischaemic stroke by providing a ‘bridging strategy’ be-tween intravenous and intra-arterial
Mechanical devices of different designs can be classified by the basic working principles into two major approaches: proximal and distal thrombectomy.
Devices deployed proximal to the clot works by ‘disruption-suction’ and those devices deployed at or distal to the clot work by ‘catch-retrieval’. Over the years, improvements made in designs of these mechanical devices have greatly improved their clot re-trieval ability.
At NNI, a combination of me-chanical techniques is tailored to each individual patient, depend-ing on the situation encountered. By and large, the ‘catch-retrieval’ technique is favoured for larger clots located in a more proxi-mal vessel and the ‘disruption-suction’ technique reserved for smaller clots locally in more dis-tally located vessels.
Through a right groin femoral artery puncture, a catheter is navigated into the vessel of interest and the mechani-cal device will then be introduced through the catheter to engage the
Ischaemic stroke is one of the leading causes of disability and mortality in the world. At pres-ent, medical intravenous thrombolysis is the only approved treatment for this devastating dis-ease with a narrow therapeutic window of up to 4.5 hours after symptom onset. Beyond this crucial window, success rates for dissolution of clots in the brain drastically fall as the risk of haemorrhagic complication from thrombolytic therapy outweighs its benefit. In patients with large vessel occlusions due to a large clot, the chances of clot clearance is even lower.
Clot retrieval devices now play an important role as a bridging strategy, extending the thera-peutic window for treatment up to 8 hours, circumventing the problems of haemorrhagic risk as well as large clot burden at the same time.
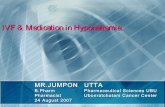
Figure 1 Unenhanced axial CT scan demon-strates no evidence of hypodensity or intra-cranial haemorrhage.
Figure 2A and 2B showed restriction diffusion on MRI DWI scan confirming the presence of an acute infarct in the right striatocapsular-corona radiata corresponding to right MCA territory stroke.
A
B
Figure 3 MR angiogram showed abrupt ‘cut-off’ with no flow signal seen distal to the mid-right MCA M1 segment indicating the site of acute thrombus causing the occlusion.
Figure 4 Digital subtraction angiography (DSA). Right internal carotid artery (ICA) angiogram demonstrates the site of acute occlusion from thrombus at right MCA M1 corresponding to MR angiogram finding.
clot. Once the device is deployed in place, the retrieval process begins and the clot pulled through the catheter.
caSe STuDYMrs LJA is a 73-year-old lady with past medical history of asthma, mitral regur-gitation and hypertension. One after-noon at 16:00hrs, after using the toilet at home, she presented sudden onset of left upper and lower limb weakness associated with slurring of speech, which her grandson spotted.
She was sent to the emergency de-partment at Tan Tock Seng Hospital (TTSH) and was examined by neurolo-gists from the NNI at 16:41hrs. She was noted to be fully conscious with a Glasgow Coma Scale (GCS) score of 15 but was found to have profound loss of left upper and lower limb power with grade 0 strength (Medical Research Council grading 0-5). She was imme-diately diagnosed as having suffered from an acute ischaemic stroke.
An emergent CT brain scan was per-formed to rule out the possibility of a haemorrhagic stroke (Figure 1), fol-
lowed by a MRI scan, which showed acute infarct in the right striatocapsule-corona radiata (Figure 2A and 2B). The MRA revealed loss of flow signal in the right middle cerebral artery M1 seg-ment consistent with acute occlusion by thrombus (Figure 3).
Intravenous rTPA 5.9 mg was given at 17:46hrs and it was decided that mechanical thrombectomy should be performed, in view of the large clot burden in the proximal right middle cebrebral artery (MCA) M1 segment.
She was transferred immediately to the Angiography Suite and put under gen-eral anaesthesia. Based on the vascular information obtained from the MR an-giography, an 8F balloon guide cath-eter was placed directly into the right internal carotid artery (ICA) and the ini-tial angiographic injection confirmed the site of occlusion (Figure 4).
NeurologyFocus: medical update
appointments: 6357 7095 email: [email protected]

54
Oct-Dec 2014
coNcluSioNThe present case illustrates the efficacy of treating patients with large vessel stroke with a retractable stent used as a clot retrieval device. It permits fast deployment and recanalisation of the occluded vessel, therefore making me-chanical methods a promising adjunct to current medical intravenous/intra-arterial thrombolysis.
ReFeReNceS
1. Bergui M, Stura G, Daniele D, et al. Mechanical thrombolysis in ischemic stroke attribut-able to basilar artery occlusion as first-line treatment. Stroke 2006;37:145e50.
2. Brekenfeld C, Schroth G, Mordasini P, Fischer U, Mono ML, Weck A, et al. Impact of retrievable stents on acute ischemic stroke treatment. AJNR Am J Neuroradiol. 2011;32:1269–1273.
3. Broderick JP, Palesch YY, Demchuk AM, Yeatts SD, Khatri P, Hill MD, et al; Interventional Management of Stroke (IMS) III Investigators. Endovascular therapy after intravenous t-PA versus t-PA alone for stroke. N Engl J Med. 2013;368:893–903.
4. Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C, et al. Intra-arterial prou-rokinase for acute ischemic stroke. The PROACT II study: a randomized controlled trial. Prolyse in Acute Cerebral Thromboembolism. J Am Med Assoc. 1999;282:2003–2011.
5. Hacke W, Kaste M, Bluhmki E, Brozman M, Dávalos A, Guidetti D, et al; ECASS Investi-gators. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359:1317–1329.
6. Khatri P, Abruzzo T, Yeatts SD, Nichols C, Broderick JP, Tomsick TA; IMS I and II Investi-gators. Good clinical outcome after ischemic stroke with successful revascularization is time-dependent. Neurology. 2009;73:1066–1072.
7. Kidwell CS, Jahan R, Gornbein J, Alger JR, Nenov V, Ajani Z, et al; MR RESCUE Investiga-tors. A trial of imaging selection and endovascular treatment for ischemic stroke. N Engl J Med. 2013;368:914–923.
8. Levy EI, Mehta R, Gupta R, et al. Self-expanding stents for recanalization of acute cere-brovascular occlusions. AJNR Am J Neuroradiol 2007;28:816e22.
9. Mazighi M, Serfaty JM, Labreuche J, Laissy JP, Meseguer E, Lavallée PC, et al; RECANA-LISE investigators. Comparison of intravenous alteplase with a combined intravenous-endovascular approach in patients with stroke and confirmed arterial occlusion (RECA-NALISE study): a prospective cohort study. Lancet Neurol. 2009;8:802–809.
10. Mordasini P, Frabetti N, Gralla J, Schroth G, Fischer U, Arnold M, et al. In vivo evaluation of the first dedicated combined flow-restoration and mechanical thrombectomy device in a swine model of acute vessel occlusion. AJNR Am J Neuroradiol. 2011;32:294–300.
11. Nogueira RG, Lutsep HL, Gupta R, Jovin TG, Albers GW, Walker GA, et al; TREVO 2 Trial-ists. Trevo versus Merci retrievers for Thrombectomy revascularisation of large vessel oc-clusions in acute ischaemic stroke (TREVO 2): a randomised trial. Lancet. 2012;380:1231–1240.
12. Nogueira RG, Yoo AJ, Buonanno FS, et al. Endovascular approaches to acute stroke, part 2: a comprehensive review of studies and trials. AJNR Am J Neuroradiol 2009;30:859e75.
13. Saver JL, Jahan R, Levy EI, Jovin TG, Baxter B, Nogueira RG, et al;SWIFT Trialists. Solitaire flow restoration device versus the MerciRetriever in patients with acute ischaemic stroke (SWIFT): a randomised, parallel-group, non-inferiority trial. Lancet. 2012;380:1241–1249.
14. Smith WS, Sung G, Saver J, Budzik R, Duckwiler G, Liebeskind DS, et al; Multi MERCI Investigators. Mechanical thrombectomy for acute ischemic stroke: final results of the Multi MERCI trial. Stroke. 2008;39:1205–1212.
15. Smith WS, Sung G, Starkman S, Saver JL, Kidwell CS, Gobin YP, et al; MERCI Trial Inves-tigators. Safety and efficacy of mechanical embolectomy in acute ischemic stroke: results of the MERCI trial. Stroke. 2005;36:1432–1438.
16. The Penumbra Pivotal Stroke Trial Investigators. The Penumbra Pivotal Stroke Trial. Safe-ty and effectiveness of a new generation of mechanical devices for clot removal in intra-cranial large vessel occlusive disease. Stroke. 2009; 40: 2761–2768.
17. The Thrombolysis in Myocardial Infarction (TIMI) trial. Phase I findings. TIMI Study Group. N Engl J Med. 1985;312:932e6.
18. Tomsick T. TIMI, TIBI, TICI: I came, I saw, I got confused. AJNR Am J Neuroradiol. 2007;28:382–384.
19. Wakhloo AK, Gounis MJ. Retrievable closed cell intracranial stent for foreign bodyand clot removal. Neurosurgery 2008;62(5 Suppl 2):ONS390e3.
GP coNTacTGPs can call for appointments through the NNI Neuroscience Clinic at 6357 7095.
Under fluoroscopic control, a micro catheter was manipulated over a mi-cro-guide wire across the occlusion site until the tip of the micro catheter was distal to the thrombus. A Stent-re-triever device was deployed across the thrombus and clot retrieval was per-formed twice, resulting in complete re-moval of the clot. The final angiogram showed complete recanalisation of the right MCA M1 (Figure 5), and the follow-up CT scan on the fourth day re-vealed a small residual infarction at the right basal ganglion. The patient was discharged from the hospital and was able to return to activities of daily liv-ing with rehabilitation.
Figure 4 DSA. Right ICA angiogram after the clot retrieval procedure shows complete reca-nalisation (TICI 3).
Figure 5 CT scan done on Day 4 post clot retrieval showed a small area of hypodensity at the right basal ganglia/external capsule, corresponding to a small residual area of in-farction.
Parkinson Disease and Related Disorders
Parkinson Disease (PD) is the second most common neurodegenerative disease in Sin-gapore with a prevalence of three in every 1,000 patients above the age of 50. In a re-cent study, the burden of Parkinson Disease had risen every year for the last 10 years in line with an ageing population in Singapore.
Parkinson Disease exerts a considerable burden on patients, the healthcare system and society in Singapore. It is estimat-ed that the total annual cost incurred while suffering from Par-kinson Disease is SGD11,345 per patient, with the main cost component derived from pharmacotherapy, home care and productivity loss. As the disease becomes more prevalent in the future, healthcare programmes with potential for return-ing patients to higher productivity are urgently needed.
caSe HiSToRYMr TJS was a 61-year-old man who complained of right-sided resting tremor, ‘weakness’ and slowness, which had been progressive for the last six months. He did not have any past medical history and was not on any medical treatment for his condition. This rest-ing tremor worsened whenever he was anxious and he had described his weakness as feeling fatigued, caus-ing him to drag his right lower limbs when he walked. These symptoms made it difficult for him to cope with his job as a ground supervisor in a factory. He was referred to the National Neuroscience Institute (NNI) Movement Disorders Centre for a consultation. It was further elicited that he has had hypophonia for six months and that his hand-writing had worsened. He also highlighted that he had been having problems with his sense of smell for some years now and that he had been constipated for a long time. His wife also acknowledged that the patient had been having sleep-talking and shouting, seemingly acting out his dream for some years now.
Clinically, his eye movements were normal. There was resting tremor of about 6 Hz, rigidity and bradykinesia on the right side. There was no postural hypotension and he had no idiomotor apraxia. His MMSE was 29/30.
He was diagnosed as having Parkinson Disease and was started on levodopa/benserazide combination medication. Education on the condition, pharmaco-therapy and resources available in the Movement Dis-orders Centre were given to the patient. He was seen again eight weeks later. By then, he showed improve-ment by more than 70 per cent and was feeling more confident and secure in continuing his job. He also received commendation on improvement of his work from his employers.
NeurologyFocus: medical update
Dr Tay Kay Yaw, Consultant, Department of Neurology, National Neuroscience Institute
5
appointments: 6357 7095 email: [email protected]

76
Oct-Dec 2014
wHaT iS PaRkiNSoN DiSeaSe?Parkinson Disease is a neurodegenerative disease with a de-position of Lewy Bodies in the substantia nigra, causing dis-ruption in the generation of dopamine. This in turn causes the symptoms of Parkinson Disease, namely resting tremor, rigidity, bradykinesia or akinesia and postural instability; bet-ter known with the acronym TRAP.
While Parkinson Disease is known for its motor symptoms, we must not forget about the non-motor complications of Parkinson Disease. This comes in various forms such as auto-nomic dysfunction, sleep disorders, pain, mood and psychi-atric issues and memory issues. These non-motor symptoms may affect patients’ quality of life more than the motor symp-toms, especially in the advanced stages of Parkinson Disease and thus must be dealt with promptly.
TABle 3: ScHwaB aND eNGlaND acTiviTieS oF DailY liviNG Scale
100% Completely independent. Able to do all activities without slowness, difficulty, or impairment.
90% Completely independent. Able to do all activities with some slowness, difficulty, or impairment. May take twice as long to complete.
80% Independent in most activities. Takes twice as long. Consciousness of difficulty and slowing.
70% Not completely independent. More difficulty with activities. Three to four times as long for some. May take large part of day for chores.
60% Some dependency. Can do most activities, but very slowly and with much effort, but some chores are impossible.
50% More dependent. Help required with half of chores. Difficulty with everything.
40% Very dependent. Can assist with all chores but few alone.
30% With effort, now and then does a few chores alone or begins alone. Much help needed.
20% Cannot do anything alone. Can give some slight help with some chores. Severe invalid
10% Totally dependent, helpless.
0% Vegetative functions such as swallowing, bladder and bowel functions are not functioning. Bedridden.
0 Normal. Patient takes 1 step behind.
1 Retropulsion, but recovers unaided. (More than 1 step)
2 Absence of postural response; would fall if not caught by examiner.
3 Very unstable, tends to lose balance spontaneously.
4 Unable to stand without assistance.
TABle 2: PoSTuRal iNSTaBiliTY (FallS RiSk): ReSPoNSe To SuDDeN, STRoNG PoSTeRioR DiS-PlacemeNT PRoDuceD BY Pull oN SHoulDeRS wHile PaTieNT iS eRecT wiTH eYeS oPeN aND FeeT SliGHTlY aPaRT. (PaTieNT iS PRePaReD.)
UPDRS Rating scale for Falls (see Table 2)
Schwab and England Activities of Daily Living Scale (see Table 3)
TABle 1: cHRoNic DiSeaSe maNaGemeNT PRoGRamme cliNical iNDicaToRS
multidisciplinary approach remains as the best option in treating patients with Parkinson Disease, with the goal of keeping the patients’ expectations of quality of life.
Medical treatments, including dopaminergic medication such as levodopa or dopamine agonists are the mainstay of Parkin-son Disease treatment. Anti-cholinergics are also useful es-pecially for reducing resting tremors. Allied health interven-tion, including physiotherapy, occupational therapy, speech therapy and medical social workers are important to keep the patient physically and mentally active.
Generally, after initiating treatment, the patient goes into a ‘honeymoon period’, where the medication is long-lasting and highly effective with no motor complications. These pa-tients are best to be followed up by our GP colleagues to keep the patient functional in the community. With the admis-sion of Parkinson Disease into the Chronic Disease Manage-ment Program (CDMP) under the Ministry of Health (MOH), we strongly encourage our GP colleagues to leverage on this incentive to follow up with these patients. However, under this program, there are certain clinical indicators to be ob-tained by the GPs as outlined in Table 1.
NeurologyFocus: medical update
cardinal features of Parkinson Disease
Tremor
akinesia
RigidityPostural
instability PD
Generally, patients who are younger (<60 years old) with milder disease are started with dopamine agonist. There are various drugs under this category such as bromocriptine, rop-inirole, pramipexole and rotigotine. Older patients with more severe disease are generally started with levodopa/bensera-zide combination.
HoeHN aND YaHR STaGiNG oF PaRkiNSoN DiSeaSe
Stage 0 No signs of disease
Stage 1 Unilateral disease
Stage 1.5 Unilateral plus axial involvement
Stage 2 Bilateral disease, without impairment of balance
Stage 2.5 Mild bilateral disease; recovery on pull test
Stage 3 Mild to moderate bilateral disease; some postural instability; capacity for living independent lives
Stage 4 Severe disability, still able to walk or stand unassisted
Stage 5 Wheelchair bound or bedridden unless aided
It is advisable to start these medications with a low dose and uptitrate the medication slowly (generally 62.5 mg levodopa/benserazide every week till intended dose) while monitoring for possible side effects such as nausea and vomiting, pos-tural hypotension and hallucinations. If indeed there is nau-sea and vomiting from the medications, domperidone can be used.
Metoclopromide and stemetil are generally contraindicated in Parkinson Disease because they can potentially worsen Parkinsonism features. As a guide, bradykinesia and rigidity generally respond better to dopmainergic medication than resting tremor. Therefore, the target dose for the patients is mainly to alleviate bradykinesia and rigidity. However, if rest-ing tremor is the main concern of the patients, then anti-cho-linergics such as trihexyphenidyl will be a good choice.
How DoeS PaRkiNSoN DiSeaSe PRoGReSS?
0 years
-10 years
5 years
10 years
15 years
2 years
Preclinical PD• Olfactory loss• REM Behavior Disorder (RBD)• Constipation• Anxiety• Depression• Impaired colour vision
early Treated PD (Stable)• Bradykinesia• Rigidity• Rest-tremor• (+/– non-motor symptoms)
advanced PDmotor complications• Wearing off/Dyskinesias• Gait & balance problems• Axial deformities• Dysarthria/Dysphagia
Non-motor complications• Cognitive decline/Dementia• Depression• Psychosis• Autonomic dysfunction• Sleep-awake dysregulation
onset motor symptoms
Various Stages of Parkinson Disease
wHeN GPs caN ReFeR To a SPecialiSTManagement of the late stages of Parkinson Disease are more complex. Patients may experience motor complications, pos-tural instability and various non-motor problems. We highly recommend for these patients to be referred to NNI Move-ment Disorders Centre.
likelY TReaTmeNT oPTioNS BY GPsParkinson Disease is generally staged with the Hoehn and Yahr stage. Treatment options must be individualised and tai-lored according to patients’ needs. As a guide, treatment can be divided into early (Hoehn and Yahr 1-2.5) and late stages (Hoehn and Yahr 3-5) of Parkinson Disease.
In the early stages of Parkinson Disease, the question of neu-roprotection comes into mind. Unfortunately, no medication has been proven to consistently halt or slow down the neuro-degenerative process in Parkinson Disease.
appointments: 6357 7095 email: [email protected]

Assoc Prof Ang Beng Ti, Christopher, Head and Senior Consultant, Department of Neurosurgery (SGH Campus), National Neuroscience Institute
Dr Loh Lih Ming, Senior Consultant, Department of Endocrinology, Singapore General Hospital
Pituitary Tumours
Pituitary tumours are not un-common and require a multi-disciplinary approach to their diagnosis and management. In SingHealth, we involve endocrinologists and neu-rosurgeons from the Singa-pore General Hospital (SGH) and neuro-ophthalmologists from the Singapore National Eye Centre (SNEC). As such, there is a dedicated Pitu-itary Clinic sited at the SNEC which incorporates such a model of care.
PRevaleNceRecent literature report higher preva-lence of pituitary tumours than previous estimates conducted in the pre-MRI era. Population based surveys, done pre-dominantly in Europe, put the preva-lence of these tumours between 75 to 94 cases per 100,000 population, and standardised incidence ratios around 4 per 100,000. Such tumours are found 2-3 times more often in women than men.
TYPeS oF TumouRSThe commonest pituitary tumours are prolactinomas, making up half to two-thirds of all cases. About one third are clinically non-functioning tumours. These are often gonadotroph adeno-mas, which do not produce any clini-cal syndrome. Growth hormone, ACTH and TSH producing tumours, while causing clearly-defined syndromes, are relatively rare.
cliNical PReSeNTaTioNProlactinomas usually present in the re-productive age group, with symptoms of hypogonadism including menstrual irregularities, erectile dysfunction, low libido and subfertility. Patients may also present with galactorrhoea.
Prolactinomas in women tend to pres-ent as smaller intrasellar tumours, whereas prolactinomas in men tend to be macroadenomas which are often locally invasive. Although a possible reason could be a delay in diagnosis in men due to lack of specific symp-tomatology, it has also been shown that prolactinomas in men show more aggressive biology, with higher index of proliferating cells and greater resis-tance to dopamine agonist therapy.
Gonadotroph tumours may either be non-secreting, or secrete gonadotro-phins in a non-pulsatile manner, which may also result in hypogonadism. Due to lack of specific symptoms, these are clinically termed as non-functioning pi-tuitary tumours. These tumours usually present late, with mass effect on sur-rounding structures.
The commonest presentation is visual field loss due to compression of the optic chiasm. Hypopituitarism is often detected at diagnosis, and attributed to mass effect causing increased intra-sellar pressure and vascular compro-mise of the normal pituitary tissue.
acromegaly, due to growth hormone secreting pituitary adenomas, make up about 10% of pituitary tumours. As the clinical features of growth hormone ex-cess cause insidious and subtle physi-cal changes, there is usually a delay in diagnosis of acromegaly averaging 7-10 years. Cushing’s disease, due to ACTH-secreting tumours, make up less than 5%. TSHomas are even rarer and are usually locally invasive by the time the time they are diagnosed.
Pituitary apoplexy is a rare but po-tentially fatal complication of pituitary tumours. It is characterised by sud-den onset of severe headache, visual
Oct-Dec 2014
GP coNTacTGPs can call for appointments through the NNI Neuroscience Clinic at 6357 7095.
likelY TReaTmeNT oPTioNS BY THe SPecialiSTin NNi movement Disorders centre, there is a holistic multidisciplinary program to welcome our Parkinson Disease patients. Patients will be assessed and diag-nosed by our movement disorders specialists, who in turn will work hand-in-hand with the nursing fraternity and allied health personnel to formulate an acceptable treatment regime for the patients.
The Movement Disorder Centre also leads the Commu-nity Care Partnership Program with various day rehabilita-tion centres throughout Singapore, to train therapists in the highly specialised field of Parkinson Disease rehabilit-
Holistic Parkinson Disease Program in Movement Disorders Centre, National Neuroscience Institute
ation. This is to ensure that our patients’ rehabilita-tion needs are met and well taken care of in the com-munity setting. It works closely with the Parkinson Soci-ety Singapore to promote awareness of the disease and support various rehabilitation and social programs for patients.
Due to the extent of the outreach programmes, our Par-kinson Disease and Movement Disorders Centre has been recognised as a centre of excellence by the National Par-kinson Foundation. Last but not least, the Centre is also a leading centre for Deep Brain Stimulation in advanced Parkinson Disease treatment.
NeurologyFocus: medical update
8 9
appointments: 6357 7095 email: [email protected]

1110
Oct-Dec 2014Services
11
The Screening Colonoscopy Clinic at SGHsymptoms, altered mental status and hormonal dysfunction. It is caused by an acute haemorrhage or infarction of a pituitary tumour, often previously undiagnosed. Apoplexy constitutes a neurosurgical and endocrine emergen-cy, and requires close monitoring, pos-sibly neurosurgical intervention if there is acute neurologic deterioration, and acute corticosteroid support.
At the other end of the clinical spec-trum, incidental findings of pituitary masses are increasing due to the more extensive use of cranial imaging tech-nologies. Pituitary incidentalomas have an average frequency of 10% in various series. In pooled series, most of these are microadenomas (tumours less than 1 cm). Patients with pituitary incidentalomas should undergo clini-cal and laboratory evaluation for evi-dence of hypopituitarism or hormone hypersecretion. Serial MRI imaging of these tumours to monitor for growth is also recommended.
viSioN aSSeSSmeNTProblems with vision are a frequent presentation for patients with pituitary macroadenomas (lesions larger than 1cm in size). The classical feature is that of a bitemporal hemianopia which arises from chiasmal compression by the tumour. A full clinical vision exami-nation involves the assessment of vi-sual acuity, visual fields, colour vision, extra-ocular eye movements, pupillary assessment and fundal examination. The clinical findings obtained dur-ing initial diagnosis constitute a valu-able baseline for comparison. In this way, opthalmological examinations become crucial to ascertain if there is improvement following treatment and also to help detect for tumour recurrence.
meDical maNaGemeNT More than 90% of prolactinomas re-spond to dopamine agonist therapy
(bromocriptine or cabergoline). Rapid clinical, biochemical and radiological response is seen. Remarkable improve-ment in visual field deficits, resumption of menses, sex hormones and fertility can be achieved within a few weeks of therapy. Impressive tumour shrinkage is often seen within months.
As such, medical therapy is usually the first line treatment for prolactinomas. If initiated with care, dopamine agonists are generally well-tolerated. Treatment is for at least three years from the time of clinical efficacy, following which a gradual withdrawal of treatment can be attempted.
Medical therapy for acromegaly and Cushing’s disease are reserved as a temporary measure, when there is lack of remission following surgery and be-fore the definitive effects of radiother-apy occur. As opposed to dopamine agonist therapy in prolactinomas which is usually curative, medical therapy in these conditions are only for symptom control and do not contribute to long-term cure of the condition.
HoRmoNal RePlacemeNTPatients with hypopituitarism require physiologic hormone replacement. Depending on the underlying cause, these may be temporary, or more of-ten, required lifelong. Most cost-effec-tive medications that mimic physiology are used, where possible. This includes use of multiple day doses of hydrocor-tisone to reproduce the diurnal corti-costeroid rhythm, once daily levothy-roxine, female hormone replacement therapy in women in premenopausal age group and various options of an-drogen replacement therapy in men.
For men and women desiring fertility, the use of various types of gonadotro-phin injections, often combined with assisted reproductive techniques, have resulted in successful childbirths.
SuRGical maNaGemeNTFor lesions other than macroprolacti-nomas (where the first line of treatment is medical), pituitary macroadenomas do often come to surgery. For non-functioning tumours, the issue is mass effect and the surgery serves to maxi-mally resect the tumour to relieve chi-asmal compression, most commonly. This would allow for preservation of the patient’s vision status and in many cases lead to significant improvement as well. For the functioning tumours with an en-docrine syndrome, the ideal treatment would be complete surgical resection so as to achieve a cure.
Traditionally, large pituitary macroad-enomas with significant extension an-teriorly along the anterior skull base, laterally and posteriorly towards the brainstem would require a craniotomy for resection. At present, the propor-tion of tumours requiring a transcranial approach has fallen due to the advent of expanded endonasal approaches, where in addition to the standard trans-phenoidal route, additional exposure of the anterior skull base along the pla-num and inferiorly along the clivus, is now technically possible. Hence, many pituitary tumours can now be dealt with via a endonasal endoscopic approach.
An important adjunct to surgical and medical treatment is radiosurgery. This refers to the focused delivery of radia-tion to a well-defined volume. Follow-ing surgery, tumour remnants which show evidence of enlargement may be treated in this manner.
GP coNTacTGPs can call for appointments through the NNI Neuroscience Clinic at 6357 7095.
appointments: 6357 7095 email: [email protected]: medical
update
10
Screening colonoscopyScreening colonoscopy examines the entire colon and removes polyps for histological assessment. A complete colonoscopy with normal findings in an average risk individual is repeated in 10 years. This is in contrast to FOBT that is repeated annually following a negative result.
In individuals with polyps, colonos-copy is repeated at an earlier interval – typically 3-5 years – depending on the number and histological severity of polyps.
eNDoScoPic TReaTmeNT oF aDvaNceD PolYPS aND eaRlY caNceRSA minority of patients may have ad-vanced polyps that may be missed or poorly characterised on routine colo-noscopy. These patients may undergo colonoscopy with advanced imaging capabilities (e.g. narrow band imag-ing, chromoendoscopy) that enables improved detection and delineation of polyps.
A proportion of patients undergoing screening colonoscopy may be found
GP coNTacTThe Screening Colonoscopy Clinic is lo-cated at the Centre for Digestive and Liver Diseases (CDLD) and operates ev-ery Wednesday morning.
Appointments can be made through the Specialist Outpatient Clinic Ap-pointment Centre at 6321 4402.
For a friendly chat or discussion, our GP partners can call 6222 3322 to get in touch with the the Screening Colonos-copy Clinic.
The Screening Colonoscopy Clinic at the Singapore General Hospital (SGH) caters to patients aged 45 and above who require colonoscopy for assessment of altered bowel habits, positive faecal occult blood test (FOBT), rectal bleed-ing and asymptomatic patients eligible for screening colonoscopy according to Ministry of Health guidelines.
wHY ScReeN FoR coloRecTal caNceR?Colorectal cancer (CRC) is the common-est cancer in Singapore. This is related to increasing affluence that drives obe-sity and a sedentary lifestyle. CRC can be largely prevented by screening as there is a lag time of several years be-tween the occurrence of precancerous polyps (adenomas) and cancer. The re-moval of polyps may arrest its progres-sion to cancer. Adenomas are found in approximately 25% of the general pop-ulation aged 50 years and above. The prevalence is even higher in subjects with a positive FOBT.
How Do You ScReeN?CRC screening is currently recommend-ed to begin at age 50 years or earlier in those with a positive family history. Screening involves 2 main methods – faecal occult blood testing (FOBT) and screening colonoscopy.
Faecal occult blood testing (FoBT)FOBT detects blood in the stool and is based on the principle that colorec-tal cancers may bleed giving rise to a positive FOBT. Since bleeding may be intermittent, at least 2 FOBT specimens must be collected each time. It enables detection of cancers but not adenomas as the latter do not normally bleed.
A positive FOBT mandates further as-sessment by diagnostic colonoscopy. A negative FOBT should be followed up with repeat FOBT annually.
The clinic caters to outpatients aged 45 and above who require colonos-copy for the following indications:
1. Assessment of altered bowel habits
2. Positive faecal occult blood test (FOBT)
3. Rectal bleeding 4. Screening colonoscopy for eligi-
ble asymptomatic patients aged 50 and above
The clinic offers the following ser-vices:
1. Routine screening colonoscopy with polypectomy
2. Follow-up surveillance colonos-copy
3. Advanced endoscopic imaging4. Endoscopic resection of ad-
vanced polyps and early cancers
wHaT DoeS THe ScReeNiNG coloNoScoPY cliNic oFFeR?
to have large high grade polyps and early cancers that may be not be treat-able by conventional polypectomy. These lesions may be amenable to re-moval using newer endoscopic resec-tion techniques. These patients may undergo endoscopic treatment thus obviating the need for surgery.

1312
Oct-Dec 2014News
A cardiothoracic surgery team at KK Women’s and Children’s Hospital (KKH) has successfully performed a complex Rastelli-Senning surgical procedure to repair the heart of a 16-year-old patient with a rare congenital abnormality.
Born with a rare variant of congenitally corrected transposition of the great arteries (ccTGA), the patient’s cardiac ventricles were reversed during foetal development – resulting in each ven-tricle being connected to the incorrect atrium and great artery. The condition was compounded by a large hole in the patient’s ventricular septum and a ste-nosed pulmonary valve.
Due to the abnormal cardiac blood flow pathway and lack of blood permitted to the lungs, the patient was frequently cyanotic due to low levels of oxygen in the body. While able to attend school, the patient experienced poor effort tol-erance and was unable to participate in any activity requiring physical exertion.
“Carefully considering the patient’s very impaired quality of life and the almost-certain prospect of heart failure in their 40s, our care team of radiology, cardiol-ogy and cardiothoracic surgery special-ists decided to proceed with the Rastelli-Senning procedure to surgically repair the patient’s heart and correct the cardiac blood flow,” shared Dr Loh Yee Jim, Con-sultant, Cardiothoracic Surgery Service, KKH, who led the surgical procedure.
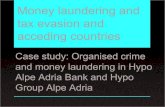
THe SeNNiNG aND RaSTelli PRoceDuReSFollowing a thorough diagnostic evalu-ation to determine the patients’ suit-ability for the highly complex surgery, the Senning procedure was carried out to reroute cardiac blood flow from each atrium to the correct ventricle. This in-volved the creation of a baffle within the atria to redirect the deoxygenated caval blood to the tricuspid valve and the oxygenated pulmonary venous blood to the mitral valve.
Rastelli-Senning Repair for Rare Congenital Heart Defect
illustration of the Rastelli-Senning Procedure
Heart with ccTGa, ventricular septal defect and pulmonary stenosis after
Rastelli-Senning repair.
©2014SingHealth
leGeND
RA Right atrium
RV Right ventricle
LA Left atrium
LV Left ventricle
Ao Aorta
PA Pulmonary artery
PS Pulmonary stenosis
VSD Ventricular septal defect
Tricuspidvalve
Valveconduit
Mitralvalve
Normal heart
Tricuspidvalve
Mitralvalve
Heart with ccTGa, ventricular septal defect and pulmonary stenosis.
Mitralvalve
Tricuspidvalve
Physiotherapy Support for GPs in the Community
GP coNTacTFor enquires on the AHPP programme, please call 6377 8014 or email [email protected]
Services
12
General practitioners (GPs) can soon look forward to phy-siotherapy support in the ma-nagement of their patients.
Starting in 2015, GPs will be able to refer eligible patients who will enjoy subsidised rates from a panel of private physiotherapists under the SingHealth Allied Health Partnership Programme.
wHaT GPs caN exPecT FRom THe aHPP PRoGRamme:
• Adirectoryofprivatephysio-therapy clinics islandwide that GPs can refer patients to.
• Astandardisedphysiotherapyreferral form for the conve-nience of GPs when referring patients for physiotherapy.
• Physiotherapy sessionscapped at a discounted rate of $60/session for subsidised patients.
Some PHYSioTHeRaPY SeRviceS THaT will Be availaBle:
• Musculoskeletal• SportsInjuryRehabilitation• Geriatrics• NeurologicalRehabilitation• PaediatricPhysiotherapy
The AHPP programme is part of a series of SingHealth programmes to right-site patients and aims to foster a closer rela-tionship between GPs and allied health professionals to better provide a con-tinuum of care to benefit patients.
The AHPP Programme is brought to you by the SingHealth Group Allied Health and SingHealth Physiotherapists.

1514
Oct-Dec 2014
PaeDiaTRic oBSTRucTiveSleeP aPNoea Paediatric OSA belongs to a group of sleep disorders, termed sleep disordered breathing (SDB). The global prevalence of paediat-ric SDB ranges from 0.9 percent to as high as 13 percent, increasing alongside the growing incidence of obesity.
Common signs and symptoms of paediatric sleep disordered breathing include:
• Loudsnoring,choking or grunting during sleep• Sleepinessduringtheday• Behavioural problems, such
as short attention span and hyperactivity
• Pooracademicperformance
Children who experience snoring in addition to one or more of the above symptoms should be re-ferred for tertiary assessment.
The condition has also been shown to negatively impact the child’s neurocognitive and car-diovascular systems, quality of life, behaviour and school perfor-mance, as well as increase health-care utilisation. Further, evidence shows that the implications of OSA on cardiovascular health in childhood adversely affect cardio-vascular outcomes in adulthood.
KK Women’s and Children’s Hospital (KKH) has successfully performed the first paediatric transoral robotic sur-gery (TORS) for obstructive sleep ap-noea (OSA) in Singapore.
The child had previously undergone an adenotonsillectomy to treat OSA sev-en years ago, however her symptoms returned. Further assessment revealed an obstruction at the tongue base – an area which has traditionally posed a challenge for surgical intervention, due to difficult access and a high risk of bleeding.
By combining the dexterity of a ro-bot with the skills of a surgeon, and modifying the types of instrumenta-tion to be used with the robotic arm, the team at KKH’s Sleep Disorders Unit successfully carried out TORS of the tongue base to treat the child’s OSA. The patient consequently experienced complete resolution of symptoms and normalisation of sleep study results.
imPRoveD ouTcomeS wiTH RoBoTic SuRGeRYThe robotic surgery was performed us-ing the da Vinci surgical robotic system, which features high definition three-dimensional imaging and articulated
News
KKH Performs Singapore’s First Paediatric Transoral Robotic Surgery
arms, allowing for precise surgical ma-nipulation within the narrow confines of the child’s mouth.
The visualisation of the tissue planes and access to the surgical site that this approach offers is unparalleled, allow-ing the surgeon to perform a more complete assessment and precise re-section of tissue in a very limited space. This translates to minimised blood loss and better post-operative outcomes.
eNHaNceD maNaGemeNT FoR oBSTRucTive SleeP aPNoea iN cHilDReNCurrent treatment protocols for OSA centre on initial adenotonsillectomy. If the surgery is unsuccessful, long-term use of a continuous positive airway pressure (CPAP) machine may be re-quired to help the child breathe during sleep. CPAP compliance in children is difficult and many do not tolerate the discomfort associated with it. In severe or complex cases, a tracheostomy may even be necessary to alleviate the air-way obstruction and allow oxygenation.
Even after undergoing an adenotonsil-lectomy, a significant population of chil-dren with OSA continue to experience residual or recurrent symptoms, up to 85 percent of which are caused by ob-struction at the tongue base. Recurrent or persistent OSA is especially preva-lent in children with obesity, genetic syndromes, craniofacial abnormalities and neuromuscular disease. The Sleep Disorders Unit at KKH comprises respi-ratory physicians, ear nose and throat surgeons, dietitians, endocrinologists, anaesthetists and neurologists, who work closely to provide specialist care for patients with sleep disorders.
KKH has also introduced a TORS service to treat various conditions in women and children, which include oral cavity cancers, lesions of the tongue, oropharynx and hypopharynx as well as OSA.
coNTacT kkHGeneral enquiriesTel: 6225 5554
Then, the Rastelli procedure was per-formed. This involved closing the size-able hole in the patient’s ventricular septum at an angle, to direct blood flow from the left ventricle to the aorta; and the insertion of a valve conduit into the right ventricle to direct blood flow to the pulmonary artery.
Post-surgery, the patient was tempo-rarily placed on extra-corporeal mem-brane oxygenation (ECMO) support to allow time for the left ventricle to accustom itself to the increased pres-sure and blood flow. The patient’s heart
coNTacT kkHGeneral enquiriesTel: 6225 5554
cRiTical caRe FoR coNGeNiTal HeaRT aBNoRmaliTieS Congenital heart abnormalities are the most common structural anomalies among babies born in Singapore, occurring in nine per 1,000 live births. At KKH, babies and children requiring critical care for heart and lung con-ditions are managed by comprehensive multidisciplinary teams comprising radiology, cardiology, cardiothoracic surgery, paediatric and neonatal intensive care, anaes-thesia and allied health specialists.
The KKH team performs the largest number of complex congenital heart surgeries for babies, children and adults in Singapore, and also provides critical cardiac and tho-racic care for many patients in Singapore and the region. Despite this, the hospital maintains the lowest mortality rate for paediatric cardiac surgery in Singapore, with a core success rate of 97-98 percent over the last five years.
The hospital’s ECMO programme also provides life-sus-taining support to young patients requiring emergency care for high-risk heart and lung conditions. Singapore’s first mobile ECMO service for infants and children was recently created by KKH to assist patients urgently re-quiring ECMO support at other locations before being brought to the KKH intensive care unit for ongoing care.
To advance cardiac care for the region, the KKH team also provides training and medical expertise to assist in the establishment of congenital cardiac programmes in countries such as Myanmar and Vietnam.
coNGeNiTallY coRRecTeD TRaNSPoSiTioN oF THe GReaT aRTeRieS A rare congenital heart abnormality, ccTGA occurs in 0.5 percent of patients diagnosed with congenital heart disease. The condition is characterised by the reversal of the ventricles during foetal development, resulting in each ventricle being connected to the incorrect atrium and incorrect great artery.
This complex malformation places great strain on the patient’s heart – particularly on the smaller right ven-tricle, which is forced to bear a greater blood pressure and volume than it was genetically meant to. This can lead to further health problems, such as irregular heart rhythm, valvular regurgitation, impaired heart function and heart failure.
Several associated problems can also co-exist in pa-tients with ccTGA, potentially further complicating their quality of life and the type of intervention that is re-quired. These can include:
• Ventricularseptaldefect–aholebetweentheven-tricles of the heart
• Pulmonarystenosis–obstructionofbloodflowfromthe right ventricle to the pulmonary artery
• Leakageofthetricuspidvalve• Obstructedcardiacelectricalconductionsystem
Medical literature reports that 67 percent of patients with ccTGA and associated heart defects develop heart failure by the age of 45, eventually requiring a heart transplant. However, with appropriate surgical interven-tion, over 90 percent of patients with ccTGA can have a 20-year survival.
soon stabilised and was able to func-tion without external support.
In the weeks following the operation, the patient underwent physiotherapy, respiratory therapy and dietetic advice to facilitate full recovery. Currently, the patient is asymptomatic and able to participate in recreational activities re-quiring moderate levels of effort.
“The successful Rastelli-Senning pro-cedure allows patients with ccTGA to have a much better quality of life, with very much improved exercise tolerance.
Most importantly, as the patient’s blood now flows through the correct cham-bers of the heart, this greatly reduces the likelihood of heart failure and the need for a heart transplant later, during their prime years,” said Dr Loh.
“Due to the complexity of the condition, patients with ccTGA require life-long follow-up. Our patient will be monitored by the KKH care team until adulthood. We will then work closely with the adult congenital team at the National Heart Centre Singapore to ensure our patient’s seamless transition into their care.”

1716
Oct-Dec 2014
Dr lee Phong ching Associate Consultant Dept Endocrinology Sub-specialty General Endocrinology
Dr cherng Pei Zhi Benjamin Associate Consultant Dept Infectious Disease
Dr Navin Bajaj Associate ConsultantDept Respiratory & Critical Care MedicineSub-specialtyCritical Care Medicine, Sleep Medicine
Dr Tay ci an Gerald Associate Consultant Dept General Surgery; SingHealth Duke-NUS Head and Neck Surgery CentreSub-specialty Head & Neck Surgery
SingapOre generaL HOSpitaLappOintmentS
Dr lim chee Hooi Senior Consultant
Dept Gastroenterology & HepatologySub-specialtyGastroenterology, Procedures - Screening Derived Colonoscopy, Diagnostic & Interventional/Therapeutic Endoscopy, Endoscopic Mucosal Resection (EMR)
Dr lim wei inng Francesca lorraine Associate Consultant Dept Haematology Sub-specialty General Haematology
Dr moey Hui lin Tammy Associate Consultant Dept Diagnostic RadiologySub-specialty Breast Imaging
Dr ang chia liang Associate Consultant Dept Orthopaedic Surgery Sub-specialty Musculoskeletal Tumour and Adult Reconstruction
Dr Fong weng Seng warren Associate Consultant Dept Rheumatology & Immunology Sub-specialty General Rheumatology
Dr Tan Tze Sheng edwin Associate Consultant Dept Orthopaedic Surgery
Dr lim chin Hong Associate Consultant Dept Upper Gastrointestinal & Bariatric Surgery
Dr Tay kae Jack Associate Consultant Dept Urology
prOmOtiOnS
Dr khor li Yan Associate ConsultantDept PathologySub-specialty Cytopathology and Urologic Pathology
Dr chong Si Jack Associate ConsultantDept Plastic, Reconstructive & Aesthetic Surgery
Dr mok un Sam ConsultantDept AnaesthesiologySub-specialty Obstetric Anaesthesia
Dr vidyarthi arpana Ramanathan ConsultantDept Internal Medicine
prOmOtiOnS
Dr abey matthew varughese matthews Associate Consultant Dept Anaesthesiology
Dr Tay wei Yi Associate Consultant Dept Family Medicine & Continuing Care
Dr Sueziani Binte Zainudin Associate Consultant Dept Endocrinology Sub-specialty Diabetes Mellitus, Diabetes and Fasting, Diabetes Education
neW appOintmentDr chang Tou en kenneth Deputy Head (Research & Education) Dept Pathology and Laboratory Medicine
SengKang HeaLtHappOintmentS
Dr Farhad Fakhrudin vasanwala Consultant Dept Internal Medicine
Dr anandakumar s/o vellasamy Associate Consultant Dept Orthopaedic Surgery
KK WOmen’S anD cHiLDren’S HOSpitaL
appointments
Dr Shailesh kumar Associate Consultant Dept Gastroenterology & Hepatology

1918
Oct-Dec 2014
Dr koh Yeow Hoay Associate Consultant Dept Neurology (SGH Campus)
Recruitment
If you are a qualified doctor, a challenging career awaits you at SingHealth. We seek suitably qualified candidates to join us as:
•ResidentPhysicians/FamilY PHYSiciaNS
•RegistRaRs
Interested applicants to email CV with full personal particulars, educa-tional and professional qualifications (including housemanship details), career history, present and expected salary, names of at least two profes-sional references, contact numbers and e-mail address together with a non-returnable photograph.
Please email your CV to the respec-tive institutions’ email addresses/online career portals below with the Reference Number MN1410.
Singapore General HospitalDepartments seeking Resident Physicians and Registrars:•Anaesthesiology•ColorectalSurgery•DiagnosticRadiology•EmergencyMedicine•Endocrinology•FamilyMedicine& Continuing Care •Gastroenterology&Hepatology•GeneralSurgery•GeriatricMedicine•Haematology•HandSurgery• InfectiousDiseases• InternalMedicine•Neonatal&Developmental Medicine •NuclearMedicine&PET•Obstetrics&Gynaecology•OrthopaedicSurgery•Otolaryngology•Plastic,Reconstructive& Aesthetic Surgery •RenalMedicine•RehabilitationMedicine•Respiratory&CriticalCare Medicine •Rheumatology&Immunology•Urology•StaffClinic-Locum
website: www.sgh.com.sgcareer Portal: www.sgh.com.sg/subsites/sgh-careers/medical/pages/career-opportunites.aspxemail: [email protected]
kk women’s and children’s Hospital
Departments seeking Resident Physicians:•BreastSurgery•CardiothoracicSurgery•ObstetricAnaesthesia
website: www.kkh.com.sgemail: [email protected]
National cancer centre SingaporeSeeking Resident Physicians
website: www.nccs.com.sgemail: [email protected]
National Heart centre SingaporeDepartments seeking Registrars:•CardiothoracicSurgery
website: www.nhcs.com.sgemail: [email protected]
Singapore National eye centreSeeking Resident Physicians and Registrars
website: www.snec.com.sgemail: [email protected]
SingHealth PolyclinicsDepartments seeking Resident Physicians and Family Physicians:•Polyclinic(FamilyMedicine)
website: http://polyclinic.singhealth.com.sgemail: [email protected]
Sengkang HealthDepartments seeking Resident Physicians and Registrars:•Anaesthesiology•DiagnosticRadiology•Endocrinology•EmergencyMedicine•Gastroenterology•GeneralSurgery•GeriatricMedicine• InfectiousDiseases• InternalMedicine•Neurology•OrthopaedicSurgery•Otolaryngology•Pathology•RehabilitationMedicine•RenalMedicine•RespiratoryMedicine•Urology
website: www.singhealth.com.sg/AboutSingHealth/CorporateOverview/sengkang-health/pages/home.aspxemail: [email protected]
Singapore Health Services (SingHealth), Singapore’s largest Academic Healthcare Cluster, is committed to providing afford-able and accessible quality healthcare to patients. With a total of 42 clinical specialties, its network of 2 Hospitals, 5 National Specialty Centres, 9 Polyclin-ics and a Community Hospital delivers a comprehensive range of multidisciplinary and integrated medical care.
SingHealth is responsible for develop-ing Sengkang Health, a new healthcare system to deliver patient-centric care to the community in the north-east of Sin-gapore. By 2018, a general hospital and a community hospital will be fully opera-tional in Sengkang. Sengkang Health will commence operations in Alexandra Hos-pital in 2015, prior to the completion of its new hospitals. The collective strengths of SingHealth and Duke-NUS, its partner in research and medical education, pave the way for the transformation of healthcare.
Don’t limit Your challenges. challenge Your limits.
appointments
natiOnaL cancer centre SingapOreappOintment
Dr Tiffany Priyanthi Hennedige Associate Consultant Dept Oncologic Imaging
Dr amit Jain Associate Consultant Dept Medical Oncology
prOmOtiOnSDr koo Si-lin Associate Consultant Dept Medical Oncology
Dr kiattisa Sommat Associate Consultant Dept Radiation Oncology
Dr ang kexin Associate Consultant Dept Neurology (TTSH Campus) Sub-specialty Palliative Care in Neurology
assoc Prof ang Beng Ti, christopher Head and Senior Consultant Dept Neurology (SGH Campus) Sub-specialty Endoscopic Pituitary and Skull Base Surgery, Radiosurgery, Neurotrauma
prOmOtiOnS
natiOnaL neUrOScience inStitUte
Dr lim ee wei Associate Consultant Dept Neurology (SGH Campus)
Dr lin xuling Associate Consultant Dept Neurology (TTSH Campus) Sub-specialty Neuro-oncology
Dr Tu Tian ming Associate Consultant Dept Neurology (TTSH Campus) Sub-specialty Stroke, Neuro-intensive Care

20
Reg. No.: 200002698Z
gpep HOtLine
6377 8550
6321 4402
6294 4050
6436 8288
6324 8798
6704 2222
6321 4402/6357 7095
6322 9399
gp FaSt tracK appOintment HOtLineS
6321 4822
6394 1180
Direct WarD reFerraL cOntact nUmBerS
SingHeaLtH acaDemic HeaLtHcare cLUSter
courses
Inaugural Singapore Breast Oncoplastic Surgery Symposium (SBOSS)
Therapeutic mammoplasty in asian women
20
Symposium Highlights• Anatomyandbloodsupplytothebreast.• SecretsofasuccessfuloncoplasticsurgeryanditslimitationsinAsianwomen.• OncoplasticexperienceinKoreaandNottingham,UK.• Incisionsonthebreastandavoidingdogears.• Howtodoroundblock,verticalandwisepatternmammoplasty.• Casediscussionsonthemanagementofcomplicationsandchallengingcases.
Date30 January 2015, Friday
Time9.00am to 4.30pm
venueKKH Auditorium,Training Centre, Level 1,Women’s Tower
FeesDoctors – $450Others* – $150*Nurses, medical and nursing students, allied health professionals. Registration fee includes educational materials, lunch and tea break.
cme Points4 points
contactTel: 6394 8746Fax: 6394 1555Email: [email protected]
Registrations by 23 January 2015. For more details, please call 6394 8746 (Monday to Friday, 8.30am to 5.30pm) or log on to www.kkh.com.sg/SBoSS2015.