Suffocation Deaths Associated with Use of Infant Sleep Positioners
Upload
jennifer-roweCategory
view
212download
0
Nursing Inquiry 2003; 10(3): 184–192
F e a t u r e
© 2003 Blackwell Publishing Ltd
Blackwell Publishing Ltd.
A room of their own: the social landscape of infant sleep
Jennifer RoweSchool of Nursing, Griffith University, Nathan, Queensland, Australia
Accepted for publication 28 November 2002
ROWE J. Nursing Inquiry 2003; 10: 184–192A room of their own: the social landscape of infant sleepThis paper draws on findings of a study in which new and experienced mothers’ caregiving practices were investigated, inorder to examine social perspectives of infant sleep. Health professionals who work to support early parenting andpromote child health and well-being provide guidance to their clients concerning infant sleep cares. Currently, advice ispredominantly informed by understandings and strategies derived from Sudden Infant Death Syndrome (SIDS) risk reduc-tion campaigns and behavioural training models. The social context of caregiving is a significant if somewhat neglectedperspective. The analysis presented in this paper suggests that in sleep arrangements, a complex social locale is revealed,an elaboration of carers’ values and understandings about infants as developing persons, juxtaposed with their own desiresand needs. Tensions between child-centred nurturing and adult-focused concerns are expressed and reconciled in care-giving. These understandings may assist health professionals to develop proactive and responsive practices in the area ofearly childrearing support.
Key words: child health, co-sleeping, infant care, infant sleep, mothering, narrative.
The topic of sleep, that is how, where, when and with whoman infant sleeps, is an important one for parents, mostparticularly mothers as the primary carers, as well as for thehealth professionals who seek to support parenting practice.Attending to sleep needs is one of a number of seeminglyunremarkable cares (Murcott 1993) that represent much ofthe everyday reality of life with an infant. These cares depictparenting behaviours and also show ways in which the phys-ical, emotional and social, health and well-being of an infantis nurtured (Liem and Ling 1994). Mothers develop thesecares over time and in the context of their particular life-style. In the process they draw on their previous experiences,the wisdom of friends and family, as well as the advice andexpertise of parenting guides and health professionals.
Midwives and community child health nurses are pre-dominant among health professionals in Australia who are
involved in supporting early parenting. Various national andstate policy agendas (Commonwealth Department of Health1995; Commonwealth Department of Health 1997; Queens-land Health 2001) underpin services in which these practi-tioners conduct a range of physical and developmentalassessments as well as counsel parents about infant caressuch as feeding, settling, and sleep. Current advice on thetopic of sleep is informed first, by biomedical and publichealth discourse associated with the prevention of SuddenInfant Death Syndrome (SIDS), and second, by develop-mental psychology discourse. This paper aims to extend asocial perspective of caregiving in regard to infant sleep,arguing that knowledge of the social contexts or locales (Gid-dens 1991; Curtis and Jones 1998) within which practices aredeveloped is an important perspective for professionals toincorporate. To do this the paper draws upon the findingsof a qualitative study that explored the way mothers, as partof their experience of raising infants, developed specificcare practices associated with infant sleep. The paper con-centrates, primarily, on the implications these practices havefor infants.
Correspondence: Jennifer Rowe, School of Nursing, Griffith University, NathanCampus, Kessels Road, Nathan, Queensland, 4111, AustraliaE-mail: <[email protected]>

Social perspectives of infant sleep
© 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192 185
INFANT SLEEP, A BIOPHYSICAL AND SOCIAL ACTIVITY
Sleep is an essential biophysical and social activity (McKennaet al. 1993; Williams and Bendelow 1998). It is a phenomenon,which, in relation to infants, has been the focus of publichealth attention nationally and internationally, primarilybecause of the problem of SIDS and the efforts to reducemortality associated with it (Henderson-Smart, Ponsonbyand Murphy 1998). As part of this agenda, everyday care-giving has become a topic for research scrutiny, the outcomesinforming national parenting education campaigns. Guide-lines place emphasis on infant safety and suitable environ-ments and sleeping positions for infants (Scragg, Mitchelland Stewart 1996; Henderson-Smart, Ponsonby and Murphy1998; Beal and Byard 2000; Willinger et al. 2000; SIDSAustralia Online 2001).
Within this literature biomedical concerns dominate, yetsocial aspects of caregiving are also evident. For instance,there are investigations and debates concerning the relativesafety and benefits, not only of the position of an infant ona bed surface but also in proximity to others, that is, betweenco-sleeping (where this term refers to a number of sleeparrangements from bedsharing to room sharing), and soli-tary sleep arrangements (Mosko et al. 1993; Young 1998;Young, Sawczenko and Fleming 1998; Ball, Hooker andKelly 1999; Beal and Byard 2000; Buckley et al. 2002). It isaccepted that there are different cultural norms concerningthe place for infants to sleep and their proximity to their car-ers. Countries such as Australia, the United Kingdom andAmerica have a greater expectation of solitary sleep places incomparison to many other societies (Morelli et al. 1992;Ball, Hooker and Kelly 1999). However there is evidenceestablishing the bio-physically nurturing and protectivepotential of co-sleeping, which highlights the mutual bodilyresponsiveness between mother and infant in co-sleepingmaternal-infant pairs (McKenna et al. 1993; Mosko et al.1993; Yelland, Gifford and MacIntyre 1994; Mosko et al.1996; Young 1998; Young, Sawczenko and Fleming 1998).
A small body of literature reports research conductedfrom a developmental stance. In this view caregiving is con-structed as behaviour management, and is underpinned bythe idealisation of all-night sleep as an achievable norm andan unquestioned acceptance of a belief in the trainability ofinfants. (Quillin 1997; Hiscock and Wake 2002; Renfrewet al. 2002). There is also some literature that has pointed tothe tensions between expectations, ideals and actual care-giving practices (Morelli et al. 1992; Ball, Hooker and Kelly1999). However there is little emphasis or attention placedon a social view of the phenomenon, that is on how parents’
expectations, personal desires, beliefs and lifestyle influencethe development of practices, and how, in turn, this perspec-tive may inform professional guidance.
It is argued in the sociology literature, that sleep is a socio-logical phenomenon, albeit a neglected one, its role in socialinteraction most perceptible at ‘the intersection of physio-logical need, environmental constraint and socio-culturalelaboration’ (Williams and Bendelow 1998, 175, italics in ori-ginal). The manner in which mothers and other carers seekto nurture their infants’ sleep needs, as well as meet theirown needs and desires, presents such an intersection, oneaddressed in this paper, by examining everyday practicesin the lives of a group of middle-class urban Australianmothers.
While there are fewer risks to infant health and well-being in groups with high social and material capital than inones less well-resourced, middle-class women represent asignificant study population, for two reasons. First, they area group who seek assistance with their practices and soinformation about their needs and practices can assist healthprofessionals to support their parenting efforts. Second, it isrecognized that maternal experience is significantly differ-entiated through social conditions, such as social position orclass and ethnicity and there is assumed to be a trickle-oneffect exerted through middle-class members of society,effectively normalising certain practices as ‘right ways’ in thebroader community (Crook, Paluski and Walters 1992;Nakano Glenn, Chang and Forcey 1994; Turner 1996). Theway women, such as the participants of the current study,experience caregiving, is therefore of interest. Further, it isrecognized that while men increasingly share parentingtasks, it remains women who, in large part, organize house-holds. Thus whilst the development of practices also inter-sects with male partners’ experiences, these were not thefocus of this study, both a limitation but also a means offacilitating a clear focus on the experience of the primarycare givers, that is, the mothers.
THE STUDY
The study investigated and theorized ways in which new andexperienced mothers of an infant, specifically in a middleclass, urban context, constructed specific care practices.A qualitative approach based on narrative research princi-ples was adopted for the study. The approach taken wasto present accounts of women’s experiences, gatheredtogether from the fragments of stories they told during in-depth interviews (Holstein and Gubrium 1997; Emden1998). The process is an interpretive one of presenting andre-telling or theorising a phenomenon but in a way that

J Rowe
186 © 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192
sustains the context of personal experience (Denzin 1989;Crouch and Manderson 1993; Bergum 1997; Lupton andBarclay 1997).
The participants were 21 middle-class mothers, all withan infant aged between one and 12 months at the time of thestudy. The sampling approach was purposive (Patton 2002)and homogenous (Sandelowski 1995) in terms of socio-economic and geographical criteria, providing a means ofenhancing data adequacy and analytic credibility. Recruit-ment of participants was conducted through three mechan-isms, via public health sponsored well baby clinics (11), aprivate association playgroup (4) and convenience samplingvia personal networks (6). The participants in this studywere all aged 25 or older. Fourteen were first-time mothers,five had two children and two women, three. Highly educated,18 women had post secondary, technical or tertiary qualifi-cations. Nineteen of the women had male partners, twowere alone. All were Anglo-Saxon Australians. All the womenlived within the one urban district, another homogenizingfactor, in that the women had access to the same governmentand commercial, health and parenting support services.
The major data for the project was comprized of in-depth interviews, and reflective journals, completed byinterview participants. Ethics approval was granted by theresearcher’s University Human Research Ethics Committee.After providing written informed consent, each participanttook part in one interview. The interview was framed to be aminimally guided, yet focused conversation about her lifewith an infant. The interview sought to elicit a participant’smothering experiences and understandings, while also pro-viding her with access to the researcher’s interests in specificcares (Pawson 1996; Holstein and Gubrium 1997). Follow-ing the interview each participant was given a journal withcovering instructions and a page to use for each week of aone month period. Each was requested to make notes at leastonce a week, concerning anything she thought was interest-ing or different about her baby’s care. Six women returnedthese journals, a couple writing at great length about thingsthey found important, others making brief notes.
Each interview transcript was organized into a morecoherent presentation of the participant’s experience byremoving the bulk of questions and incidental words, as wellas by signposting the narrative content, using descriptiveheadings and numbers. In the next step, material belongingin a care topic was then moved out of the chronologicalorder of the interview transcript in order to produce a narra-tive concerning that topic (Riessman 1993, 2002; Gubriumand Holstein 1997; Emden 1998). This was then augmented,where possible, with material from journals. Through thisprocess a coherent if partial view was evoked, one that
captured each participant’s experience, including her actions,motives and understandings about infant cares. Furtheranalysis and interpretation was conducted by system-atically comparing all the available transcripts and narrativescase summaries. From this process, themes about sleepcares, reflecting the commonalities and distinctions inthe participants experiences, were developed and theorized(Morse and Field 1996; Gubrium and Holstein 1997). In thenext section of this paper the experiences of one partici-pant, Rachel, are presented in a narrative summary. Themesare then presented and discussed.
INFANT SLEEP: NURTURING THE BABY – SUSTAINING SELF
Rachel’s experience
Rachel has two children. A woman in her mid-thirties, shedoes not work outside the home, but rather stays at home tocare for the children. Her husband works long hours at hisjob. She has developed a network of friends, who also haveyoung children and has some support from her mother. Hersleep practices with each of her two infants have been dis-tinct. Her first child, now three, had slept in a crib beside herbed for just five days before she decided to move him to aseparate room:
I couldn’t stand it, I couldn’t stand the snuffling and every-thing and noises and I found that every time he snuffled orsomething I’d be almost out of the bed — you know I felt asif I were sleeping with one ear open. I moved him into thenursery into the cot then — two rooms down the corridorand I worried I wouldn’t hear him but you hear them if theywant to be heard.
For pragmatic reasons, her second child has co-slept withher quite a lot:
He was in a crib beside our bed ‘cause I was really worriedabout him waking John [her older son] but then he endedup in our bed which I swore never to do but I just found Igot more sleep … and I found I barely needed to wake tofeed but I think that’s why I got in such a mess with him —he’d cry and I’d attach him because I was lying down besidehim I’d go back to sleep and I don’t know if he had a properfeed … but it was a way of keeping my sanity with two kidsto look after.
Her experience was paradoxical, on the one hand:
We disturbed each other, I disturbed him, he’d disturb meand it’s there all the time, he can smell the milk.
and on the other hand:
I loved having him in the bed though from the point of viewof — it was a real bond, he was a lovely little thing, it was areal bonding thing …

Social perspectives of infant sleep
© 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192 187
She reflected on her practices:
it was an absolute needs thing and I didn’t look beyond that,to any sort of impact or anything like that …
I don’t know whether he’s (the second) a more social sortof child because he’s had the family bed thing and John(the first) from a very very early age, well he was down thecorridor in the nursery, so I’m not sure …
Rachel described the motive for her choices as ‘sanityprotecting’ and the results ‘sleep messes’. What is apparent isthat she developed arrangements that helped her respondto the needs of her situation and her family’s. However, therewere tensions for her, concerning what was right for theinfant’s development and socialisation, balanced againstwhat she perceived as right or ideal for herself, other familymembers and their lifestyle. Rachel’s story is not uncommonto that of other participants, if not in the substance of care-giving strategies, at least in terms of the web of contingency,desire and need that shaped them.
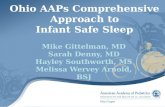
Close examination of the women’s stories reveals child-centred but also self- or other-centred desires and needs, thatinformed care activities, as well as the way sleep problemswere constructed. A central theme, nurturing the baby —
sustaining self, captures the issues predicaments and tensionsinherent in the women’s stories (see Fig. 1). It is fleshedout by describing a series of interleaving priorities that shapedtheir caregiving strategies or practices. These prioritiesare named; nurturing good sleep habits, nurturingsocial development, sustaining self and sustaining otherrelationships.
Nurturing good sleep habits
Woven through Rachel’s story was a concern for developinggood or proper sleep habits in her infants, a concernreflected in a number of the participants’ accounts. Estab-lishing proper sleep habits was a child-centred task, involv-ing decisions about where and when and how to get the babyto sleep. Where the baby slept was a central part of this task.
Chris, whose baby was 5 months old at the time of interview,had relocated her home when her baby was only a few weeksold. Prior to the move they were living with her mother andthe baby slept in a bassinette beside her bed. This was not agood sleep habit according to Chris, who said:
As soon as we moved up, the first night she was into her cot(in her own room). We didn’t want to get into that habit.
Just that sort of realisation that ‘mum will take me backinto her bed and then I’ll go to sleep’. You sort of don’t wantto get into the habit … I want her to know that where shesleeps is in her cot and that’s in her room …
Establishing routine in terms of both time and place forsleep was also central to the task of nurturing good sleephabits. Ingrid, for instance, described the sleep routine shehad organized for her baby, who was just over 4 months old-and slept in her own cot in her own room:
One of the niceties is that she’ll go to sleep around 6 in theevening so we’ve got the evening together and then I’ll puta disposable on her and feed around 9. She’ll sort of stiraround then. and then it’ll be around 1–1.30 and 4.00 (fora breastfeed).
All-night sleep is of course, part of an adult sleep habit, aresult of ongoing socialisation and bio-physiological develop-ment throughout childhood (Cooper 1994). Among theparticipants there seemed to be an underlying assumptionthat their babies, from their earliest weeks, could or shouldquite easily, learn to sleep for long night periods. Thisassumption shaped their expectations of good infant sleephabits, although for some, like Tina, the tension between theideal and reality was clear:
(it’s) a little dream we all fantasise about but um — well Idon’t think it’s realistic.
Good infant sleep habits were also linked to the women’sefforts to safeguard the sleep of other members of theirfamilies, a priority actioned by manipulating their infant’ssleep place and company. This was certainly a motivation forRachel as she persevered with co-sleeping with her youngest
Figure 1 Summary of central findings.

J Rowe
188 © 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192
child, despite her reservations. Marci put quite a lot of effortinto her evening infant feeding/sleep routine, one thatinvolved moving her baby from a cot in her bedroom to hisown room and introducing a formula feed prior to settlinghim in this space. In part she was concerned about herhusband’s sleep being disturbed:
Now we all go to bed at the same time which is more relax-ing for me. I don’t have to worry about waking Jim (herhusband) up.
She also felt this routine was nurturing for her infant:
Well they grow when they sleep.
Nurturing social development
The women in this study were all attuned to their infants’physical health and well-being. Fostering their children’spsycho-social development was another important and inter-esting focus of the women’s efforts that shaped caregivingand sleep practices. The value that they placed on independ-ence as a developmental goal was notable. Rachel, for exam-ple, pondered whether the different sleep arrangements shefostered in her two infants accounted for their differentsociability. Lotty, motivated by her understanding of thedevelopmental needs of her infant, had carefully prepareda nursery room:
Bright colours. I wanted lots of visual stimulation …What I’d heard is that it is extremely important for
children up to 10 to have constant stimulation, um also toencourage her to enjoy her own company.
Her baby was specifically allocated solitary time in this spaceto nurture independence.
Many of the women also went to great lengths to get theirbabies to go to sleep without nursing or the physical contactof others. This was also part of a desire to instil independ-ence in their children. Participants identified a range ofartifacts that helped them to provide nurturing contact, in waysthey assumed were soothing and settling. These approachesand devices allowed carers some distance and wooed thesenses of the baby. Ingrid, for instance, described a musicbox and a cuddle rug; Chris, a ‘wormy thing’ for her baby tosnuggle up to. The baby’s sleep place was also organized, bymany of the participants, to be as quiet as possible. Whilehuman noise and household routine were minimized, theywere replaced in some households with music or other vocalsources, such as audio-tapes of whale sounds.
Getting babies to sleep independently was not withoutproblem. It was a task linked explicitly by one participant, tothe broader goal of nurturing the child toward independentpersonhood. Georgia believed that the right thing to do was
to put her baby, while still awake, down in her crib, so theinfant would learn to put herself to sleep. Yet Georgia didn’tdo this; rather she nursed her baby to sleep. However sheworried that there would be a consequence to maintainingthis practice:
She doesn’t go to sleep by herself and that means she’snever going to be an independent person.
In contrast to this perspective, Karla explicitly placedgreater emphasis on the link between a child’s security (adesire of all the women), the infant’s bodily senses, and closeproximity. She consciously maximized closeness and bodilycontact for her infant in sleep:
Well I think that that’s a sense of insecurity, he feels insecurehe feels lost in such a big cot or something and I bring himinto bed with us and he settles down and goes to sleep, andthat time with us I think helps him feel secure … I thinkbabies, their senses, that’s what is most active at themoment.
Sustaining self
Sustaining self describes a range of self-focused prioritiesthat informed caregiving practices. Getting enough sleepwas the more pragmatic of these priorities. Yet there werealso issues about personal boundaries and sense of self thatwere reflected in participants’ stories.
Interestingly, one of the things that many of the womendescribed as challenging concerned the smell, noises andother bodily or sensory awareness and connection, experi-enced between themselves and their babies. They describedthese sensate experiences as disturbing, disrupting thedevelopment of good sleep habits in their infants or suffi-cient sleep for themselves. Rachel, for example, describedhow the sounds of her first baby, sleeping next to her bed,were disturbing. As a result, she moved him, placing himfurther away from her. Smell was a problem for her with hersecond baby. She complained that both her own and herbaby’s sleep was disturbed because he could smell her milk,an awareness with which she did not seem comfortable.Bound by other priorities, she continued to co-sleep but sheremained uneasy and did not accept this arrangement as agood sleeping habit.
Another woman, Oni, was more pragmatic. She was ableto normalize the close bodily contact she maintained withher second baby for sleep periods, worth sustaining in orderto do two things; nurture the infant and protect the sleep ofher husband and older daughter. She commented:
With Bela I do believe that going into the bassinette andbeing put into the bassinette after the feed meant that shevery quickly settled into patterns of sleeping longer,

Social perspectives of infant sleep
© 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192 189
whereas I’m sure with this one [who was described as a nap-per] she smells me, being next to me and has a quick slurp,etc.
The intensity of bodily sensitivity or awareness createddifficulties for Barbara who also described moving her veryyoung infant away from her. She was feeling tired followingher son’s birth, and after just a few days at home, she movedhim, stating:
Every time he moved, I was awake … I heard every move-ment that he did … I was listening too hard for him and hedidn’t even have to make any real noise for me to — I wasvery tired.
She believed that sleeping her baby in a crib next to her was,in her words:
Probably the worst thing I could have done.
Barbara’s expectation was that proper sleep habits wouldrevolve around her placing her baby close to her, for anumber of months. This plan was disrupted by herunexpected bodily awareness of her infant, a negativeexperience for her, as it was for a number of the women.Again in her case, the baby was relocated to a solitary sleepplace, effectively creating a boundary between her own bodyand that of her infant. She, like other women, perceivedsuch strategies as self-sustaining, a belief also reliant ontheir understanding of what a baby’s real communicationrepertoire consisted of. Creating solitary sleep places for thebabies altered the communicative possibilities that wereavailable to the infant and between mother and child andcreated boundaries. The boundaries were material, psycho-logical and social and reflect tensions in caregiving betweennurturing or child-centred concerns and self-sustaining oradult-centred concerns.
Sustaining other relationships
The participants’ caregiving was also shaped by a concernnot only for protecting the sleep of others in the house butalso for preserving or sustaining their other family relation-ships. Zoe, a mother of two children, discussed the impact ofher having first baby close by for sleep periods:
I found having her in the room really disturbing. I think, Iwas quite, for some reason with her I was regimented aboutsleep and we were going to have our sleep, I guess we weregoing to have our privacy. I guess it makes a fairly dramaticdifference to your relationship first up as well.
Space such as the parental bed and bedroom and time,particularly evenings was fairly quickly cordoned off or madeconditional to the children, babies re-organized into otherplaces for sleep. Overall, for the infants, sleep arrangements
were generally, and at first, quite dynamic, with many babiesstarting in a space quite close to their parents, or joining themduring the night. But the trajectory for the majority wasfor the infant to go to a special child place, most commonly aroom on their own, as early as possible, in a routine way.
A SENSE OF PLACE
The place in which infants sleep is more than a physicalspace. It may be thought of as a locale (Giddens 1991;Curtis and Jones 1998), that is, a place, rich with socialmeaning, mediating understandings about what is right,nurturing and accommodating, within the context ofspecific lifestyles (Giddens 1991). The analysis suggeststhis to be a place in which two important sets of prioritiesare reconciled. On the one hand, there are child-centredpriorities, those focused on nurturing. On the other hand,an infant’s sleep place emerges as a function of adult-focused priorities. These find expressions in the narrativesas needs and desires that sustain women’s sense of self andsense of order in their mothering and other subjectivities.From this study depictions of maternal experience andsubjectivity are provided; ones that support well recognizedand documented issues and tensions associated with earlychildrearing and motherhood. In addition, ways in whicheveryday caregiving strategies shape a child’s earliest socialexperience are revealed. This aspect of the findings isdiscussed further here.
The analysis suggests that infant sleep arrangements area place of infant learning and a path to inculcating in-dependence in the child, evidenced in the efforts of most ofthe participants to establish a solitary space for the infant tosleep in, to get the infant out of the adult bed, or to inducethe infant to sleep without nursing. Independence is cer-tainly perceived as an important developmental achieve-ment, one of the qualities of the self which have currency incontemporary Western society (Lupton 1994). This inter-pretation of the role of infant sleep practices is different tothat adopted in other studies, which have tended to focusupon trainability and behaviour management as develop-mental milestones (Pinilla and Birch 1993; Quillin 1997;Renfrew et al. 2002). It requires that the concept of fosteringindependence through everyday caregiving be acknowl-edged and existing practices challenged.
Cycles of dependence and individuation or attachmentand otherness mark the mother–infant relationship, withthe normal course being a gradual individuation of childfrom mother (Bowden 1997). Further, it has been arguedby Maurice Merleau-Ponty (1964, 124) that the inability ofinfants to distinguish themselves from others leads to an

J Rowe
190 © 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192
experience of, in the absence of others, ‘incompleteness’.Healthy psychosocial development, toward independentand autonomous personhood, thus requires that youngchildren have consistent and close contact (Chodorow 1978,1985; Bowden 1997). Everyday practices that organize infantsleep, embody these developmental cycles and reinforcesleep’s social role. The developing child may learn a sense ofbody, self, and others; which in time lead to independenceand autonomy.
The emphasis and value placed on a solitary sleep placefor infants, at least as an ideal, suggests that through thesepractices, infants’ lessons in bodily independence beginearly. Yet it is important to keep in mind that an infant isnot able to adjust the bedding, room temperature, airflow, physical contact, or choose who to communicate with,snuggle up to, or move to a space where they can see whatthey hear, smell what is familiar, or be closer to their carers(Nolan 1996). These activities are beyond the independ-ent physical or social ability of infants. Others suggestthat infants may be at risk without the bio-physiologicallynurturing qualities inherent in co-sleeping (Mosko et al.1993). The caregiving responses to SIDS risks outlined inprevention guidelines appeared to be accommodated by theparticipants of the present study. However, in the absence ofany perceived significant health risk indicators associatedwith solitary infant sleep arrangements, or public healthmessages promoting co-sleeping, other values and priorities,such as those discussed above, may shape sleep arrange-ments. In the context of the present study these includedidealising more distant arrangements as right ways, in turnproducing an ambivalence toward co-sleeping and its associ-ated bodily interactions.
Dialogue focusing upon sensate or bodily sensitivityor awareness and synchronicity as a parenting care tool,is not particularly accessible to women similar to theparticipants in this study. These sensitivities, if acknowl-edged, valued and promoted, may provide a strong mother-ing tool for women to use as caregivers by assisting them tobalance the often competing demands of nurturing theirinfants while meeting and sustaining their own needs.Explicitly valuing the communicative potential afforded inclose bodily orientation of mother (and/or other carers)and infant, may also serve the interests of nurturing secureattachment for the infant and later, independence andautonomy.
CONCLUSION
This study, while limited by its small and homogenouscontext, helps to bring sleep into the foreground as a
significant social practice. It provides evidence of social intri-cacies and their relationship to practical cares that areworthy of further inquiry. Of particular interest is inquiryinto the experiences and contexts of different socialgroups. Infant sleep arrangements emerge as a placerich with social meaning, and in which tensions betweenchild- and adult-centred interests are both expressed andreconciled. These understandings, along with further explor-ation of the social needs and ideals embedded in everydaycaregiving of their client groups, will assist health pro-fessionals to develop proactive and responsive practicesin the area of early childrearing.
REFERENCES
Ball H, E Hooker and P Kelly. 1999. Where will the babysleep? Attitudes and practices of new and experiencedparents regarding co-sleeping. American Anthropologist101: 143–51.
Beal S and RW Byard. 2000. Sudden Infant Death Syndromein South Australia 1968–97. Part 3: Is bed sharingsafe for infants? Journal of Paediatric Child Health 36: 552–4.
Bergum V. 1997. A child on her mind. The experience of becominga mother. CT: Bergin & Garvey.
Bowden P. 1997. Caring. A gender-sensitive ethics. London:Routledge.
Buckley P, RS Rigda, L Mundy and C McMillen. 2002. Inter-action between bed sharing and other sleep environ-ments during the first six months of life. Early HumanDevelopment 66: 123–32.
Chodorow N. 1978. The reproduction of mothering. Psychoanaly-sis and the sociology of gender. Berkeley, CA: University ofCalifornia Press.
Chodorow N. 1985. Beyond drive theory. Object relationsand the limits of radical individualism. Theory and Society14: 271–319.
Commonwealth Department of Health and Family Services.1997. The national health plan for young Australians. Can-berra: Australian Government Publishing Service.
Commonwealth Department of Health and Housing. 1995.The health of young Australians: A national health policy forchildren and young people. Canberra: Australian Govern-ment Publishing Service.
Cooper R, ed. 1994. Sleep. London: Chapman & Hall.Crook SJ, J Paluski and M Walters. 1992. Postmodernization.
Change in advanced society. London: Sage.Crouch M and L Manderson. 1993. New motherhood. Cultural
and personal transitions in the 1980s. Yverdon, Switzerland:Gordon and Breach.

Social perspectives of infant sleep
© 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192 191
Curtis S and IR Jones. 1998. Is there a place for geographyin the analysis of health inequality? Sociology of Health andIllness 205: 645–72.
Denzin NK. 1989. Interpretive interactionism. Newbury Park,CA: Sage.
Emden C. 1998. Conducting narrative analysis. Collegian 5: 34–9.Giddens A. 1991. Modernity and self identity. Cambridge:
Polity Press.Gubrium J and J Holstein. 1997. The new language of qualita-
tive method. New York: Oxford University Press.Henderson-Smart D, AL Ponsonby and E Murphy. 1998.
Reducing the risk of sudden infant death syndrome. Areview of the scientific literature. Journal of PaediatricChild Health 34: 213–29.
Hiscock H and M Wake. 2002. Randomized controlled trialof behavioural infant sleep intervention to improveinfant sleep and maternal mood. British Medical Journal324: 1062–5.
Holstein J and J Gubrium. 1997. Active interviewing. In Quali-tative research. Theory, method and practice, ed. D Silverman,113–29. London: Sage.
Liem I and I Ling. 1994. The challenge of migrant mother-hood: The childrearing practices of Chinese first-timemothers in Australia. In Asian mothers, Australian birth.Pregnancy, childbirth and childrearing: The Asian experiencein an English speaking country, ed. PL Rice, 135–60. Mel-bourne: Ausmed Publications.
Lupton D and L Barclay. 1997. Constructing fatherhood.London: Sage.
Lupton D. 1994. Medicine as culture. Illness, disease and the bodyin Western societies. London: Sage.
McKenna JJ, E Thoman, T Anders, A Sadeh, V Schechtmanand S Glotzbach. 1993. Infant-parent co-sleeping in anevolutionary perspective: implications for understand-ing infant sleep development and the sudden infantdeath syndrome. Sleep 16: 263–82.
Merleau-Ponty M. 1964. The child’s relations with others. InThe primacy of perception and other essays on phenomenologicalpsychology, the philosophy of art, history and politics, ed. JMEdie, 96–155. Evanston: Northwestern University Press.
Morelli GR, B Rogoff, D Oppenheim and D Goldsmith. 1992.Cultural variations in infants’ sleeping arrangements: Ques-tions of independence. Developmental Psychology 28: 604–13.
Morse J and P Field. 1996. Nursing research: The application ofqualitative approaches. London: Chapman & Hall.
Mosko S, JJ McKenna, M Dickel and L Hunt. 1993. Parent-infant co-sleeping: The appropriate context for the studyof infant sleep and implications for Sudden Infant DeathSyndrome (SIDS) Research. Journal of Behavioural Medi-cine 16: 589–610.
Mosko S, C Richard, JJ McKenna and S Drummond. 1996.Infant sleep architecture during bedsharing and possibleimplications for SIDS. Sleep 19: 677–84.
Murcott A. 1993. Purity and pollution: Body managementand the social place of infancy. In Body matters: Essays onthe sociology of the body, eds S Scott and D Morgan, 122–34.London: Falmer Press.
Nakano Glenn E, G Chang and L Forcey. 1994. Mothering:Ideology, experience, and agency. New York: Routledge.
Nolan M. 1996. When mother knows best. Modern Midwife 6:11–13.
Patton M. 2002. Qualitative research and evaluation methods,3rd edn. Thousand Oaks, CA: Sage.
Pawson R. 1996. Theorizing the interview. British Journal ofSociology 47: 295–314.
Pinilla T and L Birch. 1993. Help me make it through thenight: Behavioural entrainment of breast-fed infants’sleep patterns. Pediatrics 91: 436–44.
Queensland Health Child and Youth Health Unit. 2001. Astrategic policy framework for children’s and young people’shealth, 2001–6. Brisbane: Queensland Health.
Quillin S. 1997. Infant and mother sleep patterns during 4thpostpartum week. Issues in Comprehensive Pediatric Nursing20: 115–23.
Renfrew MJ, S Lang, L Martin and M Woolridge. 2002. Inter-ventions for influencing sleep patterns in exclusivelybreastfed infants (Cochrane Review). The CochraneLibrary. Oxford: Update Software.
Riessman CK. 1993. Narrative analysis. Newbury Park, CA: Sage.Riessman CK. 2002. Analysis of personal narratives. In
Handbook of interview research: Context and method, edsJF Gubrium and JA Holstein, 695–710. Thousand Oaks,CA: Sage.
Sandelowski M. 1995. Sample size in qualitative research.Research in Nursing and Health 18: 179–83.
Scragg RK, E Mitchell, R Stewart et al. 1996. Infant room-sharing and prone sleeping position in sudden infantdeath syndrome. Lancet 347: 7–13.
SIDS Australia Online. Reducing the risk of Sudden InfantDeath Syndrome. www.sidsaustraliaonline.org.au accessed31 March 2001.
Turner BS. 1996. The body and society : Explorations in socialtheory. London: Sage Publications.
Williams SJ and G Bendelow. 1998. The lived body: Sociologi-cal themes, embodied issues. London: Routledge.
Willinger M, C Ko, HJ Hoffman, R Kessler and M. Corwin.2000. Factors associated with caregivers’ choice for infantsleep position 1994–98: The National Infant Sleep Posi-tion Study. JAMA, the Journal of the American MedicalAssociation 283: 2135–42.

J Rowe
192 © 2003 Blackwell Publishing Ltd, Nursing Inquiry 10(3), 184–192
Yelland J, S Gifford and M MacIntyre. 1994. Explanatorymodels about maternal and infant health and SuddenInfant Death Syndrome among Asian-born mothers. InAsian mothers, Australian birth. Pregnancy, childbirth andchildrearing: The Asian experience in an English speakingcountry, ed. PL Rice, 175–90. Melbourne: Ausmed.
Young J, A Sawczenko and P Fleming. 1998. Observations ofnight-time behaviour between low SIDS risk infants andtheir mothers: A longitudinal comparison between room-sharing and bed-sharing. Human Development 50: 224–5.
Young J. 1998. Babies and bedsharing. MIDIRS MidwiferyDigest 8: 364–9.