A review of the use of human factors classification ...
30
A review of the use of human factors classification frameworks that identify causal factors for adverse events in the hospital setting R.J. Mitchell a *, A.M. Williamson a,b , B. Molesworth b and A.Z.Q. Chung b a Transport and Road Safety (TARS) Research, University of New South Wales, Sydney, Australia; b School of Aviation, University of New South Wales, Sydney, Australia (Received 8 August 2013; accepted 4 June 2014) Various human factors classification frameworks have been used to identified causal factors for clinical adverse events. A systematic review was conducted to identify human factors classification frameworks that identified the causal factors (including human error) of adverse events in a hospital setting. Six electronic databases were searched, identifying 1997 articles and 38 of these met inclusion criteria. Most studies included causal contributing factors as well as error and error type, but the nature of coding varied considerably between studies. The ability of human factors classification frameworks to provide information on specific causal factors for an adverse event enables the focus of preventive attention on areas where improvements are most needed. This review highlighted some areas needing considerable improvement in order to meet this need, including better definition of terms, more emphasis on assessing reliability of coding and greater sophistication in analysis of results of the classification. Practitioner Summary: Human factors classification frameworks can be used to identify causal factors of clinical adverse events. However, this review suggests that existing frameworks are diverse, limited in their identification of the context of human error and have poor reliability when used by different individuals. Keywords: patient safety; hospital; medical errors; causal factors; reliability 1. Introduction It is estimated that clinical adverse events contribute to between 44,000 and 98,000 deaths each year in the USA (Kohn, Corrigan, and Donaldson 2000); in the UK this figure has been estimated at 2181 based on data from 2004 to 2005 (Shah et al. 2004), whereas in Australia during the same time frame there were 1809 known surgical and medical care-related deaths (Henley and Harrison 2009). The estimated proportion of hospitalised adverse events has ranged from 3.8% to 16.6% across countries (Brennan et al. 1991; Wilson et al. 1995; Vincent, Neale, and Woloshynowych 2001; Davis et al. 2002; Baker et al. 2004). Identifying and describing adverse event characteristics are the essential initial first step to improving patient safety. Patient safety has been recognised by the World Health Organization (WHO) as a global area of importance, with the WHO calling for the ‘strengthen[ing of] science-based systems necessary for improving patients’ safety and the quality of health care’ (WHO 2006). The core feature of any improvement to health system performance relating to patient safety is having the capacity to report, analyse and feedback information from adverse incident reporting systems, so preventive action can be undertaken. Over the past decade, there has been a growth in the development and number of human factors classification systems in health care, including both in hospital and in general practice settings (Elder and Dovey 2002; Woloshynowych et al. 2005). The focus of these classification frameworks has largely been on adverse outcomes as a result of medication errors (Santell et al. 2003), although some setting-specific areas have also been examined, such as for the Emergency Department (Cosby 2003), and other types of adverse events, including during air medical transport (MacDonald, Banks, and Morrison 2007). Within health-care settings, there have been various attempts to analyse adverse events from a human factors perspective. The most widely known approach is the London Protocol developed by Vincent et al. (2000). The Protocol prescribes a systematic process to analyse adverse events and is largely based on Reason’s Organisational Accident Causation Model (Reason 1997). While mostly viewed as a success, the Protocol has inherent limitations, the most notable being the focus on describing what went wrong and linking this to surface, job or task-related features associated with the event, as opposed to identifying the underlying cause of human behaviour (such as the type of error) and understanding the context in which it occurs. A human factors approach involves investigating all factors contributing to the occurrence of an adverse event. In this approach, it is essential to establish how human behaviour fits among the range of factors that cause adverse events in order to understand its causal role and how human behavioural failures might be prevented. q 2014 Taylor & Francis *Corresponding author. Email: [email protected] Ergonomics, 2014 Vol. 57, No. 10, 1443–1472, http://dx.doi.org/10.1080/00140139.2014.933886
Transcript of A review of the use of human factors classification ...

A review of the use of human factors classification frameworks that identify causal factors foradverse events in the hospital setting
R.J. Mitchella*, A.M. Williamsona,b, B. Molesworthb and A.Z.Q. Chungb
aTransport and Road Safety (TARS) Research, University of New South Wales, Sydney, Australia; bSchool of Aviation, University of NewSouth Wales, Sydney, Australia
(Received 8 August 2013; accepted 4 June 2014)
Various human factors classification frameworks have been used to identified causal factors for clinical adverse events.A systematic review was conducted to identify human factors classification frameworks that identified the causal factors(including human error) of adverse events in a hospital setting. Six electronic databases were searched, identifying 1997articles and 38 of these met inclusion criteria. Most studies included causal contributing factors as well as error and errortype, but the nature of coding varied considerably between studies. The ability of human factors classification frameworks toprovide information on specific causal factors for an adverse event enables the focus of preventive attention on areas whereimprovements are most needed. This review highlighted some areas needing considerable improvement in order to meet thisneed, including better definition of terms, more emphasis on assessing reliability of coding and greater sophistication inanalysis of results of the classification.
Practitioner Summary: Human factors classification frameworks can be used to identify causal factors of clinical adverseevents. However, this review suggests that existing frameworks are diverse, limited in their identification of the context ofhuman error and have poor reliability when used by different individuals.
Keywords: patient safety; hospital; medical errors; causal factors; reliability
1. Introduction
It is estimated that clinical adverse events contribute to between 44,000 and 98,000 deaths each year in the USA (Kohn,
Corrigan, and Donaldson 2000); in the UK this figure has been estimated at 2181 based on data from 2004 to 2005 (Shah
et al. 2004), whereas in Australia during the same time frame there were 1809 known surgical and medical care-related
deaths (Henley and Harrison 2009). The estimated proportion of hospitalised adverse events has ranged from 3.8% to 16.6%
across countries (Brennan et al. 1991; Wilson et al. 1995; Vincent, Neale, and Woloshynowych 2001; Davis et al. 2002;
Baker et al. 2004). Identifying and describing adverse event characteristics are the essential initial first step to improving
patient safety.
Patient safety has been recognised by the World Health Organization (WHO) as a global area of importance, with the
WHO calling for the ‘strengthen[ing of] science-based systems necessary for improving patients’ safety and the quality of
health care’ (WHO 2006). The core feature of any improvement to health system performance relating to patient safety is
having the capacity to report, analyse and feedback information from adverse incident reporting systems, so preventive
action can be undertaken.
Over the past decade, there has been a growth in the development and number of human factors classification systems in
health care, including both in hospital and in general practice settings (Elder and Dovey 2002; Woloshynowych et al. 2005).
The focus of these classification frameworks has largely been on adverse outcomes as a result of medication errors (Santell
et al. 2003), although some setting-specific areas have also been examined, such as for the Emergency Department (Cosby
2003), and other types of adverse events, including during air medical transport (MacDonald, Banks, and Morrison 2007).
Within health-care settings, there have been various attempts to analyse adverse events from a human factors
perspective. The most widely known approach is the London Protocol developed by Vincent et al. (2000). The Protocol
prescribes a systematic process to analyse adverse events and is largely based on Reason’s Organisational Accident
Causation Model (Reason 1997). While mostly viewed as a success, the Protocol has inherent limitations, the most notable
being the focus on describing what went wrong and linking this to surface, job or task-related features associated with the
event, as opposed to identifying the underlying cause of human behaviour (such as the type of error) and understanding the
context in which it occurs. A human factors approach involves investigating all factors contributing to the occurrence of an
adverse event. In this approach, it is essential to establish how human behaviour fits among the range of factors that cause
adverse events in order to understand its causal role and how human behavioural failures might be prevented.
q 2014 Taylor & Francis
*Corresponding author. Email: [email protected]
Ergonomics, 2014
Vol. 57, No. 10, 1443–1472, http://dx.doi.org/10.1080/00140139.2014.933886

Errors, defined as ‘the failure of a planned action to proceed as planned’ (US Institute of Medicine 2000), have been
analysed retrospectively using human factors classification frameworks in health care, but these studies have differed in the
way that medical errors are classified. Many studies used job-related descriptions of the nature of errors. For example, in a
study of errors in radiology, the error classification included ‘illegible request’ or ‘duplicate request’ (Martin 2005). This
type of approach is informative in providing direction in which task or job areas errors are most likely to occur, but it is not
descriptive in terms of the type of cognitive failure that explains why the particular error type occurred. The main advantage
of cognitive classifications of error is that they provide insight into the nature of error itself which is helpful in
understanding both why it occurred and developing methods to prevent a recurrence.
However, there are some disadvantages of a cognitive approach. The most prominent being when it is used in isolation,
just knowing the cognitive failure type says nothing about the context in which the error occurs. Several error classification
techniques used human factors classification methods in other settings and have had this problem, for example the Human
Factors Accident Classification System and the Systematic Human Error Reduction and Prediction Approach both of which
provide significant detail on the cognitive typology of error, but both have difficulty providing interpretation of the meaning
of the error type for preventive action in the setting in which it occurred.
A significant number of studies in health care have used human factors classification frameworks, but they often vary in
the type of causal factors they identify and the depth and/or detail of the factors examined. The classification frameworks
vary significantly in the sophistication of their development including their capacity to be reliable tools for describing the
causes of adverse events. To be successful in providing insight into the involvement of human factors in adverse events,
analytic methods need to: reflect how human factors sits in the causal sequence leading to an incident; understand the nature
of human factors involvement, especially the role and nature of human failure; and the classification and coding must
include reliable and valid measures.
The aim of this paper is to review the range of human factors classification systems that have been applied in hospital
settings and to evaluate their ability to provide information about the human factors involvement in adverse events.
Specifically, it aims to: (1) identify from the published literature human factors classification frameworks that have been
used to identify the causal factors to medical adverse events in a hospital setting and (2) describe the type of adverse events
examined, the type of causal factors able to be identified (including error) and whether any inter-rater reliability assessment
was conducted.
2. Method
2.1 Search strategy
The review was undertaken using Medline, PsycINFO, Embase, CINAHL, Web of Science and PubMed from 1980 to
January 2012. Each database was searched using the search string: (‘error’ OR ‘slip’ OR ‘human factor’ OR ‘mistake’ OR
‘unsafe act’ OR ‘accident’) AND (‘patient safety’ OR ‘adverse event’ OR ‘complications of care’ OR ‘patient harm’ OR
‘iatrogenic’) AND (‘tool’ OR ‘framework’ OR ‘classification’ OR ‘model’ OR ‘taxonom*’). The PubMed search was
conducted by searching the ‘title’ and ‘abstract’ only, and the PsycINFO database search was conducted using ‘abstract’
only. The limitations on the search tactics for these two databases were necessary due to the nature of the keyword search
terms. For PubMed, if ‘all fields’ were searched this resulted in .3000 citations and for PsycINFO it resulted in .11,000
citations. All non-English research was excluded. In addition to the systematic keyword search, snowballing using journal
reference lists was conducted to identify additional articles. Grey literature searches were conducted to identify relevant
documents and reports.
2.2 Stage one – abstract review
The abstracts of citations identified were independently assessed by three reviewers (RM, BM, AW) for relevance. For stage
one, a broad search strategy was adopted to limit the exclusion of possible relevant studies. Citations moved to stage two if
they described the creation or use of a human factors classification framework for medical adverse events. For this review,
human factors were considered in a broad sense to include ‘unsafe acts (including human error and violations), and also
other factors, such as individual, organisational, technological, and environmental factors, that might be considered to have
an effect on human or system performance’.
A classification framework was considered to be a conceptual, hierarchical structure that enabled the classification of
factors involved in an incident. For stage one, citations were also included for further review if there was evidence in the
abstract that classification of human error had occurred, even though no specific classification framework was mentioned.
The index of concordance between the three reviewers was 92.5%. The reviewers met and resolved any disagreements on
citation abstracts by consensus. All citations that were assessed as relevant moved to stage two.
R.J. Mitchell et al.1444

2.3 Stage two – article review and data extraction
For each citation that was identified as relevant for inclusion, the full-text article was assessed by three reviewers (RM, BM,
AW) for relevance. A full-text article moved to the next stage if it described the use of a human factors classification
framework that identified the causal factors to medical adverse events that had occurred in a hospital setting. This included
classification systems that had been developed for another industry, but had been adapted for use in a hospital setting.
However, it excluded studies that identified potential failure modes. The index of concordance between the three reviewers
was 72.4%.
During this stage, two reviewers (RM, BM) extracted information from the final selection of full-text articles. The
following information, where available, was extracted from the final selection of full-text articles: author(s) and publication
year, study aim, type of adverse event, setting and sample size, reliability assessment method and result(s), and the types of
causal factors identified. A third reviewer (AC) compared the extract information for consistency, and disagreements were
resolved by consensus.
3. Results
Citations that were identified from each database using the search string were imported into the reference management
software, Endnote X3 (Thomson Reuters 2009). After deletion of duplicate references, erratum and corrections, 1997
references were identified using the search strategy.
3.1 Stage one
The initial review of citation abstracts identified 242 citations for further full article review. The abstracts identified either
mentioned a classification framework (or tool) that had been developed and/or used to identify the human factors
contribution to adverse events or there was evidence that classification of human error had occurred, even though no specific
classification framework was mentioned in the abstract.
3.2 Stage two
The review of 242 full-text articles identified 38 articles that used classification frameworks that identified causal factors to
adverse events in a hospital setting. There were also 22 potential articles identified from reference lists of full-text articles
during the stage two review. Of these, none were retained as they did not meet the review criteria.
Appendix 1 summarises the details of the 38 studies identified in the review and Table 1 summaries the key strengths
and limitations of the classification frameworks. The majority of published research that used classification frameworks to
Table 1. Strengths and limitations of existing human factors classification frameworks that identify the causal factors of adverse eventsin a hospital setting.
Strengths Limitations
Most human factors classification frameworks recordedinformation on a fairly comprehensive list of causalfactors, leading to a wide range of event causalfactors being able to be identified
Almost all human factors classification frameworks describedwhat went wrong in the context of either job/task errors orcognitive errors, rather than using both approaches. Only usingcognitive error classifications provides no information on thecontext in which the error occurs, while only using job/taskerrors fails to identify the cause of human behaviour
Around half the human factors classification frameworksrecorded information on job/task errors (e.g. duplicaterequest), which are useful to identify during whichactivity errors are likely to occur
There was considerable variety in the quantity, depth and definitionsof the causal factors examined in each human factors classificationframework. The frameworks did not often included factors relatedto the patient, e.g. complexity of the patient’s medical condition
Half the human factors classification frameworks recordedinformation on cognitive errors (e.g. skill-, rule-,knowledge-based errors), which can provide insight intothe nature of human error
None of the human factors classification frameworks examined thecausal sequence of events leading to the occurrence of theadverse incident
One-third of the human factors classification frameworks did not havea theoretical model underpinning the human factors framework
There was limited assessment of inter-rater reliability and noassessment of intra-rater reliability for the human factorsclassification frameworks
Ergonomics 1445

identify the causal factors in medical adverse events in the hospital setting took place in the USA (57.9%) and Europe
(26.3%). The size of studies varied considerably, with 21.1% involving fewer than 30 cases (including the four case studies)
and 21.1% involving more than 1000 cases with the remainder of studies between these two extremes. Around half of the
studies (55.3%) looked at error-related outcome events, mainly involving medication-related errors (26.3% of studies), with
studies of diagnostic, surgical and medical errors (5.3% of studies each) and single studies of errors including anaesthetic,
hypertension maintenance, medical imaging, nursing and simulation training errors (2.6% of cases each).
Approaching one-third (31.6%) of studies focussed on different types of incidents, some of which were specific types,
such as wrong-site surgery, neurosurgery and spinal surgery incidents (each with one study), but most were general and
unspecified such as avoidable failures, unintended incidents, adverse events and health-care incidents. In most studies, the
source data were from existing databases (68.4%) but six studies (15.8%) involved observational methodologies and three
involved questioning of health-care professionals by survey (7.9%) or interview (2.6%). Importantly, half the studies failed
to provide a definition of the outcome or adverse event that was the objective of the study with roughly equal proportions
involving general patient safety or adverse events and different types of error.
In over two-thirds of studies (71.1%), the framework was based on a specific model or an existing categorisation, in
particular Reason’s organisational accident causation model (31.6%) (Reason 1997), the Joint Commission on
Accreditation of Healthcare Organizations (JCAHO) classification including the Eindhoven classification of error (13.2%)
(Chang et al. 2005; Van der Schaaf and Habraken 2005) or the National Coordinating Council for Medication Error
Reporting and Prevention (NCCMERP) classification using the MEDMARX database (13.2%) (NCCMERP 2013). Just
over one-third (36.8%) developed the classification system for the context from the data set itself.
Most studies used a hierarchical classification system involving at least two levels of classification (63.2%) and up to
four levels in two studies. Most of the studies involved classification of both error type and contributing causal factors
(68.4%), 21.1% only classified contributing causal factors and 13.2% only classified error type. Of the studies that classified
causal factors, the most common were organisational factors, like supervision and training (76.3% of studies),
communication and teams (63.2%) and equipment-related factors (57.9%). In addition, some studies included factors
relating to procedures (42.1%), patients (42.1%), environment (26.3%) and workload (23.7%).
The studies that included classification of error type were split fairly equally between task-related classifications
(42.1%) and cognitive-related classifications (55.3%) and two studies used both (5.3%). While the task-related
classifications often reflected the nature of the outcome being studied, one-third used theMEDMARX classification (34.2%)
as they were applied to medication errors (Phillips et al. 2001; Hicks et al. 2004; Hicks, Cousins, and Williams 2004; Hicks,
Becker, and Jackson 2008; Santell et al. 2009). Half of the cognitive classifications of error type involved the skill, rule,
knowledge classification based on Rasmussen’s work (1982) or Reason’s modification of it (1990). Seven studies (18.4%)
also included classification of violations also based on the Reason classification. Three studies used the Eindhoven error
classification (Nast et al. 2005; Henneman et al. 2010; Rodrigues et al. 2011). The remainder involved variations mainly of
the Reason classification, including simple classification like active failures or not, faulty information processing or
cognitive or non-cognitive errors to more complex classifications including inattention, memory failure and confusion (Itoh,
Omata, and Andersen 2007), or carelessness and distraction, poor assessment of the situation (Kantelhardt et al. 2011).
Most studies simply described the occurrence of causal factors and error types by reporting of univariate results for the
presence or not of individual factors and types. Despite many studies putting forward a systems approach to the analysis of
causes, very few studies looked at the patterns of causation for patient safety incidents through looking at relationships
between causal features. Two studies looked at the relationships between causal factors and outcomes by statistical
modelling (Wiegmann et al. 2007; Chang and Mark 2009), both including organisational causal factors in the modelling but
not error types. Two studies described the framework for studying relationships between causal features through case
studies alone (Eagle, Davies, and Reason 1992; Taylor-Adams, Vincent, and Stanhope 1999).
Just over one-third of the studies (34.2%) conducted some sort of reliability assessment as part of the research, including
one (2.6%) study where the results of the reliability assessment were published in a second article relating to the same
research (Brennan et al. 1991, cited in Leape et al. 1991) and four (10.5%) studies used the same classification framework
where a reliability assessment was conducted as part of other research (Forrey, Pedersen, and Schneider 2007, cited in Hicks
et al. 2004; Hicks, Cousins, and Williams 2004; Hicks, Becker, and Jackson 2008; Santell et al. 2009).
The method of reliability assessment varied and included Cohen’s Kappa statistic (31.6%), Yule’s Q (2.6%),
Cronbach’s a (2.6%) and percent agreement (2.6%). Two (5.3%) studies reported using informal consensus to achieve
agreement on classifications. Of the 12 studies that involved a formal reliability estimate, most (75.0%) looked at the
reliability of coding of causal factors or error types, while the remainder looked only at the classification of outcome events
such as actual/potential adverse events, or whether a failure was involved or not. The studies that looked at reliability of the
classification of outcome typically involved a binary decision and found high reliabilities (e.g. Kappa scores, Cronbach’s aand Q scores exceeding 0.8) (Battles and Shea 2001; Tran and Johnson 2010; Albayati et al. 2011). The reliabilities of
R.J. Mitchell et al.1446

causal factors including error were considerably more variable. Some studies reported very good reliabilities such as Kappa
scores around 0.8 (Friedman et al. 2007; Tourgeman-Bashkin, Shinar, and Zmora 2008; Parker et al. 2010), whereas for
others Kappa scores were more moderate (e.g. 0.61 (Forrey, Pedersen, and Schneider 2007)) or low (e.g. 0.34, 0.42 (Itoh,
Omata, and Andersen 2007); 0.38 (Astion et al. 2003)). One study reported the results for four observers in a study of spinal
surgery, and found that Kappa scores ranged from 0 to 0.85 between observers and that reliability varied greatly between
factors being coded (Mirza et al. 2006).
4. Discussion
The current study identified a comparatively small number of peer-reviewed published research papers that have attempted
to identify causal factors of adverse events in a hospital setting, with only 38 studies identified in the last 32 years. While a
number of standard taxonomic systems have emerged, such as the JCAHO Patient Safety Event Taxonomy (Chang et al.
2005), most of the studies reviewed developed new approaches for understanding the causes of patient safety events using
existing databases and sometimes data collected for the purpose by observation, surveys or interview.
This review demonstrated that most of the classification frameworks were fairly comprehensive and acknowledged the
breadth of causes that might potentially be involved in patient safety including human factors-related causes, although there is
considerable diversity in the type of human factors classification frameworks used. Someof this diversity naturally occurred due
to the nature of the event studied,with causal factors identified for spinal surgery differing for those related tomedication errors,
yetmost classification systems had common categories, such as organisational factors. Classification systems ranged frombasic
frameworks with only single broad-level categories, to more sophisticated frameworks breaking down these single broad
categories into between two to four sub-levels to describe in more detail the causal factors of adverse events.
Most taxonomies included a number of different causal factors, reflecting thewide range of possible features that could play
a role in patient safety events, although there was considerable variation in specific factors between taxonomies. Almost all
studies included causal factors falling into broad organisational, equipment, communications and teamwork categories. The
majority of taxonomies included some classification of error type and these were split fairly evenly between task-related
classifications, such as the NCCMERP taxonomy formedication errors, and cognitive-related classifications based onReason’s
work. In contrast, only a few of the classification frameworks considered the role of patients in contributing to the adverse event,
with just over one-third (36.8%) identifying causal factors related to the patient. The role of the complexity of the patient’s
medical condition was rarely included. Leape et al. (1991), while not identifying complexity issues in their classification
framework, stated that complexity of the health condition or treatmentwas amajor determinant of adverse event risk, alongwith
patient co-morbid health conditions, and recommended that information on these items as potential contributing factors be
obtained.Benavidez et al. (2008) used the only framework that identified any complexity issues thatmay have contributed to the
event in terms of ‘rare or complex anatomy’ of the patient. Clearly, new classification systems need to be comprehensive and
reflect the potential factors and agents that might contribute to adverse events.
While comprehensiveness is an essential attribute of a patient safety classification system, to be useful, the classification and
codingmust alsobe reliable. The codingof factorsmust be consistent and reproducible between coders and betweenoccasions of
coding. Reliability assessments provide information on inter-rater (or intra-rater) agreement and can provide an indication of the
agreement between raters on the identification of events of interest (Stemler 2004). High inter-rater reliability, especially for
adverse event and causal factor identification, is important for validity of the framework and ultimately for the development of
effective preventive strategies.Unfortunately,most of the studies identified in this review failed to examine this important aspect
of their classification system. Although around one-third made at least some mention of reliability, it was often at the highest
level of coding and no studies looked at intra-coder reliability. Nevertheless, where assessed, the reliability scores reportedwere
generally moderate to good (Altman 1991). The exceptions were two studies that attempted coding of deeper classifications.
Itoh, Omata, and Andersen (2007) found that the reliability of the coded content was only fair, andMirza et al. (2006) obtained
quite low reliabilities between pairs of observers identifying causal factors to adverse surgical events. Reliability could be
improved by ensuring that causal factor categories are mutually exclusive, by developing a data dictionary that contains clear
definitions of each causal factor, along with examples of causal factor classifications. Improvements can also be made by
conducting exhaustive pilot testing of the framework and by providing training opportunities for staff in using the framework,
and regular discussion of difficult event classifications (Gliklich and Dreyer 2010).
There are a number of reasons why deeper coding might be expected to be less reliable. First, it can be difficult to
categorise the types of causal factors identified in the frameworks due to their divergent classification structures. For
example, when examining communication problems, Chang and colleagues (Chang et al. 2005; Chang and Mark 2009)
include ‘communication problems’ as a second sub-level classification within ‘team factors’, while Graber, Franklin, and
Gordon (2005) includes ‘teamwork or communications’ within ‘organisational factors’, as does Meurier (2000). However,
Mirza et al. (2006) and Leape et al. (1991) include ‘communication failures’ under ‘system factors’. Itoh, Omata, and
Ergonomics 1447

Andersen (2007), Phillips et al. (2001), Santell et al. (2009), Taxis and Barber (2003) and Webb et al. (1993) all include
‘communication’ problems as a broad first-order category. Some of these differences between frameworks will stem from
their method of development. Some classification frameworks were derived through naturalistic means, such as by grouping
natural categories within existing data (Runciman et al. 1998), while others were derived from a theoretical basis and/or
literature reviews (Vincent, Tayor-Adams, and Stanhope 1998; ElBardissi et al. 2007) so terms used for causal factors may
not be mutually exclusive, standardised nor formally defined. Second, some of the features included in the taxonomies may
be difficult to verify. This particularly applies to error-type coding especially of errors in decision-making or violations,
both of which require knowledge of the person’s intention. This is usually not known from the sources used to code adverse
events and is only available from the individual involved and only post hoc, which may in turn influence the recall of the
event. Both cases will make coding more difficult and unreliable. It is important to have high inter-rater reliability scores in
the identification of the circumstances leading to these events as this is an indicator that the classification framework can be
used consistently by a range of individuals to reflect the causes of adverse events.
Many of the studies reviewed recognised the importance of a systems-based approach to understanding the causes of
adverse events, in particular by reference to the Reason model of organisational accidents. The major conceptual basis to
this approach is that accidents occur due to interactions between features in the sequence of causes leading to the accident
event. In this approach, errors are created by systems that make them either more likely to occur in the first place or fail to
prevent them from occurring through use of safety barriers. Despite this acknowledgement, almost all of the studies simply
catalogued the existence of causal factors, errors and error types. They failed to look at the relationships between errors and
error types and the types of factors or events that typically occur with them. It is known from studies of occupational
fatalities, for example, that particular factors influence the occurrence of different types of errors. For instance, in an
analysis of the causes of all workplace fatalities in Australia over a three year period, errors in skilled behaviour were most
likely to be preceded by unsafe standard operating procedures, whereas errors in applying known rules were more likely to
occur with a range of other precursors (Williamson, Feyer, and Cairns 1996). Similarly, an analysis of the causes of safety-
related incidents in aircraft maintenance showed that errors due to memory lapses occurred most often under conditions of
time pressure (Hobbs and Williamson 2003). In the current study, the importance of other factors in the system in which the
error occurred is recognised, but no studies examined the relationships between these factors and particular error types.
Further work in this area might consider the capability of classification frameworks in identifying a causal sequence of
events to the adverse event. This would provide additional assistance to identify appropriate preventive measures. Eagle,
Davies, and Reason (1992) recognise the benefit of establishing a temporal sequence of key events leading to medication
errors. Likewise, Itoh, Omata, and Andersen (2007) also considered that obtaining information on the ‘relationship between
errors, situations, performance shaping factors and consequences’ was necessary to effectively establish the root causes of
an adverse event. Clearly, just knowing that an error occurred is not very useful for developing strategies to prevent them.
We need to understand when and why errors occur and what factors make them more likely. This requires more in-depth
analysis than is currently being conducted in studies of the causes of adverse events.
A notable feature of nearly half of the studies was that the outcome or focus of the study was unclear and not defined.
Occasionally, the outcome of interest was inherently defined such as wrong-site surgery events (Chang et al. 2005);
however, lack of definition is a particular issue for outcomes such as avoidable failures (Albayati et al. 2011) that could
include a range of possible outcomes, both severe and minor. The problem was not limited to general adverse events. Error-
related outcomes were also often not clearly defined, including surgical errors (ElBardissi et al. 2007), hypertension-related
errors (Lee, Cho, and Bakken 2010) and anaesthetic errors (Nast et al. 2005; Nyssen and Blavier 2006). Even more
troubling, a number of studies used the terms medical adverse events and medical errors interchangeably (e.g. Friedman
et al. 2007) which simply add to the confusion. Clear definitions of adverse events exist: for example, in the seminal paper
by Leape et al. (1991), an adverse event was defined as an unintended injury that was caused by medical management and
that resulted in measurable disability. Similarly, there are many definitions of error, usually involving planned or intended
human action that does not achieve its planned or intended outcome (Reason 1990). It seems that many of these attempts to
develop taxonomies for patient safety need firmer foundations in which the objective or outcome is much better defined.
It should be acknowledged that some of the classification frameworks were developed for a specific purpose, such as
MEDMARX, which is used to report on and classify medication-related adverse events. Therefore, it is possible that all
categories of causal factors in all classification frameworks may not necessarily be relevant for all types of adverse incidents
due to their being designed to principally identify and describe a particular type of event, such as medication errors.
However, there is still likely to be value in adopting a classification framework for a more generic application (i.e. for all
types of adverse events) to enable comparisons between facilities, if the information gained was still specific enough to
target effective preventive measures for all types of adverse events. The WHO has recognised the need for such standard
terminology in the patient safety areas, developing a conceptual framework for patient safety (WHO 2009). However, in its
current form, the WHO’s conceptual framework does not provide unique identifiers nor definitions for each item, key
R.J. Mitchell et al.1448

‘concepts’, ‘classes’ of items and hierarchical links and relationships between items are not clearly identified, not all of the
classification categories are mutually exclusive or exhaustive, and the effectiveness of the framework to classify causal
factors to adverse events is yet to be tested extensively in the field (Schulz et al. 2009; Feijter et al. 2012). It is essential that
any recommended classification framework designed for use in health care uses recognised and well-defined standard terms
relating to adverse events so it provides the capability to benchmark safety performance internationally, nationally and
between local facilities.
There are limitations of the current review. It is possible that some unpublished research and grey literature were not
examined and thus some classification frameworks that have been used in a hospital setting were not considered. It is also
possible that some of the frameworks examined had some form of reliability testing conducted as part of their development
process that was not reported, although clearly it should have been.
5. Conclusion
Few peer-review studies have been published regarding the identification of causal factors of adverse events in a hospital
setting. Having information on specific causal factors for an adverse event enables attention to be focused on areas where
improvements are most needed. This enables, as much as possible, information to assist with the elimination or limitation of
the effect of antecedent events in the contribution to adverse events. This review has highlighted some opportunities for
improvement in the development and use of patient safety classification systems. These include that, first, more emphasis
needs to be placed on developing comprehensive, but reliable coding systems that allow understanding of what led to the
event. This means clearly defined outcomes and well-defined, mutually exclusive classifications that include the range of
possible factors that might contribute to the patient safety outcomes of interest. Second, and most importantly, more effort
needs to be placed on obtaining an understanding of and why these adverse events occur through more sophisticated
analysis of the relationships between causal factors, including the role of human factors, especially that of error.
Acknowledgements
R. Mitchell was supported by an ARC-linkage post-doctoral fellowship (LP0990057). A. Williamson is supported by an NHMRC SeniorResearch Fellowship. The views expressed in this paper are the views of the authors that do not necessarily reflect the views or policies ofthe funding agencies.
Funding
This research was funded by an Australian Research Council linkage grant (LP0990057) and the NSW Clinical Excellence Commissionand the NSW Ministry of Health.
References
Albayati, M. A., M. S. Gohel, S. R. Patel, C. V. Riga, N. J. W. Cheshire, and C. D. Bicknell. 2011. “Identification of Patient SafetyImprovement Targets in Successful Vascular and Endovascular Procedures: Analysis of 251 Hours of Complex Arterial Surgery.”European Journal of Vascular and Endovascular Surgery 41 (6): 795–802.
Altman, D. 1991. Practical Statistics for Medical Research. London: Chapman and Hall.Astion, M. L., K. G. Shojania, T. R. Hamill, S. Kim, and V. L. Ng. 2003. “Classifying Laboratory Incident Reports to Identify Problems
that Jeopardize Patient Safety.” American Journal of Clinical Pathology 120 (1): 18–26.Baker, G., P. Norton, V. Flintolf, R. Blais, A. Brown, J. Cox, E. Etchells, W. Ghali, P. Hebert, S. Majumdar, M. O’Beirne, L. Palacios-
Derflingher, R. Reid, S. Sheps, and R. Tamblyn. 2004. “The Canadian Adverse Events Study: The Incidence of Adverse Eventsamong Hospital Patients in Canada.” Canadian Medical Association Journal 179 (11): 1678–1686.
Battles, J. B., and C. E. Shea. 2001. “A System of Analyzing Medical Errors to Improve GME Curricula and Programs.” AcademicMedicine 76 (2): 125–133.
Benavidez, O. J., K. Gauvreau, K. J. Jenkins, and T. Geva. 2008. “Diagnostic Errors in Pediatric Echocardiography: Development ofTaxonomy and Identification of Risk Factors.” Circulation 117 (23): 2995–3001.
Brennan, T., L. Leape, N. Laird, L. Hebert, R. Localio, A. Lawthers, J. Newhouse, P. Weiler, and H. Hiatt. 1991. “Incidence of AdverseEvents and Negligence in Hospitalized Patients. Results of the Harvard Medical Practice Study 1.” The New England Journal ofMedicine 324 (6): 370–376.
Cagliano, A. C., S. Grimaldi, and C. Rafele. 2011. “A Systemic Methodology for Risk Management in Healthcare Sector.” Safety Science49 (5): 695–708.
Catchpole, K. R., A. E. B. Giddings, M. R. de Leval, G. J. Peek, P. J. Godden, M. Utley, S. Gallivan, G. Hirst, and T. Dale. 2006.“Identification of Systems Failures in Successful Paediatric Cardiac Surgery.” Ergonomics 49 (5–6): 567–588.
Chang, Y. 2007. Testing a Theoretical Model for Severe Medication Errors, . PhD, University of North Carolina at Chapel Hill.Chang, Y., and B. A. Mark. 2009. “Antecedents of Severe and Nonsevere Medication Errors.” Journal of Nursing Scholarship 41 (1):
70–78.
Ergonomics 1449

Chang, A., P. Schyve, R. Croteau, D. O’Leary, and J. Loeb. 2005. “The JCAHO Patient Safety Event Taxonomy: A StandardizedTerminology and Classification Schema for Near Misses and Adverse Events.” International Journal for Quality in Health Care17 (2): 95–105.
Chipps, E., C. E. Wills, R. Tanda, E. S. Patterson, V. Elfrink, M. Brodnik, S. Schweikhart, and N. Ryan-Wenger. 2011. “RegisteredNurses’ Judgments of the Classification and Risk Level of Patient Care Errors.” Journal of Nursing Care Quality 26 (4): 302–310.
Cosby, K. S. 2003. “A Framework for Classifying Factors that Contribute to Error in the Emergency Department.” Annals of EmergencyMedicine 42 (6): 815–823.
Davis, P., R. Lay-Yee, R. Briant, W. Ali, A. Scott, and S. Schug. 2002. “Adverse Events in New Zealand Public Hospitals I: Occurrenceand Impact.” New Zealand Medical Journal 115 (1167): U271.
Eagle, C. J., J. M. Davies, and J. Reason. 1992. “Accident Analysis of Large-Scale Technological Disasters Applied to an AnestheticComplication.” Canadian Journal of Anaesthesia 39 (2): 118–122.
ElBardissi, A. W., D. A.Wiegmann, J. A. Dearani, R. C. Daly, and T. M. Sundt III. 2007. “Application of the Human Factors Analysis andClassification SystemMethodology to the Cardiovascular Surgery Operating Room.” Annals of Thoracic Surgery 83 (4): 1412–1418,(discussion 1418–1419).
Elder, N. C., and S. M. Dovey. 2002. “Classification of Medical Errors and Preventable Adverse Events in Primary Care: A Synthesis ofthe Literature.” Journal of Family Practice 51 (11): 927–932.
Feijter, J., W. de Grave, A. Muijtjens, A. Scherpbier, and R. Koopmans. 2012. “A Comprehensive Overview of Medical Error in HospitalsUsing Incident-Reporting Systems, Patient Complaints and Chart Review of Inpatient Deaths.” PLoS ONE 7 (2): e31125.
Forrey, R., C. Pedersen, and P. Schneider. 2007. “Interrater Agreement with a Standard Scheme for Classifying Medication Errors.”American Journal of Health-System Pharmacy 64 (2): 175–181.
Friedman, A. L., S. R. Geoghegan, N. M. Sowers, S. Kulkarni, and R. N. Formica. 2007. “Medication Errors in the Outpatient Setting –Classification and Root Cause Analysis.” Archives of Surgery 142 (3): 278–283.
Gliklich, R., and N. Dreyer. 2010. Registries for Evaluating Patient Outcomes: A User’s Guide. Rockville: Agency for HealthcareResearch and Quality.
Graber, M. L., N. Franklin, and R. Gordon. 2005. “Diagnostic Error in Internal Medicine.” Archives of Internal Medicine 165 (13):1493–1499.
Henley, G., and J. Harrison. 2009. “Injury Deaths, Australia 2004–05.” Injury Research and Statistics Series Number 51. Adelaide,AIHW. INJCAT 127.
Henneman, E. A., J. P. Roche, D. L. Fisher, H. Cunningham, C. A. Reilly, B. H. Nathanson, and P. L. Henneman. 2010. “ErrorIdentification and Recovery by Student Nurses Using Human Patient Simulation: Opportunity to Improve Patient Safety.” AppliedNursing Research 23 (1): 11–21.
Hicks, R. W., S. C. Becker, and D. G. Jackson. 2008. “Understanding Medication Errors: Discussion of a Case Involving a UrinaryCatheter Implicated in a Wrong Route Error.” Urologic Nursing 28 (6): 454–459.
Hicks, R. W., S. C. Becker, D. Krenzischeck, and S. C. Beyea. 2004. “Medication Errors in the PACU: A Secondary Analysis ofMEDMARX Findings.” Journal of PeriAnesthesia Nursing 19 (1): 18–28.
Hicks, R. W., D. D. Cousins, and R. L. Williams. 2004. “Selected Medication-Error Data from USP’s MEDMARX Program for 2002.United States Pharmacopeia.” American Journal of Health-System Pharmacy 61 (10): 993–1000.
Hobbs, A., and A. Williamson. 2003. “Associations between Errors and Contributing Factors in Aircraft Maintenance.” Human Factors45 (2): 186–201.
Itoh, K., N. Omata, and H. B. Andersen. 2007. A Human Error Taxonomy for Analysing Healthcare Reporting Culture and Its Effects onSafety Performance. European Safety and Reliability Conference (ESREL 2007), Stavanger, NORWAY, Taylor & Francis.
Itoh, K., N. Omata, and H. Andersen. 2009. “A Human Error Taxonomy for Analysing Healthcare Incident Reports: Assessing ReportingCulture and Its Effects on Safety Performance.” Journal of Risk Research 12 (3–4): 485–511.
Kantelhardt, P., M. Muller, A. Giese, V. Rohde, and S. R. Kantelhardt. 2011. “Implementation of a Critical Incident Reporting System ina Neurosurgical Department.” Central European Neurosurgery 72 (1): 15–21.
Kim, C. H., and M. Kim. 2009. “Defining Reported Errors on Web-Based Reporting System Using ICPS from Nine Units in a KoreanUniversity Hospital.” Asian Nursing Research 3 (4): 167–176.
Kohn, L., J. Corrigan, and M. Donaldson. 2000. To Err is Human: Building a Safer Health System. Washington, DC: National AcademiesPress.
Leape, L. L., T. A. Brennan, N. Laird, A. G. Lawthers, A. R. Lacolio, B. A. Barnes, L. Hebert, J. P. Newhouse, P. C. Weiler, and H. Hiatt.1991. “The Nature of Adverse Events in Hospitalized Patients: Results of the Harvard Medical Practice Study II.” New EnglandJournal of Medicine 324 (6): 377–384.
Lee, N. J., E. Cho, and S. Bakken. 2010. “Identification of Hypertension Management-Related Errors in a Personal Digital Assistant-Based Clinical Log for Nurses in Advanced Practice Nurse Training.” Asian Nursing Research 4 (1): 19–31.
MacDonald, R. D., B. A. Banks, and M. Morrison. 2007. Epidemiology of Adverse Events in Air Medical Transport. Canadian HealthcareSafety Symposium 2007, Ottawa, CANADA, Blackwell.
Martin, C. 2005. “A Survey of Incidents in Radiology and Nuclear Medicine in the West of Scotland.” The British Journal of Radiology78: 913–921.
Meurier, C. E. 2000. “Understanding the Nature of Errors in Nursing: Using a Model to Analyse Critical Incident Reports of Errors whichhad Resulted in an Adverse or Potentially Adverse Event.” Journal of Advanced Nursing 32 (1): 202–207.
Mirza, S. K., R. A. Deyo, P. J. Heagerty, J. A. Turner, L. A. Lee, and R. Goodkin. 2006. “Towards Standardized Measurement of AdverseEvents in Spine Surgery: Conceptual Model and Pilot Evaluation.” BMC Musculoskeletal Disorders 7: 53.
Nast, P. A., M. Avidan, C. B. Harris, M. J. Krauss, E. Jacobsohn, A. Petlin, W. C. Dunagan, and V. J. Fraser. 2005. “Reporting andClassification of Patient Safety Events in a Cardiothoracic Intensive Care Unit and Cardiothoracic Postoperative Care Unit.” Journalof Thoracic and Cardiovascular Surgery 130 (4): 1137–1143.
R.J. Mitchell et al.1450

NCCMERP (National Coordinating Council for Medication Error Reporting and Prevention). 2013. “Type of Medication Errors.”Accessed August 6, 2013, from http://www.nccmerp.org/medErrorCatIndex.html
Nyssen, A., and A. Blavier. 2006. “Error Detection: A Study in Anaesthesia.” Ergonomics 49 (5–6): 517–525.Parker, S. E., A. A. Laviana, R. K. Wadhera, D. A. Wiegmann, and T. M. Sundt III. 2010. “Development and Evaluation of an
Observational Tool for Assessing Surgical Flow Disruptions and Their Impact on Surgical Performance.” World Journal of Surgery34 (2): 353–361.
Phillips, J., S. Beam, A. Brinker, C. Holquist, P. Honig, L. Y. Lee, and C. Pamer. 2001. “Retrospective Analysis of Mortalities Associatedwith Medication Errors [erratum appears in Am J Health Syst Pharm 2001 Nov 15; 58 (22): 2130].” American Journal of Health-System Pharmacy 58 (19): 1835–1841.
Portaluri, M., F. I. M. Fucilli, E. A. L. Gianicolo, F. Tramacere, M. C. Francavilla, C. De Tommaso, R. Castagna, and G. Pili. 2010.“Collection and Evaluation of Incidents in a Radiotherapy Department a Reactive Risk Analysis.” Strahlentherapie Und Onkologie186 (12): 693–699.
Rasmussen, J. 1982. “Human Errors: A Taxonomy for Describing Human Malfunction in Industrial Installations.” Journal ofOccupational Accidents 4: 311–333.
Reason, J. 1990. Human Error. New York: Cambridge University Press.Reason, J. 1997. Managing the Risks of Organisational Accidents. Aldershot: Ashgate.Rodrigues, S., P. Brandao, L. Nelas, J. Neves, and V. Alves. 2011. “A Logic Programming Approach to Medical Errors in Imaging.”
International Journal of Medical Informatics 80 (9): 669–679.Runciman, W. B., S. C. Helps, E. J. Sexton, and A. Malpass. 1998. “A Classification for Incidents and Accidents in the Health-Care
System.” Journal of Quality in Clinical Practice 18 (3): 199–211.Santell, J., R. Hicks, J. McMeekin, and D. Cousins. 2003. “Medication Errors: Experience of the United States Pharmacopeia (USP)
MEDMARX Reporting System.” The Journal of Clinical Pharmacology 43 (7): 760–767.Santell, J. P., J. G. Kowiatek, R. J. Weber, R. W. Hicks, and C. A. Sirio. 2009. “Medication Errors Resulting from Computer Entry by
Nonprescribers.” American Journal of Health-System Pharmacy 66 (9): 843–853.Schulz, S., D. Karlsson, C. Daniel, H. Cools, and C. Lovis. 2009. “Is the ‘International Classification for Patient Safety’ a Classification?”
Proceedings of MIE 2009, K. Adlassnig, Amsterdam, IOS Press BV. 150: 502–506.Shah, R. K., E. Kentala, G. B. Healy, and D. W. Roberson. 2004. Classification and Consequences of Errors in Otolaryngology. Annual
Meeting of the Triological-Society, Scottsdale, AZ, Lippincott Williams & Wilkins.Stemler, S. 2004. “A Comparison of Consensus, Consistency, and Measurement Approaches to Estimating Interrater Reliability.”
Practical Assessment, Research, and Evaluation 9 (4). Accessed June 23, 2014, from http://PAREonline.net/getvn.asp?v=9&n=4Taxis, K., and N. Barber. 2003. “Causes of Intravenous Medication Errors: An Ethnographic Study.” Quality & Safety in Health Care
12 (5): 343–347.Taylor-Adams, S., C. Vincent, and N. Stanhope. 1999. “Applying Human Factors Methods to the Investigation and Analysis of Clinical
Adverse Events.” Safety Science 31 (2): 143–159.Thomson Reuters. 2009. EndNote X3. Carlsbad, CA: Thomson Reuters.Tourgeman-Bashkin, O., D. Shinar, and E. Zmora. 2008. “Causes of Near Misses in Critical Care of Neonates and Children.” Acta
Paediatrica 97 (3): 299–303.Tran, D., and M. Johnson. 2010. “Classifying Nursing Errors in Clinical Management within an Australian Hospital.” International
Nursing Review 57 (4): 454–462.US Institute of Medicine. 2000. To Err is Human: Building a Safer Health System. Washington, DC: National Academy Press.Van der Schaaf, T. W., and M. N. P. Habraken. 2005. PRISMA-Medical: A Brief Description. Eindhoven: Eindhoven University of
Technology.Vincent, C., G. Neale, and M. Woloshynowych. 2001. “Adverse Events in British Hospitals: Preliminary Retrospective Record Review.”
British Medical Journal 322: 517–519.Vincent, C., S. Taylor-Adams, E. Chapman, D. Hewett, S. Prior, P. Strange, and A. Tizzard. 2000. “How to Investigate and Analyse
Clinical Incidents: Clinical Risk Unit and Association of Litigation and Risk Management Protocol.” British Management Journal320: 777–781.
Vincent, C., S. Tayor-Adams, and N. Stanhope. 1998. “Framework for Analysing Risk and Safety in Clinical Medicine.” British MedicalJournal 316 (11 April): 1154–1157.
Webb, R. K., M. Currie, C. A. Morgan, J. A. Williamson, P. Mackay, W. J. Russell, and W. B. Runciman. 1993. “The Australian IncidentMonitoring Study: An Analysis of 2000 Incident Reports.” Anaesthesia & Intensive Care 21 (5): 520–528.
WHO (World Health Organization). 2006. Fifty-Ninth World Health Assembly. Patient Safety. Report by the Secretariat, Geneva.WHO. 2009. The conceptual framework for the International Classification for Patient Safety. Geneva: World Alliance for Patient Safety,
WHO.Wiegmann, D. A., A. W. ElBardissi, J. A. Dearani, R. C. Daly, and T. M. Sundt III. 2007. “Disruptions in Surgical Flow and Their
Relationship to Surgical Errors: An Exploratory Investigation.” Surgery 142 (5): 658–665.Williamson, A., A. Feyer, and D. Cairns. 1996. “Industry Differences in Accident Causation.” Safety Science 24 (1): 1–12.Wilson, R., W. Runciman, R. Gibberd, T. Harrison, L. Newby, and J. Hamilton. November 6, 1995. “The Quality in Australian Health
Care Study.” Medical Journal of Australia 163: 458–471.Woloshynowych, M., S. Rogers, S. Taylor-Adams, and C. Vincent. 2005. “The Investigation and Analysis of Critical Incidents and
Adverse Events in Healthcare.” Health Technology Assessment 9 (19): 1–158.
Ergonomics 1451

Appendix
1.
Summaryofresearch
usingclassificationfram
eworksthat
identified
thecausalfactors
ofadverse
eventsin
ahospital
setting.
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
Astionet
al.
(2003)
Developanduse
aclassificationsystem
tocharacterise
incident
reportsrelatedto
lab-
oratory
services
Adverse
events
(actual
orpotential)
Academ
icmedical
centrein
theUSA,
June2000–September
2001.A
totalof129
laboratory
incident
reportswereexam
ined.
Ofthese,122were
potential
adverse
events,6wereactual
adverse
eventsand1
involved
actual
and
potential
adverse
events
Inter-raterreliability
measuredusing
Cohen’sK-statisticand
was
0.79forthe
identificationofthe
typeofevent(i.e.
actual
versuspoten-
tial),0.10forprevent-
ability,0.38for
cognitive/non-cogni-
tiveerrortype
1Non-cognitiveonly
(i.e.slips)
1Cognitiveonly
1Cognitiveandnon-cognitive
1Unable
todetermine
Albayatiet
al.
(2011)
Investigateavoidable
failuresin
patient
safety
forpatients
undergoingvascular
andendovascular
procedures
Avoidable
failures
Therewere1145fail-
uresidentified
from
1847eventsfrom
Sep-
tember
2009to
May
2010at
StMary’s
Hospital,London
Inter-raterreliability
was
assessed
forfailure
detection.Cronbach’s
awas
0.84
1Absence
1Communicationfailure
1Decision-related
surgical
error
1Directequipmentfailure
1Equipmentunavailability
1Equipment/workspacemanagem
entfailure
1Equipmentconfigurationfailure
1External
pressures
1External
resourcefailure
1Fatigue
1Faultresolutionfailure
1Patient-relatedproceduraldifficulties
1Planningfailure
1Procedure-related
error
1Psychomotorerror(general)
1Psychomotorerror(surgical-related)
1Psychomotorerror(radiological-related)
1Resourcemanagem
ent
1Safetyconsciousness
1Team
conflict
1Technical
failure
1Vigilance/awarenessfailure
Battles
andShea
(2001)
Comparisonstudyto
testthereliabilityof
therootcause
classifi-
cationprocess
ofthe
Eindhoven
Classifi-
cationModel
Medical
errors
Atotalof25cases
from
emergency
medicineandintensive
care
from
ateaching
hospital
intheUSA
Classificationofroot
causeswas
assess
usingYule’s
Q,witha
correlationof0.86
1Technical
1external
1design
1construction
1materials
1Organisational
1external
1protocols/procedures
(Continued)
R.J. Mitchell et al.1452

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1transfer
ofknowledge
1managem
entpriorities
1culture
1Knowledge-based
behaviour
1Rule-based
behaviour
1qualifications
1coordination
1verification
1intervention
1monitoring
1Skill-based
behaviours
1slip
1tripping
1Other
factors
1patient-related
Benavidez
etal.
(2008)
Describeataxonomy
forandexam
ine
diagnostic
errors
inpaediatric
echocardiography
Diagnostic
errors
Children’s
Hospital
Boston,USA,Decem
-ber
2004–August
2007.Around50,660
echocardiogramsper-
form
edand87diag-
nostic
errors
identified
Inform
alconsensus
usedto
finalisecateg-
orisationoferror,
severity,preventability
androotcause
1Administrativeordataentryerrors
1incorrectnam
eassigned
toim
agingdata
1schedulingerror
1incorrectdataentry
1Proceduralorconditional
factors
1failure
toconfirm
patientidentity
ordiagnosis
1incomplete
physicalexam
ination
1poorim
agingenvironment
1failure
toim
proveim
agingconditions
1Communicationorinform
ationerrors
1lackingormisleadingpatienthistory
1noaccess
topriorstudies
1failure
toreportcritical
findingsin
atimely
fashionto
referringphysician
1incorrectrequisition
1Cognitiveerrors
1insufficientknowledgebase
1insufficienttechnical
skills
1faultydatasynthesis
1lackofconsiderationofpatient’ssituation/
conditionrelevantto
diagnosis
1misidentification/interpretationofafinding
1premature
case
closure
1distractionbyother
diagnoses/findings/
focusedquestion
1under
appreciation/considerationof
afinding
(Continued)
Ergonomics 1453
Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1over
appreciationofafinding
1confirm
ationbias
1incorrect/im
proper
calculation
1Technical
factors
1artefact
1modalitylimitation
1pooracoustic
windows
1equipmentmalfunction
1Patient-ordisease-related
factors
1rareorcomplexanatomy
1misleadinganatomyorphysiology
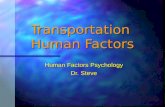
Cagliano,
Grimaldi,and
Rafele(2011)
Operationalise
Reason’s
theory
of
failuresbydeveloping
amethodologyto
investigatehealth-care
processes
andrelated
risksim
pactingeither
directlyorindirectly
onpatients
Drugmanagem
ent
process
inaphar-
macy
A1372bed
teaching
hospital
locatedin
Torino,Italy.Thiswas
anexam
pleapplication
Nil
1Internal
risk
sources
1organisational
1organisational
structure
1human
resources
1operations
1technology
1inform
ationsystem
1equipment
1communication
1inform
ationexchanges
1communicatingvariationsanddecisions
1structure
1layout
1networks
1External
risk
sources
1product
supplying
1deliverylead
times
1qualityofdelivered
products
1documentationmanagem
ent
1delivered
item
s1fi
nance
1supplier
assets
1contractspecifications
1environment
1guidelines
byregional
council
1social
issues
1epidem
iological
events
1naturalevents
(Continued)
R.J. Mitchell et al.1454
Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
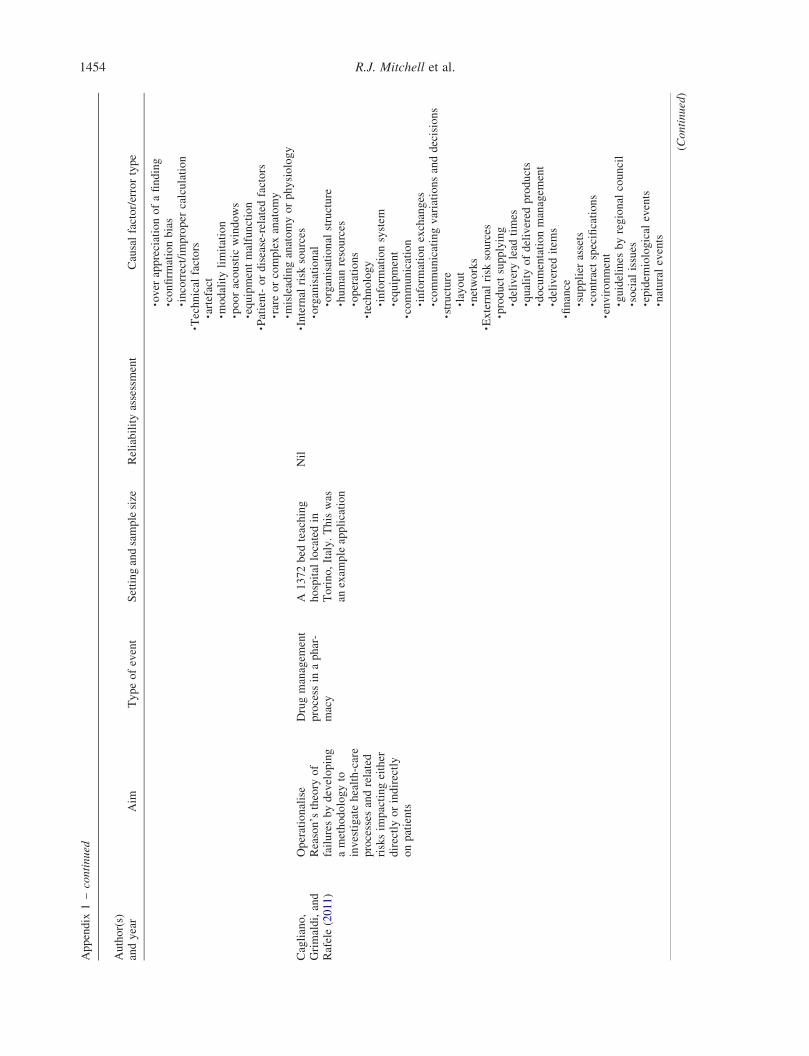
Catchpole
etal.
(2006)
Developaprospective
directobservation
methodologyforiden-
tifyingweaknessesin
thesystem
ofsurgery
Majorandminor
failuresin
surgery
Atotalof24paediatric
cardiacsurgeriesin
the
UK,October
2003–
July
2004.Therewere
366minorfailures
identified
Nil
1Threats
1culturalandorganisational
threats,e.g.
external
pressures,fatigue,safety
consciousness
1patientthreats,e.g.patient-sourced
procedural
difficulties,temperature
controldifficulties
1taskthreats,e.g.cannulationdifficulties,fault
resolutionfailure
1environmentalthreats,e.g.equipment/work-
spacemanagem
entfailure,external
resource
failure
1Errors
1technical
errors,e.g.decision-related
surgical
error,expertise/skillfailures
1non-technical
errors,e.g.planningfailure,
vigilance/awarenessfailure
Changet
al.
(2005)
Developandapply
amethodofclassifi-
cationfornear-misses
andadverse
events.
Wrongsite
sur-
geries
JointCommissionsen-
tinel
eventdatain
the
USA,January1995–
Decem
ber
2002.
Identified
209wrong
site
surgeries
Nil
1Organisational
1external
1managem
ent
1maintenance
oforganisational
resources
(selection,training,staffing)
1monetarybudgets
1organisational
culture
1chainofcommand
1delegationofauthority
andresponsibility
1communicationchannels
1form
alaccountability
1safetyculture
1protocols/processes
1processes
(tim
epressure,incentivesystem
s,schedules)
1organisational
procedures(perform
ance
standards,objectives,documentation,
instructionsaboutprocedures)
1oversight(riskmanagem
ent,establishment
anduse
ofsafety
programmes)
1transfer
ofknowledge
1supervision
1training
1Technical
1facilities–equipment/materials
1design,construction
(Continued)
Ergonomics 1455

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1malfunction,obsolescence
1availability
1external
1Error(actual
andnearmisses)
1patientfactors
1practitioner
1skill-based
1rule-based
1knowledge-based
1unclassifiable
1external
1Violations
1negligence
1recklessness
1intentional
rule
violations
Chang(2007)
Investigatethecharac-
teristicsofnursing
unitsthat
contribute
tomedicationerrors
Severemedication
errors
Atotalof286nursing
unitsin
146acute
care
hospitalsin
theUSA,
January–June2003for
firstgrouphospitals
andJanuary–June
2004forsecondgroup
hospitals.Therewas
anaverageof3.71errors
over
sixmonths
Nil
1Work
environmentfactors
1carecomplexity
1work
dynam
ics
1RN
proportion
1RN
hours
1Team
factors
1communicationwithphysicians
1communicationwithpharmacists
1expertise
1commitmentto
care
1Personfactors
1education
1unitexperience
1Supportservices
availability
1unit-dose
system
1CPOE
1automated
medicationadministrationsystem
1IV
team
services
1transcribingorders
1pharmacistconsultation
1Patientfactors
1age
1health
1previoushospitalisation
(Continued)
R.J. Mitchell et al.1456

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
ChangandMark
(2009)
Comparetheantece-
dentsofsevereand
non-severemedication
errors
Severeandnon-
severemedication
errors
Atotalof146acute
care
hospitalsin
the
USA.Duringasix-
month
period,1671
observationswere
conducted,withan
averageof0.61severe
and3.86non-severe
medicationerrors
per
month
Nil
1Work
environmentfactors
1work
dynam
ics
1RN
hours
1Team
factors
1communicationwithphysicians
1nursingexpertise
1Personfactors
1education
1experience
1medication-related
supportservices
1Patientfactors
1age
1healthstatus
1previoushospitalisation
Chippset
al.
(2011)
Exam
inenurses’jud-
gem
entsoferror
classificationandlevel
ofrisk
severityassoci-
ated
witherrors;deter-
minewhether
thereare
differencesin
error
classificationandrisk
severityjudgem
entsby
years
ofexperience,
clinical
specialty,level
ofeducationandjob
title,
anddescribe
nurses’judgem
ents
aboutspecificfactors
contributingto
anerror
andtheassociationof
contributingfactors
withrisk
severity
judgem
ents
Fourclinical
vign-
ettes
Survey
of435nurses
whoreceiveem
ails
from
theOhio
Nurses
Association(9%
response
rate)
Nil
1Knowledgeandexperience
1inadequateknowledge
1inadequateclinical
experience
1poorclinical
decision-m
aking
1Clinical
practice
1compromised
physicalstateofnurse
1automatic/habitual
response
1poorhandoff
1Failure
tofollow
standardsofpractice
1Work
environment
1excessiveworkload
1poorteam
work
1stressfulworkingenvironment
1unexpectedchangein
workload
1disruption/interruptionin
workflow
Eagle,Davies,
andReason
(1992)
Toillustrate
theprin-
cipal
featuresofthe
active/latentfailure
model
usingacase
reportofpulm
onary
aspirationofgastric
contents
Casestudy
Operatingroom,
unspecified
hospital.
Onecase
studyin
Canada
Nil
1Human
error
1Personnel
1Equipment
1Procedures
1Policies
(Continued)
Ergonomics 1457

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
ElBardissiet
al.
(2007)
Determinethetrans-
ferabilityofahuman
factors
model
devel-
oped
intheaviation
industry
topatient
safety
Surgical
errors
MayoClinic
inthe
USA.Structuredinter-
viewswith68individ-
uals
Nil
1Organisational
influences
1climate
1process
1resourcemanagem
ent
1Unsafe
supervision
1inadequatesupervision
1problem
correction
1inappropriateoperations
1Preconditionsto
unsafe
acts
1environmentalfactors:technological,physical
1adverse
mentalstates
1adverse
physiological
states
1physical/mentallimitations
1teamwork
1personal
readiness
1Unsafe
acts
1decisionerrors
1skill-based
errors
1perceptual
errors
1routineviolations
1exceptional
violations
Friedman
etal.
(2007)
Understandandclas-
sify
causalfactors
linked
tomedication
errors
Medicationerrors
YaleNew
Haven
Organ
Transplantation
Center,April2004–
March
2005.Identified
149errors
in93
patientswhowerepre-
scribed
ameanof10.9
medicationseach
Inter-rateragreem
ent
forerrortypes
assessed
bycalculatingkcoef-
ficients.Pairw
isecom-
parisonsofthethree
raters
had
coefficients
of0.87,0.93and0.88.
Therewas
anoverallk
of0.89(95%
CI:0.84–
0.94)
1Finance
1Pharmacy
1Other
physician
1Outpatienttransplantteam
1Inpatienttransplantteam
1Nursinghome
1Patient
(Continued)
R.J. Mitchell et al.1458
Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
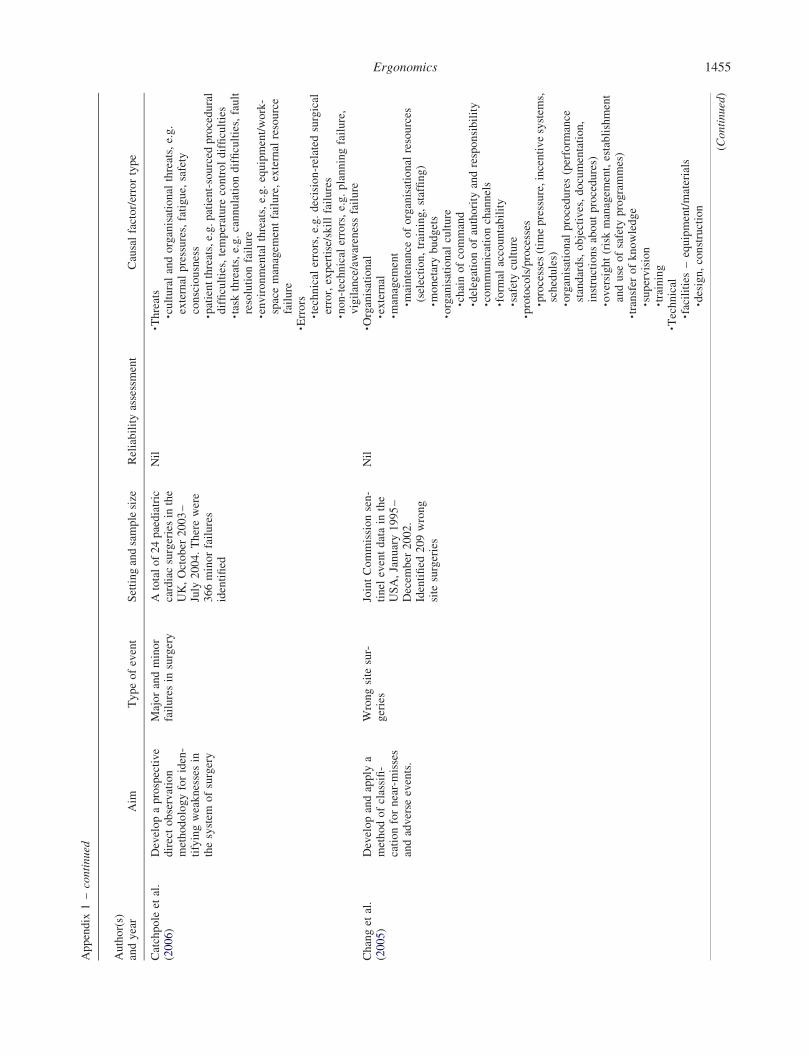
Graber,Frank-
lin,andGordon
(2005)
Clarify
theaetiologyof
diagnostic
errors
ininternal
medicineand
todevelopaworking
taxonomy
Diagnostic
errors
Fivelargeacadem
ictertiary
care
medical
centres
intheUSA.
Identified
100diag-
nostic
errors
over
five
years
Inform
alconsensus
1System
-related
contributionsto
diagnostic
error
1technical
1technical
failure
andequipmentproblems
1organisational
1clustering
1policy
andprocedures
1inefficientprocesses
1teamwork
orcommunications
1patientneglect
1managem
ent
1coordinationofcare
1supervision
1expertise
unavailable
1trainingandorientation
1personnel
1external
interference
1Cognitivecontributionsto
diagnostic
error
1faultyknowledge
1knowledgebaseinadequateordefective
1skillsinadequateordefective
1faultydatagathering
1ineffective,
incomplete
orfaultyworkup
1ineffective,
incomplete,orfaultyhistory
andphysicalexam
ination
1faultytestorprocedure
techniques
1failure
toscreen
(pre-hypothesis)
1pooretiquette
leadingto
poordataquality
1Faultysynthesis:faultyinform
ationproces-
sing
1faultycontextgeneration
1overestimatingorunderestimatinguseful-
nessorsalience
ofafinding
1faultydetectionorperception
1failedheuristics
1failure
toactsooner
1faultytriggering
1misidentificationofasymptom
orsign
1distractionbyother
goalsorissues
1faultyinterpretationofatestresult
1reportingorremem
beringfindingsnot
gathered
1Faultysynthesis:faultyverification (Continued)
Ergonomics 1459

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1premature
closure
1failure
toorder
orfollow
uponappropriate
test
Hennem
anet
al.
(2010)
Describethetypes
of
errors
committedor
recovered
inasimu-
latedenvironmentby
studentnurses
Sim
ulatederror
Atotalof50senior
nursingstudentspar-
ticipated
inoneoftwo
simulationexercises
lastingbetween15and
30minutesin
theUSA
Inter-raterreliabilityof
95%
betweentwo
researcherswhoinde-
pendentlyreviewed
fivevideotapes
(not
included
infinal
anal-
ysis)
1Coordination
1errorrelatedto
communicationwithMD
1errorrelatedto
communicationwithpatient/
family
1Verification
1errorrelatedto
identificationofpatient
1errorrelatedto
patientallergyinform
ation
1Monitoring
1errorrelatedto
failure
tomonitororcorrectly
monitorcritical
patientassessmentinfor-
mation
1errorrelatedto
failure
torecogniseabnorm
alfindings
1Intervention
1errorsrelatedto
failure
toinstituteappropriate
intervention/treatment(omission)
1errors
relatedto
incorrectordelayed
intervention/treatment(commission)
Hicks,Becker,
andJackson
(2008)
Describetheerror
term
susedin
MED-
MARX
Medicationerrors
Medical
intensivecare
unitin
theUSA.One
case
study
Forrey,Pedersen,and
Schneider
(2007)
obtained
inter-rater
reliabilityofk¼
0.61
incategorisingmedical
errors
usingMED-
MARX
in27medical
errorscenarios
1Situational
1Environmental
1Organisational
Hickset
al.
(2004)
Describemedication
errorrecordsfrom
MEDMARX
inpost-
anesthesia
care
units
(PACU)
Medicationerrors
Atotalof189facilities
intheUSA
that
sub-
mittedamedication
errorrecord
specificto
PACUs,August1998–
March
2002.There
were645medication
errors
specificto
aPACU
Forrey,Pedersen,and
Schneider
(2007)
obtained
inter-rater
reliabilityofk¼
0.61
incategorisingmedical
errors
usingMED-
MARX
in27medical
errorscenarios
1Distractions
1Workload
increase
1Staff,inexperienced
1Noaccess
topatientinform
ation
1Shiftchange
1Cross
coverage
1Emergency
situation
1Staffing,insufficient
1Stafffloating
1No24-hourpharmacy
1Staff,agency/tem
porary
1Poorlighting
(Continued)
R.J. Mitchell et al.1460

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
Hicks,Cousins,
andWilliam
s(2004)
Describemedication
errors
from
MED-
MARX
Medicationerrors
Atotalof482MED-
MARX
participating
healthcentres
inthe
USA,2002.There
were192,477medi-
cationerrors
inthe
database
Forrey,Pedersen,and
Schneider
(2007)
obtained
inter-rater
reliabilityofk¼
0.61
incategorisingmedical
errors
usingMED-
MARX
in27medical
errorscenarios
1Distractions
1Workload
increase
1Staffinexperienced
1Staffinginsufficient
1Shiftchange
1Stafffrom
agency
ortemporary
1Emergency
situation
Itoh,O
mata,and
Andersen(2007,
2009)
Describeahuman
error
taxonomysystem
and
itsapplicationto
eval-
uatingsafety
perform
-ance
andreporting
culture
Patentsafety
event
Tworegional
hospitals
inJapan,hospital
AApril2002–September
2004andhospital
BApril2000–September
2002.Therewere3749
incidentreports
Inter-raterreliability
Kappaonsixdim
en-
sionsfor138randomly
selected
incidents:out-
comeseverity
k¼
0.87;eventcap-
ture
cuek¼
0.47;time
ofreportingk¼
0.27;
reported
content
k¼
0.34;timebandof
descriptionk¼
0.36;
anddescriptionlevel
k¼
0.42
1Communicationfactors
1communicationproblem
betweendifferent
professional
groups(e.g.doctorandnurse)
1betweenmem
bersin
thesameprofessional
group(e.g.betweennurses)
1betweenstaffandpatient
1betweenstaffandpatientfamilyorrelatives
1inter-departm
entcollaborationorcommuni-
cationproblem
1Staffhuman
factors
1knowledgeandskills(includingwork
experi-
ence)
1health
1fatigue
1mem
ory
failure
1inattention
1confusion
1wrongassumptionorpreconception
1tim
epressure
1personal
fear
1emotional
stress
1decreased
motivation
1other
psychological
orem
otional
factors
1Patienthuman
factors
1age(e.g.elderly
orbaby)
1dem
entia
1cognitivefailure
1motordisability
1perceptual
impairm
ent
1reducedconsciousness
1anaesthetised
orsleep
1mentalinstability
1other
specificfactors
1Taskfactors
(Continued)
Ergonomics 1461

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1overload
(hightask
dem
and)
1complicatedtask
1novel
task
1multiple
goals
1work
interruption
1busy
situation
1exceptional
work
condition
1midnight
1holiday
1other
task-related
factors
1Equipment/materialfactors
1equipment/materialsfailure
1obsolescentequipment/materials
1accessproblems
1bad
interfacedesign
1bad
materialsdesign
1inconsistentdesignofequipment/materials
1Organisational
factors
1bad/inappropriatemedical
document
1rulesorprocedures
1training
1manualsandchecklists
1taskallocationorstaffing
1lackofresources
1scheduling
1decision-m
akingprocedure
1leadership
1safetyculture-related
problem
1other
organisational
issues
1Environmentalfactors
1layoutin
sickroom/workplace
1lightingin
sickroom/workplace
1available
spacein
sickroom/workplace
1patientswithsameorsimilar
nam
es1m
edicines
withsimilar
nam
es/bottles/colour
1other
environmentalfactors
(Continued)
R.J. Mitchell et al.1462

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
Kantelhardt
etal.(2011)
Applicationofneuro-
surgical
critical
inci-
dentmonitoring
Neurosurgical
criti-
calincidents
Allstafffrom
aneuro-
surgical
departm
entin
Germanyadvised
toreportcritical
inci-
dents.Therewere216
incidentsduringone
year
Nil
1Communication
1Missingknowledge
1Organisation
1Overwork
1Technical
problems
1Material
1Carelessness
1Distraction
1Poorassessmentofthesituation
1Sound-alike
1Misinterpretationofclinical
data
1Oralprescription
1Social
factors
1Abbreviations
1Bad
handwriting
1Others
1Unknown
Kim
andKim
(2009)
Delineate
andevaluate
thefeasibilityofaweb-
based
errorreporting
system
usingtheInter-
national
Classification
ofPatientSafety
(ICPS)in
aKorean
university
hospital
Fourcommoninci-
denttypes:medi-
cationerror;aseptic
techniqueerror;
falls;others(e.g.
pressure
ulcer,use
ofrestraint,delayed
treatm
ent,burns)
Therewere75.4
errors
per
10,000patientdays
duringan
eight-week
periodfrom
Decem
ber
2008to
February2009
inaKorean
university
hospital
Nil
1Staff
1slip/lapse
error/absent-mindedness/forgetful-
ness
1violationofrule
1communicationproblem
withstafforpatient
1emotional
problem
1others
1Patient
1lackofperceptionorunderstandingof
treatm
ent
1communicationproblem
withstaff
1pathophysiological
problem
1slip/lapse
error/absentmindedness/forgetful-
ness
1emotional
problem
1violationofrule
1others
1Organisation/work
environmentfactors
1overworked
1defectofphysicalenvironmental/infrastruc-
ture
1others
(Continued)
Ergonomics 1463
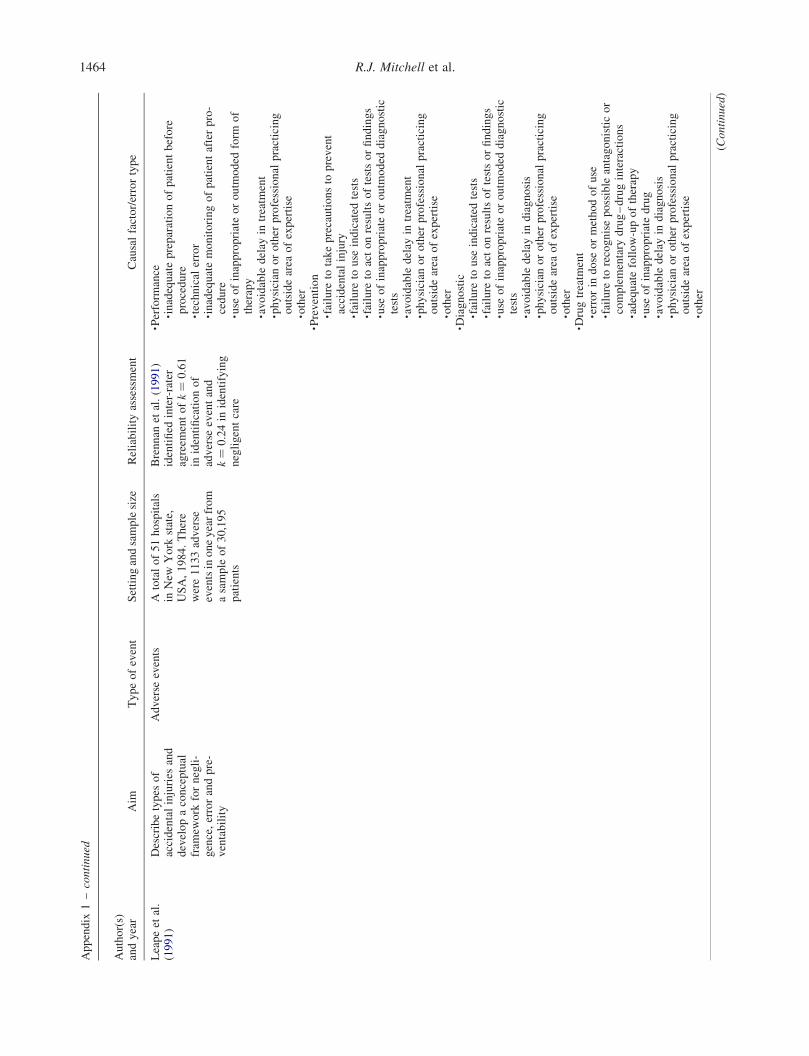
Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
Leapeet
al.
(1991)
Describetypes
of
accidentalinjuries
and
developaconceptual
fram
ework
fornegli-
gence,errorandpre-
ventability
Adverse
events
Atotalof51hospitals
inNew
York
state,
USA,1984.There
were1133adverse
eventsinoneyearfrom
asample
of30,195
patients
Brennan
etal.(1991)
identified
inter-rater
agreem
entofk¼
0.61
inidentificationof
adverse
eventand
k¼
0.24in
identifying
negligentcare
1Perform
ance
1inadequatepreparationofpatientbefore
procedure
1technical
error
1inadequatemonitoringofpatientafterpro-
cedure
1use
ofinappropriateoroutm
oded
form
of
therapy
1avoidable
delay
intreatm
ent
1physician
orother
professional
practicing
outsidearea
ofexpertise
1other
1Prevention
1failure
totakeprecautionsto
prevent
accidentalinjury
1failure
touse
indicated
tests
1failure
toactonresultsoftestsorfindings
1use
ofinappropriateoroutm
oded
diagnostic
tests
1avoidable
delay
intreatm
ent
1physician
orother
professional
practicing
outsidearea
ofexpertise
1other
1Diagnostic
1failure
touse
indicated
tests
1failure
toactonresultsoftestsorfindings
1use
ofinappropriateoroutm
oded
diagnostic
tests
1avoidable
delay
indiagnosis
1physician
orother
professional
practicing
outsidearea
ofexpertise
1other
1Drugtreatm
ent
1errorin
dose
ormethodofuse
1failure
torecognisepossible
antagonisticor
complementary
drug–druginteractions
1adequatefollow-upoftherapy
1use
ofinappropriatedrug
1avoidable
delay
indiagnosis
1physician
orother
professional
practicing
outsidearea
ofexpertise
1other
(Continued)
R.J. Mitchell et al.1464
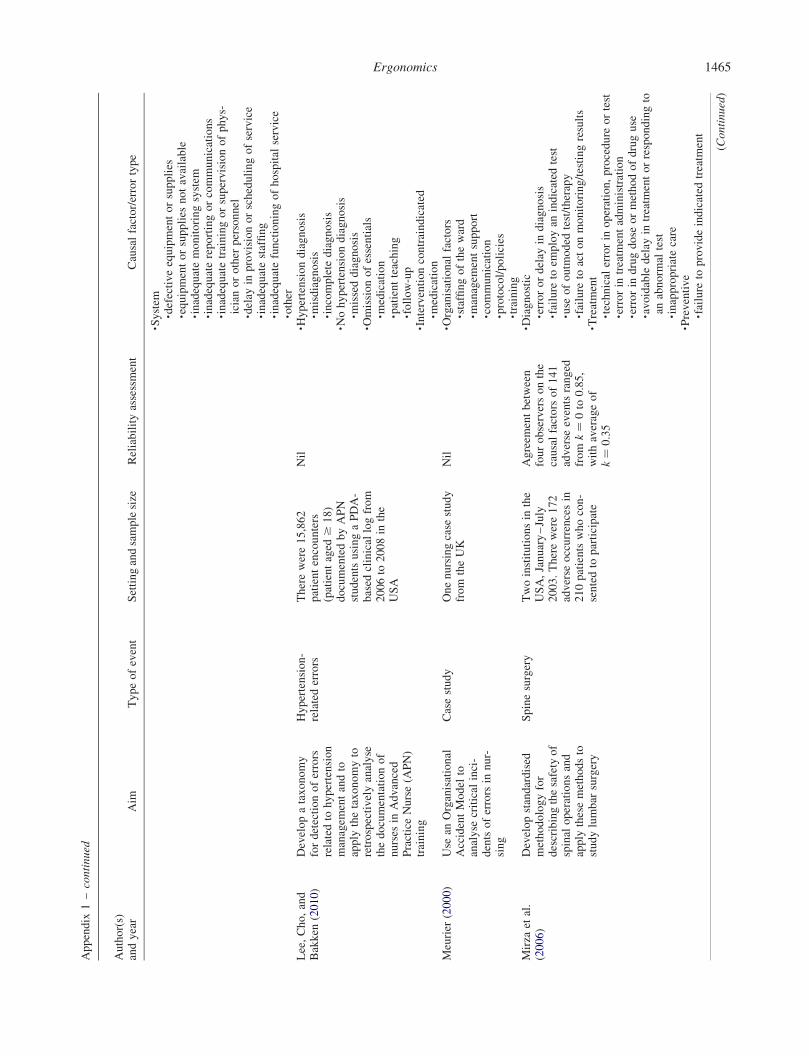
Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1System
1defectiveequipmentorsupplies
1equipmentorsupplies
notavailable
1inadequatemonitoringsystem
1inadequatereportingorcommunications
1inadequatetrainingorsupervisionofphys-
icianorother
personnel
1delay
inprovisionorschedulingofservice
1inadequatestaffing
1inadequatefunctioningofhospital
service
1other
Lee,Cho,and
Bakken
(2010)
Developataxonomy
fordetectionoferrors
relatedto
hypertension
managem
entandto
apply
thetaxonomyto
retrospectivelyanalyse
thedocumentationof
nurses
inAdvanced
PracticeNurse(A
PN)
training
Hypertension-
relatederrors
Therewere15,862
patientencounters
(patientaged
$18)
documentedbyAPN
studentsusingaPDA-
based
clinical
logfrom
2006to
2008in
the
USA
Nil
1Hypertensiondiagnosis
1misdiagnosis
1incomplete
diagnosis
1Nohypertensiondiagnosis
1misseddiagnosis
1Omissionofessentials
1medication
1patientteaching
1follow-up
1Interventioncontraindicated
1medication
Meurier
(2000)
Use
anOrganisational
AccidentModel
toanalyse
critical
inci-
dentsoferrors
innur-
sing
Casestudy
Onenursingcase
study
from
theUK
Nil
1Organisational
factors
1staffingoftheward
1managem
entsupport
1communication
1protocol/policies
1training
Mirza
etal.
(2006)
Developstandardised
methodologyfor
describingthesafety
of
spinal
operationsand
apply
thesemethodsto
studylumbar
surgery
Spinesurgery
Twoinstitutionsin
the
USA,January–July
2003.Therewere172
adverse
occurrencesin
210patientswhocon-
sentedto
participate
Agreem
entbetween
fourobserversonthe
causalfactors
of141
adverse
eventsranged
from
k¼
0to
0.85,
withaverageof
k¼
0.35
1Diagnostic
1errorordelay
indiagnosis
1failure
toem
ployan
indicated
test
1use
ofoutm
oded
test/therapy
1failure
toactonmonitoring/testingresults
1Treatment
1technical
errorin
operation,procedure
ortest
1errorin
treatm
entadministration
1errorin
drugdose
ormethodofdruguse
1avoidable
delay
intreatm
entorrespondingto
anabnorm
altest
1inappropriatecare
1Preventive
1failure
toprovideindicated
treatm
ent
(Continued)
Ergonomics 1465

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1inadequatemonitoringorfollow-upof
treatm
ent
1System
1communicationfailure
1equipmentfailure
1other
system
sfailure
1Other
1Noerror
1patientdisease,expectedrisk
1patientnon-compliance
1patientdisease,unrelatedto
surgery
Nastet
al.
(2005)
Evaluateanew
mech-
anismforreportingand
classifyingpatient
safety
eventsto
increase
reportingand
identify
patientsafety
priorities
Medical
errors,
nearmissesand
riskysituations
CardiothoracicInten-
siveCareandPost
Anesthesia
CareUnits
attheBarnes-Jew
ish
Hospital
intheUSA,
January?D
ecem
ber
2003.Therewere163
reportsdescribing157
events
Nil
1Human
factors
1slip
1coordination
1intervention
1verification
1monitoring
1knowledge
1qualifications
1tripping
1Organisational
factors
1protocols/procedures
1transfer
ofknowledge
1culture
1managem
entpriorities
1external
1Technical
factors
1design
1materials
1external
1construction
1Other
1patient-relatedfactors
1unclassifiable
Nyssen
and
Blavier(2006)
Synthesisetheexisting
scientificknowledge
onerrordetectionand
tofurther
knowledge
throughtheanalysisof
casescollectedin
acomplexsystem
,anesthesia
Anesthesia
errors
Anesthesia
depart-
mentsattwouniversity
hospitalsin
Belgium.
Therewere212reports
duringoneyearand
177errors
Nil
1Equipment
1Individual
1Team
1Organisation
(Continued)
R.J. Mitchell et al.1466

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
Parker
etal.
(2010)
Developatoolto
clarifyandcategorise
precursoreventsto
designinterventions
that
reduce
thenumber
ofprecursorevents
Surgical
flow
dis-
ruptionsandthe
conditionsthat
pre-
dispose
asurgical
team
toadverse
events
Atotalof10cardio-
vascularoperations
perform
edbyeight
differentsurgeons,
with328surgical
flow
disruptionsobserved
atStMary’s
Hospital
attheMayoClinic
Inter-raterreliability
was
measuredusing
Kappa.Kappascores
werecalculatedfor
each
category,then
averaged
foreach
cat-
egory
across
the10
observations.Aver-
aged
kappascoresran-
ged
from
0.71to
0.89
1Technical
factor
1technical/skillissue
1Environmentalfactors
1case-irrelevantconversations
1pagers/phones
1noises/alarm
s/music
1Technologyandinstruments
1instruments/devices
notat
table
1equipmentmalfunction/notready
1Trainingandprocedures
1unexpectedpatientissues
1training/difficultyperform
ingprocedure
1Teamwork
1miscommunication/coordination
1Other
1notspecified
(e.g.visitors/shiftturnover)
Phillipset
al.
(2001)
Describemedication
errors
from
FDA’s
Adverse
EventReport-
ingSystem
Medicationerrors
resultingin
death
FDA’s
Adverse
Event
ReportingSystem
intheUSA,1993–1998.
Therewere5366
medicationerror
reportswith217deaths
resultingfrom
error
and219deathsposs-
ibly
relatedto
error
Nil
1Human
factors
1perform
ance
deficit
1knowledgedeficit
1miscalculationofdosage
1drugpreparation
1other
1Communication
1misinterpretationoforder
1oralmiscommunication
1written
miscommunication
1Nam
econfusion
1proprietarynam
econfusion
1established
nam
econfusion
1Labelling
1immediatecontainer
labelofthemanufacturer
1label
ofdispensedproduct
(practitioner)
1manufacturer’scarton
1printedreference
material
1Packageanddesign
1deviceproblems
1inappropriatepackagingordesign
1tabletorcapsule
confusion
(Continued)
Ergonomics 1467
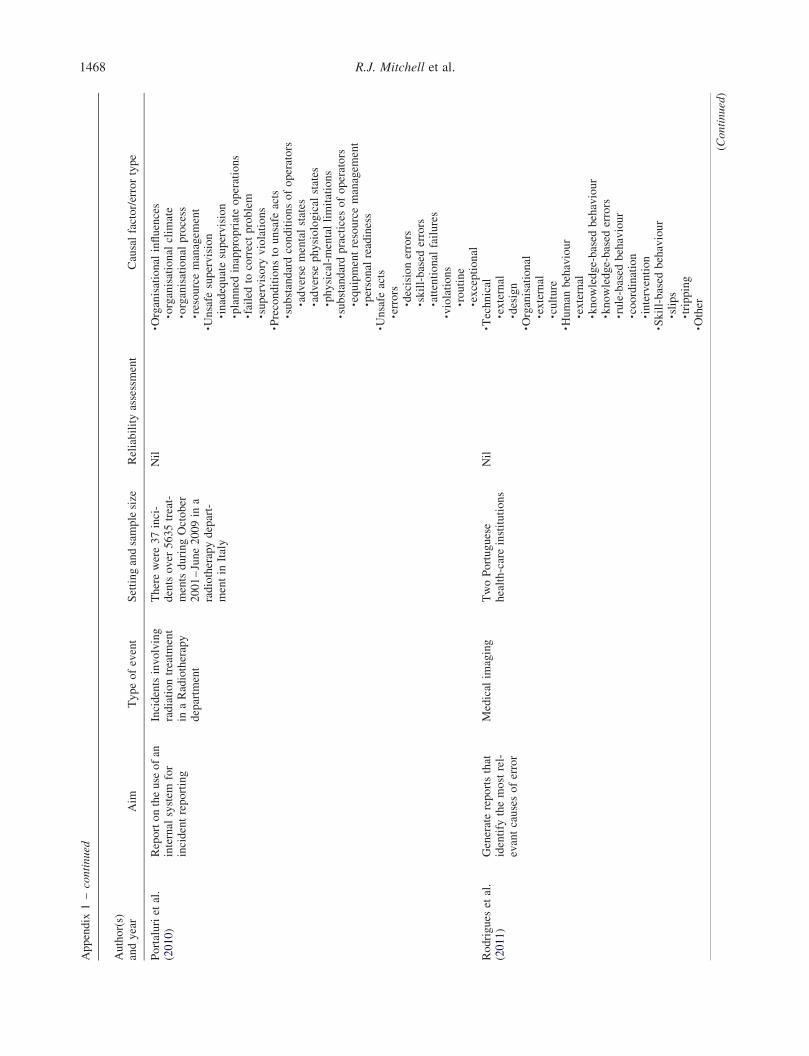
Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
Portaluriet
al.
(2010)
Reportontheuse
ofan
internal
system
for
incidentreporting
Incidentsinvolving
radiationtreatm
ent
inaRadiotherapy
departm
ent
Therewere37inci-
dentsover
5635treat-
mentsduringOctober
2001–June2009in
aradiotherapydepart-
mentin
Italy
Nil
1Organisational
influences
1organisational
clim
ate
1organisational
process
1resourcemanagem
ent
1Unsafe
supervision
1inadequatesupervision
1planned
inappropriateoperations
1failedto
correctproblem
1supervisory
violations
1Preconditionsto
unsafe
acts
1substandardconditionsofoperators
1adverse
mentalstates
1adverse
physiological
states
1physical-mentallimitations
1substandardpractices
ofoperators
1equipmentresourcemanagem
ent
1personal
readiness
1Unsafe
acts
1errors
1decisionerrors
1skill-based
errors
1attentional
failures
1violations
1routine
1exceptional
Rodrigues
etal.
(2011)
Generatereportsthat
identify
themostrel-
evantcausesoferror
Medical
imaging
TwoPortuguese
health-careinstitutions
Nil
1Technical
1external
1design
1Organisational
1external
1culture
1Human
behaviour
1external
1knowledge-based
behaviour
1knowledge-based
errors
1rule-based
behaviour
1coordination
1intervention
1Skill-based
behaviour
1slips
1tripping
1Other
(Continued)
R.J. Mitchell et al.1468

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1patient-relatedfactor
1unclassifiable
Santellet
al.
(2009)
Describecomputer-
relatedmedication
errors
madebynon-
prescribers
Computer-related
medicationerrors
Datavoluntarily
sub-
mittedto
MEDMARX
andUniversity
of
PittsburghMedical
Centerhealthsystem
intheUSA,July
2001–
Decem
ber
2005.
Duringthistime
period,693unique
facilities
submitted
90,001medication
errors
Forrey,Pedersen,and
Schneider
(2007)
obtained
inter-rater
reliabilityofk¼
0.61
incategorisingmedical
errors
usingMED-
MARX
in27medical
errorscenarios"]
1Perform
ance
deficit
1Transcriptioninaccurate
oromitted
1Procedure
orprotocolnotfollowed
1Documentation
1Communication
1Knowledgedeficit
1Written
order
1Workflow
disruption
1Computersoftware
1System
safeguard(s)
1Fax
orscanner
involved
1Monitoringinadequateorlacking
1Pre-printedmedicationorder
form
1Handwritingillegible
orunclear
1Dispensingdeviceinvolved
1Drugdistributionsystem
1Abbreviations
1Calculationerror
1Incorrectmedicationactivation
1Inform
ationmanagem
entsystem
1Dosageform
confusion
1Verbal
order
1Patientidentificationfailure
1Brandorgeneric
nam
eslook-alike
1Generic
nam
eslook-alike
TaxisandBar-
ber
(2003)
Toinvestigatecauses
oferrors
inIV
drug
preparationand
administrationusinga
fram
ework
ofhuman
errortheory
IVdrugpreparation
errors
Observationswere
conducted
during6–
10consecutivedays
(n¼
76days)
on10
wardsin
twohospitals
(oneuniversity
teach-
inghospital
andone
non-teachinghospital)
intheUK,June–
Decem
ber
1999.There
were483IV
drug
preparationsand447
drugadministrations
observed
and265
errors
identified
Nil
1Handlingtechnology
1lackofknowledge,routineandexperience
in1drugpreparation
1drugadministration
1inadequateuse
oftechnology,e.g.drugcharts
1Designoftechnology
1ambiguousmanufacturerleaflets
1unsuitable
workingenvironment
1designofdrugvialpresentations/equipment
1unsuitable
preparationsprocedures
1Communicationproblemsbetween
1nurses
(Continued)
Ergonomics 1469

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1nurses
andpharmacists
1doctors
andother
healthprofessionals,e.g.
ambiguousprescriptions
1Workload
1several
tasksat
thesametime
1endofshift
1lackofqualified
staff
1Patient-relatedfactors
1lim
ited
venousaccess
1non-cooperativepatient
1Supervision
1lackofsupervisionofstudentnurse/agency
nurse
1Other
factors
1tryingto
savedisposable
equipment
Taylor-Adam
s,Vincent,and
Stanhope(1999)
Utilise
asemi-struc-
turedinterview
toana-
lyse
aclinical
adverse
event
Casestudy
Labourwardofhospi-
talin
theUK.Onecase
study
Nil
1Organisational/corporate
culture
1Localwork,task
andenvironmentalconditions
1Individual
TranandJohn-
son(2010)
Developaclassifi-
cationsystem
fornur-
singerrors
relatingto
clinical
managem
ent
(NECM
taxonomy)
andto
describecon-
tributingfactors
and
patientconsequences
Nursingerrors
Therewere241self-
reported
incidents
relatingto
clinical
managem
entinnursing
inametropolitanhos-
pital
inAustralia.
Thesewereidentified
throughtheIncident
Inform
ationManage-
mentSystem
(IIM
S)
databasebetween1
July
2007and30June
2008
Nil
1Nursingcare
processes
1clinical
judgem
ent
1patientassessment
1failedassessment
1misinterpretationofassessment
1clinical
decision
1inappropriatedecision
1failedto
consultrelevantHPs
1confrontunsafe
orders
1failedrecognition
1failedresponse
1clinical
task
execution
1taskperform
ing
1poornursingcare
1failedpatientID
/consent
1failedto
follow
protocol/procedure
1missedordersfrom
other
HPs
1beyondnursingscope
1technologyapplied/required
1incorrecttechnique
1inappropriateequipment
1precautionaryaction
1failedassessingenvironment (C
ontinued)
R.J. Mitchell et al.1470

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
1failedcheckingnotes
1failedseekingclarification
1continuityofcare
1failedescortingpatient
1inadequateprovisionofinform
ation
1tonurses
1toother
HPs
1missedreferral/follow-up
1Communication
1verbal
communication
1nurse–nursecommunication
1nurse–patientcommunication
1nurse–other
HPscommunication
1written
communication
1incomplete
chart
1omissionin
documentation
1incomplete
paper
work
1Administrativeprocesses
1inappropriatebed
managem
ent
1staffsupervisionandplanning
1insufficientstaffroster
planning
1inadequatesupervision
1Knowledgeandskill
1lackofknowledge
1lackofskillsandexperience
Tourgem
an-
Bashkin,Shinar,
andZmora
(2008)
Exam
inethenature
andcausesofmedical
errorsknownas
almost
adverse
events(A
AEs)
andpotential
adverse
events(PAEs)
inintensivecare
units
(ICU)
Alm
ostadverse
events(A
AEs)
and
potential
adverse
events(PAEs)
TwoICUsin
Soroka
Medical
Center,Israel.
Therewere114AAEs
observed
inthecourse
of500hofobser-
vation:49in
theneo-
natal
ICU
(NICU)and
65in
thepaediatric
ICU
(PICU)
Inter-rateragreem
ent
forall114AAEsfor
thethreemaincauses
k¼
0.79andforall
causesk¼
0.73.
Agreem
entforthe49
NICU
AAEsforthe
threemaincauseswas
k¼
0.75andforall
causesk¼
0.58.
Agreem
entforthe65
PICU
AAEsforthe
threemaincauseswas
k¼
0.82andforall
causesk¼
0.76
1Work
environmentfactors
1System
factors
1Human
factors
(Continued)
Ergonomics 1471

Appendix
1–continued
Author(s)
andyear
Aim
Typeofevent
Settingandsamplesize
Reliabilityassessment
Causalfactor/errortype
Webbet
al.
(1993)
Describethefirst2000
Australian
Incident
MonitoringStudy
(AIM
S)incident
reports
Unintended
inci-
dentsinvolving
anaesthetists
Atotalof90hospitals
orgrouppractices
inAustraliaandNew
Zealand.First2000
incidentsreported
toAIM
S
Nil
1Communicationproblem
1Druglabel
1Errorofjudgem
ent
1Failure
tocheckequipment
1Fatigue
1Faultoftechnique
1Haste
1Illness
1Inadequateassistance
1Inattention
1Inexperience
1Lackoffacility
1Monitorproblem
1Pre-oppatientassessmentinadequateorincor-
rect
1Pre-oppatientpreparationinadequateorincor-
rect
1Reliefanaesthetistorstaffchange
1Unfamiliarenvironmentorequipment
1Other
factor
1Other
equipmentproblem
1Other
stress
Wiegmannet
al.
(2007)
Studysurgical
errors
andtheirrelationship
tosurgical
flow
dis-
ruptionsin
cardiovas-
cularsurgery
prospectivelyto
understandbetterthe
effect
ofthesedisrup-
tionsonsurgical
errors
andpatientsafety
Surgical
errors
Cases
werechosen
randomly
from
the
non-emergency
oper-
ativeschedule
ofcar-
diovascularsurgeons
whoagreed
toallow
observationsto
take
place
intheiroperating
room;MayoClinic
Rochester,USA.There
were31cardiacsur-
geriesover
athree-
weekperiodand155
technical
operative
errors
wereidentified
(3.7
per
h,5.0
per
operation)
Nil
1Teamwork
1Extraneousinterruptions
1Equipmentandtechnology
1Resource-based
issues
1Supervisory/training-related
issues
R.J. Mitchell et al.1472