A review of a case of a patient presenting with low back pain leading to a low back emergency...
57
“A disconcerting cause of back pain” Doctor Chad PulmCrit.com Pulmonary & Critical Care
description
This is a case guided review of the literature by viewing this powerpoint, the aim is to:Review a case of severe low back pain in a critical care settingAppreciate the importance of the history and physical in assessing low back painReview the emergency causes of low back pain, including the work-up, imaging and management
Transcript of A review of a case of a patient presenting with low back pain leading to a low back emergency...

“A disconcerting cause of back pain”
Doctor ChadPulmCrit.com
Pulmonary & Critical Care

Objectives
• Review a case of severe low back pain in a critical care setting
• Appreciate the importance of the history and physical in assessing low back pain
• Review the emergency causes of low back pain, including the work-up and management

Who is this?

William Osler (1849–1919)
• Canadian physician and “Father of Modern Medicine”
• One of four founding professors of Johns Hopkins Hospital
• Osler created the first internal medicine residency program
• Pioneer of bedside teaching for medical students
Case PresentationChief Complaint: Back painHPI• 63 year old man who presents with severe lower
back pain• First noted pain when walking dog 4 days prior to
admission• Came to ED – given dexamethasone, toradol and
dilaudid• Sent home with mobic, medrol dose pack and
percocet• Went to an outpatient clinic and received a steroid
hip injection
Case Presentation cont’d
• Pain did not improve – in fact it got worse• Was unable to ambulate due to pain• Pain was sharp, in left lower back/flank radiating
to groin• On admission denies any chills, vomiting
• ROS: Positive for subjective fevers, diarrhea, weight loss, nausea and poor PO intake.

Past Medical History
• HTN• Degenerative Joint Disease• Psoriatic arthritis• Anxiety and Depression• Hypercholesterolemia• Benign Prostatic Hyperplasia• Vocal Cord Disease• Sleep Apnea but does not use CPAP

Medications
• ASPIRIN 81 MG EC TABLET • ATORVASTATIN 10 MG ORAL TABLET • CARISOPRODOL (SOMA) • FINASTERIDE 5 MG ORAL TABLET • MELOXICAM 15 MG ORAL TABLET • METOPROLOL 50 MG EXTENDED-RELEASE TABLET • OXYCODONE• TERAZOSIN 10 MG CAPSULE • VALSARTAN 160 MG ORAL TABLET
Social History & Family Hx
Social History• He works as an accountant• Lives with his roommate• The patient denies any tobacco use – never smoker,
no alcohol use. • Denies any recreational and IV drug useFamily History • Mother – Dementia • Father - Emphysema

PE• Vitals: 97.6 °F (36.4 °C), BP: 97/55 mmHg, Heart Rate: 89 Resp Rate: 16, SpO2: 97 %/RA• General: Alert, cooperative, mild distress, appears stated age, hoarse voice. • Head: Normocephalic, without obvious abnormality, atraumatic. • Eyes: Conjunctivae/corneas clear. PERRL, EOMs intact. • Throat: Lips, mucosa, and tongue normal. Teeth and gums normal. • Neck: Supple, symmetrical, trachea midline, no adenopathy, thyroid: no
enlargment/tenderness/nodules, no carotid bruit and no JVD. • Pulmonary: Clear to auscultation bilaterally. • Chest wall: No tenderness or deformity. • Heart: Regular rate and rhythm, S1, S2 normal, no murmur, click, rub or gallop. • Abdomen: Soft, non-tender. Bowel sounds normal. No masses, No organomegaly. • Extremities: Extremities normal, atraumatic, no cyanosis or edema. SLR negative• Pulses: 2+ and symmetric all extremities. • Back: patient defers exam for now, states his pain is too severe to move • Skin: Skin color, texture, turgor normal. No rashes or lesions. • Neurologic: CNII-XII intact. Normal strength, sensation and reflexes throughout.

What is the differential diagnosis for his low back pain?

Anatomy of the Lumbar Spine
EB Medicine 2013

EB Medicine 2013

Labs on admission• Troponin 1.42 • CBC 2.5>14.4/42<82• Na 131 /K 4.4 Cl 96/ HCO3 20 BUN 35/ Cr 0.8 Gluc 164 • Anion Gap 15• Lactate 2.9• Calcium, Serum 7.8• Albumin 2.2• Alkaline Phosphatase 48• ALT 21• AST 40• Bilirubin, Direct 1.7 Indirect 0.4 Total 2.1• Total Protein 4.4

Lumbar X-ray obtained in ED 2 days before admission
Significant joint space narrowing at L4-L5. End plate degenerative change at L4-L5 and L5-S1. Disk space narrowing at L5-S1. Facet athropathy at L4-L5 and L5-S1. No acute fracture.

MRI Lumbar spine (no gadolinium) in ED 2 days before admission

Hospital Course
• Admitted to the medical floors• Started on pain control with oxycodone,
dilaudid and muscle relaxants robaxin• Reviewed MRI lumbar spine• PT evaluation• Home medications continued

Day 2• Became hypotensive, febrile, abdomen became distended,
developed bloody diarrhea, nausea, vomiting and epigastric pain.
• Lactate elevated (3.6), surgery consult was called for evaluation for SBO
• Hypotension was refractory to multiple fluid boluses (7Liters)• NGT output suspicious for coffee ground emesis• He was transferred to the ICU shortly thereafter for continuing
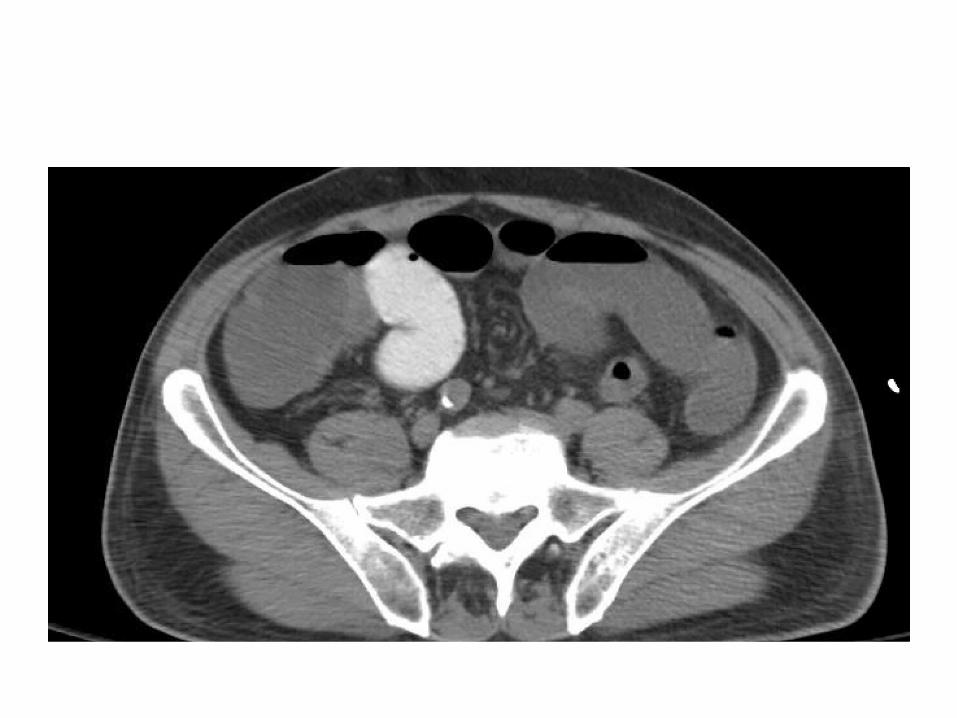
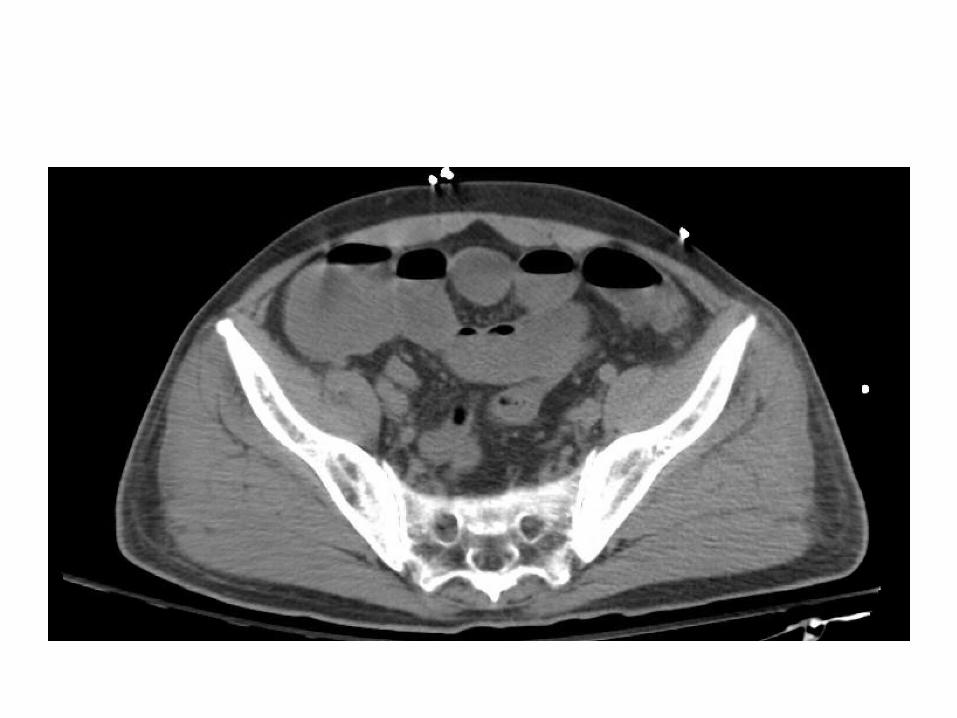
care.• KUB performed this morning demonstrated dilated loops of
bowel concerning for ileus vs SBO, no free air.

Labs on ICU transfer• Troponin I 1.42• CBC 1.9>12.4/42<82• Na 132 /K 4.3 Cl 100/ HCO3 16 BUN 65/ Cr 1.8 Glucose 125 • Anion Gap 16• Calcium, Serum 7.0• Lactate 3.7• Albumin 1.9 AP 51 ALT 46 AST 100• Bilirubin, Direct 2.6 Indirect 0.4 Total 3.0• Total Protein 4.1 (L)• ABG 7.33 28 93 14.8 96.5% on 5L nc• Blood cultures x 2 Staph Aureus• UA Positive – Staph Aureus >100,000 CFU in Urine

CXR on Transfer




Day 2 Continued
• Central line placed and Vasopressors started• Surgery consult for concern for SBO – recommend
NGT to suction (decompress)• Broad spectrum antibiotics (vancomycin and zosyn
IV) initiated• GI consulted for UGIB – PPI started• TTE negative for Vegetation• Low back pain continued – Pain management
consulted

Problem List Day 3 ICU• Septic Shock requiring vasopressors• Nodules, consolidations and pleural effusions on CT Chest• SBO vs ileus• Thrombocytopenia• Leukopenia• AKI• NSTEMI• Transaminitis• Excruciating back pain• Afib with RVR

WHAT IS THE DIFFERENTIAL DIAGNOSIS FOR BACK PAIN AT THIS TIME?

WHAT WORK UP WOULD YOU OBTAIN AT THIS POINT?

Day 4
• Cultures remained positive for MSSA• UA suggestive of MSSA• WBC scan performed:
1. Findings consistent with osteomyelitis at T4-T5 and L3-L4 as described above. 2. Findings suspicious for inflammatory/infectious process of the left hip. 3. Infectious process of the right mid and left lower lung. 4. Likely inflammatory/infectious process of the colon.
• Cr. Improved so MRI with Gad obtained
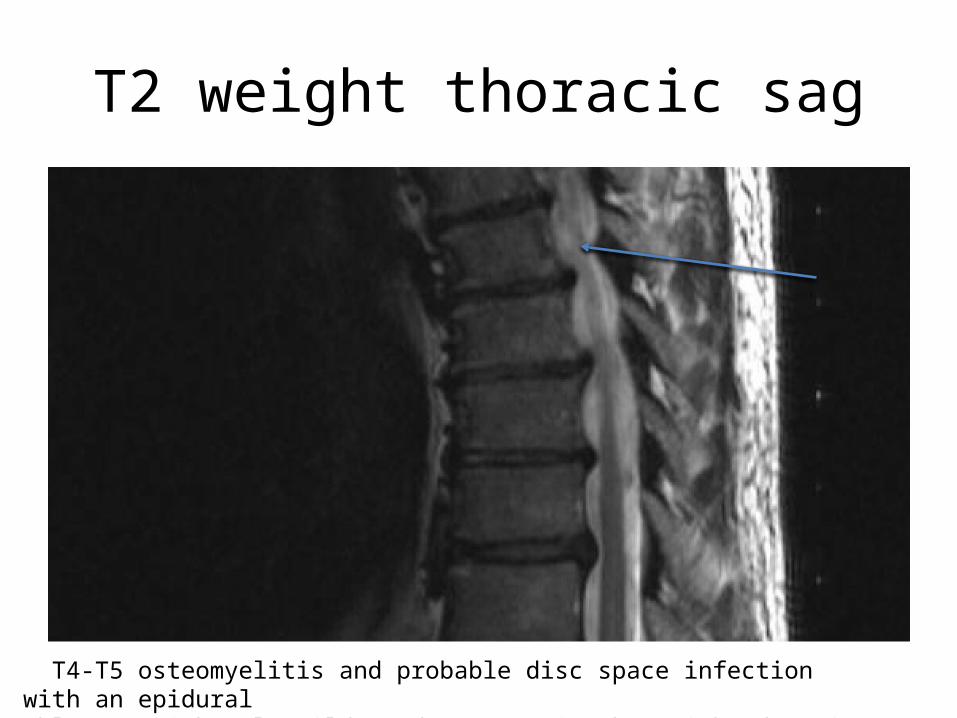
T2 weight thoracic sag
T4-T5 osteomyelitis and probable disc space infection with an epidural phlegmon with only mild cord compression but with edema in the cord.

T2 weight Sag Lumbar
Disc space infection L3-4 with epidural pannus extending from L1 to L5 with moderate central canal stenosis at L3 and L4. Involvement of both psoas muscles.

Hospital Course continued
• Came off pressors and was able to leave the ICU• Left hip arthrocentesis and fluid grew MSSA• EGD demonstrating duodenal ulcers and multiple
gastric ulcers• Blood cultures eventually sterilized after 1 week• Back pain improved after draining psoas abscess• SBO improved and diet advanced• Leukopenia and thrombocytopenia improved• Spine consulted conservative management
Diagnosis
T4-T5 osteomyelitis, L3-L4 diskitis and epidural phlegmon with mild cord compression
MSSA Bacteremia with UTI and pulmonary dissemination
L hip MSSA Septic Arthritis

Acute Low Back Pain
• Low back pain is the most common type of pain reported by adults in the United States
• 26% of the population reporting pain lasting at least a day in the past 3 months
• 1% of the United States workforce considered “permanently disabled” by lumbago.
• In 1998, direct healthcare costs attributed to lower back pain - estimated at $90 billion

Definitions: Acute Low Back Pain• Acute low back pain: Symptoms lasting < 4 weeks (up for 3
months)• Chronic Back pain: Pain syndrome lasting longer than 3
months.• Sciatica: Leg pain that localizes to lumbar sacral nerve
roots(90% of pathology occurs at L4-L5 and L5-S1 levels.)• Spondylosis: Degenerative arthritis of the spine• Disc protrusion, extrusion, and sequestration – Protrusion, the disc is intact but out of place.– Extrusion, the gelatinous nucleus pulposus is squeezed out
from a tear in the annulus fibrosus.– Sequestration, some parts of the disc nucleus pulposus are
completely separated from the main disc (sequestered fragment)

Definitions: Acute Low Back Pain• Spinal stenosis: Crowding of the spinal canal, either by
osteoarthritis, osteophytes, ligamentous thickening, and/or bulging intervertebral discs
• Myelitis: An inflammatory condition that affects the spinal cord. (often white matter and demyelination are involved)
• Cauda equina syndrome: Compression of the cauda (nerve roots)
• Spondylolisthesis: Vertebra slips out of position in relation to the vertebra beneath it.

Evaluation of the low back pain patient
Clinicians should conduct a focused history and physical examination to help place patients with low back pain into 1 of 3 broad categories: 1. Red Flag low back pain (potentially serious)2. Back pain potentially associated with
radiculopathy or spinal stenosis3. Nonspecific back pain (most common)(strong recommendation, moderate-quality evidence).
Ann Intern Med. 2007;147(7):478-491

Physical Exam in Acute Lumbago
• It is fundamental to perform a systematic neurologic examination.
• Include pertinent negatives and positives regarding strength, sensory, reflexes, gait, rectal sensation examination and assessment for urinary retention
• The PE findings (or lack of findings) should be the foundation of the decision to pursue imaging
• More than 90% of disc herniations occur at the L4/L5 or L5/S1 levels so a focus on this level


When to Obtain imaging• Most low back pain self resolves in 4 to 6 weeks so imaging is not
recommended* in patients without red flags • A meta-analysis of 6 randomized trials of 1800 patients found no
outcome differences between routine care and no imaging and patients who underwent imaging with plain x-ray, CT, or MRI
• Additionally, MRI reveals many abnormalities in asymptomatic patients.
• In a study of asymptomatic patients aged ≥ 60, 36% had a herniated disc, 21% had spinal stenosis, and 90% had a degenerated or bulging disc.

Plain Radiographs• Routine plain films are not indicated - very low for an
intervenable lesion or pathology
• In a study of 68,000 radiographs, clinically unsuspected lesions occurred in 1:2500 patients aged 20 to 50 years.
• X-ray is recommended in patients who have: – Direct trauma-related back pain – Suspected of having a possible vertebral compression fracture– Young patients with lower back pain where ankylosing spondylitis
is suspected

After Conservative Management
• In patients with low back pain and radiculopathic symptoms who are still symptomatic after 4 weeks of conservative management and self-care
• Imaging should be discussed that can be intervened upon i.e. injection therapy and surgery.
• Usually MRI is preferred

WITH THE HIGH PREVALENCE OF LUMBAGO, WHEN DOES IT BECOME AN EMERGENCY?


T2-weighted sagittal MRI of the spine showing osteomyelitis at T12 (top arrow) and partial cord
compression at L1 (bottom arrow).
AAFP

Acute Low Back Pain Emergencies
• Cauda Equina Syndrome• Abdominal Aortic Aneurysm Rupture• Spinal Hematoma• Epidural Abscess
• In CASE of Emergency…

Cauda Equina Syndrome• Cauda equina provide motor and sensory function to the
lower extremities, perineum, and bladder. • Herniated disks are most common lesions causing cauda
equina syndrome • Other causes are tumors, spinal stenosis, infection, and
hematoma• Presentation: low back pain, b/l weakness in lower
extremities, saddle anesthesia, and abnormalities in bladder sensation and function (complete versus incomplete syndromes)
• TIP: Measure post void residual (PVR). PVR > 300 ml is always abnormal.
• Diagnosis: MRI or CT myelogram is needed to make this diagnosis.

Abdominal Aortic Aneurysm Rupture
• Abdominal aortic diameter > 3 cm is aneurysmal (1/1000 patients)• Abdominal aortic aneurysms are uncommon in patients aged < 60
years. • An aneurysm’s size correlates with risk of rupture• 0.5% rupture risk for aneurysms < 4 cm and 3%-15% for aneurysms 5
cm-5.9 cm. • Presentation: contained rupture can cause abdominal pain, back
pain, and groin pain, and it may be associated with nausea, diaphoresis, or syncopal symptoms.
• TIP: May assess aortic size with bedside ultrasound. • Diagnosis: CT scan with IV contrast and vascular surgery consultation
are key

Spinal Hematoma• TIP: Spinal epidural hematomas are rarely
spontaneous. Usually related to trauma, postoperative spinal surgery, anticoagulation, thrombolysis, lumbar puncture, epidural anesthesia,vascular malformation, or chiropractic manipulation.
• Presentation: Back pain and possible neurologic complaints
• Diagnosis: A low threshold for imaging with MRI with Gad or CT myelogram with contrast is needed in suspected patients
• Reverse of coagulopathy, and patients require an emergent consultation for surgical evacuation

Epidural Abscess
• Epidural abscess is a rare condition (0.2-2.8 cases/10,000/y)
• Most common in the 60- to 70-year age group • Risk factors are diabetes mellitus, alcoholism,
AIDS/immunocompromised states, cancer, and IVDU, trauma and spinal surgery
• 20% of patients will have no predisposing factors• Staphylococcus aureus – most common organism
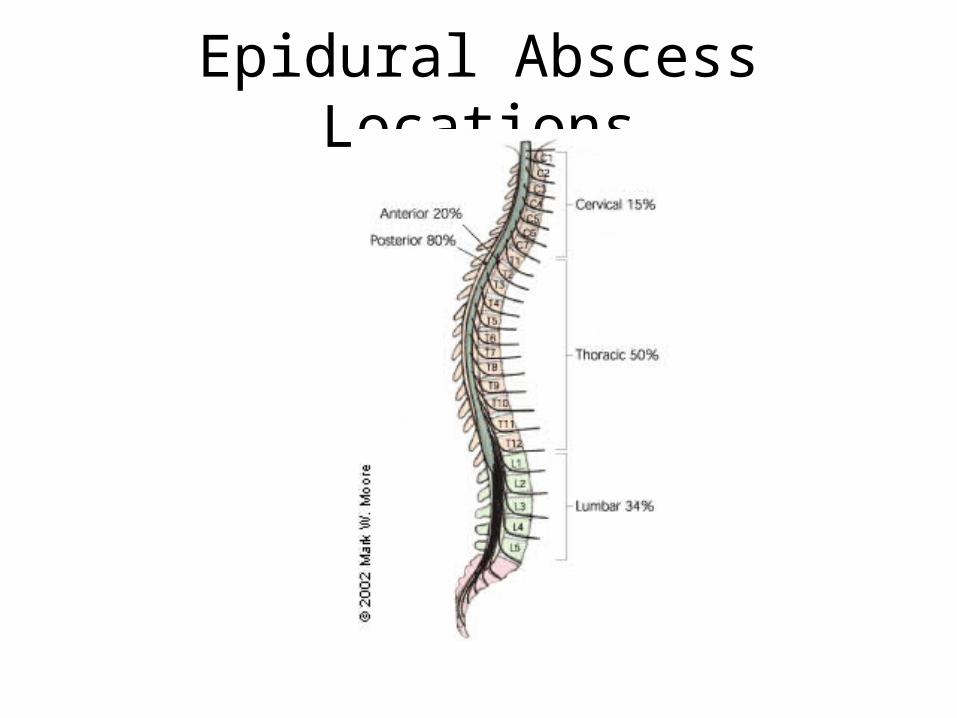
Epidural Abscess Locations

Epidural Abscess• Posterior epidural abscesses tend to be related to a distant
focus• Anterior infections are generally related to osteomyelitis or
diskitis (which can be related to a distant focus or contiguous spread, such as psoas abscess)
• Presentation: Nonspecific - can include fever, back pain, and malaise
• Diagnosis: MRI with gad (preferred) or CT myelogram with contrast
• Treatment: 4-6 weeks antibiotics and consider surgical decompression.

Spinal Epidural Abscess - Experience with 46 Patients
• Chart review 46 patients (36 men and 10 women) with spinal epidural abscess over a 10-year period
• Risk factors: diabetes (46%), frequent venous puncture (35%), spinal trauma (24%), and history of spinal surgery (22%)
• ESR was elevated uniformly (mean, 86.6 mm/h) • Staphylococcus aureus was the most common cause
(39%)• Presentation: Localized spinal pain (89%), paralysis
(80%), fever/chills (67%), and radicular pain (57%)
Journal of Infection (2002) 45: 76±81

William Osler
The key to this case?"Listen to your patient, for he is telling you the diagnosis"

References• Andersson GB. Epidemiological features of chronic low-back
pain. Lancet. 1999;354(9178):581-585. (Review)• Chou R, Qaseem A, Snow V, et al. Diagnosis and treatment of
low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007;147(7):478-491. (Clinical practice guideline)
• NICE. National Institute for Health and Clinical Excellence - low back pain (CG88). 2009. (Clinical practice guideline)
• An Evidence-Based Approach To The Evaluation And Treatment Of Low Back Pain In The Emergency Department. EB Medicine. 2013.
• Spinal epidural abscess – experience with 46 patients and evaluation of prognostic factors, J Infect 2002; 45: 76-81. (http://pmid.us/12217707)

Leave a post with any questions, comments or contributions you have on this topic