A Rare Cause of Chest Pain in a Healthy Teen Rare Cause of Chest Pain in a Healthy Teen Monisha...
13
A Rare Cause of Chest Pain in a Healthy Teen Monisha Shah, MD 1 , Barra Alabd Alrazzak, MD 2 , Ann Marshburn, MD 1 , Benjamin Mouser , MD 1 , Adil Solaiman, MD 1 1 Department of Pediatrics 2 Department of Pediatric Gastroenterology and Nutrition University of Texas Health Science Center at Houston, Houston, TX PRESENTED BY: Monisha Shah, MD, PGY3 McGovern Medical School Disclosure of Financial Relationships • No financial disclosures
Transcript of A Rare Cause of Chest Pain in a Healthy Teen Rare Cause of Chest Pain in a Healthy Teen Monisha...
A Rare Cause of Chest Pain in a Healthy Teen
Monisha Shah, MD1, Barra Alabd Alrazzak, MD2, Ann Marshburn, MD 1, Benjamin Mouser , MD1, Adil Solaiman, MD1
1Department of Pediatrics 2Department of Pediatric Gastroenterology and NutritionUniversity of Texas Health Science Center at Houston, Houston, TX
PRESENTED BY: Monisha Shah, MD, PGY3
McGovern Medical School
Disclosure of Financial Relationships
• No financial disclosures
McGovern Medical School
History of Present Illness• 17 y/o healthy M presented to OSH ER with 2 days of subjective fevers,
difficulty breathing and severe, sharp substernal chest pain
• Gradually worsening
• Constant
• Achy, non-pleuritic
• Radiating to mid chest
• Unchanged with position
• No history of trauma
• No aggravating/relieving factors
• Associated symptoms: diaphoresis, shortness of breath, sore throat, odynophagia, denies nausea/vomiting
McGovern Medical School
Other relevant past history
• Recent strep throat infection
• Other PMH/PSH/FH/SH non-contributory
• Denies smoking, alcohol use or recreational drug use
McGovern Medical School
Additional questions
• No family history of premature sudden cardiac death
• No prior episodes of chest pain
• No history of heart murmur
• No history of episodes of syncope
McGovern Medical School
Physical examination
•ER vital signs:
• T: 98.5°F (Oral)
• HR: 106 bpm
• RR: 18 breaths/min
• BP: 116/77
• SpO2: 97%
• HT: 185 cm (91%)
• WT: 73.5 kg (75%)
Physical Exam GEN: Alert, No acute distress
HEENT: PERRL. TMs clear. Posterior pharynx benign without lesions.
LUNGS: Clear bilaterally. No pleuritic pain.
HEART: Tachycardia. No murmurs. Capillary refill 2-3 seconds
CHEST WALL: No tenderness with palpation
MSK: Normal ROM, no swelling or deformities in any extremities
GI: Soft, NTND. No rebound or guarding. Negative Murphy’s sign.
McGovern Medical School
Initial Differential Diagnosis
What would you be worried about for this patient?
McGovern Medical School
Initial Differential Diagnosis• Life-threatening conditions:
• Cardiac : Classic and Variant angina, Myocarditis, Pericarditis, Arrhythmia, Aortic dissection, HOCM, DCM
• Pulmonary : Pneumothorax, Pulmonary hypertension, Pulmonary embolism
• Gastrointestinal: Esophageal rupture
• Common conditions:
• Musculoskeletal: costochondritis, muscle strain, or trauma
• Ingestion: caustic/corrosive agents, cocaine
• Psychogenic : panic attack, hyperventilation syndrome, or psychosomatic complaints
• Respiratory : asthma, pneumonia, or pleuritis
• Gastrointestinal disease: pill esophagitis, pancreatitis, GERD, or gastritis
McGovern Medical School
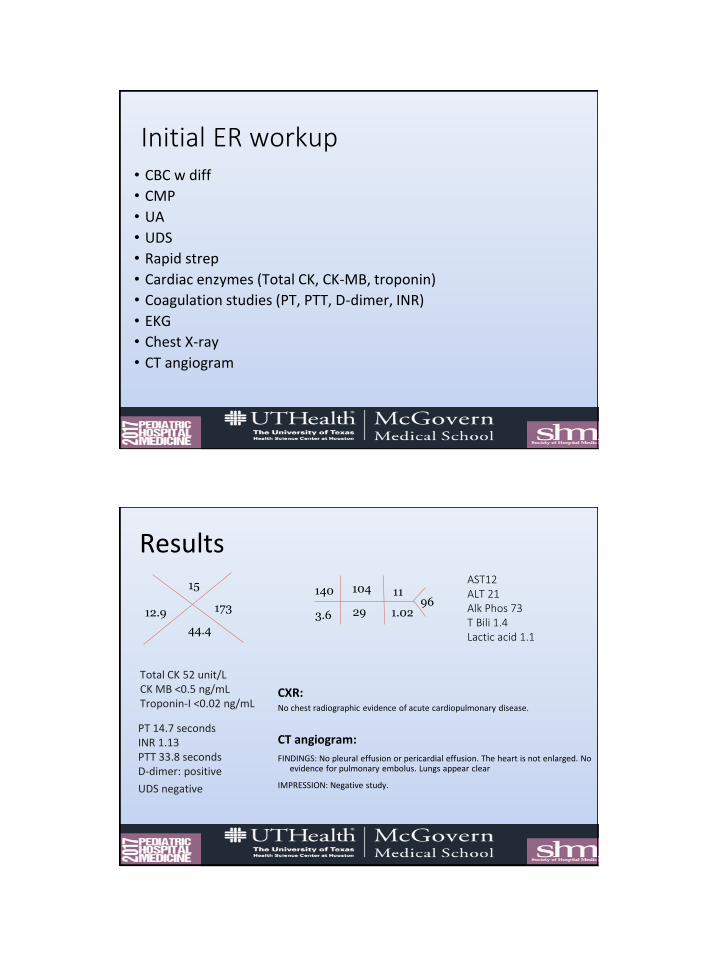
Initial ER workup • CBC w diff
• CMP
• UA
• UDS
• Rapid strep
• Cardiac enzymes (Total CK, CK-MB, troponin)
• Coagulation studies (PT, PTT, D-dimer, INR)
• EKG
• Chest X-ray
• CT angiogram
McGovern Medical School
Results
CXR:No chest radiographic evidence of acute cardiopulmonary disease.
CT angiogram:
FINDINGS: No pleural effusion or pericardial effusion. The heart is not enlarged. No evidence for pulmonary embolus. Lungs appear clear
IMPRESSION: Negative study.
140 104
293.6 1.02
1196
15
12.9
44.4
173
AST12ALT 21Alk Phos 73T Bili 1.4Lactic acid 1.1
Total CK 52 unit/L CK MB <0.5 ng/mL Troponin-I <0.02 ng/mL
PT 14.7 seconds INR 1.13PTT 33.8 seconds D-dimer: positive
UDS negative
McGovern Medical School
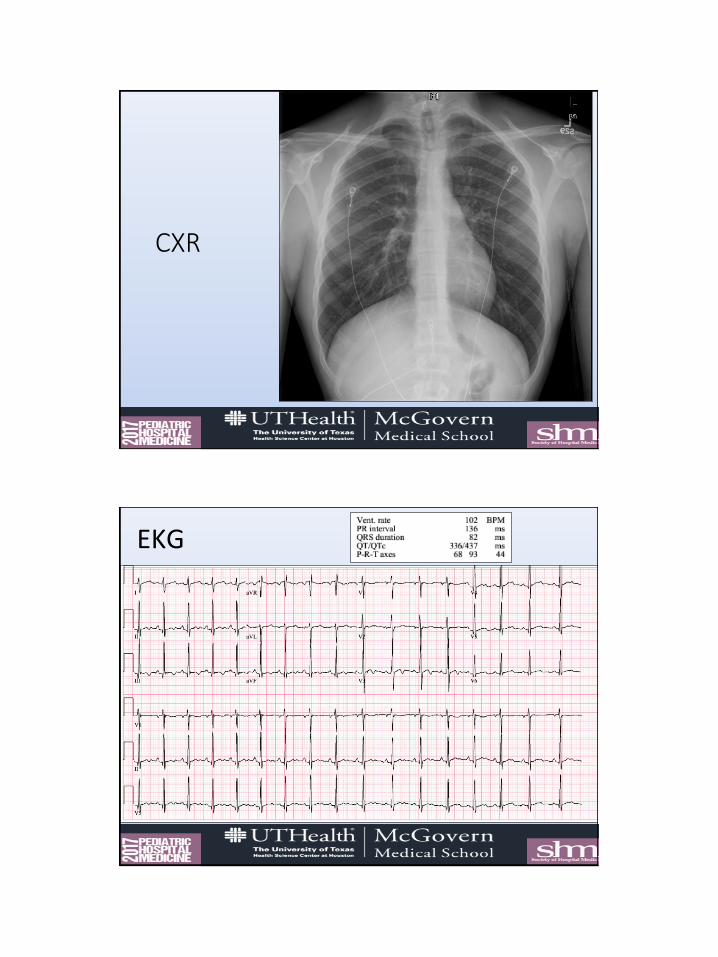
CXR
McGovern Medical School
EKG
McGovern Medical School
• Severe, progressive odynophagia
• Pain located in epigastric region
• Dehydrated due to decreased fluid intake
• Failed PO challenge at ER, transferred to our inpatient facility for higher level of care, pain control, and subspecialty consultation.
Inpatient Admission
McGovern Medical School
Inpatient Physical Exam• Admission vitals:
• T: 99.2 °F (Oral) HR: 79 (Peripheral) RR: 10 BP: 137/70
SpO2: 99%
• Admission exam:GEN: Alert, No acute distress
HEENT: PERRL. TMs clear. Posterior pharynx benign without lesions. Dry mucus membranes.
LUNGS: Clear bilaterally. No pleuritic pain.
HEART: Regular rate and rhythm, no murmurs. Capillary refill ~3 seconds
CHEST WALL: No tenderness with palpation
MSK: Normal ROM, no swelling or deformities in any extremities
GI: Soft, NTND. No rebound or guarding. Negative Murphy’s sign.
McGovern Medical School
Diagnostic Pause• How would order of DDx change with new information?
• Are there new items you would like to add to DDx?
McGovern Medical School
Hospital Course
• Failed PO challenge with exacerbation of pain on
oral intake
• Started on IV fluids, IV pantoprazole with sucralfate
and morphine for pain management
• Pediatric GI consulted
McGovern Medical School
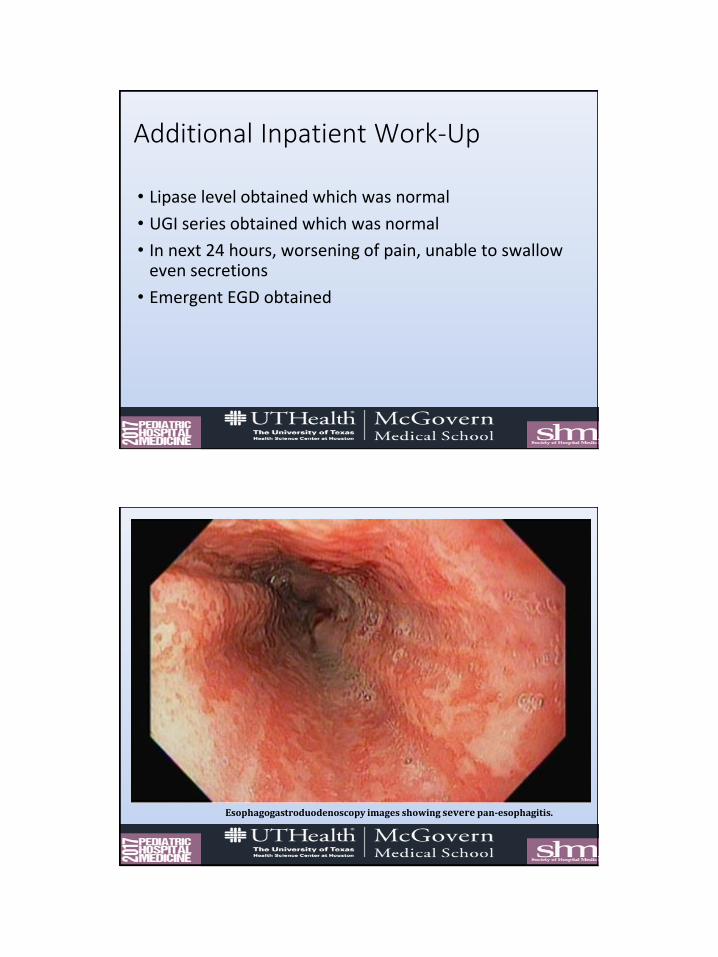
• Lipase level obtained which was normal
• UGI series obtained which was normal
• In next 24 hours, worsening of pain, unable to swallow even secretions
• Emergent EGD obtained
Additional Inpatient Work-Up
McGovern Medical School
Middle esophagus
Esophagogastroduodenoscopy images showing severe pan-esophagitis.
McGovern Medical School
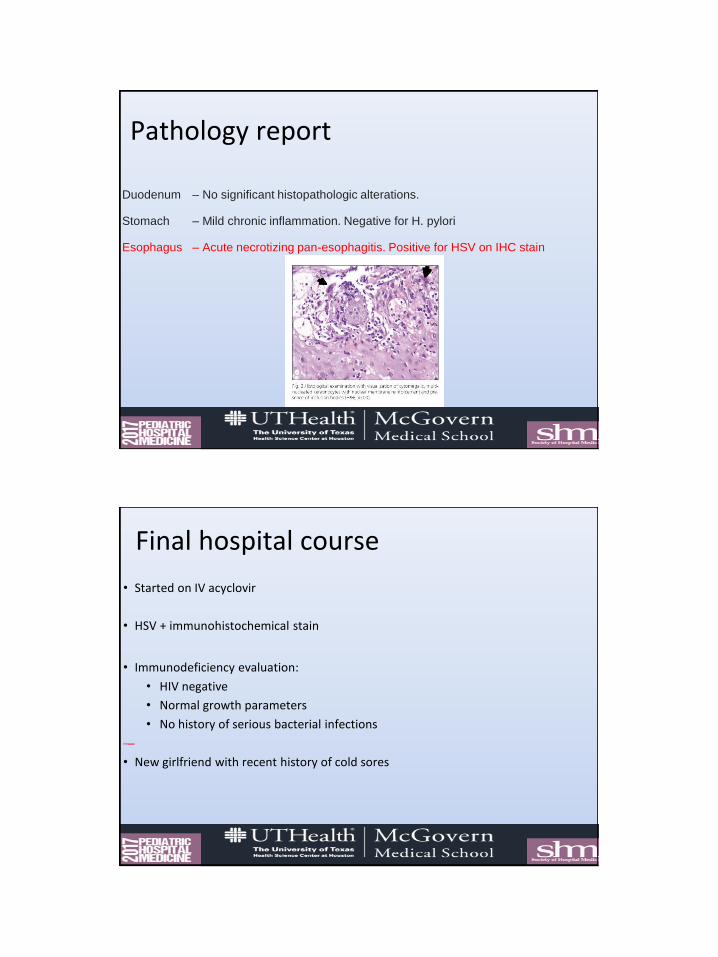
Pathology report
Duodenum – No significant histopathologic alterations.
Stomach – Mild chronic inflammation. Negative for H. pylori
Esophagus – Acute necrotizing pan-esophagitis. Positive for HSV on IHC stain
McGovern Medical School
Final hospital course
• Started on IV acyclovir
• HSV + immunohistochemical stain
• Immunodeficiency evaluation:
• HIV negative
• Normal growth parameters
• No history of serious bacterial infections
• New girlfriend with recent history of cold sores
McGovern Medical School
HSV Esophagitis• Extensively described in immunocompromised hosts
• Can be devastating and fatal in this population (1, 2).
• Only handful of case reports in healthy patients (1-10).
• A review looked at 38 healthy patients, both adult and pediatric with HSV esophagitis (1)
• 3:1 male predominance overall (increased to 90% in the pediatrics)• Typical patient was young, healthy, male (less than 18 years old in ¼ of
cases) presenting with :• acute odynophagia/dysphagia• chest pain• Heartburn • +/- Prodromal symptoms or oral lesions.
McGovern Medical School
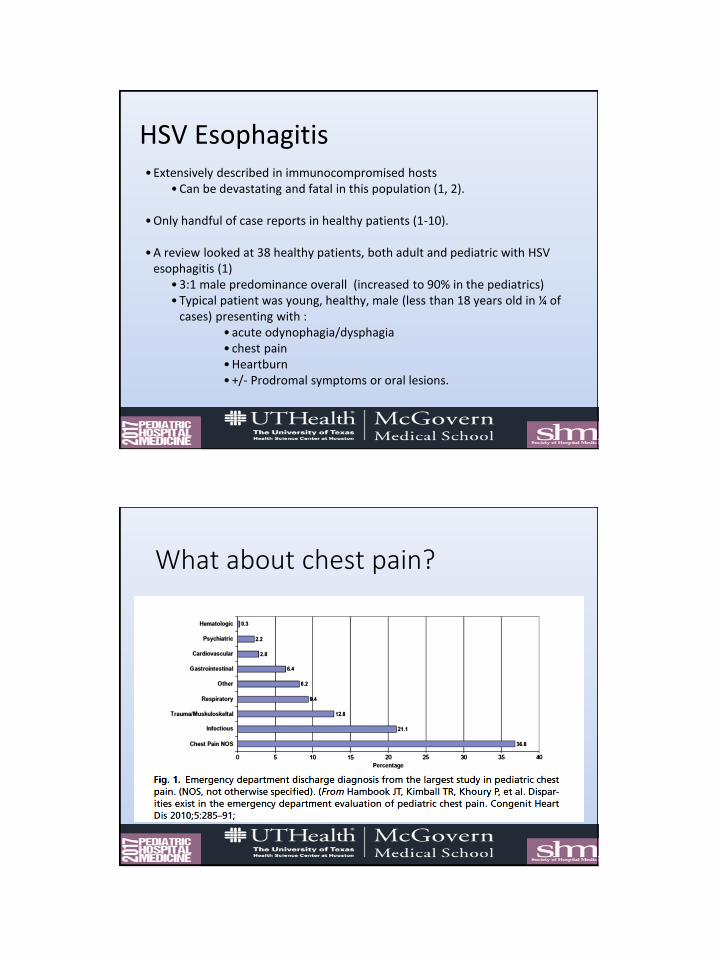
What about chest pain?
McGovern Medical School
Remainder of clinical course• Rapid improvement in clinical status with resolution of chest
pain and dysphagia on initiation of acyclovir therapy
• Able to tolerate adequate PO intake on discharge
• Discharged to complete 7-day course of PO valacyclovir
• Scheduled to follow up in GI clinic in 2 weeks, but by that time, symptoms had resolved and family canceled the follow up visit.
McGovern Medical School
Take Home Points• Cardiac etiology least common cause of chest pain in pediatrics (4-6%)
(11)
• Patients with esophagitis frequently present with retrosternal “chest pain” (1, 7, 9).
• Diagnosis achieved by characteristic appearance on EGD, biopsy specimens, positive HSV IHC stain
• Esophagitis should be considered for all patients presenting with the triad of chest pain, odynophagia, and fever, as early recognition can prevent broad cardiopulmonary workups (10).
McGovern Medical School
References 1. Ramanathan J, Rammouni M, Baran J, Khatib R. Herpes simplex virus esophagitis in the immunocompetent host: an overview.
Am J Gastroenterol. 2000;95(9):2171-6.
2. Lee B, Caddy G. A rare cause of dysphagia: herpes simplex esophagitis. World J Gastroenterol. 2007;13(19):2756-7.
3. Canalejo castrillero E, García durán F, Cabello N, García martínez J. Herpes esophagitis in healthy adults and adolescents: report of 3 cases and review of the literature. Medicine (Baltimore). 2010;89(4):204-10.
4. De-la-riva S, Muñoz-navas M, Rodríguez-lago I, Carrascosa J, Idoate MÁ, Carias R. Herpetic esophagitis: a case report on an immunocompetent adolescent. Rev Esp Enferm Dig. 2012;104(4):214-7.
5. Galbraith JC, Shafran SD. Herpes simplex esophagitis in the immunocompetent patient: report of four cases and review. Clin Infect Dis. 1992;14(4):894-901.
6. Marinho AV, Bonfim VM, De alencar LR, Pinto SA, De araújo filho JA. Herpetic esophagitis in immunocompetent medical student.Case Rep Infect Dis. 2014;2014:930459.
7. Al-hussaini AA, Fagih MA. Herpes simplex ulcerative esophagitis in healthy children. Saudi J Gastroenterol. 2011;17(5):353-6.
8. Kurahara K, Aoyagi K, Nakamura S, et al. Treatment of herpes simplex esophagitis in an immunocompetent patient with intravenous acyclovir: a case report and review of the literature. Am J Gastroenterol. 1998;93(11):2239-40.
9. Rongkavilit C, El-baba MF, Poulik J, Asmar BI. Herpes simplex virus type 1 esophagitis in an immunocompetent adolescent. DigDis Sci. 2004;49(5):774-7.
10. Jibaly R, LaChance J, Abdulhammour W. Herpes simplex esophagitis: Report of 4 pediatric cases in immunocompetent patients. JPediatr Infect Dis 2011;6(3):205-9
11. Eslick GD. Epidemiology and risk factors of pediatric chest pain: a systematic review. Pediatr Clin North Am. 2010;57(6):1211-9.
McGovern Medical School
Questions?..