A Randomized Controlled Trial Comparing Efficacy and ... · 6/4/2018 · diverse range of...
9
A Randomized Controlled Trial Comparing Efficacy and Safety of Insulin Glargine 300 Units/mL Versus 100 Units/mL in Older People With Type 2 Diabetes: Results From the SENIOR Study https://doi.org/10.2337/dc18-0168 OBJECTIVE SENIOR compared the efficacy and safety of insulin glargine 300 units/mL (Gla-300) with glargine 100 units/mL (Gla-100) in older people (‡65 years old) with type 2 diabetes. RESEARCH DESIGN AND METHODS SENIOR was an open-label, two-arm, parallel-group, multicenter phase 3b trial designed to enroll ∼20% of participants aged ‡75 years. Participants were randomized 1:1 to Gla-300 or Gla-100, titrated to a fasting self-monitored plasma glucose of 5.0–7.2 mmol/L (90–130 mg/dL). RESULTS In total, 1,014 participants were randomized (mean age: 71 years). Comparable reductions in HbA 1c were observed from baseline to week 26 for Gla-300 (20.89%) and Gla-100 (20.91%) in the overall population (least squares mean difference: 0.02% [95% CI 20.092 to 0.129]) and for participants aged ‡75 years (20.11% [20.330 to 0.106]). Incidence and rates of confirmed (£3.9 mmol/L [£70 mg/dL]) or severe hypoglycemia events were low and similar between both treatment groups, with lower rates of documented symptomatic hypoglycemia with Gla-300. The lower risk of hypoglycemia with Gla-300 versus Gla-100 was more apparent in the subgroup aged ‡75 years versus the overall population. Significantly lower annualized rates of documented symptomatic (£3.9 mmol/L [£70 mg/dL]) hypoglycemia were observed (Gla-300: 1.12; Gla-100: 2.71; rate ratio: 0.45 [95% CI 0.25–0.83]). CONCLUSIONS Efficacy and safety of Gla-300 was demonstrated in older people (‡65 years of age) with type 2 diabetes, with comparable reductions in HbA 1c and similarly low or lower risk of documented symptomatic hypoglycemia versus Gla-100. A significant benefit in hypoglycemia reduction was seen in participants aged ‡75 years. 1 Klinikum Schwabing and Klinikum Bogenhausen, St¨ adtisches Klinikum M¨ unchen GmbH, Munich, Germany 2 The University of Western Ontario, London, Ontario, Canada 3 University of Southern California, Los Angeles, CA 4 Miller School of Medicine, University of Miami, Coral Gables, FL 5 Bichat Hospital, Paris, France 6 Sanofi, Paris, France 7 Sanofi Deutschland GmbH, Frankfurt am Main, Germany 8 Sanofi R&D China, Beijing, China 9 Joslin Diabetes Center, Harvard University, Boston, MA 10 Department of Medicine, Perugia University Medical School, Perugia, Italy Corresponding author: Robert Ritzel, robert.ritzel@ klinikum-muenchen.de. Received 23 January 2018 and accepted 7 May 2018. Clinical trial reg. no. NCT02585674, clinicaltrials .gov. This article contains Supplementary Data online at http://care.diabetesjournals.org/lookup/ suppl/doi:10.2337/dc18-0168/-/DC1. © 2018 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered. More infor- mation is available at http://www.diabetesjournals .org/content/license. Robert Ritzel, 1 Stewart B. Harris, 2 Helen Baron, 3 Hermes Florez, 4 Ronan Roussel, 5 Melanie Espinasse, 6 Isabel Muehlen-Bartmer, 7 Nianxian Zhang, 8 Monica Bertolini, 6 Claire Brulle-Wohlhueter, 6 Medha Munshi, 9 and Geremia B. Bolli 10 Diabetes Care 1 EMERGING THERAPIES: DRUGS AND REGIMENS Diabetes Care Publish Ahead of Print, published online June 12, 2018
Transcript of A Randomized Controlled Trial Comparing Efficacy and ... · 6/4/2018 · diverse range of...

A Randomized Controlled TrialComparing Efficacy and Safety ofInsulin Glargine 300 Units/mLVersus 100 Units/mL in OlderPeople With Type 2 Diabetes:Results From the SENIOR Studyhttps://doi.org/10.2337/dc18-0168
OBJECTIVE
SENIOR compared the efficacy and safety of insulin glargine 300 units/mL (Gla-300)with glargine 100 units/mL (Gla-100) in older people (‡65 years old) with type 2diabetes.
RESEARCH DESIGN AND METHODS
SENIOR was an open-label, two-arm, parallel-group, multicenter phase 3b trialdesigned to enroll ∼20% of participants aged ‡75 years. Participants wererandomized 1:1 to Gla-300 or Gla-100, titrated to a fasting self-monitored plasmaglucose of 5.0–7.2 mmol/L (90–130 mg/dL).
RESULTS
In total, 1,014 participants were randomized (mean age: 71 years). Comparablereductions in HbA1c were observed from baseline to week 26 for Gla-300 (20.89%)and Gla-100 (20.91%) in the overall population (least squares mean difference:0.02% [95% CI 20.092 to 0.129]) and for participants aged ‡75 years (20.11%[20.330 to 0.106]). Incidence and rates of confirmed (£3.9mmol/L [£70mg/dL]) orsevere hypoglycemia events were low and similar between both treatment groups,with lower rates of documented symptomatic hypoglycemia with Gla-300. Thelower risk of hypoglycemia with Gla-300 versus Gla-100 was more apparent in thesubgroup aged ‡75 years versus the overall population. Significantly lowerannualized rates of documented symptomatic (£3.9 mmol/L [£70 mg/dL])hypoglycemia were observed (Gla-300: 1.12; Gla-100: 2.71; rate ratio: 0.45 [95% CI0.25–0.83]).
CONCLUSIONS
Efficacy and safety of Gla-300 was demonstrated in older people (‡65 years of age)with type 2 diabetes, with comparable reductions in HbA1c and similarly low orlower risk of documented symptomatic hypoglycemia versus Gla-100. A significantbenefit in hypoglycemia reduction was seen in participants aged ‡75 years.
1Klinikum Schwabing and Klinikum Bogenhausen,Stadtisches Klinikum Munchen GmbH, Munich,Germany2The University of Western Ontario, London,Ontario, Canada3University of Southern California, Los Angeles,CA4Miller School of Medicine, University of Miami,Coral Gables, FL5Bichat Hospital, Paris, France6Sanofi, Paris, France7Sanofi Deutschland GmbH, Frankfurt am Main,Germany8Sanofi R&D China, Beijing, China9Joslin Diabetes Center, Harvard University,Boston, MA10Department of Medicine, Perugia UniversityMedical School, Perugia, Italy
Corresponding author: Robert Ritzel, [email protected].
Received 23 January 2018 and accepted 7 May2018.
Clinical trial reg. no. NCT02585674, clinicaltrials.gov.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc18-0168/-/DC1.
© 2018 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered. More infor-mation is available at http://www.diabetesjournals.org/content/license.
Robert Ritzel,1 Stewart B. Harris,2
Helen Baron,3 Hermes Florez,4
Ronan Roussel,5 Melanie Espinasse,6
Isabel Muehlen-Bartmer,7
Nianxian Zhang,8 Monica Bertolini,6
Claire Brulle-Wohlhueter,6
Medha Munshi,9 and Geremia B. Bolli10
Diabetes Care 1
EMER
GINGTH
ERAPIES:
DRUGSANDREG
IMEN
S
Diabetes Care Publish Ahead of Print, published online June 12, 2018

Diabetes is common in older adults,affecting an estimated 20% of people65–79 years of age (94 million people)worldwide in 2015 (1). Prevalence oftype 2 diabetes increases with age owingto attenuated b-cell function and insulinresistance (2). Coupled with the growingproportion of older individuals in the globalpopulation (3) is an increasing requirementfor effective diabetes management forolder people.Therapies for lowering blood glucose
include: several classes of oral antihy-perglycemic drugs; and injectables, suchas rapid-acting and basal insulins andglucagon-like peptide receptor agonists.When insulin is used, a fine balance isrequired between achieving glycemiccontrol and avoiding hypoglycemia. Com-pared with younger populations, olderpeople with diabetes more often requireinsulin and are more prone to hypogly-cemia for multiple reasons such as erraticfood ingestion, insufficient adjustment ofinsulin dose, reduced responses to coun-terregulatory hormones, lower bloodglucose threshold for autonomic symp-toms, andhigher bloodglucosethresholdfor cognitive dysfunction. The latter leadsto impaired awareness of hypoglycemiaand an increased risk of severe hypo-glycemia (4–7). Cognitive impairment inolder adultsmay itself increase the risk ofhypoglycemia owing to difficulties indiabetes management (8). Moreover,the frequent asymptomatic hypoglyce-mic episodes that may result from im-paired awareness can further lower thethreshold for autonomic symptoms andlead to further hypoglycemic episodes(9).Hypoglycemic events in older people
are associated with an increased inci-dence of acute cardiovascular events,impaired cognitive function, dementia,hospitalizations, andmortality (4,6,10–15).Hypoglycemia and its consequences arean even greater burden in people $75years of age than in those 65–74 yearsof age, with hospitalization rates two-fold higher (16). Furthermore, the careof older people is complicated by thediverse range of functional ability, cog-nitive function, comorbid conditions, andfrailty present in this group (8). Despitethese considerations, there are few long-term studies in this population demon-strating the possible benefits of betterglycemic, blood pressure, and lipid con-trol (17).
The basal insulin glargine is availableas insulin glargine 100 units/mL (Gla-100; Sanofi, Paris, France) or insulinglargine 300 units/mL (Gla-300; Sanofi).Compared with Gla-100, Gla-300 providesmore stable and prolonged steady-state pharmacokinetic and pharmaco-dynamic profiles, with blood insulinlevels that more closely resemble nor-mal physiological conditions (18,19).The EDITION 1, 2, and 3 trials comparedthe efficacy and safety of Gla-300 withGla-100 in people with type 2 diabetesanddemonstrated comparable glycemiccontrol over 6months, whichwas bettersustained with Gla-300 throughout the12-month studyperiod, and a significantlylower risk of confirmed (#3.9 mmol/L[#70 mg/dL]) or severe hypoglycemia(definitions based on American Diabe-tes Association [ADA] criteria [20]), atnight (0000–0559 h) and at any time ofday (24 h) with Gla-300 compared withGla-100. A recent post hoc analysisof participants $65 years of age withtype 2 diabetes from EDITION 1–3 con-firmed the comparable glycemic con-trol and reduction in hypoglycemia riskfor Gla-300 versus Gla-100 in this sub-group, with significantly lower rates ofnocturnal (0000–0559 h) hypoglycemia(21).
The SENIOR study was the first pro-spectively designed clinical trial toaddress the efficacy and safety ofbasal insulin (insulin glargine) specificallyin older people ($65 years of age) withtype 2 diabetes. The study was alsodesigned such that;20% of the peopleenrolled would be $75 years of age toexplore Gla-300 versus Gla-100 treat-ment in this population at elevated riskof hypoglycemia (6) and its consequences(4,6,10–15).
RESEARCH DESIGN AND METHODS
Study DesignSENIOR (NCT02320721) was a multina-tional, multicenter, phase 3b, active-controlled, randomized, open-label,two-arm parallel-group study in older peo-ple ($65 years of age) with type 2 di-abetes comprising a 4-week screeningperiod, followed by a 26-week treat-ment period, conducted in 162 centersacross 18 countries.
Key inclusion criteria were age $65years, type 2 diabetes for$1 year treatedwith a pharmacologic antihyperglycemicregimen for $8 weeks before screening,
and glycated hemoglobin (HbA1c) atscreening of 7.5–11% (58–97 mmol/mol)in insulin-naıve participants or 7–10%(53–86 mmol/mol) in insulin-pretreatedparticipants. Exclusion criteria includedthe chronic use of short-acting insulin,participants not on a stable basal insulindose, and cognitive disorder and de-mentia (Mini-Mental State Examinationscore,24). A list of key exclusion criteriafor thestudy isprovided inSupplementaryTable 1.
The study was approved by indepen-dent ethics review boards and conductedaccording to Good Clinical Practice andtheDeclarationofHelsinki. All participantsprovided written, informed consent.
Randomization and TreatmentParticipants were randomized 1:1 to re-ceive Gla-300 or Gla-100. Randomizationwas stratified by HbA1c at screening(,8.0/$8.0% [,64/$64 mmol/mol]),previous use of insulin (naive/pretreated),and by use of sulfonylurea or meglitinideat screening (yes/no).
Basal insulins were self-administeredonce daily. Evening administration wasrecommended, although other times ofday were permissible provided adminis-tration occurred at the same time eachday 63 h. Starting doses were deter-mined by previous dose history: insulin-naıve patients started on a dose of 0.2units/kg, and participants pretreatedwith basal insulin received a startingdose equivalent to their median basalinsulindoseof the3daysbeforebaseline,unless receiving NPH insulin more thanonce daily, in which case a dose 20%lower than the total daily dosewas given.The insulin dose was adjusted every3–4 days to achieve a target fasting self-monitored plasma glucose (SMPG) levelof 5.0–7.2 mmol/L (90–130 mg/dL), theADA-recommended target for healthyolder individuals (8). Dose adjustmentswere as follows: an increase of 3 unitsif .7.2 mmol/L (.130 mg/dL) or a de-creaseof 3 units (or an adjustment at theinvestigators’ discretion) if ,5.0 mmol/L(,90 mg/dL) or in the event of twoor more symptomatic or one severehypoglycemic episode in the precedingweek.
Participants continued their previousantihyperglycemic drugs, if approved foruse with insulin, with the exception ofthiazolidinediones, which were stoppedat randomization.
2 Gla-300 in Older People With Type 2 Diabetes Diabetes Care

OutcomesThe primary efficacy end point waschange in HbA1c from baseline to week26. The main secondary efficacy endpoints were the percentage of partici-pants with one or more confirmed(#3.9 mmol/L [#70 mg/dL]) or severehypoglycemic events occurring at anytime of day (24 h) or at night (0000–0559 h or 2200–0859 h) over 26 weeksof treatment. Other secondary endpoints were assessed in the overall pop-ulation and in a subgroup of participants$75 years of age. These included changein fasting plasma glucose (FPG) frombaseline to week 26, the percentage of
participants experiencing hypoglyce-mic events and annualized rates of hypo-glycemia at either threshold (#3.9mmol/L[#70 mg/dL] and ,3.0 mmol/L [,54mg/dL]) at any time of day [24 h] andat night [0000–0559 h] over 26 weeksof treatment), and the percentage ofparticipants achieving HbA1c ,7.5 and,7.0% (58 and 53mmol/mol) at the endof 26 weeks of treatment. A compositeend point of HbA1c target achievement(,7.5 or,7.0% [58 and 53 mmol/mol])without confirmed (#3.9 mmol/L [#70mg/dL]) or severe hypoglycemia wasalso assessed. Hypoglycemia was definedbased on the ADA workgroup definitions
(20). Data are presented for docu-mented symptomatic hypoglycemia, se-vere hypoglycemia, and as a combinationof confirmed or severe hypoglycemicevents.
Participant-reported outcomes (PROs)were assessed for mobility scores taken
from the EQ-5D, the EuroQol Research
Foundation’s questionnaire that assesses
five dimensions of health: mobility, self-
care, usual activities, pain/discomfort, and
anxiety/depressionas a single utility index
and on a visual analog scale. Safety out-
comes included treatment-emergent ad-
verse events (TEAEs) and severe adverse
events (SAEs).
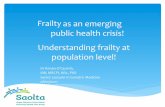
Figure 1—Mean (SE) HbA1c in the overall population (A) and in participants$75 years of age (B) and mean (SE) FPG in the overall population (C) andin participants $75 years of age (D) by visit during the 26-week (W) treatment period (intent-to-treat population). BL, baseline; LS, least squares.
care.diabetesjournals.org Ritzel and Associates 3

Data Analysis and StatisticsA sample size of 460 randomized partic-ipants for each treatment group provided98% power to show noninferiority of Gla-300 versus Gla-100 in HbA1c change frombaseline toweek 26 on the basis of a truedifference between the two groups ofzero and a noninferiority margin of 0.3%.This calculation assumes a common SDof 1.1%, with a one-sided t test at the2.5% significance level. Change in HbA1c(primary end point) and FPG from baselineto week 26 were assessed using a multipleimputation approach for missing dataand ANCOVA using fixed categorical ef-fects of treatment group, randomizationstrata, and continuous fixed covariatesof baseline value. Least squared meanand least squared mean differences werecombined using the Rubin formula.The main secondary end point and
HbA1c target achievement, with or with-out hypoglycemia, was analyzed usingthe Cochran–Mantel–Haenszel methodwith treatment group as a factor andstratified on randomization strata. Non-inferiority and, subsequently, superior-ity of Gla-300 compared with Gla-100was assessed for the primary and mainsecondary end points using a hierarchicalstep-down testing procedure (Supple-mentary Table 2), with two-sided testsfor superiority performed at the levelof a = 0.05. Analyses of safety outcomeswere descriptive. Analyses were per-formed for the overall population andfor the subgroup of participants $75years of age.Exploratory analyses of the percent-
age of patients experiencing one ormore confirmed (#3.9 mmol/L [#70mg/dL]) or severe hypoglycemic event inthe overall population was analyzed byprespecified baseline categories of age(65–70, 70–75, or $75 years), BMI(,30/$30 kg/m2), HbA1c (,8.0/$8.0%[,64/$64 mmol/mol), sulfonylurea ormeglitinide use at screening (yes/no),
diabetes duration (,10/$10 years), his-tory of diabetic neuropathy (yes/no), andestimated glomerular filtration rate cat-egories ($60, 30 to,60, or,30mL/min/1.73 m2). Mean HbA1c and hypoglycemia(incidence and rates) by mobility PROscore subgroup (“no problems”/“slight toextreme problems”) were also performedas exploratory analyses. HbA1c by baselinemobility PRO score subgroup was as-sessed using a similar approach to theprimary analysis. Analyses of hypoglyce-mia by baseline category subgroups weredescriptive. Safety outcomes includedTEAEs and SAEs.
RESULTS
Study ParticipantsA total of 1,014 participants were ran-domized to receive Gla-300 (n = 508) orGla-100 (n = 506) (Supplementary Fig. 1);of these, 135 (26.6%) and 106 (20.9%)participants were $75 years of agefor Gla-300 and Gla-100, respectively.Overall, baseline characteristics weresimilar for the Gla-300 and Gla-100groups (Supplementary Table 3), al-though participants $75 years of agehad a lower mean estimated glomerularfiltrationrate, longerdurationofdiabetes,ahigheroverall rateofdiabetes-relatedcom-plications, and a smaller proportion werepreviously treated with insulin comparedwiththeoverallpopulation(SupplementaryTable 3).
Glycemic Control
Change in HbA1c
Theprimaryobjective of noninferiority ofGla-300 versus Gla-100 for change inHbA1c from baseline to week 26 wasmet (Fig. 1A).Mean (SD) HbA1c decreasedsimilarly in both treatment groups, from8.20% (0.91) for Gla-300 and 8.22% (0.92)for Gla-100 (66.1 [9.9] vs. 66.3 [10.1]mmol/mol) at baseline to 7.31% (0.91)and 7.28% (0.84) (56.4 [9.5] vs. 56.0 [9.2]mmol/mol), respectively.
Change in HbA1c in Participants ‡75 Years
of Age
Within the subpopulation of participants$75 years old, similar reductions inHbA1cfrombaseline toweek 26were observed,from 8.17 (SD 0.89) to 7.29% (0.84) (65.9[9.9] to 56.2 [9.2] mmol/mol) for Gla-300and 8.18 (0.97) to 7.39% (0.87) (65.9[10.64] to 57.3 [9.5] mmol/mol) for Gla-100 (Fig. 1B).
Plasma Glucose
Comparable reductions inmeanFPGwereobserved for both treatment groups frombaseline to week 26 in the overall pop-ulation (Fig. 1C), with reductions of 1.68(SD 0.12) mmol/L and 1.77 (0.14) mmol/L(30.4 [2.2] and 31.8 [2.4] mg/dL, re-spectively). Similar results were ob-served in participants $75 years of age(Fig. 1D).
Reductioninaverage5-pointSMPGandbedtime SMPGwas comparable betweentreatmentgroupsintheoverallpopulationand in participants$75 years of age (datanot shown).
Hypoglycemia
Confirmed (£3.9 mmol/L [£70 mg/dL]) or
Severe Hypoglycemia
Superiority of Gla-300 versus Gla-100 forthe main secondary efficacy end points,the proportion of participants in theintent-to-treat population experiencingone or more confirmed (#3.9 mmol/L[#70 mg/dL]) or severe hypoglycemicevents occurring between 2200–0859 hand 0000–0559 h, was not detected(Table 1).
For the safety population, the pro-portion of participants experiencingone or more confirmed or severe hypogly-cemic events was similar for both treat-ment groups at both the #3.9 mmol/L(#70mg/dL)and,3.0mmol/L(,54mg/dL)thresholds at any time of day (24 h)(Fig. 2A). Similar results were observedat night (0000–0559 h) (Fig. 2A).
Table 1—Percentage of participants experiencing one or more confirmed or severe hypoglycemic event over 26 weeks oftreatment (intent-to-treat population)
Gla-300 (n = 508) Gla-100 (n = 506)RR Gla-300 vs Gla-100a
Confirmed or severe hypoglycemia % participants RR 95% CI P value (CMH)
2200–0859 h 48.3 47.7 1.01 0.890–1.153 0.8415
0000–0559 h 20.2 22.5 0.90 0.706–1.140 d
Any time of the day (24 h) 59.4 62.7 0.95 0.859–1.046 d
CMH, Cochran–Mantel–Haenszel; RR, relative risk. Confirmed hypoglycemia defined as#3.9 mmol/L (#70 mg/dL). aRR stratified by randomizationstrata of screeningHbA1c (,8.0/$8.0%), randomization strata of previoususe of insulin (naıve/pretreated), randomization strataof use of sulfonylureaor meglitinides at screening (yes/no), using a CMH methodology.
4 Gla-300 in Older People With Type 2 Diabetes Diabetes Care

Annualized event rates for confirmed(#3.9 mmol/L [#70 mg/dL]) or severehypoglycemia were similar betweentreatment groups, at night (0000–0559 h)or any time of day, but a trend towardlower rates with Gla-300 compared withGla-100was observed at the lower thresh-old of,3.0mmol/L (,54mg/dL) (Fig. 3A).
Documented Symptomatic Hypoglycemia
The results reported for documentedsymptomatic hypoglycemia were in keep-ing with those seen for confirmed orsevere hypoglycemia. A comparable pro-portionofparticipantsexperiencedoneormore events in both treatment groups atany time of day (24 h) and at night (0000–0559 h); however, fewer participantsexperienced a hypoglycemic event at thelower glycemic threshold of,3.0 mmol/L(,54 mg/dL) with Gla-300 compared withGla-100, although this was not signifi-cant (Fig. 2A).
A trend toward lower annualized eventratesofhypoglycemiawithGla-300versusGla-100 was observed at both glycemicthresholds. These differences were statis-tically significant for anytime (24 h) for the#3.9 mmol/L (#70 mg/dL) and for the,3.0 mmol/L (,54 mg/dL) threshold (Fig.3A).
Severe Hypoglycemia
The incidence and annualized rate ofsevere hypoglycemia were low, withfour participants (0.8%; 0.02 events perparticipant-year) in the Gla-300 group andthree participants (0.6%; 0.01 events perparticipant-year) in the Gla-100 group re-porting one event each.
Hypoglycemia in Participants ‡75 Years
of Age
In general, the proportion of participants$75 years of age experiencing one ormore hypoglycemic event was similar tothe overall SENIOR population.
Within the subgroup of participants$75 years of age, the incidence of con-firmedor severehypoglycemic events forboth glycemic thresholds and docu-mented symptomatic hypoglycemia forthe higher threshold were comparablebetween treatment groups at any timeof day (24 h). The incidence of any time(24 h) documented symptomatic (,3.0mmol/L [,54mg/dL]) hypoglycemiawassignificantly lower with Gla-300 com-pared with Gla-100 (1.5% vs. 10.4%;relative risk 0.33; 95% CI 0.12–0.88)(Fig. 2B).
Statistically significant reductions inannualized rates of hypoglycemia atany time of day (24 h) were observedfor Gla-300 compared with Gla-100 forconfirmed (,3.0 mmol/L [,54 mg/dL])or severehypoglycemiaanddocumentedsymptomatic hypoglycemia at eitherglycemic threshold (Fig. 3B). Nocturnal
Figure 2—Incidence (number and percentage of participants experiencing one or more hypoglycemic event) for the overall population ($65 yearsof age) (A) and for participants $75 years of age (safety population) (B). RR, relative risk.
care.diabetesjournals.org Ritzel and Associates 5

(0000–0559 h) incidence and rates were
comparable between treatment groups
for both confirmed and severe and fordocumented symptomatic hypoglycemiaat the#3.9mmol/L (#70mg/dL) thresh-old (Fig. 3B).No severe hypoglycemic events were
observed in participants $75 years ofage.
Hypoglycemia Incidence by Baseline
Characteristics
The results observed in the overall pop-ulation were consistent across the base-line subgroups, with a similar percentageof participants experiencing confirmed orsevere hypoglycemia and documentedsymptomatic hypoglycemia (#3.9 mmol/L[#70 mg/dL]) with Gla-300 compared withGla-100 irrespective of age, BMI, HbA1c,previous insulin use, sulfonylurea or megli-tinide use, diabetes duration, nutritionalstatus, diabetic neuropathy, or kidney func-tion (Supplementary Fig. 2).
HbA1c Target Achievement andComposite End PointThe proportion of participants achiev-ing HbA1c ,7.5% (,58 mmol/mol) and,7.0% (,53 mmol/mol) was compara-ble between treatment groups for theoverall population and for participants$75 years of age (Supplementary Table4). Similar results were observed for thecomposite end points of HbA1c targetachievement without confirmed (#3.9mmol/L [#70 mg/dL]) or severe hypogly-cemia, although significantly more partic-ipants inthe$75yearsagegroupachievedHbA1c ,7.5% (,58 mmol/mol) withoutconfirmed (#3.9mmol/L [#70mg/dL]) orsevere hypoglycemia with Gla-300 versusGla-100.
The incidence of confirmed or severehypoglycemic events and documentedsymptomatic events (#3.9 mmol/L [#70mg/dL]) was similar between treatmentgroups, irrespective of HbA1c level achievedat week 26 (Supplementary Fig. 3).
Efficacy and Safety by Mobility PROScoreThe majority of participants (;60%) inboth treatment groups reported no mo-bility problems, and few participants(,1.0%) reported extreme problemsat baseline. No difference in meanHbA1c change from baseline to week26 was observed between participantswho reported no mobility problems atbaseline and those who reported slighttoextremeproblems (SupplementaryFig. 4).No differences were observed in theincidence or rates of hypoglycemia be-tween treatment groups at any timeof day or at night for participants whoreported mobility problems at baselineandfor thosewhodidnot (SupplementaryFig. 5).
Adverse EventsTEAEs were reported in 299 partici-pants (58.9%) in the Gla-300 groupand in 304 (60.2%) in the Gla-100 group
Figure 3—Annualized rates (events per participant-year) of hypoglycemia for the overall population ($65 years of age) (A) and for participants$75 years of age (safety population) (B). RR, rate ratio. (A high-quality color representation of this figure is available in the online issue.)
6 Gla-300 in Older People With Type 2 Diabetes Diabetes Care

(Supplementary Table 5), with infections(25.8% and 29.7% for Gla-300 and Gla-100, respectively) the most commonlyreported TEAEs. The incidence of TEAEsin participants $75 years of age wassimilar to theoverall$65 yearspopulation(59.3% for Gla-300 and 54.7% for Gla-100)(Supplementary Table 5).
CONCLUSIONS
SENIOR was the first prospective studydesigned to evaluate the efficacy andsafety of basal insulin in older peoplewith type 2 diabetes, with ;20% ofparticipants $75 years of age (4). Re-sults of SENIOR demonstrate that theefficacy and safety profile of Gla-300and Gla-100 observed in the EDITIONstudies (22–25) is also apparent in olderadults ($65 years of age) with type 2diabetes. The incidence of TEAEs wassimilar between treatment groups for theoverall population and for participants$75 years of age (54.7–60.2%) andwas consistent with that observed forthe older population of the EDITIONstudies (21).Reductions in HbA1c were comparable
between treatment groups, with .50%of participants in either age groupachieving HbA1c of ,7.5%. Reduc-tions in FPG were also comparable be-tween treatment groups and betweenage groups, indicating that insulin wasadjusted similarly in the overall pop-ulation and in participants $75 yearsof age.A consistent trend for reduced hy-
poglycemia for Gla-300 versus Gla-100was observed in the overall SENIORpopulation, with statistically significantreductions seen for rates of documentedsymptomatic hypoglycemia at any timeof day (24 h). Interestingly, reductions inhypoglycemia for Gla-300 versus Gla-100were more pronounced in individuals$75 years of age, who are known to beat a greater risk of hypoglycemia (4),with a significantly lower risk of docu-mented symptomatic hypoglycemia atany timeof day (24h) observedwithGla-300 compared with Gla-100 in this sub-group. This is an important finding in anunderstudied and particularly vulnera-ble population and might be consideredwhen deciding among basal insulin op-tions in older adults, particularly in thoseolder than 75 years. Although some di-fferences were observed in baselinecharacteristics in the participants $75
years of age compared with the overallSENIOR population (predominantly age-related changes that may be expected),whether thesedifferences contributed tothe more pronounced hypoglycemiabenefit with Gla-300 versus Gla-100 inthe $75 years population is unknownbecause this is outside the remit of thepresent study.
When hypoglycemia incidence wasassessed according to baseline charac-teristics (age, BMI, HbA1c, previous in-sulinuse, sulfonylureaormeglitinideuse,diabetes duration, nutritional status, di-abetic neuropathy, or kidney function),no differences were observed in hypo-glycemia risk between treatment groupsfor any subgroup. In addition, hypo-glycemia risk profiles did not differbetween participants who reportedmo-bility problems and those who did not.Hypoglycemia is associated with mor-bidities that may lead to physical dys-function, and this can create a cyclicalrelationship between hypoglycemia andincreased frailty (4). As such, it is reas-suring to note that the hypoglycemia riskprofiles for both insulins did not differbetween participants who experiencedmobility problems and those who didnot. Furthermore, good glycemic con-trol was demonstrated in both groups,suggesting that the observed comparablehypoglycemia profiles were not due tohypoglycemia avoidance through poorglycemic control.
The small differences in hypogly-cemia risk reductions observed betweenGla-300andGla-100 in theoverall popula-tion in SENIOR may be due, in part, tothe low number of hypoglycemic eventsobserved. Participants in EDITION 2, forexample, experienced a greater numberof hypoglycemic events compared withSENIOR participants (SupplementaryTable 6), and significant differences inhypoglycemia rates and incidence wereobserved between Gla-300 and Gla-100(25). This hypothesis is supported bythe comparable low incidence of hy-poglycemia in SENIOR and EDITION 3(Supplementary Table 6), with similarlyfew significant differences in hypogly-cemia risk observed between treatmentgroups for both studies (22,23). Factorsunderpinning the low number or hypo-glycemic events reported in SENIOR mayinclude the higher glycemic treatmenttarget set in SENIOR (5.0–7.2 mmol/L[90–130 mg/dL]) compared with that
used in the EDITION trials (22–25) orthe less frequent SMPG monitoring re-quired for SENIOR, which, coupled withthe lower perception of hypoglycemiasymptoms in older individuals (4,5),may have allowed for undetected hypo-glycemic events to have occurred. Im-paired awareness of hypoglycemia inolder people ($65 years of age) mayalso explain the lack of nocturnal hypo-glycemia risk reduction with Gla-300versus Gla-100 in the present study, de-spite this being a consistent finding re-ported in all EDITION studies (22–25). Forexample,astudyusingcontinuousglucosemonitoring to examine hypoglycemia in apopulation aged $69 years old reportedthat 93% of events were unrecognized(26).Giventhattheriskofhypoglycemia inolder people is likely to be underesti-mated, the trend toward a greater re-duction in hypoglycemic risk observedwith Gla-300 versus Gla-100, which wasconsistent with those observed in theoverall EDITION population (27,28) andin the older population of the EDITIONstudies (21), may be beneficial in olderpeopleandwill be the focusof future real-world investigations.
In keepingwith ADA recommendationsfor older people (8), the SENIOR studyused a titration algorithm with a higherglycemic target of 5.0–7.2 mmol/L(90–130 mg/dL) compared with 4.4–7.2 mmol/L (80–130 mg/dL) recommen-ded for the overall population, owingto the diversity of cognitive function,frailty, comorbidities, polypharmacy,and pathophysiology observed in olderadults. Despite this, similar reductions inHbA1c and FPG were observed in SENIORcompared with the overall EDITION popu-lation with type 2 diabetes (27,28) and thecombined older ($65 years) populationsof EDITION 1–3 studies (21), whereas alower glycemic target (4.4–7.2 mmol/L[80–130 mg/dL]) was used (22–25).Furthermore, .50% of participants inSENIOR achieved a target HbA1c of,7.5%(,58 mmol/mol), similar to HbA1c tar-get achievement observed in partici-pants $65 years of age from EDITION1–3 (21).Hence, the results fromSENIORshow that Gla-300 can be used in olderpeople with type 2 diabetes, in accor-dance with the ADA safety recommen-dations to use higher glycemic targets,without compromising efficacy.
Limitations of SENIOR include theopen-label design (owing to the different
care.diabetesjournals.org Ritzel and Associates 7

pen injectors) and the lack of functionalmobility assessments. Although mobilitywas assessed using PROs, the standardizedEQ-5D questionnaire used may not havehad sufficient sensitivity to detect anydifferences in mobility score during thecourse of the study. Owing to the rela-tively small number of hypoglycemicevents reported, the power to detectsignificant differences in hypoglycemiariskwas low. In addition, further analysesare required to explain the lower hypo-glycemia risk with Gla-300 comparedwith Gla-100 observed in participantsaged $75 years.In summary, Gla-300 demonstrated
good efficacy and safety in older peoplewith type 2diabetes, particularly in thoseof advanced age ($75 years). In theoverall population, comparable reduc-tions in HbA1c and lower rates of docu-mented symptomatic hypoglycemiawere observed with Gla-300 versusGla-100. Although the risk of hypoglyce-mia was similar in all prespecified base-line characteristic subgroups, a greaterreduction in the rate of documentedsymptomatic hypoglycemia with Gla-300 versus Gla-100 was observed inthe subgroup of people $75 years ofage. Results of SENIOR confirm thosepreviously observed in both the overalland the older population of the EDITION1–3 studies (21–23,25), with similar re-ductions in HbA1c observed despite theless stringent glycemic target used inSENIOR, indicating that Gla-300 is suitablefor use in this vulnerable population.
Acknowledgments. The authors thank thestudy participants, trial staff, and investigatorsfor their participation.Funding. This study was sponsored by Sanofi.The clinical trial considered in this analysis wassponsored by Sanofi, Paris, France. Editorial andwriting assistance was provided by HannahBrown, PhD, of Fishawack Communications,and was funded by Sanofi.Duality of Interest. R.Ri. is a consultant forAstraZeneca, Merck, Novo Nordisk, Sanofi, andServier and is on the speakers bureau forAstraZeneca, Boehringer Ingelheim, Eli Lilly,Merck,Novartis, Novo Nordisk, and Sanofi. S.B.H. is aconsultant for Abbott, AstraZeneca, BoehringerIngelheim,Eli Lilly, Janssen,Merck,NovoNordisk,and Sanofi and receives research and supportfrom Abbott, AstraZeneca, Boehringer Ingel-heim, Eli Lilly, Janssen, Novo Nordisk, and Sanofi.H.B. is a consultant for Intarcia, Novo Nordisk,and Sanofi and is on the speakers bureau forNovo Nordisk and Sanofi. H.F. is a consultant forSanofi. R.Ro. is on the advisory panel of Amgen,
AstraZeneca, Sanofi, MSD, Eli Lilly, Janssen, NovoNordisk, Physiogenex, and Danone Research andis a consultant for Sanofi.M.E., I.M.-B.,N.Z.,M.B.,and C.B.-W. are employees of Sanofi and disclosestocks and shares of Sanofi. M.M. is a consultantfor Sanofi. G.B.B. is on the Sanofi advisory panel,is a consultant for Novartis, and is on the Eli Lillyspeakers bureau. No other potential conflicts ofinterest relevant to this article were reported.Author Contributions. Sanofi was responsiblefor the design and coordination of the trial,monitoring clinical sites, collecting andmanagingdata, andperformingall statistical analyses.R.Ri.,S.B.H., H.B., H.F., R.Ro., M.E., I.M.-B., N.Z., M.B.,C.B.-W., M.M., and G.B.B. contributed to inter-preting the findings and to writing, reviewing,and editing the manuscript. R.Ri., M.E., I.M.-B.,and N.Z. developed the initial concept for thisanalysis. H.B., H.F., and M.M. were responsiblefor data acquisition. R.Ri. is the guarantor of thiswork and, as such, had full access to all thedata inthe study and takes responsibility for the inte-grity of the data and the accuracy of the dataanalysis.
References1. The International Diabetes Federation. IDF Di-abetesAtlas.7thed. [Internet],2015.Availablefromhttps://www.idf.org/e-library/epidemiology-research/diabetes-atlas/13-diabetes-atlas-seventh-edition.html.Accessed 8 November 20162. Helman A, Avrahami D, Klochendler A, et al.Effects of ageing and senescence on pancreaticb-cell function. Diabetes Obes Metab 2016;18(Suppl. 1):58–623. World Health Organization. Global health andaging [Internet], 2011. Available from http://www.who.int/ageing/publications/global_health.pdf?ua51. Accessed 20 July 20174. Abdelhafiz AH, Rodrıguez-Ma~nas L,Morley JE,Sinclair AJ. Hypoglycemia in older people - a lesswell recognized risk factor for frailty. Aging Dis2015;6:156–1675. Matyka K, Evans M, Lomas J, Cranston I,Macdonald I, Amiel SA. Altered hierarchy ofprotective responses against severe hypoglyce-mia in normal aging in healthy men. DiabetesCare 1997;20:135–1416. Kirkman MS, Briscoe VJ, Clark N, et al. Di-abetes in older adults. Diabetes Care 2012;35:2650–26647. Dhaliwal R, Weinstock RS. Managementof type 1 diabetes in older adults. DiabetesSpectr 2014;27:9–208. American Diabetes Association. Standards ofMedical Care in Diabetes–2017. Diabetes Care2017;40(Suppl. 1):S1–S1359. Cryer PE. Mechanisms of hypoglycemia-associated autonomic failure and its compo-nent syndromes in diabetes. Diabetes 2005;54:3592–360110. Sinclair A, Morley JE, Rodriguez-Ma~nas L,et al. Diabetes mellitus in older people: positionstatement on behalf of the International Asso-ciation of Gerontology and Geriatrics (IAGG), theEuropean Diabetes Working Party for OlderPeople (EDWPOP), and the International TaskForce of Experts in Diabetes. J AmMed Dir Assoc2012;13:497–50211. Whitmer RA, Karter AJ, Yaffe K, QuesenberryCP Jr., Selby JV. Hypoglycemic episodes and
risk of dementia in older patients with type 2diabetes mellitus. JAMA 2009;301:1565–157212. Geller AI, Shehab N, Lovegrove MC, et al.National estimates of insulin-related hypoglyce-miaanderrors leading toemergencydepartmentvisits and hospitalizations. JAMA Intern Med2014;174:678–68613. KaganskyN,LevyS,RimonE,etal.Hypoglycemiaas a predictor of mortality in hospitalized elderlypatients. Arch Intern Med 2003;163:1825–182914. Majumdar SR, Hemmelgarn BR, Lin M,McBrien K, Manns BJ, Tonelli M. Hypoglycemiaassociated with hospitalization and adverseevents in older people: population-based cohortstudy. Diabetes Care 2013;36:3585–359015. StepkaM,RogalaH,CzyzykA.Hypoglycemia:a major problem in themanagement of diabetesin the elderly. Aging (Milano) 1993;5:117–12116. Lipska KJ, Ross JS, Wang Y, et al. Nationaltrends in US hospital admissions for hypergly-cemia and hypoglycemia among Medicare ben-eficiaries, 1999 to 2011. JAMA Intern Med 2014;174:1116–112417. Lakey WC, Barnard K, Batch BC, Chiswell K,Tasneem A, Green JB. Are current clinical trialsin diabetes addressing important issues in dia-betes care? Diabetologia 2013;56:1226–123518. Becker RH, Dahmen R, Bergmann K,Lehmann A, Jax T, Heise T. New insulin glargine300 unitszmL21 provides a more even activityprofile and prolonged glycemic control atsteady state compared with insulin glargine100 unitszmL21. Diabetes Care 2015;38:637–64319. Porcellati F, Lucidi P, Andreoli AM, et al.More physiological circulating insulin and mod-ulationofhepatic glucoseproductionwith insulinglargine U300 vs. U100 in type 1 diabetes. Di-abetes 2017;66:A26920. Workgroup on Hypoglycemia; American Di-abetes Association. Defining and reporting hy-poglycemia in diabetes: a report from theAmerican Diabetes Association Workgroup onHypoglycemia. Diabetes Care 2005;28:1245–124921. Yale JF, Aroda VR, Charbonnel B, et al. Olderpeoplewithtype2diabetes:glycemiccontrolandhypoglycaemic risk with new insulin glargine300 U/mL. Diabetes 2015;64(Suppl. 1):A26122. Bolli GB, Riddle MC, Bergenstal RM,Wardecki M, Goyeau H, Home PD; EDITION3 Study Investigators. Glycaemic control andhypoglycaemia with insulin glargine 300U/mLversus insulin glargine 100U/mL in insulin-naıvepeople with type 2 diabetes: 12-month resultsfrom the EDITION 3 trial. Diabetes Metab 2017;43:351–35823. Bolli GB, Riddle MC, Bergenstal RM, et al.;EDITION 3 Study Investigators. New insulin glar-gine 300 U/ml compared with glargine 100 U/mlin insulin-naıve people with type 2 diabetes onoral glucose-lowering drugs: a randomized con-trolled trial (EDITION 3). Diabetes Obes Metab2015;17:386–39424. Riddle MC, Bolli GB, Ziemen M, Muehlen-Bartmer I, Bizet F, Home PD; EDITION 1 StudyInvestigators. New insulin glargine 300 units/mLversus glargine 100 units/mL in people withtype 2 diabetes using basal andmealtime insulin:glucose control and hypoglycemia in a 6-monthrandomized controlled trial (EDITION 1). Diabe-tes Care 2014;37:2755–276225. Yki-Jarvinen H, Bergenstal R, Ziemen M,et al.; EDITION 2 Study Investigators. New insulin
8 Gla-300 in Older People With Type 2 Diabetes Diabetes Care

glargine 300 units/mL versus glargine 100 units/mLin people with type 2 diabetes using oral agentsand basal insulin: glucose control and hypo-glycemia in a 6-month randomized controlledtrial (EDITION 2). Diabetes Care 2014;37:3235–324326. MunshiMN, Segal AR, Suhl E, et al. Frequenthypoglycemia among elderly patients with poor
glycemic control. Arch Intern Med 2011;171:362–36427. Ritzel R, Roussel R, Bolli GB, et al. Patient-level meta-analysis of the EDITION 1, 2 and3 studies: glycaemic control and hypoglycaemiawith new insulin glargine 300 U/ml versus glar-gine 100 U/ml in people with type 2 diabetes.Diabetes Obes Metab 2015;17:859–867
28. Ritzel R, Roussel R, Giaccari A, Vora J, Brulle-Wohlhueter C, Yki-Jarvinen H. Better glycaemiccontrol and less hypoglycaemia with insulinglargine 300 U/mL vs glargine 100 U/mL:1-year patient-level meta-analysis of theEDITION clinical studies in people with type 2diabetes. Diabetes Obes Metab 2018;20:541–548
care.diabetesjournals.org Ritzel and Associates 9