A randomized controlled clinical trial to evaluate a new xenograft for ...
131
Monica Calasans-Maia Rodrigo Resende Gustavo Fernandes Jose Calasans-Maia Adriana Terezinha Alves Jos e Mauro Granjeiro A randomized controlled clinical trial to evaluate a new xenograft for alveolar socket preservation Authors’ affiliations: Monica Calasans-Maia, Rodrigo Resende, Department of Oral Surgery, Fluminense Federal University, Niteroi, Brazil Gustavo Fernandes, Cell and Molecular Biology Department, Fluminense Federal University, Niteroi, Brazil Jose Calasans-Maia, Department of Orthodontics, Fluminense Federal University, Nova Friburgo, Brazil Adriana Terezinha Alves, Department of Oral Pathology, Gama Filho University, Rio de Janeiro, Brazil Jos e Mauro Granjeiro, Fluminense Federal University, Niteroi, Brazil Bioengineering Program, National Institute of Metrology Standardization and Industrial Quality, Duque de Caxias, Brazil Corresponding author: Monica Calasans-Maia Department of Oral Surgery Fluminense Federal University Rua Mario Santos Braga 30. Centro Niteroi Rio de janeiro CEP: 24020-140 Brazil e-mail: [email protected] Key words: bone implant interactions, bone substitutes, clinical research, clinical trials Abstract Objective: The aim of this clinical trial was to compare the effect of Bio-Oss â and a new bovine xenograft (Osseus â ) in alveolar sockets after a 24-week healing period. Materials and methods: A total of 20 adult volunteers ages 30–60 were subjected to single tooth extraction. A tooth extraction was performed at the baseline. All sites were randomly allocated to two test groups (TG1: grafted using a new bovine xenograft, Osseus â , and TG2: grafted using commercially available bovine xenograft-Bio-Oss â ). Six months later, a sample of the grafted area was obtained and implants were inserted in the same site. Histological sections were examined focusing on the presence of fibrous connective tissue (CT), and newly formed bone in direct contact with the graft. The HE-stained sections were subjected to histomorphometrical evaluation using Image Pro-Plus â software (Release 7.0). The definitive crown was placed 3 months later. Results: Upon completion of the study, no patients were removed from the study and all inserted implants (10 in each group) were eventually integrated. After 6 months, in the TG1, the mean value of new bone formation was 33.7 ( 7.1), for CT was 32.3 ( 8.9) and for the remaining biomaterial was 10.7 ( 16.2). In the TG2, the mean value of new bone formation was 19.3 ( 22.6), of the CT was 49.9 ( 14.1) and of the remaining biomaterial was 22.6 ( 7.9). Conclusions: No statistically significant difference was observed between TG1 and TG2 after 6 months (P > 0.05), and both biomaterials afforded a more favorable implant position. The aim of implant dentistry is to restore missing or extracted teeth by placing implants in anatomical, esthetical, and long-term functional restorative positions (Kutkut et al. 2012). The amount of hard tissue resorption following tooth extraction occasionally involves prosthetically driven implant place- ment; therefore, the development of ridge preservation techniques that result in less alveolar bone loss is of great interest (Sisti et al. 2012). Extraction socket wound healing is characterized by resorption of the alveolar bone at the extraction site, which reduces the bone volume available for implant place- ment. Major changes in the extraction socket occur during the first year after tooth extrac- tion, with two-thirds of the bone loss occur- ring within the first 3 months (Schropp et al. 2003; Ara ujo et al. 2008; Van der Weijden et al. 2009), although dimensional changes are observed up to 1 year after tooth extrac- tion, resulting in a 50% reduction in the buc- colingual dimension of the alveolar ridge (Schropp et al. 2003), primarily due to the resorption of the buccal bone plate (Ara ujo & Lindhe 2011). The ridge preservation proce- dures facilitate the preservation of the alveo- lar architecture to prevent hard and soft tissue collapse and minimize or eliminate the necessity for future augmentation proce- dures (Tan et al. 2012). Many graft materials, such as autogenous bone grafts (Pelegrine et al. 2010), allografts (Wood et al. 2012; xenografts (Calasans-Maia et al. 2009; Fernan- des et al. 2011; Spinato et al. 2012; Festa et al. 2011), and alloplasts (Gonshor et al. 2011; Ruga et al. 2011; Brkovic et al. 2012), have been used to maintain the dimensions of the alveolar ridge after extraction in humans. Although some of these graft mate- rials preserved the post-extraction alveolar ridge dimensions to some extent, the quan- tity and the quality of the bone tissue forma- tion in the socket varied and the presence of these materials has often affected the usual healing process (Heberer et al. 2011). Date: Accepted 3 July 2013 To cite this article: Calasans-Maia M, Resende R, Fernandes G, Calasans-Maia J, Alves AT, Granjeiro JM. A randomized controlled clinical trial to evaluate a new xenograft for alveolar socket preservation. Clin. Oral Impl. Res. 00, 2013, 1–6 doi: 10.1111/clr.12237 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 1
Transcript of A randomized controlled clinical trial to evaluate a new xenograft for ...

Monica Calasans-MaiaRodrigo ResendeGustavo FernandesJose Calasans-MaiaAdriana Terezinha AlvesJos�e Mauro Granjeiro
A randomized controlled clinical trialto evaluate a new xenograft foralveolar socket preservation
Authors’ affiliations:Monica Calasans-Maia, Rodrigo Resende,Department of Oral Surgery, Fluminense FederalUniversity, Niteroi, BrazilGustavo Fernandes, Cell and Molecular BiologyDepartment, Fluminense Federal University,Niteroi, BrazilJose Calasans-Maia, Department of Orthodontics,Fluminense Federal University, Nova Friburgo,BrazilAdriana Terezinha Alves, Department of OralPathology, Gama Filho University, Rio de Janeiro,BrazilJos�e Mauro Granjeiro, Fluminense FederalUniversity, Niteroi, BrazilBioengineering Program, National Institute ofMetrology Standardization and Industrial Quality,Duque de Caxias, Brazil
Corresponding author:Monica Calasans-MaiaDepartment of Oral SurgeryFluminense Federal UniversityRua Mario Santos Braga30. CentroNiteroiRio de janeiroCEP: 24020-140Brazile-mail: [email protected]
Key words: bone implant interactions, bone substitutes, clinical research, clinical trials
Abstract
Objective: The aim of this clinical trial was to compare the effect of Bio-Oss� and a new bovine
xenograft (Osseus�) in alveolar sockets after a 24-week healing period.
Materials and methods: A total of 20 adult volunteers ages 30–60 were subjected to single tooth
extraction. A tooth extraction was performed at the baseline. All sites were randomly allocated to
two test groups (TG1: grafted using a new bovine xenograft, Osseus�, and TG2: grafted using
commercially available bovine xenograft-Bio-Oss�). Six months later, a sample of the grafted area
was obtained and implants were inserted in the same site. Histological sections were examined
focusing on the presence of fibrous connective tissue (CT), and newly formed bone in direct
contact with the graft. The HE-stained sections were subjected to histomorphometrical evaluation
using Image Pro-Plus� software (Release 7.0). The definitive crown was placed 3 months later.
Results: Upon completion of the study, no patients were removed from the study and all inserted
implants (10 in each group) were eventually integrated. After 6 months, in the TG1, the mean
value of new bone formation was 33.7 (�7.1), for CT was 32.3 (�8.9) and for the remaining
biomaterial was 10.7 (�16.2). In the TG2, the mean value of new bone formation was 19.3 (�22.6),
of the CT was 49.9 (�14.1) and of the remaining biomaterial was 22.6 (�7.9).
Conclusions: No statistically significant difference was observed between TG1 and TG2 after
6 months (P > 0.05), and both biomaterials afforded a more favorable implant position.
The aim of implant dentistry is to restore
missing or extracted teeth by placing implants
in anatomical, esthetical, and long-term
functional restorative positions (Kutkut et al.
2012). The amount of hard tissue resorption
following tooth extraction occasionally
involves prosthetically driven implant place-
ment; therefore, the development of ridge
preservation techniques that result in less
alveolar bone loss is of great interest (Sisti
et al. 2012). Extraction socket wound healing
is characterized by resorption of the alveolar
bone at the extraction site, which reduces
the bone volume available for implant place-
ment. Major changes in the extraction socket
occur during the first year after tooth extrac-
tion, with two-thirds of the bone loss occur-
ring within the first 3 months (Schropp et al.
2003; Ara�ujo et al. 2008; Van der Weijden
et al. 2009), although dimensional changes
are observed up to 1 year after tooth extrac-
tion, resulting in a 50% reduction in the buc-
colingual dimension of the alveolar ridge
(Schropp et al. 2003), primarily due to the
resorption of the buccal bone plate (Ara�ujo &
Lindhe 2011). The ridge preservation proce-
dures facilitate the preservation of the alveo-
lar architecture to prevent hard and soft
tissue collapse and minimize or eliminate
the necessity for future augmentation proce-
dures (Tan et al. 2012). Many graft materials,
such as autogenous bone grafts (Pelegrine
et al. 2010), allografts (Wood et al. 2012;
xenografts (Calasans-Maia et al. 2009; Fernan-
des et al. 2011; Spinato et al. 2012; Festa
et al. 2011), and alloplasts (Gonshor et al.
2011; Ruga et al. 2011; Brkovic et al. 2012),
have been used to maintain the dimensions
of the alveolar ridge after extraction in
humans. Although some of these graft mate-
rials preserved the post-extraction alveolar
ridge dimensions to some extent, the quan-
tity and the quality of the bone tissue forma-
tion in the socket varied and the presence
of these materials has often affected the
usual healing process (Heberer et al. 2011).
Date:Accepted 3 July 2013
To cite this article:Calasans-Maia M, Resende R, Fernandes G, Calasans-Maia J,Alves AT, Granjeiro JM. A randomized controlled clinicaltrial to evaluate a new xenograft for alveolar socketpreservation.Clin. Oral Impl. Res. 00, 2013, 1–6doi: 10.1111/clr.12237
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 1

Xenografts are obtained from a species that is
different from that of the recipients, and as
osteoconductors, these grafts are predomi-
nantly made from the inorganic portion of
animal bone tissue (Granjeiro et al. 2005;
Munhoz et al. 2006; Calasans-Maia et al.
2009; Accorsi-Mendonc�a et al. 2011; Zam-
buzzi et al. 2012). The processing of bovine
bone results in two distinct types of materi-
als: inorganic and organic (predominantly col-
lagen type I). Inorganic material is free of
proteins and cells because it only consists of
hydroxyapatite. The proteins are removed
through heat treatment at temperatures
above 300°C or alkali treatment, followed by
neutralization, thus eliminating the risk of
disease transmission. However, the bioab-
sorption of these materials is reduced with
increasing temperature (Wenz et al. 2001).
Indeed, bovine materials obtained from Brazil
are regarded favorably, as Brazilian cattle are
free of spongiform encephalopathy (BSE or
mad cow disease). A new Brazilian bone sub-
stitute (Osseous�; SIN, S~ao Paulo, SP, Brazil),
comprising an inorganic bovine bone matrix,
has been used as an alternative graft material
for ridge preservation after tooth extraction
prior to implant placement. In previous in
vivo studies, we confirmed that this bovine
xenograft is a biocompatible, bioabsorbable
osteoconductor (Calasans-Maia et al. 2009;
Jardelino-Lima et al. 2008). The aim of this
study was to compare the effects of two
deproteinized bovine bone minerals in the
healing of fresh extraction sockets using
clinical, histological, and histomorphometric
analyses.
Material and methods
This study was performed in compliance
with the principles outlined in the Declara-
tion of Helsinki concerning experimentation
involving human subjects. Quality assess-
ment was carried out based on the RCT-
checklist of the CONSORT-statements
(Schulz et al. 2010). All procedures and mate-
rials in the present study were approved
through the relevant independent committee
on the Ethics of Human Research of Flumin-
ense Federal University (CEP/HUAP nº 118),
and the volunteer subjects were informed
about the study protocol and required to sign
a consent form. Twenty patients (ten women
and 10 men) participated in this randomized,
controlled clinical trial, which took place in
the Dental Clinical Research Center at Flu-
minense Federal University, Rio de Janeiro,
Brazil (Table 1, Data S1). A minimum sample
size (10 subjects per group) was established
in an attempt to minimize the publication
bias (Vignoletti et al. 2012, Sisti et al. 2012).
Patient selection
All the patients were in general good health.
Any patient requiring one tooth extraction
(hopeless tooth for periodontal, traumatic, or
caries reasons) and showing a bone defect
between 3 and 5 mm at the buccal wall and
no soft tissue recession was eligible for this
study according to specific exclusion and
inclusion criteria (Table 2). The recruitment
of the volunteers was carried out during
6 months, and all volunteers were followed
up for a period of 12 months after prosthetic
rehabilitation. The volunteer subjects were
randomly assigned to the tests groups using
an envelope system distribution provided by
the principal investigator.
Presurgical procedures
The medical and dental histories of the
patients were reviewed, and each patient
was evaluated using periapical radiographs,
clinical photographs, study casts, and clinical
examinations of the extraction sites. Sub-
sequently, the volunteers were provided
with detailed oral hygiene instructions, and
customized surgical splints were fabricated
on the study casts for use in reentry proce-
dures to accurately obtain bone biopsies from
the center of the grafted sockets.
Surgical procedures
The following implant procedure was used at
all extraction sites. The extraction was
performed under local anesthesia, without the
elevation of a mucoperiosteal flap (Fig. 1a,b,
Data S1). A periotome and the appropriate
dental forceps were used to minimize surgical
trauma of the surrounding tissue. The thor-
ough curettage of all soft tissue debris in the
alveolus was performed during the extraction
at all extraction sites to ensure the removal of
all granulation tissue and stimulate bleeding
from the osseous base to promote healing. A
caliper (Dentaurum�; Dentaurum Dental
Technology, Ispringen, Germany) was subse-
quently used to measure the horizontal ridge
width (buccolingually) at the midpoint of the
alveolar crest using the mid-buccal and mid-
palatal marks on the cervical bone surface as
published before (Mardas et al. 2011, Vigno-
letti et al. 2012). After completion of the mea-
surements, the randomization envelope was
opened and the assigned treatment test Osse-
ous� (SIN) or control (Geistlich Biomaterials,
Wollhusen, Switzerland) was revealed to the
surgeon. The implant did not exceed the
height of the alveolar crest, and the site was
visually inspected to ensure that the biomate-
rial was saturated with blood (Fig. 1c). Pri-
mary wound closure was performed following
the elevation and rotation of the mucoperio-
steal flap (Fig. 1d,e). Postoperative antibiotic
therapy (500-mg Azithromycin) was adminis-
tered once a day for the first postoperative
week, and a disinfectant mouth rinse (0.12%
Chlorhexidine) was prescribed two times per
day, for the first two postoperative weeks.
Postoperative clinical evaluations of the
patients were performed at 1, 7, 30, and
Table 1. List of volunteer subjects investigated
Patient Gender Age ToothExperimentalgroups
1 Female 30 46* 12 Female 52 37* 23 Female 53 37* 24 Male 44 21‡ 15 Female 34 46* 26 Male 58 46‡ 17 Male 50 47‡ 28 Female 51 46* 29 Female 34 36* 110 Female 34 16* 111 Female 53 22† 112 Male 50 27‡ 213 Male 60 15† 214 Male 52 36‡ 215 Male 23 47* 216 Female 56 36† 117 Female 48 26* 118 Female 45 24† 119 Female 33 34† 220 Female 31 36† 1
*Extraction due to periodontal reason.†caries.‡tooth/root fracture.
Table 2. Inclusion and exclusion criteria
Inclusion criteria Exclusion criteria
Age between 30 and 60 yearsGood general healthPresence of a hopeless tooth requiringextraction
The extraction site would be suitable forreplacement by a dental implant
Volunteer subjects had voluntarily signedthe informed consent
Pregnancy or lactating periodSmokingChronic treatment with any medication knownto affect oral status and bone turnover
Contraindicate surgical treatmentSuffering from a known psychological disorder
2 | Clin. Oral Impl. Res. 0, 2013 / 1–6 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Calasans-Maia et al �Alveolar socket preservation with xenograft

90 days to determine the presence of compli-
cations, such as infection with inflammation,
wound dehiscence, or loss of graft material.
After 6 months, all sockets were evaluated
through clinical and radiographic examination
(Fig. 1f,g).
Surgical reentry
At 24 weeks after extraction, the implants
were placed. A mucoperiosteal flap was
raised, and the site of extraction was identi-
fied using a customized surgical splint. A
caliper was used to measure the horizontal
ridge width buccolingually. A core biopsy
with a depth of 6 mm was obtained from the
center of the extraction site. A trephine bur
(2 mm in diameter, SIN) was used to collect
the biopsy specimen (Fig. 2a), followed by
dental implant placement according to the
manufacturer’s surgical protocol. Try-On or
Strong implants (SIN) were used (Fig. 2b,c).
The mucoperiosteal flaps were closed with
interrupted sutures (Silk suture 4-0, Ethi-
con�). After 6 months, the implants were
successfully placed at all sites in the control
and test groups (Fig. 2d).
Histological evaluation
Bone biopsy specimens (6 9 2 mm) obtained
from the grafted and ungrafted sockets were
fixed in 10% formalin for 2 days and subse-
quently decalcified in bone decalcification
solution (Alkimia�; Allkimia, Campinas, Bra-
zil) for 48 h. After routine processing, the tis-
sues were embedded in paraffin, sectioned
longitudinally into multiple 4lm-thick sec-
tions and stained with Hematoxylin and
Eosin (H&E) and Masson’s trichrome stain.
The two most central sections were obtained
from each specimen. For the qualitative and
morphologic analysis of the remodeling pro-
cess, the stained preparations were examined
under a light microscope (Zeiss Axioplan) at a
minimum 209 magnification and the entire
section was evaluated. Ten digital images of
each section were acquired and used to trace
the areas identified as vital bone, biomaterial
particles, and connective tissue (CT)/other
non-bone components. Image analysis soft-
ware (Image ProPlus�, Release 7.0; MediaCy-
bernetics, Silver Spring, MD, USA) was used
to create individual layers of newly formed
bone, biomaterial particles, and CT/other non-
bone components, which were assessed by a
single observer blinded to the clinical data.
Statistical analysis
The results were expressed as the means �95%CI. The Mann–Whitney unpaired test were
performed, considering significant differences if
P < 0.05.
Results
Clinical findings
Clinical healing was uneventful and free of
infection or symptoms in all volunteers from
both groups. Age and gender did not signifi-
cantly affect the clinical outcomes of this
study.
Almost complete soft tissue closure was
observed at 10 days after extraction in both
test groups. After 6 months of healing, when
the bone specimen sample was obtained, both
groups exhibited the same bone density and
showed the same resistance on trephine appli-
cation. Bone core samples were retrieved, and
implants were placed in all sockets. The hori-
zontal ridge width (buccolingually) was mea-
sured at the midpoint of the alveolar crest
using the mid-buccal and mid-palatal marks
on the cervical bone crest before the tooth
extraction and after 6 months of socket heal-
ing, and the results are showed in Table 3.
Statically significant differences were not
observed between the groups.
(a) (b)
(c)
(d)
(e)
(f)
(g)
Fig. 1. (a, b) Clinical and radiographic aspects of the hopeless tooth; (c) socket filled with the osseus xenograft; (d)
The flap was advanced coronally for primary closure; (e) radiographic aspect of the immediate area post grafting; (f,
g) clinical and radiographic aspects at 6 months after grafting.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 3 | Clin. Oral Impl. Res. 0, 2013 / 1–6
Calasans-Maia et al �Alveolar socket preservation with xenograft

Histological observations
Test sites
One experienced blinded pathologist performed
the histological evaluation. Histological slides
were prepared, and the cores were examined at
209 and 409 magnification, revealing new
bone formation in all grafted sockets. The for-
mation of new well-mineralized vital trabecu-
lar bone was observed in all examined sections.
The new bone showed trabecular organization,
with collagen fibers arranged in a meshwork
pattern and osteocytes randomly distributed
(a)
(b)
(c)
(d)
Fig. 2. (a) Before implant installation a 2-mm specimen was removed using a trephine; (b, c) Clinical and
radiographic images of the installed implant; (d) Prosthetic rehabilitation.
Table 3. Clinical outcomes with respect towidth in millimeters (standard deviation inparentheses)
Tooth Group Baseline EndChange inwidth (mm)
46 1 11 10.6 0.437 2 10 9.5 0.537 2 9.5 9.1 0.421 1 8.0 7.8 0.246 2 11.2 10.9 0.346 1 12.1 11.6 0.547 2 12.3 12 0.346 2 11 10.4 0.636 1 11.5 11.1 0.416 1 11 10.8 0.222 1 7.0 6.8 0.227 2 12.0 11.7 0.315 2 6.5 6.3 0.236 2 11.5 11.2 0.347 2 12.4 12 0.436 1 11.8 11.6 0.226 1 12.1 12 0.124 1 9.0 8.8 0.234 2 7.0 6.4 0.636 1 11.9 11.4 0.5
(a) (b)
Fig. 3. (a, b) Photomicrographs of the interface between xenograft and the new formed bone, Stain HE, 109 and
409 augmentation.
(a)
(b)
(c)
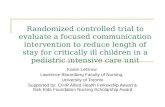
Fig. 4. Histomorphometric evaluation of the alveolar
sockets grafted with Bio-Oss� and Osseus�, consider-
ing the volume density of (a) newly-formed bone; (b)
connective tissue and (c) residual biomaterial particles.
Points in the plot represent all data, mean 95% of confi-
dence interval (bars).
4 | Clin. Oral Impl. Res. 0, 2013 / 1–6 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Calasans-Maia et al �Alveolar socket preservation with xenograft

within the trabeculae in large spindle-shaped
lacunae (Fig. 3a,b). Loose fibrous tissue with
thin vessels filled the trabecular spaces. Dense,
trabecular bone patterns were observed in both
test groups. The overall mean value of the
newly formed vital bone area fraction for TG1
was 33.6% (�7.1) and 19.3% (�22.5) for TG2.
For TG1, the mean value of the newly formed
CT was 32.3% (�8.8), and the mean value
of the remaining biomaterial was 10.6%
(�16.2). For TG2, the mean value of the CT
was 49.9% (�14.0), and the mean value of the
remaining biomaterial was 22.5% (�7.9)
(Fig. 4).
Discussion
The present randomized clinical trial com-
pared two bovine xenografts (Bio-Oss� and
Osseus�) for the preservation of the alveolar
ridge dimensions following tooth extraction.
The clinical, histological, and histomorpho-
metrical evaluations did not show significant
differences between the two materials. In the
present study, biopsy specimens were
obtained and dental implants were placed
after a 6-month healing period. A healing
period of 6 months was selected because this
time point was used in two previously
reported systematic reviews. The first sys-
tematic review showed 29–63% horizontal
bone loss and 11–22% vertical bone loss
after 6 months following tooth extraction
and demonstrated rapid reductions in the
first 3–6 months, followed by gradual reduc-
tions in the dimensions (Tan et al. 2012).
The second systematic review showed a
3.8 mm horizontal reduction in width and a
1.24 mm vertical reduction in height of the
alveolar ridge within 6 months after tooth
extraction (H€ammerle et al. 2012). These
studies demonstrated rapid reductions in the
first 3–6 months, followed by gradual reduc-
tions in the dimensions. A previous study
discussed so-called ridge preservation tech-
niques, which are categorized into two differ-
ent groups: techniques for maintaining the
ridge profile (ridge preservation) and tech-
niques for enlarging the ridge profile (ridge
augmentation). The reasons for ridge preser-
vation include the maintenance of the exist-
ing soft and hard tissue envelope,
maintenance of a stable ridge volume for
optimizing the functional and esthetic out-
comes, and the simplification of treatment
procedures subsequent to ridge preservation
(Vignoletti et al. 2012). Contraindications for
ridge preservation were considered in patients
irradiated in the area planned for ridge preser-
vation, patients taking biphosphonates and
when general contraindications against oral
surgical interventions and infections at the
site planned for ridge preservation were
observed, which could not be treated during
ridge preservation surgery (H€ammerle et al.
2012). The volunteer subjects included in the
present clinical trial did not present contrain-
dications for ridge preservation. In the pres-
ent study, mucoperiosteal flaps were raised
to preserve the ridge profile and facilitate
primary wound closure. The primary closure
of the wound is beneficial with respect to
the volume gained as a result of this
approach (H€ammerle et al. 2012). Cellular
differentiation, augmentation material break-
down, and bone replacement were evidenced
at the grafted sites, largely preserving the
dimensions of the alveolar ridge after
6 months of healing. In the present study, a
very small horizontal resorption of the bone
crest after the two types of treatments was
observed in both groups, confirming previous
clinical and preclinical reports that post-
extraction healing is always characterized by
osseous resorption and significant contour
changes especially in the horizontal plane of
the residual alveolar ridge (Schropp et al.
2003; Ara�ujo & Lindhe 2011). These changes
may be limited because our sample is mainly
composed by molars. A shorter 3-month
healing period should be evaluated in future
studies. A recent systematic review evalu-
ated bone healing after tooth extraction,
with or without an intervention, and the
histological evaluation revealed a large pro-
portion of residual graft material that might
account for some of the differences in the
alveolar ridge dimensions observed during
the follow-up exam (Morjaria et al. 2012).
Another recent systematic review evaluated
the effectiveness of bone preservation using
graft materials in non-molar alveolar regions
and suggested that the graft materials might
not prevent physiological resorptive bone
processes after tooth extraction, although
these materials might reduce changes in the
resulting bone dimensions (Ten Heggeler
et al. 2011).
Conclusions
The alterations in the dimension of the alve-
olar ridge following tooth extraction were
similar between the groups, affording a more
favorable implant position.
Acknowledgements: The authors
thank Sistema de Implantes Nacional, S~ao
Paulo, Brazil (SIN) for providing financial
support for this study. We also want to
express our thanks to Dr. Alfredo Schnetzler
Neto and Frederico, Prosthodontists, Rio de
Janeiro, Brazil for his significant
contributions to developing the
prosthodontic rehabilitation.
References
Accorsi-Mendonc�a, T., Zambuzzi, W.F., Bramante,
C.M., Cestari, T.M., Taga, R., Sader, M., Almeida
Soares, G.D. & Granjeiro, J.M. (2011) Biological
monitoring of a xenomaterial for grafting: an eval-
uation in critical-size calvarial defects. Journal of
Materials Science. Materials in Medicine 22:
9971004.
Ara�ujo, M.G., Linder, E., Wennstrom, J. & Lindhe,
J. (2008) The influence of Bio-Oss collagen on
healing of extraction socket: an experimen-
tal study in the dog. International Journal of
Periodontics & Restorative Dentistry 28: 123–
135.
Ara�ujo, M.G. & Lindhe, J. (2011) Socket grafting
with the use of autologous bone: an experimental
study in the dog. Clinical Oral Implants
Research 1: 9–13.
Brkovic, B.M.B., Prasad, H.S., Rohrer, M.D., Konan-
dreas, G., Agrogiannis, G., Antunovic, D. &
S�andor, G.K.B. (2012) Beta-tricalcium phosphate/
type I collagen cones with or without a barrier
membrane in human extraction socket healing:
clinical, histologic, histomorphometric, and
immunohistochemical evaluation. Clinical Oral
Investigations 16: 581–590.
Calasans-Maia, M.D., Ascoli, F.O., Novellino,
A.T.N.A., Rossi, A.M. & Granjeiro, J.M. (2009)
Comparative histological evaluation of tibial bone
repair in rabbits treated with xenografts. Acta
Ortopedica Brasileira 17: 340–343.
Fernandes, P.G., Novaes, A.B. Jr, de Queiroz, A.C.,
de Souza, S.L.S., Taba, M. Jr, Palioto, D.B. &
Grisi, M.F.M. (2011) Ridge preservation with
acellular dermal matrix and anorganic bone
matrix cell-binding peptide P-15 after tooth
extraction in humans. Journal of Periodontology
82: 72–79.
Festa, V.M., Addabbo, F., Laino, L., Femiano, F. &
Rullo, R. (2011) Porcine-derived xenograft com-
bined with a soft cortical membrane versus
extraction alone for implant site development: a
clinical study in humans. Clinical Implant Den-
tistry and Related Research doi: 10.1111/j.1708-
8208.2011.00398.x. [Epub ahead of print].
Gonshor, A., Saroff, S.A., Anderegg, C.R., Joachim,
F.P.C., Charon, J.A., Prasad, H. & Katta, S. (2011)
Histologic and clinical evaluation of a bioactive
calcium phosphosilicate bone graft material in
postextraction alveolar sockets. International
Journal of Oral Implantology and Clinical
Research 2: 79–84.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 5 | Clin. Oral Impl. Res. 0, 2013 / 1–6
Calasans-Maia et al �Alveolar socket preservation with xenograft

Granjeiro, J.M., Oliveira, R.C., Bustos-Valenzuela,
J.C., Sogayar, M.C. & Taga, R. (2005) Bone mor-
phogenetic proteins: from structure to clinical
use. Brazilian Journal of Medical and Biological
Research 38: 1463–1473.
H€ammerle, C.H.F., Ara�ujo, M.G. & Simion, M.
(2012) On behalf of the Osteology Consensus
Group 2011. Evidence-based knowledge on the
biology and treatment of extraction sockets. Clin-
ical Oral Implants Research 23: 80–82.
Heberer, S., Al-Chawaf, B., Jablonski, C., Nelson,
J.J., Lage, H. & Nelson, K. (2011) Healing of
ungrafted and grafted extraction sockets after
12 weeks: a prospective clinical study. The Inter-
national Journal of Oral & Maxillofacial
Implants 26: 385–392.
Jardelino-Lima, C, Takamori, E., Rossi, A.M. &
Granjeiro, J.M. (2008) Biocompatibility of bovine
anorganic xenograft. Key Engineering Materials 3:
396–398.
Kutkut, A., Andreana, S., Kim, H. & Monaco, E. Jr
(2012) Extraction socket preservation graft before
implant placement with calcium sulfate hemihy-
drate and platelet-rich plasma: a clinical and
histomorphometric study in humans. Journal of
Periodontology 83: 401–409.
Mardas, N., D’Aiuto, F., Mezzomo, L., Arzoumanidi,
M. & Donos, N. (2011) Radiographic alveolar bone
changes following ridge preservation with two dif-
ferent biomaterials. Clinical Oral Implants
Research 22: 416–423.
Morjaria, K.R., Wilson, R. & Palmer, R.M. (2012)
Bone healing after tooth extraction with or
without an intervention: a systematic review of
randomized controlled trials. Clinical Implant
Dentistry and Related Research doi: 10.1111/j.
1708-8208.2012.00450.x. [Epub ahead of print].
Munhoz, E.A., Ferreira Junior, O., Yaedu, R.Y. &
Granjeiro, J.M. (2006) Radiographic assessment of
impacted mandibular third molar sockets filled
with composite xenogenic bone graft. Dentomax-
illofacial Radiology 35: 371–375.
Pelegrine, A.A., da Costa, C.E.S., Correa, M.E.P.
& Marques, J.F.C. Jr (2010) Clinical and histo-
morphometric evaluation of extraction sockets
treated with an autologous bone marrow
graft. Clinical Oral Implants Research 21: 535–
542.
Ruga, E., Gallesio, C., Chiusa, L. & Boffano, P.
(2011) Clinical and histologic outcomes of cal-
cium sulfate in the treatment of postextraction
sockets. The Journal of Craniofacial Surgery 22:
494–498.
Schropp, L., Wenzel, A., Kostopoulos, L. & Karring,
T. (2003) Bone healing and soft tissue contour
changes following single tooth extraction: a clini-
cal and radiographic 12-month prospective study.
International Journal of Periodontics and Restor-
ative Dentistry 23: 313–323.
Schulz, K.F., Altman, D.G. & Moher, D. (2010)
Consort 2010 statement: updated guidelines for
reporting parallel group randomized trials. Obste-
trics and Gynecology 115: 1063–1070.
Sisti, A., Canullo, L., Mottola, M.P., Covani, U.,
Barone, A. & Botticelli, D. (2012) Clinical
evaluation of a ridge augmentation procedure for
the severely resorbed alveolar socket: multicen-
ter randomized controlled trial, preliminary
results. Clinical Oral Implants Research 23: 526–
535.
Spinato, S., Agnini, A., Chiesi, M., Agnini, A.M. &
Wang, H.L. (2012) Comparison between graft and
no-graft in an immediate placed and immediate
nonfunctional loaded implant. Implant Dentistry
21: 97–103.
Tan, W.L., Wong, T.L.T., Wong, M.C.M. & Lang,
N.P. (2012) A systematic review of post-extract-
ional alveolar hard and soft tissue dimensional
changes in humans. Clinical Oral Implants
Research 23: 1–21.
Ten Heggeler, J.M.A.G., Slot, D.E. & Van der Weij-
den, G.A. (2011) Effect of socket preservation
therapies following tooth extraction in non-molar
regions in humans: a systematic review. Clinical
Oral Implants Research 22: 779–788.
Van der Weijden, F., Dell’Acqua, F. & Slot, D.E.
(2009) Alveolar bone dimensional changes of
post-extraction sockets in humans: a systematic
review. Journal of Clinical Periodontology 36:
1048–1058.
Vignoletti, F., Matesanz, P., Rodrigo, D., Figuero,
E., Martin, C. & Sanz, M. (2012) Surgical proto-
cols for ridge preservation after tooth extraction.
A systematic review. Clinical Oral Implants
Research 23: 22–38.
Wenz, B., Oesch, B. & Horst, M. (2001) Analysis of
the risk of transmitting bovine spongiform
encephalopathy through bone grafts derived from
bovine bone. Biomaterials 22: 1599–1606.
Wood, R.A., Brian, L & Mealey, B.L. (2012) Histo-
logic comparison of healing after tooth extraction
with ridge preservation using mineralized versus
demineralized freeze-dried bone allograft. Journal
of Periodontology 83: 329–336.
Zambuzzi, W.F., Oliveira, R.C., Subitoni, B.L.,
Menezes, R., Taga, R. & Granjeiro, J.M. (2012)
Biological monitoring of a promissory xenogenic
pin for biomedical applications: a preliminary
intraosseous study in rats. Clinical Oral Implants
Research 23: 367–372.
Supporting Information
Additional Supporting Information may be
found in the online version of this article:
Data S1. CONSORT statement 2001 check-
list.
6 | Clin. Oral Impl. Res. 0, 2013 / 1–6 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Calasans-Maia et al �Alveolar socket preservation with xenograft

REVIEW
Alveolar ridge preservation. A systematic review
Attila Horváth & Nikos Mardas & Luis André Mezzomo &
Ian G. Needleman & Nikos Donos
Received: 31 December 2011 /Accepted: 14 May 2012 /Published online: 20 July 2012# Springer-Verlag 2012
AbstractObjective The objective of this paper is to examine theeffect of alveolar ridge preservation (ARP) compared tounassisted socket healing.Methods Systematic review with electronic and hand searchwas performed. Randomised controlled trials (RCT), controlledclinical trials (CCT) and prospective cohort studies wereeligible.Results Eight RCTs and six CCTs were identified. Clinicalheterogeneity did not allow for meta-analysis. Average changein clinical alveolar ridge (AR) width varied between −1.0and −3.5±2.7 mm in ARP groups and between −2.5and −4.6±0.3 mm in the controls, resulting in statisticallysignificantly smaller reduction in the ARP groups in five outof seven studies. Mean change in clinical AR height variedbetween +1.3±2.0 and −0.7±1.4 mm in the ARP groups andbetween −0.8±1.6 and −3.6±1.5 mm in the controls. Heightreduction in the ARP groups was statistically significantly less
in six out of eight studies. Histological analysis indicatedvarious degrees of new bone formation in both groups. Somegraft interfered with the healing. Two out of eight studiesreported statistically significantly more trabecular bone for-mation in the ARP group. No superiority of one technique forARP could be identified; however, in certain cases guidedbone regeneration was most effective. Statistically, signifi-cantly less augmentation at implant placement was neededin the ARP group in three out of four studies. The strength ofevidence was moderate to low.Conclusions Post-extraction resorption of the AR might belimited, but cannot be eliminated by ARP, which at histolog-ical level does not always promote new bone formation. RCTswith unassisted socket healing and implant placement in theARP studies are needed to support clinical decision making.Clinical relevance This systematic review reports not only onthe clinical and radiographic outcomes, but also evaluates thehistological appearance of the socket, along with site specificfactors, patient-reported outcomes, feasibility of implantplacement and strength of evidence, which will facilitate thedecision making process in the clinical practice.
Keywords Tooth extraction . Bone resorption . Implant sitedevelopment . Bone substitute . Bone regeneration .
Human histology
Introduction
Periodontal disease, periapical pathology and mechanical trau-ma often result in bone loss prior to tooth removal [1]. Further-more, traumatic extraction has also been associated withadditional loss of bone. In the healing phase after extraction,alveolar bone undergoes additional atrophy as a result of thenatural remodelling process [2–7]. This begins immediately
A. Horváth :N. Mardas : L. A. Mezzomo : I. G. Needleman :N. Donos (*)Unit of Periodontology, Department of Clinical Research,UCL Eastman Dental Institute,256 Gray’s Inn Road,London WC1X 8LD, UKe-mail: [email protected]
A. HorváthDepartment of Periodontology, Semmelweis University,Budapest, Hungary
L. A. MezzomoPontifical Catholic University of Rio Grande do Sul,Porto Alegre, Brazil
I. G. NeedlemanInternational Centre for Evidence-Based Oral Health,UCL Eastman Dental Institute,London, UK
Clin Oral Invest (2013) 17:341–363DOI 10.1007/s00784-012-0758-5

after extraction and may result in up to 50 % resorption of thealveolar ridge (AR) width even in 3 months [1]. Post-extractionAR resorption may have an impact on dental implant place-ment, since sufficient vertical and horizontal volume of alveolarbone should ideally be present at the site of insertion [8].
Alveolar ridge preservation (ARP) procedures have beenintroduced to maintain an acceptable ridge contour in areasof aesthetic concern, as well as to prevent alveolar ridgeatrophy and maintain adequate dimensions of bone in orderto facilitate implant placement in prosthetically driven posi-tions [9, 10]. Several methods have already been investigat-ed for ARP in preclinical models [11–14] and clinicalstudies, such as socket grafting with autogenous bone[15], demineralised freeze-dried bone allograft (DFDBA)[15–17], xenografts, like deproteinized bovine-bonemineral (DBBM) [18], alloplasts [19] and bone morpho-genic proteins (BMP) [20]. Guided bone regeneration(GBR) with or without bone grafts has also been evaluated[9, 10, 21–25].
Although some of the above bone substitutes wereable to limit the resorption of post-extraction alveolarridge up to a certain extent, the quality of the newtissue in the socket varied broadly. The remnants ofthe grafts often interfered with the normal healing pro-cess in line with preclinical results [15–17, 26]. Anumber of review articles on ARP have been publishedin the last decade [27–32]. However, a systematic as-sessment of the nature and quality of the newly formedtissue alongside methodological quality and risk of biasof the studies has not been carried out. Furthermore,non-controlled prospective and retrospective studies aswell as case series were also included in most of theprevious reviews without the comparison to the controlgroup of unassisted socket healing [33–36].
Therefore, the objective of the present systematic reviewwas to investigate the effect of ridge preservation on theresidual alveolar ridge dimensions and on histological char-acteristics, compared to unassisted socket healing.
Methods
Prior to commencement of the study, a detailed protocol wasdeveloped and agreed upon by the authors based on theCochrane Collaboration guidelines and previous reviewspublished by our group [37–41].
Focused question
Following tooth/root extraction in humans, what is the effectof ridge preservation on the residual alveolar ridge dimensionand on histological characteristics, compared to unassistedsocket healing?
Definition
Whilst ‘socket preservation’ has widely been employed todepict a certain procedure, we believe that the objective ofthese interventions is to preserve the dimension of the AR.Therefore, we have used the term ‘Alveolar Ridge Preser-vation’ to define such procedures.
Types of studies
Longitudinal prospective studies were included, i.e. RCTs,CCTs and cohort studies with control group.
Populations of studies
Healthy individuals, without any age limit, who underwentany type of ridge preservation following permanent toothextraction, were included. Smokers and patients with historyof periodontal disease were not excluded. The minimumnumber of subjects per group was five. However, no limitwas set for study follow-up period.
Types of interventions
Test groups
Studies reporting on any of the following types of interven-tions were included: socket grafting (autograft, allograft,xenograft, alloplastic materials); socket sealing (soft tissuegrafts); GBR (resorbable/non-resorbable barriers); biologicalactive materials (growth factors) and combinations of theabove techniques/materials.
Control groups
The control groups of the included studies comprised emptysockets, i.e. unassisted socket healing.
Outcome variables
The primary outcomewas the change in oro-facial (horizontal)and apico-coronal (vertical) AR dimensions. Secondary out-comeswere the following: (1) change in buccal plate thickness;(2) bone volume alteration following extraction; (3) complica-tions; (4) histological healing characteristics; (5) site eligibilityfor placement of an adequate size dental implant with orwithout further augmentation; (6) patient-reported outcomes,such as quality of life and (7) health economics.
Risk of bias and methodological quality assessment
In order to evaluate the methodological quality and risk ofbias of individual studies, we used a combination of
342 Clin Oral Invest (2013) 17:341–363

parameters from the Cochrane Collaboration and Consoli-dated Standards of Reporting Trials (CONSORT) statement.The following parameters were assessed and taken intoconsideration in the final analysis: sample size calculation,statement of eligibility criteria, ethics approval, informedconsent, baseline homogeneity, randomisation method, allo-cation concealment, masking, calibration, follow up, protocolviolation, method of statistics, unit of analysis, CONSORTimplementation, International Standard Randomised Con-trolled Trial Number Register (ISRCTN) and funding disclo-sure. Methodology unique to RCTs was not assessed in CCTs,i.e. randomisation and concealment of allocation.
Randomisation was accepted as adequate, in case theallocation sequence was correctly generated either bycomputer, toss of a coin, throwing dice, etc. Quasirandomisation, e.g. birth dates, hospital numbers werenot accepted. Adequacy of allocation concealment wasaccepted if the sequence was concealed, until interven-tion was assigned (e.g. in sequentially numbered andsealed opaque envelopes, remote computer or centraltelephone). Statistical analysis was judged as adequateif appropriate statistical method was selected to accom-modate to the characteristic of the each individual data(e.g. number of groups and investigated categories, sizeof samples, normally distributed or skewed data, para-metric or non-parametric, paired or unpaired, numericalor categorical variables). Statistical significance was ac-cepted in case of confidence interval (CI) >95 % (p<0.05), while ‘statistically highly significant’ referred toCI>99.9 % (p<0.001).
Based on the above, we attempted to categorize thepossible risk of bias as low, moderate or high. Low riskreferred to studies with adequate randomisation method,sequence concealment and masking of examiner. Studieswere classified as moderate, if one of the above keycategories were missing, or high risk of bias, if morethan one were lacking.
Inclusion criteria
1. All prospective longitudinal studies (i.e. RCTs, CCTsand cohort studies) were included, where one of theabove mentioned types of interventions were carriedout in the test group, whereas unassisted socket healingserved as control.
2. Studies on healthy individuals, without any age limit,who underwent ARP following tooth extraction, wereincluded.
3. Studies had to report on minimum of five patients pergroup.
4. Studies, performing clinical or three-dimensional (3D)radiographic evaluation of hard tissue or histologicalassessment, were included.
Exclusion criteria
1. Case reports, case series, retrospective analyses wereexcluded.
2. Studies without a control group comprising unassistedsocket healing were excluded.
3. Studies on medically compromised patients, e.g. uncon-trolled diabetes mellitus or cancer were excluded.
4. Studies reporting on immediate placement of dentalimplant were excluded.
5. Studies describing extraction of third molars wereexcluded.
Search strategy
A sensitive search strategy was designed as we anticipatedthat relevant studies might be difficult to locate. The searchstrategy incorporated both electronic and hand searches. Thefollowing electronic databases were utilised in Apr 2010: (1)MEDLINE In-Process & Other Non-Indexed Citationsand MEDLINE 1950 to present via Ovid interface; (2)EMBASE Classic + EMBASE 1947 to present via Ovidinterface; (3) The Cochrane Central Register of ControlledTrials (CENTRAL); (4) LILACS.
The electronic search strategy used the following combi-nation of key words and MeSH terms: (“tooth extraction”OR “tooth removal” OR “socket” OR “alveol$” OR “ridge”OR “crest” OR “tooth socket” OR “alveolar bone loss” OR“bone resorption” OR “bone remodeling”) AND (“preserv$” OR “reconstruct$” OR “augment$” OR “fill$” OR “seal$” OR “graft$” OR “repair$” OR “alveolar ridge augmen-tation” OR “bone regeneration” OR “bone substitutes” OR“transplantation”).
Cochrane search filters for RCTs and CCTs were imple-mented. In addition, cohort trials were also searched. Theresults were limited to humans only.
An extensive hand search was also performed encom-passing the bibliographies of the included papers and reviewarticles. Furthermore the following journals were screenedfrom 2001 to April 2010: Clinical Oral Implants Research,Clinical Implant Dentistry and Related Research, EuropeanJournal of Oral Implantology, Implant Dentistry, Interna-tional Journal of Oral and Maxillofacial Implants, Interna-tional Journal of Periodontics and Restorative Dentistry,Journal of Clinical Periodontology, Journal of Dental Re-search, Journal of Oral and Maxillofacial Surgery, Journalof Periodontology, Oral Surgery, Oral Medicine, Oral Ra-diology, Oral Pathology and Endodontics, Periodontology2000. No language restrictions were applied. Translationswere carried out as necessary by two reviewers (AH, LAM).
The extracted data were copied into Reference Manager10 software (Thomson Reuters, New York, NY, USA). Thusthe further steps of screening were performed on this
Clin Oral Invest (2013) 17:341–363 343

interface. A three-stage selection of the resulted hits wasperformed independently and in duplicate by two reviewers(AH and LAM). In order to reduce errors and bias, a cali-bration exercise was performed with the first 500 titles,resulting in 96.4 % agreement. In case of disagreement atthe title selection stage, the trial was included in the abstractstage. At the abstract and full text selection any disagree-ments between the above reviewers were resolved by dis-cussion. If unresolved, a third reviewer (NM) was involvedfor arbitration. The reasons for exclusion were recordedeither in the Reference Manager (abstract stage) or in aspecific data extraction form (full text stage). The level ofagreement was determined by Kappa score calculation.
Research synthesis
Studies were grouped by research design and their chiefcharacteristics. Outcomes were recorded in evidence tables.In view of the marked heterogeneity, no meta-analysis wasconducted. Instead, a narrative synthesis was undertaken.
Results
Search sequence
The electronic search yielded 6,216 relevant hits after re-moval of duplicates (Fig. 1). Subsequently, 157 titles wereselected for the abstract stage. Following investigation ofthe abstracts, 42 articles qualified for full text evaluation.Four extra papers were then added as a result of the handsearch. Assessment of these articles resulted in the following
14 publications eligible for the review [17, 19–21, 23–25,42–48]. The excluded full text papers along with the reasonsfor exclusion are listed in Table 1. The most typical reasonsfor exclusion were lack of control group with unassistedsocket healing; use of retrospective design; assessment ofdimensional changes of the AR only on periapical two-dimensional radiographs, or on casts taken from soft tissuelevel; and surgical removal of third molars.
The Kappa score for agreement between the reviewers (AH,LAM) at the abstract and full text selection level, was 0.96 and0.90, respectively, indicating a high level of agreement.
Study characteristics
In the 14 included articles (eight RCTs and six CCTs) theefficacy of ARP techniques was evaluated clinically bymeans of direct measurements of the residual alveolar ridgedimensions during re-entry procedures, radiographically bymeans of computer tomography or histologically from tre-phine biopsies taken at re-entry during osteotomies forimplant placement (Tables 3 and 4). No cohort studies wereindentified. Limited data were reported on confoundingfactors, such as periodontitis, smoking, systemic diseaseand medication. The extraction site distribution was fairlyheterogeneous. In some studies ARP was performed only inmaxillary anterior sockets [42, 46, 47], whereas such restric-tion was not employed in other studies. The residual bonevolume around the investigated sockets, e.g. the presence/absence and width of the buccal bone plate varied fromseverely compromised [20, 46], to completely intact, buccalbone (Table 3) [17, 21, 42].
Intervention characteristics
With regard to the techniques or materials used for ARP, theincluded studies were grouped into three categories (Table 3);
1. Bone grafts/substitutes2. GBR3. Biological active materials.
In the majority of the included studies, various bonegrafts were utilised, such as autologous bone marrow [47],plasma rich in growth factor (PRGF) with or without autol-ogous bone [43], DFDBA [17], DBBM [46], calcium sul-phate hemihydrates [42, 45] and bioactive glass [17].Alloplastic polyglycolide/polylactide (PGPL) sponge wasalso employed [19, 48]. GBR technique was applied usingnon-resorbable expanded polytetrafluoroethylene (e-PTFE)[24] or resorbable (PGPL) [25] barrier. Resorbable collagenmembrane was also employed in combination with FDBA[23] or corticocancellous porcine bone [21]. Biological ac-tive material, namely bone morphogenic protein (rhBMP-2)was used on a collagen sponge carrier in one study [20].
Electronic search6.216 titles
Included publications14
Relevantabstracts
Full-text analysis 45
Relevant full-texts42
6,059 Excluded based
on the title
115Excluded based on the abstract
32Excluded based on the full-text
3 Included as a result of hand search
Kappa score 0.96
Kappa score 0.90
1 Included as a result of final search
Fig. 1 Flow chart of the screening process
344 Clin Oral Invest (2013) 17:341–363

Table 1 List of excluded full text papers and reasons for exclusion
First author(year of publication)
Journal Reasons for exclusion
Bianchi (2004) Int J Periodont Rest Dent Retrospective analysis
Single-arm of the included Fiorellini et al. (2005)
Bolouri (2001) Comp Cont Educ Dent Reported on optical density on two-dimensional radiographs
Brawn (2007) Impl Dent Case report
Brkovic (2008) J Can Dent Assoc Case report
Carmagnola (2003) Clin Oral Impl Res Lack of real control group, resembles to a retrospective analysis(extreme difference in follow-up period between tests and controls.T1: 4 months; T2: 7 months; C: 1-15 years, mean: 7.8 years)
Cranin (1988) J Biomed Mat Res Case series without control group
De Coster (2009) Clin Impl Dent Relat Res Case series
Retrospective study as stated by the authors in the discussion
Healing period varied between 1.5 months and 1.5 years
Neither histomorphometry nor clinical or radiographic measurementsreported in the results
Graziani (2008) J Cranofac Surg Extraction of fully impacted third molars
Linear measurements on OPG
Gulaldi (1998) Oral Surg Oral MedOral Pat Oral Rad End
Extraction of fully impacted third molars
Linear measurements on OPG and scintigraphy
Primary outcome was to analyze bone metabolism
Heberer (2008) Clin Oral Impl Res Case series without control group
Hoad-Reddick (1994) Eur J Prosth Rest Dent Two-dimensional linear measurements obtained from OPG and cephalometry
Lack of defined landmarks
Surgical procedure was not described
Hoad-Reddick (1999) Eur J Prosth Rest Dent Description of a method for measurements on casts
Neither socket preservation procedure nor the results were described.Soft tissue punch technique only
Howell (1997) Int J Periodont Rest Dent Case series without control group
Jung (2004) Int J Periodont Rest Dent Case series without control group
Primary outcome was soft tissue healing
Kangvonkit (1986) Int J Oral Maxillofac Surg Based on OPG and lateral cephalogram only
Evaluation method remains unclear
Primary outcome was the biocompatibility of HA cones
Karapataki (2000) J Clin Periodontol Extraction of fully impacted third molars
Primary outcome was to assess the periodontal status ofsecond molars after extraction of third molars
Kerr (2008) J Periodontol No biomaterials were used to preserve the ridge dimensions,therefore did not address the focused question
Kwon (1986) J Oral Maxillofac Surg Based on OPG and lateral cephalogram only
Evaluation method remains unclear
Lack of description of the measurement methods
Molly (2008) J Periodontol Control group was covered by an e-PTFE membrane,thus lack of unassisted control sockets
Munhoz (2006) Dento Maxillofac Radiol Extraction of fully impacted third molars
Two-dimensional evaluation of periapical radiographs
Norton (2002) Int J Oral Maxillofac Impl Case series without control group
Resembles to a retrospective design(healing period ranged from 3 to 11 months)
Page (1987) J Oral Maxillofac Surg Case report
Pape (1988) Deutsche ZahnarztlicheZeitschrift
Augmentation of a resorbed ridge
Clin Oral Invest (2013) 17:341–363 345

None of the included studies used the socket sealing tech-nique. Primary flap closure was achieved in 9 out of 14studies, while the sockets left uncovered in the rests. Varioustypes and amounts of antibiotics and antiseptic rinses wereadministered for different duration in studies reporting onpostoperative care. Finally, average healing period rangedfrom one to nine months.
Outcome characteristics
Clinical outcomes
Eight out of the 14 included studies investigated the efficacyof various ARP techniques to preserve the pre-extractionridge dimensions using intra-surgical hard tissue measure-ments taken during re-entry procedure [19, 21, 23–25, 42,44, 47]. In these studies, ARP was performed in 137 socketsof 119 patients and compared to 120 sockets that left to healwithout any treatment in a total of 92 patients (Table 3).
Bone ‘graft’ Four studies evaluated changes in AR dimen-sions following grafting of the socket. Two studies were RCTs[42, 47] and two were CCTs [19, 44]. Healing time variedfrom 3 to 6 months [19, 42, 44, 47].
The horizontal (bucco-lingual) changes of the alveo-lar ridge were assessed in three studies [42, 44, 47].The AR reduced in width from baseline to re-entrybetween −1.0 mm and −3.5±2.7 mm following ARP(p<0.05) and between −2.5 mm and −3.2±1.8 mm in
the control groups (p<0.05). In two out of the three studies,the width reduction was statistically significantly smaller inthe test groups compared to the controls [42, 47].
Four studies investigated the mean change in ridge heightat the mid-buccal aspect [19, 42, 44, 47]. The AR heightchanged from baseline to re-entry between +1.3±1.9 mmand −0.5±1.1 mm following ARP, and between −0.8±1.6 mm and −1.2±0.6 mm in the control groups. The heightreduction between baseline and re-entry was not statisticallysignificant in one study in both test and control groups [44],while one study reported an increase in height instead ofloss following ARP with a PGPL sponge (p<0.05) [19]. Intwo out of the four studies, the height reduction was statis-tically significantly smaller in the test groups compared tothe controls [42, 47].
The vertical dimension changes at the mesial and distalaspects of the socket were measured in two studies [19, 42]and did not present any statistically significant difference forboth groups.
Three studies captured data on socket fill and reportedstatistically significant differences between baseline and re-entry in both groups [42, 44, 47], but only one reportedstatistically significantly higher socket fill, where bioactiveglass was covered by calcium sulphate, compared to theunassisted healing [44].
GBR Four studies evaluated changes in AR dimensionsfollowing ARP with GBR alone [24, 25], or in combinationwith bone graft [21, 23]. Three studies were RCTs [21, 23,
Table 1 (continued)
First author(year of publication)
Journal Reasons for exclusion
Case series without control group
Penteado (2005) Braz J Oral Sci Immunohistochemical analysis
Did not address the focused question
Quinn (1985) J Am Dent Assoc Clinical measurements at soft tissue level only based on tattoo points,thus failed to address the focused question
Resembles to a retrospective analysis
Schepers (1993) Impl Dent Retrospective case series without control group
Simon (2004) Ind J Dent Res Extraction of fully impacted third molars
Evaluated soft tissue healing and radiographic analysis basedon the two-dimensional periapical radiographs
Simion (1994) Int J Periodont Rest Dent Titanium implants placed simultaneously
No control group
Primary outcome was microbiological analysis
Smukler (1999) Int J Oral Maxillofac Impl Healed edentulous ridge as control instead of empty socket
No compatibility of the follow-up periods of the different groups
Svrtecky (2003) J Prosth Dent Case report
Throndson (2002) Oral Surg Oral MedOral Pat Oral Rad End
Extraction of fully impacted third molars
Measurements based on two-dimensional periapical radiographs
Yilmaz (1998) J Clin Periodontol Measurement at soft tissue level on study casts
346 Clin Oral Invest (2013) 17:341–363

25] and one was CCT [24]. Healing time varied between 4and 9 months.
Horizontal (bucco-lingual) changes of the AR wereassessed in all four studies. AR width reduction from base-line to re-entry varied between −1.2±0.9 mm and −2.5±1.2 mm in the GBR-treated sockets and between −2.6±2.3 mm and −4.6±0.3 mm in the control groups. With theexception of one study [23], a statistically significantlysmaller reduction of the alveolar ridge width was observedwhen e-PTFE [24], PGPL [25], or collagen membranes incombination with xenograft [21] were used.
All the four studies investigated the mean change in ARheight at the mid-buccal aspect. The AR height changedfrom baseline to re-entry between +1.3±2.0 mm and −0.7±1.4 mm in the ARP groups and between −0.9±1.6 mmand −3.6±1.5 mm in the control groups. The resorption inthe ARP group was not statistically significant in three outof four studies [23–25]. All studies reported a statisticallysignificantly less post-extraction reduction in AR heightwhen the socket was treated by GBR compared to unassistedhealing.
Vertical dimension changes at mesial and distal aspectsof the socket were measured in two studies [21, 23]. Theobserved differences between baseline and re-entry were notstatistically significant in both groups. In one out of the twostudies the height reduction was statistically significantlysmaller in the test group compared to the control [23].
Two studies captured data on the socket fill [24, 25] andreported statistically significant socket fill in both groupsbetween baseline and re-entry, as well as between tests andcontrols.
No data were found on either initial buccal plate thick-ness or alteration of bone volume. However, one studymeasured the buccal bone thickness loss and reported sta-tistically significantly less reduction in the ARP group [47].
Radiographic measurements
Two RCTs, reporting on 3D radiographic assessment, metthe inclusion criteria [20, 46]. The healing time varied from1 to 4 months. In one study, where the post-extraction socketwas grafted with a radiopaque material (DBBM), treatmentresulted in significantly less reduction in radiographic ARheight compared to unassisted socket healing [46]. The testgroup in the other study, where the higher concentration(1.5 mg/ml) of RhBMP-2 was utilised [20], resulted in amean increase of the radiographic AR width by 3.27±2.53 mm at the most coronal part, compared to the 0.57±2.56 mm increase in the group of unassisted healing. ARheight was reduced by 0.02±1.2 mm in the same test groupand by 1.17±1.23 mm in the control group (Table 3). Thedifferences between test and control were statisticallysignificant.
Histological results
Eleven studies carried out a histological analysis based ontrephine biopsies retrieved at re-entry [17, 19–21, 23, 42,43, 45–48]. Seven studies were RCTs [17, 20, 21, 23, 46,47] and four were CCTs [19, 43, 45, 48]. In these studies,ARP was performed in 181 sockets of 158 patients andcompared to 149 sockets that left to heal without anytreatment in 131 patients (Table 4). Only two out ofeight studies reported statistically significantly higher tra-becular bone volume following ARP in comparison to unas-sisted socket healing [21, 42] and two studies reportedstatistically significantly more connective tissue in the post-extraction socket when no ARP was performed [17, 21]. Onthe contrary, one study reported more vital bone in theunassisted socket healing group compared to the ARPgroup [23]. None of the differences of the investigatedhistomorphometric parameters reached statistical signifi-cance in other studies.
Bone ‘grafts’ Eight studies evaluated histologically thehealing of post-extraction sockets following the applicationof some type of bone grafts/substitutes [17, 19, 42, 43,45–48]. Four studies were RCTs [17, 42, 46, 47] and fourwere CCTs [19, 43, 45, 48]. New mineralised bone wasobserved at various levels in all studies in both ARP andcontrol groups in a healing period from 2.5 to 8 months.Connective tissue occupied a portion of the socket in bothgroups. When DFDBA, bioactive glass or DBBM wereused, the graft particles were embedded either in new boneor in connective tissue. In most studies, there was no sig-nificant difference in the type of healing, or amount of boneformation between bone grafts and unassisted sockethealing.
GBR in combination with graft GBR in combination withgraft was utilised in two RCTs. ARP with a collagen mem-brane and deproteinized porcine bone resulted in statisticallysignificantly higher new bone and lower connective tissueformation after 7 to 9 months of healing in comparison tounassisted socket healing [21]. However, residual graftmaterials were present in the ARP biopsies. FDBA andcollagen membrane resulted in similar amounts of new boneformation to untreated sockets, although more vital bonewas observed in the untreated sockets at 4 to 6 months ofhealing (p>0.05) [23].
Biological active material RhBMP-2 in a collagen spongecarrier was completely resorbed at 4 months following ARPregardless of the concentration of the growth factor [20].Mineralised tissue was found and trabecular bone formationwas noticed in two third of both the test and control biopsiesin the RCT.
Clin Oral Invest (2013) 17:341–363 347

Adverse events, complications
Adverse events were reported in six RCTs [17, 20, 21, 25,42, 47] and four CCTs [19, 24, 44, 48] including oedema,pain, erythema and membrane exposure/infection. In twostudies, more adverse events, i.e. oedema, erythema [20] ormembrane exposure [24] were observed in the ARP groupcompared to the natural socket healing. No comparisonbetween tests and controls were reported in the other studies(Table 3).
Feasibility of implant placement
Seven studies [17, 19, 23, 42, 45, 46, 48] reported thatimplant placement in the previous sockets were successful,but no differences between the ARP and untreated sites wererevealed. The outcome of implant placement remained un-clear in one article [43] and only re-entry without implanta-tion was performed in three trials [24, 44]. Four studiesreported the need of further augmentation at the stage ofimplant placement. Three of them favoured the ARP groupover the controls, since less [20] or no sites [21, 47] in theARP group presented with residual dehiscence or fenestra-tion defects around the inserted implants (Table 3).
Patient-reported outcome and health economics
No data were found for patient-reported outcome measuresor health economic evaluation.
Quality assessment
Considerable heterogeneity was found among the studies interms of methodological quality. Detailed description of thequality assessment of the included studies is presented inTable 2. Among the 14 included controlled studies, eightwere randomised [17, 20, 21, 23, 25, 42, 46, 47] although infour of them the randomisation technique was not reported[20, 42, 46, 47]. None of the RCTs reported the method ofallocation concealment. Masking of the examiner wasreported at the clinical level in two out of eight [23, 25], atradiological level in one out of two [20] and at histologicallevel in four out of 11 studies [17, 21, 42, 43]. Examinercalibration was declared in three papers [20, 23, 42], whilstinclusion and exclusion criteria were defined in seven pub-lications [17, 21, 23, 42, 43, 46, 47]. Apart from threestudies [21, 43, 46] all the other reported the approval ofthe ethical committee. Three studies were funded by indus-try [17, 20, 44], two studies by academic institution [45, 48]and the remaining nine did not report the source of funding.
Nine trials implemented patient-based analysis [20, 21,23–25, 42, 44, 47, 48], whilst the extraction site served asunit of analysis in the rest of the five investigations [17, 19,
43, 45, 46]. Sample size calculations were reported only inthree studies [20, 23, 42], although with insufficient data toevaluate the validity of the calculations. Statistical analysiswas appropriately carried out and described in one studyonly [47]. Appropriate statistics were either not carried out[17, 19–21, 43, 45, 46], or the reported data were insuffi-cient to determine the validity [23–25, 42, 43, 48]. In addi-tion, no RCTs were either registered with ISRCTN orreported using the CONSORT guidelines (Table 3).
Risk of bias
Four studies were classified as moderate risk of bias [17, 21,23, 25] and the rest were categorised as high risk of bias(Table 2).
Discussion
Key findings
This systematic review has demonstrated that different ARPtechniques do not totally eliminate post-extraction alveolarridge resorption or predictably promote new bone forma-tion. However, the reduction in ridge width and heightfollowing ARP may be less than that which occurs follow-ing natural socket healing. The clinical data suggest that thehorizontal ridge contraction was most successfully limitedin the two studies applying GBR without additional bonegrafts [24, 25], whereas the vertical shrinkage was mostefficiently limited by employing GBR with additional bonegraft [21, 23].
Strengths of the review
The present systematic review was limited to randomisedcontrolled trials, controlled clinical trials and prospectivecohort studies with a control group of empty untreatedsockets. Furthermore, the inclusion criteria of our systematicreview were based on the fact that the clinical merit ofapplying the different ARP techniques could only be vali-dated, if the clinical and histological outcomes following theapplication of a technique are superior to that of unassistedsocket healing.
In comparison to the previous systematic reviews [28,32] the present review has evaluated the histological char-acteristics of the alveolar socket healing with or withoutARP. The amount and the quality of the newly formedosseous tissues in the socket area are essential, especiallywhen the justification of ARP is to facilitate the placementof a dental implant in the position of a previously extractedtooth. It is doubtful, whether an ARP technique should beclaimed successful, if it only preserves the external contour
348 Clin Oral Invest (2013) 17:341–363

Tab
le2
Qualityassessmentof
theinclud
edstud
ies
Study
QualityCriteria
Estim
ated
risk
ofbias
Firstauthor
Randomisation
Masking
Calibratio
nElig
ibility
Criteria
Follow
upEthical
considerations
Funding
Statistical
analysis
Miscellaneous
Yearof
publication
1.Randomised
1.Therapist
1.Intra-exam
iner
1.Inclusion
criteriadefined
1.Percentage
ofcompleted
follo
wups
1.Ethicsapproval
Sourceof
Funding
1.Appropriate
samplesize
calculationandpower
1.Com
parable
experimentalgroups
2.CONSORT
implem
ented
2.Inform
edconsent
3.ISRCTN
registered
2.Unitof
analysis
4.Other
comments
3.Appropriate
statisticsapplied
2.Exclusion
criteriadefined
2.Adequate
correctio
n
2.Patient
2.Inter-exam
iner
2.Adequate
sequence
generatio
n3.
Examiner
Type
4.Statistician
3.Allo
catio
nconcealm
ent
Reference
number
4.Concealment
adequate
Aim
etti
1.Yes
1.N/R
1.Yes
(histo),
N/R
(clin
)1.
Yes
1.N/R
1.Yes
N/R
1.Insufficient
data
todeterm
ine
1.Yes
High
2.N/R
2009
2.N/R
2.N/R
2.N/A
2.Yes
2.N/A
2.Yes
2.Patient
3.N/R
3.Insufficient
data
todeterm
ine
RCT
3.N/R
3.Yes
(histo),
N/R
(clin
).#42
4.N/A
4.N/R
*Reportedas
‘doubleblind’
Anitua
1.Yes
(btw
T-C)
No(w
ithin
T)
1.N/R
1.N/R
1.Yes
1.100%
1.N/R
N/R
1.N/R
1.N/R
High
1999
2.N/A
2.N/R
2.N/A
2.Yes
2.Yes
2.Yes
2.Patient
+site
2.N/R
CCT
3.N/R
3.Yes
3.Nostatistical
analysis
was
carriedout
3.N/R
#43
4.N/A
4.N/R
4.Atsevere
defects
autogenous
bone
was
addedto
PRGF.
Different
healingperiods.
Barone
1.Yes
1.N/R
1.N/R
1.Yes
1.100%
1.N/R
N/R,declared
noconflict
ofinterest
1.N/R
1.Yes
Moderate
2008
2.Yes
2.N/R
2.N/A
2.Yes
2.Yes
2.Yes
2.Patient
2.N/R
RCT
3.N/R
3.Yes
(histo),
N/R
(clin
)3.
No
3.N/R
#21
4.N/A
4.N/R
4.Different
healing
periods.
Cam
argo
N/A
1.N/R
1.N/R
1.Yes
1.100%
1.Yes
Industry
1.N/R
1.N/R
High
2000
2.N/R
2.N/A
2.Yes
2.Yes
2.Yes
2.Patient
2.N/R
CCT
3.N/R
3.Insufficient
data
todeterm
ine
3.N/R
#44
4.N/R
Fiorellini
1.Yes
1.N/R
1.N/R
1.No
1.100%
1.Yes
Industry
1.Insufficient
data
1.N/R
High
2005
2.N/R
2.N/R
2.Yes
2.No
2.Unclear
2.Yes
todeterm
ine
2.N/R
RCT
3.N/R
3.Yes
(CTscans)
2.Patient
3.N/R
#20
4.N/A
4.N/R
*Reported
as‘double
blind’
3.No
4.Standardisatio
nof
CTscansN/R.
Final
number
ofsockets,patients
remainunclear.
Froum
1.Yes
1.N/R
1.N/R
1.Yes
1.100%
1.Yes
Industry
1.N/R
1.N/R
Moderate
2002
2.Yes
2.N/R
2.N/A
2.Yes
2.Unclear
2.Yes
2.Site
2.N/R
RCT
3.N/R
3.Yes
3.No
3.N/R
#17
4.N/A
4.N/R
4.Different
healingperiods.
Enrolmentof
sitesof
subjectsinconsistent.
Clin Oral Invest (2013) 17:341–363 349

Tab
le2
(con
tinued)
Study
QualityCriteria
Estim
ated
risk
ofbias
Firstauthor
Randomisation
Masking
Calibratio
nElig
ibility
Criteria
Follow
upEthical
considerations
Funding
Statistical
analysis
Miscellaneous
Yearof
publication
1.Randomised
1.Therapist
1.Intra-exam
iner
1.Inclusion
criteriadefined
1.Percentage
ofcompleted
follo
wups
1.Ethicsapproval
Sourceof
Funding
1.Appropriate
samplesize
calculationandpower
1.Com
parable
experimentalgroups
2.CONSORT
implem
ented
2.Inform
edconsent
3.ISRCTN
registered
2.Unitof
analysis
4.Other
comments
3.Appropriate
statisticsapplied
2.Exclusion
criteriadefined
2.Adequate
correctio
n
2.Patient
2.Inter-exam
iner
2.Adequate
sequence
generatio
n3.
Examiner
Type
4.Statistician
3.Allo
catio
nconcealm
ent
Reference
number
4.Concealment
adequate
Guarnieri
N/A
1.N/R
1.N/R
1.Yes
1.N/R
1.Yes
Governm
ent;
institu
tion
1.N/R
1.N/R
High
2004
2.N/R
2.N/A
2.No
2.N/A
2.Yes
2.Site
2.N/R
CCT
3.N/R
3.No
3.N/R
#45
4.N/R
Iasella
1.Yes
1.N/R
1.Yes
1.Yes
1.100%
1.Yes
N/R
1.Insufficient
data
todeterm
ine
1.Yes
Moderate
2003
2.Yes
2.N/R
2.N/A
2.Yes
2.Yes
2.Yes
2.Patient
2.N/R
RCT
3.N/R
3.Yes
3.Insufficient
data
todeterm
ine
3.N/R
#23
4.N/A
4.N/R
Lekovic
N/A
1.N/R
1.N/R
1.No
1.70%
(premature
exposure
ofe-PTFE
barrierin
3/10)
1.Yes
N/R
1.N/R
1.Yes
High
1997
2.N/R
2.N/A
2.No
2.N/R
2.Patient
2.N/R
CCT
3.N/R
2.Yes
3.Insufficient
data
todeterm
ine
3.N/R
#24
4.N/R
Lekovic
1.Yes
1.N/R
1.N/R
1.No
1.100%
1.Yes
N/R
1.N/R
1.Yes
Moderate
1998
2.Yes
2.N/R
2.N/A
2.No
2.Yes
2.Yes
2.Patient
2.N/R
RCT
3.N/R
3.Yes
3.Insufficient
data
todeterm
ine
3.N/R
#25
4.N/A
4.Yes
Nevins
1.Yes
1.N/R
1.N/R
1.Yes
1.100%
1.N/R
N/R
1.N/R
1.Yes
High
2006
2.N/R
2.N/R
2.N/A
2.Yes
2.Yes
2.N/R
2.Site
2.N/R
RCT
3.N/R
3.N/R
3.No
3.N/R
#46
4.N/A
4.N/R
4.Standardisationof
CT
scansN/R.T
estm
aterial
radiopaque.D
ifferent
healingperiods.
Pelegrine
1.Yes
1.N/R
1.N/R
1.Yes
1.100%
1.Yes
N/R
1.N/R
1.N/R
High
2010
2.N/R
2.N/R
2.N/A
2.Yes
2.Yes
2.Yes
2.Patient
2.N/R
RCT
3.N/R
3.N/R
3.Yes
3.N/R
#47
4.N/A
4.N/R
Serino
N/A
1.N/R
1.N/R
1.Yes
1.80%
1.Yes
N/R
1.N/R
1.N/R
High
2003
2.N/R
2.N/A
2.No
2.Unclear
2.Yes
2.Site
2.N/R
CCT
3.N/R
3.No
3.N/R
#19
4.N/R
4.Molarsonly
inT.
350 Clin Oral Invest (2013) 17:341–363

of the AR, but the newly formed tissue is of inferior qualityand quantity (percentage of matured trabecular bone) towhat is normally achieved following a tooth extraction.
Finally, the quality of the included studies has also beenmeticulously assessed in this review. Such a quality evalu-ation of the retrieved data is essential to estimate the sourceand magnitude of potential bias that may lead to delusiveconclusions.
Strength of evidence—risk of bias
The quality assessment of the included studies in this sys-tematic review revealed that none of the trials have qualifiedfor a low risk of bias category. Ten out of the 14 studiespresented with high risk of bias thus their results must beevaluated with caution. The lack of clear reporting of re-search methodology elements, such as adequate randomiza-tion and concealment and/or masking of the therapist andthe examiner were among the primary reasons for the highrisk of bias [49]. We did not contact authors for clarificationof unclear methodology. Therefore, it is possible that actualstudy conduct was better than that reported in the publica-tion. Statistical considerations played important role as well,since appropriate analytical statistics was completed andreported merely in one study [47]. Power calculation wasconducted in three trials only [21, 23, 42], nevertheless thereported data were insufficient to determine the validity ofthe calculation.
Dimensional changes and histological characteristics
Sufficient ridge width and height have been considered asone of the key requirements for successful implant therapyand for the establishment of an aesthetically pleasing emer-gence profile at fixed partial dentures [8, 50, 51]. Therefore,the alterations in oro-facial (horizontal) and apico-coronal(vertical) AR dimensions were selected as the primary out-comes of the present review. Direct intra-surgical measure-ments on the AR at re-entry are considered as the mostprecise method to evaluate the bone volume changes fol-lowing ARP. It is desirable though to establish and validate asurrogate measure that avoids the need for re-entry surgery,while providing the clinician with a reliable measure. Two-dimensional radiographs, such as periapical or panoramicradiographs, are not ideal to estimate the 3D changes of theAR [52]. Also, measurements of the alveolar mucosa levelor study casts incorporate not only the alveolar bone, butalso the overlaying soft tissue. For these reasons onlystudies performing clinical or 3D radiographic evaluationof hard tissue were included in this review. Cone-beamcomputerised tomography (CBCT) appears to offer a validtechnique to assess alveolar ridge changes, with newer mod-els greatly reducing radiation exposure [53]. However, aT
able
2(con
tinued)
Study
QualityCriteria
Estim
ated
risk
ofbias
Firstauthor
Randomisation
Masking
Calibratio
nElig
ibility
Criteria
Follow
upEthical
considerations
Funding
Statistical
analysis
Miscellaneous
Yearof
publication
1.Randomised
1.Therapist
1.Intra-exam
iner
1.Inclusion
criteriadefined
1.Percentage
ofcompleted
follo
wups
1.Ethicsapproval
Sourceof
Funding
1.Appropriate
samplesize
calculationandpower
1.Com
parable
experimentalgroups
2.CONSORT
implem
ented
2.Inform
edconsent
3.ISRCTN
registered
2.Unitof
analysis
4.Other
comments
3.Appropriate
statisticsapplied
2.Exclusion
criteriadefined
2.Adequate
correctio
n
2.Patient
2.Inter-exam
iner
2.Adequate
sequence
generatio
n3.
Examiner
Type
4.Statistician
3.Allo
catio
nconcealm
ent
Reference
number
4.Concealment
adequate
Serino
N/A
1.N/R
1.N/R
1.Yes
1.80%
1.Yes
Governm
ent;
institu
tion
1.N/R
1.N/R
High
2.Patient
2.N/R
3.Insufficient
data
todeterm
ine
3.N/R
2008
2.N/R
2.N/A
2.No
2.Unclear
2.Yes
CCT
#48
3.N/R
4.N/R
N/A
notapplicable;N/R
notrepo
rted,Ttest;C
control;RCTrand
omised
controlledtrial;CCTcontrolledclinical
trial;PRGFplatelet-richgrow
thfactor;CONSO
RTCon
solid
ated
Stand
ards
ofReportin
gTrials;ISRCTNInternationalStand
ardRando
mised
Con
trolledTrial
Num
berRegister
Clin Oral Invest (2013) 17:341–363 351

Tab
le3
Firstauthor
Trial
characteristics
Population
characteristics
Confounding
factors
Defect
characteristics
Testmaterial
(num
berof
sockets/
subjects)
Control
(num
berof
sockets/
subjects)
Surgical
managem
ent
Follow-up
Alveolarridge
dimension
changesin
horizontal
width
Alveolarridge
dimension
changesin
vertical
height
Implant
1.Feasibility
ofim
plant
placem
ent
2.Necessityof
simultaneous
augm
entation
Mean/medianmm
(reference
point)
Mean/medianmm
1.Whole
ridge
1.Mid-buccal
1.Healin
gperiod
Year
ofpublication
2.Buccalplate
2.Mesial
1.Socket
locatio
n1.
Type
offlap
3.Distal
2.Num
ber
ofdrop-outs
4.SocketFill
2.Softtissue
closure
2.Defect
morphology
1.Country
1.Age
range
(mean)
inyears
1.Smoking
3.Adverse
events
3.Postoperativ
eantim
icrobials
2.Num
berof
centres
2.Periodontitis
Type
Design
2.Num
berof
patients
(sockets)
3.Settin
gMethodology
Reference
number
Aimetti
1.Italy
1.36-68
(51.27
±8.4)
1.No
1.Maxillary
anterior
Calcium
sulphate
Empty
(18/18)
1.Flapless
1.3months
1.T:-2.0±1.1**
1.T:
-0.5±1.1*,
C:-1.2±0.6**,***
1.Im
plants
were
inserted
2009
2.1
RCT
Parallel
2.N/R
3.University
Clin
+Histo
Hem
ihydrate
(22/22)
#42
2.40
(40)
2.Noprim
ary
closure
2.4-wall
configuration
2.N/R
C:-3.2±1.8**,
***
3.Uneventful
healing
3.Amoxicillin
2g/day
for
5days,
Chlorexidine
0.12%
for
2weeks
2.N/R
2.T:-0.2±0.6,
C:-0.5±0.9
3.T:-0.4±0.9,
C:-0.5±1.1
4.T:
11.3±2.8**,
C:10.0±2.3**
(Acrylic
stent)
2.N/R
Anitua1999
1.Spain
1.T:35-55
(41)
1.Yes
1.Any
T1:
PRGF
(5+3/5+3)
Empty
(10+3/
10+3)
1.Full-thickness
1.2.5–4
months
N/A
N/A
1.N/R
2.N/R
2.Variable
2.Yes
2.Primary
closure
2.0
3.N/R
T2:
PRGF+
Autologous
bone
(5/5)
3.Amoxicillin
1.5g/day
for
5days
2.1
C:38-54(42)
CCT
3.Private
practice
2.23
(26)
Parallel+Split-
mouth
Histo
#43
Barone
2008
1.Italy
1.26-69
1.<10/day
1.Non-m
olars
Corticocancellous
porcinebone+
collagen
mem
brane
(20/20)
Empty
(20/20)
1.Full-thickness
1.7-9months
1.T:-2.5±1.2*,
C:-4.5±0.8*,***
1.T:-0.7±1.4*,
C:-3.6±1.5*,***
1.‘Implantswere
inserted
inboth
groups’
2.1
2.Primaryclosure
2.0
2.T:-0.2±0.8,
C:-0.4±1.2
2.Som
eGBR
wereneeded
dueto
buccal
dehiscence
inthecontrol
group
2.N/R
3.T:-0.4±0.8,
C:-0.5±1.0
3.Amoxicillin
2g/day
for
4days+
Chlorexidine
0.12%
for
3weeks
3.Uneventful
healing
(pain,
swellin
g)
2.Yes
(treated)
2.4-wall
configuration
4.N/R
2.40
(40)
(Acrylic
stent)
3.Hospital
RCT
Parallel
Clin
+Histo
#21
Cam
argo
2000
1.USA,
Yugoslavia
1.28-60
(44±15.9)
1.N/R
1.Maxillary
anterior,
prem
olars
Bioactiv
eglass+
coveredby
calcium
sulphate
layer(16/8)
Empty
(16/8)
1.Full-thickness
with
4vertical
releasing
incisions
1.6months
1.T:-3.48
±2.68**,
C:-3.06
±2.41**
1.T:-0.38
±3.18,
C:-1.00
±2.25
(titanium
tack)
1.Reentry
only
2.N/R
2.Noprim
ary
closure
3.N/R
2.N/R
4.T:
6.43
±2.78**,
C:4.00±2.33**,***
(tobuccal
bone
crest)
2.N/A
3.Penicillin
1.5g/day
for
7days+
Chlorexidine
0.12%
for
2weeks
2.N/R
2.N/R
2.16
(32)
3.Uneventful
healing
2.N/R
CCT
2.N/R
3.University
Split-mouth
Clin
#44
352 Clin Oral Invest (2013) 17:341–363

Tab
le3
(con
tinued)
Firstauthor
Trial
characteristics
Population
characteristics
Confounding
factors
Defect
characteristics
Testmaterial
(num
berof
sockets/
subjects)
Control
(num
berof
sockets/
subjects)
Surgical
managem
ent
Follow-up
Alveolarridge
dimension
changesin
horizontal
width
Alveolarridge
dimension
changesin
vertical
height
Implant
1.Feasibility
ofim
plant
placem
ent
2.Necessity
ofsimultaneous
augm
entation
Mean/medianmm
(reference
point)
Mean/medianmm
1.Whole
ridge
1.Mid-buccal
1.Healin
gperiod
Year
ofpublication
2.Buccalplate
2.Mesial
1.Socket
locatio
n1.
Typeof
flap
3.Distal
2.Num
ber
ofdrop-outs
4.SocketFill
2.Softtissue
closure
2.Defect
morphology
1.Country
1.Age
range
(mean)
inyears
1.Smoking
3.Adverse
events
3.Postoperativ
eantim
icrobials
2.Num
berof
centres
2.Periodontitis
Type
Design
2.Num
berof
patients
(sockets)
3.Settin
gMethodology
Reference
number
Fiorellini
2005
1.USA
1.47.4
1.N/R
1.Maxillary
anterior,
prem
olars
T1:
1.5m
g/ml
rhBMP-2
(?/21?)
Empty
(?/20?)
1.Full-thickness
with
vertical
incisions
1.4months
1.Coronal:
T1:+3
.27±2.53*,
T2:+1
.76±1.67*,
T3:+0
.82±1.40,
C:+
0.57
±2.56,***
(T1vs
T2/T3/C)
1.T1:-0.02±1.2,
T2:-0.62±1.39*,
T3:-1.00±1.40*,
C:-1.17
±1.23*,
***(T1vs
C)
1.N/R
2.Noneed
for
augm
entatio
n2.
Nodrop-outs
reported.
(3patients
incorrectly
random
ized,
1patient
received
different
graft)
T1:
18/21(86%
)T2:
0.75mg/ml
rhBMP-2
(?/22?)
T2:
12/22(55%
)
2.Primary
closure
2.N/R
T3:
10/17(59%
)
2.N/R
3.N/R
C:9/20
(45%
)
3.250(T
>C)
4.N/R
(T1vs
T2/C)***
3.Penicillin
(?mg)
for7-10
days+
Chlorexidine
0.12%
T3:
Collagen
sponge
(?/17?)
2.≥5
0%buccal
bone
loss
2.8centres
2.80
(95)
2.N/R
RCT
3.University
Parallel
Radiogr+
Histo
#20
Froum 2002
1.USA
1.35-77
(54.9±11.9)
1.No
1.Any
T1:
Bioactiv
eglass(10/8)
Empty
(10/10)
1.Full-thickness
with
outvertical
incisions
1.6-8months
N/A
N/A
1.‘A
nim
plant
ofappropriate
size
was
placed
inthehealed
sockets.’
2.0
3.Uneventful
healing
T2:
DFDBA
(10/8)
2.Primary
closure
2.N/R
3.Doxycyclin
e100m
g/day
for13
days+
Chlorexidine
0.12%
for
30days
2.N/R
2.4-wall
configuration,
≤2mm
buccal
plateloss
2.19
(30)
2.Single
centre
RCT
Splitmouth
3.University
Histo
#17
Guarnieri
2004
1.Italy
1.35-58
1.N/R
1.Maxillary,
mandibular
anteriors,
prem
olars
Calcium
sulphate
Empty
(5/5)
1.Full-thickness
with
outvertical
incisions
1.3months
N/A
N/A
1.‘Bucco-lingual
dimensionsof
thealveolar
ridge
enabled
safeinsertion
oftitanium
implant.’
2.socket
with
ridge
resorptio
n≥5
0%were
excluded
2.Primaryclosure
3.Amoxicillin
(?mg)
for
1week+Chlorexidine
0.2%
for2weeks
2.N/R
Hem
ihydrate
(10/10)
2.N/R
2.Yes
3.N/R
2.10
(25)
2.N/R
3.N/R
CCT
Parallel+
Split
mouth
Histo
#45
Iasella
2003
1.USA
1.28-76
(51.5±13.6)
1.Yes
1.Maxillary
anteriors,
prem
olars
and
mandibular
prem
olars
Tetracycline
hydrated
FDBA
+
Empty
(12/12)
1.Full-thickness
with
outvertical
incisions
1.4or
6months
(com
bined)
1.T:-1.2±0.9*,
C:-2.6±2.3*
1.T:
+1.3±2.0,
C:-0.9±1.6***
1.Im
plants
successfully
placed
atall
sites
2.N/R
2.N/R
2.T:
-0.1±0.7,
C:-1
.0±0.8***
2.Somesiteshad
slightdehiscence
andrequired
furth
eraugm
entation
2.Noprim
aryclosure
2.N/R
3.T:
-0.1±0.7,
C:-0.8±0.8***
3.Doxycyclin
200m
g/dayfor
1week+
Chlorexidine
0.12%
for
2weeks
collagen
mem
brane
(12/12)
2.0
4.N/R
3.N/R
(Acrylic
stent)
3.N/R
2.24
(24)
RCT
2.N/R
Parallel
Clin
+Histo
#23
Clin Oral Invest (2013) 17:341–363 353

Tab
le3
(con
tinued)
Firstauthor
Trial
characteristics
Population
characteristics
Confounding
factors
Defect
characteristics
Testmaterial
(num
berof
sockets/
subjects)
Control
(num
berof
sockets/
subjects)
Surgical
managem
ent
Follow-up
Alveolarridge
dimension
changesin
horizontal
width
Alveolarridge
dimension
changesin
vertical
height
Implant
1.Feasibility
ofim
plant
placem
ent
2.Necessity
ofsimultaneous
augm
entation
Mean/medianmm
(reference
point)
Mean/medianmm
1.Whole
ridge
1.Mid-buccal
1.Healin
gperiod
Year
ofpublication
2.Buccalplate
2.Mesial
1.Socket
locatio
n1.
Typeof
flap
3.Distal
2.Num
ber
ofdrop-outs
4.SocketFill
2.Softtissue
closure
2.Defect
morphology
1.Country
1.Age
range
(mean)
inyears
1.Smoking
3.Adverse
events
3.Postoperativ
eantim
icrobials
2.Num
berof
centres
2.Periodontitis
Type
Design
2.Num
berof
patients
(sockets)
3.Settin
gMethodology
Reference
number
Lekovic
1997
1.Yugoslavia
/USA
1.(49.8)
1.N/R
1.Maxillary
and
mandibular
anteriors,
prem
olars
e-PTFE
mem
brane
(10/10)
Empty
(10/10)
1.Full-thickness
with
4vertical
releasing
incisions
1.6months
1.10/10:,
T:-1.80±0.51,
C:-4.40±0.61**,
***
1.10/10:
T:-0.5±0.22,
C:-1.2±0.13**,
***
1.Reentry
only
7/10:T:-1.71±0.75,
C:-4.43±0.72**,
***
7/10:
T:-0.28±0.18,
C:-1.0±0.0**,
***
3/10:T:-2.00±0.00,
C:-4.33±0.88*
3/10:T:-1.0±0.58,
C:-1.66±0.33
(titanium
tack)
2.N/R
3.N/R
4.10/10:
T:4.9±0.86*,
C:3.0±0.63,
***
2.N/R
7/10:T
:5.43±1.1*,
C:2.92±1.61,***
3/10:T
:3.66±1.20,
C:4
.33±1.45
(tobuccalbone
crest)
2.Primaryclosure
3.Penicillin
1g/day
for
7days+
Chlorexidine
0.2%
2.N/A
2.3/10
drop-outs
dueto
prem
ature
mem
brane
exposure
3.3/10
exposed,
7/10
noinfection
2.10
(20)
2.N/R
CCT
2.N/R
(presumably
singlecentre)
Split-mouth
2.N/R
Clin
3.University
#24
Lekovic
1998
1.Yugoslavia
1.(52.6±11.8)
1.N/R
1.Maxillary
and
mandibular
anteriors,
prem
olars
PG/PL
mem
brane
(16/16)
Empty
(16/16)
1.Full-thickness
with
4vertical
releasingincisions
1.6months
1.T:-1.31±0.24*
1.T:-0.38
±0.22,
C:-1.50
±0.26*,
***(titanium
tack)
1.Reentry
only
2.N/A
2.0
C:-4.56
±0.33*,
***
3.Uneventful
healing
2.N/R
2.Primaryclosure
2.N/R
3.Penicillin1g/day
for7days+
Chlorexidine0.12%
for2weeks
3.N/R
2.Yes
(treated)
2.N/R
4.T:5.81
±0.29*,
C:3.94
±0.35*,
***
(tobuccal
bone
crest)
2.16
(32)
2.1
3.University
RCT
Split-mouth
Clin
#25
Nevins2006
1.USA
/Italy
1.N/R
1.N/R
1.Maxillaryanterior
DBBM
(19/9)
Empty(17/9)
1.Partial
thickness
1.1–3months
(biopsiesat6M
)N/A
1.T:-2.42±2.58,
C:-5.24±3.72***
1.Im
plantswere
placed,but
number
unknow
n
2.Buccalplatewas
comprom
ised
2.Primary
closure
2.0
3.N/R
2.N/R
2.N/R
3.N/R
3.N/R
4.N/R
(At6mm
ridgewidth)
2.Yes
RCT
2.N/R
Split-mouth
3.N/R
Radiogr+
Histo
#46
2.9(36)
354 Clin Oral Invest (2013) 17:341–363

Tab
le3
(con
tinued)
Firstauthor
Trial
characteristics
Population
characteristics
Confounding
factors
Defect
characteristics
Testmaterial
(num
berof
sockets/
subjects)
Control
(num
berof
sockets/
subjects)
Surgical
managem
ent
Follow-up
Alveolarridge
dimension
changesin
horizontal
width
Alveolarridge
dimension
changesin
vertical
height
Implant
1.Feasibility
ofim
plant
placem
ent
2.Necessity
ofsimultaneous
augm
entation
Mean/medianmm
(reference
point)
Mean/medianmm
1.Whole
ridge
1.Mid-buccal
1.Healin
gperiod
Year
ofpublication
2.Buccalplate
2.Mesial
1.Socket
locatio
n1.
Typeof
flap
3.Distal
2.Num
ber
ofdrop-outs
4.SocketFill
2.Softtissue
closure
2.Defect
morphology
1.Country
1.Age
range
(mean)
inyears
1.Smoking
3.Adverse
events
3.Postoperativ
eantim
icrobials
2.Num
berof
centres
2.Periodontitis
Type
Design
2.Num
berof
patients
(sockets)
3.Settin
gMethodology
Reference
number
Pelegrine
2010
1.Brazil
1.28-70
(47.5±10.3)
1.No
1.Maxillary
anteriors
Autologous
bone
marrow
(15/7)
Empty
(15/6)
1.Full-thickness
with
2buccal
vertical
releasing
incisions
1.6months
1.T:-1.0*,
C:-2.5*,***
1.T:
-0.5*,
C:-1.0*,***
(Titanium
screw)
1.Allimplants
osseointegrated
2.N/R
2.13
(30)
2.N/R
2.Primaryclosure
3.N/R
2.1
2.0
3.University
2.T:-0.75,
C:-1.75,***
4.T:10.33*,C:10.32*
(tobuccal
bone
crest)
2.T:with
out
further
augm
entatio
n,C:At5sites
augm
entatio
nor
expansion
carriedout
3.N/R
3.Uneventful
healing
RCT
2.Socketswith
severe
bone
loss
were
excluded
Parallel
Clin
+histo
#47
Serino
2003
1.Italy
1.35-64
1.N/R
1.Any
PG/PLsponge
(26/24)after
drop-out
Empty
(13/12)
afterdrop-out
1.Full-thickness
buccally
and
lingually
1.6months
N/A
1.T:+1.3±1.9*,
C:-0.8±1.6
1.Placementof
implantsin
all
CandTsites
with
good
prim
arystability
2.Buccalplate
couldbe
partially
orcompletely
lost
2.1
CCT
Parallel+
split-m
outh
2.45
(39)
before
drop-out
3.N/R
2.Yes
(treated)
Clin
+Histo
#19
2.Noprim
ary
closure
2.9drop-outs
forreasons
unrelatedto
thetherapy
2.T:-0.2±1.0,
C:-0.6±1.0
3.T:-0.1±1.1,
C:-0.8±1.5
3.No
antib
iotics;
Chlorexidine
0.2%
for
2weeks
3.Uneventful
healing
4.N/R
(Acrylic
stent)
2.N/R
Serino
2008
1.Italy
1.32-64
1.N/R
1.Any
non-molars
PG/PLsponge
(7/7)
Empty(9/9)
afterdrop-out
1.Full-thickness
buccally
and
lingually
1.3months
N/A
N/A
1.Placementof
implantsin
all
CandTsites
with
good
prim
arystability
2.1
2.Yes
(treated)
2.4drop-outs
forreasons
unrelatedto
thetherapy
afterdrop-out
CCT
2.Alveolar
bone
height
≥8mm
2.Noprim
ary
closure
Parallel
2.N/R
Histo
3.NoAntibiotics;
Chlorexidine
0.2%
for2weeks
3.Uneventful
healing
2.20
(20)
before
drop-out
#48
3.N/R
*p<0.05;statistically
sign
ificantintra-grou
pdifference,baselin
eto
final;**
p<0.00
1statistically
high
lysign
ificantintra-grou
pdifference,baselin
eto
final;**
*p<0.05
statistically
sign
ificant
inter-groupdifference,betweentestandcontrol;
N/A
notapplicable;N/R
notrepo
rted;Ttest;C
control;M=mon
th(s);Clin
clinical
analysis;Histo
histolog
ical
analysis;Rad
iogr
radiog
raph
icanalysis;RCTrand
omised
controlledtrial;CCT
controlledclinicaltrial;PRGFplasmarich
ingrow
thfactors;DFDBAdemineralised
freeze-dried
bone
allograft;FDBAfreeze-dried
bone
allograft;e-PTFEexpand
ed-polytetrafluo
rethylen;PG/PL
polyglycolide/po
lylactide;
DBBM
demineralised
bovine-bon
emineral
Clin Oral Invest (2013) 17:341–363 355

Tab
le4
Firstauthor
Num
berof
biopsies
Histomorphology
Histomorphom
etry
Statistical
difference
betweentestand
control
Test
Control
(meanor
median%)
Yearof
publication
(testmaterial)
Type
Healin
gperiod
Reference
number
Aimetti2009
T:N/R
22?
(MGCSH)
Noresidual
graftmaterial.Noinflam
matory
infiltrate.New
bone
form
ationin
all
specim
ens,100%
livingtrabecular
bone
with
woven
andlamellarstructure.
100%
livingbone
(mostly
woven)
inallbiopsies.Lam
ellarbone
remodelingwas
starting.
Trabecular
bone:
Residual
substitute
material:
Woven
bone:
Lam
ellar
bone:
Tvs
C*
T:58.8±3.5
Coronal:
Coronal:
T:0.0
T:83.6±6.6
T:16.4±6.6
C:11.1±7.6
C:88.9±7.6
Middle:
T:40.4±13.2
Middle:
T:59.6±13.2
C:18.9±7.6
C:81.1±7.6
Apical:
Apical:
T:56.4±10.9
T:43.6±10.9
C:77.8±8.1
RCT
C:N/R
18?
C:22.2±8.1
C:N/A
C:47.2±7.7
3M
#42
Anitua
1999
T:N/R
(PRGF±
autogenbone)
Com
pact
maturebone
with
well-organized
trabeculae
andmorphologyin
8/10
patients.
Connectivetissuewith
non-organized
trabeculae
in2/10
patients.Significant
intra-groupdifferences10
vs.16
weeks!
Connectivetissuefills
themain
partof
thedefect.Nomature
bone.
N/R
CCT
2.5–4M
C:N/R
#43
Barone2008
T:20 (Corticocancellous
porcinebone+
collagen
mem
brane)
Residualgraftmaterialem
bedded
innewly
form
edbone
inallspecim
ens.Com
plete
bone
fill.
Typically
trabecular
bone
pattern.
Large
marrow
spaces
filledwith
adipocytes.Lam
ellarbone
was
also
presentwith
inthebone
marrow.
Totalbone
volume:
Connective
tissue:
Residualgraft
material:
Bone:
T>C*
Connectivetissue:
T<C*
RCT
T:35.5±10.4
T:36.6±12.6
T:29.2±10.1
C:25.7±9.5
C:59.1±10.4
C:N/A
7–9M
C:20
#21
Fiorellini
2005
T1:16
(rhB
MP-2
1.5m
g/ml)
Noevidence
ofinflam
mationor
residualgraft.Trabecularbone
form
ationin
2/3
ofthesamples.M
ineralized
tissueform
ationpresentedwith
differentlevelof
remodeling.Minor
osteoclasticactiv
ity.N
ocomparisonreported
between
TandC!
N/R
T2:
15(0,75m
g/ml)
T3:11
(Collagensponge)
RCT
C:14
4M
#20
Froum
2002
T1:
10(Bioactiv
eglass)
T1:
New
bone
form
ation.
Osteoid
surrounded
andpenetrated
thebioactiveglassparticles.
N/R
Vitalbone:
Connective
tissue:
Residualbone
substitute:
Connectivetissue:
T1<T2or
C*
T1:
59.5
T1:
35.3
T1:
5.5
T2:
13.5
T2:
34.7
T2:
51.6
C:N/A
C:67.0
C:32.4
T2:
Varying
degreesof
reossificatio
naround
DFDBA.
RCT
T2:
10(D
FDBA)
C:10
6–8M
#17
356 Clin Oral Invest (2013) 17:341–363

Tab
le4
(con
tinued)
Firstauthor
Num
berof
biopsies
Histomorphology
Histomorphom
etry
Statistical
difference
betweentestand
control
Test
Control
(meanor
median%)
Yearof
publication
(testmaterial)
Type
Healin
gperiod
Reference
number
Guarnieri2004
T:10
(MGCSH)
Alm
ostcompleteabsenceof
MGCSH.
Absence
ofconnectiv
etissueand
inflam
matorycells.In
allsections
trabecular
bone
form
ationwith
nodifferencesbetweentheapical,middle
andcoronallevels.
Lessbone
form
ationcompared
totestsites.
Trabecular
bone
area:
Nostatisticalsignificance
couldbe
draw
ndue
tosm
allnum
berof
controlspecimens.
CCT
C:5
T:Coronal:58.6±9.2
3M
Middle:
58.1±6.2
Apical:58.3±7.8
C:≤46
#45
Iasella
2003
T:4M
:5,
6M:7
Residualgraftparticlessurrounded
bywoven
bone
orby
connectiv
etissue.
Similaram
ount
oftotalb
oneand
trabecular
spaces
asin
test.
Vitalbone:
Non-vitalbone:
N/R
(Tetracycline
hydrated
FDBA+
Collagen
mem
brane)
(Nobiopsy
from
2Csitesdue
tominim
albone
fill)
4M4M
T:31
±9
T:32
±19
C:58
±11
C:N/A
6M T:41
±18
C:N/A
Com
bined
6M
T:37
±18
C:N/A
T:25
±17
C:50
±14
Com
bined
RCT
T:28
±14
C:54
±12
4–6M
#23
C:4M
:5,
6M:5
Nevins2005
T:5(D
BBM)
DBBM
granules
present.Apically
integrated
incancellous
bone
butcoronally
insoft
tissue.Nosignsof
inflam
mationor
foreignbody
reactio
n.
New
bone
form
ation
Nocomparisonmade.
RCT
6M
#46
C:5
Pelegrine
2010
T:7
(Autologous
bone
marrow)
Mineralized
bone:
Nosignificantdifference.
T:45.0
RCT
C:43.75
C:6
6M
#47
Serino
2003
T:10 (PG/PLsponge)
Noresidual
graftmaterial.Presenceof
matured,mineralized
bone.Lackof
coronalsofttissueingrow
th.
Presenceof
mineralized
bone.
Widemarrow
spaces.
Mineralized
bone:
Statisticalcomparison
cannotbe
madedue
tothesm
allnum
ber
ofcontrolspecimens.
T:66.7
C:3
C:43.7
CCT
6M
#19
Serino
2008
T:7 (PG/PLsponge)
Noresidualgraftm
aterial.Scarce
presence
ofinflammatorytissue.Coronal:new
lyform
edtrabecularbone
with
largemarrowspaces.
Apical:morematureandcompactbone.
Coronal:trabecularbone
with
wide
marrowspaces
with
connective
tissue.Apical:morematureand
compactbone.
Mineralized
bone:
Nosignificant
difference.
T:59.9±22.4
CCT
C:9
C:48.8±14.4
3M
#48
*p<0.05
;statistically
sign
ificantdifference
betweentestandcontrol
Ttest;Ccontrol;M
mon
th(s);N/R
notrepo
rted;N/A
notapplicable;vs.v
ersus;TBVtotalbo
nevo
lume;MGCSH
medicalgradecalcium
sulphatehemihyd
rate;DFDBAdemineralised
freeze-dried
bone
allograft;FDBAmineralised
freeze-dried
bone
allograft;DBBM
demineralised
bovine-bon
emineral;PG/PLpo
lyglycolide/po
lylactide
Clin Oral Invest (2013) 17:341–363 357

prerequisite of this technique would be some type of stand-ardisation, so that the captured image is being always takenfrom exactly identical positions [54]. None of the two includedradiographic studies reported on such standardisation [20, 46].
For the interpretation of the results we attempted tocluster the studies in respect to the type of intervention.
Unassisted sockets In the present review, the mean reduc-tion of the AR width of the untreated sites varied between2.6±2.3 mm and 4.6±0.3 mm and the mean reduction of theAR height was between 0.8±1.6 mm and 3.6±1.5 mm after1 to 9 months of healing. This corroborates the result of aprevious clinical study which indicated that 95 % of ARreduction should be expected after three months of extrac-tion [1]. Furthermore, it is in agreement with a recent sys-tematic review, which reported that the average reduction ofthe AR width seemed to be higher (3.87 mm), than thereduction in AR height (1.67 mm) [55].
Even though both AR width and height present resorp-tion, histologically, new bone formation up to a variableextent was also observed in some studies as result of unas-sisted socket healing [19–21, 23, 42, 45, 46, 48]. In addi-tion, a large area was occupied by bone marrow [19, 21, 48],as reported in preclinical studies [11, 13, 56]. Only a singlestudy reported on connective tissue fill and lack of maturebone [43].
Bone grafts and substitutes Effective grafting procedures forbone augmentation have been associated with the osteocon-ductive, osteoinductive or osteogenetic properties of the graft[56–59]. This led to the assumption that the placement of thesematerials in the extraction socket may accelerate new boneformation by the above biological properties and may alsoreduce AR resorption by stabilising the blood clot, providing ascaffold and external source of minerals and/or collagen [11,12, 60, 61]. The placement of DBBM with collagen in freshextraction sockets resulted in limited reduction of the ARdimensions, although delayed initial socket healing in termsof new bone formation was also observed [11, 12]. Humanstudies reported similar unfavourable histological observa-tions when DFDBAwas employed for ARP [15, 16].
In the present review of human experiments, two out ofthree studies reported that socket grafting with autologousbone marrow [47] or alloplastic material [42] have signifi-cantly limited the reduction of the AR width compared tothe unassisted socket healing. Three out of five studiesreported that reduction of the resorption in AR height wassignificant [42, 46, 47], while the ridge height was evenincreased in one study, where sockets were grafted withpolymer sponge [19]. We should emphasise though thatsince the graft material (DBBM) in a CT study possessedradiopaque characteristic, the alteration of the AR contouron the CT image should be interpreted with caution [46].
Based on the histological evaluation of these studies, theabove AR dimensional changes were not necessarily accom-panied by higher amount of new bone formation in thesocket, since the quality of newly formed tissue in theARP sites was comparable to that in the control sites.Furthermore, the sockets were occupied by a mixture ofnew bone and connective tissue which in many occasionswas surrounding the graft particles [17, 21, 46] (Table 4).
GBR (membrane alone or in combination with ‘graft’) Theconception of guided bone and tissue regeneration [62] wastranslated to ARP procedures in order to exclude epithelialcells from the extraction socket by the use of barrier mem-brane in four studies of the present review [21, 23–25].
(a) GBR with membrane aloneARP with GBR resulted in statistically significantly
less resorption in ridge width and height compared tounassisted socket healing, regardless of the type ofmembrane [24, 25]. It should be noted that in one study[24], in three out of 10 cases, the exposed non-resorbable e-PTFE barrier had to be removed prema-turely, highlighting the importance of sufficient softtissue closure and timing of removal of the barrier.The outcomes in these three cases were similar to thecontrol sites. Where healing was uncompromised, astatistically significant difference was found after6 months in width and height changes in favour ofthe ARP group.
(b) GBR with membrane and ‘graft’ARP resulted in statistically significantly less re-
sorption in width [21, 23] and height [23] in compar-ison to unassisted socket healing. The histologicalevaluation of the GBR procedures in the includedstudies demonstrated new bone formation [21, 23],but the presence of graft particles was also evident inboth studies, embedded either in newly formed bone[21] or in connective tissue [23]. This is in agreementwith a recent trial, where a collagen membrane incombination with DBBM or a biphasic bone substitutewas used for ARP [9, 10].
Biological active materials The potential benefit of biologi-cal active molecules was investigated in periodontal and boneregeneration through fostering the proliferation and differen-tiation of different mesenchymal cells in various preclinicalmodels [63, 64]. The safety and feasibility of rhBMP-2 onhuman ARP or ridge augmentation was evaluated and shownto be safe in a two-centre clinical study [35]. Dimensionalchanges of the alveolar ridge were measured on CTscans in anRCT [20]. Treatment with recombinant BMP-2 resulted in anincrease in ridge width which was statistically significantlygreater than controls. However, this observation needs to be
358 Clin Oral Invest (2013) 17:341–363

interpreted in light of the surprise finding of an increase inridge width of the untreated controls. This was a uniquefinding amongst the studies that we reviewed. Histologically,no comparison between ARP and controls sites was reported.
The human histological results of the included papers ofthe present review were generally found to be comparable topreclinical studies [11–13, 60, 65]. There are a number ofaspects to consider in the interpretation of the results. First-ly, it has to be kept in mind that whilst the biopsies of theanimal model incorporate the cross section of the whole AR,the biopsy retrieval at human studies is limited to a trephinecore sample of part of the former socket. This location maynot necessarily coincide with the exact position of the pre-vious extraction, thus making interpretation of the resultschallenging. Furthermore, the differentiation between api-cal, mid and coronal, as well as the central and lateralaspects of the biopsies was not always apparent.
Another important parameter when considering a histo-logical overview of the studies was the variation in healingtime. Due to the nature of post-extraction healing, the directcomparison of the new tissue formation in studies between 1and 9 months of healing could be misleading. This washighlighted in three studies which did not make a distinctionbetween the variable healing times within the groups, rang-ing from 2.5 months to 9 months [17, 21, 43]. It has to bekept in mind also that the only study, which completed andreported appropriate statistical methodology [47], did notobserve statistically significant difference between the testand control biopsies.
Furthermore, small sample sizes in the majority of thestudies may also limit the generalisability of the histologicalfindings.
Two studies found statistically significant histologicaldifferences in new bone formation favouring the test group[21, 42]. Drawing conclusions across the studies is difficultsince the test groups differed in many respects comparedwith each other, including different technique (bone sub-stitute only [42]/GBR + graft [21]), different material(MGCSH [42]/porcine bone with collagen membrane[21]), different flap management (flapless, no primary clo-sure [42]/mucoperiosteal flap, primary closure [21]), dif-ferent healing time (3 months [42]/7–9 months [21]). Onecommon feature was that both groups limited their inter-vention to sockets with four intact walls. It is noteworthythat all three studies that included intact socket walls only,reported statistically significant differences both on ARwidth and height in favour of ARP [21, 42, 47], while onlyone [20] out of two studies [19, 20] with initial buccal boneloss reported similar significant difference between testand control. Therefore, socket morphology could be animportant predicator of improved ARP. The need forARP in such sockets, in terms of future clinical success/implant placement needs further investigation.
Flap management All studies reporting statistically signifi-cant inter-group differences in both horizontal and verticalclinical measurements achieved either primary flap closure[21, 24, 25, 47], or did not detach the periosteum in aflapless procedure [42]. Furthermore, none of the studieswithout primary closure demonstrated statistically signifi-cant differences between test and control in terms of bothhorizontal and vertical clinical measurements [19, 23, 44].Therefore, both achieving and maintaining the epithelialseal above the socket may be crucial to improving ARP.Further corroboration of this concept was suggested wheree-PTFE barriers were prematurely exposed. The healing ofthese three exposed cases demonstrated no statistically sig-nificant differences compared to the control sites [24].
Other factors affecting interpretation of the findings
Healing time
The optimal timing of re-entry following ARP is determinedby the implant insertion. Since the volume of the AR isgradually decreasing, while the quality of the newly formedtissue is gradually increasing during the post-extractionremodelling [1, 6] the implant placement could be consid-ered as early as possible, but as late as necessary, in order tomaintain AR volume, as well as to achieve complete epi-thelial seal with some extent of osseous fill. The healingperiods of the trials in the present review varied consider-ably (one to nine months). Therefore, interpretation of theresults was complicated by the heterogeneity present in theincluded studies.
Antimicrobials
Improvement of clinical parameters was demonstrated as aresult of regular rinsing with chlorhexidine following toothextraction [66]. Subjects of the included trials in the presentreview were prescribed various types of antibiotics andinstructed to rinse with chlorhexidine for 2 to 3 weeks.Therefore, no conclusion could be drawn on the necessityor benefit of employment of antibiotics/antimicrobials fol-lowing ARP.
Smoking
Smoking is associated with delayed socket healing andincreased reduction in post-extraction alveolar width [67].Three trials in this review included smokers [21, 23, 43] andthe half of the studies did not report on smoking as anexclusion factor, thus any conclusions about the impact ofthis well-recognised risk factor for impaired healing aredifficult to draw [68].
Clin Oral Invest (2013) 17:341–363 359

Periodontal treatment/health
Four studies included patients whose periodontal treatmentwas carried out prior to the ARP [19, 21, 25, 48]. ARPresulted in statistically significant difference between testsand controls in clinical [21, 25] and in histological param-eters [21]. In addition, in the studies where periodontitis waspresent, but periodontal treatment was not reported, nostatistically significant histological differences were demon-strated [43, 44, 46]. This suggests that treated periodontitismay not hinder the success of ARP.
Hard and soft tissue morphology
No data were reported on factors, such as gingival biotype,width of the keratinised gingiva, thickness of buccal plate ortotal volume of AR that may modify the outcome of ARP.Therefore, the possible impact of these factors on ARPcannot be determined.
Clinical relevance
The clinical rationale for ARP is to minimise the necessityfor one or two stage alveolar ridge reconstruction to allowsuccessful implant placement. If the ARP procedure failsto meet this requirement, it may be considered as an un-necessary or even unsuccessful procedure. Therefore, astatistical significance favouring ARP does not necessarilylead to a clinical benefit, unless the whole treatment issimplified or made more successful [9]. In the presentsystematic review, seven out of ten studies did not reportdifferences in feasibility of implant insertion at re-entry[17, 19, 23, 42, 45, 46, 48]. Only two studies reported thatthere was no need for further reconstruction in the ARPgroup, whilst GBR or ridge expansion were carried out insome of the control sites alongside implant insertion [21,47]. One study reported that statistically significantly lessaugmentation had to be performed in the ARP group,compared to the control [20]. In relation to illuminatingthe understanding of possible long term benefits of ARP,the success rate of the inserted dental implants in theformer test, versus control sites should be examined. Nostudies have yet reported this.
Patient-reported outcome and health economics
It would be helpful to understand patient experiences suchas concomitant discomfort at/following ARP in order toavoid a further, extensive reconstructive surgery. On theother hand, the additional costs of ARP at the time ofextraction may not be desirable if the outcome and benefitof such extra treatment were not predictable. There are nodata yet to inform on these questions.
Conclusions
Within the limits of the above findings the following con-clusions can be drawn:
1. The results of the control groups confirm that toothextraction results in a statistically significant horizontaland vertical resorption of the AR, as part of the naturalremodelling.
2. The magnitude of the horizontal shrinkage is morepronounced than the vertical.
3. The resorption of the AR cannot be totally preventedby ARP.
4. Dimensional changes of the AR may be limited bysome of the ARP techniques.
5. No evidence was identified to inform on the possibleimpact of the following factors on ARP outcomes: (a)site location, (b) buccal plate thickness, (c) healingtime, (d) antibiotic regime, (e) light smoking, (f) his-tory of treated periodontitis.
6. The presence of intact socket walls and primary flapclosure are often associated with favourable results.
7. Conflicting evidence exists on the benefit of ARPat the histological level. ARP does not appear topromote de novo hard tissue formation routinely.In addition, some graft materials may interfere withhealing.
8. Due to the broad variety of employed materials, tech-niques, defect morphologies, healing periods, as wellas the relatively small sample sizes, meta-analysis orcomparative assessment of ARP cannot be made. Con-sequently no material or method can be claimed toserve superior to another. However, in certain casesGBR appeared to be most effective.
9. Only limited evidence supports the clinical benefit ofARP, namely the reduction of necessity of furtheraugmentation in conjunction with implant placement.
10. No evidence exists on comparison of the survival orsuccess rate of implants, placed in the former ARP orcontrol sites.
11. No evidence exists on cost-effectiveness, patient’spreference or quality of life following ARP.
12. The case selection criteria for performing ARP remainstill undetermined.
13. The strength of evidence ranges from weak to moder-ate and therefore, the conclusions of this review shouldbe interpreted with caution.
Recommendations for further research
& Randomised controlled trials on adequately poweredsample sizes are needed where unassisted socket healingserves as the negative control.
360 Clin Oral Invest (2013) 17:341–363

& Appropriate follow-up periods are required. Ideally, thisshould reflect implant insertion protocols, such as sixweeks (Type 2), three to four months (Type 3) or>6 months (Type 4) placement following extraction.
& Clinical studies should be designed to perform not onlyclinical (quantitative), but also histological (qualitative)assessment.
& The role of additional factors like smoking, reason forextraction, tooth location, initial buccal plate thickness,flap reflection and closure, antimicrobial regime shouldalso be investigated.
& Comparative studies should also be designed in order toidentify the most successful treatment options.
& It may be beneficial to seek for a cell occlusive barriermembrane that does not require extensive soft tissuemobilization for flap approximation.
& Necessity of re-augmentation at implant placementshould be investigated.
& Survival and success rates of implants, placed in formerARP sites should be evaluated.
& Outcome evaluation should ideally incorporate patient’spreference, quality of life, as well as treatment economy.
Acknowledgments The authors wish to express their gratitude toAviva Petrie for her invaluable contribution to the statistical assessment.
Conflict of interest and source of funding There was no known conflictof interest among the review team. The trial was self funded and supportedby the Research Discretionary Account of the Unit of Periodontology, UCLEastman Dental Institute. This work was undertaken at UCLH/UCL whoreceived a proportion of funding from the Department of Health’s NIHRBiomedical Research Centres funding scheme.
References
1. Schropp L, Wenzel A, Kostopoulos L, Karring T (2003) Bonehealing and soft tissue contour changes following single-toothextraction: a clinical and radiographic 12-month prospective study.Int J Periodontics Restor Dent 23:313–323
2. Amler MH, Johnson PL, Salman I (1960) Histological and histo-chemical investigation of human alveolar socket healing in undis-turbed extraction wounds. J Am Dent Assoc 61:47–58
3. AmlerMH (1969) The time sequence of tissue regeneration in humanextraction wounds. Oral Surg Oral Med Oral Pathol 27:309–318
4. Araújo MG, Lindhe J (2005) Dimensional ridge alterations follow-ing tooth extraction. An experimental study in the dog. J ClinPeriodontol 32:212–218
5. Boyne PJ (1966) Osseous repair of the postextraction alveolus inman. Oral Surg Oral Med Oral Pathol 21:805–813
6. Cardaropoli G, Araújo M, Lindhe J (2003) Dynamics of bonetissue formation in tooth extraction sites. An experimental studyin dogs. J Clin Periodontol 30:809–818
7. Claflin RS (1936) Healing of disturbed and undisturbed extractionwounds. J Am Dent Assoc 23:945–959
8. Albrektsson T, Brånemark PI, Hansson HA, Lindström J (1981)Osseointegrated titanium implants: requirements for ensuring along-lasting, direct bone-to-implant anchorage in man. ActaOrthop 52:155–170
9. Mardas N, Chadha V, Donos N (2010) Alveolar ridge preservationwith guided bone regeneration and a synthetic bone substitute or abovine-derived xenograft: a randomized, controlled clinical trial.Clin Oral Implants Res 21:688–698
10. Mardas N, D’Aiuto F, Mezzomo L, Arzoumanidi M, Donos N(2011) Radiographic alveolar bone changes following ridge pres-ervation with two different biomaterials. Clin Oral Implants Res22:416–423
11. Araújo M, Linder E, Lindhe J (2009) Effect of a xenograft on earlybone formation in extraction sockets: an experimental study in dog.Clin Oral Implants Res 20:1–6
12. Araújo MG, Lindhe J (2009) Ridge preservation with the use ofBio-Oss® collagen: a 6-month study in the dog. Clin Oral ImplantsRes 20:433–440
13. Fickl S, Zuhr O, Wachtel H, Bolz W, Huerzeler MB (2008) Hardtissue alterations after socket preservation: an experimental studyin the beagle dog. Clin Oral Implants Res 19:1111–1118
14. Fickl S, Zuhr O, Wachtel H, Kebschull M, Hurzeler MB (2009)Hard tissue alterations after socket preservation with additionalbuccal overbuilding: a study in the beagle dog. J Clin Periodontol36:898–904
15. Becker W, Becker BE, Caffesse R (1994) A comparison of demin-eralized freeze-dried bone and autologous bone to induce boneformation in human extraction sockets. J Periodontol 65:1128–1133
16. Becker W, Urist M, Becker BE, Jackson W, Parry DA, Bartold M,Vincenzzi G et al (1996) Clinical and histologic observations ofsites implanted with intraoral autologous bone grafts or allografts.15 human case reports. J Periodontol 67:1025–1033
17. Froum S, Cho SC, Rosenberg E, Rohrer M, Tarnow D (2002)Histological comparison of healing extraction sockets implantedwith bioactive glass or demineralized freeze-dried bone allograft: apilot study. J Periodontol 73:94–102
18. Artzi Z, Tal H, Dayan D (2000) Porous bovine bone mineral inhealing of human extraction sockets. Part 1: histomorphometricevaluations at 9 months. J Periodontol 71:1015–1023
19. Serino G, Biancu S, Iezzi G, Piattelli A (2003) Ridge preservationfollowing tooth extraction using a polylactide and polyglycolidesponge as space filler: a clinical and histological study in humans.Clin Oral Implants Res 14(5):651–658
20. Fiorellini JP, Howell TH, Cochran D, Malmquist J, Lilly LC,Spagnoli D et al (2005) Randomized study evaluating recombinanthuman bone morphogenetic protein-2 for extraction socket aug-mentation. J Periodontol 76:605–613
21. Barone A, Aldini NN, Fini M, Giardino R, Calvo Guirado JL,Covani U (2008) Xenograft versus extraction alone for ridgepreservation after tooth removal: a clinical and histomorphometricstudy. J Periodontol 79:1370–1377
22. Horvath A, Windisch P, Gera I (2010) Post-extraction site man-agement by a novel nanoporous polytetrafluoroethylene barrier.Clin Oral Implants Res 21(10):1121
23. Iasella JM, Greenwell H, Miller RL, Hill M, Drisko C, Bohra AAet al (2003) Ridge preservation with freeze-dried bone allograftand a collagen membrane compared to extraction alone for implantsite development: a clinical and histologic study in humans. JPeriodontol 74:990–999
24. Lekovic V, Kenney EB, Weinlaender M, Han T, Klokkevold P,Nedic M et al (1997) A bone regenerative approach to alveolarridge maintenance following tooth extraction. Report of 10 cases. JPeriodontol 68:563–570
25. Lekovic V, Camargo PM, Klokkevold PR, Weinlaender M, KenneyEB, Dimitrijevic B et al (1998) Preservation of alveolar bone inextraction sockets using bioabsorbable membranes. J Periodontol69:1044–1049
26. Heberer S, Al Chawaf B, Hildebrand D, Nelson JJ, Nelson K(2008) Histomorphometric analysis of extraction sockets
Clin Oral Invest (2013) 17:341–363 361

augmented with Bio-Oss Collagen after a 6-week healing period: aprospective study. Clin Oral Implants Res 12:1219–1225
27. Darby I, Chen S, De Poi R (2008) Ridge preservation: what is itand when should it be considered. Aust Dent J 53:11–21
28. Darby I, Chen ST, Buser D (2009) Ridge preservation techniquesfor implant therapy. Int J Oral Maxillofac Implants 24:260–271
29. Fiorellini JP, Nevins ML (2003) Localized ridge augmentation/preservation. A systematic review. Ann Periodontol 8:321–327
30. Fugazzotto PA (2005) Treatment options following single-rootedtooth removal: a literature review and proposed hierarchy of treat-ment selection. J Periodontol 76:821–831
31. John V, De Poi R, Blanchard S (2007) Socket preservation as aprecursor of future implant placement: review of the literature andcase reports. Compend Contin Educ Dent 28:646–653
32. Ten Heggeler JMAG, Slot DE, Van der Weijden GA (2011) Effectof socket preservation therapies following tooth extraction in non-molar regions in humans: a systematic review. Clin Oral ImplantsRes 22:779–788
33. Bianchi J, Fiorellini JP, Howell TH, Sekler J, Curtin H, Nevins MLet al (2004) Measuring the efficacy of rhBMP-2 to regeneratebone: a radiographic study using a commercially available soft-ware program. Int J Periodontics Restor Dent 24:579–587
34. Cranin AN, Ronen E, Shpuntoff R, Tobin G, Dibling JB (1998)Hydroxylapatite (H/A) particulate versus cones as post-extractionimplants in humans. Parts I & II. J Biomed Mater Res 22:1165–1180
35. Howell TH, Fiorellini J, Jones A, Alder M, Nummikoski P, LazaroM et al (1997) A feasibility study evaluating rhBMP-2/absorbablecollagen sponge device for local alveolar ridge preservation oraugmentation. Int J Periodontics Restor Dent 17:124–139
36. Schepers EJ, Ducheyne P, Barbier L, Schepers S (1993) Bioactiveglass particles of narrow size range: a new material for the repair ofbone defects. Implant Dent 2:151–156
37. Donos N, Mardas N, Chadha V (2008) Clinical outcomes ofimplants following lateral bone augmentation: systematic assess-ment of available options (barrier membranes, bone grafts, splitosteotomy). J Clin Periodontol 35:173–202
38. Needleman IG (2002) A guide to systematic reviews. J ClinPeriodontol 29:6–9
39. Needleman I, Suvan J, Moles DR, Pimlott J (2005) A systematicreview of professional mechanical plaque removal for preventionof periodontal diseases. J Clin Periodontol 32:229–282
40. Needleman I, Worthington HV, Giedrys-Leeper E, Tucker R(2006) Guided tissue regeneration for periodontal infra-bonydefects. Cochrane Database of Systematic Reviews Issue 2
41. Ong CT, Ivanovski S, Needleman IG, Retzepi M, Moles DR,Tonetti MS, Donos N (2008) Systematic review of implant out-comes in treated periodontitis subjects. J Clin Periodontol 35:438–462
42. Aimetti M, Romano F, Griga FB, Godio L (2009) Clinical andhistologic healing of human extraction sockets filled with calciumsulfate. Int J Oral Maxillofac Implants 24(5):902–909
43. Anitua E (1999) Plasma rich in growth factors: preliminary resultsof use in the preparation of future sites for implants. Int J OralMaxillofac Implants 14:529–535
44. Camargo PM, Lekovic V, Weinlaender M, Klokkevold PR,Kenney EB, Dimitrijevic B et al (2000) Influence of bioactiveglass on changes in alveolar process dimensions after exodon-tia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod90:581–586
45. Guarnieri R, Pecora G, Fini M, Aldini NN, Giardino R, Orsini G etal (2004) Medical grade calcium sulfate hemihydrate in healing ofhuman extraction sockets: clinical and histological observations at3 months. J Periodontol 75:902–908
46. Nevins M, Camelo M, De Paoli S, Friedland B, Schenk RK,Parma-Benfenati S et al (2006) A study of the fate of the buccal
wall of extraction sockets of teeth with prominent roots. Int JPeriodontics Restor Dent 26:19–29
47. Pelegrine AA, da Costa CES, Correa MEP, Marques JFC Jr (2010)Clinical and histomorphometric evaluation of extraction socketstreated with an autologous bone marrow graft. Clin Oral ImplantsRes 21:535–542
48. Serino G, Rao W, Iezzi G, Piattelli A (2008) Polylactide andpolyglycolide sponge used in human extraction sockets: boneformation following 3 months after its application. Clin OralImplants Res 19:26–31
49. Fenwick J, Needleman I, Moles D (2008) The effect of allocationconcealment and examiner blinding on outcome magnitude inperiodontology. J Clin Periodontol 35:775–782
50. Belser UC, Buser D, Hess D, Schmid B, Bernard JP, Lang NP(1998) Aesthetic implant restorations in partially edentulouspatients—a critical appraisal. Periodontol 2000 17:132–150
51. Buser D, von Arx T, ten Bruggenkate C, Weingart D (2000) Basicsurgical principles with ITI implants. Clin Oral Implants Res11:59–68
52. Garg AK, Vicari A (1995) Radiographic modalities for diag-nosis and treatment planning in implant dentistry. Implant Soc5:7–11
53. Quirynen M, Lamoral Y, Dekeyser C, Peene P, van Steenberghe D,Bonte J, Baert AL (1990) CT scan standard reconstruction tech-nique for reliable jaw bone volume determination. Int J OralMaxillofac Implants 5:384–389
54. Economopoulos TL, Asvestas PA, Matsopoulos GK, Molnár B,Windisch P (2012) Volumetric difference evaluation of registeredthree-dimensional preoperative and postoperative CT dental data.Dentomaxillofac Radiol 41:328–339
55. Van der Weijden F, Dell’Acqua F, Slot DE (2009) Alveolar bonedimensional changes of post-extraction sockets in humans: a sys-tematic review. J Clin Periodontol 36:1048–1058
56. Dragoo MR, Sullivan HC (1973) A clinical and histological eval-uation of autogenous iliac bone grafts in humans. I. Wound healing2 to 8 months. J Periodontol 45:599–613
57. Evian CI, Rosenberg ES, Coslet JG, Com H (1982) The osteogenicactivity of bone removed from healing extraction sockets inhumans. J Periodontol 53:81–85
58. Simion M, Baldoni M, Rossi P, Zaffe D (1994) A comparativestudy of the effectiveness of e-PTFE membranes with and withoutearly exposure during the healing period. Int J Periodontics RestorDent 14:166–180
59. Zitzmann NU, Schärer P, Marinello CP, Schüpbach P, Berglundh T(2001) Alveolar ridge augmentation with Bio-Oss: a histologicstudy in humans. Int J Periodontics Restor Dent 21:289–295
60. Araújo M, Linder E, Wennstrom J, Lindhe J (2008) The influenceof Bio-Oss Collagen on healing of an extraction socket: an exper-imental study in the dog. Int J Periodontics Restor Dent 28:123–135
61. Brkovic BMB, Prasad HS, Rohrer MD, Konandreas G, Agrogian-nis G, Antunovic D, Sándor GKB (2012) Beta-tricalcium phos-phate/type I collagen cones with or without a barrier membrane inhuman extraction socket healing: clinical, histologic, histomor-phometric and immunohistochemical evaluation. Clin Oral Invest16:581–590
62. Retzepi M, Donos N (2010) Guided Bone Regeneration: biologicalprinciple and therapeutic applications. Clin Oral Implants Res21:567–576, Review
63. Wikesjö UM, Xiropaidis AV, Thomson RC, Cook AD, Selvig KA,Hardwick WR (2003) Periodontal repair in dogs: rhBMP-2 signif-icantly enhances bone formation under provisions for guided tissueregeneration. J Periodontol 30:705–714
64. Wikesjö UM, Qahash M, Thomson RC, Cook AD, Rohrer MD,Wozney JM, Hardwick WR (2004) rhBMP-2 significantly enhan-ces guided bone regeneration. Clin Oral Implants Res 15:194–204
362 Clin Oral Invest (2013) 17:341–363

65. De Coster P, Browaeys H, De Bruyn H (2011) Healing of extrac-tion sockets filled with BoneCeramic(R) prior to implant place-ment: preliminary histological findings. Clin Implant Dent RelatRes 13:34–45
66. Lang NP, Schild U, Brägger U (1994) Effect of chlorhexidine(0.12 %) rinses on periodontal tissue healing after tooth ex-traction. (I). Clinical parameters. J Clin Periodontol 21:415–421
67. Saldanha JB, Casati MZ, Neto FH, Sallum EA, Nociti FH Jr(2006) Smoking may affect the alveolar process dimensions andradiographic bone density in maxillary extraction sites: a prospec-tive study in humans. J Oral Maxillofac Surg 64:1359–1365
68. Tonetti MS, Pini-Prato G, Cortellini P (1995) Effect of cigarettesmoking on periodontal healing following GTR in infrabonydefects. A preliminary retrospective study. J Clin Periodontol22:229–234
Clin Oral Invest (2013) 17:341–363 363

Ren E. WangNiklaus P. Lang
Ridge preservation after tooth extrac-tion
Authors’ affiliations:Ren E. Wang, Niklaus P. Lang, The University ofHong Kong, Prince Philip Dental Hospital,
Corresponding author:Prof. Niklaus P. Lang, DDS, MS, PhD, Dr, odont.hc.mult.The University of Hong Kong Faculty of DentistryPrince Philip Dental Hospital,34 Hospital Road, Sai Ying Pun, Hong Kong SARPR ChinaTel.: +852 2859 0526Fax: +852 2559 9013Mobile: + 41 79 301 5505e-mail: [email protected]
Conflicts of interest:The authors declare no potential conflicts.
Key words: bone substitutes, GBR, implant dentistry, membrane, ridge preservation, tooth
extraction
Abstract
Background: Following tooth extraction, the alveolar ridge will undergo dimensional changes.
This change may complicate the subsequent restorative procedure when oral implants are chosen.
“Alveolar ridge preservation” has been assessed in various studies.
Aim: To evaluate the more recent studies on this topic and to explore new insights under this
topic.
Material and methods: Animal studies and clinical studies have addressed different techniques.
Results and conclusions: Implants placed into the fresh extraction sockets do not prevent the
resorption of the alveolar bone. Simultaneous guided bone regeneration could partially resolve
alveolar bone resorption. The use of root-formed implants does not preserve alveolar ridges.
Moreover, various bone substitutes have been tested: magnesium-enriched hydroxyapatite, human
demineralized bone matrix, and deproteinized bovine bone mineral have been shown to be
effective in ridge preservation. Applying the guided bone regeneration principle using bone
substitutes together with a collagen membrane has shown clear effects on preserving alveolar
ridge height as well as ridge width. Soft tissue grafts or primary closure did not show beneficial
effect on preserving the alveolar bone.
Following tooth extraction, the alveolar ridge
will undergo structural changes. These
changes in extraction sockets were amply
demonstrated with histological observations
in dog studies (Cardaropoli et al. 2003). At
day 1 after extraction, the socket was occupied
by a coagulum; this coagulum was comprised
mainly of erythrocytes and platelets that were
trapped in a fibrous matrix. Immediately adja-
cent to the hard tissue wall was the “bundle
bone”, and principal fibers from periodontal
ligament (Sharpey’s fibers) could be found
invested in the bundle bone. These were also
in direct contact with the coagulum. At day
3, the coagulum had been replaced by a richly
vascularized granulation tissue. At day 7,
newly formed blood vessels were evident in
the primary matrix. Various types of leuko-
cytes and collagen fibers had taken the place
of the residual periodontal ligament as well as
the granulation tissue. At day 14, most of the
bundle bone had disappeared, and instead,
adjacent to the newly formed blood vessels,
“woven bone” started extending from the old
bone of the socket walls toward the center of
the socket. At day 30, woven bone underwent
resorption, suggesting that the remodeling
process had begun. At day 60, hard tissue
bridges separated the marginal mucosa from
the socket, and bone marrow replaced woven
bone at the center of the previous socket. At
day 90, woven bone was replaced by lamellar
bone. At days 120 and 180, most of the woven
bone had been replaced by lamellar bone.
The role of bundle bone in the dimensional
change in the alveolar ridge was investigated in
several dog studies (Araujo & Lindhe 2005;
Araujo et al. 2005) At 1 week after extraction
(Araujo & Lindhe 2005), the buccal bony crest
was 0.3 mm coronal to the lingual bony crest,
but at 2 weeks after extraction, the buccal crest
became 0.3 mm apical to the lingual crest.
This relative distance was increased to 0.9 and
1.9 mm at 4 and 8 weeks after extraction,
respectively. It was also observed that the cres-
tal region of the buccal bone wall was made up
exclusively of bundle bone, whereas the corre-
sponding region of the lingual bone was made
of a combination of bundle bone and lamellar
bone. Obviously, the function of bundle bone
is to anchor the tooth in the alveolar bone
through the invested periodontal ligament. As
the tooth is extracted, the bundle bonewill lose
its function, and subsequently, will resorb.
This may explain the more pronounced resorp-
tion of the buccal than the lingual bony crest.
Date:Accepted 03 July 2012
To cite this article:Wang RE, Lang NP. New insights into ridge preservation aftertooth extractionClin. Oral Implants Res. 23(Suppl. 6), 2012, 147–156doi: 10.1111/j.1600-0501.2012.02560.x
© 2012 John Wiley & Sons A/S 147

A recent systematic review evaluated the
dimensional changes in the hard and soft tis-
sues of the alveolar process up to 12 months
following tooth extraction (Tan et al. 2012).
It was concluded that after 3 months of
healing, the horizontal resorption of the
alveolar bone was 2.2 mm at the crest, and
1.3, 0.59, and 0.3 mm at 3, 6, and 9 mm api-
cal to the crest, respectively; after 6 months
of healing, the vertical resorption of the
alveolar bone was 11–22%, whereas the hori-
zontal resorption of the alveolar bone was 29
–63%. When soft tissue was included
together with the hard tissue in the dimen-
sional assessments at 3 months of healing,
there was even an increase of 0.4 mm in the
vertical dimension. At 12 months of healing,
the vertical resorption of the alveolar ridge
was 0.8 mm. Horizontally, the resorption of
the soft and hard tissue together was 1.3mm
and 5.1mm after 3 and 12 months of heal-
ing, respectively.
This vertical as well as horizontal dimen-
sional changes of the alveolar ridge may com-
plicate the subsequent restorative procedures
when dental implants are chosen. Over the
past 20 years, increasing interest has arisen
regarding a concept called “alveolar ridge
preservation”, which was defined as “any
procedure undertaken at the time of or fol-
lowing an extraction that is designed to mini-
mize external resorption of the ridge and
maximize bone formation within the socket”
(Darby et al. 2008). As suggested by that
review, studies promoting various techniques
have been performed. Most of the studies
included the measurements of dimensional
changes of the alveolar ridge after a ridge
preservation procedure.
The purpose of this review was to evaluate
these more recent studies and to explore new
insights under this topic. Within the context
of exploring new insights for ridge preserva-
tion, also studies of lower levels in the
evidence hierarchy may be of interest to shed
some light on the techniques designed to pre-
serve the alveolar ridge after tooth extraction.
These low evidence papers are generally case
series that combine various protocols. How-
ever, this approach, should lead to clinical
validation before recommendable for routine
clinical application.
Animal studies
Implants for ridge preservation
Immediate implants alone
A decade ago, it was proposed that “early
implantation may preserve the alveolar anat-
omy and that the placement of a fixture in a
fresh extraction socket may help to maintain
the bony crest structure” (Paolantonio et al.
2001). However, this statement has been
scrutinized later in a dog study (Araujo et al.
2005). In the right jaw of five dogs, implants
were placed into the fresh extraction sockets,
while in the left jaw, fresh sockets were left
for spontaneous healing. After 3 months of
healing, histological sections were obtained
to assess the distance from the SLA level to
the first bone-to-implant contact under
microscope. On the buccal aspect, this dis-
tance was 2.6 mm at implant sites and
2.2 mm at the corresponding extraction
socket sites. Hence, the immediate place-
ment of dental implants clearly failed to pre-
vent the resorption of the buccal bone walls.
To further study the modeling of the buc-
cal bony plate, the same group of researchers
designed another dog study (Araujo et al.
2006). In that study, the implants were
placed into the fresh extraction sockets in
the right jaw and 2 months later, the same
procedure was performed again in the left
jaw. Following another 1 month, the dogs
were sacrificed, and it was observed that after
1 month of healing, at the buccal aspect,
good osseointegration had been achieved
above the first thread of the implant. How-
ever, after 3 months of healing, the level of
this osseointegration had receded to below
the first thread as a result of the modeling of
the buccal bone. In the molar regions, the
degree of this modeling was much less
compared with the premolar regions, most
likely because of the wider original combined
defect and bone wall dimensions in the molar
regions. This study provided strong evidence
for the continued modeling process of the
buccal bony wall leading to buccal bone loss
despite the good osseointegration that had
already been achieved in early healing
phases. Obviously, this phenomenon was less
pronounced in sites with thicker buccal bony
walls. Again, immediate implant installation
failed to preserve the alveolar bone.
In a study aimed at observing bone-
to-implant contact of orthodontic implants
subjected to horizontal loading (Wehrbein
et al. 1998), immediately placed implants
with simultaneous horizontal loading
achieved better osseointegration than those
with delayed loading. Moreover, it was sug-
gested in another dog study that “a static
load may stimulate bone mineralization adja-
cent to titanium implants” (Gotfredsen et al.
2001). Finally, the hypothesis was tested
whether or not immediate implant place-
ment together with simultaneous loading
would help to preserve the buccal bone
(Blanco et al. 2011). In a dog model, two
implants were placed into the fresh extrac-
tion sockets at the premolar sites on each
side of the mandible. At the time of the
implantation, the implants on one side of the
jaw received a prosthesis with occlusal con-
tacts, while the implants on the other side
remained unloaded during the whole experi-
mental period. Three months later, the dogs
were sacrificed. The histomorphometric
results showed that the vertical distance
from the implant shoulder to the first bone-
to-implant contact was on average 3.66 mm
in the simultaneously loaded group and
4.11 mm in the unloaded group. This
difference was not statistically significant,
and hence it was concluded that “immediate
implant placement with or without loading
does not prevent bone resorption that occurs
following tooth extraction.”
Immediate implant with bone grafts
The effect of bone fillers (magnesium-
enriched hydroxyapatite) on preservation of
the alveolar bone around immediate implants
was evaluated in a dog study (Caneva et al.
2011). Implants with a sandblasted acid
etched surface (Zirti®, Sweden & Martina,
Due Carrare, PD, Italy) were placed into the
fresh extraction sockets bilaterally in the
dogs’ jaws. The margin of the rough surface
was placed at the level of the buccal bony
crest. On one side of the jaw, the bone filler
was applied into the gaps around the
implants. The contralateral sites were left
unfilled as controls. After 4 months of sub-
merged healing, the dogs were sacrificed. His-
tomorphometric evaluations showed that the
vertical distance from the junction between
rough and smooth surface to the buccal bony
crest was on average 0.7 mm in the group
with the bone filler and 1.2 mm in the
control group with no statistically significant
differences between the groups. Obviously,
the use of bone fillers around implants
immediately placed into extraction sockets
did not contribute significantly to the preser-
vation of the buccal bone. In a recent experi-
ment (Araujo et al. 2011), it has been
demonstrated that the use of Bio-Oss� col-
lagen as a bone substitute filler in the space
between the implant and the buccal bony
wall resulted in the prevention of buccal soft
tissue recession and a reduction in peri-
implant bone loss and allowed the buccal
bone to be thicker at the marginal level.
However, another similar animal study
(Favero et al. 2012) was not able to confirm
these differences in outcomes.
148 | Clin. Oral Implants Res. 23, 2012 / 147–156 © 2012 John Wiley & Sons A/S
Wang & Lang �Ridge preservation revisited

Immediate implant with GBR
In an AAP-commissioned review on bone
augmentation techniques, it was recom-
mended that immediate implant placement
together with GBR techniques may yield out-
comes comparable to delayed placed implants
(McAllister & Haghighat 2007). Recently,
a dog study was conducted to evaluate the
influence of absorbable membranes on hard
tissue alterations around the immediately
placed implants (Caneva et al. 2010a,b,c).
Implants with a rough surface (zirconium
sandblasted acid etched) were placed immedi-
ately following extraction on both sides of
the mandibles, on the test side of the jaw,
collagen resorbable membranes were placed
to cover the implants. On the control side of
the jaw, the implants were left without
membranes.
After 4 months of intended submerged
healing, all implants were found exposed to
the oral cavity because of soft tissue dehi-
scences. The dogs were sacrificed and biop-
sies were obtained. The distance between the
most coronal margin of the implant and the
bone crest were measured. At the buccal
aspect, this distance was 1.7 mm on the
implants placed with GBR procedures, and
2.2 mm on the implants placed without
GBR, and this difference was statistically sig-
nificant. At the lingual aspect, this distance
was 0.6 and 0.4 mm on the test sites and
control sites, the difference not reaching sta-
tistical significance. There was no difference
between the groups regarding the level of
first bone-to-implant contact and the percent-
age of bone-to-implant contact. This study
provided evidence that the use of collagen
resorbable membranes at immediate implant
sites contributed partially (23%) to the pres-
ervation of the buccal bony wall.
Further studies of the same group of
researchers (Caneva et al. 2011, 2012)
explored the effect of GBR based on deprotei-
nized bovine bone mineral on alveolar ridge
preservation and the reparation of defects
around osseointegrated implants. After
hemi-sectioning the third mandibular premo-
lars and extracting the distal roots, a recipi-
ent site was prepared for an implant. This
was placed lingually, leaving a defect of
about 0.6mm in width and 3mm in depth at
the buccal aspect. While the other side of
the jaw was used as control without GBR,
deproteinized bovine bone mineral (DBBM)
was place into the defects of the test site and
covered with a collagen membrane. This
treatment contributed to improved bone
regeneration in the defects. However, regard-
ing the buccal bony crest preservation only a
limited contribution of DBBM particles was
obtained (Caneva et al. 2011).
In the second study on the same material
the dimensional changes of the alveolar bony
crest following the placement of DBBM parti-
cles into sockets immediately after tooth
extraction, in conjunction of the placement
of a collagen membrane, were addressed
(Caneva et al. 2012). After 4 months of heal-
ing, no differences in soft tissue dimensions
were found based on histological evaluations.
Yet, the location of the soft tissue at the buc-
cal aspect was more coronally at the test
compared to the control sites. Hence, it was
concluded that the application of DBBM con-
comitantly with the placement of a collagen
membrane at implant sites placed in the
socket immediately after tooth extraction
contributed positively to the preservation of
the alveolar process.
In a similar study recently published (Park
et al. 2011), immediate implants (Institute
Straumann AG, Basel, Switzerland) were
placed bilaterally in the dogs’ jaws in the pre-
molar region. On the experimental side, a
non-resorbable ePTFE membrane (Tefgen®,
Lifecore Biomedical, Chaska, MN, USA) was
placed on the buccal plate of the implant
sites without coverage of the bone crest and
was fixed with mini screws. In the control
site, no membrane was placed. After
3 months of non-submerged healing, no
membrane exposure occurred. The dogs were
sacrificed and after histometric observation,
the vertical distance from the rough and
smooth surface interface to the buccal bone
crest was on average 1.72 mm in the control
group and 0.92 mm in the experimental
group. This difference was statistically signif-
icant. Moreover, at the level 2 mm below the
buccal bony crest, the mean thickness of the
buccal bone walls was 0.4 mm in the control
group and 1.49 mm in the test group. Again,
this difference was statistically significant.
From the above two animal studies, it
appeared that the outcomes of using non-
resorbable ePTFE membranes is superior to
that achieved by resorbable collagen mem-
branes. It should be realized that the tech-
niques applied in the two studies were
different. In the first study, the resorbable
collagen membranes were placed on top of
the implants without fixation, and primary
closure was achieved at the completion of
the surgery. However, during the healing per-
iod, all implants were exposed because of soft
tissue dehiscences. In the later study, the
non-resorbable membrane was placed on the
buccal bone wall and fixed with mini screws
to avoid membrane exposure. The mem-
branes were placed below the buccal bony
crests, and no primary closure was intended,
which meant that the flaps healed without
tension. Consequently, membrane exposure
was absent during healing.
Shape of implants and implant positioning
Tapered or root-formed implants were
designed to reduce the gaps around implants
that were placed immediately into the fresh
extraction sockets, thus filling the defect par-
tially with titanium. The question arises if
this type of implant design will help in pre-
venting alveolar bone resorption around such
implants. In a split-mouth design, mandibles
of dogs received cylindrical implants 3.3 mm
in diameter (Premium®, Sweden & Martina,
Due Carrare, PD, Italy) immediately after
tooth extraction (control) (Caneva et al.
2010c). A similar procedure was carried out
with root-formed implants 5 mm in diameter
(Kohno®, Sweden & Martina, Due Carrare,
PD, Italy) on the test sites. After 4 months of
non-submerged healing, the dogs were sacri-
ficed and histomorphometric evaluations
were performed. The mean vertical buccal
bone resorption was significantly greater in
the test group (2.7 mm) than in the control
group (1.5 mm). In essence, the filling of gaps
with root-formed implants failed to preserve
the buccal bone. On the contrary, the bone
resorption was more pronounced around the
root-formed immediate implants that filled
the extraction socket to a greater extent than
did the cylindrical implants. The root-formed
implants with a wider diameter occupied the
entire socket, leaving no space between the
implant and the buccal bony wall. In other
words, the implant body was located closer
to the outer surface of the buccal bony wall.
Consequently, a greater portion of the
implant was exposed in the supracrestal
region after modeling and remodeling pro-
cess, as the distance between the implant
outline and the outer surface of the buccal
bone appears to be a crucial factor for the
preservation of the buccal bone.
To evaluate the influence of implant posi-
tioning into extraction sockets on the main-
tenance of the buccal bone level (Caneva
et al. 2010a), implants (Premium®, Sweden &
Martina, Due Carrare, PD, Italy) were placed
in the center of the sockets in control sites
of mandibles, whereas in the test sites, the
same implants were placed 0.8 mm deeper
and more lingually. After 4 months of non-
submerged healing, the histometric evalua-
tions showed that the mean vertical distance
from the rough and smooth surface interface
to the buccal bone crest was significantly less
© 2012 John Wiley & Sons A/S 149 | Clin. Oral Implants Res. 23, 2012 / 147–156
Wang & Lang �Ridge preservation revisited

in the test group (0.6 mm) compared with
the control group (2 mm). Hence, the posi-
tion of the implant had a greater impact on
the preservation of the buccal bone resorp-
tion than the shape of the implant.
Bone substitutes
Bone substitutes alone
The effectiveness of ridge preservation with
bone grafting in the extraction sockets alone
was evaluated in a dog study (Boix et al.
2006). The maxillary and mandibular premo-
lars were extracted. The sockets of the distal
roots were filled with an injectable bone sub-
stitute (a polymer solution and granules of a
biphasic calcium phosphate ceramic), and the
sockets of the mesial roots were left unfilled
as controls. Primary closure was achieved by
overlapping hermetic sutures. After 3 months
of healing, a tangent vector was drawn con-
necting the buccal and lingual crests, and the
distance from the highest point of the alveo-
lar ridge and this tangent vector was mea-
sured. There was a significant difference
between the groups in the mandible (0.5mm
and �0.4mm in test and control, respectively)
and the maxilla (�0.3 and �0.5 in the test
and control, respectively).
In another dog study (Shi et al. 2007), man-
dibular premolars and molars were extracted,
the extraction sockets on the test side were
treated with Surgical-Grade Calcium Sulfate
(SGCS) + platelet-rich plasma (PRP) or with
SGCS alone. On the control side, the sockets
were left unfilled. Primary closure was
achieved by periosteal releasing incisions and
coronally advanced flaps. At baseline and
2 months after healing, CT scans were taken.
Alveolar bone height was assessed on CT
scans as the distance from the midpoint of
the cortical bone to the inferior border of the
mandible. It was found that the reduction in
the ridge height was significantly greater in
the control group compared with the test
group (2.77, 1.39 mm, respectively), although
no difference was found between SGCS +
PRP treatment and SGCS treatment alone.
In five beagle dogs (Fickl et al. 2008a,b),
the 3rd and 4th mandibular premolars were
extracted. In the test sites, the sockets were
filled with Bio-Oss® collagen (Geistlich
Biomaterials, W olhusen, LU, Switzerland).
The collagen was fixed with sutures. The
control sites were left untreated. After
4 months of healing, the histomorphometric
evaluation documented a mean vertical buc-
cal bone loss that was significantly lower in
the test (2.8 mm) than in the control sites
(3.2 mm). At 1 mm below the crest, the
untreated group had a significantly narrower
ridge width than the test group (3.7 mm vs.
4.4 mm). However, at 3 mm/5 mm below
the crest, the ridge width was similar
between the groups. Using digital image anal-
ysis on study casts for the same material
(Fickl et al. 2008a,b) at the buccal aspect, the
volumetric differences from baseline to after
4 months of healing was significantly greater
in the control group (-2.2mm) than the test
group (-1.5mm). These results showed small
benefits toward using Bio-oss® collagen.
A similarly designed study (Araujo & Lind-
he 2009) compared sockets healing without
treatment (control) and sockets treated with
Bio-oss® collagen (test). Flaps were coronally
replaced and primary closure was achieved in
both types of sockets. After 6 months of
healing, biopsies were obtained. Histometric
analysis revealed that the dimensional
changes in the apical and middle portion of
the sockets were moderate in both sites, but
in the coronal portion, the ridge width reduc-
tion was three times greater in the control
sockets (�35%) compared with the test sock-
ets (�12%). However, the composition
between two sites was similar. The xenograft
(Bio-Oss®, Geistlich Biomaterials, W olhusen
LU, Switzerland)) only served as a scaffold and
did not stimulate new bone formation.
Another histometric study (Rothamel et al.
2008) compared sockets treated by Nanocrys-
talline hydroxyapatite paste (test) with un-
filed sockets (control). Primary closure was
achieved in both groups. After 3 and
6 months of healing, the dogs were sacrificed.
Histometric analysis on lingual and buccal
bone height, alveolar wall, and total bone
width showed no difference for any parame-
ters between groups. It could be concluded
that Nanocrystalline hydroxyapatite paste
does not appear to be effective for ridge pres-
ervation.
Xenografts versus autografts
For many years, the use of autologous bone
was regarded as a “gold standard” for augmen-
tation procedures. To evaluate its efficacy in
ridge preservation, a dog study was conducted
(Araujo & Lindhe 2011). Extraction sockets in
the mandibles of dogs were filled with either
anorganic bovine bone or autogenous bone
chips. After 3 months of healing, a histomet-
ric analysis was performed. The cross-sec-
tional area of the ridge alteration was
estimated by subtracting the cross-sectional
ridge area identified after extraction from the
corresponding area at the adjacent root. In the
apical and middle portions of the sockets, no
resorption was observed. However, in the
coronal portions, the ridge underwent resorp-
tion (�25%) in the autogenous bone graft
group. In the xenograft group, there was a posi-
tive change (3.6%). The residual grafting mate-
rial was found to be 24.4%. Non-vital
autogenous bone chips were found to be 1.9%.
It seemed that autologous bone did not pre-
serve the alveolar ridge.
Primary flap closure
Soft tissue grafts versus no soft tissue grafts
In five beagle dogs, the 3rd and 4th mandibu-
lar premolars were extracted (Fickl et al.
2008a). In the test group, the sockets were
filled with Bio-oss® collagen, and free gingi-
val grafts were obtained to cover the sockets.
The control sites were also filled with
Bio-oss® collagen (Geistlich Biomaterials, W
olhusen, LU, Switzerland). The collagen was
fixed with sutures, but no soft tissue grafts
were applied. After 4 months of healing, the
histomorphometric evaluation showed a
mean vertical buccal bone loss that was sig-
nificantly lower in the control group
(2.8 mm) than in the test group (3.3 mm). At
1mm below the crest, the control group had
significantly narrower ridge width than the
test group (4.4 mm vs. 4.8 mm). But at
3 mm/5 mm below the crest, the ridge width
was similar between the test and control
groups. In another study digital image analy-
sis on study casts from the same material
(Fickl et al. 2008b), the remodeling process at
the buccal aspect from baseline to after
4 months of healing was similar between the
control and test groups (�1.5 mm vs. �1.6
mm). These results, therefore, indicate the
need for further human research using free
gingival grafts to obtain primary closure for
alveolar ridge preservation in well preserved
alveoli.
Clinical trials
Implants for ridge preservation
Immediate implants alone
To observe the alteration of hard tissues fol-
lowing tooth extraction and immediate
implant placement, a clinical study was con-
ducted (Botticelli et al. 2004). In 18 patients,
21 SLA surface implants were placed. After
4 months of non-submerged healing without
loading, a re-entry surgery was performed.
The differences between the clinical mea-
surements made before implant placement
and after 4 months of healing yielded a hori-
zontal resorption of the buccal bone of about
56%. The corresponding resorption of the lin-
150 | Clin. Oral Implants Res. 23, 2012 / 147–156 © 2012 John Wiley & Sons A/S
Wang & Lang �Ridge preservation revisited

gual/palatal bone was 30%, whereas the ver-
tical bone resorption was on average 0.3 mm
at the buccal aspect and 0.6 mm at the lin-
gual/palatal aspect. This amount of resorp-
tion is very similar with the resorption at
human alveolar ridges after extraction
reported recently in a systematic review (Tan
et al. 2012). This, in turn, means that
implants immediately placed into extraction
sockets, also in humans, do not prevent the
resorption of the alveolar bony ridge.
Immediate implant with bone GBR
The effect of membrane placement in con-
junction with or without bone substitutes for
preserving the alveolar bony around implants
immediately placed into extraction sockets of
the anterior region (Chen et al. 2007) was
studied in 30 patients that randomly received
immediate implants (SLA surface, Institute
Straumann AG, Basel, Switzerland) with Bio-
oss® + collagen membrane (Geistlich Bioma-
terials, W olhusen, LU, Switzerland), Bio-oss®
alone, or were left un-grafted. The dimen-
sions of the alveolar bony crest were assessed
at baseline and at the re-entry surgery after
6 months of healing. The implants were
loaded after further 2 months, and the
patients were followed up to 3 years after
completion of restoration delivery. Standard-
ized peri-apical radiographs and peri-implant
examinations were performed every year. At
the re-entry surgery, there was no significant
difference between the groups on the vertical
and horizontal defect reduction around the
implants. On the other hand, the reduction
in the horizontal distance from the outer sur-
face of the buccal bony ridge to the implant
surface was significantly greater in the con-
trol group (48.3 ± 9.5%) than in the bone
graft alone group (15.8 ± 16.9%) and the bone
graft with membrane group (20 ± 21.9%).
During the 3-year post-restorative follow-up,
all patients kept excellent oral hygiene. No
difference was found regarding the peri-
implant or radiographic parameters between
baseline and 1-year/3-year follow-ups or
among the groups. This clinical study dem-
onstrated that the bone defect around the
immediately placed implants will heal pre-
dictably irrespective of the usage of mem-
branes or bone grafts. However, the
membrane or bone graft treatment may
reduce the horizontal resorption of the buccal
bony plate by 25% of the original dimension.
Another clinical study was performed in
the molar region, to examine the alteration
of the alveolar bony ridge around implants
immediately placed into molar extraction
sockets after 6 months of healing (Matarasso
et al. 2009); 12 immediate transmucosal
implants with an sandblasted acid etched
surface were placed in 12 patients. GBR was
performed by placing a resorbable collagen
membrane supported by a bone substitute
(Bio-oss®). The alveolar bone dimensions
around the implants were assessed at the
time of implant surgery and at the re-entry
surgery after 6 months of healing. The gaps
around the implants healed as expected.
However, the horizontal distance from the
outer surface of the alveolar ridge to the
implant surface at the buccal aspect was
reduced by 58% on average. Unfortunately,
no control group was provided in this study.
An interesting aspect of this study was the
influence of bone thickness on the buccal
bone resorption. If the buccal bony wall was
initially 1-mm thick, the buccal bone resorp-
tion was as high as 52%. However, when the
buccal bone wall was initially 2-mm thick,
the buccal bone resorption was significantly
reduced to 33%.
Shape of implants and implant positioning
As one of the proposed benefits of using root-
formed implants was to avoid the need for
bone augmentation, a multi-center random-
ized controlled clinical trial was conducted to
test this hypothesis (Lang et al. 2007). In nine
centers, 216 patients received either cylindri-
cal or tapered implants (Institute Straumann
AG, Basel, Switzerland) installed into the
extraction sockets in non-molar regions. Dur-
ing the surgery, the type of implants was allo-
cated at random and the need for guided bone
regeneration was assessed. Whenever the gap
around the implants was more than 0.5 mm
or whenever buccal bony plate was thin (less
than 1 mm), augmentation procedures were
performed. Questionnaires were given to both
patients and the operators to assess the prefer-
ence to these two types of implants. The
results revealed that 90% of both implant
designs required GBR procedures. Patient-
reported outcomes did not show any prefer-
ence toward any type of the implants. How-
ever, the surgeons’ perception was in favor of
the tapered implants. Therefore, it is evident
that root-formed implants do not offer an
advantage in the need for avoiding GBR
procedures.
Another multi-center study aimed to a com-
parison of the dimensional bony changes
around the two types of implants (Sanz et al.
2010). The hypothesis of the study was that,
by providing more space for the coagulum
around the implants, the cylindrical implants
(test) should have a positive effect in preserv-
ing the alveolar bone and to reduce the hori-
zontal bone resorption by 20% when
compared with the tapered implants (control).
In three centers, 93 patients were included in
the study. Forty-five cylindrical implants
(Astra Tech AB, Molndal, Sweden) were
installed into extraction sockets in the test
group, and 48 tapered implants (Astra Tech
AB, Molndal, Sweden) were placed in the con-
trol group. At baseline and at the re-entry sur-
gery after 4 months healing, the results
indicated that there was a marked reduction
in the distance from the outer surface of the
ridge to the implant in both groups (43% and
30%, respectively), although this difference
was not statistically significant. Once again, it
was evidenced that tapered implants cannot
preserve the alveolar bony ridge. On the con-
trary, tapered implants were associated with
more bone resorption.
Non-surgical treatment
Ultrasonic non-surgical treatment
The effect of ultrasonic application on bone
healing has been studied in the orthopedic lit-
erature. In vitro experiments showed a signifi-
cant influence of ultrasound on the
proliferation of mandibular osteoblasts. Clini-
cal evidence has also demonstrated that ultra-
sound treatment may accelerate the healing
process of tibial diaphysis fractures by 38% in
time (Kerr et al. 2008). In a randomized con-
trolled split-mouth clinical trial, 12 patients
who were scheduled for tooth extraction on
both sides of the jaw were enrolled. At 7–
10 days following extraction, ultrasound ther-
apy was delivered on the alveolar ridge of the
test site for 20 min using a piezoelectric
transducer for 10 sessions over the subsequent
4 weeks. Standardized cone-beam volumetric
tomography (CBVT) scans were acquired at
baseline (7–10 days post extraction), comple-
tion of ultrasound therapy (4 weeks after ther-
apy), and 3 months post extraction.
Dimensional changes of the buccal and lin-
gual bony plates were analyzed through
CBVT. However, given the limitations of
small sample size and a short observational
period with CBVT scans in this study, no sig-
nificant differences could be found in absolute
bony dimensional changes.
Bone substitutes
Bone fillers alone
In a randomized controlled clinical trial (Nei-
va et al. 2008), the effectiveness of an
anorganic bovine-derived hydroxyapatite
matrix delivered in a putty-form combined
with a synthetic cell-binding peptide P-15
© 2012 John Wiley & Sons A/S 151 | Clin. Oral Implants Res. 23, 2012 / 147–156
Wang & Lang �Ridge preservation revisited

(Putty P15) on ridge preservation was investi-
gated. Comparisons were made between
untreated control sockets and sockets treated
with this putty-form matrix (test). Collagen
dressing material was applied in both groups.
After 4 months of healing, at the re-entry
surgery, no difference was found between the
groups in ridge width reduction (�1.31 and
�1.43mm in test and control, respectively).
However, significantly less ridge height
reduction was found in the test group
(0.15 mm) compared with the control group
(�0.56 mm). The bone density assessed dur-
ing implant surgery was found significantly
higher in the test group as well.
Another biomaterial, medical-grade calcium
sulfate hemihydrates (MGCSH) was evaluated
in a randomized controlled clinical trial (Ai-
metti et al. 2009). In the test group, 22
patients received this material in their sock-
ets. As control group, 18 patients did not
receive any treatment after extraction at all.
Clinical measurements were performed at
baseline and at the re-entry surgery (implant
surgery). After 3 months of healing, signifi-
cantly greater reduction in ridge height was
found in the control group (1.2 mm) compared
with test group (0.5 mm). Moreover, signifi-
cantly greater ridge width reduction was found
in the control group (3.2 mm) compared with
the test group (2.0 mm). A histological analy-
sis also found less lamellar bone and more
woven bone in the control group.
Two new materials were evaluated in a
split-mouth clinical trial (Crespi et al. 2009).
In 15 patients, three teeth were extracted in
each patient. One of the sockets was treated
with magnesium-enriched hydroxyapatite
(Test 1). Another socket was treated with
Calcium sulfate (Test 2). The third socket
was left unfilled (control). The filling materi-
als in the two test groups were secured with
a collagen sheet covering and sutures to affix
the membrane. Applying standardized intra-
oral radiographs obtained at baseline and
3 months later at the re-entry surgery, signif-
icant differences in ridge height reduction
was found among all groups (�0.48, �2.48,
and �3.75 mm in the Test 1, Test 2, and
control group, respectively). In histological
analyses, the amount of vital bone was found
to be significantly different among all groups
(40.0, 45.0, and 32.8% in the Test 1, Test 2,
and control group, respectively). The amount
of connective tissue was not different
between the test groups, but it was signifi-
cantly different between the test and control
groups. Significantly, less residual grafting
material was found in sockets treated with
Calcium sulfate. Based on this study, magne-
sium-enriched hydroxyapatite was found to
be more useful in alveolar ridge preservation
than calcium sulfate.
In a recent clinical split-mouth design
study (Fernandes et al. 2011), sockets treated
with anorganic bovine bone matrix (ABM)
+ synthetic cell-binding peptide P-15 (Test)
were compared with unfiled sockets (control).
The sockets in both groups were covered
with Acellular dermal matrix (ADM). Clini-
cal measurements were made at baseline and
after 6 months of healing. No statistically
significant differences could be found on
ridge height reduction between the groups
(1.5 and 1.2 mm in the control and test
groups, respectively). But the ridge width
resorption was significantly greater in the
control (3.40 mm) compared with the test
group (2.52 mm).
The effectiveness of an allograft material
in ridge preservation was recently tested in a
randomized controlled clinical trial (Brown-
field & Weltman 2012). Twenty patients
were divided into two groups. The extraction
sockets in the test group were treated with
an allograft paste composed of “osteoinduc-
tive” demineralized bone matrix and cancel-
lous bone chips, and the sockets in the
control group were left unfilled. The sockets
in both groups were covered with an absorb-
able collagen wound dressing. No significant
difference on ridge resorption was found
between the two groups as studied by CBCT/
Micro CT and histological analysis, although
CBCT analysis found a significant correlation
between initial buccal bony plate thickness
and loss of ridge height.
Different particle size
In general, smaller particles of bone substi-
tutes are preferred because they may be
resorbed more rapidly. They may enhance
osteogenesis because of a greater surface area.
On the other hand, the optimal particle size
may depend on the bony defect to be grafted.
Extraction sockets may benefit more using
larger particles, as the sockets are usually lar-
ger than the periodontal defects.
To elaborate on the most appropriate parti-
cle size to be used in extraction sockets, a
randomized controlled clinical trial was
conducted (Hoang & Mealey 2012) in 20
patients. One molar was extracted in each
patient. The sockets were either filled with
human demineralized bone matrix (DBM)
putty with a single particle size (2–4 mm) or
with multiple particle sizes (125–710 lm).
Clinical assessments of the ridge dimensions
were made at baseline and at re-entry surgery
after 4–5 months of healing. No difference
was found on ridge width reduction between
the single particle size group (1.4 mm) and
multiple particle size group (1.3 mm). The
vertical buccal and lingual bone loss was less
than 0.5 mm in both groups. Histological
analysis did not find any difference between
the groups. Obviously, ridge preservation
using this grafting material irrespective of its
particle sizes was effective.
Demineralized allografts versus mineralized allografts
Although both demineralized freeze-dried
bone allograft (DFDBA) and mineralized
freeze-dried bone allograft (FDBA) are claimed
to be osteoconductive; only DFDBA has been
proven to be osteoinductive. Both DFDBA
and FDBA contain bone morphogenic pro-
teins (BMP). As the process of demineraliza-
tion facilitates the release of soluble factors
like BMP, evidence suggested that a maxi-
mum of osteoinduction was observed when
there was approximately 2% residual calcium
in DFDBA. However, FDBA may serve as a
superior scaffold compared with DFDB for
space maintenance and may also be more os-
teoconductive. When osteoclasts break down
the mineral content in FDBA until it is also
demineralized, there could be a prolonged os-
teoinductive effect. To evaluate the clinical
effectiveness of these two materials on ridge
preservation, a randomized controlled clinical
trial was performed (Wood & Mealey 2011).
Forty patients were randomly allocated into
two groups. The extraction sockets of the
patients were filled with FDBA or DFDBA,
respectively. All grafting materials were
obtained from a single donor. Clinical mea-
surements were performed at baseline and at
re-entry surgery after 4–5 months of healing.
No difference between the groups was found
on ridge height reduction (1 mm in both
groups) or ridge width reduction (2 mm in
both groups). However, histological analysis
yielded that the vital bone content was signif-
icantly higher in the DFDB group (38.42% vs.
24.63%), while the residual graft content was
significantly lower in DFDBA group (8.88%
vs. 25.42%). Although DFDBA may seem to
be more osteoinductive, its effect on ridge
preservation is similar to that of FDBA.
Synthetic bone substitutes versus xenografts
Bone Ceramic® is a biphasic ceramic bone
substitute. It is composed of a combination
of hydroxyapatite (HA) and b-tricalcium
phosphate (b-TCP). HA is insoluble.
Although it is well tolerated in bone, its os-
teoconductive properties have been ques-
tioned. To be osteoconductive, the material
should leave space for new bone to be depos-
152 | Clin. Oral Implants Res. 23, 2012 / 147–156 © 2012 John Wiley & Sons A/S
Wang & Lang �Ridge preservation revisited

ited. Unlike HA, b-TCP is soluble. When it
slowly resorbs, it is replaced by new bone.
The objective of combining the insoluble HA
with b-TCP, therefore, is that HA would
maintain the space (scaffold function), while
the b-TCP would resorb and promote new
bone formation.
A randomized controlled clinical trial was
conducted to compare the ability of preserving
alveolar ridges with this synthetic material
(Bone Ceramic®,Institute Straumann AG,
Basel, Switzerland) and a xenograft material,
deproteinized bovine bone mineral (DBBM)
(Mardas et al. 2010). Thirty patients were ran-
domly assigned to two groups. One non-molar
tooth in each patient was extracted, and the
sockets in one group were filled with Bone
Ceramic®, whereas in the other group, the
sockets were filled with DBBM. A resorbable
bi-layer collagen membrane was applied to
cover each socket. Flaps were coronally
advanced to close the wound as well as possi-
ble. Clinical assessments on ridge dimensions
were made at baseline and at re-entry surgery
after 8 months of healing. The reduction in
the ridge width was significantly less in the
Bone Ceramic® group (�1.1 mm) than in
DBBM group (�2.1 mm). The reduction in the
ridge height was negligible in both groups.
Both materials partially preserved the width
and interproximal bone height of the alveolar
ridge. Bone Ceramic® achieved a better out-
come in preserving the alveolar ridge. In a
clinical study (De Coster et al. 2011), whereby
bone regeneration in healing extraction sock-
ets substituted with Bone Ceramic� was com-
pared with unfilled sockets, biopsies were
obtained from the sites during later performed
implant bed preparation. Healing was evalu-
ated using transmitted light microscopy after
6–74 weeks (mean 22 weeks). 15 Bone cera-
mic� sites were compared with 10 naturally
healed sockets. During implant placement it
was clinically observed that bone at the sub-
stituted sites was softer than in control sites
and large amount of loose biomaterial were
found requiring thorough debridement. Con-
sequently, some of the recipient beds were too
large to get normal diameter implants initially
stable. Hence, wider implants were necessary,
and in 4 substituted sites, implants could not
be installed at all. Additionally, it was
reported that 2 out of ten implants installed in
substituted sockets failed within 3 months
after insertion. The histology showed that 5/
15 substituted sites showed clearly incom-
plete healing. Overall, new bone formation
was consistently poorer than in controls and
presented with predominantly loose connec-
tive tissue and less woven bone. The grafting
material appeared to interfere with the normal
healing process. Hence, using this material for
crestal bone preservation when implants are
considered, even after long healing time,
should be revised and based on additional
scientific studies.
Collagen plugs
Ideally, ridge preservation procedures should
be easy and should not involve additional
surgery. The use of collagen plug was intro-
duced, as it has the mentioned advantages.
To test its effectiveness on preserving alveo-
lar ridges, a randomized controlled clinical
trial was conducted (Kim et al. 2011).
Twenty patients were divided into two
groups. After the extraction of one molar in
each patient, the sockets in one group were
grafted with Bio-oss® and a collagen plug.
Sutures were applied to fix the material. The
sockets in the other group were left unfilled
as controls. Study casts were obtained imme-
diately at baseline and after 3 months of
healing. Assessments of the bony height and
ridge width were performed. After calcula-
tion, the average resorption rate of the bone
height was 6.8% in the control group and
5.8% in the test group. There was no signifi-
cant difference between the groups. The aver-
age resorption rate of the alveolar ridge width
at 3 mm below the crest was 20.7% in the
control group and 14.3% in the test group.
Although this technique may be advanta-
geous in preserving the alveolar ridge, no def-
inite recommendations may be made.
Collagen plugs with soft tissue grafts
To evaluate the effectiveness of a collagen
plug together with soft tissue graft on ridge
preservation (Oghli & Steveling 2010), 125
patients were divided into three groups. After
tooth extraction, the sockets were treated
with either a cone comprised of collagen (Test
1), a cone comprised of collagen and impreg-
nated with gentamicin (Test 2), or left unfilled
(control). In the two test groups, soft tissue
grafts were harvested from the palate, and the
sockets were covered with the sutured grafts.
Study casts were obtained at baseline and after
3 months of healing. Assessments of the verti-
cal dimension of the alveolar ridge were made
on the casts. No difference was found among
the three groups on vertical ridge resorption
(0.8, 0.1, and 0.3 mm in Test 1, Test 2, and
control groups, respectively). However, cau-
tion should be taken while interpreting these
results. While using study casts to measure
the ridge dimensions, soft and hard tissue
alterations are included as indicated in a sys-
tematic review (Tan et al. 2012). Soft tissue
may increase in dimension to partially com-
pensate the hard tissue resorption, especially
in vertical direction. Hence, the assessment of
study casts may not be appropriate to evaluate
the effectiveness of ridge preservation proce-
dures.
Guided Bone Regeneration (GBR)
Ridge preservation with or without GBR
A cohort study was performed to follow 30
patients who received ridge preservation pro-
cedures with resorbable b-TCP of small parti-
cle size and resorbable collagen barriers after
tooth extraction (Horowitz et al. 2009). Eval-
uating clinically the alveolar ridge width at
baseline and at re-entry surgery 6 months
later, a mean reduction in the ridge width of
12.4% was reported. Although there was no
control group, it could be estimated from his-
torical controls of a systematic review that
reported on horizontal ridge resorption at
6 months after extraction (29–63%) (Tan
et al. 2012) that this ridge preservation proce-
dure applying the guided tissue regeneration
principle was certainly effective.
In a randomized controlled clinical trial (Ba-
rone et al. 2008), 40 patients were randomly
allocated into two groups. After tooth extrac-
tion, the sockets of the patients in test group
received guided bone regeneration procedures
with cortico-cancellous porcine bone and col-
lagen membranes. The sockets of the patients
in the control group were left to heal sponta-
neously. Clinical measurements were per-
formed at baseline and at re-entry surgery
after 7 months of healing. It was found that
the reduction in ridge width and height were
significantly lower in the GBR group com-
pared with control group (2.5 mm vs. 4.5 mm;
0.4 mm vs. 3 mm, respectively). Histological
analysis revealed that the amount of cancel-
lous bone was significantly greater in the GBR
group (35.5% vs. 25.7%), and the amount of
connective tissue was significantly less in the
GBR group (36.6% vs. 59.1%).
Membranes versus no membranes
To evaluate the adjunctive effect of resorb-
able collagen membranes to bone substitutes,
a randomized clinical study was conducted
(Brkovic et al. 2012). Twenty patients were
randomly allocated into two groups. After
tooth extraction, each socket was filled with
a cone that is comprised of b-tricalcium
phosphate (b-TCP) and type I collagen. The
sockets in the test group were covered with
collagen membranes, whereas the sockets in
the control group were not. Primary closure
was achieved in both groups by muco-perio-
© 2012 John Wiley & Sons A/S 153 | Clin. Oral Implants Res. 23, 2012 / 147–156
Wang & Lang �Ridge preservation revisited

steal flaps. Clinical assessments were per-
formed at baseline and at re-entry surgery
after 9 months of healing. No statistical sig-
nificant differences were found between the
test and control groups on horizontal ridge
resorption (�0.86 mm vs. �1.29 mm, respec-
tively) or on vertical dimensional changes
(0.12 mm vs. 0.5 mm, respectively). Histo-
metric analysis showed that there was no dif-
ference between the test and control groups
regarding the amount of new bone (45.3% vs.
42.4%, respectively). Obviously, applying the
cone material with or without membranes
was effective in preserving the alveolar bone.
Primary flap closure
Primary closure versus no primary closure
Primary closure can also be attained by
means of an implant-supported provisional
prostheses, or using a customized healing
abutment. In a recent split-mouth clinical
trial (Engler-Hamm et al. 2011), molars or
premolars were extracted bilaterally in 11
patients. The sockets on both sides were
filled with an inorganic bovine-derived
hydroxyapatite matrix, cell-binding peptide
P-15 (ABM/P-15), DFDBA, and covered with
collagen membranes. Primary closure was
achieved on one side (control). On the other
side, the membranes were left uncovered
(test). Clinical assessments of the ridge width
were made using a caliper through a stent at
baseline and at after 6 month of healing. In
addition, questionnaires regarding the post-
operative discomfort were filled by the
patients. No significant differences were
found on the ridge width changes (3 mm vs.
3.42 mm). However, the post-operative dis-
comfort was significantly lower in the group
without primary closure. The mucogingival
junction was significantly more coronally
displaced in the group with primary closure.
Conclusions
Implants and associated techniques for alveolarridge preservation
• Implants placed into the fresh extraction
sockets do not prevent the resorption of
the alveolar bone. Although osseointegra-
tion is achieved in the early stage
(1 month in dogs), modeling of the bone
may cause this level to recede apically.
• Immediate loading of the implants in dogs
as well as in humans does not preserve the
alveolar bone ridge. The use of bone fillers
in residual defects around immediate
implants placed in well preserved, intact
alveoli in dogs may reduce soft tissue
recession as well as vertical and horizontal
resoprtion of the buccal bony plate.
• Simultaneous guided bone regeneration
procedures could partially resolve alveolar
bone resorption. However, this is
depended on the type of membrane as
well as the techniques applied.
• The use of root-formed implants, aiming
at closing the space between the implant
surface and alveolar bone of the extrac-
tion socket, does not preserve alveolar
bone ridges. On the contrary, their use
with this association was associated with
accentuated bone resorption.
• It was demonstrated that thicker bony
walls results in less resorption.
• The position of the implants was also an
essential factor for the alveolar bone ridge
preservation. Placing the immediate
implant 0.8mm deeper and more lingually
led to a reduction in the vertical buccal
bone resorption by 70% in dogs after
4 months of healing.
Non-surgical treatment
• There is not enough evidence to recom-
mend ultrasonic instrumentation for
alveolar ridge preservation and no conclu-
sions on its clinical benefits can be made.
Bone substitutes
• The only relevant dog study showed that
unfilled sockets underwent three times
the amount of horizontal resorption as
sockets filled with xenograft (Bio-oss®).
However, the xenograft only served as a
scaffold and did not stimulate new bone
formation.
• Various bone substitute materials have
been tested in clinical trials for their
effects on ridge preservation.
• Ridge preservation using human deminer-
alized bone matrix was effective in ridge
preservation irrespective of the particle
sizes used, but allograft paste showed no
effect.
• Although DFDBA may be claimed to be
more osteoinductive, its effect on ridge
preservation is similar to that of FDBA.
• A combination of hydroxyapatite and b-tri-
calcium phosphate (Bone Ceramic®) was
twice as effective on preserving the alveo-
lar ridge width when compared with de-
proteinized bovine bone mineral (Bio-
oss®). However, the use of BoneCeramic®
as a grafting material in fresh extraction
sockets appears to interfere with normal
healing processes of the alveolar bone, and
hence its indication as a material for bone
augmentation, when implant placement is
considered, should be reconsidered (De
Coster et al. 2011).
• Although collagen plugs were claimed to
have an advantage in avoiding surgery, no
definite recommendations can be made
based on their poor outcome on preserv-
ing the alveolar ridge.
Guided bone regeneration
• Applying the guided bone regeneration
principle using bone substitutes together
with a collagen membrane has shown
clear effects on preserving alveolar ridge
height as well as ridge width.
Primary flap closure
• A dog study revealed that using free gingi-
val grafts in combination with bone sub-
stitutes did not provide additional effects
on ridge preservation compared with bone
substitutes alone.
• A clinical trial showed that achieving pri-
mary flap closure did not present addi-
tional beneficial effects on preserving the
ridge width. On the other hand, patients
experienced more discomfort with pri-
mary closed flaps. Moreover, the muco-
gingival junction was significantly more
coronally displaced in the primary closed
flap sites.
Acknowledgements: This manuscript
was supported by a grant of the Clinical
Research Foundation (CRF) for the Promotion
of Oral Health, Brienz, Switzerland. The
senior author was an ITI Scholar 2010–2012
at the University of Hong Kong.
References
Aimetti, M., Romano, F., Griga, B. & Godio, L.
(2009) Clinical and histologic healing of human
extraction sockets filled with calcium sulfate.
International Journal of Oral and Maxillofacial
Implants 24: 902–909.
Araujo, M.G. & Lindhe, J. (2005). Dimensional
ridge alterations following tooth extraction. An
154 | Clin. Oral Implants Res. 23, 2012 / 147–156 © 2012 John Wiley & Sons A/S
Wang & Lang �Ridge preservation revisited

experimental study in the dog. Journal of Clinical
Periodontology 32: 212–218.
Araujo, M.G. & Lindhe, J. (2009). Ridge preserva-
tion with the use of bio-oss collagen: A 6-month
study in the dog. Clinical Oral Implants
Research 20: 433–440.
Araujo, M.G. & Lindhe, J. (2011a). Socket grafting
with the use of autologous bone: An experimen-
tal study in the dog. Clinical Oral Implants
Research 22: 9–13.
Araujo, M.G., Linder, E. & Lindhe, J. (2011b). Bio-
Oss� Collagen in the buccal gap at immediate
implants: a 6-months study in the dog. Clinical
Oral Implant Research 22: 1–8.
Araujo, M.G., Sukekava, F., Wennstrom, J.L. &
Lindhe, J. (2005). Ridge alterations following
implant placement in fresh extraction sockets:
An experimental study in the dog. Journal of
Clinical Periodontology 32: 645–652.
Araujo, M.G., Sukekava, F., Wennstrom, J.L. &
Lindhe, J. (2006). Tissue modeling following
implant placement in fresh extraction sockets.
Clinical Oral Implants Research 17: 615–624.
Barone, A., Aldini, N.N., Fini, M., Giardino, R.,
Calvo Guirado, J.L. & Covani, U. (2008). Xeno-
graft versus extraction alone for ridge preserva-
tion after tooth removal: A clinical and
histomorphometric study. Journal of
Periodontology 79: 1370–1377.
Blanco, J., Linares, A., Perez, J. & Munoz, F. (2011).
Ridge alterations following flapless immediate
implant placement with orwithout immediate load-
ing. Part ii-a histometric study in the beagle dog.
Journal of Clinical Periodontology 38: 762–770.
Boix, D., Weiss, P., Gauthier, O., Guicheux, J.,
Bouler, J.M., Pilet, P., Daculsi, G. & Grimandi,
G. (2006). Injectable bone substitute to preserve
alveolar ridge resorption after tooth extraction: A
study in dog. Journal of Material Science and
Material Medicine 17: 1145–1152.
Botticelli, D., Berglundh, T. & Lindhe, J. (2004).
Hard-tissue alterations following immediate
implant placement in extraction sites. Journal of
Clinical Periodontology 31: 820–828.
Brkovic, B.M., Prasad, H.S., Rohrer, M.D.,
Konandreas, G., Agrogiannis, G., Antunovic, D.
& Sandor, G.K. (2012) Beta-tricalcium phosphate/
type i collagen cones with or without a barrier
membrane in human extraction socket healing:
Clinical, histologic, histomorphometric, and
immunohistochemical evaluation. Clinical Oral
Investigation 16: 581–590.
Brownfield, L.A. & Weltman, R.L. (2012) Ridge
preservation with or without an osteoinductive
allograft. A clinical, radiographic, micro-ct, and
histologic study evaluating dimensional changes
and new bone formation of the alveolar ridge.
Journal of Periodontology 83: 581–589.
Caneva, M., Botticelli, D., Salata, L.A., Scombatti
Souza, S.L., Carvalho Cardoso, L. & Lang, N.P.
(2010a). Collagen membranes at immediate
implants: A histomorphometric study in dogs.
Clinical Oral Implants Research 21: 891–897.
Caneva, M., Botticelli, D., Stellini, E., Souza, S.L.,
Salata, L.A. & Lang, N.P. (2011). Magnesium-
enriched hydroxyapatite at immediate implants:
A histomorphometric study in dogs. Clinical
Oral Implants Research 22: 512–517.
Caneva, M., Salata, L.A., de Souza, S.S., Baffone, G.,
Lang, N.P. & Botticelli, D. (2010b). Influence of
implant positioning in extraction sockets on
osseointegration: Histomorphometric analyses in
dogs. Clinical Oral Implants Research 21: 43–49.
Caneva, M., Salata, L.A., de Souza, S.S., Bressan, E.,
Botticelli, D. & Lang, N.P. (2010c). Hard tissue
formation adjacent to implants of various size
and configuration immediately placed into extrac-
tion sockets: An experimental study in dogs. Clin
Oral Implants Res 21: 885–890.
Cardaropoli, G., Araujo, M. & Lindhe, J. (2003).
Dynamics of bone tissue formation in tooth
extraction sites. An experimental study in dogs.
Journal of Clinical Periodontology 30: 809–818.
Chen, S.T., Darby, I.B. & Reynolds, E.C. (2007). A
prospective clinical study of non-submerged
immediate implants: Clinical outcomes and
esthetic results. Clinical Oral Implants Research
18: 552–562.
Crespi, R., Cappare, P. & Gherlone, E. (2009). Mag-
nesium-enriched hydroxyapatite compared to cal-
cium sulfate in the healing of human extraction
sockets: Radiographic and histomorphometric
evaluation at 3 months. Journal of Periodontol-
ogy 80: 210–218.
Darby, I., Chen, S. & De Poi, R. (2008). Ridge pres-
ervation: What is it and when should it be con-
sidered. Australian Dental Journal 53: 11–21.
De Coster, P., Browaeys, H. & De Bruyn, H. (2011)
Healing of extraction sockets filled with BoneCe-
ramic® prior to implant placement: Preliminary
histological findings. Clinical Implant Dentistry
and Related Research 13: 34–45.
Engler-Hamm, D., Cheung, W.S., Yen, A., Stark, P.
C. & Griffin, T. (2011). Ridge preservation using
a composite bone graft and a bioabsorbable mem-
brane with and without primary wound closure:
A comparative clinical trial. Journal of Periodon-
tology 82: 377–387.
Favero, G., Botticelli, D., Favero, G., Garcıa, B.,
Mainetti, T & Lang, N.P. (2012). Alveolar bony
crest preservation at implants installed immedi-
ately after tooth extraction: an experimental
study in the dog. Clinical Oral Implants
Research doi: 10.1111/j.1600-0501.2011.02365.x.
[Epub ahead of print] PubMed.
Fernandes, P.G., Novaes, A.B., Jr, de Queiroz, A.C.,
de Souza, S.L., Taba, M, Jr, Palioto, D.B. & Grisi,
M.F. (2011). Ridge preservation with acellular der-
mal matrix and anorganic bone matrix cell-bind-
ing peptide p-15 after tooth extraction in humans.
Journal of Periodontology 82: 72–79.
Fickl, S., Zuhr, O., Wachtel, H., Bolz, W. & Hurzel-
er, M.B. (2008a). Hard tissue alterations after
socket preservation: An experimental study in
the beagle dog. Clinical Oral Implants Research
19: 1111–1118.
Fickl, S., Zuhr, O., Wachtel, H., Stappert, C.F.,
Stein, J.M. & Hurzeler, M.B. (2008b). Dimen-
sional changes of the alveolar ridge contour after
different socket preservation techniques. Journal
of Clinical Periodontology 35: 906–913.
Gotfredsen, K., Berglundh, T. & Lindhe, J. (2001).
Bone reactions adjacent to titanium implants sub-
jected to static load of different duration. A study
in the dog (iii). Clinical Oral Implants Research
12: 552–558.
Hoang, T.N. & Mealey, B.L. (2012) Histological
comparison of healing following ridge preserva-
tion using human demineralized bone matrix
putty with one versus two different sized bone
particles. Journal of Periodontology 83: 174–181.
Horowitz, R.A., Mazor, Z., Miller, R.J., Krauser, J.,
Prasad, H.S. & Rohrer, M.D. (2009) Clinical eval-
uation alveolar ridge preservation with a beta-tri-
calcium phosphate socket graft. Compendium of
Continuing Education in Dentistry 30: 588–590,
592, 594 passim; quiz 604, 606.
Kerr, E.N., Mealey, B.L., Noujeim, M.E., Lasho, D.
J., Nummikoski, P.V. & Mellonig, J.T. (2008).
The effect of ultrasound on bone dimensional
changes following extraction: A pilot study. Jour-
nal of Periodontology 79: 283–290.
Kim, Y.K., Yun, P.Y., Lee, H.J., Ahn, J.Y. & Kim, S.
G. (2011) Ridge preservation of the molar extrac-
tion socket using collagen sponge and xenogeneic
bone grafts. Implant Dentistry 20: 267–272.
Lang, N.P., Tonetti, M.S., Suvan, J.E., Pierre
Bernard, J., Botticelli, D., Fourmousis, I., Hallund,
M., Jung, R., Laurell, L., Salvi, G.E., Shafer, D. &
Weber, H.P. (2007). Immediate implant placement
with transmucosal healing in areas of aesthetic
priority. A multicentre randomized-controlled
clinical trial i. Surgical outcomes. Clinical Oral
Implants Research 18: 188–196.
Mardas, N., Chadha, V. & Donos, N. (2010). Alveo-
lar ridge preservation with guided bone regenera-
tion and a synthetic bone substitute or a bovine-
derived xenograft: A randomized, controlled clini-
cal trial. Clinical Oral Implants Research 21: 688
–698.
Matarasso, S., Salvi, G.E., Iorio Siciliano, V., Cafi-
ero, C., Blasi, A. & Lang, N.P. (2009). Dimen-
sional ridge alterations following immediate
implant placement in molar extraction sites: A
six-month prospective cohort study with surgical
re-entry. Clinical Oral Implants Research 20:
1092–1098.
McAllister, B.S. & Haghighat, K. (2007). Bone aug-
mentation techniques. Journal of Periodontology
78: 377–396.
Neiva, R.F., Tsao, Y.P., Eber, R., Shotwell, J., Billy,
E. & Wang, H.L. (2008). Effects of a putty-form
hydroxyapatite matrix combined with the
synthetic cell-binding peptide p-15 on alveolar
ridge preservation. Journal Periodontology 79: 291
–299.
Oghli, A.A. & Steveling, H. (2010). Ridge preserva-
tion following tooth extraction: A comparison
between atraumatic extraction and socket seal
surgery. Quintessence International 41: 605–609.
Paolantonio, M., Dolci, M., Scarano, A., d’Archivio,
D., di Placido, G., Tumini, V. & Piattelli, A.
(2001). Immediate implantation in fresh extrac-
tion sockets. A controlled clinical and histologi-
cal study in man. Journal of Periodontology 72:
1560–1571.
Park, S.Y., Kye, S.B., Yang, S.M. & Shin, S.Y. (2011)
The effect of non-resorbable membrane on buccal
bone healing at an immediate implant site: An
experimental study in dogs. Clinical Oral
Implants Research 22: 289–294.
Rothamel, D., Schwarz, F., Herten, M., Engelhardt,
E., Donath, K., Kuehn, P. & Becker, J. (2008).
Dimensional ridge alterations following socket
© 2012 John Wiley & Sons A/S 155 | Clin. Oral Implants Res. 23, 2012 / 147–156
Wang & Lang �Ridge preservation revisited

preservation using a nanocrystalline hydroxyapa-
tite paste: A histomorphometrical study in dogs.
International Journal of Oral and Maxillofacial
Surgery 37: 741–747.
Sanz, M., Cecchinato, D., Ferrus, J., Pjetursson, B.
E., Lang, N.P. & Lindhe, J. (2010) A prospective,
randomized-controlled clinical trial to evaluate
bone preservation using implants with different
geometry placed into extraction sockets in the
maxilla. Clinical Oral Implants Research 21: 13–
21.
Shi, B., Zhou, W., Yang, Y. N. & Cheng, X. R.
(2007) Alveolar ridge preservation prior to
implant placement with surgical-grade calcium
sulfate and platelet-rich plasma: A pilot study in
a canine model. International Journal of Oral
and Maxillofacial Implants 22: 656–665.
Tan, W.L., Wong, T.L., Wong, M.C.M. & Lang, N.P.
(2012) A systematic review of post-extractional
alveolar hard and soft tissue dimensional changes
in humans. Clinical Oral Implants Research 23
(Suppl 5): 1–21.
Wehrbein, H., Merz, B.R., Hammerle, C.H. & Lang,
N.P. (1998) Bone-to-implant contact of orthodontic
implants in humans subjected to horizontal load-
ing. Clinical Oral Implants Research 9: 348–353.
Wood, R.A. & Mealey, B.L. (2012) Histological com-
parison of healing following tooth extraction with
ridge preservation using mineralized vs. Deminer-
alized freeze dried bone allograft. Journal of Peri-
odontology 83: 329–336.
156 | Clin. Oral Implants Res. 23, 2012 / 147–156 © 2012 John Wiley & Sons A/S
Wang & Lang �Ridge preservation revisited

Wah Lay TanTerry L. T. WongMay C. M. WongNiklaus P. Lang
A systematic review of post-extrac-tional alveolar hard and soft tissuedimensional changes in humans
Authors’ affiliations:Wah Lay Tan, Terry L. T. Wong, May C. M. Wong,Niklaus P. Lang, Implant Dentistry, The Universityof Hong Kong, Prince Philip Dental Hospital,Implant Dentistry, Hong Kong, China
Corresponding author:Prof. Niklaus P. Lang, DMD, MS, PhD, Dr odont.h.c. mult.The University of Hong Kong Faculty of DentistryPrince Philip Dental Hospital34 Hospital Road, Sai Ying PunHong Kong, ChinaTel.:+852 2859 0526Fax: +852 2858 6114e-mail: [email protected]
Conflicts of interestThe authors declare no conflict of interest.
Key words: alveolar bone, dimensional change, extraction, hard tissue, human, removal of
teeth, resorption, soft tissue, systematic review
Abstract
Background: Removal of teeth results in both horizontal and vertical changes of hard and soft
tissue dimensions. The magnitude of these changes is important for decision-making and
comprehensive treatment planning, with provisions for possible solutions to expected
complications during prosthetic rehabilitation.
Objectives: To review all English dental literature to assess the magnitude of dimensional changes
of both the hard and soft tissues of the alveolar ridge up to 12 months following tooth extraction
in humans.
Methods: An electronic MEDLINE and CENTRAL search complemented by manual searching was
conducted to identify randomized controlled clinical trials and prospective cohort studies on hard
and soft tissue dimensional changes after tooth extraction. Only studies reporting on undisturbed
post-extraction dimensional changes relative to a fixed reference point over a clearly stated time
period were included. Assessment of the identified studies and data extraction was performed
independently by two reviewers. Data collected were reported by descriptive methods. Weighted
means and percentages of the dimensional changes over time were calculated where appropriate.
Results: The search provided 3954 titles and 238 abstracts. Full text analysis was performed for 104
articles resulting in 20 studies that met the inclusion criteria. In human hard tissue, horizontal
dimensional reduction (3.79 ± 0.23 mm) was more than vertical reduction (1.24 ± 0.11 mm on
buccal, 0.84 ± 0.62 mm on mesial and 0.80 ± 0.71 mm on distal sites) at 6 months. Percentage
vertical dimensional change was 11–22% at 6 months. Percentage horizontal dimensional change
was 32% at 3 months, and 29–63% at 6–7 months. Soft tissue changes demonstrated 0.4–0.5 mm
gain of thickness at 6 months on the buccal and lingual aspects. Horizontal dimensional changes of
hard and soft tissue (loss of 0.1–6.1 mm) was more substantial than vertical change (loss 0.9 mm to
gain 0.4 mm) during observation periods of up to 12 months, when study casts were utilized as a
means of documenting the changes.
Conclusions: Human re-entry studies showed horizontal bone loss of 29–63% and vertical bone
loss of 11–22% after 6 months following tooth extraction. These studies demonstrated rapid
reductions in the first 3–6 months that was followed by gradual reductions in dimensions
thereafter.
The periodontium is an important structure
that supports the tooth and is affected by any
changes that the tooth may undergo, includ-
ing eruption and extraction (Cohn 1966; Pie-
trokovski & Massler 1967, 1971). The
alveolar process is a tooth-dependent tissue;
the shape and volume of the alveolar process
is influenced by tooth form, as well as the
direction of eruption of the tooth (Marks
1995; Marks & Schroeder 1996), and the pres-
ence or absence of teeth (Tallgren 1972). Sim-
ilarly, gingival tissues undergo changes
together with eruption and eventual exfolia-
tion or extraction of the tooth. Subsequent to
removal of a tooth, the periodontium under-
goes atrophy (Cohn 1966; Schropp et al.
2003), with the complete loss of attachment
apparatus including cementum, periodontal
ligament fibres and bundle bone (Araujo &
Lindhe 2005).
Tooth extraction is one of the most widely
performed dental procedures. In general, post-
extraction healing of both the hard and soft
tissues proceeds uneventfully. However, the
removal of a tooth will generally result in
some alveolar bone loss, as well as structural
Date:Accepted 15 October 2011
To cite this article:Tan WL, Wong TLT, Wong MCM, Lang NP. A systematicreview of post-extractional alveolar hard and soft tissuedimensional changes in humans.Clin. Oral. Impl. Res. 23(Suppl. 5), 2012, 1–21doi: 10.1111/j.1600-0501.2011.02375.x
© 2011 John Wiley & Sons A/S 1
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza

and compositional changes in the overlying
soft tissue (Schropp et al. 2003). Both hori-
zontal and vertical changes in dimensions are
expected in hard tissue (Van der Weijden
et al. 2009) as well as soft tissue. Studies in
the canine model (Araujo & Lindhe 2005;
Araujo et al. 2005) have demonstrated that
there are marked dimensional changes of the
alveolar ridge in the first 2–3 months post-
extraction, with the changes more pro-
nounced on the buccal (Araujo et al. 2005).
Critically, horizontal buccal bone resorption
has been shown reach as much as 56% while
lingual bone resorption has been reported to
be up to 30% (Botticelli et al. 2004); the over-
all reduction in width of the horizontal ridge
has been reported to reach 50% (Schropp
et al. 2003).
A narrower and shorter ridge can be an
expected sequelae of the resorptive process
(Pinho et al. 2006), and in effect, the process
of resorption often results in the relocation of
the ridge to a more lingual position (Botticelli
et al. 2004). The process of ridge remodelling
is further complicated if the buccal bone wall
is lost (Iasella et al. 2003) as a result of
inflammatory processes or the extraction
itself.
Extraction of one or more teeth results
not only in changes of the bony architec-
ture, but also affects the overlying soft tis-
sues of the alveolus (Schropp et al. 2003).
Immediately following tooth extraction,
there is absence of soft tissue covering over
the socket entrance, and hence the socket
defect is left to heal by secondary intention.
In the subsequent weeks, cell proliferation
will result in an increase in soft tissue vol-
ume, and a soft tissue covering will seal the
socket entrance. The changes in the muco-
sal contours are dependent on the corre-
sponding changes in the external profile of
the alveolar bone surrounding the extraction
site.
The magnitude of these dimensional
changes are important for informed decision-
making and comprehensive treatment plan-
ning, with provisions for possible solutions
to expected complications during prosthetic
rehabilitation. In addition, with the advent of
greater emphasis on aesthetics in the last
decade, a thorough understanding of the
resorptive pattern and alterations in bony and
mucosal contours post-extraction would
greatly enhance our ability to reconstruct our
patients to a level of optimal function cou-
pled with satisfactory aesthetics.
There have been numerous studies that
have researched the magnitude of hard tissue
changes post-extraction, with the consensus
that alveolar bone loss can be quite marked
after tooth removal (Araujo & Lindhe 2009),
especially in the horizontal dimension (Botti-
celli et al. 2004). Soft tissue changes
post-extraction have largely been described
qualitatively, and usually as a single entity
together with the hard tissue changes
assessed using serial study casts (e.g. Schropp
et al. 2003).
In recent years, there has been one system-
atic review addressing the dimensional
changes of the alveolar ridge after tooth
extraction (Van der Weijden et al. 2009);
however, there is as yet no systematic review
addressing the dimensional changes of both
the hard and soft tissues after tooth extrac-
tion.
This study aims to review all existing liter-
ature published between 1st January 1960
and 30th January 2011, to assess the magni-
tude of dimensional change of both the hard
and soft tissues of the alveolar ridge after
tooth extraction.
Material and methods
The Preferred Reporting Items for Systematic
Reviews and Meta-Analyses (PRISMA) state-
ment was consulted throughout the process
of this systematic review.
Focused question
What is the magnitude of dimensional
changes in the hard and soft tissues of the
alveolar process, up to 12 months following
tooth extraction?
Search strategy
A comprehensive and systematic electronic
search of both the MEDLINE–Pubmed data-
base and the Cochrane Central Register of
Controlled Trials (CENTRAL) was con-
ducted, for articles published in English
between 1st January 1960 and 30th June
2010 in the dental literature. The search
was performed again at a later stage, to
include any relevant new studies published
between 1st July 2010 and 31st Janu-
ary 2011. The following key words were
used:
Intervention:
(<[MeSH terms/all subheadings] “Tooth
Extraction”>
OR
<[text words] Tooth Extraction OR Dental
Extraction OR Tooth Removal OR Tooth
Pulling OR Tooth Loss OR Exodontia OR
Surgery OR Surgical Tooth Extraction OR
Surgical Tooth Removal>
OR
<[text words] Tooth AND Extraction>)
AND
Outcome:
(<[MeSH terms/all subheadings] “Bone
Resorption “ OR “Alveolar Bone Loss” OR
“Periodontal Atrophy”>
OR
<[text words] Bone Defect OR Bone Resorp-
tion OR Alveolar Bone Loss OR Alveolar
Resorption OR Alveolar Healing OR Ridge
Changes OR Ridge Alterations OR Ridge
Resorption OR Ridge Healing OR Mucosal
Alterations OR Mucosal Changes OR Muco-
sal Atrophy OR Mucosal Healing OR Gingi-
val Alterations OR Gingival Changes OR
Gingival Atrophy OR Gingival Healing OR
Socket Healing OR Socket>)
The following journals between 2004 and
2010 inclusive, were hand-searched for rele-
vant articles: Clinical Oral Implants
Research, International Journal of Oral &
Maxillofacial Implants, Implant Dentistry,
Journal of Periodontology, Journal of Clinical
Periodontology and Journal of Oral Implan-
tology.
Furthermore, the bibliographies of all pub-
lications selected for inclusion in this review
were also scanned for potentially relevant
articles.
Selection criteria
Studies were included if they were published
in English and conducted on human subjects,
with the intervention being tooth extraction,
and the outcome to be assessed in the form
of changes in the clinical or radiographic
alveolar bone dimensions, as well as dimen-
sional soft tissue changes. Similarly, exclu-
sion criteria were applied; letters and
narrative or retrospective reviews, single case
reports, case series with less than three cases,
and third molar extraction cases were all
excluded. Only studies reporting on undis-
turbed post-extraction dimensional changes
relative to a fixed reference point over a
clearly stated time period were included. In
addition, in the event of duplicate publica-
tions, the study with the most inclusive data
was preferentially selected.
Selection of studies
Screening was performed independently by
two reviewers (L. T. Wong and W. L. Tan);
any disagreement between the reviewers was
resolved by discussion. The initial electronic
search resulted in the identification of 2843
titles from the MEDLINE–Pubmed database
and 1111 titles from the Cochrane Central
2 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

Register of Controlled Trials (CENTRAL).
After careful independent screening of the
titles and elimination of duplicate titles by
both the examiners, a total of 238 titles were
considered for possible inclusion. Retrieval of
the 238 abstracts and further perusal led to
104 full-text articles being selected. From
these full-text articles, 19 were identified for
inclusion in the review.
Another article was deemed suitable from
the secondary electronic search, but no addi-
tional publications from the hand-search or
the bibliography search of the selected arti-
cles were identified for inclusion.
In total, 20 articles were identified for
eventual inclusion in this review (Fig. 1).
A j-score of 0.84 was obtained, for consen-
sus between the two reviewers.
Exclusion of studies
Of the 104 full-text articles examined, 85
were excluded from the final analysis
(Table 1). The main reasons for exclusion
were that there were no actual measure-
ments of the dimensional changes of the
alveolar ridge, the reported parameters were
not useful for this review and that there was
the presence of a foreign material in the
extraction site during the healing phase,
among other reasons.
Data collection
From the selected papers that met the crite-
ria, data addressing dimensional changes
Potentially relevantpublications identified from
electronic search ofCochrane Central Register of Controlled Trials (CENTRAL)
database from 1st January1960 to 30th June 2010
(n = 1111)
Potentially relevantpublications identified from
electronic search of MEDLINE-Pubmed databasefrom 1st January 1960 to 30th
June 2010(n = 2843)
Publications excluded on the basis of titleand summary evaluation; also excluded
duplicate publications(n = 3716)
Potentially relevant full textsretrieved for detailed
evaluation(n = 104)
Publications excluded on the basis of fulltext evaluation
(n = 85)
Studies included based onthe initial electronic search ofthe MEDLINE-Pubmed and
CENTRAL database from 1st
January 1969 to 30th June2010
(n = 19) Publications included based on the hand-
search and bibliography search ofrelevant articles
(n = 0)
Publications included based on thesecondary electronic search of theMEDLINE-Pubmed and CENTRALdatabase from 1st July 2010 to 31st
January 2011(n = 1)
Studies included in thepresent systematic review
(n = 20)
Fig. 1. Search strategy. Post-extraction dimensional changes.
Table 1. Studies failing to meet inclusion criteria
Reference Rationale for exclusion
Richardson 1965; Guglielmotti & Cabrini 1985; Guglielmotti et al. 1985; Mathai et al. 1989;Ubios et al. 1991; Boyne 1995; Gauthier et al. 1999; Teofilo et al. 2001; Brandao et al. 2002;Indovina & Block 2002; Magro-Ernica et al. 2003; Altundal & Guvener 2004; Bianchi et al. 2004;Gorustovich et al. 2004; Nevins et al. 2006; Ortega et al. 2007; Araujo et al. 2008; Iino et al. 2008;Agbaje et al. 2009; Puia et al. 2009; Alissa et al. 2010; Normando et al. 2010
Reported parameters not relevant or not useful
Pietrokovski & Massler 1967a; Matsumoto 1968 Length of observation period not reportedAmemori 1966; Mizutani & Ishihata 1976; Olson & Hagen 1982; Hahn et al. 1988; Oltramari et al.2007; Shi et al. 2007; Fickl et al. 2008a; Fickl et al. 2008b
Studies carried out on animals
Loo 1968; Ashman & Bruins 1985; Ashman & Bruins1987; Scheer & Boyne 1987; Sclar 1999;Minsk 2005
Descriptive report on procedure/ technique;commentary
Guglielmotti et al. 1986; Hsieh et al. 1995; Fickl et al. 2008c; Rothamel et al. 2008; Araujo &Lindhe 2009a; Pessoa et al. 2009
No baseline data available for comparison, thus unableto arrive at an estimate of dimensional change overtime
Carlsson & Persson 1967; Pietrokovski & Massler 1967b; Pietrokovski 1967; Green et al. 1969;Huebsch & Hansen 1969; Berkovitz 1971; Pietrokovski & Massler 1971; Hars & Massler 1972;Librus et al. 1973; Thilander & Astrand 1973; Horn et al. 1979; Olson et al. 1982; Quinn &Kent 1984; Lavelle 1985; Boyes-Varley et al. 1988; Magro-Filho & de Carvalho 1990; Dayanet al. 1992; Alves-Rezende & Okamoto 1997; Anitua 1999; Pinto et al. 2002; Carmagnolaet al. 2003; Cardaropoli et al. 2005; Smith 1974; Ahn & Shin 2008; Serino et al. 2008; Sharan &Madjar 2008; Luvizuto et al. 2010; Teofilo et al. 2010
No measurements of alveolar dimensional changes (e.g.description of healing process or bony shape change,or histology only)
Bergstedt et al. 1973; Michael & Barsoum 1976; Kangvonkit et al. 1986; Sattayasanskul et al.1988
Study subjects had immediate dentures after extraction,hence they did not have undisturbed healingpost-extraction
Bahat et al. 1987; Iizuka et al. 1992; Yugoshi et al. 2002; Araujo et al. 2005; Lindeboom et al.2006; Wu et al. 2008; Araujo & Lindhe 2009b; Nevins et al. 2009
Sample did not include untreated/undisturbed extractionsockets left to heal spontaneously
Araujo & Lindhe 2005 Only measured relative difference in height betweenbuccal and lingual plates of the alveolus
© 2011 John Wiley & Sons A/S 3 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

of both soft and hard tissues of the alveolar
ridge were retrieved for analysis. Mean
values and standard deviations, where
available, were extracted in duplicate by
the two reviewers (L. T. Wong and W. L.
Tan).
Quality assessment
Assessment of study quality was performed
for all the included papers. The Cochrane
Collaboration’s tool for assessing risk of bias
was used in the case of randomized con-
trolled clinical trials and controlled clinical
trials. Methodological quality assessment of
cohort studies was based on the Newcastle–
Ottawa Quality Assessment Scale for Cohort
studies (Tables 2 and 3).
Data synthesis
Preliminary evaluation of the selected publi-
cations revealed that there was considerable
heterogeneity between the studies with
regard to study design, study population,
study period, method of assessment of
dimensional change of the alveolar ridge as
well as reference point from which the
changes were measured. Taking this into
consideration, it was not appropriate to con-
duct a quantitative data synthesis for all
studies, leading to a meta-analysis. In this
case, we attempted to report the data by
applying descriptive methods. In addition,
as a selected few of the included studies
demonstrated some similarity in measure-
ment methods and reference points, we pre-
sented weighted means of the dimensional
change of the alveolar ridge over time as
appropriate, taking into account the values
of the relevant standard deviation and
applying inverse variance weighting (Meier
1953).
Inverse variance weighting
For the weighted mean of the list of data for
which each mean xi comes from a different
probability distribution with a known
variance ri2, the weight for each study is
given by:
Wi "1
ri2
The weighted mean in this case is:
!x "Pn
i"1#xi=r2i $Pni"1#1=r2i $
and the variance of the weighted mean is:
r2!x " 1Pni"1#1=r2i $
Assessment of heterogeneity
Statistical heterogeneity between all the
included studies was not assessed because all
the studies had different observation time
points as well as measurement methods,
making a statistical comparison impossible.
However, assessment of heterogeneity
between studies with similar characteristics
were performed using Cochran’s Q-test:
Q "X
wi#xi % !x$
The P-value was then calculated for the Q
statistic and a value of P < 0.05 would indi-
cate significant statistical heterogeneity
between the studies.
When Q > df, where df is its degree of free-
dom, the I2 index was also calculated using
the following formula:
I2 " Q% df
Q
! "& 100%
where, I2 = 0% to 40% would indicate
there is little to no heterogeneity
I2 = 30% to 60% would indicate there is
moderate heterogeneity
I2 = 50% to 90% would indicate there is
substantial heterogeneity
I2 = 75% to 100% would indicate consider-
able heterogeneity
Similarly, the P-value was calculated for
the I2 statistic, and a value of P < 0.05 would
indicate a result that is statistically signifi-
cant.
Results
Collectively, a total of 20 studies satisfied
the inclusion criteria and were included in
this systematic review.
The 20 studies included 11 randomized
controlled clinical trials, five controlled clini-
cal trials and four cohort studies (Tables 2
and 3). The majority of studies did not state
the reasons for tooth extraction, but in the
studies that did, they included fractures, car-
ies, trauma, endodontic, prosthodontic,
orthodontic and periodontal reasons. Thirteen
papers only studied non-molar extraction
sites (Carlsson & Persson 1967; Lekovic et al.
1997, 1998; Yilmaz et al. 1998; Camargo
et al. 2000; Iasella et al. 2003; Serino et al.
2003; Fiorellini et al. 2005; Saldanha et al.
2006; Rodd et al. 2007; Barone et al. 2008;
Aimetti et al. 2009; Pelegrine et al. 2010),
while six studies (Bragger et al. 1994; Schropp
et al. 2003; Kerr et al. 2008; Crespi et al.
2009; Moya-Villaescusa & Sanchez-Pérez
2010; Rasperini et al. 2010) reported on data
including molar extraction sites and one
study (Oghli & Steveling 2010) did not spec-
ify where the extractions were performed.
Most of the data extracted concerned teeth in
control groups of studies that evaluated vari-
ous ridge preservation procedures (Lekovic
et al. 1997, 1998; Yilmaz et al. 1998; Camar-
go et al. 2000; Iasella et al. 2003; Serino et al.
2003; Fiorellini et al. 2005; Barone et al.
2008; Aimetti et al. 2009; Crespi et al. 2009;
Oghli & Steveling 2010; Pelegrine et al. 2010;
Rasperini et al. 2010), but other studies were
either designed specifically to evaluate post-
extraction alveolar changes (Carlsson & Pers-
son 1967; Schropp et al. 2003; Rodd et al.
2007; Moya-Villaescusa & Sanchez-Perez
2010) or the effect of smoking (Saldanha
et al. 2006) or ultrasound treatment (Kerr
et al. 2008) on these changes. In addition,
one included study (Bragger et al. 1994) was
actually designed to test the effect of
chlorhexidine mouthrinse on post-extraction
healing. Each paper that was included in
this review contributed a number of extrac-
tion sites, ranging from three to over a
hundred sites. The age range of the patients
in these studies was between 10.8 and
53.3 years.
Included studies
There were a total of 20 studies addressing
the hard and soft tissue dimensional changes
of the alveolar ridge in humans, with sponta-
neous undisturbed healing. The studies were
grouped according to the reported changes in
hard tissue, soft tissue, or a combination of
both hard and soft tissue.
Hard tissue changes
Vertical and horizontal linear hard tissue
changes in humans were reported indepen-
dently or in combination by 17 studies
(Tables 4 and 7).
Vertical linear hard tissue alteration
All 17 studies that reported on post-extrac-
tion hard tissue changes looked into the ver-
tical linear dimensional change of the
alveolus. Eight studies (Lekovic et al. 1997,
1998; Camargo et al. 2000; Iasella et al. 2003;
Serino et al. 2003; Barone et al. 2008; Aimetti
et al. 2009; Pelegrine et al. 2010) utilized
re-entry procedures with stents or titanium
pins as reference points (Fig. 2), one other
study (Rasperini et al. 2010) did not carry out
a re-entry procedure but nevertheless utilized
a stent for reference. An additional eight
studies (Carlsson & Persson 1967; Bragger
et al. 1994; Schropp et al. 2003; Fiorellini
et al. 2005; Saldanha et al. 2006; Kerr et al.
4 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

Table 2. Cochrane Collaboration’s tool for assessing risk of bias
Study design
Carlsson & Persson (1967) Bragger et al. (1994)Controlled clinical trial Randomized controlled clinical trialParallel Parallel
Adequate sequence generation No UnclearRemark Quote “alternate patients were assigned to respective
groups”Quote “then randomly assigned”
Insufficient information about sequence generationAllocation concealment Unclear UnclearRemark No information provided. No information provided.Blinding Unclear YesRemark Study did not address this outcome. Quote “ double-blind clinical trial”Incomplete outcome data addressed Yes NoRemark Quote “one patient from each group had to be
discarded….one had moved…other case first radiographunsuccessful and could not be repeated..”
Initially mentioned that 40 patients were enrolled instudy, but subsequently only obtained radiographs for23 patients with no explanation
Free of selective reporting Yes NoRemark Initially mentioned that 40 patients were enrolled in
study, but subsequently only obtained radiographs for23 patients with no explanation
Free of other sources of bias Yes YesRemarkOverall risk of bias High High
Study design
Lekovic et al. (1997) Lekovic et al. (1998)Controlled clinical trial Randomized controlled clinical trialSplit-mouth Split-mouth
Adequate sequence generation Unclear YesRemark No information provided Quote “ control and experimental sites were assigned by
the flip of a coin”Allocation concealment Unclear UnclearRemark No information provided No information providedBlinding Unclear YesRemark Study did not address this outcome Quote “clinical measurements were performed by one
clinician who did not have knowledge of control andexperimental sites”
Incomplete outcome data addressed Yes YesRemark Mentioned that three patient had dehiscence in test
group, hence did not measure values at 6 months;re-entry was planned at 6 months, but if membraneexposure occurred, re-entry and measurements wasdone at 3 months. Refer to Tables 3–5 and will see thatthey analysed the results with various combinations,including with or without the patients that exited early,suggesting an intention-to-treat analysis
No missing outcome data
Free of selective reporting Yes YesRemarkFree of other sources of bias Yes YesRemarkOverall risk of bias Unclear Unclear
Study design
Camargo et al. (2000) Iasella et al. (2003) Serino et al. (2003) Fiorellini et al. (2005)
Controlled clinical trialRandomized controlledclinical trial Controlled clinical trial
Randomized controlled clinicaltrial
Split-mouth Parallel Parallel and split-mouth Parallel
Adequate sequencegeneration
Unclear Yes Unclear Unclear
Remark No information provided Quote “randomly selectedusing a coin toss”
No information provided Quote “ cohorts of 40 patientrandomized in a double-blindmanner”
Insufficient information aboutsequence generation
Allocationconcealment
Unclear Unclear Unclear Unclear
Remark No information provided No information provided No information provided No information providedBlinding Unclear Yes Unclear YesRemark Study did not address this
outcomeQuote “measurements weretaken by 2 maskedexaminers”
No information provided Quote “all the patients in the studyunderwent the same surgicalprocedure, regardless of thetreatment
Incomplete outcomedata addressed
Yes Yes Yes Yes
© 2011 John Wiley & Sons A/S 5 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

Table 2. (continued)
Study design
Camargo et al. (2000) Iasella et al. (2003) Serino et al. (2003) Fiorellini et al. (2005)
Controlled clinical trialRandomized controlledclinical trial Controlled clinical trial
Randomized controlled clinicaltrial
Split-mouth Parallel Parallel and split-mouth Parallel
Remark No missing outcome data Quote “implants weresuccessfully placed at allsites….none have beensubsequently lost”
Quote “nine subjectsdropped out from thestudy for reasons unrelatedto the therapy”
Quote “ No subjects werewithdrawn or lost to follow-up”
Free of selectivereporting
Yes Yes Yes Yes
RemarkFree of other sourcesof bias
Yes Yes Yes Yes
RemarkOverall risk of bias Unclear Unclear Unclear Unclear
Study design
Barone et al. (2008) Kerr et al. (2008) Aimetti et al. (2009)
Randomized controlled clinical trial Randomized controlled clinical trialRandomized controlled clinicaltrial
Parallel Split-mouth Parallel
Adequate sequence generation Yes Unclear UnclearRemark Quote “using a
computer-generatedrandomisation list…”
Quote “ one site was assignedrandomly as test, whereas theother site was assigned as control”
Quote “ were consecutivelyselected..” and “ all sockets weremeasured and assigned randomlyto test or control”
Insufficient information aboutsequence generation
Insufficient information aboutsequence generation
Allocation concealment Unclear Unclear NoRemark No information provided No information provided Assignment not explicitly
concealedBlinding Yes Yes YesRemark Quote “all measurements were
taken by one examiner who wasnot involved in performing thesurgical treatment…”
Quote “examiner was masked as towhether sites were test or control”
Quote “recorded by the sameexaminer, who was not involvedin providing therapy”
Incomplete outcome data addressed Yes Yes UnclearRemark No loss to follow-up in test and
control groupNo missing outcome data Study did not address this
outcomeFree of selective reporting Yes Yes YesRemarkFree of other sources of bias Yes Yes YesRemarkOverall risk of bias Unclear Unclear High
Study design
Crespi et al. (2009) Pelegrine et al. (2010) Rasperini et al. (2010)
Controlled clinical trial Randomized controlled clinical trialRandomized controlled clinicaltrial
Split-mouth Parallel Parallel
Adequate sequence generation No Unclear YesRemark Quote “sockets on right side of jaw
received MHA….sockets on leftside received CS…”
Quote “teeth to be extracted wererandomized into two groups”
Quote “treatment regimens wereassigned randomly to the subjectswith a balanced random permutedblock approach”
Allocation by left or right sideof jaw
Insufficient information aboutsequence generation
Allocation concealment Unclear Unclear YesRemark No information provided. No information provided. Quote “treatment regimens
assigned randomly…communicated to the operatorimmediately after toothextraction”
Blinding Yes Unclear YesRemark Quote “a masked examiner
measured the bone level changes.”Study did not address this outcome Quote “tubes included into the
stent by a blind examiner…..aftersurgery, blinded examinerpositioned the stent.”
Incomplete outcome data addressed Yes Unclear YesRemark No missing outcome data Study did not address this outcome. Missing outcome data balanced in
numbers across groupsFree of selective reporting Yes Yes YesRemarkFree of other sources of bias Yes Yes YesRemarkOverall risk of bias High Unclear Low
6 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

2008; Crespi et al. 2009; Moya-Villaescusa &
Sanchez-Perez 2010) utilized imaging meth-
ods to obtain the required information.
Only one re-entry study (Aimetti et al.
2009) addressed the vertical linear change of
the alveolar hard tissue post-extraction at
3 months. In this study, 3 months after
extraction of anterior maxillary teeth, a mean
vertical reduction of 1.2 ± 0.8 mm on the
buccal, 0.9 ± 1.1 mm on the palatal and
0.5 ± 0.9 mm on the mesial and distal sites
were reported when an acrylic stent was used
as a fixed reference during re-entry.
A total of six re-entry studies (Lekovic et al.
1997, 1998; Camargo et al. 2000; Iasella et al.
2003; Serino et al. 2003; Pelegrine et al. 2010)
reported data on 6-month post-extraction ver-
tical linear hard tissue changes of the alveolus;
four studies (Lekovic et al. 1997, 1998; Camar-
go et al. 2000; Pelegrine et al. 2010) utilized a
titanium screw or pin, while two studies (Ia-
sella et al. 2003 and Serino et al. 2003) used an
acrylic stent as a fixed reference point.
Six months following the extraction of
anterior teeth or premolars, Lekovic et al.
(1997) reported a mean reduction of
1.2 ± 0.13 mm in buccal vertical ridge height,
while Lekovic et al. (1998) and Camargo
et al. (2000) reported a mean reduction of
1.50 ± 0.26 mm and 1.00 ± 2.25 mm respec-
tively. Later, Pelegrine et al. (2010) showed
that 6 months after extraction of maxillary
anterior teeth, the mean buccal vertical alve-
olar ridge height reduction was
1.17 ± 0.26 mm. All the four studies men-
tioned above measure changes relative to a
titanium pin or screw at re-entry.
Iasella et al. (2003) and Serino et al. (2003)
utilized re-entry procedures and acrylic stents
as fixed references, 6 months after extraction
of non-molar teeth. The former study reported
an average alveolar vertical hard tissue reduc-
tion of 0.9 ± 1.6 mm at the mid-buccal,
0.4 ± 1.0 mm at the mid-lingual, 1.0 ± 0.8
mm at the mesial and 0.8 ± 0.8 mm on the
distal sites; the latter study recorded a mean
reduction of 0.7 ± 1.2 mm on the buccal.
Taking into consideration the similarities
between these six re-entry studies that
reported 6-month data (Lekovic et al. 1997,
1998; Camargo et al. 2000; Iasella et al. 2003;
Serino et al. 2003; Pelegrine et al. 2010), the
weighted mean was calculated for the rele-
vant sites, using the inverse variance
method, to give a more robust value of the
6-month post-extraction vertical change
(Fig. 3). On the buccal, all six studies were
included to give a weighted mean reduction
of 1.24 ± 0.11 mm (Q = 1.3, P = 0.94). Only
two studies (Iasella et al. 2003; Serino et al.
2003) were included when mesial and distal
sites were investigated; the respective
weighted reductions were 0.84 ± 0.62 mm on
the mesial (Q = 0.10, P = 0.75) and
0.80 ± 0.71 mm on the distal (Q = 0, P = 1).
After a 7-month undisturbed healing period
in non-molar extraction sites, Barone et al.
(2008) observed vertical linear reduction of
3.6 ± 1.5 mm, 3.0 ± 1.6 mm, 0.4 ± 1.2 mm
and 0.5 ± 1.0 mm on the mid-buccal, mid-lin-
gual, mesial and distal sites respectively, at re-
entry. A stent was used as a fixed reference.
Rasperini et al. (2010) reported on 3- and 6-
month dimensional changes of the alveolar
ridge after extraction of maxillary molar
teeth, using a custom acrylic stent and a peri-
odontal probe or endodontic file to obtain the
measurements; measurements were made
from the surface of the bone to the external
surface of the stent. The observed reduction
in height of the buccal plate at 3 and
6 months were 2.2 and 5.7 mm respectively,
when the buccal plates were intact after
extraction. However, when the buccal plates
were lost at time of extraction, there was a
corresponding gain of buccal bone height of 1
and 0.6 mm at 3 and 6 months respectively.
Radiographic methods used for the relevant
studies were: lateral cephalometric radiogra-
phy in one study (Carlsson & Persson 1967),
cone beam computed tomography in two
studies (Fiorellini et al. 2005 and Kerr et al.
2008), linear tomography in one study (Salda-
nha et al. 2006), and intraoral peri-apical radi-
ography in four studies (Bragger et al. 1994;
Schropp et al. 2003; Crespi et al. 2009 and
Moya-Villaescusa & Sanchez-Perez 2010).
Carlsson & Persson (1967) attempted to
use lateral cephalometric radiography to dem-
onstrate the longitudinal height change in
the mandibular alveolar ridge after extraction
of at least five to six lower anterior teeth and
loading with conventional full dentures
2 months post-extraction. The study had
observation time points at 2, 4, 6, 12, 24 and
60 months. The reductions in alveolar height
were 2.0 mm at 2 months, 2.9 mm at
4 months, 3.4 mm at 6 months and 4.1 mm
at 12 month, compared to baseline. From this
study, we can see a trend where there is a
large reduction in alveolar bone height in the
first 2 months post-extraction, followed by a
continual gradual resorption thereafter. Take
note that we should interpret the values
obtained in this study, with observation time
points greater than 2 months, with caution;
2 months after teeth extraction, full dentures
were inserted in the conventional group, and
we cannot with full confidence, state that
insertion and use of denture prostheses did
not have an impact on the resorptive pattern
and extent of the alveolar hard and soft tis-
sues in this case.
Two studies (Fiorellini et al. 2005; Kerr
et al. 2008) utilized computed tomography to
detect vertical height changes in the alveolar
Table 2. (continued)
Study design
Yilmaz et al. (1998) Oghli & Steveling (2010)Controlled clinical trial Randomized controlled clinical trialParallel Parallel
Adequate sequence generation Unclear UnclearRemark No information provided Quote “patients were divided randomly into three groups”
Insufficient information about sequence generationAllocation concealment Unclear UnclearRemark No information provided No information providedBlinding Unclear UnclearRemark Study did not address this outcome Study did not address this outcomeIncomplete outcome data addressed Unclear YesRemark Study did not address this outcome All exclusions accounted forFree of selective reporting Yes YesRemarkFree of other sources of bias Yes YesRemarkOverall risk of bias Unclear Unclear
© 2011 John Wiley & Sons A/S 7 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

hard tissue. Fiorellini et al. (2005) reported a
4-month mean height reduction of
1.17 ± 1.23 mm in patients after extraction
of maxillary non-molar teeth; of note is that
all the patients in this sample had a buccal
defect of ' 50% bone loss of the extraction
socket at baseline. In the study by Kerr et al.
(2008), following extraction of a permanent
tooth, the corresponding vertical resorption
of the alveolar ridge were 1.01 ± 0.39 mm on
the buccal, 0.62 ± 0.28 mm on the lingual at
1 month and 0.95 ± 0.39 on the buccal,
1.12 ± 0.28 on the lingual at 3 months.
Six months after extraction of upper ante-
rior teeth, Saldanha et al. (2006) observed a
vertical resorption of 1.5 mm in smokers and
1.0 mm in non-smokers when using linear
tomography.
Assessing interproximal bone height
change on intraoral periapical radiographs,
Bragger et al. (1994) demonstrated a vertical
reduction of 0.61 ± 0.67 mm, 0.67 ±
0.66 mm, 1.19 ± 1.50 mm and 0.93 ± 0.74
mm at 1, 2, 3 and 6 months respectively,
while Schropp et al. (2003) documented a
0.3 mm loss at 12 months. Crespi et al.
(2009) went on to show an overall 3-month
Table 3. Newcastle–Ottawa Quality Assessment Scale for Cohort Studies (max 9*)
Study designSchropp et al. (2003) Saldanha et al. (2006)Cohort Cohort
SelectionRepresentativeness of the exposedcohort
Truly representative of the average implantpatient in the community
Representative of the average patientrequiring extraction in the community
Rating * *Selection of non exposed cohort No description of the derivation of non-exposed
cohortNo description of the derivation of the non-exposedcohort
RatingAscertainment of exposure Secure record (radiograph, study model, clinical
exam)Secure record (radiograph, linear tomography, clinicalexam)
Rating * *Demonstration that outcome ofinterest was not present atstart of study
Yes Yes
Rating * *ComparabilityComparability of cohorts on thebasis of the design or analysis
No mention of control of any confounding factors (e.g.smoking, health)
Controlled for confounding factors (smoking, oralhygiene, ethnicity, systemic health)
Rating **OutcomeAssessment of outcome Records (radiograph, study models) Independent blind assessmentRating * *Was follow-up long enough foroutcomes to occur
Yes; 12 months follow up (early soft/hard tissue healingusually 6–8 weeks)
Yes; 6 months (early hard tissue healing usually6–8 weeks)
Rating * *Adequacy of follow up of cohorts Description of those lost to follow-up No statementRating *Overall 6* 7*
Study designRodd et al. (2007) Moya-Villaescusa & Sanchez-Perez (2010)Cohort Cohort
SelectionRepresentativeness of the exposedcohort
Truly representative of the average young patientwith dental trauma in the community
Representative of the average patient requiringextraction in the community
Rating * *Selection of non exposed cohort No description of the derivation of non-exposed
cohortNo description of the derivation of non-exposedcohort
RatingAscertainment of exposure Secure record (study model, photograph, clinical
exam)Secure record (radiograph, clinical exam)
Rating * *Demonstration that outcome of interestwas not present at start of study
Yes Yes
Rating * *ComparabilityComparability of cohorts on the basisof the design or analysis
Sample size too small to allow statisticaladjustment of confounders
Controlled for confounding factors (smoking, numberof roots, oral hygiene, periodontal disease)
Rating **OutcomeAssessment of outcome Records (study model, photograph) Records (radiograph)Rating * *Was follow-up long enough foroutcomes to occur
Yes; 4–61 months follow up (early soft/hard tissuehealing usually 6–8 weeks)
Yes; 3 months follow up (early hard tissue healingusually 6–8 weeks)
Rating * *Adequacy of follow up of cohorts No statement No statementRatingOverall 5* 7*
8 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

loss of 3.75 ± 0.63 mm when the buccal plate
was lost during extraction. One study (Moya-
Villaescusa & Sanchez-Pérez 2010) further
discerned between the bone loss at 3 months
after extraction of single-rooted teeth
(4.16 ± 0.32 mm) vs. multiple-rooted teeth
(4.48 ± 0.39 mm loss), although the differ-
ence was not statistically significant. The
average bone loss when both groups were
combined was 4.32 ± 0.24 mm.
Percentage change of vertical linear hard tissuealteration
All the four re-entry studies (Lekovic et al.
1997, 1998; Camargo et al. 2000; Pelegrine
et al. 2010) utilizing a titanium pin or screw
had data on the baseline internal socket
height. This facilitated a calculation of the
percentage reduction of the vertical dimen-
sion of the alveolus post-extraction as fol-
lows:
%vertical linear change #hard tissue$
" vertical linear resortion #hard tissue$baseline internal socket height
The calculated percentage vertical change
of the alveolar hard tissue ranged from 11%
to 22% (Fig. 4) at buccal sites, 6 months
post-extraction.
Horizontal linear hard tissue alteration
A total of eight studies (Lekovic et al. 1997,
1998; Camargo et al. 2000; Iasella et al. 2003;
Barone et al. 2008; Kerr et al. 2008; Aimetti
et al. 2009; Pelegrine et al. 2010) reported on
horizontal changes over time in the hard tis-
sue at the level of the alveolar crest (Fig. 5).
Two studies (Kerr et al. 2008; Aimetti et al.
2009) reported 3-month horizontal reduction
to be between 2.20 and 3.20 mm; another
study (Barone et al. 2008) reported 7-month
reduction to be 4.5 ± 0.8 mm. Lekovic et al.
(1997, 1998), Camargo et al. (2000), Iasella
et al. (2003) and Pelegrine et al. (2010) docu-
mented 6-month horizontal reduction in the
hard tissue of the alveolar ridge to be 4.40,
4.56, 3.06, 2.63 and 2.46 mm respectively.
The five latter studies (Lekovic et al. 1997,
1998; Camargo et al. 2000; Iasella et al. 2003
and Pelegrine et al. 2010) have quite a few
methodological similarities, however, results
of the heterogeneity testing reveal that there
is considerable heterogeneity between the
Table 4. Characteristics of studies included for hard tissue change only
TitleAuthor,publishing year Species QA Tissue Methods
Samplesize
No. ofextractionsites
Morphologic changes of the mandible after extractionand wearing of denture
Carlsson 1967 human CCT Hard Radio 17 5–6 per pt
Effect of chlorhexidine(0.12%) rinses on periodontaltissue healing after tooth extraction(II)radiographicparameters
Bragger 1994 Human RCCT Hard Radio 12 21
A bone regeneration approach to alveolar ridgemaintenance following tooth extraction. Report of10 cases
Lekovic 1997 Human CCT Hard Re-entry (pin) 10 10
Preservation of alveolar bone in extraction socketsusing bioabsorbable membranes
Lekovic 1998 Human RCCT Hard Re-entry(pin 2–5 mm)
16 16
Influence of bioactive glass on changes in alveolarprocess dimensions after exodontia
Camargo 2000 Human CCT Hard Re-entry(pin 1–8 mm)
16 16
Ridge preservation with freeze-dried bone allograftand a collagen membrane compared to extractionalone for implant site development: a clinical andhistological study in humans
Iasella 2003 Human RCCT Soft+ hard
Re-entry(stent)
12 12
Ridge preservation following tooth extraction usinga polylactide and polyglycolide sponge as space filler:a clinical and histological study in humans
Serino 2003 Human CCT Hard Re-entry(stent)
12 13
Bone healing and soft tissue contour changesfollowing single-tooth extraction: a clinical andradiographic 12-month prospective study
Schropp 2003 Human Cohort Hard Radio 46 46
Randomized study evaluating recombinant humanbone morphogenetic protein-2 for extraction socketaugmentation
Fiorellini 2005 Human RCCT Hard CT scan 20 ?
Smoking may affect the alveolar process dimensionsand radiographic bone density in maxillary extractionsites: a prospective study in humans
Saldanha 2006 Human Cohort Hard Radio 21 21
Xenograft vs. extraction alone for ridge preservationafter tooth removal: a clinical and histomorphometricstudy
Barone 2008 Human RCCT Hard Re-entry(stent)
20 20
The effect of ultrasound on bone dimension changesfollowing extraction: a pilot study
Kerr 2008 Human RCCT Hard CBVT (refplate)
12 12
Clinical and histological healing of human extractionsockets filled with calcium sulphate
Aimettl 2009 Human RCCT Hard Re-entry(stent)
18 18
Magnesium-enriched hydroxyapatite compared tocalcium sulphate in the healing of human extractionsockets: radiographic and histomorphometricevaluation at 3 months
Crespi 2009 Human RCCT Hard Radio 15 15
Measurement of ridge alterations following toothremoval:a radiographic study in humans
Moya-Villaescusa2010
Human Cohort Hard Radio 100 100
Clinical and histomorphometric evaluation ofextraction sockets treated with an autologous bonemarrow graft
Pelegrine 2010 Human RCCT Hard Re-entry (pin) 6 15
Socket grafting in the posterior maxilla reduces theneed for sinus augmentation
Rasperini 2010 Human RCCT Hard Stent 3 3
© 2011 John Wiley & Sons A/S 9 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

studies (Q = 17.8, P < 0.05; I2 = 77.6%,
P < 0.05). In this case, although the weighted
mean was calculated by applying the inverse
variance method to arrive at a value of
3.79 ± 0.23 mm horizontal reduction at
6 months (Fig. 6) across all five studies, the
robustness and applicability of this value
should be questioned.
Saldanha et al. (2006) reported the horizon-
tal reduction of the alveolar bone at 0% and
50% the distance from the crest. This study
demonstrated a 6-month reduction of 0.6 and
1.3 mm for non-smokers and smokers respec-
tively at 0% from the alveolar crest and cor-
responding values of 0.1 and 0.8 mm at 50%
from the crest. This study utilized linear
tomography to track the changes.
Of note, Kerr et al. (2008) demonstrated
beautifully that 3 months after tooth extrac-
tion, there was a relative decrease in horizon-
tal ridge reduction as the distance from the
alveolar crest increased (Fig. 7).
Percentage change of horizontal linear hard tissuealteration
All but one study (Kerr et al. 2008) reporting
changes in the ridge width also reported the
baseline ridge width immediately post-extrac-
tion. This facilitated a calculation of the per-
centage reduction of the horizontal dimension
of the alveolus post-extraction as follows:
%horizontallinear change#hard tissue$
" horizontal linear resortion#hard tissue$baseline internal socket height
The calculated percentage horizontal
change of the alveolar hard tissue at the alve-
olar crest ranged from 32% at 3 months, and
between 29% and 63% after 6–7 months
post-extraction (Fig. 8).
Overall hard tissue changes
In general, with regard to vertical dimen-
sional change, we can see a trend where
there is a greater reduction on the buccal and
lingual sites as compared to the mesial and
distal sites. Looking at the horizontal dimen-
sional change, there is a distinct pattern of
resorption where the resorption decreases
with increased distance from the alveolar
crest. Overall, the observed horizontal resorp-
tion of the hard tissues (29–63%) is far
greater than the resorption in the vertical
dimension (11–22%), over an observation per-
iod of 3–7 months. It can be seen that the
bulk of the resorption occurs in the first
3 months post-extraction, and the changes
are much more subtle thereafter.
Fig. 2. Vertical (linear) hard tissue change for re-entry
studies only.
Fig. 3. Vertical (linear) hard tissue change for re-entry
studies only; weighted means shown.
Fig. 4. Vertical (linear) hard tissue percentage change in
four studies.
Fig. 5. Horizontal (linear) hard tissue change for re-
entry studies only.
Fig. 6. Horizontal (linear) hard tissue change for re-
entry studies only; weighted means shown.
10 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

Soft tissue changes
Only a single study (Iasella et al. 2003)
reported on longitudinal changes of soft tis-
sue dimensions in the alveolus post-extrac-
tion (Tables 5 and 7). This study
demonstrated a 0.4–0.5 mm gain of soft tis-
sue thickness at 6 months, measured at buc-
cal and lingual sites 3 mm from the alveolar
crest. Occlusally, soft tissue with thickness
of 2.1 mm developed after 6 months to com-
plete soft tissue coverage of the wound
(Fig. 9).
Combined hard and soft tissue changes
To date, a total of five studies (Carlsson &
Persson 1967; Yilmaz et al. 1998; Schropp
et al. 2003; Rodd et al. 2007; Oghli & Stevel-
ing 2010) presented data on the longitudinal
change in the combined hard and soft tissue
dimension of the alveolus post-extraction
(Tables 6 and 7). One study (Carlsson & Pers-
son 1967) utilized lateral cephalometric radi-
ography whereas study casts were employed
in the other four studies (Yilmaz et al. 1998;
Schropp et al. 2003; Rodd et al. 2007; Oghli
& Steveling 2010). Vertical and horizontal
linear tissue alterations were reported inde-
pendently or in combination; in one study
(Rodd et al. 2007) the overall areal change of
the alveolar hard and soft tissue combined,
was reported.
Vertical linear combined hard and soft tissuealteration
Three studies (Carlsson & Persson 1967; Yil-
maz et al. 1998 and Schropp et al. 2003)
addressed the combined hard and soft tissue
changes in the vertical dimension of the alve-
olus.
With the aid of lateral cephalometric radi-
ography, Carlsson & Persson (1967) was able
to demonstrate the combined hard and soft
tissue changes of the mandibular alveolus in
the vertical dimension over time. The verti-
cal reductions of the conjugated tissue
dimension from baseline were 2.1 mm at
2 months, 2.9 mm at 4 months, 3.4 mm at
6 months and 4.0 mm at 12 month. This
degree of resorption of the combined hard
and soft tissues followed a similar trend as
that of hard tissue alone.
Utilizing sectioned study casts, Yilmaz
et al. (1998) demonstrated a vertical reduc-
tion of 0.1 ± 0.52 mm and 0.5 ± 0.76 mm at
Fig. 7. Horizontal (linear) hard tissue change with
respect to distance from alveolar crest.
Fig. 8. Horizontal (linear) hard tissue percentage
change.
Table 5. Characteristic of study included for soft tissue change only
TitleAuthor,Publishing Year Species QA Tissue Methods Sample size
No. ofextraction site
Ridge preservation with freeze-dried bone allograftand a collagen membrane compared to extractionalone for implant site development: a clinical andhistological study in humans
Iasella 2003 Human RCCT Soft + hard Re-entry (stent) 12 12
Table 6. Characteristics of studies included for both hard and soft tissue changes combined
Title Authors Species QA Tissue Method Sample sizeNo. ofextraction sites
Morphologic changes of the mandible after extractionand wearing of denture
Carlsson 1967 Human CCT Soft + hard Radio 17 5/6 per pt
Alveolar ridge reconstruction and/or preservationusing root form bioglass cones
Yilmaz 1998 Human CCT Soft + hard Cast 5 10
Bone healing and soft tissue contour changesfollowing single-tooth extraction: A clinical andradiographic 12-month prospective study
Schropp 2003 Human CCT Soft + hard Cast 46 46
Change in supporting tissue following loss of apermanent maxillary incisor in children
Rodd 2007 Human Cohort Soft + hard Cast 16 16
Ridge preservation following tooth extraction:A comparison between atraumatic extraction andsocket seal surgery
Oghli 2010 Human RCCT Soft + hard Cast 72 101
Fig. 9. Change in soft tissue dimensions over time.
© 2011 John Wiley & Sons A/S 11 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

3 and 12 months respectively, post-extrac-
tion of maxillary incisor teeth (Fig. 10).
Schropp et al. (2003) took measurements
from study casts taken immediately after as
well as 3, 6 and 12 months after extraction
of maxillary posterior teeth. Taking the
occlusal surfaces of adjacent teeth as refer-
ence, a reduction of 0.1 mm at 3 months
was followed by a net gain of 0.1 mm at
6 months and 0.4 mm at 12 months of the
buccal sites. Lingual sites demonstrated a
loss of 0.8–0.9 mm between 3 and 6 months,
Table 7. Overall results from all studies
Author,Publishing Year Species Tissue Methods
Samplesize
No. ofextractionsites
Vertical dimensionalchange
Horizontal dimensionalchange
Carlsson 1967 Human Hard Radio 17 5–6 per pt 2 month: %2.0(0.9) 2 month: %2.2(1.1)4 month: %2.9(1.7) 12 month: %3.6(0.5)6 month: %3.4(2.1) 60 month: %4.0(1.5)12 month: %4.1(2.7)24 month: %4.9(3.7)60 month: %7.3(3.7)
Bragger 1994 Human Hard Radio 12 21 1 month: %0.61(0.67)2 month: %0.67(0.66)3 month: %1.19(1.50)6 month: %0.93(0.74)
Lekovic 1997 Human Hard Re-entry (pin) 10 10 6 month: %1.2(0.13) 6 month: %4.4(0.61)Lekovic 1998 Human Hard Re-entry (pin2–
5 mm)16 16 6 month: %1.50(0.26) 6 month: %4.56(0.33)
Camargo 2000 Human Hard Re-entry (pin1–8 mm)
16 16 6 month: %1.00(2.25) 6 month: %3.06(2.41)
Iasella 2003 Human Soft+hard
Re-entry (stent) 12 12 6 month: B %0.9(1.6) 6 month: %2.6(2.3)L %0.4(1.0)M %1.0(0.8)D %0.8(0.8)
Iasella 2003 Human Soft Re-entry (stent) 12 12 6 month: B 0.4(0.6)L 0.5(1.5)(Soft tissue thickness change)
Serino 2003 Human Hard Re-entry (stent) 12 13 6 month: B %0.8(1.6)M %0.6(1.0)D %0.8(1.5)
Schropp 2003 Human Hard Radio 46 46 12 month: M %0.3D %0.3
Schropp 2003 Human Soft+hard
Cast 46 46 3 month: B %0.1 3 month: %3.8L %0.8 6 month: %5.16 month: B 0.1 12 month: %6.1L %0.912 month: B 0.4L %0.8
Fiorellini 2005 Human Hard CT scan 20 ? 4 month: %1.17(1.23)Saldanha 2006 Human Hard Radio 21 21 6 month: %1.0 to 1.5 6 month: %0.1 to 1.3Barone 2008 Human Hard Re-entry (stent) 20 20 7 month: B %3.6(1.5) 7 month: %4.5(0.8)
L %3.0(1.6)M %0.4(1.2)D %0.5(1.0)
Kerr 2008 Human Hard CBVT(ref plate)
12 12 1 month:B %1.01(0.39) 1 month: %0.16(0.96)L %0.62(0.28) %0.62(0.24)3 month:B %0.95(0.9) %0.26(0.17)L %1.12(0.28) %0.10(0.10)
3 month: %2.20(0.81)%1.30(0.24)%0.59(0.17)%0.28(0.10)
Aimettl 2009 Human Hard Re-entry (stent) 18 18 3 month: B%1.2(0.6)L %0.9(1.1)M %0.5(0.9)D %0.5(1.1)
Crespi 2009 Human Hard Radio 15 15 3 month: %3.75(0.63)Moya-Villaescusa2010
Human Hard Radio 100 100 3 month: %4.32(0.23)
Pelegrine 2010 Human Hard Re-entry (pin) 6 15 6 month: %1.17(0.26)Rasperini 2010 Human Hard Stent 3 3 3 month: %2.2
6 month: %5.7(4.2)Yilmaz 1998 Human Hard Cast 5 10 3 month: %0.1(0.52) 3 month: %0.1(0.23)
12 month: %0.5(0.76) 12 month: %0.4(0.48)Rodd 2007 Human Hard Cast 16 16 3 month: 15.7%
6 month: 25.3%9 month: 22%(Bone surface area)
Oghli 2010 Human Hard Cast 72 101 3 month: %0.3(0.5)
12 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

with a net loss of 0.8 mm at 12 months
(Fig. 10).
Horizontal linear combined hard and soft tissuealteration
Four studies (Carlsson & Persson 1967; Yil-
maz et al. 1998; Schropp et al. 2003; Oghli &
Steveling 2010) presented data on the com-
bined hard and soft tissue change in the hori-
zontal dimension following extraction.
The only study using radiographic methods
(Carlsson & Persson 1967) demonstrated a
reduction of the alveolar width in the magni-
tude of 2.2 mm at 2 months, which subse-
quently increased to 3.6 mm at 12 months;
this measurement was taken 3 mm from the
alveolar crest.
Study casts were used in some of the stud-
ies (Yilmaz et al. 1998; Schropp et al. 2003;
Oghli & Steveling 2010) to evaluate the
change in the horizontal dimension (Fig. 11).
Yilmaz et al. (1998) showed a 3- and 12-
month reduction in width of 0.1 ± 0.23 mm
and 0.4 ± 0.48 mm respectively, while Oghli
& Steveling (2010) reported a 3-month reduc-
tion of 0.3 ± 0.5 mm. Horizontal resorption
of the alveolar hard and soft tissue between 3
and 12 months was also reported by Schropp
et al. (2003); at 3 months the resorption was
3.8 mm, this increased to 5.1 mm at
6 months and culminated to a value of
6.1 mm at 12 months.
The latter three studies (Yilmaz et al.
1998; Schropp et al. 2003; Oghli & Steveling
2010) had quite many similarities and an
attempt to calculate the weighted means for
these three studies was launched. However,
the study by Schropp et al. (2003) failed to
provide any information on the standard
deviations in the study, so it was impossible
to utilize the inverse variance method to cal-
culate the weighted means.
Cross-sectional surface area alteration of combinedalveolar hard and soft tissues
A single study reported on change in alveolar
surface area of the hard and soft tissues com-
bined (Rodd et al. 2007); measurements were
obtained from study casts acquired prior to,
and at 3, 6 and 9 months following extrac-
tion of maxillary central incisors in children.
The reductions in surface area were presented
as a percentage of the surface area on the pre-
extraction cast, and were as follows: 15.7%
at 3 months, 25.3% at 6 months and 22% at
9 months.
Overall combined hard and soft tissue changes
With the aid of various assessment methods,
a longitudinal change of the combined hard
and soft tissues in the vertical dimension
was found to be anywhere between a loss of
4.0 mm to a gain of 0.4 mm over a period of
2–12 months.
Study casts and radiographs were employed
to assess the reduction of the combined hard
and soft tissues in the horizontal dimension.
This reduction was demonstrated to be
between 0.1 and 6.1 mm when the observa-
tion periods varied from 3 to 12 months, and
the measurements were taken at the alveolar
crest. When the measurements were taken
3 mm apical to the alveolar crest, the corre-
sponding horizontal reductions of the com-
bined hard and soft tissues were 2.2 mm at
2 months and 3.6 mm at 12 months. Reduc-
tions in cross-sectional surface area of the tis-
sues were up to 22% after 9 months.
Mimicking the changes of the alveolar hard
tissue, there is a similar pattern of resorption
when we look at the combined hard and
soft tissue entity; the horizontal alteration is
always more substantial than the vertical
change.
Discussion
The 20 included studies in this systematic
review were of different study designs and
measured dimensional change in various
ways.
Eleven randomized controlled clinical tri-
als, five controlled clinical trials and four
cohort studies were included in this review.
It is common knowledge that randomized
controlled clinical trials and the systematic
review of randomized controlled clinical tri-
als provide the highest level of evidence
related to intervention and therapy. However,
in the case of post-extractional dimensional
changes of the alveolar hard and soft tissues,
there are no randomized controlled clinical
trials where the control procedure is where
the tooth was left in situ and the test proce-
dure was extraction. Hence, the cohort stud-
ies where post-extraction alveolar hard and
soft tissues changes were monitored longitu-
dinally might provide better insight and be
the more appropriate study design.
The three main measuring methods uti-
lized were: (i) re-entry (ii) imaging and (iii)
study models. The re-entry method consti-
tuted of elevating a flap during extraction
and again at re-evaluation. All the studies
using the re-entry method measured the
parameters from a fixed reference, namely an
acrylic stent or a titanium pin or screw. The
imaging method included the utilization of
periapical radiographs, lateral cephalometric
radiography, or computer tomography. The
method where study models were utilized
required that study impressions be taken
before, or immediately after extraction, and
again at re-evaluation.
Re-entry studies evaluated hard tissue as
well as soft tissues as separate entities, while
imaging studies evaluated either hard tissue
dimension only, or the combined hard and
soft tissue changes. Study model studies
focused on combined hard and soft tissue
dimensional changes. During data analysis
process, we subdivided the data into different
groups, mainly according to measurement
methods and the tissues involved. The
groups include (i) hard tissue group, (ii) soft
tissue group, and (iii) combined hard and soft
tissue group.
Heterogeneity assessment
The 20 included studies had different obser-
vation time points, methodologies, and
Fig. 10. Vertical (linear) change of hard and soft tissues
combined.
Fig. 11. Horizontal (linear) change of hard and soft tis-
sues combined.
© 2011 John Wiley & Sons A/S 13 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

measurement methods. Heterogeneity assess-
ment was performed in six re-entry studies
(Lekovic et al. 1997, 1998; Camargo et al.
2000; Iasella et al. 2003; Serino et al. 2003
and Pelegrine et al. 2010) calculating mean
vertical hard tissue change, and five studies
(Lekovic et al. 1997, 1998; Camargo et al.
2000; Iasella et al. 2003 and Pelegrine et al.
2010,) calculating horizontal hard tissue
change. These studies had similarity in terms
of the method of measurements employed.
The studies all employed re-entry methods,
utilizing an acrylic stent or a titanium pin or
screw as a fixed reference from which to
measure the dimensional changes. The differ-
ences in sample sizes, different behaviours of
study populations, varied observation time
points and measurement parameters contrib-
uted to the heterogeneity. Although weighted
means were calculated, the resultant values
should really only be used for reference pur-
poses. The robustness and applicability of the
weighted means should be interpreted with
caution.
Hard tissue vertical dimensional change
Buccal/lingual vs. mesial/distal
Three studies (Iasella et al. 2003; Barone
et al. 2008; Aimetti et al. 2009) measured
vertical dimensional changes of all the buc-
cal, lingual, mesial and distal bone plates.
Two of the three studies, namely Barone
et al. (2008) and Aimetti et al. (2009), demon-
strated that buccal/lingual sites (0.9–3.6 mm
loss at 3–7 months) had more resorption than
mesial/distal sites (0.4–0.5 mm loss at 3–
7 months). Referring to the calculated values
of the respective weighted mean, buccal bone
plates (1.24 mm loss at 3–7 months) also had
a tendency to resorb more than mesial/distal
bone sites (0.8–0.84 mm at 3–7 months)
(Fig. 2). One possible explanation for this
trend is that the mesial and distal bone levels
are partially determined by the presence or
absence of neighbouring teeth; mesial/distal
bone levels are held stable by the presence of
adjacent teeth.
Buccal vs. lingual
Iasella et al. (2003), Barone et al. (2008) and
Aimetti et al. (2009) measured vertical
dimensional changes at both buccal and lin-
gual bone plates. All three studies showed
that the buccal plate resorption (0.9–3.6 mm
at 3–7 months) was of greater magnitude
than that of the lingual plate (0.4–3 mm at 3
–7 months). This finding was similar to pre-
vious studies in the canine model (Araujo &
Lindhe 2005; Araujo et al. 2005). This pattern
of resorption can be explained by the bundle
bone concept as proposed by Araujo & Lind-
he (2005). According to this theory, a larger
proportion of the buccal plate is made up of
bundle bone relative to the lingual plate; as
bundle bone is a tooth-dependent tissue, it is
quickly resorbed after tooth extraction and
with its resorption, a substantial portion of
the buccal plate is lost. In our review of the
literature, however, the relative height differ-
ence between the buccal and lingual bone
plates in humans was less marked compared
to the canine model by Araujo & Lindhe
(2005). The relative difference in height of
the buccal and lingual plate is estimated to
be around 0.3–0.6 mm over a period of 3 and
7 months, in our review. One possible expla-
nation for the observed differences between
human models and canine models is that the
buccal plate in humans is on average equally
prone to resorption as the lingual aspect of
the ridge (Van der Weijden et al. 2009).
Mesial vs. distal
Four studies (Iasella et al. 2003; Serino et al.
2003; Barone et al. 2008 and Aimetti et al.
2009) measured vertical dimensional changes
of both mesial and distal bone plates. All four
studies showed the extent of resorption to be
between 0.4 and 0.8 mm over an observation
period of 3–7 months.
Hard tissue vertical dimensional percentagechange
Lekovic et al. (1997, 1998), Camargo et al.
(2000), Pelegrine et al. (2010) reported base-
line data of the internal socket height imme-
diately post-extraction. Internal socket height
is a measurement from buccal bone crest to
the bottom of the extraction socket. The pro-
vision of baseline internal socket height
enabled us to calculate the percentage change
in height of the buccal bone wall relative to
the baseline height of the buccal bone wall
over time. The percentage change reflected
the amount of vertical resorption of the buc-
cal plate only; this was found to be between
11% and 22% six months post-extraction.
Percentage changes of lingual, mesial and
distal bony plates could not be calculated due
to lack of baseline data, but it is expected to
be less than 11–22%, as the amount of
resorption in these areas have been shown to
be of a comparatively lesser magnitude. Cor-
respondingly, from this this percentage, we
can interpret that there might be 78–89%
bone fill of the original socket height, calcu-
lated as percentage vertical bone fill equals
one minus vertical dimensional percentage
change.
Hard tissue horizontal dimensional change
Five re-entry studies (Lekovic et al. 1997,
1998; Camargo et al. 2000; Iasella et al. 2003;
Pelegrine et al. 2010) showed that there was
range of 2.46–4.56 mm horizontal bone loss
and weighted mean resorption of 3.79 mm at
6 months. However, theses studies only pro-
vided data for horizontal resorption at the
level of the alveolar crest, no data was avail-
able on magnitude of horizontal resorption a
distance away from the alveolar crest. Kerr
et al. (2008) demonstrated a relative decrease
in horizontal ridge reduction as the distance
from the alveolar crest increased. This find-
ing was similar to a dog study done by Ara-
ujo & Lindhe (2009), which observed more
resorption at coronal third and least resorp-
tion at apical third of the alveolar ridge.
Hence, it is expected that the amount of hor-
izontal resorption might be less than
weighted mean of 3.79 mm at 6 months
when the measurement is taken at a distance
from the alveolar crest.
Hard tissue horizontal dimensional percentagechange
There was 32% reduction at 3 months, and
29–63% reduction in horizontal dimension
at 6 months. This demonstrated that possi-
bly more than half of the ridge width could
be resorbed after 6 months in some patients.
However, a definite conclusion cannot be
drawn from these data, on whether the
resorption was from the buccal or lingual.
Studies by Pietrokovski & Massler (1967),
Schropp et al. (2003), Araujo & Lindhe
(2005) and Barone et al. (2008) all suggest
that tissue loss is more pronounced on the
buccal aspect than from the lingual or pala-
tal aspect.
Vertical hard tissue vs. horizontal hard tissuechange
The amount of horizontal dimensional
change was found to be greater than that of
the vertical dimension, in both absolute val-
ues and percentage change. Horizontal reduc-
tion (3.79 ± 0.23 mm) was more than vertical
reduction (1.24 ± 0.11 mm on buccal, 0.84 ±
0.62 mm on mesial and 0.80 ± 0.71 mm on
distal) at 6 months. Percentage vertical
change was 11–22% at 6 months while per-
centage horizontal change was 32% at
3 months, and 29–63% between 6 and
7 months.
Soft tissue changes
Only one study by Iasella et al. (2003) was
found to have measured soft tissue thickness
change after extraction. There was a 0.4–
14 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

0.5 mm gain in soft tissue thickness on buc-
cal and lingual sites at 6 months. Interest-
ingly, from this study, a difference was found
in the change of soft tissue thickness over a
natural healing socket, and sockets aug-
mented using bio-resorbable membranes and
grafts. There was net gain of soft tissue
thickness in the natural healing group and a
net loss in the augmented group. One possi-
ble explanation for this observation was that
the membrane or graft placed might have
interfered with the soft tissue vascularity in
the augmented group. We must remember
that the vascular supply to the soft tissue is
derived from the underlying bone, and the
placement of membranes or grafts might
interfere with re-vascularization of the soft
tissues. In contrast, there is no interposing
material between the bone and the overlying
soft tissues in the naturally healing sockets.
Although there was an observed gain in soft
tissue thickness over a naturally healing
socket, a robust conclusion cannot be drawn
from this single study.
In addition, this study also demonstrated a
trend where the lingual soft tissues were
thicker than that on the buccal; lingual soft
tissues were nearly twice as thick. The meth-
ods and materials in the study could explain
this difference; majority of teeth extracted
within the study were maxillary teeth where
palatal soft tissue is expected to be much
thicker than that of the buccal. Hence, this
finding may only be applicable to the maxil-
lary extraction sockets, but not mandibular
ones. Note that this study only had a sample
size of 12 non-molar extraction sockets,
hence we should be cautious when trying to
interpret the results of this study.
Vertical combined hard and soft tissue change
Two studies by Yilmaz et al. (1998) and Sch-
ropp et al. (2003) demonstrated very subtle
changes in the vertical dimension of the hard
and soft tissues combined, between 3 and
12 months post-extraction. The changes ran-
ged from a gain of 0.1 mm to a loss of
0.9 mm at 6 months and a gain of 0.4 mm to
a loss of 0.8 mm at 12 months. Schropp et al.
(2003) also observed a small increase buccally
and a reduction orally.
Horizontal combined hard and soft tissuechange
Three studies (Yilmaz et al. 1998; Schropp
et al. 2003 and Oghli & Steveling 2010)
reported data on horizontal hard and soft tis-
sue changes. The studies by Yilmaz et al.
(1998) and Schropp et al. (2003) had a follow-
up of up to 12 months; both studies exhib-
ited a trend where there was a rapid reduc-
tion in first 3 months and gradual change
from thereafter, up to 12 months. Weighted
mean reduction showed this change to be
1.3 mm at 3 months and 5.1 mm at
12 months.
Vertical vs. horizontal combined hard and softchange
Hard and soft tissue showed a combined hori-
zontal reduction of 0.1–3.8 mm and 5.1 mm
at 3 and 6 months respectively. Correspond-
ingly, in the vertical dimension, this change
was between 0.1 and 0.8 mm reduction at
3 months, and 0.1 mm gain to 0.9 mm
reduction at 6 months. Overall, the demon-
strated horizontal change was more substan-
tial than the vertical change.
Combined hard and soft tissue change vs. hardtissue change only
In the horizontal dimension, the combined
hard and soft tissue reduction was 5.1 mm at
6 months, while the corresponding hard
tissue reduction was between 2.46 and
4.56 mm, with a weighted mean reduction of
3.79 mm.
Hence, at 6 months post-extraction, the
combined hard and soft tissues demonstrated
a tendency towards a more substantial reduc-
tion than hard tissue only; this observation is
not corroborated in the vertical aspect.
In the vertical dimension, when consider-
ing only hard tissue change (loss of 0.4–
1.5 mm at 6 months), the magnitude of this
change was greater than that of the hard and
soft tissues combined (0.1 mm gain to
0.9 mm reduction at 6 months). A plausible
explanation might be that the increase in soft
tissue thickness (gain of 2.1 mm occlusally
vs. gain of only 0.4–0.5 mm on buccal/lin-
gual) compensated for the reduction in hard
tissue height.
Possible factors affecting dimensional changeafter tooth extraction
Flap vs. flapless
Using a canine model, Fickl et al. (2008a)
demonstrated that there was significant dif-
ference of the extent of bone resorption
between flap and flapless extractions. The
flapless group had lower extent of resorption
compared to the flap group. Blanco et al.
(2008) also showed similar trend in another
study, although the study was investigating
ridge alterations after immediate implants
with or without flap. However, Araujo &
Lindhe (2009) found that the differences
between the flap and flapless groups in their
study were negligible after 6 months. Hence,
raising a flap during extraction may only
affect the short-term dimensional alterations
of the alveolar ridge.
Overeruption of adjacent teeth
Mizutani & Ishihata (1976) found that the
over-eruption of teeth adjacent to the extrac-
tion socket affected the overall dimensional
change of ridge. The vertical alveolar ridge
height in this study decreased slightly ini-
tially, followed by a gradual increase later on,
which negated the previous reduction or even
surpassed the amount of resorption to result
in a net gain. The study speculated that the
over-eruption of teeth adjacent to extraction
sites might have affected the pattern of
dimensional change observed.
Smoking
Smoking may affect the extent of vertical
reduction of the alveolar ridge after extrac-
tion. Saldanha et al. (2006) showed that
there was a significant difference in dimen-
sional reduction between smoking and non-
smoking groups. There was vertical alveolar
ridge reduction of 1.5 mm in smokers and
1.0 mm in non-smokers, 6 months post-
extraction.
Single-rooted vs. multiple-rooted teeth
Moya-Villaescusa & Sanchez-Perez (2010)
study showed there was no significant differ-
ence in vertical dimensional change between
single-rooted (4.16 mm loss) and multi-rooted
teeth (4.48 mm loss), although there was a
tendency that multi-rooted teeth exhibited
greater resorption of the alveolar ridge.
Chlorhexidine
Rinsing with 15 ml of 0.12% chlorhexidine
digluconate mouthrinse twice daily for
1 month, starting 2 days after extraction may
have some effect on the observed vertical
change of the mesial and distal bone. Bragger
et al. (1994) showed that patients rinsing for
1 month with a placebo solution lost almost
1 mm of bone height over a 6-month period
after extraction, while in patients rinsing
with the chlorhexidine solution, the crestal
alveolar bone level was maintained.
Immediate denture
Carlsson & Persson (1967) showed that there
was no significant difference in alveolar
dimensional change between patients with
immediate or conventional dentures in the
long-term. Take note, however, that the
usage of immediate dentures had a tendency
to affect dimensional change in short-term,
© 2011 John Wiley & Sons A/S 15 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

but the effect would be negligible after
2 years post-extraction.
Bone resorption pattern after 12 months
Only one study (Carlsson & Persson 1967)
followed dimensional changes in human
alveolar ridge for up to 5 years. This study
displayed a similar pattern where there was a
relatively rapid reduction in the first
6 months in both vertical and horizontal
dimension, followed by a gradual reduction
thereafter; the reduction continued at a
steady rate for up to 5 years. This finding
could suggest that bone resorption will con-
tinue throughout life once the teeth are
extracted. Take note, however, that all the
patients in this study wore complete den-
tures; dentures were inserted 2 months after
extractions in the conventional group and
immediately after extractions in the immedi-
ate group. We can speculate that the usage of
removable complete dentures may also affect
the pattern of resorption of the alveolar tis-
sues.
Conclusions
In conclusion, the studies included in this
review demonstrated that horizontal bone
loss (29–63%, 2.46–4.56 mm, weighted mean
3.79 mm at 6 months) was more substantial
than vertical bone loss (11–22%, 0.8–1.5 mm,
weighted mean 1.24 mm at 6 months) after
tooth extraction. The buccal aspect generally
displayed more resorption than the lingual/
palatal aspect. There is an observed resorp-
tion pattern of rapid reduction in the first 3–
6 months, followed by gradual reduction
thereafter, throughout life.
Soft tissue on the buccal and lingual sur-
faces of the alveolar ridge has a tendency to
increase in thickness after extraction, as
reported in one study; the significance of this
finding is as yet unknown. The same study
also documented that 6 months post-extrac-
tion, a soft tissue cover of 2.1 mm in thick-
ness developed over the original socket; this
soft tissue thickness that develops post-
extraction may mask the real extent of hard
tissue resorption and impact on the overall
outcome of any reconstructive efforts, espe-
cially with regard to aesthetics. However,
more studies might be required to arrive at a
more definitive value of soft tissue changes
post-extraction, and clarify the influence of
this change.
Overall, dimensional alterations of the
alveolar hard and soft tissues can be quite
extensive, and an astute clinician will do
well to understand the pattern and sequelae
of these changes, to arrive at predictable
treatment outcomes
Acknowledgement: This study has
been made possible by an educational grant
of the Osteology Foundation, Lucerne,
Switzerland.
References
Aimetti, M., Romano, F., Griga, F.B. & Godio, L.
(2009) Clinical and histologic healing of human
extraction sockets filled with calcium sulfate.
The International Journal of Oral & Maxillofa-
cial Implants 24: 902–929.
Araujo, M.G. & Lindhe, J. (2005) Dimensional ridge
alterations following tooth extraction. An experi-
mental study in the dog. Journal of Clinical Peri-
odontology 32: 212–218.
Araujo, M.G. & Lindhe, J. (2009) Ridge alterations
following tooth extraction with and without flap
elevation: an experimental study in the dog. Clin-
ical Oral Implants Research 20: 545–549.
Araujo, M.G., Sukekava, F., Wennstrom, J.L. &
Lindhe, J. (2005) Ridge alterations following
implant placement in fresh extraction sockets: an
experimental study in the dog. Journal of Clinical
Periodontology 32: 645–652.
Barone, A., Aldini, N.N., Fini, M., Giardino, R.,
Calvo Guirado, J.L. & Covani, U. (2008) Xenograft
versus extraction alone for ridge preservation after
tooth removal: a clinical and histomorphometric
study. Journal of Periodontology 79: 1370–1377.
Blanco, J., Nunez, V., Aracil, L., Munoz, F. & Ra-
mos, I. (2008) Ridge alterations following imme-
diate implant placement in the dog: flap versus
flapless surgery. Journal of Clinical Periodontol-
ogy 35: 640–648.
Botticelli, D., Berglundh, T. & Lindhe, J. (2004)
Hard-tissue alterations following immediate
implant placement in extraction sites. Journal of
Clinical Periodontology 31: 820–828.
Bragger, U., Schild, U. & Lang, N.P. (1994) Effect of
chlorhexidine (0.12%) rinses on periodontal tissue
healing after tooth extraction. (II). Radiographic
parameters. Journal of Clinical Periodontology
21: 422–430.
Camargo, P.M., Lekovic, V., Weinlaender, M., Klok-
kevold, P.R., Kenney, E.B., Dimitrijevic, B.,
Nadic, M., Jancovic, S. & Orsini, M. (2000) Influ-
ence of bioactive glass on changes in alveolar pro-
cess dimensions after exodontia. Oral Surgery
Oral Medicine Oral Pathology Oral Radiology &
Endodontology 90: 581–586.
Carlsson, G.E. & Persson, G. (1967) Morphologic
changes of the mandible after extraction and
wearing of dentures. A longitudinal, clinical, and
x-ray cephalometric study covering 5 years. Od-
ontologisk Revy 18: 27–54.
Cohn, S.A. (1966) Disuse atrophy of the periodon-
tium in mice following partial loss of function.
Archives of Oral Biology 11: 95–105.
Crespi, R., Cappare, P. & Gherlone, E. (2009) Mag-
nesium-enriched hydroxyapatite compared to cal-
cium sulfate in the healing of human extraction
sockets: radiographic and histomorphometric
evaluation at 3 months. Journal of Periodontol-
ogy 80: 210–218.
Fickl, S., Zuhr, O., Wachtel, H., Bolz, W. & Huerz-
eler, M. (2008a) Tissue alterations after tooth
extraction with and without surgical trauma: a
volumetric study in the beagle dog. Journal of
Clinical Periodontology 35: 356–363.
Fiorellini, J.P., Howell, T.H., Cochran, D., Malm-
quist, J., Lilly, L.C., Spagnoli, D., Toljanic, J.,
Jones, A. & Nevins, M. (2005) Randomized study
evaluating recombinant human bone morphoge-
netic protein-2 for extraction socket augmenta-
tion. Journal of Periodontology 76: 605–613.
Iasella, J.M., Greenwell, H., Miller, R.L., Hill, M.,
Drisko, C., Bohra, A.A. & Scheetz, J.P. (2003)
Ridge preservation with freeze-dried bone allo-
graft and a collagen membrane compared to
extraction alone for implant site development: a
clinical and histologic study in humans. Journal
of Periodontology 74: 990–999.
Kerr, E.N., Mealey, B.L., Noujeim, M.E., Lasho, D.
J., Nummikoski, P.V. & Mellonig, J.T. (2008) The
effect of ultrasound on bone dimensional changes
following extraction: a pilot study. Journal of
Periodontology 79: 283–290.
Lekovic, V., Camargo, P.M., Klokkevold, P.R., We-
inlaender, M., Kenney, E.B., Dimitrijevic, B. &
Nedic, M. (1998) Preservation of alveolar bone in
extraction sockets using bioabsorbable mem-
branes. Journal of Periodontology 69: 1044–1049.
Lekovic, V., Kenney, E.B., Weinlaender, M., Han, T.,
Klokkevold, P., Nedic, M. & Orsini, M. (1997) A
bone regenerative approach to alveolar ridge main-
tenance following tooth extraction. Report of 10
cases. Journal of Periodontology 68: 563–570.
Marks, S.C. Jr (1995) The basic and applied biology
of tooth eruption. Connective Tissue Research
32: 149–157.
Marks, S.C. Jr & Schroeder, H.E. (1996) Tooth erup-
tion: theories and facts. Anatomical Record 245:
374–393.
Meier, P. (1953) Variance of a weighted mean. Bio-
metrics 9: 59–73.
Mizutani, H. & Ishihata, N. (1976) Decrease and
increase in residual ridges after extraction of
teeth in monkeys (part I). Bulletin of Tokyo Med-
ical & Dental University 23: 157–168.
Moya-Villaescusa, M.J. & Sanchez-Pérez, A. (2010)
Measurement of ridge alterations following tooth
removal: a radiographic study in humans. Clini-
cal Oral Implants Research 21: 237–242.
Oghli, A.A. & Steveling, H. (2010) Ridge preserva-
tion following tooth extraction: a comparison
between atraumatic extraction and socket seal
surgery. Quintessence International 41: 605–609.
16 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

Pelegrine, A.A., da Costa, C.E., Correa, M.E. &
Marques, J.F. Jr (2010) Clinical and histomorpho-
metric evaluation of extraction sockets treated
with an autologous bone marrow graft. Clinical
Oral Implants Research 21: 535–542.
Pietrokovski, J. (1967) Healing of the socket follow-
ing tooth extraction. Alpha Omegan 60: 126–129.
Pietrokovski, J. & Massler, M. (1967) Alveolar ridge
resorption following tooth extraction. Journal of
Prosthetic Dentistry 17: 21–27.
Pietrokovski, J. & Massler, M. (1971) Residual ridge
remodeling after tooth extraction in monkeys.
Journal of Prosthetic Dentistry 26: 119–129.
Pinho, M.N., Roriz, V.L., Novaes, A.B.Jr, Taba, M.
Jr, Grisi, M.F., de Souza, S.L. & Palioto, D.B.
(2006) Titanium membranes in prevention of
alveolar collapse after tooth extraction. Implant
Dentistry 15: 53–61.
Rasperini, G., Canullo, L., Dellavia, C., Pellegrini,
G. & Simion, M. (2010) Socket grafting in the
posterior maxilla reduces the need for sinus aug-
mentation. International Journal of Periodontics
& Restorative Dentistry 30: 265–273.
Rodd, H.D., Malhotra, R., O’Brien, C.H., Elcock, C.,
Davidson, L.E. & North, S. (2007) Change in sup-
porting tissue following loss of a permanent max-
illary incisor in children. Dental Traumatology
23: 328–332.
Saldanha, J.B., Casati, M.Z., Neto, F.H., Sallum, E.
A. & Nociti, F.H. Jr (2006) Smoking may affect
the alveolar process dimensions and radiographic
bone density in maxillary extraction sites: a pro-
spective study in humans. Journal of Oral &
Maxillofacial Surgery 64: 1359–1365.
Schropp, L., Wenzel, A., Kostopoulos, L. & Karring,
T. (2003) Bone healing and soft tissue contour
changes following single-tooth extraction: a clini-
cal and radiographic 12-month prospective study.
International Journal of Periodontics & Restor-
ative Dentistry 23: 313–323.
Serino, G., Biancu, S., Iezzi, G. & Piattelli, A.
(2003) Ridge preservation following tooth extrac-
tion using a polylactide and polyglycolide sponge
as space filler: a clinical and histological study in
humans. Clinical Oral Implants Research 14:
651–658.
Tallgren, A. (1972) The continuing reduction of
the residual alveolar ridges in complete denture
wearers: a mixed-longitudinal study covering
25 years. Journal of Prosthetic Dentistry 27: 120
–132.
Van der Weijden, F., Dell’Acqua, F. & Slot, D.E.
(2009) Alveolar bone dimensional changes of
post-extraction sockets in humans: a systematic
review. Journal of Clinical Periodontology 36:
1048–1058.
Yilmaz, S., Efeoglu, E. & Kilic, A.R. (1998) Alveolar
ridge reconstruction and/or preservation using
root form bioglass cones. Journal of Clinical Peri-
odontology 25: 832–839.
List of included articles:
Aimetti, M., Romano, F., Griga, F.B. & Godio, L.
(2009) Clinical and histologic healing of human
extraction sockets filled with calcium sulfate.
The International Journal of Oral & Maxillofa-
cial Implants 24: 902–929.
Barone, A., Aldini, N.N., Fini, M., Giardino, R.,
Calvo Guirado, J.L. & Covani, U. (2008) Xenograft
versus extraction alone for ridge preservation
after tooth removal: a clinical and histomorpho-
metric study. Journal of Periodontology 79: 1370–
1377.
Bragger, U., Schild, U. & Lang, N.P. (1994) Effect of
chlorhexidine (0.12%) rinses on periodontal tissue
healing after tooth extraction. (II). Radiographic
parameters. Journal of Clinical Periodontology
21: 422–430.
Camargo, P.M., Lekovic, V., Weinlaender, M., Klok-
kevold, P.R., Kenney, E.B., Dimitrijevic, B.,
Nadic, M., Jancovic, S. & Orsini, M. (2000) Influ-
ence of bioactive glass on changes in alveolar pro-
cess dimensions after exodontia. Oral Surgery
Oral Medicine Oral Pathology Oral Radiology &
Endodontology 90: 581–586.
Carlsson, G.E. & Persson, G. (1967) Morphologic
changes of the mandible after extraction and
wearing of dentures. A longitudinal, clinical, and
x-ray cephalometric study covering 5 years. Od-
ontologisk Revy 18: 27–54.
Crespi, R., Cappare, P. & Gherlone, E. (2009) Mag-
nesium-enriched hydroxyapatite compared to cal-
cium sulfate in the healing of human extraction
sockets: radiographic and histomorphometric
evaluation at 3 months. Journal of Periodontol-
ogy 80: 210–218.
Fiorellini, J.P., Howell, T.H., Cochran, D., Malm-
quist, J., Lilly, L.C., Spagnoli, D., Toljanic, J.,
Jones, A. & Nevins, M. (2005) Randomized study
evaluating recombinant human bone morphoge-
netic protein-2 for extraction socket augmenta-
tion. Journal of Periodontology 76: 605–613.
Iasella, J.M., Greenwell, H., Miller, R.L., Hill, M.,
Drisko, C., Bohra, A.A. & Scheetz, J.P. (2003)
Ridge preservation with freeze-dried bone allo-
graft and a collagen membrane compared to
extraction alone for implant site development: a
clinical and histologic study in humans. Journal
of Periodontology 74: 990–999.
Kerr, E.N., Mealey, B.L., Noujeim, M.E., Lasho, D.
J., Nummikoski, P.V. & Mellonig, J.T. (2008) The
effect of ultrasound on bone dimensional changes
following extraction: a pilot study. Journal of
Periodontology 79: 283–290.
Lekovic, V., Camargo, P.M., Klokkevold, P.R., We-
inlaender, M., Kenney, E.B., Dimitrijevic, B. &
Nedic, M. (1998) Preservation of alveolar bone in
extraction sockets using bioabsorbable mem-
branes. Journal of Periodontology 69: 1044–1049.
Lekovic, V., Kenney, E.B., Weinlaender, M., Han, T.,
Klokkevold, P., Nedic, M. & Orsini, M. (1997) A
bone regenerative approach to alveolar ridge main-
tenance following tooth extraction. Report of 10
cases. Journal of Periodontology 68: 563–570.
Moya-Villaescusa, M.J. & Sanchez-Perez, A. (2010)
Measurement of ridge alterations following tooth
removal: a radiographic study in humans. Clini-
cal Oral Implants Research 21: 237–242.
Oghli, A.A. & Steveling, H. (2010) Ridge preserva-
tion following tooth extraction: a comparison
between atraumatic extraction and socket seal
surgery. Quintessence International 41: 605–609.
Pelegrine, A.A., da Costa, C.E., Correa, M.E. &
Marques, J.F. Jr (2010) Clinical and histomorpho-
metric evaluation of extraction sockets treated
with an autologous bone marrow graft. Clinical
Oral Implants Research 21: 535–542.
Rasperini, G., Canullo, L., Dellavia, C., Pellegrini,
G. & Simion, M. (2010) Socket grafting in the
posterior maxilla reduces the need for sinus aug-
mentation. International Journal of Periodontics
& Restorative Dentistry 30: 265–273.
Rodd, H.D., Malhotra, R., O’Brien, C.H., Elcock, C.,
Davidson, L.E. & North, S. (2007) Change in sup-
porting tissue following loss of a permanent max-
illary incisor in children. Dental Traumatology
23: 328–332.
Saldanha, J.B., Casati, M.Z., Neto, F.H., Sallum, E.
A. & Nociti, F.H. Jr (2006) Smoking may affect
the alveolar process dimensions and radiographic
bone density in maxillary extraction sites: a pro-
spective study in humans. Journal of Oral &
Maxillofacial Surgery 64: 1359–1365.
Schropp, L., Wenzel, A., Kostopoulos, L. & Karring,
T. (2003) Bone healing and soft tissue contour
changes following single-tooth extraction: a clini-
cal and radiographic 12-month prospective study.
International Journal of Periodontics & Restor-
ative Dentistry 23: 313–323.
Serino, G., Biancu, S., Iezzi, G. & Piattelli, A.
(2003) Ridge preservation following tooth extrac-
tion using a polylactide and polyglycolide sponge
as space filler: a clinical and histological study in
humans. Clinical Oral Implants Research 14:
651–658.
Yilmaz, S., Efeoglu, E. & Kilic, A.R. (1998) Alveolar
ridge reconstruction and/or preservation using
root form bioglass cones. Journal of Clinical Peri-
odontology 25: 832–839.
List of excluded full text articles and the reason for exclusion:
Agbaje, J.O., Jacobs, R., Michiels, K., Abu-Ta’a, M.
& van Steenberghe, D. (2009) Bone healing after
dental extractions in irradiated patients: a pilot
study on a novel technique for volume assess-
ment of healing tooth sockets. Clinical Oral
Investigations 13: 257–261.
Exclusion criteria: reported parameters not
relevant or not useful.
© 2011 John Wiley & Sons A/S 17 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

Ahn, J.J. & Shin, H.I. (2008) Bone tissue formation
in extraction sockets from sites with advanced
periodontal disease: a histomorphometric study
in humans. The International Journal of Oral &
Maxillofacial Implants 23: 1133–1138.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Alissa, R., Esposito, M., Horner, K. & Oliver, R.
(2010) The influence of platelet-rich plasma on
the healing of extraction sockets: an explorative
randomised clinical trial. European Journal of
Oral Implantology 3: 121–134.
Exclusion criteria: reported parameters not
relevant or not useful.Altundal, H. & Guvener, O. (2004) The effect of
alendronate on resorption of the alveolar bone fol-
lowing tooth extraction. The International Jour-
nal of Oral & Maxillofacial Surgery 33: 286–293.
Exclusion criteria: reported parameters not
relevant or not useful.Alves-Rezende, M.C. & Okamoto, T. (1997) Effects
of fibrin adhesive material (tissucol) on alveolar
healing in rats under stress. Brazilian Dental
Journal 8: 13–19.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Amemori, H. (1966) An experimental study of
changes in the form of the mandible after extrac-
tion of lower posterior teeth. I. The areal change
of mandibular frontal sections.. Bulletin of Tokyo
Medical & Dental University 13: 59–74.
Exclusion criteria: study carried out on ani-
mals.Anitua, E. (1999) Plasma rich in growth factors: pre-
liminary results of use in the preparation of
future sites for implants. The International Jour-
nal of Oral & Maxillofacial Implants 14: 529–
535.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Araujo, M., Linder, E., Wennstrom, J. & Lindhe, J.
(2008) The influence of bio-oss collagen on heal-
ing of an extraction socket: an experimental
study in the dog. International Journal of Peri-
odontics & Restorative Dentistry 28: 123–135.
Exclusion criteria: reported parameters not
relevant or not useful.Araujo, M.G. & Lindhe, J. (2005) Dimensional ridge
alterations following tooth extraction. An experi-
mental study in the dog.. Journal of Clinical Peri-
odontology 32: 212–218.
Exclusion criteria: only measured relative
difference in height between buccal and lin-
gual plates of the alveolus.Araujo, M.G. & Lindhe, J. (2009a) Ridge alterations
following tooth extraction with and without flap
elevation: an experimental study in the dog. Clin-
ical Oral Implants Research 20: 545–549.
Exclusion criteria: no baseline data avail-
able for comparison, thus unable to arrive at
an estimate of dimensional change over time.Araujo, M.G. & Lindhe, J. (2009b) Ridge preserva-
tion with the use of bio-oss collagen: a 6-month
study in the dog. Clinical Oral Implants
Research 20: 433–440.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.Araujo, M.G., Sukekava, F., Wennstrom, J.L. &
Lindhe, J. (2005) Ridge alterations following
implant placement in fresh extraction sockets: an
experimental study in the dog. Journal of Clin
Periodontology 32: 645–652.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.Ashman, A. & Bruins, P. (1985) Prevention of alveo-
lar bone loss postextraction with htr grafting
material. Oral Surgery Oral Medicine & Oral
Pathology 60: 146–153.
Exclusion criteria: descriptive report on
procedure/technique; commentary.Ashman, A. & Bruins, P. (1987) Prevention of alveo-
lar bone loss postextraction with htr polymer
grafting material. Journal of Oral Implantology
13: 270–281.
Exclusion criteria: descriptive report on
procedure/technique; commentary.Bahat, O., Deeb, C., Golden, T. & Komarnyckij, O.
(1987) Preservation of ridges utilizing hydroxyapa-
tite. International Journal of Periodontics &
Restorative Dentistry 7: 34–41.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.Bergstedt, H., Wictorin, L. & Lundquist, G. (1973)
Transplantation of bone treated with ethylenedia-
mine into tooth sockets in immediate denture
patients. Sven Tandlak Tidskr 66: 39–48.
Exclusion criteria: study subjects had
immediate dentures after extraction, hence
they did not have undisturbed healing post-
extraction.Berkovitz, B.K. (1971) The healing process in the
incisor tooth socket of the rat following root
resection and exfoliation. Archives of Oral Biol-
ogy 16: 1045–1054.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Bianchi, J., Fiorellini, J.P., Howell, T.H., Sekler, J.,
Curtin, H., Nevins, M.L. & Friedland, B. (2004)
Measuring the efficacy of rhbmp-2 to regenerate
bone: a radiographic study using a commercially
available software program. International Journal
of Periodontics & Restorative Dentistry 24: 579–
587.
Exclusion criteria: reported parameters not
relevant or not useful.Boyes-Varley, J.G., Cleaton-Jones, P.E. & Lownie, J.
F. (1988) Effect of a topical drug combination on
the early healing of extraction sockets in the ver-
vet monkey. The International Journal of Oral &
Maxillofacial Surgery 17: 138–141.
Exclusion criteria: no measurements of
alveolar dimensional changes (e.g. description
of healing process or bony shape change, or
histology only).Boyne, P.J. (1995) Use of htr in tooth extraction
sockets to maintain alveolar ridge height and
increase concentration of alveolar bone matrix.
General Dentistry 43: 470–473.
Exclusion criteria: reported parameters not
relevant or not useful.Brandao, A.C., Brentegani, L.G., Novaes, A.B. Jr,
Grisi, M.F., Souza, S.L., Taba Junior, M. & Salata,
L.A. (2002) Histomorphometric analysis of rat
alveolar wound healing with hydroxyapatite alone
or associated to bmps. Brazilian Dental Journal
13: 147–154.
Exclusion criteria: reported parameters not
relevant or not useful.Cardaropoli, G., Araujo, M., Hayacibara, R., Sukek-
ava, F. & Lindhe, J. (2005) Healing of extraction
sockets and surgically produced – augmented and
non-augmented – defects in the alveolar ridge. An
experimental study in the dog.. Journal of Clini-
cal Periodontology 32: 435–440.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Carlsson, G.E., Thilander, H. & Hedegard, B. (1967)
Histologic changes in the upper alveolar process
after extractions with or without insertion of an
immediate full denture. Acta Odontolologica
Scandinavica 25: 21–43.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Carmagnola, D., Adriaens, P. & Berglundh, T.
(2003) Healing of human extraction sockets filled
with bio-oss. Clinical Oral Implants Research
14: 137–143.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Dayan, D., Bodner, L. & Horowitz, I. (1992) Effect
of salivary gland hypofunction on the healing of
extraction wounds: a histomorphometric study in
rats. Journal of Oral & Maxillofacial Surgery 50:
354–358.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Fickl, S., Zuhr, O., Wachtel, H., Bolz, W. & Huerz-
eler, M. (2008b) Tissue alterations after tooth
extraction with and without surgical trauma: a
volumetric study in the beagle dog. Journal of
Clinical Periodontology 35: 356–363.
Exclusion criteria: study carried out on ani-
mals.Fickl, S., Zuhr, O., Wachtel, H., Stappert, C.F.,
Stein, J.M. & Hurzeler, M.B. (2008c) Dimensional
18 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

changes of the alveolar ridge contour after differ-
ent socket preservation techniques. Journal of
Clinical Periodontology 35: 906–913.
Exclusion criteria: study carried out on ani-
mals.Fickl, S., Zuhr, O., Wachtel, H., Bolz, W. & Huerz-
eler, M.B. (2008c) Hard tissue alterations after
socket preservation: an experimental study in the
beagle dog. Clinical Oral Implants Research 19:
1111–1118.
Exclusion criteria: no baseline data avail-
able for comparison, thus unable to arrive at
an estimate of dimensional change over time.Gauthier, O., Boix, D., Grimandi, G., Aguado, E.,
Bouler, J.M., Weiss, P. & Daculsi, G. (1999) A
new injectable calcium phosphate biomaterial for
immediate bone filling of extraction sockets: a
preliminary study in dogs. Journal of Periodontol-
ogy 70: 375–383.
Exclusion criteria: reported parameters not
relevant or not useful.Gorustovich, A., Veinsten, F., Costa, O.R. & Gug-
lielmotti, M.B. (2004) Histomorphometric evalua-
tion of the effect of bovine collagen granules on
bone healing. An experimental study in rats. Acta
Odontologica Latinoamericana 17: 9–13.
Exclusion criteria: reported parameters not
relevant or not useful.Green, L.J., Gong, J.K. & Neiders, M.E. (1969) Rela-
tionship between sr85 uptake and histological
changes during healing in dental extractionwounds
in rats.Archives of Oral Biology 14: 865–872.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Guglielmotti, M.B. & Cabrini, R.L. (1985) Alveolar
wound healing and ridge remodeling after tooth
extraction in the rat: a histologic, radiographic,
and histometric study. Journal of Oral & Maxil-
lofacial Surgery 43: 359–364.
Exclusion criteria: reported parameters not
relevant or not useful.Guglielmotti, M.B., Ubios, A.M. & Cabrini, R.L.
(1985) Alveolar wound healing alteration under
uranyl nitrate intoxication. Journal of Oral
Pathology 14: 565–572.
Exclusion criteria: reported parameters not
relevant or not useful.Guglielmotti, M.B., Ubios, A.M. & Cabrini, R.L.
(1986) Alveolar wound healing after x-irradiation:
a histologic, radiographic, and histometric study.
Journal of Oral & Maxillofacial Surgery 44: 972–
976.
Exclusion criteria: no baseline data avail-
able for comparison, thus unable to arrive at
an estimate of dimensional change over time.Hahn, E., Sonis, S., Gallagher, G. & Atwood, D.
(1988) Preservation of the alveolar ridge with
hydroxyapatite-collagen implants in rats. Journal
of Prosthetic Dentistry 60: 729–734.
Exclusion criteria: study carried out on ani-
mals.Hars, E. & Massler, M. (1972) Effects of fluorides,
cortico-steroids and tetracyclines on extraction
wound healing in rats. Acta Odontologica Scan-
dinavica 30: 511–522.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Horn, Y., Sela, M.N., Shlomi, B., Ulmansky, M. &
Sela, J. (1979) Effect of irradiation-timing on the
initial socket healing in rats. International Jour-
nal of Oral Surgery 8: 457–461.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Hsieh, Y.D., Devlin, H. & McCord, F. (1995) The
effect of ovariectomy on the healing tooth socket
of the rat. Archives of Oral Biology 40: 529–531.
Exclusion criteria: no baseline data avail-
able for comparison, thus unable to arrive at
an estimate of dimensional change over time.Huebsch, R.F. & Hansen, L.S. (1969) A histopatho-
logic study of extraction wounds in dogs. Oral
Surgery Oral Medicine & Oral Pathology 28: 187
–196.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Iino, G., Nishimura, K., Omura, K. & Kasugai, S.
(2008) Effects of prostaglandin e1 application on
rat incisal sockets. The International Journal of
Oral & Maxillofacial Implants 23: 835–840.
Exclusion criteria: reported parameters not
relevant or not useful.Iizuka, T., Miller, S.C. & Marks, S.C. Jr (1992)
Alveolar bone remodeling after tooth extraction
in normal and osteopetrotic (ia) rats. Journal of
Oral Pathology & Medicine 21: 150–155.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.Indovina, A. Jr & Block, M.S. (2002) Comparison of 3
bone substitutes in canine extraction sites. Journal
of Oral & Maxillofacial Surgery 60: 53–58.
Exclusion criteria: reported parameters not
relevant or not useful.Kangvonkit, P., Matukas, V.J. & Castleberry, D.J.
(1986) Clinical evaluation of durapatite sub-
merged-root implants for alveolar bone preserva-
tion. The International Journal of Oral &
Maxillofacial Surgery 15: 62–71.
Exclusion criteria: study subjects had
immediate dentures after extraction, hence
they did not have undisturbed healing post-
extraction.Lavelle, C.L. (1985) Preliminary study of mandibu-
lar shape after tooth loss. Journal of Prosthetic
Dentistry 53: 726–730.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Librus, H., Pietrokovski, J., Ulmanski, M. & Geda-
lia, I. (1973) The effect of fluoride on molar
socket healing in the rat. Archives of Oral Biol-
ogy 18: 1283–1289.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Lindeboom, J.A., Tjiook, Y. & Kroon, F.H. (2006)
Immediate placement of implants in periapical
infected sites: a prospective randomized study in
50 patients. Oral Surgery Oral Medicine Oral
Pathology Oral Radiology & Endodontology 101:
705–710.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.Loo, W.D. (1968) Ridge preservation with immedi-
ate treatment dentures. Journal of Prosthetic
Dentistry 19: 5–11.
Exclusion criteria: descriptive report on
procedure/technique; commentary.Luvizuto, E.R., Queiroz, T.P., Dias, S.M., Okamoto,
T., Dornelles, R.C., Garcia, I.R. Jr & Okamoto, R.
(2010) Histomorphometric analysis and immunol-
ocalization of rankl and opg during the alveolar
healing process in female ovariectomized rats
treated with oestrogen or raloxifene. Archives of
Oral Biology 55: 52–59.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Magro Filho, O. & de Carvalho, A.C. (1990) Appli-
cation of propolis to dental sockets and skin
wounds. Journal of Nihon University School of
Dentistry 32: 4–13.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Magro-Ernica, N., Magro-Filho, O. & Rangel-Garcia,
I. (2003) Histologic study of use of microfibrillar
collagen hemostat in rat dental sockets. Brazilian
Dental Journal 14: 12–15.
Exclusion criteria: reported parameters not
relevant or not useful.Mathai, J.K., Chandra, S., Nair, K.V. & Nambiar, K.
K. (1989) Tricalcium phosphate ceramic as imme-
diate root implants for the maintenance of alveo-
lar bone in partially edentulous mandibular jaws.
A clinical study. Australian Dental Journal 34:
421–426.
Exclusion criteria: reported parameters not
relevant or not useful.Matsumoto, M. (1968) Changes in residual ridge of
the mandible after extraction and wearing exten-
sion saddle type of removable partial dentures. (a
longitudinal, clinical and roentgenographic inves-
tigation). Bulletin of Tokyo Medical & Dental
University 15: 67–89.
Exclusion criteria: length of observation
period not reported.Michael, C.G. & Barsoum, W.M. (1976) Comparing
ridge resorption with various surgical techniques
in immediate dentures. Journal of Prosthetic
Dentisty 35: 142–155.
© 2011 John Wiley & Sons A/S 19 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

Exclusion criteria: study subjects had
immediate dentures after extraction, hence
they did not have undisturbed healing post-
extraction.Minsk, L. (2005) Extraction-site ridge preservation.
Compendium of Continuing Education in Den-
tistry 26: 272.
Exclusion criteria: descriptive report on
procedure/technique; commentary.Mizutani, H. & Ishihata, N. (1976) Decrease and
increase in residual ridges after extraction of
teeth in monkeys (part I). Bulletin of Tokyo Med-
ical & Dental University 23: 157–168.
Exclusion criteria: study carried out on ani-
mals.Nevins, M., Camelo, M., De Paoli, S., Friedland, B.,
Schenk, R.K., Parma-Benfenati, S., Simion, M.,
Tinti, C. & Wagenberg, B. (2006) A study of the
fate of the buccal wall of extraction sockets of
teeth with prominent roots. International Journal
of Periodontics & Restorative Dentistry 26: 19–
29.
Exclusion criteria: reported parameters not
relevant or not useful.Nevins, M.L., Camelo, M., Schupbach, P., Kim, D.
M., Camelo, J.M. & Nevins, M. (2009) Human his-
tologic evaluation of mineralized collagen bone
substitute and recombinant platelet-derived
growth factor-bb to create bone for implant place-
ment in extraction socket defects at 4 and
6 months: a case series. International Journal of
Periodontics & Restorative Dentistry 29: 129–139.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.Normando, A.D., Maia, F.A., Ursi, W.J. & Simone,
J.L. (2010) Dentoalveolar changes after unilateral
extractions of mandibular first molars and their
influence on third molar development and posi-
tion. World Journal of Orthodontics 11: 55–60.
Exclusion criteria: reported parameters not
relevant or not useful.Olson, H.M. & Hagen, A. (1982) Inhibition of post-
extraction alveolar ridge resorption in rats by di-
chloromethane diphosphonate. Journal of Peri-
odontal Research 17: 669–674.
Exclusion criteria: study carried out on ani-
mals.Olson, R.A., Roberts, D.L. & Osbon, D.B. (1982) A
comparative study of polylactic acid, gelfoam,
and surgicel in healing extraction sites. Oral Sur-
gery Oral Medicine & Oral Pathology 53: 441–
449.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Oltramari, P.V., Navarro Rde, L., Henriques, J.F.,
Taga, R., Cestari, T.M., Janson, G. & Granjeiro, J.
M. (2007) Evaluation of bone height and bone
density after tooth extraction: an experimental
study in minipigs. Oral Surgery Oral Medicine
Oral Pathology Oral Radiology & Endodontology
104: 9–16.
Exclusion criteria: study carried out on ani-
mals.Ortega, K.L., Rezende, N.P., Araujo, N.S. & Ma-
galhaes, M.H. (2007) Effect of a topical antimicro-
bial paste on healing after extraction of molars in
hiv positive patients: randomised controlled clini-
cal trial. British Journal of Oral & Maxillofacial
Surgery 45: 27–29.
Exclusion criteria: reported parameters not
relevant or not useful.Pessoa, R.S., Oliveira, S.R., Menezes, H.H. & de
Magalhaes, D. (2009) Effects of platelet-rich
plasma on healing of alveolar socket: split-mouth
histological and histometric evaluation in cebus
apella monkeys. Indian Journal of Dental
Research 20: 442–447.
Exclusion criteria: no baseline data avail-
able for comparison, thus unable to arrive at
an estimate of dimensional change over time.Pietrokovski, J. (1967) Healing of the socket
following tooth extraction. Alpha Omegan 60:
126–129.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Pietrokovski, J. & Massler, M. (1967a) Alveolar
ridge resorption following tooth extraction. Jour-
nal of Prosthetic Dentistry 17: 21–27.
Exclusion criteria: length of observation
period not reported.Pietrokovski, J. & Massler, M. (1967b) Ridge remod-
eling after tooth extraction in rats. Journal of
Dental Research 46: 222–231.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Pietrokovski, J. & Massler, M. (1971) Residual ridge
remodeling after tooth extraction in monkeys.
Journal of Prosthetic Dentistry 26: 119–129.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Pinto, J.R., Bosco, A.F., Okamoto, T., Guerra, J.B. &
Piza, I.G. (2002) Effects of nicotine on the healing
of extraction sockets in rats. A histological study.
Brazilian Dental Journal 13: 3–9.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Puia, S.A., Renou, S.J., Rey, E.A., Guglielmotti, M.
B. & Bozzini, C.E. (2009) Effect of bismuth sub-
gallate (a hemostatic agent) on bone repair; a his-
tologic, radiographic and histomorphometric
study in rats. The International Journal of Oral
& Maxillofacial Surgery 38: 785–789.
Exclusion criteria: reported parameters not
relevant or not useful.Quinn, J.H. & Kent, J.N. (1984) Alveolar ridge
maintenance with solid nonporous hydroxylapa-
tite root implants. Oral Surgery Oral Medicine &
Oral Pathology 58: 511–521.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Richardson, A. (1965) The pattern of alveolar bone
resorption following extraction of anterior teeth.
Dental Practitioner & Dental Record 16: 77–80.
Exclusion criteria: reported parameters not
relevant or not useful.Rothamel, D., Schwarz, F., Herten, M., Engelhardt,
E., Donath, K., Kuehn, P. & Becker, J. (2008)
Dimensional ridge alterations following socket
preservation using a nanocrystalline hydroxyapa-
tite paste: a histomorphometrical study in dogs.
The International Journal of Oral & Maxillofa-
cial Surgery 37: 741–747.
Exclusion criteria: no baseline data avail-
able for comparison, thus unable to arrive at
an estimate of dimensional change over time.Sattayasanskul, W., Brook, I.M. & Lamb, D.J. (1988)
Dense hydroxyapatite root replica implantation:
measurement of mandibular ridge preservation.
The International Journal of Oral & Maxillofa-
cial Implants 3: 203–207.
Exclusion criteria: study subjects had
immediate dentures after extraction, hence
they did not have undisturbed healing post-
extraction.Scheer, P. & Boyne, P.J. (1987) Maintenance of alve-
olar bone through implantation of bone graft sub-
stitutes in tooth extraction sockets. Journal of
the American Dental Association 114: 594–597.
Exclusion criteria: descriptive report on
procedure/technique; commentary.Sclar, A.G. (1999) Preserving alveolar ridge anatomy
following tooth removal in conjunction with
immediate implant placement. The bio-col tech-
nique. Atlas of the Oral & Maxillofacial Surgery
Clinics of North America 7: 39–59.
Exclusion criteria: descriptive report on
procedure/technique; commentary.Serino, G., Rao, W., Iezzi, G. & Piattelli, A. (2008)
Polylactide and polyglycolide sponge used in
human extraction sockets: bone formation fol-
lowing 3 months after its application. Clinical
Oral Implants Research 19: 26–31.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Sharan, A. & Madjar, D. (2008) Maxillary sinus
pneumatization following extractions: a radio-
graphic study. The International Journal of Oral
& Maxillofacial Implants 23: 48–56.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Shi, B., Zhou, Y., Wang, Y.N. & Cheng, X.R. (2007)
Alveolar ridge preservation prior to implant place-
ment with surgical-grade calcium sulfate and
platelet-rich plasma: a pilot study in a canine
20 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21 © 2011 John Wiley & Sons A/S
Tan et al !Dimensional tissue changes post extraction

model. The International Journal of Oral & Max-
illofacial Implants 22: 656–665.
Exclusion criteria: study carried out on ani-
mals.Smith, N. (1974) A comparative histological and
radiographic study of extraction socket healing in
the rat. Australian Dental Journal 19: 250–254.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Teofilo, J.M., Brentegani, L.G. & Carvalho, T.L.
(2001) A histometric study in rats of the effect of
the calcium antagonist amlodipine on bone heal-
ing after tooth extraction. Archives of Oral Biol-
ogy 46: 375–379.
Exclusion criteria: reported parameters not
relevant or not useful.
Teofilo, J.M., Leonel, D.V. & Lamano, T. (2010)
Cola beverage consumption delays alveolar bone
healing: a histometric study in rats. Brazilian
Oral Research 24: 177–181.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Thilander, H. & Astrand, P. (1973) The effect of tet-
racyclines on socket healing. Acta Odontologica
Scandinavica 31: 131–139.
Exclusion criteria: no measurements of
alveolar dimensional changes (eg. description
of healing process or bony shape change, or
histology only).Ubios, A.M., Jares Furno, G. & Guglielmotti, M.B.
(1991) Effect of calcitonin on alveolar wound
healing. Journal of Oral Pathology & Medicine
20: 322–324.
Exclusion criteria: reported parameters not
relevant or not useful.Wu, Z., Liu, C., Zang, G. & Sun, H. (2008) The
effect of simvastatin on remodelling of the alveo-
lar bone following tooth extraction. The Interna-
tional Journal of Oral & Maxillofacial Surgery
37: 170–176.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.Yugoshi, L.I., Sala, M.A., Brentegani, L.G. & Lama-
no Carvalho, T.L. (2002) Histometric study of
socket healing after tooth extraction in rats trea-
ted with diclofenac. Brazilian Dental Journal 13:
92–96.
Exclusion criteria: sample did not include
untreated/undisturbed extraction sockets left
to heal spontaneously.
© 2011 John Wiley & Sons A/S 21 | Clin. Oral. Impl. Res. 23(Suppl. 5), 2012/1–21
Tan et al !Dimensional tissue changes post extraction

Copyright of Clinical Oral Implants Research is the property of Wiley-Blackwell and its content may not becopied or emailed to multiple sites or posted to a listserv without the copyright holder's express writtenpermission. However, users may print, download, or email articles for individual use.

Osteology Consensus Report
Christoph H.F. HammerleMauricio G. AraujoMassimo SimionMauricio G. Araujo
Evidence-based knowledge on thebiology and treatment of extractionsockets
Authors’ affiliations:Christoph H.F. Hammerle, Center of DentalMedicine, Clinic of Fixed and RemovableProsthodontics and Dental Material Science,University of Zurich, Zurich, SwitzerlandMauricio G. Araujo, Department of Dentistry, StateUniversity of Maringa, Parana, BrazilMassimo Simion, Departmet of Periodontology,IRCCS Ca Granda Foundation – Ospedale MaggiorePoliclinico, Department of Reconstructive, Surgicaland Diagnostic Science, University of Milan,Department of Periodonology, College of Dentistry,King Saud University, Riyadh, Saudi ArabiaMauricio G. Araujo, Department of Dentistry, StateUniversity of Maringa, Parana, Brazil
Corresponding author:Mauricio G. AraujoDepartment of DentistryState University of MaringaParana, BrazilTel.: +41 44 634 32 51Fax: +41 44 634 43 05e-mail: [email protected]
Conflicts of interestThe authors declare no conflicts of interest.
Key words: bone regeneration, clinical research, clinical trials, guided tissue regeneration,
wound healing
Abstract
Objectives: The fresh extraction socket in the alveolar ridge represents a special challenge in
everyday clinical practice. Maintenance of the hard and soft tissue envelope and a stable ridge
volume were considered important aims to allow simplifying subsequent treatments and
optimizing their outcomes in particular, when implants are planned to be placed.
Material and Methods: : Prior to the consensus meeting four comprehensive systematic reviews
were written on two topics regarding ridge alteration and ridge preservation following tooth
extraction and implant placement following tooth extraction. During the conference these
manuscripts were discussed and accepted thereafter. Finally, consensus statements and
recommendations were formulated.
Results: : The systematic reviews demonstrated that the alveolar ridge undergoes a mean
horizontal reduction in width of 3.8 mm and a mean vertical reduction in height of 1.24 mm
within 6 months after tooth extraction. The techniques aimed at ridge preservation encompassed
two different approaches: i) maintaining the ridge profile, ii) enlarging the ridge profile.
Regarding timing of implant placement the literature showed that immediate implant placement
leads to high implant survival rates. This procedure is primarily recommended in premolar sites
with low esthetic importance and favorable anatomy. In the esthetic zone, however, a high risk for
mucosal recession was reported. Hence, it should only be used in stringently selected situations
with lower risks and only by experienced clinicians. In molar sites a high need for soft and hard
tissue augmentation was identified.
Conclusions: : Future research should clearly identify the clinical and patient benefits resulting
from ridge preservation compared with traditional procedures. In addition, future research should
also aim at better identifying parameters critical for positive treatment outcomes with immediate
implants. The result of this procedure should be compared to early and late implant placement.
The fresh extraction socket in the alveolar
ridge represents a special challenge in every-
day clinical practice. Regardless of the subse-
quent treatment maintenance of the ridge
contour will frequently facilitate all further
steps of therapy. This is particularly true for
treatments involving the placement and
reconstruction of dental implants. It has been
demonstrated in numerous animal and clini-
cal studies in humans that following tooth
extraction undisturbed wound healing will
lead to loss of ridge volume and change in
ridge shape.
The aim of the present consensus report
was to critically evaluate the scientific evi-
dence regarding ridge alterations following
tooth extraction and to assess the effects of
treatment strategies aiming at preservation of
the ridge following tooth extraction. Further-
more, this consensus analyzed the clinical
outcomes of implant placement into sockets
at different time spans following tooth
extraction.
Workshop discussion andconsensus
The group discussing the evidence and gener-
ating the consensus statements consisted of
individuals competent in different disciplines
of medical dentistry with a special emphasis
on implant therapy. Prior to the consensus
meeting, two groups of researchers wrote
comprehensive systematic reviews on two
topics each regarding ridge alterations and
*Osteology Consensus Group 2011: Mauricio G. Araujo,Maringa, Parana, Brazil; Dieter Bosshardt, Daniel Buser,Berne, Switzerland; William V. Giannobile, Ann Arbor,Michighan, USA; Reinhard Gruber, Vienna, Austria; Chr-istoph H.F. Hammerle, Ronald E. Jung, Zurich, Switzer-land; Niklaus P. Lang, Hong Kong SAR PRC; MyronNevins, Boston, Massachusetts, USA; Friedrich Neukam,Nuremberg, Germany; Mariano Sanz, Madrid, Spain;Massimo Simion, Milano, Italy; Georg Watzek, Vienna,Austria
Date:Accepted 8 October 2011
To cite this article:CHF Hammerle, Araujo MG, Simion M, On Behalf of theOsteology Consensus Group 2011. Evidence-based knowledgeon the biology and treatment of extraction sockets.Clin. Oral Impl. Res. 23(Suppl. 5), 2012, 80–82doi: 10.1111/j.1600-0501.2011.02370.x
© 2011 John Wiley & Sons A/S 80
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza

ridge preservation following tooth extraction
and implant placement following tooth
extraction.
During the conference, the reviewers first
presented their manuscripts explaining how
the literature search was conducted, how the
data were extracted, analyzed, which results
were found and which conclusions could be
drawn. The entire group then discussed these
reports. Thereafter, all four manuscripts were
accepted. Another thorough discussion fol-
lowed on published data on lower levels of
evidence than the one included in the manu-
scripts and its impact on the conclusions to
be drawn. Finally, the group formulated con-
sensus statements and recommendations for
clinical practice and for future research.
Ridge preservation
Definition of terms
The group considered it important to define
terms regarding the various procedures,
which previously had been described in the
literature under the general term of “ridge
preservation.” It was obvious that a distinc-
tion needed to be made as described below.
Ridge preservation = preserving the ridge
volume within the envelope existing at the
time of extraction
Ridge augmentation = increasing the ridge
volume beyond the skeletal envelope existing
at the time of extraction
Consensus statements regarding ridgepreservation
The systematic review by Lang et al. (2012)
demonstrated that based on clinical studies
the alveolar ridge undergoes the following
dimensional changes within 6 months after
tooth extraction:
• Mean horizontal reduction in ridge width:
3.8 mm.
• Mean vertical reduction in ridge height:
1.24 mm.
Based on the systematic review by Vigno-
letti et al. (2012) the group concluded that
the reasons for ridge preservation included:
• Maintenance of the existing soft and hard
tissue envelope.
• Maintenance of a stable ridge volume for
optimizing functional and esthetic out-
comes.
• Simplification of treatment procedures
subsequent to the ridge preservation
(i) Generation of a good soft tissue volume
for the time of implant placement thus
simplifying implantation procedures at
earlier time points.
(ii) Generation of a good hard tissue volume
for the time of implant placement thus
simplifying implantation procedures at
later time points.
No high level evidence was found in the
literature regarding contraindications specific
for ridge preservation. Hence, the group made
the following consensus.
Contraindication for ridge preservation was
considered to encompass:
• General contraindication against oral sur-
gical interventions.
Furthermore:
• Infections at the site planned for ridge
preservation, which cannot be taken care
of during the ridge preservation surgery.
• Patients radiated in the area planned for
ridge preservation.
• Patients taking bisphosphonates.
Various techniques have been described in
the literature for so called ridge preserva-
tion. These techniques may be categorized
into two different groups: (i) techniques aim-
ing at maintaining the ridge profile (ridge
preservation), (ii) techniques aiming at
enlarging the ridge profile (ridge augmenta-
tion).
To enlarge the ridge profile flaps have
generally been raised and augmentation pro-
cedures using biomaterials for ridge contour-
ing with or without barrier membranes
have been performed. It appears that pri-
mary closure of the wound is beneficial
regarding the volume gained applying this
approach.
These indications were identified for ridge
preservation:
• Implant placement is planned at a time
point later than tooth extraction i.e.,
(i) When immediate or early implanta-
tion is not recommendable
(ii) When patients are not available for
the immediate or early implant
placement (pregnancy, holidays, …)
(iii) When primary stability of an
implant cannot be obtained
(iv) In adolescent people
• Contouring of the ridge for conventional
prosthetic treatment.
• Provided the cost/benefit ratio is positive.
• Reducing the need for elevation of the
sinus floor.
Regarding indication other than the ones
mentioned above, there is little or no evi-
dence.
Clinical recommendations regarding ridgepreservation
In general, the group made the following clin-
ical recommendations:
• Raising of a flap and placement of bioma-
terials (biomaterial for ridge contouring
and/or barrier membrane).
• Primary would closure.
• Materials with a low resorption and
replacement rate.
• Raising of flaps and placement of a
device/devices for contouring the ridge
profile.
Regarding the different materials applied in
clinical studies the systematic review did not
show significant differences between the var-
ious materials, (i.e., filler, membranes) except
for the collagen plug alone, which revealed
negative results.
Although primary wound closure was gen-
erally considered an important factor for suc-
cess, the literature did not allow a
meaningful comparison of different tech-
niques for primary wound closure (soft tissue
punch, connective tissue graft, barrier mem-
brane, soft tissue replacement matrix).
Future research regarding ridge preservation
Regarding future research the consensus sta-
ted the following:
• Focus on patient centered outcomes.
• Focus on clinical short-, medium-, and
long-term outcomes including biological,
technical, phonetic, and esthetic parame-
ters.
• Studies regarding possible benefits during
subsequent implant therapy encompass-
ing:
(i) Assessing the need for further hard and
soft tissue augmentation
(ii) Assessing the amount of further hard
and soft tissue augmentation.
(iii) Assessing esthetic outcomes.
• Conditions of the soft tissues, i.e., dis-
placement of the muco-gingival junction,
color of the ridge mucosa, amount of ker-
atinized mucosa.
• Techniques for soft tissue management, i.
e., raising of flaps yes/no.
• Method for soft tissue closure.
• Influence of the hard and soft tissue anat-
omy following tooth extraction: presence
or absence of bony socket walls, thick-
© 2011 John Wiley & Sons A/S 81 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/80–82
Hammerle et al !Evidence for treatment of extraction sockets
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza

ness of the bony socket walls, soft tissue
area, volume, color, scars.
• Effect of various biomaterials applied for
ridge contouring.
• Effect of various biomaterials applied as
barrier membranes.
• Methodological studies on the optimal
type of measurements to assess the out-
come of treatment regarding soft tissue
and hard tissues.
• Development of consistent reference
points for 3D imaging technologies, when
studying changes in ridge morphology
regarding soft and/or hard tissues.
• Studies on the normal anatomy regarding
bone and soft tissue thickness and types
in different regions of the jaws.
• Studies on the effects of different extrac-
tion techniques on subsequent healing.
• Identify the most appropriate control
group for pre-clinical and clinical studies.
Timing for implant placement
Two systematic reviews were available (Lau
et al. 2012; Sanz et al. 2012) regarding timing
of implant placement into extraction sockets.
Both reviews focused on the highest level of
scientific evidence and were conducted with
reasonable and clearly defined inclusion and
exclusion criteria.
Consensus statements regarding timing forimplant placement
Limited to esthetic sites the systematic
reviews lead to following conclusions:
• Immediate implant placement leads to
high implant survival rates.
• Immediate implant placement is associ-
ated with a high risk for mucosal recession.
A wide range regarding the amount of
recessions is reported in the literature.
• Several risk factors for the development
of mucosal recession have been identified:
(i) Smoking
(ii) Presence of a thin buccal bone plate
(i.e., <1 mm thick)
(iii) Presence of a thin soft tissue biotype
(iv) Facial implant position
• Augmentation of soft and hard tissues is
frequently necessary.
• The procedure of immediate implant place-
ment into extraction sockets should be
used very restrictively in the esthetic area.
Limited to posterior sites the systematic
review by Lau et al. 2012 lead to the follow-
ing conclusions:
• For single tooth implants high survival
and low complication rates have been
reported.
• Molar sites present situations with lim-
ited indications due to anatomical rea-
sons.
• When immediate implants are placed in
molar sites, soft and hard tissue augmen-
tation is frequently necessary.
• Premolars represent the sites with the
most favorable indication due to the nor-
mally favorable anatomical situation and
the generally low esthetic demands.
The treatments of fully edentulous jaws
and of multiple extraction sites have not
been duly addressed in the literature.
Clinical recommendations regarding timing forimplant placement
As based on the literature the group con-
cluded that in situations, where no risk fac-
tors are present (situations rarely occurring),
this procedure may be recommended for
experienced clinicians.
Immediate implant placement is primarily
recommended in premolar sites with low
esthetic importance and favorable anatomy.
In areas of esthetic priority implant installa-
tion into the fresh extraction socket (Type I
placement) is not recommended.
Several published prospective case series
not included in the present systematic review
using the early implant placement protocol
have reported intermediate to long-term
excellent esthetic results (Belser et al. 2009;
Buser et al. 2011). These results lend addi-
tional support to the recommendation of type
II instead of type I implant placement follow-
ing tooth extraction in esthetic sites.
Future research regarding timing for implantplacement
These recommendations are valid for both
anterior and posterior sites.
• Reporting of frequency analyses of com-
plication should become standard.
• Studies addressing immediate implanta-
tion in the absence of risk factors.
• Comparison of surgical approaches with
and without the elevation of flaps.
• Comparison of surgical approaches with
and without filler materials in the gap
between the buccal aspect of the implant
and the buccal bone wall.
• Assess the influence of the distance of
the implant to the buccal bone wall on
bone formation.
• Comparison of different filler materials in
different clinical situations.
• Comparison of type 1 (immediate) and
type 2 (early) implant placement in low
risk situations.
• Comparison of type 2 (early) and type 3
(delayed) implant placement.
• Identify the ideal clinical protocols and
the best biomaterials for type 1, type 2,
and type 3 implant placement.
• Changes in the contours of the ridge over
extended periods of time.
References
Belser, U.C., Grutter, L., Vailati, F., Bornstein, M.
M., Weber, H.-P. & Buser, D. (2009) Outcome
evaluation of early placed maxillary anterior sin-
gle-tooth implants using objective esthetic crite-
ria: a cross-sectional, retrospective study in 45
patients with a 2- to 4-year follow-up using pink
and white esthetic scores. Journal of Periodontol-
ogy 80: 140–151.
Buser, D., Wittneben, J., Bornstein, M.M., Grutter,
L., Chappuis, V. & Belser, U.C. (2011) Stability of
contour augmentation and esthetic outcomes of
implant-supported single crowns in the esthetic
zone: 3-year results of a prospective study with
early implant placement postextraction. Journal
of Periodontology 82: 342–349.
Lang, N.P., Pun, B.L., Lau, I.K.Y., Li, K.Y. & Wong,
M.C.M. (2012) A systematic review on survival
and success rates of implants placed immediately
into fresh extraction sockets after at least one
year. Clinical Oral Implants Research 23(Suppl.
5): 39–66.
Sanz, I., Garcia-Gargallo, M., Herrara, D., Martin,
C., Figuero, E. & Sanz, M. (2012) Surgical proto-
cols for early implant placement in post-extrac-
tion sockets. A systematic review. Clinical Oral
Implants Research 23(Suppl. 5): 67–79.
Tan, W.L., Wong, T.W.L., Wong, M.C.M. & Lang,
N.P. (2012) A systematic review of post-extract-
ional alveolar bone dimensional changes in
humans. Clinical Oral Implants Research 23
(Suppl. 5): 1–21.
Vignoletti, F., Matesanz, P., Rodrigo, D., Figuero,
E., Martin, C. & Sanz, M. (2012) Surgical proto-
cols for ridge preservation after tooth extraction.
A systematic review. Clinical Oral Implants
Research 23(Suppl. 5): 22–38.
82 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/80–82 © 2011 John Wiley & Sons A/S
Hammerle et al !Evidence for treatment of extraction sockets
Daniel Jiménez Cabeza

Copyright of Clinical Oral Implants Research is the property of Wiley-Blackwell and its content may not becopied or emailed to multiple sites or posted to a listserv without the copyright holder's express writtenpermission. However, users may print, download, or email articles for individual use.

The International Journal of Periodontics & Restorative Dentistry
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

Volume 33, Number 1, 2013
71
Tooth extraction may lead to dif-ferent patterns of bone resorption, apposition, and remodeling that make it dif!cult to predict the !-nal ridge contour and dimension. The clinician’s decision to augment extraction sockets is important be-cause ungrafted extraction sockets may undergo progressive bone resorption without intervention.1–3 Complete bone regeneration to the pre-extraction crestal bone level is not always possible, regard-less of grafting materials or the use of barrier membranes.2–4
Autogenous bone has been considered the gold standard for bone grafting, but the morbidity and complications associated with harvesting have provided a reason to consider alternatives. Alloplas-tic biomaterials such as hydroxy-apatite (HA) and !–tricalcium phosphate (!-TCP) are promising bone substitutes because of their unlimited supply, but a lack of evi-dence and inconsistent clinical re-ports have made clinicians weary of their use.5–8
A barrier membrane is com-monly used in conjunction with a bone graft to maintain space and foster selective osteogenic cells
1 Assistant Professor, Division of Periodontology, Department of Oral Medicine, Infection and Immunity, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
2 Assistant Professor, University of Genoa, Genoa, Italy.3 Institute for Advanced Dental Studies, Belo Horizonte, Brazil.4 Assistant Clinical Professor, Division of Periodontology, Department of Oral Medicine, Infection and Immunity, Harvard School of Dental Medicine, Boston, Massachusetts, USA.
5 Schupbach Ltd, Service and Research for Histology, Microscopy and Imaging, Horgen, Switzerland.6 Associate Clinical Professor, Division of Periodontology, Department of Oral Medicine, Infection and Immunity, Harvard School of Dental Medicine, Boston, Massachusetts, USA. Correspondence to: Dr David M. Kim, Harvard School of Dental Medicine, 188 Longwood Ave, Boston, MA 02115, USA; fax: 617-432-1897; email: [email protected]. ©2013 by Quintessence Publishing Co Inc.
David M. Kim, DDS, DMSc1/Nicola De Angelis, DDS2/Marcelo Camelo, DDS3 Marc L. Nevins, DMD, MMSc4/Peter Schupbach, PhD5/Myron Nevins, DDS6
The purpose of this study was to determine the clinical and histologic ef!cacy of the combination of alloplastic biphasic calcium phosphate composed of 30% hydroxyapatite and 70% !–tricalcium phosphate (Osteon II) and a cross-linked collagen membrane used to reconstruct an extraction socket with new bone formation. Twelve patients, from two private dental practices, requiring extraction of maxillary and mandibular nonmolar teeth (n = 30) received both Osteon II (0.5- to 1.0-mm particle size) and the collagen membrane. The primary healing intention group (group A, n = 12) received primary "ap closure over the membrane, while in the secondary healing intention group (group B, n = 18), the membrane was left exposed. Early wound healing seemed to be slower in group B when compared to group A, but the difference was not noticeable after 4 weeks. Clinical reentry revealed that the dimensions of the ridge appeared to be maintained in both groups, and internal socket bone !ll was evident. The grafted area appeared to be well vascularized, but clinically visible graft particles were noted in some cases. Light microscopic analysis revealed the formation of new bone directly apposing the surfaces of graft particles and bridging the space between them, indicating that the graft material behaved as an osteoconductive scaffold. The mean amount of vital bone in group A was 40.3% ± 7.8%, while the remaining graft was 6.0% ± 4.0%. The mean amount of vital bone in group B was 47.3% ± 11.3%, while the remaining graft was 18.0% ± 20.0%. The absence of primary "ap closure did not affect the percentage of vital bone formation or residual graft. (Int J Periodontics Restorative Dent 2013;33:71–78. doi: 10.11607/prd.1463)
Ridge Preservation With and Without Primary Wound Closure: A Case Series
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza

The International Journal of Periodontics & Restorative Dentistry
72
to populate the defect while ex-cluding epithelial cells and !bro-blasts.9 Resorbable membranes are accompanied by fewer adverse events than nonresorbable mem-branes when exposed because they degrade naturally.10,11 Ex-posed non–cross-linked collagen membranes may resorb too quickly to accommodate bone formation, while cross-linked collagen mem-branes may allow stabilization of the collagen !bers to maintain the membrane’s integrity.11,12
The purpose of this study was to determine the clinical and histo-logic ef!cacy of the combination of alloplastic biphasic calcium phos-phate composed of 30% HA and 70% !-TCP (Osteon II, Dentium) and a cross-linked collagen mem-brane (Collagen Membrane, Dentium) used to reconstruct an extraction socket with new bone formation. In addition, the safety and ef!cacy of soft and hard tis-sue regeneration in sites with in-
tentional exposure of the collagen membrane was investigated.
Method and materials
Twelve patients (2 men, 10 women; age range, 33 to 70 years), from two private dental practices, requiring extraction of maxillary and mandib-ular nonmolar teeth (n = 30) partici-pated in this outpatient study. They required removal of one or more teeth and expressed a desire for replacement with dental implants. Patients were systemically healthy with no surgical contraindications. Oral and written explanations of the study, including the risks, bene-!ts, and alternative therapies, were thoroughly discussed. All patients volunteered for the protocol and signed an informed consent form based on the Helsinki Declaration of 1975, as revised in 2000. Preop-erative assessments including intra-oral examination, and radiographic
evaluations (periapical radiographs and computed tomography [CT] scans) were performed.
The surgical procedure was performed under local anesthe-sia (2% xylocaine with 1:100,000 epinephrine). An intrasulcular inci-sion was extended along the study teeth followed by elevation of buc-cal and lingual full-thickness "aps (Fig 1). Atraumatic tooth extrac-tions were performed to minimize trauma to the socket walls, and careful investigation was done to identify possible bone dehiscences and fenestrations. Sockets with a thin or partially missing labial plate (< 50%) were selected to undergo the proposed ridge regeneration.
Thirty extraction sockets re-ceived both Osteon II (0.5- to 1.0-mm particle size) and Collagen membrane. The primary healing intention group (group A, n = 12) received primary "ap closure over the membrane, while in the sec-ondary healing intention group
Fig 1 The patient presented with a failed root canal treatment and recurrent caries beneath the crown margins on the maxillary left canine and second premolar. Implants were selected to replace the two teeth.
Fig 2 Atraumatic extraction was performed to preserve the buccal plate, and both sockets were grafted with Osteon II.
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

Volume 33, Number 1, 2013
73
(group B, n = 18), the membrane was left exposed. All extraction sites were incrementally graft-ed with Osteon II until the graft was level with the existing crestal bone, and a barrier membrane was trimmed and closely adapted to !t the contours of the grafted site (Figs 2 and 3). Simple inter-rupted sutures (Silk and Vicryl, Ethicon) were used to position the "ap over the augmented area (Fig 4). Both verbal and written postoperative instructions were given to patients, and appropri-ate antibiotics and analgesics were prescribed. Sutures were removed 7 to 10 days postsurgery, and pa-tients were seen at regular intervals during the 6 months of healing.
Postoperative periapical ra-diographs and a CT scan were obtained 6 months after the ridge regeneration procedure prior to the implant surgery. Soft and hard tissue biopsy specimens of the grafted areas were obtained using
either 3- or 4-mm trephine burs (Dentium) along the long axis of the treated sites prior to implant place-ment. Twenty-three cores were ob-tained (11 from group A, 12 from group B). The collected cores were kept in the trephine burs, placed in formalin, and shipped to a his-tologist. Tapered dental implants (SuperLine, Dentium) were placed into the biopsy sites, and primary stability was veri!ed in all cases.
Light microscopy
The bone cores were embedded following complete dehydration in ascending grades of ethanol in a light-curing one-component res-in (Technovit 7200 VLC, Heraeus Kulzer). Polymerized blocks were initially ground to bring the tissue
components closer to the cutting surface. A 100-µm-thick section was cut away from the block us-ing a bandsaw equipped with a
diamond-coated blade (Exakt). The !nal thickness of 40 μm was achieved by grinding and !nal pol-ishing steps with 1,200-, 2,400-, and 4,000-grit sandpaper. Sec-tions from each block were used for staining with Sanderson rapid bone stain (methylene blue and so-dium permanganate).
Backscatter scanning electron microscopy
Following the light microscopic evaluation, the ground sections were destained by polishing with 6-μm diamond paste. They were then washed and sputter-coated with a 6-nm-thick carbon layer and examined in the backscatter modus of a Supra 40VP scanning electron microscope (Zeiss). Back-scatter scanning electron micros-copy (BSEM) micrographs were produced from the same levels as those for light microcopy.
Fig 3 Collagen membrane placed to protect the underlying graft material.
Fig 4 Membrane intentionally exposed at both grafted sites.
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

The International Journal of Periodontics & Restorative Dentistry
74
Results
Clinical and radiographic evaluations
All 12 patients completed the study without signi!cant adverse events or complications (Fig 5). Early wound healing seemed to be slower at the intentionally exposed sites (group B) when compared to primary "ap closure sites (group A), but the dif-ference was not noticeable after 4 weeks. Continuous maturation of the tissue covering the membrane was noted after 4 weeks in group B. No spontaneous membrane expo-sure was noted in group A.
Radiographic analysis revealed that mesial and distal crestal bone levels were maintained in both groups. Sockets in both groups un-derwent similar radiographic matu-ration (Figs 6a and 6b).
The soft tissue that formed over the exposed membrane ap-peared to be !rm in texture at the 6-month biopsy sampling. The re-sistance of the regenerated bone to trephine and osteotomy drills indicated that the regenerated bone was dense and !rm. Clinical reentry was performed after rais-ing a full-thickness "ap to assess the quality of regenerated bone. The dimensions of the ridge ap-peared to be maintained in both groups, and internal socket bone !ll was evident (Fig 7). The grafted area appeared to be well vascu-larized, but clinically visible graft particles were noted in some cas-es. The buccolingual dimensions of the augmented alveolar ridge allowed placement of dental im-plants that were at least 4.5 mm in width.
Light microscopy and BSEM analyses
Histologic evaluation of the bone cores from the augmented area provided an opportunity to ex-amine the quality and quantity of newly formed bone and remnants of grafting material (Figs 8 to 12). The connective tissue was devoid of in"ammatory cell in!ltrate but was characterized by the presence of a dense network of collagen !-bers with no membrane remnants (Figs 8b and 11b). Evidence of mature bone formation and resid-ual bone grafting material was ob-served to varying degrees (Figs 8b and 11b). Newly formed bone seemed to be directly apposed to the surfaces of graft particles and bridged the space between them, indicating that the graft material behaved as an osteoconductive
Fig 5 Excellent soft tissue healing was observed at the 15-week postoperative visit.
Figs 6a and 6b Six-month postoperative CT scans revealed preserved ridge dimensions of the sockets as well as radiographic maturation of bone grafts for the (a) canine and (b) second premolar.
a
b
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

Volume 33, Number 1, 2013
75
Fig 7 Clinical reentry with a full-thickness !ap revealed that the dimensions of the ridge were maintained, and internal socket bone "ll was evident.
Figs 8a and 8b (a) BSEM and (b) light microscopic micrograph from the same section through a core showing new bone formation (NB), marrow space (M), and graft particles (G) (group A).
500 μm
500 μm
NB M NB Ga
b
500 μm
500 μm
NB G G M NB G CT
a
b
Fig 9 Light microscopic micrograph showing newly formed bone (NB) and marrow space (M) (group A).
Fig 10 Ongoing bone formation was characterized by the pres-ence of osteoblasts and osteoid (group A). NB = new bone.
NB
M
NBNB
OsteoblastsOsteoid
50 μm500 μm
Figs 11a and 11b (a) BSEM and (b) light microscopic micrograph from the same section through a core showing new bone formation (NB), marrow space (M), and graft particles (G) (group B). CT = connec-tive tissue.
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

The International Journal of Periodontics & Restorative Dentistry
76
scaffold (Fig 12). The presence of both osteoblasts and osteoclasts indicated active bone formation as well as bone remodeling.
BSEM evaluation of cores con!rmed the presence of newly formed bone surrounding the graft particles (Figs 8a and 11a). BSEM enabled the graft particles to be dis-tinguished from bone and nonmin-eralized tissue by their more dense and whiter appearance and shape.
Histomorphometric analysis
Histomorphometric analysis was performed on 10 selected speci-mens (5 from group A, 5 from group B). There were no signi!-cant differences between the two groups regarding the amount of vi-tal bone and residual graft (P > .05). The mean amount of vital bone in group A was 40.3% ± 7.8%, while the remaining graft was 6.0% ± 4.0%. The mean amount of vi-tal bone in group B was 47.3% ± 11.3%, while the remaining graft
was 18.0% ± 20.0%. Therefore, the absence of primary "ap closure did not affect the percentage of vital bone formation or residual graft.
Discussion
Ridge preservation immediately after tooth extraction has been ad-vocated to preserve the ridge and soft tissue dimension to allow ideal implant placement.3,13 Ideal bone substitutes should not only pre-serve the socket dimension but also encourage new bone ingrowth into the grafted area, thereby forming a living bridge between the existing bone, new bone, and remaining bone substitutes.14 With time, newly formed bone should penetrate and replace much of the graft through the bone remodeling process.14
This study investigated the role of an alloplastic biomaterial and collagen membrane in preserv-ing the ridge dimension after the extraction of teeth. The biocom-patibility and osteoconductivity of
the combination of HA and !-TCP have been previously reported.15–22 Osteon II is composed of 30% HA and 70% !-TCP (granules are 70% porous with interconnected pores of 250 μm). The reason to combine an insoluble HA with a resorbable !-TCP is that the slow-resorbing HA will maintain the volume while the faster-resorbing !-TCP will pro-mote bone regeneration.
This study provided a healing period of 6 months to induce incor-poration of the grafts with subse-quent maturation of newly formed bone tissue. A similar amount of bone regeneration as well as pres-ervation of alveolar ridge dimen-sions was observed in both primary and secondary healing intention groups. It was apparent that after a 6-month healing period, the graft-ed area was stable enough to en-sure successful implant placement.
Histologic analysis of obtained bone cores revealed intimate con-tact between mineralized bone tissue and graft particles, con!rm-ing the osteoconductive property
Fig 12 Graft particles (G) were seen partially embedded in newly formed bone (NB) (group B).
NB
NB
NBG
GG
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

Volume 33, Number 1, 2013
77
of the biomaterial. The percent-age of vital bone volume (40.3% for group A and 47.3% for group B) was equivalent to other studies of HA and !-TCP composite bone graft. For example, Froum et al16 reported a 28.35% mean vital bone volume when a mixture of 60% HA and 40% !-TCP was used as a sinus augmentation material. While the amount of vital bone formed after the augmentation may not corre-late to implant survival, it can be an accurate indicator to assess and compare the healing potential of the graft.16 Because of the higher !-TCP content in Osteon II (70%), a signi!cant amount of graft particles were resorbed histologically. Thus, it appeared as though new bone formation was occurring simultane-ously with material degradation.
A barrier membrane is used along with bone graft material to stabilize the blood clot, exclude epithelial and connective tissue, and enable osteogenic cells to pro-liferate and differentiate.9 Early or spontaneous membrane exposure may lead to bacterial colonization, infection, or membrane degrada-tion with a poor regenerative out-come because soft tissue growth progresses at the rate of 0.5 to 1.0 mm per day and can take 7 to 10 days to granulate.23–27 Cross-linked collagen membranes remain intact longer than non–cross-linked membranes, but the non– cross-linked or low–cross-linked collagen membranes may not pro-vide effective barrier function if ex-posed prematurely.27
Recent publications support the idea that the intentional ex-
posure of a resorbable membrane does not adversely affect the re-generative outcome.13,28 Primary "ap closure was not necessary to achieve bone augmentation when healing was marked by minimal in"ammation and rapid epithelial migration over the exposed mem-brane.28 The similarity between the treatments indicated that the ab-sence of primary closure did not affect the percentage of vital bone regeneration or the difference in graft stability or osseointegration.
Conclusions
The use of a composite alloplastic biomaterial in combination with a collagen membrane allowed postextraction ridge preservation as well as suf!cient bone qual-ity and quantity to place dental implants. Although intentional membrane exposure could have resulted in compromised barrier function to support regeneration, the sites that healed by second-ary intention revealed similar clini-cal, radiographic, and histologic !ndings as those that healed by primary intention. The use of this alloplastic biomaterial can be con-sidered as a viable alternative to the use of autogenous bone or other bone substitutes.
Acknowledgments
This study was funded by a grant from Dentium.
References
1. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. Int J Peri-odontics Restorative Dent 2003;23: 313–323.
2. Fiorellini JP, Howell TH, Cochran D, et al. Randomized study evaluating re-combinant human bone morphogenetic protein-2 for extraction socket augmen-tation. J Periodontol 2005;76:605–613.
3. Nevins M, Camelo M, De Paoli S, et al. A study of the fate of the buccal wall of ex-traction sockets of teeth with prominent roots. Int J Periodontics Restorative Dent 2006;26:19–29.
4. Araújo M, Linder E, Wennström J, Lindhe J. The in"uence of Bio-Oss Collagen on healing of an extraction socket: An exper-imental study in the dog. Int J Periodon-tics Restorative Dent 2008;28:123–135.
5. Mellonig JT, Valderrama P, Cochran DL. Clinical and histologic evaluation of cal-cium-phosphate bone cement in inter-proximal osseous defects in humans: A report in four patients. Int J Periodontics Restorative Dent 2010;30:121–127.
6. Lupovici J. Regenerative strategies for anterior esthetic rehabilitation: A clini-cal and histologic case report. Compend Contin Educ Dent 2010;31:614–618, 620, 622–623.
7. Kim DM, Nevins M, Camelo M, et al. Hu-man histologic evaluation of the use of the dental putty for bone formation in the maxillary sinus: Case series. J Oral Implantol 2012;38:391–398.
8. De Coster P, Browaeys H, De Bruyn H. Healing of extraction sockets !lled with BoneCeramic prior to implant placement: Preliminary histological !ndings. Clin Im-plant Dent Relat Res 2011;13:34–45.
9. Melcher AH. On the repair potential of periodontal tissues. J Periodontol 1976; 47:256–260.
10. Fontana F, Maschera E, Rocchietta I, Simion M. Clinical classi!cation of com-plications in guided bone regeneration procedures by means of a nonresorb-able membrane. Int J Periodontics Re-storative Dent 2011;31:265–273.
11. Moses O, Pitaru S, Artzi Z, Nemcovsky CE. Healing of dehiscence-type defects in implants placed together with different barrier membranes: A comparative clini-cal study. Clin Oral Implants Res 2005;16: 210–219.
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

The International Journal of Periodontics & Restorative Dentistry
78
12. Bornstein MM, Bosshardt D, Buser D. Effect of two different bioabsorbable collagen membranes on guided bone regeneration: A comparative histomor-phometric study in the dog mandible. J Periodontol 2007;78:1943–1953.
13. Cardaropoli D, Cardaropoli G. Preser-vation of the postextraction alveolar ridge: A clinical and histologic study. Int J Periodontics Restorative Dent 2008;28: 469–477.
14. Hing KA. Bioceramic bone graft substi-tutes: In!uence of porosity and chem-istry. Int J Appl Ceram Technol 2005;2: 184–199.
15. Cordaro L, Bosshardt DD, Palattella P, Rao W, Serino G, Chiapasco M. Maxillary sinus grafting with Bio-Oss or Straumann Bone Ceramic: Histomorphometric re-sults from a randomized controlled mul-ticenter clinical trial. Clin Oral Implants Res 2008;19:796–803.
16. Froum SJ, Wallace SS, Cho SC, Elian N, Tarnow DP. Histomorphometric com-parison of a biphasic bone ceramic to anorganic bovine bone for sinus aug-mentation: 6- to 8-month postsurgical assessment of vital bone formation. A pilot study. Int J Periodontics Restorative Dent 2008;28:273–281.
17. Kim YK, Yun PY, Lim SC, Kim SG, Lee HJ, Ong JL. Clinical evaluations of OS-TEON as a new alloplastic material in si-nus bone grafting and its effect on bone healing. J Biomed Mater Res B Appl Bio-mater 2008;86:270–277.
18. Kim YK, Yun PY, Kim SG, Lim SC. Analy-sis of the healing process in sinus bone grafting using various grafting materials. Oral Surg Oral Med Oral Pathol Oral Ra-diol Endod 2009;107:204–211.
19. Frenken JW, Bouwman WF, Braven-boer N, Zijderveld SA, Schulten EA, ten Bruggenkate CM. The use of Straumann Bone Ceramic in a maxillary sinus !oor elevation procedure: A clinical, radiologi-cal, histological and histomorphometric evaluation with a 6-month healing period. Clin Oral Implants Res 2010;21:201–208.
20. Mardas N, Chadha V, Donos N. Alveo-lar ridge preservation with guided bone regeneration and a synthetic bone sub-stitute or a bovine-derived xenograft: A randomized, controlled clinical trial. Clin Oral Implants Res 2010;21:688–698.
21. Mardas N, D’Aiuto F, Mezzomo L, Ar-zoumanidi M, Donos N. Radiographic alveolar bone changes following ridge preservation with two different bioma-terials. Clin Oral Implants Res 2011;22: 416–423.
22. Kim DM, Camelo M, Nevins M, Fateh A, Schupbach P, Nevins M. Alveolar ridge construction with a composite alloplastic biomaterial. Int J Periodontics Restor-ative Dent 2012;32:e204–e209.
23. Engler WO, Ramfjord SP, Hiniker JJ. Heal-ing following simple gingivectomy. A triti-ated thymidine radioautographic study. I. Epithelialization. J Periodontol 1966;37: 298–308.
24. Simion M, Baldoni M, Rossi P, Zaffe D. A comparative study of the effectiveness of e-PTFE membranes with and without ear-ly exposure during the healing period. Int J Periodontics Restorative Dent 1994;14: 166–180.
25. Simion M, Maglione M, Iamoni F, Scar-ano A, Piattelli A, Salvato A. Bacterial penetration through Resolut resorbable membrane in vitro. An histological and scanning electron microscopic study. Clin Oral Implants Res 1997;8:23–31.
26. Hämmerle CH, Jung RE. Bone augmen-tation by means of barrier membranes. Periodontol 2000 2003;33:36–53.
27. Oh TJ, Meraw SJ, Lee EJ, Giannobile WV, Wang HL. Comparative analysis of collagen membranes for the treatment of implant dehiscence defects. Clin Oral Implants Res 2003;14:80–90.
28. Kim DM, Nevins M, Camelo M, et al. The feasibility of demineralized bone matrix and cancellous bone chips in conjunc-tion with an extracellular matrix mem-brane for alveolar ridge preservation: A case series. Int J Periodontics Restor-ative Dent 2011;31:39–47.
�������%<�48,17(66(1&(�38%/,6+,1*�&2��,1&��35,17,1*�2)�7+,6�'2&80(17�,6�5(675,&7('�72�3(5621$/�86(�21/<��12�3$57�0$<�%(�5(352'8&('�25�75$160,77('�,1�$1<�)250�:,7+287�:5,77(1�3(50,66,21�)520�7+(�38%/,6+(5��

Copyright of International Journal of Periodontics & Restorative Dentistry is the property of QuintessencePublishing Company Inc. and its content may not be copied or emailed to multiple sites or posted to a listservwithout the copyright holder's express written permission. However, users may print, download, or emailarticles for individual use.

The International Journal of Periodontics & Restorative Dentistry
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Volume 32, Number 4, 2012
459
Socket Site Preservation Using Bovine Bone Mineral With and Without a Bioresorbable Collagen Membrane
Mally Perelman-Karmon, DMD, MS*/Avital Kozlovsky, DMD** Roman Lilov, DMD***/Zvi Artzi, DMD****
Tooth extraction leads to morpho-logic changes and resorption of the alveolar ridge as a result of a lack of biomechanical forces on the bone.1,2 In the immediate postextraction phase, the fresh extraction socket possesses a unique wound-healing cascade.3–5 Marked dimensional al-terations occur in the edentulous ridge after extraction.1,5,6
In the anterior maxilla, there is consistent bone resorption where the buccal plate is thin. Bone re-sorption leads to palatal/lingual and apical positioning of the alveo-lar crest, since resorption is more prominent in the buccal plate.1,5
Thus, preserving the alveolar ridge and achieving appropriate ridge dimensions are important7,8 when an implant-supported fixed partial denture is required.
The increasing demand for es-thetic implant dentistry challenges the clinician. The implant location should comply with the patient’s esthetic, functional, and phonetic needs. Guided tissue regeneration (GTR), a biologic principle based on a selective cell population, achieves sufficient volume of regenerated
The purpose of this study was to compare extraction sites augmented with bovine bone mineral (BBM) with and without resorbable membrane coverage. BBM particles were grafted in fresh human extraction sockets of 23 patients; in 12 of these patients, a guided tissue regeneration (GTR) membrane was applied. After 9 months of histomorphometric evaluation, cylindric hard tissue specimens were obtained. Percent bone area fractions (BAFs) of the crestal, middle, and apical sections from each specimen were calculated using the point-counting technique. Changes in values were compared. In sites augmented with BBM, the mean BAF ranged from 22.8% (coronal) to 36.3% (apical) compared to sites augmented with BBM and collagen membrane (35.2% [coronal] to 47% [apical]). Comparison between the different depths and the two groups showed a distinct increase in BAF from coronal to apical regions (P < .001). This pattern was observed in both groups (P < .001) and was significantly higher in the group augmented with BBM and collagen membrane (P < .05). In the immediate postextraction phase, BBM as a grafted biomaterial preserved the socket volume and enabled newly formed bone for future implant site preparation. The amount of the osseous fraction increased with GTR membrane. (Int J Periodontics Restorative Dent 2012;32:459–465.)
* Department of Oral Sciences, School of Dental Medicine, State University of New York, Buffalo, New York, USA; Formerly, Undergraduate Student, The Maurice and Gabriela Goldschleger Scool of Dental Medicine, Tel Aviv University, Tel Aviv, Israel.
** Associate Professor, Department of Periodontology, The Maurice and Gabriela Goldschleger School of Dental Medicine, Tel Aviv University, Tel Aviv, Israel.
*** Private Practice, Netanya, Israel.**** Associate Professor and Director of Graduate Periodontics, Department of
Periodontology, The Maurice and Gabriela Goldschleger School of Dental Medicine, Tel Aviv University, Tel Aviv, Israel. Correspondence to: Prof Zvi Artzi, School of Dental Medicine, Tel Aviv University, Ramat Aviv, Tel Aviv 61390, Israel; email: [email protected].
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
460
bone.9 Different types of GTR mem-branes are used with and without a biomaterial scaffold10,11 to maintain space over a bony defect (extrac-tion socket void) and to prevent undesired cells from migrating into the defect. The membrane protects the blood clot formed in the socket. By protecting and secluding the socket from the adjacent interfer-ing connective tissue cells, the membrane enables and promotes osteogenic cell migration into the defect.9
After extraction, the defined area serves as a wound-healing site. The healing cascade of the socket is dominated by coagulum, which is gradually occupied by granula-tion tissue followed by a provision-al matrix (connective tissue).4 One week postextraction, the socket is characterized by granulation tissue consisting of a vascular network, im-mature connective tissue, osteoid formation in the apical portion, and epithelial coverage over the wound. At 1 month postextrac-tion, the socket is characterized by dense connective tissue overlying the residual sockets and filled with granulation tissue. A trabecular pattern of bone starts to emerge. Epithelium used for wound cover-age is complete following the se-quence of bone formation.3,4
In a periodontal deteriorating situation, when destruction of par-tial or complete socket walls is evi-dent, ingrowth of connective tissue into the extraction site is unavoid-able, leading to a deficient ridge. The use of bone substitute, such as bovine bone mineral (BBM), pre-
serves the alveolar ridge by stabiliz-ing the blood clot, thus maintaining the volume at the site and simulta-neously serving as an osteoconduc-tive guide rail to facilitate continual bone formation.12–17 BBM applied in conjunction with a bioresorbable membrane after a healing period of 9 months has shown complete hori-zontal bone augmentation.11
While the significant contri-bution of applying a selective se-cluded barrier in GTR or guided bone regeneration (GBR) proce-dures is evident, the application of membrane coverage at a fresh extraction socket while at the same time obtaining complete soft tis-sue closure is a challenge. Further-more, since bone tissue has been formed with and without the use of a membrane in animal and human studies,7,8,12,13,16–18 the indication of a GBR surgical modality in a unique healing site (ie, fresh extraction socket) should be interpreted.
The objective of this study was to compare the amount of bone area fraction in fresh extraction sites using BBM as the grafting biomaterial, protected or unpro-tected with a resorbable collagen membrane, and by using a rotating pedicle flap or coronally advanced flap to achieve complete soft tissue closure.
Method and materials
This study included 23 fresh single- root extraction sockets in 23 healthy patients (16 women, 7 men) with no systemic diseases. Patients
ranged from 26 to 68 years of age and were nonsmokers. The proce-dure was explained, and patients signed consent forms. The study was in accordance with the Helsinki Declaration.
Before extraction, clinical (probing) and radiographic param-eters were collected (Figs 1a and 1b). Sites exhibiting severe to com-plete socket wall destruction were excluded.
Extracted teeth included max-illary incisors (n = 10) and maxil-lary (n = 8) and mandibular (n = 5) single-root premolars. At least 50% of sockets were partially resorbed/destructed at one to two walls, but not circumferentially so that the inclusion criteria of containing the grafted particles and supporting the applied over-latticed resorb-able membrane could be met. Immediately following extraction, BBM particles (250 to 1,000 µm; Bio-Oss, Geistlich) were placed to fill the site completely (Fig 1c). The decision to use sites with or with-out the application of a resorbable membrane was determined ran-domly by flipping a coin before ex-traction. A double layer of collagen membrane (Bio-Gide, Geistlich) was applied in 11 sites (Fig 1d). The membrane covered the entire site and was secured labially and lin-gually under soft tissue flaps.
In the maxilla, complete soft tissue closure was obtained using a rotating pedicle flap from the pala-tal side. Advanced coronal, buccal, and lingual flaps ensured soft tissue closure in mandibular premolars. The distal superficial end of the
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Volume 32, Number 4, 2012
461
pedicle flap was de-epithelialized and sutured (4-0 Vicryl, Ethicon) to the inner layer of the buccal flap to obtain complete soft tissue clo-sure over the membrane-protected grafted site (Fig 1e). The same soft tissue management was performed in the unprotected group (n = 13) but without applying the GTR membrane. The exposed palatal area was left for secondary healing.
Patients were prescribed anal-gesics (naproxen 275 mg; Narocin, Teva Pharmaceutical) and instruct-ed to rinse with 0.2% chlorhexidine gluconate (Tarodent, Taro Pharma-ceutical) twice a day for 30 seconds for 2 weeks. Complete soft tissue healing was observed at 1 month postgrafting (Fig 1f). Computed to-mography scans were taken to plan the future implant prosthetic recon-struction (Fig 1g).
Since BBM is a slow biodegrad-able material,17 an extended heal-ing phase was allowed for possible interpretation between membrane-protected and unprotected healing sites. At 9 months, at implant place-ment, a midcrestal incision was made to expose the grafted site (Fig 1h). At this stage, instead of the usual sequence of step-up drill-ing for implant site preparation, a 2.5-mm–internal diameter trephine bur was applied to harvest a cylin-dric hard tissue core approximately 8 mm in length. The apical end of each specimen was marked for ori-entation to identify the peripheral versus deep ends.
Specimens (n = 23) were fixed in 10% neutral buffered formalin for 1 week and then decalcified
with 5% formic acid for 2 weeks. The decalcified cylindric speci-mens were embedded in paraffin and transversely cut into serial sec-tions 5-µm wide using a microtome (Leica RM 2245, Leica Microsys-tems). Each core was cut uniform-ly from the peripheral to deeper regions. Slides were stained with hematoxylin-eosin. From each tis-sue cylinder, six representative cuts undamaged during microtome cut-ting were selected for morphomet-ric analysis: two from the coronal portion (1 to 2 mm), two from the middle core, and two from the apical end (1 to 2 mm). Data from each pair were averaged and used as such.
Histomorphometry
In each section, bone area fraction at membrane-protected (m-BAF) and biomaterial-only (BAF) grafted sites was measured using an adap-tation of the point-counting proce-dure.12,17,19–22 Briefly, each section was examined in a projection mi-croscope (Visopan, Reichart, Leica) at 20× magnification. A 64-square (1.5 × 1.5 cm) graticule was su-perimposed on the screen for the point-counting calculation. Bone tissue was recorded whenever the graticule center (marked with “+”) hit the bone tissue.12,21,22 The sum (Pi) of the points overlying the bone tissue was calculated. Percentage of bone tissue was evaluated as a portion of the entire section area (Pi / Σi), where Σi represents the to-tal number of points superimposed on each section.
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
462
All measurements were taken by the same investigator. To de-termine the reproducibility of the
measurements and the coefficient of variation (CV) for each parameter, 10 randomly selected slides were
Fig 1a (left) Clinical appearance of a maxillary right central incisor. The marginal gingiva was inflamed, and the tooth had migrated slightly labially and mesially be-cause of the periodontal condition.
Fig 1b (right) Periapical radiograph of the maxillary central incisor. Severe periodontal destruction is evident.
Fig 1c Fresh extraction socket filled with BBM particles.
Fig 1d Bioresorbable membrane applied to cover the augmented socket.
Fig 1e Complete soft tissue closure was obtained using a pedicle palatal rotated flap.
Fig 1f At 1 month, soft tissue healing was evident.
Fig 1g Buccolingual computed tomogra-phy section of the grafted extraction site.
Fig 1h At reentry, a wide buccolingual os-seous table had been established.
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Volume 32, Number 4, 2012
463
measured 5 times, not consecu-tively, without reference to the pre-vious data. The mean CV of bone (2.2%), biomaterial particle (2%), and remaining concavity area fractions (1.8%) indicated that these measure-ments were highly reproducible.
During measurements, the in-vestigator was masked to the type of site with respect to whether the mea-surement was conducted on protect-ed or unprotected membrane sites; the same applied for its depth.
Repeated-measures analysis of variance was used. The within-subject factor was depth, and the between-subject factor was mem-brane coverage. Values were con-sidered significant at P < .05.
Results
All patients were observed fre-quently, and postoperative heal-ing was immaculate. Histologic examination revealed that all cores harbored an abundance of BBM particles surrounded by newly formed bone. In the membrane-protected group, total bone frac-tion ranged from 23% to 72% (mean, 40.8% ± 10.61%) (Figs 2a and 2b). m-BAF ranged from 24.0% to 52.5% (mean, 35.2% ± 9.18%), 24.5% to 59.5% (mean, 40.2% ± 10.74%), and 23.0% to 72.0% (mean, 46.95% ± 12.83%) at the crestal, middle, and apical regions, respectively. In the unprotected
group, total BAF ranged from 15% to 54% (mean, 29.7% ± 7.21%). BAF ranged from 15.0% to 33.0% (mean, 22.8% ± 5.11%), 16.5% to 47.5% (mean, 29.9% ± 8.98%), and 21.5% to 54.0% (mean, 36.3% ± 11.3%) at the crestal, middle, and apical regions, respectively.
Mean m-BAF was significantly greater than BAF at all respective depths (P < .05). In both groups (m-BAF and BAF), a gradual in-crease in bone area fraction was observed from the coronal to apical areas. Within each type, the bone area fraction in the apical region was statistically greater than that in the middle and crestal areas (P < .001) (Fig 3).
Fig 2a (left) Typical coronal decalcified section cut. An abundance of soft tissue (ST) and grafted particles (P) surrounded by newly formed bone (B) can be seen (hematoxylin-eosin, original magnification ×25).
Fig 2b (right) Apical section with a high percentage of bone area fraction (B) (hematoxylin-eosin, original magnification ×25).
0
10
20
30
40
50
60
70
Crestal Middle
**
††
††
**
***
Apical
Membrane-protected
Unproteced
Mea
n B
AF
(%)
Fig 3 Mean BAF at the crestal, middle, and apical regions of the membrane-protected and unprotected extraction sites augmented by BBM particles. **P < .05; ***P < .001, †P < .001 (within-subject data).
ST
ST
P PP
B
B
B
B
BB
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

The International Journal of Periodontics & Restorative Dentistry
464
Discussion
BBM, which has been used for over 20 years, has proven to be a suitable biomaterial in augmentation proce-dures. Clinical and histologic stud-ies have shown the efficacy of this osteoconductive material.11,18,23,24 A high osteoconductive property by BBM has also been shown in a recent comparative study in human extraction sockets.15
BBM particles have been shown to be well integrated with regenerated bone in extraction and alveolar ridge deficiency sites in animal16,23,25 and human clinical studies,11,18,24,26 as well as in mor-phometric studies.12,22 In a human study,27 excellent osseointegration and crestal bone level maintenance were shown when implant place-ment was combined with bone augmentation using BBM as the grafting biomaterial.
In the current study, all 23 con-secutive patients showed primary soft tissue closure and excellent healing whether GTR membrane coverage was applied or not. However, the point-counting his-tomorphometry disclosed a distin-guishable observation. Regardless of the depth of the examined his-tologic section, a membrane- protected grafted socket site showed greater newly formed bone when compared with unpro-tected grafted sites. It should be considered that a membrane-pro-tected site is advantageous since the GTR membrane confines the grafted particles during the first period of healing and stabilizes the
entire site, in addition to its bio-logic contributions. In unprotected sites, some particulate biomate-rial would be lost or reside in the overlying soft tissue. Nevertheless, in both sites, BBM particles were surrounded by newly formed bone, and all sites exhibited clinical hard tissue formation, which was suit-able for implant site preparation.
The slow resorption rate of BBM does not inhibit continuous bone formation. On the contrary, it enhances it progressively.17
In unprotected grafted human sockets,12,26 BAF increases when approaching the apical area. In-trabony defects healed with BBM alone or with BBM and a resorb-able membrane. It has been shown that the amount of bone regenera-tion is further enhanced with the latter.28
Caution should be taken when internalizing the morphometric data if the examined sites are nei-ther identical nor standardized before grafting. However, the re-peated outcomes at the 12 versus 11 consecutively examined sockets should strengthen the findings.
In this study, the least BAF was found in the crestal zone, regardless of whether the site was membrane-protected. This could be explained by the distance between the socket walls.12 In the extraction site, the distance between the socket walls is reduced toward the apical region. Thus, this is an amply nourished site.
The fact that a membrane-pro-tected socket site showed greater newly formed bone was anticipat-
ed. In a computed tomography– derived bone density study in dogs,29 similar findings were shown with regard to the contribution of the GTR modality. Moreover, wound site stability and undesired micromovement,30 which can occur in this region, might influence the remodeling process.
Conclusions
BBM, as a grafted biomaterial in fresh extraction sockets, preserved its volume and enabled newly formed bone for future implant site preparation. The application of GBR increased the osseous fraction.
Acknowledgments
The authors thank Mrs Ilana Gelerntner for the statistical analysis and Ms Rita Lazar for editorial assistance.
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Volume 32, Number 4, 2012
465
References
1. Carlsson GE, Bergman B, Hedegård B. Changes in contour of the maxillary alve-olar process under immediate dentures. A longitudinal clinical and x-ray cepha-lometric study covering 5 years. Acta Odontol Scand 1967;25:45–75.
2. Pietrokovski J, Massler M. Alveolar ridge resorption following tooth extraction. J Prosthet Dent 1967;17:21–27.
3. Amler MH, Johnson PL, Salman I. Histo-logical and histochemical investigation of human alveolar socket healing in un-disturbed extraction wounds. J Am Dent Assoc 1960;61:32–44.
4. Cardaropoli G, Araújo M, Lindhe J. Dynamics of bone tissue formation in tooth extraction sites. An experimental study in dogs. J Clin Periodontol 2003;30: 809–818.
5. Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol 2005;32:212–218.
6. Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue con-tour changes following single tooth extrac-tion: A clinical and radiographic 12-month prospective study. Int J Periodontics Re-storative Dent 2003;23:313–323.
7. Nevins M, Camelo M, De Paoli S, et al. A study of the fate of the buccal wall of ex-traction sockets of teeth with prominent roots. Int J Periodontics Restorative Dent 2006;26:19–29.
8. Araújo MG, Lindhe J. Ridge preserva-tion with the use of Bio-Oss collagen: A 6-month study in the dog. Clin Oral Im-plants Res 2009;20:433–440.
9. Dahlin C, Linde A, Gottlow J, Nyman S. Healing of bone defects by guided tissue regeneration. Plast Reconstr Surg 1988; 81:672–676.
10. Diès F, Etienne D, Abboud NB, Ouhay-oun JP. Bone regeneration in extraction sites after immediate placement of an e-PTFE membrane with or without a bioma-terial. A report on 12 consecutive cases. Clin Oral Implants Res 1996;7:277–285.
11. Hämmerle CH, Jung RE, Yaman D, Lang NP. Ridge augmentation by applying bioresorbable membranes and deprot-einized bovine bone mineral: A report of twelve consecutive cases. Clin Oral Im-plants Res 2008;19:19–25.
12. Artzi Z, Tal H, Dayan D. Porous bovine bone mineral in healing of human extraction sockets. Part 1: Histomorphometric eval-uation at 9 months. J Periodontol 2000; 71:1015–1023.
13. Artzi Z, Nemcovsky CE, Tal H. Efficacy of porous bovine bone mineral in vari-ous types of osseous deficiencies: Clini-cal observations and literature review. Int J Periodontics Restorative Dent 2001;21:395–405.
14. Cardaropoli G, Araújo M, Hayaci- bara R, Sukekava F, Lindhe J. Healing of extraction sockets and surgically pro-duced—augmented and non-augment-ed—defects in the alveolar ridge. An experimental study in the dog. J Clin Periodontol 2005;32:435–440.
15. Lee DW, Pi SH, Lee SK, Kim EC. Com-parative histomorphometric analysis of extraction sockets healing implanted with bovine xenografts, irradiated cancellous allografts, and solvent-dehydrated al-lografts in humans. Int J Oral Maxillofac Implants 2009;24:609–615.
16. Artzi Z, Givol N, Rohrer MD, Nemcovsky CE, Prasad HS, Tal H. Qualitative and quantitative expression of bovine bone mineral in experimental bone defects. Part 1: Description of a dog model and histo-logical observations. J Periodontol 2003; 74:1143–1152.
17. Artzi Z, Givol N, Rohrer MD, Nemcovsky CE, Prasad HS, Tal H. Qualitative and quantitative expression of bovine bone mineral in experimental bone defects. Part 2: Morphometric analysis. J Peri-odontol 2003;74:1153–1160.
18. Artzi Z, Nemcovsky CE. The application of deproteinized bovine bone mineral for ridge preservation prior to implantation. Clinical and histological observations in a case report. J Periodontol 1998;69: 1062–1067.
19. Chalkey HW. Method for quantitative morphologic analysis of tissues. Natl Can-cer Inst 1943;4:47–53.
20. Bellhouse DR. Area estimation by point counting techniques. Biometrics 1981;37: 303–312.
21. Artzi Z, Nemcovsky CE, Dayan D. Nonce-ramic hydroxyapatite bone derivative in sinus augmentation procedures: Clinical and histomorphometric observations in 10 consecutive cases. Int J Periodontics Restorative Dent 2003;23:381–389.
22. Artzi Z, Kozlovsky A, Nemcovsky CE, Weinreb M. The amount of newly formed bone in sinus grafting procedures de-pends on tissue depth as well as the type and residual amount of the grafted mate-rial. J Clin Periodontol 2005;32:193–199.
23. Berglundh T, Lindhe J. Healing around implants placed in bone defects treated with Bio-Oss. An experimental study in the dog. Clin Oral Implants Res 2007;8: 117–124.
24. Skoglund A, Hising P, Young C. A clinical and histologic examination in humans of the osseous response to implanted natu-ral bone mineral. Int J Oral Maxillofac Im-plants 1997;12:194–199.
25. Hockers T, Abensur D, Valentini P, Legrand R, Hämmerle CH. The combined use of bioresorbable membranes and xenografts or autografts in the treatment of bone de-fects around implants. A study in beagle dogs. Clin Oral Implants Res 1999;10: 487–498.
26. Artzi Z, Tal H, Dayan D. Porous bovine bone mineral in healing of human extrac-tion sockets: 2. Histochemical observa-tions at 9 months. J Periodontol 2001; 72:152–159.
27. Meijndert L, Raghoebar GM, Schüpbach P, Meijer HJ, Vissink A. Bone quality at the implant site after reconstruction of a local defect of the maxillary anterior ridge with chin bone or deproteinised cancellous bo-vine bone. Int J Oral Maxillofac Surg 2005; 34:877–884.
28. Camelo M, Nevins ML, Schenk RK, et al. Clinical, radiographic, and histologic evaluation of human periodontal defects treated with Bio-Oss and Bio-Gide. Int J Periodontics Restorative Dent 1998;18: 321–331.
29. Kim M, Kim JH, Lee JY, et al. Effect of bone mineral with or without collagen mem-brane in ridge dehiscence defects follow-ing premolar extraction. In Vivo 2008;22: 231–236.
30. Haney JM, Nilvéus RE, McMillan PJ, Wikesjö UM. Periodontal repair in dogs: Expanded polytetrafluoroethylene barrier membranes support wound stabilization and enhance bone regeneration. J Peri-odontol 1993;64:883–890.
© 2012 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

Copyright of International Journal of Periodontics & Restorative Dentistry is the property of Quintessence
Publishing Company Inc. and its content may not be copied or emailed to multiple sites or posted to a listserv
without the copyright holder's express written permission. However, users may print, download, or email
articles for individual use.

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
1
Ridge Preservation Comparing a Socket Allograft Alone to a Socket Allograft Plus a Facial Overlay Xenograft: A Clinical and Histologic Study in Humans
Evmenios Poulias, DDS, MS*, Henry Greenwell, DMD, MSD†, Margaret Hill, DMD‡, Dean Morton, DMD, MS§, Ricardo Vidal, DDS, MS‖, Brian Shumway, DMD, MS¶,
Thomas L. Peterson, DDS, MS#
Private Practice, Athens, Greece.
Professor, Director of Graduate Periodontics, University of Louisville, Louisville, KY.
Associate Professor, Assoc Dean Postdoctoral Education, University of Louisville, Louisville, KY.
Professor, Chair, Dept of Oral Health & Rehabilitation, University of Louisville, Louisville, KY.
Assistant Professor, Periodontics, University of Louisville, Louisville, KY.
Assistant Professor, Oral Pathology, University of Louisville, Louisville, KY.
Private Practice, Macon, Georgia. Background. Previous studies of ridge preservation showed a loss of about 18% or 1.5 mm of
crestal ridge width in spite of treatment. The primary aim of this randomized, controlled, blinded clinical trial was to compare a socket graft to the same treatment plus a buccal overlay graft, both with a polylactide membrane, to determine if loss of ridge width can be prevented by use of an overlay graft.
Methods. Twelve positive control patients received an intrasocket mineralized cancellous allograft (Socket group) while twelve test patients received the same socket graft plus buccal overlay cancellous xenograft (Overlay group). Horizontal ridge dimensions were measured with a digital caliper and vertical ridge changes were measured from a stent. Prior to implant placement at 4 months a trephine core was obtained for histologic analysis.
Results. The mean horizontal ridge width at the crest for the Socket group decreased from 8.7 ± 1.0 mm to 7.1 ± 1.5 mm for a mean loss of 1.6 ± 0.8 mm (p < 0.05) while the Overlay group decreased from 8.4 ± 1.4 mm to 8.1 ± 1.4 mm for a mean loss of 0.3 ± 0.9 mm (p > 0.05). The Overlay group was significantly different from the Socket group (p < 0.05). Histologic analysis revealed that the Socket group had 35 ± 16% vital bone while the Overlay group had 40 ± 16% (p > 0.05).
Conclusions. The Overlay treatment significantly prevented loss of ridge width and preserved or augmented the buccal contour. The Socket and Overlay groups healed with a high percentage of vital bone.
KEY WORDS: allograft; xenograft; grafting, bone; socket graft; bone regeneration.
Following extraction there is substantial resorption of the alveolar ridge resulting in compromised ridge dimensions. Araujo et al. have shown that bone resorption is most pronounced on the buccal.1-5 This is due to loss of bundle bone that results in the loss of a portion of the buccal plate. When human extraction alone studies are reviewed as a
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
2
group they show that, on average, approximately 3.7 mm or 45% of horizontal ridge width is lost within a 4 to 6 month period.6-14 Ridge height, on the other hand, is less affected and on average only about 1.6 mm is lost.6-14
In an effort to reduce post-extraction bone loss clinicians have performed what is known as a ridge preservation procedure. This treatment utilizes an osseous graft and/or a barrier membrane to manage the extraction socket. The goal of this procedure is to ensure that adequate ridge width is preserved to allow implant placement totally within bone and to avoid complications such as implant dehiscence and fenestration. In spite of these efforts, most studies of ridge preservation show that there is still some loss of horizontal ridge width that can lead to a concave buccal contour and may lead to a dehiscence or fenestration at the time of implant placement. Ridge preservation studies as a group show that, on average, about 1.5 mm or 18% of horizontal ridge width is lost.6-
9,11-32 Ridge height is minimally affected and, on average, less than about 0.5 mm of height is lost.6-15,17,18,20,21,23,24,27,29-33
Wang et al. have described a "sandwich" technique of layered osseous grafting that utilizes an outer layer that resists resorption and will remain in place for an extended or indefinite period.34 The inner layer, on the other hand, is resorbed and replaced more quickly by newly formed vital bone. These principles will be utilized in this study.
Bovine xenograft has been reported to resorb very slowly and become fibrous encapsulated while cancellous allograft is resorbed and replaced more quickly through a process known as creeping substitution.18,34-40 These two materials fulfill the principles proposed by Wang et al.34 Therefore the cancellous allograft was chosen as a rapidly resorbing socket graft while the bovine xenograft was chosen as a buccal overlay to resist resorption and preserve the buccal contour. The specific aim of this study was to determine if ridge preservation treatment can be performed in a manner that will prevent the loss of crestal ridge width thereby preserving the original buccal contour. Comparing a socket graft alone to a socket graft plus a facial overlay will provide a valid test of the hypothesis that loss of crestal ridge width can be prevented when a slowly resorbing facial overlay graft is utilized.
METHODS
Study Design A total of 24 patients participated in this 4-month randomized, controlled, blinded clinical study of ridge preservation in sequentially entered single extraction sites of nonmolar teeth to be replaced by a dental implant. Twelve positive control patients were randomly selected, using a coin toss, to receive ridge preservation treatment with an intrasocket, mineralized, cancellous, particulate allograft (500-800 µm, Socket group).* The twelve test patients received the same intrasocket allograft plus a facial overlay with a mineralized, cancellous, particulate bovine xenograft (250-1000 µm, Overlay group).† A bioresorbable polylactide membrane was used to cover the osseous graft in both groups.‡ Four months after the grafting procedure the implant placement surgery was performed and a trephine core was removed from the osteotomy site for histologic analysis. All surgical procedures were completed by one operator (EP) under the direction of one mentor (HG). The surgeon was trained in the procedures until considered proficient. All

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
3
blinded measurements were performed by one blinded examiner (TP), who was unaware of the treatment assignment at all time points. The mentor performed the coin toss after flap reflection and immediately prior to graft placement and verified the measurements taken by the blinded examiner. All patients signed an informed consent approved by the University of Louisville Institutional Review Board in August 2011, when this study 11.0352 was also approved. This study was conducted in accordance with the Helsinki Declaration of 1975, as revised in 2000. The study was conducted between September 2011 and July 2012 in the Graduate Periodontics clinic at the University of Louisville.
Outcome Variables The primary outcome variable was crestal horizontal ridge width and the power analysis was based on this variable. Other variables evaluated included vertical ridge dimension change and histologic assessment of vital bone, non-vital bone and trabecular space.
Inclusion/Exclusion Criteria Subjects met the eligibility criteria if they were at least 18 years of age and had one nonmolar tooth requiring extraction that would be replaced by a dental implant. Extraction sites were bordered by at least one tooth. Exclusion criteria included: 1) debilitating systemic diseases, or diseases that have a clinically significant effect on the periodontium; 2) molar extraction sites; 3) presence of or history of osteonecrosis of the jaws; 4) history of IV bisphosphonate treatment; 5) history of oral bisphosphonate treatment for more than three years; 6) pregnancy or lactation; 7) known allergy to any material or medication used in the study; 8) required antibiotic prophylaxis; 9) previous head and neck radiation therapy; 10) history of chemotherapy in the last 12 months; 11) long term steroid or non-steroidal anti-inflammatory drug therapy; or 12) failure to sign an informed consent approved by the Human Studies Committee. Patients were excluded post-treatment if they developed infection or had an adverse reaction to any of the materials used in the study.
Clinical and Radiographic Parameters Each patient received a diagnostic work-up that included standardized periapical radiographs, study casts, clinical photographs, and a full periodontal examination. Radiographic and study cast data will not be presented or discussed. Customized occlusal stents were fabricated on the study casts to serve as fixed reference guides for the vertical measurements.9
Clinical parameters on adjacent teeth assessed at baseline and at the 4-month re-entry included Plaque Index, Gingival Index, bleeding on probing (dichotomous), keratinized tissue width, recession, probing depth, clinical attachment level, CEJ to alveolar crest distance, and tooth mobility.41,42 Horizontal ridge width was recorded with a modified digital caliper measuring to the nearest 10-2 at the mid-socket crestal level and 5 mm apically. Vertical distance from the acrylic stent to the alveolar crest was measured mesially, mid-socket and distally on all buccal, occlusal and lingual surfaces using a 15 mm North Carolina periodontal probe.9

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
4
Surgical Treatment Full thickness flaps were elevated to expose both the facial and the palatal/lingual aspects of the alveolar ridge. The flaps were extended one tooth mesial and distal to the preservation site on the buccal and vertical incisions were placed on the buccal and palatal. Papillae preservation incisions were used to keep the papilla intact.43 The teeth were extracted as atraumatically as possible using periotomes, elevators and forceps. After the extraction, the socket was carefully curetted to remove all soft tissue.
The allograft and xenograft materials were hydrated in a 50 mg/ml solution of tetracycline. The socket allograft was placed to the level of the alveolar crest and the facial overlay xenograft was placed over the buccal wall of the extraction socket from the alveolar crest to about 12 mm apical and was extended about half a tooth to the mesial and distal. The polylactide barrier membrane was trimmed to completely cover the socket and extended at least 3 mm past the alveolar crest and at least 3 mm past the lateral and apical borders of the facial xenograft. The membrane overlying the central portion of the socket was left exposed. Flaps were replaced or slightly coronally positioned. If needed, an apical periosteal split was performed to permit adequate flap release for tension-free closure. Flaps were sutured with a 4-0 polytetrafluoroethylene suture.§ Compression of the facial overlay graft was avoided by ensuring that flap closure was tension free. Patients were given a post-surgical regimen consisting of 375 mg naproxen (twice a day for one week), 50 mg doxycycline hyclate (once a day for two weeks) and narcotic analgesics as needed. Patients were seen every two weeks until soft tissue closure was complete and then monthly until the 4-month implant placement.
Implant Placement Full-thickness flaps were elevated on the buccal and palatal/lingual using a papilla preservation technique. All baseline clinical measurements were repeated and a standardized radiograph was taken. A 2.7 x 6.0 mm trephine was used with copious chilled saline irrigation to remove a core from the osteotomy site prior to implant placement.║ The core was subsequently placed in 10% buffered formalin for histologic processing. A dental implant was placed and flaps were replaced and sutured with 4-0 silk or the polytetrafluoroethylene sutures described previously.
Contour Data Pre- and post-treatment unlabelled occlusal clinical photographs were compared to determine the initial and final buccal contour. Each contour was subjectively categorized as a concave, flat or convex contour. Two blinded examiners (HG, EP) had to agree on each contour categorization. Since this was a subjective evaluation it was considered important to use two examiners. Subsequently the pre-and post-treatment categories were compared to determine if there was a loss, no change or a gain in terms of contour.
Tooth Type Data Data from previous studies of ridge preservation at this institution (this study, 2 publications, and 5 Master's theses) that were measured using the same technique as in this study were grouped according to tooth type to determine initial and final ridge

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
5
dimensions, the change and the percent change.9,18 Data for this analysis came from sites that received socket treatment alone without an overlay graft.
Histologic Analysis Trephine cores (2.7 X 6 mm) were decalcified and 12-15 step serial sections were taken from the center of each longitudinally sectioned core. The sections were stained with hematoxylin and eosin. Ten slides per patient were prepared, each containing at least 4 sections. Six randomly selected fields, 1 per section if possible, were used to obtain percent cellular bone, acellular bone, and trabecular space using an American Optics light microscope at 150x with a 10x objective and 15x reticle eyepieces.9
Statistical Methods Means and standard deviations were calculated for all parameters. A paired t-test was used to evaluate the statistical significance of the differences between initial and final data. An unpaired t-test was used to evaluate statistical differences between the test and control groups. The sample size of 11 per group gave 80% statistical power to detect a difference of 1 mm between groups for crestal ridge width. Power calculations were based on data from previous studies.9,18
RESULTS A total of 24 patients were entered in this study. For the Socket group 8 females and 4 males with a mean age of 52 ± 16, ranging from 26 to 77 years, were enrolled while 5 females and 7 males with a mean age of 58 ± 11, ranging from 38 to 71 years, were enrolled in the Overlay group. All sites were bordered by at least one tooth mesially or distally. The Socket group consisted of 1 maxillary incisor, 2 maxillary canines, 8 maxillary premolars, and 1 mandibular premolar. The Overlay group consisted of 5 maxillary incisors, 1 maxillary canine, and 6 maxillary premolars. There were 2 smokers enrolled in the Socket group and 2 in the Overlay group. The reason for extraction in the Socket group was 9 due to caries, 2 due to root fracture and 1 due to root resorption; in the Overlay group 6 were extracted due to caries, 5 due to root fracture and 1 due to root resorption. There were no adverse events that occurred due to this treatment.
All 24 patients completed the study, however, one patient in the Overlay group (1/12) was excluded following data analysis. This patient had a buccal wall missing at the time of extraction and the amount of ridge width gain was large. This represented an outlier value that skewed the data and did not represent what typically happens following a ridge preservation procedure.
Clinical Indices Plaque index, gingival index and bleeding on probing had low initial values for both groups, about 0.1 ± 0.1, and were virtually unchanged at the 4-month implant placement visit. There were no significant differences between initial and final values or between the test and the control groups (p > 0.05).

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
6
Horizontal Ridge Width Changes The Socket group had a statistically significant mean loss of crestal width of 1.6 ± 0.8 mm (p < 0.05) while the Overlay group had mean loss of only 0.3 ± 0.9 mm, which was not statistically significant (p > 0.05, Table 1). The difference between the 2 groups was statistically significant (p < 0.05). At 5 mm apical to the crest the Socket group had a significant mean loss of 0.8 ± 0.5 mm (p < 0.05) while the Overlay showed a statistically significant mean gain of 0.5 ± 0.6 mm (p < 0.05). The difference between the test and control groups was statistically significant (p < 0.05, Table 1).
Vertical Ridge Height Change On the mid-buccal the Socket group gained a mean of 0.5 ± 2.9 mm while the Overlay group gained 0.3 ± 2.6 mm, which was not statistically significant for either group (p > 0.05). The difference between the test and control groups was not statistically significant (p > 0.05, Table 2). Data and statistical significance for the mid-lingual, the mesial and the distal portion of the socket are shown in Table 2.
CEJ to Osseous Crest Changes Mesial CEJ to osseous crest distance for the Socket group showed a significant mean loss of 0.3 ± 0.3 mm (p < 0.05), while the Overlay group also had a significant mean loss of 0.5 ± 0.4 mm (p < 0.05). Distal CEJ to osseous crest distance for the Socket group showed a significant mean loss of 0.5 ± 0.7 mm (p < 0.05), while the Overlay group had a mean loss of 0.3 ± 0.5 mm, which was not statistically significant (p > 0.05). There were no statistically significant differences between groups for either mesial or distal sites.
Buccal Contour For the Socket group 5 sites ended with a concave contour while 7 were flat. For the Overlay group 4 sites ended with a flat contour while 7 were convex. In the Socket group this represented a loss of contour for 9 sites and no change for 3. For the Overlay group 4 sites had no change in contour while 7 showed a gain.
Histologic evaluation The Socket group healed with a mean of 35 ± 16% vital bone, 21 ± 13% non-vital bone and 44 ± 9% trabecular space, while the Overlay group healed with a mean of 40 ± 16% vital bone, 17 ± 11% non-vital bone, and 43 ± 12% trabecular space. There were no statistically significant differences between the Socket and Overlay groups for vital or non-vital bone or trabecular space (p > 0.05, Table 3).
DISCUSSION The primary aim of this 4-month randomized, controlled, blinded clinical study was to test the hypothesis that crestal ridge width could be preserved when a facial overlay xenograft that resists resorption was used. It was demonstrated that crestal ridge width can be almost entirely preserved when a slowly resorbing buccal overlay xenograft is used therfore the hypothesis should be accepted. This is in contrast to previous ridge

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
7
preservation studies where about 18% of crestal ridge width was lost.6-9,11-32 Furthermore at 5 mm apical to the crest there was a gain of 0.5 mm of ridge width. This supports the concept proposed by Wang et al. that a slowly resorbing outer layer of grafting material may resist resorption and have a beneficial effect on the final result.34 They also proposed that a rapidly resorbing inner graft layer is beneficial since it will be replaced by newly formed vital bone. In this study the socket graft was mineralized particulate cancellous allograft that healed with a high percentage of vital bone present. This means that at the site of implant placement, the previous socket area, there was a high percentage of vital bone present to promote osseointegration.
One question that needs to be considered is when an overlay graft is indicated. It adds time and expense to the ridge preservation procedure so there should be a compelling reason to complicate the grafting procedure by using an additional graft material. Data from ridge preservation sites from this study and other studies at the University of Louisville (2 publications and 5 Master's theses) indicate that maxillary sites tend to have more resorption than mandibular sites and that maxillary anterior sites tend to have the highest percentage of lost ridge width when compared to other sites (Table 4).9,18 Another consideration in maxillary anterior sites is that there is often a significant undercut or ridge concavity that extends corono-apically. This phenomenon can lead to a fenestration at the time of implant placement while narrow crestal ridge width may lead to dehiscence.
According to Woelfel's Dental Anatomy textbook maxillary incisors are about 6.0 mm in buccal-palatal width at the cervix, canines are about 7.5, premolars are about 8.1 and molars are about 10.7 mm.44 Mandibular dimensions are about 5.5 mm for incisors, 7.5 for canines, 7.1 for premolars and 8.9 mm for molars. This means that the smaller the initial ridge (socket) dimension the more likely that the site will need an overlay graft. Thus incisor, canine and premolar sites are the most likely candidates for an overlay graft, especially if a significant undercut is present. Mandibular incisor sites are the narrowest, however, the greatest percent resorption occurs in the maxilla (Table 4). Thus initial site width, likely percent resorption, and depth of the undercut are all factors that may influence the decision to use an overlay graft. Site analysis following tooth extraction utilizing these factors will lead to the best treatment decision.
Another advantage of the bovine xenograft is preservation of the original buccal contour in a mesio-distal direction. Without an overlay graft this contour is likely to become concave (Figure 1a) while use of the overlay most often results in a convex (Figure 1b) or at least a flat contour. In this study all pre- and post-op contour clinical photos were evaluated and scored for initial and final contour. This demonstrated that the overlay graft preserved or gained ridge contour, which is an esthetic advantage, while the Socket group lost contour at most sites.
If the goal of implant surgery is to place the implant totally within vital bone with no dehiscence or fenestration defects then the selection of a ridge preservation procedure can be an important decision. Development of an adequate ridge is also important if implant placement will be done using a flapless procedure, which may have esthetic advantages for the soft tissue and papillae. Another advantage of adequate ridge width is that following implant placement having 2 mm of bone buccal to the implant will help prevent soft tissue recession.45,46 Inadequate crestal ridge width, on the other hand, could

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
8
lead to implant dehiscence and potentially peri-implantitis. While additional grafting can be performed at the time of implant placement, the goal of the initial grafting procedure should be to establish adequate ridge dimensions so that no further grafting will be necessary at the time of implant placement. Therefore the overlay graft may be useful in successful development of adequate ridge width.
The most difficult aspect of the ridge preservation procedure is maintaining or gaining crestal ridge width. This means graft compression at the crest must be avoided and graft displacement either apically or laterally must be prevented. This was accomplished in this study by extending the flap one tooth mesial and distal to the extraction site. For the papilla preservation flap, the papillary incision was similar to that recommended by Bernimoulin et al. for a coronally positioned flap.43 Thus a new papilla tip was created about 3 mm apical to the existing papilla tip. The existing papilla was then de-epithelialized and the new papilla tip was positioned coronally to the tip of the existing papilla. An apical periosteal release gave adequate flap mobility to allow coronal positioning and to accommodate a thick layer of xenograft.
About 3 to 4 mm of xenograft thickness was placed as a buccal overlay, and perhaps more thickness was achieved apically. Also the graft was extended mesially and distally to the mid-root prominence of the adjacent teeth. This helped prevent apical and lateral displacement of the graft. Crestally the flap was closed with minimal tension to avoid graft compression. Another factor may have been the slight rigidity of the polylactide membrane, which also helped resist crestal compression.
Two previous studies tested the effect of an overlay graft.16,17 One showed a gain and one showed a slight loss of ridge width. Simon et al. showed a gain and the overlay graft was applied to the buccal, the crest and to the palatal/lingual.16 The gain was about 1.1 mm of ridge width, however, the measurement was at 3 mm apical to the crest rather than at the crest as was done in this study. Also different graft and membrane materials were used. Thus, although the data are not directly comparable, the present study confirms that the overlay graft approach can have a beneficial effect. Zubillaga et al. was performed in a similar fashion to Simon et al. but they used different graft materials, which resulted in a slight loss of about 0.5 mm of ridge width at 3 mm apical to the crest.17
Histologic analysis showed a high percentage of vital bone in the mid-socket area where the trephine core was harvested, which is where the cancellous allograft was placed (Table 3). This indicated that the goal of the Wang et al. layered graft had been achieved and that the implant would be placed in an area with a high percentage of vital bone.34 None of the histologic sections showed any signs of the xenograft. This indicates that it served to maintain and gain space and did not collapse into the socket area as the bundle bone and the allograft resorbed. The cancellous allograft used followed the healing pattern described by Burchardt et al. for cancellous autograft.37 Figure 2a-c demonstrates the vital bone, osteoblasts and appositional bone growth they reported as prominent features of cancellous graft healing.
A resorbable polylactide barrier membrane was used to contain the graft particles and to fulfill the objectives of guided bone regeneration. Thus the membrane was used to promote more rapid bone formation by preventing the ingrowth of connective tissue or

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
9
epithelium due to its barrier function. Since the primary objective of this study was to compare two grafting techniques the same membrane was used at all sites. The membrane was easy to use and all sites healed without any membrane associated complications. The portion of the membrane overlying the socket opening was left exposed and this resorbed by 6 to 8 weeks. Soft tissue had formed in this area by the time of membrane resorption and thus the graft was completely covered by either membrane or soft tissue at all times.
While there are many different ridge preservation procedures to choose from, the buccal overlay approach using a xenograft appears to be a viable option. When site analysis is used it can be determined whether the overlay or the intrasocket approach is the most appropriate treatment. The choice of graft materials to accomplish different purposes within the same graft as proposed by Wang et al. appears to be a valid and useful concept in implant site development surgery.34 Preservation of the original buccal contour is an esthetic advantage of this periodontal plastic surgery procedure.
Conflict of Interest Statement: This study was performed in Graduate Periodontics, University of Louisville without any grant funding. No commercial interests were involved and the authors report no conflict of interest. Dr. Greenwell has previously performed research for Sunstar Americas. Their membranes were used in this study but they supplied no funding or materials for this study.
Sources of support: This study received no support from outside sources. Drs. Poulias, Greenwell, Hill, Morton, Vidal, Shumway and Peterson report no financial relationships related to any products involved in this study. Dr. Greenwell performs research for Sunstar Americas, Chicago, IL.
REFERENCES 1. Araujo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study
in the dog. J Clin Periodontol 2005;32:212-218.
2. Araujo MG, Sukekava F, Wennstrom JL, Lindhe J. Ridge alterations following implant placement in fresh extraction sockets: an experimental study in the dog. J Clin Periodontol 2005;32:645-652.
3. Araújo M, Linder E, Wennström J, Lindhe J. The influence of Bio-Oss Collagen on healing of an extraction socket: an experimental study in the dog. Int J Periodontics Restorative Dent 2008;28:123-135.
4. Araújo MG, Lindhe J. Ridge alterations following tooth extraction with and without flap elevation: an experimental study in the dog. Clin Oral Implants Res 2009;20:545-549.
5. Araujo MG, Lindhe J. Socket grafting with the use of autologous bone: an experimental study in the dog. Clin Oral Implants Res 2011;22:9-13.
6. Lekovic V, Kenney EB, Weinlaender M, et al. A bone regenerative approach to alveolar ridge maintenance following tooth extraction. Report of 10 cases. J Periodontol 1997;68:563-570.
7. Lekovic V, Camargo PM, Klokkevold PR, et al. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. J Periodontol 1998;69:1044-1049.
8. Camargo PM, Lekovic V, Weinlaender M, et al. Influence of bioactive glass on changes in alveolar process dimensions after exodontia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;90:581-586.

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
10
9. Iasella JM, Greenwell H, Miller RL, et al. Ridge preservation with freeze-dried bone allograft and a collagen membrane compared to extraction alone for implant site development: A clinical and histologic study in humans. J Periodontol 2003;74:990-999.
10. Serino G, Biancu S, Iezzi G, Piattelli A. Ridge preservation following tooth extraction using a polylactide and polyglycolide sponge as space filler: A clinical and histological study in humans. Clin Oral Implants Res 2003;14:651-658.
11. Barone A, Aldini NN, Fini M, Giardino R, Calvo-Guirado JL, Covani U. Xenograft versus extraction alone for ridge preservation after tooth removal: A clinical and histomorphometric study. J Periodontol 2008;79:1370-1377.
12. Pelegrine AA, da Costa CE, Correa ME, Marques JF Jr. Clinical and histomorphometric evaluation of extraction sockets treated with an autologous bone marrow graft. Clin Oral Implants Res 2010;21:535-542.
13. Ahead of print. Festa VM, Addabbo F, Laino L, Femiano F, Rullo R. Porcine-derived xenograft combined with a soft cortical membrane versus extraction alone for implant site development: A clinical study in humans. [published online ahead of print November 14, 2011]. Clin Implant Dent Relat Res; doi 10.1111/j.1708-8208.2011.00398.
14. Brownfield LA, Weltman RL. Ridge preservation with or without an osteoinductive allograft: A clinical, radiographic, micro-computed tomography, and histologic study evaluating dimensional changes and new bone formation of the alveolar ridge. J Periodontol 2012;83:581-589.
15. Nemcovsky CE, Serfaty V. Alveolar ridge preservation following extraction of maxillary anterior teeth. Report on 23 consecutive cases. J Periodontol 1996;67:390-395.
16. Simon BI, Von Hagen S, Deasy MJ, Faldu M, Resnansky D. Changes in alveolar bone height and width following ridge augmentation using bone graft and membranes. J Periodontol 2000;71:1774-1791.
17. Zubillaga G, Von Hagen S, Simon BI, Deasy MJ. Changes in alveolar bone height and width following post-extraction ridge augmentation using a fixed bioabsorbable membrane and demineralized freeze-dried bone osteoinductive graft. J Periodontol 2003;74:965-975.
18. Vance GS, Greenwell H, Miller RL, Hill M, Johnston H, Scheetz JP. Comparison of an allograft in an experimental putty carrier and a bovine-derived xenograft used in ridge preservation: A clinical and histologic study in humans. Int J Oral Maxillofac Implants 2004;19:491-497.
19. Cardaropoli D, Cardaropoli G. Preservation of the post-extraction alveolar ridge: A clinical and histologic study. J Periodont Res 2008;28:469-477.
20. Neiva RF, Tsao YP, Eber R, Shotwell J, Billy E, Wang HL. Effects of a putty-form hydroxyapatite matrix combined with the synthetic cell-binding peptide P-15 on alveolar ridge preservation. J Periodontol 2008;79:291-299.
21. Beck TM, Mealey BL. Histologic analysis of healing after tooth extraction with ridge preservation using mineralized human bone allograft. J Periodontol 2010;81:1765-1772.
22. Mardas N, Chadha V, Donos N. Alveolar ridge preservation with guided bone regeneration and a synthetic bone substitute or a bovine-derived xenograft: A randomized, controlled clinical trial. Clin Oral Implants Res 2010;21:688-698.
23. Toloue SM, Chesnoiu-Matei I, Blanchard SB. A clinical and histomorphometric study of calcium sulfate compared with freeze-dried bone allograft for alveolar ridge preservation. J Periodontol 2012;83:847-855.
24. Fernandes PG, Novaes AB Jr, de Queiroz AC, et al. Ridge preservation with acellular dermal matrix and anorganic bone matrix cell-binding peptide P-15 after tooth extraction in humans. J Periodontol 2011;82:72-79.
25. Engler-Hamm D, Cheung WS, Yen A, Stark PC, Griffin T. Ridge preservation using a composite bone graft and a bioabsorbable membrane with and without primary wound closure: A comparative clinical trial. J Periodontol 2011;82:377-387.

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
11
26. Gholami GA, Najafi B, Mashhadiabbas F, Goetz W, Najafi S. Clinical, histologic and histomorphometric evaluation of socket preservation using a synthetic nanocrystalline hydroxyapatite in comparison with a bovine xenograft: A randomized clinical trial. Clin Oral Implants Res 2012;23:1198-1204.
27. Nam HW, Park JB, Lee JY, et al. Enhanced ridge preservation by bone mineral bound with collagen-binding synthetic oligopeptide: A clinical and histologic study in humans. J Periodontol 2011;82:471-480.
28. Stimmelmayr M, Guth JF, Iglhaut G, Beuer F. Preservation of the ridge and sealing of the socket with a combination epithelialised and subepithelial connective tissue graft for management of defects in the buccal bone before insertion of implants: A case series. Br J Oral Maxillofac Surg 2012;50:550-555.
29. Brkovic BM, Prasad HS, Konandreas G, et al. Simple preservation of a maxillary extraction socket using beta-tricalcium phosphate with type I collagen: Preliminary clinical and histomorphometric observations. J Can Dent Assoc 2008;74:523-528.
30. Kutkut A, Andreana S, Kim HL, Monaco E Jr. Extraction socket preservation graft before implant placement with calcium sulfate hemihydrate and platelet-rich plasma: A clinical and histomorphometric study in humans. J Periodontol 2012;83:401-409.
31. Wood RA, Mealey BL. Histologic comparison of healing after tooth extraction with ridge preservation using mineralized versus demineralized freeze-dried bone allograft. J Periodontol 2012;83:329-336.
32. Hoang TN, Mealey BL. Histologic comparison of healing after ridge preservation using human demineralized bone matrix putty with one versus two different-sized bone particles. J Periodontol 2012;83:174-181.
33. Fotek PD, Neiva RF, Wang HL. Comparison of dermal matrix and polytetrafluoroethylene membrane for socket bone augmentation: A clinical and histologic study. J Periodontol 2009;80:776-785.
34. Wang HL, Misch C, Neiva RF. "Sandwich" bone augmentation technique: Rationale and report of pilot cases. Int J Periodontics Restorative Dent 2004;24:232-245.
35. Wallace SS, Froum SJ, Cho S-C, et al. Sinus augmentation utilizing anorganic bovine bone (Bio-Oss) with absorbable and nonabsorbable membranes placed over the lateral window: Histomorphometric and clinical analyses. Int J Periodontics Restorative Dent 2005;25:551-559.
36. Scarano A, Pecora G, Piattelli M, Piattelli A. Osseointegration in a sinus augmented with bovine porous bone mineral: Histological results in an implant retrieved 4 years after insertion. A case report. J Periodontol 2004;75:1161-1166.
37. Burchardt H. The biology of bone graft repair. Clin Orthop Relat Res 1983;174:28-42.
38. Goldberg VM, Stevenson S. The biology of bone grafts. Semin Arthroplasty 1993;4:58-63.
39. Sbordone C, Toti P, Guidetti F, Califano L, Santoro A, Sbordone L. Volume changes of iliac crest autogenous bone grafts after vertical and horizontal alveolar ridge augmentation of atrophic maxillas and mandibles: A 6-year computerized tomographic follow-up. J Oral Maxillofac Surg 2012;70:2559-2565.
40. Sbordone L, Levin L, Guidetti F, Sbordone C, Glickman A, Schwartz-Arad D. Apical and marginal bone alterations around implants in maxillary sinus augmentation grafted with autogenous bone or bovine bone material and simultaneous or delayed dental implant positioning. Clin Oral Implants Res 2011;22:485-491.
41. Silness J, Löe H. Periodontal disease in pregnancy. II. Correlation between oral hygiene and periodontal condition. Acta Odontol Scand 1964;22:121-135.
42. Löe H. The gingival index, the plaque index and the retention index systems. J Periodontol 1967;38(Suppl):610-616.
43. Bernimoulin JP, Luscher B, Mühlemann HR. Coronally repositioned periodontal flap. Clinical evaluation after one year. J Clin Periodontol 1975;2:1-13.

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
12
44. Scheid RC, Weiss G. Woelfel's Dental Anatomy. Eighth Edition. Philadelphia: Lippincott Williams & Wilkins; 2012:65-162.
45. Spray JR, Black CG, Morris HF, Ochi S. The influence of bone thickness on facial marginal bone response: Stage 1 placement through stage 2 uncovering. Ann Periodontol 2000;5:119-128.
46. Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int J Oral Maxillofac Implants 2004;19(Suppl):43-61.
Address correspondence and requests for reprints to Dr. Henry Greenwell, Graduate Periodontics, School of Dentistry, University of Louisville, Louisville, KY 40292
(address is complete); Phone 502 852-6928; Fax 502 852-1317; email [email protected]
Submitted September 26, 2012; accepted for publication December 12, 2012.
Figure 1a.
Concave ridge contour associated with intrasocket graft alone treatment at 4 months associated with the extraction of tooth #5.
Figure 1b.
Convex ridge contour associated with the overlay graft treatment at 4 months associated with the extraction of tooth #4.
Figure 2a.
Vital bone harvested from the cancellous allograft site, which contains osteocytes in the lacunae. 100X.
Figure 2b.
Osteoblasts lined up along the surface of vital bone. Arrows indicate osteoblasts. 200X.
Figure 2c.
Appositional bone growth with vital bone growing on non-vital residual graft particles. Arrows indicate vital bone that has formed on non-vital bone. 200X.
Table 1
Horizontal Ridge Width for Intrasocket and Overlay Sites Mean ± sd in mm Group Initial Final Change % Change Range
Intrasocket at Crest 8.7 ± 1.0 7.1 ± 1.5 -1.6 ± 0.8* -19 ± 11 -3.4 to - 0.5
Overlay at Crest 8.4 ± 1.4 8.1 ± 1.4 -0.3 ± 0.9† -3 ± 10 -2.0 to 0.9
Intrasocket at 5 mm 9.1 ± 0.9 8.4 ± 0.9 -0.8 ± 0.5* -8 ± 5 -1.8 to 0.0
Overlay at 5 mm 8.6 ± 1.9 9.1 ± 2.0 0.5 ± 0.6*† 7 ± 8 -0.8 to 1.5
* = p < 0.05 between initial and 4-month values
† = p < 0.05 between overlay and intrasocket groups

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
13
Table 2
Vertical Ridge Height Change for Intrasocket and Overlay Sites Mean ± sd in mm
Location Intrasocket Overlay Intrasocket Overlay
Mean Change ± sd in mm Range in mm
Mid-Buccal 0.5 ± 2.9 0.3 ± 2.6 -2.0 to 8.0 -3.0 to 5.0
Mid-Lingual -0.4 ± 0.6 -0.5 ± 0.7* -1.5 to 0.5 -1.5 to 0.5
Mesial -0.5 ± 0.4* -0.6 ± 0.4* -1.2 to 0.0 -1.1 to 0.0
Distal -0.8 ± 0.3* -0.4 ± 0.4*† -1.3 to -0.1 -1.0 to 0.0
* = p < 0.05 between initial and 4-month values
† = p < 0.05 between overlay and intrasocket groups
Table 3
Histologic Data at Implant Placement for Intrasocket and Overlay Sites Mean ± sd Group Time n % Vital % Non-vital % Trabecular
Intrasocket 4 month 12 35 ± 16 21 ± 13 44 ± 9
Overlay 4 month 11 40 ± 16 17 ± 11 43 ± 12
Table 4
Ridge Dimensions by Tooth Type Mean ± sd in mm Tooth Type n Initial Final Change % Change
Maxillary Incisor 38 7.7 ± 1.0 5.8 ± 1.4 -1.9 ± 1.2 -24 ± 15
Mandibular Incisor 2 5.9 ± 0.2 5.1 ± 0.0 -0.9 ± 0.2 -15 ± 3
Maxillary Canine 8 8.8 ± 0.7 6.4 ± 2.1 -2.4 ± 2.0 -28 ± 22
Mandibular Canine 3 7.8 ± 1.8 7.0 ± 2.5 -0.8 ± 1.7 -10 ± 23
Maxillary Premolar 99 9.4 ± 1.2 8.0 ± 1.3 -1.4 ± 1.1 -14 ± 11
Mandibular Premolar 24 7.8 ± 1.3 7.4 ± 1.3 -0.4 ± 1.0 -4 ± 13
* RegenerOssTM, BioMet 3i, Palm Beach Gardens, FL 33410 † Bio-Oss, Geistlich Pharma North America, Inc, Princeton, NJ 08540 ‡ Guidor®, Sunstar Americas, Inc, Chicago, IL 60630 § Cytoplast® PTFE Suture, Osteogenics Biomedical, Inc, Lubbock, TX 79424 ║ H & H Company, Ontario, CA 91761

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
14

Journal of Periodontology; Copyright 2013 DOI: 10.1902/jop.2013.120585
15

Dimensional alterations ofextraction sites after differentalveolar ridge preservationtechniques – a volumetric studyThalmair T, Fickl S, Schneider D, Hinze M, Wachtel H. Dimensional alterations ofextraction sites after different alveolar ridge preservation techniques – a volumetricstudy. J Clin Periodontol 2013; doi: 10.1111/jcpe.12111.
AbstractObjectives: The aim of this randomized controlled clinical study was to assesssoft tissue contour changes after different alveolar ridge preservation procedures.Material and Methods: Following tooth extraction, 30 patients were randomlyassigned to the following treatments (Tx) - Tx 1: xenogenic bone substitute (pre-hydrated collagenated cortico-cancellous porcine bone) and free gingival graft; Tx2: free gingival graft alone; Tx 3: xenogenic bone substitute; Tx 4: no furthertreatment (control). Impressions were obtained before tooth extraction (baseline)and 4 months after surgery. Cast models were optically scanned, digitally super-imposed and horizontal measurements of the contour alterations between timepoints were performed using digital imaging analysis.Results: All groups displayed contour shrinkage at the buccal aspect rangingfrom a mean horizontal reduction of !0.8 " 0.5 mm (Tx 1) to !2.3 " 1.1 mm(control). Statistically significant differences were found between Tx 1 and Tx 4as well as Tx 2 and Tx 4. A significant positive influence of the free gingival grafton the maintenance of the ridge width was recorded (p < 0.001).Conclusion: In this study, alveolar ridge preservation techniques were not able toentirely compensate for alveolar ridge reduction. Covering the orifice of theextraction socket with a free gingival tissue graft seems to have the potential tolimit but not avoid the post-operative external contour shrinkage based on opticalscans.
Tobias Thalmair1, Stefan Fickl2,David Schneider4, Marc Hinze1 andHannes Wachtel1,3
1Private Institute for Periodontology andImplantology, Munich, Germany; 2Departmentof Periodontology, Julius-MaximiliansUniversity, Wurzburg, Germany; 3Departmentof Prosthodontics, Dental School, FreeUniversity of Berlin, Berlin, Germay; 4Clinic ofFixed and Removable Prosthodontics andDental Material Science, University of Zurich,Zurich, Switzerland
Key words: alveolar ridge preservation;dimensional alterations; extraction socket;soft tissue punch
Accepted for publication 28 March 2013
Marked morphological and dimen-sional alterations of the alveolarridge occur after tooth extraction(Cardaropoli et al. 2003, Schroppet al. 2003, Araujo and Lindhe,2005). Both horizontal and vertical
changes in dimensions are expectedin hard tissue as well as soft tissue(Van der Weijden et al. 2009). Theresulting dimensional changes havebeen evaluated by volumetric analy-sis in a clinical study (Schropp et al.2003). The loss of volume in the hor-izontal dimension amounts 5–7 mmwithin the first 12 months. This cor-responds with approximately 50% ofthe original width of the alveolarbone (Schropp et al. 2003). Theresorption of the ridge is morepronounced on the buccal than on
the lingual aspect of the extractionsocket (Araujo and Lindhe, 2005)and limited to the marginal one-third of the post-extraction site (Ara-ujo et al. 2008). It was suggestedthat the higher amount of resorptionat the buccal aspect is due to therelatively greater proportion of bun-dle or “tooth-derived” bone faciallythat loses its function after toothextraction and undergoes atrophy(Araujo and Lindhe, 2005). As thebuccal wall of the tooth socket isfrequently partially or completely
Conflict of interest and source offunding statement:
The authors declare that they have noconflicts of interest. This study wassupported in part by Tecnoss, Torino,Italy.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd 1
J Clin Periodontol 2013; doi: 10.1111/jcpe.12111
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza
Daniel Jiménez Cabeza

resorbed (Araujo and Lindhe, 2005),consequently a collapse of thebuccal soft tissue leads to markedbucco-oral alterations (Schroppet al. 2003). In particular, in theanterior zone the mentioned altera-tions of the extraction socket canjeopardize the aesthetic outcome ofany dental treatment involving toothextraction.
To reduce volumetric changesoccurring after tooth extraction,different treatment modalities havebeen recommended. As implantinstallation was not able to alterbiological procedures (Ara!ujo et al.2005, Botticelli et al. 2004), it wassuggested that incorporation ofbiomaterials into a fresh extractionsocket could be a suitable techniquefor socket augmentation with theability to maintain the ridge dimen-sion to a certain extent (Nevins et al.2006, Cardaropoli et al. 2005). Sev-eral studies have proposed variousridge preservation techniques follow-ing tooth extraction including theplacement of graft materials and/orthe use of occlusive membranes(Camargnola et al. 2003, Lekovicet al. 1998, Lekovic et al. 1997,Cardaropoli et al. 2005) showingthat a significant reduction in alveo-lar bone resorption could beavoided. However, data obtainedfrom experimental studies showedthat incorporation of biomaterialsinto the extraction socket is not ableto diminish the biological process ofthe buccal bone plate (Fickl et al.2008a, Fickl et al. 2008b).
Techniques to achieve soft tissueclosure of extraction sites have beendeveloped, mainly related toimmediate implant placement. Junget al. (2004) introduced the soft tissuepunch technique, the extractionsocket was filled with a bone substi-tute and covered with an epithelial-ized free connective tissue graft. Itwas proposed that stabilizing the softtissue architecture with a free gingivalgraft has beneficial effects on mini-mizing the soft tissue shrinkage (Junget al. 2004). It was demonstrated thatplacing a deproteinized bovine bonematerial (DBBM) into the extractionsocket and closing the socket with afree gingival graft was beneficial inlimiting the volumetric shrinkage(Fickl et al. 2008b, Fickl et al. 2008a).
To date, it is still uncertain whichalveolar ridge preservation technique
is the most predictable. Therefore,the aim of this clinical investigationwas to evaluate, to which extent afiller or a soft tissue socket sealcontributes to ridge preservation.
Materials and Methods
The research protocol and the con-sent form of this clinical investiga-tion were approved by the ethicalcommittee of the Julius-MaximiliansUniversity, Wuerzburg, Germany(183/11).
Study population
Subjects selected for participating inthis prospective clinical study werecounselled and written informedconsent was obtained prior to thesurgical procedure (Helsinki Declara-tion of 1975 as revised in 2000). Thepatients were enrolled and treated ina period of time between January2011 and September 2011.
The study population consistedof 30 adult patients (mean age 46.2,range 24–72 years, 13 females)requiring treatment of tooth extrac-tion in the anterior zone ranging tothe second bicuspid. The reasons forextraction included root fractures,endodontic treatment failures andadvanced caries lesions.
The following exclusion criteriawere applied:(1) Age <18 years.(2) Smoking status of more than 10cigarettes/day.(3) Presence of relevant medical con-ditions: Patients with diabetes mell-itus, unstable or life-threateningconditions, or requiring antibioticprophylaxis. Patients with medica-tion of drugs influencing the bonemetabolism were also excluded.(4) Pregnant or lactating women.(5) History of malignancy, radiother-apy, or chemotherapy for malignancyin the past 5 years.(6) History of autoimmune disease.(7) Presence of acute periodontal orperiapical pathology.
Only teeth with an intact buccalbone plate were included in thestudy population. The condition ofthe buccal bone plate was evaluatedintra-surgically after tooth extrac-tion. All extraction sites presented aminimum width of 2 mm of kerati-nized gingival tissue.
All patients received instructionsin oral hygiene and underwent initialperiodontal evaluation includingprofessional tooth cleaning with scal-ing and polishing until full-mouthplaque score and full-mouth bleedingscore <20% were reached.
Inter-examiner accuracy control
All surgical procedures were per-formed by four operators (H.W.,T.T., S.F. and M.H.) in the sameclinic (Private Institute for Periodon-tology and Implantology, Munich,Germany).
To control the accuracy andrepeatability between surgeons, a cali-bration meeting was held in Munich(October 2010). Procedures wereexplained using digital images and sur-gical videos. Within the discussion atthe calibration meeting, it was decidedto make a variation to the originalapproved protocol (two-arm studywith Tx 1 and Tx 3) and to add twoadditional groups (Tx 2 and Tx 4).
Clinical procedure
Before surgery, impressions of thejaws were obtained in a one-step/two-viscosity technique with polye-ther impression materials (Perma-dyne Garant 2:1/Permadyne PentaH; 3M Espe, St. Paul, MN, USA).
Following the administration oflocal anaesthesia, an intra-sulcularincision was performed and the teethwere gently extracted withoutelevation of a mucoperiosteal flap orcompromising the marginal gingiva.Care was taken to produce as littletrauma as possible to the bonearound the alveolus. If necessary, theteeth were sectioned to allow atrau-matic extraction and, more impor-tantly, preservation of all bone walls.In case of deep fractured teeth, whenthe remaining supragingival toothstructure was insufficient for the useof a forceps, a specific root extractiondevice with intra-canalicular anchor-age (Benex-Extractor, Zepf Medizin-technik GmbH, Seitingen-Oberflacht,Germany) was used to avoid traumato the surrounding tissues. The extr-action sockets were carefully curettedto remove granulation tissue.
Patients were enrolled sequen-tially. A randomization list wasgenerated. Randomization envelopeswere supplied and numbered sequen-
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
2 Thalmair et al.

tially containing the treatmentallocation according to the randomi-zation list.
The extraction sites were ran-domly assigned to one of the follow-ing treatments:
Treatment 1 (Tx 1): The extrac-tion socket was treated using thesocket seal technique (Jung et al.2004). The internal marginal gingivaof the extraction socket was deepi-thelialized with a diamond bur untilbleeding was evident. The extractionsocket was filled with a xenogenicbone substitute (pre-hydrated colla-genated cortico-cancellous porcinebone; mp3 OsteoBiol, Tecnoss, Tor-ino, Italy) to the level of the bonecrest. A free gingival graft with athickness of 3 mm was harvestedfrom the palate/tuberosity andsutured to the marginal gingiva of theextraction socket with several inter-rupted sutures (Seralene 7–0, SeragWiesner, Naila, Germany) (Fig. 1).
Treatment 2 (Tx 2): The internalmarginal gingiva of the extractionsocket was deepithelialized with adiamond bur and a free gingivalgraft was sutured into the orifice ofthe extraction socket in the samemanner as in Tx 1, however, withoutthe use of a filler material.
Treatment 3 (Tx 3): The extrac-tion socket was filled with mp3(OsteoBiol, Tecnoss, Torino, Italy)and secured with a non-resorbablesuture material (Gore-Tex CV5,W.L. Gore & Associates, Putzbrunn,Germany) without the use of a gingi-val graft (Fig. 2).
Treatment 4 (Tx 4): The extrac-tion socket remained with its bloodclot only (control).
Consecutively, a pre-fabricatedresin-bonded bridge was fixed to theadjacent teeth without any contactof the pontics to the extractionsocket with an auto-polymerizingresin material (Clearfil Cores; Kura-ray, Tokyo, Japan).
Post-surgical protocol
The patients were instructed to rinsewith 0.2% chlorhexidine digluconatetwice a day for at least 2 weeks(Vaughan and Garnick, 1989). Toreduce swelling, Ibuprofen (600 mg)was prescribed (Pearlman et al.1997). Sutures were removed 7 daysafter surgery. Polyether impressions(Permadyne Garant 2:1/Permadyne
Penta H; 3M Espe) were obtained4 months after tooth extraction.
Evaluation of tissue contour changes
The analysis of the soft tissue contourchanges was performed at the Clinicof Fixed and Removable Prosthodon-tics and Dental Material Science,University of Zurich, according toprevious studies (Fickl et al. 2009,Thoma et al. 2010).
Master casts of each patient weremade with dental stone (CAM-Base,Dentona AG, Dortmund, Germany)utilizing the pre-extraction and fol-low-up impressions after 4 months.The cast models were opticallyscanned and digitized (Iscan D101,Imetric GmbH, Courgenay, Switzer-land) creating STL files (StandardTessellation Language). The STL filesof these digital models representingthe two treatment time points wereimported into a specific software(SMOP, Swissmeda, Zurich, Switzer-land) and were superimposed accord-ing to the buccal surface of theadjacent teeth using the best-fit algo-rithm. The same software was used tomeasure the dimensional changes inthe relevant buccal alveolar ridge areacomparing the contour before toothextraction and 4 months after ther-apy (Fig. 3). The area of measure-ment was defined by a line parallel tothe tooth axis in the middle of the
mesial and distal papilla, by themucogingival line and the most coro-nal contour line of the alveolar ridge.As the size of this area differed fromsite due to the difference in tooth/gapsize, the mean volume change perarea was calculated as a distance inbuccal direction (!d [mm] = !vol[mm3]/area [mm2]) to allow a directcomparison of dimensional changesbetween the sites.
Before the beginning of the evalua-tion, a calibration exercise was per-formed to obtain reproducibility forthe measurement of the relevant buccalarea. This analysis was conducted bytwo examiners (D.S. and T.T.), one ofthem was blinded (D.S.).
Statistical analysis
Sample size calculation was per-formed on the results of previousstudies (Fickl et al. 2009, Ficklet al. 2008b) and resulted in sevensubjects per group. For the primaryoutcome variable (mean dimensionalchange) it was assumed that thetrue difference between groupswould amount to 0.75 mm with aSD of 0.5. The Type I error proba-bility was set at 0.05, the statisticalpower at 80%.
Statistical analysis was performedusing a statistical software program(SPSS 20, IBM Corporation, Arm-onk, NY, USA) by a statistician (M.
(a) (b)
(c) (d)
Fig. 1. Treatment group 1. (a) after gentile extraction of tooth 21 the buccal wall isintact, (b) a xenogenic bone substitute is applied into the extraction socket, (c) a gingi-val autograft is sutured to the marginal soft tissue, (d) clinical situation 4 monthspost-surgically.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Different alveolar ridge preservation techniques 3

Roos) at the Division of Biostatistics,University of Zurich.
The primary outcome variable washorizontal soft tissue dimensionalchange at 4 months after toothextraction.
Descriptive statistics including boxplots were used to indicate the mean,median, minimum, maximum valuesand the standard deviation in eachtreatment group. Kolmogorov–Smir-nov Test was used to check the cor-
rectness of the normality assumption.Differences in mean distance changebetween groups were tested by apply-ing one-way analysis of variance(ANOVA) and post hoc Scheffe test.
Influence of bone filler materialand soft tissue seal and other variableslike age, gender, jaw or tooth typewere the secondary outcome variables.
Two-way ANOVA was used to iden-tify possible influence of the bonesubstitute filler and the soft tissue seal
on the mean distance change. Spear-man correlation was computed toindicate associations between themean distance change and variables(age, gender, jaw, jaw location andmethod of extraction). Fisher’s exacttest was applied to find associationsbetween two binary variables. Krus-kal–Wallis tested the influence of thesurgeons. The level of significancewas set at p < 0.05.
Results
All patients completed the study. Thirtypatients were included (13 females);eight were smokers. The mean age was46.2 years, ranging from 24 to 72 years(Table 1 and Appendix S1).
Qualitative assessment
Healing of all treatment groups wasuneventful. No intra-operative or post-operative complications occurred.Clinically, 1 week after insertion of thegingival graft, all areas were vascular-ized, some parts were covered withfibrin and responded by bleeding afterremoval of the fibrinoid surface.Necrotic parts or incomplete woundclosure were not observed.
After 4 months, all free gingivalgrafts of group Tx 1 and Tx 2 werefully integrated.
Quantitative assessment
The results of the dimensional evalua-tion are displayed in Tables 2 and 3and Appendix S1.
Horizontal contour shrinkage at thebuccal aspect during the 4 month heal-ing period was observed in all groupsand ranged from !0.8 " 0.5 mm (Tx1) to !2.3 " 1.1 mm (Tx 4/Control).
The following dimensional changesoccurred according to the treatmentoption (descriptive data betweenstages):
Treatment 1 (Tx 1): Meandimensional differences betweenbaseline and the 4 month scan were!0.79 " 0.5 mm (range: !0.13 to!1.33 mm) buccally.
Treatment 2 (Tx 2): Fourmonths after tooth extraction, thefollowing dimensional changes wererecorded for the buccal aspect:!0.85 " 0.6 mm (range: !0.15 to!1.60 mm).
Treatment 3 (Tx 3): The meandifferences between baseline and the
(a) (b)
(c) (d)
Fig. 2. Treatment group 3. (a) tooth 14 needs to be extracted, (b) a xenogenic bonesubstitute is applied into the extraction socket, (c) buccal view and (d) occlusal view at4 months post-surgically display the contour preservation.
(a) (b)
(c) (d)
Fig. 3. Measured area of tissue volume changes. (a) and (b) superimposed images dem-onstrating volumetric changes between baseline (yellow colour area) and 4 months(green colour area). (c) and (d) buccal and occlusal view of the measured area (regionof interest) in blue colour.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
4 Thalmair et al.

4 month scans were !1.45 " 0.7 mm(range: !0.73 to !2.14 mm).
Treatment 4 (Tx 4): The meandifference of the dimensional con-tour changes was !2.29 " 1.1 mm(range: !1.23 to !3.34 mm).
The comparison of the groups byunpaired t-tests (one-way ANOVA)resulted in significant differences indimensional change between the testgroups Tx 1 and Tx 2 comparedwith control group Tx 4. No othersignificant differences were observedbetween groups (Fig. 4).
Two-way ANOVA showed a signifi-cant influence of the soft tissuesocket seal leading to a lower degreein shrinkage (B = 1.05; p < 0.001).The influence of the filler was esti-mated to be not significant(B = 0.42; p = 0.125).
The extraction procedure – sepa-ration of the root, extraction withforceps or with a mechanical device– had no influence on the buccalcontour changes.
There was no difference in thevolume alterations regarding thelocation of the tooth. No differencewas found between teeth located inmaxilla or mandibula.
Spearman correlation did notshow any significant associationbetween predictors (age, gender,smoking, jaw, jaw location andmethod of extraction) and the meandistance difference.
Kruskal–Wallis test revealed nostatistically significant differenceamong the different surgeons(p = 0.964).
Discussion
Indications for ridge preservationare maintaining a stable ridge vol-ume for optimizing functional andaesthetic outcome and simplifyingthe treatment procedures subsequentto ridge preservation.
This study evaluated differenttechniques for alveolar ridge preser-vation following tooth extraction,generating sufficient soft tissue vol-ume for the time of implant place-ment thus simplifying implantationprocedures at earlier time points.The use of xenogenic bone substi-tute, a free gingival graft and thecombination of both for alveolarridge preservation were assessed.Preserving the extraction socket by
the application of a free gingivalgraft with or without a xenogenicbone substitute reduced post-opera-tive tissue shrinkage to a certainextent. The outcome of this random-ized controlled clinical investigationdemonstrated that the different alve-olar ridge preservation techniquesresulted in less contour reductionfrom the buccal aspect when com-pared with unassisted socket healing.
The findings of this study can bewell compared to previous animalstudies using a similar volumetricdata analysis. The horizontal contourchanges on the buccal aspect, afterextraction the socket was filled withDBBM and covered with a free gin-gival graft, demonstrated !1.5 mm.It was concluded that the applicationof DBBM seemed to limit the tissueshrinkage (Fickl et al. 2008b).
A xenogenic porcine bone substi-tute was used in this clinical trial, itwas investigated as natural scaffold fornew bone formation. An almost com-plete incorporation of the cortico-can-cellous particles surrounded by vitalbone was observed (Barone et al.2008). Compared to ridge preservationwith a bovine bone substitute, thegrafted sites comprised connective tis-sue including the graft particles andsmall amounts of newly formed bone(Carmagnola et al. 2003).
The results of this study indicatethat the free gingival graft for cover-ing the extraction socket revealedstatistically significant superiorresults in minimizing the buccal con-tour shrinkage, irrespective of addi-tionally a xenogenic bone substitutewas applicated or not. The biologicalintegration of the free gingival graftwas successful as no complicationregarding graft necrosis could beobserved. It can be assumed that thesoft tissue cover at the extraction sitehas the potential to limit the post-operative contour alterations to acertain extent.
This is in accordance with theclinical study of Jung et al. (2004),who reported that 3 weeks after sur-gery, 99.7% of the soft tissue graftswere fully integrated (Jung et al.2004). Landsberg and Bichacho(1994) stated that due to primarywound closure and the additionalmechanical stability of the free auto-graft, the soft tissue collapse mightbe avoided to a certain extent. A sta-tistically significant effect of the
Table 1. Randomization of treatment options per extraction sites
Group Number Gender(M/F)
Smoker Maxilla(anter/premol)
Mandibula(premol)
Reason fortooth
extraction(endo/
fract/caries)
Tx 1 8 3/5 2 7 (4/3) 1 5/3/–Tx 2 8 7/1 1 7 (4/3) 1 4/2/2Tx 3 7 5/2 2 5 (2/3) 2 3/2/2Tx 4 7 3/4 2 5 (2/3) 2 3/2/2
endo, endodontic reason; fract, root fracture; caries, advanced caries lesion.
Table 3. Volumetric data describing the distribution according to mean dimensional change
Group <0.5 mm 0.5–1.0 mm 1.0–1.5 mm 1.5–2.0 mm >2.0 mm
Tx 1 3 2 3 – –Tx 2 2 3 2 1 –Tx 3 – 2 2 2 1Tx 4 – – 2 1 3
Table 2. Descriptive statistics with measured area (mm2/mm3) and volume changes (mean,minimum and maximum)
Group Area (mm2) ! Vol (mm3) Mean ! distance(mm)
Min/max ! distance(mm)
Tx 1 22.04 " 3.70 19.92 " 3.77 !0.79 " 0.5 !0.13 " 0.17/!1.33 " 0.21Tx 2 23.46 " 2.16 24.89 " 7.68 !0.85 " 0.6 !0.15 " 0.20/!1.60 " 0.19Tx 3 19.63 " 1.29 32.89 " 6.96 !1.45 " 0.7 !0.73 " 0.15/!2.14 " 0.35Tx 4 19.72 " 3.35 41.41 " 15.96 !2.29 " 1.1 !1.23 " 0.26/!3.34 " 0.54
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Different alveolar ridge preservation techniques 5

gingival autograft with respect to themaintenance of the tissue contoursat the buccal aspect was found(Landsberg and Bichacho, 1994).
Within the limits of this studyevaluating the soft tissue contour vol-ume, primary wound closure bymeans of a free gingival graft to sealthe orifice of the extraction socketmight be more beneficial compared tohealing by secondary intention. Thisis contrary to several clinical trialsreporting successful treatment out-comes with secondary wound healing(Camargnola et al. 2003, Serino et al.2003, Serino et al. 2008).
Ridge preservation by simplyusing a xenogenic bone substituteseemed to be more effective thanhealing by clot alone, but this differ-ence was statistically not significantin the present investigation. Thislack of evidence may be due to thesmall number of subjects. This find-ing would be in accordance with sev-eral clinical trials indicating a strongevidence that ridge preservation withgrafting materials is more effective(Barone et al. 2008, Cardaropoli andCardaropoli, 2008). However, it wasdemonstrated that in marginal por-tions of some sockets bone substituteparticles surrounded by granulationtissue occurred (Araujo et al. 2010,Araujo and Lindhe, 2009).
According to previous studiesshowing that the resorption of thealveolar ridge is more pronouncedon the buccal than on the lingualaspect of the extraction socket (Ara-ujo and Lindhe, 2005, Schropp et al.2003), only the buccal soft tissue
compartment of the experimentalsites was analysed. This is a limita-tion of the study. Because measure-ments were based on master models,no statements can be made as towhether the documented horizontalvolume resorption was caused byloss of soft tissue or underlyingbone. However, no complete preser-vation of the outline of the alveolarcrest could be assessed in particularat the buccal aspect.
The applied technique showed ahigh reproducibility and an excellentaccuracy for measuring volumechanges with a measurement errorbelow 10 mm (Mehl et al. 1997,Windisch et al. 2007). This methodoffers advantages including its non-invasive character, absence of radia-tion and the fact that it can easily beapplied. Currently, there is oneshortcoming of the techniquebecause optical scans were per-formed on study casts in this study.The accuracy of the method is highlyinfluenced by the accuracy of theimpressions and the casts.
Another limitation of the study isthe small number of patients in eachgroup. Further clinical investigationshould be conducted to recruit alarger patient collective to increasethe statistical power of clinical inves-tigations.
It is generally assumed that theanterior segment of the dentitionresponded differently than premolarsites to horizontal ridge reduction.This may indicate that anterior sitesare more susceptible to ridge altera-tions than premolar sites. The results
of this clinical trial did not show adifference in location and type oftooth.
The most important clinicalimpact of alveolar ridge preservationtechniques on patient-related out-come should be to optimize implantplacement in the correct position andto avoid additional augmentationprocedure. However, a statistical sig-nificance favouring one alveolar ridgepreservation technique does not nec-essarily lead to a clinical benefit forthe patient, unless the whole treat-ment is simplified or made more suc-cessful. There is still a lack ofsufficient evidence on implant-relatedoutcome. Only few studies reportedon a possible influence of alveolarridge preservation on placingimplants and need of further augmen-tation therapies (Serino et al. 2008,Fiorellini et al. 2005). Therefore, thepositive influence of alveolar ridgepreservation techniques on patient-related outcome may be attributedmore to achieving enhanced restor-ative and aesthetic outcomes, as wellas better maintenance of healthy peri-implant soft tissues (Vignoletti et al.2012).
In conclusion, the present clinicalstudy demonstrates that the investi-gated alveolar ridge preservationtechniques were not able to preventsoft tissue contour alterations entirelyafter tooth extraction. It appears thatcomplete ridge preservation is notpossible with the alveolar ridge pres-ervation techniques evaluated. Theuse of a free gingival graft coveringthe extraction socket was beneficialfor maintaining soft tissue volume.More studies including a higher num-ber of patients or sites are needed tofurther investigate these findings.
References
Araujo, M. G., Liljenberg, B. & Lindhe, J. (2010)Dynamics of Bio-Oss Collagen incorporation infresh extraction wounds: an experimental studyin the dog. Clinical Oral Implants Research 21,55–64.
Araujo, M. G. & Lindhe, J. (2009) Ridge preser-vation with the use of Bio-Oss collagen: a6-month study in the dog. Clinical OralImplants Research 20, 433–440.
Araujo, M., Linder, E., Wennstrom, J. & Lindhe, J.(2008) The influence of Bio-Oss Collagen on heal-ing of an extraction socket: an experimental studyin the dog. The International Journal of Periodon-tics & Restorative Dentistry 28, 123–135.
Araujo, M. & Lindhe, J. (2005) Dimensional ridgealterations following tooth extraction. An
Fig. 4. Volumetric changes indicated as mean change distance in millimetres.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
6 Thalmair et al.

experimental study in the dog. Journal of Clini-cal Periodontology 32, 212–218.
Ara!ujo, M., Sukekava, F., Wennstrom, J. & Lind-he, J. (2005) Ridge alterations followingimplant placement in fresh extraction sockets:an experimental study in the dog. Journal ofClinical Periodontology 32, 645–652.
Barone, A., Aldini, N., Fini, M., Giardino, R.,Calvo Guirado, J. & Covani, U. (2008)Xenograft versus extraction alone for ridgepreservation after tooth removal: a clinical andhistomorphometric study. Journal of Periodon-tology 79, 1370–1377.
Botticelli, D., Berglundh, T. & Lindhe, J. (2004)Hard-tissue alterations following immediateimplant placement in extraction sites. Journalof Clinical Periodontology 31, 820–828.
Carmagnola, D., Adriaens, P. & Berglundh, T.(2003) Healing of human extraction socketfilled with Bio-Oss. Clinical Oral ImplantsResearch 14, 137–143.
Cardaropoli, D. & Cardaropoli, G. (2008) Preser-vation of the postextraction alveolar ridge: aclinical and histologic study. The Internationaljournal of periodontics & restorative dentistry28, 469–477.
Cardaropoli, G., Araujo, M., Hayacibara, R.,Sukekava, F. & Lindhe, J. (2005) Healing ofextraction sockets and surgically produced -augmented and non-augmented - defects in thealveolar ridge. An experimental study in thedog. Journal of Clinical Periodontology 32,435–440.
Cardaropoli, G., Araujo, M. & Lindhe, J. (2003)Dynamics of bone tissue formation in toothextraction sites. An experimental study in dogs.Journal of Clinical Periodontology 30, 809–818.
Fickl, S., Schneider, D., Zuhr, O., Hinze, M.,Ender, A., Jung, R. E. & Hurzeler, M. B.(2009) Dimensional changes of the ridge con-tour after socket preservation and buccal over-building: an animal study. Journal of ClinicalPeriodontology 36, 442–448.
Fickl, S., Zuhr, O., Wachtel, H., Bolz, W. & Hu-erzeler, M. B. (2008a) Hard tissue alterationsafter socket preservation: an experimentalstudy in the beagle dog. Clinical Oral ImplantsResearch 19, 1111–1118.
Fickl, S., Zuhr, O., Wachtel, H., Stappert, C. F.,Stein, J. M. & Hurzeler, M. B. (2008b) Dimen-sional changes of the alveolar ridge contourafter different socket preservation techniques.Journal of Clinical Periodontology 35, 906–913.
Fiorellini, J. P., Howell, T. H., Cochran, D.,Malmquist, J., Lilly, L. C., Spagnoli, D., Tolj-anic, J., Jones, A. & Nevins, M. (2005) Ran-domized study evaluating recombinant humanbone morphogenetic protein-2 for extraction
socket augmentation. Journal of Periodontology76, 605–613.
Jung, R., Siegenthaler, D. & H"ammerle, C. (2004)Postextraction tissue management: a soft tissuepunch technique. The International Journal ofPeriodontics & Restorative Dentistry 24, 545–553.
Landsberg, C. & Bichacho, N. (1994) A modifiedsurgical/prosthetic approach for optimal singleimplant supported crown. Part I - The socketseal surgery. Practical Periodontics and Aes-thetic Dentistry : PPAD 6, 11–17.
Lekovic, V., Carmargo, P., Klokkevold, P., We-inlaender, M., Kenney, E., Dimitrijevic, B. &Nedic, M. (1998) Preservation of alveolar bonein extraction sockets using bioabsorbable mem-branes. Journal of Periodontology 69, 1044–1049.
Lekovic, V., Kenney, E., Weinlaender, M., Han,T., Klokkevold, P., Nedic, M. & Orsini, M.(1997) A bone regenerative approach to alveo-lar ridge maintenance following tooth extrac-tions. Report of 10 cases. Journal ofPeriodontology 68, 563–570.
Mehl, A., Gloger, W., Kunzelmann, K. H. & Hic-kel, R. (1997) A new optical 3-D device for thedetection of wear. Journal of Dental Research76, 1799–1807.
Nevins, M., Carmelo, M., De Paoli, S., Friedland,B., Schenk, R., Parma-Benfenati, S., Simion,M., Tinti, C. & Wagenberg, B. (2006) A studyof the fate of the buccal wall of extractionsockets of teeth with prominent roots. TheInternational Journal of Periodontics & Restor-ative Dentistry 26, 19–29.
Pearlman, B., Boyatzis, S. & Daly, C. (1997) Theanalgesic efficacy of ibuprofen in periodontalsurgery: a multicenter study. Australian DentalJournal 42, 328–334.
Schropp, L., Wenzel, A., Kostopoulos, L. & Kar-ring, T. (2003) Bone healing and soft tissuecontour changes following single-tooth extrac-tion: a clinical and radiographic 12-monthprospective study. The International Journal ofPeriodontics & Restorative Dentistry 23, 313–323.
Serino, G., Biancu, S., Iezzi, G. & Piattelli, A.(2003) Ridge preservation following toothextraction using a polylactide and polyglycolidesponge as space filler: a clinical and histologicalstudy in humans. Clinical Oral ImplantsResearch 14, 651–658.
Serino, G., Rao, W., Iezzi, G. & Piattelli, A.(2008) Polylactide and polyglycolide spongeused in human extraction sockets: bone forma-tion following 3 months after its application.Clinical Oral Implants Research 19, 26–31.
Thoma, D. S., Jung, R. E., Schneider, D., Coch-ran, D. L., Ender, A., Jones, A. A., Gorlach,
C., Uebersax, L., Graf-Hausner, U. & Ham-merle, C. H. (2010) Soft tissue volume augmen-tation by the use of collagen-based matrices: avolumetric analysis. Journal of Clinical Peri-odontology 37, 659–666.
Van der Weijden, F., Dell’Acqua, F. & Slot, D.E. (2009) Alveolar bone dimensional changesof post-extraction sockets in humans: a system-atic review. Journal of Clinical Periodontology36, 1048–1058.
Vaughan, M. & Garnick, J. (1989) The effect of a0.125% chlorhexidine rinse on inflammationafter periodontal surgery. Journal of Periodon-tology 60, 704–708.
Vignoletti, F., Matesanz, P., Rodrigo, D., Figu-ero, E., Martin, C. & Sanz, M. (2012) Surgicalprotocols for ridge preservation after toothextraction. A systematic review. Clinical OralImplants Research 23(Suppl 5), 22–38.
Windisch, S. I., Jung, R. E., Sailer, I., Studer, S.P., Ender, A. & Hammerle, C. H. (2007) Anew optical method to evaluate three-dimen-sional volume changes of alveolar contours: amethodological in vitro study. Clinical OralImplants Research 18, 545–551.
Supporting Information
Additional Supporting Informationmay be found in the online versionof this article:
Appendix S1. Individual data of the30 patients. The table reports base-line patient characteristics, treatmentassignement, surgeon and outcomevariables for each patient. The volu-metric changes from baseline to 4months postoperative are expressedin mean, minimum and maximumchange distance.
Address:Tobias ThalmairPraxis Dr. ThalmairKammergasse 1085354 FreisingGermanyE-mail: [email protected]
Clinical Relevance
Scientific rational for the study:Effective ridge preservation tech-niques could reduce the need forridge augmentation proceduresassociated with the subsequentimplant treatment.Principal findings: Ridge preserva-tion procedures using an
autogenous free connective tissuegraft as a socket seal are able toreduce horizontal ridge alterations inpost-extraction sites.Practical implications: In clinicalcases where significant ridge resorp-tion is expected after tooth extrac-tion, the use of a free gingival graft– with or without the application of
a bone substitute – could provide arelatively simple and inexpensivetreatment to limit the contourshrinkage, eventually eliminatinglater augmentation procedures.
© 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd
Different alveolar ridge preservation techniques 7

Fabio VignolettiPaula MatesanzDaniel RodrigoElena FigueroConchita MartinMariano Sanz
Surgical protocols for ridgepreservation after tooth extraction.A systematic review
Authors’ affiliations:Fabio Vignoletti, Paula Matesanz, Daniel Rodrigo,Elena Figuero, Conchita Martin, Mariano Sanz,ETEP Research Group, University Complutense,Madrid, Spain
Corresponding author:Prof. Mariano SanzFacultad de OdontologıaUniversidad Complutense de MadridPlaza Ramon y Cajal, 28040 Madrid, SpainTel.: +34 913 941 901Fax: +34 913 941 910e-mail: [email protected]
Key words: bone grafts, bone regeneration, bone substitutes, dental implants, ridge preserva-
tion, systematic review, tooth extraction
Abstract
Objective: This systematic review aims to evaluate the scientific evidence on the efficacy in the
surgical protocols designed for preserving the alveolar ridge after tooth extraction and to evaluate
how these techniques affect the placement of dental implants and the final implant supported
restoration.
Material and methods: A thorough search in MEDLINE-PubMed, Embase and the Cochrane Central
Register of controlled trials (CENTRAL) was conducted up to February 2011. Randomized clinical
trials and prospective cohort studies with a follow-up of at least 3 months reporting changes on
both the hard and soft tissues (height and/or width) of the alveolar process (mm or %) after tooth
extraction were considered for inclusion.
Results: The screening of titles and abstracts resulted in 14 publications meeting the eligibility
criteria. Data from nine of these 14 studies could be grouped in the meta-analyses. Results from
the meta-analyses showed a statistically significant greater ridge reduction in bone height for
control groups as compared to test groups (weighted mean differences, WMD = !1.47 mm; 95% CI
[!1.982, !0.953]; P < 0.001; heterogeneity: I2 = 13.1%; v2 P-value = 0.314) and a significant greater
reduction in bone width for control groups compared to the test groups (WMD = !1.830 mm; 95%
CI [!2.947, !0.732]; P = 0.001; heterogeneity: I2 = 0%; v2 P-value = 0.837). Subgroup analysis was
based on the surgical protocol used for the socket preservation (flapless/flapped, barrier
membrane/no membrane, primary intention healing/no primary healing) and on the measurement
method utilized to evaluate morphological changes. Meta-regression analyses demonstrated a
statistically significant difference favoring the flapped subgroup in terms of bone width (meta-
regression; slope = 2.26; 95% IC [1.01; 3.51]; P = 0.003).
Conclusions: The potential benefit of socket preservation therapies was demonstrated resulting in
significantly less vertical and horizontal contraction of the alveolar bone crest. The scientific
evidence does not provide clear guidelines in regards to the type of biomaterial, or surgical
procedure, although a significant positive effect of the flapped surgery was observed. There are no
data available to draw conclusions on the consequences of such benefits on the long-term
outcomes of implant therapy.
The alveolar processes in the jaws are tooth-
dependent structures that will undergo signif-
icant structural changes whenever the teeth
are lost. The dynamics and magnitude of
these changes have been investigated in the
dog model (Kuboki et al. 1988; Devlin et al.
1997; Cardaropoli et al. 2003; Araujo & Lind-
he 2005; van Kesteren et al. 2010) as well as
in humans (Amler et al. 1960; Evian et al.
1982; Devlin & Sloan 2002; Trombelli et al.
2008). These investigations have identified
the key processes of tissue modelling and
remodelling after tooth extraction that even-
tually lead to a reduction on the overall ridge
dimensions with significant changes in both
the buccal and lingual bone crests.
The amount of vertical and horizontal
resorption of the socket walls has been inves-
tigated with different methods, ranging from
studying and measuring cast models (Pietro-
kovski & Massler 1967; Johnson 1969;
Schropp et al. 2003), to radiographic analysis
Date:Accepted 26 August 2011
To cite this article:Vignoletti F, Matesanz P, Rodrigo D, Figuero E, Martin C,Sanz M. Surgical protocols for ridge preservation after toothextraction. A systematic review.Clin. Oral Impl. Res. 23(Suppl. 5), 2012, 22–38doi: 10.1111/j.1600-0501.2011.02331.x
© 2011 John Wiley & Sons A/S 22

(Schropp et al. 2003), clinical assessment
with individually pre-fabricated acrylic stents
during re-entry surgeries (Lekovic et al. 1998;
Camargo et al. 2000) and histological studies
in experimental animal models (Cardaropoli
et al. 2003; Araujo & Lindhe 2005). These
studies have evidenced that most of the
resorption occurs during the first 3 months
of healing, although dimensional changes can
be observed up to 1 year after tooth extrac-
tion, resulting in approximately 50% reduc-
tion of the bucco-lingual dimension of the
alveolar ridge (Schropp et al. 2003), mainly
due to the resorption of the buccal bone plate
(Araujo & Lindhe 2005).
The clinical consequences of these physio-
logical hard and soft tissue changes may
affect the outcome of the ensuing therapies
aimed to restore the lost dentition, either by
limiting the bone availability for ideal
implant placement or by compromising the
aesthetic result of the prosthetic restorations.
To counteract these early tissue changes after
tooth extraction, different socket preservation
therapies have been proposed, ranging from a
careful flapless tooth extraction aiming for an
undisturbed socket healing (Fickl et al.
2008a, 2008b), to the immediate placement
of dental implants (Paolantonio et al. 2001),
to filling the resulting alveolar socket with
different grafting materials, with and without
barrier membranes (Fickl et al. 2008a, 2008b).
The possible beneficial effect of a flapless
surgery during tooth extraction for limiting
the resorptive process of the alveolar crest
has been investigated in pre-clinical models
by comparing the outcomes with a flapped
conventional surgery. Although some studies
have shown slightly less pronounced bone
remodelling of the alveolar ridge after flapless
tooth extraction (Fickl et al. 2008a, 2008b),
other studies have failed to encounter signifi-
cant differences between flapped and flapless
tooth extractions (Araujo & Lindhe 2009).
Similarly, the possible beneficial effect of
using grafting procedures or guided bone
regeneration (GBR) to preserve the ridge after
tooth extraction has been tested in both ani-
mal and human studies. Using the dog experi-
mental model (Araujo & Lindhe 2009; Araujo
et al. 2008) filled the socket immediately after
tooth extraction with bovine-derived hydroxy-
apatite or with an autogenous bone graft (Ara-
ujo & Lindhe 2011). While the placement of
the xenograft counteracted the ridge contrac-
tion in the buco-lingual dimension, grafting
with autogenous bone did not significantly
alter the ridge resorptive process. In humans,
the application of regenerative bio-materials,
such as bone autografts, allografts, guided tis-
sue regeneration procedures, xenografts and
most recently, growth factors, has also been
evaluated with varying degrees of success to
maintain the anatomical dimensions of the
alveolar ridge after tooth extraction. A recent
systematic review (Ten Heggeler et al. 2010)
evaluated the efficacy of these therapies in
non-molar alveolar regions suggesting that
these techniques may not prevent the physio-
logical resorptive bone processes after tooth
extraction, although they may aid in reducing
the resulting bone dimensional changes. This
investigation, however, could not draw firm
conclusions due to the limitations in the
existing clinical research.
In terms of histological outcomes in
humans (Becker et al. 1999), used different
biomaterials, such as demineralized freeze-
dried bone, autologous bone, human morpho-
genetic proteins in a carrier to graft human
extraction sockets, reporting that the graft
materials were, 3–7 months later, mainly
surrounded by connective tissue. In contrast
(Artzi et al. 2000), using the same xenogeneic
graft material found the graft particles in
direct contact with bone, although in a simi-
lar study, using the same grafting material
(Carmagnola et al. 2003) found the graft par-
ticles remained within the socket more than
6 months after the extraction and only 40%
of the particles were in direct contact with
bone. It is, therefore, uncertain whether these
socket preservation therapies improve the
outcomes of the different rehabilitation
approaches after tooth loss.
The objective of the present study was to
systematically review all the scientific evi-
dence regarding these therapeutic interven-
tions for socket preservation after tooth
extraction and to assess systematically
the potential benefit of such techniques/
materials when compared with what occurs
when the socket is left to heal spontane-
ously.
The specific objectives were: (1) to describe
the surgical techniques and biomaterials
most commonly used to preserve the socket
architecture after tooth extraction; (2) to eval-
uate their expected outcome on the alveolar
ridge dimension and (3) to assess their impact
on the bone availability for ideal implant
placement or on the resulting prosthetic res-
toration.
Material and methods
Development of a protocol
A protocol covering all aspects of the system-
atic review methodology was developed
before the start of the review, including the
following definitions (Needleman 2002):
• Focused question.
• Study population.
• Types of intervention.
• Types of comparisons.
• Search strategy.
• Eligibility criteria for study inclusion.
• Outcome measures.
• Screening methods and data extraction.
• Quality assessment and data synthesis.
• Assessment of heterogeneity and drawing
of conclusions.
Focused question
“Which are the effects of the different socket
preservation approaches used immediately
after tooth extraction, compared to the spon-
taneous healing of the socket, in terms of the
alveolar ridge hard and soft tissue dimen-
sional changes and in terms of providing suf-
ficient bone availability for implant
placement and/or a restorative final success-
ful outcome?”
Population of study, type of intervention and type ofcomparison
The population of interest for this review
was represented by humans with at least one
tooth to be extracted, older than 18 years and
in good general health. A minimum sample
size (10 subjects per group) was established
in an attempt to minimize the publication
bias. The definition used for extraction
socket preservation therapy was: “Any thera-
peutic approach carried out immediately after
tooth extraction aimed to preserve the alveo-
lar socket architecture and to provide the
maximum bone availability for implant
placement.”
The specific therapeutic interventions eval-
uated in this study were:
• filling the socket with autologous bone
grafts or bone substitutes (allogenic, xeno-
genic and synthetic grafts);
• isolating the socket with the use of bar-
rier membranes, soft tissue autografts or
soft tissue substitutes (allogenic and oth-
ers) and,
• promoting the healing process of the
socket by the addition of growth factors
or bone morphogenetic proteins.
These interventions were compared to the
spontaneous healing of the socket.
Search strategy
Three electronic databases were used as
sources in the search for studies satisfying the
© 2011 John Wiley & Sons A/S 23 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

inclusion criteria: (1) The National Library of
Medicine (MEDLINE via Pubmed); (2) Embase
and (3) Cochrane Central Register of Con-
trolled Trials. These databases were searched
for studies published until February 2011.
The search was limited to human subjects.
The following search terms were used:
Population
(<[text words] Tooth> OR <[MeSH terms/
all subheadings] “Tooth”>) AND
([text words] Extraction)
OR
(<[Text words] Tooth extraction OR Extrac-
tion socket* OR Alveolar socket* OR dental
extraction* OR tooth removal OR socket*
OR ridge-socket* OR post-extraction socket*
OR fresh extraction socket* OR alveolar
crest> OR <[MeSH terms/all subheadings]
“Tooth Extraction*” OR “Tooth socket*”>)
Intervention
[text words] Socket*preservation OR Ridge
preservation OR bone preservation OR socket*
seal OR Site* preservation OR Bone filler* OR
Autologous bone graft* OR autologous bone
OR autogenous bone graft* OR Autogenous
bone OR bone substitute* OR growth factor*
OR rhBMP OR bone morphogenetic protein*
OR allogenic graft* or Allograft* OR xenogen-
ic graft* OR OR xenogeneic graft* OR xeno-
graft* OR synthetic graft* OR Barrier
membrane* OR membrane* OR resorbable
membrane* or non-resorbable membrane OR
guided bone regeneration OR GBR OR freeze
dried bone allograft* OR demineralized freeze
dried bone allograft* OR DFDBA OR FDBA
OR Bio-Oss OR Bio-Oss Collagen OR Allo-
plast* OR tricalciumphosphate OR cerasorb
OR Bioglass OR polymeric OR collagen sponge
OR Collagen OR collagen fleece OR collagen
plug* OR Bioguide OR Ossix OR Gore tex OR
ePTFE OR soft tissue* autograft* OR connec-
tive tissue graft* OR punch OR free gingival
graft*OR soft tissue* substitute*OR allogenic
soft tissue* OR alloderm OR acellular dermal
matrix OR collagen matrix.
There were no language restrictions. All
reference lists of the selected studies were
checked for cross-references. The following
journals were hand-searched: Journal of Clin-
ical Periodontology, Journal of Periodontol-
ogy, Journal of Periodontal Research;
Clinical Oral Implants Research, Interna-
tional Journal of Oral & Maxillofacial
Implants and Clinical Implant Dentistry and
Related Research.
Eligibility criteria for study inclusion
Randomized clinical trials (RCT) or prospec-
tive cohort studies with a follow-up of at
least 3 months after tooth extraction were
considered for inclusion in this review.
Outcome measures
The primary outcome variable chosen was the
bone dimensional changes occurring in the
socket wall after the tooth extraction and
the socket preservation therapy, measured as
the changes in the height and width of the
alveolar process (mm or %).
As secondary outcome variables, we con-
sidered the soft tissue dimensional changes
(in mm or %), the presence and amount of
keratinized tissue at time of implant place-
ment (yes/no or mm), the changes in clinical
attachment levels (CAL) evaluated at the
mesial and distal adjacent teeth, the avail-
ability of bone for implant placement (yes or
no), the need for soft and/or hard tissue aug-
mentation techniques at the time of implant
placement (number and type), the outcome of
the final implant supported restoration evalu-
ated in terms of the prosthetic and/or aes-
thetic result and assessed by the dentist or
the patient using different parameters or
indexes (Jemt index, VAS scale, etc.), and the
peri-implant health status evaluated radio-
graphically or clinically by means of probing
pocket depths, CAL, bleeding on probing and
the plaque index.
Screening methods and data extraction
First, two reviewers (PM and DR) screened
independently the titles and abstracts and did
the primary search. Subsequently, the studies
appearing to meet the inclusion criteria, or
those with insufficient data in the title and
abstract to make a clear decision, were
selected for evaluation of the full manuscript,
which was carried out independently by the
same two reviewers who determined their
eligibility. Any disagreement was resolved by
discussion with a third reviewer (FV). To pre-
vent selection bias, the reviewers were blind
to the name of the authors, institutions and
journal titles. All studies that met the inclu-
sion criteria underwent a validity assess-
ment. The reasons for rejecting studies at
this or at subsequent stages were recorded.
Special attention was paid to duplicate publi-
cations to avoid a likely bigger impact of the
same data on the overall result.
Data extraction
Two reviewers (PM and DR) independently
extracted the data using specially designed
data extraction forms. Any disagreement was
discussed and a third reviewer (EF or FV) was
consulted when necessary. The inter-
reviewer reliability of the data extraction was
calculated by determining the percentage of
agreement and the correlation coefficients
with Kappa analysis. Authors of studies were
contacted for clarification when data were
incomplete or missing. Data were excluded
until further clarification could be available
if agreement could not be reached. When the
results of a study were published more than
once or if the results were presented in a
number of publications, the most complete
dataset was included only once.
Quality assessment
The quality assessment of the included stud-
ies was undertaken independently and in
duplicate by one reviewer (PM) who was blind
to the name of the authors, institutions and
journal titles. This assessment was based on
the study design utilized according to the fol-
lowing criteria for Randomized controlled tri-
als: Quality assessment was carried out
following the recommendations by Cochrane
for assessing risk of bias (Higgins et al. 2009)
and also based on criteria proposed by Ten
Heggeler et al. (2010), which are based on the
RCT-checklist of the Dutch Cochrane Center
(2009), the CONSORT-statements (Schulz
et al. 2010), MOOSE-statement (Stroup et al.
2000), STROBE statements (von Elm et al.
2007) and the recommendations by Needle-
man (2002) and Esposito et al. (2001). Studies
were defined as low risk of bias if these six
criteria were clearly met in the study: random
allocation, definition of inclusion/exclusion
criteria for selecting the population, measures
to blind the patient and examiner, selection
of a representative population group, use of
identical treatment between groups except for
the intervention and detailed reporting of the
follow-up. When missing one of these criteria,
the study was classified as moderate potential
risk of bias. Missing two or more of these cri-
teria resulted in a high potential risk of bias
(Ten Heggeler et al. 2010).
The statistical heterogeneity among studies
was assessed using the Q test according to
Dersimonian and Laird, as well as the I2
index (Higgins et al. 2003) to know the per-
centage of variation in the global estimate
that was attributable to heterogeneity (I2 =
25%: low; I2 = 50%: moderate; I2 = 75%:
high heterogeneity). When the heterogeneity
values were high, a subgroup analysis was
carried out using the following explanatory
variables: (1) use of membrane (Yes/No); (2)
surgical technique (flap Yes/No); (3) primary
wound closure and (4) measurement tool
used to assess the morphological changes.
This subgroup analysis was performed using
meta-regression.
24 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

Data analysis
To summarize and to compare the selected
studies, the data on the primary outcome
(mean bone dimensional changes) were pooled
and analysed using means and 95% confi-
dence intervals. The data on secondary out-
comes were analysed depending on the type of
variable. For dichotomous variables (e.g. suc-
cessful implant placement), the estimates of
the effect were expressed as risk ratio and
95% confidence intervals. For continuous
variables (bone level changes, soft tissue
changes), weighted mean differences (WMD)
and 95% confidence intervals were used.
The study-specific estimates were pooled
using both the fixed effect model (Mantel-
Haenzel-Peto test) and the random effect
model (Dersimonian-Laird test). If a signifi-
cant heterogeneity was found, the random
effect model results were presented.
A Forest Plot was created to illustrate the
effects on the meta-analysis of the different
studies and the global estimation. The publi-
cation bias was evaluated using a Funnel
plot and the Egger’s linear regression
method. A sensitivity analysis of the meta-
analysis results was also performed (Tobias
1999). STATA® (StataCorp LP, Lakeway
Drive, College Station, TX, USA) inter-
cooled software was used to perform all
analyses. Statistical significance was defined
as a P-value <0.05.
Results
Screening
The search strategy resulted in 296 articles.
After an initial phase of screening (agreement
between reviewers of 89.53%; kappa = 0.46),
17 potentially relevant articles were identi-
fied. After reading the complete manuscripts,
three studies were excluded due to inade-
quate study design (Block & Jackson 2006);
inadequate control group (Yilmaz et al. 1998)
and due to only reporting secondary out-
comes (Norton et al. 2003). Hand-search or
cross-reference did not result in any addi-
tional article. Therefore, 14 studies were
finally included (Fig. 1).
Study design and study population
Twelve studies were RCTs with two to five
study groups and with a follow-up period
between 3 and 7 months (Hoad-Reddick et al.
1994; Lekovic et al. 1997; Lekovic et al.
1998; Bolouri et al. 2001; Froum et al. 2002;
Iasella et al. 2003; Fiorellini et al. 2005; Ba-
rone et al. 2008; Aimetti et al. 2009; Crespi
et al. 2009; Casado et al. 2010; Oghli & Ste-
veling 2010) (Table 1). Two studies were con-
trolled clinical studies, one with two study
groups and a 6-month follow-up period (Seri-
no et al. 2003) and the other with three study
groups and a 3-month follow-up (Serino et al.
2008). Six studies presented a split-mouth
design, whereas eight studies presented a par-
allel design.
The study population ranged from 10 indi-
viduals to 125. Smoking habit was reported
in four studies (Hoad-Reddick et al. 1994; Le-
kovic et al. 1997; Lekovic et al. 1998; Bolouri
et al. 2001; Froum et al. 2002; Iasella et al.
2003; Fiorellini et al. 2005; Barone et al.
2008; Aimetti et al. 2009; Crespi et al. 2009;
Casado et al. 2010; Oghli & Steveling 2010)
ranging from 0% to 12%. The periodontal
status of the extracted teeth was defined in
three studies (Serino et al. 2003; Serino et al.
2008). The localization of extracted teeth in
the mouth was reported in nine studies
(Hoad-Reddick et al. 1994; Lekovic et al.
1997; Lekovic et al. 1998; Bolouri et al. 2001;
Froum et al. 2002; Iasella et al. 2003; Fiorel-
lini et al. 2005; Barone et al. 2008; Aimetti
et al. 2009; Crespi et al. 2009; Casado et al.
2010; Oghli & Steveling 2010) in which
most, studied non-molar sites (Hoad-Reddick
et al. 1994; Lekovic et al. 1997; Lekovic et al.
1998; Bolouri et al. 2001; Froum et al. 2002;
Iasella et al. 2003; Fiorellini et al. 2005; Ba-
rone et al. 2008; Aimetti et al. 2009; Crespi
et al. 2009; Casado et al. 2010; Oghli & Ste-
veling 2010), although some were very spe-
cific to mandibular (Hoad-Reddick et al.
1994) or maxillary anterior teeth (Aimetti
et al. 2009), whereas others included any
teeth (Bolouri et al. 2001; Crespi et al. 2009).
Type of intervention and type of biomaterials
Most of the studies (Hoad-Reddick et al.
1994; Lekovic et al. 1997; Lekovic et al.
1998; Bolouri et al. 2001; Froum et al. 2002;
Iasella et al. 2003; Fiorellini et al. 2005; Ba-
Studies included in quantitative synthesis
(meta-analysis)
(n = 9)
Records excluded
(n = 279)
Records screened
(n = 296)
Records after duplicates removed
(n = 296)
Identification
Eligibility
Inclusion
Screening
Additional records identified through other sources
(n = 0)
Records identified through database searching
(n = 296)
Full-text articles excluded, with reasons
(n = 3)
Did not fulfill the inclusion criteriaStudies included in
qualitative synthesis
(n = 14)
Full-text articles assessed for eligibility
(n = 17)
Fig. 1. Flow diagram (PRISMA format) of the screening and selection process.
© 2011 John Wiley & Sons A/S 25 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

UNCO
RREC
TEDPR
OOF
Table
1.Methods,
participants,interventions,
outcomes,
site
andfundingoftheselectedstudies
Study(#)
Method
Participants
Surgicalco
nsiderations
Intervention
Measurementmethod
Outcome
Site
andfunding
Hoad-Reddick
etal.
(1994)
(1)
RCTTwo
study
groups
Parallel
groups
6months
follow-up
18individuals
(-na)
Aged
54.4
years
Smokinghabit:
na
Periodontal
status:
na
Flapless
Primary
closure:na
Typ
eofsocket:
na
Test:Hyd
roxyapatite
granules
Control:Nosocketfilling
Lateral
cephalographs
anddental
pantomograms
Hard
tissue
dim
ensions:
defect
height(m
m)
Not
exp
lained
Not
ava
ilable
Lekovic
etal.
(1997)
(2)
RCTTwo
study
groups
Split
mouth
6months
follow-up
10individuals
(-3)
Aged
49.8
years
Smokinghabit:
na
Periodontal
status:
na
Flap
Primary
closure:YES
Typ
eofsocket:
na
Test:ePTFE
®membrane
Control:
Nosocketfilling
Reentrysurgery
Hard
tissue
dim
ensions:
defect
height(m
m),defect
width
(mm)
Yugoslavia
Not
ava
ilable
Lekovic
etal.
(1998)
(3)
RCTTwo
study
groups
Split
mouth
6months
follow-up
16individuals
(-0)
Aged
52.6
years
Smokinghabit:
na
Periodontal
status:
na
Flap
Primary
closure:YES
Typ
eofsocket:
na
Test:membraneofglyco
lide
andlactidepolimers
Control:
Nosocketfilling
Reentrysurgery
Hard
tissue
dim
ensions:
defect
height(m
m),defect
width
(mm)
Yugoslavia
Not
ava
ilable
Bolouri
etal.
(2001)
(4)
RCTTwo
study
groups
Split
mouth
24months
follow-up
18individuals
(-14)
Aged
54.4
years
Smokinghabit:
na
Periodontal
status:
na
Flap
Primary
closure:YES
Typ
eofsocket:
na
Test:BioplantHTR®
Control:
Nosocketfilling
Hard
tissue
dim
ensions:
optical
density
USA
BioplantInc.
South
Norw
alk,
CT
Froum
etal.
(2002)
(5)
RCTThree
study
groups
Split
mouth
6–8
months
follow-up
19individuals
(-na)
Aged
na
Smoking
habit:0%
Periodontal
status:
na
Flap
Primary
closure:YES
Typ
eofsocket:
4-w
all
Test
1:Bioactiveglass
Test
2:
DFD
BA
Control:Nosocket
filling
Histological
analysis
Histologicalanalysis
USA
Orthovita
Serino
etal.
(2003)
(6)
CTTwo
study
groups
Parallel
groups
6month
follow-up
45individuals
(-na)
Aged
na
Smoking
habit:na
Periodontal
status:
periodontitis
Flap
Primary
closure:YES
Typ
eofsocket:
na
Test:Sp
ongeofpolylactide-
polyglyco
lideacid
Control:No
socketfilling
Reentry
surgery
+stent
Hard
tissue
dim
ensions:
defect
height(m
m)
Histologicalanalysis
Italy
Not
ava
ilable
Iasella
etal.
(2003)
(7)
RCTTwo
study
groups
Parallel
groups
4–6
months
follow-up
24individuals
(-na)
Aged
51.5
Smoking
habit:na
Periodontal
status:
periodontitis
Flap
Primary
closure:NO
Typ
eofsocket:
na
Test:FD
BA
+tetracycline+
collagen
\mombrane
Control:
Nosocketfilling
Clinical+stent
Hard
tissue
dim
ensions:
defect
height(m
m),defect
width
(mm)
Soft
tissuedim
ensions
Histologicalanalysis
USA
Not
ava
ilable
Fiorellini
etal.
(2005)
(8)
RCTFive
study
groups
Parallel
groups
6months
follow-up
80individuals
(-0)
Aged
47.4
Smoking
habit:na
Periodontal
status:
na
Flap
Primary
closure:YES
Typ
eofsocket:
3-w
all(nobuccal
wall)
Test
1:0.75mg/m
lrhBMP/ACS
Test
2:1.50mg/m
lrhBMP/ACS
Control1:Nosocketfilling
Control2:placebo
CTscan
Defect
heightand
width
(mm
CTscan)
Needfor
augmentation
tech
nique
Histologicalanalysis
USA
Wye
th/Genetics
Institute,
Cambridge,MA
Barone
etal.
(2008)
(9)
RCTTwo
study
groups
Parallel
groups
7months
follow-up
40individuals
(-0)
Aged:na
Smokinghabit:
12.5%
Periodontal
status:
na
Flap
Primary
closure:YES
Typ
eofsocket:
4-w
all
Test:Corticocancellousporcine
bone+co
llagenmembrane
Control:Nosocketfilling
Reentry+stent
Hard
tissue
dim
ensions:
defect
height(m
m),defect
width
(mm)
Histologicalanalysis
Italy
Not
ava
ilable
26 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

Table
1.(continued)
Study(#)
Method
Participants
Surgicalco
nsiderations
Intervention
Measurementmethod
Outcome
Site
andfunding
Serino
etal.
(2008)
(10)
CTTwo
study
groups
Parallel
groups
3months
follow-up
20individuals
(-0)
Aged:
na
Smoking
habit:na
Periodontal
status:
Periodontitis
Flap
Primary
closure:NO
Typ
eofsocket:
na
Test:Sp
ongeof
polylactide-polyglyco
lide
acid
Control:No
socketfilling
Histological
analysis
Histological
analysis
Italy
Not
ava
ilable
Aim
etti
etal.
(2009)
(11)
RCTTwo
study
groups
Parallel
groups
3months
follow-up
40individuals
(na)
Aged:
51.27
Smoking
habit:0%
Periodontal
status:
na
Flapless
Primary
closure:NO
Typ
eofsocket:
na
Test:Medical-gradecalcium
sulphate
hemihyd
rate
Control:
Nosocketfilling
Reentry+stent
Dim
ensions
changes:
defect
height(m
m),
defect
width
(mm)
Histological
analysis
Italy
Not
ava
ilable
Crespi
etal.
(2009)
(12)
RCTThree
study
groups
Splitmouth
3months
follow-up
15individuals
(na)
Aged:
51.3
Smoking
habit:0%
Periodontal
status:
na
Flapless
Primary
closure:YES
(tissuegraft)
Typ
eofsocket:
3-w
all
(nobuccalwall)
Test
1:Magnesium-enrich
ed
hyd
roxyapatite
Test
2:Calcium
sulphate
Control:Nosocket
filling
PeriapicalXrays
Dim
ensions
changes:
defect
height(m
m).
Radiological
outcomes
Histological
analysis
Italy
Not
ava
ilable
Casado
etal.
(2010)
(13)
RCTFo
ur
study
groups
Split
mouth
4months
follow-up
19individuals
(na)
Aged:
na
Smoking
habit:na
Periodontal
status:
na
Flap
Primary
closure:YES
Typ
eofsocket:
na
Test
1:bovineBMP+bOM
Test
2:bovineBMP+bOM
+absorbable
membrane
Test
3:
absorbable
membrane
Control:
Nosocketfilling
Clinical+stent
Dim
ensions:
defect
width
(mm)
Histological
analysis
Brazil
Not
ava
ilable
Oghli&
Steve
ling
(2010)
(14)
RCTThree
study
groups
Parallel
groups
3months
follow-up
125individuals
(-14)
Aged:na
Smokinghabit:
na
Periodontal
status:
na
Flapless
Primary
closure:YES(soft
tissuegraft)
Typ
eofsocket:
na
Test
1:Autogenoussoft
tissue
graft
+co
llagenplug2
Test
2:
Autogenoussoft
tissuegraft
+co
llagenmatrix
with
gentamicin
Control:Nosocket
filling
Cast
Dim
ensions
changes:
defect
height(m
m)
Saudi
Arabia
+Germ
any
Not
ava
ilable
Abbreviationsoftheinterventions:
NA,data
notava
ilable;RCT,randomized
clinicaltrial;ACS,
absorbable
collagensponge;e-PTFE
,exp
anded
polytetrafluoroethylene;BMP,bonemorphogeneticpro-
tein;bOM,bovineorganic
matrix;CTscan,co
mputerize
dtomographyscanner;
RhBMP,reco
mbinanthuman
BMP-2;FD
BA,freeze
-dried
boneallograft;DFD
BA,demineralize
dfreeze
-dried
boneallo-
graft.
© 2011 John Wiley & Sons A/S 27 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

rone et al. 2008; Aimetti et al. 2009; Crespi
et al. 2009; Casado et al. 2010; Oghli & Ste-
veling 2010) elevated buccal and lingual mu-
coperiosteal flaps to perform the tooth
extraction and achieved primary closure,
except two studies that did not aim for pri-
mary closure (Iasella et al. 2003; Serino et al.
2003; Serino et al. 2008) (Table 1). Flapless
extraction of the teeth was performed in four
studies (Hoad-Reddick et al. 1994; Aimetti
et al. 2009; Crespi et al. 2009; Oghli & Ste-
veling 2010) with two studies aiming to pri-
mary closure through a soft tissue autograft
(Crespi et al. 2009; Oghli & Steveling 2010).
Four studies reported on the socket status
after the extraction, with two studies report-
ing full integrity of the socket walls (Barone
et al. 2008) or minimum buccal bone loss
(Froum et al. 2002) (<2 mm), whereas two
studies (Fiorellini et al. 2005; Crespi et al.
2009) reported the absence of the buccal bone
wall.
Different biomaterials were used in the
test groups of the studies included in the
review. Test treatment could be either graft
alone (Hoad-Reddick et al. 1994; Lekovic
et al. 1997; Lekovic et al. 1998; Bolouri et al.
2001; Froum et al. 2002; Iasella et al. 2003;
Fiorellini et al. 2005; Barone et al. 2008; Ai-
metti et al. 2009; Crespi et al. 2009; Casado
et al. 2010; Oghli & Steveling 2010) or mem-
brane alone (Lekovic et al. 1997; Lekovic
et al. 1998; Casado et al. 2010), a combina-
tion of both (Iasella et al. 2003; Barone et al.
2008; Casado et al. 2010) or a combination of
graft and autogenous soft tissue graft (Crespi
et al. 2009 and Oghli & Steveling 2010).
Methods of measurement
The changes in the primary outcomes were
assessed by clinical and radiographical
examinations, as well as, by evaluation of
cast models. Hoad-Reddick et al. (1994), Fio-
rellini et al. (2005) and Crespi et al. (2009)
used radiographs (orto-pantomography, CT
scans, and periapical X-rays respectively).
Lekovic et al. (1998), Lekovic et al. (1997),
Serino et al. (2003), Barone et al. (2008), Se-
rino et al. (2008) and Aimetti et al. (2009)
assessed directly the bone changes at a re-
entry surgery. Within this group, four stud-
ies (Serino et al. 2003; Serino et al. 2008;
Barone et al. 2008; Aimetti et al. 2009) used
an acrylic stent to allow for reproducible
measurements, whereas two studies (Leko-
vic et al. 1997; Lekovic et al. 1998) utilized
titanium pins (Table 1). Two studies used
clinical measurements combined with
acrylic stents (Iasella et al. 2003; Casado
et al. 2010), whereas other two (Lekovic
et al. 1997; Oghli & Steveling 2010)
used cast models to evaluate the
dimensional changes between baseline and
the end of the investigation. The most fre-
quent method was the mid-buccal measure-
ment.
Quality assessment
Data from the quality assessment are
reported in Table 2. All studies except one
randomized controlled trial (Barone et al.
2008) and two controlled trials (Serino et al.
2003; Serino et al. 2008) were considered to
have a high risk of bias.
Study outcomes. Descriptive analyses of thechanges in the hard tissue dimensions
Table 3a depicts the differences in the bone
crest height between baseline and the end of
the investigations reported for test and con-
trol groups. Eleven of 14 studies evaluated
the changes in the height of the bone crest
comparing the socket preservation therapy
with sockets left to heal spontaneously
(Hoad-Reddick et al. 1994; Lekovic et al.
1997; Lekovic et al. 1998; Iasella et al. 2003;
Barone et al. 2008; Aimetti et al. 2009; Cres-
pi et al. 2009). Overall, the control groups
demonstrated a mean vertical bone loss that
ranged from !0.3 to !3.75 mm, whereas in
the test groups, results were more heteroge-
neous demonstrating mean vertical bone
changes ranging from !2.48 to 1.3 mm.
Differences between test and control
groups, as reported by the authors, were
statistically significant in four studies
included in the systematic review (Lekovic
et al. 1997; Lekovic et al. 1998; Iasella et al.
2003; Fiorellini et al. 2005). Lekovic et al.
(1997) evaluated the ridge bone dimensional
changes at re-entry using titanium pins
after GBR with e-PTFE membranes covering
the socket walls in submerged healing or
an untreated socket control. The same
research group used a similar experimental
design to assess GBR with a biabsorbable
membrane (Lekovic et al. 1998). Results
from both studies demonstrated statistically
significant differences (P < 0.0005) in favour
of the GBR approach demonstrating a
greater vertical resorption in the control
group.
Table 2. Quality assessment of the articles included
Quality criteria
# Author (year)
Adequatesequencegeneration?
Allocationconcealment? Blinding?
Incompleteoutcome dataaddressed?
Free ofselectivereporting?
Free ofotherbias?
Risk ofbias
1 Hoad-Reddick et al. (1994) c c 0 c a a High2 Lekovic et al. (1997) c c 0 a a a High3 Lekovic et al. (1998) a c 1 a a a High4 Bolouri et al. (2001) b c 1 c a a High5 Froum et al. (2002) c a 1 c a a High6 Serino et al. (2003) b b b a a a Moderate7 Iasella et al. (2003) b c 0 c a a High8 Fiorellini et al. (2005) b b 2 a a a High9 Barone et al. (2008) a c 1 a a a Moderate10 Serino et al. (2008) b b b a a a Moderate11 Aimetti et al. (2009) b c 1 c a a High12 Crespi et al. (2009) b c 1 c a a High13 Casado et al. (2010) c c 0 c a a High14 Oghli & Steveling (2010) b c 0 a a a High
Abbreviations of the interventions: a: adequate explanation in the text; b: inadequate explanation in the text; c: not listed; 0: not blinded; 1: single-blinded;2: double-blinded.
28 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

Iasella et al. (2003) with a similar design,
although evaluating the bone dimensional
changes at re-entry using an acrylic stent,
assessed the efficacy of filling the sockets
with freeze-dried bone allografts + tetracy-
cline and a collagen membrane in semi-sub-
merged healing. Differences with the
untreated control group were statistically
significant for the mid-buccal as well as
mesial and distal locations (P < 0.05), but not
for the mid-lingual locations.
Fiorellini et al. (2005) evaluated the ridge
height changes after therapy by computed
tomography reporting statistically significant
differences (P = 0.007) when comparing the
use of an absorbable collagen sponge (ACS)
soaked with 1.50 mg/ml rhBMP-2 with the
untreated control group.
Table 3b depicts the differences in the
width of the bone crest between baseline
and the end of the evaluation period
reported for test and control groups in eight
of the 14 studies (Lekovic et al. 1997; Leko-
vic et al. 1998; Iasella et al. 2003; Fiorellini
et al. 2005; Barone et al. 2008; Aimetti et al.
2009; Casado et al. 2010; Oghli & Steveling
2010). Overall, the control groups demon-
strated a mean horizontal bone loss that
ranged from !0.16 to !4.50 mm, whereas in
the test groups, results were more homoge-
neous demonstrating mean horizontal bone
changes ranging from 3.25 to !2.50 mm.
The differences between test and control
groups were statistically significant in five
studies.
Changes in soft tissue dimensions
Mean dimensional changes of soft tissues are
presented in Table 4. Two studies evaluated
the dimensional changes of the overall alveo-
lar ridge contour combining the changes of
hard and soft tissues (Lekovic et al. 1997; Og-
hli & Steveling 2010). Whereas Iasella et al.
(2003) evaluated the changes in gingival
thickness at different locations of the crest,
Lekovic et al. (1997) measured these changes
on cast models, both reporting significantly
less vertical and horizontal resorption in the
test group (P = 0.001). Oghli & Steveling
(2010), however, could not demonstrate dif-
ferences between using a collagen sponge
with/without gentamicine plus a circular soft
tissue graft to protect the wound, with the
untreated control socket (P = 0.07). Iasella
et al. (2003) also evaluated the gingival thick-
ness with an ultrasonic device at buccal and
lingual/palatal locations. Differences between
the ridge preservation therapy and the
untreated control were only statistically sig-
nificant for buccal sites.
Implant-related outcomes
Table 5 shows the studies with reported out-
comes on implant placement after tooth
extraction (Hoad-Reddick et al. 1994; Bolouri
et al. 2001; Froum et al. 2002; Iasella et al.
2003; Serino et al. 2003; Fiorellini et al. 2005;
Serino et al. 2008; Crespi et al. 2009; Aimetti
et al. 2009; Casado et al. 2010). Two studies
(Barone et al. 2008; Aimetti et al. 2009)
reported the placement of implants after 3
and >7 months without providing any details
on further soft or hard tissues augmentation
procedures. Two studies (Serino et al. 2003;
Serino et al. 2008) reported the placement of
dental implants after 6 and 3 months of heal-
ing respectively, specifying that all implants
achieved good primary stability in both test
and control groups. In one study (Fiorellini
et al. 2005), implants were inserted after
4 months of healing and statistically signifi-
cant differences were reported in favour of
the test group 1 (ACS+ 1.50 mg/ml rhBMP-2)
when compared to test group 2 (ACS+
0.75 mg/ml rhBMP-2) and the control treat-
ment, in regards to the number of secondary
augmentation surgeries needed, although no
further details were provided in regards to
the number and type of these procedures. In
the test 1 sites, 56.25% demonstrated ade-
quate bone volume for implant placement,
whereas the corresponding figures in test 2
and control groups were 25% and 12.5%
respectively.
Histological outcomes
Nine studies evaluated histologically, the
type of bone healing after 3 to >7 months
from the tooth extraction. Biopsies were
taken using a trephine before the osteotomy
preparation for implants insertion. Serial
decalcified sections were analysed under light
microscopy for qualitative and quantitative
histo-morphometrical analysis. Fiorellini
et al. (2005) and Casado et al. (2010) provided
descriptive histological observations, whereas
Froum et al. (2002), Barone et al. (2008), Seri-
no et al. (2008), Aimetti et al. (2009) and
Crespi et al. (2009) calculated fractions of
bone mineral, connective tissue and residual
graft material at different apico-coronal levels
of the socket. Serino et al. (2003) described
the fraction of bone mineral, whereas Iasella
et al. (2003) evaluated fractions of cellular/
acellular and trabecular bone.
Meta-analysis
Nine of the 14 included studies reported sim-
ilar comparisons and could be grouped in the
meta-analyses (Figs 2 and 3). The primary
outcome variables, defined as bone dimen-
sional changes (height and width of alveolar
process) were analysed and compared
between the test (socket preservation ther-
apy) and control group (spontaneous socket
healing). None of the other secondary out-
come variables could be grouped in meta-
analysis.
Seven studies were grouped in the meta-
analysis for bone height as the outcome vari-
able (Fig. 2). Two studies Fiorellini et al.
(2005), Crespi et al. (2009) evaluated two dif-
ferent preservation procedures, consequently,
each test socket preservation procedure vs.
the control group was considered as an inde-
pendent study in the meta-analysis. As there
was a high heterogeneity among the studies
(I2 = 95.2%; Tau2 = 0.639; v2 P-value <0.001),
we selected the random effect model for the
statistical evaluation. A statistically signifi-
cant greater reduction in bone height for con-
trol groups was demonstrated when
compared to the test groups (WMD =
!1.47 mm; 95% CI [!1.982, !0.953]; P
< 0.001; heterogeneity: I2 = 13.1%; v2 P-
value = 0.314). Due to this high heterogene-
ity, several subgroup analyses were performed
based on the surgical protocol used for the
socket preservation (flapless/flapped, barrier
membrane/no membrane, primary intention
healing/no primary healing) and on the mea-
surement method utilized to evaluate the
morphological changes.
None of the subgroup analyses achieved a
non-significant heterogeneity value. A ten-
dency towards greater weighted mean differ-
ences in favour of the test groups was
observed with flapless surgical protocol, no
membrane, primary intention healing and
with use of X-rays as measurement method
(Table 6). The meta-regression analysis failed
to encounter statistically significant differ-
ences among subgroups (data not shown).
Seven studies were grouped in the meta-
analysis on bone width as outcome variable
(Fig. 3). In two studies, more than one test
group were evaluated in comparison with the
control, and therefore they were considered
as independent (Serino et al. 2008; Oghli &
Steveling 2010). Also one study presented
data measured with two different outcome
measurements (cast models and re-entry sur-
gery) and they were also included indepen-
dently in the analyses (Lekovic et al. 1997).
As there was a high heterogeneity detected
among studies (I2 = 99.0%; Tau2 = 2.997; v2
P-value <0.001), the random effect model was
selected for the analysis. The results showed
a statistically significant greater reduction in
bone width for control groups when
compared to the socket preservation thera-
© 2011 John Wiley & Sons A/S 29 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

Table
3a.Outcomevariables:
changesin
boneheight,
expressedasmean(m
m)
Publication(#)
Verticalch
angesofthealveolarcrest
Interventions/groups
Measurement
method
Surgicalco
nsiderations
Control
Test
Diff.
P-value
Hoad-Reddick
etal.(1994)(1)
Test:Hyd
roxyapatite
granules
Control:No
socketfilling
Lateral
cephalographsand
dental
pantomograms
Flapless
Primary
closure:NO
Typ
eofsocket:
NA
2.42
0.65
ND:1.77
NA
Lekovicetal.
(1997);_1
(2)
Test:ePTFE
®membrane
Control:No
socketfilling
Reentrysurgery
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!1.2
!0.5
Mb:!0.7
0.001
Lekovicetal.
(1998)(3)
Test:membraneofglyco
lideandlactide
polimers
Control:Nosocketfilling
Reentrysurgery
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!1.5
!0.38
Mb:!1.12
<0.0005
Serinoetal.(2003)(6)
Test:Sp
ongeofpolylactide–p
olyglyco
lide
acid
Control:Nosocketfilling
Reentrysurgery
+stent
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!0.8
1.3
Mb:!2.1
NA
Iasellaetal.(2003)(7)
Test:FD
BA
+tetracycline+co
llagen
mombrane
Control:Nosocketfilling
Clinical+stent
Flap
Primary
closure:NO
Typ
eof
socket:
NA
!0.9
1.3
Mb:!2.2
<0.05
Fiorellinietal.
(2005)_1(8)
Test
1:0.75mg/m
lrhBMP/ACS
Control:
Nosocketfilling
CTscan
Flap
Primary
closure:YES
Typ
eof
socket:
3-w
all(nobuccalwall)
!1.17
!0.62
ND:!0.55
NS
Fiorellinietal.
(2005)_2(8)
Test
2:1.50mg/m
lrhBMP/ACS
Control:
Nosocketfilling
CTscan
Flap
Primary
closure:YES
Typ
eof
socket:
3-w
all(nobuccalwall)
!1.17
!0.02
ND:!1.15
0.007
Baroneetal.(2008)
(9)
Test:Corticocancellousporcinebone+
collagenmembrane
Control:Nosocket
filling
Reentry+stent
Flap
Primary
closure:YES
Typ
eof
socket:
4-w
all
!3.6
!0.7
Mb:!2.9
NA
Baroneetal.(2008)
(9)
Test:Corticocancellousporcinebone+
collagenmembrane
Control:Nosocket
filling
Reentry+stent
Flap
Primary
closure:YES
Typ
eof
socket:
4-w
all
!3.6
!0.7
Mb:!2.9
NA
Aim
ettietal.(2009)
(11)
Test:Medical-gradecalcium
sulphate
hemihyd
rate
Control:Nosocketfilling
Reentry+stent
Flapless
Primary
closure:NO
Typ
eofsocket:
NA
!1.2
!0.5
Mb:!0.7
NA
Crespietal.(2009)_1
(12)
Test
1:Magnesium-enrich
ed
hyd
roxyapatite
Control:Nosocketfilling
PeriapicalX-rays
Flapless
Primary
closure:YES
(tissuegraft)
Typ
eofsocket:
3-w
all(nobuccalwall)
!3.75
!0.48
ND:!3.27
NA
Crespietal.(2009)_2
(12)
Test
2:Calcium
sulphate
Control:No
socketfilling
PeriapicalX-rays
Flapless
Primary
closure:YES
(tissuegraft)
Typ
eofsocket:
3-w
all(nobuccalwall)
!3.75
!2.48
ND:!1.27
NA
Abbreviationsoftheinterventions:
P-valuesofthestatisticalanalysisoftheintergroupdifferencesin
thech
angesbetw
eenbaselineandendofthestudy.
SDofthemeansoftheintergroupdifferences
inthech
angesbetw
eenbaselineandendofthestudy.
NS,
notstatisticallysignificant;
NA,data
notava
ilable;Mb,midbuccal;ND,notdefinedsite;ACS,
absorbable
collagensponge;RhBMP,reco
mbi-
nanthumanBMP-2;e-PTFE
,exp
andedpolytetrafluoroethylene;FD
BA,freeze
-driedboneallograft.
30 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

Table
3b.Outcomevariables:
changesin
bonewidth,expressedasmean(m
m)
Publication(#)
Horizo
ntalch
angesofthealveolarcrest
Interventions/groups
Measurement
method
Surgicalco
nsiderations
Control
Test
Diff.
P-value
Lekovicetal.(1997)_2
(2)
Test:ePTFE
®membrane
Control:No
socketfilling
Reentrysurgery
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!4.4
!1.8
!2.6
0.002
Lekovicetal.(1998)
(3)
Test:membraneofglyco
lideandlactide
polimers
Control:Nosocketfilling
Reentrysurgery
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!4.56
!1.31
!3.25
<0.00001
Iasellaetal.(2003)(7)
Test:FD
BA
+tetracycline+co
llagen
mombrane
Control:Nosocketfilling
Clinical+stent
Flap
Primary
closure:NO
Typ
eof
socket:
NA
!2.6
!1.2
!1.4
<0.05
Fiorellinietal.
(2005)_1(8)
Test
1:0.75mg/m
lrhBMP/ACS
Control:
Nosocketfilling
CTscan
Flap
Primary
closure:YES
Typ
eof
socket:
3-w
all(nobuccalwall)
0.57
1.76
!1.19
NS
Fiorellinietal.
(2005)_2(8)
Test
2:1.50mg/m
lrhBMP/ACS
Control:
Nosocketfilling
CTscan
Flap
Primary
closure:YES
Typ
eof
socket:
3-w
all(nobuccalwall)
0.57
3.27
!2.7
0.000
Baroneetal.(2008)
(9)
Test:Corticocancellousporcinebone+
collagenmembrane
Control:Nosocket
filling
Reentry+stent
Flap
Primary
closure:YES
Typ
eof
socket:
4-w
all
!4.5
!2.5
!2
NA
Aim
ettietal.(2009)
(11)
Test:Medical-gradecalcium
sulphate
hemihyd
rate
Control:Nosocketfilling
Reentry+stent
Flapless
Primary
closure:NO
Typ
eofsocket:
NA
!3.2
!2
!1.2
NA
Casadoetal.(2010)_1
(13)
Test
1:bovineBMP+bOM
Control:No
socketfilling
Clinical+stent
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!0.16
3.05
!3.21
NA
Casadoetal.(2010)_2
(13)
Test
2:bovineBMP+b
OM+resorbable
membrane
Control:Nosocketfilling
Clinical+stent
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!0.16
2.42
!2.58
NA
Casadoetal.(2010)_3
(13)
Test
3:resorbable
membrane
Control:No
socketfilling
Clinical+stent
Flap
Primary
closure:YES
Typ
eof
socket:
NA
!0.16
2.9
!3.06
NA
Oghli&
Steve
ling
(2010)_1(14)
Test
1:Autogenoussoft
tissuegraft
+co
llagenplug2
Control:Nosocketfilling
Cast
Flapless
Primary
closure:YES
(soft
tissuegraft)
Typ
eofsocket:
NA
!0.3
!0.8
0.5
0.001
Oghli&
Steve
ling
(2010)_2(14)
Test
2:Autogenoussoft
tissuegraft
+co
llagenmatrix
withgentamicin
Control:
Nosocketfilling
Cast
Flapless
Primary
closure:YES
(soft
tissuegraft)
Typ
eofsocket:
NA
!0.3
!0.1
!0.2
0.07
Abbreviationsoftheinterventions:
P-valuesofthestatisticalanalysisoftheintergroup
differencesin
thech
angesbetw
eenbaselineandendofthestudy.
NS,
notstatisticallysignificant;
NA,data
not
ava
ilable;bOM,bovineorganic
matrix.
© 2011 John Wiley & Sons A/S 31 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

pies (WMD = !1.830 mm; 95% CI [!2.947,
!0.732]; P = 0.001; heterogeneity: I2 = 0%; v2
P-value = 0.837). Due to the high heterogene-
ity initially detected among the studies, sev-
eral subgroup analyses were performed. None
of the subgroup analyses achieved a non-sig-
nificant heterogeneity value for all groups. A
tendency towards greater weighted mean dif-
ferences in favour of test groups was observed
with the use of membranes, a flapped surgi-
cal protocol, primary intention healing and
with CT as outcome measurement (Table 7).
The meta-regression analyses demonstrated a
statistically significant difference only in the
flapless/flapped subgroup (meta-regression;
slope = 2.26; 95% CI [1.01; 3.51]; P = 0.003).
Publication bias and sensitivity analyses
No publication bias was detected for changes
in bone height (P = 0.352; Egger’s test), nor in
bone width (P = 0.357; Egger’s test). The sen-
sitivity analysis to assess the effect of indi-
vidual studies on the summary estimates of
the meta-analysis showed that the exclusion
of single studies did not substantially alter
any estimates. In terms of bone height
changes, the greater change in WMD could
be attributed to Crespi et al. (2009)
(!23.25%) (Table 8). In regards to bone
width, the sensitivity analyses identified
three potential studies as responsible for
most of the heterogeneity (Fiorellini et al.
[2005] [!10.49%], Lekovic et al. [1998]
[!11.46%] and Oghli & Steveling [2010]
[15.15% and 10.79%]) (Table 9).
Discussion
Socket preservation therapies have been pro-
posed with the aim of maintaining the hard
and soft tissue dimensions of the alveolar
ridge that are partially lost after tooth extrac-
tion as part of the natural physiological heal-
ing process. This objective is particularly
pursued in preparation for dental implant
installation to have the best bone avail-
ability for successful implant prosthesis
(Tarnow & Eskow 1996). Unfortunately,
there are very few well-designed clinical
studies evaluating the efficacy of these thera-
peutic procedures and the potential benefit of
the different techniques/materials used is
still debatable.
The present systematic review seeks to
provide scientific evidence on the existing
RCTs and CTs evaluating different surgical
protocols aimed for preserving the bone of
the alveolar ridge after tooth extraction. The
primary outcome variables selected were the
vertical and horizontal hard and soft tissue
dimensional changes of the bone crest at
least 3 months after the tooth extraction.
Overall, the results from the meta-analysis
demonstrated statistically significant higher
alveolar bone crest preservation in both
height and width in the test groups (interven-
tions for ridge preservation) when compared
with the healing of the untreated control
socket. In regards to the changes in bone
height, the overall WMD difference between
test and control groups amounted to
1.47 mm. Hence, the results from the meta-
analysis suggest that the use of socket preser-
vation therapies limits the dimensional
changes (vertical and horizontal) of the alveo-
lar ridge after tooth extraction. These data
are in agreement with a recent similar sys-
tematic review also assessing the influence
and potential benefit of socket preservation
procedures after tooth extraction in non-
molar regions of the mouth (Ten Heggeler
et al. 2010). These authors concluded, how-
ever, that although a benefit of such tech-
niques could be observed, vertical and
horizontal bone loss can be expected.
These results must be evaluated with cau-
tion as the quality assessment of the selected
studies demonstrated that all but two studies
(Barone et al. 2008; Serino et al. 2008) had a
high potential risk of bias. Furthermore, the
use of different biomaterials and surgical
techniques has been combined in this meta-
analysis, as well as the use of different types
of sockets (single/multiple, position in the
mouth and number of residual bony walls),
different reason of tooth extraction and differ-
ent methods of evaluation. This lack of con-
Table 4. Outcome variables. Soft tissue changes
Publication (#)
Soft tissue changes
Interventions/groupsMeasurementmethod Surgical considerations Control Test Diff. P-value
Lekovic et al.(1997)_1 (2)
Test: ePTFE®
membrane Control:No socket filling
Cast Flap; primary closure: YES Type ofsocket: NA Verticalmeasurements
!1 !0.2 Mb: !0.8 0.001
Flap; Primary closure: YES Type ofsocket: NA Horizontalmeasurements
!4.2 !1.8 !2.4 0.001
Iasella et al.(2003) (7)
Test: FDBA+ tetracycline+ collagenmombrane Control:No socket filling
Ultrasonic metre Flap Primary closure: NO Type ofsocket: NA
0.4 !0.1 0.5 <0.05
Oghli & Steveling(2010)_1 (14)
Test 1: Autogenoussoft tissue graft +collagen plug2Control: No socketfilling
Cast Flapless Primary closure: YES(soft tissue graft) Type of socket:NA Horizontal measurements
!0.3 !0.8 0.5 0.001
Oghli & Steveling(2010)_2 (14)
Test 2: Autogenoussoft tissue graft +
collagen matrix withgentamicin
Control: No socketfilling
Cast Flapless Primary closure: YES(soft tissue graft) Type of socket:NA Horizontal measurements
!0.3 !0.1 !0.2 0.07
P-values of the statistical analysis of the intergroup differences in the changes between baseline and end of the study.
32 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

Table
5.Im
plant-relatedoutcomes
Publication
Implant-relatedoutcomes
Interventions/groups
Implant
placement
Tim
eafter
extraction
Control
Test
Seco
ndary
augmentation
surgery
Histology
Restoration
Hoad-Reddicketal.
(1994)(1)
Test:Hyd
roxyapatite
granules
Control:No
socketfilling
No
––
––
No
NA
Bolouri
etal.(2001)
(4)
Test:BioplantHTR
Control:Nosocket
filling
No
––
––
No
NA
Froum
etal.(2002)(5)
Test
1:Bioactiveglass
Test
2:DFD
BA
Control:Nosocketfilling
No
––
––
Yes
NA
Serinoetal.(2003)(6)
Test:Sp
ongeofpolylactide–p
olyglyco
lide
acid
Control:Nosocketfilling
Yes
6months
Allsites
Allsites
NA
Yes
NA
Iasellaetal.(2003)(7)
Test:FD
BA
+tetracycline+co
llagen
mombrane
Control:Nosocketfilling
Yes
4–6
months
––
–Yes
NA
Fiorellinietal.(2005)
_1(8)
Test
1:0.75mg/m
lrhBMP/ACS
Control:
Nosocketfilling
Yes
4months
Yes
12.5%
adequate
bonevo
lume
Yes
25%
adequate
bonevo
lume
10
Yes
NA
Fiorellinietal.(2005)
_2(8)
Test
2:1.50mg/m
lrhBMP/ACS
Control:
Nosocketfilling
Yes
4months
Yes
12.5%
adequate
bonevo
lume
Yes56.25%
adequate
bone
volume
3P<0.05
test
1vs.test
2andco
ntrol(11)
NA
Baroneetal.(2008)
(9)
Test:Corticocancellousporcinebone+
collagenmembrane
Control:Nosocket
filling
Yes
>7months
NA
NA
NA
Yes
NA
Serinoetal.(2008)
(10)
Test:Sp
ongeofpolylactide–p
olyglyco
lide
acid
Control:Nosocketfilling
Yes
3months
Allsites
Allsites
NA
Yes
NA
Aim
ettietal.(2009)
(11)
Test:Medical-gradecalcium
sulphate
hemihyd
rate
Control:Nosocketfilling
Yes
3months
NA
NA
NA
Yes
NA
Crespietal.(2009)
(12)
Test
1:Magnesium-enrich
ed
hyd
roxyapatite
Test
2:Calcium
sulphate
Control:Nosocketfilling
Yes
3months
––
Yes
NA
Casadoetal.(2010)
(13)
Test
1:bovineBMP+bOM
Test
2:
bovineBMP+bOM
+resorbable
membrane
Test
3:resorbable
membrane
Control:Nosocketfilling
No
––
––
Yes
NA
Abbreviationsoftheinterventions:
NA,data
notava
ilable;RCT,randomized
clinicaltrial;ACS,
absorbable
collagensponge;e-PTFE
,exp
anded
polytetrafluoroethylene;BMP,bonemorphogeneticpro-
tein;bOM,bovineorganic
matrix;CTscan,co
mputerize
dtomographyscanner;
RhBMP,reco
mbinanthuman
BMP-2;FD
BA,freeze
-dried
boneallograft;DFD
BA,demineralize
dfreeze
-dried
boneallo-
graft.
© 2011 John Wiley & Sons A/S 33 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

sistency and standardization, in spite of the
lack of publication bias, may have contrib-
uted to the high heterogeneity of the results.
In fact, in terms of vertical bone height
changes, 23.25% of this effect was attributed
to the study by Crespi et al. (2009) utilizing
magnesium-enriched hydroxyapatite com-
bined with the closing of the socket with a
soft tissue autograft. This individual study,
Fig. 2. Meta-analysis: changes in bone height.
Fig. 3. Meta-analysis: changes in bone width.
34 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

reporting mean differences between test and
control groups of 3.27 mm, however, only
selected sockets without full integrity of
their bone walls, usually lacking the buccal
cortical bone. This negative prognostic factor
for bone regeneration during undisturbed
socket healing may in part, have contributed
to the bigger effect of the socket preservation
therapy, compared with the other studies
included in the meta-analysis. Likewise, in
regards to the changes in bone width, three
studies provided the bigger heterogeneity in
the meta-analysis, contributing to 15.15%,
11.46% and 10.49% of the overall change
respectively (Lekovic et al. 1998; Fiorellini
et al. 2005; Oghli & Steveling 2010). In par-
ticular, on the negative effect side, Oghli &
Steveling (2010) that utilized a collagen
sponge as socket filler reported a higher bone
horizontal resorption in the test group. Apart
from the null efficacy of the filler used, the
fact that cast models were used to measure
these horizontal changes may have prevented
an accurate evaluation of the true dimen-
sions of the alveolar crest. In contrast, Fiorel-
lini et al. (2005) observed a difference of
3.85 mm in bone width when comparing the
use of 1.50 mg/ml rhBMP/ACS vs. the con-
trol socket.
The factors that may have contributed to
the obtained outcomes may be categorized
as: (1) the clinical conditions of the socket
site, i.e. integrity/non-integrity of the socket
bone walls, dimension and presence/absence
of adjacent teeth; (2) the surgical protocol uti-
lized, i.e. flapped/flapless surgery or primary
flap closure/secondary intention healing; (3)
the biomaterial used, i.e. membrane/no
membrane, type of graft material and (4) the
type of evaluation method utilized. In an
attempt to assess the influence of each of
these factors, a subgroup analysis was per-
formed, as well as meta-regression. The sub-
group analysis of flapped/flapless surgery
demonstrated a minor influence in the verti-
cal resorption process, although it showed a
significant difference in favour of the flapped
group in regards to the ridge horizontal
dimensional changes. When comparing the
relative efficacy of using barrier membranes
and/or grafts, while the use of membranes
alone reported more vertical bone change
than the use of grafts alone, membranes
obtained better results than grafts (either
alone or the combination of membrane and
graft) in terms of horizontal bone changes.
The subgroup analysis to assess the influence
of flap closure demonstrated a slight ten-
dency towards less bone loss in the horizon-
tal direction when the sockets healed by
Table 6. Meta-analyses by subgroups for changes in bone height
WMD 95% CI P-value I-squared
Membrane(a) No !1.511 !2.583; !0.440 0.006 95.2%(b) Yes !1.192 !1.589; !0.834 0.000 87.9%Flap(a) No !1.756 !3.400; !0.112 0.036 97.6%(b)Yes !1.179 !1.516; !0.842 0.000 81.7%Primary closure(a) No !1.293 !2.730; 0.145 0.078 72.4%*
(b) Yes !1.506 !2.077; !0.935 0.000 96.1%Outcome variable(a) Reentry + stent !1.861 !3.606; !0.386 0.013 89.3%(b) X-rays !2.276 !4.236; !0.316 0.023 97.9%(c) CT !0.866 !1.453; !0.279 0.004 14.5%(d) Clinical (stent) !2.200 !3.649; !0.751 0.003 NA(e) Cast !0.800 !1.039; !0.561 0.000 NA(f) Reentry surgery !0.912 !1.324; !0.501 0.000 90.6
NA, not applicable, as only one study was included in the subgroup.*Non-statistically significant differences.
Table 7. Meta-analyses by subgroups for changes in bone width
WMD 95% CI P-value I-squared
Membrane(a) No !0.982 !1.738; !0.227 0.011 93.3%(b) Yes !2.465 !3.074; !1.856 0.000 86.6%Flap(a) No !0.148 !0.788; 0.492 0.650 92.6%(b)Yes !2.563 !3.101; !2.795 0.000 81.2%Primary closure(a) No !1.263 !2.049; !0.478 0.002 0%(b) Yes !1.968 !3.217; !0.732 0.002 99.2%Outcome variable(a) Reentry + stent !1.682 !2.449; !0.914 0.000 47.0%*
(b) CT !3.026 !4.501; !1.551 0.000 52.3%*
(c) Clinical (stent) !1.400 !2.797; !0.003 0.050 NA(d) Cast !0.682 !1.841; 0.476 0.248 98.4%(e) Reentry surgery !2.986 !3.612; !2.361 0.000 76.2%
CT, computerized tomography; NA, not applicable, as only one study was included in the subgroup.*Non-statistically significant differences.
Table 8. Sensitivity analyses of the outcome variable bone heigth changes made with randomeffect model
Random estimation
WMD change (%)
Heterogeneity
Study omitted WMD 95% CI I-squared (%) P-value
Aimetti (2009) !1.55 !2.10; !1.00 5.70 12.44 0.328Barone (2008) !1.34 !1.86; !0.82 !8.70 4.85 0.396Crespi_1 (2009) !1.13 !1.41; !0.84 !23.25 49.25 0.038Crespi_2 (2009) !1.49 !2.05; !0.93 1.69 16.14 0.295Fiorellini_1 (2005) !1.55 !2.10; !1.01 5.93 12.6 0.327Fiorellini_2 (2005) !1.50 !2.05; !0.95 2.18 19.07 0.268Iasella (2003) !1.42 !1.95; !0.89 !3.07 18.87 0.269Lekovic_1 (1997) !1.55 !2.15; !0.96 5.83 0 0.447Lekovic_2 (1997) !1.57 !2.17; !0.96 6.69 0 0.465Lekovic (1998) !1.52 !2.19; !0.86 3.89 0 0.561Serino (2003) !1.42 !1.95; !0.89 !3.27 19.07 0.268None !1.47 !1.98; !0.95 0 13.71 0.314
Crespi_1: Magnesium-enriched hydroxyapatite vs. no socket filling.Crespi_2: Calcium sulphate vs. no socket filling.Fiorellini_1: 0.75 mg/ml rhBMP/ACS vs. no socket filling.Fiorellini_2: 1.5 mg/ml rhBMP/ACS vs. no socket filling.Lekovic_1: outcome measured in cast model.Lekovic_2: outcome measured in reentry surgery.
© 2011 John Wiley & Sons A/S 35 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

primary intention. In terms of the evaluation
methods used, only the radiographic evalua-
tion demonstrated significant vertical (X-
ray) and horizontal (CT) changes when com-
paring test and control groups. The use of
cast models and re-entry procedures was not
able to demonstrate such significant differ-
ences.
The results of the meta-regression analysis
showed that the surgical procedure (flapped/
flapless) was the most important factor influ-
encing the results. Flapped surgical proce-
dures demonstrated a significantly lesser
horizontal resorption of the socket, when
compared to flapless surgeries (meta-regres-
sion; slope = 2.26; 95% CI [1.01; 3.51];
P = 0.003). These results may be due to the
importance of achieving full closure and first
intention healing, mainly when the socket is
filled with a biomaterial or covered with a
barrier membrane. The effect of raising a flap
on the healing process of the socket after
tooth extraction is still controversial with
results from experimental models reporting
less pronounced bone remodelling of the
alveolar ridge after tooth extraction with a
flapless approach (Fickl et al. 2008a, 2008b)
or when using socket preservation procedures
(Fickl et al. 2008a, 2008b; Blanco et al. 2010)
and when placing implants immediately after
the tooth extraction (Blanco et al. 2010).
Other studies with a similar experimental
design, however, have failed to encounter sig-
nificant bone dimensional differences
between flapped and flapless tooth extrac-
tions (Araujo & Lindhe 2009).
The changes in the horizontal dimension
have been the ones benefited most by the
socket preservation techniques evaluated in
this systematic review. Precisely bone loss in
a horizontal dimension is the most important
consequence of tooth extraction during the
first 3–6 months of healing (Schropp et al.
2003). In this meta-analysis, the bone hori-
zontal changes in the control group were het-
erogeneous, ranging from !0.16 to
!4.50 mm. These differences may be due to
different factors, such as the socket location
and the thickness of the socket walls. Recent
studies in humans have shown the influence
of the location and the thickness of the
socket walls in the ensuing modelling and
remodelling processes after tooth extraction
(Ferrus et al. 2010; Januario et al. 2011).
One major limitation of this systematic
review is that no meta-analyses could be per-
formed on implant-related outcomes, due to
the lack of sufficient data. This fact is impor-
tant as there is no clear evidence that the
occurrence of bone resorption after tooth
extraction may significantly limit the place-
ment of dental implants. In fact, one study
(Serino et al. 2008) reported that implants
could be placed in all patients independently
of the group of treatment. The positive influ-
ence of the socket preservation therapy may
be attributed more to achieving enhanced
restorative and aesthetic outcomes, as well
as better maintenance of healthy peri-
implant soft tissues. These possible influ-
ences were not evaluated in the reviewed
studies. Only one study assessed the possible
influence of the socket preservation therapy
on the need of further augmentation thera-
pies and in fact, the test group reported
reduced needs of bone augmentation (Fiorel-
lini et al. 2005).
In conclusion, the results from this sys-
tematic review and meta-analysis have
shown that although some degree of bone
modelling and remodelling will occur after
tooth extraction, different ridge preservation
procedures resulted in significantly less verti-
cal and horizontal contraction of the alveolar
bone crest. The obtained results, however,
could not indicate which is the type of surgi-
cal procedure or biomaterial most suitable
for this clinical indication, although the use
of barrier membranes, a flap surgical proce-
dure and full flap closure demonstrated bet-
ter results. There are limited data, however,
on the possible influence of these therapies
on the long-term outcomes of implant ther-
apy.
References
Aimetti, M., Romano, F., Griga, F.B. & Godio, L.
(2009) Clinical and histologic healing of human
extraction sockets filled with calcium sulfate The
International Journal of Oral & Maxillofacial
Implants 24: 902–909.
Amler, M.H., Johnson, P.L. & Salman, I. (1960) His-
tological and histochemical investigation of
human alveolar socket healing in undisturbed
extraction wounds. Journal of the American Den-
tal Association 61: 32–44.
Araujo, M.G. & Lindhe, J. (2005) Dimensional ridge
alterations following tooth extraction: an experi-
mental study in the dog. Journal of Clinical Peri-
odontology 32: 212–218.
Araujo, M., Linder, E., Wennstrom, J. & Lindhe, J.
(2008) The influence of Bio-Oss Collagen on heal-
ing of an extraction socket: an experimental
study in the dog. The International journal
of periodontics & restorative dentistry 28: 123–
135.
Araujo, M.G. & Lindhe, J. (2009) Ridge alterations
following tooth extraction with and without flap
elevation: an experimental study in the dog. Clin-
ical oral implants research 20: 545–549.
Araujo, M.G. & Lindhe, J. (2011) Socket grafting
with the use of autologous bone: an experimental
study in the dog. Clinical oral implants research
22: 9–13.
Artzi, Z., Tal, H. & Dayan, D. (2000) Porous bovine
bone mineral in healing of human extraction
sockets. Part 1: Histomorphometric evaluations
at 9 months. Journal of Periodontology 71: 1015–
1023.
Barone, A., Aldini, N.N., Fini, M., Giardino, R.,
Calvo Guirado, J.L. & Covani, U. (2008) Xenograft
versus extraction alone for ridge preservation
Table 9. Sensitivity analyses of the outcome variable bone width made with random effect model
Random estimationWMDchange (%)
Heterogeneity
Study omitted WMD 95% CI I-squared (%) P-value
Aimetti (2009) !1.91 !3.09; !0.73 3.84 0 0.785Barone (2008) !1.82 !3.01; !0.63 !0.94 0 0.780Fiorellini_1 (2005) !1.79 !2.96; !0.62 !2.71 0 0.773Fiorellini_2 (2005) !1.65 !2.80; !0.49 !10.49 0 0.875Iasella (2003) !1.88 !3.05; !0.72 !2.41 0 0.772Lekovic_1 (1997) !1.77 !2.97; !0.58 !3.47 0 0.797Lekovic_2 (1997) !1.75 !2.93; !0.57 !4.73 0 0.792Lekovic (1998) !1.63 !2.46; !0.80 !11.46 0 0.381Oghli_1 (2010) !2.12 !3.35; !0.88 15.15 0 0.953Oghli_2 (2010) !2.04 !3.31; 0.77 10.79 0 0.903None !1.84 !2.95; !0.73 0 0 0.837
WMD, weighted mean differences; CI, confidence interval.Fiorellini_1: 0.75 mg/ml rhBMP/ACS vs. no socket filling.Fiorellini_2: 1.5 mg/ml rhBMP/ACS vs. no socket filling.Lekovic_1: outcome measured in cast model.Lekovic_2: outcome measured in reentry surgery.Oghli_1: autogenous soft tissue graft + collagen plug vs. no socket filling.Oghli_2: autogenous soft tissue graft + collagen matriz with gentamicin vs. no socket filling.
36 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

after tooth removal: a clinical and histomorpho-
metric study Journal of Periodontology 79: 1370–
1377.
Becker, W., Dahlin, C., Lekholm, U., Bergstrom,
C., van Steenberghe, D., Higuchi, K. & Becker, B.
E. (1999) Five-year evaluation of implants placed
at extraction and with dehiscences and fenestra-
tion defects augmented with eptfe membranes:
results from a prospective multicenter study.
Clinical Implant Dentistry & Related Research
1: 27–32.
Blanco, J., Alves, C.C., Nunez, V., Aracil, L.,
Munoz, F. & Ramos, I. (2010) Biological width
following immediate implant placement in the
dog: Flap vs. Flapless surgery. Clinical Oral
Implants Research 21: 624–631.
Block, M.S. & Jackson, W.C. (2006) Techniques for
grafting the extraction site in preparation for dental
implant placement. Atlas of the Oral and Maxillo-
facial Surgery Clinics of North America 14: 1–25.
Bolouri, A., Haghighat, N. & Frederiksen, N. (2001)
Evaluation of the effect of immediate grafting of
mandibular postextraction sockets with synthetic
bone Compendium of Continuing Education in
Dentistry (Jamesburg, N.J.: 1995) 22: 955–958,
960, 962 passim; quiz 966.
Camargo, P.M., Lekovic, V., Weinlaender, M., Klok-
kevold, P.R., Kenney, E.B., Dimitrijevic, B.,
Nedic, M., Jancovic, S. & Orsini, M. (2000) Influ-
ence of bioactive glass on changes in alveolar pro-
cess dimensions after exodontia. Oral Surgery,
Oral Medicine, Oral Pathology, Oral Radiology
and Endodontics 90: 581–586.
Cardaropoli, G., Araujo, M. & Lindhe, J. (2003)
Dynamics of bone tissue formation in tooth
extraction sites. An experimental study in dogs.
Journal of Clinical Periodontology 30: 809–818.
Carmagnola, D., Adriaens, P. & Berglundh, T.
(2003) Healing of human extraction sockets filled
with bio-oss. Clinical Oral Implants Research
14: 137–143.
Casado, P.L., Duarte, M.E., Carvalho, W., Esmer-
aldo da Silva, L. & Barboza, E.P. (2010) Ridge
bone maintenance in human after extraction.
Implant Dentistry 19: 314–322.
Crespi, R., CapparE, P. & Gherlone, E. (2009) Mag-
nesium-enriched hydroxyapatite compared to cal-
cium sulfate in the healing of human extraction
sockets: radiographic and histomorphometric
evaluation at 3 months. Journal of Periodontol-
ogy 80: 210–218.
Devlin, H., Hoyland, J., Newall, J.F. & Ayad, S.
(1997) Trabecular bone formation in the healing
of the rodent molar tooth extraction socket. Jour-
nal of Bone and Mineral Research 12: 2061–2067.
Devlin, H. & Sloan, P. (2002) Early bone healing
events in the human extraction socket. The Inter-
national Journal of Oral and Maxillofacial Sur-
gery 31: 641–645.
Esposito, M., Coulthard, P., Worthington, H.V. &
Jokstad, A. (2001) Quality assessment of rando-
mized controlled trials of oral implants. The
International Journal of Oral & Maxillofacial
Implants 16: 783–792.
Evian, C.I., Rosenberg, E.S., Coslet, J.G. & Corn, H.
(1982) The osteogenic activity of bone removed
from healing extraction sockets in humans. Jour-
nal of Periodontology 53: 81–85.
Ferrus, J., Cecchinato, D., Pjetursson, E.B., Lang, N.
P., Sanz, M. & Lindhe, J. (2010) Factors influenc-
ing ridge alterations following immediate implant
placement into extraction sockets. Clinical Oral
Implants Research 21: 22–29.
Fickl, S., Zuhr, O., Wachtel, H., Bolz, W. & Huerz-
eler, M. (2008a) Tissue alterations after tooth
extraction with and without surgical trauma: a
volumetric study in the beagle dog. Journal of
Clinical Periodontology 35: 356–363.
Fickl, S., Zuhr, O., Wachtel, H., Stappert, C.F.,
Stein, J.M. & Hurzeler, M.B. (2008b) Dimensional
changes of the alveolar ridge contour after differ-
ent socket preservation techniques. Journal of
Clinical Periodontology 35: 906–913.
Fiorellini, J.P., Howell, T.H., Cochran, D., Malm-
quist, J., Lilly, L.C., Spagnoli, D., Toljanic, J.,
Jones, A. & Nevins, M. (2005) Randomized study
evaluating recombinant human bone morphoge-
netic protein-2 for extraction socket augmenta-
tion. Journal of Periodontology 76: 605–613.
Froum, S., Cho, S.C., Rosenberg, E., Rohrer, M. &
Tarnow, D. (2002) Histological comparison of
healing extraction sockets implanted with bioac-
tive glass or demineralized freeze-dried bone allo-
graft: a pilot study. Journal of Periodontology 73:
94–102.
Higgins, J.P., Thompson, S.G., Deeks, J.J. &
Altman, D.G. (2003) Measuring inconsistency in
meta-analyses. BMJ 327: 557–560.
Higgins, J.P.T. & Green, S. (eds) Cochrane Hand-
book for Systematic Reviews of Interventions
Version 5.1.0 [updated March 2011]. The
Cochrane Collaboration, 2011. Available from
www.cochrane-handbook.org (accessed on 31
May 2010).
Hoad-Reddick, G., Grant, A.A. & McCord, J.F.
(1994) Osseoretention? Comparative assessment
of particulate hydroxyapatite inserted beneath
immediate dentures. The European Journal of
Prosthodontics and Restorative Dentistry 3: 61–
65.
Iasella, J.M., Greenwell, H., Miller, R.L., Hill, M.,
Drisko, C., Bohra, A.A. & Scheetz, J.P. (2003)
Ridge preservation with freeze-dried bone allo-
graft and a collagen membrane compared to
extraction alone for implant site development: a
clinical and histologic study in humans. Journal
of Periodontology 74: 990–999.
Januario, A.L., Duarte, W.R., Barriviera, M., Mesti,
J.C., Araujo, M.G. & Lindhe, J. (2011) Dimension
of the facial bone wall in the anterior maxilla: a
cone-beam computed tomography study. Clinical
Oral Implants Research 22: 1168–1171.
Johnson, K. (1969) A study of the dimensional
changes occurring in the maxilla following tooth
extraction. Australian Dental Journal 14: 241–
244.
van Kesteren, C.J., Schoolfield, J., West, J. & Oates,
T. (2010) A prospective randomized clinical study
of changes in soft tissue position following
immediate and delayed implant placement. The
International Journal of Oral & Maxillofacial
Implants 25: 562–570.
von Elm, E., Altman, D.G., Egger, M., Pocock, S.J.,
Gotzsche, P.C. & Vandenbroucke, J.P. (2007) The
strengthening the reporting of observational stu-
dies in epidemiology (strobe) statement: guide-
lines for reporting observational studies. Lancet
370: 1453–1457.
Kuboki, Y., Hashimoto, F. & Ishibashi, K. (1988)
Time-dependent changes of collagen crosslinks in
the socket after tooth extraction in rabbits. Jour-
nal of Dental Research 67: 944–948.
Lekovic, V., Camargo, P.M., Klokkevold, P.R.,
Weinlaender, M., Kenney, E.B., Dimitrijevic, B.
& Nedic, M. (1998) Preservation of alveolar
bone in extraction sockets using bioabsorbable
membranes. Journal of Periodontology 69: 1044–
1049.
Lekovic, V., Kenney, E.B., Weinlaender, M., Han,
T., Klokkevold, P., Nedic, M. & Orsini, M. (1997)
A bone regenerative approach to alveolar ridge
maintenance following tooth extraction. Report
of 10 cases. Journal of Periodontology 68: 563–
570.
Needleman, I.G. (2002) A guide to systematic
reviews. Journal of clinical periodontology 29:
[Suppl. 3]: 6–9; discussion 37–38.
Norton, M.R., Odell, E.W., Thompson, I.D. &
Cook, R.J. (2003) Efficacy of bovine bone mineral
for alveolar augmentation: a human histologic
study. Clinical Oral Implants Research 14: 775–
783.
Oghli, A.A. & Steveling, H. (2010) Ridge preserva-
tion following tooth extraction: a comparison
between atraumatic extraction and socket seal
surgery. Quintessence International 41: 605–
609.
Paolantonio, M., Dolci, M., Scarano, A., d’Archivio,
D., di Placido, G., Tumini, V. & Piattelli, A.
(2001) Immediate implantation in fresh extraction
sockets: A controlled clinical and histological
study in man. J Periodontol 72: 1560–1571.
Pietrokovski, J. & Massler, M. (1967) Alveolar ridge
resorption following tooth extraction. Journal of
Prosthetic Dentistry 17: 21–27.
Schulz, K.F., Altman, D.G. & Moher, D. (2010)
Consort 2010 statement: updated guidelines for
reporting parallel group randomized trials. Obste-
trics and Gynecology 115: 1063–1070.
Schropp, L., Wenzel, A., Kostopoulos, L. & Karring,
T. (2003) Bone healing and soft tissue contour
changes following single-tooth extraction: a clini-
cal and radiographic 12-month prospective study.
The International Journal of Periodontics &
Restorative Dentistry 23: 313–323.
Serino, G., Biancu, S., Iezzi, G. & Piattelli, A.
(2003) Ridge preservation following tooth extrac-
tion using a polylactide and polyglycolide sponge
as space filler: a clinical and histological study in
humans. Clinical Oral Implants Research 14:
651–658.
Serino, G., Rao, W., Iezzi, G. & Piattelli, A. (2008)
Polylactide and polyglycolide sponge used in
human extraction sockets: bone formation fol-
lowing 3 months after its application. Clinical
Oral Implants Research 19: 26–31.
Stroup, D.F., Berlin, J.A., Morton, S.C., Olkin, I.,
Williamson, G.D., Rennie, D., Moher, D., Becker,
B.J., Sipe, T.A. & Thacker, S.B. (2000) Meta-analy-
sis of observational studies in epidemiology: a
proposal for reporting. Meta-analysis of observa-
tional studies in epidemiology (moose) group.
Journal of the American Medical Association.
283: 2008–2012.
© 2011 John Wiley & Sons A/S 37 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38
Vignoletti et al "Ridge preservation after tooth extraction

Tarnow, D.P. & Eskow, R.N. (1996) Preservation of
implant esthetics: soft tissue and restorative con-
siderations. Journal of Esthetic Dentistry 8: 12
–19.
Ten Heggeler, J.M., Slot, D.E. & Van der Weijden,
G.A. (2010) Effect of socket preservation therapies
following tooth extraction in non-molar regions
in humans: a systematic review. Clinical Oral
Implants Research 22: 779–788.
Tobıas, A. (2008) Preferred reporting items for sys-
tematic reviews and meta-analyses: the prisma
statement. Stata Techical Bulletin 47: 15–17.
Trombelli, L., Farina, R., Marzola, A., Bozzi, L., Lil-
jenberg, B. & Lindhe, J. (2008) Modeling and
remodeling of human extraction sockets. Journal
of Clinical Periodontology 35: 630–639.
Yilmaz, S., Efeoglu, E.& Kilic, A.R. (1998) Alveolar
ridge reconstruction and/or preservation using
root form bioglass cones. Journal of Clinical Peri-
odontology 25: 832–839.
38 | Clin. Oral Impl. Res. 23(Suppl. 5), 2012/22–38 © 2011 John Wiley & Sons A/S
Vignoletti et al "Ridge preservation after tooth extraction

I Workshop BQDC Octubre 2013
Protocolo de Preservación del Alveolo José Nart e Ignacio Sanz
El proceso alveolar es una estructura dependiente de los dientes que se
desarrolla durante la erupción dental. El volumen y la forma del proceso
alveolar están determinados por la forma del diente, su eje de erupción
e inclinación (Schroeder et al. 1986).
La pérdida dental conlleva una pérdida de volumen en sentido
horizontal y vertical resultando en un reborde alveolar más estrecho y
más corto. Debido a que la cicatrización natural está asociada a una
pérdida de volumen de hasta el 50% durante el primer año, las técnicas
de preservación alveolar tienen como objetivo minimizar los cambios
volumétricos que se producen en los procesos alveolares con la
utilización de materiales de relleno óseo (van der Weijden et al. 2009).
El objetivo de esta revisión es conocer los resultados clínicos de la
técnica de preservación alveolar, las distintas variantes de la técnica
quirúrgica, los materiales de relleno óseo que podemos utilizar y crear un
árbol de decisiones que nos facilite la toma decisiones en la clínica para
conseguir los mejores resultados para nuestros pacientes en función de
la literatura disponible.
CICATRIZACIÓN ALVEOLAR
El primer paso cuando aparece una técnica es conocer las mejoras que
puede aportar al protocolo que se considera estándar. Es por ello que
debemos conocer los cambios dimensionales que se producen cuando
extraemos un diente y dejamos cicatrizar el alveolo por si mismo.
• Cambios en sentido vertical: Los estudios con reentrada en
humanos han mostrado que se produce una pérdida vertical del
11 al 22% a los 6 meses de la extracción de un diente. Si lo
miramos en valores absolutos, esta pérdida es de 1,24 mm de

I Workshop BQDC Octubre 2013
media.
• Cambios en sentido horizontal: Los estudios con reentrada en
humanos han mostrado que se produce una pérdida horizontal
del 29 al 63%. En valores absolutos, la pérdida media es de 3.8
mm.
Si tenemos en cuenta que la mayor pérdida se produce en los primeros
3 meses y ésta continúa hasta los 6 meses, es importante conocer si
disponemos de alguna terapia que pueda contrarrestar estos cambios
volumétricos o, a lo sumo, limitarlos.
PRESERVACION ALVEOLAR La técnica de preservación del alveolo consiste en rellenar el alveolo
que queda tras la extracción de un diente con algún tipo de injerto
óseo, tratando de disminuir la pérdida del hueso alveolar. Al tratarse de
una técnica que se sale de lo que podríamos considerar como el
estándar, es importante revisar los siguientes puntos: eficacia clínica en
cuanto reducción de la pérdida tridimensional del hueso, indicaciones y
contraindicaciones, variantes de la técnica, resultados histológicos y
beneficios que pueden obtener nuestros pacientes.
1. Preservación de alveolo Vs. Extracción convencional
La reabsorción de la cresta que se produce al extraer un diente puede
limitarse con la técnica de preservación alveolar, pero no se puede
prevenir al 100%.
De 7 estudios, 5 han demostrado una menor reabsorción
estadísticamente significativa en sentido horizontal y 6 de 8 estudios lo
han demostrado estos resultados positivos para la reabsorción en
sentido vertical.
Para valorar el beneficio clínico en términos absolutos, disponemos de
varias revisiones sistemáticas que han evaluado a nivel global en cuánto
podemos reducir la pérdida ósea que se produce tras la extracción al
preserval el alveolo. En los meta-ánalisis de la revisión sistemática de
Vignoletti et al. 2012, la preservación de alveolo reduce de manera

I Workshop BQDC Octubre 2013
significativa los cambios en los volúmenes óseos en sentido horizontal
(1.83 mm) y en sentido vertical (1.47 mm) en comparación a no realizar
la preservación tras la extracción. En otra revisión sistemática más
reciente (Orgeas et al. 2013) se mostró como la técnica de preservación
de alveolo es efectiva en reducir la reabsorción de hueso en sentido
horizontal (2.9mm) y vertical (0.9mm).
De estas revisiones podemos sacar además otras conclusiones, cómo
que la pérdida de hueso no sólo va a depender de la técnica
quirúrgica, sino también de la anatomía del alveolo. De este modo, se
ha demostrado que si las paredes óseas del alveolo son gruesas, se
reducen los cambios tridimensionales tras la extracción, sobre todo a
nivel de la tabla vestibular. Si tenemos en cuenta que la mayor parte de
las tablas vestibulares van a ser menores a 1 mm (Ferrus et al. 2010),
puede ser importante aplicar esta técnica en sectores estéticos para
limitar los cambios de volumen y, con ello, los problemas estéticos que
pueden acontecer tras la extracción.
2. Indicaciones y contraindicaciones
Indicaciones:
(i) Cuando los implantes inmediatos o tempranos no están
recomendados.
(ii) Cuando los pacientes no están disponibles para recibir un implante
inmediato o temprano (embarazo, vacaciones,…).
(iii) Cuando no se puede conseguir estabilidad primaria del implante
inmediato.
(iv) En pacientes adolescentes.
(v) Contorneado de la cresta para el tratamiento protésico
convencional.
(vi) El ratio coste/beneficio es positivo.
(vii) Reducción de la necesidad de realizar elevación del seno maxilar.

I Workshop BQDC Octubre 2013
Contraindicación:
(i) Infecciones intralveolares que no se pueden controlar/eliminar.
(ii) Cuando el coste-beneficion para el paciente no sea justificable.
3. Técnica quirúrgica
Se ha demostrado que el uso de implantes dentales tras la extracción
de un diente no previene la reabsorción tridimensional de la cresta que
se produce cuando tras la exodoncia. Es por ello que hay que valorar
muy bien las indicaciones de los implantes inmediatos a la extracción.
Debido a esto, la preservación de la cresta alveolar puede suponer una
opción terapéutica alternativa a los implantes inmediatos en pacientes
con un alto riesgo de problemas estéticos.
Se han propuesto distintas modalidades quirúrgicas y distintos materiales
para rellenar el alveolo, entre las que destacan las siguientes:
(i) Cirugía sin elevación de colgajo, relleno del alveolo con algún
injerto óseo (hueso autólogo, hidroxiapatita enriquecida con
magnesio, matriz de hueso humano
desmineralizado/mineralizado y el mineral de hueso bovino
desproteinizado) y cierre del alveolo con injerto de tejido
blando autólogo (injerto libre de encía tipo punch o injerto de
tejido conectivo en sobre) o xenoinjerto (matriz de colágeno).
La indicación principal de esta técnica es para alveolos
íntegros que mantienen la totalidad de la tabla vestibular.
(ii) Cirugía sin elevación de colgajo, relleno del alveolo con algún
injerto óseo (hueso autólogo, hidroxiapatita enriquecida con
magnesio, matriz de hueso humano
desmineralizado/mineralizado y el mineral de hueso bovino
desproteinizado) y cierre del alveolo con una membrana
reabsorbible o no reabsorbibles. A esta técnica se le podría
añadir un injerto de tejido blando para proteger los materiales
de regeneración. De nuevo, la indicación principal de esta
técnica es para alveolos con una tabla vestibular íntegra.

I Workshop BQDC Octubre 2013
(iii) Cirugía con elevación de colgajo, relleno del alveolo con
algún injerto óseo (hueso autólogo, hidroxiapatita enriquecida
con magnesio, matriz de hueso humano
desmineralizado/mineralizado y el mineral de hueso bovino
desproteinizado), membrana barrera reabsorbibles o no
reabsorbibles para proteger al injerto y cierre con colgajos
desplazados o con un injerto de tejido blando adicional. La
indicación principal de esta técnica es alveolos que han
perdido parcialmente alguna de las tablas vestibular o
palatina.
En cuanto a la revisión de la literatura, el uso de sustitutos óseos
(hidroxiapatita enriquecida con magnesio, la matriz de hueso humano
desmineralizado/mineralizado y el mineral de hueso bovino
desproteinizado) junto a una membrana de colágeno ha mostrado ser
efectivo en minimizar los cambios volumétricos de la cresta que se
producen al extraer un diente y el uso únicamente de membranas
barrera mejora la cicatrización del alveolo.
Por otro lado se ha demostrado que obtenemos una mayor ganancia
ósea significativa en sentido horizontal cuando elevamos un colgajo y
colocamos una membrana barrera, lo que supone un mayor trauma
quirúrgico para el paciente y un mayor gasto económico, por lo que
hay que valorar muy bien el coste-beneficio de esta técnica.
Y en cuanto al papel del cierre por primera intención del alveolo, se ha
mostrado que el cubrir por completo el alveolo y el material de injerto
tienen un efecto limitado en la reducción de la reabsorción
tridimensional del hueso. Además, los injertos de tejido blando junto al
material de injerto no han mostrado ser factores claves para mejorar los
resultados de la técnica de preservación de alveolo.
Hoy por hoy, con la evidencia científica disponible, no podemos afirmar
que un injerto óseo en particular o una técnica quirúrgica concreta

I Workshop BQDC Octubre 2013
sean superiores, por lo que resulta difícil establecer guías clínicas
concretas para la preservación de alveolo. No obstante, en un
apartado posterior proponemos un árbol de toma de decisiones que
nos puede ayudar a optimizar los resultados de la preservación y a
elegir las mejores indicaciones posibles.
4. Histología
A nivel histológico se han mostrado distintos grados de formación de
hueso. Lo más característico es que con algunos injertos se interfieren en
la cicatrización del alveolo y del hueso, retardándolas.
De 8 estudios analizados, 6 han demostrado que en el grupo de
preservación de alveolo hay mayor formación de hueso trabecular,
aunque con técnica, no siempre se promueve la formación de nuevo
hueso.
Además, el uso de xenoinjertos solo sirven como un andamio
(osteoconducción) y no estimulan la formación de nuevo hueso.
5. Beneficios
Cuando nosotros realizamos una técnica adicional al tratamiento
convencional (implante en cresta cicatrizada), lo que esperamos es no
sólo que se facilite la colocación del implante y que necesitemos una
menor regeneración ósea, si no que los resultados a largo plazo sean
mejores. Sin embargo, no disponemos de literatura que demuestre que
la preservación del alveolo mejore los resultados a largo plazo de los
implantes en comparación a los implantes inmediatos o a los colocados
en cresta cicatrizada.
Cabe destacar que de 4 estudios, 3 han demostrado que en el grupo
de preservación de alveolo se ha necesitado menos aumento óseo en
el momento de colocar los implantes.

I Workshop BQDC Octubre 2013
Workshop BQDC Octubre 2013

I Workshop BQDC Octubre 2013
PROTOCOLO QUIRÚRGICO
INSTRUCCIONES POST-OPERATORIAS Farmacoterapia: Hoy en día no tenemos evidencia de que los antibióticos sistémicos sean necesarios en la técnica de preservación de alveolo. En función del tipo de biomateriales que empleemos, podemos considerar dar las siguientes pautas:
- Amoxicilina 500mg. 1 comprimido/8 horas. 8 días. - Ibuprofeno 600 mg. 1 comprimido / 6-8 horas. 3-4 primeros días.
Alérgicos - Azitromicina 500 mg. 1compr / 24h. 3 días - Paracetamol 500mg. 1 compr/6-8 horas. 3-4 primeros días.
Instrucciones de higiene oral:
- Colutorio clorhexidina 0,2% o 0,12% durante 30 seg. 2 veces/día 14 días post-tratamiento.
- No cepillado en la zona durante 14 días. Tras dicho periodo, el cepillado será suave y progresivamente el paciente realizará su higiene con normalidad.