A quantitative comparison of handwriting in children with high-functioning autism and attention...
9
A quantitative comparison of handwriting in children with high-functioning autism and attention deficit hyperactivity disorder Beth P. Johnson a, *, Nicole Papadopoulos b , Joanne Fielding a , Bruce Tonge a , James G. Phillips a , Nicole J. Rinehart b a School of Psychology and Psychiatry, Monash University, Wellington Road, Clayton, Victoria, Australia b School of Psychology, Deakin University, 221 Burwood Highway, Burwood, Victoria, Australia 1. Introduction Autism and attention deficit hyperactivity disorder-combined type (ADHD-CT) are highly prevalent childhood disorders associated with atypical development and behavior. Autism is defined in the Diagnostic and statistical manual of mental disorders, 5th edition by communication deficits, impaired social interactions and stereotyped or repetitive behaviors (American Psychiatric Association, 2013). Attention deficit hyperactivity disorder (ADHD) is clinically defined by symptoms of hyperactivity, inattention or impulsivity (American Psychiatric Association, 2013). The release of DSM- 5 in 2013 has included many highly anticipated changes to diagnostic criteria for neurodevelopmental disorders, including allowing a dual diagnosis of ASD and ADHD. The change in diagnostic criteria will present new opportunities as well as challenges for understanding similarities and differences between autism and ADHD. While motor abnormalities are increasingly being recognized as a key part of the clinical picture of children diagnosed with neurodevelopmental disorders, there is a lack of research directly focused on comparing the motor profile of autism and ADHD. Handwriting is a skill that requires complex coordination of both motor and cognitive abilities, such as planning, Research in Autism Spectrum Disorders 7 (2013) 1638–1646 A R T I C L E I N F O Article history: Received 28 July 2013 Accepted 9 September 2013 Keywords: Handwriting Fine motor Dysgraphia Autism Attention deficit hyperactivity disorder A B S T R A C T Children with high-functioning autism (HFA) and attention deficit hyperactivity disorder (ADHD) often experience significant handwriting difficulties, which can hamper their academic progress and ability to express themselves through symbols and words. Handwriting of children with HFA was compared to those with ADHD based on performance on the speed subtest of the Handwriting Performance Test. Differences in handwriting speed, size and alignment of words, and proportion of handwriting errors, such as corrections and substitutions, were assessed between groups. Results indicated distinct profiles of handwriting problems in HFA and ADHD: children with HFA demonstrated poorer spatial arrangement of words and reduced handwriting speed, and those with ADHD made more handwriting errors, such as corrections and transpositions. These findings have important implications in understanding the similarities and differences for children with HFA and ADHD and lay the groundwork for effective intervention strategies. ß 2013 Elsevier Ltd. All rights reserved. * Corresponding author at: School of Psychology and Psychiatry, Building 17, Monash University, Wellington Road, Victoria 3800, Australia. Tel.: +61 3 99054040. E-mail address: [email protected] (B.P. Johnson). Contents lists available at ScienceDirect Research in Autism Spectrum Disorders Jo u rn al h om ep ag e: h ttp ://ees .elsevier .co m /RASD/d efau lt.as p 1750-9467/$ – see front matter ß 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.rasd.2013.09.008
Transcript of A quantitative comparison of handwriting in children with high-functioning autism and attention...

Research in Autism Spectrum Disorders 7 (2013) 1638–1646
Contents lists available at ScienceDirect
Research in Autism Spectrum Disorders
Jo u rn al h om ep ag e: h t tp : / /ees .e lsev ier . co m /RASD/d efau l t .as p
A quantitative comparison of handwriting in children
with high-functioning autism and attention deficithyperactivity disorderBeth P. Johnson a,*, Nicole Papadopoulos b, Joanne Fielding a,Bruce Tonge a, James G. Phillips a, Nicole J. Rinehart b
a School of Psychology and Psychiatry, Monash University, Wellington Road, Clayton, Victoria, Australiab School of Psychology, Deakin University, 221 Burwood Highway, Burwood, Victoria, Australia
A R T I C L E I N F O
Article history:
Received 28 July 2013
Accepted 9 September 2013
Keywords:
Handwriting
Fine motor
Dysgraphia
Autism
Attention deficit hyperactivity disorder
A B S T R A C T
Children with high-functioning autism (HFA) and attention deficit hyperactivity disorder
(ADHD) often experience significant handwriting difficulties, which can hamper their
academic progress and ability to express themselves through symbols and words.
Handwriting of children with HFA was compared to those with ADHD based on
performance on the speed subtest of the Handwriting Performance Test. Differences in
handwriting speed, size and alignment of words, and proportion of handwriting errors,
such as corrections and substitutions, were assessed between groups. Results indicated
distinct profiles of handwriting problems in HFA and ADHD: children with HFA
demonstrated poorer spatial arrangement of words and reduced handwriting speed,
and those with ADHD made more handwriting errors, such as corrections and
transpositions. These findings have important implications in understanding the
similarities and differences for children with HFA and ADHD and lay the groundwork
for effective intervention strategies.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
Autism and attention deficit hyperactivity disorder-combined type (ADHD-CT) are highly prevalent childhooddisorders associated with atypical development and behavior. Autism is defined in the Diagnostic and statistical manual
of mental disorders, 5th edition by communication deficits, impaired social interactions and stereotyped or repetitivebehaviors (American Psychiatric Association, 2013). Attention deficit hyperactivity disorder (ADHD) is clinically definedby symptoms of hyperactivity, inattention or impulsivity (American Psychiatric Association, 2013). The release of DSM-5 in 2013 has included many highly anticipated changes to diagnostic criteria for neurodevelopmental disorders,including allowing a dual diagnosis of ASD and ADHD. The change in diagnostic criteria will present new opportunitiesas well as challenges for understanding similarities and differences between autism and ADHD. While motorabnormalities are increasingly being recognized as a key part of the clinical picture of children diagnosed withneurodevelopmental disorders, there is a lack of research directly focused on comparing the motor profile of autism andADHD. Handwriting is a skill that requires complex coordination of both motor and cognitive abilities, such as planning,
* Corresponding author at: School of Psychology and Psychiatry, Building 17, Monash University, Wellington Road, Victoria 3800, Australia.
Tel.: +61 3 99054040.
E-mail address: [email protected] (B.P. Johnson).
1750-9467/$ – see front matter � 2013 Elsevier Ltd. All rights reserved.
http://dx.doi.org/10.1016/j.rasd.2013.09.008

B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–1646 1639
working memory, language and visual perception (Cartmill, Roger, & Ziviani, 2009). Consequently, handwritingdifficulties are among the most salient problems for both children with autism and ADHD in the classroom environment(Adi-Japha et al., 2007; Cartmill et al., 2009; Racine, Majnemer, Shevell, & Snider, 2008). A study conducted inQueensland, Australia, found that children with ASDs accounted for 40% of occupational therapists’ case loads, and that86% of those with 20 consecutive referrals required assistance with fine motor or handwriting difficulties (Cartmill et al.,2009). With respect to ADHD, a USA-based study found that 70% of children with ADHD had impairments in writtenexpression, which manifested as illegible handwriting, poor letter formation and poor written composition relative tooral expression skills; these deficits were two times more common than difficulties in reading, or mathematics (Mayes,Calhoun, & Crowell, 2000). Despite the clear clinical need to develop effective, targeted intervention strategies forhandwriting difficulties in autism and ADHD, we do not yet fully understand the similarities and differences common toeach of these disorders. Furthermore, it is necessary to compare and contrast the handwriting impairments in autismand ADHD to help further inform diagnosis, offer insights into functional impairments, and develop appropriateinterventions.
Handwriting problems have largely been evaluated independently in autism and ADHD; only two studies have directlycompared handwriting or fine motor control in HFA and ADHD (Booth, Charlton, Hughes, & Happe, 2003; Mayes & Calhoun,2007). Mayes and Calhoun (2007) directly compared graphomotor abilities between the two groups using theDevelopmental Test of Visual-Motor Integration (VMI) and the coding subtest of the WISC-III. This study revealed that58% of children with ADHD, and 50% of children with autism had dysgraphia, and both groups performed significantly morepoorly on both VMI and coding scores compared to typically developing children. Booth et al. (2003) found qualitativedifferences in graphomotor performance between children with ADHD and autism using a drawing and planning task. It wasfound that boys with HFA (IQ > 80) tended toward a piecemeal, detail-focused drawing style that resulted in difficultyexecuting correct spatial arrangement of the picture elements; however, both HFA and ADHD showed planning deficits(Booth et al., 2003).
Of the few studies that have characterized handwriting impairments in children with autism alone, the commonlyreported problems relate to overall legibility and poor letter formation (Cartmill et al., 2009; Fuentes, Mostofsky, & Bastian,2009; Kushki, Chau, & Anagnostou, 2011), and difficulty maintaining consistent size (Cartmill et al., 2009; Hellinckx, Roeyers,& Van Waelvelde, 2013). Macrographia (atypically large handwriting) has been observed in both children (Hellinckx et al.,2013; Johnson et al., 2013) and adults with ASD (Beversdorf et al., 2001). With respect to handwriting speed, reports areconflicting: Hellinckx et al. (2013) found slower handwriting in children with ASD, whereas Cartmill et al. (2009) found nosignificant difference. Hellinckx et al. (2013) also reported that spatial alignment was significantly poorer in the ASD group.The relationship between IQ, motor skills and handwriting performance in ASD is also unclear. Fuentes et al. (2009) foundmotor skills but not age or FSIQ were predictors of handwriting performance in children with ASD aged 8–13 (Fuentes et al.,2009), however, in children with ASD aged 12–14, perceptual reasoning index (PRI) but not motor skills predictedhandwriting performance (Fuentes, Mostofsky, & Bastian, 2010). Hellinckx et al. (2013) found age, gender, and visual-motorintegration were significant predictors of handwriting quality; while age, reading abilities, and fine motor coordination werepredictors of handwriting speed (Hellinckx et al., 2013).
With respect to handwriting difficulties in children with ADHD, problems with illegibility and greater proportion ofwritten errors have been identified (Adi-Japha et al., 2007; Racine et al., 2008; Re, Caeran, & Cornoldi, 2008; Tsai, Meng, Hung,Chen, & Lu, 2011). The higher incidence of writing errors in children with ADHD, such as letter transpositions, substitutionsand corrections, has been found in English (Re et al., 2008), Hebrew (Adi-Japha et al., 2007) and Chinese written languages(Tsai et al., 2011). Adi-Japha et al. (2007) suggested that spelling problems in children with ADHD occur irrespective ofvocabulary and reading ability (VIQ), and instead result from impaired motor processes. Macrographia and difficultymaintaining consistent handwriting size has also been reported in children with ADHD (Frings et al., 2010; Langmaid,Papadopoulos, Johnson, Phillips, & Rinehart, 2012). Reports on handwriting speed are inconsistent: children with ADHDwrite individual letters faster (Adi-Japha et al., 2007; Langmaid et al., 2012; Tucha, Mecklinger, Walitza, & Lange, 2006), butoverall writing speed in ADHD has been found to be slower (Mayes & Calhoun, 2007; Shen, Lee, & Chen, 2012) or no differentto typically developing groups (Flapper, Houwen, & Shoemaker, 2006; Racine et al., 2008).
Although both children with autism and ADHD experience handwriting difficulties, to date no study has directlycontrasted the types of handwriting difficulties in these groups. Therefore the focus of the present research was to examinewhether there are any commonalities or differences in handwriting impairments characteristic to HFA or ADHD andexamine predictive factors of handwriting performance in these groups. We used a simple handwriting task, the speedsubtest of the Handwriting Performance Test, to assess (1) spatial arrangement of words (handwriting size and spacing,consistency of size and spacing), (2) handwriting errors, such as corrections and letter substitutions and (3) handwritingspeed. With respect to handwriting speed, it was hypothesized that children with autism would write significantly moreslowly than ADHD or TD children. We predicted that both children with HFA and ADHD would show larger handwriting(Beversdorf et al., 2001; Frings et al., 2010; Johnson et al., 2013) but that HFA group would show reduced spacing betweenwords. Regarding handwriting errors (poor formation, corrections and letter substitutions), we expected to see worseperformance in the ADHD group, and that the proportion of errors would relate to overall handwriting speed. We alsoexamined the contribution of age, verbal comprehension, perceptual reasoning and motor coordination to handwritingdifficulties in HFA, ADHD and TD groups to determine the extent to which perceptual, cognitive or motoric elementscontribute to handwriting deficits.

B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–16461640
2. Method
2.1. Participants
Forty-nine boys aged between 7 and 14 years participated in the study: 14 with HFA, 14 with ADHD-combined type(ADHD-CT), and 21 typically developing (TD) boys. Ethical approval was obtained from Monash University and SouthernHealth Human Research Ethics Committees. Parents of participants provided informed consent prior to the commencementof the study, and written assent was provided by the participants in accordance with the Declaration of Helsinki.
Boys with HFA were recruited from private pediatricians in Melbourne, Victoria and the Autism Victoria database.Reports from pediatricians were reviewed to ensure that all children were diagnosed according to Diagnostic and statistical
manual of mental disorders–4th edition, revised (DSM-IV-TR; American Psychiatric Association, 2000) criteria for autisticdisorder. Further diagnostic information was gathered using the Social Responsiveness Scale (SRS), Developmental BehaviorChecklist-parent version (DBC-P), structured parent interviews, direct child observations and information from teachers andother therapists involved in the assessment process. The DBC-P has good psychometric properties, includes five subscales(disruptive/antisocial, self-absorbed, communication disturbance, anxiety and social relating) (Brereton, Tonge, Mackinnon,& Einfeld, 2002; Witwer & Lecavalier, 2007). Participants were excluded if they were suffering from any co-morbidneurological (e.g. tuberous sclerosis), hearing or visual impairment, genetic (e.g., Fragile X syndrome) or otherneuropsychiatric diagnosis (e.g. Tourette’s syndrome). As there was no discrepancy between pediatrician’s diagnosisand parental report and questionnaires administered, no participants were excluded from the study. No children in the HFAgroup were reported to have been taking medication.
Boys diagnosed with ADHD-CT were recruited from private pediatricians in Melbourne. These children fulfilled DSM-IV-TRcriteria for ADHD-CT, with diagnosis confirmed in a two-stage process. Firstly, pediatricians were asked to refer clients with adiagnosis of ADHD-CT with no other co-morbid diagnoses. Exclusion criteria included elevated social-communicationdisturbances in the clinical opinion of the referring pediatrician, co-morbid medical (e.g. tuberous sclerosis), hearing or visualimpairment, movement (e.g. developmental coordination disorder), psychiatric (e.g. Tourette’s syndrome), or genetic (e.g.fragile X syndrome) disorders other than the primary diagnosis of ADHD-CT. Secondly, a doctoral level trained graduate studentindividually assessed the participants. A medical, developmental and behavioral history was taken in an interview with parents,during which it was confirmed that the child met criteria for ADHD-CT according to the DSM-IV. Parents also completed theConner’s rating scale-parent report to assist in the confirmation of diagnosis and to quantify severity of ADHD symptoms.Internalizing disorders and developmental coordination disorder were screened for using the DBC-P and the Movement
assessment battery for children, 2nd edition, respectively. As there was no discrepancy between pediatrician’s diagnosis andparental report and questionnaires administered, no participants were excluded from the study. The majority of participants inthe study were taking medication ranging from long to short acting. Participants on medication were asked to discontinuemedication at least 24–72 h prior to testing as per previously described standardized procedures (Leitner et al., 2007).
TD boys were recruited from public schools and community-wide organizations. Normal behavioral functioning wasscreened for using the DBC-P, SRS, Conner’s rating scale in order to exclude the presence of autism or ADHD or otherpreviously listed psychiatric diagnosis.
All HFA and ADHD children completed the Wechsler intelligence scale for children, 4th edition (WISC-IV; (Wechsler, 2003),while TD children were administered either the WISC-IV (10 TD boys) or Wechsler Abbreviated Scale of Intelligence (11 TDboys; WASI; (Wechsler, 1999). All children had a full-scale IQ (FSIQ), VCI/verbal IQ (VIQ) and PRI/performance IQ (PIQ)greater than 70. Analysis of variance (ANOVA) revealed that HFA, AD and TD groups did not differ on FSIQ [F(2, 48) = 2.75,p = .07], VIQ [F(2, 48) = 1.60, p = .20] or PIQ [F(2,48) = 0.13, p = .88].
Motor skills of all children were assessed using the Movement assessment battery for children, 2nd edition (MABC-2;(Henderson, Sugden, & Barnett, 2007), which consists of eight items grouped in three sections: manual dexterity, aiming andcatching skills and balance. A summary of participant demographics is presented in Table 1.
2.2. Apparatus and procedure
Participants completed the speed subtest of the Handwriting Performance Test (HPT) (Cartmill et al., 2009; Ziviani &Elkins, 1984; Ziviani & Watson-Wills, 1998). This task involved copying the words ‘‘cat and dog’’ as many times as possible ina 2-min period using a black pen on 8 mm lined paper. Participants were given the instructions: ‘I want you to write thewords ‘‘cat and dog’’ as many times as you can on these lines. Do not stop to correct mistakes. Write as you would normallywrite’. This test has previously been used to assess handwriting in a large population of students aged 7–14 (Ziviani & Elkins,1984; Ziviani & Watson-Wills, 1998). In the present study, this instrument was used as a measure of handwriting speed, asassessed by number of letters written per minute, and also allowed for the consistency of specific handwriting elements to beassessed as the same phrase was copied numerous times.
2.3. Data screening and statistical analysis
Samples were scanned at 600 dpi and analyzed using GNU Image Manipulation Program v2.6.1. A sample of five ‘cat anddog’ phrases was selected for each participant: the first and last phrases, as well as the phrases at the 25th, 50th and 75th

Table 1
Participant demographics and scores.
Characteristics ADHD (n = 14), mean (SD) HFA (n = 14), mean (SD) Typically developing (n = 21), mean (SD)
Age (years) 11.00 (1.95) 11.50 (1.83) 11.08 (2.14)
FSIQ 97 (12.47) 94 (14.67)a 104 (12.21)
PIQ 105 (14.24) 105 (17.75) 102 (13.00)
VIQ 96 (16.67) 94 (14.13)a 106 (13.17)
MABC-2
Total MABC-2 score 83.64 (10.23) 65.50 (16.96)a,b 85.47 (13.11)
Manual dexterity 9.57 (3.22) 7.35 (3.17)a,b 9.63 (2.85)
Aiming and catching 11.64 (2.73) 7.53 (3.06)a,b 13.94 (31.01)
Balance 8.80 (3.40) 11.64 (2.73)a,b 11.87 (3.11)
ADHD: attention deficit hyperactivity disorder; HFA: high functioning autism; FSIQ; full scale IQ, PIQ: performance IQ; VIQ: verbal IQ; MABC-2: Movemen
assessment battery for children, 2nd edition.a HFA vs. Typically developing, p < .05,b ADHD vs. HFA, p < .05.
Table 2
Variables of handwriting performance on the speed subtest of the Handwriting Performance Test.
Variable ADHD (n = 14), mean (SD) HFA (n = 14), mean (SD) Typically developing (n = 21), mean (SD)
Speed subtest of the Handwriting Performance Test
Total letters written 137(51) 131(43)b 168(45)
Word and phrase dimensions
Height of the phrase ‘cat and dog’ (mm) 62 (14.32) 63 (28.71) 61 (15.00)
Width of the phrase ‘cat and dog’ (mm) 216 (69.60) 200 (38.12) 232 (48.78)
Consistency of phrase height 44.59 (16.58) 46.90 (23.55) 60.70 (40.50)
Consistency of phrase width 13.07 (2.03) 12.97 (1.56) 13.21 (1.27)
Spacing
Average distance between words (mm) 6.34 (4.64) 4.73 (4.21)b 8.73 (2.78)
Consistency of distance between words 11.49 (12.76) 10.85 (13.93)b 22.60 (19.66)
% Total handwriting errors 5.00 (4.48)a,c 0.95 (1.09) 1.27 (1.15)
% formation errors 0.74 (1.19)a,c 0.05 (0.22) 0.04 (0.21)
% extra strokes 1.67 (2.60)c 0.4 (0.54) 0.24 (0.29)
% letter transpositions 0.45 (1.20)a 0.00 (0.00) 0.06 (0.20)
% letter corrections 2.06 (2.3)a 0.52 (0.68s) 0.81 (1.03)
ADHD: attention deficit hyperactivity disorder; HFA: high functioning autism.a ADHD vs. Typically developing, p < .05,b HFA vs. Typically developing, p < .05,c ADHD vs. HFA, p < .05.
B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–1646 1641
t
quartiles. The height and width of each word and whole phrase, and the distance between words was measured. Theconsistency of parameters of handwriting (phrase height, width and total phrase area (height � width), and distancebetween words) was used as a pattern-based measure of handwriting quality. The consistency of a parameter wasdetermined by the ratio between the mean of that parameter and its standard deviation (coefficient of variability; COV).Therefore, lower values indicated a reduced ability to control the consistency of that parameter.
Handwriting errors were examined across the entire handwriting sample. Handwriting errors were defined as: formationerrors (parts of letters not formed, such as the cross of the letter ‘t’ touching the upright), extra strokes or lines, lettertranspositions (e.g. swapping a/c, d/g) and corrections (crossing out or writing over incorrect letters). The proportion ofhandwriting errors was determined as the number of errors performed over total letters written.
Handwriting speed was assessed as the number of letters written across the 2-min writing period.A series of one-way ANOVAs were used to compare HFA, ADHD and TD groups across each group of variables: (1)
participant demographics (age, IQ, MABC-2 scores), (2) handwriting size and size consistency, (3) spacing between words, (4)handwriting errors and (5) handwriting speed. Normality was determined using Levene’s test of normality.
Stepwise multiple regression analysis was performed with age, VCI/VIQ, PRI/PIQ, manual dexterity, aiming and catching,and balance entered as predictive factors of spacing between words and handwriting errors for each group separately. Toexamine whether the proportion of handwriting errors was a predictive factor for handwriting speed, age, VCI/VIQ, PRI/PIQgender, manual dexterity, aiming and catching, balance and proportion of handwriting errors were entered as predictivefactors of handwriting speed for each group separately.
3. Results
Table 2 shows summary results of handwriting performance.
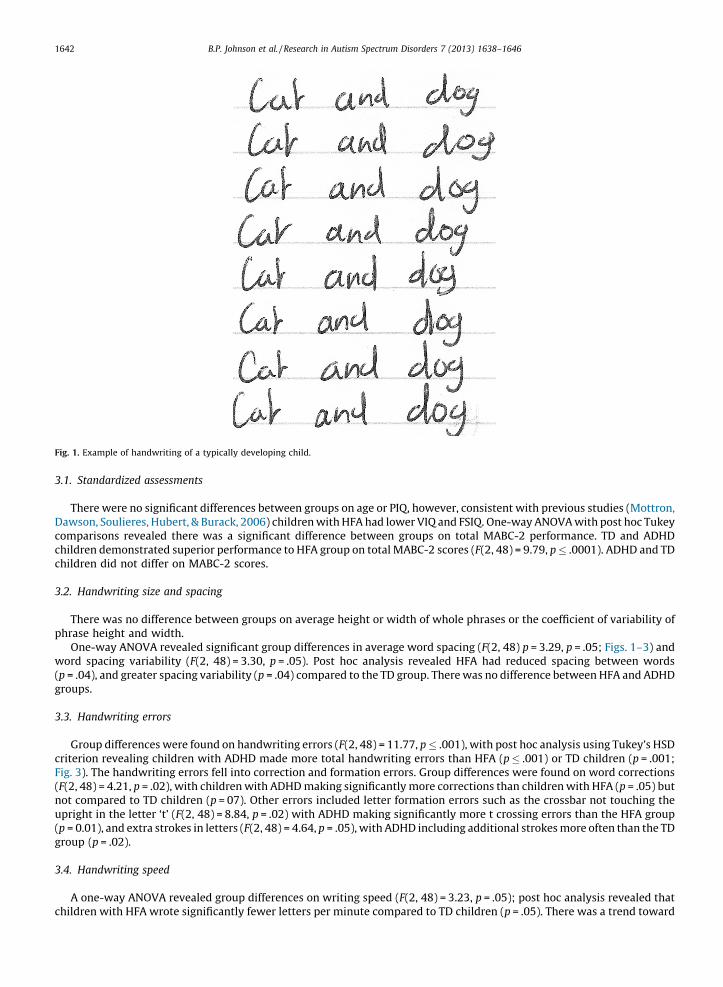
Fig. 1. Example of handwriting of a typically developing child.
B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–16461642
3.1. Standardized assessments
There were no significant differences between groups on age or PIQ, however, consistent with previous studies (Mottron,Dawson, Soulieres, Hubert, & Burack, 2006) children with HFA had lower VIQ and FSIQ. One-way ANOVA with post hoc Tukeycomparisons revealed there was a significant difference between groups on total MABC-2 performance. TD and ADHDchildren demonstrated superior performance to HFA group on total MABC-2 scores (F(2, 48) = 9.79, p � .0001). ADHD and TDchildren did not differ on MABC-2 scores.
3.2. Handwriting size and spacing
There was no difference between groups on average height or width of whole phrases or the coefficient of variability ofphrase height and width.
One-way ANOVA revealed significant group differences in average word spacing (F(2, 48) p = 3.29, p = .05; Figs. 1–3) andword spacing variability (F(2, 48) = 3.30, p = .05). Post hoc analysis revealed HFA had reduced spacing between words(p = .04), and greater spacing variability (p = .04) compared to the TD group. There was no difference between HFA and ADHDgroups.
3.3. Handwriting errors
Group differences were found on handwriting errors (F(2, 48) = 11.77, p � .001), with post hoc analysis using Tukey’s HSDcriterion revealing children with ADHD made more total handwriting errors than HFA (p � .001) or TD children (p = .001;Fig. 3). The handwriting errors fell into correction and formation errors. Group differences were found on word corrections(F(2, 48) = 4.21, p = .02), with children with ADHD making significantly more corrections than children with HFA (p = .05) butnot compared to TD children (p = 07). Other errors included letter formation errors such as the crossbar not touching theupright in the letter ‘t’ (F(2, 48) = 8.84, p = .02) with ADHD making significantly more t crossing errors than the HFA group(p = 0.01), and extra strokes in letters (F(2, 48) = 4.64, p = .05), with ADHD including additional strokes more often than the TDgroup (p = .02).
3.4. Handwriting speed
A one-way ANOVA revealed group differences on writing speed (F(2, 48) = 3.23, p = .05); post hoc analysis revealed thatchildren with HFA wrote significantly fewer letters per minute compared to TD children (p = .05). There was a trend toward

Fig. 2. Example of handwriting of a child with high functioning autism.
Fig. 3. Example of handwriting of a child with attention deficit hyperactivity disorder.
B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–1646 1643
significant difference between ADHD and TD groups (p = .06). No significant difference in handwriting speed was foundbetween HFA and ADHD groups.
3.5. Regression analyses
3.5.1. Spacing between words
Ninety-two percent of the variance in handwriting spacing in children with HFA was explained by the regression model(F(6,7) = 35.42, p = .002, R2 = .92, R2 adjusted = .85). The best predictors of handwriting spacing in HFA were PRI(standardized b = �.66, t = �5.61, p = .001) and MABC-2 aiming and catching (standardized b = �.58, t = 4.46, p = .003),indicating that poorer perceptual reasoning, visuospatial and visuomotor coordination are significant predictors of poorerhandwriting spacing.
The model was not significant in either ADHD (F(6,7) = .39, p = .91, R2 = .25, R2 adjusted = �.39) or TD groups(F(6,11) = 2.20, p = .12, R2 = .54, R2 adjusted = .30).
3.5.2. Handwriting errors
Eighty-one percent of the variance of handwriting errors in children with HFA was explained by the regression model(F(6,7) = 4.86, p = .03, R2 = .81, R2 adjusted = .64). The best predictor of handwriting errors in HFA was balance (standardizedb = �1.08, t = �3.98, p = .005) and manual dexterity (standardized b = �1.11, t = 4.16, p = .004), indicating that motorcoordination contributes significantly to handwriting errors in this group.

B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–16461644
The model was not significant in either ADHD (F(6,7) = .32, p = .90, R2 = .21, R2 adjusted = �.45) or TD groups (F(6,11) = .72,p = .12, R2 = .26, R2 adjusted = �.10).
3.5.3. Handwriting speed
Eighty-five percent of the variance in handwriting speed in children with HFA was explained by the regression model(F(7,6) = 5.06, p = .03, R2 = .85, R2 adjusted = .72). The best predictor of handwriting speed in HFA was VCI (standardizedb = .78, t = 3.00, p = .02), revealing that verbal abilities impact upon handwriting speed in individuals with HFA, even duringtasks of relatively low linguistic demand.
Eighty-four percent of the variance in handwriting speed in children with ADHD was explained by the regression model(F(7,6) = 4.61, p = .04, R2 = .84, R2 adjusted = .66). The best predictors of handwriting speed in ADHD were age (standardizedb = .78, t = 3.13, p = .02) and % total handwriting errors (standardized b = �.57, t = �3.12, p = .02), indicating that morecorrections are associated with slower handwriting speed, and that maturational processes may contribute to handwritingperformance.
The model was not significant for the TD group (F(7,18) = 1.88, p = .17, R2 = .54, R2 adjusted = .26).
4. Discussion
The purpose of this study was to compare the handwriting profiles in children with HFA and ADHD using a simplehandwriting task, with particular attention to size and spacing, handwriting errors and handwriting speed. Overallassessment of the handwriting data indicates a distinction between the handwriting profiles of HFA and ADHD: the HFAgroup was characterized by poorer spatial arrangement of words, yet made few writing errors, while the ADHD group madeconsiderably more spelling corrections and letter transpositions. The HFA group wrote significantly more slowly, and therewas a trend toward slower handwriting speed in the ADHD group.
That handwriting was slower in both HFA and ADHD is concordant with previous findings by Mayes and Calhoun (2007),however our study revealed important differences in the factors that contribute to handwriting speed for the two groups:VCI significantly influenced handwriting speed in HFA, whereas age and the proportion of total handwriting errors mostsignificantly affected speed in ADHD. Our findings in HFA are similar to recent findings by Hellinckx et al. (2013), who foundthat reading abilities were significant predictors of writing speed (Hellinckx et al., 2013). However, unlike Hellinckx et al.(2013), we did not find that age and fine motor coordination contributed to handwriting speed. This may be related todifferences in the length of the writing period and complexity of the written tasks between the two studies. Handwritingerrors in the ADHD group was also found to be a significant predictor of handwriting speed, which is consistent with speed-accuracy findings by Adi-Japha et al. (2007), who observed that poorer tracing accuracy was significantly correlated withslower writing speeds. Additionally, that age was a significant predictor of handwriting quality suggests that maturationalprocesses might help improve handwriting performance in ADHD.
Fuentes et al. (2009) found motor skills was the main predictor of handwriting performance in children with ASD aged 8–13, but PRI and not motor skills predicted handwriting performance in children aged 12–14 (Fuentes et al., 2010). We foundthat both motor skills and PRI were significant predictors of handwriting spacing and errors in HFA. It is likely, therefore, thatboth visual/non-verbal organization and reasoning and motor coordination may contribute to handwriting difficulties inthese groups, and this may impact handwriting differently depending on the length and complexity of the text to be written,and the duration of the writing task.
Smaller and more irregular spacing between words in the HFA group is consistent with previous studies of drawing andwriting in children with ASD, which have reported a more detail focused drawing style that resulted in poorer spatialarrangement of drawing (Booth et al., 2003) and writing (Hellinckx et al., 2013) elements. The ability to appropriately spacewords may relate to difficulty in movement planning; bias to local versus global processing is considered a key feature ofautism (Booth et al., 2003). Studies by Fabbri-Destro, Cattano, Boria, and Rizzolatti (2009) revealed that when chainingmultiple upper limb motor actions into a global actions, children with autism perform more slowly and perform the wholemovement as series of independent steps, with little planning of subsequent movements in preparation for global movementendpoint (Fabbri-Destro et al., 2009). During handwriting, TD children make motor preparations for an entire syllable of aword in advance; the movement required for the first syllable of a word is prepared before starting to write, and preparationfor the second syllable occurs during production of the first (Kandel, Soler, Valdois, & Gros, 2006). Reduced spacing betweenwords in the HFA group therefore may relate to planning each letter individually, rather than preparation of syllables, wordsand sentences as a whole, with a lack of anticipation of each movement endpoint. Another contributing factor to slowhandwriting speed may also be increased motor noise, i.e. inefficient motor movements while writing (Johnson et al., 2013).As more physical effort is required to perform the movements to write the letters correctly, this may contribute to fatigueduring extended writing periods.
Handwriting in children with ADHD was characterized by a greater number of handwriting errors, predominantlyspelling corrections and letter substitutions. Indeed, there is a growing consensus in the literature that errors such astranspositions and corrections are a prominent characteristic of handwriting in ADHD, and that these errors are unrelated toVIQ or spelling ability (Adi-Japha et al., 2007), a finding that supports our results. In the present study, children with ADHDoften made letter substitutions or corrections when writing letters of similar shaped characters (e.g. a and c, d and g; seeFig. 3). This may reflect an inability to suppress or inhibit similar or irrelevant information from entering working memory,

B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–1646 1645
i.e. having difficulty suppressing similar shaped graphemes or similar sounding phonemes during writing (Adi-Japha et al.,2007; Kandel et al., 2006). We also found that the proportion of handwriting errors was also predictive of slower writingspeed, which may reflect a speed/accuracy trade-off. Importantly, however, the process of correcting written work maydisrupt higher level writing processes in children with ADHD. When handwriting motor plans are well formed (automated)with few errors, cognitive demands can then be directed toward higher level processes, such as idea formulation, prosecomposition and review (Berninger et al., 1997).
Although handwriting remains an important skill to master, both in the classroom and in daily life, for children with HFAwho show considerable slowness during writing exercises, alternating handwriting with keyboarding may be a useful aid forthese children (Ashburner, Ziviani, & Pennington, 2012). Our findings revealed that VCI was significantly predictive ofhandwriting speed in the HFA group, and for children with lower VCI, increased support during writing exercises by using akeyboard may be recommended. Ashburner et al. (2012) recently found that for children with HFA, keyboarding helped toimprove handwriting speed, as well as length and quality of written compositions, when compared to handwriting.Furthermore, motivation for writing was typically higher when children with HFA were able to use a keyboard (Ashburneret al., 2012). Although interventions for keyboarding are yet to be examined directly in ADHD, the ability to rapidly correcttypographical errors while using a word processor may improve writing composition in children with ADHD.
A significant limitation of the present study was the small sample size of the HFA and ADHD groups. Despite this, we havedemonstrated key differences that may exist in the handwriting profiles of HFA and ADHD. However this study was unable toexamine the interplay between autistic and ADHD symptoms and their severity, gender and handwriting performance,which is of particular importance in light of changes within the DSM-5. Further qualitative and kinematic examination ofhandwriting performance is required in children who have comorbid autism and ADHD, as they may have additionalburdens and require unique strategies to help improve motor coordination and written language skills (Kopp, Beckung, &Gillberg, 2010).
The findings from the present study reveal distinct profiles of handwriting impairments for HFA and ADHD groups. Forexample, while both groups show significantly slower handwriting, the contributing factors for slower handwriting wereunique to each group: slow handwriting in HFA was associated with VCI, whereas in ADHD it was associated with theproportion of corrections made. Problems with spacing were more common in the HFA group, while spelling mistakes weremore common in the ADHD group. The divergence in handwriting difficulties between HFA and ADHD provides importantinsight into the underlying functional deficits in each of these conditions and informs the development of tailored, evidence-based handwriting therapies in these groups.
References
Adi-Japha, E., Landau, Y., Frenkel, L., Teicher, M., Gross-Tsur, V., & Shaley, R. (2007). ADHD and dysgraphia: Underlying mechanisms. Cortex, 43(6), 700–709 http://dx.doi.org/10.1016/S0010-9452(08)70499-4
American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (revised 4th ed.). Arlington, VA: American Psychiatric Publishing.American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: American Psychiatric Publishing.Ashburner, J., Ziviani, J., & Pennington, A. (2012). The introduction of keyboarding to children with autism spectrum disorders with handwriting difficulties: A help
or a hindrance? Australasian Journal of Special Education, 36(1), 32–61.Berninger, V., Vaughan, K., Abbott, R., Abbott, S., Rogan, L., Brooks, A., et al. (1997). Treatment of handwriting problems in beginning writers: Transfer from
handwriting to composition. Journal of Educational Psychology, 89(4), 652–666.Beversdorf, B., Anderson, J., Manning, S., Anderson, S., Nordgren, R., Felopulos, G., et al. (2001). Brief report: Macrographia in high-functioning adults with autism
spectrum disorder. Journal of Autism and Developmental Disorders, 31(1), 97–101 http://dx.doi.org/10.1023/A:1005622031943Booth, R., Charlton, R., Hughes, C., & Happe, F. (2003). Disentangling weak coherence and executive dysfunction: Planning drawing in autism and attention-deficit/
hyperactivity disorder. Philosophical Transactions of the Royal Society B: Biological Sciences, 358(1430), 387–392.Brereton, A., Tonge, B., Mackinnon, A., & Einfeld, S. (2002). Screening young people for autism with the developmental behaviour checklist. Journal of American
Academy of Child & Adolescent Psychiatry, 41(11), 1369–1375.Cartmill, L., Roger, S., & Ziviani, J. (2009). Handwriting of eight-year-old children with Autism Spectrum Disorder: An exploration. Journal of Occupational Therapy,
Schools and Early Intervention, 2(2), 103–118 http://dx.doi.org/10.1080/19411240903146426Fabbri-Destro, M., Cattano, L., Boria, S., & Rizzolatti, G. (2009). Planning actions in autism. Experimental Brain Research, 192, 521–525.Flapper, B., Houwen, S., & Shoemaker, M. (2006). Fine motor skills and effects of methylphenidate in children with attention deficit hyperactivity disorder and
developmental coordination disorder. Developmental Medicine & Child Neurology, 48, 165–169 http://dx.doi.org/10.1017/S0012162206000375Frings, M., Gaertner, K., Buderath, P., Christiansen, H., Gerwig, M., Hein-Kropp, C., et al. (2010). Megalographia in children with cerebellar lesions and in children
with attention-deficit/hyperactivity disorder. Cerebellum, 9(3), 429–432 http://dx.doi.org/10.1007/s12311-010-0180-yFuentes, C., Mostofsky, S., & Bastian, A. (2009). Children with autism show specific handwriting impairments. Neurology, 73, 1532–1537 http://dx.doi.org/10.1212/
WNL.0b013e3181c0d48cFuentes, C., Mostofsky, S., & Bastian, A. (2010). Perceptual reasoning predicts handwriting impairments in adolescents with autism. Neurology, 75(20), 1825–1829
http://dx.doi.org/10.1212/WNL.0b013e3181fd633dHellinckx, T., Roeyers, H., & Van Waelvelde, H. (2013). Predictors of handwriting in children with Autism Spectrum Disorder. Research in Autism Spectrum Disorders,
7(1), 176–186 http://dx.doi.org/10.1016/j.rasd.2012.08.009Henderson, S., Sugden, D., & Barnett, A. (2007). Movement assessment battery for children (Movement ABC-2) (2nd ed.). London: The Psychological Corporation.Johnson, B., Phillips, J., Papadopoulos, N., Fielding, J., Tonge, B., & Rinehart, N. (2013). Understanding macrographia in children with autism spectrum disorders.
Research in Developmental Disabilities, 34(9), 2917–2926 http://dx.doi.org/10.1016/j.ridd.2013.06.003Kandel, S., Soler, O., Valdois, S., & Gros, C. (2006). Graphemes as motor units in the acquisition of writing skills. Reading and Writing, 19, 313–337.Kopp, S., Beckung, E., & Gillberg, C. (2010). Developmental coordination disorder and other motor control problems in girls with autism spectrum disorder and/or
attention-deficit/hyperactivity disorder. Research in Developmental Disabilities, 31(2), 350–361 http://dx.doi.org/10.1016/j.ridd.2009.09.017Kushki, A., Chau, T., & Anagnostou, E. (2011). Handwriting difficulties in children with autism spectrum disorders: A scoping review. Journal of Autism &
Developmental Disorders, 41(12), 1706–1716 http://dx.doi.org/10.1007/s10803-011-1206-0Langmaid, R., Papadopoulos, N., Johnson, B., Phillips, J., & Rinehart, N. (2012). Handwriting in children with attention deficit hyperactivity disorder. Journal of
Attention Disorders http://dx.doi.org/10.1177/1087054711434154 (Ahead of print)

B.P. Johnson et al. / Research in Autism Spectrum Disorders 7 (2013) 1638–16461646
Leitner, Y., Barak, R., Giladi, N., Peretz, C., Eshel, R., Gruendlinger, L., et al. (2007). Gait in attention deficit hyperactivity disorder: Effects of methylphenidate anddual tasking. Journal of Neurology, 254(10), 1330–1338.
Mayes, S., & Calhoun, S. (2007). Learning, attention, writing, and processing speed in typical children and children with ADHD, autism, anxiety, depression, andoppositional-defiant disorder. Child Neuropsychology, 13(6), 469–493 http://dx.doi.org/10.1080/09297040601112773
Mayes, S., Calhoun, S., & Crowell, E. (2000). Learning disabilities and ADHD: Overlapping spectrum disorders. Journal of Learning Disabilities, 33(5), 417–424 http://dx.doi.org/10.1177/002221940003300502
Mottron, L., Dawson, G., Soulieres, I., Hubert, B., & Burack, J. (2006). Enhanced perceptual functioning in autism: An update, and eight principles of autisticperception. Journal of Autism and Developmental Disorders, 36(1), 27–43.
Racine, M., Majnemer, A., Shevell, M., & Snider, L. (2008). Handwriting performance in children with attention deficit hyperactivity disorder (ADHD). Journal ofChild Neurology, 12(4), 399–406 http://dx.doi.org/10.1177/0883073807309244
Re, A. M., Caeran, M., & Cornoldi, C. (2008). Improving expressive writing skills of children rated for ADHD symptoms. Journal of Learning Disabilities, 41(6), 535–544.
Shen, I., Lee, T., & Chen, C. (2012). Handwriting performance and underlying factors in children with Attention Deficit Hyperactivity Disorder. Research inDevelopmental Disabilities, 33(4), 1301–1309 http://dx.doi.org/10.1016/j.ridd.2012.02.010
Tsai, L. H., Meng, L. F., Hung, L. Y., Chen, H. Y., & Lu, C. P. (2011). Coincidence of homophone spelling errors and attention problems in school children: A surveystudy. Research in Developmental Disabilities, 32, 75–80.
Tucha, O., Mecklinger, L., Walitza, S., & Lange, K. (2006). Attention and movement execution during handwriting. Human Movement Science, 25, 536–552 http://dx.doi.org/10.1016/j.humov.2006.06.002
Wechsler, D. (1999). Wechsler abbreviated scale of intelligence (WASI). San Antonio, TX: Harcourt Assessment.Wechsler, D. (2003). Wechsler intelligence scale for children (4th ed.). San Antonio, TX: Harcourt Assessment.Witwer, A., & Lecavalier, L. (2007). Autism screening tools: An evaluation of the Social Communication Questionnaire and the Developmental Behaviour
Checklist—Autism Screening Algorithm. Journal of Intellectual and Developmental Disability, 32(3), 179–187.Ziviani, J., & Elkins, J. (1984). An evaluation of handwriting performance. Educational Review, 36(3), 249–261.Ziviani, J., & Watson-Wills, A. (1998). Writing speed and legibility of 7–14-year-old school students using modern cursive script. Australian Occupational Therapy
Journal, 45(2), 59–64.