A NEW PROTOCOL FOR CERVICAL SPINE CLINICAL AND ...
6
a) A NEW PROTOCOL FOR CERVICAL SPINE CLINICAL AND BIOMECHANICAL EVALUATION USING MOTION CAPTURE TECHNIQUES DURING UNCONSTRAINED PACED HEAD ROTATIONS Nicola Petrone 1 , Gianluca Milan 1 , Matteo Marchiori 1 , Valerio Tegon 2 , Andrea Perissinotto 3 , Andrea Zonta 4 , Giampietro Bonivento 5 1 Dept. of Mechanical Engineering, University of Padova, Italy, [email protected] 2 Blu Center s.r.l., Rehabilitation Centre, Padova, Italy 3 Center for Rehabilitation and Biomechanical Assessment, Umberto I° Hospital, Venice, Italy 4 Orthopaedic Rehabilitation Service, Padova Civil Hospital, Padova, Italy 5 Ca’ Foncello Hospital, Treviso, Italy INTRODUCTION In the last decades several research projects have focussed on the biomechanical evaluation of lumbar spine instability by using either imaging techniques and isokinetik tests, the latter being now currently used for clinical assessment. To our knowledge a similar approach is still not available for the cervical spine at least as a routinely adopted practice, also because of the risk related to restrained motions of the head, mainly in the case of injured subjects. The aim of the present study was therefore to provide a new protocol for cervical spine clinical and biomechanical evaluation during unconstrained paced head rotations as an integrated tool in diagnostic procedures, based on the application of a totally non-invasive motion capture technique. MATERIALS AND METHODS The adopted experimental approach was based on previous analogous experiences on lumbar spine isokinetic tests in which the torque/flexion curves were measured on a Cybex machine and clinically analyzed to reveal lumbar instabilities in correspondence of peak/valley local features of the curve [1]. In the present work, given the lower experience and the high risk of additional injuries that misuse of cervical spine may present [2-4], a totally non- invasive approach was adopted: head rotational behavior was therefore studied without any restraint or loading device and the clinical analysis was based on kinematics of head and shoulder [5]. The project developed following several stages, corresponding to the type and number of tester involved: (i) pilot tests were performed on a group of healthy subjects and on a group of patients with different degrees of whiplash injuries [2-4], without any particular imp osition during the tests apart from performing the highest range head rotations; (ii) analysis of the pilot tests was performed to identify clear differences in the kinematics of the head [6-11]; (iii) a more specified test protocol was defined to allow for consis tent results and to improve the comparison between healthy and injured subjects. The motion capture technique was defined during the pilot tests and progressively refined. A set of 21 spherical reflective markers were placed directly on the skin of each volunteer with the aid of adhesive dots. Facial glabella, temporum mandibular joints, acromions, shoulder blade posterior spines, C7, T3, T6, T9, T12, L1, L3 and L5 spinal processes, sacrum and PSIS were selected as anatomical marker sites (see Figure 1a). An adjustable helmet carrying three additional markers was used to investigate the physiological motion-match with respect to head rigid-body- like movement. A motion capture system (Smart - eMotion s.r.l., Padova, Italy) supplied with six infrared cameras allowed the capture and software tracking of each marker position in a virtual anatomically-oriented coordinates system. Figure 1 : (a) Positioning of markers in accordance with the proposed protocol for motion capture–based analysis of cervical spine disorders. (b) Right/left paced unconstrained head rotation in seated position, shoulders restrained by hands holding the seat. The pilot tests, namely stage (i), were conducted on a control group of three healthy subjects and on four injured subjects with different degrees of injury seriousness and at different moments of the rehabilitation period. All subjects were requested to perform at least five complete head rotations aiming to reach the maximum range of motion, at their natural speed, without any visual or acoustic reference signal. b)
Transcript of A NEW PROTOCOL FOR CERVICAL SPINE CLINICAL AND ...

a)
A NEW PROTOCOL FOR CERVICAL SPINE CLINICAL AND BIOMECHANICAL EVALUATION USING MOTION CAPTURE TECHNIQUES DURING UNCONSTRAINED PACED HEAD ROTATIONS
Nicola Petrone1, Gianluca Milan1, Matteo Marchiori1, Valerio Tegon2,
Andrea Perissinotto3, Andrea Zonta4, Giampietro Bonivento5
1Dept. of Mechanical Engineering, University of Padova, Italy, [email protected] 2Blu Center s.r.l., Rehabilitation Centre, Padova, Italy
3 Center for Rehabilitation and Biomechanical Assessment, Umberto I° Hospital, Venice, Italy 4 Orthopaedic Rehabilitation Service, Padova Civil Hospital, Padova, Italy
5 Ca’ Foncello Hospital, Treviso, Italy INTRODUCTION
In the last decades several research projects have focussed on the biomechanical evaluation of lumbar spine instability by using either imaging techniques and isokinetik tests, the latter being now currently used for clinical assessment. To our knowledge a similar approach is still not available for the cervical spine at least as a routinely adopted practice, also because of the risk related to restrained motions of the head, mainly in the case of injured subjects. The aim of the present study was therefore to provide a new protocol for cervical spine clinical and biomechanical evaluation during unconstrained paced head rotations as an integrated tool in diagnostic procedures, based on the application of a totally non-invasive motion capture technique. MATERIALS AND METHODS
The adopted experimental approach was based on previous analogous experiences on lumbar spine isokinetic tests in which the torque/flexion curves were measured on a Cybex machine and clinically analyzed to reveal lumbar instabilities in correspondence of peak/valley local features of the curve [1]. In the present work, given the lower experience and the high risk of additional injuries that misuse of cervical spine may present [2-4], a totally non-invasive approach was adopted: head rotational behavior was therefore studied without any restraint or loading device and the clinical analysis was based on kinematics of head and shoulder [5]. The project developed following several stages, corresponding to the type and number of tester involved: (i) pilot tests were performed on a group of healthy subjects and on a group of patients with different degrees of whiplash injuries [2-4], without any particular imp osition during the tests apart from performing the highest range head rotations; (ii) analysis of the pilot tests was performed to identify clear differences in the kinematics of the head [6-11]; (iii) a more specified test protocol was defined to allow for consis tent results and to improve the comparison between healthy and injured subjects. The motion capture technique was defined during the pilot tests and progressively refined. A set of 21 spherical reflective markers were placed directly on the skin of each volunteer with the aid of adhesive dots. Facial glabella, temporum mandibular joints, acromions, shoulder blade posterior spines, C7, T3, T6, T9, T12, L1, L3 and L5 spinal processes, sacrum and PSIS were selected as anatomical marker sites (see Figure 1a). An adjustable helmet carrying three additional markers was used to investigate the physiological motion-match with respect to head rigid-body-like movement.
A motion capture system (Smart - eMotion s.r.l., Padova, Italy) supplied with six infrared cameras allowed the capture and software tracking of each marker position in a virtual anatomically-oriented coordinates system.
Figure 1: (a) Positioning of markers in accordance with the proposed protocol for motion capture–based analysis of cervical spine disorders. (b) Right/left paced unconstrained head rotation in seated position, shoulders restrained by hands holding the seat. The pilot tests, namely stage (i), were conducted on a control group of three healthy subjects and on four injured subjects with different degrees of injury seriousness and at different moments of the rehabilitation period. All subjects were requested to perform at least five complete head rotations aiming to reach the maximum range of motion, at their natural speed, without any visual or acoustic reference signal.
b)

Data processing, namely stage (ii), was performed by using in house automatic routines implemented in Matlab. The analysis was aimed to determine (1) the head unconstrained functional range of motion and natural angular velocity, (2) any right/left side ROM asymmetry, (3) any right/left side rotation velocity asymmetry, (4) the head instantaneous rotational axis trajectory, (5) the head motion control capabilities at different motion rates. After the first stage of pilot tests, a test protocol was specified to improve the relevance of comparison [5]. At stage (iii), a group of ten healthy volunteers ranging from 25 to 36 years old was examined. None suffered from cervical pain or other related symptoms. The subjects were instructed to perform five unconstrained paced head rotation in seated position (see Figure 1b) at medium and fast motion rate – 20 and 45 cycles/min respectively – trying to span uniformly the whole ROM in both right and left side following the pace given by an acoustic signal. Besides the head, two other groups of markers were separately identifiable: the markers located in the shoulder upper district and the low back cluster. In such a way it was possible to refer the head position alternatively to the shoulder or to the pelvis, obtaining a deeper insight into the contribution of each motion unit. The protocol developed allows the determination of full head movements in absolute or relative coordinates: in particular the absolute rotation in an horizontal plane of the head (θH) and shoulder (θS) and the relative rotation between head and shoulder (θHS) can be evaluated as shown in Figure 2. In addition, head angular velocity relative to the shoulder (ωHS) can be plotted in polar coordinates as function of the head-shoulder relative angle (θHS) as shown in Figure 3 and 4. When comparing right side and left side, θHS may result asymmetric. Moreover, as the head approaches the range motion limits, ωHS shows clear oscillations due to the muscle activation and the increasing of anatomical restraints. Figure 2: System of reference adopted (a) absolute xz horizontal reference frame (b) θH = head absolute rotation, θS = shoulder absolute rotation, θHS = head-to-shoulder relative rotation.
To date, two main indexes have been adopted to allow clinical objective evaluation, one being related to rotational motion range, the other to angular velocity in the so called “neutral position” i.e. when x’’ axis is coincident with x axis (see Figure 2). This additional parameter intends to gain a consistent picture of patient’s deficiency in dynamic physiological movements, like those entiling a sudden rotation from the right to the left side, typical of daily receptive and interactive actions (talking, crossing the road, driving and so forth). Each test consisted of four or five complete movements (cycle) spanning the whole range of motion from the right to the left. Therefore in order to evaluate data coming out from several cycles with a single index, postprocessing was conducted as follows: first, the maximum right and left head angles (θHSr and θHSl respectively) were separately averaged as well the head angular velocity at neutral position in both directions, left-to-right and right-to-left, denoted as ωHSr and ωHSl . Subsequently, Rotational Symmetry Index (RSIHS) and Velocity Symmetry Index (VSIHS) were evaluated for the relative head-shoulder angles as reported below:
{ }{ } { }
{ }{ } { }
θ=θθθθ
θθ−
θ=θθθθ
θθ
=
HSlHSlHSrHSlHSr
HSlHSr
HSrHSlHSrHSlHSr
HSlHSr
HS
;minif;max
;min
;minif;max
;min
RSI
(1)
{ }{ }
ωω
ωω=
HSlHSr
HSlHSr
HS;max
;minVSI
(2) Pedix “r” and “l” refer to right and left respectively, while the line over θ and ω denotes the average value. The RSI has a double relevance, in that the absolute value measures the degree of symmetry whereas the plus/minus sign highlights the affected side. With respect to a preliminary study a similar definition seemed to be redundant for the VSI, and that was the reason why angular velocity modulus was considered. Besides the RSI and VSI index, the difference between θHSr and θHSl , namely ∆θHS was evaluated believing that, to a certain extent, injured patients could show a noticeable reduction of “span” capability. Statistically speaking, since healthy subjects and injured patients are expected to belong to two different populations, it was of primary importance to verify the expectations. Within this verification an unpaired T-test was performed by adopting an interval of confidence equal to 95% and by comparing the absolute level of RSI index. In such a way the laterality effect was neglected since the main objective of the analysis was to find out any differences among the two classes of subjects rather than the percentage of right/left affected side incidence. Whenever p value resulted greater than 0.05, a statistical difference between the two populations has to be ruled out. The need for a test standardization arose from the observation that free head rotation did not enable a consistent comparative analysis even within the same group of volunteers. So the subsequent step (iii) was to define precise test features moving from unpaced to paced head
x’’

rotation by selecting two rotational rates: 20 cycle/min and 45 cycles/min respectively. RESULTS
Data collected during the pilot tests on healthy and injured subjects were analyzed and compared. Two representative diagrams are reported to clarify the general outline of ωHS versus θHS curves; one (see Figure 3) refers to an injured patient, the other to an healthy subject (see Figure 4). The first reveals a remarkable ROM reduction, a motion shift towards the left side likely due to a trauma on the right district and eventually a loss of kinematic control across the neutral position (shown by the cusps and the scattering of ωHS).
- 9 0
- 75
- 60
- 45
- 30 - 15 0 15
30
45
60
75
90 0 250 500 - 250 - 500
[ ° ]
[ ° s - 1 ]
Figure 3: Angular velocity ωHS (red line) versus angular position θHS (blue line) during free unconstrained head rotation on a injured patient (subject I4).
- 9 0
- 75
- 60
- 45
- 30 - 15 0 15
30
45
60
75
90 0 250 500 - 250 - 500
[ ° ]
[ ° s - 1 ] Figure 4: Angular velocity ωHS (red line) versus angular position θHS (blue line) during free unconstrained head rotation on a healthy subject (subject H3). As expected, the diagram plotted on the basis of data coming out from an healthy subject (see Figure 4), shows a more regular signal, a larger amplitude of rotation both on right and on left side and finally a controlled crossing of neutral position. Actually this is not a necessary condition to state whether or not a subject has a cervical disorder because muscular stress and facets distance is less critical in the neutral position rather than at the extreme angle of ROM. Therefore an overall analysis aiming at the correlation study between injured patients and painful symptoms must be considered first. The results of a quantitative analysis of available data on healthy and injured subjects are collected in Tables 1 and 2
respectively, using the angles and velocity definitions previously introduced. Table 3 reports the comparison of average results on healthy and injured subjects in terms of overall range of motion ∆θHS and of symmetry indexes RSI and VSI.
Table 1 Healthy subjects’ head-to-shoulder average values; angles in extreme position on both sides and angular velocities in neutral position in both directions (pedix “r” and “l” are related to right and left side respectively).
Subject θHSr [°] θHSl [°] ωHSr [°/s] ωHSl [°/s] H1 66.1 -69.0 118.1 -138.6 H2 78.7 -67.0 113.8 -122.5 H3 80.9 -75.6 97.6 -196.7
Average 75.2 -70.5 109.8 152.6 Std. Dev. 7.9 4.5 10.8 39.0
Table 2 Injured patients’ head-to-shoulder average values; angles in extreme position on both sides and angular velocities in neutral position in both directions (pedix “r” and “l” are related to right and left side respectively).
Subject θHSr [°] θHSl [°] ωHSr [°/s] ωHSl [°/s]
I1 64.0 -68.0 232.1 -262.0 I2 69.5 -73.4 87.8 -69.9 I3 65.2 -49.0 133.2 -86.6 I4 43.2 -57.6 157.2 -126.3
Average 60.5 -62.0 128.7 136.2 Std. Dev. 11.7 10.8 60.3 87.16
Table 3 Comparison between healthy and injured subjects in terms of symmetry indexes relating to rotation (RSI) and angular velocity (VSI).
Subject (∆θHS)AV [°]
RSI Std. Dev. VSI Std. Dev.
Healthy 145.7 0.91 0.06 0.76 0.23 Injured 122.5 0.85 0.11 0.87 0.09
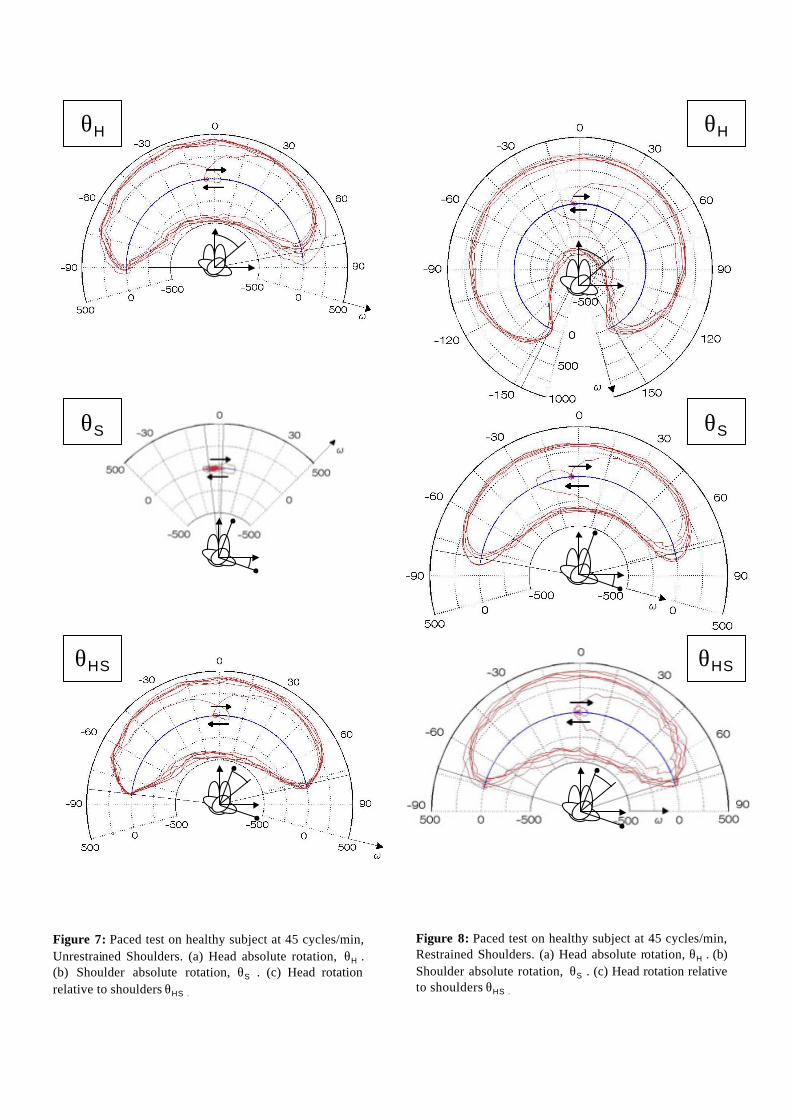
The preliminary pilot tests, despite the lower average values of ∆θHS and RSI of injured subjects with respect to healthy ones, did not show any significant differences between the two groups (p>0.05), and this was fairly in contradiction with authors’ expectations: nevertheless, qualitative comparison of plots like those in figure 3 and 4 confirmed the possibility of clinical evaluations and comparison based on quantitative analytical indexes. Apart from these objective remarks, it was assumed that by increasing the amount of available data, and by introducing a more standardised test procedure different analysis outcome might strike out. In fact, generally speaking, having a larger set of tests may give the statistical analysis a lower scatter and the comparative investigations a greater relevance with respect to differences detection. The results of paced unconstrained head rotations collected on a healthy subject after refinement of the tests protocol are reported in figure 5 and 6, respectively with hands holding the seat and hands resting on the chest, at 20 cycles/min. Figure 7 and 8 report the corresponding results for the highest pace of 45 cycles/min.

Figure 5: Paced test on healthy subject at 20 cycles/min, Restrained Shoulders. (a) Head absolute rotation, θH . (b) Shoulder absolute rotation, θS. (c) Head rotation relative to shoulders θHS .
Figure 6: Paced test on healthy subject at 45 cycles/min, Unrestrained Shoulders. (a) Head absolute rotation, θH . (b) Shoulder absolute rotation, θS. (c) Head rotation relative to shoulders θHS .
θH
θS
θHS
θH
θS
θHS
20 cycles /min 45 cycles /min Table 4: results on healthy subject of paced tests. RS US RS US
θHr deg 89.40 147.68 80.54 150.12 θHl deg -94.43 -148.64 -90.23 -154.53 ωH+ deg/sec 166.67 288.46 416.67 701.25
Absolute head Angle
ωH- deg/sec -187.50 -269.23 -458.33 -725.00 θHSr deg 81.10 71.06 76.96 72.74 θHSl deg -84.46 -72.72 -81.69 -73.65
RSIHS - 0.96 0.98 0.94 0.99 ωHs+ deg/sec 158.33 145.83 395.83 362.50 ωHS- deg/sec -187.50 -114.58 -437.50 -395.83
Relative head to shoulder
angle
VSIHS - 0.84 1.27 0.90 0.92
SUMMARY Aim of this study was to provide a reliable method for cervical spine biomechanical evaluation by using motion capture system. A new protocol for clinical assessment and reporting was formulated in terms of markers placement, test procedures and data processing. Head rotational axis path, speed and ROM features might be related to injury background or to pathological disorders.
θH
θS
θHS
θH
θS
θHS
Figure 8: Paced test on healthy subject at 45 cycles/min, Restrained Shoulders. (a) Head absolute rotation, θH . (b) Shoulder absolute rotation, θS . (c) Head rotation relative to shoulders θHS .
Figure 7: Paced test on healthy subject at 45 cycles/min, Unrestrained Shoulders. (a) Head absolute rotation, θH . (b) Shoulder absolute rotation, θS . (c) Head rotation relative to shoulders θHS .

DISCUSSION
Several definitions and data representations, like polar plots and symmetry indexes, were introduced in the present work: some of them were conventional and oriented to the development of a set of clinical tools useful to an immediate quantitative evaluation of tests results. The polar plot of angular velocity versus angle of rotation may result particularly efficient to the clinical staff and to patients for motion representation. The symmetry indexes were introduced to give a synthetic quantification on information commonly expressed by several angles and tables: speed indexes were proposed to go well beyond the common measure of static bilateral ROM and to help the clinical staff to evaluate the dynamic functional behaviour. Some results were not in agreement with ideal expectations. First of all, even for healthy subjects, the RSI resulted smaller than 1, as result of the presence of a dominant side, recurring movements and so forth. Secondly, the absence of a statistically significant difference between healthy and injured subjects was due to the small number of pilot tests and to the insufficient instruction to testers during the execution of the pilot tests. The proposed final protocol, with two paced tests at medium and high rotational speed has to be seen as a starting point to collect consistent and comparable data from a wide control group of healthy subjects and from injured volunteers: further development will regard the introduction of irregularity indexes like kurtosis and skewness for the evaluation of velocity peaks and the development of virtual reality games or predator-prey tasks to avoid most voluntary simulations and to evaluate the real functional ability and degree of rehabilitations of patients. CONCLUSIONS
The work presents a new protocol for cervical spine clinical evaluation in unconstrained axial head rotations using motion capture techniques. Results from a set of pilot tests on healthy and whiplash injured subjects are reported introducing polar plots of angular velocity versus head to shoulder rotation angle: the plots allow for an immediate evaluation whereas the Rotation Symmetry Index and the Velocity Symmetry Index give a quantification of the act. A new standardized protocol, based on natural angular velocity developed in the pilot tests, was introduced with paced head rotations at 20 and 45 cycles/min and results on healthy subjects are analysed. REFERENCES [1] Bari E., Analisi numerica del tratto lombare della
colonna vertebrale nella flesso-estensione isocinetica, Degree Thesis, Univesity of Padova, 1998 (in Italian).
[2] Panjabi M.M., Cholewicki J., Nibu K., Grauer J.N., Babat L.B., Dvorak J., Mechanism of whiplash injury, Clinical Biomechanics 1998, vol.13, pp. 239-249.
[3] Yoganandan N., Pintar F.A., Cusick J.F., Biomechanical analysis of whiplash injuries using an experimental model, Accident Analysis & Prevention 2002, vol.34, pp. 663-671.
[4] Cusick J.F., Yoganandan N., Biomechanics of the cervical spine 4: major injuries, Clinical Biomechanics 2002, vol 17, pp. 1-20.
[5] Bottazzo C., Analisi biomeccanica del tratto cervicale della colonna vertebrale e metodi numerici per lo studio della flessoestensione e rotazione libera, Degree Thesis, Univesity of Padova, 2003 (in Italian).
[6] Moroney S.P., Schultz A.B., Miller J.A., Andersson G.B., Load-displacement properties of lower cervical spine motion segments, Journal of Biomechanics 1988, vol.21, pp. 769-779.
[7] Lee S.W., Draper E.R.C., Hughes S.P.F., Instantaneous center of rotation and instability of the cervical spine, Spine 1997, vol.22, pp. 641-648.
[8] Bogduk N., Mercer S., Biomechanics of the cervical spine. I: normal kinematics, Clinical Biomechanics 2000, vol.15, pp. 633-648.
[9] Feipel V., Rondelet B., Le Pallec J.P., Rooze M., Normal global motion of the cervical spine: an electrogoniometric study. Clinical Biomechanics 1999, vol.14, pp. 462-470.
[10] Frobin W., Leivseth G., Biggemann M., Brinckmann P.A., Sagittal plane segmental motion of the cervical spine. A new precision measurement protocol and normal motion data of healthy adults, Clinical Biomechanics 2002, vol.17, pp. 21-31.
[11] Sforza C., Grassi G.P., Fragnito N., Turci M., Ferrario V.F., Three-dimensional analysis of active head and cervical spine range of motion: effect of age in healthy male subjects, Clinical Biomechanics 2002, vol.17, pp. 611-614.
[12] Harrison D.D., Janik T.J., Troyanovich S.J., Holland B., Comparison of lordotic cervical spine curvatures to a theoretical ideal model of the static sagittal cervical spine, Spine1996, vol.21, pp.667-675.
[13] Shea M., Edwards W.T., White A.A., Hayes W.C., Variation of stiffness and strength along the human cervical spine, Journal of Biomechanics 1991, vol.24, pp. 95-107.
[14] Nightingale R.W., Winkelstein B.A., Knaub K.E., Richardson W.J., Luck J.F., Myers B.S., Comparative strenghts and structural properties of the upper and lower cervical spine in flexion and extension, Journal of Biomechanics 2002, vol.35, pp.725-732.
[15] Bernhardt P., Wilke H.J., Wenger K.H., Jungkunz B., Böhm A., Claes L.E., Multiple muscle force simulation in axial rotation of the cervical spine, Clinical Biomechanics 1999, vol.14, pp. 32-40.
[16] Kettler A., Hartwig E., Schultheiß M., Claes L., Wilke H.J., Mechanically simulated muscle forces strongly stabilize intact and injured upper cervical spine specimens, Journal of Biomechanics 2002, vol 35, pp. 339-346.
[17] Choi H., Vanderby R., Muscle forces and spinal loads at C4-C5 level during isometric voluntary efforts, Medicine & Science in Sports & Exercise 2000, vol.32 (4), pp. 830-838.
[18] Brault J.R., Siegmund G.P., Wheeler J.B., Cervical muscle response during whiplash: evidence of a lengthening muscle contraction, Clinical Biomechanics 2000, vol.15, pp. 426-435.