A new approach to characterize postural deficits in ...
32
1 Preprint: Please note that this article has not completed peer review. A new approach to characterize postural deficits in chemotherapy-induced peripheral neuropathy and to analyze postural adaptions after an exercise intervention CURRENT STATUS: ACCEPTED Sarah Kneis Medical Center, University of Freiburg [email protected]Corresponding Author ORCiD: https://orcid.org/0000-0001-8350-8309 Anja Wehrle Medical Center, University of Freiburg Daniela Dalin Medical Center, University of Freiburg Isabella Katharina Wiesmeier Medical Center, University of Freiburg Johann Lambeck Medical Center, University of Freiburg Albert Gollhofer University of Freiburg Hartmut Bertz Medical Center, University of Freiburg Christoph Maurer Medical Center, University of Freiburg DOI: 10.21203/rs.2.16028/v1 SUBJECT AREAS Neurosurgery KEYWORDS
Transcript of A new approach to characterize postural deficits in ...

1
Preprint:Pleasenotethatthisarticlehasnotcompletedpeerreview.
Anewapproachtocharacterizeposturaldeficitsinchemotherapy-inducedperipheralneuropathyandtoanalyzeposturaladaptionsafteranexerciseinterventionCURRENTSTATUS:ACCEPTED
SarahKneisMedicalCenter,UniversityofFreiburg
[email protected]:https://orcid.org/0000-0001-8350-8309
AnjaWehrleMedicalCenter,UniversityofFreiburg
DanielaDalinMedicalCenter,UniversityofFreiburg
IsabellaKatharinaWiesmeierMedicalCenter,UniversityofFreiburg
JohannLambeckMedicalCenter,UniversityofFreiburg
AlbertGollhoferUniversityofFreiburg
HartmutBertzMedicalCenter,UniversityofFreiburg
ChristophMaurerMedicalCenter,UniversityofFreiburg
DOI:10.21203/rs.2.16028/v1
SUBJECTAREASNeurosurgery
KEYWORDS

2
Posturalstability,chemotherapy-inducedperipheralneuropathy,motorcontrol,sensoryweighting,model
3
AbstractBackgroundPosturalinstabilitypresentsacommonanddisablingconsequenceofchemotherapy-
inducedperipheralneuropathy(CIPN).However,knowledgeaboutposturalbehaviorofCIPNpatients
issparse.Withthispilotstudy,weusedanewapproachtoi)characterizeposturalimpairmentsas
comparedtohealthysubjects,ii)allocatepossibleabnormalitiestoasetofparametersdescribing
sensorimotorfunction,andiii)evaluatetheeffectsofabalance-basedexerciseintervention.
MethodsWeanalyzedspontaneousandexternallyperturbedposturalcontrolineightCIPNpatients
beforeandafterabalance-basedexerciseinterventionbyusingamodificationofanestablished
posturalcontrolmodel.Thesefindingswerecomparedto15matchedhealthysubjects.
ResultsSpontaneousswayamplitudeandvelocitywerelargerinCIPNpatientscomparedtohealthy
subjects.CIPNpatients’reactionstoexternalperturbationsweresmallercomparedtohealthy
subjects,indicatingthatpatientsfavorvestibularoverproprioceptivesensoryinformation.The
balance-basedexerciseinterventionup-weightedproprioceptiveinformationinpatients.
ConclusionsCIPNpatients’majorposturaldeficitmayrelatetounderuseofproprioceptiveinformation
thatresultsinalessaccurateposturecontrolasspontaneousswayresultsindicate.Thebalance-
basedexerciseinterventionisabletopartiallycorrectforthisabnormality.Ourstudycontributestoa
betterunderstandingofposturalimpairmentsinCIPNpatientsandsuggestsaneffectivetreatment
strategy.
1.IntroductionChemotherapy-inducedperipheralneuropathy(CIPN)isacommonandclinicallyrelevantside-effect
ofcancertreatment(1–3).CIPNcancausetreatmentdelaysanddosereductions,interferingwith
generaloutcomeorcompromisingsurvival(3–6).ConsequencesofCIPNcanleadtoexcessive
healthcarecostsandresourceuse(7).SymptomsofCIPNprimarilyincludeparaesthesia,dysesthesia,
numbnessandpainwithasymmetric,distal,length-dependent"gloveandstocking"distribution(3,8)
andlimitpatients’everydaylifeconsiderably.Additionally,CIPNpatientsoftensufferfrompostural
instability(9–17),contributingtoalowerqualityoflife(5,18),ahigherriskofmortality(19–22)and
increasedhealthcarecosts(23,24).

4
QuantitativereportsaboutCIPNpatients’posturalinstabilityarecurrentlyrising:CIPNhasbeen
associatedwithreducedgaitabilities(13,14)andchangesincenterofpressure(COP)displacements
(10,12,25).However,underlyingmechanismsaresparselydescribed(10,25):Wampleretal.(10)
assumedthatbesidessomatosensoryimpairmentsalsodiminishedvestibularfunctioncauses
increasedposturalswayinCIPNpatients.Furthermore,inanearlierstudywefoundchangesin
elicitabilityandsensitivityofspinalreflexcircuitryassociatedwithposturalinstabilityinCIPNpatients
(25).Morecomprehensiveknowledgeaboutneuropathy-inducedposturalinstabilityhasbeenderived
frompatientsdiagnosedwithdiabetes:Bonnetetal.(26)deducedlargerCOPdisplacements,which
weremorepronouncedwithvisualdisturbance.Diabeticneuropathypatientsseemtodelaypostural
reactions(27),shiftfromankletohipstrategy(26,28,29),andseemtousevestibularratherthan
proprioceptivecues(30).However,proprioceptionmaybeessentialforstabilityinbothquietstance
andduringunexpectedposturalperturbations(26,31–33),sinceitprovidesinformationaboutlower
limborientationwithrespecttothesupportbase(34,35).Theyreportaclearincreaseinpostural
swaywhenproprioceptivecuesaredeficient(10,26,32).Ourfirstaimhereistocharacterizethe
posturaldeficitsinCIPNandtoextractthesensorimotorabnormalitiesusingawell-establishedmodel
ofposturalcontrol(36–38).
Concerningtreatment,knowledgeaboutthemanagementofCIPN-inducedposturalinstabilityisstill
sparse(39–41).Generally,itisincreasinglysuggestedtofocusonstrengthandespeciallybalance
exercisesinordertoimprovephysicalfunctioningofCIPNpatients(11),whatwecouldconfirmina
randomizedcontrolledtrialbyourselves(42).Untilrecently,thereareonlytwootherinterventional
studiesshowingthatbalanceexercisesimprovedCIPN-relatedposturalcontroldeficits(39,41).
However,evidencefromdiabetesresearchonneuropathyfurthersupportsthisassumption(43–45).
Balancetrainingingeneralhasproventoenhanceposturalstabilitybyinducingneuronaladaptations
andimprovingmuscularoutput(46,47).Hence,weaimedtoimplementabalance-basedexercise
interventionforCIPNpatients.
Insum,thepresentstudywasundertakentoi)specifytheposturalabnormalitiesassociatedwith
CIPNduringspontaneousandexternallyperturbedstance,ii)toidentifytheunderlyingsensorimotor

5
malfunction,andiii)tomonitortheeffectofabalance-basedexerciseinterventioninapilotapproach.
2.Methods2.1.Patients
Thepresentpilotstudyprovidestwoapproaches:across-sectionalapproachtoidentifypostural-
controldifferencesbetweenCIPNpatientsandmatchedhealthycontrolsubjectsandaone-armed
longitudinalapproachtoevaluatetheeffectsofabalance-basedexerciseinterventiononCIPN-related
posturaldeficits.
Therefore,weexaminedeightcancerpatientswithdifferentcancerlocalizationsandtreatment
status,allreportingsevereneuropathysymptomsduetochemotherapy(CIPN).Thechemotherapies
appliedentailedtheneurotoxicagentsbortezomib,carboplatin,cisplatin,paclitaxal,docetaxaland
vincristine.Noneofthepatientshadanyneuropathysymptombeforetheapplicationofneurotoxic
agents.CIPNwasclinicallyandelectrophysiologicallyconfirmedinallpatients.Moreover,weassessed
patients’subjectiveCIPNsymptomsviatheneurotoxicitysubscale(NtxS)ofFACT&GOG(Functional
AssessmentofCancerTherapy/GynaecologyOncologyGroup)scoredfrom0–44(0=severe
symptoms;44=nosymptoms);Table1summarizesourpatients’clinicalinformation.
Weexcludedpatientswithotherpossiblesourcesofneuropathy(eghereditary,diabetes-oralcohol-
induced)andpatientssufferingfromadditionaldeficitsthatmightinteractwiththeirposturalcontrol
suchasarelevantreductionofmuscularstrengthorcertaincomorbidities(egosteolysis,severe
vertebraldegeneration,vestibulardeficits).Specifically,allpatientsunderwentdetailedvestibular
testingusingarotatingchair.Inaddition,patientsperformedanincrementalstresselectrocardiogram
onastationarybicycleintheInstituteforExercise-andOccupationalMedicine,MedicalCenter–
UniversityofFreiburginordertoexcludecardiovascularrisksduringexerciseandtodeterminethe
lactatethresholdforexercisecontrol.
Thecontrolgroupfortheposturalcontrolexperimentsconsistedof15healthysubjectsmatchedto
patients’age,weightandheight.Patientsunderwentassessmentsofposturecontroltwice(before
andafter12weeksofasupervisedexerciseintervention)whilehealthycontrolsubjectsunderwent
theassessmentonlyonce.

6
Patients'recruitmentanddatacollectiontookplaceintheClinicofInternalMedicineIandposture
analysesandclinicalassessmentstookplaceintheDepartmentofNeurologyandClinical
Neurophysiology,MedicalCenter–UniversityofFreiburg.
ThestudywasapprovedbytheEthicsCommissionofUniversityofFreiburg.Allsubjectsprovided
writteninformedconsenttotheexperimentalprocedureinaccordancewiththeDeclarationof
Helsinki.
2.2.Intervention
Theone-on-onetrainingsessionstookplaceinthedivisionofSportsOncologyintheClinicofInternal
MedicineI,twiceperweekover12weeks.Theinterventionprotocolincludedacardiovascularwarm-
upofupto20minutesonastationarybicyclewithanintensityof75–80%ofmaximumheartrate,
followedbythebalance-basedexercisesfor30minutesandmuscularendurancetrainingforthemain
musclegroups.Themainfocuswasonthebalancepartofthetraining.Balancetrainingprescription
includedaprogressiveincreaseovertheinterventionperiodintheexerciseamount(threetoeight
exerciseswiththreerepetitionseachà20–30s)anddifficultybyreducingthesupportsurfaceand
visualinput,addingmotor/cognitivetasksandinducinginstabilitytostimulatethesensorimotor
systemadequately(46,48).Wedocumentedvitalparameters,trainingprogress,andreasonsfor
missedsessions.
2.3.Procedureanddataanalysis
Forevaluatingposturalcontrol,spontaneousswayandperturbedstanceweremeasuredwitha
custom-builtmotionplatform(49,50)undertwovisualconditions,witheyesopenandwitheyes
closed.Eachtriallastedoneminute.Theparticipantsweretoldtostanduprightontheplatformin
comfortableshoes.Stancewidthwaspredeterminedwithinamarkedarea.Forsafetyreasons,
participantshadtoholdtworopeshangingfromtheceilinginacrossed-armspositionsothatthey
couldnotperceiveasomatosensoryspatialorientationsignal(Figure1D).
Dataanalysiswasconductedoff-linewithcustom-madesoftwareprogrammedinMATLAB®(The
MathWorksInc.,Natick,MA,USA).
Spontaneousswaywasmeasuredonthenon-movingplatform.Thecenterofpressure(COP)sway

7
pathwasdetectedwithaforcetransducingplatform(Figure1E-G,Kistlerplatformtype9286,
Winterthur,Switzerland).FromtheCOPexcursionsovertimeinanterior-posterior(ap)andmedio-
lateral(ml)swaydirections,wecalculatedtherootmeansquare(RMS)aroundthemeanCOP
position.Afterdifferentiatingthetimeseries,wecalculatedmeanvelocity(MV).Inaddition,center
frequency(CF)wasextractedfromthepowerspectrum(51,52).
Perturbedstancewasmeasuredonthemovingplatformtodifferentiatesensorycontributionsin
reactiontoexternaldisturbances.Weanalyzedrotationaltiltsinthesagittalplanewiththetiltaxis
passingthroughtheparticipant’sanklejoints.Platformrotationsweredesignedaspseudorandom
stimuli(PRTS,pseudorandomternarysequence,seeFigure1C)(53).ThePRTSstimulushasawide
spectralbandwidthwiththevelocitywaveformhavingspectralandstatisticalproperties
approximatingawhitenoisestimulus(53).Assuch,thisstimulusappearedtobeunpredictabletothe
testsubject.Weappliedtwopeakangulardisplacements(stimulusamplitude:0.5°and1°peak-to-
peak)andanalyzedatelevenstimulusfrequencies(0.05,0.15,0.3,0.4,0.55,0.7,0.9,1.1,1.35,1.75
and2.2Hz).
Angularexcursionsofthelower(hip-to-ankle:hipmovement)andupper(shoulder-to-hip:shoulder
movement)bodysegmentsandtheplatforminspaceweremeasuredusinganoptoelectronicmotion-
measuringdevicewithmarkersattachedtoshoulderandhip(Optotrak3020,Waterloo,Canada).
Eachmarkerconsistedofthreelight-emittingdiodes(LED)fixedtoarigidtriangle.Thetriangleswere
fixedtotheparticipant’shipsandshouldersandtoarigidbarontheplatform(Figure1D).3-DLED
positionsofthetriangleswereusedtocalculatemarkerpositions(Figure1A,B).Optotrak®and
Kistler®outputsignalsaswellasthestimulussignalsweresampledat100Hzusingananalogue-
digitalconverter.WerecordedalldatawithsoftwareprogrammedinLabView®(National
Instruments,Austin,Texas,USA).
Toanalyseposturalreactionsinrelationtoplatformstimuli,transferfunctionsfromstimulus-response
datawerecalculatedviaadiscreteFouriertransform.Fouriercoefficientsofstimulusandresponse
timeseriesareusedtodetermineGAINandPHASEwithrespecttostimulusfrequencies.GAIN
representsthesizeoftheposturalreactionasafunctionofstimulussize(platformangle),while

8
PHASEisrelatedtotherelativetimingbetweenposturalreactionandstimulus(54).
Furthermore,wecalculatedCOHERENCE,ameasureofreproducibilityoftheresponse.Whereasa
COHERENCEvalueofonereflectsperfectreproducibility,avalueofzeromeansnoreproducibilityat
all.
insertFigure1.
2.4.Parameteridentification
Transferfunctionsservedastheexperimentaldatabasisformodelsimulationsusingaspecific
versionofanestablishedposturalcontrolmodel(36,49,53,55–57)withactivetime-delayed
proportional,derivative,andintegralfeedbackaswellaspassivestiffnessanddampingtoextract
basicconstituentsofposturalcontrol.Thephysicalpartofthemodelisasingleinvertedpendulum
modelwithcorrectivetorqueappliedattheanklejoint.Themodelusedhereincludesanegative
feedbackloopthatrelatesbodyexcursiondetectedbyvisual,vestibular,andproprioceptivesensors
toacorrectivetorqueviaaneuralcontroller.Withthehelpofanautomatedoptimizationtool
(fmincon,MATLAB®,TheMathWorksInc.),whichminimizedthedifferencebetweenexperimentaland
simulatedGAINandPHASEcurves,weestimatedtheneuralcontroller’sparameterswithproportional
(Kp),derivative(Kd)andintegral(Ki)contributions(PDI-controller).Neuralcontrollergainsare,in
part,determinedbymassandheightofeachsubject’scenterofmass(COM).(53)Peterka,2002)
Becauseourcontrolgrouppresentedlowermassesandheightsthanpatients,wehadtocorrect
neuralcontrollergainsforthiseffect.Thatiswhyweprovidenumbersfor(Kp/mgh),(Kd/mgh),and
(Ki/mgh),where(mgh)representsthegravitationalpull(mass)x(gravitationalconstant)x(heightof
COM).Moreover,wederivedtimedelay(Td),proprioceptivesensoryweight(Wp),andbiomechanical
elasticity(Ppas)anddamping(Dpas)ofthemusclesandtendons.Wefittedmodelsimulationsto
experimentaltransferfunctionsunderdifferentstimulusamplitudesandvisualconditions.
2.5.Statistics
StatisticalanalyseswereperformedusingMicrosoftExcel,JMP®andStatview(SASInstituteInc.,
Cary,NC,USA).Weappliedparametricmethodsaftertestingthenormaldistributionand
homogeneityofvarianceswiththeKolmogorov-Smirnovtest.Duetotheexpecteddependency

9
betweenexperimentalconditionsandoutcomemeasures,statisticalsignificancewastestedbyan
analysisofvariance(ANOVA)forthecomparisonofhealthysubjectsandpatients.Visualcondition,
swaydirection,andbodysegment(hip,shoulder)werethewithin-subjects’factorsforspontaneous
sway.Forperturbedstance,weappliedvisualcondition,stimulusamplitude,stimulusfrequency,and
bodysegment(hip,shoulder)aswithin-subjects’factors.Fortheanalysisofthebalancebased
exerciseinterventioneffectonpatients,weusedamultivariateanalysisofvariance(MANOVA)witha
timeastherepeatedmeasurevariable,inaddition.Thelevelofstatisticalsignificancewassetat
p=0.05.
3.ResultsNoadverseeventswereobservedduringthestudyperiod.Theinterventioncomplianceintermsof
numberofsessionsperformedbythepatientswas70.1%,mainlyduetotheunderlyingdisease.
3.1.Spontaneoussway
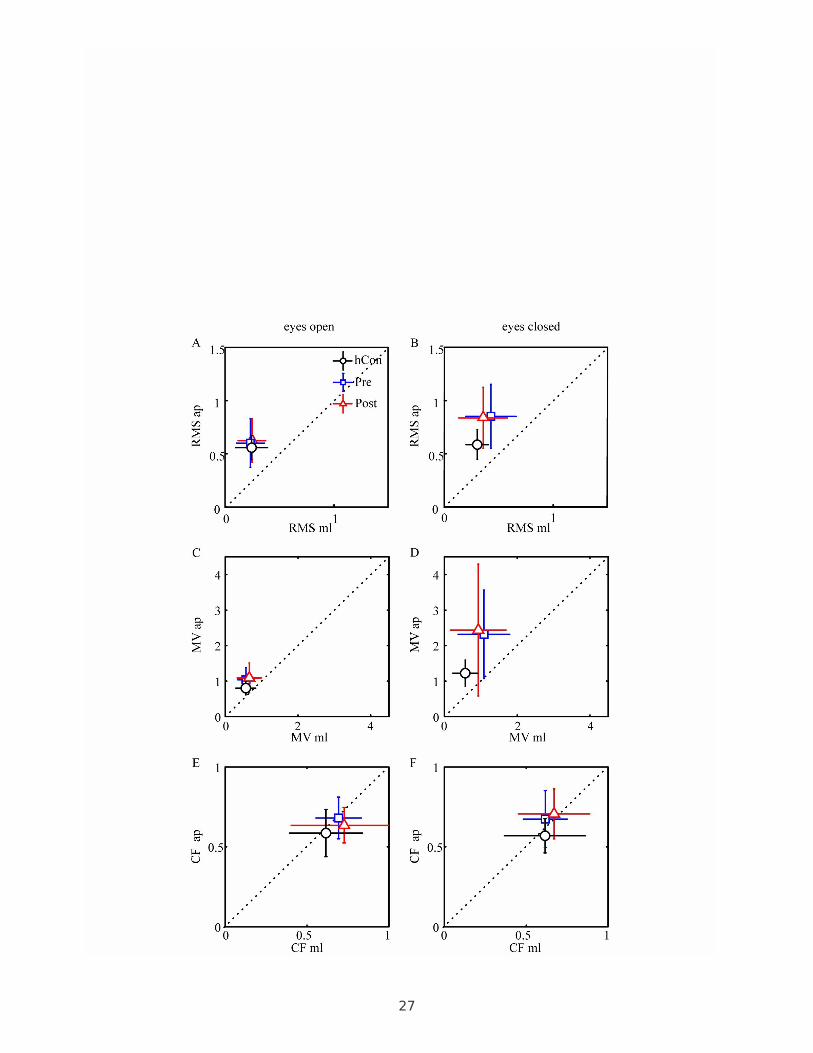
ThepatientgroupbeforeinterventiondisplayedasignificantlylargerCOPRMSthancontrolsubjects
(Figures2A-BandTable2).Groupdesignationsignificantlyinteractedwithswaydirection,iethe
differencebetweencontrolsubjectsandCIPNpatientsislargerinapdirection.Moreover,group
designationsignificantlyinteractedwithvisualcondition,duetothelargeRMSinpatientswitheyes
closed.Afterintervention,thepatients’RMStendedtobesmaller(beforeintervention0.533cm;after
it0.501cm;F=2.98;p<0.088).
AswithRMS,thepre-interventionMVofthepatientgroupwassignificantlylargerthanincontrol
subjects(Figures2C-D,Table2).Thegroupdesignationsignificantlyinteractedwithvisualcondition
(seeTable2):MVvaluesdidnotdifferbetweengroupsintheeyes-opencondition,whereasthe
patients’MVwassignificantlylargerintheeyes-closedcondition.MVdidnotchangeafter
intervention.
CFdidnotdiffersignificantlybetweenpatientsandcontrolsubjects(Figures2E-F,Table2).
Furthermore,patientsdisplayednointerventioneffectsonCF.
[insertFigure2.]
3.2.Perturbedstance

10
ThetransferfunctionbetweenplatformtiltandbodyangulardisplacementischaracterizedbyGAIN
andPHASEbehavior.
Thedisturbance-inducedbodysway,ieGAINwassignificantlysmallerinpatientsbeforeintervention
(1.57)comparedtocontrolsubjects(1.87;F=62.3;p<0.0001;Fig.3A)andincreasedafter
intervention(1.63;F=18.0;p<0.0001;Fig.3A,Fig.4A-D).Furthermore,groupdesignationinteracted
significantlywithstimulusfrequency(F=3.70;p<0.0001),duetoadistortionofthetransferfunction
(Fig.3A,Fig.4A-D).Moreover,controlsubjects'GAINislargerwithclosedeyesthanopeneyes
whereaspatients’GAINwasalmostsimilarindependentofthevisualcondition:groupdesignation
significantlyinteractedwithvisualcondition(eyesopen:controlsubjects1.58;patientsbefore
intervention1.46;afterintervention1.51;eyesclosed:controlsubjects2.15;patientsbefore
intervention1.67;afterintervention1.74;visualcondition:F=25.6;p<0.0001,Fig.3D,Fig.4A-D).
Thedifferencebetweenshoulderandhipswayasafunctionofplatformtiltswasgreaterincontrol
subjectsthaninpatients(Fig.3E,Fig.4A-D):withasignificantinteractionbetweengroupdesignation
andbodysegment(F=2.85;p=0.022).Groupdesignationandstimulusamplitudedidnotinteract
significantlyastheeffectofstimulusamplitude(non-linearity)onGAINdidnotdifferbetweengroups.
ThePHASElaginthepatients’groupbeforeinterventionwasslightlybutsignificantlylesspronounced
thaninthecontrolgroup(controlsubjects-118.3;patients-107.6,F=10.3;p<0.0001;Fig.3B).After
intervention,PHASEchangedsignificantlyandfellintherangeofthecontrolsubjects’values(-121.3;
F=15.4;p<0.0001;Fig.3B).Groupdesignationsignificantlyinteractedwithvisualcondition(F=4.45,
p=0.01,Fig.3F),bodysegment(F=13.1,p<0.0001,Fig.3G),andstimulusamplitude(F=9.89,
p<0.0001).Theinteractionwithvisualconditionisbasedonthefactthatpatientswithopeneyes
displayedaPHASEadvanceof20degreeswithrespecttocontrolsubjects,whereastherewasno
significantPHASEdifferencebetweenpatientsandcontrolsubjectswitheyesclosed.Theinteraction
withbodysegmentisbasedonthefactthatthedifferencebetweenshoulderandhipPHASEwas
largerincontrolsubjectsthaninpatients.Theinteractionwithstimulusamplitudeisbasedona
pronouncedphasedifferencewithsmallstimulusamplitudes.Groupdesignationandstimulus
frequencydidnotinteractsignificantly(F=0.41;p=0.99):thePHASEeffectsweredistributedequally

11
acrossallfrequencies.
COHERENCEasameasureforthereproducibilityoftheresponsewassmallerinpatientsbefore
intervention(0.43)comparedtocontrolsubjects(0.50;F=103;p<0.0001;Fig.3C).COHERENCEdid
notchangeafterintervention(0.45).However,COHERENCEsignificantlyvariedwithstimulus
amplitude,frequency,visualcondition,andbodysegment,similarlyinbothgroups.
[insertFigure3and4.]
Thefollowingresultsarederivedfromthemodel-basedparameteridentificationprocedure(Fig.5D),
andpresenttherelevantparameterdifferencesbetweenpatientsandcontrolsubjects.
Therewasnosignificanteffectfortheintegralpartoftheneuralcontroller(Ki),aswellasforthe
proportional(Kp)andderivativepart(Kd)oftheneuralcontroller.
ThesensoryweightingfactorWpdifferedsignificantlybetweenpatientsandcontrolsubjects(F=9.89,
p=0.0001;Fig.5B).Whereaspatientsrelywithanaveragefactorof0.53onproprioceptivecuesand
hence0.47onspatialcues,controlsubjectsrelywithafactorof0.67onproprioceptiveand0.33on
spatialcues.Afterintervention,therewasasmallbutsignificantchangetowardscontrolsubjects(Wp
0.56,F=9.13,p=0.006).Groupdesignationdidnotinteractwithvisualconditionorstimulus
amplitude.
Thetimedelaybetweenstimulusandresponse(Td)didnotdiffersignificantlybetweenpatientsand
controlsubjects(F=1.10;p=0.34;Fig.5C).However,wedidnoteatendencytowardslargertime
delaysinpatientsbeforeintervention(175ms)comparedtocontrolsubjects(167ms)andpatients
afterintervention(168ms).
Parametersrelatedtopassivemuscleandtendonbehavior(PpasandDpas)didnotdiffersignificantly
betweengroupsandwerenotaffectedbytheintervention.
[insertFigure5.]
4.DiscussionAsposturalinstabilityisamomentoussymptomofCIPN(9–16),thefirstaimofthisstudywasto
assessthespecificsetofposturalcontroldeficitsassociatedwithCIPNcomparedtohealthysubjects.
Furthermore,sinceCIPNtreatmentoptionsareverylimitedsofar(3)andhintsintherecentliterature

12
indicatethatCIPNpatientsmightbenefitfromexercising(39,41,58),weevaluatedabalance-based
exerciseinterventionaimingtotreatpatients'functionalimpairmentsduetoCIPN.Whileformer
studiesmostlyinvestigatedspontaneousswaymeasures(displacement-,velocity-,andfrequency-
relatedmeasures),weaimedtodescribeCIPNpatients'sensorimotorbehaviorinmuchgreaterdetail
andtherefore,weadditionallygeneratedtransferfunctionsofpatients’behaviorasafunctionof
stanceperturbationwithpseudorandomstimulitoachieveourobjectives.
Concerningspontaneoussway,wefoundgreaterposturalswayinCIPNpatientssimilarlytoprevious
CIPNstudies(10,12,14,39).Additionally,ourfindingscorrespondtothatofothertypesofneuropathy.
Forexample,manyworkinggroups(59–63)reportincreasedRMSandMVinpatientswithdiabetic-
inducedneuropathy.Inourstudy,RMSandMVweresignificantlylargerinCIPNpatientsthanin
healthysubjects.Moreover,weobservedaspecificpreponderanceofdeficitsinanterior-posterior
direction(60)andamorepronouncedposturalswaywithclosedratherthanopeneyes(60,61).
Generally,closingtheireyescausessubjectstousevestibularandproprioceptivecuesforcontrolling
balance.Asproprioceptiveinformationareoftendeficientinneuropathypatients(26),itseems
reasonabletoassumethatpatientsmayprefervestibularoverproprioceptivecues.However,itiswell
knownthatthevestibularsignalcarriesalargeramountofnoisethantheproprioceptivesignal(64)
leadingtolessaccurateposturecontrol.Wespeculateatthispointthatthemainsourceforthelarger
RMSandMVisrelatedtoasensoryshifttowardsvestibularcues(seebelowsensoryweighting,and
Horaketal.(65)).Ifthatistrue,wemightbeabletorecoverthisfindingwhendissociating
proprioceptivefromvestibularframesoforientationusingplatformtilts.Whereasproprioceptivecues
maydragthebodyalongplatformmovements,quantifiedbyarelativelargerGAINastransfer
functionbetweenbodyexcursionsandplatformtilts,vestibularcueswouldstabilizethebodyin
space,quantifiedbyarelativesmallerGAIN.Infact,CIPNpatientspresentedsmallerGAINvalues
sincetheirreactiontoplatformtiltswerelesspronouncedthanthatofcontrolsubjects.Thus,they
mightratherusespacecoordinatesthanplatformmovementsforposturecontrol.Furthermore,GAIN
wassignificantlyaffectedbyvisualconditionandbodysegment.ThelargerGAINdifferencebetween
CIPNpatientsandcontrolsubjectsintheeyes-closedcomparedtotheeyes-openconditionsuggests

13
thatunder-usageofproprioceptionisdominantwhentherearelessadditionalorientingcues.
Moreover,thefindingofrelativelysmallGAINsinCIPNpatients’lowercomparedtotheirupperbody
segmentpointtoaslightlydifferentintersegmentalstrategy(29).OurPHASEfindings,representing
therelativetimingbetweenposturalreactionandstimulusalsopointtoadifferentintersegmental
behaviorintermsofupperwithrespecttolowerbodyangulardisplacements(26,28,29).Weassume
thatpatientsproactivelyorientatethemselves,especiallytheirupperbody,moretowardsspace
coordinates.ThisalsoindicatesanespeciallylowuseofproprioceptionaccordingtoourGAINresults.
Moreover,wespeculatethatCIPNpatientsproactivelyassumeasafetystrategythatmayfollowan
enhancedmuscleco-contraction(25),leadingtosmallerbodyexcursions.However,greaterco-
contractionlimitsone’sabilitytopreciselycontrolposture(66,67).
Toaddressthetransfer-functionabnormalitiesinCIPNpatients,wefittedthesubjects’dataviaa
simplefeedbacksystem(36,56,64,68).Usingthemodel-basedparameterestimation,weidentified
andquantifiedtheCIPNpatients’diminisheduseofproprioceptivecues:Thesensory-weightingfactor
forproprioception(Wp)issignificantlysmallerinCIPNpatientsthanincontrolsubjects.However,
patientsdidnotpresentadifferenterrorcorrectiongain(KpandKd)ofthefeedbackloop.
Furthermore,parametersrelatedtopassivemuscleandtendonbehavior(passivestiffnessand
damping,KpasandBpas)didalsonotdifferbetweenCIPNpatientsandcontrolsubjects.Thisseems
tobeinlinewiththenotionthatdifferencesinposturalcontrolbetweenCIPNpatientsandhealthy
subjectsmainlyrelyonthedifferentuseofsensorycues.Moreover,thisfindingmightindicatethat
musclesandtendonswerenotaffectedsupportingCIPN'sprimarilysensorycharacteristic.
HowdoestheexerciseinterventioninfluenceCIPNpatients’behavior?Interestingly,weobservedthat
CIPNpatients’mainabnormality(down-weightedproprioception)wasmodifiedbyexercise
intervention.CIPNpatients’GAINandPHASEvaluesapproachedthoseofhealthysubjectsduetothe
proprioceptiveup-weightingmentionedabove.Interestingly,theeffectofup-weightingproprioception
istheonlysignificantmodel-basedparametermodificationafterintervention.WhywouldCIPN
patientsprofitfromup-weightingproprioceptionwhilesufferingfromasupposedproprioceptive
deficit?Ourclinicalassessmentsdidnotsufficetoconclusivelyspecifyneurallesionsoridentify

14
CIPN'snervefibercontributionoccurringinourpatients.However,allpatientssufferedfromstrong
paresthesiaandreportedsignificantbalanceproblemsconfirmedbyourspontaneoussway
experiments.CIPNsensorysymptomsaredescribedtoreferto‘terminalarbordegeneration’andthe
preferentialdamageofmyelinatedprimaryafferentsensorynervefibers(2,69).Therefore,we
speculatethatpatients'peripheralinformationandsubsequentstimulusconductionarealtered,but
notcompletelydysfunctional.Thedown-weightingofproprioceptivecuescouldbeinterpretedasan
excessivecompensatorymechanism,whichletsCIPNpatientspre-interventionremaininasuboptimal
state.Theexerciseinterventionmaythuspartiallycorrectthisexcessandmaystimulatetheuseof
lessdamagedpathways.Asasideeffectofproprioceptiveup-weighting,theinterventionmaytrigger
down-weightingofvestibularcues,therebyreducingvestibularnoise.Asaconsequence,postural-
controlbehaviormightbemoreaccurateintermsoflessvariability.
Conclusively,wemaintainthatup-weightingproprioceptionandtherebydown-weightingvestibular
informationtowardsthebehaviorofhealthysubjectsrepresentsaclearbenefitforCIPNpatients.The
proprioceptivecueisconsideredtobemoreaccuratethanvestibularcuesforposturalstability(64).
Regardingtimedelay,patientsafterinterventiontendedtoimprovetheirreactiontimebetween
stimulusandresponse.WealsoidentifiedatendencyofspontaneousswayRMSvaluestobesmaller
afterintervention,beinginlinewithposturalswayfindingsafterbalancetraininginastudyof
Schwenketal.(39).Although,ourinterventioneffectsaresmall,weareconvincedthatCIPNpatients
benefitfromexercisingintermsofimprovedposturebehavoirthatsubstantiallycontributesto
patients'functionalstatus.Functionalperformanceisanacknowledgedprognosisfactorforcancer
survivor(70)whywestronglyproposetoverifyourinterventionresultsinagreaterrandomized
controlledtrial.Ourfindingsarelimitedbythesmallsamplesizeandthelackofpatientcontrol
group.Furthermore,expandingneurophysiologicalassessmentswouldprovideinsightsinadaptive
processesunexaminedinthisstudy.
5.ConclusionWebelievethatournewapproachcontributedtoadeeperunderstandingofCIPNpatients’postural
instability.Proprioceptivedown-weightingmightrepresentthemainposturaldeficitinCIPN.Our

15
exerciseinterventiontargetedspecificallythisabnormalitypresumablybyprimarilycorrectingthe
overactivecompensation,whichledtoasignificantimprovementinposturalstability.Webelievethat
abalance-basedexerciseinterventionisapromisingstrategytomanagefunctionalimpairmentsdue
toCIPNandthatitshouldthereforeberoutinelyintegratedwithinthetreatmentregimensofpatients
receivingneurotoxicagents.
6.Abbreviationsapanterior-posterior
CFcenterfrequency
CIPNchemotherapy-inducedperipheralneuropathy
COPcenterofpressure
Dpaspassivedamping
Kdderivativecontributionoftheneuralcontroller
Kiintegralcontributionoftheneuralcontroller
Kpproportionalcontributionoftheneuralcontroller
NtxSneurotoxicitysubscaleofFACT&GOG
mlmedio-lateral
MVmeanvelocity
Ppaspassivestiffness
RMSrootmeanssquare
Tdtimedelay
Wpproprioceptivesensoryweight
7.Declarations7.1.Ethicsapprovalandconsenttoparticipate
ThisstudywasapprovedbytheEthicsCommitteeoftheUniversityofFreiburg(478/11).All
proceduresperformedinstudiesinvolvinghumanparticipantswereinaccordancewiththeethical
standardsoftheinstitutionaland/ornationalresearchcommitteeandwiththe1964Helsinki
declarationanditslateramendmentsorcomparableethicalstandards.Writteninformedconsentwas

16
obtainedfromallindividualparticipantsincludedinthestudy.
7.2.Consentforpublication
Notapplicabl
7.3.Availabilityofdataandmaterial
Thedatasetsupportingtheconclusionsofthisarticleisincludedwithinthisarticle.Thedatathat
supportthefindingsofthisstudyareavailablefromthecorrespondingauthoruponreasonable
request.
7.4.Competinginterests
Theauthorsdeclarethattheresearchwasconductedintheabsenceofanycommercialorfinancial
relationshipsthatcouldbeconstruedasapotentialconflictofinterest.
7.5.Funding
SK,AWandCMcontributedtotheconceptionofthework,todataacquisition,analysisand
interpretation,wrotethefirstdraftandrevisedit.IW,DD,andJLcontributedtodataacquisitionand
analysisandrevisedtheworkcritically.AGandHBcontributedtothedesignoftheworkandrevised
itcritically.Allauthorsapprovedthefinalversionofthisarticleandagreetobeaccountableforall
aspectsoftheworkinensuringthatquestionsrelatedtotheaccuracyorintegrityofanypartofthe
workareappropriatelyinvestigatedandresolved.
7.6.Authors'contributions
SK,AWandCMcontributedtotheconceptionofthework,todataacquisition,analysisand
interpretation,wrotethefirstdraftandrevisedit.IW,DD,andJLcontributedtodataacquisitionand
analysisandrevisedtheworkcritically.AGandHBcontributedtothedesignoftheworkandrevised
itcritically.Allauthorsapprovedthefinalversionofthisarticleandagreetobeaccountableforall
aspectsoftheworkinensuringthatquestionsrelatedtotheaccuracyorintegrityofanypartofthe
workareappropriatelyinvestigatedandresolved.
7.7.Acknowledgements
Weacknowledgethecooperationandtrainingimplementationofsports-andphysiotherapistsofthe
SportsOncologyofDepartmentofMedicineI,MedicalCenter–UniversityofFreiburgandwethank

17
thepatientsandcontrolindividualsfortheircollaboration.
8.References1.ArgyriouAA,KyritsisAP,MakatsorisT,KalofonosHP.Chemotherapy-inducedperipheralneuropathy
inadults:acomprehensiveupdateoftheliterature.CancerManagRes.2014;6:135–47.
2.HanY,SmithMT.Pathobiologyofcancerchemotherapy-inducedperipheralneuropathy(CIPN).
FrontPharmacol.2013Dec18;4:156.
3.HershmanDL,LacchettiC,DworkinRH,SmithEML,BleekerJ,CavalettiG,etal.Preventionand
ManagementofChemotherapy-InducedPeripheralNeuropathyinSurvivorsofAdultCancers:
AmericanSocietyofClinicalOncologyClinicalPracticeGuideline.JClinOncol.2014Jun
20;32(18):1941–67.
4.Gutiérrez-GutiérrezG,SerenoM,MirallesA,Casado-SáenzE,Gutiérrez-RivasE.Chemotherapy-
inducedperipheralneuropathy:clinicalfeatures,diagnosis,preventionandtreatmentstrategies.Clin
TranslOncolOffPublFedSpanOncolSocNatlCancerInstMex.2010Feb;12(2):81–91.
5.StubblefieldMD,BursteinHJ,BurtonAW,CustodioCM,DengGE,HoM,etal.NCCNtaskforce
report:managementofneuropathyincancer.JNatlComprCancerNetwJNCCN.2009Sep;7Suppl
5:S1–26;quizS27-28.
6.WindebankAJ,GrisoldW.Chemotherapy-inducedneuropathy.JPeripherNervSyst.2008;13(1):27–
46.
7.PikeCT,BirnbaumHG,MuehlenbeinCE,PohlGM,NataleRB.Healthcarecostsandworklossburden
ofpatientswithchemotherapy-associatedperipheralneuropathyinbreast,ovarian,headandneck,
andnonsmallcelllungcancer.ChemotherResPract.2012;2012:913848.
8.AsburyA,ThomasP.PeripheralNerveDisorders2.Butterworth-Heinemann;1995.336p.
9.TofthagenC,OvercashJ,KipK.Fallsinpersonswithchemotherapy-inducedperipheralneuropathy.
SupportCareCancer.2012;20(3):583–9.
10.WamplerMA,ToppKS,MiaskowskiC,BylNN,RugoHS,HamelK.QuantitativeandClinical
DescriptionofPosturalInstabilityinWomenWithBreastCancerTreatedWithTaxaneChemotherapy.
ArchPhysMedRehabil.2007Aug;88(8):1002–8.

18
11.Winters-StoneKM,HorakF,JacobsPG,TrubowitzP,DieckmannNF,StoylesS,etal.Falls,
Functioning,andDisabilityAmongWomenWithPersistentSymptomsofChemotherapy-Induced
PeripheralNeuropathy.JClinOncol.2017Aug10;35(23):2604–12.
12.HermanHK,MonfortSM,PanXJ,ChaudhariAMW,LustbergMB.Effectofchemotherapy-induced
peripheralneuropathyonposturalcontrolincancersurvivors.JClinOncol.2017Feb
10;35(5_suppl):128–128.
13.MarshallTF,ZippGP,BattagliaF,MossR,BryanS.Chemotherapy-induced-peripheralneuropathy,
gaitandfallriskinolderadultsfollowingcancertreatment.JCancerResPract.2017Dec1;4(4):134–
8.
14.MonfortSM,PanX,PatrickR,RamaswamyB,WesolowskiR,NaughtonMJ,etal.Gait,balance,and
patient-reportedoutcomesduringtaxane-basedchemotherapyinearly-stagebreastcancerpatients.
BreastCancerResTreat.2017Jul1;164(1):69–77.
15.GewandterJS,FanL,MagnusonA,MustianK,PepponeL,HecklerC,etal.Fallsandfunctional
impairmentsincancersurvivorswithchemotherapy-inducedperipheralneuropathy(CIPN):a
UniversityofRochesterCCOPstudy.SupportCareCancer.2013Jul;21(7):2059–66.
16.BaoT,BasalC,SeluzickiC,LiSQ,SeidmanAD,MaoJJ.Long-termchemotherapy-induced
peripheralneuropathyamongbreastcancersurvivors:prevalence,riskfactors,andfallrisk.Breast
CancerResTreat.2016Sep;159(2):327–33.
17.KolbNA,SmithAG,SingletonJR,BeckSL,StoddardGJ,BrownS,etal.TheAssociationof
Chemotherapy-InducedPeripheralNeuropathySymptomsandtheRiskofFalling.JAMANeurol.2016
Jul1;73(7):860–6.
18.MolsF,BeijersT,VreugdenhilG,vandePoll-FranseL.Chemotherapy-inducedperipheral
neuropathyanditsassociationwithqualityoflife:asystematicreview.SupportCareCancer.2014
Aug;22(8):2261–9.
19.CesariM,KritchevskySB,NewmanAB,SimonsickEM,HarrisTB,PenninxBW,etal.Addedvalueof
physicalperformancemeasuresinpredictingadversehealth-relatedevents:resultsfromtheHealth,
AgingAndBodyCompositionStudy.JAmGeriatrSoc.2009;57(2):251–9.

19
20.CesariM,CerulloF,ZamboniV,PalmaRD,ScambiaG,BalducciL,etal.FunctionalStatusand
MortalityinOlderWomenWithGynecologicalCancer.JGerontolABiolSciMedSci.2013;68(9):1129–
33.
21.KlepinHD,GeigerAM,ToozeJA,NewmanAB,ColbertLH,BauerDC,etal.Physicalperformance
andsubsequentdisabilityandsurvivalinolderadultswithmalignancy:resultsfromthehealth,aging
andbodycompositionstudy.JAmGeriatrSoc.2010Jan;58(1):76–82.
22.OnderG,PenninxBWJH,FerrucciL,FriedLP,GuralnikJM,PahorM.Measuresofphysical
performanceandriskforprogressiveandcatastrophicdisability:resultsfromtheWomen’sHealth
andAgingStudy.JGerontolABiolSciMedSci.2005Jan;60(1):74–9.
23.AleknaV,StukasR,Tamulaitytė-MorozovienėI,ŠurkienėG,TamulaitienėM.Self-reported
consequencesandhealthcarecostsoffallsamongelderlywomen.MedKaunasLith.2015;51(1):57–
62.
24.AlexanderBH,RivaraFP,WolfME.Thecostandfrequencyofhospitalizationforfall-related
injuriesinolderadults.AmJPublicHealth.1992;82(7):1020–3.
25.KneisS,WehrleA,FreylerK,LehmannK,RudolphiB,HildenbrandB,etal.Balanceimpairments
andneuromuscularchangesinbreastcancerpatientswithchemotherapy-inducedperipheral
neuropathy.ClinNeurophysiol.2016Feb;127(2):1481–90.
26.BonnetC,CarelloC,TurveyMT.DiabetesandPosturalStability:ReviewandHypotheses.JMot
Behav.2009Mar;41:172–92.
27.DicksteinR,PeterkaRJ,HorakFB.Effectsoflightfingertiptouchonposturalresponsesinsubjects
withdiabeticneuropathy.JNeurolNeurosurgPsychiatry.2003Jan5;74(5):620–6.
28.DicksteinR,ShupertCL,HorakFB.Fingertiptouchimprovesposturalstabilityinpatientswith
peripheralneuropathy.GaitPosture.2001Dec;14(3):238–47.
29.SimmonsRW,RichardsonC,PozosR.Posturalstabilityofdiabeticpatientswithandwithout
cutaneoussensorydeficitinthefoot.DiabetesResClinPract.1997Jun;36(3):153–60.
30.HorakFB,HlavackaF.Somatosensorylossincreasesvestibulospinalsensitivity.JNeurophysiol.
2001Aug;86(2):575–85.
20
31.FitzpatrickR,McCloskeyDI.Proprioceptive,visualandvestibularthresholdsfortheperceptionof
swayduringstandinginhumans.JPhysiol.1994Jul1;478(Pt1):173–86.
32.NashnerLM,BlackFO,WallC.Adaptationtoalteredsupportandvisualconditionsduringstance:
patientswithvestibulardeficits.JNeurosci.1982May;2(5):536–44.
33.PeterkaRJ,BenolkenMS.Roleofsomatosensoryandvestibularcuesinattenuatingvisually
inducedhumanposturalsway.ExpBrainRes.1995;105(1):101–10.
34.CornaS,TarantolaJ,NardoneA,GiordanoA,SchieppatiM.Standingonacontinuouslymoving
platform:isbodyinertiacounteractedorexploited?ExpBrainRes.1999Feb;124(3):331–41.
35.SchieppatiM,GiordanoA,NardoneA.Variabilityinadynamicposturaltaskattestsample
flexibilityinbalancecontrolmechanisms.ExpBrainRes.2002May;144(2):200–10.
36.EngelhartD,PasmaJH,SchoutenAC,MeskersCGM,MaierAB,MergnerT,etal.Impairedstanding
balanceinelderly:anewengineeringmethodhelpstounravelcausesandeffects.JAmMedDir
Assoc.2014Mar;15(3):227.e1-6.
37.PasmaJH,EngelhartD,MaierAB,SchoutenAC,vanderKooijH,MeskersCGM.Changesinsensory
reweightingofproprioceptiveinformationduringstandingbalancewithageanddisease.J
Neurophysiol.2015Dec;114(6):3220–33.
38.WiesmeierIK,DalinD,MaurerC.ElderlyUseProprioceptionRatherthanVisualandVestibular
CuesforPosturalMotorControl.FrontAgingNeurosci.2015;7:97.
39.SchwenkM,GrewalGS,HollowayD,MuchnaA,GarlandL,NajafiB.InteractiveSensor-Based
BalanceTraininginOlderCancerPatientswithChemotherapy-InducedPeripheralNeuropathy:A
RandomizedControlledTrial.Gerontology.2016;62(5):553–63.
40.StreckmannF,ZopfEM,LehmannHC,MayK,RizzaJ,ZimmerP,etal.ExerciseIntervention
StudiesinPatientswithPeripheralNeuropathy:ASystematicReview.SportsMed.2014Jun14;44(9).
41.ZimmerP,TrebingS,Timmers-TrebingU,SchenkA,PaustR,BlochW,etal.Eight-week,
multimodalexercisecounteractsaprogressofchemotherapy-inducedperipheralneuropathyand
improvesbalanceandstrengthinmetastasizedcolorectalcancerpatients:arandomizedcontrolled
trial.SupportCareCancer.2017Sep30;26(2):615–24.

21
42.KneisS,WehrleA,MüllerJ,MaurerC,IhorstG,GollhoferA,etal.It’snevertoolate-balanceand
endurancetrainingimprovesfunctionalperformance,qualityoflife,andalleviatesneuropathic
symptomsincancersurvivorssufferingfromchemotherapy-inducedperipheralneuropathy:resultsof
arandomizedcontrolledtrial.BMCCancer.2019May2;19(1):414.
43.AlletL,ArmandS,deBieRA,GolayA,MonninD,AminianK,etal.Thegaitandbalanceofpatients
withdiabetescanbeimproved:arandomisedcontrolledtrial.Diabetologia.2010Mar;53(3):458–66.
44.LeeK,LeeS,SongC.Whole-bodyvibrationtrainingimprovesbalance,musclestrengthand
glycosylatedhemoglobininelderlypatientswithdiabeticneuropathy.TohokuJExpMed.
2013;231(4):305–14.
45.SongCH,PetrofskyJS,LeeSW,LeeKJ,YimJE.Effectsofanexerciseprogramonbalanceand
trunkproprioceptioninolderadultswithdiabeticneuropathies.DiabetesTechnolTher.2011
Aug;13(8):803–11.
46.TaubeW,GruberM,GollhoferA.Spinalandsupraspinaladaptationsassociatedwithbalance
trainingandtheirfunctionalrelevance.ActaPhysiolOxf.2008Jun;193(2):101–16.
47.ZechA,HübscherM,VogtL,BanzerW,HänselF,PfeiferK.Balancetrainingforneuromuscular
controlandperformanceenhancement:asystematicreview.JAthlTrain.2010Aug;45(4):392–403.
48.GranacherU,MuehlbauerT,TaubeW,GollhoferA,GruberM.SensorimotorTraining.In:Strength
andconditioning:biologicalprinciplesandpracticalapplications.SanFrancisco:Wiley-Blackwell;
2011.p.399.
49.CnyrimC,MergnerT,MaurerC.Potentialrolesofforcecuesinhumanstancecontrol.ExpBrain
Res.2009Feb14;194(3):419–33.
50.MaurerC,MergnerT,PeterkaRJ.Multisensorycontrolofhumanuprightstance.ExpBrainRes.
2006May;171(2):231–50.
51.MaurerC,PeterkaRJ.Anewinterpretationofspontaneousswaymeasuresbasedonasimple
modelofhumanposturalcontrol.JNeurophysiol.2005Jan;93(1):189–200.
52.PrietoTE,MyklebustJB,HoffmannRG,LovettEG,MyklebustBM.Measuresofposturalsteadiness:
differencesbetweenhealthyyoungandelderlyadults.IEEETransBiomedEng.1996Sep;43(9):956–

22
66.
53.PeterkaRJ.Sensorimotorintegrationinhumanposturalcontrol.JNeurophysiol.2002
Sep;88(3):1097–118.
54.WiesmeierIK,DalinD,WehrleA,GranacherU,MuehlbauerT,DietterleJ,etal.BalanceTraining
EnhancesVestibularFunctionandReducesOveractiveProprioceptiveFeedbackinElderly.FrontAging
Neurosci.2017;9:273.
55.KooijHvander,JacobsR,KoopmanB,HelmFvander.Anadaptivemodelofsensoryintegration
inadynamicenvironmentappliedtohumanstancecontrol.BiolCybern.2001Jan1;84(2):103–15.
56.MergnerT,MaurerC,PeterkaRJ.Sensorycontributionstothecontrolofstance:aposturecontrol
model.AdvExpMedBiol.2002;508:147–52.
57.WelchTDJ,TingLH.AFeedbackModelExplainstheDifferentialScalingofHumanPostural
ResponsestoPerturbationAccelerationandVelocity.JNeurophysiol.2009Jun;101(6):3294–309.
58.StreckmannF,KneisS,LeifertJA,BaumannFT,KleberM,IhorstG,etal.Exerciseprogram
improvestherapy-relatedside-effectsandqualityoflifeinlymphomapatientsundergoingtherapy.
AnnOncol.2014Jan2;25(2):493–9.
59.BoucherP,TeasdaleN,CourtemancheR,BardC,FleuryM.Posturalstabilityindiabetic
polyneuropathy.DiabetesCare.1995May;18(5):638–45.
60.CorriveauH,PrinceF,HébertR,RaîcheM,TessierD,MaheuxP,etal.EvaluationofPostural
StabilityinElderlywithDiabeticNeuropathy.DiabetesCare.2000Jan8;23(8):1187–91.
61.DiNardoW,GhirlandaG,CerconeS,PitoccoD,SoponaraC,CosenzaA,etal.Theuseofdynamic
posturographytodetectneurosensorialdisorderinIDDMwithoutclinicalneuropathy.JDiabetes
Complications.1999Apr;13(2):79–85.
62.SimoneauGG,UlbrechtJS,DerrJA,BeckerMB,CavanaghPR.Posturalinstabilityinpatientswith
diabeticsensoryneuropathy.DiabetesCare.1994Dec;17(12):1411–21.
63.UccioliL,GiacominiPG,MonticoneG,MagriniA,DurolaL,BrunoE,etal.Bodyswayindiabetic
neuropathy.DiabetesCare.1995Mar;18(3):339–44.
64.vanderKooijH,PeterkaRJ.Non-linearstimulus-responsebehaviorofthehumanstancecontrol

23
systemispredictedbyoptimizationofasystemwithsensoryandmotornoise.JComputNeurosci.
2011Jun;30(3):759–78.
65.HorakFB,DicksteinR,PeterkaRJ.Diabeticneuropathyandsurfacesway-referencingdisrupt
somatosensoryinformationforposturalstabilityinstance.SomatosensMotRes.2002Jan
1;19(4):316–26.
66.TuckerMG,KavanaghJJ,BarrettRS,MorrisonS.Age-relateddifferencesinposturalreactiontime
andcoordinationduringvoluntaryswaymovements.HumMovSci.2008Oct;27(5):728–37.
67.AllumJHJ,CarpenterMG,HoneggerF,AdkinAL,BloemBR.Age-dependentvariationsinthe
directionalsensitivityofbalancecorrectionsandcompensatoryarmmovementsinman.JPhysiol.
2002Jul15;542(Pt2):643–63.
68.MergnerT,MaurerC,PeterkaRJ.Amultisensoryposturecontrolmodelofhumanuprightstance.
ProgBrainRes.2003;142:189–201.
69.CataJP,WengHR,LeeBN,ReubenJM,DoughertyPM.Clinicalandexperimentalfindingsin
humansandanimalswithchemotherapy-inducedperipheralneuropathy.MinervaAnestesiol.2006
Mar;72(3):151–69.
70.BrownJC,HarhayMO,HarhayMN.Physicalfunctionasaprognosticbiomarkeramongcancer
survivors.BrJCancer.2015;112(1):194–8.
TablesTable1Subjects'characteristic

24
Pat Sex Height(cm)
Weight(kg)
Age(years)
Diagnosis Status MonthssinceED(n)
Cyclesofneurotoxicdrugs(n)
1 m 182 125 55 B-NHL PR 185 14
2 m 182 80 67 MM SD 58 34
3 f 161 86 60 MM Relapse 82 7
4 f 162 60 68 Breastcancer SD 66 19
5 m 180 80 64 MM SD 8 4
6 m 167 92 63 Breastcancer SD 195 25
7 m 176 64 67 Rectalcancer PD 118 79
8 m 188 107 42 Germcellcancer CR 66 4mean±SD
m:f6:2
174.8±10.1
86.8±21.5
60.8±8.7
97.3±64.8
23.3±24.9
hCon mean±SD
m:f9:6
17.0±9.1
78.0±6.3
59.6±10.0
Pat,CIPNpatients;SD,standarddeviation;hCon,healthycontrolsubjects;m,male;f,female;B-NHL,
B-NonHodgkinLymphoma;MM,multiplemyeloma;PR,partialremission;SD,stabledisease;PD,
progressivedisease;CR,completeremission;NCV,nerveconductionvelocity(normalvalues:
≥41m/s);APA,actionpotentialamplitude(normalvalues:≥6µV);ATR,Achillestendonreflex;PRT,
Patellatendonreflex;"-",noreflex;"(-)",reducedreflex;"+",normalreflex;NtxS,neurotoxicity
subscaleofFACT/GOG(FunctionalAssessmentofCancerTherapy/GynaecologyOncologyGroup)
scoredfrom0(severesymptoms)–44(nosymptoms)
Table2Spontaneousswaymeasures(RMS,MV,CF)withgroupeffects,andinteractionsbetween
groupsandvisualconditions/swaydirections.

25
hControl PATpre PATpost F-value p-value RMS(cm) 0.46±0.1810.926 <0.000
10.56±0.27
visualcondition eyesopeneyesclosed
0.45±0.180.56±0.19
5.06 0.007 0.49±0.230.63±0.30
swaydirection anterior-posteriormedio-lateral
0.52±0.160.35±0.17
4.06 0.018 0.67±0.280.41±0.19
MV(cm/s) 0.35±0.147.80 0.0005 0.69±0.57
visualcondition eyesopeneyesclosed
0.32±0.130.39±0.14
8.00 0.0004 0.45±0.310.92±0.84
swaydirection anterior-posteriormedio-lateral
0.41±0.130.27±0.12
n.s. 0.82±0.780.51±0.44
CF(Hz) 0.37±0.11 n.s. 0.46±0.18
hControl=healthycontrolsubjects,PATpre=patientsbeforeintervention,PATpost=patientsafter
intervention,RMS=rootmeanssquare,MV=meanvelocity,CF=centerfrequency,n.s.=not
significant.
Figures

26
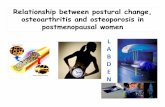
Figure1
ExperimentalsetupPerturbedstance:PosturalreactionsofAupperbodyandBlowerbody
on1°peak-to-peakplatformrotation(Cstimulus)over20secondswitheyesopenina
representativehealthycontrolsubject(hCon)andapatientbefore(pre)andafter(post)
intervention.Bodyreaction(A/B)followstheplatformmovement(C).Schemeofasubject
standingontheplatforminanuprightpositionD.Spontaneoussway:COPdisplacementof
onerepresentativesubjectofthecontrolsubjects'group(E,hCon)andthepatients'groupF
before(pre)andGafter(post)intervention.Patients'COPdisplacement(F/G)ismore
pronouncedthancontrolsubjects'(E),butreducedafterintervention(G).deg,degrees,sec,
seconds,ap,anterior-posterior,ml,medio-lateral,cm,centimeter.
27

28
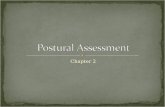
Figure2
SpontaneousswayMeanandstandarddeviationofA/Brootmeansquare(RMS),C/Dmean
velocity(MV)andE/Fcenterfrequency(CF)ofCOPswayinanterior-posterior(ap)and
medio-lateral(ml)directioneachfortheeyes-openandeyes-closedconditioninhealthy
controlsubjects(hCon),patientsbefore(pre)andafter(post)intervention.Significant
differencesofRMSandMVbetweencontrolsubjectsandpatientsaremorepronouncedin
theapdirectionandtheeyes-closedcondition.NotethatthelargeerrorbarsinDare
specificallyrelatedtohighfrequencycontentofpatients’sway.

29
Figure3
TransferfunctionsMeanandstandarddeviationofAGain,BPhaseandCCoherence
behaviorasafunctionoffrequency(f)andD/EmeanGainandF/GmeanPhasebehaviorfor
lowerbody(LB)andupperbody(UB)andforeyes-open(eo)andeyes-closed(ec)condition
inhealthycontrolsubjects(hCon),patientsbefore(pre)andafter(post)intervention.
Differencesbetweenhealthysubjectsandpatientsaremorepronouncedfortheupperbody
andwithclosedeyes.Postintervention,patientsshiftedtheirGain,PhaseandCoherence
valuestowardstherangeofcontrolsubjects'values.

30
Figure4
GainfactorMeanandstandarddeviationofA/BupperbodyandC/DlowerbodyGAINFACTOR
behaviorofpatientsbefore(pre)andafter(post)interventionasafunctionoffrequency(f).
GAINFACTORrepresentspatients’GAINvaluesnormalizedtovaluesofhealthycontrol
subjects(hCon)intheeyes-openandeyes-closedcondition.Differencesbetweenhealthy
subjectsandpatientsaremorepronouncedforupperbodyandwitheyesclosed.After
interventionpatientsshiftedtheirGAINandPHASEvaluestowardstherangeofcontrol
subjects'values.

31
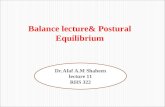
Figure5
ModelparametersMeanandstandarddeviationofAtheneuralcontrollerwiththe
proportional(Kp/mghin1/°),derivative(Kd/mghins/°)andintegral(Ki/mghin1/s*°)
contributioncorrectedforsubjects’massesandheights,ofBtheproprioceptivesensory
weight(Wpin°/°)andCthelumpedtimedelay(Tdinseconds)forhealthycontrolsubjects
(hCon),patientsbefore(pre)andafter(post)intervention,eachshownintheeyes-open(eo)
andeyes-closed(ec)conditionandforBWpin0.5and1degree(deg)platformrotation.D

32
showsthemodifiedpostural-controlmodelusedtoidentifyabnormalposturalcontrol
parametersinCIPNpatientsviaanoptimizationprocedurewheredifferencesbetween
experimentaldataandmodelsimulationswereminimized:Themodelconsistsofabody
representedbyaninvertedpendulumwiththemassconcentratedatthecenterofmass
(COM)ofthebodyandthesensorsandneuromuscularsystemsincludingaNeural
Controller.θ,bodyswayangle;h,heightoftheCOMabovetheanklejoints;θref,external
stimulus;Kp,proportionalgain(stiffnessfactor),Kd,derivativegain(dampingfactor),Ki,
integralgainoftheNeuralController;Ppas,passivestiffnessfactor;Dpas,passivedamping
factor;Wp,proprioceptivesensoryweight;Td,feedbacktimedelay;T,controltorque;J,
momentofinertiaofthebody;mgh,bodymass*gravitationalconstant*heightoftheCOM
fromtheanklejoint;s,Laplacetransformvariable.