A method for corneal nerves automatic segmentation and morphometric analysis
8
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60 jo ur n al hom ep age : www.intl.elsevierhealth.com/journals/cmpb A method for corneal nerves automatic segmentation and morphometric analysis Ana Ferreira a,∗ , António Miguel Morgado a,b , José Silvestre Silva b,c a IBILI – Institute of Biomedical Research in Light and Image, Azinhaga de Santa Comba, Celas, 3000-548 Coimbra, Portugal b Department of Physics, Faculty of Sciences and Technology, University of Coimbra, Rua Larga, P-3004 516 Coimbra, Portugal c Instrumentation Center, Faculty of Sciences and Technology, University of Coimbra, Rua Larga, P-3004 516 Coimbra, Portugal a r t i c l e i n f o Article history: Received 20 February 2011 Accepted 23 September 2011 Keywords: Diabetic neuropathy Corneal nerves Segmentation methods Phase symmetry a b s t r a c t The segmentation and morphometric analysis of corneal sub-basal nerves, from corneal confocal microscopy images, has gained recently an increased interest. This interest arises from the possibility of using changes in these nerves as the basis of a simple and non- invasive method for early detection and follow-up of peripheral diabetic neuropathy, a major cause of chronic disability in diabetic patients. Here, we propose one method for automatic segmentation and analysis of corneal nerves from images obtained in vivo through corneal confocal microscopy. The method is capable of segmenting corneal nerves, with sensitivity near 90% and a percentage of false recognitions with an average of 5.3%. The nerves tortuos- ity was calculated and shows statistically significant differences between healthy controls and diabetic individuals, in accordance to what is reported in the literature. © 2011 Elsevier Ireland Ltd. All rights reserved. 1. Introduction There is a growing interest on the segmentation and analy- sis of corneal nerves images. These images, obtained in vivo, in conscious patients, through corneal confocal microscopy (CCM), can document corneal nerve changes. There is increas- ing evidence that it is possible to diagnosis and assess peripheral diabetic neuropathy through the morphometric analysis of the sub-basal nerve plexus of the cornea. The development of a simple, non-invasive method for diagnosis and follow-up of peripheral diabetic neuropathy will have great social impact. Peripheral diabetic neuropathy, is a major cause of morbidity in diabetic patients [1,2] affecting 50% of diabetic patients 25 years after diagnosis of diabetes [3], and being implicated in 50–75% of non-traumatic amputations [4,5]. Early diagnosis and assessment of disease progression are important to accurately define at risk patients, evaluate therapies and decrease patient morbidity [6]. Currently, this ∗ Corresponding author. Tel.: +351 239480200. E-mail addresses: [email protected], [email protected] (A. Ferreira). diagnosis often fails or occurs only when patients became symptomatic [7]. The follow-up, through the documentation of small-fiber damage, is only possible with invasive biopsy [8–10]. Being one of the most innervated tissues in humans and directly assessable to inspection using light, the cornea became a natural target for the diagnosis of peripheral diabetic neuropathy. This is particularly true since the development of CCM allowed non-invasive in vivo imaging of corneal sub-basal nerve plexus. CCM has been used to quantify the corneal nerve morphologic features [11], nerve den- sity in normal and diabetic patients [12], and the extent of degeneration and regeneration of corneal nerve fibers in dia- betic patients with increasing neuropathic severity [13,14]. It was also demonstrated that the number of fibers in the cornea sub-basal nerve plexus of diabetic patients was sig- nificantly lower than in healthy humans, even for short diabetes duration [15,16]. So, there is evidence to suggest that the quantification of sub-basal plexus morphometric 0169-2607/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.cmpb.2011.09.014
-
Upload
ana-ferreira -
Category
Documents
-
view
217 -
download
1
Transcript of A method for corneal nerves automatic segmentation and morphometric analysis

Am
Aa
b
c
a
A
R
A
K
D
C
S
P
1
Tsi(ipa
dhm5a[at
0d
c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60
jo ur n al hom ep age : www.int l .e lsev ierhea l th .com/ journa ls /cmpb
method for corneal nerves automatic segmentation andorphometric analysis
na Ferreiraa,∗, António Miguel Morgadoa,b, José Silvestre Silvab,c
IBILI – Institute of Biomedical Research in Light and Image, Azinhaga de Santa Comba, Celas, 3000-548 Coimbra, PortugalDepartment of Physics, Faculty of Sciences and Technology, University of Coimbra, Rua Larga, P-3004 516 Coimbra, PortugalInstrumentation Center, Faculty of Sciences and Technology, University of Coimbra, Rua Larga, P-3004 516 Coimbra, Portugal
r t i c l e i n f o
rticle history:
eceived 20 February 2011
ccepted 23 September 2011
eywords:
iabetic neuropathy
a b s t r a c t
The segmentation and morphometric analysis of corneal sub-basal nerves, from corneal
confocal microscopy images, has gained recently an increased interest. This interest arises
from the possibility of using changes in these nerves as the basis of a simple and non-
invasive method for early detection and follow-up of peripheral diabetic neuropathy, a major
cause of chronic disability in diabetic patients. Here, we propose one method for automatic
segmentation and analysis of corneal nerves from images obtained in vivo through corneal
orneal nerves
egmentation methods
hase symmetry
confocal microscopy. The method is capable of segmenting corneal nerves, with sensitivity
near 90% and a percentage of false recognitions with an average of 5.3%. The nerves tortuos-
ity was calculated and shows statistically significant differences between healthy controls
and diabetic individuals, in accordance to what is reported in the literature.
cornea sub-basal nerve plexus of diabetic patients was sig-
. Introduction
here is a growing interest on the segmentation and analy-is of corneal nerves images. These images, obtained in vivo,n conscious patients, through corneal confocal microscopyCCM), can document corneal nerve changes. There is increas-ng evidence that it is possible to diagnosis and assesseripheral diabetic neuropathy through the morphometricnalysis of the sub-basal nerve plexus of the cornea.
The development of a simple, non-invasive method foriagnosis and follow-up of peripheral diabetic neuropathy willave great social impact. Peripheral diabetic neuropathy, is aajor cause of morbidity in diabetic patients [1,2] affecting
0% of diabetic patients 25 years after diagnosis of diabetes [3],nd being implicated in 50–75% of non-traumatic amputations
4,5]. Early diagnosis and assessment of disease progressionre important to accurately define at risk patients, evaluateherapies and decrease patient morbidity [6]. Currently, this∗ Corresponding author. Tel.: +351 239480200.E-mail addresses: [email protected], [email protected]
169-2607/$ – see front matter © 2011 Elsevier Ireland Ltd. All rights resoi:10.1016/j.cmpb.2011.09.014
© 2011 Elsevier Ireland Ltd. All rights reserved.
diagnosis often fails or occurs only when patients becamesymptomatic [7]. The follow-up, through the documentationof small-fiber damage, is only possible with invasive biopsy[8–10].
Being one of the most innervated tissues in humansand directly assessable to inspection using light, the corneabecame a natural target for the diagnosis of peripheral diabeticneuropathy. This is particularly true since the developmentof CCM allowed non-invasive in vivo imaging of cornealsub-basal nerve plexus. CCM has been used to quantifythe corneal nerve morphologic features [11], nerve den-sity in normal and diabetic patients [12], and the extent ofdegeneration and regeneration of corneal nerve fibers in dia-betic patients with increasing neuropathic severity [13,14].It was also demonstrated that the number of fibers in the
m (A. Ferreira).
nificantly lower than in healthy humans, even for shortdiabetes duration [15,16]. So, there is evidence to suggestthat the quantification of sub-basal plexus morphometric
erved.

54 c o m p u t e r m e t h o d s a n d p r o g r a m s i n
Fig. 1 – Algorithm overview.
(4)
parameters may constitute a basis for diabetic neuropathydiagnosis [17,18].
At present, the analysis of sub-basal corneal nerve parame-ters is usually based on a manual laborious task [11–13,19] thatis subjective and prone to errors. Fully automatic methods,requiring no specific expertise from the user, were recentlyproposed. Holmes et al. [20] developed a method to automat-ically trace the nerve fibers in corneal micrographs and usedit to show a relationship between the presence of peripheralneuropathy and the density and shape of corneal nerve fibers.
As far as we know, Scarpa et al. [21] were the first to pro-pose automatic methods for the recognition and tracing of thecorneal nerve structures, in CCM images [22].
In this work, we propose and evaluate the performance ofa segmentation method for automatic extraction of sub-basalcorneal nerves morphometric parameters. Our method startsby normalizing the image contrast and reducing the noise,using contrast equalization, a phase symmetry-based methodand histogram procedure. Then a fast search is done to locatecandidate regions that are expanded to identify each cornealnerve. Discarding false positives and merging all remainingnerves results in the identification of complete nerve structure[23,24].
2. Methods
2.1. Corneal nerves segmentation algorithm
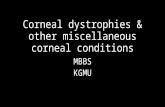
The segmentation algorithm method is schematicallydescribed by the functional block diagram of Fig. 1. Thealgorithm comprises several steps:
1) Local equalization, for enhancing image details.2) Phase symmetry, using wavelet transform filter, to identify
the nerves structures.3) Nerve reconstruction using morphologic operations.
These steps are detailed in the next sections.
b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60
2.1.1. Local equalizationImages acquired through CCM show corneal nerves as brightlinear structures over a dark background. This background isusually characterized by a gradual intensity variation from theperiphery to the center. Therefore, it is necessary to correctthis non-uniformity.
Histogram equalization is usually used to improve imagecontrast [25,26]. We applied the contrast-limited adaptive his-togram equalization method, which uses information fromseveral histograms corresponding to small image regions. Thecontrast is limited to avoid amplifying image noise, particu-larly in homogeneous areas. The method was applied usingan 8 × 8 pixel square mask.
2.1.2. Phase symmetrySymmetry is an important mechanism to identify thestructure of objects. Symmetries indicate the invariance ofobjects under geometric transformations. Different image fea-tures (lines, ridges, valleys, blobs, etc.) have different phaseresponses with the phase beings congruent for each of thesefeatures.
To obtain local phase frequency information, a method-ology based on wavelet transform filters, namely log-Gaborfilters was used. We followed the methodology proposed byKovesi [27], using two filters in quadrature, one to calculatethe amplitude and the other the signal phase, for a particularscale and frequency, at a given spatial location. These filterscan be defined with arbitrary bandwidth. The 1D log-Gabor fil-ters were extended to 2D by applying 1D analysis over severalorientations r and combining the results.
Thus, local phase symmetry extracted from a 2D image,I(x,y), can be obtained by convolving I(x,y) with the 2Dlog-Gabor filters (an even-symmetric filter lGne and an odd-symmetric filter lGno) at a scale n. The responses of eachquadrature pair of filters is expressed by the vector:
[en(x, y), on(x, y)] = [I(x, y) ∗ lGne, I(x, y) ∗ lGno] (1)
where, en(x,y) is the real part and on(x,y) is the imaginary partof the complex frequency component.
From Eq. (1), the amplitude and the phase at a given waveletscale, are respectively:
An(x, y) =√
(en(x, y))2 + (on(x, y))2 (2)
�n(x, y) = atan2(en(x, y), on(x, y)), (3)
in which, atan2 is the four-quadrant inverse tangent (arctan-gent).
The 2D phase symmetry measure (PS) is calculated for dif-ferent scales n and orientations r by:
PS(x, y) =∑
n
∑r
⌊An(x, y)
[∣∣cos(�n(x, y))∣∣−
∣∣sin(�n(x, y))∣∣]− T
⌋∑
n
∑rAn(x, y) + ε
,
where the term ε is a small number included to avoid divisionby zero; factor T is a threshold to compensate image noise

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60 55
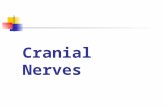
Fig. 2 – Initial steps of the segmentation algorithm: (a) original CCM image, (b) local equalization applied to CCM image, and(c) phase-shift applied to CCM image.
ap
s
ms
2Fsblc
rwl(sntcr
rbw
nd �Quantity� corresponds to the enclosed function value ifositive, or zero when the function returns a negative value.
The resulting image appears with highlighted tubulartructures indicating the nerves position.
The phase-shift procedure used six orientations for sym-etry searching. An example of the results after the first two
teps of the algorithm is shown in Fig. 2.
.1.3. Nerve reconstructionull reconstruction of the corneal nerves, from the tubulartructures identified by the phase symmetry step, is achievedy a reconstruction process, from selected seed points, fol-owed by a rejection step where structures with features notompatible with corneal nerves are excluded.
The reconstruction process requires the selection of cor-ect seed points. As the nerves cross the whole image,e calculated the diagonal of the image, from the lower
eft to the upper right corner, and detected all regionsSTARTING ROI regions) that intersected this diagonal. Sinceome smaller nerves were not intersected by the diago-al, a second diagonal was defined, from the upper lefto the lower right corner of the image. Regions inter-epted by this diagonal were added to the STARTING ROIegions.
The next step was to quantify each of the STARTING ROIegions and to exclude those that had properties incompati-le with corneal nerves: regions with a very small area; regionshere the ratio between their area and bounding-box area
is too high; regions with a width value and a bounding-boxlength of the same order of magnitude.
From the STARTING ROI regions, a sequence of simplemorphologic operations was used to reconstruct the nerves.Finally, the algorithm analyzed the segmented image exclud-ing those structures which do not correspond to nerves; theseresult mainly from stromal keratocytes (cells located at lay-ers posterior to the sub-basal nerve plexus) present in theimage. To perform this procedure, the skeleton of the imagewas computed. Then, the branches of the skeleton were found,being discarded branches with length smaller than 10 pixels.Each disconnected segment was identified. Isolated segmentswith length smaller than 130 pixels were discarded, since theyrepresent non-nerve regions or noise.
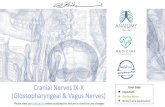
The final results of the nerve reconstruction step are illus-trated in Fig. 3.
2.2. Morphometric parameters
From the representation obtained through automatic segmen-tation it is possible to extract morphometric parameters suchas the nerves tortuosity, nerve length and nerve density.
2.2.1. TortuosityThe tortuosity coefficient (TC) is a parameter that quantifiesif a structure is curved or winding. We used calculated the

56 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60
Fig. 3 – Representative examples of the results obtained. The first column contains the original images while the secondincludes the final reconstructed nerves. The first and second rows are the images representing the best cases and the thirdrow is the image that represents the worst case, in terms of sensitivity.
tortuosity according to the expression proposed by Kallinikoset al. [19]:
TC =
√√√√N−1∑i=1
((FD(xi, yi))2 + (SD(xi, yi))
2) (5)
The tortuosity for each segment of the image was calcu-lated, treating them as a mathematical function on the image
space and computing the function first (FD) and second (SD)derivatives. We identify the endpoints of each segment, drawa straight line between them and rotate the image in orderto align this line with the x-axis. The FD is calculated as thedifference of two consecutive points on the nerve, divided bythe distance between the projections on the x-axis of two con-secutive pixels of the segment (dx). The SD is given by thedifference of two consecutive values of the FD, divided by dx.The value of dx is constant and equal to 1 pixel.
2.2.2. Nerve lengthThe nerve length was calculated by computing the distancebetween adjacent pixels along the nerve skeleton, in �m:
Length = scale ×∑
I(skeleton) (6)

c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60 57
Table 1 – Lengths and densities of automatically andmanually segmented nerves.
Lengths (�m) Densities (�m/mm2)
Manual Automatic Manual Automatic
AllMean 603.5 511.6 3748.5 3177.5Std. Dev. 373.0 285.8 2316.6 1775.0
Non-diabeticMean 614.0 517.6 3813.7 3214.9Std. Dev. 406.7 298.8 2525.9 1855.9
Diabetic
2Tn
D
3
Tadtdstrais
iaga
o
C
4
Crsr
Table 2 – Pixel classification for algorithm performanceevaluation.
Algorithm Reference
TP Nerve Nerve
We calculated the TC for non-diabetic and diabetic corneas
Mean 577.1 496.4 3584.4 3083.4Std. Dev. 274.4 254.0 1704.6 1577.7
.2.3. Nerve densityhe nerve density was calculated by dividing the sum of theerve lengths by the image area, in �m/mm2:
ensity = scale ×∑
I(skeleton)
I(area)(7)
. Materials
he method described herein was implemented in Matlabnd was applied on 47 images (36 healthy controls and 11iabetic patients) from a database available online [22], con-aining 90 images. Two images with stromal nerves wereiscarded. Images whose en face section traverses obliquelyeveral corneal layers were not considered. In these images,he sub-basal nerves appear only on a small region, with theemaining field of view containing other corneal features, suchs stromal keratocytes or basal epithelial cells. A group ofmages with extremely low quality was also discarded. Theame happened to a set of repeated images.
The images have a size of 768 × 576 pixels and were storedn JPEG compressed format. These images were captured by
ConfoScan 4 corneal confocal microscope (Nidek Technolo-ies, Padova, Italy) with a 460 �m × 350 �m field of view, using
40× objective.Those have already been used to evaluate the performance
f automatic segmentation methods for corneal nerves [22].The processing time was approximately 1 min on an Intel
entrino Core 2 at 2.4 GHz computer.
. Results
orneal nerves segmentation results for the developed algo-
ithm are illustrated in Fig. 3, where the first and second rowshow the best results, while the third row shows the worstesult, in terms of sensitivity.Table 3 – Evaluation of the algorithm performance.
Average St
Nerve length correctly detected 89.8%
Nerve length falsely detected 5.3%
TN Non-nerve Non-nerveFP Nerve Non-nerveFN Non-nerve Nerve
Table 1 shows the values of automatically and manuallysegmented nerve lengths and densities. Densities values areobtained dividing the nerve length by the image area. Theresults show that the automatic algorithm underestimatesthe nerve length. They also show that the nerve lengths anddensities vary considerably between images.
The algorithm was evaluated by comparing the nervelength identified by the algorithm, with the length of man-ually traced nerves by an experienced ophthalmologist, onthe same image. The manual segmentation was performedby tracing all clearly visible nerves with a commercial graphiceditor program. Every segmented image pixel was classifiedas specified in Table 2.
The length of correctly segmented nerves is given by thelength of true positive classifications, expressed as percentageof the manual segmented nerve length. Therefore, it corre-sponds to the algorithm sensitivity, given by the followingexpression:
Sensitivity = TPTP + FN
(8)
The use of specificity, defined as the number of properlyclassified pixels in the true negative class, is not adequate forthe evaluation of the algorithm performance, since the num-ber of non-nerve pixels far outnumber the number of nervepixels. Therefore, and following the approach used by otherauthors [22], we choose to use the percentage of nerve falselydetected, given by the length of false positive pixels expressedas percentage of the total segmented nerve length to evaluatethe algorithm specificity. In this case a lower figure indicatesa better performance. Results are shown in Table 3. On thisset of images, almost 90% of the nerve length was correctlysegmented, with an average of 5.3% false recognitions by theautomatic segmentation method.
The limits of concordance between automatic and manualsegmentation, were calculated, using the Bland and Altmanmethod [28]. Results are shown in Fig. 4. The mean differencein nerve length, between automatic and manual segmentationis −80.7 �m, a result that confirms length underestimation bythe automatic algorithm.
and compared the values between automatic and manuallysegmented images, using the Bland and Altman plots. The TCwas calculated only for nerve segments with lengths greater
d. Deviation Minimum Maximum
12.0% 72.0% 99.0%8.9% 0% 43.1%

58 c o m p u t e r m e t h o d s a n d p r o g r a m s i n b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60
Table 4 – Tortuosity coefficient on diabetic and non-diabetic corneas.
Average Std. Deviation Minimum Maximum
.5 4.6 51.0
.9 3.0 42.5
Diabetic 19.1 8Non-diabetic 16.2 6than 60 �m. The results are shown in Table 4 and Figs. 5 and 6.These results show that the automatic algorithm can retrievetortuosity coefficients in agreement to those obtained by man-ual segmentation, both on non-diabetic and diabetic corneas.
As the literature shows that diabetic corneas present highertortuosity than non-diabetic corneas [19], we compared theTC values between the two groups using the non-parametricMann–Whitney test, as the TC samples were not normallydistributed, accordingly to the Shapiro–Wilk normality test.Significant differences were found between the two groups(p = 0.03).
Fig. 4 – The Bland–Altman plot comparing automaticsegmentation against the manual segmentation, in termsof nerve length. The mean difference between automaticand manual segmentation as well as the limits ofagreement for a confidence of 95% are shown.
Fig. 5 – The Bland–Altman plot comparing tortuosity valuesbetween automatic and manual segmentation, fornon-diabetic corneas.
Fig. 6 – The Bland–Altman plot comparing tortuosity valuesbetween automatic and manual segmentation, for diabeticcorneas.
5. Discussion and conclusions
In this work we presented a fully automatic segmentationalgorithm for the identification of corneal nerves in CCMimages. We evaluated the algorithm performance in a set of 47images of the sub-basal nerve plexus from non-diabetic anddiabetic corneas. This set was extracted from a larger set of90 images available online, by rejecting low quality imagesand images whose en face section traverses obliquely sev-eral corneal layers, in order to have a set representative of theimages obtained by an ophthalmologist with experience oncorneal confocal microscopy.
Intensity correction is mandatory when processing cornealnerves image obtained through corneal confocal microscopy.The images have a non-uniform luminosity and contrast, withhigher illumination in the central region when compared withthe peripheral regions. This is due not only to the non-uniformlight reflection caused by the corneal spherical shape but alsoto attenuation differences among the illumination paths, aneffect particularly evident in cornea confocal microscopes ofthe scanning-slit type, like the one used to acquire the imagesused in this work.
The non-uniform illumination results in fewer nervesdetected on the peripheral regions when compared to cen-tral region of the image. Therefore it was necessary to correctthe non-uniform illumination. This was done by applyingthe contrast-limited adaptive histogram equalization method.The usefulness of this pre-processing correction is demon-strated when we compare the sensitivity of the segmentation
without and with illumination correction. By applying the illu-mination correction, the segmentation sensitivity improved
s i n
ft
auaaraktbtu
ckscieiitniap
owuoitae
ecnsmbrtn
fnh
sudummel
r
c o m p u t e r m e t h o d s a n d p r o g r a m
rom 70.5% to 89.8%, a very significant variation that proveshe importance of illumination correction.
The main difference between our algorithm and otherutomatic methods for corneal nerves segmentation is these of phase symmetry techniques. Being an important mech-nism to identify the structure of objects, symmetry is verydequate to identify linear structure of corneal nerves whileejecting the regular oval shape typical of most stromal ker-tocytes nuclei appearing in sub-basal plexus images. Theseeratocyte nuclei can often have brightness levels identicalo those of corneal nerves, preventing their discriminationy simple threshold techniques. The use of phase symmetryechniques allowed use to segment the corneal nerves withoutsing complex tracking strategies.
The algorithm main difficulties result from nerve dis-ontinuities or from confounding non-nerve structures likeeratocytes. Although most keratocytes are rejected by phaseymmetry, some, presenting a more linear shape, are not dis-riminated. When a segmented keratocyte intersects a nervet can be erroneously treated as a nerve branch. Anotherrror situation occurs when two or more keratocytes aren close vicinity. In this case, the morphological operationsn the nerve reconstruction phase may join these struc-ures resulting in a size that prevents exclusion by theerve reconstruction process. Improvements on the abil-
ty of the algorithm in dealing with nerve discontinuitiesnd confounding keratocytes require more sophisticatedost-processing.
The algorithm sensitivity was near 90%, with an averagef 5.3% false recognitions. These values cannot be comparedith those obtained by Scarpa et al. [22] since these authorssed the full set of 90 images, while our results were obtainedn a subset of 47 images. In our opinion, the set we used
s representative of the image quality achievable by an oph-halmologist with experience in corneal confocal microscopynd the performance of our algorithm is adequate for clinicalvaluation of sub-basal nerves.
For assessing the adequacy of our algorithm for clinicalvaluation of sub-basal nerves we calculated the tortuosityoefficient (TC) in automatically and manually segmentederves. The tortuosity values obtained by automatic nerveegmentation were in agreement to those calculated fromanually segmented images, both for non-diabetic and dia-
etic corneas. This shows that the segmentation method canetrieve an important morphometric parameter, suggesting,herefore that it is suitable for clinical evaluation of cornealerves morphology.
Significant differences were found between the TC valuesor diabetic and non-diabetic corneas. However, since we doot have any knowledge on the patient’s disease state andistory, we do not draw any conclusions from this observation.
The major objective of our work is the development of aimple, non-invasive technique, capable of accurately doc-menting the extent of nerve damage and repair, for earlyiagnosis of peripheral diabetic neuropathy, based on the eval-ation of corneal nerves morphology from corneal confocal
icroscopy images. It is necessary to establish if the seg-entation method here presented is capable of doing thisvaluation. This will be done, in the near future, using aarge set of corneal nerve images of diabetic patients and
b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60 59
non-diabetic volunteers from the Ophthalmology Clinic at theCoimbra University Hospital.
Acknowledgements
This work was supported by the following Grants: PortugueseFoundation for the Science and Technology (FCT), PTDC/SAU-BEB/73425/2006 and PTDC/SAU-BEB/104183/2008.
e f e r e n c e s
[1] C. Gooch, D. Podwall, The diabetic neuropathies, TheNeurologist 10 (2004) 311–322.
[2] P. Hossain, A. Sachdev, R.A. Malik, Early detection of diabeticperipheral neuropathy with corneal confocal microscopy,The Lancet 366 (2005) 1340–1343.
[3] C.E. Argoff, B.E. Cole, D.A. Fishbain, G.A. Irving, Diabeticperipheral neuropathic pain: clinical and quality-of-lifeissues, Mayo Clinic Proceedings 81 (2006) S3–S11.
[4] A.J.M. Boulton, A.I. Vinik, J.C. Arezzo, V. Bril, E.L. Feldman, R.Freeman, R.A. Malik, R.E. Maser, J.M. Sosenko, D. Ziegler,Diabetic neuropathies, Diabetes Care 28 (2005) 956–962.
[5] D.J. Margolis, L. Allen-Taylor, O. Hoffstad, J.A. Berlin, Diabeticneuropathic foot ulcers and amputation, Wound Repair andRegeneration 13 (2005) 230–236.
[6] T.S. Park, J.H. Park, H.S. Baek, Can diabetic neuropathy beprevented? Diabetes Research and Clinical Practice 66 (2004)S53–S56.
[7] M. Rahman, S.J. Griffin, W. Rathmann, N.J. Wareham, Howshould peripheral neuropathy be assessed in people withdiabetes in primary care? A population-based comparison offour measures, Diabetic Medicine 20 (2003) 368–374.
[8] R.A. Malik, S. Tesfaye, P.G. Newrick, D. Walker, S.M.Rajbhandari, I. Siddique, A.K. Sharma, A.J.M. Boulton, R.H.M.King, P.K. Thomas, J.D. Ward, Sural nerve pathology indiabetic patients with minimal but progressive neuropathy,Diabetologia 48 (2005) 578–585.
[9] G. Lauria, D.R. Cornblath, O. Johansson, J.C. McArthur, S.I.Mellgren, M. Nolano, N. Rosenberg, C. Sommer, EFNSguidelines on the use of skin biopsy in the diagnosis ofperipheral neuropathy, European Journal of Neurology 12(2005) 747–758.
[10] A.G. Smith, J.R. Howard, R. Kroll, P. Ramachandran, P. Hauer,J.R. Singleton, J. McArthur, The reliability of skin biopsy withmeasurement of intraepidermal nerve fiber density, Journalof the Neurological Sciences 228 (2005) 65–69.
[11] D.V. Patel, C.N. McGhee, Contemporary in vivo confocalmicroscopy of the living human cornea using white lightand laser scanning techniques: a major review, Clinical andExperimental Ophthalmology 35 (2007) 71–88.
[12] C. Quattrini, M. Tavakoli, M. Jeziorska, P. Kallinikos, S.Tesfaye, J. Finnigan, A. Marshall, A.J.M. Boulton, N. Efron,R.A. Malik, Surrogate markers of small fiber damage inhuman diabetic neuropathy, Diabetes 56 (2007) 2148–2154.
[13] D.V. Patel, C.N.J. McGhee, Mapping of the normal humancorneal sub-basal nerve plexus by in vivo laser scanningconfocal microscopy, Investigative Ophthalmology andVisual Science 46 (2005) 4485–4488.
[14] M. Tavakoli, A. Marshall, L. Thompson, M. Kenny, S. Waldek,N. Efron, R.A. Malik, Corneal confocal microscopy: a novelnoninvasive means to diagnose neuropathy in patients with
Fabry disease, Muscle and Nerve 40 (2009) 976–984.[15] M. Popper, M.J. Quadrado, A.M. Morgado, J.N. Murta, J.A. VanBest, L.J. Muller, Subbasal nerves and highly reflective cellsin corneas of diabetic patients: in vivo evaluation by

m s i n
60 c o m p u t e r m e t h o d s a n d p r o g r aconfocal microscopy, Investigative Ophthalmology andVisual Science 46 (2005) 879.
[16] E. Midena, E. Brugin, A. Ghirlando, M. Sommavilla, A.Avogaro, Corneal diabetic neuropathy: a confocalmicroscopy study, Journal of Refractive Surgery 22 (2006)S1047–S1052.
[17] O. Stachs, A. Zhivov, R. Kraak, J. Stave, R. Guthoff, In vivothree-dimensional confocal laser scanning microscopy ofthe epithelial nerve structure in the human cornea, GraefesArchive for Clinical and Experimental Ophthalmology 245(2007) 569–575.
[18] M. Mocan, I. Durukan, M. Irkec, M. Orhan, Morphologicalterations of both the stromal and subbasal nerves in thecorneas of patients with diabetes, Cornea 25 (2006) 769–773.
[19] P. Kallinikos, M. Berhanu, C. O’Donnell, A.J.M. Boulton, N.Efron, R.A. Malik, Corneal nerve tortuosity in diabeticpatients with neuropathy, Investigative Ophthalmology andVisual Science 45 (2004) 418–422.
[20] T.J. Holmes, M. Pellegrini, C. Miller, T. Epplin-Zapf, S. Larkin,S. Luccarelli, G. Staurenghi, Automated software analysis ofcorneal micrographs for peripheral neuropathy, InvestigativeOphthalmology and Visual Science 51 (2010) 4480–4491.
[21] A. Ruggeri, F. Scarpa, M. De Luca, C. Meltendorf, J. Schroeter,A system for the automatic estimation of morphometricparameters of corneal endothelium in alizarine red-stainedimages, British Journal of Ophthalmology 94 (2010) 643–647.
b i o m e d i c i n e 1 0 7 ( 2 0 1 2 ) 53–60
[22] F. Scarpa, E. Grisan, A. Ruggeri, Automatic recognition ofcorneal nerve structures in images from confocalmicroscopy, Investigative Ophthalmology and Visual Science49 (2008) 4801–4807.
[23] A. Ferreira, A.M. Morgado, J.S. Silva, Corneal nervessegmentation and morphometric parameters quantificationfor early detection of diabetic neuropathy, in: Proceedings ofIFMBE MEDICON 2010, Greece, 29, 2010,264–267.
[24] A. Ferreira, A.M. Morgado, J.S. Silva, Automatic cornealnerves recognition for earlier diagnosis and follow-up ofdiabetic neuropathy, Lecture Notes in Computer Science6112 (Part II) (2010) 60–69.
[25] R.C. Gonzalez, R.E. Woods, S.L. Eddins, Digital ImageProcessing Using Matlab, 2nd ed., Gatesmark Publishing,2009.
[26] J.S. Silva, A. Silva, B.S. Santos, Image denoising methods fortumor discrimination in high resolution computedtomography, Journal of Digital Imaging 24 (2011)464–469.
[27] P. Kovesi, Symmetry and asymmetry from local phase, in:Tenth Australian Joint Converence on Artificial Intelligence,
Australia, 1997, pp. 185–190.[28] D.G. Altman, Assessing new methods of clinicalmeasurement, British Journal of General Practice 59 (2009)399–400.