› kma › pdf › kmj › kmj_2006_03.pdf · EDITORIAL Evidence-based Medicine: Why and How? 1...
82
EDITORIAL Evidence-based Medicine: Why and How? 1 Ibrahim Hadi REVIEW ARTICLE Mirizzi Syndrome: A Review of the Literature 3 George J Xeroulis, Ward Davies ORIGINAL ARTICLES Dislocation of the Extensor Tendons Over the Metacarpophalangeal Joints 7 Ahmed F El-Morshidy, Foad Rabia, Husam Basheer Frequency of Thyroid Microsomal and Thyroid Peroxidase Antibody Levels in a Selected Group of Omani Patients with Graves’Disease 10 Masoud Al-Maskari, Adel Alnaqdy Prevalence of Osteoporosis and Determinants of Bone Mineral Density in Healthy Community- dwelling Kuwaiti Men Aged 50 Years or Older 14 Nadia S Al-Ali, Jameela M Al-Faraj, Suad A Mahseen, Fotooh A Al-Jarki, Jameela A Al-Khaldy, Prem N Sharma Antibody Prevalence and Genotype-specific Protective Immunity against Mumps Virus Infection in Children from Kuwait 21 Ola Moghnai, Alexander Pacsa, Gyorgy Szucs, Widad Al-Nakib Accuracy of Axillary Temperature Compared with Rectal Temperature in Sick Children 25 Ali Akbar Asadi-Pooya, Sara Kashef Comparison of Compliance Versus Non-compliance to Anti-hypertensive Agents in Primary Health Care - An Area Based Study 28 Ali A Al-Yahya, Amal M Al-Mehza, Huda Al-Ghareeb Risk Factors in Acute Poisoning in Children - A Retrospective Study 33 Syeda Akhtar, Gulati Raj Rani, Fahad Al-Anizi CASE REPORTS Breast Lymphoma: Case Report and Review of Literature 37 Maha SAAbdelhadi, Dalal M Tamimi, Amir M Khan Burns and Congenital Indifference to Pain in Two Sisters: A Case Report 40 Alexander George, Ibrahim Ghoneim, Mohammed Khalaf Ibrahim Transient Central Diabetes Insipidus in a Female Patient with Thrombotic Thrombocytopenic Purpura and Ectopic Pregnancy: A Possible Link - Case Repor t 43 Tarek Abdel Hamed Mostafa Dowod, Ashraf Hashem Early Neonatal Hypernatremia with Intraventricular Hemorrhage - An Unusual Presentation in Two Cases 46 Hussain Parappil, Amrit L Soni, Rima MZ Al-Sawan Caffey Silverman Disease: Case Report and Literature Review 49 Mohamed Al Fahmy Guillain-Barré Syndrome in a Patient with Romano-ward Syndrome: A Case Report 53 Thomas Vurgese, Osman Abdulwahab Mapkar, Soondal Kumar Surrun A Novel use of Ureteroscope for a Non-urological Cause - A Point of Technique 56 Shanmugasundaram Rajaian, Amitava Mukherjee, Ganesh Gopalakrishnan MARCH 2006 VOLUME 38 NUMBER 1 KMJ KUWAIT MEDICAL JOURNAL The Official Journal of The Kuwait Medical Association KU ISSN 0023-5776 Continued inside KMJ
Transcript of › kma › pdf › kmj › kmj_2006_03.pdf · EDITORIAL Evidence-based Medicine: Why and How? 1...

EDITORIALEvidence-based Medicine: Why and How? 1Ibrahim Hadi
REVIEW ARTICLEMirizzi Syndrome: A Review of the Literature 3George J Xeroulis, Ward Davies
ORIGINAL ARTICLESDislocation of the Extensor Tendons Over the Metacarpophalangeal Joints 7Ahmed F El-Morshidy, Foad Rabia, Husam Basheer
Frequency of Thyroid Microsomal and Thyroid Peroxidase Antibody Levels in a Selected Group of Omani Patients with Graves’Disease 10Masoud Al-Maskari, Adel Alnaqdy
Prevalence of Osteoporosis and Determinants of Bone Mineral Density in Healthy Community-dwelling Kuwaiti Men Aged 50 Years or Older 14Nadia S Al-Ali, Jameela M Al-Faraj, Suad A Mahseen, Fotooh A Al-Jarki, Jameela A Al-Khaldy, Prem N Sharma
Antibody Prevalence and Genotype-specific Protective Immunity against Mumps Virus Infection inChildren from Kuwait 21Ola Moghnai, Alexander Pacsa, Gyorgy Szucs, Widad Al-Nakib
Accuracy of Axillary Temperature Compared with Rectal Temperature in Sick Children 25Ali Akbar Asadi-Pooya, Sara Kashef
Comparison of Compliance Versus Non-compliance to Anti-hypertensive Agents in Primary HealthCare - An Area Based Study 28Ali A Al-Yahya, Amal M Al-Mehza, Huda Al-Ghareeb
Risk Factors in Acute Poisoning in Children - A Retrospective Study 33Syeda Akhtar, Gulati Raj Rani, Fahad Al-Anizi
CASE REPORTS Breast Lymphoma: Case Report and Review of Literature 37Maha SAAbdelhadi, Dalal M Tamimi, Amir M Khan
Burns and Congenital Indifference to Pain in Two Sisters: A Case Report 40Alexander George, Ibrahim Ghoneim, Mohammed Khalaf Ibrahim
Transient Central Diabetes Insipidus in a Female Patient with Thrombotic ThrombocytopenicPurpura and Ectopic Pregnancy: A Possible Link - Case Report 43Tarek Abdel Hamed Mostafa Dowod, Ashraf Hashem
Early Neonatal Hypernatremia with Intraventricular Hemorrhage - An Unusual Presentation in Two Cases 46Hussain Parappil, Amrit L Soni, Rima MZ Al-Sawan
Caffey Silverman Disease: Case Report and Literature Review 49Mohamed Al Fahmy
Guillain-Barré Syndrome in a Patient with Romano-ward Syndrome: A Case Report 53Thomas Vurgese, Osman Abdulwahab Mapkar, Soondal Kumar Surrun
A Novel use of Ureteroscope for a Non-urological Cause - A Point of Technique 56Shanmugasundaram Rajaian, Amitava Mukherjee, Ganesh Gopalakrishnan
MARCH 2006VOLUME 38 NUMBER 1
K M JKUWAIT MEDICAL JOURNAL
The Official Journal of The Kuwait Medical Association
KU ISSN 0023-5776 Continued inside
KMJ

THE KUWAIT MEDICAL JOURNAL March 2006March 2006Vol. 38 No. 1
C O N T E N T S
KUWAIT MEDICAL JOURNAL
Continued from cover
THE PUBLICATION OF ADVERTISEMENTS IN THE KUWAIT MEDICALJOURNALDOES NOT CONSTITUTE ANYGUARANTEE OR ENDORSEMENT BYTHE KUWAITMEDICAL ASSOCIATION OR THE EDITORIAL BOARD OF THIS JOURNAL, OF THE ADVERTISED PRODUCTS, OR SERVICES, OR OF CLAIMS MADE BY THEA D V E RTISERS. THE PUBLICATION OF A RTICLES AND OTHER EDITO R I A L M AT E R I A L IN THE JOURNAL DOES NOT NECESSARILY REPRESENT POLICYRECOMMENDATIONS OR ENDORSEMENT BYTHE ASSOCIATION.
View these articles at
http://www.kma.org.kw/KMJ
P U B L I S H E R : The Kuwait Medical Journal (KU ISSN-0023-5776) is a quarterly publication of THE KUWAIT MEDICALA S S O C I AT I O N .Address: P.O. Box 1202, 13013 Safat, State of Kuwait; Telephone: 5316023, 5317972, 5333278 Fax: 5312630, 5333276.
E-mail address: kmj @kma.org.kw
COPYRIGHT: The Kuwait Medical Journal. All rights reserved. No part of this publication may be reproduced without writtenpermission from the publisher. Printed in Kuwait.
INSTRUCTIONS FOR AUTHORS: Authors may submit manuscripts prepared in accordance with the Uniform Requirements forManuscripts Submitted to Biomedical Journals. These Requirements are published in each issue of the Kuwait Medical Journal.
CHANGE OF ADDRESS: Notice should be sent to the Publisher six weeks in advance of the effective date. Include old and newaddresses with mail codes.
KUWAIT MEDICAL JOURNAL is listed in the Index Medicus for the WHO Eastern Mediterranean Region (IMEMR), the IMEMRCurrent Contents and available at : http://emro.who.int/EMRJorList/online.aspx
KUWAIT MEDICAL JOURNAL is added to the list (The Journal of the Kuwait Medical Association) of journals adhering to the“Uniform Requirements for Manuscripts Submitted to Biomedical Journals”, American College of Physicians, Independence Mall West,Sixth Street at Race, Philadelphia, PA 19106-1572, USA, and can be located at http://www.icmje.org/jrnlist.html
❈ ❈ ❈
LETTER TO THE EDITORATravel Abroad - Associated Case of Legionella Pneumonia 59Nada Al Terkait, Sherif A Sadak
SELECTED ABSTRACTS OF ARTICLES PUBLISHED ELSEWHERE BYAUTHORS IN KUWAIT 61
FORTHCOMING CONFERENCES AND MEETINGS 65
WHO-FACTS SHEET 72
1. Avian Influenza: The Disease in Birds
2. WHO Calls for Global Action to Avert 8 Million Cancer-related Deaths by 2015
3. Cancer
ARABIC ABSTRACTS OF ARTICLES PUBLISHED IN THIS ISSUE 80

Kuwait Medical Journal (KMJ)Published by the Kuwait Medical Association
Previously known as The Journal of the Kuwait Medical Association (Est. 1967)
Honorary President: Abdulaziz Al-Babtain
EDITORIAL BOARDEditor-in-Chief: Fuad Abdulla M Hasan
Editor: Adel Khader AyedInternational Editor: Pawan K Singal
Associate Editors: Adel A AlzayedMousa KhoursheedMustafa M RidhaNasser Behbehani
Circulation Manager: Homoud Fahad Al-Zuabi
INTERNATIONALADVISORY BOARD
Allan Templeton, UK Ananda S Prasad, USAAnders Lindstrand, Sweden Andrew J Rees, UKArie van Dalen, NetherlandsBelle M Hegde, IndiaBengt Jeppsson, SwedenCharles A Dinarello, USAChristian Imielinski, PolandElizabeth Dean, CanadaFiona J Gilbert, UK
Neva E Haites, UKNirmal K Ganguli, IndiaOleg Eremin, UKPeter JB Helms, UKPeter RF Bell, UKRaymond M Kirk, UKS Muralidharan, IndiaTulsi D Chugh, IndiaWilliam ATweed, CanadaWilliam B Greenough, USAZoheir Bshouty, Canada
REGIONAL ADVISORY BOARD
Abdulla BehbehaniAbdul Mohsen JaffarAbeer K Al-BahoAlexander E OmuAli Al-MukaimiAli Al-SayeghAsmahan Al-ShubailiChacko MathewEiman M MokaddasFaisal A Al-KandariHabib Abul
Hilal Al-SayerJasbir Singh JuggiJohn F Greally Joseph C LongeneckerKamal Al-Shoumer Kefaya AM AbdulmalekKhalid Al-JarallahMarie T Greally Mazen Al EssaMohamed AA MoussaMohammed Al-Jarallah
Mousa KhadadahMubarak Al-Ajmi Mustafa Al-Mousawi Nasser J HayatNebojsa RajacicSadika Al-AwadiSaleema Al-RamadanSami AsfarSoad Al-BaharSukhbir Singh UppalWaleed Alazmi
ARABIC TRANSLATION: Arabization Centre for Medical Science (ACMLS), Kuwait
EDITORIAL OFFICEEditorial Manager : Babichan K Chandy
Language Editor : Abhay U Patwari
EDITORIALADDRESSP.O. Box: 1202, 13013-Safat, Kuwait
Telephone: (00-965) 5316023, 5317972, 5333278 - Fax: (00-965) 5312630, 5333276E-mail: [email protected] - website: www.kma.org.kw/KMJ
KMJ
Frank D Johnston, UKGabrielle M Hawksworth, UKGeorge Russell, UKGraeme RD Catto, UKJan T Christenson, SwitzerlandJaroslav Slipka, Czech RepJasbir S Bajaj, IndiaJohn V Forester, UKJulian Little, CanadaLubomir Karagiosov, BulgariaLewis D Ritchie, UK

KUWAIT MEDICAL JOURNAL
i
KUWAIT MEDICAL JOURNAL (KMJ)Instructions for Authors
AIMS AND SCOPEThe Kuwait Medical Journal (KMJ) is the official
publication of the Kuwait Medical Association. It ispublished four times annually. Clinical, scientific orlaboratory investigations of relevance to medicineare considered by the journal. Original articles, casereports, brief communications, book re v i e w s ,insights and letters to the editor can also bec o n s i d e red. Basic medical science articles arepublished under the section on ExperimentalMedicine.
GENERALThe Kuwait Medical Journal is a signatory
journal to the Uniform Requirements forManuscripts Submitted to Biomedical Journals, thefifth (1997) revision of a document by theinternational Committee of Medical JournalEditors. A description of important features of thisdocument is available on the Lancet website athttp://www.thelancet.com. Alternatively, you mayconsult the following: N Engl J Med 1997; 336:307-315 or order the leaflet “Uniform Requirements forManuscripts Submitted to Biomedical Journals”[GB£ 1 per copy] by writing to the Editor of theBritish Medical Journal (BMJ), BMA H o u s e ,Tavistock Square, London WC1H 9JR, UK.
To present your original work for consideration,one complete set of the manuscript, written inEnglish, accompanied by tables, and three sets offigures (if applicable), should be submitted to theEditor. Authors shall provide the manuscript on anIBM compatible floppy disk also (if not sent by e-mail). Details of the type of computer used, thesoftware employed and the disk system, if known,would be appreciated. The KMJ editorial office usesMicrosoft ‘Office 2003’ word processing and ‘Excel’programs.
Submissions through e-mail shall be followedby one set of hard copy, tables, figures (3 sets oforiginal), if any, and the signed consent (of all theauthors), mailed (by post/courier) to the editorialoffice. To speed up processing, author(s)’ consentletter should be faxed to the journal office (00965-5312630 or 5333276) or a scanned copy enclosed asattachment along with the article, in the e-mail. Amanuscript will be considered for processing, only ifall the relevant documents are available.
Following a peer review process, thec o r responding author will be advised of theacceptance or rejection of the paper and, in the eventof an acceptance, the approximate date of
publication. Galley proof will be forwarded to thec o r responding author and must be returned within48 hours. Corrections in the galley proof must belimited to typographical errors or missing contents,if any.
ETHICAL CONSIDERATIONSW h e re human investigations or animal
experiments are a part of the study, the journalassumes that the design of the work has beenapproved by the local ethics committee.
PREPARATION OF THE MANUSCRIPTThe manuscript should be typed as ‘normal text’
on one side of A4 size (29.7 x 21 cm) paper in singlecolumn format, preferably in font size no. 12. Italicsshould be used only to write fore i g n / L a t i ne x p ressions/terminologies. There should be a 2 cmm a rgin at both sides of the text and a 3 cm margin atthe top and bottom of each page.
The order of the text should be as follows: titlepage, abstract (stru c t u red) of no more than 250 word s(for original articles), Key Wo rds (no more than fivein small case and arranged in alphabetical ord e r ) ,followed by introduction, subjects (or materials) andmethods, results, discussion, acknowledgments,re f e rences, tables, legends to figures, and figure s .Each section should begin on a new page. For CaseStudies, provide a summary insted of the stru c t u re dabstract followed by Key words. All pages should ben u m b e red consecutively, commencing with the titlepage. Main headings, introduction, subjects andmethods, etc., should be placed on separate lines.Key Wo rds should be MeSH terms, and must notduplicate words already in the manuscript title;M e s H terms can be checked at:< h t t p : / / w w w. n l m . n i h . g o v / m e s h / M B ro w s e r. h t m l >
THE TITLE PAGETitle page of the submitted manuscript should
provide a clear title of the study. Include the fullnames of all the authors, together with the nameand address of the institution/s in which the workwas done. Also, the name and address of thec o r responding author to whom proofs andcorrespondences could be sent, are also required,together with contact e-mail address (if available)and telephone/fax numbers. If more than sixauthors are listed, the authors may be asked todescribe the contribution of each individual. Forcase reports, no more than three authors areacceptable.

Instructions for Authors
ii
STRUCTURED ABSTRACTThe stru c t u red abstract (no more than 250
words) must provide an overview of the entirepaper, and should contain succinct statements onthe following, where appropriate: Objective(s),Design, Setting, Subjects, Intervention, MainOutcome Measures, Results, and Conclusions. (See:Haynes RB, Mulrow CD, Huth AJ, Altman DG,Gardner MJ. More informative abstracts revisited.Annals of Internal Medicine 1990; 113:69-76). Thestructured abstract is required only for studiesunder the section “Original Articles”. For all othercategories, a short summary followed by Keywords should precede the report or review.
TABLESTables must be typed on separate pages and
should follow the re f e rence list. All the tables mustbe numbered consecutively. Each of them shouldhave a brief heading describing its contents and dulyre f e r red to in the main text. They should be simpleand information therein, not duplicated in the text.
DESIGN OF THE WORKThis should be stated clearly. The rationale
behind the choice of sample size should be given.Those about to begin randomized contro l l e dstudies may wish to study the CONSORTstatement (JAMA 1996; 276: 637-639).
ILLUSTRATIONSP h o t o m i c rographs, electron micrographs or
radiographs must be of high quality, and suppliedin three original final copies (not photocopies, laserprints or scanned images) of size 10 x 15 cm.Photographs should fit within a print area of 164 x235 mm. All the figures must be numbered seriallyand the figure number should appear on the backof each together with an arrow drawn to indicatethe top edge. A photomicrograph should providedetails of the staining technique and a scale bar. Forfigures where patient’s identity is not concealed,authors should submit a written consent of thepatient or of the patient’s guardian, in case ofminors. Color figures will incur a printing charge(contact the Editorial office for details). Figurelegends should be listed separately on the last pageof the article. If any tables, illustrations orphotomicrographs have been published elsewhere,a written consent for re-production is required fromthe copyright holder and the author(s). The samemust be attached to the manuscript. Charts anddrawings must be done professionally. When chartsare submitted, the numerical data on which theywere based should be supplied.
ABBREVIATIONSAbbreviations should be defined on first use
and then applied consistently throughout thearticle. Non-standard abbreviations or thoseappearing fewer than three times are not accepted.
NUMBERS AND UNITSMeasurements of length, height, weight and
volume must be reported in metric units (meter,kilogram, liter etc.) or their decimal multiples.Temperature should be given in degrees Celsius.Blood pressure should be expressed in mm Hg, andhematological and biochemical measurements inS.I. (Systeme International) units. Use a decimalpoint, and not a comma, e.g., 5.7. Use a comma fornumbers ≥ 10,000 (i.e., 103); for numbers ≤ 9999, donot use a comma (e.g., 6542). Numbers <10 shouldbe written in words.
TRADE NAMESN o n - p roprietary (generic) names of pro d u c t
should be employed. If a brand name for a drug isused, the British or international non-proprietary(approved) name should be given. The source ofany new or experimental preparation should alsobe given.
REFERENCESUse double spacing. References should appear
in sequence and must be numbered [by Arabicnumerals, in square brackets, and as superscript(e.g., [1])] in the order in which they appear in thetext. At the end of the article, the full list ofreferences should give the names and initials of allauthors unless there are more than six, in whichcase only the first three should be given, followedby et al.
The authors’ names should be followed by thetitle of the article, the title of the journal abbre v i a t e din the style of the Index Medicus, the year ofpublication, the volume number and the first and lastpage numbers. References to books should give thetitle of the book, followed by the place of publication,the publisher, the year and the relevant pages.
EXAMPLESArticle
B u r rows B, Lebowitz MD. The β a g o n i s t sdilemma (editorial). N Engl J Med 1992; 326:560-561.
BookRoberts NK. The cardiac conducting system and
His bundle electrogram. New York, A p p l e t o n -Century-Crofts, 1981: 49-56.

KUWAIT MEDICAL JOURNAL
iii
Book chapterPhilips SJ, Whisnam JP. Hypertension and
s t roke. In: Laragh JH, Bremner BM, editors.Hypertension: pathophysiology, diagnosis, andmanagement. 2nd ed. New York: Raven Press; 1995,p 465-478.
References should be limited to those relatingdirectly to the contents of the paper.
AUTHORSHIP AND CONSENT FORMAll authors must give signed consent for
publication in a letter of submission, which shouldaccompany the manuscript. This letter shouldcontain the statement that “This manuscript is anunpublished work which is not under consideratione l s e w h e re and the results contained in this paperhave not been published previously in whole or part,except in abstract form”. Each author should haveparticipated sufficiently in the work to take publicresponsibility for its content. Such participationmust include: conception, design, analysis,i n t e r p retation, or drafting the article for criticallyimportant intellectual content.
COPY RIGHTThe publisher reserves copyright on the
Journal’s contents. No part may be reproduced,translated or transmitted in any form by anymeans, electronic or mechanical, includingscanning, photocopying, recording or any otherinformation storage and retrieval system withoutprior permission from the publisher. The publishershall not be held responsible for any inaccuracy ofthe information contained therein.
SUBMISSION OF A MANUSCRIPTManuscripts should be submitted to:
The EditorKuwait Medical JournalP.O. Box: 120213013-SafatKuwait
Telephone: (965) 5316023, 5333278; 5317972Fax: (965) 5312630; 5333276E-mail : [email protected] Website: www.kma.org.kw/KMJ

KUWAIT MEDICAL JOURNALMarch 2006
Editorial
Evidence-based Medicine: Why and How?Ibrahim Hadi
Department of Anesthesia and Perioperative Medicine, University of Western Ontario, St Joseph Health Care, London,Canada
Department of Anesthesia and Intensive Care, Farwaniya Hospital, Ministry of Health, Kuwait
As physicians, how can we use published datato guide our practice? When seeing a patient, therewill be instances where questions arise either bymedical students, training residents or evennursing staff about the most appropriate diagnosis,prognosis or treatment. Often management is basedon the patterns of practice within the hospital orwithin own departmental protocols. In otherwords, on the basis of evidence from our personalexperience of treating patients over the years(anecdote) and from our personal knowledge basethat includes information that can be as old as amedical school course done in the past or as recentas an article just read. The application of evidence-based medicine (EBM) principles can help us withthis daunting task that challenges us daily toimprove the care we provide to our patients. Butwhy bother? How can EBM be applied to our dailypractice including teaching and training residents,medical students and attending physicians?
Evidence-based medicine (EBM) has beenrapidly developing over the past ten years and it isdefined by Sackett and colleagues as “theconscientious, explicit, and judicious use of currentbest evidence in making decisions about the care ofindividual patients”. The practice of EBM meansintegrating individual clinical expertise with thebest available external clinical evidence fro msystematic research[1]. This approach to patient caremay improve clinical decision making byincorporating the best available scientific literature,and reducing biases that occur when medicaldecision making is based on unsystematicobservations (anecdote), weighing the risks andbenefits of a clinical decision. EBM does notdevalue clinical skills and clinical judgment. To thecontrary, EBM demands a high level of clinical skilland judgment. The practice of EBM requires us toapply the evidence to the right patient, at the righttime and using the right resources. We need torecognize the correct patient diagnosis before
Address correspondence to:Dr. Ibrahim Hadi, MB, BCh, FRCPC, 268 Grosvenor Street St Joseph’s Health Care Room E 147, London, Ontario, Canada N6A4L6. Tel: (519)646-6000, Ext. 64219, Fax : (519) 646-6116 E-mail: [email protected]
applying the evidence to the care of the patient.Baucher[2] has identified four initiatives that are vitalto evidence-based practice which includes (A)clinician access to the Internet, (B) provision ofseminars for clinicians inexperienced withcomputers, (C) identification of reputable We bsites, and (D) accessibility of relevant informationthrough different sources.
T h e re are many sources for finding theevidence. Textbooks are ineffective sources ofrecent evidence because the information theycontain is often outdated. That is not to say thattextbooks are not useful. In fact, they are useful as as o u rce of background information on anatomy,physiology, and pharmacology. A text book is agood source for students to find large amounts offactual information. However, textbooks generallyare not good sources of best evidence. A PubMedsearch (http://www.pubmed.gov) is an inefficientmethod of finding the best evidence, because itusually returns an overwhelming amount ofinformation. For example, typing the sentence“mechanical ventilation” will yield approximately2,540 citations and it is difficult for any one personto read all of this literature and assess its validity.However, the efficient approach to finding the bestevidence is to identify a systematic review orevidence-based clinical practice guidelines[ 3 ]. Asystematic review is a summary of the literaturethat uses explicit methods which are based on athorough literature search and performs criticalappraisal of individual studies using statisticaltechniques to combine data from valid studies(meta-analysis)[4].
Evidence-based medicine categorizes differenttypes of clinical evidence and ranks them accordingto the strength of their freedom from various biases.For example, the strongest evidence for therapeuticinterventions is provided by randomized, double-blind, placebo-controlled trial. However, EBM isnot restricted to randomized trials and meta-
Kuwait Medical Journal 2006, 38 (1): 1-2

Evidence-Based Medicine: Why and How? March 20062
analysis. In fact EBM asks us to seek the bestevidence and, when randomized trials areunavailable, to fall back on observational studies.When observational studies are unavailable, it asksus to fall back on our less systematic clinicalobservations. The concept underlying EBM suggeststhat a formal set of rules must complement ourmedical training and clinical experience toeffectively apply the results of clinical research[5].The application of EBM in our daily clinical practiceremains a challenge and requires a very structuredapproach to clinical care.
Although EBM is quickly becoming the “golds t a n d a rd” for clinical practice and tre a t m e n tguidelines, there are some situations where it lacksa strong evidence base. For example, as ananesthesiologist, perhaps the longest-lived contro v e r s yin the history of obstetric anesthesia is the effect ofepidural analgesia on labor outcome. The moderndebate has centered on several main issues such as:(A) does regional analgesia for labor affect thelength of labor? (B) does regional labor analgesiaincreases the risk of cesarean section? No definitivestudy has adequately addressed any of thesequestions, and methodological problems haveplagued all available evidence. However, recentevidence from large multicenter trials demonstratesthat epidural analgesia minimally affects theprogress of established labor[6], and the risk ofc e s a rean section is not increased by epiduralanalgesia [7].
In summary, if we want to improve health carein the region and provide the best care to our
patients, EBM is an answer. It may sharpen ourskills and thus improve the way we practice, teach,and conduct research. In my opinion, evidence-based medicine practice should start early inmedical schools and college so it becomes a routineof practice in our hospitals and other healthsystems. Convenient and adequate computerresources and access should be provided where wediagnose and treat our patients. Clinical expertiseand best available external evidence shouldcomplement each other. Without either, clinicalpractice can prove detrimental to patients.
REFERENCES
1. Sackett DL, Rosenberg WMC, Gray J, et al. Evidence basedmedicine: What it is and it isn’t. British Medical Journal1996; 312: 71-72.
2. Bauchner H. Evidence-based medicine: A new science or anepidemiologic fad? Pediatrics 1999; 103:1029-1031.
3. Doig GS, Simpson F. Efficient literature searching: a coreskill for the practice of evidence-based medicine. IntensiveCare Med 2003; 29:2119-2127.
4. Cook DJ. Moving toward evidence- based practice. RespirCare 2003; 48:859-868.
5. Guyatt GH, Haynes RB, Jaeschke RZ, et al . Evidence-basedmedicine: principles for applying the users guides topatient care. Evidence-Based Medicine Working Group.JAMA2000; 284:1290-1296.
6. Halpern SH, Leighton BL, Ohlsson A, et al. Effect ofepidural vs parenteral opioid analgesia on the progress oflabor: A meta-analysis. JAMA1998; 280:2105-2110.
7. Comparative Obstetric Mobile- Epidural Trial (COMET)study group UK. Effect of low-dose mobile versustraditional epidural techniques on mode of delivery: arandomized controlled trial. Lancet 2001; 358:19-23.

KUWAIT MEDICAL JOURNALMarch 2006
Kuwait Medical Journal 2006, 38 (1): 3-6
Review Article
Mirizzi Syndrome: A Review of the Literature
Address correspondence to:George J Xeroulis, Department of Surgery, University of Western Ontario London, Ontario, Canada. E-mail: [email protected]
George J Xeroulis, Ward Davies
Department of Surgery, University of Western Ontario, London, Ontario, Canada
Mirizzi syndrome is a rare cause of obstructivejaundice. This entity should be considered in thed i ff e rential diagnosis of all patients with obstru c t i v ejaundice. Failure to recognize the conditionpreoperatively can result in a major bile duct injury,particularly during laparoscopic surg e r y[ 1 ]. Thesyndrome refers to obstruction of the commonhepatic duct by extrinsic compression usually froma gallstone impacted in Hartmann’s pouch or thecystic duct. Large gallstones that become impactedin this area produce common hepatic ducto b s t ruction by two mechanisms: mechanicalobstruction by direct compression of the commonhepatic duct, or they can cause obstru c t i o nsecondary to repeated bouts of local inflammation.
In 1948, A rgentinean surgeon Pablo LuisMirizzi, first described a syndrome of commonhepatic duct obstruction in the setting oflongstanding cholelithiasis and cholecystitis[2]. Theclassic description of the disease includes fourcomponents: (a) a close parallel course of the cysticduct and the common hepatic duct, (b) an impactedstone in the cystic duct or the neck of thegallbladder, (c) common hepatic duct obstructionsecondary to external compression by the cysticduct stone (and the surrounding inflammation),and (d) jaundice, with or without cholangitis.
Mirizzi’s syndrome is a rare complication ofcholelithiasis, with an estimated incidence of 0.05-2.7%[1,3,4]. It presents as a spectrum of disease thatvaries from extrinsic compression of the commonhepatic duct to the presence of a cholecystobiliaryfistula. Often, this dangerous alteration to anatomyis not recognized pre o p e r a t i v e l y, and has thepotential to lead to significant morbidity andbiliary injury, particularly in the laparoscopic era.
CLASSIFICATION There are three classifications which have been
proposed to describe variants of Mirizzi syndrome,and to aid in selecting the appropriate therapeuticprocedure. The original classification, by McSherry
et al[5], described two types. Type I referred tocompression of the common hepatic duct by a stoneimpacted in the cystic duct or Hartmann’s pouch.Type II referred to erosion of the calculus from thecystic duct into the common hepatic duct,producing a cholecystocholedochal fistula.
Csendes et al[6] created a second classificationtaking into account the extent of fistula. Type Iremained the same, external compression of thecommon hepatic duct due to a stone impacted atthe neck of the gallbladder or at the cystic duct.Types II to IV lesion referred to the presence andextent of a cholecystobiliary (cholecystohepatic orcholecystocholedochal) fistula, due to erosion ofthe anterior or lateral wall of the common hepaticduct by impacted stones. The fistula involved lessthan one-third of the circumference of the commonhepatic duct in type II. Involvement of betweenone-third and two-thirds of the circumference ofthe common hepatic duct was called a type IIIlesion, while destruction of the entire wall of thecommon hepatic duct was called a type IV lesion.In their original paper, a total of 219 patients wereidentified with Mirizzi’s syndrome. The incidenceof type I lesions was 11 per cent, type II, 41 per cent,type III, 44 per cent and type IV, four per cent. Themajority had obstructive jaundice.
The third classification, proposed by Nagakawaand colleagues[7], expanded upon the definition ofthe Mirizzi syndrome. Type I referred to a stoneimpacted in the cystic duct or gallbladder neck.Type II was characterized by a fistula of thecommon duct. Type III was defined by hepatic ductstenosis due to a stone at the confluence of thehepatic and cystic ducts. Type IV was characterizedby hepatic duct stenosis as a complication ofcholecystitis in the absence of calculi impacted inthe cystic duct or gallbladder neck.
In one series of 30 patients, the frequency ofthese four types as described by Nagakawa et alwas 14, 2, 6, and 8%, respectively[8].
INTRODUCTION

Mirizzi Syndrome: A Review of the Literature March 20064
Mirizzi syndrome is part of the differentialdiagnosis of all patients with obstructive jaundice,and re q u i res a high index of suspicion. Mostpatients present with jaundice, and right upperquadrant pain[1]. Elevations in the serum concentra-tions of alkaline phosphatase and bilirubin arepresent in over 90 per cent of patients[8,9]. Theclinical and laboratory findings are similar topatients who present with obstructive jaundicesecondary to choledocholithiasis. Once a diagnosisof obstructive jaundice has been made anabdominal ultrasound is often the first imaging testpreformed. Imaging generally reveals gallstones,dilated intrahepatic ducts, with a long parallelcystic duct and a contracted gallbladder[10]. Thepresence of a stone impacted in the gallbladderneck and an abrupt change to a normal width of thecommon duct below the level of the stone are alsovery suggestive of Mirrizi’s syndrome. Thesensitivity of ultrasound in detecting Mirizzi’ss y n d rome is 23-46%[ 3 , 4 ]. In Csendes’ series,ultrasound revealed dilated ducts in 81% ofpatients and raised suspicion of Mirizzi’s syndromein only 27% of cases. CT scanning has a similarsensitivity to ultrasound, but can be helpful indiagnosing other causes of obstructive jaundicesuch as gallbladder cancer, cholangiocarcinoma, ormetastatic tumor [11].
CHOLANGIOGRAPHY Direct cholangiography is usually necessary to
establish the correct diagnosis and to delineate thehepatic duct anatomy[10]. Pre-operative diagnosis is
Table 1: Various Classification Systems of Mirizzi’s Syndrome
McSherry Csendes Nagakawa
Extrinsic compression ofthe common hepatic ductby stones generally impac-ted in the cystic duct or inthe infundibulum of thegallbladder
Presence of cholecystobi-liary fistula
Extrinsic compression of thecommon hepatic duct by stonesgenerally impacted in the cysticduct or in the infundibulum ofthe gallbladder
P resence of cholecystobiliaryfistula with diameter one thirdof circumference of the commonhepatic duct wall
P resence of cholecystobiliaryfistula with diameter two thirdof circumference of the commonhepatic duct wall
P resence of cholecystobiliaryfistula which involves the entirecircumference of the commonhepatic duct wall
Extrinsic compression (stenosis) ofthe common hepatic duct by stonesgenerally impacted in the cysticduct or in the infundibulum of thegallbladder
Fistulization of common hepaticduct from a stone impacted in thecystic duct or in the infundibulumof the gall bladder
Common hepatic duct stone at thecystic duct-hepatic duct confluence
Common hepatic duct stenosiscaused by cholecystitis withoutstones in the cystic duct orinfundibulum of the gallbladder
Type I
Type II
Type I
Type II
Type III
Type IV
Type I
Type II
Type III
Type IV
essential in avoiding CBD injuries[12,13,14]. If it wasunexpectedly encountered at the time of surgery, acautious approach should be taken. Periductalinflammation and the potential for a cholecysto-choledochal fistula make a trial dissectionparticularly challenging and should only beundertaken by an experienced surgeon. Additionalimaging is often needed to obtain details of thebiliary anatomy. Intraoperative cholangiogram orclosing and obtaining a postoperative ERCP orMRCP should be considered. Cholangiography(intraoperative or ERCP) as well as MRCP willallow for an accurate assessment of anatomy andclassification of the type of Mirizzi’s syndrome (Fig. 1).
The possibility of stone retrieval and biliarystenting during ERCP is an added advantage ini m p roving surgical outcome, and stenting alsofacilitates identification of the CBD duringoperative dissection[ 7 , 1 5 , 1 6 ]. When ERCP i sunsuccessful or difficult, percutaneous transhepaticcholangiography (PTC) is a viable alternative.
MRCP and ERCP are equivalent in their abilityto diagnosis and to delineate details of biliarystrictures, and to detect a cholecystocholedochalfistula [4]. In addition, T2 weighted images cand i ff e rentiate a neoplastic mass from aninflammatory one which US or CT scan may not becapable of [17]. Early ERCP is preferred when biliarysepsis is the dominant clinical issue and where abeneficial endoscopic therapeutic procedure can beinstituted at the same time. By contrast, MRCP isused in the non-septic patient to corroborate thesuspicion of malignancy or stones after initialimaging with US or CT scans[4].

KUWAIT MEDICAL JOURNAL 5March 2006
TREATMENT Surgery is the mainstay of therapy of Mirizzi
s y n d rome, the dense inflammatory reaction inCalot’s triangle, as well as the frequent aberrantbiliary anatomy, pose a difficult challenge to theunsuspecting surgeon when dealing with a Mirizzisyndrome. The two principal aims are (a) the safecompletion of cholecystectomy without injuringthe biliary system and (b) the appro p r i a t emanagement of the cholecystocholedochal fistula.Meticulous dissection and vigilance are essential inorder to avoid inadvertent bile duct injury. If thediagnosis of Mirizzi syndrome is made pre o p e r a t i v e l y,an operative strategy that minimizes the risk ofinjury to the biliary tract can be carried out.H o w e v e r, a preoperative diagnosis of Mirizzisyndrome is seldom made because ERCPand directcholangiography are not widely used. ERCP, directcholangiography, or magnetic resonance cholangio-graphy should be performed in patients withclinical jaundice and signs and symptomssuggestive of biliary obstruction.
A s t a n d a rdized surgical approach has beenrecommended based on the Csendes classificationof the variants of Mirizzi syndrome [6]:
l Type I - Cholecystectomy plus common bileduct exploration with T-tube placement.Exploration should be performed only if the CBD iseasily exposed. l Type II - Suture of the fistula with absorbable
material or choledochoplasty with the re m n a n tgallbladder.
l Type III - Choledochoplasty; suture of thefistula is not indicated. l Type IV - Bilio-enteric anastomosis is
preferred since the entire wall of the common bileduct has been destroyed.
l The approach may vary with the type offistula present; both the operative mortality andpostoperative morbidity increase according to theseverity of the lesion [6].
LAPAROSCOPIC SURGERYThe Mirizzi syndrome presents a diff i c u l t
challenge for laparoscopic surgery because thedense adhesions and edematous inflammatorytissue cause distortion of the normal anatomy andincrease the risk for biliary injury. While it appearsto be feasible, especially for type I anatomy[18,19], theroutine use of laparoscopic surgery as the primarytreatment of Mirizzi syndrome is controversial[20,21].It has been suggested, that a prudent approach fortype 1 Mirizzi syndrome is to perform a triallaparoscopic dissection, but to have a low thresholdto convert to an open procedure. This approachshould be undertaken only by experiencedlaparoscopic surgeons[18,20].
ENDOSCOPIC THERAPY Endoscopic treatment with or without
electrohydraulic lithotripsy (EHL) can be effectiveas a temporizing measure before surgery and canbe definitive treatment for unsuitable surg i c a lc a n d i d a t e s[ 9 , 2 2 , 2 3 ]. One report described theexperience with 14 patients with Mirizzi syndrometreated with EHL[9]. Twelve patients had a singlestone and complete clearance was achieved withone treatment session; two had multiple stones andre q u i red an additional treatment session.Asymptomatic leakage of contrast medium fromthe cystic duct into the peritoneal cavity wasobserved in one patient after removal of a largeimpacted cystic duct stone. This patient recoveredwith conservative therapy and suffered no adverseevents. In another series of 25 patients withcholangiographic evidence of Mirizzi syndrome, 12w e re re f e r red for surgery after pre l i m i n a r yendoscopic therapy and 13 were treated solely withendoscopy[23]. Stones were completely removed inthree and nine were treated with long-term stents;complications occurred in four patients[23].
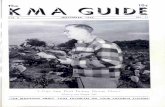
Fig. 1: Endoscopic re t rograde cholangiopancreatography (ERCP) ofpatient with obstructive jaundice and Mirizzi’s syndrome. Noticeimpacted stone in cystic duct causing obstruction of common hepaticduct. Adapted from UptoDate “Mirizzi Syndrome” James B McGee.

Mirizzi Syndrome: A Review of the Literature March 20066
Endoscopic treatment of Mirizzi syndro m eshould be used as a temporizing measure beforesurgery. It can serve as a definitive treatment forthose patients who are unsuitable surg i c a lcandidates when further endoscopic attempts canbe made to disimpact and remove the stones. Long-term success appears to be most likely in patientswith type II disease who do not have residualgallbladder stones[24].
CONCLUSIONMirizzi syndrome is a rare complication of
cholelithiasis and requires a high index of suspicionin the setting of obstructive jaundice. Diagnosispreoperatively may be elusive with bloodwork, USand CT alone. Cholangiography (intraoperativeand ERCP) as well as MRCP aids in both thediagnosis and identification of anatomy and mayp revent serious biliary injury. Surgery is themainstay of therapy of Mirizzi syndrome, andrequires the safe completion of cholecystectomywithout injuring the biliary system and thea p p ropriate management of the cholecysto-choledochal fistula. The aberrant anatomy intrinsicto this syndrome presents a difficult challenge tosurgeons and the laparoscopic approach should beundertaken with caution and probably left tospecialized minimally invasive centres. Endoscopict reatment may be effective as a temporizingm e a s u re before surgery and can be definitivetreatment for unsuitable surgical candidates.
REFERENCES
1. Waisberg J, Corona A, de Abreu IW, Farah JFM, LupinacciRA, Goffi FS. Benign Obstruction of the Common HepaticDuct (Mirizzi Syndrome): diagnosis and operativemanagement. Arq Gastroenterol 2005; 42:13-18.
2. Mirizzi, PL. Syndrome del conducto hepatico. J Int de Chir1948; 8:731-733.
3. Yeh, CN, Jan, YY, Chen, MF. Laparoscopic treatment forMirizzi syndrome. Surg Endosc 2003; 17:1573-1578.
4. Chan CY, Liau KH, Ho CK, Chew SP. Mirizzi syndrome: adiagnostic and operative challenge. Surgeon 2003;1:273-278.
5. McSherry, CK, Ferstenberg, H, Virshup, M. The Mirizzisyndrome: Suggested classification and surgical treatment.Surg Gastroenterol 1982; 1:219-225.
6. Csendes, A, Diaz, CJ, Burdiles, P, et al. Mirizzi syndromeand cholecystobiliary fistula: A unifying classification. Br JSurg 1989; 76:1139-1143.
7. Nagakawa, T, Ohta, T, Kayahara, M, et al. A n e wclassification of Mirizzi syndrome from diagnostic andtherapeutic viewpoints. Hepatogastro e n t e rology 1997;44:63-67.
8. I b r a rullah, M, Saxena, R, Sikora, SS, et al. Mirizzi’ssyndrome: Identification and management strategy. Aust NZ J Surg 1993; 63:802-806.
9. B i n m o e l l e r, KF, Thonke, F, Soehendra, N. Endoscopictreatment of Mirizzi’s syndrome. Gastrointest Endosc 1993;39:532-536.
10. Becker, CD, Hassler, H, Terrier, F. Preoperative diagnosis ofthe Mirizzi syndrome: Limitations of sonography andcomputed tomography. Am J Roentgenol 1984; 142:591-596.
11. Berland, LL, Lawson, TL, Stanley, RJ. CT appearance ofMirizzi syndrome. J Comput Assist Tomogr 1984; 8:165-166.
12. Baer, HU, Matthews, JB, Schweizer, WP, et al. Managementof the Mirizzi syndrome and the surgical implications ofcholecystocholedochal fistula. Br J Surg 1990; 77:743-745.
13. Dewar G, Chung SCS, Li AKC. Operative strategy inMirizzi syndrome. Surg Gynecol Obstet 1990; 171:157-159.
14. Fan ST, Lau WY, Lee MJR, et al. Cholecysto-hepaticodochalfistula: the value of pre-operative recognition. Br J Surg1985; 72:743-744.
15. Cotton PB. Endoscopic management of bile duct stones.Gut 1984; 25:587-597.
16. Siegel JH, Yatto RP. Biliary endoprosthesis for themanagement of retained bile duct stones. Am JGastroenterol 1984; 79:50-54.
17. Choi BW, Kim MJ, Chung JJ, et al. Rdiologic findings ofMirizzi with emphasis on MRI. Yonsei Med J 2000;41(1):144-146.
18. Vezakis A, Davides D, Birbas K, et al. Laparo s c o p i ctreatment of Mirizzi syndrome. Surg Endosc 2000; 10(1): 15-18.
19. Chowbey PK, Sharma A, Mann V, Khullar R, Baijal M,Vashistha A. The management of Mirizzi syndrome in thel a p a roscopic era. Surg Laparosc Endosc Percutan Te c h2000;10:11-14.
20. Targarona EM, Andrade, E, Balague, C, et al. Mirizzi’ssyndrome. Diagnostic and therapeutic controversies in thelaparoscopic era. Surg Endosc 1997; 11:842-845.
21. Sare M, Gurer S, Taskin V, et al. Mirizzi’s syndrome: Choiceof surgical procedure in the laparoscopic era. Surg LaparoscEndosc 1998; 8:63-67.
22. Binnie NR, Nixon SJ, Palmer KR. Mirizzi syndro m emanaged by endoscopic stenting and laparo s c o p i ccholecystectomy. Br J Surg 1992; 79:647.
23. England RE, Martin, DF. Endoscopic management ofMirizzi’s syndrome. Gut 1997; 40:272-276.
24. Tsuyuguchi T, Saisho H, Ishihara T, et al. Long-term follow-up after treatment of Mirizzi syndrome by pero r a lcholangioscopy. Gastrointest Endosc 2000; 52:6390-644.

KUWAIT MEDICAL JOURNALMarch 2006
ABSTRACT
Objectives: To describe our experience and resultsin treating extensor tendon dislocation and toreview the related literature.Subjects and methods: A total of seven patientswith dislocation of the extensor tendon over themetacarpophalangeal joints were seen during the last15 years in Al-Razi Hospital, Kuwait. All patientsw e re diagnosed and treated surg i c a l l y. There was nohistory of trauma and no case proved to berheumatoid. All cases have full flexion and mildlimited extension. A complete tear in the sagittalband of the extensor tendon was diagnosed. This wast reated by release of the juncturae tendinum on the
side of the dislocation, and imbrication of the rent ofthe sagittal band. This realigned the tendon overthe metacarpophalangeal joint. All patients werefollowed for upto one to three months from injuryto operation time.R e s u l t s : All patients had full re c o v e r y. Theyremained asymptomatic, attained full range ofmotion with no re c u r rence of the dislocation. Conclusion: Release of the juncturae tendinum onthe side of dislocation of the extensor tendon andrepair of the sagittal band will cure the dislocation ofthe extensor tendon over the metacarpophalangealj o i n t .
KEYWORDS: extensor tendon dislocation, juncturae tendinum, metacarpophalangeal joint, sagittal band
Original Article
Dislocation of the Extensor Tendons Over theMetacarpophalangeal Joints
Address correspondence to: Ahmed F. El-Morshidy, MD, Al-Razi Orthopedic Hospital, P. O. Box 4235, Safat 13043, Kuwait. Tel: 4843922, Fax: 5636657, E- mail:[email protected]
Kuwait Medical Journal 2006, 38 (1): 7-9
Ahmed F El-Morshidy, Foad Rabia, Husam BasheerDepartment of Hand Surgery, Al-Razi Orthopedic Hospital, Kuwait
INTRODUCTIONThe extensor mechanism of the metacar-
pophalyngeal joint (MCPJ) is comprised of thelongitudinal extensor digitorum communis (EDC)tendon and the transverse peripheral fibers, termedthe sagittal bands. Intact sagittal bands preventsubluxation of the EDC tendon[1-4]. The extensortendons are also stabilized by the juncturaetendinum, which are fibrous connections betweenthe tendons proximal to the MCP joints. Beneaththe extensor hood is the thick dorsal capsule, whichcontributes to the protection of the MCP joint[1].
Dislocation of the extensors over the MCPJ hasbeen extensively reported in patients withrheumatoid disease [ 5 ]. However, reports in thel i t e r a t u re on patients with other etiologies arescarce. There is a controversy over the etiology andthe pathology of dislocation[6]. Several studies andstandard texts suggest that the sagittal bands of theextensor hood form the principle centralizingstructure for the extensor tendons; they tighten andhold the tendons over the MCP joints duringflexion[7]. Without these restraining structures, thetendons tend to follow the ulnar slope of the
metacarpal heads[8] and generally would dislocatein an ulnar direction on flexion. Radial dislocationhas also been reported[9]. Other anatomic structuresalso play a role in maintaining the central positionof the extensor tendon, for example, theintertendinous fascia, the dorsal hood, and thejuncturae tendinum[10].
Abnormalities of these stru c t u res may thencontribute to extensor tendon dislocation. Failureof the sagittal bands to centralize the tendon maybe due to congenital pathology[5]. We report onseven cases with dislocation of the extensor tendonover the MCPJ.
MATERIAL AND METHODBetween 1988 and 2003, seven patients with
dislocation of the extensor tendon over the MCPJwere treated at our unit. They were five female andtwo male patients, between the ages of 14 and 25years (mean = 20 years). All cases pre s e n t e dwithout any clear history of trauma and with avariable duration of at least a month. A l ldislocations occurred during daily activities,

Dislocation of the Extensor Tendons Over the Metacarpophalangeal Joints March 20068
including finger flicking or paper crumpling. Thelong finger was affected in six patients and theindex finger in one. The displacement of theextensor tendon was in an ulnar direction in the longf i n g e r, while the dislocation in the index was radial.T h e patients complained of disabling discomfort andsnapping over the involved joints. In addition, thepatient with the index dislocation had inability toactively extend the MCPJ after full flexion due tolocking of the extensor tendon volary.
All patients were operated between one to thre emonths from injury after failed conservativet reatment. They were operated under local anestheticinfiltration and arm tourniquet. On exploration, therewas an obvious tear of the sagittal band on theopposite side of the dislocation. The juncturaetendinum on the side of the dislocation was incised.For the patient with the index dislocation we incisedonly the radial sagittal band. In all patients the rent inthe sagittal band was re p a i red by imbrication of theedges. Asking the patient to actively mobilize themetacarpophalangeal joint and to extend the fingeragainst resistance tested stability. The MCPJ wasimmobilized in extension, in a custom made staticsplint for six weeks, and was later re f e r red forp h y s i o t h e r a p y. Follow-up evaluation was betweenone year and three years using a short questionnaireand a physical examination.
RESULTSAll patients had no recurrence of the dislocation.
They regained full range of motion. Six patientswere symptom free at the last appointment. Onepatient, in spite of no recurrence, persisted to havesome discomfort and tenderness at the site of tear o fthe sagittal band for more than a year. She wasgenerally satisfied with the result at the last follow-up.
DISCUSSIONG l a d d e n[ 11 ] reported on dislocation of the
extensor tendon over the MCPJ in athletes andnamed it “Boxer’s Knuckle”; he operated on theadvanced cases and found soft tissue injury of thedorsal stru c t u res of the MCPJ. Koniuchi [ 1 2 ]
described a similar presentation in a different set ofpatients; they discovered a tear in the sagittal bands(SB). Although they did not notice a tear in thedorsal hood, they described an evidence of chronicinflammation. Posner and Ambrose[1] reported oncapsular injury in six patients with clear history oftrauma. Ryan and Murray[2] found SB tear only intheir operated cases and their patients did notreport a history of trauma. Arai et al[13] describedsimilar injuries to the MCPJ in patients who gave adefinitive history of trauma. In their series hereports on dislocation occurring in all fingers albeitmostly in the middle finger. They also found the
dislocation to occur in both directions but mostly inan ulnar direction. All their operated cases hadcapsular injury in addition to a tear in the SB. Bentset al[ 1 4 ] reported on a boxer with diverg e n tdislocation of the extensor tendons over the MCPJ.He was found to have a torn dorsal hood andcapsule, as well as torn SB. Ishizuki M[ 7 ]
differentiated between two types of injuries. Thefirst type was due to direct trauma to the MCPJ,and in this group there was a tear of the dorsalhood, capsule and the SB. In the second type, therewas no history of trauma and in this group therewas a tear in the SB’s superficial layer with an intactdorsal hood and capsule.
We agree with Ishizuki that there are twodifferent entities according to the pathology andthey should be differentiated. The traumatic type isthe one with capsular tear which will not healwithout surgery. Patients that presented without aclear history of trauma are divided into two groupsaccording to the duration of the injury[2]. If theduration is less than three weeks they wouldrespond to splinting of the MCPJ in extension.Otherwise, they should be operated. The type ofsurgery is also variable with many suggestions inthe literature[1-5]. Release of the SB and imbricatingthe edges of the injured SB, strengthening withre routed slip of the extensor tendon with orwithout release of the juncturae tendinum or usingthe latter as a flap to strengthen the extensor tendonbalance were all tried with good results.
We operated on all our cases because in all ofthem conservative management had failed. Wereleased the juncturae tendinum for the long fingeron the side of the dislocation, and imbricated therent in the SB. This aligned the tendon in a stableposition. Because the index does not have ajuncturae tendinum on the radial side, we felt itwould be safer to release the radial SB in additionto repair of the rent in the ulnar SB. This wass u fficient to stabilize the tendon in a re d u c e dposition.
CONCLUSIONBased on our experience, we feel that such cases
should be treated conservatively for one to threemonths. However, surgery should not be delayedbeyond three months so that the repair is easy andscarring in the SB and plasties can be avoided.
REFERENCES
1. Posner MA, Ambrose L. Boxer’s knuckle dorsal capsularrupture of the metacarpophalangeal joint of the finger. JHand Surg 1989; 14:229-236.
2. Rayan GM, Murray D. Classification and treatment ofclosed sagittal band injuries. J Hand Surg 1994; 19:590-594.
3. Hame SL, Melone CP. Boxer’s knuckle in the professional

KUWAIT MEDICAL JOURNAL 9March 2006
athlete. Am J Sports Med 2000; 28:879-882.4. Hame SL, Melone CP. Boxer’s knuckle. Hand Clinics 2000;
16:375-380.5. Inoue G, Tamura Y. Dislocation of the extensor tendons
over the metacarpophalangeal joints. J Hand Surg 1996;21:464-469.
6. Wehbe A. Juncturae anatomy. J Hand Surg 1992; 17:1124-1129.
7. Ishizuki M. Traumatic and spontaneous dislocation ofextensor tendon of the long finger. J Hand Surg 1990;15:967-972.
8. Hakstain RW, Tubiana R. Ulnar deviation of the fingers: therole of joint structure and function. J Bone Joint Surg 1967;49:299-316.
9. Posner MA, McMahon MS. Congenital radial sublaxationof the extensor tendons over the metacarpophalangeal
joints: a case report. J Hand Surg 1994; 19:659-662. 10. Lourie GM, Lundy DW, Rudolph HP, Bayne LG. Abducted,
hyperextended small finger deformity of nonneurologicetiology. J Hand Surg 1999; 24:315-319.
11. Gladden JR. Boxer’s knuckle. A preliminary report. Am JSurg 1957; 93:388-397.
12. Koniuchi MP, Peimer CA, Va n G o rder T, Moncada A .Closed crush injury of the metacarpophalangeal joint. JHand Surg 1987; 12:750-757.
13. Arai K, Toh K, Nakahara S, Nishikawa, Harata S. Treatmentof soft tissue injuries to the dorsum of the metacarpo-phalangeal joint (Boxer’s knuckle). J Hand Surg 2002;27:90-95.
14. Bents RT, Metz JP, Topper SM. Traumatic extensor tendondislocation in a boxer. Med Sci Sports Exerc 2003; 35:1645-1647.

KUWAIT MEDICAL JOURNAL March 2006
ABSTRACT
Introduction: Recent literature has suggested thatanti-thyroid peroxidase antibody (TPO) is a moresensitive marker of autoimmune thyroid diseases(AITD) including Graves’ disease (GD) than thea n t i - t h y roid microsomal antibody (ATMA). Wecompared serum values for TPO and ATMA inOmani Patients with GD.Material and Methods: Anti-TPO antibodies andATMA were measured on sera from 111 Omanipatients with GD. Sera from patients with systemiclupus erythematosus (SLE) and 50 healthy normalsubjects were also included as control.
Results: T h e re was a significant dif f e rence (p< 0.001) between the percentage of positive sera forboth TPO and ATMA (72% and 64%) in GD whencompared to those from SLE (15% and 17.5%) andnormal controls (6% and 8%) respectively. Therewere no differences in their levels between treatedand untreated GD patient groups. There was apositive correlation between TPO and ATMA (r =0.0914, p < 0.00001) in GD patients.Conclusion: We conclude that there is a strongcorrelation between the two assays (ATMA andTPO) and TPO assay can replace the old ATMAassay in diagnosing AITD such as GD.
KEY WORDS: autoantibody,ATMA, A-TG-A, Graves’ disease, TPO
Original Article
Frequency of Thyroid Microsomal and Thyroid PeroxidaseAntibody Levels in a Selected Group of Omani Patients
with Graves’ Disease
Address correspondence to:Dr. M. AL-Maskari, College of Medicine and Health Sciences, P.O. Box 35, Al-Khod 123, Sultanate of Oman. Tel: 00968-9311312, Fax: 00968-686332, E-mail: [email protected]
Kuwait Medical Journal 2006, 38 (1): 10-13
Masoud Al-Maskari1, Adel Alnaqdy2
Departments of 1Medicine and 2Microbiology and Immunology, College of Medicine and Health Sciences, Sultan Qaboos University, Sultanate of Oman
INTRODUCTIONA n t i - t h y roid microsomal antibodies (AT M A )
are circulating immunoglobulins directed against acomponent of the smooth endoplasmic reticulum ofthyroid cells. ATMA was found in the blood ofpatients with Hashimoto’s thyroiditis, idiopathicmyxedema and in the patients with Graves’ disease(GD)[1]. ATMA have been used as a marker ofautoimmune thyroid diseases (AITD). Later, it wasdemonstrated that microsomal antigen isantigenically related with thyroid pero x i d a s eantibodies (TPO) and that TPO is responsible forthe autoimmune reactivity of the micro s o m a lantigen[2].
Several methods have been used to detectATMAand TPO antibodies since the tanned red cellhemagglutination technique described by Boyden [3]
in 1951 for thyroglobulin antibodies. They includei m m u n o f l u o rescence,radio-immunoassay andELISA. Immunofluorescence and RIAare graduallyabandoned for practical reasons while both passivehemagglutination assays and ELISA are widelyused. Independently of the intrinsic quality ofcommercial assays, it seems that ELISA techniques
are more suitable for quantitative determinationsand may reflect more accurately the response of theautoimmune process to treatment[4].
The use of thyroid autoantibody measurementhas been hampered by specificity problems inwhich results vary widely depending on themethod used due to diff e rences in both thesensitivity and specificity of the methods and theabsence of adequate standardization. The questionof whether TPO accounts for part or all of theantigenic activity that is recognized by circulatingATMA remains to be determined.
In this study, we tried to evaluate theprevalence, correlation and diagnostic significanceof both antibodies in Omani patients with GD as amodel for autoimmune thyroid disease.
MATERIALS AND METHODS S u b j e c t s : One hundred and eleven adult
subjects (75 female and 36 male) with a clinicaldiagnosis of Graves’ disease and age rangingbetween 16-66 years (mean = 32.4 years) wereincluded in the study. On the basis of treatment

KUWAIT MEDICAL JOURNAL 11March 2006
with thyroid iodine therapy (I131), patients weregrouped into treated (78 patients; 54 female and 24male) and untreated (33 patients; 21 female and 12male) groups. A further 40 patients with SLE (asautoimmune non-thyroid controls, 27 female and13 male; age range = 14-59; mean = 28.7 years) and50 healthy control subjects (25 female and 15 male;age range = 19-62; mean = 25.1 years) wereincluded in the study. The three selected groupsconsisted of Omani individuals and were matchedin terms of age and sex (no significant diff e re n c e s ;p > 0.005). Sera from all patients and normalsubjects were screened for the presence of ATMA,TPO and A-TG-A.
MEASUREMENT OF ATMA AND A-TG-A:The test used a passive hemagglutination
commercial Kit (Murex Thymune T & Thymune M,Biotech Limited, Kent-England). Turkey erythro-cytes coated with the thyroglobulin or microsomalantigens are agglutinated by ATMA and A-TG-Ayielding an even carpet of cells at the bottom of amicrotiter well; lack of agglutination is indicated bythe cells settling into a tight ring or button.Complement in sera was heat-inactivated at 56 0Cfor 30 minutes prior to testing, to avoiderythrocytes lysis. Positive and negative controlsw e re included in each microtiter plates. Non-specific reactions were detected by usingunsensitised control cells. Sera and erythrocyteswere mixed, then incubated at room temperaturefor one hour in the case of ATMA and for 30minutes in the case of A-TG-A tests. Titers greaterthan 1:20 (A-TG-A) and greater than 1:100 (ATMA),w e re re g a rded as positive. The coefficiency ofvariation (CV) was less than 7%.
MEASUREMENT OF TPO:An ELISA assay (Medizym anti-TPO, Medipan
Diagnostica; Germany) was employed for thequantitative measurement of human thyro i dperoxidase antibodies (TPO) in serum. A standardELISA technique was employed using buffers andreagents supplied with the kit. All the procedureswere performed according to the manufacturers’instructions. TPO antibody values of > 30 IU/mlwere considered as positive. The CV was 5.1%.
STATISTICAL ANALYSIS:Statistical analysis was performed using χ2 test
from SPSS for windows program. A p-value < 0.05was considered as significant.
RESULTSThe overall frequency of A M TA and TPO
antibodies among patients with GD tested were64% and 72% respectively. In the SLE and normalcontrol groups, ATMA and TPO antibodies werepositive in 17.5% and 15% and 8% and 6% subjectsre s p e c t i v e l y. There was a significant diff e rence (p< 0.001) in the frequency of each of ATMA, TPOand A-TG-A antibodies in sera from GD patientswhen compared to each SLE patients and normalcontrols (Fig. 1). A significant positive correlationwas observed between ATMA and TPO antibodylevels (r = 0.914, p < 0.00001) in patients with GD.
A-TG-A serum levels were the lowest in allgroups when comparing to those of ATMAor TPO.Their levels were 6%, 8% and 2% for the GD, SLEand normal groups respectively. No difference wasobserved between groups according to female /male ratio and age.
Fig. 1: Positive anti-thyroid peroxidase (TPO), anti-thyroid microsomal(ATMA) and anti-thyroglobulin (A-TG-A) antibodies in patients withGraves’ disease (GD) showed a significantly high difference whencompared to same levels in sera from patients with systemic lupuserythematosus (SLE) and healthy normal subjects (p < 0.001)
Fig. 2: Percentage of patients with Graves’ disease positive for anti-thyroid peroxidase (TPO), anti-thyroid microsomal (ATMA) and anti-thyroglobulin (A-TG-A) antibodies according to treatment status (nosignificant differences)

Frequency of Thyroid Microsomal and Thyroid Peroxidase Antibody Levels in a Selected ..... March 200612
Fig. 2 shows the differences between patientstreated with I131 (n = 78) and untreated ones (n =33). Positive ATMA levels in the treated groupwere lower (42%) than similar levels among theuntreated group (67%) though this difference didnot reach a significant level. No significantdifference was observed, between positive valuesof treated (70%) and untreated group (75%) whenTPO values were compared. Similarly, there was nosignificant difference between positive sera for A-TG-A in treated (26%) and untreated (42%) patientswith GD.
Out of the 71 patients with GD who werepositive for ATMA, 43 had high titer (> 1:400) and28 patients had low titer (< 1:400). On the otherhand, out of 80 patients who were positive for TPOantibodies, 54 had high titer and 26 patients hadlow levels. There was no significant difference inthe distribution of high and low titers of bothATMA and TPO among the treated and untreatedgroups. In the normal control group; four subjectsgave low titer and none had high positive whentested for ATMA. On the other hand, only twonormal subjects had low titer and only one showeda moderately high titer.
DISCUSSION The present study showed a high frequency of
anti-TPO antibodies in Omani patients with GDwhich agreed with earlier studies [5-8]. Nevertheless,another group had found TPO antibody in GDpatients to be much lower[9]. The wide range offrequency in various reports may be due to thedifferences in ethnic background, geographical areaor the sensitivity and specificity of the methodemployed.
The significance of TPO antibody titerdifferences in GD is not well defined. Patients withGD are usually positive for several thyro i dautoantibodies and there f o re, it is difficult toseparate the effects related to one of the antibodies.Some investigators have correlated those titers withsome clinical importance for instance, elevated TPOantibodies in early pregnancy was suggested torepresent a risk factor for post-partum thyroiditis[10].
An earlier study had surveyed 17,000 subjectswithout apparent thyroid disease and re p o r t e dTPO antibody levels in 12% of subjects[ 11 ]. Thefrequency of ATMAand TPO antibodies among thegeneral population in Oman is not known. In the40 normal control subjects included in our studythis was found to be less than 5% for eitherantibody. The estimate for those antibodies amongthe general population in another study was ashigh as 15%[12]. Titers in normal population havebeen found to rise with age[13]. This may partially
explain the diff e rence in those levels. Omanisubjects included in this study were mainlyyounger individuals.
Many investigators had suggested that, for theroutine detection of thyroid autoantibodies, it isjustifiable to determine TPO antibodies only[16,17]. Inagreement with our findings, ATMA titers werefound to be closely correlated with thec o r responding average anti-TPO antibodyl e v e l s[ 7 , 1 4 , 1 5 ]. Knowing that AT M A tests usedunpurified microsomes as an antigen preparation,the anti-TPO tests use purified peroxidase. Ourresults may provide further support for the conceptthat AT M A accounts for virtually all of theantigenic determinants reacting with the TPOautoantibody.
Results from this study showed that there wasno significant difference in positive sera, for bothATMA and TPO antibodies, between treated anduntreated groups of GD patients. This agreed withearlier findings[18] but disagreed with some whofound either a significant decre a s e[ 1 4 ] or anincrease[19] in serum levels of those autoantibodiesafter treating patients with I131. These variationsmay be due to the differences in the immunologicalresponse caused by a decline in disease activity, ormay be a direct effect of the drug. It is possible thatthose factors have different impacts on the Omanisubjects when compared to subjects included inother studies.
Traditionally, in thyroid autoimmune diseases,ATMAare usually measured in parallel with A-TG-A. Unlike the case with ATMAand TPO antibodies,our study had demonstrated that the A - T G - Afrequency in GD was less frequently positive, asimilar observation having been reported before[20].It has been suggested that A-TG-A tests add verylittle to the diagnostic information already obtainedwith an appropriately sensitive anti-TPO antibodya s s a y, yet the presence of A - T G - A may haveprognostic significance in thyroid-ablated thyroidcancer patients[21].
Higher titers for both AT M A and anti-TPOantibodies were also observed among the SLEpatients group, which we employed as a non-thyroid autoantibody control. This agrees with anearlier study on patients with SLE[22,23]. While thereis no clear-cut mechanism to explain theseassociations, complex genetic factors are thought toplay role and a common genetic link is possible.
In conclusion, Omani patients with Graves’disease express high frequency of anti-TPOantibody which is correlated positively withATMA. Both assay anti-TPO antibody (determinedby ELISA) and ATMA (determined by hemagg-lutination) appear to have the same specificity.H o w e v e r, since the ELISA is easy to perform,

KUWAIT MEDICAL JOURNAL 13March 2006
employs a purified antigen and can easily beautomated, these characteristics should allow itsrapid application to the clinical routine, replacingthe ATMA assay. Furthermore, this study showedthat using TPO assay alone is diagnostic forautoimmune thyroid disease. This would have abearing in decreasing the cost of investigations.
REFERENCES
1. Mariotti S, Russova A, Pisani S, Pinchera AA. New solidPhase immunoradiometric assay for antithyroid micro -somal antibody. J Clin Endocrinol Metab 1983; 56:467-73.
2. Czarnocka B, Ruf J, Ferrand M, Carayon P, Lissitzky S.Purification of the human thyroid peroxidase and itsidentification as the microsomal antigen involved inautoimmune thyroid diseases. FEBS Lett 1985; 190:47-52.
3. Boyden SV. The adsorption of proteins on erythrocytestreated with tannic acid and subsequent hemagglutinationby antiprotein sera. J Exp Med 1951; 190:107-120.
4. Engler H, Staub J, Althaus B, Ryff-deLeche A, Gerber H.Assessment of antithyroglobulin and microsomal autoan-tibodies in patients with autoimmune thyroid disease:comparison of haemagglutination assay, enzyme-linkedimmunoassay and radioligand assay. Clin Chim Acta 1989;179:251-263.
5. Engler H, Riesen WF, Keller B. Anti-thyroid peroxidase(anti-TPO) antibodies in thyroid diseases, non-thyroidalillness and controls. Clinical validity of a new commercialmethod for detection of anti-TPO (thyroid microsomal)autoantibodies. Clin Chim Acta 1994; 225:123-136.
6. Bermann M, Magee M, Koenig RJ, Kaplan MM, Arscott P,Maastricht J, Johnson J, Baker JR. Differential autoantibodyresponses to thyroid peroxidase in patients with Graves’disease and Hashimoto’s thyroiditis. J Clin EndocrinolMetab 1993; 77:1098-1101.
7. Mariotti S, Caturegli P, Piccolo P, Barbesino G, Pinchera A.Antithyroid peroxidase autoantibodies in thyroid diseases.J Clin Endocrinol Metab 1990; 71:661-669.
8. Gauna A, Segura G, Sartorio G, Soto R, Segal-Eiras A.Immunological aspects of Graves’ disease patients indifferent clinical stages. J Endocrinol Invest 1989; 12:671-677.
9. Hasanat MA, Rumi MA, Alam MN, Hasan KN, SalimullahM, Salam MA, Faridulddin M, Mahtab H, Khan AK. Statusof antithyroid antibodies in Bangladesh. Postgrad Med J2000; 76:345-349.
10. Jannson R, Bernander S., Karlsonn A, Levin K, Nilson G.Autoimmune thyroid dysfunction in the post partumperiod. J Clin Endocr 1984; 58:681-687.
11. Hollowell JG, Staehlig NW, Hannon WH, Flanders WD,Gunter EW, Spencer SA. Serum thyrotropin, thyroxine and
thyroid antibodies in the United Sate population (1988 to1994): NHANES III. J Clin Endocrinol Metab 2002; 87:489-499.
12. Takamatsu J, Hosoya T, Kohno Y, Naito N, Sakeda K, KumaK, Ohsawa N. Changes in serum autoantibodies to thyroidperoxidase during antithyroid drug therapy for Graves’disease. Endocrinol Jpn 1990; 37:275-283.
13. Mariotti S, Sansoni P, Barbesino G, Caturegli P, Monti D,Cossarizza A, Giacomelli T, Passeri G, Fagiolo U, PincheraA. Thyroid and other organ-specific autoantibodies inhealthy centenarians. Lancet 1992; 339:1506-1508.
14. Mariotti S, Anelli S, Ruf J, Bechi R, Czarnocka B, LombardiA, Carayon P, Pinchera A. Comparison of serum thyroidm i c rosomal and thyroid peroxidase autoantibodies inthyroid diseases. J Clin Endocrinol Metab 1987; 65: 987-993.
15. Paschke R, Vogg M, Swillens S, Usadel KH. Correlation ofm i c rosomal antibodies with the intensity of theintrathyroidal autoimmune process in Graves’ disease. JClin Endocrinol Metabol 1993; 77:939-943.
16. Goodburn R, Williams DL, Marks V. The preparation ofthyroid microsomal antigen for use in the indirect micro-ELISAmethod for the detection of antithyroid microsomalautoantibodies. Clin Chim Acta 1982; 119:291-297.
17. Mc Kenzie JM, Zakarija M. Antibodies in autoimmunethyroid disease. In: Braverman LE, Utiger R, eds. Wernerand Ingbars The Thyroid. Philadelphia: Lippincott-RavenPublishers; 1996, p 416-432.
18. Maugendre D, Gatel A, Campion L, Massart C, Guihem I,Lorcy Y, Lescouarch J, Herry JY, Allannic H. Antithyroidd rugs and Graves’ disease-prospective randomizedassessment of long-term treatment. Clin Endocrinol (Oxf)1999; 50:127-132.
19. Feldt-Rasmussen U, Bech K, Date J, Petersen PH, Johansenk, Madsen SN. Thyroid stimulating antibodies, thyroglobinantibodies and serum proteins during antithyr o i dtreatment with radioiodine or propylthiouracil of Graves’disease. Allergy 1982; 32:161-172.
20. Beever K, Bradbury J, Phillips D, McLachlan SM, Pegg C,Goral A, Overbeck W, Feifel G, Smith BR. Highly sensitiveassays of autoantibodies to thyroglobulin and to thyroidperoxidase. Clin Chem 1989; 35:1949-1954.
21. Spencer CA, Takeuchi M, Kazarosyan M. Current statusand performance goals for serum thyroglobulin assays.Clin Chem 1996; 42:164-173.
22. Silman Aj, Olliver WER, Bubel MA. Autoimmune thyroiddisease and thyroid autoantibodies in rheumatoid arthritispatients and their families. British J Rheumatol 1989; 28:18-21.
23. Tsai RT, Chang TC, Wang CR, Lee SL, Wang CJ, Tsay GJ.Thyroid peroxidase autoantibodies and their effects onenzyme activity in patients with systemic lupuserythematosus. Lupus 1995; 4:280-285.

KUWAIT MEDICAL JOURNAL March 2006
ABSTRACT
O b j e c t i v e s : To investigate the prevalence ofosteoporosis and examine certain determinants ofbone mineral density among healthy community-dwelling Kuwaiti males aged 50 years or older.Setting: Endocrinology and Metabolism Unit andDepartment of Nuclear Medicine, Amiri Hospital,Kuwait.Design: One hundred and seventy two volunteerKuwaiti men aged ≥ 50 years with no risk factorsfor osteoporosis responded to a questionnaire thatincluded demographic data, complete medical anddrug history and information about lifestyle andphysical activity. Each subject underwent anth-ropometric measurements (height, weight) andtheir body mass index (BMI) was calculated. Bonemineral density (BMD) was measured at the lumbarspine, femoral neck and total hip by dual-energy X-raya b s o r p t i o m e t r y. Univariate and age and weight adjusted linearre g ression analysis were used to evaluate the associationbetween the independent variables and BMD.
R e s u l t s : O s t e o p o rosis was detected in 1.2%(lumbar spine), 1.2% (femoral neck) and 0.6% (totalhip) cases. Osteopenia was detected in 14.5%, 33.1%and 9.3% patients in the spine, femoral neck andtotal hip respectively. The determinants of BMD inour study were identified as age, weight and BMI.Common medical conditions (hypertension, type 2Diabetes Mellitus) and lifestyle factors such ascaffeine consumption, current physical exercise andsmoking habits were not shown to have anyrelation to BMD.Conclusion: We conclude that the prevalence ofo s t e o p o rosis among selected group of healthyKuwaiti men aged ≥ 50 year is low, where a sosteopenia is common in the femoral neck region.However, further studies to establish the normativedata of BMD in Kuwaiti male population areneeded. Age, low weight and low BMI wereindependent risk factors for low BMD in men afterthe age of 50 years.
KEYWORDS: bone mineral density (BMD), Kuwaiti male population, osteoporosis, risk factors
Original Article
Prevalence of Osteoporosis and Determinants of BoneMineral Density in Healthy Community-dwelling Kuwaiti
Men Aged 50 Years or Older
Address correspondence to: Dr. Nadia Al-Ali, P.O.Box 3005, Safat 13031, Kuwait. Tel: +965 252 7830, Fax: +965 251 8468, E-mail: [email protected]
Kuwait Medical Journal 2006, 38 (1): 14-20
Nadia S Al-Ali1, Jameela M Al-Faraj2, Suad A Mahseen3, Fotooh A Al-Jarki4, Jameela A Al-Khaldy5,Prem N Sharma6
1Unit of Endocrinology and Metabolism, Amiri Hospital, Kuwait2Nuzha Primary Care Centre, Kuwait
3Nuclear Medicine Department, Amiri Hospital, Kuwait4Khaldiya Primary Care Centre, Kuwait
5Thunayan Al-Ghanim Center, Kuwait6Faculty of Medicine/HSCC, Kuwait
INTRODUCTION Although osteoporosis in women has been
extensively investigated, osteoporosis in men hasreceived much less attention until recently. Recentyears have witnessed increased recognition of age-related bone loss in men as a significant healthproblem[1, 2]
The prevalence of male osteoporo s i s ,particularly in the most prone age group of men (50years and older) has been ascertained in manycommunities (Table 1). Most of these studies wereconducted in the western population of Europe and
America as well as Australia [3]
Risk factors for osteoporosis in men such as age,race, low body mass index (BMI), low dietarycalcium intake, high caffeine consumption,smoking habits, alcohol intake, physical activityand hypertension have already been described bymany studies[10-17].
Studies have shown extensive diff e rence innormative BMD values among geographical andethnic groups. Caucasians have higher BMD thanAsians but lower BMD when compared to blacksubjects[18].

KUWAIT MEDICAL JOURNAL 15March 2006
There are few studies on BMD of the MiddleEastern population. These studies, which wereconducted on healthy Lebanese [ 1 9 ] and Saudi [ 2 0 ]
women have shown lower BMD values ascompared to US / North European population.H o w e v e r, a study from Kuwait revealed nosignificant difference between the Kuwaiti womenand the Caucasian normative BMD data [ 2 1 ].Another study from Jordan[22] has addressed the riskfactors for osteoporosis in Jordanian women butthere has been hardly any study from the MiddleEast region to determine the factors affecting bonehealth in senior men except for the two studiesfrom Turkey by Cetin et al [23] and Marisah et al[24].
This has stimulated us to investigate theproblem of osteoporosis among older Kuwaiti malepopulation and investigate a host of physical,medical and lifestyle factors that might have aneffect on the bone mineral density.
SUBJECTS AND METHODStudy population:
The total population of Kuwait in 2002 was
about 1.4 million with 430,000 Kuwaiti men ofwhom about 35,000 were ≥ 50 years of age. Kuwaitimen aged ≥ 50 years constituted 8.3 % of the totalpopulation[25].
The study was conducted over a period of sixmonths (from July 2003 until January 2004) by theUnit of Endocrinology and Metabolism and theDepartment of Nuclear Medicine, Amiri Hospital,Kuwait.
An informed consent was obtained from 200volunteer ambulatory healthy Kuwaiti men aged ≥ 50years who were recruited by referrals from differentprimary care centers all over Kuwait. Twenty-eightcases with medical conditions or those on treatmentknown to affect BMD were excluded from the study(eight on thyroxin, five on inhaled steroids, three onoral steroids, two on anti-convulsants, two oncalcium and vitamin D, three with rheumatoidarthritis, two with liver disease, two withgastrectomy and one with primary hyperparathy-roidism). One hundred and seventy two subjectsqualified to be included in the study.
Table1 : The prevalence of osteoporosis, osteopenia and normal BMD among different male populations.
Country No of Age range Site Osteoporosis Osteopenia Normalsubjects (years) % % %
Brazil (3) 325 ≥ 50 Femoral neck 15.4 44.6 40.0
Britain (4) 2253 ≥ 50 Femoral neck 1.2 30.1 68.7
USA (5) 3090 ≥ 50 Femoral neck 4.0 33.0 63.0
Total femur 2.0 16.0 82.0
Canada (6) 1871 ≥ 50 Lumbar spine 2.9 - -
Femoral neck 4.8 26.7 68.5
Austria (7) 435 21-76 Lumbar spine 4.5 30.1 65.4
Femoral neck 5.9 41.0 53.1
Total hip 1.0 19.0 80.0
China (8) 789 ≥ 40 Any other site 11.5 20.0 68.5
Australia (Sydney) (9) 113 ≥ 70 Femoral neck 31.0 - -
Lumbar spine 11.5 - -
Fig 1 : Distribution of 172 men aged 50 years and older according to agegroup.
Fig 2 : Distribution of 172 subjects according to BMD at different sites
Age groups

Prevalence of Osteoporosis and Determinants of Bone Mineral Density in Healthy ..... March 200616
Study design:Each subject was instructed to respond to a
q u e s t i o n n a i re designed to solicit informationincluding demographic data, complete medical andd rug history and lifestyle habits including smoking,daily caffeine consumption (tea, coffee andbeverages) and current level of physical exercise.
Smoking was defined as using cigarettes, pipes,cigars or chewing tobacco on daily basis for at leastsix months. Volunteers were classified as non-,former or current smokers. Caffeine consumptionwas categorized as either low (< 2 cups/day) orhigh (≥ 2 cups/day). Current physical exercise wasrecorded as the number of hours spent weekly inphysical weight bearing exercise such as jogging,weightlifting or carrying heavy loads. Subjectswere categorized as low (< 2 hours / week), or high(≥ 2 hours / week).
Anthropometry:Weight was measured with a balance beam scale
and height with a calibrated stadiometer. Bodymass index (BMI) was calculated as the ratiobetween weight (Kg) and the square of height inmeters (m2).
Bone mineral density (BMD):Bone mineral density (BMD) was measured in
the anteroposterior lumbar spine L2-L4, femoralneck and total hip using a Lunar dual-energy X-rayabsorptiometer (DPX-L, Madison, MI). Softwarereference data were obtained from more than 12,000
subjects (NHANES III- national health andnutrition examination survey III USA). Thep recision for the BMD measurement wasdetermined by double measurement in 20volunteers, all men over 50 years old, and was 1.5%spine, 1.2% femoral neck and 1.6% total hip.
The stability of the DPX-L equipment waschecked daily with a phantom.
Statistical analysis:SPSS (PC version 11.0) was used. Univariate
linear regression analysis was used to test thepotential association between each pre d i c t o rvariable and BMD. These associations were thenadjusted for both age and weight.
RESULTSThe physical, medical and lifestyle
characteristics as well as the BMD results of the 172subjects studied are shown in Table 2. The agedistribution is illustrated in Fig 1. The distributionof the subjects according to BMD at different sitesshowed extremely low prevalence of osteoporosisat all sites (1.2%, 1.2% and 0.6%) and variableprevalence of osteopenia (14.5%, 33.1%, 9.3% atlumbar spine, femoral neck and total hiprespectively - Fig. 2).
Determinants of BMD:Univariate linear regression analysis between
different physical, medical and lifestyle factors andBMD at lumbar spine, femoral neck and total hipsites are shown in Table 3. These results were thenre-analyzed after adjusting for age and weight(Table 4).
Age: Age was negatively correlated with BMD at allsites, more significantly in the hip region bothfemoral neck and total hip (p < 0.001). For everyfive year increase in age, BMD tended to decline by-1.73, -3.6 and -3.2 % at lumbar spine, femoral neckand total hip respectively.
Height: Height: was significantly associated withhigher BMD at all sites, more so on the femoralneck. This positive correlation was lost afteradjusting for age and weight.
Weight: A very significant positive corre l a t i o nbetween weight and BMD was detected at all sites.A 10 kg increase in weight would increase BMD by3.767% (spine), 3.613% (femoral neck) and 3.347%(total hip).
Body mass index (BMI) :Univariate analysis revealed a very significant
Table 2: Subjects’ characteristics and BMD results
Characteristics Prevalence / Rangemean (SD )
Number of patients 172Physical factorsAge (years ) 65 .58 (7.71) 50 – 83 Height (cm) 168 (6.53) 150 – 185Weight (kg ) 78 .90 (12.79) 49.0 – 117.0BMI (body mass index)(kg/m2) 28 .06 (4.26) 18.36 – 41.40
Medical conditionsHypertension 55 (32 %)Diabetes mellitus (type 2 ) 60 (34.9 %)
Life style factorsSmoking
Current smoker 16 (9 .3 %)Ex-smoker 52 (30.2%)Non-smoker 104 (60.5%)
Caffeine consumption low < 2 cups/day 40 (23.3 %)high ≥ 2 cups/day 132 (76.7 %)
Current physical exercise habitslow < 2 hours/week 96 (62.2 %)high ≥ 2 hours/week 76 (37.8 %)
Bone mineral density (gm/cm 2)Lumbar spine 1 .17 (0.17) 0.74 – 1.61Femoral neck 0 .94 (0.11) 0.65 – 1.25Total hip 1 .04 (0.12) 0.70 – 1.39

KUWAIT MEDICAL JOURNAL 17March 2006
positive correlation between BMI and BMD at thehip region (femoral neck and total hip) (p < 0.001).The association was less significant at the spine (p =0.012 ).
Hypertension:No significant correlation was found between
hypertension and BMD at all sites. There was aweak positive correlation at the spine (p = 0.047),but this was lost when age and weight adjustedanalysis was performed.
Type 2 Diabetes Mellitus (DM):34.9% of the study population was diabetics. No
association was observed between type 2 diabetesand BMD at all sites.
Smoking, caffeine and current physical exercise:Statistical analysis revealed that none of these
factors have any significant relation to BMD.
DISCUSSION This study revealed a low prevalence of
o s t e o p o rosis but high prevalence of osteopeniaespecially at the femoral neck amongst healthycommunity-dwelling Kuwaiti men aged 50 years orolder.
The low prevalence of osteoporosis observed inour study population might have been due to smallsample size, applying rather strict exclusion criteria(which had excluded any secondary cause ofosteoporosis) and / or due to selection bias as mostof the volunteer subjects tend to be more healthconscious and may have healthier and more activelifestyle.
Considering that t-score was calculated from thedata base of NHANES III study, one could concludethat Kuwaiti male population might have higherBMD compared to American male population.
However a previous study from Kuwaitrevealed no significant diff e rence between theKuwaiti women and the Caucasian normativeBMD data[21]. There are no data yet on normal BMDamong Kuwaiti men.
Determinants of BMD:Age: Our results confirmed the observation madeby previous studies that aging was associated withlower BMD at all sites(14,17,23,26,27). Many other studieshave found that only femoral BMD is inverselyaffected by age[7,10,28,29]
Height: The results of studies on the relation ofheight and BMD in men are inconsistent. WhereasKroger et al[30] and Nguyen et al[15] showed a positiverelation between height and BMD, Huuskonen etal[14] and Orwell et al[11] could not demonstrate anyrelation. In our study although a significantpositive correlation was detected initially,adjustment for age and weight made heightrelation to BMD insignificant.
Body weight: Several studies have shown a strongpositive correlation between body weight and BMDin both genders at all age groups[30,31]. Orwell et al[11]
found that weight in men was the best predictor ofBMD at the spine and the femoral neck. This is inagreement with the studies by Smerdlely et al[9] andNguyen et al[32] who reported higher BMD inrelation to obesity in men. Our results confirmedwhat other studies had reported.
Table 3 : Univariate linear regression analysis of different variables in relation to BMD at spine, femoral neck and total hip sites.
Lumbar spine Femoral neck Total hip
Variable Mean(SD) / p- p- p-Prevalence Unit Change value value value
Age (years) 62.58 (7.72) 5 -1.730 0.04* -2.49 <.001*** -2.05 0.001***Height (cm) 168 (6.53) 5 2.745 0.006** 2.467 <.001*** 1.568 0.028*Weight (kg) 78.9 (12.7) 10 3.767 <.001*** 3.613 <.001*** 3.347 <.001***BMI (kg/cm2) 28.06 (4.26) 1 0.759 0.012* 0.765 <.001*** 0.792 <.001***Hypertension 32 % n/y 5.513 0.047* 2.995 0.122 3.739 0.059DM 34.90% n/y 3.437 0.207 0.232 0.903 -0.016 0.993Caffeine 19.20% low/high -0.814 0.805 -1.15 0.617 -1.170 0.619Exercise 29.70% low/high -0.497 0.832 0.798 0.693 -0.134 0.932Non-smoker 60.50% n/y 2.18 0.412 0.415 0.823 0.471 0.804Current smoker 9 .30% n/y -6.86 0.124 0.541 0.862 -1.25 0.696Ex-smoker 30.20% n/y 0.274 0.923 -0.687 0.728 -0.033 0.987
Caffeine: low (< 2 cups/day), high (≥ 2 cups/day)Exercise: low (< 2 hrs/week), high (≥ 2 hrs/week)
*p<0.05 , **p<0.01, ***p<0.001.
% change inBMD/unit changein variable
% change inBMD/unitchange invariable
% change inBMD/unit change invariable

Prevalence of Osteoporosis and Determinants of Bone Mineral Density in Healthy ..... March 200618
Body mass index (BMI):BMI was shown by many studies to have
positive correlation with BMD[ 2 8 , 2 9 , 3 3 ].Unlike thereport from Cetin et al[23]who found that BMI is amajor predictor of lumbar spine BMD, our resultssuggest that the femoral site is more stro n g l yrelated to BMI.
Hypertension:There is a dearth of literature on the relation
between hypertension and BMD in males.Cappuccio et al[34] reported that hypertension wasassociated with increased bone mineral loss inelderly white healthy community-dwellingKuwaiti men aged 50 years or older postmeno-pausal women. Tsuda K[35] confirmed the previousobservation and reported a significant decrease inBMD of female hypertensive patients which wasinversely correlated with systolic blood pressure.He also found that the 24-hour urinary calcium wassignificantly greater in hypertensive females. Thefew studies in men that had looked into this issueare contradictory. Whereas Orwell et al[11] in hisstudy on males ≥ 60 years reported thathypertension was associated with lower BMD,Hanley et al[ 3 6 ] found that hypertension wasassociated with higher BMD in males ≥ 50 years.Our results did not demonstrate any re l a t i o nbetween hypertension and BMD.
Type 2 Diabetes Mellitus (DM):Previous studies[36-39] agreed that females with
type 2 DM have significantly higher BMD at allsites.
There is inconsistent data in males as to whichsite is mostly affected. Hanley et al [36] found higherBMD in older diabetic males to be mostpronounced at the femoral neck, whereas Lunt[40]
reported significantly higher BMD at the spine intype 2 diabetic males ≥ 50 years. The present study
could not confirm the positive relation betweentype 2 DM and BMD.
Smoking:Smoking has been shown to have a negative
relation to BMD in both genders[ 1 6 , 4 1 ]. SeveralStudies in men have demonstrated that any lifetime smoking exposure tend to reduce BMD[11,14,17,20,40,41].
Eegger et al[43] found that the adverse effect ofsmoking on BMD is more profound in men thanwomen and more pronounced at the level oflumbar spine with a BMD that is 7.3% lower thannon smokers. Yet, Orwell et al [11] and Hollenbach etal(44) showed that hip is the site generally moreinversely affected by smoking. Orwell et al[ 11 ]
reported 8% lower BMD in the femoral region ofmale smokers compared to non-smokers. Studiesby Szuluc et al[17] and Vogel et al[42] revealed thatthere is an increased bone resorption in currentsmokers but not in former smokers. In the presentstudy, no significant association between smokingand BMD was observed. Our results are inconcordance with the reports of Bendavid et al[13],Huuskonen et al[14], and Kroger et al[30]. Yet, it isworth noting that only 9.3% of our population werecurrent smokers. This small number might haveaffected the statistical significance of the results.
Caffeine consumption:Our study revealed no correlation between
Caffeine consumption and BMD, confirming whatprevious studies had shown[2,3,10]. However, Orwellet al[11] had reported. A slight negative correlationbetween the caffeine intake and femoral BMD.
Current physical activity:There are few studies that have looked into the
actual effect of exercise on BMD. Tanaka et al[3],Glynn et al[10] and Snow-Harter et al[47] all reported
Table 4 : Linear regression analysis after adjusting for age and weight
Adjusted for age & weight Lumbar spine Femoral neck Total hip
Height (cm) 168 (6.53) 5 1.12 0.312 0.52 0.469 -0.41 0.588
hypertension 32% n/y 4.53 0.100 2.411 0.176 3.105 0.100
DM 34.9% n/y 3.415 0.200 0.598 0.729 0.158 0.931
Caffeine 19.2% low/high- 0.746 0.817 -1.65 0.427 -1.47 0.504
Exercise 29.7% low/high 0.179 0.952 1.545 0.472 0.507 0.876
Non-smoker 60.5% n/y 3.351 0.201 0.933 0.583 1.111 0.537
Current smoker 9.3% n/y -6.58 0.125 1.106 0.691 -0.816 0.782
Ex-smoker 30.2% n/y -1.01 0.717 -1.52 0.400 -0.909 0.635
Variable Mean(SD) /Prevalence
Unit Change % change inBMD/unitchange invariable
p-
value
% change inBMD/unitchange invariable
% change inBMD/unitchange invariable
p-
value
p-
value

KUWAIT MEDICAL JOURNAL 19March 2006
higher BMD with the history of previous or currentphysical exercise. In our study we could not proveany beneficial effect of current physical exercise onBMD.
CONCLUSIONThis is the first study from Kuwait on BMD
among healthy community-dwelling Kuwaitimales aged 50 years or older. Applying rather strictexclusion criteria and recruiting volunteer healthysubjects might have resulted in underestimation oflow BMD prevalence. However, about one third ofthis healthy volunteer population have osteopeniaof the femoral neck region which will progress too s t e o p o rosis if preventive measures are notundertaken.
It is quite important to establish an unbiased,community-based normative BMD data among theKuwaiti male population in order to ascertain theaccurate prevalence of low BMD and toacknowledge the problem size to consider adoptingprevention campaigns.
The determinants of BMD in our study wereidentified as age, weight and BMI. Other factorssuch as height, hypertension, type 2 DM caffeineconsumption, current physical exercise andsmoking were not found to correlate with lowBMD in men. This might be a true finding or anerror created by a small population size.
The need for larger studies remains a necessitybefore solid conclusions could be made in order tomodify risk factors and improve the olderpopulation bone health.
REFERENCES
1. Clarke BL, Ebeling PR, Jones JD, Wahner HW, O’FallonWM, Riggs BL, Fitzpatrick LA. J Clin EndocrinolMetabolism 1996; 81:2264-2270.
2. Slemenda CW, Longcope C, Zhou L, Hui SL, Peacock M,Johnston CC. Sex steroid and bone mass in older men. J ClinInvest 1997; 100:1755-1759.
3. Tanaka T, Latorre MRDO, Jaime PC, Florindo AA, PippaMGB, Zerbini CAF. Risk factors for proximal femurosteoporosis in men aged 50 years or older. OsteoporosisInternational 2001; 12:942-949.
4. Holt G, Khaw KT, Reid DM, Compston JE. Prevalence ofosteoporotic bone mineral density at the hip in Britaind i ffers substantially from US over 50 years of age:implications for clinical densitometry. Br J Radiol 2002;75:736-742.
5. Looker AC, Orwell ES, Johnston Jr CC, Lindsay RL, WahnerHW, Dunn WL. Prevalence of low femoral bone density inolder US adults from NHANES III. J Bone Miner Res 1997;12: 1761-1768.
6. Tenenhouse A, Joseph L, Kreiger N, Poliquin S, Murray TM.caMos Research Group. Osteopor Int 2000; 11:897-904.
7. Kudlacek S, Schneider B, Peterlik M, Leb G, Klaushofer K,Weber K. Normative data of bone mineral density in anunselected adult Austrian population. Europ J Clin Invest2003; 33:332-339.
8. Li N, Ou P, Zhu H, Yang D, Zheng P. Prevalence rate ofosteoporosis in the mid-age and elderly in selected parts ofChina. Chin Med J 2002; 115:773-775.
9. S m e rdley P, Seller M, Smith A, Day P, Diamond T.P redictors of bone mass in healthy older men in thecommunity. Med J Aust 2000; 173:183-186.
10. Glynn NW, Meilahn EN, Charron M. Determinants of bonemineral density in older men. J Bone Miner Res 1995;10:1769-1777.
11. Orwell ES, Bevan L,Philipps KR. Determinants of bonemineral density in older men. Osteoporos Int 2000; 11:815-821.
12. Slemenda CW, Christian JC, Reed T. Long term bone loss inmen: effects of genetic and enviromental factors. Ann InterMed 1992; 117:286-291.
13. Bendavid ER, Shan J, Barrett-Connor E. Factors associatedwith bone mineral density in middle - aged men. J BoneMiner Res 1996; 11:1185-1190.
14. Huuskonen J,Väisänen SB, Kröger H, Jurvelin C, BouchardC, Alhava E, Rauramaa R. Determinants of bone mineraldensity in middle aged men: a population - based study.Osteoporos Int 2000; 11: 702-708.
15. Nguyen TV, Kelly PJ, Sambrook PN, Gilbert C, Pocock NA,Eisman JA. Lifestyle factors and bone density in theelderly:implication for osteoporosis prevention. J BoneMiner Res 1994; 9:1339-1346.
16. Burger H, de Laet CE, van Daele PL, Weel AE, WittermanJC, Hofman A. Risk factors for increasing bone loss inelderly population:the rotterdam study. Am J Epidemiol1998; 147:871-879.
17. Szluc P, Garnero P, Claustrat B, Marchand F, Duboeuf F,Delmas PD. Increased bone resorption in moderate smokerswith low body weight : the Minos study. J EndocrinolMetabol 2002; 87:666-674.
18. Tobias JH, Cook DG, Chambers TJ, Dalzell N. A comparisonof bone mineral density between Caucasian, Asian andAfro-Caribbean women. Clin Sci 1994; 87:587-591.
19. Maalouf G, Salem S, Sandid M, Attallah P, Eid J, Saliba N,Nehmet I, Johnell O. Bone mineral density of the Lebanesereference population. Osteoporos Int 2000;11:756-764.
20. El-Desouki M. Bone mineral density of the spine and femurin the normal Saudi population. Saudi Med J 1995; 16:30-35.
21. Dougherty G, Al-Marzouk N. Bone density measured ByD u a l - E n e rgy X-Ray absorptiometry in healthy Kuwaitiwomen. Calcif Tissue Int 2001; 68:225-229.
22. Shalbayeh S. Prevalence of osteoporosis and itsreproductive risk factors among Jordanianwomen: a cross-sectional study. Osteoporos Int 2003; 14:929-940.
23. Cetin A, Gokce-KustalY, Celiker R. Predictors of bonemineral density in healthy males. Rheumatol Int 2001;21:85-88.
24. Marisah M, Ozakosoy D, Yilmaz E, Senocak O. Bonemineral density reference values in the normal female andmale population of Azmir, Turkey. Eur Radiol 2003; 13:157-162.
25. Public Authority for Civil Information. State of Kuwait.2002.
26. Meier DE, Orwell ES, Jones JM. Marked disparity betweentrabecular and cortical bone loss with age in healthy men.Ann Inter Med 1984; 101:605-612.
27. Jones G, Nguyen T, Sambrook P. Progressive loss of bone inthe femoral neck in elderly people: longitudinal findingsfrom the Dubbo osteoporosis epidemiology study. BMJ1994; 309:691-695.
28. Hannan MT, Felson DT, Anderson JJ. Bone mineral densityin elderly men and women: results from the FraminghamOsteoporosis Study. J Bone Miner Res 1992; 7:547-553.
29. Zerbini CAF, Latorre MRO, Jaime PC. Bone mineral density

Prevalence of Osteoporosis and Determinants of Bone Mineral Density in Healthy ..... March 200620
in Brazilian men 50 years and older. Braz J Med Bio Res2000; 33; 1429-1435.
30. Kröger H, Laitinen K. Bone mineral density measured bydual-energy x-ray absorptiometry in normal men. Eur JClin Invest 1992; 22: 454-460.
31. Felson DT, Zhang Y, Hannan MT, Anderson JJ. Effect ofweight and body mass index on bone mineral density inmen and women: the framingham study. J Bone Miner Res1993; 8:567-573.
32. Nguyen TV, Eisman JA, Kelly PJ, Sambrook PN. Riskfactors for osteoporotic fractures in elderly men. Am JEpidemiol 1996; 144:255-263.
33. Evans SF, Davie MW. Low body size and elevated sex-hormone binding globulin distinguish men with idiopathicvertebral fracture. Calcif Tissue Int 2002; 70:9-15.
34. CappucioFP, Meilahn E, Zmuda JM. High blood pressureand bone mineral loss in elderly white women: aprospective study. Lancet 1999; 345:971-975.
35. Tsuda K, Nishio I, Masuyama Y. Bone mineral density inwomen with essential hypertension. Amer J Hypertens2001; 14:704-707.
36. Hanley DA, Brown JP, Tenenhouse A. Association amongdisease conditions, bone mineral density, and prevalentvertebral deformities in men and women 50 years of ageand older: cross-sectional results from the CanadianMuticentre Osteoporosis Study. J Bone Miner Res 2003;18:784-790.
37. B a r rett-Connor E, Holbrook T. Sex diff e rences inosteoporosis in older adults with noninsulin dependent
diabetes mellitus. JAMA1992; 268:3333-3337.38. Van Dale P, Stolk R, Burger H, Algera D. Bone density in
noninsulin dependent diabetes mellitus. The Rotterdamstudy. Ann Inter Med 1995; 122:409-414.
39. Johnston Jr C, Hui S, Longcope C. Bone mass and sexs t e roids in postmenopausal caucasian diabetics.Metabolism 1985; 34:554-560.
40. Lunt M, Masaryk P, Scheidt-Nave C, Nijs J, Poor G, Pols H.The effects of lifestyle, dietary intake and diabetes on bonedensity and vertebral deformity: the EVOS study.Osteoporos Int 2001; 12:688-698.
41. Kiel DP, Zhang Y, Hannan MT, Andersson JJ, Baron JA,Felson DT. The effect of smoking at different life stages onbone mineral density in elderly men and women.Osteoporos Int 1996; 6:240-248.
42. Vogel JM, Davis JW, Nomura A. The effect of smoking onbone mass and the rates of bone loss among elderlyJapanese-American men. J Bone Miner Res 1997; 12:1495-1501.
43. Egger P, Duggleby S, Hobbs R, Fall C, Cooper C. Cigarettesmoking and bone mineral density in the elderly. JEpidemiol Community Health 1996; 50:47-50.
44. Hollenbach KA, Barrett-Connor E, Edelstein SL, HolbrookT. Cigarette smoking and bone mineral density in oldermen and women. Am J Public Health 1993; 83:1265-1270.
45. Snow-Harter C, Whalen R, Myburgh K, et al. Bone mineraldensity, muscle strength, and recreational exercise in men. JBone Miner Res.1992; 7:1291-1296.

KUWAIT MEDICAL JOURNALMarch 2006
ABSTRACT
Objectives: To determine the prevalence of mumpsvirus-specific antibodies and investigate the level ofprotective immunity against the mumps virus inKuwaiti children. Methods: The effectiveness of mumps vaccinationcampaign in Kuwait was studied by determiningthe prevalence of mumps virus-specific antibodiesby an enzyme-linked immunosorbent assay in 150s e rum samples, while the protective level ofimmunity against mumps virus genotypes A and Bwas investigated by virus neutralization test in 98serum samples.Results: The prevalence of mumps virus-specificantibodies after two doses of measles-mumps-rubella vaccine reached 92% by the age of 5-12years. The protective, neutralizing antibodies to
both genotypes could be detected in 94% of sera inchildren aged 11-16 years. In the younger age group(5-10 years), protective antibodies were found morefrequently (94%) to the homologous vaccine strain(genotype A) than to the heterologous genotype B(77%) mumps virus strain. Conclusion: The two dose measles-mumps-rubellavaccination schedule implemented in Kuwait since1994 resulted in a high prevalence rate of antibodiesindicating adequate vaccination coverage ofc h i l d ren. Determining the level of neutralizingantibodies to homologous and hetero l o g o u smumps virus strains revealed the possibility thatantigenically diff e rent mumps virus genotypesmay be present in Kuwait.
KEYWORDS: immunity, mumps vaccine, neutralizing antibodies
Original Article
Antibody Prevalence and Genotype-Specific ProtectiveImmunity against Mumps Virus Infection in Children from
Kuwait
Address correspondence to: Dr. Gyorgy Szucs, Visiting Associate Professor and Consultant Virologist, Department of Microbiology, Faculty of Medicine, Kuwait University,P.O. Box 24923, Zip Code 13110, Kuwait. Tel: +965-5312300/ext. 6529, Fax: +965-5332719, E-mail:[email protected]
Kuwait Medical Journal 2006, 38 (1): 21-24
Ola Moghnai, Alexander Pacsa, Gyorgy Szucs, Widad Al-NakibDepartment of Microbiology, Faculty of Medicine, Kuwait University, Kuwait
INTRODUCTIONMumps is one of the commonly acquired acute,
benign childhood viral infections. Complications ofmumps include aseptic meningitis and encephalitis,deafness, orchitis and oophoritis, pancreatitis andarthralgias[1]. Mumps virus (MuV) is classified as amember of the Paramyxoviridae family, genusRubulavirus[2], and has a non-segmented, negativesense, single-stranded ribonucleic acid genomecontaining approximately 15,000 nucleotides[ 3 ].With the advent of molecular techniques, MuVcould be divided into different genotypes based onthe sequence variability of its SH genomic re g i o n[ 4 - 6 ].At present, MuV strains are classified into tendifferent genotypes from A to J [7-9].
Mumps outbreaks still occur even in areas withhigh vaccine coverage [10-12] because the vaccine maynot be effective against heterologous viru sgenotypes. Neutralizing antibodies could bedetected against different mumps genotypes. It is
known that antibodies produced in animals anddirected against genotype A did not neutralizegenotypes C and D eff e c t i v e l y. Consequently,immunity produced by genotype A may not beeffective against infection caused by genotype C orD[11,13]. Mumps has worldwide endemicity. Due tothe administration of live attenuated vaccineduring the 25 years between 1968 and 1993, theincidence of mumps declined dramaticallyreaching a 99% drop in the cases registered in USA(from 152,209 to 1692 cases). There are differentways of giving mumps vaccine. There is amonovalent vaccine which contains only MuV, thebivalent one contains measles and mumps strains(MM) and the recent trivalent one, containingmeasles, mumps, rubella viruses together(MMR)[14]. The MMR vaccine is preferred to be partof the vaccination schedule of many countries andit was also first introduced in Kuwait in 1994.Kuwait has implemented an excellent compulsory

Antibody Prevalence and Genotype-Specific Protective Immunity against Mumps Virus ..... March 200622
MMR vaccination programme. Despite the rigorousvaccination campaign, a number of mumps casescontinue to be reported every year in the country[15].In order to find a possible answer as to why mumpscases continue to occur, we investigated theprevalence of MuV-specific antibodies and the levelof protective immunity of children in Kuwait totwo different MuV genotypes.
METHODSStudy population:
For determining the prevalence of mumpsv i rus-specific antibodies by enzyme-linkedimmunosorbent assay (ELISA), serum samples of150 children were selected from the clinicalspecimens sent to the Virology Unit, Faculty ofMedicine from the Department of Pediatrics,Mubarak Al-Kabeer Hospital. Samples included inthis study were obtained from children presentingwith minor ailments and negative for otherinfectious agents. In Kuwait, for the last five years,the MMR vaccination targeted young children agedbetween one and four years. Therefore, we formedthree age groups designated as Groups A to C ofc h i l d ren accordingly to the time of MMRvaccinations. Group A comprised of children (n =50) aged less than one year (0 to 11 months). Thiswas the pre-vaccination group. Group B wascomprised of children aged 1-3 years (n = 50) whohad received one dose of MMR vaccine at the age of12 months. Group C comprised of children aged 5-12 years (n = 50) who had received two doses ofMMR vaccine at the age of four years.
For determining the level of pro t e c t i v eimmunity to MuV, 47 and 51 serum samples of 5-10and 11-16 years old children, respectively, wereselected and tested by virus neutralization test.
ELISA test:To determine the prevalence of MuV-specific
antibodies, an ELISA test (Virion / Serion GmbH,
Wurzburg, Germany) was used. The assay wascarried out according to the manufacture r’ sinstructions. As controls, standard negative andpositive serum samples were included in eachassay run.
Virus neutralization test (NT): Using flat-bottomed tissue culture microplates
(Falcon), 200 µl of serum samples dilutedp reviously 1:5 in Dulbecco’s Modified EagleMinimal Essential Medium (MEM; Gibco-BRL)were added to three parallel wells in the first rowand, subsequently, serial 2-fold dilutions were donein 100 µl of MEM. One-hundred µl (100 TCID50) ofreference MuV strains, namely, 1) Enders VR-106,genotype A (American Type Culture Collection,ATCC, Rockville, Maryland, USA); 2) Jeryl-Lynn(JL) vaccine strain, genotype A (DRT-MMR, MSD,Rahway, New Jersey, USA); 3) Urabe vaccine strain,genotype B / propagated and titrated in Vero cells,were added to each well of the first, second andthird rows, respectively, in the plate. The last wellsremained without serum serving as viral and cellcontrols, respectively. The serum-virus mixtureswere incubated for 30 minutes at 37ºC. Finally, 104Vero cells in 100 µl of MEM with 10 % FCS (Gibco-BRL) were added to each well in the plate and wereincubated in a CO2 incubator. After four days ofincubation when the viral controls showedcomplete cell destruction, the neutralization titersof serum samples were evaluated. The neutralizingantibody titer of a serum sample was the lastdilution where the cytopathic effect of the virus wascompletely prevented by the antibodies present inthe serum.
RESULTSPrevalence of MuV-specific IgG antibodiesdetermined by ELISA:
Out of the three age groups of children living inKuwait, in the first group (0-11 months old), half of
Fig. 1: Neutralizing antibodies detected in 47 sera of 5-10 year oldchildren to two MuV genotypes A strains (Enders and Jeryl-Lynn) andone genotype B strain (Urabe)
Fig. 2: Neutralizing antibodies detected in 51 sera of 11-16 year oldchildren to two MuV genotypes A strains (Enders and Jeryl-Lynn) andone genotype B strain (Urabe)

KUWAIT MEDICAL JOURNAL 23March 2006
the infants without vaccination had antibodies toMuV. The prevalence of antibodies was 80% in thesecond group (1-3 years old). These childre nreceived one dose of MuV vaccine. After receivingan additional booster dose of MMR vaccine (thirdgroup of children aged 5-12 years), the antibodyprevalence rate increased to 92%.
Immunity of children to MuV genotype A and Bdetermined by neutralization test:
Vi rus neutralization test (NT) was used tomeasure the level of genotype specific protectiveimmunity against three different strains of MuV.Two strains (Enders and JL) belonged to genotypeA and one strain (Urabe) to genotype B. The first setof serum samples (n = 47) represented 5-10 year oldchildren who had received two doses of MMRvaccine while the second set of serum samples (n =51) represented 11-16 years old children who hadreceived the vaccine between 5-10 years ago. Asshown in Fig. 1, in the 5-10 years old group, therew e re only three samples without neutralizingantibodies to the homologous JL genotype Avaccine strain which is currently used in Kuwait.On the other hand, 12 and 19 samples did not haveneutralizing antibody against Enders (genotype A)and Urabe (genotype B) strains, respectively. Inother words, the prevalence of neutralizingantibody was 94% for the JL vaccine strain, while itwas only 77% and 60% for Enders and Urabe strain,respectively.A different picture was obtained in theolder age group (11-16 years). As shown in Fig. 2,both the prevalence rate and the level ofneutralizing antibody were very similar for thehomologous and heterologous MuV strains.Therefore, results show that in the older age groupthe level of immunity does not differ significantlyin relation to MuV genotypes.
DISCUSSIONAlthough there is a worldwide mumps
vaccination program, epidemics and outbreaks ofmumps still occur. Despite the fact that here inKuwait an excellent and comprehensive vaccinationp rogram had been introduced against mumps,measles and rubella in 1994, still a number ofmumps cases have been reported[15]. Though thevaccination has resulted in a considerable drop(88%) in the number of cases, still, between 1997and 2001, there were 555 reported mumps cases inKuwait[15]. Therefore, it was important to determinethe prevalence rate of MuV-specific antibodies inc h i l d ren which should provide re l e v a n tinformation about the possibility of primaryvaccine failure, and the number of children whomay be at risk of acquiring mumps infection. Inorder to obtain data about the impact of vaccination
on MuV infection in children in Kuwait, wedetermined the prevalence of MuV-IgG antibodiesin three age groups. Results showed a sharpincrease in the number of children with antibody byage. This was mainly due to the vaccination. In thenon-vaccinated age group (0-11 months), 50% ofc h i l d ren had MuV-IgG antibodies probably ofmaternal origin. The first dose of the vaccine hasresulted in an increase in the prevalence of IgG-type antibodies to MuV from 50% to 80% in the 1-3years old children, and the rate reached 92% in the5-11 years old ones who received two doses of thevaccine. It is, therefore, presumed that the highlevel of antibody prevalence breaks the transmissioncycle of the wild mumps virus in such a wellvaccinated population. There f o re, the questionarises, as to why some cases of mumps continue tobe reported each year in Kuwait where thevaccination coverage of the population is extensive.To answer this question, factors like the MuVgenotypes present in the country, and thespecificity of the vaccine-induced immunity shouldbe taken into consideration. Though the prevalencerate of MuV-specific IgG antibodies determined bythe ELISA indicates the effectiveness of thevaccination, it does not provide a true picture of thelevel of immunity to MuV. Determination of thespecificity and the level of immunity to MuVinfection require the measurement of neutralizingantibodies.
The serum level of neutralizing antibodies isconsidered to be a reliable indicator of immunityand it has a restricted strains specificity[ 1 6 , 1 7 ].T h e re f o re, the immuogenecity and the implicitefficacy of live, attenuated mumps vaccine haveoften been evaluated by the ability of the vaccine toinduce the production of neutralizing antibodies[18].In order to obtain an accurate picture of the level ofgenotype-specific immunity, titers of neutralizingantibodies have been determined in sera of 98individuals (aged between 5-16 years). In the 5-10years old group (n= 47), 94% of children (whoreceived two doses of MuV vaccine) had thehomologous antibodies similar to those detected byELISA. However, in this group, the antibodiesagainst the heterologous genotype B Urabe straincould be found only in 77% of samples. Therefore,the immunity developed to the homologousvaccine strain may not have been fully protectiveagainst the heterologous MuV strain. In a situationwhere different genotypes of viruses are circulatingin a given area, mumps cases can be caused bythese antigenically heterologous strains. Indeed, itis known that mumps outbreaks occur even in wellvaccinated populations[10-12]. There are data fromSwitzerland and Portugal where MuV strainscaused epidemics in the population vaccinated w i t h

Antibody Prevalence and Genotype-Specific Protective Immunity against Mumps Virus ..... March 200624
d i ff e rent genotype[ 1 9 , 2 0 ]. Immunological diff e re n c e sbetween genotypes A and B has also been clearlydemonstrated[21,22]. In fact, neutralizing antibodiesformed after infection with genotype D, did notp rotect against infection with genotype A[ 2 3 ].Furthermore, data showed that vaccination withgenotype A does not provide protection againstother genotypes like C or D[19,20]. Therefore, it may bepossible that here too in Kuwait, despite the highvaccination coverage, diff e rent MuV genotypesmay be circulating from time to time. These maycontribute to the number of mumps cases recordedin Kuwait. This possibility is strengthened by ourdata obtained for older age group (11-16 years). Inthis group, the prevalence of protective neutralizingantibodies was at the same level for homologousand heterologous MuV strains. The possibleexplanation for this fact may be that wild virusstrains, other than genotype A a re present inKuwait infecting children who may not have hadthe adequate genotype-specific protective antibodiesat the age of 5-10 years.
We conclude that in any vaccination campaign,it is important to reach as high as 95% coverage ofthe target population. Low vaccination coverage(primary vaccine failure) may leave a number ofindividuals unprotected, hence giving the possibilityfor wild virus strains to circulate in the community.In addition to the coverage, vaccine-inducedantibodies should be able to neutralize the wildvirus strains circulating in a given area and thenumber of vaccine-associated adverse eff e c t sshould be kept at the minimum level. A comparisonbetween ELISA and NT showed that ELISA can beused to monitor the effectiveness of the vaccinationin general. However, to obtain more pertinent andprecise data on the vaccine induced immunity,virus neutralization test is the method of choice.
ACKNOWLEDGMENTThis study was funded by Kuwait University,
College of Graduate studies and Researc hAdministration, Grant MI 03 / 02.
REFERENCES
1. Leinikki P. Mumps. In: Principles and Practice of ClinicalVirology. Eds. Zuckerman AJ, Banatvala JE, Pattison JR,Griffith PD and Schoub BD. 5th ed. John Wiley & Sons Ltd,Chichester, UK; 2004, p 459-466.
2. Virus Taxonomy. 7th Report of the International Committeeon Taxonomy of Vi ruses. Eds. Van Regenmortel MH, FauguetCM, Bishop DH. Academic Press, San Diego; 2000, p 551.
3. Elango N, Varsanyi TM, Kövamees J, Norrby E. Molecularcloning and characterization of six genes, determination ofgene order and intergenic sequences and leader sequence ofmumps virus. J Gen Virol 1988; 69:2893- 2900.
4. Jin L, Beard S, Brown DWG. Genetic heterogeneity of
mumps virus in the United Kingdom: Identification of twonew genotypes. J Infect Dis 1999; 180:829-833.
5. Yeo R., Afzal MA, Forsey T, Rima BK. Identification of anew mumps virus lineage by nucleotide sequence analysisof the SH gene of ten different strains. Arch Virol 1993;128:371-377.
6. Örvell C, Tecle T, Johansson B, Saito H, Samuelson A.Antigenic relationships between six genotypes of the smallhydrophobic protein gene of mumps virus. J Gen Virol2002; 83:2489-2496.
7. Johansson B, Tecle T, Örvell C. Proposed criteria forclassification of new genotypes of mumps viru s .Scandinavian J Infec Dis 2002; 34:355-357.
8. Kim SH, Song KJ, Shin YK, Kim JH, Choi SM, Park KS, BeakLJ, Lee YJ, Song JW. Phylogenetic analysis of the smallh y d rophobic (SH) gene of mumps virus in Korea: Identificationof a new genotype. Microbiol Immunol 2000; 44:173-177.
9. Tecle T, Böttiger B, Örvell C, Johansson B. Characterizationof two decades of temporal co-circulation of four mumpsv i rus genotypes in Denmark: identification of a newgenotype. J Gen Virol 2001; 82:2675-2680.
10. Wharton M, Cochi SL, Hutcheson RH, Bistowish JM,Schaffner W.A large outbreak of mumps in the postvaccineera. J Infect Dis 1988; 158:1253-1260.
11. Hersh BS, Fine PEM, Kent WK, Cochi SL, Kahn LH, Zell ER,Hays PL, Wood CL. Mumps outbreak in a highlyvaccinated population. J Pediatr 1991; 119:187-193.
12. Briss PA, Fehrs LJ, Parker RA, Wright PF, Sannella EC,Hutcheson RH, Schaffner W. Sustained transmission ofmumps in a highly vaccinated population: assessment ofprimary vaccine failure and waning vaccine- inducedimmunity. J Infec Dis 1994; 169:77-82.
13. Tecle T, Johansson B, Jejcic, A, Forsgren, M, Örvell C.Characterization of three co-circulating genotypes of thesmall hydrophobic protein gene of mumps virus. MicrobiolImmunol 1998; 79:2929-2937.
14. Galazka AM, Robertson SE, Kraigher A. Mumps andmumps vaccine: a global re v i e w. Bulletin WHO 1999; 77:3-14.
15. Annual Reports, Volumes 1991 to 2001. Health and VitalStatistics Division. Department of Statistics and MedicalRecords. Ministry of Health, Kuwait.
16. Ennis FA. Immunity to mumps in an institutional epidemic:correlation of insusceptibility to mumps with serum plaqueneutralizing and haemagglutination-inhibiting antibodies. JInfect Dis 1969; 119:654-657.
17. Hilleman MR, Weibel RE, Buynak EB, Stokes J, Whitman JE.Live, attenuated mumps-virus vaccine. Protective efficacy asmeasured in a field evaluation. N E J Med 1967; 276:252-258.
18. Shehab ZM, Brunell PA, Cobb E. Epidemiologicalstandardization of a test for susceptibility to mumps. J InfecDis 1984; 149:810-812.
19. Ströhle A, Bernasconi A, Germann D. A new mumps viruslineage found in the 1995 mumps outbreak in WesternSwitzerland identified by nucleotide sequence analysis ofthe SH gene. Arch Virol 1996; 141:733-741.
20. Afzal MA, Buchanan JA, Cordeiro M, Bentley ML, ShorrokCA, Minor PD. RT-PCR based diagnosis and molecularcharacterization of mumps viruses derived from clinicalspecimens collected during the 1996 mumps outbreak inPortugal. J Med Virol 1997b; 52:349-353.
21. Örvell C. The reaction of monoclonal antibodies with stru c t u r a lproteins of mumps virus. J Immunol 1984; 132:2622-2629.
22. Yates PJ, Afzal MA, Minor PD. Antigenic and geneticvariation of the HN protein of mumps virus strains. J GenVirol 1996; 77:2491-2499.
23. Nöjd J, Tecle T, Samuelsson A, Örvell C. Mumps virusneutralizing antibodies do not protect against reinfectionwith a heterologous mumps virus genotype. Vaccine 2001;19:1727-1731.

KUWAIT MEDICAL JOURNALMarch 2006
ABSTRACT
Objective: To determine the correlation betweenaxillary and rectal temperatures in hospitalizedchildren.Subjects and Methods: This cross-sectional studywas conducted in the general pediatric ward ofDastgheib Hospital, Shiraz, Iran in spring 2002.One hundred and ninety six in-patients aged twomonths to five years were studied. The re c t a ltemperature was measured at a depth of 3 cm forthree minutes and the axillary temperature wasread after five minutes, both by using a mercury inglass thermometer.Results: The mean difference (SD) between therectal and axillary temperatures was 0.55 ºC (0.44)with the 95% confidence interval being 0.490 to
0.615. Twenty seven of 196 (13.8%) adjusted axillarytemperatures differed from rectal measurements bymore than 0.5 ºC but only seven (3.6%) differed bymore than 1 ºC. The mean difference (SD) betweenthe rectal and adjusted axially temperatures (Ax +0.55ºC) was only 0.0026 ºC (0.445), with the 95% CIbeing 0.06 to 0.06.C o n c l u s i o n s : Adefinite diff e rence was demonstratedbetween the rectal and axillary temperatures. Whenthe axillary temperature was adjusted by adding0.55 ºC, it provided a very good estimate of therectal temperature. Axillary temperature should beread after five minutes as demonstrated in thisstudy.
KEYWORDS: axillary, rectal, mean difference, temperature
Original Article
Accuracy of Axillary Temperature Compared with RectalTemperature in Sick Children
Address correspondence to:A.A. Asadi-Pooya, Assistant Professor, Department of Pediatrics, Nemazee Hospital, Shiraz, Iran 71937-11351. Tele/fax: 98-711-6265024, E-mail:[email protected]
Kuwait Medical Journal 2006, 38 (1): 25-27
Ali Akbar Asadi-Pooya1, Sara Kashef2
Departments of 1Pediatrics and 2Pediatric Immunology, Shiraz University of Medical Sciences, Shiraz, Iran
INTRODUCTIONThe degree of body temperature is an important
indicator of illness in children. The ideal techniquefor measuring body temperature should bepainless, reproducible, rapid, and accurately reflectthe core temperature. Measuring body temperatureby the rectal route is accurate and reproducible butunpleasant and sometimes dangerous. In contrastm e a s u rement of the axillary temperature isconvenient and safe[1-3], but there are conflictingreports about the accuracy of temperaturemeasured by the axillary route and its correlationwith the rectal temperature (the standardcriterion)[4-9].
This study was conducted to compare theaxillary temperature with the rectal temperature inill children admitted to hospital and to determine ifthe axillary temperature accurately reflects therectal temperature. The second purpose of thisstudy was to determine whether axillarytemperature could be adjusted to provide a goodestimate of rectal temperature if a clear correlationbetween the two measurements was found.
SUBJECTS AND METHODSOne hundred and ninety six in-patients aged
two months to five years were studied in this cross-sectional study in spring 2002 in the generalpediatric ward of Dastgheib Hospital, Shiraz, Iran,where the daytime temperature usually rangedfrom 20 ºC to 30 ºC. These children were routinelyhospitalized in this general pediatric ward forevaluation and treatment of their illnesses. Thepatient sample included a spectrum of mild andmoderate but not very severely ill children. Therectal temperature was measured at a depth ofthree cm by using a mercury in glass thermometerplaced in situ for three minutes. A x i l l a r ytemperature was taken with a mercury in glassthermometer inserted deeply in the axilla for fiveminutes, at the same time while taking the rectalt e m p e r a t u re in each patient. Thermometerplacement time was based on evidence fro mprevious studies[10,11]. The glass thermometers couldbe read within 0.1 ºC. The thermometers werecalibrated in a water bath adjusted to 37 ºC.Calibration was repeated periodically to ensure

Accuracy of Axillary Temperature Compared with Rectal Temperature in Sick Children March 200626
a g reement within ± 0.1 ºC of the standardlaboratory thermometer. All measurements weremade in the morning between 8-9 am. The sameobserver re c o rded both readings. A g roup oftrained medical students did the measurements.
Statistical Analysis:The difference between the rectal and axillary
temperatures was calculated for each patient. Themean difference and the 95% confidence interval(CI) were calculated. Statistical analyses were doneby t-test, re g ression analysis and Pearsoncorrelation coefficient. The Kolmogorov-Smirnovtest was used for rechecking the accuracy of theresults.
RESULTS:Out of 196 patients who were studied, 11 2
patients were in the 2-12 month age group and 84were one to five years of age. Forty five percent ofthe patients had an acute respiratory tract infection,40% had gastroenteritis, 5% had meningitis (viral orbacterial), 4% had urinary tract infections and 6%had other diagnoses.
The rectal temperature in these patients rangedfrom 36.3 ºC to 42 ºC, with a mean (SD) of 37.6 ºC(0.7). The axillary temperature in these patientsranged from 35.5 ºC to 40 ºC with a mean (SD) of 37ºC (0.68) (Table 1). Axillary temperature wascompared with the rectal temperature, which wasthe standard criterion. The mean difference (SD)between the rectal and axillary temperatures was0.55 ºC (0.44); there f o re in all subsequentcalculations, the axillary temperature was adjustedby adding 0.55 ºC (Table 2). Twenty-seven of 196(13.8%) adjusted axillary temperatures diff e re dfrom rectal temperature by more than 0.5 ºC, butonly seven (3.6%) differed by more than 1 ºC. Alinear relationship was derived between the rectaland axillary temperatures by regression analysis.The derived equation was: Rectal temperature ºC = 0.82 (Axillary temperatureºC) + 7.38.
The test of Kolmogorov-Smirnov did not show ad e p a r t u re from normality of the diff e re n c e sbetween the rectal and axillary temperature s(Kolmogorov-Smirnov Z = 2.12, p < 0.0001) butshowed a departure from normality intemperatures taken by the rectal route (K-S Z =
1.213, p = 0.106) and also in temperatures taken bythe axillary route (K-S Z = 1.177, p = 0.077) in theseill children.
The mean difference (SD) between the rectal andaxillary temperatures in the 2-12 month age groupwas 0.52 ºC (0.42) and in the 1-5 year age group was0.6ºC (0.47). This difference was not significant (p =0.207).
DISCUSSIONIn this study, the axillary temperature was on
average 0.55 ºC lower than the rectal temperature.When the axillary temperature was adjusted byadding 0.55 ºC, it provided a very good estimate ofthe rectal temperature; the mean difference (SD)between the rectal and adjusted axillary tem-peratures was only 0.0026 (0.445), with the 95% CIbeing 0.06 to 0.06 (Table 2). Only 3.6% of theadjusted axillary temperatures differed from therectal temperatures by more than 1 ºC. Absence ofd e p a r t u re from normality of the diff e re n c e sbetween rectal and axillary temperatures (p <0.0001) in spite of the presence of departure fromnormality in temperatures taken by the rectal route(p = 0.106) and also in temperatures taken by theaxillary route (p = 0.077) in these ill children alsoconfirms the reliability of this adjusted axillarytemperature. In the study designed by F Shann andA Mackenzie[1], axillary temperature was adjustedby adding 1 ºC, and it provided less accurateestimate of the rectal temperature in comparison toour study (the mean difference (SD) between therectal and adjusted axillary temperatures [A+1 ºC]was - 0.04 (0.45) with the 95% CI of - 0.94 to 0.86) .These differences can be explained by the differencein the methodology of taking temperatures. Theymeasured the axillary temperature only after twominutes but in our study, axillary temperature wasassessed after five minutes; the difference betweenaxillary and rectal temperatures was smaller in ourstudy and the 95% CI was narrower, which is areflection of increased accuracy. In the studyperformed by Kocoglu et al[11], axillary temperaturewas assessed after five minutes and adjusted byadding 0.72 ºC to the rectal temperature which isalmost similar to our study. In a recent study doneby Chaturvedi et al, the placement time for thestabilization of body temperature was reported to
StandardDeviation(SD)
Table 1: Rectal and axillary temperatures in 196 patients studied*
Temperature Minimum Maximum Mean
Rectal 36.3 42 37.6 0.70
Axillary 35.5 40 37 0.675
Rectal - Axillary - 0.8 2.7 0.55 0.44
*Data are given as 0C.
Table 2: Difference between the rectal and axillary temperatures in 196patients aged 2 months to five years, with the 95% CI*
Temperature Mean (SD); 95 % CI
Axillary + 0.55 - rectal 0.0026 (0.445); - 0.06 to 0.06
Axillary + 1 - rectal 0.45 (0.44); 0.38 - 0.51
Axillary - rectal 0.55(0.44); - 0.615 to - 0.49
*Data are given as mean (SD), 0C. CI indicates confidence interval

KUWAIT MEDICAL JOURNAL 27March 2006
be three minutes for the rectal and six minutes forthe axillary temperature measurements. Theyfound that the mean (SD) temperature differencebetween the rectal and axillary temperatures was0.3 (0.2) with the 95% CI of - 0.8 to 0.76 in infantsaged less than one year. An equation was derived intheir study [Rectal temp = 0.98 (Axillary temp) +0.8] which is different from our equation, despitethe fact that the mean of the rectal temperature intheir study was 37.5 ± 0.8 ºC, which is similar to ourstudy [37.6 ± 0.7 ºC; (p = 0.269)] and the mean of theaxillary temperature in their study was 37.1 ± 0.7ºC, which is also similar to our study [37 ± 0.68 ºC;(p = 0.234)]. It should be mentioned that the meand i ff e rence (SD) between the rectal and axillarytemperatures was significantly different betweenthe two studies [0.3 (0.2) vs. 0.55 (0.44); p = 0.0001].These differences with our findings could be due tothe difference in the placement time for the axillaryt e m p e r a t u re measurements between the twostudies. These studies also showed a high degree ofc o r relation between the rectal and axillarytemperatures[12], similar to our study (r = 0.79; P =0.0001).
In conclusion, temperature measured at theaxilla is convenient, painless, and safe and closelyreflects the rectal temperature. However, it is timeconsuming and for the best results, if mercury inglass thermometer is used, it should be read afterfive minutes as demonstrated in this study. In oursetting, the rectal temperature can be calculated byadding 0.55 ºC to the recorded axillary temperature.
ACKNOWLEDGMENTThe authors thank Dr MG Taiebee, MD, SHR
Tabatabaee, MS (Epidemiology) and Z Shayan, MS,(Biostatistics) for their help. The Shiraz Universityof Medical Sciences and Center for Development ofClinical Studies of Nemazee Hospital supportedthis work.
REFERENCES
1. Shann F, Mackenzie A. Comparison of rectal, axillary, andforehead temperatures. Arch Pediatr Adolesc Med 1996;150:74-78.
2. Payne D, Johnson A, Mc Kenzie S, Rogers M. Chemical andglass thermometers for axillary temperature. A rch DisChild 1994; 71:259-260.
3. Robinson JL, Seal RF, Spady DW, Joffres MR. Comparisonof esophageal, rectal, axillary, bladder, tympanic andpulmonary artery temperatures in children. J Pediatr 1998;133:553- 556.
4. Jensen BN, Jensen FS, Madsen SN, Lossl K. Accuracy ofdigital tympanic, oral, axillary, and rectal thermometerscompared with standard rectal mercury thermometers. EurJ Surg 2000; 166:848- 851.
5. Craig JV, Lancaster GA, Williamson PR, Smyth RL.Temperature measured at the axilla compared with rectumin children and young people: systematic review. BMJ 2000;320:1174-1178.
6. Lodha R, Mukerji N, Sinha N, Pandey RM, Jain Y. Is axillarytemperature an appropriate surrogate for core temperature? Indian J Pediatr 2000; 67:571-574.
7. Wilshaw R, Beckstrand R, Waid D, Schaalje GB. Acomparison of the use of tympanic, axillary, and rectalthermometers in infants. J Pediatr Nurs 1999; 14:88 -93.
8. Sund-Levander M, Forsberg C, Wahren LK. Normal oral,rectal, tympanic, and axillary body temperature in adultmen and women: a systematic literature review. Scand JCaring Sci 2002; 16:122-128.
9. Falzon A, Grech V, Caruana B, Magro A, Attard-Montalo S.How reliable is axillary temperature measurement? ActaPaediatr 2003; 92:309-313.
10. Morley CJ, Hewson PH, Thornton AJ, Cole JJ. Axillary andrectal temperature measurements in infants. Arch Dis Child1992; 67:122-125.
11. Kocoglu H, Goksu S, Isik M, Akturk Z, Bayazit YA. Infraredtympanic thermometer can accurately measure the bodytemperature in children in an emergency room setting. Int JPediatr Otorhinolaryngol 2002; 65:39-43.
12. Chaturvedi D, Vilhekar KY, Chaturvedi P, Bharambe MS.Comparison of axillary temperature with rectal or oralt e m p e r a t u re and determination of optimum placementtime in children. Indian Pediatr 2004; 41:600-603.

KUWAIT MEDICAL JOURNAL March 2006
ABSTRACT
Objectives: Adherence to treatment is a key factorin achieving blood pre s s u re control amonghypertensives. We examined correlates of non-adherence to hypertension treatment.Design: Patients attending the hypertension clinicof Hadiya center and receiving medication forhypertension, were followed up for at least threemonths. Subjects who had consumed less than 80%of the prescribed drugs were labeled as being non-compliant.Setting: Hadiya family practice center in Ahmadihealth district, Kuwait. S u b j e c t s : One hundred fifty four hypertensivepatients were included in the study.Main outcome measures: Compliance (measuredby pill count method in the last three months),demographic variables, patient knowledge ofhypertension, past and family history of chronicdiseases (including hypertension, diabetes mellitus,vascular disease and renal disease), the number ofantihypertensive drugs and the daily dose fre q u e n c y.
Results: Non-compliance was associated with lackof knowledge about hypertension, negative familyhistory of chronic diseases; multiple anti-hypertensive medications prescribed and increaseddaily dose frequency (p < 0.05). These factors,except for family history of chronic diseases, werefound to be statistically significant independentpredictors of non-compliance in multiple logisticre g ression analysis. There was no statisticallysignificant difference in the demographic variables(mean age, sex distribution, marital status,occupational status, educational level and income),mean duration of hypertension and personalhistory of chronic diseases between compliant andnon-compliant hypertensives.C o n c l u s i o n : Patient’s lack of knowledge abouthypertension, multiple antihypertensive medicationsprescribed and increased daily dose frequency arethe major correlates of non-adherence tohypertension treatment.
KEYWORDS: blood pressure control, compliance, hypertension
Original Article
Comparison of Compliance Versus Non-Compliance toAnti-hypertensive Agents in Primary Health Care - An Area
Based Study
Address correspondence to:Dr. Ali A. Al-Yahya, RCGP(UK), Primary Health Care, Abu Halifa Clinic, P.O.Box: 32/889 Rumaithya, Kuwait. Tel:(965)3725592, 3728758,Fax: (965)3725592
Kuwait Medical Journal 2006, 38 (1): 28-32
Ali A Al-Yahya1, Amal M Al-Mehza2, Huda Al-Ghareeb3
Primary Health Care, 1Abu Halifa Clinic, 2Hadiya Clinic, 3Qurain special Clinic, Kuwait.
INTRODUCTIONHypertension is an internationally common
disease[1,2] and an important treatable public healthp ro b l e m[ 3 , 4 ]. It is defined as a blood pre s s u re(systolic /diastolic) ≥ 140 / 90 mmHg[5,6]. It is amajor risk factor and a powerful predictor ofcardio-vascular morbidity and mortality[4,7-12] withp roven benefits after tre a t m e n t[ 1 3 - 1 5 ]. Impro v e dcontrol of hypertension, in turn, has contributed toreductions in incidence rates for stroke andischemic heart disease[7,10-17]. Despite these gains,poorly controlled hypertension remains a majorhealth problem[18-24]. Data in literature suggests that79% of people with hypertension do not have theirblood pressure under control[18]. The Third National
Health and Nutrition Survey in the United Statesshowed that only 14 - 25% of treated hypertensiveadults had achieved effective blood pre s s u recontrol of < 140 / 90[19]. This supports the “rule ofhalves”, which indicates sub-optimal health carestandards in hypertension, first described in theUnited States in the 1970s [25,26].A generally acceptedpublic health approach to achieving blood pressurecontrol involves a sequential model, the steps beingdetection, patient awareness of the diagnosis,t reatment adherence and blood pre s s u recontrol[27,28]. Of these, adherence to treatment hasbeen widely recognized as key to controlling bloodpressure[24,29-36]. In one study a drug non-compliancerate was 34% and this was the strongest predictor

KUWAIT MEDICAL JOURNAL 29March 2006
of poor blood pressure control[29]. In Eastern Sudanit was found that 92% of compliant patients hadcontrolled blood pressure in comparison with 18%of non-compliant patients [2].
In the current study, we examined correlates ofcompliance and non-compliance to hypertensiontreatment.
SUBJECTS AND METHODSSubjects:
Hypertensive patients (n = 154) attending thehypertension clinic of Hadiya Center and receivingmedications were included in the study. HadiyaCenter is the only family medicine center inAhmadi health district in Kuwait serving a totalpopulation of 13,000. It has an establishedhypertension clinic with a registry. These subjectswere followed for at least three months.
Setting and measurements: During this time three blood pre s s u re (BP)
measures were taken at an interval of at least twoweeks after patients were maintained on theirmedication for at least six weeks. The blood
pressure control was assessed and a questionnairewas completed to determine compliance rate andfactors responsible for patient non-compliance.Patients were labeled as uncontrolled hyper-tensives if the mean of three measures of systolicblood pressure (SBP) was ≥ 140 mmHg and/ordiastolic blood pressure (DBP) was > 90 mmHg[5,6].
Factors of non-compliance studied included:demographic information, age, sex, marital status,occupational status, income, patient knowledge ofhypertension, mean duration of hypertension,personal history of chronic diseases (includingvascular and renal disease), family history ofchronic diseases (including hypertension, vascularand renal disease) and number of antihypertensivedrugs (diuretic, ß-blocker, ca++ antagonist, angio-tensin converting enzyme inhibitor, angio-tensin 2antagonist, α-blocker and others) and the dailydose frequency.
Patient non-compliance with antihypertensivedrugs was measured at the end of follow-up bytaking history and doing a pill count. Subjects whohad consumed less than 80% of the prescribeddrugs were labeled as being non-compliant[29,37]. Thefactors were measured by an interviewer-administered questionnaire.
Statistical analysis:Data were collected and analyzed using the
statistical package for social sciences (SPSS). Thechi-square test was used to compare categoricalvariables like occupational status, educational leveland knowledge of BP in the two groups ofcompliant and non-compliant hypertensives. Thetwo sample t-test was used to compare means ofage and duration of hypertension. A p value ≤ 0.05was used as the cut-off level for statisticalsignificance. Multivariate analysis (multiple logisticregression) was performed with non-compliance asthe dichotomous outcome variable with thosevariables which were significant in the chi-squareas predictor variables in order to calculate adjustedodds ratios (OR) and 95% confidence intervals (CI).
RESULTSOut of the 154 subjects recruited into the study,
132 completed the follow-up period of thre emonths. Of the 132 subjects who completed follow-up, 84 (64%) subjects had uncontrolled hyper-tension. The overall rate of compliance was 88.6%.One out of 48 (2%) of controlled hypertensives wasnon-compliant by pill count as compared with 14out of 84 (17%) uncontrolled hypertensives. Thisdifference was statistically significant (p < 0.05).
The mean age (SD) in years in the compliant andnon-compliant group was 54.4 (9.9) and 55.1 (9.8)re s p e c t i v e l y. Smilarly, the mean duration of
Table 1: Comparison of the mean age, sex distributionand socio-demographic feature rates in compliant andnon-compliant hypertensives
Variables Compliant Non-compliant p- value*
(n = 117) (n = 15)
n (%) n (%)
FemaleMale
Marital statusCurrently marriedUnmarried(single, widow,divorced)
Occupational statusUnemployedRetiredHousewifeEmployed
Educational levelIlliterateElementary schoolIntermediate schoolSecondary schoolAbove (college, post
graduate)
IncomeLow (< 500 KD)Middle (500-<1000KD)High (≥ 1000KD)
* based on chi-square test
72 (61.5)45 (38.5)
25 (21.4)92 (78.6)
19 (16.2)34 (29.1)38 (32.5)26 (22.2)
43 (36.8)22 (18.8)22 (18.8)15 (12.8)15 (12.8)
29 (28.2)34 (33)40 (38.
7 (46.7)8 (53.3)
03 (20)12 (80)
2 (13.3)6 (40)4 (26.7)3 (20)
6 (40)2 (13.3)2 (13.3)2 (13.3)3 (20)
3 (21.4)3 (21.4)8 (57.1)
0.269
0.903
0.857
0.913
0.420

Comparison of Compliance Versus Non-Compliance to Anti-hypertensive Agents in Primary ..... March 200630
hypertension in years for the same group was 8.7(7.2) and 6.4 (5.1) respectively. These differenceswere evaluated using independent t’test and p-values, not statistically significant (0.739 and 0.231respectively).
There was no statistically significant differencein the sex distribution, marital status, occupationalstatus, educational level, income and personal pasthistory of chronic disease in compliant and non-compliant subjects (Table 1 and 2).
There was significant difference in the patient’sknowledge of hypertension in compliant and non-compliant hypertensives (p < 0.05) (Table 2). Non-compliant hypertensives were ignorant about thefact that hypertension is a chronic disease.
I n c reased number of drugs and daily dosefrequency of medication were more in the non-compliant group and this was statisticallysignificant (p < 0.05) (Table 2). Patients on twicedaily dose regimen - as perindopril (“coversyl”) - orthree times daily dose regimen - as methyldopa(”aldomet”) - showed lower compliance rate thanthose on once daily dose regimen (11.1%, 9.4%,79.5% respectively)
Patients who had negative family history ofchronic diseases were more in the non-compliantg roup and this was statistically significant (p < 0.05)(Table 2).
Multiple logistic regression analyses revealedthat patient’s knowledge of hypertension (p < 0.05),number of drugs (p < 0.05) and daily dosef requency of medication (p < 0.01) were independentpredictors of non-compliance, while family historyof chronic diseases was not (Table 3).
DISCUSSIONOur study showed a compliance rate of 88.6%
and this is encouraging in comparison with otherstudies[29,37,38]. We investigated the non-compliancerate at the end of follow-up and this wassignificantly associated with uncontrolled BP.Hence, compliance strategies are needed[39]. Thisnumber of non-compliant and uncontro l l e dhypertensives formed about 17% of our studypopulation and would be an ideal target for healtheducation.
The patient’s knowledge and awareness ofhypertension was significantly associated withcompliance to medication for hypertension. Thiss t resses the importance of health education toincrease the knowledge of hypertension and it’ssequelae to improve patient’s non-compliantb e h a v i o r. The relationship between healthknowledge and compliance was supported in somestudies[24,37] but not in others [38,40]. Data in literaturesuggests that patients who knew about theimportance of compliance had a significantlyhigher compliance rate than those who had beenignorant of that aspect[37]. Other literature revealedrelatively little support for a strong relationshipbetween health knowledge and medicationcompliance[38,40].
Another significant association with non-compliance is the number of drugs and the dailydose frequency of antihypertensive medicationprescribed. This is self-explanatory, since multipledrug therapy and more frequent daily dose makethe patient more non-compliant to medication andthey may be exposed to more side effects. Thisrelationship is supported in other studies[41]. Data inliterature suggests that compliance improved from59% on a three-time daily regimen to 83.6% on aonce-daily regimen[41]. Thus compliance improvesdramatically as prescribed dose fre q u e n c ydecreases. As a result, it is important for the healthcare providers to improve compliance by selectingmedications that permits the lowest dailyprescribed dose frequency.
Negative family history of chronic diseases wasassociated with non-compliance and this can be
Table 2: Comparison of mean duration of hypertension,patient’s knowledge of hypertension, personal history ofchronic diseases (vascular and renal diseases), familyhistory of chronic diseases (hypertension, vascular andrenal diseases), the number of drugs and the daily dosefrequency of medication
Variable Compliant Non-compliant p- value(n=117) (n=15)n (%) n (%)
Patient knowledge ofhypertension
GoodPoor
Personal history ofchronic diseases
Positive historyNegative history
Family history ofchronic diseases
Positive historyNegative history
Number of drugs:1 drug2 drugs3 or more drugs
Daily dose frequencyof medication
Once dailyTwice dailyThree times daily
84 (71.8)33 (28.2)
80 (68.4)37 (31.6)
80 (79.2)21 (20.8)
53 (45.3)59 (50.4)05 (4.3)
93 (79.5)13 (11.1)11 (9.4)
6 (40) 9 (60)
12 (80)03 (20)
5 (45.5)6 (54.5)
9 (60)3 (20)3 (20)
8 (53.3)5 (33.3)2 (13.3)
0.013
0.356
0.013
0.013
0.045

KUWAIT MEDICAL JOURNAL 31March 2006
explained by the fact that a patient with positivefamily history of chronic disease will have moreexperience about diff e rent diseases and theircomplications since it is present in the family. Thismakes him more aware about the importance ofcompliance.
Our study showed no significant relationshipbetween demographic features and the compliancerates. Regarding this aspect, reports differ on then a t u re of such associations. In one study,compliance was associated positively with malesex, and negatively with older age[ 3 7 ] while inanother study, compliance was associatednegatively with younger age and male sex[38]. Oneother study showed no statistical significantdifference in the demographic features in compliantand non-compliant subjects[35].
The study has certain limitations. This is anarea-based study conducted in one health district.The result of this study may therefore, be morerelevant and significant, if it included several healthdistricts of Kuwait. The simple pill count method ofquantitating medication compliance has potentialshortcomings. It does not provide informationabout day or time of dose removal. There f o re, bettermethods of detecting poor compliance need to bedeveloped such as the use of electronic devices. Itconsists of special pill containers that electronicallyrecord date and time of medication removal[41].
In conclusion, it is recommended that healtheducation should be stressed upon to improve therate of compliance by improving the patient’sknowledge about hypertension and its sequalae.Another important action that health careproviders can take to improve compliance is toselect medications that permit the lowest daily dose
frequency possible.
REFERENCES
1. Arauz- Pacheco C, Parrott M A, Raskin P. The treatment ofhypertension in adult patients with diabetes. Diabetes Care2002; 25:134-147.
2. Elzubier AG, Husain AA, Suleiman IA, et al. D ru gcompliance among hypertensive patients in Kassala,Eastern Sudan. EMHJ 2000; 6:100-105.
3. Chobanian AV, Bakris GL, Black HR, et al. The Seventhreport of the Joint National Committee on prevention,detection, evaluation and treatment of High BloodPressure: The JNC 7 Report. JAMA2003; 289:2560-2571.
4. Houston MC. Hypertension strategies for therapeuticintervention and prevention of end-organ damage. PrimCare 1991; 18:713-753.
5. 2003 World Health Organization- International Society ofHypertension (ISH) Statement on Management ofHypertension. J Hypertens 2003; 21:1983-1992.
6. Primary Health Care Clinical Practice Guideline Series:Hypertension, Kuwait. Ministry of Health, CentralDepartment of Primary Health care. 2001; 2.
7. Glasser SP. Hypertension syndrome and cardiovascularevents; high blood pressure is only one risk factor. PostgradMed 2001; 110:29-36.
8. Pocok SJ, Mccormack V, Gueyffier F, et al. A score forpredicting risk of death from cardiovascular disease inadults with raised blood pressure, based on individualpatients data from randomized controlled trials. BMJ 2001;323:75-81.
9. Palatini P, Frigo G, Vriz O, et al. Early signs of cardiacinvolvement in hypertension. Am Heart J 2001; 142:1016-1023.
10. Palmieri V, Wachtell K, et al. Left ventricular function andhemodynamics of inappropriate left ventricularhypertrophy in patients with systemic hypertension: theleft study . Am Heart J 2001; 141:784-791.
11. Sung J, Ouyang P, Bacher AC , et al. Peripheral endothelium-dependent flow - mediated vasodilatation is associatedwith left ventricular mass in older persons withhypertension - Am Heart J 2002; 144:39-44.
12. Wachtell K, Palmieri V, Olsen MH, et al. Urine albumin/creatinine ratio and echo cardio graphic left ventriculars t ru c t u re and function in hypertensive patient withelectrocardio graphic left ventricular hypertrophy : The LeftStudy. Am Heart J 2002; 143:319-326.
13. The 2001 Candian Hypertension Recommendation - what isnew and what is old but still important. Can J Cardiol 2002,18(6). WWW. Pulsus. Com / CARDIOL/18-60/camped.htm
14. Rosei EA. Assessment of Pre clinical Target Organ Damagein Hypertension : Left Ventricular Hypertrophy . EuropeanSociety of Hypertension Scientific Newsletter: Update onHypertension Management 2001; 10.
15. MacMachons, Rodgers A. The effect of blood pressurereduction in older patients: an overview of five randomizedc o n t rolled trials in elderly hypertensives. Clinic ExpHypertens 1993, 15:967-978.
16. Ostfeld AM, Wilk E. Epidemiology of stroke, 1980-1990: aprogress report. Epidemiol Rev 1990; 12:253-256.
17. Goldman L, Cook EF. The decline in ischemic heart diseasemortality: an analysis of the comparative effects of medicalintervention and changing lifestyles. Ann Intern Med. 1984;101: 825-836.
18. Adults taking action to control their blood pressure- UnitedStates, 1990. MMWR Morb Mortal Wkly Rep 1994; 43:509-511, 517.
Table 3: Multiple logistic regression analysis to identifypredictors of non-compliance
Variables ratio Coefficient (SE) Odds
Patient knowledge of hypertension (ref = good)
Poor 2.552 ( 1.039) 12.829*
Family history of chronic diseases (ref = positive history)
Negative history 1.606 (0.881) 4.983
Number of drugs (ref =1 drug)2 drugs - 2.772 (1.138) 0.063*3 drugs 1.158 (1.174) 3.184
Daily dose frequency of medication (ref = once daily)
Twice daily 4.105 (1.31) 60.657** Three times daily 1.425 (1.349) 4.160
* p < 0.05 ** p < 0.01 SE = standard error

Comparison of Compliance Versus Non-Compliance to Anti-hypertensive Agents in Primary ..... March 200632
19. Burt VL, Whelton P, Roccella FJ, et al. P revalence ofhypertension in the US adult population. Results from thethird national health nutrition examination survey, 1988-1991. Hypertension 1995; 25:305-313.
20. Winickoff RN, Murphy PK. The Persistent problem of PoorBlood Pressure Control. Arch Intern Med 1987; 147:1393-1396.
21. Caro JJ, Salas M, Speckman JL. Persistence with treatmentfor hypertension in actual practice. CMAJ 1999; 160:31- 37.
22. Manicia G, Sega R, Milesi C, et al. Blood pressure control inthe hypertensive population. Lancet 1997; 349:454-457.
23. Stock well DM, Madhavan S, Cohenm, et al. Thedeterminants of hypertension awareness, treatment andcontrol in an insured population. Am J Public Health 1994;84:1768 -1774.
24. Shea S, Misra D, Ehrlich MH, et al. Predisposing factors fors e v e re, uncontrolled hypertension in an inner - cityminority population . N Engl J Med 1992; 327:776-781.
25. Mashru M, Lant A. Inter practice audit of diagnosis andmanagement of hypertension in primary care: educationalintervention and review of medical records. BMJ 1997;314:942-946.
26. Whelton PK. Epidemiology of hypertension. Lancet 1994;344:101-106.
27. National Heart, Lung, and Blood Institute. Hypertensionprevalence and the status of awareness, treatment, andc o n t rol in the United States: final report of theSubcommittee on Definition and Prevalence of the 1984Joint National Committee. Hypertension 1985; 7:457-468.
28. 1988 Joint National Committee. The 1988 report of the JointNational Committee on Detection, Evaluation, andTreatment of High Blood Pressure. Arch Intern Med 1988;148:1023-1038.
29. Joshi PP, Salkar RG, Heller RF. Determinants of poor bloodpressure control in Urban hypertensives of central India. J
Hum Hyperten 1996; 10:299-303.30. Buck CW, Donner A P. Blood pre s s u re control in
hypertensives a model for the study of life events . J Chr Dis1984; 4:247-253.
31. Leenen FHH. Intermittent blood pressure control: Potentialconsequences for out come. Can J Cardiol 1999; 15:13c-18c.
32. Bittar N. Maintaining long - term control of blood pressure:the role of improved compliance . Clin Cardiol 1995; 18:312-317.
33. Jones JK Gorkin L, Lian et al. Discontinuation of andchanges in treatment after start of new courses ofantihypertensive drugs: a study of a United Kingdompopulation. BMJ 1995; 311:293-295.
34. Psaty BM, Savage PJ, Tell GS, et al. Temporal patterns ofantihypertensive medication use among elderly patients.JAMA1993, 270:1837-1841.
35. Shea S, Misra D, Ehrilch MH, et al. Correlates of Nonadherence to Hypertension treatment in an Inner- CityMinority population . Am J public Health 1992; 82:1067-1612.
36. Setaro JF, Blacck HR. Refractory hypertension. N Engl Med1992; 327:543-547.
37. Khalil SA, Al zubier AG. Drug compliance amonghypertensive patients in Tabuk, Saudi Arabia. J Hypertens1997; 15:561-565.
38. Klein LE. Compliance and Blood Pre s s u re Contro l .Antihypertensive Drug Effects Suppl II. Hypertension1988; 11:61-64.
39. Clark LT. Improving compliance and increasing control ofhypertension: needs of special hypertensive populations.Am Heart J 1991; 121:664-669.
40. Klein LE, German PS, McPhee ST, et al. Aging and itsrelationship to health knowledge and medicationcompliance. Gerontologist 1982; 22:384-387.
41. Eisen SA, Miller DK, Woodward RS, et al. The Effect ofPrescribed Daily Dose Frequency on Patients MedicationCompliace. Arch Intern Med 1990; 150:1881-1884

KUWAIT MEDICAL JOURNALMarch 2006
ABSTRACT
Objective: To identify the risk factors and thecausative agents for acute poisoning in children inthe Jahra Health Region.Methods: The medical re c o rds of 209 childre nhospitalized during the four and a half year periodfollowing acute poisoning were reviewed. The datawas analyzed and compared with the previousstatistics of Kuwait and other parts of the world.Results: Pediatric acute poisoning accounted for1.58% (209) of all the pediatric admissions (13,080)during our study period. The majority of children
(73.97%) were in the age group of 1-3 years.K e rosene ingestion was identified as thecommonest (53.97 %) causative household product.Psychotropics and antihistaminics were implicatedas common medicinal causative agents. Majority ofour poisoning cases were accidental in nature(97.11%). All children were discharged home ingood condition. Lack of education, overcrowding,poor socio-economic status and improper chemicaldispensing were the leading risk factors identifiedin our study.
KEY WORDS: accidental, hospitalization, poisoning
Original Article
Risk Factors in Acute Poisoning in Children - ARetrospective Study
Address correspondence to:Dr. Raj Rani Gulati, P.O.Box 1853, Pin Code 13019, Safat – Kuwait. Tel: 6074570.
Kuwait Medical Journal 2006, 38 (1): 33-36
Syeda Akhtar, Gulati Raj Rani, Fahad Al-AneziDepartment of Pediatrics, Al-Jahra Hospital, Kuwait
INTRODUCTIONChildhood poisoning is a major cause of
morbidity in the developing as well as thedeveloped world. Inspite of the success of someinterventions to prevent accidental poisoning in thepediatric population[1,2], toxic ingestions continue tobe a common occurrence[3,4]. Globally, the pattern ofchildhood poisoning is changing rapidly[5]. After1972, the incidence of accidental poisoning andmortality from drug poisoning has fallendramatically among children less than five years ofage in the USAand after 1976 in the UK due to theuse of child resistant containers “(Sibert et al, 1977;Walton 1982; Craft 1983; Jackson 1983) andTurkey[5]. In 1986, Falaki and Fernando reported3.7% of all pediatric admissions due to accidentalpoisoning in Kuwait[6]. In most reports, the victimsare predominantly boys[7,8]. Recent stress in thefamily[9,10] and recent change of residence have beenimplicated as predisposing factors[10]. Behaviouralcharacteristics and the temperament of childrenhave been suggested as contributing factors inaccidental poisoning[ 11 - 1 3 ]. Socio-economic diff e re n c e sin the incidence have been reported in the childrenfrom the same community [8].
The type of poisoning and causative agents varyin different parts of the world depending on theeducational status, local beliefs and customs etc.[14-
16]. The mortality has declined significantly[17].
MATERIALS AND METHODSMedical records of 209 children admitted with
acute poisoning during the four and half yearperiod starting from January 1992 until June 1996were reviewed. The clinical data obtained fromthese medial re c o rds included: (1) historicalinformation, (2) physical findings and (3) chemicalidentification. The positive historical informationincluded witnessed exposures or observation of thechild in proximity to the opened or available toxicsubstance. Physical findings were considere dpositive, if the patient exhibited signs andsymptoms specific for the overdosage such as,recent repetitive cough in case of kero s e n eingestion and depressed level of consciousnessassociated with psychotropic ingestion. Chemicalidentification was established by qualitative andquantitative analysis of blood. Our 24-hourlaboratory services provided toxicology screen forthe following drugs: barbiturates, tricyclica n t i d e p ressants, salicylates, carbamezpine andphenytoin (Machine Kopas Integera). These druglevels were measured by florescent polarizationmethod and result were avilable to us within 30minutes.
Each medical re c o rd was reviewed by oneauthor and 20% of these charts were re-reviewed toreconfirm the appropriate data which includedcharacteristics like age, sex, nationality, socio-

Risk Factors in Acute Poisoning in Children - A Retrospective Study March 200634
economic status and the agent implicated in theacute poisoning. The age factor was divided intofour subgroups; (a) less than 1 year, (b) 1-3 years,(c) 3-6 years and (d) 6-12 years. The causative agentimplicated was categorized into (a) householdp roduct, (b) medicinal product and (c) plantproduct. The type of poisoning was categorized asaccidental or non-accidental.
RESULTSOut of 13,080 total pediatric admissions during
the study period, 209 cases accounted for acutepoisoning. Overall 203 cases (97.11 %) were due toaccidental and six cases (2.89 %) due to non-accidental poisoning.
The age distribution of these 209 cases is shownin Table 1. The majority of children (n = 155,73.91%) were in age groups less than three years. Atotal of 200 (95.65 %) children belonged to less thansix years of age. A male predominance (n = 126)was found among our cases (1.55:1). The ratio ofKuwaiti to non-Kuwaiti children was 1:1.78. Thisratio reflected the population pattern in the JahraHealth region during the study period.
Improperly stored household products were thecommonest causative agents implicated in 57.97%of cases (Table 2). Kerosene ingestion aloneaccounted for 43.47% of all admissions. Shampoos,detergents and rodenticides contributed to 14.49%admissions.
In the medicinal products group (Table 3), thepsychotropic drugs were ingested by 14 children(6.76 %) and antihistaminics by 13 children (6.31 %).The other medicinal products implicated wereantiepileptics in 12, analgesics in 10 and methylsalicylates in nine children. Miscellaneous drugsand antibiotics prescribed to any other familymember at home were taken by at least one child,where the child was reported to be playing with thecolourful attractive container full of drug. He wasseen mouthing, spitting and vomiting with orwithout altered sensorium. Two children (0.96 %)w e re admitted with vomiting and diarrh e afollowing castor seed ingestion. A single substancewas implicated in 99% of our cases. Two school-going children (one eight year old boy withparacetamol and another nine year old girl withtegretol ingestion) were considered cases of para-suicidal poisoning after detailed interro g a t i o n .Four children were poisoned iatrogenically (a nineyear old boy by his peer in the school, a six year oldboy who took belladonna mixture himself and amother who used methyl salicylate in two cases).Two cases were admitted twice, poisoned with twodifferent products on two occasions during thestudy period.
The majority of cases were discharged homeafter 24 hours. The maximum duration of stay was
five days in one case. He had psychotro p i cingestion followed by respiratory failure whichre q u i red ventilation. Local hospital investigatorwas informed in all the cases. All the patients weregiven relevant information prior to discharge fromthe hospital.
DISCUSSIONAcute exposure to drugs and household
products in children are common clinical problemsof important concern to the general pediatrician.Our study showed that 1.58% of all the pediatricadmissions during the study period were due toacute poisoning. Some previous studies havereported 3.71% [ 6 ] and 5%[ 1 4 ] admissions due toaccidental poisoning in children. It appears that theintroduction of child proof caps did influence thetotal number of hospitalizations due to accidentalpoisoning. Here we should not forget the fact thatmuch minimal ingestion at home may not warranta visit to the hospital and there f o re, the tru eincidence may be higher than reported here.
The commonest age group involved in acutepoisoning universally (1-3 years)[1-8] is the same asseen in our study (Table 1). Children in this agegroup are reported to have a higher propensity toe x p l o re and put everything in their mouth.However, they are unable to discriminate betweendangerous and safe products. Above three years ofage, there are fewer cases as these children can bewarned against harmful products by a responsiblecaretaker. Nevertheless, majority of children undersix year of age do need strict supervision[15-21].
Drugs were shown to be the leading causativeagents for acute poisoning in children in 1986 byFalaki in Kuwait[6]. Our study showed that 120(57.11 %) cases were due to household products.Kerosene alone was implicated in 90 (43.48%) cases.Kerosene is a common multipurpose householdp roduct available in low socio-economic statusfamilies in the region. It was found to beimproperly stored in their kitchens and kept atreachable levels. Kerosene has been reported as theleading causative household product by differentauthors[14-17].
Insecticides, rodenticides, shampoos andd e t e rgents were the next common household
Table 1: Hospitalization by age group and sex ratio (n = 209)
Age group (%) M : F
< 1yr = 6 (2.9) 1 : 11 - 3 year = 155 (73.9) 10 : 73 - 6 year = 39 (18.8) 9 : 46 - 12 year = 9 (4.4) 2 : 1
M = Male, F = Female

KUWAIT MEDICAL JOURNAL 35March 2006
products implicated in poisoned children (Table 2).No child died in last 20 years due to their accidentali n g e s t i o n[ 1 8 , 1 9 ]. It is possible most ro d e n t i c i d e savailable contain less concentration of a long actinganticoagulant. It has been recommended that allsymptomatic children with caustic ingestionshould be endoscoped[20].
Pharmaceutical products have caused 53 deathsout of total fatalities in one series[21]. In our study, 88(42.03%) children ingested various drugs (Table 3).Although no child died in our series, this is notintended to relax our current state of poisonprevention vigilance. We need to intensify theareas where further efforts will effectively decreasepoisoning morbidity and mortality.
D rug poisoning profile depends on thegovernment policies for (a) pre s c r i p t i o n s ,(b) availability, (c) packaging, (d) formulation etc.Aspirin and acetaminophen despite their frequentuse at home, were not ingested even by one childin this study. Aspirin induced fatality was reportedin another study from Australia[17]. The decrease inadmission due to aspirin and acetaminopheningestion probably re p resents the effects ofimproved safety packaging of both these agents.Psychotropics were ingested by 14 (6.76%) children.The reported case fatality due to psychotro p i cingestion in one of the series is 1:44[17]. .
Antihistaminics ranked number two in the listof medicinal products. Similar data has beenreported pre v i o u s l y[ 1 7 ]. Benzodiazapines wereequally implicated in that study. These are drugs ofintermediate toxicity and commonly prescribed.P o t e n t i a l l y, toxic iron ingestion has decre a s e dc o n s i d e r a b l y. Easy availabily of commonlyprescribed drugs in the health region includeda n t i c h o l i n e rgics, analgesics, methyl salicylate,chocolate colored iron tablets, salbutamol, oralcontraceptives and multi colored multi vitamins.
Non-accidental poisoning was seen in six(2.89%) of our cases as explained in the results. It is
commonly seen in older children (6-12 years). Theprecipitating factors may be minor arguments withfriends or parents. Such episodes should not beregarded as trivial.
It is said that more than 75 percent of thepoisoning exposures can be managed at homewithout medical intervention, because either theproduct involved is inherently not very toxic or thequantity of the product ingested is not sufficient toproduce toxic effects. Although all our children lefthome in good condition this does not permit uscomplacency in our approach to the poisonprevention.
Lack of education, poor socio-economic status,overcrowding in large families were identified asthe leading risk factors in our study. The improperstorage of dangerous household products likekerosene, rodenticides, detergents, caustics etc. leadto the majority of our poisoning. Commonlyp rescribed toxic as well as non-toxic dru g s(psychotropics, antiepileptics, methyl salicylates,antihistaminics) were easily accessible to theunattended children near their beds or in theirmothers’ hand bag. Although our study showed adecline in the morbidity and there was no mortality,still the number of children poisoned remains high.We need to raise our level of awareness towardspresent trends and patterns of pediatric poisoningin our area.
A poisoning prevention program should be anintegral part of all well-baby clinics, even before achild is mobile. The counselling for parents andcaretakers must include how to poison- proof theirchild’s environment.
CONCLUSIONIn this study, we have identified several risk
factors and causative agents for acute poisoning inchildren in the Jahra Health Region. These factorscould be useful in strategy planning as well as
Table 2: Spectrum of various household productsimplicated in poisoning (n =121).
Table 3: Spectrum of various drug poisonings (n = 88)
Nature of Drugs No. of Cases n(%)
Tricyclic antidepressants 14 (6.7)Antihistaminics 13 (6.3)Anticholinergics 12 (6.4)Analgesics (Brufen) 10 (5.7)Methyl salicylates 10 (5.7)Iron tablets 4 (2.1)Salbutamol 3 (1.5)Unknown 6 (3.1)Miscellaneous 16 (7.9)(oral contraceptive, carbamezapine,pyridium, eltroxin, mosegor,oral hypoglycemic, multivitamin, antihypertensive)
Nature of Household Product No. of Cases (%)
Petroleum Distillates 90 ( 43.4)
Rodenticides 8 (3.9)
Insecticides 4 ( 1.9)
Antiseptics 8 (3.9)
Detergents 1 (0.4)
Plant (Castor seeds) 2 (0.9)
Unknown 1 (0.4)
Miscellaneous(Shampoo, 7 (3.3)
Musk oil, Super-glue etc.)

Risk Factors in Acute Poisoning in Children - A Retrospective Study March 200636
formatting protocols for the primary, secondaryand tertiary level management of this problem. Weare continuing to work for our next study (part II)to learn more about the present patterns of thepediatric poisoning in the Jahra Health Region.
REFERENCES
1. Clark A, Walton WW. Effect of safety packaging on aspiriningestion by children. Pediatrics 1979; 63:687–693.
2. Walton WW. An evaluation of the Poison PreventionPackaging Act. Pediatrics 1982; 69:363–370.
3. Poisoning among children – United States. MMWR 1984;33:129–131.
4 . Epidemiology of serious poisonings. Clin Toxicol Rev 1983; 5.5. Ahmet Pinar, John Fowler, G. Randall. Acute poisoning in
Izmir, Turkey – A pilot Epidmiological Study. Clin Toxicol1993; 31:595–601.
6. N.N. Falaki, N.P. Fernndo. Acute poisoning in children –one year one hospital experience. J Kwt Med Assoc 1986;20:3–11.
7. Williams BC, Kotch JB. Excess injury mortality amongc h i l d ren in the United States: comparison of re c e n tinternational statistics. Pediatrics 1990; 86:1067–1073.
8. Trinkoff AM, Baker SP. Poisoning hospitalizations anddeaths from solids and liquids among children andteenagers. Am J Public Health 1986; 76:657–660.
9. Sibert R. Stress in families of children who have ingestedpoisons. Br Med J 1975; 3:87–89.
10. Eriksson M, Larson G, Winbladh B, Zetterstom R.Accidental poisoning in preschool children in the
Stockholm area. Acta Paediatr Scand 1975; 275:96–101.11. Sobel R. The psychiatric implications of accidental
poisoning in childhood. Pediatr Clin North Am 1970; 17:653–685.
12. Sibert JR, Newcombe RG. Accidental ingestion of poisonsand child personality. Postgrad Med J 1977; 53:254–256.
13. Nyman G. Infant temperament, childhood accidents andhospitalization. Clin Pediatr 1987; 26:398-404.
14. VP Choudhary, et al: Spectrum of accidental poisoningsamong children in Afghanistan. Ann Trop Pediatrics 1987;7:278-281.
15. NA Nagi, ZA Abdulla: Kerosene poisoning in children inIraq. Postgrad Med J 1995; 71:419 – 422.
16. G. N. Lucas. Kerosene oil poisoning in Children: A Hospitalbased prospective study in Sri-Lanka. Indian J Pediatr 1994;61:683-687.
17. J Pearn, J Nixon, et al: Accidental poisoning in Childhood:Five year urban population study with 15 year analysis offatality. Br Med J 1984; 288:44-46.
18. PB Casey, JP Thompson, JA Vale. Suspected PediatricPesticide Poisoning in the UK I – Home A c c i d e n tSurveillance system 19820\-1988. Hum Exp Toxicol 1994;13:529–533.
19. J P Thompson, PB Casey, JA Vale. Suspected PediatricPesticide Poisoning in the UK II – Home A c c i d e n t a lSurveillance system 1989 – 1991. Hum Exp Toxicol 1994;13:534–536.
20. HBT Christsen. Prediction of complications followingunintentional caustic ingestions in children. Is Endoscopyalways necessary ? Acute Pediatr 1995; 84:1177 -1182.
21. Toby Litovitz and Anthony Manoguerza. Comparison ofPediatric Poisoning Hazards: An Analysis of 3.8 MillionExposure Incidents. Pediatrics 1992; 89:999-1006.

KUWAIT MEDICAL JOURNAL March 2006
ABSTRACT
Congenital indiff e rence to pain (CIP) is a rared i s o rder uncommonly reported in the burnliterature. Patients with this disorder are known tomanifest with a complete absence of pain, thoughother sensations and mental development areunaffected. We report two sisters, who suffer fromthis disorder to highlight their fre q u e n tinvolvement with burns and trauma resulting inmultiple scars, contractures, corneal ulcers and
opacities, oral burns, auto-amputation of fingertipsand tongue, bone fractures and joint deformities.While routine pain evaluation at birth should helpin the early recognition of this disorder, educatingthe parents, caretakers and the patients themselvesabout CIP and providing a safe and secure environ-ment will help in preventing the enormoussuffering that the families undergo in taking care ofsuch unfortunate children.
KEY WORDS: burns, congenital indifference to pain
Case Report
Burns and Congenital Indifference to Pain in Two Sisters:A Case Report
Address correspondence to:Dr Alexander George, Plastic Surgeon, Al -Babtain Center for Burns and Plastic Surgery, Ibn-Sina Hospital, Post Box No, 2542, Safat 13115,Kuwait. Fax: +(965) 4811784, E-Mail: [email protected]
Kuwait Medical Journal 2006, 38 (1): 40-42
Alexander George, Ibrahim Ghoneim, Mohammed Khalaf IbrahimAl-Babtain Center for Burns and Plastic Surgery, Ibn Sina Hospital, Kuwait
INTRODUCTION Congenital indiff e rence to pain (CIP) is an
unique disorder characterized by absence fro mbirth of pain perception, universal lack of responseto noxious stimuli, normal sensitivity to othermodalities, normal myotactic responses andnormal mental development[1]. While CIP may beeither autosomal recessive or dominant, fewassociated features have been reported: primarym y o p a t h y, relative anosmia, chro m o s o m a labnormalities, hypomyelination of subcallosalfasciculus and thalamic gliosis[2]. Though patientswith CIP frequently suffer burns, they have rarelybeen reported in the English burn literature. Wepresent two sisters with CIP in view of its rarity aswell as to highlight their frequent encounter withburns and trauma and discuss the management.
CASE REPORTPatient 1: AH, a six-year-old girl, was the first childof consanguineous parents. Besides her sister, hermaternal cousin also suffered from CIP. She wasfirst thought of being abnormal at the age of sixmonths, when she did not show any reaction topain following hot iron burns to her thigh. A deepsecond-degree burn resulted, which healed withresidual scarring and hypopigmentation. At the ageof one and half years she had a fall, which resultedin fracture of nasal bones and a deformed nose. At
age three years, she developed keratitis and cornealulceration, which healed with corneal opacification.She also had osteoarthritis of the left knee joint atthe age of four years, which resulted in ashortening of the left lower limb and an abnormalgait. During her lifetime she suffered numerousepisodes of oral burns and accidental tongue bitesand tip auto-amputation which resulted in ascarred buccal mucosa and tongue along with lossof dentition. She frequently suffered from burnsand trauma to the hands, which resulted in scarsand fingertip shortening. She did well at school,appeared to be of normal intelligence and did nothave any thermoregulatory problems. Neurologicalexamination revealed presence of all sensationsexcept response to noxious stimuli. Pain wasidentified as a sensation of touch. Orthostatichypotension was not detected and sweatingpattern was normal. Routine blood tests, urineanalysis, liver function test, renal function test,ultrasonography of the abdomen, electro m y o -graphy and nerve conduction studies were foundto be normal. The parents did not agree for a suralnerve biopsy.
Patient 2: SH, a four-year-old girl, the youngersister of AH, was first thought to be suffering fromCIP when she showed no response to needle pricksduring immunization. Since the first born had CIP,the parents were vigilant and immediately took SH

KUWAIT MEDICAL JOURNAL 41March 2006
for a neurological evaluation to confirm CIP. As atoddler she suffered contact burns to both hands inthe kitchen which healed with contractures of bothindex fingers. Exposure keratitis and re p e a t e dtrauma resulted in bilateral corneal opacities. At theage of three years, she had painless fractures of theright second and third metatarsal. At age of threeand half years, she was diagnosed as an asthmatic.In addition, she had repeated episodes of burns andtrauma to the oral mucosa and tongue with loss ofdentition. She appeared to be of normal intelligenceand did not have orthostatic hypotension. Hersweating pattern was normal and thermo-regulatory problems were not detected. Generalexamination revealed multiple post burn scars overboth upper limbs with irregular fingertips andbilateral index finger contractures. Neurologicalexamination showed presence of all sensationsexcept response to pain. Routine blood tests, urineanalysis, liver function test, renal function tests,ultrasonography of the abdomen, electro m y o -graphy and nerve conduction studies were foundto be normal. The parents refused consent for asural nerve biopsy.
DISCUSSIONPain is a protective phenomenon and since the
origin of life, it has helped organisms escape injury,destruction and death. In the absence of pain, livingcreatures become victims rather than masters oftheir environment, since the very recognition ofdanger is lost. Absence of pain may occur in avariety of disorders: CIP, congenital insensitivity topain, Asymbolia for pain, Swanson’s syndrome,Riely Day’s syndrome, Lesch Nyhan’s syndromeand peripheral neuropathies[3]. The exact etiology ofC I P is still unknown. Though the peripheralnervous system is thought to be unaffected andmorphometric studies by Landrieu et al, did notshow any abnormality, Dyck et al found a reductionin small myelinated fibers and unmyelinated fibersin these patients and suggested that CIP was avariety of hereditary sensory and autonomicneuropathy (HSAN)[1,4]. Congenital indifference topain is often confused to congenital insensitivity topain, where in addition to pain, other sensorymodalities are also affected along with autonomicdysfunction, mental re t a rdation and detectabledefects of sensory pathways[1,5]. As autopsy doesnot show any abnormality and skin and nervebiopsies appear normal, a dysfunction of theendomorphinic systems has been suggested[ 6 ].Fabbri et al injected cerebrospinal fluid from apatient with CIP in the intracerebral ventricularregion of a rat and observed that it inducedanalgesia. They suggested that hyperactive opiatemechanisms might be responsible for CIP[ 7 ]. In
addition to a reduction in the expression of thenatural killer cells, plasma beta - endorphin (beta -E) levels in two patients with CIP were found to besignificantly higher than controls[8]. These eventswere thought to represent the possible role of theneuroendocrinal feedback mechanism in exposingCIP patients to increased skin infection.
CIP patients form a unique group of patientswho are functionally handicapped because of theabsence of pain. Burns and trauma are thecommonest cause of injury, from which they suffermostly in infancy and childhood. Hand burns andoral burns are most frequent. Recurrent trauma andexposure keratitis result in corneal opacities. Lossof dentitions and autoamputation of tips of fingersand tongue occur from unrecognized trauma andburns. Bone fractures and neuropathic arthro p a t h i e sresult in deformities and gait disturbances. CIPpatients perceive pain but recognize it as non-painful as a touch or a tickle and hence thesepatients can learn to take precautions so thattrophic changes and arthropathy are less commonthan in the sensory neuropathies[9]. CIP patientsneed to be identified from birth to prevent injuryand routine pain evaluation at birth should help inthe early identification of these children. In regionssuch as the Middle East where summertemperatures can reach very high levels, contactburns can occur fre q u e n t l y. Children with CIPshould not be allowed to come in contact with sunexposed objects and footwear should always beworn to prevent pavement burns. Tap water burnsfrom hot water is another source of scald burns andhence the need to have a temperature regulatorinstalled. As with all children, these patients shouldespecially be kept away from cigarettes, pipes,ashtrays, matches, lighters, domestic cleaners,acids, ironing appliances, heaters, electric wires andsockets, as well as all scalding liquids like hotsoups, tea and coffee. By providing a safe andsecure environment, it will be possible to preventfrequent burns and trauma. Moreover, educatingparents, care givers and patients themselves will goa long way in reducing the suffering of theseunfortunate victims of CIP.
The parents of our patients were educated andvery well oriented about CIP since the maternalcousin was the first individual in the family tosuffer from CIP. When they realized that their firstchild suffered from the same condition, they wereextra-vigilant and took special precautions to avoidburns and trauma in their offspring. As infants andtoddlers, the sisters were never left unattended. Aschildren, they were advised to stay away from allhot objects and games likely to cause burns ortrauma. Water temperature was always checkedmanually by a parent before bathing the children.

Burns and Congenital Indifference to Pain in Two Sisters: A Case Report March 200642
S i m i l a r l y, they were banned from entering thekitchen by fixing a child-door that could be openedonly by an adult. Further, food that was broughtout of the kitchen was always at a safe temperature.As daytime visits to the beach or park were foundto cause sunburns to the face and exposed parts ofthe body, the children were taken there only atnight or during the winter season. Routine use ofs u n s c reens helped to reduce the incidence ofsunburns. Likewise, since playing barefoot oncemented blocks or pavements in the hot summerseason led to frequent burns of the feet, the childrenwere strictly advised to wear protective footwear atall times outside the house. This case re p o r thighlights the fact that with intelligent caring,parents and caretakers can significantly reduce theincidence of burns and trauma in children with CIPthereby improving their quality of life.
REFERENCES
1: Landrieu P, Said G, Allaire C. Dominantly transmittedcongenital indifference to pain. Ann Neurol 1990; 27: 574-
578.2: Davis BJ, Reed LA, Schelper RL. A unique autosomal
dominant disorder with indiff e rence to pain:clinicopathologic correlation of indifference to pain andthalamic gliosis. Eur Neurol 1998; 40:141-145.
3: Biswal N, Sundaram VM, Mathai B, Balasubramanian S.Congenital indifference to pain. Indian J Pediatr 1998;65:755-757.
4: Dyck PJ, Mellinger JF, Reagan TJ, et al . Not indifference topain but varieties of hereditary sensory and autonomicneuropathy. Brain 1983; 106:373-390.
5: Aslan D, Sarikayalar F. Congenital insensitivity to pain withanhydrosis. Cutis 1997; 60:188-190.
6: Serratrice G. Congenital indiff e rence and congenitalinsensitivity to pain. [French]. Bull Acad Natl Med 1992;176:609-616.
7: Fabbri A, Fraioli F, Cruccu G, Manfredi M, Pert CB, Pert A.I n t r a c e re b roventricular injection of cere b rospinal fluid(CSF) from a patient with congenital indifference to paininduces analgesia in rats. Experientia 1984; 40:1365-1366.
8: B e r n a rdini R, Tine A, Mauceri G, Mazzarino MC,Malaponte G, Nicosia A, Parano E, Fiumara A. Plasma beta-endorphin levels and natural-killer cells in two cases ofcongenital indifference to pain. Childs Nerv Syst 1992; 8:83-85.
9: Bundey S. In: Genetics and Neurology. 2nd Ed. Edinburgh:Churchill Livingstone, 1993, p294.

KUWAIT MEDICAL JOURNALMarch 2006
ABSTRACT
This case report describes the occurrence of transientcentral diabetes insipidus (CDI) in a young female whopresented with thrombotic thrombocytopenic purpura(TTP) and ectopic pregnancy. CDI developed four daysafter termination of ectopic pregnancy and after initialresponse to desmopressin (dDAVP) nasal spray, she onlyfully re c o v e red after reversal of TTP with plasmaphere s i s .
The association of CDI with TTP is very rare and only asingle case report exists in the literature. However, it isknown that TTP can induce ischemic micro v a s c u l a rchanges in neurohypophyseal axis leading to CDI. Isthere a possible causal role for ectopic pregnancy? Weattempt to answer this question.
KEYWORDS: central diabetes insipidus, diabetes insipidus, pregnancy, thrombotic thrombocytopenic purpura
Case Report
Transient Central Diabetes Insipidus in a Female Patientwith Thrombotic Thrombocytopenic Purpura and Ectopic
Pregnancy: A Possible Link
Address correspondence to:Tarek Abdel Hamed Mostafa Dowod, P.O 47854, Fahaheel-Kuwait. Tel: 009656052897- 009653718245, E-mail:[email protected]
Kuwait Medical Journal 2006, 38 (1): 43-45
Tarek Abdel Hamed Mostafa Dowod, Ashraf HashemDepartment of Medicine, Al-Adan Hospital, Kuwait
INTRODUCTIONBoth Central diabetes insipidus (CDI) and
T h rombotic thrombocytopenic purpura ( T T P )independently are uncommon diseases. Expectedly,the association of CDI with TTP is extremely rare.Only one case report of CDI complicating TTPexists in English literature[ 1 ]. TTP is a life-threatening episodic multisystem disease that ischaracterized by formation of microthrombi in them i c ro c i rculation (capillaries and arterioles) ofseveral organs. Clinical presentation typicallyconsists of a pentad of (a) micro a n g i o p a t h i chemolytic anemia, (b) t h rombocytopenic purpura,(c) variable neuro l o g i c a l m a n i f e s t a t i o n sunaccompanied by objective evidence ofneurological deficit, (d) renal function compromiseand (e) fever [2]. Although the complete pentad maynot always manifest at presentation, neurologicalf e a t u res constitute an important diagnosticcomponent[3, 4].
Diabetes insipidus may be central (ADH-sensitive) or nephrogenic (ADH-resistant). Centraldiabetes insipidus (CDI) is a temporary or chronicdisorder of the neurohypophyseal system due todeficiency of vasopressin (ADH) and characterizedby excretion of excessive quantity of very dilute butotherwise normal urine. CDI may be primary orsecondary and is caused be a variety of pathologiclesions including vascular lesions such asaneurysm and thrombosis[5].
Our case suggests that CDI can also be includedas one of the many varied neurological features ofTTP. Paucity of its description in the literaturemerits its presentation here.
CASE REPORTA 32 - year old female, mother of five children
presented with a four-day history of fever, exhau-stion, lower abdominal pain and wide spre a dpurpuric spots over both legs and upper trunk. Shehad amenorrhea for the last two weeks.
On examination, she looked quite sick, wasfebrile (temperature 38.5 0C) mentally confused anddisoriented. She had obvious pallor, was jaundicedwith purpuric spots over both legs and uppertrunk. There was marked tenderness in the rightiliac fossa. The cardio-respiratory and neurologicalsystems were normal.
Investigations: CBC: Hb = 4 g/dL, MCV = 80.4fl, MCH = 29.1 pg , WBC 5.4 x 109/L, and plateletcount = 8 x 109/L. Blood smear showed numerousfragmented RBCs (schistocytes), marked poly-chromasia and several normoblast (8/100 WBC)with a high reticulocyte count (30%). Thesefindings along with markedly raised LDH (2990iu/L) provided the basis for diagnosis of TTP.G6PD screen and assay showed normal values.Direct and indirect antiglobulin tests were nega-tive.

Transient Central Diabetes Insipidus in a Female Patient with Thrombotic .... March 200644
Biochemical profile: S. urea = 4.5 mmol/L, S.creatinine = 53 umol/L, S. total bilirubin = 56umol/L (direct = 5 umol/L). Other biochemicalfindings such as plasma glucose, seru melectrolytes, hepatic enzymes, serum lipids, serumcalcium, phosphate and A L P w e re normal.Coagulation profile: prothrombin time (11.3 sec,control = 10.8 sec), activated partial thromboplastintime (32.2 sec, control = 31.1 sec), plasma fibrinogen(3.1 g/L) and fibrinogen degradation product (< 10mg/L) were normal. Pregnancy test foramenorrhea was postive. Raised serum HCG levelof 325 mIU/ml was confirmatory. Transvaginalultrasound showed right tubal pregnancy with al a rge peritubal hematoma. Serum antidiur e t i chormone level was low normal < 1.8 pmol/L(normal < 7.4 pmol/L). CT scan of the brainshowed no abnormality.
MANAGEMENTActively bleeding tubal pregnancy complicated
by severe anemia (Hb = 4gm/dL) and severethrombocytopenia (platelet count = 8000/cumm)posed a life-threatening situation requiring urgentsurgical intervention. Emergency evacuation of thetubal pregnancy was inevitable. Fortunately, thiscould be performed uneventfully under cover ofjudicious intraoperative minimal platelettransfusion and perioperative blood transfusion.
For TTP, the patient was initially given cryo-depleted plasma followed by aggre s s i v ep l a s m a p h e resis. Daily plasmapheresis with 1.8volume replacement with cryo-depleted plasmawas carried out. Initially, for a week neither plateletcount nor serum LDH (remaining > 3000 iu/L)showed any signs of recovery. Intravenous methylpredinsolone (1 gm/day for 3 days) was addedwhile plasmapheresis was continued on a dailybasis. Only after 21 sessions, was somei m p rovement noticeable, and it re q u i red 35sessions of plasmapheresis for full recovery.
On the 5th day of admission, the patientdeveloped marked diuresis with 24-hour urineoutput of 5-9 liter/day and this continued for 11days. Urine specific gravity was recorded as 1010and osmolality as 100 mosm/kg water. Seru mosmolality was 287 mosm/kg water.
Due to the patient’s critical condition, waterdeprivation test was not performed. Pituitary MRIdid not show any abnormality. The patient wasgiven dDAVP nasal spray (20 unit twice daily) towhich she showed a good response with completerecovery from diuresis in six days. Urine specificgravity (1023) , urine osmolality (350 mOsm/kgwater) and serum osmolality (275 mOsm/kg)returned to values within the normal referencerange.
DISCUSSIONExcept for renal functional compromise, all the
pentad features of TTP, i.e., fever, microangiopathichemolytic anemia, thrombocytopenic purpura,neurological findings of variable confusion anddisorientation were present. With support fromhighly raised LDH values the diagnosis wasobvious and made promptly. Most likely it couldhave been precipitated by pregnancy which isreportedly associated with 10-25% cases of TTP[2].TTP that is associated with pregnancy presentsb e f o re 24 weeks of gestation and may not beaffected by its termination[6]. Oral contraceptives,which our patient also had been using, are believedto contribute to TTP[7]. Occurrence of CDI in ourpatient appears to be unique as only one earlierreport of its association with TTP exists in theliterature[1]. Suddenly occurring diuresis with hypo-osmolar urine and concentrated hypero s m o l a rplasma at the point of diuresis along with itscomplete reversal with dDAVP therapy providedthe basis for its diagnosis[8]. This is supported by thelow serum ADH level.
CDI has been described to occur in pregnancy[9]
and its transient episodes have been described withincreasing frequency[10]. In the six cases reported byHamai et al [11], CDI in pregnancy was associatedwith raised hepatic enzymes and hypertensionsuggesting its possible relationship with eclampsiaand chronic liver disease.
In our patient, CDI does not appear to be relatedto pregnancy, as it was observed during very earlypregnancy, liver enzymes were normal and thepatient did not have hypertension. On the otherhand, we believe that CDI in our patient had acausal relationship with TTP.
CDI is characterized by reduced secretion ofa n t i d i u retic hormone (ADH) also known asArginine vasopressin[12]. All the pathologic lesionsassociated with CDI involve the supraoptic andparaventricular nuclei of the hypothalamus or amajor portion of the pituitary stalk. Simpledestruction of the posterior lobe of the pituitaryleads to temporary unsustained diabetesinsipidus[5].
Although CDI is not described as a text bookfeature of TTP, the possibility of its occurrence canfind justification in mirothrombus related ischemicchanges that we often observed in neuro h y -pophyseal axis induced by TTP[13]. The transientnature of CDI in our case reflects the fleetingn e u rological manifestations of TTP related tofluctuating ischemic changes brought about bymicrothrombi in TTP.

KUWAIT MEDICAL JOURNAL 45March 2006
CONCLUSIONWe suggest that transient central diabetes
insipidus should be included among the variableneurological manifestations of TTP. Its awarenessmay result in more frequent observation and timelyhelp with dDAV P, thereby thwarting acutecomplications of severe diabetes insipidus.Although the causal relationship between TTP andCDI emerges strongly in the present case, thepossible role of pregnancy in this case cannot beunequivocally excluded.
REFERENCES
1. Vanslyck EJ, Jurgensen JC, and Cargill JW. Diabetesinsipidus complicating thrombotic thro m b o c y t o p e n i cpurpura. JAMA1969; 209:768 -770.
2. Elliott MA, Nicholas WL. Thrombotic thrombocytopenicpurpura and hemolytic uraemic syndrome. Mayo Clin Proc2001; 76:1154 -1162.
3. George JN, Gilcher RO, Smith JW, Chandler L, Duvall D,Ellis C. Thrombotic thrombocytopenic purpura - Hemolytic
uraemic syndrome: Diagnosis and Mana-gement. J ClinApheresis 1998; 13:120 -125.
4. Saleem S, Saleem A. Thrombotic thro m b o c y t o p e n i cpurpura: A brief review of recent literature. Tex Med 1989;85:46 -49.
5. Nicholas J. Posterior lobe disorders:Diabetes Insipidus. In:Merck Manual 17th ed. Merck Research Laboratories 1999,p 78-80.
6. Ezra Y, Rose M, Elder A. Therapy and prevention ofthrombotic thrombocytopenic purpura during pregnancy:clinical study of 16 pregnancies. Am J Hematol 1996; 51:1-6.
7. Mc shane PM, Bern MM, Schiff J. Thrombotic thrombo-cytopenic purpura associated with oral contraceptive: Acase report. Am J Obstet Gynecol 1983; 145:762 -763.
8. Michael Cooperman. Diabetes Insipidus. eMedicine online2003 ; 7:1 -10.
9. Durv JA. Diabetes Insipidus in pregnancy. Am J Kidney Dis1987; 9:276 -283.
10. Krege J, Katz VL, Bowes WA Jr. Transient diabetes insipidusof pregnancy. Obstet Gynecol Surv 1989; 44:789 -795.
11. Hamai Y, Fujii T, Nishina H, Kozuma S, Yo s h i k a w a ,TaketaniY. Differential clinical courses of pregnancy com-plicated by diabetes insipidus, which does, or does not, pre-date the pregnancy. Hum Reprod 1997; 12:1816 -1818.

KUWAIT MEDICAL JOURNAL March 2006
ABSTRACT
Two full-term intrauterine growth retarded babiespresented at 8 and 12 hours of age with respiratorydistress and severe mixed acidosis. Both cases wereventilated and received intravenous sodiumbicarbonate due to ignorance of initial seru msodium (S. Na+) level. Within one and a half andthree hours of birth respectively, they developed
severe hypernatremia (S. Na+ 176 and 187 mmol /L) and severe intraventricular hemorrh a g efollowed by cerebral palsy in case 1, and death incase 2. None was breastfed and none received extrasodium prior to admission to the neonatal unit.The etiology and possible prevention are discussed.
KEYWORDS: cerebral palsy, intraventricular hemorrhage, neonatal, hypernatremia
Case Report
Early Neonatal Hypernatremia with IntraventricularHemorrhage - An Unusual Presentation in Two Cases
Address correspondence to: Dr. Amrit LSoni, P.B No 2532, Ardiya 92400, Kuwait. Tel/Fax: 4802940, E- mail [email protected]
Kuwait Medical Journal 2006, 38 (1): 46-48
Hussain Parappil, Amrit L Soni, Rima MZ Al-SawanDepartment of Pediatrics, Farwaniya Hospital, Kuwait
INTRODUCTIONS e v e re hypernatremia with intraventricular
h e m o r rhage (IVH) is a rare occurrence in theneonatal unit [ 1 ]. Many cases are re p o r t e dworldwide; implicating dehydration, intrauterineg rowth re t a rdation (IUGR), iatrogenic administrationof oral / intravenous (IV) sodium and high sodiumin breast milk as etiology[2-7]. We present two casesof severe hypernatremia within 12 hours of birthpresenting as respiratory distress and unrelated tobreast feeding.
CASES REPORTSCase 1
A male baby was born to a 34 year old para 5Kuwaiti mother at full term (FT) by lowersegmental cesarean section (LSCS), indicated forfetal distress. The baby was born with an apgarscore of 8 and 9 at one and six minutes, weighed 2.4kg and had a head circumference (HC) of 34 cm andlength of 48 cm. The newborn was kept with themother and fed on S-26 ready to feed formula twoh o u r l y. At the age of eight hours, the babydeveloped respiratory distress and was admitted tothe neonatal unit and was ventilated due to severemixed acidosis (pH 7.12, pCO2 9.2, BE -10.5, HCO315). Sodium bicarbonate 2 mmol/kg was givenintravenously twice in one hour for correction ofmetabolic acidosis. After half an hour, the babydeveloped seizures that were controlled with IVphenobarbitone. Head ultrasound at nine and halfhours of age showed IVH grade 3 (Fig. 1). Serum
sodium was 152 mmol/L on admission (the resultwas received late) and 176 mmol/Lat nine and halfhours. Urine sodium was very high (216 mmol /L). The baby was treated with half saline andserum sodium returned to normal by 58 hours.Ultrasound at 19 days showed hydrocephalus andCT scan showed obstructive hydrocephalus. Renal,a d renal and posterior pituitary functions werenormal (Table 1).
The baby’s general condition improved and thechild was discharged at the age of 41 days. At two-month follow up, the baby had a delayeddevelopment with arrested hydrocephalus, aweight of 4 kg, HC 41.5 cm, S. Na+ of 137 mmol/kgand CT head showing mild hydrocephalus. Followup at six months showed spastic cerebral palsy(CP), weight of 4.3 kg, length 66 cm and HC 43 cm.
Case 2A male baby boy was born to a 25 year old,
primi, Pakistani mother at full term by LSCS due tofetal distress. The baby was born with an apgarscore of 7 and 9 at one and five minutes, weighed2.45 kg with a HC 33 cm and length of 49 cm. Babywas kept with mother and fed on S-26 ready to feedformula but developed respiratory distress at theage of 12 hours. The newborn was admitted to theneonatal unit and was ventilated due to severemixed acidosis (pH 7.05, pCO2 10.5, BE -10, HCO313.8). Metabolic acidosis was treated with sodiumbicarbonate 4 mmol/kg intravenous boluses in onehour. After two hours, the baby developed seizures

KUWAIT MEDICAL JOURNAL 47March 2006
which were controlled with IV phenobarbitone.Head ultrasound at the age of 15 hours had shownIVH grade - 4. The serum sodium on admission was154 mmol/L (the result was received late) and1 8 7 m m o l / L at 16 hours. Renal, adrenal andposterior pituitary functions were normal.
The baby was treated with half normal salineand serum Na + gradually returned to normal in 65hours. Serum K+ was normal. Urine Na+ was veryhigh (218 mmol/L). Baby’s general conditiondeteriorated with hypoxia, seizures, disseminatedintravascular coagulation (DIC) and hypotension.The baby died at the age of five days.
The clinical and laboratory features of bothcases are summarized in Table 1.
DISCUSSIONIntrauterine malnutrition may cause water
depletion and predisposition to hypernatremia[1].Most reported cases are FT and have IUGR [2-7]. Bothour cases were also FT and had IUGR. Age of onsetvaries from ‘soon after birth’ to three weeks. Mostcases reported are more than a week old andexclusively breastfed[1-7]. Our cases presented veryearly (at 8 and 12 hours of age) and were notbreastfed.
Presenting features of neonatal hypernatremiaare lethargy, dehydration, fever, jaundice, apnea,oliguria, shock and seizure s[ 1 - 7 ]. Both the cases
presented with respiratory distress andmetabolic acidosis and neededventilation. In the absence of availablevalues of S.Na+, they were treated withboluses of IV sodium bicarbonate (4mmol/kg within 1 hr) which had causedserum sodium to rise to a very high level(180-190 mmol/L) and resulted in IVHgrade 3 in case 1 and grade 4 in case 2.Association of hypernatremia withmetabolic acidosis and re s p i r a t o r yd i s t ress is well re c o g n i z e d[ 8 ].Tr i s h y d ro x y - m e t h y l a m i n o - m e t h a n e(THAM) should be used for treatment ofacidosis in place of sodium bicarbonatein cases of metabolic acidosis associatedh y p e r n a t remia to avoid furtheraggravation of the critical situation.
Etiology of neonatal hypernatremiais multi-factorial; dehydration, IUGR,i a t rogenic admini-stration of oral/IVsodium, central or nephrogenic diabetesinsipidus and high sodium in bre a s tmilk are implicated[ 2 - 7 ]. Rare l ye r y t h rodermic ichthyosis may causesevere hypernatremia[9]. This was absentin our case. High urine Na+ a n d
osmolality rules out renal and central causes andindicates iatrogenic salt poisoning. Our babies werenot breastfed and bottle-feed was given few timeswith normal sodium formulas. Their initial S. Na+
was slightly higher then normal (152 and 154respectively) and could be explained by IUGR andmild dehydration. Both babies received IV sodiumbicarbonate 10 ml (4 mmol/kg) within one hour formetabolic acidosis which contributed to severehypernatremia (S. Na 176 and 187 respectively). Ifnot excreted by the kidney and distributedintravascularly, 4 mmol/kg will increase S.Na+ by40-50 mmol/L (as blood volume is 80-90 ml/kg).Any acute rise of Serum Na+ to 175 mmol/L maygive rise to IVH and DIC[10]. Our case 1 had IVHgrade 3 followed by hydrocephalus and CP andcase 2 had IVH grade 4 and DIC severe enough tocause death within five days. Seizures are acommonly reported complication ofhypernatremia, especially during management anda few cases of IVH also develop mentalretardation[11].
Treatment of hypernatremia should be gradualover 48-72 hours, in order to avoid IVH ands e i z u re s[ 1 ]. No more than half normal saline isrecommended initially[1]. We were cautious for slowreduction of S. Na during therapy. Early onset ofIVH indicates that hypernatremia was responsiblefor IVH. The most important aspect of preventionof hypernatremia is to avoid bolus doses of IV
Table 1: Comparison of clinical and laboratory features of two cases
Features Case 1 Case 2
Sex /GA/ Mode of delivery M/39 wks/LSCS M/40 wks /LSCSBirth Weight in gms/IUGR 2400/+ 2450/+ Age of presentation 8 hrs 12 hrsPresenting features RD, mixed acidosis RD, mixed acidosis Weight loss on admission 1.5% 2.1%S.Na+(mMol/L):
On admission 152 154After IV sodiumbicarbonate 176 187
Serum Potassium (mmol/L) 4.2 3.4Urine Na+ ( mmol/L) 216 218Urine specific gravity High HighS Urea (mmol/L) 5.3 4.6S Creatinine (ummol/L) 75 86S Aldosterone (pmol/L) Normal (3120) Normal (3330)Serum rennin (mu/L) Normal (1500) Normal (1800)Serum 17-OH-progsgestrone Normal (6.8 mmol) Normal (6.5 mmol)S-26 ready to feed Sodium level 27 mmol/L(Normal) 27 mmol/L(Normal)Fall of sodium to 144 mmol/Lin 58 hrs 141 mmol/Lin 65 hrsAbdomen ultrasound Normal NormalComplications IVH grade 3 bilateral IVH grade 4 bilateral
at age 9 1/2 hours at age 15 hoursFollow- up Spastic CPat 6 months, and Died at 5 days of age
arrested hydrocephalus.
RD= respiratory distress, GA = gestational age, IUGR = intrauterine growth retardation,LSCS= lower segment cesarian section, IVH = intraventricular hemorrhage, CP = cerebralpalsy

Early Neonatal Hypernatremia with Intraventricular Hemorrhage - An Unusual Presentation..... March 200648
sodium bicarbonate or to use THAM for correctionof acidosis. (1 mmol/kg of sodium bicarbonate canincrease sodium level by10 mmol/L). Ventilatedbabies do not need sodium bicarbonate unless pHis persistently below 7.2.
CONCLUSIONNeonatal hypernatremia can manifest as
respiratory distress due to metabolic acidosis at anearly age. Therefore, serum sodium level should bedone in such cases. Boluses of IV sodiumbicarbonate should be avoided for the treatment ofmetabolic acidosis in order to prevent iatrogenichypernatremia and IVH. THAM is indicated forc o r rection of metabolic acidosis with hyperna-tremia.
Fig. 1: Showing IVH grade 3 in case 1 at 91/ hours of age
REFERENCES
1. Bajpai A, Aggarwal R, Deodari AK, Paul VK. Neonatalhypernatremia due to high breast milk sodium. IndianPediatrics 2002; 39:193-196.
2. Scott JX, Regunath, Gnananayagam JE, Simon RE. Neonatalhypernatremic dehydration and malnutrition associatedwith inadequate breastfeeding and elevated bre a s t m i l ksodium. J Indian Med Assoc 2003; 101:318-321.
3. Roddey OF, Martin ES, Swetenburg RL, Critcal weight lossand malnutrition in breast fed infants. Am J Dis Child 1989;135:579-599.
4. Rowland TW, Lafleur WR, Malnutrition and hypernatremicdehydration in breastfeed infants. JAMA 1982; 247:1016-1017.
5. Arboit JM, Gildengers E. Breast feeding and hypernatremia.J Pediatr 1989; 97:335-336.
6. Ghisnan FK, Roloff JS, Malnutrition and hypernatremicdehydration in two breast feed infants. Clin Pediatr 1983;22:592-594.
7. Thullen DJ. Management of hypernatremic dehydrationdue to insufficient lactation. Clin Pediatr 1988; 27:370-372.
8. Robson AM. Parental fluid therapy. In: Behrman RE,Klugman RM, Nelson WE, Vaughan III VC, editors. TextBook of Pediatrics, 15th ed. 1992, p 210.
9. Stoll C, Alembik Y, Tchomakov D,Messer J, Heid E, BoehmN, Calvas I Hovnanian A. Severe hypernatremic dehy-dration in an infant with Netherton syndrome. GenetCouns 2001; 12:237-243.
10. Korkz A, Yigit S, Firat M, Oran O. Cranial MRI in neonatalhypernatremic dehydration. Pediatr Radiol 2000; 30:323-325.
11. Roberton NR, Howat P. Hypernatremia as a cause ofintracranial hemorrhage. Arch Dis Child 1975; 50:938-942.
2

KUWAIT MEDICAL JOURNALMarch 2006
ABSTRACTCaffey Silverman disease is a rare self-limiting disease ofearly infancy. Diagnosis is difficult as it can mimic a widerange of orthopedic problems ranging from traumaticdisorders, bone infections, hypervitaminosis A, scurvyand even primary or metastatic bone disease. Theemphasis on a high index of suspicion avoids unne-cessary surgical or radiological interventions. This is acase report of a 25-days-old infant who presented with a
rapidly growing mass of the left collar bone. Another leftscapular swelling appeared during the course of thefollow-up. Spontaneous and complete resolution of themasses was the final outcome, but only after a period ofeight months. The pitfalls and clues for the diagnosis areoutlined. The final functional and radiological outcomesafter one year of follow-up were excellent.
KEY WORDS: Caffey’s disease, infantile cortical hyperostosis
Case Report
Caffey Silverman Disease: Case Report and LiteratureReview
Address correspondence to:Mohamed AL Fahmy, FRCSEd, Specialist orthopedic surgeon, Al-Razi Orthopedic Hospital, P.O. Box 4235, Safat code 13043, Kuwait. Tel: 965-4846000-Ext.2565, Fax: 965-4844240, E-mail [email protected]
Kuwait Medical Journal 2006, 38 (1): 49-52
Mohamed A Lotfy Fahmy Al-Razi Orthopedic Hospital, Sulaibhikhat, Kuwait
INTRODUCTIONCaffey Silverman disease, otherwise known as
infantile cortical hyperostosis, is a self limitingdisease of early infancy and is characterized by atriad of soft tissue swelling, cortical thickening ofthe underlying bone and hyperirritability.
This is a report of an infant who presented withl a rge swellings affecting the left clavicle andscapula. Spontaneous and complete resolution ofthese masses was the final outcome but only after aperiod of eight months.
Case presentationA twenty-five-days old Kuwaiti male infant
presented with fullness of the left supraclavicularregion and swelling of the left collar bone noticedby the mother two days back (Fig. 1). She alsonoticed that her baby was crying and irritable andwas not moving the affected left upper limb asfreely as the right side. She did not recall anyhistory of trauma or fever. He was born full term,was the product of a normal and uncomplicatedvaginal delivery and he was only breast fedthroughout the postnatal period. Family historywas negative with no members affected withsimilar conditions. His three siblings were normal.
Clinical examination showed an irritable baby,afebrile, and had a uniform swelling of entire of leftclavicle. It was not tender, firm in consistency andthe overlying skin appeared normal.
Radiological examination showed hypertrophiccallus formation of the left clavicle. The initialdiagnosis was healing fracture clavicle withexcessive callus formation (birth injury).
As the swelling was getting larger, the motherreturned to the hospital four days later and wasadmitted with the diagnosis of a mass of the leftclavicle for investigation.
At admission:The blood test showed an elevated ESR of 120
mm, C-reactive protein of 73 mg/L, WBC count of13 x 109/L with predominant lymphocytosis. Hissickling test was negative and the alkalinephosphatase reported on two separate occasionswas within normal range. His temperature over thefollowing days ranged from being afebrile to 37.9 0 C .
Differential diagnosis was a healing fracture ofthe left clavicle with excessive callus formation,acute osteomyelitis of the left clavicle or the possi-bility of Caffey Silverman disease.
A CT scan was arranged which showed uniformbone expansion of the left clavicle and scapula,cortical thickening and periosteal reaction withnon-enhancing soft tissue mass noticed more on thescapula anteriorly (Fig. 2 and 3).
Over the following weeks, the scapular swellingappeared clinically and reached an enormous size(Fig. 4). Spontaneous and complete resolution ofthese masses was the final outcome but only after aperiod of eight months. Review after a lapse of oneyear showed no evidence of recurrence.

Caffey Silverman Disease: Case Report and Literature Review March 200650
DISCUSSIONInfantile cortical hyperostosis is a self-limiting
disease of early infancy that is characterized by atriad of soft tissues swelling, cortical thickening ofthe underlying bone, and hyperirritability. In 1945,Caffey and Silverman described earlier this diseaseentity[1]. Similar cases have been described by Roskein 1930 and Ellis in 1938. The condition is describedas being rare with no sex or racial predilection[2].
Etiology:The cause of infantile cortical hyperostosis is
unknown. There seems to be two subtypes, thefamilial type and the spontaneous type. Theincidence is reported to be 3/1000; there is aworldwide decrease in the number of cases in thepast two decades particularly in the non familialsubtype[3,4]. Reports of familial occurrence suggestsa possible hereditary defect of the arterioles of theperiosteum, but it has been difficult to establish themode of inheritance[5].
Infection as a cause has been proposed by othersbecause of the acute inflammatory findings, butisolation of bacteria or viruses has been failed andserological tests for infection have been negative[5].Because of the response of the disease tocorticosteroids and the precipitation of symptomswith dietary changes, an allergic basis also has beenpostulated[6].
Clinical features:The mandible is the most commonly affected
site. In the limbs, the ulna is most commonlyaffected. Next in frequency are the tibiae, clavicle,scapula and ribs. The humerus, femur, fibula areless frequently affected. Occasionally, the hypero s t o s i saffects the frontal and parietal bones, the ilium andmetatarsals[4]. Involvement of neither the phalangesnor the vertebrae has been reported. Affection ofmore than one bone is common and, if involvementis bilateral, it is often asymmetrical. In this case,there was no affection of mandible or skull bones;
there was ipsilateral affection of the left clavicle andthe scapula.
Onset of the disease is often around the 9thweek of postnatal life (in this case it was around the4th week). It may however, be present at birth andhas been demonstrated in the utero as early as the24 weeks of gestation. It rarely occurs after the 5thmonth of postnatal life [2].
Numerous complications have been reported inthe literature: synostosis between the ulna and theradius, tibia and fibula, or ribs, persistent faciala s y m m e t r y, anterior tibio-femoral bowing, leglength discrepancy, pleural effusion, diaphragmaticparalysis, exophthalmos and Erb’s palsy [8].
The commonest clinical manifestations arehyperirritability and the presence of a local mass,often over the mandible. There is however, noincrease of local heat or redness. Moderate fever isf requently present in the early stages. Highsedimentation rate is present, there is elevateds e rum alkaline phosphatase and anemia is notuncommon. In this case, the alkaline phosphatasewas normal on two occasions.
Radiographic features:The characteristic feature is the formation of
abundant new bone by the periosteum with
Fig. 1. Initial X-ray at presentation
Fig. 3. CT scan films of the left clavicle and scapula
Fig. 2 CT scan films of the left clavicle and scapula

KUWAIT MEDICAL JOURNAL 51March 2006
enlargement of the diameter of the affected bone(Fig. 5). In the long bones, hyperostosis is confinedto the diaphysis. The epiphysis and the metaphysisare not involved. In the early stages the surface ofthe affected bone is coarse and the underlyingcortex is still visible. As the disease progresses thenew bone becomes more homogenous with thecortex. At the time overlying soft tissue swellingwill be visible. Several months sometimes years arerequired for resolution to be complete (Fig. 6). Laterecurrences have been reported in the literature[9].
DIAGNOSISIn the differential diagnosis one should consider
osteomyelitis, syphilis, scurvy, hypervitaminosis A,trauma, Ewing sarcoma and metastatic tumor liken e u roblastoma. Mandibular swelling could bemistaken for parotitis.
The diagnostic features of the disease arespecific:1. Narrow age group i.e., between birth and 5
months.2. The triad of irritability, swelling, and bone
lesions.3. Mandibular involvement if present strongly
suggests diagnosis.
4. Though the elevated sedimentation rate and C reactive protein with leucocytosis may point to infection, the rapid onset of the swelling with almost absence of local tenderness, redness in association of radiological massive bone formation in a short period of time excludes acute osteomyelitis. Other serological tests aid in diagnosis in cases of doubt for e.g., syphilis.
5. Though the mandibular involvement is almost always present in Caffey’s disease there arereports of clavicular and scapular involvement without mandibular involvement.
6. Hypervitaminosis A was excluded as the infant was only breast fed without any other source ofsupplementary feeding. It also occurs in children above one year of age. Scurvy also occurs in infants above one year of age. Measurement of serum levels of vitamin A or C could be done in cases of doubt.
7. Tumors are excluded in this case because of therapid onset of symptoms and the swelling (days rather than weeks). The affection of more than one bone strongly suggested Caffey’s disease. Biopsy of the lesions is not indicated unless there are other reasons to suggest malignancy.
8. Trauma was excluded because of the more thanone bone involvement, uncomplicated delivery,the excessive nature of the callus seen on X-ray without evidence of a fracture.
TREATMENTThere is no specific treatment for this disease
entity. The disease is self- limiting and completerecovery within six to nine months is the rule. Thisinfant has recovered completely after eight monthsof follow up with full remodeling of the affectedbones (Fig. 6). There is no need for antibiotics,biopsies or other surgical interventions. Caffey hasrecommended the use of steroids for alleviatingsymptoms[10] but this is now not indicated except fors e v e re cases with extensive involvement and
Fig. 4. Clinical appearance of the swellings of the left shoulder (maximalsize)
Fig. 5. X-ray of affected clavicle and scapula two months after diseaseonset
Fig. 6. X-ray of the affected bones after remodeling eight months from thedisease onset

Caffey Silverman Disease: Case Report and Literature Review March 200652
recurrence. A Caffey’s disease like syndrome ofcortical hyperostosis and periostitis has beendescribed in patients receiving prostaglandins E1or E2 therapy, particularly in infants treated forpatent ductus arteriosus. This has raised thepossibility of the therapeutic role for PE inhibitorsin treating symptoms and shortening course ofCaffey’s disease[11]. This infant received ibuprofen200 mg syrup three times daily during the acutestages of disease.
CONCLUSIONIt is important to highlight this disease entity to
avoid unnecessary invasive investigations speciallysince the diagnosis of this case needs a high indexof suspicion and it necessitates no more thanobservation and simple treatment methods. Longterm follow- up would be wise as late recurrencesare reported in the literature. In this case there wasno recurrence up to thirteen months of follow up.
REFERENCES
1. C a ffey J, Silverman W. Infantile cortical hypero s t o s i s .Preliminary report in a new syndrome. AJR 1945; 54:1.
2. Tachdjian M. In: Pediatric orthopedics. 2nd ed. W. B.Saunders company; 1990, vol. 2, p 817 - 824.
3. Cayler GC, Peterson CA. Infantile cortical hyperostosis -Report of 17 cases. Am J Dis Child 1956; 91:119 -125.
4. Harris VI, Ramilo J. Caffey’s disease: A case originating inthe first metatarsal bone and review of a 12 yearsexperience. Am J Roentgenol 1978; 130: 335-337.
5. Sidbury JB Jr, Sidbury JB. Infantile cortical hyperostosis. Aninquiry into the etiology and pathogenesis. N Engl J Med1954; 250:309.
6. Bowman JG, Piston RE, Meeks EA. Further observations onthe etiology of infantile cortical hyperostosis. Ann Allergy1961; 19:1154.
7. Jackson DR, Lyne ED. Infantile cortical hyperostosis, Casereport. JBJS 1979; 61:770.
8. Holtzman D. Infantile cortical hyperostosis of the scapulapresenting as an ipsilateral Erb’s palsy. J Pediatr 1972;81:785.
9. Swerdloff BA, Ozonoff MB, Gyepes MT. Late recurrence ofinfantile cortical hyperostosis (Caffey’s disease). AJR 1970;108:461.
10. Caffey J. Pediatric X-ray Diagnosis. 5th ed. Chicago, YearBook, 1967.
11. Thometz JG, DiRaimondo CA. A case of recurrent Caffey’sdisease treated with naproxen. Clin Orthop 1996; 323:304 -309.

KUWAIT MEDICAL JOURNALMarch 2006
ABSTRACT
C l a s s i c a l l y, Guillain-Barre’ syndrome (GBS) ischaracterised clinically by a rapidly progressingbilateral ascending paralysis and areflexia. GBS isprecipitated by a variety of infective agents. It issometimes complicated by autonomic neuropathythat may produce hypotension and troublesomea r rhythmias. It usually re g resses completely orwith minimal neurological sequelae. Romano-Ward syndrome is a rare clinical entity. Inthis syndrome, there are episodes of palpitations,dizziness, syncope or sudden death as a result of
a r rhythmias associated with a prolonged QT-interval on the electrocardiogram. Guillain-Barr’e syndrome occurring in a patientwith Romano-Ward syndrome, to our knowledge,has not been reported before. In this report, wepresent and discuss a case of Guillain-Barre’ syn-drome in a patient with Romano-Ward syndrome.The management of such a case is expected to bedifficult as both syndromes can lead to dangerousarrhythmias.
KEYWORDS: autonomic neuropathy, Guillain-Barre’ syndrome, malignant long QT-interval, Romano-Ward syndrome
Case Report
Guillain-Barré Syndrome in a Patient with Romano-WardSyndrome: a Case Report
Address correspondence to:Dr. Thomas Vurgese, P.O. 62276, Jahra, Kuwait 02153. Tel: 5640487, Fax; 4575201, E-mail: [email protected]
Kuwait Medical Journal 2006, 38 (1): 53-55
Thomas Vurgese, Osman Abdulwahab Mapkar, Soondal Kumar SurrunDepartment of Medicine, Al-Jahra Hospital, Kuwait
INTRODUCTIONG u i l l a i n - B a r re’ syndrome (GBS) is clinically
characterised by an acute, rapidly pro g re s s i v e ,symmetrical weakness, associated with areflexia. Itis a polyneuropathy that is mediated by anautoimmune response[1-5]. The disease may progressand involve the phrenic nerves causing respiratoryembarrassment and may also involve the cranialnerves. Even the autonomic nervous system can beinvolved producing malignant arrhythmias[2-5].
R o m a n o - Wa rd syndrome (RWS) is a rareautosomal dominant disorder characterised byepisodes of palpitations, syncope or sometimessudden death in apparently normal youngindividuals with a history of similar problems inthe family[6,7]. It is a hereditary autosomal dominantdisorder where mutations in ion channels lead toabnormal excitation of the myocytes and neuronsp recipitating malignant arrh y t h m i a s[ 8 , 9 ]. Theelectrocardiogram (ECG) in RWS usually shows aprolonged QT interval in excess of 440 msec[10,11].This prolongation of the QT interval is thought tobe responsible for arrhythmias that includeventricular tachycardia and torsade de pointes[12].Sudden death is probably due to ventricularfibrillation. Because of the possibility of the familialoccurrence of these malignant arrhythmias it isessential that patients’ families are screened and
o ff e red medical assistance in the form ofmedications and/or an automatic intracard i a cdefibrillator[13-16]. The association of RWS with GBS,to our knowledge, has not been reported before. Asthe latter condition also may give rise to autonomicneuropathy and arrhythmias, the management ofsuch a combined case is challenging.
CASE PRESENTATIONA35-year-old right-handed male patient of Arab
ancestry, presented with the chief complaints offleeting pain in both upper and the lower limbs,tingling sensation in both upper and lower limbsand mild weakness in the lower limbs of four days’duration. He was continent of urine and faeces. Hehad been previously in reasonably good healthwith normal hearing. However, he was admittedp reviously with complaints of syncope andpalpitations. He was prescribed beta-blockers buthe discontinued the medication at his owndiscretion. Two sisters, one brother and a first-degree relative died suddenly following admissionwith complaints of palpitations and syncope.
The general examination was normal. The basalparameters were within normal limits. The breathholding time was 44 seconds. The re s p i r a t o r ysystem, the cardiovascular system and abdominalexaminations were normal. The CNS examination

Guillain-Barré Syndrome in a Patient with Romano-Ward Syndrome: a Case Report March 200654
revealed a conscious well-oriented gentleman withnormal cranial nerves and fundi. There was mildhypotonia in the lower limbs. The power was 4 / 5at the ankles (which decreased to 1 / 5 by the thirdday of admission) and both plantar reflexes wereflexors. The ankle and knee jerks were absentbilaterally. The sensory system was normal.
The investigations revealed a normal hemogramwith an ESR of 52 mm at the end of the 1st hour.The serum electrolytes, the renal and liver functiontests were normal. The serum calcium level wasalso normal. The cold agglutinin test was 1: 512(positive > 1: 32) and the Mycoplasma serology,IgA, IgM, IgG, were all positive. The chest-X-raywas normal and the corrected Q-T interval on theECG was 505 msec (Fig. 1). The cardiac marker,Troponin I, was 0.146 ug/L. The CSF studiesrevealed glucose of 3.76 mmol/L (simultaneousblood glucose being 4.20 mmol/L), and a totalprotein of 1.49 g/L with a cell count of less than5/cmm. The nerve conduction studies showednerve conduction slowing, prolongation of distallatencies, prolongation of the F-waves andconduction blocks suggestive of demyelinatingpolyneuropathy.
A clinical diagnosis of GBS associated with RWSwas entertained. The patient was closely monitoredfor respiratory embarrassment, arrhythmias and forautonomic neuro p a t h y. He was treated withintravenous immunoglobulin at a dose of 0.4 g/kg/dayfor five days. There was however, no autonomicneuropathy and no arrhythmias were noted on them o n i t o r. After a week, the power in the legsreturned. He was discharged a few days laterwithout any neurological deficit. He was prescribedatenolol 25 mg that was later increased to 50 mg perday, and all his relatives were requested to come tothe hospital for evaluation. He has been advised tohave an automated cardioverter defibrillatorimplanted.
DISCUSSIONThe progressive bilateral weakness of the limbs,
the cytoalbumino-disproportion in the cere b ro -spinal fluid and suggestive nerve conductionstudies clinches the diagnosis of GBS in ourpatient[17-21]. It is known that various infective agentscan precipitate GBS[22]. Our patient had a probable
recent infection with Mycoplasma pneumonia assuggested by the positive antibody and serologytests. This infection had probably triggered theonset of GBS[22]. We were very apprehensive aboutthe possibilities of arrhythmias in this patient, notonly because of the autonomic neuropathy but alsobecause of associated RWS. The patient was startedon beta-blockers, which is recommended for casesof RWS to decrease the QT-interval and theprobability of arrhythmias[15]. This was a difficultdecision, as we did not know how the patientwould respond should autonomic neuro p a t h ydevelop. We started with a low dose of 25 mgatenolol daily and increased to 50 mg daily on thethird day. The QT interval decreased from 505 msecto 410 msec. The necessary precautions were takento detect arrhythmias and respiratory embarrassment.Fortunately the disease did not progress to involvethe phrenic nerves or the autonomic nervoussystem. The patient did not have any arrhythmiasand gradually the power in his legs improved andhe could walk. On discharge, he had noneurological deficit.
CONCLUSIONG u i l l a i n - B a r re’ syndrome and Romano-Wa rd
syndrome are rare diseases. Association of the twodiseases in the same patient would therefore be anextremely rare event. We are reporting, to the bestof our knowledge, the first patient with RW Sa fflicted with GBS. Such an association isdangerous as both diseases may trigger dangerousa r rhythmias. Initiation of treatment withbetablockers in an attempt to decrease the QT-interval in the acute phase of GBS should be donecautiously and preferably when there are facilitiesfor urgent cardiac pacing.
REFERENCES
1. Albers JW, Kelly JJ Jr. A c q u i red inflammatory demy-elinating polyneuropathies: clinical and electrodiagnosticfeatures. Muscle Nerve 1989; 12:435-451.
2. Bradley WG, Daroff RB, Fenichel GM, et al, editors.: In:N e u rology in Clinical Practice. 3rd ed. Boston, Mass:Butterworth-Heinemann; 2000.
3. Hahn AF. Guillain-Barre syndrome. Lancet 1998; 352: 635-641.
4. Ho T, Griffin J: Guillain-Barre syndrome. Curr Opin Neurol1999; 12:389-394.
5. Ropper AH. The Guillain-Barre syndrome. N Engl J Med1992; 326:1130-1136.
6. Romano C, Gemme G, Pongiglione R. Aritmie cardiacherare in eta pediatrica. Clin Pediarr 1963; 45:656-683.
7. Ward OC. A new familial cardiac syndrome in children. J IrMed Assoc 1964; 54:103-106.
8. Hatta S, Sakamot J, Horio Y. Ion channels and diseases.Med Electron Microsc 2002; 35:117-126.
9. Clancy CE, Rudy Y. Na+ channel mutation that causes bothBrugada and long-QT syndrome phenotypes: a simulation
Fig. 1: ECG showing prolonged QT interval

KUWAIT MEDICAL JOURNAL 55March 2006
study of mechanism. Circulation 2002; 105:E9081-9082.10. Schwartz PJ. Idiopathic long QT syndrome: progress and
questions. Am Heart J 1985; 109:399-411. 11. Schwartz PJ, Moss AJ, Vincent GM, et al. Diagnostic criteria
for the long QT syndrome: an update. Circulation 1993;88:782-784.
12. Algra A, Tijssen JGP, Roelandt JR, et al. QTc prolongationmeasured by standard 12-lead electrocardiography is anindependent risk factor for sudden death due to cardiacarrest. Circulation 1991; 83:1888-1894.
13. Towbin JA, Wang Z, Li H. Genotype and severity of longQT syndrome. Arch Pathol Lab Med 2001; 125:116-121.
14. Viskin S, Fish R. Prevention of ventricular arrhythmias inthe congenital long QT syndrome. Curr Cardiol Rep 2000;2:492-497.
15. Moss AJ, Zareba W, Hall WJ, et al. E ffectiveness andlimitations of beta-blocker therapy in congenital long-QTsyndrome. Circulation 2000; 101:616-623.
16. K ron J, Oliver RP, Norsted S, et al. The automaticimplantable cardioverter-defibrillator in young patients. J
Am Coll Cardiol 1990; 16:896-902.17. Annals of Neurology: Criteria for diagnosis of Guillain-
Barre syndrome. Ann Neurol 1978; 3:565-566. 18. Asbury AK, Cornblath DR. Assessment of curre n t
diagnostic criteria for Guillain-Barre syndrome. A n nNeurol 1990; 27: S21-24.
19. Meulstee J, van der Meche FG. Electrodiagnostic criteria forp o l y n e u ropathy and demyelination: application in 135patients with Guillain-Barre syndrome. Dutch Guillain-Barre Study Group. J Neurol Neurosurg Psychiatry 1995;59:482-486.
20. Matthews PM, Arnold DL. In: Diagnostic Tests inNeurology. New York, NY: Churchill Livingston; 1991.
21. Cornblath DR. Electrophysiology in Guillain-Barresyndrome. Ann Neurol 1990; 27 Suppl: S17-20.
22. Jacobs BC, Rothbart PH, van der Meche FG, Herbrink P,Schmitz PI, de Klerk MA, van Doorn PA. The spectrum ofantecedent infections in Gullain-barre syndrome. a case-control study. Neurology 1998; 51:1110-1115.

KUWAIT MEDICAL JOURNAL March 2006
ABSTRACT
The advent of extracorporeal shockwave lithotripsy(ESWL) has extended the treatment armamentariumfor calculi outside of the urinary tract. The use ofESWL for treatment of hepatic duct and pancreaticcalculi is well documented, particularly for thosethat cannot be accessed by endoscopic retrograde
cholangio - pancreatography (ERCP). However,not all stones can be treated by ESWL or accessedby ERCP. We report the case of recalcitrant hepaticduct calculi removed by the use of a semi rigidureteroscope after failure of all other methods oftreatment.
KEYWORDS: cholelithiasis, endoscopy, lithotripsy
Case Report
A Novel Use of Ureteroscope for a Non-urological Cause -A Point of Technique
Address correspondence to:Dr. Ganesh Gopalakrishnan, Professor and Head, Dept of Urology, Christian Medical College and Hospital, Vellore-632 004, Tamilnadu, INDIA.E-mail: [email protected]
Kuwait Medical Journal 2006, 38 (1): 56-58
Shanmugasundaram Rajaian, Amitava Mukherjee, Ganesh GopalakrishnanDepartment of Urology, Christian Medical College, Vellore, Tamilnadu, India
INTRODUCTIONExpertise in the endourological techniques and
in handling endourological instruments has madeurologists to look beyond the urinary tract and helpin managing conditions where other tre a t m e n tmodalities have failed. Intra hepatic calculi causeo b s t ruction, cholestasis, cholangitis, abscesses,post-obstructive atrophy, biliary cirrhosis andc h o l a n g i o c a rcinoma. They cause increased morbidityand mortality due to these complications. The goalin the management of intrahepatic calculi is to getcomplete clearance of these calculi and to re s t o renormal drainage of bile. The high rate of morbidityand mortality associated with open surg i c a lmanagement has triggered the search for alternatemethods of treatment. The other tre a t m e n tmodalities like ERCP and ESWL have been used inthe management of these calculi. However, thesemodalities have their own limitations due toassociated stone impaction, angulated ductalanatomy, and large stone burden. We describe ourexperience in managing such a situation successfully,w h e re other modalities of treatment had failed toretrieve the intrahepatic calculi.
CASE REPORTA 43-year-old woman had a Type IV choledochal
cyst with choledocholithiasis (Fig. 1). She underwentc yst excision and choledocholithotomy with hepatico-jejunostomy five years ago. She p re sented recently tosurgery with abdominal pain, jaundice and fever.
During the work up she was found to havemultiple left hepatic duct calculi and cholangitis.Percutaneous drainage of the obstructed biliarytract (Fig. 2) was done and her cholangitis settled.The percutaneous tract was allowed to mature fortwo weeks. ESWL with Dornier compact Slithotriptor was attempted for the clearance ofcalculi, as there was difficulty in getting access tothe calculi by the endoscopic and percutaneousmethods. Since ESWL and other methods hadfailed to remove the calculi, the urologist’s helpwas sought for the retrieval of the calculi. Due tothe non-availability of laser, 8/9.8 Fr. Wolf semirigid ure t e roscope was used. The stones wereaccessed and were fragmented using Swisslithoclast. The fragments were pushed into thejejunum to be passed out via naturalis.P e rcutaneous drainage of the biliary tract wascontinued postoperatively. Postoperative cholangiogram(Fig. 3) showed complete clearance of the calculiand the drainage of bile was normal.
TechniqueThe attempt to remove the calculi by the
percutaneous route using a semi rigid ureteroscopewas made because of the maneuverability of thetract passing through the left lobe of liver, beingunsupported by the costal margin. Multiple calculiof about 1-1.5 cm size were noted on thecholangiogram (Fig. 4). A 0.035-inch guidewire wasplaced through the mature percutaneous tract. A 10Fr cobra catheter was then placed over the guide

57March 2006 A Novel Use of Ureteroscope for a Non-urological Cause - A Point of Technique
wire to accommodate another safety guide wire.The tract was dilated up to 14 Fr using Teflon serialdilators. A 8/9.8 Fr Wolf semi rigid ureteroscopewas introduced and stones were fragmented with1.0 mm pneumatic intracorporeal probe. Thefragments were pushed into the jejunum andwashed out with the irrigating fluid. A 12 Fr pigtailcatheter was placed over the guide wire in thejejunum. Postoperative PTC showed completeclearance of calculi (Fig. 3). The pigtail catheter wasremoved after two weeks.
DISCUSSIONHepatolithiasis is a potential cause of morbidity
and mortality. Biliary obstruction caused byhepatic duct stones can lead to stricture ,cholangitis, abscess formation, post-obstru c t i v eatrophy, biliary cirrhosis and portal hypertension[1].Before effective surgical and endoscopic methodswere introduced, treatment was often postponed orneglected until the entire liver was involved orbiliary cirrhosis or cholangitis occurred [2]. Earlier,treatment of these stones was by open surgicalmethods. These procedures were associated with
high morbidity and mortality. Even with treatment,it has been estimated that nearly 30% developrecurrent stones, 18.7% need re-operation and 6.8%have secondary biliary cirrhosis[3]. The attemptsmade earlier to decrease the morbidity andmortality of the open surgical procedures wereintraoperative stone localization using ultrasoundthat avoids the critical blood vessels and normalbiliary ducts. The other method was to use ESWLfor fragmentation of the hepatic ducts stones[3].Unfortunately, the former is an additional opensurgical procedure and the latter does not allowdrainage and clearance of fragments, if the stonebulk is large or it is associated with strictures. Thelack of smooth muscle and peristalsis in the hepaticand common bile duct is a further impediment tostone clearance. For these reasons, percutaneousapproach for treating biliary stones was considered.
Percutaneous approach to intrahepatic stonesalong with laser lithotripsy is considered a safe andeffective option for the recalcitrant stones in thebiliary tree[4]. There are potential complications ofthe procedure but they are minor when comparedto the open procedure. When advanced techniques
Fig. 1: Endoscopic Retrograde Cholangio Pancreatography (ERCP)showing the choledochal cyst with calculi and hepatic duct calculi
Fig. 2: Preoperative cholangiogram via the drainage catheter placed inthe left hepatic duct showing the calculi

March 200658
like laser and small flexible endoscopes are notavailable, semi-rigid ure t e roscope along withpneumatic lithotripsy can be used as a method forremoving the recalcitrant hepatic duct calculi. Thec u r rent generation of semi-rigid ure t e ro s c o p eincorporates fiberoptic light and image bundlesinto smaller semi rigid metal sheath allowing muchv e r s a t i l i t y [ 5 ]. These fiberoptic imaging bundlespermit vertical flexibility of the endoscope withoutcausing image distortion (i.e. no half moon effect)[6].The good extent of flexibility of the semi-rigidmetal sheath and tapered tip helps in negotiatingthe acute angles during the manipulation withoutcausing image distortion and damage to the hepatic
ducts. Thus the urologists have a role in providingexpertise in small caliber endoscopy and lithotripsyin other disciplines [7]. There is extensive data in thel i t e r a t u re showing that the use of flexiblecholangioscope / ureteroscope and laser lithotripsyis effective in the management of intrahepatic ductcalculi[4,7]. However, no report exists for treatment ofrecalcitrant hepatic duct calculi using semi-rigidureteroscope and pneumatic lithotripsy. We havedescribed our own technique that has been used inthis patient successfully as a minimally invasive,safe alternative to open surgery especially whenother modalities had failed to retrieve the calculi.
REFERENCES
1. Fan ST, Lai EC, Wong J. Hepatic resection forhepatolithiasis. Arch Surg 1993; 128:1070-1074.
2. Jan Y Y, Chen MF, Wang CS. Surgical treatment ofhepatolithiasis, long-term results. Surgery 1996; 120:509-514.
3. Wolf JS Jr, Stoller ML. Applications of Urological techniquesto nonurinary calculi. Urology 1990; 36:383-389.
4. Nadler RB, Rubeinstein JN. Percutaneous Hepatolithotomy,The northwestern experience. J Endourology 2002; 16:293-297.
5. Ferraro.RF, Abraham VE. A new generation of semi rigidfiberoptic ureteroscopes. J Endourology 1999; 13:35-40.
6. Basillote JB, Lee DI, Eichel L. Ureteroscopes: flexible, rigid,semirigid. Urol Clin N Am 2004; 31:21-31.
7. Tarman GJ, Lenert TJ. Holmium:YAG Laser lithotripsy ofintrahepatic biliary calculi. J Endourology 1999; 13:381-383.
Fig. 4: Preoperative cholangiogram showing the calculi and the guidewire in position
Fig. 3: Postoperative cholangiogram showing complete clearance of thecalculi and the pigtail catheter across the hepaticojejunostomy

KUWAIT MEDICAL JOURNALMarch 2006
Letter to the Editor
A Travel Abroad - Associated Case of LegionellaPneumonia
Nada Al Terkait, Sherif A SadakDepartment of Pediatrics, Al Sabah Hospital, Kuwait
Dear SirWe would like to report two cases of Legionella
pneumonia associated with travel abroad. A ten-year-old Kuwaiti boy and his father had traveled toGermany ten days before they presented with fever,flu-like symptoms and productive cough. They hadno history of bronchial asthma or any chestproblems before. Their disease was diagnosed aspneumonia at the out-patient clinic of anotherhospital and they were treated with amoxicillin, buttheir symptoms continued. Their chest X-ray doneat our hospital showed bilateral pulmonaryinfiltrates. Laboratory findings revealed mildleucocytosis. The IgM antibody titers againstLegionella pneumophilia m e a s u red by ELISAwas 1 / 450(titer of 1:128 or greater indicates the presence ofdisease). Urinary antigen for L. pneumophila wasnegative. It is well known that legionella spp. existubiquitously in environmental water. However,environmental investigations at several points intheir bathroom and airconditioning system failed toisolate the organism. They were treated withclarithromycin for two weeks and their symptomswere promptly resolved.
Legionnaires disease is estimated to be respon-sible for 3 to 15% of community acquired pneu-monia and 10 to 50% of nosocomial infection inE u ropean countries and the United States[ 1 ].E n v i ronmental systems such as airc o n d i t i o n i n g ,cooling towers, evaporative condensers, whirlpoolsand spring baths have hosted and transmitted theorganisms[2]. Transmission is thought to occur viainhalation of aerosolized mist from water sourcescontaminated with the bacterium. Person to persontransmission has not been documented[ 3 ]. Theincubation period for Legionnaire’s disease isgenerally two to 10 days. Current methods forlaboratory detection of legionella pneumoniare q u i re a respiratory specimen or paired seracollected at two to six weeks interval for accuratediagnosis. These techniques include legionella
Address correspondence to:Sherif ASadek, P.O. Box 1940, Al Ardyia 92400, Kuwait. Tel: 9077495, E-mail:[email protected]
c u l t u re, direct fluorescent antibody (DFA ) ,indirect fluorescent antibody (IFA) and DNAprobe.The most widely used serological tests arei m m u n o f l u o rescent antibody and ELISA w h i c hwere used in our cases, The sensitivity of these testsranges from 50 - 60% (the use of immunoglobulinM (IgM) and immunoglobulin G (IgG) significantlyi n c reases the sensitivity) and specificity rangesfrom 96 - 99%[4]. The usefulness of urinary antigendetection for diagnosis of legionella disease hasbeen well documented. Detection of legionellaantigen in urine is achieved through ELISA andradioimmunoassay (RIA). The sensitivity andspecificity of urinary antigen assay are 70% and100% respectively[5].
Legionella pneumonia has been treated withcombination of macrolides, tetracyclins, rifampicinand new quinolones. It has recently been confirmedin basic and chemical studies that variousf l u roquinolones and some new macrolides aree ffective against legionella [ 6 ]. Guidelines of theAmerican Society for Microbiology and AmericanThoracic Society recommend new injectablem a c rolides including azithromycin and IVfluroquinolones as the first choice for treatment oflegionellea pneumonia[7].
In conclusion, these two cases increased oura w a reness about Legionella pneumophila as animportant cause of both community-acquired andnosocomial pneumonia and this must beconsidered as a possible diagnosis in any patientpresenting with pneumonia and history of havingtraveled abroad.
REFERENCES
1. Chang FY, Yu VL. Legionella infections. In: Harrison’sPrinciples of Internal Medicine 2001, p 945-949.
2. Marrie TJ, Johnson W, Tyler S, et al. Potable water andnosocomial Legionnaires disease. Epidemiol Infect 1995;114:267-276.
3. Jemigon DB, Hoffman J, Certran MS, et al. Outbreak of
Kuwait Medical Journal 2006, 38 (1): 59-60

ATravel Abroad - Associated Case of Legionella Pneumonia March 200660
L e g i o n n a i res disease among cruise ship passengersexposed to contaminated whirpool spa. Lancet 1996;347:494-499.
4. Benin A, Benson RF and Besser RE. Trends in Legionnairesdisease and new pattern of diagnosis. Clin Infect Dis 2002;35:1039-1046.
5. Kohler RB. Antigen detection for rapid diagnosis ofMycoplasma and Legionella pneumonia. Diagn Microbial
Infect Dis 1986; 4:475-495.6. Edelstein PH. Antimicrobial chemotherapy for Legionn-
aires disease; time for a change. Ann Intern Med 1998;129:328-330.
7. Niaderman MS, Mandell LA. Guidelines for managementof adult with community- acquired pneumonia. Am J RespCrit Care Med 2001; 163:1730-1754.

KUWAIT MEDICAL JOURNALMarch 2006
Selected Abstracts of Articles Published Elsewhere by Authors in Kuwait
Kuwait Medical Journal 2006, 38 (1): 61-64
Sex of First Child and Breast Cancer Survival: A Population-basedStudy
Thalib L, Hall PDepartment of Community Medicine and Behavioural Sciences (Biostatistics), Faculty of Medicine, Kuwait
University, Kuwait
Int J Cancer 2006; 118:1515-1518
Previous reports on the influence of the sex of a child and prognosis of a subsequent breast cancerhave been conflicting. We took advantage of a number of large and good quality, nationwideRegistries in Sweden to evaluate the prognostic value of the sex of the first child in breast cancer. Apopulation-based cohort of 32,003 women born after 1935 and diagnosed with primary breast cancerbetween 1958 and 1997 was generated by linking a number of Swedish registries including SwedishCancer Registry, Cause of Death Registry, Swedish Generation Registry and the Registry ofPopulation and Population changes. Of these, 4,251 were nulliparous, 2,732 had only a boy and 2,497had only a girl prior to diagnosis. We used this subpopulation to quantify the association betweenthe sex of the first child and breast cancer-specific mortality, using the Cox proportional hazards. Sexof the child did not significantly influence the prognosis of breast cancer. Stratifying by age andadjusting for age at diagnosis, calendar period, time since last birth and age at first child did not alterthe results. Our study, the largest up to date, failed to identify evidence to support the proposedassociation between the sex of the first child and breast cancer survival. Given the previous reportsthat advocated taking sex of the first child into consideration in making decisions related to breastcancer therapy, our findings are reassuring and clinically important. (c) 2005 Wiley-Liss, Inc.
The Impact of an ICU Liaison Nurse on Discharge Delay in PatientsAfter Prolonged ICU Stay
Chaboyer W, Thalib L, Foster M, Elliott D, Endacott R, Richards BResearch Centre for Clinical Practice Innovation, Griffith University Gold Coast Campus, Bundall, Queensland
Anaesth Intensive Care 2006; 34:55-60
The mismatch between intensive care unit (ICU) bed availability and demand may be improvedwith timely patient discharges, however little is known about the nature and contributing factors ofdischarge delays. This study investigated the impact of a specific intervention—the ICU liaisonnurse role—in reducing ICU discharge delay using a prospective block intervention study. Onehundred and eighty-six ICUpatients (101 control and 85 liaison nurse intervention) with an ICUlength of stay of three days or longer and who survived to ICU discharge were examined. Theliaison nurse was involved in assessment of patients for transfer to the ward, with a major focus oncoordinating patient transfer including liaison with ward staff prior to and following ICU discharge.Logistic regression was used to quantify the risk of discharge delay associated with the liaison nurseintervention with adjustment for potential confounding variables. While no demographic or clinicalvariables were significant predictors of ICU discharge delay, those in the liaison nurse group werealmost three times less likely to experience a discharge delay of at least two hours and about 2.5times less likely to experience a delay of four or more hours. The positive effect of the liaison nurserole in reducing the discharge delay remained after adjustingforpotential confounders. We concludethat the liaison nurse role is effective in reducing the discharge delay in ICU transfer.

Selected Abstracts of Articles Published Elsewhere by Authors in Kuwait March 200662
Characterisation of Non-Multiresistant Methicillin-ResistantStaphylococcus Aureus (including EMRSA-15) in Kuwait Hospitals
Udo EE, Al-Sweih N, Noronha BDepartment of Microbiology, Faculty of Medicine, Kuwait University, Kuwait
Clin Microbiol Infect 2006; 12:262-269
This study characterised non-multiresistant methicillin-resistant Staphylococcus aureus (nmMRSA)
isolates from Kuwait hospitals to ascertain whether they were community-acquired MRSA (CA-
MRSA). Forty-two nmMRSA isolates obtained between July 2001 and October 2003 were analysed
by staphylococcal cassette chromosome mec (SCCmec) typing, bacteriophage typing, production of
Panton-Valentine leukocidin (PVL), urease and staphylococcal enterotoxins A, B, C and D, TSST-1,
and by pulsed-field gel electrophoresis (PFGE). Forty-one isolates were SCCmec type IV, and one
isolate was SCCmec type III. The isolates belonged to six PFGE patterns, with two types, A and D,
distributed in six and four hospitals, respectively. Most (n = 26; 61.9%) isolates produced urease.
These isolates were mainly from wound and skin infections, showed low-level methicillin resistance
(MIC 8-48 mg/L), and nine carried genes for PVL. These characteristics, together with their carriage
of the type-IV SCCmec, identified the isolates as CA-MRSA. Ten of the 16 urease-negative isolates
produced staphylococal enterotoxin C; 12 reacted weakly with phage 75, and were resistant to
clindamycin and/or erythromycin, which are characteristics of EMRSA-15. Thus, this study
identified the co-existence of two types of nmMRSA, i.e., CA-MRSA and EMRSA-15, in Kuwait
hospitals.
Paediatric Burns in Kuwait: Incidence, Causes and Mortality
Sharma PN, Bang RL, Al-Fadhli AN, Sharma P, Bang S, Ghoneim IEHealth Sciences Center, Kuwait University, Kuwait. [email protected]
Burns 2006; 32:104-111
From a prospective study on burn patients admitted at the Burn Center in Kuwait during 1993-2001,
826 paediatric burn cases, in 0-14 years age group, were retrieved to study incidence, causes, and
mortality among children. The demographic characteristics, clinical features, and outcome
constituted our data file in Statistical Software, SPSS. Overall incidence rate was 17.5/100,000
children aged 0-14 years, being almost twice (34/100,000) among those between 0 and 4 years,
constituting 70.8% of all paediatric burns. Scald was the main cause of burn (67%), followed by flame
(23%). Mean age (6.4 years) of children with flame burns, was significantly higher (p < 0.001) than
those with scalds, or other causes. A positive significant correlation existed between duration of
hospital stay and TBSA% (r = 0.56, p < 0.001). Overall mortality rate was 0.23/100,000 children,
maximum (0.52/100,000) being in children below 5 years. Among 11 (1.3%) non-survivors, flame
burns caused nine fatalities. Multiple logistic regression mooring predicted children aged < 5 years,
flame burns and TBSA>or= 70%, (OR = 29.2, p < 0.001), as main contributing factors to fatal outcome
among children. Gender and nationality had no influence on incidence or mortality. These findings
will hopefully stimulate development of targeted and sustainable interventions for reducing burns
occurrence among identified paediatric high-risk groups.

KUWAIT MEDICAL JOURNAL 63March 2006
Technetium 99m-Diethylene Triamine Penta-Acetic Acid AerosolClearance in the Evaluation of Pulmonary Involvement in Sickle
Cell Disease
Onadeko BO, Marouf R, Omar AM, Hijazi Z, Khadadah M, Qurtom M, Collier BD, Elgazzar AH,Adekile AD
Department of Medicine, Faculty of Medicine, Kuwait University and Ministry of Health, Safat, Kuwait
Eur J Haematol 2006; 76:147-152
Background: Pulmonary clearance of inhaled technetium (Tc) 99m-labeled diethylene triaminepenta-acetic acid (DTPA) aerosol is a sensitive non-invasive marker of alveolar permeability andpatients with interstitial lung diseases show enhanced clearance. However, a previous study in adultpatients with diabetes mellitus showed delayed clearance. Objectives: To investigate DTPA clearance in steady-state, otherwise healthy adult sickle cell disease(SCD) patients and correlate it with pulmonary function tests (PFTs), hematologic and clinicalparameters. Materials and Methods: The subjects were randomly selected from the Hematology Clinic ofMubarak Hospital, Kuwait. Hematologic and pulmonary function data were collected with standardmethods. DTPA radio-aerosol clearance studies were performed using ultrafine nebulizer containing35 mCi (1295 MBq) of Tc 99m-DTPA in its reservoir and t(1/2) clearance in minutes was determined.Average values for both lungs were calculated and compared with normal values for our population. Results: Forty-three subjects (24 SS and 19 S-beta(0)thal) aged between 16 and 45 yr (mean of 27.1+/- 9.7) were studied. Twenty-two subjects (51.2%) had delayed, while only 10 (23.3%) showedenhanced DTPA clearance. Patients with enhanced clearance showed better PFTs than those withnormal or delayed clearance. There was significant negative correlation of DTPA clearance withforced expiratory volume in 1 s, forced vital capacity and total lung capacity and significant positivecorrelation with age.Conclusions: Majority of adult SCD patients have delayed DTPA clearance unlike in inflammatorylung diseases, but similar to diabetes mellitus. DTPA clearance may be a useful modality formonitoring pulmonary involvement in SCD.
Utility of Volume Adjusted Prostate Specific Antigen Density in theDiagnosis of Prostate Cancer in Arab Men
Sheikh M, Al-Saeed O, Kehinde EO, Sinan T, Anim JT, Ali YDepartment of Radiology, Faculty of Medicine, Kuwait University, P.O. Box 24923, 13110, Safat, Kuwait,
Int Urol Nephrol 2005; 37:721-726
Background: This study was undertaken to assess the utility of prostate specific antigen (PSA) andPSA density (PSAD) in discriminating between benign and malignant prostate disease in theKuwaiti Arab population.Methods: A total of 100 consecutive patients suspected of having prostate cancer because of serumPSA> 4 ng/ml, or detection of a prostatic nodule on rectal examination were further investigated bydetermination of PSAD, TRUS of prostate, sexant prostatic biopsy and histological analysis toestablish the correct diagnosis. Other diagnostic measures included the determination of the areaunder the receiver operating characteristic (ROC) curve, sensitivity and specificity.Results: Of the 100 prostate biopsies that were performed, 33 cases were confirmed to be prostatecancer and 67 were described as benign lesions comprising benign prostatic hyperplasia (BPH) withor without prostatitis. The age range for patients with prostate cancer was 42-90 years, and 52-90years for those without prostate cancer. The mean prostate volume was 58.82 cc (range 9-177 cc) and

Selected Abstracts of Articles Published Elsewhere by Authors in Kuwait March 200664
62.60 cc (range 15-140 cc), the mean PSA value was 36.65 ng/ml (range 5.8-200 ng/ml) and 16.49ng/ml (range 1.4-46.0 ng/ml), while the mean PSAD was 0.92 (range 0.046-5.714) and 0.452 (range0.034-2.294) for patients with prostate cancer and patients without prostate cancer respectively.Patients with PSAless than 4 ng/ml (3 cases) all had benign prostate lesions, and 7 cases with PSAmore than 50 ng/ml all had prostate cancer and were excluded because values above 50 ng/ml haveclose to 100% specificity for prostate cancer. Further analysis was done on the remaining 90 caseswhich were patients with a PSA between 4 and 50 ng/ml. The discriminating power of serum PSAfor detecting prostate cancer as estimated by the area under ROC was 0.686 while that for PSAD was0.732. The maximum likelihood for a positive PSAwas at a PSAD cut-off point of 0.32. For the PSAcut-off point of l0 ng/ml, the sensitivity was 80%, and specificity was 42.2%. For the PSAD cut-offpoint of 0.32, the sensitivity was 58% and the specificity 76.6%. Conclusions: Determination of PSAD is not a useful adjunct to serum PSAvalues in the range of 10-50 ng/ ml in our population. PSAD value less than 0.32 with PSA less than l0 ng/ml stronglysuggests benign disease.
In vivo Evaluation of Limonene-Based Transdermal TherapeuticSystem of Nicorandil in Healthy Human Volunteers
Krishnaiah YS, Chandrasekhar DV, Rama B, Jayaram B, Satyanarayana V,Al-Saidan SM
Department of Pharmaceutics, Faculty of Pharmacy, Health Science Center, Kuwait University, Kuwait. E-mail:[email protected]
Skin Pharmacol Physiol 2005; 18:263-272
Hydroxypropyl methylcellulose (HPMC) gel drug reservoir system prepared with 70:30 v/vethanol-water solvent system containing 6% w/w of limonene was effective in promoting the invitro transdermal delivery of nicorandil. The objective of the present study was to fabricate andevaluate a limonene-based transdermal therapeutic system (TTS) for its ability to provide the desiredsteady-state plasma concentration of nicorandil in human volunteers. The in vitro permeation ofnicorandil from a limonene-based HPMC gel drug reservoir was studied across excised rat skin(control), EVA2825 membrane, adhesive-coated EVA2825 membrane and adhesive-coated EVA2825membrane-excised rat skin composite to account for their effect on the desired flux of nicorandil. Theflux of nicorandil from the limonene-based HMPC drug reservoir across EVA2825 membranedecreased to 215.8 +/- 9.7 microg/cm(2).h when compared to that obtained from control, indicatingthat EVA2825 was effective as a rate-controlling membrane. The further decrease in nicorandil fluxacross adhesive-coated EVA2825 membrane and adhesive-coated EVA2825 membrane-excised ratskin composite showed that the adhesive coat and skin also controlled the in vitro transdermaldelivery. The limonene-based drug reservoir was sandwiched between adhesive-coated EVA2825-release liner composite and a backing membrane. The resultant sandwich was heat-sealed as circle-shaped patch (20 cm(2)), trimmed and subjected to in vivo evaluation in human volunteers againstimmediate-release tablets of nicorandil (reference formulation). The fabricated limonene-based TTSof nicorandil provided a steady-state plasma concentration of 21.3 ng/ml up to 24 h in healthyhuman volunteers. It was concluded that the limonene-based TTS of nicorandil provided the desiredplasma concentration of the drug for the predetermined period of time with minimal fluctuationsand improved bioavailability.

KUWAIT MEDICAL JOURNALMarch 2006
1st International Conference on P e d i a t r i cColorectal SurgeryMar 22-24, 2006 Salwa Al-Sabah Center, Kuwait Contact: Dept. of Pediatric Surg e r y, Ibn SinaHospital, KuwaitE-Mail: [email protected]: www.pedsurgery-kw.com
Up in Cancer Genetics: Clinical Translation Mar 23-25, 2006 Omaha, NE, United StatesContact: Marilyn Stockdale Tel: 402-280-1830 / 1-800-548-2633; Fax: 402-280-5180 E-Mail: [email protected]
Internal Derangements of JointsMar 23-26, 2006 St. John Virgin Islands, United StatesContact: Ryals and Associates Inc, P.O. Box 380,Springville, AL 5146 Tel: 205-467-3158; Fax: 205-467-3199 E-Mail: [email protected] / [email protected]
Breast Imaging 2006 Mar 27-30, 2006 Naples FL, United StatesContact: Ryals and Associates Inc, P.O. Box 380,Springville, AL 5146 Tel: 205-467-3158; Fax: 205-467-3199 E-Mail: [email protected] / [email protected]
HIV Pathogenesis Mar 27-Apr 02, 2006 Keystone, CO, United States Contact: Meeting OrganiserTel: 800-253-0685 / 970-262-1230; Fax: 970-262-1525 E-Mail: [email protected]
HIV Vaccines Mar 27-Apr 02, 2006 Keystone, CO, United StatesContact: Meeting OrganiserTel: 800-253-0685 / 970-262-1230; Fax: 970-262-1525 E-Mail: [email protected]
Forthcoming Conferences and Meetings
Kuwait Medical Journal 2006, 38 (1): 65-71
Compiled and edited by Babichan K Chandy
Adriatic Vascular Ultrasound Society Mar 30-Apr 01, 2006 Lugano Switzerland Contact: Guido C. Robotti M.D. Tel: 41-918-116-091; Fax: 41-918-116-090 E-Mail: [email protected]
Anesthesia and Perioperative Care in the OlderPatient Mar 31-Apr 01, 2006 Rotterdam, NetherlandsContact: Prof. dr. jan klein Tel: 00-31-104-633-458; Fax: 00-31-104-633-722 E-Mail: [email protected]
Current Practice of Vascular UltrasoundMar 31-Apr 02, 2006 Las Vegas, NV, United StatesContact: Kelly Winters Tel: 914-921-5700; Fax: 914-921-6048 E-Mail: [email protected]
Carotid and Transcranial Doppler Mar 31-Apr 02, 2006 Las Vegas, NV, United StatesContact: Kelly Winters Tel: 914-921-5700; Fax: 914-921-6048 E-Mail: [email protected]
1st International Hidradenitis SuppurativaSymposium Mar 31-Apr 02, 2006 Dessau, Germany Contact: Michelle Barlow Tel: 1-619-255-7781; Fax: 1-619-239-327 E-Mail: [email protected]
Ultrasound/Women’s Imaging 2006 Apr 02-05, 2006 Boston, MA, United StatesContact: CME Office Tel: 617-384-8600 Fax: 617-384-8686 E-Mail: [email protected]
Geriatrics 2006 Apr 02-06, 2006 Istanbul, Turkey Contact: Meeting Organiser Tel: 902-122-928-808; Fax: 902-122-928-807 E-Mail: [email protected]

Forthcoming Conferences and Meetings March 200666
Diagnostic Imaging on Kona Apr 02-07, 2006 Kamuela, HI, United States Contact: UCSF Office of Continuing MedicalEducation, 3333 California Street, Room 450, SanFrancisco, CA 94118 Tel: 415-476-4251 / 415-476-5808 Fax: 415-476-0318/ 415-502-1795 E-Mail: [email protected]
Paediatric Imaging Apr 03-04, 2006 London, England, United KingdomContact: Mrs Sarah McLellan / Miss Chloe Scragg Tel: 44-0-2-073-071-425 E-Mail: sarah.mclellan@bir. o rg.uk / hloe.scragg@bir. o rg.uk
Heart and Brain AttackApr 06-08, 2006 Hilton Head, SC, United StatesContact: Jason Norton Tel: 706-721-3967; Fax: 706-721-4642 E-Mail: [email protected]
Clinical Dermatology 2006 Apr 06-08, 2006 Vienna, AustriaContact: Organising Secretariat, CCT PostgraduateEducation Limited, 50-52 Union Street, London SE11TD United Kingdom Tel: +44-171-407-9731; Fax: +44-171-378-9268 or+44-171-403-0066 E-Mail: [email protected]
Sexual Dysfunction : Clinical Practice, Research &Trends 2006 Apr 06-09, 2006 Queenstown, New ZealandContact: Marg CraigTel: 64-33-435-900; Fax: 64-33-435-063 E-Mail: [email protected]
Allergy, Allergic Inflammation and AsthmaApr 06-11, 2006 Breckenridge, CO, United StatesContact: Meeting Organiser Tel: 800-253-0685 / 970-262-1230; Fax: 970-262-1525 E-Mail: [email protected]
Neuroradiology: Advanced CT/MR Imaging Apr 13-14, 2006 San Francisco, CA, United StatesContact: UCSF Office of Continuing MedicalEducation, 3333 California Street, Room 450, SanFrancisco, CA94118 Tel: 415-476-4251 / 415-476-5808; Fax: 415-476-0318/ 415-502-1795 E-Mail: [email protected]
International Symposium: “The Uterus in ART” &P re-Symposium Workshops on Ultrasound andHysteroscopyApr 13-16, 2006 Antalya, TurkeyContact: Mete Isikoglu Tel: 905-542-149-493; Fax: 902-423-454-747 E-Mail: [email protected]
Global Endovascular Therapeutics 2006 Apr 13-16, 2006 Singapore, SingaporeContact: Ms Felicia Teng Tel: 65-63-464-402; Fax: 65-63-464-403 E-Mail: [email protected]
Neurology for the Non-Neurologist Apr 17-21, 2006 Bradenton-Sarasota, FL, United StatesContact: Eva or Cristina Tel: 1-866-267-4263 / 1-941-388-1766; Fax: 1-941-365-7073 E-Mail: [email protected]
Echocardiography Apr 19-20, 2006 Las Vegas, NV, United StatesContact: Trish Darling Tel: 989-631-4664 E-Mail: [email protected]
3rd Annual Team EchocardiographyApr 20-23, 2006 Hilton Head Island, SC, United StatesContact: Sherri MooreTel: 800-277-7654 ext 4505; 336-716-4505; Fax: 336-716-2447 E-Mail: [email protected]
Percutaneous Tumor Ablation: Current Status andFuture Directions Apr 21-22, 2006 Boston, MA, United StatesContact: CME Office Tel: 617-384-8600; Fax: 617-384-8686 E-Mail: [email protected]
12th Annual Breast Imaging & Interventions Apr 21-23, 2006 San Diego, CA, United States Contact: Ryals and Associates Inc, P.O. Box 380,Springville, AL 5146 Tel: 205-467-3158; Fax: 205-467-3199 E-Mail: [email protected] / [email protected]

KUWAIT MEDICAL JOURNAL 67March 2006
Ob/Gyn and Abdominal Sonography Apr 21-23, 2006 San Francisco, CA, United States Contact: UCSF Office of Continuing MedicalEducation, 3333 California Street, Room 450, SanFrancisco, CA94118 Tel: 415-476-4251 / 415-476-5808; Fax: 415-476-0318/ 415-502-1795 E-Mail: [email protected]
Practical Applications of New Imaging TechniquesApr 24-26, 2006 Brugge, Belgium Contact: CME Office Tel: 617-384-8600; Fax: 617-384-8686 E-Mail: [email protected]
Pain Management in Women Apr 27-29, 2006 San Diego, CA, United StatesContact: Cheryle Genovese Tel: 888-229-6263; Fax: 858-822-5908 E-Mail: [email protected]
1st Congress of the International D e r m o s c o p ySociety Apr 27-29, 2006 Naples, Italy Contact: Stefania Livesu Tel: 00-39-0-228-172-300; Fax: 00-39-0-228-172-300 E-Mail: [email protected]
IXth International Symposium on S j π g r e n ’sSyndromeApr 27-29, 2006 Washington DC, United StatesContact: Dr. Philip C. Fox Tel: 1-301-718-0300; Fax: 1-301-718-0322 E-Mail: [email protected]
17th International Conference on the Reduction ofDrug Related Harm Apr 30-May 04, 2006 Vancouver, BC, Canada Contact: Shannon BrownTel: 1-604-688-9655 ext 2; Fax: 1-604-685-3521 E-Mail: [email protected]
9th International Symposium of Facial PlasticSurgeryMay 01-04, 2006 Las Vegas, NV, United StatesContact: American Academy of Facial Plastic andR e c o n s t ructive Surg e r y, 310 S. Henry Stre e t ,Alexandria, VA 22314 Tel: 703-299-9291; Fax: 703-299-8898 E-Mail: [email protected]
Pediatric Infectious Diseases for Primary CareMay 01-05, 2006 Bradenton-Sarasota, FL, United StatesContact: Eva or Cristina Tel: 1-866-267-4263 /1-941-388-1766; Fax: 1-941-365-7073 E-Mail: [email protected]
Paediatric Update Conference May 01-06, 2006 Toronto, ON, CanadaContact: Brenda Rau Tel: 416-813-8122; Fax: 416-813-5230 E-Mail: [email protected]
Endocrinology and Rheumatology: A C l i n i c a lReview and Up/Internal Medicine: AC o m p re h e n s i v eReview and Up for Primary Care / EmergencyMedicine: Applying an Evidence-Based Approachto Your Practice May 01-31, 2006 Sarasota, FL, United StatesContact: Eva / Cristina Tel: 1-866-267-4263 /1-941-388-1766; Fax: 1-941-365-7073 E-Mail: [email protected]
A Practical Approach to Clinical Neurology inPrimary Care / A Practical Approach to PediatricEmergency Medicine/Evidence-Based Cardiology:A Clinical Review and Up May 01-31, 2006 Sarasota, FL, United States Contact: Eva / Cristina Tel: 1-866-267-4263/1-941-388-1766; Fax: 1-941-365-7073 E-Mail: [email protected]
1st Romanian Congress of Anti-Aging MedicineMay 05- 07, 2006 Bucharest, RO, RomaniaContact: Stoian Cornel Tel: 40-745-537-003; Fax: 40-214-130-212 E-Mail: [email protected]
The 31st Annual Specialty Review Course inAnesthesiology May 06-12, 2006 Chicago, IL, United States Contact: Maria Courtney Tel: 800-328-2308; Fax: 210-641-8329 E-Mail: [email protected]
Disease Management Colloquium May 10-12, 2006 Philadelphia, PA, United States Contact: Paul TunnecliffTel: 800-684-4549; Fax: 760-418-8084 E-Mail: [email protected]

Forthcoming Conferences and Meetings March 200668
The Heart of C a r d i o l o g y is (Still) Echocardiography May 12-13, 2006 Milwaukee, WI, United StatesContact: Conference Coordinator Tel: 608-240-2150 / 608-263-2850; Fax: 608-240-2151/ 608-262-8421 E-Mail: [email protected]
CT & MR Imaging May 15-20, 2006 Las Vegas, NV, United StatesContact: Kelly Winters Tel: 914-921-5700; Fax: 914-921-6048 E-Mail: [email protected]
The 8th Iranian Congress of Immunology &AllergyMay 16-18, 2006 Tehran, Iran Contact: Meeting Organiser Tel: 00-98-218-989-484; Fax: 00-98-216-419-536 E-Mail: [email protected]
Advance Dermatology Course May 16-19, 2006 Jeddah, Saudi Arabia Contact: Dr. Gamal Hashem, Head of DermatologyDepartment and President of the Conference Tel: 00-96-626-829-000 ext. 6477/6481; Fax: 00-96-626-835-874 E-Mail: [email protected], [email protected]
Hot Topics in Primary CareMay 18-20, 2006 Las Vegas, NV, United StatesContact: Nancy Mullins Tel: 800-423-4982; Fax: 205-945-1548 E-Mail: [email protected]
Practical Advances in Diagnostic ImagingMay 21-26, 2006 Yosemite, CA, United States Contact: UCSF Office of Continuing MedicalEducation, 3333 California Street, Room 450, SanFrancisco, CA 94118 Tel: 415-476-4251 / 415-476-5808; Fax: 415-476-0318/ 415-502-1795 E-Mail: [email protected]
2nd International Forum on Pain Medicine.Medical Specialties Meet Pain Medicine. May 25-28, 2006 Guadalajara, MexicoContact: Kenes International Tel: 41-229-080-488; Fax: 41-227-322-850
Federation of Clinical Immunology Societies 2006Annual Meeting Jun 01-05, 2006 San Francisco, CA, United StatesContact: FOCIS, 555 E. Wells St, Suite 11 0 0 ,Milwaukee, WI 53202 Tel: 414-918-3192; Fax: 414-276-3349 E-Mail: [email protected]
IOF World Congress on OsteoporosisJun 02-06, 2006 Toronto, ON, CanadaContact: IOF Congress Secretariat Tel: 33-472-914-177; Fax: 33-472-369-052 E-Mail: [email protected]
Laser Aesthetics Jun 03-04, 2006 Portland, OR, United StatesContact: Trish Darling Tel: 989-631-4664 E-Mail: [email protected]
EchocardiographyJun 05-06, 2006 Portland, OR, United StatesContact: Trish Darling Tel: 989-631-4664 E-Mail: [email protected]
Critical Care Medicine and TraumaJun 08-10, 2006 San Francisco, CA, United StatesContact: UCSF Office of Continuing MedicalEducation, 3333 California Street, Room 450, SanFrancisco, CA94118 Tel: 415-476-4251 / 415-476-5808; Fax: 415-476-0318/ 415-502-1795 E-Mail: [email protected]
Advances in 3D/4D UltrasoundJun 08-10, 2006 Las Vegas, NV, United StatesContact: Kelly Winters Tel: 914-921-5700; Fax: 914-921-6048 E-Mail: [email protected]
2nd World Congress on Ultrasound in Emergencyand Critical Care Jun 11-14, 2006 New York, NY, United StatesContact: Dr. Francis Lee Tel: 65-63-793-169 E-Mail: [email protected]

KUWAIT MEDICAL JOURNAL 69March 2006
Practical MR Imaging of the Abdomen and Pelvis(with CT Correlation) Jun 12-14, 2006 Boston, MA, United States Contact: CME Office Tel: 617-384-8600; Fax: 617-384-8686 E-Mail: [email protected]
Skin Problems and Diseases Jun 15-19, 2006 Seattle, WA, United States Contact: American Academy of Family Physicians,P.O. Box 11210, Shawnee Mission, KS 66207-1210 Tel: 800-274-2237 / 913-906-6000 E-Mail: [email protected]
Advances in Diagnostic Radiology Jun 18-25, 2006 Rochester, MN, United States Contact: MSCME in Rochester, Minn Tel: 800-323-2688 USAonly/507-284-2509; Fax: 507-284-0532 E-Mail: [email protected]
Advanced MR and CT Imaging-Fundamentals,Techniques, Applications Jun 19-23, 2006 Kiawah Island, SC, United StatesContact: Sally Zimney Tel: 919-684-7758 Fax: 919-684-7158 E-Mail: [email protected]
14th International Symposium on HIV &Emerging Infectious Diseases (ISHEID) Jun 21-23, 2006 Toulon, France Contact: Scientific Secretariat, Docteur A l a i nLafeuillade, Infectiology Unit, H™pital Chalucet,83056 TOULON, FRANCETel: 33-494-227-741; Fax: 33-494-926-747 E-Mail: [email protected]
Critical Issues in Dermatopathology and ClinicalDermatology: Everything You Wanted to Knowand MoreJun 26-29, 2006 Hilton Head Island, SC, United States Contact: Carol A. Haag Tel: 925-376-0217; Fax: 925-631-9525 E-Mail: [email protected]
C a r d i o l o g y Up in Primary Care Medicine: A nEvidence-Based Approach Jun 26-30, 2006 Bradenton-Sarasota, FL, United States Contact: Eva or Cristina Tel: 1-866-267-4263/1-941-388-1766; Fax: 1-941-365-7073 E-Mail: [email protected]
Transfusion Practice and Transfusion Alternatives Jun 29-30, 2006 Riga, Latvia Contact: Leon Shapiro MD Tel: 12-018-030-191; Fax: 12-015-030-294 E-Mail: [email protected]
Cardiovascular Prevention 2006 / Setting up aRehabilitation Clinic Jun 29-Jul 01, 2006 Sophia-Antipolis, France Contact: St≥phanie Deambrosis Tel: 33-492-947-600; Fax: 33-492-941-824 E-Mail: [email protected]
Hypertension: Improving Outcomes Jun 30-Jul 02, 2006 Myrtle Beach, SC, United States Contact: Mandy Stone Tel: 800-423-4992; Fax: 205-945-1548 E-Mail: [email protected]
12th International Symposium on Viral Hepatitisand Liver Disease Jul 01-05, 2006 Paris, France Contact: Emmanuelle VIAUTel: 33-153-858-268; Fax: 33 -153-858-283 E-Mail: [email protected]
Family Medicine, Part I: Issues in Adult Medicine/Family Medicine, Part II: Issues in A d u l t ,Pediatric and GYN Medicine Jul 01-31, 2006 Sarasota, FL, United StatesContact: Eva / Cristina Tel: 1-866-267-4263/1-941-388-1766; Fax: 1-941-365-7073 E-Mail: [email protected]
Endocrinology and Rheumatology: A C l i n i c a lReview and Up/Internal Medicine: A Comprehen-sive Review and Up for Primary Care / EmergencyMedicine: Applying an Evidence-Based Approachto Your Practice Jul 01-31, 2006 Sarasota, FL, United StatesContact: Eva / Cristina Tel: 1-866-267-4263/1-941-388-1766; Fax: 1-941-365-7073 E-Mail: [email protected]
12th International Pain Clinic Congress - WorldSociety of Pain Clinicians Jul 04-07, 2006 Turin, Italy Contact: Chiara Fabbi Tel: 39-0-112-446-920; Fax: 39-0-112-446-900 E-Mail: [email protected]

Forthcoming Conferences and Meetings March 200670
Up in Cancer Genetics: Clinical Translation Jul 07-10, 2006 Honolulu, HI, United StatesContact: Continuing Medical Education Division,601 North 30th Street Suite 2130 - Omaha, NE 68131 Tel: 402-280-1830 / 800-548-2633; Fax: 402-280-5180
Surgical Pathology of Soft Tissue, Head and Neck,Gynecologic and Lymph Node Tumors Jul 10-13, 2006 Maui, HI, United States Contact: Carol A. Haag Tel: 925-376-0217; Fax: 925-631-9525 E-Mail: [email protected]
1st Annual Scientific Meeting of the Society ofCardiovascular CT Jul 13-16, 2006 New Orleans, LA, United States Contact: Office of Continuing Medical Education Tel: 800-588-5300 / 504-988-5466; Fax: 504-988-1779 E-Mail: [email protected]
World Congress of Asthma 2006 Jul 15-18, 2006 Lausanne, SwitzerlandContact: Aurélia Patty E-Mail: [email protected]
CT, MR and Ultrasound: Head-to-Toe Jul 16-21, 2006 Kamuela, HI, United StatesContact: UCSF Office of Continuing MedicalEducation, 3333 California Street, Room 450, SanFrancisco, CA94118 Tel: 415-476-4251 / 415-476-5808; Fax: 415-476-0318/ 415-502-1795 E-Mail: [email protected]
Dermatology and Aesthetic Medicine Cruise Jul 16-23, 2006 Anchorage, AK, United StatesContact: Dr. Martin Gerretsen Tel: 1-888-647-7327; Fax: 1-888-547-7337 E-Mail: [email protected]
S i n g a p o re Menopause Congress 2006 - NewHorizons in Menopause Management for theAsian Woman Jul 28-30, 2006 Singapore SingaporeContact: Ms Pam Wong / Ms Dynelle Huang Tel: 65-63-214-491/65-63-266-682; Fax: 65-62-239-789 E-Mail: [email protected] / [email protected]
Mayo Clinic 2006 Endoscopic Ultrasound Course Aug 03-05, 2006 Rochester, MN, United States Contact: MSCME in Rochester, Minn Tel: 800-323-2688 USA only / 507-284-2509; Fax:507-284-0532 E-Mail: [email protected]
Success with Failure: New Strategies for theEvaluation and Treatment of Congestive HeartFailureAug 06-08, 2006 Rochester, MN, United States Contact: MSCME in Rochester, Minn Tel: 800-323-2688 USA only / 507-284-2509; Fax:507-284-0532 E-Mail: [email protected]
11th International Congress of Human GeneticsAug 06-10, 2006 Brisbane, QLD, Australia Contact: Sarah Hamm Tel: 61-396-820-244; Fax: 61-396-820-288 E-Mail: [email protected]
Collegium Internationale Geronto Pharmacologicum(CIGP) Aug 10-13, 2006 Jakarta, IndonesiaContact: Sri Witarti Tel: 62-21-559-601-80; Fax: 62-21-559-601-79 E-Mail: [email protected]
16th World Congress of the World Society ofCardio-Thoracic Surgeons - WSCTS 2006 Aug 17-20, 2006 Ottawa, ON, Canada Contact: Dr. Tofy Mussivand, Chairman Tel: 1-613-761-5116; Fax: 1-613-761-4478 E-Mail: [email protected]
12th World Congress on Pain Aug 17-22, 2008 Glasgow, Scotland, United KingdomContact: Elizabeth Twiss Tel: 206-547-6409; Fax: 206-547-1703 E-Mail: [email protected]
Sixth International Symposium on C o c c i d i o i d o m y c o s i sAug 23-26, 2006 Stanford, CA, United StatesContact: Cheryl Featherstone Tel: 888-229-6263; Fax: 858-822-5908 E-Mail: [email protected]

KUWAIT MEDICAL JOURNAL 71March 2006
10th Informational Congress of Cardiothoracic andVascular Anesthesia with Industrial Exhibits Aug 27-30, 2006 Prague, Czech Republic Contact: Kristina Pichanicova (Ms.) Tel: 42-0-284-001-444; Fax: 42-0-284-001-448 E-Mail: [email protected]
17th International Mass Spectrometry Conference Aug 27-Sep 01, 2006 Prague, Czech RepublicContact: Secretariat Tel: 42-0-241-062-645 E-Mail: [email protected]
Radiology in Scotland: Advances inMusculoskeletal, Neuroradiology, Pediatric, andChest Imaging Aug 28-Sep 01, 2006 Westin, FL, United StatesContact: Ryals and Associates Inc, P.O. Box 380,Springville, AL 5146 Tel: 205-467-3158; Fax: 205-467-3199 E-Mail: [email protected] / [email protected]
International Conference, Advances andControversies in Laser Medicine and Surgery Aug 30-Sep 01, 2006 Barcelona, SpainContact: Marta Ventura Tel: 34-934-140-206; Fax: 34-933-177-415 E-Mail: [email protected]
World Congress of CardiologySep 02-06, 2006 Barcelona, SpainContact: Congress Secretariat E-Mail: [email protected]
16th World Congress on Ultrasound in Obstetricsand Gynecology Sep 03-07, 2006 London, England, United KingdomContact: Congress Secretariat Tel: 44-0-2-074-719-955; Fax: 44-0-2-074-719-959 E-Mail: [email protected]
Basic and Intermediate DermoscopySep 07-09, 2006 Warsaw, Poland Contact: Lidia Rudnicka Tel: 48-228-242-200; Fax: 48-225-081-492 E-Mail: [email protected]
The 4th Annual Scientific Meeting of The SaudiThoracic Society & The 10th Annual Meeting ofThe Pan-Arab Thoracic Association Sep 19-21, 2006 Jeddah, Saudi Arabia Contact: Professor Mohamed Al-Hajjaj Tel: 00-96-612-488-966; Fax: 00-96-612-487-431 E-Mail: [email protected]
13th International Symposium of The MycologySection Polish Dermatology Society “Mycology 2006” Sep 21-23, 2006 Bialowieza, Podlaskie, Poland Contact: Prof. Roman Nowicki Tel: 00-48-583-492-590; Fax: 00-48-583-492-586 E-Mail: [email protected]
2nd Asia Pacific Congress in Maternal Fetal MedicineSep 21-23, 2006 Guangzhou, China Contact: Dr TY Leung Tel: 852-26-322-810; Fax: 852-26-360-008 E-Mail: [email protected]
Radiology in Italy Sep 24-30, 2006 Fiuggi, JapanContact: D. Beatty Crawford, M.D. Tel: 00-1-860-364-502 / 800-659-0872 in USA; Fax:860-364-5040 E-Mail: [email protected]
5th Advanced Symposium on Congenital HeartDisease in the Adult Sep 25-27, 2006 London, England, United KingdomContact: Prof Michael A Gatzoulis Tel: 44-0-20-73-51-82-27; Fax: 44-0-20-73-51-86-29 E-Mail: [email protected]
39th Southeast Pediatric Cardiology S o c i e t yAnnual Meeting Sep 28-30, 2006 Atlanta, GA, United StatesContact: Marsha Elixson, Program Coordinator Tel: 1-770-448-9202 ext 270; Fax: 1-678-542-9410 E-Mail: [email protected]
From Human Genetic Variations to Prediction ofRisks and Responses to Drugs and to theEnvironment Sep 28-Oct 02, 2006 Thira - Santorini, Greece Contact: Pr Gerard Siest Tel: 00-33-0-383-682-170 / 71 / 63 / 65; Fax: 00-33-0-383-321-322 E-Mail: [email protected]

KUWAIT MEDICAL JOURNAL March 2006
WHO-Facts Sheet
1. Avian Influenza: The Disease in Birds
2. WHO Calls for Global Action to Avert 8 Million Cancer-related Deaths by 2015
3. Cancer
Compiled and edited by Babichan K Chandy
1. AVIAN INFLUENZA: THE DISEASE INBIRDS
What is avian influenza?Avian influenza is an infectious disease of birds
caused by type A strains of the influenza virus. Thedisease occurs worldwide. While all birds arethought to be susceptible to infection with avianinfluenza viruses, many wild bird species carrythese viruses with no apparent signs of harm.
Other bird species, including domestic poultry,develop disease when infected with avianinfluenza viruses. In poultry, the viruses cause twodistinctly different forms of disease - one commonand mild, the other rare and highly lethal. In themild form, signs of illness may be expressed onlyas ruffled feathers, reduced egg production, ormild effects on the respiratory system. Outbreakscan be so mild they escape detection unless regulartesting for viruses is in place.
In contrast, the second and far less commonhighly pathogenic form is difficult to miss. Firstidentified in Italy in 1878, highly pathogenic avianinfluenza is characterized by sudden onset ofsevere disease, rapid contagion, and a mortalityrate that can approach 100% within 48 hours. Inthis form of the disease, the virus not only affectsthe respiratory tract, as in the mild form, but alsoinvades multiple organs and tissues. The resultingmassive internal haemorrhaging has earned it thelay name of “chicken Ebola”.
Which viruses cause highly pathogenic disease?All 16 HA (haemagluttinin) and 9 NA
(neuraminidase) subtypes of influenza viruses areknown to infect wild waterfowl, thus providing anextensive reservoir of influenza viruses perpetuallyc i rculating in bird populations. In wild bird s ,routine testing will nearly always find some
Address correspondence to: Office of the Spokesperson, WHO, Geneva. Tel.: (+41 22) 791 2599; Fax (+41 22) 791 4858; Email: [email protected]; Website: http://www.who.int/
influenza viruses. The vast majority of these virusescause no harm.
To date, all outbreaks of the highly pathogenicform of avian influenza have been caused byv i ruses of the H5 and H7 subtypes. Highlypathogenic viruses possess a tell-tale genetic “trademark” or signature - a distinctive set of basic aminoacids in the cleavage site of the HA - thatdistinguishes them from all other avian influenzaviruses and is associated with their exceptionalvirulence.
Not all virus strains of the H5 and H7 subtypesare highly pathogenic, but most are thought to havethe potential to become so. Recent research hasshown that H5 and H7 viruses of low pathogenicitycan, after circulation for sometimes short periods ina poultry population, mutate into highlypathogenic viruses. Considerable circ u m s t a n t i a levidence has long suggested that wild waterfowlintroduce avian influenza viruses to poultry flocks,in their low pathogenic form, but do not carry ordirectly spread highly pathogenic viruses. This rolemay, however, have changed very recently: at leastsome species of migratory waterfowl are nowthought to be carrying the H5N1 virus in its highlypathogenic form and introducing it to newgeographical areas located along their flight routes.
Apart from being highly contagious amongp o u l t r y, avian influenza viruses are re a d i l ytransmitted from farm to farm by the movement oflive birds, people (especially when shoes and otherclothing are contaminated), and contaminatedvehicles, equipment, feed, and cages. Highlypathogenic viruses can survive for long periods inthe environment, especially when temperatures arelow. For example, the highly pathogenic H5N1virus can survive in bird faeces for at least 35 daysat low temperature (4 ºC). At a much highert e m p e r a t u re (37 ºC), H5N1 viruses have beenshown to survive, in faecal samples, for six days.
Kuwait Medical Journal 2006, 38 (1): 72-79

KUWAIT MEDICAL JOURNAL 73March 2006
For highly pathogenic disease, the mostimportant control measures are rapid culling of allinfected or exposed birds, proper disposal ofc a rcasses, the quarantining and rigoro u sdisinfection of farms, and the implementation ofstrict sanitary, or “biosecurity”, measure s .Restrictions on the movement of live poultry, bothwithin and between countries, are anotherimportant control measure. The logistics ofrecommended control measures are moststraightforward when applied to large commercialfarms, where birds are housed indoors, usuallyunder strictly controlled sanitary conditions, inlarge numbers. Control is far more difficult underpoultry production systems in which most birds areraised in small backyard flocks scattere dthroughout rural or periurban areas.
When culling - the first line of defence forcontaining outbreaks - fails or proves impracticable,vaccination of poultry in a high-risk area can beused as a supplementary emergency measure ,provided quality-assured vaccines are used andrecommendations from the World Organisation forAnimal Health (OIE) are strictly followed. The useof poor quality vaccines or vaccines that poorlymatch the circulating virus strain may acceleratemutation of the virus. Poor quality animal vaccinesmay also pose a risk for human health, as they mayallow infected birds to shed virus while stillappearing to be disease-free.
Apart from being difficult to control, outbreaksin backyard flocks are associated with a heightenedrisk of human exposure and infection. These birdsusually roam freely as they scavenge for food andoften mingle with wild birds or share water sourceswith them. Such situations create abundantopportunities for human exposure to the virus,especially when birds enter households or arebrought into households during adverse weather,or when they share areas where children play orsleep. Poverty exacerbates the problem: insituations where a prime source of food and incomecannot be wasted, households frequently consumepoultry when deaths or signs of illness appear inflocks. This practice carries a high risk of exposureto the virus during slaughtering, defeathering,butchering, and preparation of poultry meat forcooking, but has proved difficult to change.Moreover, as deaths of birds in backyard flocks arecommon, especially under adverse weatherconditions, owners may not interpret deaths orsigns of illness in a flock as a signal of avianinfluenza and a reason to alert the authorities. Thistendency may help explain why outbreaks in somerural areas have smouldered undetected formonths. The frequent absence of compensation tofarmers for destroyed birds further works against
the spontaneous reporting of outbreaks and mayencourage owners to hide their birds during cullingoperations.
The Role of Migratory BirdsDuring 2005, an additional and significant
source of international spread of the virus in birdsbecame apparent for the first time, but remainspoorly understood. Scientists are incre a s i n g l yconvinced that at least some migratory waterfowlare now carrying the H5N1 virus in its highlypathogenic form, sometimes over long distances,and introducing the virus to poultry flocks in areasthat lie along their migratory routes. Should thisnew role of migratory birds be scientificallyconfirmed, it will mark a change in a long-standingstable relationship between the H5N1 virus and itsnatural wild-bird reservoir.
The die-off of more than 6000 migratory birds,infected with the highly pathogenic H5N1 virus,that began at the Qinghai Lake nature reserve incentral China in late April 2005, was highly unusualand probably unprecedented. Prior to that event,wild bird deaths from highly pathogenic avianinfluenza viruses were rare, usually occurring asisolated cases found within the flight distance of apoultry outbreak. Scientific studies comparingv i ruses from diff e rent outbreaks in birds havefound that viruses from the most recently affectedcountries, all of which lie along migratory routes,are almost identical to viruses recovered from deadmigratory birds at Qinghai Lake. Vi ruses fro mTurkey’s first two human cases, which were fatal,w e re also virtually identical to viruses fro mQinghai Lake.
Countries Affected by Outbreaks in BirdsThe outbreaks of highly pathogenic H5N1 avian
influenza that began in south-east Asia in mid-2003and have now spread to a few parts of Europe, arethe largest and most severe on record. To date, nineAsian countries have reported outbreaks (listed inorder of reporting): the Republic of Korea, VietNam, Japan, Thailand, Cambodia, the Lao People’sDemocratic Republic, Indonesia, China, andMalaysia. Of these, Japan, the Republic of Korea,and Malaysia have controlled their outbreaks andare now considered free of the disease. Elsewhere inAsia, the virus has become endemic in several ofthe initially affected countries.
In late July 2005, the virus spread geographicallybeyond its original focus in Asia to affect poultryand wild birds in the Russian Federation andadjacent parts of Kazakhstan. Almost simultaneously,Mongolia reported detection of the highlypathogenic virus in wild birds. In October 2005, thev i rus was reported in Tu r k e y, Romania, and

WHO-Facts Sheet March 200674
Croatia. In early December 2005, Ukraine reportedits first outbreak in domestic birds. Further spreadof the virus along the migratory routes of wildwaterfowl is, however, anticipated. Moreover, birdmigration is a recurring event. Countries that liealong the flight pathways of birds migrating fromcentral Asia may face a persistent risk ofi n t roduction or re - i n t roduction of the virus todomestic poultry flocks.
Prior to the present situation, outbreaks ofhighly pathogenic avian influenza in poultry wereconsidered rare. Excluding the current outbreakscaused by the H5N1 virus, only 24 outbreaks ofhighly pathogenic avian influenza have beenre c o rded worldwide since 1959. Of these, 14occurred in the past decade. The majority haveshown limited geographical spread, a fewremained confined to a single farm or flock, andonly one spread internationally. All of the largeroutbreaks were costly for the agricultural sectorand difficult to control.
The Disease in HumansHistory and epidemiology: Influenza viruses are
normally highly species-specific, meaning thatviruses that infect an individual species (humans,certain species of birds, pigs, horses, and seals) stay“true” to that species, and only rarely spill over tocause infection in other species. Since 1959,instances of human infection with an avianinfluenza virus have been documented on only 10occasions. Of the hundreds of strains of avianinfluenza A viruses, only four are known to havecaused human infections: H5N1, H7N3, H7N7, andH9N2. In general, human infection with theseviruses has resulted in mild symptoms and verylittle severe illness, with one notable exception: thehighly pathogenic H5N1 virus.
Of all influenza viruses that circulate in birds,the H5N1 virus is of greatest present concern forhuman health for two main reasons. First, theH5N1 virus has caused by far the greatest numberof human cases of very severe disease and thegreatest number of deaths.
A second implication for human health, of fargreater concern, is the risk that the H5N1 virus - ifgiven enough opportunities - will develop thecharacteristics it needs to start another influenzapandemic. The virus has met all prerequisites forthe start of a pandemic save one: an ability tospread efficiently and sustainably among humans.While H5N1 is presently the virus of gre a t e s tconcern, the possibility that other avian influenzaviruses, known to infect humans, might cause apandemic cannot be ruled out.
Mechanism of TransmissibilityThe virus can improve its transmissibility
among humans via two principal mechanisms. Thefirst is a “reassortment” event, in which geneticmaterial is exchanged between human and avianviruses during co-infection of a human or pig.Reassortment could result in a fully transmissiblepandemic virus, announced by a sudden surge ofcases with explosive spread.
The second mechanism is a more gradualp rocess of adaptive mutation, whereby thecapability of the virus to bind to human cellsincreases during subsequent infections of humans.Adaptive mutation, expressed initially as smallclusters of human cases with some evidence ofhuman-to-human transmission, would pro b a b l ygive the world some time to take defensive action,if detected sufficiently early.
During the first documented outbreak of humaninfections with H5N1, which occurred in HongKong in 1997, the 18 human cases coincided with ano u t b reak of highly pathogenic avian influenza,caused by a virtually identical virus, in poultryfarms and live markets. Extensive studies of thehuman cases determined that direct contact withdiseased poultry was the source of infection.
All evidence to date indicates that close contactwith dead or sick birds is the principal source ofhuman infection with the H5N1 virus. Especiallyrisky behaviours identified include theslaughtering, defeathering, butchering andpreparation for consumption of infected birds. In afew cases, exposure to chicken faeces whenchildren played in an area frequented by free-ranging poultry is thought to have been the sourceof infection. Swimming in water bodies where thec a rcasses of dead infected birds have beendiscarded or which may have been contaminatedby faeces from infected ducks or other birds mightbe another source of exposure. In some cases,investigations have been unable to identify aplausible exposure source, suggesting that some asyet unknown environmental factor, involvingcontamination with the virus, may be implicated ina small number of cases. Some explanations thathave been put forward include a possible role ofperi-domestic birds, such as pigeons, or the use ofuntreated bird faeces as fertilizer.
At present, H5N1 avian influenza re m a i n slargely a disease of birds. The species barrier issignificant: the virus does not easily cross frombirds to infect humans. Despite the infection of tensof millions of poultry over large geographical areassince mid-2003, fewer than 200 human cases havebeen laboratory confirmed.

KUWAIT MEDICAL JOURNAL 75March 2006
Assessment of Possible CasesInvestigations of all the most recently confirmed
human cases, in China, Indonesia, and Turkey, haveidentified direct contact with infected birds as themost likely source of exposure. When assessingpossible cases, the level of clinical suspicion shouldbe heightened for persons showing influenza-likeillness, especially with fever and symptoms in thelower respiratory tract, who have a history of closecontact with birds in an area where confirmedo u t b reaks of highly pathogenic H5N1 avianinfluenza are occurring. Exposure to an environ-ment that may have been contaminated by faecesf rom infected birds is a second, though lesscommon, source of human infection. To date, not allhuman cases have arisen from exposure to dead orvisibly ill domestic birds. Research published in2005 has shown that domestic ducks can excretelarge quantities of highly pathogenic virus withoutshowing signs of illness. A history of poultryconsumption in an affected country is not a riskfactor, provided the food was thoroughly cookedand the person was not involved in foodp reparation. As no efficient human-to-humantransmission of the virus is known to be occurringa n y w h e re, simply travelling to a country withongoing outbreaks in poultry or sporadic humancases does not place a traveller at enhanced risk ofinfection, provided the person did not visit live or“wet” poultry markets, farms, or other enviro n m e n t sw h e re exposure to diseased birds may have occurre d .
Clinical FeaturesIn many patients, the disease caused by the
H5N1 virus follows an unusually aggre s s i v eclinical course, with rapid deterioration and highf a t a l i t y. Like most emerging disease, H5N1 influenzain humans is poorly understood. Clinical data fromcases in 1997 and the current outbreak are beginningto provide a picture of the clinical features ofdisease, but much remains to be learned. Moreover,the current picture could change given the pro p e n s i t yof this virus to mutate rapidly and unpredictably.
The Incubation Period The incubation period for H5N1 avian influenza
may be longer than that for normal seasonalinfluenza, which is around two to three days.C u r rent data for H5N1 infection indicate anincubation period ranging from two to eight daysand possibly as long as 17 days. However, thepossibility of multiple exposure to the virus makesit difficult to define the incubation period precisely.WHO currently recommends that an incubationperiod of seven days be used for fieldinvestigations and the monitoring of patientcontacts.
SymptomsInitial symptoms include a high fever, usually
with a temperature higher than 38 ºC, andinfluenza-like symptoms. Diarrhoea, vomiting,abdominal pain, chest pain, and bleeding from thenose and gums have also been reported as earlysymptoms in some patients. Watery diarrh o e awithout blood appears to be more common inH5N1 avian influenza than in normal seasonalinfluenza. The spectrum of clinical symptoms may,however, be broader, and not all confirmed patientshave presented with respiratory symptoms. In twopatients from southern Viet Nam, the clinicaldiagnosis was acute encephalitis; neither patienthad respiratory symptoms at presentation. Inanother case, from Thailand, the patient presentedwith fever and diarrhoea, but no re s p i r a t o r ysymptoms. All three patients had a recent history ofdirect exposure to infected poultry.
One feature seen in many patients is thedevelopment of manifestations in the lowerrespiratory tract early in the illness. Many patientshave symptoms in the lower respiratory tract whenthey first seek treatment. On present evidence,difficulty in breathing develops around five daysfollowing the first symptoms. Respiratory distress,a hoarse voice, and a crackling sound wheninhaling are commonly seen. Sputum production isvariable and sometimes bloody. Most re c e n t l y,blood-tinted respiratory secretions have beenobserved in Turkey. Almost all patients developpneumonia. During the Hong Kong outbreak, allseverely ill patients had primary viral pneumonia,which did not respond to antibiotics. Limited dataon patients in the current outbreak indicate thepresence of a primary viral pneumonia in H5N1,usually without microbiological evidence ofbacterial supra-infection at presentation. Turkishclinicians have also reported pneumonia as aconsistent feature in severe cases; as elsewhere,these patients did not respond to treatment withantibiotics.
In patients infected with the H5N1 virus, clinicaldeterioration is rapid. In Thailand, the timebetween onset of illness to the development ofacute respiratory distress was around six days, witha range of four to 13 days. In severe cases in Turkey,clinicians have observed respiratory failure three tofive days after symptom onset. Another commonf e a t u re is multiorgan dysfunction. Commonlaboratory abnormalities, include leukopenia(mainly lymphopenia), mild-to-moderatet h rombocytopenia, elevated aminotransferases,and with some instances of disseminatedintravascular coagulation.

WHO-Facts Sheet March 200676
Drugs Available for TreatmentLimited evidence suggests that some antiviral
drugs, notably oseltamivir (commercially known asTamiflu), can reduce the duration of viralreplication and improve prospects of survival,provided they are administered within 48 hoursfollowing symptom onset. However, prior to theo u t b reak in Tu r k e y, most patients have beendetected and treated late in the course of illness. Forthis reason, clinical data on the effectiveness ofoseltamivir are limited. Moreover, oseltamivir andother antiviral drugs were developed for thetreatment and prophylaxis of seasonal influenza,which is a less severe disease associated with lessprolonged viral replication. Recommendations onthe optimum dose and duration of treatment forH5N1 avian influenza, also in children, need tou n d e rgo urgent re v i e w, and this is beingundertaken by WHO.
In suspected cases, oseltamivir should beprescribed as soon as possible (ideally, within 48hours following symptom onset) to maximize itstherapeutic benefits. However, given the significantmortality currently associated with H5N1 infectionand evidence of prolonged viral replication in thisdisease, administration of the drug should also beconsidered in patients presenting later in the courseof illness.
Currently recommended doses of oseltamivirfor the treatment of influenza are contained in theproduct information at the manufacturer’s website. The recommended dose of oseltamivir for thetreatment of influenza, in adults and adolescents 13years of age and older, is 150 mg per day, given as75 mg twice a day for five days. Oseltamivir is notindicated for the treatment of children youngerthan one year of age.
As the duration of viral replication may beprolonged in cases of H5N1 infection, cliniciansshould consider increasing the duration oftreatment to seven to ten days in patients who arenot showing a clinical response. In cases of severeinfection with the H5N1 virus, clinicians may needto consider increasing the recommended daily doseor the duration of treatment, keeping in mind thatdoses above 300 mg per day are associated withi n c reased side effects. For all treated patients,consideration should be given to taking serialclinical samples for later assay to monitor changesin viral load, to assess drug susceptibility, and toassess drug levels. These samples should be takenonly in the presence of appropriate measures forinfection control.
In severely ill H5N1 patients or in H5N1patients with severe gastrointestinal symptoms,drug absorption may be impaired. This possibilityshould be considered when managing thesepatients.
Countries with Human Cases in the CurrentOutbreak
To date, human cases have been reported in sixcountries, most of which are in Asia: Cambodia,China, Indonesia, Thailand, Turkey, and Viet Nam(Tabl;e 1).
Table 1: Cumulative Number of Confirmed HumanCases of Avian Influenza A/(H5N1) Reported to WHO(February 2, 2006)
Country 2003 2004 2005 2006 Total
CasesDeaths Cases Deaths Cases DeathsCasesDeathsCasesDeaths
Cambodia 0 0 0 0 4 4 0 0 4 4
China 0 0 0 0 8 5 2 2 10 7
Indonesia 0 0 0 0 16 11 3 3 19 14
Iraq 0 0 0 0 0 0 1 1 1 1
Thailand 0 0 17 12 5 2 0 0 22 14
Turkey 0 0 0 0 0 0 12 4 12 4
Viet Nam 3 3 29 20 61 19 0 0 93 42
Total 3 3 46 32 94 41 18 10 161 86
Total number of cases includes number of deaths.
WHO reports only laboratory-confirmed cases.
Altogether, more than half of the laboratory-confirmed cases have been fatal. H5N1 avianinfluenza in humans is still a rare disease, but as e v e re one that must be closely watched andstudied, particularly because of the potential of thisvirus to evolve in ways that could start a pandemic.
For further information please contact the WHOMedia Centre, Tel.: (+41 22) 791 2222, Email:
2. WHO Calls for Global Action to Avert 8Million Cancer-related Deaths by 2015
Cancer is a leading cause of death globally: anestimated 7.6 million people died of cancer in 2005and 84 million people will die in the next 10 years ifaction is not taken. The World Health Organization(WHO) has proposed a global goal of reducingchronic disease death rates by 2% per annum from2006 to 2015. Achievement of this goal would avertover eight million of the projected 84 million deathsdue to cancer in the next decade. WHO is steppingup its response to meet this target.
More than 70% of all cancer deaths occur in low-and middle-income countries, where re s o u rc e savailable for prevention, diagnosis and treatment ofcancer are limited or nonexistent. Tobacco use aloneaccounts for some 1.5 million cancer deaths peryear.

KUWAIT MEDICAL JOURNAL 77March 2006
“ We must, first and foremost, address thetremendous inequalities between developed anddeveloping countries in terms of cancer prevention,treatment and care,” said Dr Catherine Le Galés-Camus, Assistant Dire c t o r-General forNoncommunicable Diseases and Mental Health,“Despite our knowledge that many cases areavoidable, or curable when detected early andtreated according to best evidence, sadly for manypeople tumours are detected too late and adequatetreatment is not available. Furthermore, the qualityof life of many patients with cancer can bei m p roved substantially by pain control andpalliative care.”
It is estimated that over 40% of all cancer can bep revented. However, dramatic increases in riskfactors such as tobacco use and obesity arecontributing to the rise in cancer rates, particularlyin low- and middle-income countries. A rapidlychanging global environment due to globalizationof markets and urbanization is leading to risingconsumption of processed foods high in fats, sugarsand salt, as well as tobacco products; decliningconsumption of fruit and vegetables; and moresedentary activity levels. As a consequence theburden (incidence) of cancer and other chronicdiseases is increasing. Other preventable riskfactors include many environmental carcinogensand infections caused by Hepatitis B Virus andHuman Papilloma Virus.
WHO advocates an integrated approach top revention, treatment and care for all leadingc h ronic diseases. Integrated approaches thatcombine cancer prevention, diagnosis,management with that for heart disease, stroke,diabetes and other chronic diseases are necessarybecause the diseases share common risk factors(tobacco use, unhealthy diet and physicalinactivity) and require similar responses from thehealth system. Not only is the integrated approachbest for prevention and treatment, it is also cost-effective. This approach is outlined in the recentlyreleased report, “Preventing chronic diseases: avital investment”.
For more information contact:Ms AlexandraMunro, Communication Officer, Department of
Chronic Diseases and Health Promotion,WHO/Geneva, Telephone: +41 22 791 50 53, Mobilephone:+41 79 754 77 63, E-mail: [email protected]
3. CANCER
What Is Cancer?Cancer is a generic term for a group of more
than 100 diseases that can affect any part of thebody. Other terms used are malignant tumours andneoplasms. One defining feature of cancer is therapid creation of abnormal cells which gro wbeyond their usual boundaries, and which caninvade adjoining parts of the body and spread toother organs, a process referred to as metastasis.Metastases are the major cause of death fro mcancer.
Facts About CancerCancer is a leading cause of death worldwide.
From a total of 58 million deaths worldwide in2005, cancer accounts for 7.6 million (or 13%) of alldeaths. The main types of cancer leading to overallcancer mortality are:
l lung (1.3 million deaths/year);l Stomach (almost 1 million deaths/year);l Liver (662,000 deaths/year);l Colon (655,000 deaths/year) andl Breast (502,000 deaths/year).More than 70% of all cancer deaths in 2005
o c c u r red in low and middle income countries.Deaths from cancer in the world are projected tocontinue rising, with an estimated nine millionpeople dying from cancer in 2015 and 11.4 milliondying in 2030.
The most frequent cancer types world wide are:l Among men (in order of number of global
deaths): lung, stomach, liver, colore c t a l ,oesophagus and prostate.
l Among women (in order of number of globaldeaths): breast, lung, stomach, colorectal andcervical.
Quick Cancer Factsl 40% of cancer can be prevented (by a healthy
diet, physical activity and not using tobacco).l Tobacco use is the single largest preventable
cause of cancer in the world. Tobacco use causescancer of the lung, throat, mouth, pancre a s ,bladder, stomach, liver, kidney and other types;Environmental tobacco smoke (passive smoking)causes lung cancer.
l One-fifth of cancers worldwide are due tochronic infections, mainly from hepatitis B virusesHBV (causing liver), human papilloma viru s e sHPV (causing cervix), Helicobacter pylori (causingstomach), schistosomes (causing bladder), the liverfluke (bile duct) and human immunodeficiencyvirus HIV (Kaposi sarcoma and lymphomas).

WHO-Facts Sheet March 200678
What Causes Cancer?Cancer occurs because of changes of the genes
responsible for cell growth and re p a i r. Thesechanges are the result of the interaction betweengenetic host factors and external agents which canbe categorized as:
l physical carcinogens such as ultraviolet (UV)and ionizing radiation
l chemical carcinogens such a asbestos andtobacco smoke
l biological carcinogens such asq infections by virus (Hepatitis B Virus and liver
cancer, Human Papilloma Virus (HPV) and cervical cancer) and bacteria (Helicobater pylori and gastric cancer) and parasites (schistosomiasis and bladder cancer)
q contamination of food by mycotoxins such as aflatoxins (products of A s p e rgillus fungi) causing liver cancer.
Tobacco use is the single most important riskfactor for cancer and causes a large variety of cancertypes such as lung, larynx, oesophagus, stomach,bladder, oral cavity and others . Although there arestill some open questions, there is suff i c i e n tevidence that dietary factors also play an importantrole in causing cancer. This applies to obesity as acompound risk factor per se as well as to thecomposition of the diet such as lack of fruit andvegetables and high salt intake. Lack of physicalactivity has a distinct role as risk factor for cancer.T h e re is solid evidence about alcohol causingseveral cancer types such as oesophagus, pharynx,larynx, liver, breast, and other cancer types.
How Does Cancer Develop?Cancer arises from one single cell. The
transformation from a normal cell into a tumourcell is a multistage process, typically a progressionfrom a pre-cancerous lesion to malignant tumours.The development of cancer may be initiated byexternal agents and inherited genetic factors.Ageing is another fundamental factor for thedevelopment of cancer. The incidence of cancerrises dramatically with age, most likely due to riskaccumulation over the life course combined withthe tendency for cellular repair mechanisms to beless effective as a person grows older.
How Can the Burden of Cancer be Reduced ?The existing body of knowledge about the
causes of cancer and about interventions to preventand manage cancer is extensive. Cancer control isunderstood as public health actions which areaimed at translating this knowledge into practice. Itincludes the systematic and equitableimplementation of evidence-based strategies forcancer prevention, early detection of cancer and
management of patients with cancer.l Up to one third of the cancer burden could be
reduced by implementing cancer pre v e n t i n gstrategies which are aimed at reducing theexposure to cancer risk mainly by:
q changes in tobacco and alcohol use, anddietary and physical activity patterns
q immunization against HPV infectionq the control of occupational hazardsq reducing exposure to sunlightl Another third of the cancer burden could be
cured if detected early and treated adequately.q Early detection of cancer is based on the
observation that treatment is more effective whencancer is detected earlier. The aim is to detect thecancer when it is localized. There are twocomponents of early detection programmes forcancer:
u Education to promote early diagnosis by recognizing early signs of cancer such as: lumps, sores, persistent indigestion, persistent coughing, and bleeding from the body’s orifices; and the importance of seeking p rompt medical attention for these symptoms.
u Screening is the identification by means of tests of people with early cancer or pre-cancer before signs are detectable. Screening tests areavailable for breast cancer (Mammography) and Cervical cancer (Cytology tests).
l Treatment of cancer is aimed at curing,prolonging life and improving quality of life ofpatients with cancer. Some of the most commoncancer types such as breast cancer, cervical cancerand colorectal cancer have a high cure rate whendetected early and treated according to bestevidence. The principal methods of treatment ares u rg e r y, radiotherapy and chemotherapy.Fundamental for adequate treatment is an accuratediagnosis by means of investigations involvingimaging technology (ultrasound, endoscopy,radiography) and laboratory (pathology).
l Relief from pain and other problems can beachieved in over 90% of all cancer patients bymeans of palliative care. Effective strategies existfor the provision of palliative care services forcancer patients and their families, even in lowresource settings.
WHO’s Strategy for Prevention and Control ofCancer
Following the adoption of a Cancer Preventionand Control Resolution at the 58th WHA on May2005, WHO is developing the Global WHO CancerControl Strategy. The Strategy aims at reducing thecancer burden and cancer risk factors as well as

KUWAIT MEDICAL JOURNAL 79March 2006
improving the quality of life of patients and theirfamilies worldwide by means of planning andimplementing cancer prevention and contro lstrategies. It is integrated into the overall WHOchronic disease prevention and control frameworkof the Department of Chronic Diseases and HealthPromotion. The cancer control strategy is based onthe following guiding principles:
l P e o p l e - c e n t e red: the ultimate goal is toimprove the well-being of the people, communities,families and individuals.l Equity: the strategy focuses on the needs of
low-and middle-income countries and ofvulnerable and marginalized populations.
l Ownership: the strategy guarantees the strongcommitment and active involvement of keystakeholders in each stage of the decision-makingprocess and implementation.l Partnership and multisectoral approach: the
strategy ensures the wide participation andcollaboration of all sectors: public and private,l Sustainability: the strategy emphasizes the
need for national governments and partnerscollectively strive for financial and technical self-reliance, to ensure the continuation of benefits fromestablished programmes after major assistance hasbeen completed.
l Integration: the strategy is embedded withinthe overall framework of chronic diseaseprevention and control and other related areas(such as environmental health, communicablediseases, etc).l Stepwise approach: the strategy considers the
implementation of interventions, at a national orsub-national level, in a sequential manner.
l Evidence-based: the strategy is based onresearch results, programme evaluation, economicanalysis, best practice, and lessons from countries.
WHO, in cooperation with its cancer researchagency, the International Agency for Research inCancer (IARC), and other organizations of theUnited Nations system, will provide the leadershipfor international cancer prevention and control andwill develop the following actions:
lAdvocacy and political commitment for cancerprevention and control
l Generation of new knowledge and dissemin-ation and diffusion of existing knowledge tofacilitate the application and programme deliveryof evidence-based approaches to cancer control
l Development of standards and tools forguiding effective cancer control planning andimplementation of evidence-interventions forp revention, early detection, treatment andpalliative care
l Facilitating the development of multisectoralnetworks of cancer control partners at the global,regional and national levels
l Building capacity for developing andimplementing effective policies and programmesand strengthening health systems
l Provision of technical assistance for the rapid,effective and efficient translation of evidence-basedcancer control interventions into public healthpolicies and programmes in developing countries
For more information contact: WHO Media centreTelephone: +41 22 791 2222 E-mail: