A guide to developing and implementing overdose prevention programs

of 34
Transcript of A guide to developing and implementing overdose prevention programs
-
8/2/2019 A guide to developing and implementing overdose prevention programs
1/34
A guide to
By Jaa Aaa ad Daha Och
2012
developing and implementingoverdose
preventionprograms
-
8/2/2019 A guide to developing and implementing overdose prevention programs
2/34
2
Eurasian Harm Reduction Network
Te mission o Eurasian Harm Reduction Network (EHRN) is to promote humane, evidence-based harm reduc-
tion approaches to drug use, with the aim o improving health and protecting human rights at the individual,
community, and societal level.
Founded in 1997, the Eurasian Harm Reduction Network (EHRN) unites over 340 members rom 29 countries
o Eastern and Central Europe and Central Asia (ECECA). Our members include harm reduction organisations,communities o people using drugs and/or living with HIV, drug treatment services, HIV-service organisations,
governmental institutions, researchers and experts. EHRN is governed by its members through a Steering Com-
mittee; with a Secretariat based in Vilnius (Lithuania).
EHRN relies on ECECA best practices in the sphere o harm reduction, drug policy reorm, HIV/AIDS, tuberculo-
sis, Hepatitis C and overdose prevention. EHRN works toward its mission through documentation and advocacy;
technical assistance and training; inormation and networking. Te primary goal is to advocate or non-discrim-
inatory, harm reduction-oriented drug policies, and improve the quality and range o harm reduction services in
the region.
Postal address: Svitrigailos St. 11B, Vilnius 03228, Lithuania
elephone: +370 5 269 1600
Fax: +370 5 269 1601
E-mail: [email protected]
Website: www.harm-reduction.org
Eurasian Harm Reduction Network, 2012. Citing the source is necessary when using parts o this publication.
Please contact EHRN or permission i you wish to use the entire publication.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
3/34
3
Authors
Janna Ataiants, Dasha Ocheret
Translator
Katya Smirnova
Editing
Matt Curtis
Design and layout
Design: Donaldas Andziulis, Ex Arte
Layout: Birute Vilutiene, Ex Arte
Ex Arte, Lithuania
Donors
Financial support or this publication was provided by Open Society Foundations. Te views expressed herein are
those o the authors and in no way reect the opinions/policies o the donor.
Acknowledgements
Te authors would like to thank the team o experts rom Georgia, Kazakhstan, Russia, ajikistan and Ukraine or
making this publication possible: Ketevan Bidzinashvili, Alloudin Boimatov, Yelena Borzunova, Anatoliy Volik,
Yulia Gorbunova, Nino Janashia, Saltanat Egeubaeva, Valentina Zhuravleva, Natalya Kitsenko, Andrey Mandebura,
Lyubov Nechaeva, Natalia Sidorenko, Dali Usharidze.
Suggested citation
Eurasian Harm Reduction Network (EHRN). A guide to developing and implementing overdose prevention pro-
grams. Vilnius, 2012.
Te publication is available at www.harm-reduction.org .
-
8/2/2019 A guide to developing and implementing overdose prevention programs
4/34
4
Co
INRODUCION ........................................... ........................................... ............................................ ............................... 5
I. SRAEGIC ISSUES .......................................... ........................................... ............................................ ........................ 7
Conduct situation assessment ....................................... ............................................ ............................................ ......... 7
Analyse legal ramework or the provision o naloxone ....................................... ............................................ ......... 7Garner support rom potential project partners ..................................... ............................................ ........................ 9
II. PLANNING ......................................... ............................................ ........................................... ..................................... 11
Choose a model or procurement, storage and distribution o naloxone ....................................... ...................... 11
Prepare or sta training and individual consultations ......................................... ............................................ ....... 14
Develop inormational materials .......................................... ........................................... ............................................ 18
Determine how many rst-aid kits are needed ....................................... ............................................ ...................... 19
Add technical support components ............................................ ........................................... ..................................... 21
Develop the projects advocacy strategy ..................................... ........................................... ..................................... 22
Make a budget ............................................ ........................................... ............................................ ............................. 23
III. MONIORING AND EVALUAION ....................................... ........................................... ..................................... 25
Document cases o naloxone administration .......................................... ............................................ ...................... 25
Monitor impact indicators ...................................... ............................................ ........................................... ............... 26
CONCLUSION ......................................... ............................................ ........................................... ..................................... 27
BIBLIOGRAPHY ..................................... ............................................ ........................................... ..................................... 28
ANNEXES .......................................... ............................................ ........................................... ............................................ 30ANNEX 1. Naloxone distribution models in six countries ......................................... ............................................ 30
ANNEX 2. Outcomes o overdose prevention pilot projects ...................................... ............................................ 32
ANNEX 3. Quantity and quality indicators o overdose prevention programme eectiveness ........................ 34
-
8/2/2019 A guide to developing and implementing overdose prevention programs
5/34
5
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
iodco
Tis Guide was developed in response to the growing need among service providers working with drug users
in Central and Eastern Europe and Central Asia to introduce overdose prevention work into their services. What
any organization working with drug users knows rom experience, and what has been conrmed by numerous
scientic studies in USA, Western Europe and Australia, is that overdose is a major cause o death among their
clients.1
It is nearly impossible to obtain reliable ocial data on the numbers o overdoses atal or non-atal or the
region. Foreign studies ound that at least two-thirds o injecting opiate users had experienced an overdose in their
lietime, with approximately 4 out o 100 overdose cases having a lethal outcome. 2 At the same time, ocial sta-
tistics in the region registers disproportionally low gures o atal overdoses3, which brings governments attention
away rom the problem. Funding is not being allocated to overdose prevention, medical services are insucientlyequipped with naloxone (a highly eective antidote to opioid overdose), and naloxone is only poorly available i
at all in local pharmacies.
While the governments hesitate to lead targeted responses to lower overdose mortality in their countries, non-
governmental organizations and medical acilities initiated their own pilot responses to the issue. In total, about 90
projects now work in six countries o the region (Georgia, Kazakhstan, Kyrgyzstan, Russia, ajikistan and Ukraine)
to provide access to naloxone and improve rst-aid overdose prevention skills.
In this Guide, we have summarized best regional practices to oer a useul tool to non-governmental organi-
zations working with people who use drugs and willing to expand their services and introduce overdose preven-
tion. Here you will nd a set o concise recommendations on overdose programming based on lessons learned
rom colleagues in the region. You will also nd sources o additional inormation on various issues o overdoseprevention, as well as annexes with an overview o rst pilot results that can guide you in planning, implementa-
tion and monitoring o your project.
But beore we get into some suggestions or starting and operating overdose prevention projects, there is one
thing we would like to stress: Just Do It. Its helpul to do surveys and ocus groups to determine how big a prob-
1 For the review o research on overdose as the leading cause o death among injecting drug users in dierent countries see Con P,Sherman S, & Curtis M, 2010.
2 Con P: Overdose: a major cause o preventable death in Central and Eastern Europe and Central Asia, 2008.3 For example, in Ukraine, with its estimate number o IDUs ranging rom 230 500 to 361 000 people (Reerence Group to the United
Nations on HIV and Injecting Drug Use, 2008), only 203 deaths rom poisoning due to psychoactive substance use were registeredin 2008 (according to the Ukrainian Monitoring Centre on Drug Use).
-
8/2/2019 A guide to developing and implementing overdose prevention programs
6/34
6
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
lem overdose is in your community. But 100% o harm reduction groups already see people in need o overdose
services. Naloxone is an incredibly valuable, lie-saving tool. But i you dont have it today, its a missed opportunity
not to still teach someone about rescue breathing and other rst aid skills. Money or projects is important, but
there are millions o positive steps that can be taken beore you get unding. So just do it. You have the power to
reduce the toll o overdose deaths in your community, and now is the time to use it.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
7/34
7
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
i. sac
A quality overdose prevention program requires a solid oundation. First o all, you should assess the urgency
o the issue in your city or district, analyses the legal ramework o naloxone provision, and garner support rom
potential project partners.
Conduct situation assessment
It should be your rst step: evaluate the urgency o the overdose problem in your target group in your city or
local area. Consider conducting a mini-assessment to answer three core questions:What are the drugs most commonly used (the drug scene) and what causes overdoses?
What is the ocial and not ocial statistics on atal and non-atal overdoses in your city/area?
Is medical attention or overdoses timely and adequate?
You can obtain ocial statistics on overdoses in the ollowing governmental services:
Municipal healthcare department;
Ambulance and rst-aid service;
Intensive care units in hospitals;
oxicological units in hospitals and poison-control centers;
Drug treatment acility;
Forensic examination bureau;AIDS Centre;
Law enorcement statistic services.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
8/34
8
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
You can collect data on overdose causes and the quality o medical aid, as well as alternative data on the
number o overdoses in your area through a survey among outreach workers, volunteers and clients. Ask them, in
particular:
What types o drugs are currently used in your area, how ofen, how are they administered, what is the
dose?
How would you describe the current dynamics o the situation with overdoses: more cases, less cases, orwhat reason?
How many people known to you died rom overdose in a certain period o time?
How ofen are ambulances sent or overdose, how ofen they arrive, what kind o medical help they o-
er?
What do drug users know about naloxone? Can it be purchased in pharmacies? Will it be in demand?
Tis mini-survey will help you generate valuable inormation to be used towards meeting the ollowing
objectives:
Getting hold o inormation that will assist you in rationalizing the urgency o your project in a grant
proposal;
Focusing your program on actual needs o the target group;
Obtaining baseline data or urther evaluation o project impact on the situation with overdoses at the
stage o monitoring and evaluation.45
4 Detailed inormation about this and other sources mentioned in the Additional Inormation boxes you can nd in the Bibliogra-phy chapter below.
5 , ., , ., , ., ., , . (2011). , 20082011 . : . : http://esvero.ru/les/model_prolaktiky_web.pd
nOte:
I you are not able to obtain overdose statistics online or through personal visits to institutions, try
sending out ofcial data requests. Legal regulations in many countries require governmental structuresto respond to ofcial inquiries by citizens over a certain period o time (usually one month).
ADDitiOnAl inFOrmAtiOn:
eHrn doc icdc ad ccac o jc d odo (2009) ca a a
xa o ao a.4 th doc bhd np esverO dcaoa aa th
od o odo o ad ca aa (A. Ca ad co-aho, 2011, .48-56).5
-
8/2/2019 A guide to developing and implementing overdose prevention programs
9/34
9
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Analyze legal ramework or the provision o naloxone
I your needs assessment showed that opiate overdose is an urgent issue or your target group, you should
explore ways o providing your clients with access to naloxone a highly eective antidote to acute opioid
poisonings. For that, you will need to conduct another mini-research: to identiy the legal status o naloxone inyour country, its availability in pharmacies and legal possibilities or your organization to provide naloxone.
Most ofen, naloxone has the status o a prescribed drug. Access to naloxone is ofen limited: its either in
temporary stock at pharmacies, or not available at all due to lack o demand, or is available only in big pharmacies
or in capital cities.
You should also study the legal framework for the provision of naloxone in your country, its possibilities and
limitations. In many countries o the ormer Soviet Union, an NGO with no medical or pharmaceutical license and
without a special status o research organization cannot purchase, store or distribute naloxone. You will have to
establish connections with organizations and specialists having such a license or status.
Practice shows that regardless o the legal status o naloxone in a given country, NGOs have been able to
organize legal ways to distribute naloxone in their communities. In places where prescriptions or other specialconditions are required, this is ofen accomplished through agreements between harm reduction projects and
medical institutions or pharmacies that can provide sta to write prescriptions or otherwise support the project
(or details see the section on Planning). When in doubt, try checking with an existing overdose project in your
country about how they do it, or consult a lawyer or experts with international organizations working in your
country.
ADDitiOnAl inFOrmAtiOn:
vw th a a o aoxo h ra Fdao by h Caada Hiv/AiDs la nwok,odcd o q o h ra Ha rdco nwok ( ra).
-
8/2/2019 A guide to developing and implementing overdose prevention programs
10/34
10
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Garner support rom potential project partners
Beore you start detailed project planning, dene the potential partner organizations. Tese could include
governmental acilities where you obtained ocial statistics on overdoses, pharmacies or naloxone distributors,and medical agencies, other harm reduction groups, or likeminded organizations that can help you carry out the
project.
At the preparation stage, organize meetings with
potential partners, tell them about the project, exchange
contact inormation, secure their support. Tis type o
cooperation has an added value: it will improve the
overall signicance o the project.
Use ndings o pilot overdose prevention projects to establish cooperation with specic structures:
Medical personnel
Ifnaloxoneisaprescriptiondruginyourcountry,involveanarcologistorother
medical doctor who is allowed to prescribe it to project clients. It may be useulto sign an agreement with an institution rather than individual doctors in orderto increase the number o people who can write prescriptions and the times atwhich prescriptions can be made.
Ambulance andrst-aid services
Conducttrainingonoverdosesforambulanceparamedicstoraisetheirmotivation to promptly respond to emergency calls and promote tolerantattitude towards drug users.
FromexperienceoftheTomsk-AntiSPIDfoundation(Russia),youshouldinorm ambulance sta about the project beore it starts and afer it ends,
as this inormation will be very useul or doctors.
Law enorcementbodies
Ifyouareplanningtodistributenaloxonedirectlytodrugusers,trygettingsupport rom the local law enorcement bodies.
FromexperienceofNGOAiperon(Tajikistan),itshelpfultoconducttrainingsor round tables or representatives o law enorcement to explain the purposeo the project, that naloxone is not a narcotic drug, and that project participantsposses naloxone legally.
nOte:
Faa odo a ha ay
a ch o coaoa o o
dco ak coad o oh ha
dco a, ho h ojc
ky o c o o w a, ch
a d coo c o ca hahca
da.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
11/34
11
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
ADDitiOnAl inFOrmAtiOn:
Fo dad dco o h kd o od wh xa o ojc h o, Ax 1.
ii. pa
Afer you conducted a situation assessment in your city, studied the legal ramework or prescribing naloxone
and ound project partners, its time to plan you project in detail. You need to choose a model o naloxone provision,
train sta, make a checklist o rst-aid supplies, develoip training outlines, prepare inormational materials, dene
technical support needs, sharpen advocacy strategies and make a budget.
Choose a model or procurement, storage and distribution
o naloxone
As noted above, there is no one right way to carry out an overdose project, but you should think careullyabout the model(s) you want to introduce. Some examples rom existing projects include models:
Based on harm reduction NGOs and linked to syringe exchange and other community-based services;
Based on pharmacies and medical services as a means o complimenting services delivered by harm
reduction groups;
Based on emergency services, in order to increase the availability o naloxone in ambulances and train
emergency personnel to deliver overdose education.
You will need to select the model o naloxone provision depending on your countrys legislation. Remember,
however, that evidence and practice demonstrate that distribution o overdose education and naloxone directly
to people who use opioids through low-threshold programs is the most efective method o preventing atal
overdoses.
Below you will nd inormation on how harm reduction organizations in Russia, Ukraine and Georgia,
having chosen the low-threshold model o naloxone provision, organized procurement, storage and distribution
procedures in their countries.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
12/34
12
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Procurement:
In situations where naloxone is not widely available in pharmacies, or has a limited availability, you should
purchase the medication either directly rom a producing company or through a distributor. I you are not able
to purchase large quantities o naloxone without medical or pharmaceutical licenses, sign an agreement with a
pharmacy or a trusted medical organization (such as AIDS Centre or drug treatment acility) that will arrangeprocurement o naloxone or your project.
Storage:
I you are able to store naloxone at your oce, there is one simple rule to ollow: keep naloxone out o
light and at regular room temperature. Doing so will prolong its shel lie. Usually, this means that simply storing
naloxone in its original packaging in a regular storage closet is ne.
Rules about storage o naloxone at non-medical organizations vary rom country to country. In some places
in EECA, or example, small quantities o naloxone (e.g. up to 500 ampules) may be stored in oce premises or a
period o one month. You should consult with local medical proessionals, a lawyer, or other experts to determine
the rules in your country.In EECA, larger quantities o naloxone are ofen stored in warehouses o a acility that orders its supplies (e.g.
pharmacy warehouse, drug storage in AIDS Centre or drug treatment center). I naloxone is purchased by one
organization, stored at another, and then distributed by a harm reduction group, it is usually necessary to sign an
agreement between the harm reduction project, procuring organization and storage acility.
Distribution:
You can distribute naloxone afer group or
individual training in the oce, at a mobile needle
exchange, at a hired training acility or the homes o
people who use drugs. Naloxone can be given out inexchange or a prescription provided by the doctor
partnering with your project. I naloxone is distributed
during outreach work, you should be aware laws that
may restrict how much o the medication may be
carried by an individual. Laws regarding medication
administration usually allow possession o small
quantities or personal use. Tese laws and regulations,
however, most ofen dont stipulate the exact amounts,
but it is likely that having one package o naloxone
ampoules will not be a problem, especially i pharmacies
dont sell it per ampoule. In Ukraine, or example,
outreach workers can legally carry around naloxone,
which is documented in a cooperation agreement with
ambulance service.
nOte:
e hoh aoxo dbo hoh
haac o h o c way o
odo ao h o ab
d , h ojc ca c o
haac ( aoxo aaab h)
ao wh h o oh
aoxo o . Fo xa, Haaa
Aco chay odao (s. pb,
ra) o aoxo co o
ho ojc c who a ha hy a
ab o by h.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
13/34
13
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Sometimes drug users are reluctant to carry
naloxone, earing that i searched by police, its
possession will provoke detention and subsequent drug
tests. Clearly explain to your clients what the law is, that
they should not be detained or possessing naloxone,and that i they are then they should report the incident
to the project or ollow-up. Overdose projects also have
a responsibility to try to minimize the potential or
clients to be harassed or arrested or participating, or
example by educating police, advocating or local police
orders to not interere with the project, and including
a card in each naloxone kit that briey explains the
project and gives contact inormation or the providing
organization.
nOte:
to iaoa Fodao (nabzhy
Chy, ra) c a ahco o ha aod h ck. th co
ca hod wo aoxo ao, ad hy
do daw cay ao ad k
h dcao o bak.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
14/34
14
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Prepare or staf training
and individual consultations
Quality training or sta and clients is key to the success o an overdose prevention project. While we provide
a short explanation o how to organize trainings here, or much more inormation please see the Open SocietyFoundations manual on Overdose Prevention and Response and EHRNs overdose training module (links to both
are included in the Useul Literature section at the end o this guide).
At the training preparation stage, take the ollowing steps:
Invite expert trainers or preliminary sta training. Dene what types o additional technical support in
conducting training and consultations you will need, and include them in the technical support plan and
budget (or details see section Add technical support components o this chapter).
rain all outreach workers and doctors you plan to involve in trainings and individual counseling. I
possible, train also volunteers and all sta that are in contact with the target group.
Develop a training agenda or use an existing one.
Make a checklist o necessary equipment and training materials:
manikin,
multimedia projector,
ipchart and markers,
notebooks and pens,
handout materials (brochures or instruction sheets),
naloxone ampoules or rst-aid kits.
nOte:
Wh hod a o a, h dc bw axo ad aoxo
(naca). naxo a d d ay acoho ad ood ddc aa,
wha aoxo d o a ac oa oo ad odo.
nOte:ex o h oow oazao ca h yo wh yo a: eaa Ha rdco
nwok, O socy Fodao, AiDs Fodao ea-W, mdc d mod Fac,
aoa ha dco aocao, a w a Ha rdco Coao ad Chcao rcoy
Aac.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
15/34
15
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Dene your target audiences. Tese can include:active drug users,
drug users in remission,
close ones o drug users (parents, spouses, partners, relatives or riends living together with drug
users),
sta and clients o rehabilitation centres,
medical workers,
law enorcement ocers,
ocials and decision makers.
Select location, dene training regularity and duration.
You can plan both in-oce and on-site trainings.
Sta trainings should be held at least once a year; trainings or the target group at least once a
month.
No more than 10-15 participants per group.
Hold short-lasting trainings or active drug users and longer ones or other audiences.
nOte:
You will need a manikin to develop and strengthen the skills of the closed-chest cardiac massage.
i yo oazao cao cha o, oa a h oca rd Co a oc o
a dca co.
Its handy to have two manikins: a stationary one (weighs about 20 kilos) for oce trainings
ad a oab o (abo 4 ko) o o- a.
The Tomsk Anti-AIDS foundation (Russia) uses a more expensive, but also a better alternative
o a ak: a ha- ad ba cao a dc (h max ), whch
a a oo o h Cpr k.
nOte:
The Tomsk Anti-AIDS foundation (Russia) holds trainings for active drug users, sta and clients
o habao c, dca a o h oa tB hoa ad h ca hoa
(da o co coo, y ad hac).
The Renaissance project (Kazakhstan) conducts trainings for drug using spouses.
The Timor Islamova foundation (Naberezhnye Chelny, Russia) conducts educational sessions for
d d a -a , h , a w a a ho ad cook ab.
A drug treatment clinic in Simferopol (Ukraine) provides training to nursing sta of the clinic and
c o h bo oa.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
16/34
16
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
I you dont have a possibility to hold a group training, consider conducting individual consultations another
proven educational tool to provide this type o inormation.
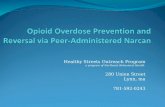
You can train drug users and give out naloxone in several possible locations (see Chart at page 14).Dont orget to distribute inormation sheets and several naloxone ampoules among all training partici-
pants!
ADDitiOnAl inFOrmAtiOn:
Odo a ada aaab a h wb o h eaa Ha rdco nwok
(h://www.ha-dco.o/hb/kowd-hb/h-a-od/ ), a w a h d
by m. C ad l. ga: Odo o ad o (2009, .87-93).
nOte:
Haaa Aco chay odao (s. pb, ra) oaz h y o a
o d adc:
15-30-minute trainings for active drug users, where all participants receive a brochure with
a oao;
2-3-hour trainings for volunteers, people in rehabilitation or remission;
4-6-hour trainings for healthcare workers with a special session on drug addiction.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
17/34
17
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Sites where drug users can be reached
TRAININGand
NALOXONE
Street-based
At homesor
cooking labs
AIDS Centres
As part
o drug
treatment
Rehabilitation
centres
Substitution
therapy
programmes
Harmreduction
project
oce
Harm
reduction
bus / mobile
unit Rehabilitation
afer
prison
-
8/2/2019 A guide to developing and implementing overdose prevention programs
18/34
18
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Develop inormational materials
You will need at least a short inormation sheet describing causes and signs o an overdose, as well as rst-
aid actions. It would also be good to have a detailed brochure on overdoses and hand it out during trainings orhealthcare workers.
You can adapt existing materials to your projects needs or use already developed materials.
Dene what types o technical support you will need to develop materials, and include them in the technical
support plan and budget (or details see section Add technical support components o this chapter).
ADDitiOnAl inFOrmAtiOn:
so xa o oaoa aa ha ca b d yo odo o ojc:
Oa odo ad sa odo (AiDs Fodao ea-W; d by np esverO 2011); Odo o ad o (m. C, l. ga, 2009).
-
8/2/2019 A guide to developing and implementing overdose prevention programs
19/34
19
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Determine how many rst-aid kits are needed
First o all, you should decide what to include in the rst-aid kits that you will distribute among project clients.
At a later stage, this will be a separate item in your budget.
Suggested minimum contents o an overdose rst-aid kit:At least 2 ampoules o naloxone;
At least one syringe or each ampule o naloxone. Ideally, syringes should be at least 1ml (2ml is better)
and have xed (not detachable) needles. Needles must be or intramuscular injection, which are longer
than needles commonly used or injecting heroin or other drugs;
Alcohol swabs;
Inormation on basic overdose prevention and rst aid techniques, including how to diagnose an over-
dose, do rescue breathing, and use naloxone;
A card or other printed material that briey explains the project and includes contact inormation or your
organization, in case the client in stopped by police.
o determine the amount o naloxone your project will need, consider the ollowing actors:Local drug scene (the project will need large quantities o naloxone i the drug in demand is injecting
heroine or some new drug that ofen causes overdoses: in this case you might get more clients willing
to get training and naloxone);
Client coverage (at the start, your overdose prevention project may attract similar amounts o clients your
organization usually gets, but as soon as the target group sees the eect o naloxone, you may see the raise
in both recurrent demand or the medication and the number o new clients);
Te number o ampoules per person at a time (ofen its two 1ml ampoules).
nOte:
Humanitarian Action (St. Petersburg) gives out at least 3 ampoules of naloxone per person. There
a chac ha a c bak o o o, o ha cocad by oc. Bd, aoh
odo ay occ a ho a aoxo add, o h cod ao ay
b dd.
Tomsk-AntiAIDS charity (Russia) hands out 2-3 ampoules to drug users, 2 ampoules to relatives
ad d a a ad 20 ao o oa aa qd by d
.
nOte:
Haaa Aco (s. pb) o a a 3 ao o aoxo o.
th a chac ha a c bak o o o, o ha cocad by oc. Bd, aoh
odo ay occ a ho a aoxo add, o h cod ao ay
b dd.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
20/34
20
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
From experience o overdose prevention pilot projects in Russian cities with a population o about hal a
million people, you may need up to 400 ampoules a month i heroin use is dominant at the drug scene.
nOte:
rb o y oach wok wh aoxo o b d ca hy w a odo.
e yo aa aoxo ca oy b cbd by a doco, oach wok a aowd o
cay 2-3 ao. thy cao b chad o ocd o oo o aoxo o oa
, a aoxo o a cood d ( o cdd h o acoc, ychooc o
o d).
-
8/2/2019 A guide to developing and implementing overdose prevention programs
21/34
21
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Add technical support components
Since overdose prevention programs are new to your organization, make special provisions or technical
support in the structure o your project. Te scale o technical support needs and proportion o the budget you
will allocate to this project component will vary depending on the experience and capacity o your organization,but some things that other organizations have ound helpul include:
Expert support in overdose-related situation assessment;
Expert site-visits to provide counseling at the launch o the program; support in talking with decision
makers and conducting round tables or workshops with potential partner organizations;
Support in conducting trainings or uture trainers rom among outreach workers;
Development o training agenda on overdose prevention or the target group, healthcare workers, law
enorcement ocers;
Expert support to improve availability o naloxone, including its registration, import and availability in
pharmacies, as well as its inclusion into the list o essential medicines;
Legal assistance related to the status o naloxone and development o legal schemes o naloxone provisionthrough outreach workers;
Consultations to adjust the project at the implementation stage (or example, changing project design ol-
lowing shifs at the drug scene);
Support in project monitoring and evaluation;
Expert assistance to document project results and successes;
Support in the development o an advocacy strategy.
nOte:
You can get technical support from such organizations as Eurasian Harm Reduction Network,O socy Fodao, poao sc iaoa, AiDs Fodao ea-W, unODC
(adocacy ) ad aoa ha dco aocao, ch a np esverO (ra).
-
8/2/2019 A guide to developing and implementing overdose prevention programs
22/34
22
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Develop the projects advocacy strategy
Since you may be new to overdose prevention activities, your advocacy activities will probably be centered
around local-level initiatives that may include:
Round tables or healthcare departments, law enorcement bodies and other external partners to inormthem about project objectives at the start-up stage, and present results and successes afer the project;
Documenting project successes and distributing related inormation;
Recording absence o naloxone in rst-aid kits o medical acilities providing services to drug users (drug
treatment acilities, B clinics, inectious hospitals, AIDS Centres in-patient wards);
raining medical and non-medical sta rom governmental healthcare services on issues o rst aid to
respond to drug overdoses as part o work aimed at expanding overdose prevention initiatives and en-
couraging tolerant attitudes o health workers towards drug users;
Round tables or meetings with drug treatment specialists to raise their motivation to prescribe naloxone
to patients o drug treatment clinics;
Campaigns on prescribing naloxone through cooperation with project-riendly narcologists and pharma-cies;
Facilitating inclusion o overdose prevention issues in advanced training programs or healthcare sta, as
well as in municipal drug use and HIV/AIDS prevention programs.
nOte:
i h ya o h odo o ojc:
NGO Novy Put (New Way Tbilisi, Georgia) and Altay Public Organization Vybor (Choice Biysk,
ra) obad o o cha aoxo o h bd o h goba Fd a, hoh h cha had o b ad h a ooa;
Timor Islamova Foundation (Naberezhnye Chelny, Russia) and drug treatment clinic of Chapayevsk
(ra) w ab o o cy ad cac o h ojc h co o od ab
wh oca da o h Fda D Coo sc;
Xenon Association (Zugdidi, Georgia) received high appraisal of their naloxone distribution
ac d a wok wh a o abac c who od
dcad o odo cy ca ad odo-ad oay;
Drug treatment clinic in Simferopol (Ukraine) secured the inclusion of Harm Reduction section
(wh odo o coo) h dy cc o d- hahca wok; In Bishkek (Kyrgyzstan), the proportion of referrals from the pilot overdose prevention project to
oa d a ac cad o 2% o 13%.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
23/34
23
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Make a budget
While most costs associated with overdose prevention projects are quite small and there are ofen many things
that can be done with your existing resources, there are costs or which you will need to budget. I the overdose
project is well integrated with your other services, it is unlikely, or example, that you would need new sta re-sources. On the other hand, purchasing naloxone (and to a lesser extent other basic supplies) can be a signicant
cost, especially or small organizations.
Te ollowing is an example o a possible budget structure or an overdose prevention project. Remember that
ew projects will require all o these expenses, and that you should adapt your budget planning to match with your
own needs and available resources.
nOte:
Budget a maximum estimated amount of naloxone, as you would not want to run out of it in
ca h a dd fow o c o h ao cha a h d c. naoxo ca
b od o h ya, o w o x.
Take into account all possible distribution channels: to participants of awareness sessions and
dda coao; hoh oach wok ad a d xcha o; hoh
acoo ad doco-co.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
24/34
24
A guide to developing And implementing
overdose prevention progrAms
BUDGET SECTION ITEM DETALISATION
Staf salaries (part-time) Coordinator (outreach-manager)Outreach workersConsultant-neurologistLawyerAccountant
First-aid supplies NaloxoneSyringesSterile wipes or rescue breathingAlcohol swabsZipper bags (plastic or other)
Trainings Trainers ees (or staf trainings)ManikinRental ees or training acility and multimedia projector or on-site trainingsCofee-break expenses
Flipchart, markers, notebooks, pens
Technical support Tickets, accommodation, travelling allowance or expertsExperts ees
Advocacy activities Rental ees or acility to conduct round tablesCofee-break expensesStationery
Monitoring and evaluation Experts eesPrint and copy costs o interview orms, questionnaires, ocus-group andin-depth interview protocols
Inormational materials Obtaining/printing/copying inormational materials
Administrative costs Costs related to brokers contracts on procurement and storage o naloxone
-
8/2/2019 A guide to developing and implementing overdose prevention programs
25/34
25
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
iii. moo ad aao
Its important to monitor and evaluate overdose prevention programs or at least two reasons: to adjust the
provision o services and streamline advocacy activities. Basic program monitoring requires keeping track o at
least our indicators:
dominating drugs and practices o use;
number o distributed naloxone ampoules and number o people who received naloxon;
number o people trained in rst-aid skills to manage overdoses;
number o naloxone-administration events in response to overdoses.
Document cases o naloxone administration
An important tool o monitoring overdose preven-
tion programs is to record cases o naloxone adminis-
tration and related circumstances. Tese real-lie cases
will not only provide you with statistics on the saved
lives, but also deliver quality inormation about shifs at
the drug scene, rst-aid skills o drug users and charac-
ter o response rom medical services.
nOte:
A good time to put down stories of your
c abo o hy ad wod
b wh hy co back o q w
ao. Ak h o dcb w
how hy d h o ock.
Discuss these stories with outreach workers
d wky wh a oach
aa.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
26/34
26
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Monitor impact indicators
I you are just about to start an overdose prevention program, or advocacy purposes it should be enough to
monitor one impact indicator: number o naloxone-administration events in response to overdoses . Tis target
alone will have a signicant value when you promote the program among donors, decision makers and healthcarecommunity.
Facts and gures collected in the process o project monitoring will be much more convincing i you had
conducted a detailed situation assessment beore the project (see the rst section o the Strategic Issues chapter)
and continue tracking the same targets in the course o project implementation. 6
6 , ., , ., , ., ., , . (2011). , 20082011 . : . : http://esvero.ru/les/model_prolaktiky_web.pd
ADDitiOnAl inFOrmAtiOn:
See Annex 2 for a list of indicators of existing pilot programs with examples from dierent countries.
See Annex 3 for a list of indicators for in-depth monitoring of overdose prevention responses. Check out outcomes of an overdose prevention pilot in Kyrgyzstan in a publication by Zh. Bakirova:
rdc ood odo oay ao ac d (2010).
S. Tsarevs research study Cost eectiveness of opiate-related overdose deaths: case study of a
o ojc h ow o Chaayk, saaa o o ra (2011) whch wa bhd np
esverO dcaoa aa: th od o odo o ad ca aa (A. Ca
ad co-aho, 2011, . 30-32)6
-
8/2/2019 A guide to developing and implementing overdose prevention programs
27/34
27
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
i a ha i d h a: id a coao o a oo o
aoxo. i ad h o aady!
O a a h a o a
ho ad w a b, h a.
sod bah. W ad h o
h ac, d c bah ad ha
aa. i dd wok, o w h ac
dow h ow ad cad a abac,
ad o o w o aoxo o
a oach wok a h ho, a w
dd ha ay wh . W jcd h
o ao h hod, h coo
d, ad h h adak. Abac ca. th h
wa aoh d who i hd: jcd
aoxo o h a ad wachd
h co back o h , b y owy.
so i jcd aoh 1 , ad h wok
day. Dd h hak.
Ad aoh i ad wh aoxo.
so w c o , ad a! i
oo aoxo, hy wod a b dad.
Coco
Introducing overdose prevention services in the structure o your organization requires careul preparation,
establishment o partnerships with other organization and consolidated eort o your project team. But your work
will make an invaluable impact in the end.
Overdose prevention activities will be in demand
among clients o your organization. Drug users are al-
ways interested to learn about rst-aid techniques and
naloxone administration to respond to an overdose.
Overdose prevention will be the most appreciated
task or outreach workers, who will eel their impor-
tance and gladly be saviours o other people.
Moreover, these initiatives will give you unique op-
portunities to engage in a dialogue with local authori-
ties and strengthen position o your organization. Your
eorts to save peoples lives will be met with under-
standing and sympathy rom ocials; they will reduce
the number o overdose emergency calls to ambulance
services, and improve statistics on overdose deaths or
law enorcement agencies. Like no other aspect o harm
reduction strategies, the goal o overdose prevention is
one o the heaviest arguments in avor o continuing
and expanding harm reduction activities in general.
Most importantly, soon afer you start prevent-
ing overdoses and gathering eedback rom clients, you
will see with your own eyes how eective and impor-
tant your work actually is. Below you will nd a real-
lie story sent by a project client rom omsk (Russia).
Please read it, and expect to get many more success
stories o your own.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
28/34
28
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Bboahy
, , : : 12
. : ; 2011.
: . 2010. [
.]
: .
-; 2006. http://www.harmreduction.ru/les/vssv_peredozirovka_narkotikami.pd
: . -
. ; 2009.[ [email protected]]
: ; 2010. http://www.harm-reduction.org/ru/images/
stories/library/od_hiv_ru.pd
, ., , ., , ., ., , . (2011).
,
20082011 . :
. : http://esvero.ru/les/model_prolaktiky_web.pd
/, : -
. ; 2008. [ LyubovN@
harmreduction.ru]
: -
. , , , . : -
; 2008. http://www.harm-reduction.org/images/stories/library/od_report_2008_ru.pd
, : . -
. (IHRD), -
. 2001 ( IHRD 2002 .). :
. : . , . , . . -; 2004:33-80. http://www.aidslex.
org/site_documents/DR-0131R.pd
, : .
. ; 2008. -: /. ; 2011.
http://esvero.ru/publications_bro.shtml
-
8/2/2019 A guide to developing and implementing overdose prevention programs
29/34
29
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
: , ,
. . . ; 2011, 1:13-15.
:
: . : .
, . : , , . . . - : / ; 2008, 2:5-9. http://www.aidsalliance.org.ua/
ru/library/our/naloxon/pd/naloxon.pd
Con P, Sharman S, Curtis M: Underestimated and overlooked: A global review o drug overdose and overdose prevention. Global
State of Harm Reduction 2010. Key issues for broadening the response. Ed. By Catherine Cook. International Harm Reduction Associa-
tion; 2010:113-119 http://www.aidslex.org/site_documents/DR-0198E.pd
Grau LE, Green C, orban M, Blinnikova K, Krupitsky E, Ilyuk R, Kozlov AP, Heimer R: Psychosocial and contextual correlates o
opioid overdose risk among drug users in St. Petersburg, Russia. Harm Reduction Journal;2009, 6:17. http://www.harmreductionjour-
nal.com/content/6/1/17
PSI Research & Metrics: HIV and B RaC study evaluating risk behaviors associated with HIV transmission and utilization oHIV prevention and HIV/B co-inection prevention among IDUs. PSI Social Marketing Research Series; 2010. http://www.psi.org/
resources/publications
PSI Research Division: Russia (2009): Overdose Prevention Study o Injecting Drug Users (IDUs) in
Ekaterinburg and St. Petersburg, Te Russian Federation. 1 Round. PSI RaC Summary Report; 2009. http://www.psi.org/research/
cat_socialresearch_smr.asp
-
8/2/2019 A guide to developing and implementing overdose prevention programs
30/34
30
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Ax
ANNEX 1.
Naloxone distribution models in six countries 7
1. HARM REDUCTION PROGRAMMES
Place odistribution
Country Distribution scheme Special requirements
Fixed-site NEPs7,outreach, medical
acilities, reha-bilitation centres,homes o drugusers, harm reduc-tion bus
Russia(Naberezhnye
Chelny, omsk,St. Petersburg)
Purchased through medical acilitieshaving medical/pharmaceutical license,
or through pharmacies. Stored partlyin medical acilities (AIDS Centre,inectious hospital, drug treatmentcentre), partly at the xed-site NEP.Given out at NEP, through street andmobile outreach, in medical acilities, athomes o drug users.
Given out to IDUs or theirrelatives afer special training or
drug consultation in exchange ora prescription.
Fixed-site NEP Russia (Elista) Purchased and stored in AIDS Centre.Given out at NEP based in AIDSCentre.
Given out to IDUs or theirrelatives in exchange or aprescription.
Fixed-site NEPs Ukraine (some
o projects)
Purchased by projects at
pharmaceutical companies or medicinedistributors. Stored at NGO oceacilities. Given out at xed-site NEPs.
Given out afer special training or
drug consultation in exchange ora prescription.
Fixed-site NEPsand prison-basedNEP
Kyrgyzstan Purchased by the Republican Drugreatment Centre, stored or most partin a pharmacies, distributed to NEPsat their request and then stored intheir lockboxes. In the penal system itsdistributed to the medical service thatsends it along to NEP.
In xed-site NEPs given outtogether with an originalprescription, in the penal system without a prescription.
7 Needle exchange programs
-
8/2/2019 A guide to developing and implementing overdose prevention programs
31/34
31
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
Fixed-site NEPs,outreach, mini-groups o drugusers
Georgia Purchased by projects in pharmacies,stored in NGO acilities. Distributedamong IDUs through xed-site NEPs,outreach and mini-groups o drug
users.
Given out afer mini-trainingwithout a prescription.
2. SPECIALISED MEDICAL SERVICES AND PHARMACIES
Place odistribution
Country Distribution scheme Special requirements
Drug treatmentacility
Russia(Chapayevsk)
Purchased, stored and given out bydrug treatment acility.
Given out to IDUs (mostly IDUswith low rehabilitation potential) ortheir relatives afer training or drugconsultation without a prescription.
Ukraine(Simeropol)
A naloxone kit is given out (i theacility can purchase it), or just aprescription.
Given out or sold in pharmacy onprescription ollowing individualdrug counselling.
AIDS Centre Kazakhstan(Renaissanceproject andSocial bureauDoverie)
Purchased though the Global HealthResearch Centre in Central Asia andsent to the AIDS Centre, where it isstored and distributed. Clients getprescriptions (vouchers) to obtainnaloxone at the AIDS Centre afertraining in the Renaissance project orSocial bureau Doverie, both havingtheir oces based on the premises othe AIDS Centre.
A naloxone kit is given out inexchange or a voucher afer aguidance session at the AIDSCentre. Te Renaissance projectvouchers are valid only or projectclients; Social bureau Doverievouchers are valid or all IDUs.
Intensive care units
o district hospitals
ajikistan
(NGOAiperon)
Purchased by the Global Fund
upon agreement with ajikistansgovernment on procurement omedicines and equipment as part othe harm reduction programme. Tendistributed to the NGO ree o charge.Stored in intensive care units, ollowinga tripartite agreement between theNGO, GF and hospitals. Prescription isgiven out by social workers afer mini-training at the xed-site NEP.
Given out upon reerral rom NGO
Aiperon.
Pharmacies Ukraine (someo the projects)
Purchased and stored in pharmacy. Given out ree o charge onprescription.
3. PROVIDING NALOXONE TO EMERGENCY SERVICES
Place odistribution
Country Distribution scheme Special requirements
Ambulance servicestation, intensivecare unit o theregional hospital
ajikistan(NGOVolonter(Volunteer)
Purchased by the Central pharmacyupon agreement with NGO, storedat ambulance service station andintensive care unit o the regionalhospital. Administered by doctors.
Not given out to IDUs.
Ambulance servicestation
Ukraine (someo the projects)
Purchased by NGO, distributed toambulance service and stored there.
Administered by doctors.
Not given out to IDUs.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
32/34
32
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
ANNEX 2.
Outcomes o overdose prevention pilot projects8
IMPACT ON DRUG USERS AND THEIR FAMILIES
Indicator Example
Reducing requency ooverdoses and overdosemortality
Georgia, Zugdidi: At a work meeting with NGO Xenon, representatives romthe ambulance service reported a sharp decrease in overdose emergency calls andoverdose deaths. Tis decrease, they stated, was the result o naloxone distribution bythe Xenon project.
Russia, Chapayevsk: As a result o project implementation, the number o ocialcases o overdose deaths in 2009 reduced twice compared to 2008 (rom 37 to 18),while in 2010 only one atal heroin overdose was registered.
Russia, Naberezhnye Chelny: Trough project activities, according to data rom thedrug treatment acility, the number o atal overdoses reduced rom 33 cases in 2007
to 4 cases in 2008. Te number o overdose emergency calls reduced rom 251 in 2008to 113 within 9 months o 2009.
Tajikistan, Khorog: Over the ve years o NGO Volonter project implementation(rom 2006 to 2010), ocial overdose cases in Gorno-Badakhshan AutonomousRegion were reduced 40-old (rom 245 in 2006 to 6 in 2010); ocially recordedoverdose atalities reduced 13.5-old: rom 27 in 2006 to 2 in 2010.
Tajikistan, Khatlon region: In one year o project implementation by NGO Aiperon(2009-2010), a total number o overdoses in three discricts o the region reduced4-old, while the amount o atal overdoses dropped 7-old. Only in the rst twomonths o 2011 our lives were saved.
Strengthening overdose-
related rst-aid skills
Kyrgyzstan, Bishkek: A survey among pilot project clients in Kyrgyzstan (2009)
demonstrated an increase in the proportion o those who administered naloxone tomanage an overdose (rom 1% at baseline survey to 19% at repeated survey), as well asa decrease in the percentage o people who administered intravenous saline solutions(rom 30% to 5% respectively).
Increasing demand ornaloxone
Russia, Chapayevsk and Tomsk: In the course o the project, increase in the recurrentdemand or naloxone was registered.
Tajikistan, Khatlon region: Over three years o project activities, naloxone be-came a popular medicine among IDUs and co-dependent people (relatives, amilymembers, etc.).
IMPACT ON COMMUNITY IN GENERAL
Indicator Example
Cost efectiveness Russia, Chapayevsk: An annual economic impact o the given average o preventedatal opiate overdoses in Chapayevsk is 9.8 times higher than costs o relatedprevention activities, which proves the projects cost-eectiveness and undingrationale.
8 Original o this Annex was published in the report by J. Ataiants, A. Latypov and D. Ocheret Overdose: situation overview andresponse in 12 countries o Eastern Europe and Central Asia, 2011.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
33/34
33
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
IMPACT ON HEALTHCARE WORKERS
Indicator Example
Introducing overdose
prevention componentsinto training curricula orhealthcare staf
Russia, Tomsk: raining activities on overdose prevention or medical personnel
in the city were approved by the Regional Healthcare Department and endorsedas part o the municipal training curriculum.Ukraine, Simeropol: Te Harm Reduction training section with its overdose pre-vention component was introduced into the study curriculum or mid-level healthcareworkers.
Improved readiness onarcologists to prescribenaloxone
Russia, NP ESVERO: Due limited availability o naloxone at the nal stages oRussian projects in 2010, trusted narcologists, at their own initiative, started pre-scribing naloxone to their patients who had suered rom an overdose.
More tolerant attitude toIDUs among healthcareworkers
Russia, Chapayevsk and Elista: A more tolerant attitude towards IDUs rom thepart o ambulance sta was reported as one o naloxone training eects.
IMPACT ON HARM REDUCTION PROGRAMMES
Indicator Example
Scaling up positive imageand trust towards harmreduction programmes,increasing the number oHR project clients
Russia, NP ESVERO: Both IDUs and regional authorities / medical acilitiesrespond with higher levels o trust to harm reduction projects; theres an inowo new clients to the projects. In omsk, the project received positive appraisalsrom medical personnel and the media. In Chapayevsk, the Federal Drug ControlService recognised the projects urgency and eectiveness. In Elista, project datawere presented by the Minister o Health o the Kalmyk Republic at the meetingo the Committee against Drugs.
-
8/2/2019 A guide to developing and implementing overdose prevention programs
34/34
A guiDe tO DevelOping AnD implementing
OverDOse preventiOn prOgrAms
ANNEX 3.
Quantity and quality indicators o overdose prevention program efectiveness
QUANTITY INDICATORS QUALITY INDICATORS
Number o naloxone administration events to managean overdose (surveys of outreach workers, volunteers,recurrent clients)
Improved overdose-response rst-aid skills amongdrug users and their relatives (questionnaire amongparticipants of trainings and consultations: pre and postevaluation, surveys of recurrent clients, records of successstories and saved lives)
Increased coverage o new and recurrent projectclients (client registry book)
Increased tolerance o ambulance service workerstowards drug users (surveys of project clients andambulance sta, surveys of recurrent clients, recordsof success stories and saved lives)
Increased demand or naloxone among drug usersand their relatives (naloxone distribution registry)
Introducing overdose prevention into advanced trainingprograms or healthcare workers
Reduced levels o overdose mortality in the city/area(local statistics on overdose mortality and acute drugpoisonings, surveys of outreach workers and volunteers)
Improved readiness o narcologists to prescribenaloxone (surveys of clients and narcologists at the initialand nal stages of the project)
Reerring overdose project clients to medical services:drug treatment acilities, rehabilitation centres, Band inectious hospitals, AIDS Centres (outreachworker reports, database of medical services)
Cost eectiveness (evaluation of project costscompared to averted harm from premature overdosemortality)