A fainting case in a fm clinic
28
A fainting case in a FM clinic Dr Aaron LEE Fook Kay NTWC Resident Family Medicine & Primary Care Unit
Transcript of A fainting case in a fm clinic

A fainting case in a FM clinic
Dr Aaron LEE Fook KayNTWC Resident
Family Medicine & Primary Care Unit

A 20 year old lady with major depressive disorder Regular FU in FM Clinic Accompanied by her mother who stated that
her daughter had taken 25 of the patient’s antidepressant tablets 2 hours earlier
The patient was alert and feel fainting with only slight abnormalities in vital signs
These include pulse of 125 bpm, and RR at 28 per minute. Bowel sounds are hypoactive

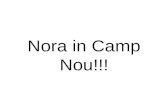
ECG changes ECG showed a sinus tachycardia and QRS
duration of 0.10 seconds Ipecac was given by mouth and emesis
contained some pill fragments The patient was closely observed for the next
2 hours in the FMC and sent to AED by ambulance because of semi-consciousness

At AED BP 90/ 60 mmHg P= 120 bpm GCS- 12/ 15 The patient was closely observed for the next
4 hours in the Emergency Department During this time, she slowly improved and was
awake, alert and able to walk unassisted to the washroom

In Medical ward She was then (3:30 am) transferred to the
medical ward for further evaluation All vital signs were now approximately normal At 5 am, a MO examined her and noted that
her speech was slurred, her gait unsteady and she was fearful, agitated and hallucinating
Another ECG was performed


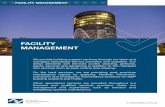
ECG now… Wide complex tachycardia (WCT), Right Axis
Deviation (RAD), hidden p wave in ST/ T complex (best seen II, aVF);
terminal R wave in aVR> 3mm. R/S ratio in aVR. 0.7;
atypical RBBB in V1-2 (Bizzare morphology with taller L rabbit ear)


What is the diagnosis? Tachycardia, wide QRS Terminal 40 ms, RAD presenting as a R wave
in lead aVR; R wave typically > 3 mm in this particular drug overdose

Final outcome During the following 2 hours, her vital signs
collapsed with respirations becoming labored, blood pressure dropping precipitously, and pulse become irregular
Despite efforts at cardiopulmonary resuscitation, she was certified dead at 6 am, 11 hours after ingestion of the drug

What was the drug which caused this woman’s death? a) Amitriptyline b) Acetaminophen c) Fluoxetine (Prozac) d) Digoxin

Answer is (a) This is a diagnostic dilemma because the
patient’s presentation is very unusual. An important point is that the drug was identified by the mother was an anti-depressant. This allows us to rule out digoxin and acetaminophen as possible causes
Of the remaining 2, the former is relatively benign & would be under less suspicion than amitriptyline, a drug that causes many deaths

There are a number of case reports that patients who have improved significantly after a TCA poisoning & then abruptly reversed course with marked increase in symptom severity

What is the expected lethal plasma level of TCA? a) > 15 ng/ mL b) >100 ng/ mL c) > 1000 ng/ mL d) > 10,000 ng/ mL

Answer is (c) Case reports show that plasma level greater
than 1000 ng/ mL have been correlated with seizure, coma, arrhythmias, cardiac arrest, and death

Specific levels Plasma level of some of the TCA can be
measured by clinical laboratories Therapeutic concentration are usually less
than 0.3 mg/L (300 ng/ mL) Total concentrations of parent drug plus
metabolite of 1 mg/ L (1000 ng/ mL) or greater are usually associated with serious poisoning
In general, QRS interval & clinical manifestations are reliable indicators of toxicity

Why was there a fluctuating course for this patient’s clinical presentation? a) TCA is known to be absorbed very slowly b) TCA takes days to become effective c) In overdose the anticholinergic effects of
TCA slow absorption from the gut d) none of the above

Answer is (c) Among the toxic effects of TCA ,
anticholinergic activity is one of the earliest to occur
This inhibition of nerve transmission across cholinergic synapses include GI peristalsis
Therefore, it makes sense that the presence of TCA would slow its own absorption

How can we rule out a second dose of TCA while the patient was in hospital? a) Drug unavailable to the patient b) She was under constant observation c) This drug is known to display this kind of
behaviour d) All of the above

Answer is (d) In view of the dramatic change in this
patient’s disease course, which occurred after she appeared to be improving, it is logical to suspect that she took a second dose of TCA
This was doubted in this case as the patient was closely watched & was dressed in a hospital gown in which she could not hide any drugs
It is, therefore, reasonable to assume that all of her symptoms were related to the original dose

Which are common signs of TCA overdose? a) Tachycardia b) Agitation c) Seizures and coma d) All of the above e) none of the above

Answer is (d) The major problem with TCA is that they are
not sufficiently specific They interfere with many different
neurotransmitters Thus,3 major organ systems are affected: the
Autonomic Nervous System, the Central Nervous System and cholinergic neurons

TCA poisoning TCA exerts its major toxicity via Na channel
blockade and anti-cholinergic effect Toxicity is expected within 6 hours after
ingestion, usually within 1-2 hours in significant poisoning, including cardiac toxicity, CNS toxicity and anti-cholinergic toxidrome
Cardiac toxicity, in form of hypotension and tachyarrhythmia, is the major concern
QRS duration in ECG predicts the probability of seizure(1/3 > 100ms) and ventricular arrhythmia (1/2 > 160ms)
Clinical worsening can be rapid and lethal

TCA poisoning Anti-cholinergic toxidrome (- atropine effect) -Blind as a bat (pupil dilatation) -Red as a beet (flushed skin) -Hot as a hare (hyperthermia secondary to
lack of sweat) Dry as a bone (dry mucous membrane)

Mx of TCA poisoning Ensure ABC intensive monitoring; consider
early intubation and hyperventilation GI decontamination with gastric lavage and
activated charcoal 1 g/ kg within 1-2 hr post-ingestion
1st-line treatment of arrhythmia: NaHCO3 Avoid Ia (Procainamide) & Ic (Flecanide)
antiarrhythmics, B-blockers & Amiodarone as may worsen hypotension & conduction abnormalities

Endpoint of Tx Early serum alkalization by NaHCO3 using
width of QRS as guide for therapeutic endpoint
Endpoint of serum alkalization: QRS < 100 ms, pH – 7.55 and Na <150 mmol/l
Treat hypotension with crystalloid & inotropic infusion; treat seizure with benzodiazepine

Q&A

The End