A Dual Closed-loop Control System For
19
A DUAL CLOSED-LOOP CONTROL SYSTEM FOR MECHANICAL VENTILATION Fleur Tehrani, PhD, 1 Mark Rogers, BS, RCP, RRT, 2 Takkin Lo, MD, 3 Thomas Malinowski, BS, RCP, RRT, 2 Samuel Afuwape, PhD, 2 Michael Lum, BS, RCP, RRT, 2 Brett Grundl, RCP, RRT, 2 and Michael Terry, RCP, RRT 2 From the 1 Department of Electrical Engineering, California State University, Fullerton, CA 92831, U.S.A., 2 Department of Respi- ratory Care, and the 3 Medical Intensive Care Unit, Loma Linda University Medical Center, Loma Linda, CA 92354, U.S.A. Received 14 May, 2003, and in revised form 10 Feb, 2004. Accepted for publication 20 Feb, 2004. Address correspondence to F.T. Tehrani, College of Engineering and Computer Science, California State University, Fullerton, P.O. Box 6870, Fullerton, CA 92834-6870, U.S.A. E-mail: [email protected] Tehrani F, Rogers M, Lo T, Malinowski T, Afuwape S, Lum M, Grundl B, Terry M. A dual closed-loop control system for mechanical ventilation. J Clin Monit 2004; 18: 111–129 ABSTRACT. Objective. Closed-loop mechanical ventilation has the potential to provide more effective ventilatory support to pa- tients with less complexity than conventional ventilation. The purpose of this study was to investigate the effectiveness of an automatic technique for mechanical ventilation. Methods. Two closed-loop control systems for mechanical ventilation are com- bined in this study. In one of the control systems several physiolog- ical data are used to automatically adjust the frequency and tidal volume of breaths of a patient. This method, which is patented under US Patent number 4986268, uses the criterion of minimal respiratory work rate to provide the patient with a natural pattern of breathing. The inputs to the system include data representing CO 2 and O 2 levels of the patient as well as respiratory com- pliance and airway resistance. The I : E ratio is adjusted on the basis of the respiratory time constant to allow for effective emp- tying of the lungs in expiration and to avoid intrinsic positive end expiratory pressure (PEEP). This system is combined with another closed-loop control system for automatic adjustment of the inspired fraction of oxygen of the patient. This controller uses the feedback of arterial oxygen saturation of the patient and combines a rapid stepwise control procedure with a proportional- integral-derivative (PID) control algorithm to automatically ad- just the oxygen concentration in the patient’s inspired gas. The dual closed-loop control system has been examined by using me- chanical lung studies, computer simulations and animal experi- ments. Results. In the mechanical lung studies, the ventilation controller adjusted the breathing frequency and tidal volume in a clinically appropriate manner in response to changes in respira- tory mechanics. The results of computer simulations and animal studies under induced disturbances showed that blood gases were returned to the normal physiologic range in less than 25 s by the control system. In the animal experiments under steady-state conditions, the maximum standard deviations of arterial oxy- gen saturation and the end-tidal partial pressure of CO 2 were ±1.76% and ±1.78 mmHg, respectively. Conclusion. The con- troller maintained the arterial blood gases within normal limits under steady-state conditions and the transient response of the system was robust under various disturbances. The results of the study have showed that the proposed dual closed-loop technique has effectively controlled mechanical ventilation under different test conditions. KEY WORDS. Mechanical ventilation, closed-loop control, work of breathing, multiple data feedback, oxygen. INTRODUCTION In the past few decades there have been many advances in mechanical ventilators to enhance their features and make them more responsive to individual patient’s needs. But Journal of Clinical Monitoring and Computing 18: 111–129, 2004. C 2004 Kluwer Academic Publishers. Printed in the Netherlands
-
Upload
estefa-tavera-velez -
Category
Documents
-
view
14 -
download
1
description
A Dual Closed-loop Control System For
Transcript of A Dual Closed-loop Control System For
-
A DUAL CLOSED-LOOP CONTROL SYSTEM FORMECHANICAL VENTILATIONFleur Tehrani, PhD,1 Mark Rogers, BS, RCP, RRT,2
Takkin Lo, MD,3 Thomas Malinowski, BS, RCP, RRT,2
Samuel Afuwape, PhD,2 Michael Lum, BS, RCP, RRT,2
Brett Grundl, RCP, RRT,2 and Michael Terry, RCP, RRT2
From the 1Department of Electrical Engineering, California StateUniversity, Fullerton, CA 92831, U.S.A., 2Department of Respi-ratory Care, and the 3Medical Intensive Care Unit, Loma LindaUniversity Medical Center, Loma Linda, CA 92354, U.S.A.
Received 14 May, 2003, and in revised form 10 Feb, 2004. Acceptedfor publication 20 Feb, 2004.
Address correspondence to F.T. Tehrani, College of Engineering andComputer Science, California State University, Fullerton, P.O. Box6870, Fullerton, CA 92834-6870, U.S.A.E-mail: [email protected]
Tehrani F, Rogers M, Lo T, Malinowski T, Afuwape S, Lum M,Grundl B, Terry M. A dual closed-loop control system for mechanicalventilation.
J Clin Monit 2004; 18: 111129
ABSTRACT. Objective. Closed-loop mechanical ventilation hasthe potential to provide more effective ventilatory support to pa-tients with less complexity than conventional ventilation. Thepurpose of this study was to investigate the effectiveness of anautomatic technique for mechanical ventilation. Methods. Twoclosed-loop control systems for mechanical ventilation are com-bined in this study. In one of the control systems several physiolog-ical data are used to automatically adjust the frequency and tidalvolume of breaths of a patient. This method, which is patentedunder US Patent number 4986268, uses the criterion of minimalrespiratory work rate to provide the patient with a natural patternof breathing. The inputs to the system include data representingCO2 and O2 levels of the patient as well as respiratory com-pliance and airway resistance. The I :E ratio is adjusted on thebasis of the respiratory time constant to allow for effective emp-tying of the lungs in expiration and to avoid intrinsic positiveend expiratory pressure (PEEP). This system is combined withanother closed-loop control system for automatic adjustment ofthe inspired fraction of oxygen of the patient. This controlleruses the feedback of arterial oxygen saturation of the patient andcombines a rapid stepwise control procedure with a proportional-integral-derivative (PID) control algorithm to automatically ad-just the oxygen concentration in the patients inspired gas. Thedual closed-loop control system has been examined by using me-chanical lung studies, computer simulations and animal experi-ments. Results. In the mechanical lung studies, the ventilationcontroller adjusted the breathing frequency and tidal volume ina clinically appropriate manner in response to changes in respira-tory mechanics. The results of computer simulations and animalstudies under induced disturbances showed that blood gases werereturned to the normal physiologic range in less than 25 s bythe control system. In the animal experiments under steady-stateconditions, the maximum standard deviations of arterial oxy-gen saturation and the end-tidal partial pressure of CO2 were1.76% and 1.78 mmHg, respectively. Conclusion. The con-troller maintained the arterial blood gases within normal limitsunder steady-state conditions and the transient response of thesystem was robust under various disturbances. The results of thestudy have showed that the proposed dual closed-loop techniquehas effectively controlled mechanical ventilation under differenttest conditions.
KEY WORDS. Mechanical ventilation, closed-loop control, work ofbreathing, multiple data feedback, oxygen.
INTRODUCTION
In the past few decades there have been many advances inmechanical ventilators to enhance their features and makethem more responsive to individual patients needs. But
Journal of Clinical Monitoring and Computing 18: 111129, 2004.C 2004 Kluwer Academic Publishers. Printed in the Netherlands
-
112 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
despite all these advances, most ventilators are mainly open-loop control devices. The added features of ventilators thathave enhanced their flexibility have also contributed totheir complexity.
Closed-loop ventilators can offer many advantages topatients as well as clinicians. These machines have the ca-pability of providing more effective and flexible ventilatorytreatment to patients with less complexity than traditionalmechanical ventilators. The idea of closing the loop in me-chanical ventilators is not new and a number of researchershave presented different closed-loop techniques for thesemachines since the mid 1950s [113]. In most of the tech-niques presented, however, only one variable, either thevolume of expired CO2 or the end-tidal partial pressureof CO2 (PetCO2) was used to adjust the output of the me-chanical ventilator. Using CO2 as a single control variabledoes not provide sufficient physiological information tothe controller and can mask respiratory problems. This de-ficiency was remedied by incorporating several importantvariables in the control procedure in one of the techniquesfor closed-loop mechanical ventilation [10]. In this tech-nique CO2 and O2 levels of the patient as well as respiratorycompliance and airway resistance data are used to controlthe outputs of the ventilator. In this system, both tidal vol-ume and the rate of breathing are adjusted automaticallyto minimize the respiratory work rate on the basis of a hy-pothesis by Otis et al. [14]. The rationale is to stimulatespontaneous breathing by providing a naturally comfort-able breathing pattern to the patient on the ventilator. Thistechnique, which was originally patented under US Patent4986268, was later used in an article by a different groupof workers [11].
In the present study, the closed-loop technique for auto-matic adjustment of the rate and tidal volume of breaths byusing multiple data [10] has been combined with anotherclosed-loop control technique for automatic adjustment ofthe inspired fraction of oxygen, FIO2 . Supplemental oxy-gen treatment commonly accompanies mechanical ventila-tion to achieve stable and sufficient oxygenation. In currentmethods of mechanical ventilation, FIO2 is manually con-trolled. The frequency of the manual adjustments dependson the severity of the patients conditions and can becomequite cumbersome for acutely ill patients. Several differenttechniques have been developed to control FIO2 automati-cally [1523]. In these techniques, feedback of arterial par-tial pressure of oxygen, PaO2 [15], or transcutaneous oxygenpressure, PtO2 [16], or arterial oxygen saturation measuredby pulse oximetry, SpO2 [1723] has been used to controlthe level of FIO2 . The aim has been to prevent hypoxemiaas well as hyperoxemia and to minimize exposure to highlevels of FIO2 . In a recent technique developed for thispurpose, two different control algorithms were combinedto optimize the performance of the controller [2223]. A
fast stepwise control mechanism and a less rapid fine-tunedcontrol algorithm were combined in this technique. Thisoxygen control system demonstrated a significantly shorterresponse time to disturbances in oxygen balance of the pa-tient as compared to the previous techniques. In this study,this system has been combined with the above-mentionedclosed-loop control technique for the ventilator.
The ventilation controller uses PetCO2 and SpO2of thepatient, as well as respiratory compliance and airway resis-tance data, to automatically adjust the rate and depth ofbreathing. The respiratory work rate is minimized in thisprocess and the I :E ratio is adjusted to allow for effec-tive emptying of the lungs in expiration. Minimization ofthe respiratory work rate reduces the load on the respira-tory muscles and stimulates natural spontaneous breathing.This, in turn, could have important implications in reduc-ing the weaning time from the mechanical ventilator. Theadjustment of the I :E ratio in accordance to breathing rateand respiratory mechanics, prevents gas trapping in lungsand development of intrinsic PEEP. The FIO2 controllerprovides an effective and rapid response to oxygen distur-bances. Using the FIO2 controller, hypoxemia is correctedrobustly while hyperoxemia is minimized and oxygen tox-icity is prevented [22, 23].
While the FIO2 controller is quite effective in oxygencontrol of the patient, it does not help the other aspectsof ventilation such as adjustment of ventilation in responseto CO2, respiratory work rate minimization, or preven-tion of gas trapping in the lungs. Combination of the twoclosed-loop control systems results in more effective and ro-bust control of arterial blood gases, stimulates spontaneousbreathing, and prevents the build up of intrinsic PEEP.Compared to previous techniques, the system presented inthis paper includes the original aspects of utilizing multipledata in control of mechanical ventilation, as well as res-piratory work rate minimization. The overall closed-loopsystem is tested by using computer simulations, mechanicallung studies, and animal experimentation.
METHODS AND MATERIALS
Description of the control system
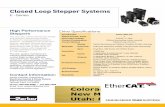
Figure 1 shows the schematic diagram of the control systemin this study. The digital processor detects and processesPetCO2 and SpO2 of the patient which are measured byusing breath-by-breath capnography and pulse-oximetry.This data, together with the airway resistance and respira-tory compliance data of the patient are used to calculatecontrol signals for the signal generator and timing con-trol circuit, which in turn generates control signals for the
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 113
Fig. 1. The schematic diagram of the dual closed-loop control system.
ventilator. The SpO2 data is further processed to calculateand generate a control signal for the oxygen mixer thatcontrols the concentration of oxygen in the inspired gas ofthe patient for every breath. The digital processor uses twoalgorithms; the ventilation control program and the FIO2control program.
The ventilation controller
The input data provided to the closed-loop controller formechanical ventilation represent arterial partial pressuresof carbon dioxide and oxygen (PaCO2 ,PaO2), respiratoryelastance, K , airway resistance, K , metabolic rate ratio,MRR, and the barometric pressure, Pb. Some of thesevariables must be measured whereas others can be storedin the software. In the experiments of this study, PetCO2 andSpO2 were measured for every breath by using capnogra-phy and pulse-oximetry. Data representative of PaCO2 andPaO2 were derived from these measurements for each breathwhereas the values of airway resistance and respiratory elas-tance were monitored and inputted to the controller. Thevalues of MRR and Pb were stored in the software.
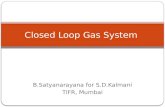
The digital processor in the ventilation controller pro-cesses the input data on a breath-by-breath basis to deter-mine the required ventilation and the breathing frequencyof the patient. A flow-chart of the sequence of steps per-formed by the ventilation controller is shown in Figure 2.As can be seen, at the start of the flow-chart, after having setup the input and the output ports in step 1, initial values for
ventilation and the breathing frequency are provided to theoutput ports of the microprocessor in step 2. The alarm,coupled with one of the output ports is reset in step 3.Values representing the difference between PaCO2 andPetCO2 , the positive end expiratory pressure (PEEP), andPb are read from the input ports or from the memory (ifstored in the software) in step 4. Also, if dead space volumeis measured, the data is read at this point. The respiratorycompliance (1/K ), and the airway resistance (K ) valuesare also read in step 4, if they are not continuously moni-tored. In step 5, the program routine is held for the intervalof the first breath (specified in step 2 by the initial value ofthe breathing frequency). Next, a program loop is startedin step 6. Once the loop is entered, the values of PetCO2and SaO2 are read from the input ports in step 7. In thenext step, the values of respiratory compliance and airwayresistance are read from the input ports, if the values ofthese variables are continuously monitored.
The next step shown at 9 is to calculate the values ofpatients PaCO2 and PaO2 . These are calculated according tothe following equations:
PaCO2 = PetCO2 + K1 (1)PaO2 = ( ln[1 (SpO2)0.5]/0.046) + CF (2)
The symbols used in the equations are also defined inthe Glossary. In Equation (1), K1 represents the differencebetween PaCO2 and PetCO2 . This value is measured in ad-vance and entered in the software in step 4. Depending on
-
114 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
Fig. 2. Flow-chart of the algorithm for the closed-loop ventilation controller. (Continued on next page)
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 115
Fig. 2. (Continued)
-
116 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
the patients conditions, the desired PaCO2 of the patientcan be set by appropriate adjustment of K1. Equation (2) isbased on the blood hemoglobin dissociation curve [24]. CFin this equation is an added correction factor that can beadjusted by the medical personnel to shift and correct PaO2based on the patients blood pH level. If the patients bloodpH is in the normal range (i.e. 7.457.55), CF is set tozero. If the desired blood pH for the patient deviates fromthe normal range, CF needs to be adjusted (3.5 mmHg per0.1 change in pH) [25].
After PaCO2 and PaO2 are calculated in step 9, they arecompared to their minimum threshold limits in step 10to detect any artifacts. If either of them is lower than itsminimum threshold limit, an artifact is assumed, data inthe previous loop for the corresponding partial pressure(or a default value if in the first loop) is resumed, andan alarm is generated. This is done in order to preventprovision of too high or too low ventilation to the patientdue to erroneous measurements of PetCO2 or SpO2 . This isparticularly important in regard to SpO2 data, which maybe subject to considerable noise due to artifact. This featureof the algorithm prevents the erroneous measurements ofSpO2 and PetCO2 from having significant effect on FIO2 andventilation.
In step 11, the calculated PaCO2 and PaO2 values are com-pared to upper and lower alarm limits (the lower alarm lim-its at this step are different from those used to detect artifactin the previous step). If either of the pressures is outside thespecified range (these ranges can be defined for differentpatients), an appropriate signal is generated and providedto the alarm unit via an output port as shown in step 12. Ifthe calculated values of PaCO2 and PaO2 are both lower thanthe minimum alarm limits, the controller detects the pos-sibility of a drastic change in the physiological dead space,such as due to pulmonary embolism, and sends a specialalarm signal in step 14. In this case, predefined ventilationand frequency values are provided by the controller in step15 and the routine is transferred to step 33. If both PaCO2and PaO2 are not found to be below their lower alarm lim-its simultaneously in step 13, the step illustrated in 16 isnext performed. In 16, if PaCO2 is too low, the net effectof CO2 on ventilation is set to zero. Otherwise, the neteffect of CO2 concentration on ventilation requirements iscalculated according to the following equation:
VC = C1 PaCO2 C2 (3)
where VC is the ratio of alveolar ventilation as the neteffect of CO2 to the resting value of ventilation, C1 isthe sensitivity factor of the controller to CO2, and C2 is aconstant. Equation (3) is based on multiple factor theoryin control of respiration [10, 26]. In the present study, C1was set at 0.405 and C2 was tuned at 13.0.
Next, as illustrated at 17, PaO2 is compared to a thresholdvalue of 104 mmHg. If the value of PaO2 is greater thanor equal to this threshold value, the effect of oxygen onventilation is zero (step 18), and program control passes tostep 20. If, on the other hand, the value of PaO2 is lessthan the threshold value, then step 19 is performed and thenet effect of PaO2 on ventilation requirement is calculatedaccording to the following equation [10, 26]:
VO = (4.27 109)(104 PaO2)4.9 (4)
where VO is the ratio of alveolar ventilation as the net ef-fect of oxygen to the resting value of ventilation. In step20, the rate of metabolism or the metabolic rate ratio (rateof metabolism/basal rate of metabolism) is read by the con-troller. This value is either read from the memory or froman input port. The metabolic rate ratio, MRR, is set equalto 1 and stored in the software in this study. The nextstep, illustrated in 21, is to calculate the effect of increasingMRR on ventilation. The following equation is used tocalculate the net effect of MRR on ventilation [10, 27]:
VM = 0.988(MRR 1) (5)
where VM is the ratio of alveolar ventilation as the net effectof increase in MRR to the resting value of ventilation. Inthe next step, illustrated in 22, total alveolar ventilation forthe next breath is calculated according to the followingequation [10, 27]:
VA = (VA at rest)(VC + VO + VM) (6)
where VA is the alveolar ventilation in l/min. Next, asshown in 23, the calculated value of VA is compared to aminimum threshold value. If VA is less than or equal to thethreshold value, ventilation and breathing frequency are setto a predefined minimum in 25. Thereafter, program con-trol turns to step 33 of the loop. If, however, in step 23, thevalue of VA is determined to be greater than the minimumthreshold value, then step 26 is performed. In step 26, thepatients physiologic dead space is determined. This value iseither measured initially and entered in step 4 as mentionedearlier, or is calculated based on a patient model describedby the following equations in step 26 [10, 27]:
VD = 0.1698VA/60 + C3 (7)VDt = VD + VED (8)
where VD is the dead space, VED the added dead space dueto the tubes and connections to the ventilator and VDt thetotal dead space volume in liters. The parameter C3 in thisequation depends on the type and conditions of the patient.
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 117
For normal adults, it is set to 0.1587 [27] and for infantsequal to 2.28 103 l [28].
As illustrated in step 27, the next step is to calculate theoptimum frequency for the next breath. This is determinedon the basis of minimum work rate criterion. This is donein order to minimize the respiratory load and to stimulatenatural breathing. The following equation, which is a mod-ified version of the equation derived by Otis et al. [14], hasbeen used to calculate the optimum breathing frequencyto minimize the work rate of breathing [10]:
f = KVD +
(K VD)2 + (4K K 2VARVD)
2K 2VD(9)
where f is the optimum breathing frequency in breaths/s,VAR the alveolar ventilation in l/s (VAR = VA/60), K therespiratory elastance (reciprocal of respiratory compliance)in cmH2O/l and K the airway resistance in cmH2O/l/s.
Next, as shown in step 28, frequency ( f ) is comparedwith a minimum threshold value. If the value of f is lessthan or equal to the threshold value, ventilation and fre-quency are set to minimum in step 30 and program controlthereafter turns to step 33. If, however, the value of f isgreater than the minimum threshold value, the next step,31, is performed. In 31, total ventilation is calculated ac-cording to the following equation [10]:
VE = VA + 60 f VDt (10)
where VE represents total ventilation in l/min. In step 32,total ventilation and frequency are compared to their upperlimit values. If they happen to be too high, their values arelimited and an alarm is sent to an output port.
In step 33, the mode of operation of the ventilator ischecked. If it is in the pressure control/assist mode, the in-spiratory pressure is calculated in 34 by using the respiratoryelastance (reciprocal of compliance) value:
Pm = K VT + PEEP (11)
where Pm is the inspiratory pressure in cm H2O, K therespiratory elastance in cmH2O/l, and VT the tidal volumein l given by [10]:
VT = VA/60 f + VDt (12)
In the next step, Pm is compared with PEEP. If it is notat least 5 cm H2O above PEEP, its value is increased as asafety measure to avoid gas trapping, and the next step in37 is performed. As illustrated in step 37, at this stage twodigital signals representing Pm and f for the next breathare transmitted to the assigned output ports. The maximumlimit of Pm is set in the ventilator by the medical personnel.
If in step 33, the ventilator is found to be in the volumecontrol (VC)/assist mode, the step in 38 is performed. Inthis step, as shown, VT is calculated by using Equation (12)and compared with a minimum threshold value of Vmin =VDt + VD. If VT Vmin, the program control turns to step40. Otherwise, VT and correspondingly VE is increased asan additional safety measure in step 39, and then the step40 is performed.
In step 40, as shown, two digital signals representing VEand f for the next breath are transmitted to the assignedoutput ports. In the next step 41, another safety measure isperformed to avoid gas trapping in the lungs. In this step,the expiratory time is compared with the respiratory timeconstant. The minimum inspiratory time is set at 20% ofthe breath period. The minimum breath period cannot beshorter than five times the respiratory time constant, ,which is the ratio of airway resistance to respiratory elas-tance (K /K ). In step 41, if the expiratory time is shorterthan 2.5 , the I :E ratio is adjusted in step 42 to allow foreffective emptying of the lungs in expiration and the nextstep 43 is then performed. If, however, the expiratory timeis found to be longer or at least equal to 2.5 in step 41,step 42 is skipped and 43 is followed.
In step 43, a delay interval is adjusted to be equal tothe period of the next breath and the program is held forthis interval in step 44. After the hold time expires, controlturns to A and the procedure is repeated for the next breath.
During the running period, the automatic control canbe turned off and respirator control can be switched tomanual control at any time if needed. It should be notedthat this system is not designed to mask problems that canoccur during mechanical ventilation. For this reason, it hasa built-in alarm circuit that produces different alarm sig-nals if ventilation, breathing frequency, pressure, oxygen,or carbon dioxide levels of the patient are outside prede-fined ranges. These ranges can be redefined in the softwarefor different patients. The controller also safeguards againsterroneous measurements of CO2 and O2 and unsafe lev-els of ventilation and breathing frequency, as well as gastrapping and intrinsic PEEP and it can communicate withpersonal computers, printers and other peripheral devicesvia an RS-232 communication port.
The FIO2 controller
In this study, the closed-loop ventilation controller whichautomatically adjusts the frequency and tidal volume ofbreaths of the patient is augmented with a closed-loop con-trol system for automatic adjustment of FIO2 . As describedearlier, oxygen level of the patient is provided via one ofthe feedback loops to the ventilation controller to adjustpatients ventilation. However, oxygen supplementation is
-
118 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
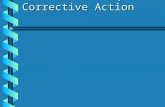
Fig. 3. The schematic diagram of the closed-loop FIO2 controller.
often necessary in the treatment of patients on mechan-ical ventilation. In providing the oxygen treatment, it isessential to prevent hypoxemia as well as hyperoxemia andto avoid exposure to toxic levels of oxygen concentrationfor prolonged periods of time.
In current practice, control of FIO2 in mechanical ven-tilation is manual. In this study, a recent technique for au-tomatic adjustment of FIO2 which is designed to be verysensitive to rapid fluctuations in SpO2 has been used incombination with the closed-loop ventilation controller[22, 23]. Figure 3 shows the schematic diagram of thisclosed-loop FIO2 controller. As can be seen in this diagram,the controller takes feedback of SpO2 which is measuredby using pulse-oximetry, to automatically adjust FIO2 . Atthe beginning, based on the conditions of the patient, allthe set points and threshold values for PaO2 and SpO2 aredefined by the medical personnel. The control algorithmtakes these values and by using the SpO2 input from thepatient determines the required level of FIO2 on a breath-by-breath basis. The control algorithm is designed to cor-rect hypoxemia within seconds if SpO2 falls sharply. This isdone by using a fast stepwise control program to respond torapidly declining levels of SpO2 . By using this program, FIO2is raised stepwise in acute hypoxemia and lowered step-wise as SpO2 stabilizes, and brought to the safe range. Thisprogram interacts with a proportional-integral-derivative
(PID) routine which is designed to provide a fine-tuned,less rapid response to hypoxemia and hyperoxemia whenthe decline in SpO2 is not abrupt. By using the combinationof the stepwise and the PID algorithms, a rapid robust re-sponse to hypoxemia is guaranteed while large fluctuationsin PaO2 as well as hyperoxemia are prevented. The FIO2controller has a built-in artifact detector and alarm circuitthat protects it against erroneous measurements of SpO2 .The flow-chart of the control program, the mathematicalequations of the system, and the details of its structure andfunction have been presented elsewhere [22, 23] and arenot repeated here for brevity.
Mechanical lung studies
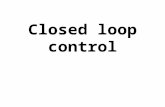
Figure 4 shows the general description of the equipmentset up for the mechanical lung studies. A prototype of theventilation controller was used in the study. The prototypecomprised a Micromint BCC52 microprocessor board,A/D and D/A boards, signal generator and timing con-trol circuits, and an alarm and protection circuit. A sepa-rate electronic data simulator network was used to simulatedata from the patient and provide them to the ventila-tion controller as shown in the figure. The controller wasconnected to a computer monitoring unit via an RS-232
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 119
Fig. 4. The general description of the equipment set up for the mechanical lung studies.
communication port. The outputs of the controller wereprovided to a Siemens Servo Ventilator 300A via an ex-ternal cable connected to the analog I/O terminal of theventilator, N81. This was done in order to bypass the man-ual settings on the front panel of the modified ventilatorand control it instead from outside. A Siemens Servo Screen390 unit was used to monitor the lung mechanics and theoutputs of the ventilator. A Michigan Instruments DualChamber Training Test Lung (TTL) with variable resis-tance and compliance was hooked up to the ventilator.
Computer simulation studies
The dual closed-loop control system was tested by usingcomputer simulations. In the simulation experiments, SpO2was provided to the FIO2 controller. The output of theFIO2 controller was applied to an O2 air mixer, which wassimulated by using the following first-order equation:
T1d FIO2/d t + FIO2 (t ) = G(t ) (13)
where G(t ) is the control signal applied to the O2 air mixerand T1 the time constant of the mixer which was set at 30 sin the experiments. The SpO2 data along with the patientslung mechanics and CO2 data were provided to the closed-loop ventilation controller. The oxygen concentration ofthe inspired gas and the frequency and tidal volume outputsof the ventilator were automatically controlled. The pa-tient was represented by a detailed mathematical modelof the human respiratory system [27]. Since the patientsrespiration was controlled by the ventilator in these exper-iments, only the plant was simulated and the respiratorycontroller of the patient was not included in the mathe-matical model. The mathematical equations of this model
are described in detail in [27] and are not repeated here forbrevity.
The simulation results of this study were obtained by us-ing the block-oriented Interactive Simulation Language,ISL, on a digital computer under different test conditions.
Animal experiments
Six 45-month-old Yorkshire pigs weighing 108132 lbwere used in the experiments. All the experiments werecarried out in accordance with the standards of the AnimalCare Committee at Loma Linda University Medical Cen-ter. The pigs were orally intubated with a 7.5 mm endotra-cheal tube. A 20 gauge angiocath was placed in an ear veinto provide vascular access. A percutaneous arterial catheterwas placed in the groin for blood gas measurements. Thepigs were sedated and paralyzed with continuous i.v. infu-sion of Fentanyl 30 mcg/kg/h and Pancuronium Bromide0.2 mg/kg/h. ECG and pulse oximetry probes were placed.Each animal was placed on the ventilator with both closed-loop controllers active throughout the experiment.
Equipment set up for animal experiments
Figure 5 shows a block diagram of the equipment set upfor the animal experiments. The equipment composed ofa Siemens Servo Ventilator 300A, a Siemens Servo Screen390 monitor, a BCI9000 capnograph, a HP78534C mon-itor for ECG and blood pressure, a Nellcor N-200 pulseoximeter, a prototype of the closed-loop ventilation con-troller, a voltage regulator for adjustment of some of theinputs, a prototype of the FIO2 controller, a computerhooked up to two closed-loop controllers for inputting dataand monitoring, and another computer monitoring system
-
120 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
Fig. 5. Block diagram of the equipment set up for the animal experiments.
equipped with LabView software package for recordingand analysis of various experimental data.
The ventilator was controlled via an external cable con-nected to its N81 analog I/O terminal. According to themanufacturers guidelines, reversible modifications weremade to one of the internal PC boards of the ventila-tor to allow for the external control of the machine. TheSiemens Servo Screen 390 monitor was used to monitor thebreathing waveforms and the respiratory mechanics data. ABCI9000 capnograph and a Nellcor N-200 pulse oximeterwere used to provide the PetCO2 and SpO2 data, respectively.These data were inputted to the closed-loop ventilation
controller. The value of K1, which represents the differ-ence between PaCO2 and PetCO2 , was adjusted periodicallyby using the voltage regulator unit. The value of K1 canbe used to set the desired PaCO2 level based on the patientsconditions as is mentioned earlier. In the experiments, K1was adjusted by comparing PetCO2 with PaCO2 by using pe-riodic blood gas measurements. The values of K and K were measured by the Siemens Servo Screen 390 monitorand the data were inputted to the ventilation controller.The SpO2 data measured by the pulse oximeter was also in-putted to the closed-loop FIO2 controller. Both controllerswere connected to a computer via RS232 communication
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 121
Table 1. Results of the mechanical lung studies
Compliance, Resistance,1/K K PEEP Measured Measured F
Test (ml/cmH2O) (cmH2O/l/s) = RC(s) (cmH2O) VT (l) (breaths/min) VE (l/min)Normal 100 7 0.70 0 0.60 12 7.2COPD 100 16 1.60 0 0.87 7 6.5COPD 41 38 1.56 5 0.86 7 6.2Low compliance 37 5 0.18 0 0.43 16 7.0ARDS 21 9 0.19 8 0.43 15 6.2ARDS 22 14 0.31 8 0.46 13 6.1Obstruction + Low compliance 35 19 0.66 5 0.57 11 6.1Obstruction + ARDS 22 27 0.59 8 0.54 11 6.2Obstruction + ARDS 21 38 0.80 8 0.59 10 6.0
ports for monitoring the outputs and adjustment of someof the initial data in the software. The control signals wereprovided to the ventilator via an external cable through theN81 analog I/O terminal of the ventilator. Another com-puter system equipped with the LabView software packagewas used to continuously record the experimental data. Thetransient and steady-state results were obtained and statisti-cal analyses of the data were performed. A p-value < 0.05was considered to determine statistical significance.
RESULTS
Mechanical lung study results
Table 1 shows the results of the mechanical lung studies.The upper limit pressure of the ventilator was set at 45cmH2O in these experiments. Chronic Obstructive Pul-monary Disease (COPD) was simulated by choosing a highresistance for the mechanical lung and Adult RespiratoryDistress Syndrome (ARDS) was simulated by setting lowthe compliance of the test lung. The Siemens Servo Screen390 monitor was used to measure the resistance, compli-ance, the breathing rate and tidal volume of the test lung.In COPD tests, the frequency was low and tidal volumewas high whereas in the ARDS simulations the reverse wastrue. The results show that the controller adjusted the out-puts of the ventilator in a manner generally perceived asclinically appropriate.
Computer simulation results
Figure 6 shows a sample of the simulation results. In Figure6a, the FIO2 controller is present but the closed-loop venti-lation controller is turned off and conventional ventilation
with fixed values of breathing rate (F ) of 15 breaths/minand tidal volume (VT) of 0.36 l is applied. The ventilationsetting is deliberately chosen to be lower than normal in thistest, a condition that can arise easily when the ventilator set-tings are manually adjusted. In Figure 6b, both closed-loopcontrollers are present. In both tests, the alveolararterialoxygen difference is increased to 25 mmHg to induce hy-poxia. The respiratory elastance is 14 cmH2O/l and theairway resistance is 8 cmH2O/l/s. As shown in 6a, PaO2initially falls to 72 mmHg due to the sudden increase inthe alveolararterial oxygen difference. With the interven-tion of the FIO2 controller, hypoxemia is prevented, andPaO2 stabilizes around 86 mmHg after an initial overshootto 98 mmHg. In the FIO2 response, there is a slight ini-tial overshoot to 27% after which it stabilizes around 25%following a few minor oscillations. As seen in the figure,although hypoxemia is prevented with the aid of the FIO2controller, but the level of PaCO2 steadily rises due to lackof sufficient ventilation and reaches about 47 mmHg inabout 20 min. In 6b, the test is repeated with the additionof the closed-loop ventilation controller. As can be seenin the figure, there is no initial drop in PaO2 . In this test,PaO2 stabilizes around 88 mmHg and FIO2 oscillates around22%. Unlike what is seen in Figure 6a, no hypercapnia isobserved in Figure 6b and PaCO2 remains around 39 mmHgthroughout the test period. Moreover, a lower FIO2 valueis required for sufficient oxygenation in Figure 6b due tothe combined effects of the controllers.
Comparison of these results shows some of the advan-tages of closed-loop mechanical ventilation versus man-ual adjustment of f and VT. As shown here, hypercap-nia and hypoxemia are both prevented and PaO2 is regu-lated in the normal range requiring lower levels of FIO2by using the dual closed-loop control system versus us-ing the FIO2 controller alone. It can also be seen that the
-
122 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
Fig. 6. A sample of computer simulation results. Transient responses of the system to hypoxia. In (a) only the closed-loop FIO2 controller is used while in (b)the closed-loop ventilation controller is also active. The symbols , and correspond to PaO2 , PaCO2 , and FIO2 , respectively.
transient response is shorter and the overall control sys-tem is more robust when both closed-loop controllers arepresent.
Results of animal experiments
In the first part of the experiments, which lasted between45 and 156 min for different animals, the ventilator wasset in the VC mode. In the second part, which took 60142 min, the mode of ventilation was changed to pressure-regulated volume control (PRVC). In each part, the animalswere subjected to periods of induced hypoxia, hypercarbia,and apnea. Hypoxia was induced by addition of high con-centrations of nitrogen (40%) and thereby diluting the airentering the mixer. Hypercarbia was caused by addition of
carbon dioxide to the inspired gas and apnea was imposedby temporarily disconnecting the animal from the venti-lator. Transient as well as steady-state responses were ob-tained. Blood gas measurements were done intermittentlyfor every 2040 min.
Two examples of the transient responses are shown inFigures 7 and 8. In Figure 7, the transient responses in hy-percarbia are shown. In this test, the ventilator was in theVC mode. As can be seen, despite continuous addition ofcarbon dioxide (flow of 5 l/min of CO2 into the air tube)to the inspired gas, there is only a slight rise in PetCO2 to 39mmHg at the onset of the test which is brought down toaround 36 mmHg in less than 15 s by the intervention ofthe ventilation controller and the rise in the level of ven-tilation. The lowered PetCO2 causes ventilation to decrease
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 123
Fig. 7. An example of transient response of the control system to hypercarbia (pig #4).
-
124 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
Fig. 8. An example of the response of the control system to imposed apnea (pig #6).
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 125
after about 50 s. Then the low values of ventilation causeSpO2 to decrease and PetCO2 to increase. The combinedeffects of high PetCO2 and low SpO2 cause a sharp rise inventilation after about 100 s. Thereafter, the oscillations inPetCO2 and SpO2 are reduced and minute ventilation sta-bilizes around 10 l/min. It should be noted that PetCO2remains in the range of 3539 mmHg and SpO2 stays above96% throughout the test while carbon dioxide is continu-ously added to the inspired gas. FIO2 falls slightly to about21.5% by the end of the test period.
Figure 8 shows the transient responses in imposed ap-nea and shortly thereafter. In this experiment, the ventila-tor was in the PRVC mode. In this test, while respiratorymechanics along with other input data were used to de-termine the optimum breathing rate and tidal volume ofthe breaths, they were also used to automatically adjust theinspiratory pressure for every breathing cycle. As can beseen in Figure 8, at the beginning of the test when apneais imposed by disconnecting the animal from the ventilatorfor 40 s, SpO2 sharply falls to around 65%. During the sametime, the reading of the capnometer for PetCO2 falls due tolack of gas flow. Since the animal was disconnected fromthe ventilator, the values shown for ventilation, breathingfrequency, tidal volume, and FIO2 in the graphs of Figure8 during 40 s of apnea were not provided to the animal.After the period of imposed apnea, as soon as the ventilatoris connected back to the animal, ventilation sharply risesto about 17 l/min at a frequency of 24 breaths/min, andFIO2 rises to 60% to correct the induced acute hypoxia. Itis seen that both SpO2 and PetCO2 are brought back to thenormal levels within 20 s of the intervention of the dualclosed-loop control system.
The summary of the steady-state results in hypoxia andhypercarbia is shown in Table 2. As shown, the experimentswere done by using the VC mode for 45156 min and thePRVC mode for 60142 min for different animals. Bothclosed-loop controllers were used in all experiments. Asshown in Table 2, SpO2 and PetCO2 were maintained in thenormal range all of the time. In hypercarbia experiments,the levels of SpO2 were higher than those in hypoxia dueto higher levels of ventilation. This is true for experimentsusing the VC as well as the PRVC mode. The blood gasresults shown in the last three columns of the table indicatesimilar results. According to these results, in hypercarbia ex-periments generally both PaCO2 and PaO2 results are highercompared to hypoxia experiments. This is due to high lev-els of CO2 in the breathing gas and the resultant higherlevels of ventilation.
The values of FIO2 listed in Table 2 are the oxygen con-centrations measured at the output of the O2 air mixerunder steady-state conditions. It should be noted that inhypoxia experiments, the air coming into the mixer was
diluted with high concentrations of nitrogen and the oxy-gen concentrations at the output of the mixer are the resultof addition of the controlled concentrations of oxygen tothe diluted air.
The largest standard deviation in hypoxia experimentsfor SpO2 under steady-state conditions was 1.17% witha mean value of 96.9% while the ventilator was in theVC mode. In these tests, minimum SpO2 was 95% andit remained above 95.05% most of the time (p < 0.05).The largest standard deviation for PetCO2 in these tests was1.77 mmHg with a mean value of 39.1 mmHg and the95% confidence interval of 38.9039.44 mmHg for themean value. The blood gas results show that PaCO2 rangedfrom 33 to 38 mmHg and PaO2 ranged between 74 and126 mmHg in this part of the experiments for differentanimals.
In the hypoxia experiments, with the ventilator in thePRVC mode, the largest standard deviation for SpO2 was1.76% with a mean value of 95.37%. The minimum valuefor SpO2 was 90.4% in these tests and it remained above91.2% most of the time (p < 0.034). The largest standarddeviation in PetCO2 was 1.43 mmHg with a mean value of34.87 mmHg and the 95% confidence interval of 34.4235.32 mmHg for the mean value. The blood gas resultsshow that PaCO2 in these tests was in the range of 3038mmHg and PaO2 was in the range of 73102 mmHg fordifferent animals.
In hypercarbia experiments, with the ventilator in theVC mode, the largest standard deviation for SpO2 was0.46% with a mean value of 97.22%. The minimum SpO2in these tests was 96.19% and it remained above 96.5% mostof the time (p < 0.019). The largest standard deviationfor PetCO2 was 1.78 mmHg with a mean value of 39.17mmHg, and the 95% confidence interval for mean between38.9 and 39.44 mmHg. According to the blood gas results,the ranges for PaCO2 and PaO2 for different animals were3341 and 80102 mmHg, respectively.
The results of the hypercarbia experiments with the ven-tilator in the PRVC mode show the largest standard devi-ation of 0.60% for SpO2 with a mean value of 97.56%.In these tests, SpO2 was always above 96.2% and remainedhigher than 96.9% most of the time (p < 0.01). The largeststandard deviation in PetCO2 was measured at 1.50 mmHgwith a mean value of 39.34 mmHg and the 95% confi-dence interval for mean of 39.139.57 mmHg. The bloodgas results show that PaCO2 ranged from 32 to 39 mmHgand PaO2 from 74 to 110 mmHg in these experiments fordifferent animals.
According to these results, the dual closed-loop controlsystem maintained PetCO2 , SpO2 , PaCO2 , and PaO2 levels ofthe animals in the normal range in all the experiments, inthe VC as well as the PRVC modes of the ventilator.
-
126 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
Tabl
e2.
Sum
mar
yof
stead
y-sta
tere
sults
ofth
ean
imal
studi
esin
hypo
xia
and
hype
rcarb
ia
Exp
erim
enta
lres
ults
Oxy
gen
conc
entr
atio
nTe
sts
S pO
2at
the
mix
erP e
tCO
2V
EV
TF
Pig
Wei
ght
(mea
n
SD)
outp
ut(m
ean
SD
)(m
ean
SD
)(m
ean
SD
)(m
ean
SD
)P a
CO
2P a
O2
no.
Sex
(lb)
(%)
(mea
n
SD)
(mm
Hg)
(l)(l)
(bre
aths
/min
)(m
mH
g)(m
mH
g)pH
Hyp
oxia
expe
rim
ents
VC
vent
ilatio
nm
ode
1F
120
96.1
9
0.60
18.1
4
0.28
39.1
0
1.77
7.19
1.
960.
54
0.06
13.1
7
2.47
3783
7.50
2M
128
96.9
0
1.17
16.0
7
1.63
33.6
1
1.00
7.34
1.
240.
52
0.04
14.0
0
1.33
3874
7.50
3M
132
95.6
1
0.69
20.5
4
1.26
32.2
2
1.36
8.75
1.
450.
54
0.04
16.2
1
1.90
3376
7.55
4F
118
96.0
6
0.36
25.6
1
0.21
36.3
8
1.29
8.04
1.
570.
49
0.04
16.3
0
2.19
3893
7.50
5F
126
96.0
6
0.62
18.2
2
0.58
33.2
4
1.45
7.87
1.
620.
55
0.05
14.1
4
1.93
3374
7.53
6F
108
95.3
4
0.57
23.0
6
1.27
34.0
6
1.53
7.51
1.
710.
51
0.05
14.4
3
2.28
3312
67.
53
Hyp
erca
rbia
expe
rim
ents
VC
vent
ilatio
nm
ode
1F
120
98.1
6
0.04
18.7
7
0.09
39.1
7
1.78
7.17
1.
950.
54
0.06
12.9
7
2.52
4182
7.46
2M
128
98.1
3
0.08
18.5
3
0.08
34.0
5
1.40
8.30
1.
640.
54
0.04
15.2
0
2.17
3884
7.49
3M
132
98.0
9
0.26
18.9
0
1.11
32.6
8
1.30
9.45
1.
500.
55
0.03
17.1
4
1.91
3389
7.55
4F
118
96.6
3
0.38
19.7
6
1.24
36.7
6
1.15
8.59
1.
500.
50
0.04
16.9
8
2.13
3910
27.
515
F12
698
.09
0.
0318
.48
0.
0933
.97
1.
358.
94
1.54
0.58
0.
0515
.26
1.
7033
807.
546
F10
897
.22
0.
4622
.67
3.
2135
.11
1.
648.
50
2.10
0.53
0.
0515
.71
2.
6537
101
7.50
Hyp
oxia
expe
rim
ents
PRV
Cve
ntila
tion
mod
e1
F12
096
.21
0.
5618
.30
0.
2837
.90
1.
185.
87
1.32
0.50
0.
0511
.53
1.
8235
737.
472
M12
895
.37
1.
7615
.42
1.
3533
.20
1.
197.
27
1.36
0.52
0.
0413
.85
1.
9038
687.
503
M13
296
.06
0.
3923
.65
0.
5731
.91
1.
308.
39
1.44
0.53
0.
0415
.74
1.
9132
857.
554
F11
895
.47
0.
6221
.23
1.
5437
.09
0.
929.
27
1.20
0.51
0.
0318
.00
1.
6135
807.
525
F12
695
.62
0.
6222
.27
1.
3434
.19
1.
169.
57
1.18
0.54
0.
0317
.56
1.
4231
787.
566
F10
896
.02
0.
4624
.49
0.
6134
.87
1.
437.
83
1.33
0.55
0.
0514
.22
1.
5330
102
7.57
Hyp
erca
rbia
expe
rim
ents
PRV
Cve
ntila
tion
mod
e1
F12
098
.08
0.
3918
.76
0.
0939
.34
1.
507.
59
1.78
0.56
0.
0613
.51
2.
1739
787.
462
M12
898
.05
0.
5418
.49
0.
1134
.26
1.
448.
03
1.45
0.54
0.
0414
.77
1.
9138
747.
503
M13
298
.14
0.
0318
.98
1.
1132
.84
1.
289.
66
1.33
0.55
0.
0417
.41
1.
6033
907.
554
F11
897
.22
0.
4718
.66
0.
1037
.50
0.
879.
60
1.44
0.52
0.
0318
.41
1.
9238
107
7.49
5F
126
97.5
6
0.60
18.5
6
0.08
34.2
6
1.16
9.39
1.
440.
54
0.04
17.3
9
1.72
3486
7.54
6F
108
96.9
9
0.54
18.7
2
0.62
35.3
1
1.42
8.74
1.
570.
56
0.05
15.4
0
1.81
3211
07.
53
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 127
DISCUSSION
A dual closed-loop control system for mechanical venti-lation is evaluated. In this system, a ventilation controllerand an oxygen concentration controller are combined. Thebreathing frequency, tidal volume, and the inspired fractionof oxygen, are automatically controlled. The closed-loopventilation controller takes data representing oxygen andcarbon dioxide levels of the patient, airway resistance, andrespiratory compliance to automatically adjust f and VT.This controller determines f and VT to minimize the res-piratory work rate based on a hypothesis by Otis et al. [14].The I :E ratio is adjusted by the controller to allow for ef-fective emptying of the lungs in expiration and many othersafeguards are provided in the system as explained above.
The closed-loop FIO2 controller uses feedback of arterialoxygen saturation, SpO2 , to determine the required level ofFIO2 for every breath. This controller uses the combinationof two algorithms to respond to both slow and rapid distur-bances in the oxygen balance of the patient. Measurementsthat look like artifacts are discarded by the dual closed-loopcontrol system and alarms are activated if any artifact or anyuntoward condition is detected in the patient.
The dual closed-loop control system was tested by us-ing a detailed mathematical model for humans, as well asin mechanical lung studies and animal experimentation.The mechanical lung studies were done to investigate theeffect of significantly changing respiratory mechanics. Inthese tests, the values of respiratory compliance and airwayresistance were varied to the extent seen under disease con-ditions such as severe COPD and ARDS. The animal ex-periments were performed on six Yorkshire pigs weighing108132 lb. In a group of animal experiments, the PRVCmode of the ventilator in which the inspiratory pressure is
GLOSSARY
Symbol Definition UnitC1 Sensitivity factor of the controller to CO2 (mmHg)1
C2 Constant tuning factor DimensionlessC3 Constant factor lCF Correction factor for arterial partial pressure of O2 mmHgf Breathing frequency breaths/sF Breathing frequency breaths/minFIO2 Inspired fraction of oxygen DimensionlessI :E Ratio of inspiration time to expiration time DimensionlessK1 Adjustment factor for CO2 mmHgK Respiratory elastance (resp. compliance)1 cmH2O/lK Airway resistance cmH2O/l/secMRR Metabolic rate ratio Dimensionless
adjusted automatically in response to changes in respiratorymechanics, and in another group the VC mode of the ven-tilator were used in this study. In these tests, hypercapniaand hypoxemia, conditions caused by respiratory insuffi-ciency and disease, were induced by continuously blendinghigh CO2 concentrations to the inspired gas and by con-stantly diluting the air entering the mixer by addition ofhigh concentration of nitrogen. Also, in some of the tests,apnea was temporarily imposed to induce hypoxia, andhypercapnia. Pulse oximetry and capnography techniqueswere used to continuously and noninvasively measure theoxygen and carbon dioxide levels of the patient. Periodicblood gas measurements were done to check and correctthe noninvasive measurements and software means weredesigned and used throughout the experiments to detectand discard measurement artifacts due to pulse oximetryand/or capnography. The respiratory mechanics were mea-sured by using a standard commercial monitor, SiemensServo Screen 390. The blood gases, the end-tidal partialpressure of CO2, and the arterial oxygen saturation levelswere maintained in the normal range by the dual closed-loop controller under different disturbances. The analysisof the results showed that the control system responded inless than 25 s to bring the end-tidal partial pressure of CO2and the arterial oxygen saturation to the normal safe range.
In conclusion, the results of this study attest to the effec-tiveness of the proposed dual closed-loop control systemunder the indicated conditions and show the potential ofthis control technique to improve ventilatory treatment.However, it should be emphasized that although there aresignificant similarities between the plant parameters in hu-mans compared to those of the animals tested, there arestill some differences that remain to be investigated in fu-ture studies.
-
128 Journal of Clinical Monitoring and Computing Vol 18 No 2 2004
PaCO2 Arterial partial pressure of CO2 mmHgPaO2 Arterial partial pressure of O2 mmHgPEEP Positive end expiratory pressure cmH2OPetCO2 End-tidal partial pressure of CO2 mmHgPm Peak inspiratory pressure cmH2OPtO2 Transcutaneous oxygen pressure mmHgRC Respiratory time constant sSpO2 Arterial oxygen saturation measured by pulse-oximetry Dimensionless Respiratory time constant sT1 Time constant of the O2 air mixer sec.VA Alveolar ventilation l/minVAR Alveolar ventilation l/sVC Ratio of alveolar ventilation as the net effect of CO2 to the resting value of ventilation DimensionlessVD The physiologic dead space volume lVDt Total dead space volume including that of the equipment lVE Total ventilation l/minVED Added dead space due to tubes and connections lVM Ratio of alveolar ventilation as the net effect of increase in the rate of metabolism to the resting dimensionless
value of ventilationVmin Minimum allowed tidal volume lVO Ratio of alveolar ventilation as the net effect of oxygen to the resting value of ventilation dimensionlessVT Tidal volume l
REFERENCES
1. Saxton GA, Jr, Myers GH. A servomechanism for automaticregulation of pulmonary ventilation. J Appl Physiol 1957; 11:326328.
2. Frumin MJ, Bergman NA, Holaday DA. Carbon dioxide andoxygen blood levels with a carbon dioxide controlled artificialrespirator. Anesthesiology 1959; 20(3): 313321.
3. Mitamura Y, Mikami T, Sugawara H, Yoshimoto C. An op-timally controlled respirator. IEEE Trans Biomed Eng 1971;BME-18: 330337.
4. Coles JR, Brown WA, Lampard DG. Computer control of ven-tilation and anesthesia. Med Biol Eng 1973; 11: 262267.
5. Mitamura Y, Mikami T, Yamamoto K, Mimura K. A dual controlsystem for assisting respiration. Med Biol Eng 1975; 13(6): 846854.
6. Coon RL, Zuperku EJ, Kampine JP. Systemic arterial blood pHservo control of mechanical ventilation. Anesthesiology 1978;49(3): 201204.
7. Ohlson KB, Westenskow DR, Jordan WS. A microproces-sor based feedback controller for mechanical ventilation. AnnBiomed Eng 1982; 10: 3548.
8. Chapman FW, Newell JC, Roy RJ. A feedback controllerfor ventilatory therapy. Ann Biomed Eng 1985; 13: 359372.
9. Ritchie RG, Ernst EA, Pate BL, Pearson JP, Sheppard LC.Closed-loop control of an anesthesia delivery system: Develop-ment and animal testing. IEEE Trans Biomed Eng 1978; BME-34(6): 437443.
10. Tehrani FT. Method and apparatus for controlling an artificialrespirator. U.S. Patent No. 4986268, 22nd January 1991.
11. Laubscher TP, Heinrichs W, Weiler N, Hartmann G, BrunnerJX. An adaptive lung ventilation controller. IEEE Trans BiomedEng 1994; 41(1): 5159.
12. Schaublin J, Derighetti M, Feigenwinter P, Petersen-Felix S,Zbinden AM. Fuzzy logic control of mechanical ventilation dur-ing anesthesia. Br J Anesth 1996; 77: 636641.
13. Fernando T, Cade J, Packer J. Automatic control of arterial car-bon dioxide tension in mechanically ventilated patients. IEEETrans Info Tech Biomed 2002; 6(4): 269276.
14. Otis AB, Fenn WO, Rahn H. Mechanics of breathing in man. JAppl Physiol 1950; 2: 592607.
15. Beddis IR, Collins P, Levy NM, Godfrey S, Silverman M. Newtechnique for servo-control of arterial oxygen tension in preterminfants. Arch Dis Child 1979; 54: 278280.
16. Sano A, Kikucki M. Adaptive control of arterial oxygen pressureof newborn infants under incubator oxygen treatments. ProcIEE 1985; 132(Part D., No. 5): 205211.
17. Yu C, He WG, So JM, Roy R, Kaufman H, Newell JC. Im-provement in arterial oxygen control using multiple model adap-tive control procedures. IEEE Trans Biomed Eng 1987; BME-34(8): 567574.
18. Morozoff PE, Evans RW. Closed loop control of SaO2 in theneonate. Biomed Instr Tech 1992; 26: 117123.
19. Tehrani FT. A microcomputer oxygen control system for venti-latory therapy. Ann Biomed Eng 1992; 20(5): 547558.
20. Tehrani FT, Bazar AR. A feedback controller for supplementaloxygen treatment of newborn infants: A simulation study. MedEng Phys 1994; 16: 329333.
21. Raemer DB, Ji X, Topulos GP. FIX controller: An instrumentto automatically adjust inspired oxygen fraction using feedbackcontrol from a pulse oximeter. J Clin Monit 1997; 13: 91101.
-
Tehrani et al: Closed-Loop Control of Mechanical Ventilation 129
22. Tehrani FT. A control system for oxygen therapy of prematureinfants. Proc IEEE Eng Med Biol Conf 2001; 23(2): 20592062.
23. Tehrani FT, Rogers M, Lo T, Malinowski T, Afuwape S, LumM, Grundl B, Terry M. Closed-loop control of the inspired frac-tion of oxygen in mechanical ventilation. J Clin Monit Comput2002; 17(6): 367376.
24. Visser BF. Pulmonary diffusion of carbon dioxide. Phys MedBiol 1961; 5: 155166.
25. Riley RL. Gas exchange and transportation. In: Ruch TC,
Patton HD, eds. Physiology and biophysics. Philadelphia andLondon: Saunders, 1966: 761787.
26. Gray JS. Pulmonary ventilation and its physiological regulation.Springfield, Illinois: Charles C. Thomas, 1949.
27. Fincham WF, Tehrani FT. A mathematical model of the humanrespiratory system. J Biomed Eng 1983; 5: 125133.
28. Tehrani FT. Mathematical analysis and computer simulationof the respiratory system in the newborn infant. IEEE TransBiomed Eng 1993; 40(5): 475481.