
A developed treatment of early abscessed implant - idjar.net TECHNIQUE.pdf · The outcome of...
5
International Dental & Medical Journal of Advanced Research ● Vol. 3 ● 2017 1 International Dental & Medical Journal of Advanced Research (2017), 3, 1–5 CLINICAL TECHNIQUE A developed treatment of early abscessed implant Hadi Bilal 1,2 1 Department of Periodontology, Faculty of Dentistry, Al-Andalus University, Tartus, Al-Kadmous, Syria, 2 Department of Oral Pathology, Faculty of Dentistry, Al-Andalus University, Tartus, Al-Kadmous, Syria Introduction Inflammation due to oral bacteria could alter soft and hard tissues around dental implant. If this degradation remains untreated, a progressive loss of supporting tissue and supportive bone will occur. This inflammation is called peri-implantitis. [1] The irreversible changes in the crestal bone levels coupled to bleeding on probing, with or without pockets presence, are the most characteristic criteria of the peri-implantitis. In addition, peri-implantitis lesion suppuration could appear. [2] Some of the risk factors of peri-implant diseases are poor oral hygiene, smoking, and history of periodontitis. [3] Nevertheless, early failure of dental implant is the most problematic incident during the healing procedure after the implant installing. Several factors of early implant failure are the low primary stability leading to minimal or non-osseointegration, the contamination of implant material and/or surgical site by pathogenic bacteria. In a recent study, author presents that patients who received pre- operative antibiotics showed fewer early implant failures. [4] Early failure rate of 0.6% is recorded in a study done by Brügger et al. [5] In another study, it is found that, among 150 failing implants in a total of 2796 implants, 57.3% of the implant failures were early no matter the cause of this failure. [6] The outcome of non-surgical periodontal treatment of peri- implantitis is unpredictable. Nevertheless, several detoxification procedures are useful to decontaminate peri-implantitis affected implant surfaces including air-powder abrasion, saline wash, citric acid application, laser therapy, peroxide treatment, ultrasonic/ manual debridement, and application of topical medication. However, a definite gold standard could not be identified. [7] Debridement and decontamination of the infected implant surface and surrounding bone are standard in a surgical approach. Once the access to the infected site is achieved, the application of bone substitutes is the answer to a regenerative procedure. A well-defined crater-like defect may improve retention of the bone graft, thereby allowing an optimal healing. [8] In fact, a regenerative surgical therapy combined to bone graft associated to a membrane has reported clinical and radiographic improvements over 3-4 years. [9-12] The aim of the current paper is to shed the light on a case of early dental implant failure, treated by a simple protocol of a surgical peri-implantitis composed of the adjunction of implant surface detoxification - by means of peroxide treatment and citric acid application - to a regenerative procedure using a bone graft particles covered by a resorbable membrane. Abstract Early peri-implantitis is one of the major causes of implant surgery failure. Caused by various factors such as pathogenic contamination, this condition needs a specific and professional intervention to re-stabilize the implant and to recreate osseointegration in the defected site. This article describes a treatment protocol that restores the bone- implant contact and renders the implant reliable and functional at the long term. In the aim of treating a peri-implantitis state and saving the implant, we opted for a simple protocol that treats the implant surface and stimulates the bone regeneration and bone-implant osseointegration. 1-year after the application of hydrogen peroxide 15% and citric acid combined with bone graft and resorbable membrane, the ex-defected implant was loaded after a neo-osseointegration formation all around the implant. 2 years later, the implant is still functional, and the peri-implant tissues show a healthy state. In conclusion, the good diagnosis and the fast intervention using implant surface etching and regenerative intervention were the key to success in this case. This case study encourages the use of the combined procedure of bone and membrane to stabilize the graft into the bone crater, which is crucial for the formation of a neo-alveolar bone that surrounds the exposure surface of the defected implant. Keywords Abscess, early peri-implantitis, implants, molecular biology, regeneration, surface etching Correspondence Hadi Bilal, Department of Periodontology, Faculty of Dentistry, Al-Andalus University, Tartus, Al-Kadmous, Syria. Email: [email protected] Received 18 March 2017; Accepted 21 April 2017 doi: 10.15713/ins.idmjar.65
Transcript of A developed treatment of early abscessed implant - idjar.net TECHNIQUE.pdf · The outcome of...
International Dental & Medical Journal of Advanced Research ● Vol. 3 ● 2017 1
International Dental & Medical Journal of Advanced Research (2017), 3, 1–5
C L I N I C A L T E C H N I Q U E
A developed treatment of early abscessed implantHadi Bilal1,2
1Department of Periodontology, Faculty of Dentistry, Al-Andalus University, Tartus, Al-Kadmous, Syria, 2Department of Oral Pathology, Faculty of Dentistry, Al-Andalus University, Tartus, Al-Kadmous, Syria
Introduction
Inflammation due to oral bacteria could alter soft and hard tissues around dental implant. If this degradation remains untreated, a progressive loss of supporting tissue and supportive bone will occur. This inflammation is called peri-implantitis.[1]
The irreversible changes in the crestal bone levels coupled to bleeding on probing, with or without pockets presence, are the most characteristic criteria of the peri-implantitis. In addition, peri-implantitis lesion suppuration could appear.[2]
Some of the risk factors of peri-implant diseases are poor oral hygiene, smoking, and history of periodontitis.[3] Nevertheless, early failure of dental implant is the most problematic incident during the healing procedure after the implant installing. Several factors of early implant failure are the low primary stability leading to minimal or non-osseointegration, the contamination of implant material and/or surgical site by pathogenic bacteria. In a recent study, author presents that patients who received pre-operative antibiotics showed fewer early implant failures.[4] Early failure rate of 0.6% is recorded in a study done by Brügger et al.[5] In another study, it is found that, among 150 failing implants in a total of 2796 implants, 57.3% of the implant failures were early no matter the cause of this failure.[6]
The outcome of non-surgical periodontal treatment of peri-implantitis is unpredictable. Nevertheless, several detoxification procedures are useful to decontaminate peri-implantitis affected implant surfaces including air-powder abrasion, saline wash, citric acid application, laser therapy, peroxide treatment, ultrasonic/manual debridement, and application of topical medication. However, a definite gold standard could not be identified.[7]
Debridement and decontamination of the infected implant surface and surrounding bone are standard in a surgical approach. Once the access to the infected site is achieved, the application of bone substitutes is the answer to a regenerative procedure. A well-defined crater-like defect may improve retention of the bone graft, thereby allowing an optimal healing.[8] In fact, a regenerative surgical therapy combined to bone graft associated to a membrane has reported clinical and radiographic improvements over 3-4 years.[9-12]
The aim of the current paper is to shed the light on a case of early dental implant failure, treated by a simple protocol of a surgical peri-implantitis composed of the adjunction of implant surface detoxification - by means of peroxide treatment and citric acid application - to a regenerative procedure using a bone graft particles covered by a resorbable membrane.
AbstractEarly peri-implantitis is one of the major causes of implant surgery failure. Caused by various factors such as pathogenic contamination, this condition needs a specific and professional intervention to re-stabilize the implant and to recreate osseointegration in the defected site. This article describes a treatment protocol that restores the bone-implant contact and renders the implant reliable and functional at the long term. In the aim of treating a peri-implantitis state and saving the implant, we opted for a simple protocol that treats the implant surface and stimulates the bone regeneration and bone-implant osseointegration. 1-year after the application of hydrogen peroxide 15% and citric acid combined with bone graft and resorbable membrane, the ex-defected implant was loaded after a neo-osseointegration formation all around the implant. 2 years later, the implant is still functional, and the peri-implant tissues show a healthy state. In conclusion, the good diagnosis and the fast intervention using implant surface etching and regenerative intervention were the key to success in this case. This case study encourages the use of the combined procedure of bone and membrane to stabilize the graft into the bone crater, which is crucial for the formation of a neo-alveolar bone that surrounds the exposure surface of the defected implant.
Keywords Abscess, early peri-implantitis, implants, molecular biology, regeneration, surface etching
Correspondence Hadi Bilal, Department of Periodontology, Faculty of Dentistry, Al-Andalus University, Tartus, Al-Kadmous, Syria. Email: [email protected]
Received 18 March 2017; Accepted 21 April 2017
doi: 10.15713/ins.idmjar.65

2 International Dental & Medical Journal of Advanced Research ● Vol. 3 ● 2017
Treatment of early implantitis Bilal
Case Report
The author executed this study during the period of 2014-2016 in his office.
A 60-year-old female patient presented with a remaining root of a first lower left premolar. The patient showed the desire to replace the defected tooth with a dental implant. Her dental history revealed previous sites treated with dental implants in a good and healthy state [Figure 1a]. While exploring the panoramic X-ray film, a mineral-decreased alveolar bone surrounded the remaining premolar root that could mean the presence of a periodontal defect or more likely a fracture of the remaining root. The clinical examination of the root area did not show frank periodontal pockets [Figure 1b], and so a diagnosis of fractured remaining root was identified. Hence, an immediate extraction was done, the fractured root was pulled out gently [Figure 1c]; after a careful curettage of the alveolar socket, the extraction site was left to be healed spontaneously.
Given the good general health of the patient, an appointment was set for a dental implant procedure.
3 months and 20 days later, the patient presented to our office with a complete clinical healing of the extraction site (the extraction cavity closed totally with no signs of inflammation). The next step was to place an implant at the position of tooth 35, and the patient was properly prepared. The dental implant diameters and length (ø3.8*10.0 mm) were decided after a careful study of the surgical site and the panoramic X-ray film.
During the surgery procedure, everything was going normally until the use of the final drill. In this moment, a serious mistake was done and a wider drill was used instead of the drill that goes with the chosen implant diameters. At this stage, we had to change the selected implant and pick up a wider implant to rectify the mistake done [Figure 1d]; a 4.5 mm implant diameter with a torque of 25 Ncm was placed.
Once we made the sutures, the patient was sent home in good and normal healthy condition.
40 days later, the patient came to the office for an appointment to replace the cover screw with a healing abutment. Clinically, the implant site appeared to be normal, unless an area of smooth redness and the presence of narrow orifice-like structure on the top of the alveolar ridge, directly above the implant [Figure 2a]. We suspected an abscess, and an early failure caused by an acute peri-implantitis was proposed. In a despaired way to save the implant, the implant-capping gingiva was removed in the goal of cleaning the implant site and debridement the tissue around the implant. Once the covering gingival tissue from the top of the implant was removed, the pus was spontaneously discharged. We detected a bone loss, and a failing osseointegration process was suspected, and then diagnosed because the implant was able to move out of its alveolar socket when using the screwdriver gently. We immediately opted for a conservative procedure applied with the following steps; the implant was re-driven into its socket again (the implant was not completely screwed out of its socket), and an antibiotic program was subscribed (Augmentine 1000 mg twice per day for a period of 6 days) (no pictures was taken because of the criticalness of the intervention). A medico-surgical treatment was decided.
3 days after, the patient came and showed a stable state with no sign of pus at the implant defected site. A gingival flap was designed in a way to ease the implant access [Figure 2b]. A remarkable bone loss (up to 6 mm of the all implant length) was observed in the vestibular wall of the implant, slightly extended to the mesiodistal axe of the implant, and a granular tissue was shown. The implant-bone contact was negative. We applied the following treatment protocol gradually. The granular tissue debridement was performed. A solution of neutral serum and hydrogen peroxide 15% was prepared and applied on the implant surface and the defected bone twice. Then, a citric acid soluble was applied on the detached part of the implant using a small ball of cotton for at least 15 s twice in the aim to acid etch and reintegrate the implant surface with the surrounding bone [Figure 2c]. The implant was then re-screwed firmly into its original bone site.
Once the implant is clean, stable, and tightly attached to its bone socket, a bioactive bone graft (Bio I, Dim: Ø1mm, Science
Figure 1: (a) Panoramic X-ray showing the fractured premolar root, (b) intraoral photography for the remnant premolar root, (c) gentle extraction of the fractured root, (d) implant reference
d
cba
Figure 2: (a) Peri-implantitis after 40 days, (b) vertical bone resorption with granular tissue, (c) debridement of granular tissue and etching, (d) the bone graft is applied with a visible blood supply, (e) the resorbable membrane is placed on the bone-grafted implant, (f) surgical site is protected by the use of Coe-Pak
d
cb
f
a
e

International Dental & Medical Journal of Advanced Research ● Vol. 3 ● 2017 3
Bilal Treatment of early implantitis
for BioMaterials, France) is applied on the implant in a manner to cover all the implant surface-bone defect area. A resorbable collagen membrane (FormaAid, Maxigen Biotech Inc., Taiwan) was used to protect the grafted sit and all its components from the surrounding epithelial tissue cells penetration. A great and sufficient blood supply was visible before suturing [Figure 2d and e].
The gingival flap was sutured, and the site was covered with the periodontal dressing Coe-Pak (GC, America Inc., USA) [Figure 2f].
Chlorhexidine 0.2% mouth rinses were prescribed starting from the day after the surgery and were extended to the next 2 weeks, to prevent post-surgical secondary infections. The sutures were removed 10 days after the surgery. Neither swelling nor pain occurred during the healing period. During the healing period, the implant was left unloaded.
Post-management and 1-year follow-up were reviewed. A panoramic X-ray radiograph was taken, there was no translucency zone around the implant nor bone loss at the alveolar crest level [Figure 3a]. Complete healing of the soft tissue at the implant site was observed. Gingiva was healthy with its normal pale pink color, and no sign of inflammation was detected. The implant was fully covered by the gingiva [Figure 3b and c]. The capping gingiva has been removed using a scalpel #15 by restricting the incision to the very small surface of the cover screw [Figure 3d and e]. The cover screw is finally taken off, and an implant immobility is detected [Figure 3f]. A gingiva former is applied [Figure 4a]. 10 days later, the gingiva former is removed [Figure 4b and c]. Classic impression is taken [Figure 4d and e]. Finally, the implant is loaded [Figure 5a].
More than once after the implant loading, the patient has visited our office. Standard checkup has been done. We had observed minimal inflammation on the interpapilla mesially to the loaded implant due to excessive flossing. No gingival pockets were seen neither bleeding on probing [Figure 5b].
Discussion
This is notthe only described surgical procedure for the treatment of abscessed peri-implantitis but it’s the first to describe a multicomponent protocol that proposes surgical intervention added to the decontamination of implant surface by several known solutions, associated to an antibiotic program to activate the osseoconduction and osseointegration on movable and abscessed implants using bone graft and collagen membrane. According to the bone’s defected shape, the clinical outcome resulting from a surgical regenerative approach of peri-implantitis lesions could be more or less significant.[8] Previous studies have proposed that defects characterized by a deep vertical component with the buccal and lingual bone plates preserved have more predictable outcomes following regenerative therapy.[13] In our paper, we have shown that even a large buccal bone defect can be treated when the proposed protocol is fully applied.
Although our patient has good oral health maintenance, the abscessed peri-implantitis occurred 40 days after the implant deposition. Since the patient is a smoker (7-8 cigarettes per day), this could be the reason of implant failure, taking into consideration the fact that mandibular cortical width was not
Figure 3: (a) Panoramic X-ray showing a healthy bone around the implant, (b) picture of healthy gingiva at the implant site, (c) picture of healthy gingiva at the implant site, (d) exposure of the cover screw, (e) exposure of the cover screw, (f) removal of the cover screw
d
cb
f
a
e
Figure 4: (a) Application of the gingiva former, (b) after removing the gingival former, a thick gingiva is seen, (c) look of the gingiva after removing of gingiva former by the 10th day, (d) impression, (e) cast
d
cba
e
4 International Dental & Medical Journal of Advanced Research ● Vol. 3 ● 2017
Treatment of early implantitis Bilal
a significant predictor of either implant failure or bone loss (in our case, the implant site was over drilled).[14,15] No matter what the reason of the studied peri-implantitis, a bacterial cause-risk is highly considered, this is why an anti-biodose was subscribed. Augmentin is known to be a broad-spectrum agent, exhibiting activity against a wide range of Gram-positive and Gram-negative bacteria. Bacteria have major contributors to the rising number of dental implant failures associated with early and late peri-implantitis.[16]
At the implant level, it was crucial to rehabilitate the implant surface to activate a re-osseointegration, taking into consideration that bacteria lead to implant surface oxidation and dissolution of metal ions.[16] Re-osseointegration requires implant surface detoxification and the application of chemotherapeutic agents such as tetracycline, chlorhexidine gluconate, and citric acid. In this case, we first used the hydrogen peroxide for its ability to decrease plaque and gingivitis indices[17] and to clean the implant surface and site at time and could prepare the implant surface to be actively treated by the citric acid. The next step was to prepare the implant surface to receive the biological components by the surrounding bone, in a way to provoke a neo- or re-osseointegration. A recent study has shown that improved bone-to-implant response was observed for the acid-etched implant surface.[18,19] One case report has mentioned the use of the citric acid but without using hydrogen peroxide at 3%. The effect of citric acid on the implant surface is not new; however, we suggest that the complementary use of hydrogen peroxide and citric acid has enhanced the alveolar bone healing and the activation of a new re-osseointegration process.
Conclusion
A wide combined treatment that adjuncts the antibiotic program to a surface implant preparation all together sustained by an
invasive but regenerating surgery led to great results in the treatment of movable implants in a defected alveolar bone next to an aggressive abscessed peri-implantitis. The good diagnosis and the fast intervention made the re-integration of the implant in a biological bone possible.
Clinical significance
Although the use of bone graft and collagen membrane, with the possible risk of membrane exposure has been fully discussed by several authors, we encourage the use of the combined procedure of bone and membrane to stabilize the graft into the bone crater. This is crucial for the formation of a neo-alveolar bone that surrounds the exposure surface of the defected implant. In addition, to keep the epithelial cells from invasion the surgical site. We performed this particular step to regenerate a biological and anatomo-physiological unit that stabilize the implant and offer a healthy reliable prognosis.
References
1. Albrektson T, Isidor F. Consensus Report: Implant Therapy. In: Lang NP, Karring T, editors. Proceedings of the 1st European Workshop on Periodontology. Berlin: Quintessence; 1994. p. 365-9.
2. Lang NP, Berglundh T; Working Group of Seventh European Workshop on Periodontology. Periimplant diseases: Where are we now? – Consensus of the Seventh European workshop on periodontology. J Clin Periodontol 2011;38 Suppl 11:178-81.
3. Lindhe J, Meyle J; Group D of European Workshop on Periodontology. Peri-implant diseases: Consensus report of the sixth European workshop on periodontology. J Clin Periodontol 2008;35 8 Suppl:282-5.
4. Balevi B. Patients who received preoperative antibiotics showed fewer early implant failures. J Am Dent Assoc 2014;145:1068-70.
5. Brügger OE, Bornstein MM, Kuchler U, Janner SF, Chappuis V, Buser D. Implant therapy in a surgical specialty clinic: An analysis of patients, indications, surgical procedures, risk factors, and early failures. Int J Oral Maxillofac Implants 2015;30:151-60.
6. Han HJ, Kim S, Han DH. Multifactorial evaluation of implant failure: A 19-year retrospective study. Int J Oral Maxillofac Implants 2014;29:303-10.
7. Claffey N, Clarke E, Polyzois I, Renvert S. Surgical treatment of peri-implantitis. J Clin Periodontol 2008;35 8 Suppl:316-32.
8. Schwarz F, Sahm N, Schwarz K, Becker J. Impact of defect configuration on the clinical outcome following surgical regenerative therapy of peri-implantitis. J Clin Periodontol 2010;37:449-55.
9. Behneke A, Behneke N, d’Hoedt B. Treatment of peri-implantitis defects with autogenous bone grafts: Six-month to 3-year results of a prospective study in 17 patients. Int J Oral Maxillofac Implants 2000;15:125-38.
10. Khoury F, Buchmann R. Surgical therapy of peri-implant disease: A 3-year follow-up study of cases treated with 3 different techniques of bone regeneration. J Periodontol 2001;72:1498-508.
11. Roos-Jansåker AM, Renvert H, Lindahl C, Renvert S. Surgical treatment of peri-implantitis using a bone substitute with or without a resorbable membrane: A prospective cohort study.
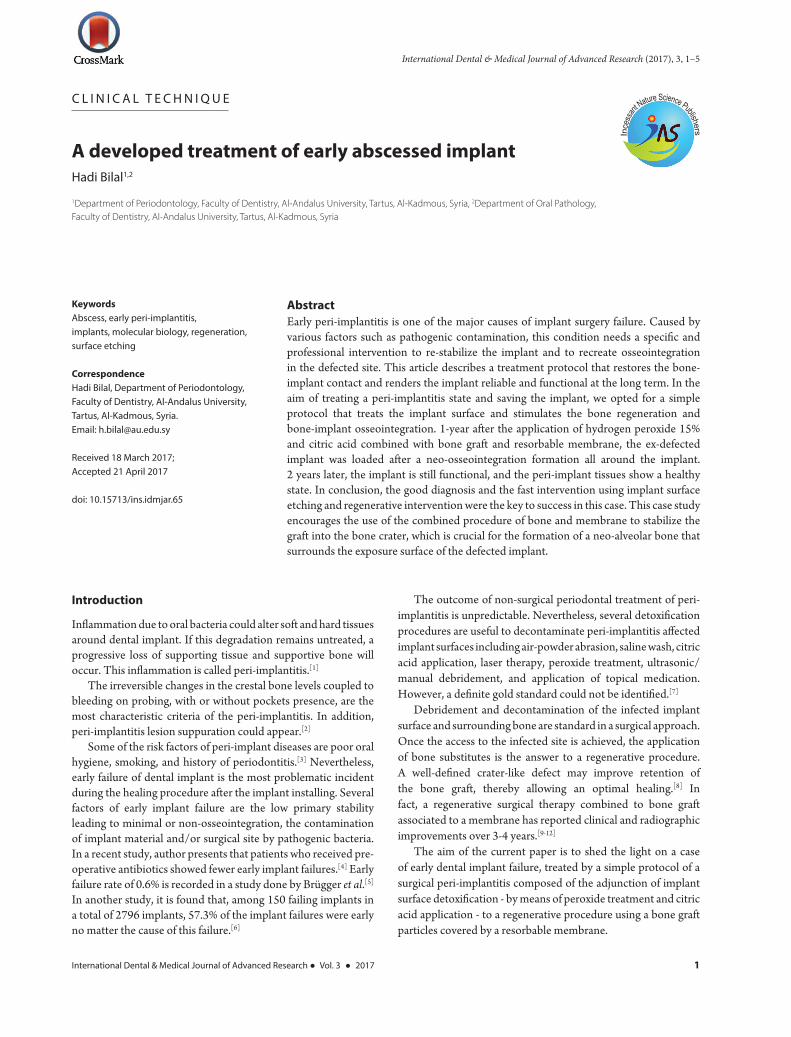
Figure 5: (a) The implant is loaded after 10 days of gingival forming, (b) photograph of the functional implant 2 years after retreatment, and more than 1 year after loading. Slight mesial and marginal inflammation with, pockets or bleeding on probing are not detected
ba

International Dental & Medical Journal of Advanced Research ● Vol. 3 ● 2017 5
Bilal Treatment of early implantitis
J Clin Periodontol 2007;34:625-32.12. Schwarz F, Sahm N, Bieling K, Becker J. Surgical regenerative
treatment of peri-implantitis lesions using a nanocrystalline hydroxyapatite or a natural bone mineral in combination with a collagen membrane: A four-year clinical follow-up report. J Clin Periodontol 2009;36:807-14.
13. Bassi F, Poli PP, Rancitelli D, Signorino F, Maiorana C. Surgical Treatment of Peri-Implantitis: A 17-year follow-up clinical case report. Case Rep Dent 2015;2015:574676.
14. Merheb J, Graham J, Coucke W, Roberts M, Quirynen M, Jacobs R, et al. Prediction of implant loss and marginal bone loss by analysis of dental panoramic radiographs. Int J Oral Maxillofac Implants 2015;30:372-7.
15. Chrcanovic BR, Albrektsson T, Wennerberg A. Smoking and dental implants: A systematic review and meta-analysis. J Dent 2015;43:487-98.
16. Sridhar S, Wilson TG Jr, Palmer KL, Valderrama P, Mathew MT, Prasad S, et al. In vitro investigation of the effect of oral bacteria in the surface oxidation of dental implants. Clin Implant Dent Relat Res 2015;17 Suppl 2:e562-75.
17. Meffert RM. How to treat ailing and failing implants. Implant Dent 1992;1:25-33.
18. Marshall MV, Cancro LP, Fischman SL. Hydrogen peroxide: A review of its use in dentistry. J Periodontol 1995;66:786-96.
19. Yoo D, Marin C, Freitas G, Tovar N, Bonfante EA, Teixeira HS, et al. Surface characterization and in vivo evaluation of dual acid-etched and grit-blasted/acid-etched implants in sheep. Implant Dent 2015;24:256-62.
How to cite this article: Bilal H. A developed treatment of early abscessed implant. Int Dent Med J Adv Res 2017;3:1-5.
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/© Bilal H. 2017


















