A Predictive Modeling and Decision-Making Tool to Facilitate

Decision support system to facilitate management of patients with acute GIB Page 1 of 41, Chu, et al
A decision support system to facilitate management of patients with acute gastrointestinal bleeding. Adrienne Chu, Hongshik Ahn, Bhawna Halwan, Everson LA Artifon, Alan Barkun, Michail G. Lagoudakis and Atul Kumar. (AC, HA and BH contributed equally to the study) The study was funded by 2005 Research and Outcomes Effectiveness Awards of the American Society of Gastrointestinal Endoscopy. Corresponding author: Atul Kumar, MD, MBA Staff Gastroenterologist-United States Department of Veterans Affairs Assistant Professor of Medicine-Stony Brook University Stony Brook, NY 11794. Phone: (631) 880-8510 FAX: (631) 486-6113 email: [email protected] Adrienne Chu, BS Department of Applied Mathematics and Statistics Stony Brook University Stony Brook, NY 11794. Hongshik Ahn, PhD Professor Department of Applied Mathematics and Statistics Stony Brook University Stony Brook, NY 11794. Bruce Kalmin, MD Division of Gastroenterology, Medical University of South Carolina Charleston, SC 29425. Everson LA Artifon, MD, PhD Assistant Professor Gastroenterology & Hepatology University of Sao Pualo School of Medicine Sao Paulo, Brazil. Alan Barkun, MD, MS Professor of Medicine, General Surgery, and Epidemiology Division Director, Gastroenterology Mc Gill University Montreal, Canada H3A 2T5.

Decision support system to facilitate management of patients with acute GIB Page 2 of 41, Chu, et al
Michail G. Lagoudakis, PhD Assistant Professor Intelligent Systems Laboratory Department of Electronic and Computer Engineering Technical University of Crete Kounoupidiana, 73100 Chania Hellas (Greece). Bhawna Halwan, MD, MS Assistant Professor of Medicine, Gastroenterology & Hepatology SUNY Downstate Brooklyn, NY 11203.

Decision support system to facilitate management of patients with acute GIB Page 3 of 41, Chu, et al
ABSTRACT
Objective: To develop a model to predict the bleeding source and identify the cohort
amongst patients with acute gastrointestinal bleeding (GIB) who require urgent
intervention, including endoscopy. Patients with acute GIB, an unpredictable event,
are most commonly evaluated and managed by non-gastroenterologists. Rapid and
consistently reliable risk stratification of patients with acute GIB for urgent
endoscopy may potentially improve outcomes amongst such patients by targeting
scarce healthcare resources to those who need it the most.
Design & Methods: Using ICD-9 codes for acute GIB, 189 patients with acute GIB
and all available data variables required to develop and test models were identified
from a hospital medical records database. Data on 122 patients was utilized for
development of the model and on 67 patients utilized to perform comparative
analysis of the models. Clinical data such as presenting signs & symptoms,
demographic data, presence of co-morbidities, laboratory data and corresponding
endoscopic diagnosis and outcomes were collected. Clinical data and endoscopic
diagnosis collected for each patient was utilized by to retrospectively ascertain
optimal management for each patient. Clinical presentations and corresponding
treatment was utilized as training examples. Eight mathematical models including
artificial neural network (ANN), support vector machine (SVM), k-nearest neighbor,
linear discriminant analysis (LDA), shrunken centroid (SC), random forest (RF),
logistic regression, and boosting were trained and tested. The performance of these
models was compared using standard statistical analysis and ROC curves.

Decision support system to facilitate management of patients with acute GIB Page 4 of 41, Chu, et al
Results: Overall the random forest model best predicted the source, need for
resuscitation, and disposition with accuracies of approximately 80% or higher
(accuracy for endoscopy was greater than 75%). The area under ROC curve for RF
was greater than 0.85, indicating excellent performance by the random forest model.
Conclusion: While most mathematical models are effective as a decision support
system for evaluation and management of patients with acute GIB, in our testing RF
model consistently provided the best accuracy. Amongst patients presenting with
acute GIB, mathematical models may facilitate the identification of the source of
GIB, need for intervention and allow optimization of care and healthcare resource
allocation; these however require further validation.
Key words: class prediction, cross validation, gastrointestinal bleeding, machine
learning

Decision support system to facilitate management of patients with acute GIB Page 5 of 41, Chu, et al
1. INTRODUCTION
Acute gastrointestinal bleeding (GIB) is an increasing healthcare problem due to rising
NSAID use and an aging population [1]. Further reductions in mortality will most likely
require introduction of novel strategies to aid identification of the cohort requiring
aggressive resuscitation and endoscopic intervention to prevent complications and
death from ongoing bleeding [2,3]. Delays in intervention usually result from failure to
adequately recognize the source and severity of the bleed. Although several models
and scores have been developed to risk-stratify patients, no single model aids the
identification of the subgroup of patients presenting with acute upper or lower GIB most
likely to benefit from urgent intervention [4,5]. Our goal was to utilize mathematical
models to formulate a decision support system utilizing clinical and laboratory
information available within a few hours of patient presentation to predict the source,
need for intervention and disposition in patients with acute upper, mid and lower GIB.
There are a number of well-known classification tools for analyzing data, including
artificial neural networks (ANN), k-nearest neighbor (kNN), decision trees, support
vector machines (SVM), and shrunken centroid (SC) [6,7]. These classification tools
are supervised learning methods where the algorithm learns from a training set and
establishes a prediction rule to classify new samples using statistical approaches for
class prediction. Logistic regression, an alternative to these classification methods, and
Fisher’s linear discriminant analysis (LDA) are both parametric approaches. Logistic
regression and LDA do not differ in functional form, and differ only in the estimation of
coefficients; LDA assumes normal distribution of the explanatory variables, while logistic
regression does not. If the Gaussian assumptions are met, then LDA is a more

Decision support system to facilitate management of patients with acute GIB Page 6 of 41, Chu, et al
powerful and efficient model than logistic regression. Standard statistical model building
relies on an a priori collection of predictor variables for identifying outcomes of clinical
interest. Often it may be computationally impossible for standard models to overcome
the complexities of problems with large dimensionality. Support Vector Machines
(SVM), introduced by Vapnik (1995) can overcome the high dimensionality problem
computationally and is consistently a good classifier and hence widely utilized as a
classification method. Following the recent introduction of ensemble-voting
approaches, two ensemble voting methods, boosting and bagging, have also gained
wide popularity [8,9]. An ensemble uses the predictions of multiple base classifiers
through majority voting. Boosting, a meta-classifier, combines weak classifiers and
takes a weighted majority vote of their predictors. Breiman (2001) developed the
random forest (RF) method by combining classification tree predictors [10]. The
bagging algorithm in RF uses bootstrap samples to build base trees. Each bootstrap
sample is formed by randomly sampling, with replacement, the same number of
observations as the training set. The final classification produced by the ensemble of
these base classifiers is obtained using equal weight voting.
The study objective was to develop and compare the performance of eight classification
models as described above to predict clinical outcomes in patients presenting with
acute GIB.

Decision support system to facilitate management of patients with acute GIB Page 7 of 41, Chu, et al
2. METHODS
2.1 Definitions
Upper GIB refers to gastrointestinal blood loss whose origin is proximal to the ligament
of Treitz; mid GIB whose source was below the ligament of Trietz but proximal to the
ileocecal valve and lower GIB referred to gastrointestinal blood loss emanating from a
source distal to the ileocecal valve [11]. Acute GIB was defined as bleeding of less than
5 days duration. Acute upper GIB was diagnosed if there was hematemesis, "coffee
ground" colored emesis, the return of red blood via a nasogastric tube, and/or melena
with or without hemodynamic compromise or hematochezia (bright red blood per rectum
in patients with brisk upper GIB) and the presence of a bleeding source in the upper GI
tract at endoscopy. Patients with melena and/or hematochezia along with clinical
evidence of bleeding (hemodynamic instability, anemia) and positive findings of a
bleeding source at enteroscopy or capsule endoscopy were designated as mid GIB.
Lower GIB was defined as the identification of a source of bleeding in the lower GI in
patients presenting with hematochezia. Hypotension was defined as systolic blood
pressure of less than 100, tachycardia as heart-rate of greater than 100 beats/minute,
orthostasis as a drop of systolic blood pressure of greater than 20mm Hg and an
increase in heart rate of greater than 20 mmHg, 2 minutes after sitting upright from
recumbency with legs dangling from the side of the bed. Urgent endoscopy was
defined as a procedure that was performed within 24 hours for upper GIB and within 48
hours for lower GIB.
2.2 Patients

Decision support system to facilitate management of patients with acute GIB Page 8 of 41, Chu, et al
Patients with acute GIB were identified from the hospital medical records database
using ICD-9 codes for GIB. The study was carried out in compliance with all institutional
human investigations committee guidelines. Eligible patients were those presenting
with clinical manifestations of acute upper or lower gastrointestinal bleeding and those
who had undergone endoscopy within 24 hours for suspected upper GIB and within 48
hours for suspected lower GIB or if upper endoscopy was negative. If no obvious
source of GIB was identified at either upper or lower endoscopy, the patient should
have undergone small bowel enteroscopy or capsule endoscopy within 1 week of the
initial episode of acute GIB. Records of patients for whom a definite source of bleeding
could not be identified or those with missing clinical variables required for model
building and testing were discarded. A total of 189 patients meeting inclusion and
exclusion criteria were identified retrospectively in hospital electronic medical records.
Clinical data on each patient was entered into a scannable data entry form which was
scanned into an SQL database and manually reviewed for errors. Variables to
ascertain clinical outcomes corresponding to patient data included clinical and
endoscopic data as listed in Box 1. Variables that correlate with and are predictive of
clinical outcomes amongst patients with acute GIB were identified from a review of the
literature [12, 21]. Initially only 70 patient data were available when first building and
testing the models. This was followed by building and testing models using a total of
122 patients which resulted in an insignificant improvement in performance of the
models (data not shown). A sample size of 122 patients was therefore deemed to be
adequate for building models. An additional 67 patient database was utilized for testing
and validation of the models.

Decision support system to facilitate management of patients with acute GIB Page 9 of 41, Chu, et al
2.3 Selection of independent variables to predict outcomes for test cases
Several studies in the past have evaluated variables predictive of adverse outcomes,
predictive of source, severity and outcomes in patients with acute upper and lower GIB.
Clinical correlates of source, severity and outcomes amongst patients with acute
gastrointestinal bleeding were reviewed and listed as in Box 3 [17-29].
Bleeding source: The definitive source of bleeding was the irrefutable identification of
a bleeding source at upper endoscopy, colonoscopy, small bowel enteroscopy or
capsule endoscopy. Variables utilized to predict the source of GIB included past
medical history & presenting symptoms (prior history of GIB, hematochezia,
hematemesis, melena, syncope/presyncope), risk factors (risk for stress ulceration,
cirrhosis, ASA/NSAID use) physical exam and laboratory tests (blood pressure
(SBP/DBP), heart rate (HR), orthostasis, NG lavage, rectal exam, platelet count (Plt),
creatinine (Cr), BUN, and INR).
Blood resuscitation: Urgent blood resuscitation referred specifically to the
administration of blood and blood products to correct loss of intravascular volume and
presence of coagulopathy. Variables utilized to predict this outcome included
symptoms (hematochezia, hematemesis, melena, duration of symptoms,
syncope/presyncope), prior history (unstable CAD), physical exam and laboratory tests
(blood pressure, heart rate, orthostasis, NG lavage, rectal exam, hematocrit (Hct), drop
in hematocrit, creatinine, BUN, and INR).
Urgent endoscopy: Variables to predict need for urgent endoscopy included
symptoms (hematochezia, hematemesis, melena, syncope/presyncope, duration of
symptoms), risk factors (cirrhosis, ASA/NSAID use) and physical exam and laboratory

Decision support system to facilitate management of patients with acute GIB Page 10 of 41, Chu, et al
tests (blood pressure, heart rate, orthostasis, NG lavage, rectal exam, hematocrit,
hematocrit drop, platelet count, creatinine, BUN, and INR).
Disposition: Variables utilized to predict disposition included patient demographics
(age), presenting symptoms (hematochezia, hematemesis, melena, duration of
symptoms, syncope/presyncope), comorbidities (unstable CAD, COPD, CRF, risk for
stress ulcer, cirrhosis), clinical exam/blood tests (blood pressure, heart rate, orthostasis,
NG lavage, rectal exam, hematocrit, drop in hematocrit, platelet count, creatinine, BUN,
and INR).
2.4 Algorithm for analysis of clinical data to ascertain outcomes for training set
The algorithm to ascertain the source of bleeding and appropriate clinical management
for each patient is as illustrated in Figure 1 and was determined jointly by authors (AK,
BH, BK) after careful analysis of the clinical and endoscopic data for each patient, in
accordance with current evidence and standard of care [13-15]. Source was
ascertained by review of endoscopic findings for each patient [16]. Patients with
findings of active bleeding or other high-risk stigmata at endoscopy were reasoned as
requiring intensive resuscitation, urgent endoscopy and admission to the medical
intensive care unit. Patients with low-risk stigmata at endoscopy and hemodynamic
instability (hypotension, tachycardia, orthostasis), elevated coagulation parameters
and/or hematocrit <30, were reasoned to require intensive resuscitation but no urgent
endoscopy. Conversely, patients under 60 years of age with no active bleeding or high-
risk stigmata and no co-morbidities were reasoned as suitable for discharge to home,
while patients with co-morbidities were categorized as requiring admission to general
inpatient. Example: A 60 year old patient with acute onset of profuse hematemesis,

Decision support system to facilitate management of patients with acute GIB Page 11 of 41, Chu, et al
melena, dizziness, tachycardia, hypotension, positive nasogastric lavage, hematocrit of
24, is admitted to the regular floor and undergoes endoscopy greater than 24 hours
after admission. Endoscopy reveals an oozing blood vessel within an ulcer bed. Since,
in retrospect the patient should have been resuscitated urgently with blood, undergone
urgent endoscopy and admitted to the ICU, the patient was classified as requiring
urgent resuscitation, endoscopy and admission to the ICU. Each case was similarly
analyzed to identify the corresponding optimal outcome and the database thus
developed was utilized to train the models.
2.5 Importance of each variable
For RF and ANN, the variable importance option was selected to see if these variables
were significant for ascertaining outcomes by the computer models. Variable
importance for RF is given in terms of the mean decrease in accuracy, hence higher the
number, greater the importance of the variable. ANN provides data about the
importance of a variable without any ranking. Hence the variable importance feature for
ANN was repeated ten times in order to obtain rankings for the variables and the
number of times a variable was shown to be important was counted; the closer the
number was to 10, the more important the variable. In addition, distributions of the
variables as well as correlation between variables were examined.
2.6 Models & Statistical Analysis
Eight predictive models including random forest (RF), support vector machines (SVM),
shrunken centroid (SC), linear discriminant analysis (LDA), k-nearest neighbor (kNN),
logistic regression (logistic), boosting, and artificial neural networks (ANN) were trained
and their performances compared [8,9]. All models were run in R (version 2.3.0,

Decision support system to facilitate management of patients with acute GIB Page 12 of 41, Chu, et al
downloadable from http://cran.cnr.berkeley.edu) except for ANN, which was run in
STATISTICA (version 7.1, Statsoft, Inc, Tulsa, OK).
Model training was performed on a randomly selected subset of patients and testing on
the remaining patients of a total of 122 patient database. The primary approach was to
use the selected explanatory variables to predict the response variable discarding any
patients with missing data. In addition, for predicting resuscitation and endoscopy, an
alternative strategy was adopted. The predicted value of “source of bleeding” and
selected input variables (hematochezia, hematemesis, syncope/presyncope, blood
pressure, heart rate, orthostasis, NG lavage, and INR) were utilized to predict the need
for resuscitation and endoscopy. Categorical variables were changed accordingly to
indicator variables.
Model Evaluation Step: Ten runs of 10-fold cross validation (CV) were performed for
each iteration to obtain a reliable result with low mean square error (MSE) and bias [30].
The MSE is a function of bias and variance and when the estimator is unbiased, MSE
reduces to variance because the bias term in MSE becomes zero. Each run of cross
validation is comprised of independent training and testing database, where 90% of the
data is put in the training set and the remaining 10% of the data is put into the test set.
For every 10-fold CV, the following statistics were calculated: sensitivity (SN), specificity
(SP), accuracy (ACC: the sum of correct predictions divided by total predictions),
positive predictive value (PPV: probability that the patient is truly positive given a
positive prediction), and negative predictive value (NPV: probability that a patient is truly
negative given a negative prediction). For each classification model, statistical results
of 10 repetitions of 10-fold CV were averaged and reported.

Decision support system to facilitate management of patients with acute GIB Page 13 of 41, Chu, et al
ROC curves were calculated and areas under the curve were compared for each of the
eight models. The Mann-Whitney statistic was calculated, which is equivalent to the
area under an ROC curve [31]. Additionally, performance measures between models
were compared using McNemar’s test. Using the Bonferroni correction to account for
multiple comparisons of models, an appropriate alpha value was used for each test to
control the error rate. For example, there were 8 models for the resuscitation response;
hence there were 28 pair-wise comparisons. Thus for an original alpha value of .05, the
new alpha used for a two-sided test was .05/28=.0018. A normal approximation and
Central Limit Theorem was used for underlying assumptions for the test.
Model Validation Step: After models had been trained using a 122 patient database,
an unseen before 67 patient database was utilized as a test set to validate the model.
Accuracies were compared for both the evaluation step and the validation step.
2.7 Individual Model Parameters
Random forest (package Random Forest): All default settings were used (500 trees
were grown and the number of variables randomly sampled at each node was
p where p is the number of explanatory variables). The variable option of importance
was set to true. To predict the outcome of a certain patient, voting was done without
normalizing.
Support vector machine (package e1071): All default settings were used, variables
were scaled, tolerance value to terminate algorithm was set to .001, epsilon set to 1 (for
insensitive-loss function). Both the radial basis (default) and linear kernels were
considered, but only the radial basis function is included in this comparison because the
two kernels gave similarly high accuracies.

Decision support system to facilitate management of patients with acute GIB Page 14 of 41, Chu, et al
Shrunken centroid (package pamr): An optimal threshold value for each response
was found by cross validation. The best threshold value was one that gave the highest
accuracies – a threshold of .2 was used for all responses.
Linear discriminant analysis (package sma), kNN (package class), and logistic
regression (package stats) models: All default settings were used. Depending on
what response variable was being classified, a different k was used for kNN. By
performing CV on several different k values, the k that yielded the highest accuracy was
chosen. The final values chosen were k=7 for source and resuscitation, k=11 for
endoscopy, and k=3 for disposition.
Boosting (package boost): No features were pre-selected (presel=0), boosting ran for
10 iterations (mfinal=10). The optimal settings were found by trying different
combinations of presel and mfinal. The R Boosting package contains four different
approaches: AdaBoost, LogitBoost, L2Boost and BagBoost. AdaBoost was excluded,
as often it did not classify patients correctly. Performance of the other three boosting
methods were similar. Among these three approaches, LogitBoost is included in the
comparison.
ANN (Neural Networks package): Multilayer perceptrons with back propagation was
performed. The error function used was the cross entropy function. A linear synaptic
function was used and a combination of the following four activation functions were
used: linear, hyperbolic, softmax, and logistic. The number of epochs to train the model
was set to 100 although the network always converged in less number of epochs. The
learning rate was set to .01 and there was one hidden layer in the network. For the
source of bleeding response, there were 30 input neurons, 11 hidden neurons (neurons

Decision support system to facilitate management of patients with acute GIB Page 15 of 41, Chu, et al
in the hidden layer), and 3 output neurons. For the resuscitation response, there were
28 input neurons, 10 hidden neurons, and 1 output neuron. For the endoscopy
response, there were 31 input neurons, 12 hidden neurons, and 1 output neuron. For
the disposition response, there were 34 input neurons, 34 hidden neurons, and 1 output
neuron.
3. RESULTS
3.1 Models
Tables 1 through 4 summarize the results for each outcome prediction variable for the
evaluation step. Eight models were run (only six of the eight models were utilized to
predict source, since logistic regression and boosting can be only used for 2-way
classification problems (while output source included three outcomes-upper, mid and
lower) using the primary approach. Figures 2 through 5 depict the accuracies obtained
from each individual model and each response variable for the evaluation step. Overall,
accuracies obtained using SVM, RF, and LDA were numerically superior to others, with
these models correctly predicting the source of bleeding, need for resuscitation, and
disposition correctly 88%-94% of the time. The need for endoscopy was correctly
predicted about 80% of the time using SVM, SC, and LDA; accuracy using RF was just
under 80% at 79%. Logistic regression did well for predicting resuscitation and
endoscopy, however it did not do well for disposition. This is because the algorithm for
obtaining the model rarely converged, that is, it was unstable (results not shown).
Accuracies using boosting were worst of all models. Accuracies obtained ANN model
was inferior to SVM, RF and LDA. At a significance level of α=0.05, kNN performed the
worst for predicting source and resuscitation. The linear discriminant analysis model

Decision support system to facilitate management of patients with acute GIB Page 16 of 41, Chu, et al
appeared to demonstrate a good overall performance with regards to sensitivity
specificity, PPV, NPV and accuracy (Tables 1 through 4). Boosting, on the other hand,
revealed an imbalance between sensitivity and specificity. ROC curves were
constructed (Figures 6 through 9 and Tables 1 through 4), and overall RF and ANN
have the highest AUC (area under the curve), followed by SVM and LDA. For
predicting resuscitation and endoscopy, the logistic model had excellent AUC. In the
validation step, RF consistently predicted responses with higher accuracies as
compared to the other models (Table 6). Overall, data from evaluation and validation
steps suggests that the RF model consistently performs the best.
3.2 Importance of variables
The importance of each variable in predicting outcomes in ascertaining relevant
outcomes when using random forest and ANN respectively are shown in Table 7 (using
122 patient database). About half the variables to predict outcomes were of common
importance to both RF and ANN models. For predicting source, explanatory variables
hematemesis through HR (heart rate) had significant weights and hence importance.
The remaining variables were of variable importance aside from ASA/NSAID, which did
not appear to have great influence on the performance of the models. For predicting
resuscitation, both models utilized the variables syncope, orthostasis, hematocrit,
hematocrit drop, blood pressure, heart rate, hematemesis and melena as important
predictor variables. The remainder of the variables was of limited and variable
importance in predicting outcomes.

Decision support system to facilitate management of patients with acute GIB Page 17 of 41, Chu, et al
4. DISCUSSION AND CONCLUSION
Although superior healthcare outcomes may be expected if gastroenterologists manage
all patients with acute GIB [32], it is logistically impossible for every patient with acute
GIB to be emergently evaluated and treated by a gastroenterologist, as the onset of
acute GIB is unpredictable. It is also impractical and economically unjustifiable to
subject every patient with acute GIB to intensive resuscitation and urgent endoscopy as
only 20% of patients with acute GIB may require urgent intervention and furthermore
because healthcare resources are expensive and limited. “Expert systems” may
potentially substitute for a specialist amongst patients with acute GIB and facilitate
triage the cohort most likely to benefit from urgent resuscitation and endoscopy.
“Machine learning” or computer-assisted predictive models have been successfully
utilized to optimize treatment and predict clinical outcomes in a variety of other
conditions [33-36], such as computerized interpretation of the electrocardiogram [37], to
help streamline and optimize care of patients with acute myocardial infarction [38],
especially in a busy practice or in the emergency room [39]. Our objective was to
develop a system to provide diagnostic and specific treatment recommendations for
patients presenting with acute GIB. Such models have previously been shown to
accurately predict the need for colonoscopy in patients with acute lower GIB [5].
However, they have not been used for all patients with acute GI bleeding. The
recommendations were designed to be in agreement with current evidence based
guidelines for management of acute GIB. Our models successfully provided patient
specific recommendations with accuracies exceeding 70-80%. In the present study, RF
performed well in classification of the four response variables, in agreement with

Decision support system to facilitate management of patients with acute GIB Page 18 of 41, Chu, et al
previous studies that have demonstrated the robustness of such models. RF and SVM
are designed for high-dimensional data with a large feature space (large number of
predictor variables) compared to the sample size and are likely to outperform other
methods for high-dimensional data unlike the current GIB data set [40]. Logistic
regression is a widely used standard regression model for binary data, and it can be
expanded to data with more than two classes. However, it often shows computational
instability such as failure to converge or the predicted value being extremely close to 1
or 0 due to the nature of the model. Our results also support the conclusion by Ahn et
al. in previous studies, that boosting strategies in general provide poor accuracies [40].
Furthermore, given its complexity, these are also cumbersome and unwieldy as
compared to other methods. Although not relevant to our problem, LDA and kNN
require a variable pre-selection for an optimal performance unlike RF or SVM for high-
dimensional data.
Statistical variable selection is often dependent on the criteria and is computer
intensive. With regards to the analysis of the importance of variable, we show that both
the RF and ANN models considered half of the variables to be important with the
remaining half being of varied importance. This appears to be consistent with prior
knowledge in regards to importance of variables identified to predict source and severity
of acute GIB. Every pre-selected variable was important for one model or the other and
therefore consistent with their identification in prior multivariate analysis. Different
models assigned varied importance to different variables due to the different methods
for evaluating variable importance. In RF, for every tree grown in the forest, test
samples are used to count the number of votes cast for the correct class. RF randomly

Decision support system to facilitate management of patients with acute GIB Page 19 of 41, Chu, et al
permutes the values of a selected variable in the test set and put these cases down the
tree. It finds the number of votes for the correct class in the data with this permuted
variable. It subtracts this number from the number of votes for the correct class in the
original data without permutation. The average of this number of all trees in the forest is
the raw importance score for the variable. ANN uses a Connection Weight Approach to
quantify variable importance. Given that a minimal variable set to predict outcomes is
desirable, overall our dataset appears to be optimal to predict clinical outcomes relevant
to management of patients with acute GIB.
Since the output utilizes training examples which are developed by individuals, bias can
potentially be introduced through using inaccurate training examples. The authors have
the ability to influence the recommendations by modulating outcomes associated with
each training example. Since, examples are utilized to train the models, flaws in
examples may lead to flaws in the model output: garbagae in-garbage out. Despite
these flaws, such systems have the potential to facilitate and standardize the care of
patients presenting with acute GIB. Given that computer based tools are more likely to
work if integrated with clinical care, prospective validation and integration of such a
model into an electronic medical record may potentially enhance care of patients with
acute GIB. It is also possible to train the model using fresh examples so as to adapt to
changing guidelines and varied clinical scenarios, allowing these predictive models to
be portable to a broad range of locales. The prospective development and testing of a
model using a larger patient cohort prospectively, its implementation and comparison of
its performance to physicians is underway.

Decision support system to facilitate management of patients with acute GIB Page 20 of 41, Chu, et al
In summary, predictive models such as shown above, allow the identification of the
high-risk cohort amongst patients presenting with acute GIB to allow optimal allocation
of resources to patients who may potentially benefit the most from urgent resuscitation,
endoscopy and intensive clinical care.

Decision support system to facilitate management of patients with acute GIB Page 21 of 41, Chu, et al
Box 2. Output variables
Source: Upper, Mid, Lower Resuscitation: Yes or No Endoscopy: Yes, No Disposition: not ICU (home, floor, monitor); ICU
Box 1: Independent variables
Presentation:
Hematemesis/Coffee Grounds Hematochezia/Melena Duration of symptoms Syncope/presyncope
Demographics:
Age, gender
Past history:
Prior GIB, Unstable CVD (MI, CHF), COPD exacerbation, CRF, Risk of Stress Ulcer, Cirrhosis
ASA/NSAID use, PPI, prior history of GIB
Clinical Exam:
SBP/DBP, HR, orthostasis, NG lavage, rectal exam
Laboratory Data:
Hematocrit, drop in Hct., platelet count, creatinine, BUN, PT/INR
Box 3: Explanatory variables used for each output Source of bleeding: prior history of GIB, hematochezia, hematemesis, melena, syncope/presyncope, risk for stress ulcer, cirrhosis, ASA/NSAID use, blood pressure, heart rate, orthostasis, NG lavage, rectal exam, platelet count, creatinine, BUN, INR Resuscitation: hematochezia, hematemesis, melena, duration of symptoms, syncope/presyncope, unstable CAD, blood pressure, heart rate, orthostasis, NG lavage, rectal exam, hematocrit, drop in hematocrit, creatinine, BUN, INR Endoscopy: hematochezia, hematemesis, melena, duration of symptoms, syncope/presyncope, cirrhosis, ASA/NSAIDs, blood pressure, heart rate, orthostasis, NG lavage, rectal exam, hematocrit, drop in hematocrit, platelet count, creatinine, BUN, INR Disposition: age, hematochezia, hematemesis, melena, duration of symptoms, syncope/presyncope, unstable CAD, COPD, CRF, risk for stress ulcer, cirrhosis, blood pressure, heart rate, orthostasis, NG lavage, rectal exam, hematocrit, drop in hematocrit, platelet count, creatinine, BUN, INR

Decision support system to facilitate management of patients with acute GIB Page 22 of 41, Chu, et al
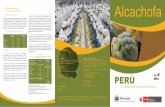
Figure 1. Schematic of training examples for classification
MANAGEMENT –RESUSCITATION, ENDOSCOPY AND DISPOSITION Upper Ulcer with High risk stigmata: Active bleeding, non-bleeding visible vessel, overlying clot, oozing. Varices: Active bleeding or stigmata of recent bleed. AVM/Dieulafoy’s/MW tear: ongoing bleeding/oozing recent bleeding. Lower
Diverticula/Colitis/AVM/Dieulafoys’s/Varices: active bleeding, visible vessel, overlying clot.
Symptoms
Dizzy, unstable CAD, SBP<90, orthostasis, Hct <30, INR >1.5
No Yes
No
Yes
URGENT RESUSCITATION
ASCERTAINING SOURCE OF BLEED Requires endoscopic evidence of a bleeding source Upper: Proximal to ligament of treitz. Mid: Distal to ligament of treitz & proximal to
ileo-cecal valve. Lower: Distal to ileo-cecal valve.
Any stigmata of bleeding (active bleeding, visible vessel, overlying clot, oozing, pigmented spot, ulcer), varices with stigmata of bleed (cherry red spot, angioectasia, red wale signs), AVM’s, MW tear, dieulafoys’s, diverticula.
Yes
URGENT ENDOSCOPY
Yes
Yes or No
ELECTIVE ENDOSCOPY
INTENSIVE CARE UNIT
ADMIT TO FLOOR
DISCHARGE
HOME
Age < 60, no comorbidities
No Yes
No

Decision support system to facilitate management of patients with acute GIB Page 23 of 41, Chu, et al
Figure 2. Accuracies for output-bleeding source (evaluation step) Accuracies for source
0.940.93
0.91
0.93
0.70
0.92
0.60
0.65
0.70
0.75
0.80
0.85
0.90
0.95
1.00
RF SVM SC LDA kNN ANN
Model Type
Accura
cy

Decision support system to facilitate management of patients with acute GIB Page 24 of 41, Chu, et al
Figure 3. Accuracies for output-resuscitation (evaluation step) Accuracies for resuscitation
0.930.94
0.92 0.92
0.88
0.92 0.92
0.65
0.60
0.65
0.70
0.75
0.80
0.85
0.90
0.95
1.00
RF SVM SC LDA kNN ANN logistic LogitBoost
Model Type
Ac
cu
ra
cy

Decision support system to facilitate management of patients with acute GIB Page 25 of 41, Chu, et al
Figure 4. Accuracies for output-endoscopy (evaluation step)
0.790.80
0.81
0.83
0.80
0.780.79
0.63
0.60
0.65
0.70
0.75
0.80
0.85
0.90
RF SVM SC LDA kNN ANN logistic LogitBoost
Model Type
Acc
ura
cy

Decision support system to facilitate management of patients with acute GIB Page 26 of 41, Chu, et al
Figure 5. Accuracies for output-disposition (evaluation step)
0.880.89
0.90 0.90
0.88
0.85
0.58
0.50
0.55
0.60
0.65
0.70
0.75
0.80
0.85
0.90
0.95
RF SVM SC LDA kNN ANN LogitBoost
Model Type
Acc
ura
cy

Decision support system to facilitate management of patients with acute GIB Page 27 of 41, Chu, et al
Figure 6. ROC curves for predicting source of bleeding (evaluation step)

Decision support system to facilitate management of patients with acute GIB Page 28 of 41, Chu, et al
Figure 7. ROC curves for predicting resuscitation (evaluation step)

Decision support system to facilitate management of patients with acute GIB Page 29 of 41, Chu, et al
Figure 8. ROC curves for predicting endoscopy (evaluation step)

Decision support system to facilitate management of patients with acute GIB Page 30 of 41, Chu, et al
Figure 9. ROC curves for predicting disposition (evaluation step)

Decision support system to facilitate management of patients with acute GIB Page 31 of 41, Chu, et al
Table 1. Evaluation step–performance of models for output source of bleeding (standard
error)
ACC SN SP PPV NPV AUC
RF 0.943 (0.007)
0.980 (0.004)
0.932 (0.007)
0.967 (0.005)
0.959 (0.006)
0.998
SVM 0.930 (0.007)
0.965 (0.005)
0.945 (0.007)
0.973 (0.005)
0.932 (0.007)
0.979
SC 0.914 (0.008)
0.965 (0.005)
0.890 (0.009)
0.946 (0.007)
0.927 (0.008)
0.978
LDA 0.931 (0.007)
0.965 (0.005)
1.000 (0.000)
1.000 (0.000)
0.935 (0.007)
0.987
kNN 0.697 (0.013)
0.901 (0.009)
0.287 (0.013)
0.717 (0.013)
0.591 (0.014)
0.658
ANN 0.917 (0.008)
0.972 (0.005)
0.936 (0.007)
0.968 (0.005)
0.944 (0.007)
0.999

Decision support system to facilitate management of patients with acute GIB Page 32 of 41, Chu, et al
Table 2. Evaluation step–performance of models for output resuscitation (standard error)
ACC SN SP PPV NPV AUC
RF 0.932 (0.007)
0.937 (0.007)
0.923 (0.008)
0.954 (0.006)
0.894 (0.009)
0.982
SVM 0.941 (0.007)
0.938 (0.007)
0.945 (0.007)
0.968 (0.005)
0.899 (0.009)
0.964
SC 0.915 (0.008)
0.929 (0.007)
0.891 (0.009)
0.936 (0.007)
0.879 (0.009)
0.920
LDA 0.922 (0.008)
0.904 (0.009)
0.955 (0.006)
0.972 (0.005)
0.852 (0.010)
0.937
kNN 0.884 (0.009)
0.903 (0.009)
0.852 (0.010)
0.914 (0.008)
0.835 (0.011)
0.890
ANN 0.921 (0.008)
0.927 (0.008)
0.910 (0.008)
0.946 (0.007)
0.880 (0.009)
0.993
logistic 0.923 (0.008)
0.939 (0.007)
0.895 (0.009)
0.940 (0.007)
0.897 (0.009)
0.985
LogitBoost 0.647 (0.014)
0.916 (0.008)
0.184 (0.011)
0.662 (0.014)
0.481 (0.014)
0.381

Decision support system to facilitate management of patients with acute GIB Page 33 of 41, Chu, et al
Table 3. Evaluation step–performance of models for output endoscopy (standard error)
ACC SN SP PPV NPV AUC
RF 0.790 (0.012)
0.854 (0.010)
0.671 (0.014)
0.828 (0.011)
0.712 (0.013)
0.871
SVM 0.803 (0.011)
0.859 (0.010)
0.700 (0.013)
0.842 (0.011)
0.728 (0.013)
0.820
SC 0.811 (0.011)
0.838 (0.011)
0.760 (0.012)
0.866 (0.010)
0.717 (0.013)
0.801
LDA 0.833 (0.011)
0.821 (0.011)
0.857 (0.010)
0.914 (0.008)
0.720 (0.013)
0.843
kNN 0.796 (0.012)
0.876 (0.010)
0.648 (0.014)
0.822 (0.011)
0.737 (0.013)
0.766
ANN 0.778 (0.012)
0.801 (0.012)
0.733 (0.013)
0.849 (0.010)
0.665 (0.014)
0.913
logistic 0.787 (0.012)
0.871 (0.010)
0.831 (0.014)
0.815 (0.011)
0.726 (0.013)
0.853
LogitBoost 0.627 (0.014)
0.891 (0.009)
0.138 (0.010)
0.658 (0.014)
0.403 (0.014)
0.404

Decision support system to facilitate management of patients with acute GIB Page 34 of 41, Chu, et al
Table 4. Evaluation step–performance of models for output disposition (standard error)
ACC SN SP PPV NPV AUC
RF 0.883 (0.009)
0.907 (0.008)
0.843 (0.011)
0.908 (0.008)
0.841 (0.011)
0.967
SVM 0.887 (0.009)
0.929 (0.007)
0.816 (0.011)
0.896 (0.009)
0.872 (0.010)
0.922
SC 0.897 (0.009)
0.916 (0.008)
0.866 (0.010)
0.921 (0.008)
0.858 (0.010)
0.891
LDA 0.897 (0.009)
0.891 (0.009)
0.909 (0.008)
0.943 (0.007)
0.830 (0.011)
0.901
kNN 0.876 (0.010)
0.923 (0.008)
0.798 (0.012)
0.886 (0.009)
0.858 (0.010)
0.881
ANN 0.850 (0.010)
0.829 (0.011)
0.889 (0.009)
0.928 (0.007)
0.752 (0.013)
0.972
LogitBoost 0.584 (0.014)
0.819 (0.011)
0.184 (0.011)
0.629 (0.014)
0.377 (0.014)
0.324

Decision support system to facilitate management of patients with acute GIB Page 35 of 41, Chu, et al
Table 5. Evaluation step–accuracies of predicting resuscitation and endoscopy using
source as a variable (standard error)
RF SVM SC LDA
Resuscitation 0.934 (.007)
0.935 (.007)
0.909 (.008)
0.922 (.008)
Endoscopy 0.783 (.012)
0.787 (.012)
0.809 (.011)
0.818 (.011)
kNN ANN logistic LogitBoost
Resuscitation 0.883 (.009)
0.915 (.008)
0.918 (.008)
0.631 (.014)
Endoscopy 0.794 (.012)
0.783 (.012)
0.792 (.012)
0.631 (.014)

Decision support system to facilitate management of patients with acute GIB Page 36 of 41, Chu, et al
Table 6. Validation step–Predictive accuracies using a 67 patient database
Source of bleeding
Resuscitation Endoscopy Disposition
RF 0.928 0.851 0.753 0.797
SVM 0.826 0.791 0.681 0.783
SC 0.855 0.866 0.696 0.768
LDA 0.768 0.821 0.681 0.797
kNN 0.783 0.821 0.667 0.783
ANN 0.884 0.821 0.638 0.754
logistic N/A 0.791 0.710 N/A
LogitBoost N/A 0.567 0.551 0.362

Decision support system to facilitate management of patients with acute GIB Page 37 of 41, Chu, et al
Table 7. Variable importance using RF and ANN
SOURCE RESUSCITATION
RF ANN RF ANN
Hematemesis 0.1388 10 Syncope 0.1097 10
NG Lavage 0.0692 10 Orthostasis 0.0782 10
Hematochezia 0.0611 10 Hct. Drop 0.0495 10
BUN 0.0484 10 DBP 0.0276 10
Rectal 0.0374 10 Hct. 0.0232 10
Melena 0.0221 9 HR 0.0139 10
Orthostasis 0.0116 10 SBP 0.0114 10
Hx. of GIB 0.0088 8 Hematemesis 0.0052 10
HR 0.0066 10 Melena 0.0032 10
Cr 0.0055 7 Cr 0.0019 1
SBP 0.0051 4 NG Lavage 0.0019 9
DBP 0.0043 9 BUN 0.0018 6
Syncope 0.0032 9 Hematochezia 0.0015 10
INR 0.0031 5 Duration 0.0011 6
Plt 0.0010 6 INR 0.0009 6
Risk for Stress Ulcer
0.0008 10 Rectal 0.0006 7
Cirrhosis 0.0004 10 Unstable CAD -0.0016 5
ASA NSAID -0.0010 1
ENDOSCOPY DISPOSITION
RF ANN RF ANN
Syncope 0.0507 10 Orthostasis 0.0585 10
Orthostasis 0.0259 10 HR 0.0431 10
Hct. 0.0223 10 Hct. 0.0340 10
HR 0.0213 9 SBP 0.0287 10
Hct. Drop 0.0188 10 Syncope 0.0271 10
DBP 0.0178 9 DBP 0.0217 10
Hematemesis 0.0133 10 Hct. Drop 0.0189 10
Rectal 0.0054 9 Rectal 0.0094 10
BUN 0.0051 5 Age 0.0070 10
SBP 0.0046 9 NG_Lavage 0.0055 8
INR 0.0043 2 BUN 0.0054 8
Cirrhosis 0.0039 8 INR 0.0051 4
Melena 0.0022 9 Risk for Stress Ulcer
0.0037 8
Plt. 0.0020 3 Plt. 0.0036 6
Risk for Stress 0.0015 9 Melena 0.0026 9

Decision support system to facilitate management of patients with acute GIB Page 38 of 41, Chu, et al
Ulcer
Duration 0.0008 8 Hematochezia 0.0022 6
Cr. 0.0003 2 Hematemesis 0.0010 7
ASA NSAID 0.00008 4 Cirrhosis 0.0007 8
Hematochezia 0.00001 9 COPD 0.0006 8
NG Lavage -0.0004 8 CRF 0.00007 4
Duration 0.00001 4
Cr. -0.00006 3
Unstable CAD -0.0002 5

Decision support system to facilitate management of patients with acute GIB Page 39 of 41, Chu, et al
References
1 T.A. Rockall, R.F. Logan, H.B. Devlin, T.C. Northfield. Incidence of and mortality from acute upper gastrointestinal haemorrhage in the United Kingdom. Steering Committee and members of the National Audit of Acute Upper Gastrointestinal Haemorrhage. British Medical Journal 311 (1995), pp. 222–226. 2 Baradarian R, Ramdhaney S, Chapalamadugu R, Skoczylas L, Wang K, Rivilis S, Remus K, Mayer I, Iswara K, Tenner S. Early intensive resuscitation of patients with upper gastrointestinal bleeding decreases mortality. American Journal of Gastroenterology. 2004 Apr; 99(4):619-22. 3 Elta GH. Urgent colonoscopy for acute lower-GI bleeding. Gastrointestinal Endoscopy. 2004 Mar;59(3):402-8. Review 4 Das A, Wong RC, Prediction of outcome of acute GI hemorrhage: a review of risk scores and predictive models. Gastrointestinal Endoscopy 2004 Jul;60(1):85-93. 5 Das A, Ben-Menacehm T, Cooper GS, Chak A, Sivak MV Jr, Gonet JA, et al. Prediction of outcome in acute lower-gastrointestinal haemorrhage based on an artificial neural network: internal and external validation of a predictive model. Lancet 2003;362:1261-6. 6 Vapnik, V. The nature of statistical learning theory. New York, NY: Springer Verlag. 7 Tibshirani, R, Hastie, T, Narasimhan, B, Chu, G. Diagnosis of multiple cancer types by shrunken centroids of gene expression. Proceedings of National Academy of Science. 2002; 99, 6567-6572. 8 Breiman, L. (1996). Bagging predictors. Machine Learning, 24, 123-140. 9 Schapire, RE. The strength of weak learnability. Machine Learning. 1990; 5, 197-227. 10 Breiman, L. Random Forest. Machine Learning. 2001; 45, 5-32. 11 Prakash C, Zuckerman GR. Gastrointest Endosc. 2003 Sep;58(3):330-5. Acute small bowel bleeding: a distinct entity with significantly different economic implications compared with GI bleeding from other locations. Gastrointestinal Endoscopy. 2003 Sep;58(3):409-12.12 Barkun A, Bardou M, Marshall JK; Nonvariceal Upper GI Bleeding Consensus Conference Group. Consensus recommendations for managing patients with nonvariceal upper gastrointestinal bleeding. Annals of Internal Medicine. 2003 Nov 18;139(10):843-57. 13 Non-variceal upper gastrointestinal haemorrhage: guidelines. Gut 2002 Oct;51 Suppl 4:iv1-6. 14 Hay JA, Maldonado L, Weingarten SR, Ellrodt AG. Prospective evaluation of a clinical guideline recommending hospital length of stay in upper gastrointestinal tract hemorrhage. JAMA. 1997 Dec 24-31;278(24):2151-6. 15 Hay JA, Lyubashevsky E, Elashoff J, Maldonado L, Weingarten SR, Ellrodt AG. Upper gastrointestinal hemorrhage clinical--guideline determining the optimal hospital length of stay. The American Journal of Medicine. 1996 Mar;100(3):313-22. 16 Adler DG, Leighton JA, Davila RE, Hirota WK, Jacobson BC, Quereshi WA, Rajan E, Zuckerman MJ, Fanelli RD, Hambrick RD, Baron T, Faigel DO. ASGE guideline: the role of endoscopy in acute non-variceal upper-GI hemorrhage. Gastrointestinal Endoscopy 2004 Oct;60(4):497-504. 17 Klebl F, Bregenzer N, Schofer L, Tamme W, Langgartner J, Scholmerich J,

Decision support system to facilitate management of patients with acute GIB Page 40 of 41, Chu, et al
Messmann H. Risk factors for mortality in severe upper gastrointestinal bleeding. International Journal of Colorectal Disease. 2004 Aug 19. 18 Rockall TA, Logan RF, Devlin HB, Northfield TC. Risk assessment after acute upper gastrointestinal haemorrhage. Gut. 1996 Mar;38(3):316-21. 19 Rockall TA, Logan RF, Devlin HB, Northfield TC. Selection of patients for early discharge or outpatient care after acute upper gastrointestinal haemorrhage. National Audit of Acute Upper Gastrointestinal Haemorrhage. Lancet. 1996 Apr 27;347(9009):1138-40. 20 Velayos FS, Williamson A, Sousa KH, Lung E, Bostrom A, Weber EJ, Ostroff JW, Terdiman JP. Early predictors of severe lower gastrointestinal bleeding and adverse outcomes: a prospective study. Clinical Gastroenterology Hepatology. 2004 Jun;2(6):485-90. 21 Strate LL, Orav EJ, Syngal S. Early predictors of severity in acute lower intestinal tract bleeding. Archives of Internal Medicine. 2003 Apr 14;163(7):838-43. 22 Kalula SZ, Swingler GH, Louw JA. Clinical predictors of outcome in acute upper gastrointestinal bleeding. South African Medical Journal. 2003 Apr;93(4):286-90. 23 Bordley DR, Mushlin AI, Dolan JG, Richardson WS, Barry M, Polio J, Griner PF. Early clinical signs identify low-risk patients with acute upper gastrointestinal hemorrhage. JAMA. 1985 Jun 14;253(22):3282-5. 24 Mortensen PB, Nohr M, Moller-Petersen JF, Balslev I. The diagnostic value of serum urea/creatinine ratio in distinguishing between upper and lower gastrointestinal bleeding. A prospective study. Danish Medical Bulletin. 1994 Apr;41(2):237-40. 25 Zimmerman J, Siguencia J, Tsvang E, Beeri R, Arnon R. Predictors of mortality in patients admitted to hospital for acute upper gastrointestinal hemorrhage. Scandinavian Journal of Gastroenterology. 1995 Apr;30(4):327-31. 26 Terdiman JP, Ostroff JW. Risk of persistent or recurrent and intractable upper gastrointestinal bleeding in the era of therapeutic endoscopy. American Journal of Gastroenterology. 1997 Oct;92(10):1805-11. 27 Corley DA, Stefan AM, Wolf M, Cook EF, Lee TH. Early indicators of prognosis in upper gastrointestinal hemorrhage. American Journal of Gastroenterology. 1998 Mar;93(3):336-40. 28 Blatchford O, Murray WR, Blatchford M. A risk score to predict need for treatment for upper-gastrointestinal haemorrhage. Lancet. 2000 Oct 14;356(9238):1318-21. 29 Zaragoza A, Tenias JM, Llorente MJ. Pre-endoscopic prognostic factors in non-varicose upper gastrointestinal bleeding. Development of a predictive algorithm. Rev Esp Enferm Dig. 2002 Mar;94(3):139-48. 30 Molinaro, AM, Simon, R, Pfeiffer, RM. Prediction error estimation: A comparison of resampling methods. Bioinformatics. 2005: 21, 3301-3307. 31 Bamber D. The area above the ordinal dominance graph and the area below the receiver operating graph. Journal of Mathematical Psychology 1975; 12:387-415. 32 Quirk DM, Barry MJ, Aserkoff B, Podolsky DK. Physician specialty and variations in the cost of treating patients with acute upper gastrointestinal bleeding. Gastroenterology 1997 Nov;113(5):1443-8. 33 Timmerman D, Verrelst H, Bourne TH, De Moor B, Collins WP, Vergote I, Vandewalle J.Artificial neural network models for the preoperative discrimination

Decision support system to facilitate management of patients with acute GIB Page 41 of 41, Chu, et al
between malignant and benign adnexal masses. Ultrasound in Obstetrics and Gynecology 1999 Jan;13(1):17-25. 34 Rosenblatt KP, Bryant-Greenwood P, Killian JK, Mehta A, Geho D, Espina V, Petricoin EF 3rd, Liotta LA. Serum proteomics in cancer diagnosis and management. Annual Review of Medicine 2004;55:97-112. 35 Selaru FM, Xu Y, Yin J, Zou T, Liu TC, Mori Y, Abraham JM, Sato F, Wang S, Twigg C, Olaru A, Shustova V, Leytin A, Hytiroglou P, Shibata D, Harpaz N, Meltzer SJ. Artificial neural networks distinguish among subtypes of neoplastic colorectal lesions. Gastroenterology 2002 Mar;122(3):606-13. 36 Chong CF, Li YC, Wang TL, Chang H. Stratification of adverse outcomes by preoperative risk factors in coronary artery bypass graft patients: an artificial neural network prediction model. Proceedings AMIA Annual Symposium 2003:160-4 37 Lund LH. Comment on: Computerized interpretation of the electrocardiogram. Archives of Internal Medicine 2004, Aug 9-23:164(15):1698-9. 38 Kennedy RL, Harrison RF, Burton AM, Fraser HS, Hamer WG, MacArthur D, McAllum R, Steedman DJ . “An artificial neural network system for diagnosis of acute myocardial infarction (AMI) in the accident and emergency department: evaluation and comparison with serum myoglobin measurements,” Computer Methods and Programs in Biomedicine 52: 93-103, 1997. 39 Lisboa PJ. “A review of evidence of health benefit from artificial neural networks in medical intervention,” Neural Networks 15:11-39, 2002. 40 Ahn, H., Moon, H., Fazzari, M. J., Lim, N., Chen, J. J. and Kodell, R. L. Classification by Ensembles from Random Partitions of High-Dimensional Data. (2007). Computational Statistics and Data Analysis, 51: 6166-6179.












![ENHANCING DECISION MAKING - eprints.dinus.ac.ideprints.dinus.ac.id/14400/1/[Materi]_laudon_-_management... · •Group Decision Support Systems (GDSS) –Interactive system to facilitate](https://static.fdocuments.us/doc/165x107/5c8427ed09d3f2a3488cbbe5/enhancing-decision-making-materilaudon-management-group-decision.jpg)