A critical account of the policy context shaping perinatal ......neonatal mortality rate at 33 per...
16
RESEARCH ARTICLE Open Access A critical account of the policy context shaping perinatal survival in Nepal: policy tension of socio-cultural versus a medical approach Mohan Paudel 1* , Sara Javanparast 2 , Gouranga Dasvarma 3 and Lareen Newman 4 Abstract Background: Nepal formulated a range of policies related to maternal and neonatal survival, especially after the year 2000. Nevertheless, Nepal’s perinatal mortality remains high, particularly in disadvantaged regions. Policy analysis can uncover the underlying values, strategies and policy formulation processes that shape the potential to reduce in-country health inequities. This paper provides a critical account of the main policy documents relevant to perinatal survival in Nepal. Methods: Six key policy documents covering the period 2000–2015 were reviewed using an adapted framework and were analyzed through qualitative content analysis. Results: The analysis shows that the policies focused mainly on the system: improvement in provision of birthing facilities; targeting staff (Skilled Birth Attendants) and health service users by providing cash incentives to staff for bringing patients to services, and to users (pregnant women) to attend health institutions. Despite a growing focus on saving women and newborn babies, there is a poor policy focus and direction on preventing stillbirth. The policy documents were found to emphasize tensions between birthing at home and at health institutions on the one hand, and between strategies to provide culturally appropriate, woman-centered care in communities and medically orientated services on the other. Policies acknowledge the need to provide and address woman-centered care, equity, social inclusion, and a rights-based approach, and identify the community based approach as the mode of service delivery. Over and above this, all policy documents are aimed at the national level, and there is no specific policy direction for the separate ecological, cultural or geographic regions such as the mountainous region, which continues to exhibit higher mortality rates and has different cultural and demographic characteristics to the rest of Nepal. Conclusions: To better address the continuing high perinatal mortality rates, particularly in disadvantaged areas, national health policies should pay more attention to the inequity in healthcare access and in perinatal outcomes by integrating both stillbirth prevention and neonatal survival as policy agenda items. To ensure effective translation of policy into practice, it is imperative to tailor the strategies according to acknowledged policy values such as rights, inclusion and socio-cultural identity. Keywords: Perinatal survival, Policy, Strategy, Newborn, Inequity, Nepal * Correspondence: [email protected] 1 Initiative for Research, Education and Community Health-Nepal, Kathmandu, Nepal Full list of author information is available at the end of the article © The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated. Paudel et al. BMC Health Services Research (2019) 19:166 https://doi.org/10.1186/s12913-019-3979-3
Transcript of A critical account of the policy context shaping perinatal ......neonatal mortality rate at 33 per...

RESEARCH ARTICLE Open Access
A critical account of the policy contextshaping perinatal survival in Nepal: policytension of socio-cultural versus a medicalapproachMohan Paudel1* , Sara Javanparast2, Gouranga Dasvarma3 and Lareen Newman4
Abstract
Background: Nepal formulated a range of policies related to maternal and neonatal survival, especially after theyear 2000. Nevertheless, Nepal’s perinatal mortality remains high, particularly in disadvantaged regions. Policyanalysis can uncover the underlying values, strategies and policy formulation processes that shape the potential toreduce in-country health inequities. This paper provides a critical account of the main policy documents relevant toperinatal survival in Nepal.
Methods: Six key policy documents covering the period 2000–2015 were reviewed using an adapted frameworkand were analyzed through qualitative content analysis.
Results: The analysis shows that the policies focused mainly on the system: improvement in provision of birthingfacilities; targeting staff (Skilled Birth Attendants) and health service users by providing cash incentives to staff forbringing patients to services, and to users (pregnant women) to attend health institutions. Despite a growing focuson saving women and newborn babies, there is a poor policy focus and direction on preventing stillbirth. Thepolicy documents were found to emphasize tensions between birthing at home and at health institutions on theone hand, and between strategies to provide culturally appropriate, woman-centered care in communities andmedically orientated services on the other. Policies acknowledge the need to provide and address woman-centeredcare, equity, social inclusion, and a rights-based approach, and identify the community based approach as themode of service delivery. Over and above this, all policy documents are aimed at the national level, and there is nospecific policy direction for the separate ecological, cultural or geographic regions such as the mountainous region,which continues to exhibit higher mortality rates and has different cultural and demographic characteristics to therest of Nepal.
Conclusions: To better address the continuing high perinatal mortality rates, particularly in disadvantaged areas,national health policies should pay more attention to the inequity in healthcare access and in perinatal outcomesby integrating both stillbirth prevention and neonatal survival as policy agenda items. To ensure effectivetranslation of policy into practice, it is imperative to tailor the strategies according to acknowledged policy valuessuch as rights, inclusion and socio-cultural identity.
Keywords: Perinatal survival, Policy, Strategy, Newborn, Inequity, Nepal
* Correspondence: [email protected] for Research, Education and Community Health-Nepal, Kathmandu,NepalFull list of author information is available at the end of the article
© The Author(s). 2019 Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, andreproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link tothe Creative Commons license, and indicate if changes were made. The Creative Commons Public Domain Dedication waiver(http://creativecommons.org/publicdomain/zero/1.0/) applies to the data made available in this article, unless otherwise stated.
Paudel et al. BMC Health Services Research (2019) 19:166 https://doi.org/10.1186/s12913-019-3979-3

BackgroundDespite the decades old global focus on improving maternal,infant and under-5 health outcomes in developing countries,perinatal mortality (which includes stillbirth and neonatalmortality in its extended definition) has remained largelyoverlooked [1]. Perinatal mortality has high social and eco-nomic costs, and is a marker of existing inequalities in coun-tries and their communities. About 2.7 million neonataldeaths and 2.6 million stillbirths are estimated to occur an-nually across the world [2, 3]. Of the total estimated neonataldeaths, 2 million occur in the first week of life. Nearly 99% ofboth stillbirths and neonatal deaths occur in developingcountries, including three-quarters in South Asian and Afri-can countries. Failure to further improve birth outcomes isestimated to cause 116 million deaths, 99 million with dis-ability or loss of potential, and additional millions of adultswith increased risk of later-life non-communicable diseasesfrom being born with Low Birth Weight [4, 5].Nepal has made good progress in reducing maternal
and under-five mortality rates over the years [6, 7] withmuch remaining still to be done on the reduction ofperinatal deaths—both stillbirths and neonatal deaths.The neonatal death rates as identified by Nepal’s 2011Demographic and Health Survey are reported to beamong the highest in the world (neonatal mortality: 33per thousand livebirths, and perinatal mortality: 37 perthousand births), [8] with one of the highest neonatalmortality differentials according to income inequalityand geographical location [9]. It is estimated that Nepalcould potentially have a reduction of 46% in its neonatalmortality rate if the existing income inequalities were re-moved [4]. Nepal’s National Demographic and HealthSurveys of 2006 and 2011 identified a stable nationalneonatal mortality rate at 33 per thousand livebirths,compared with the global average of 21 per thousandlivebirths [8, 10]. Although the most recent Demo-graphic and Health Survey conducted in Nepal in 2016reported a reduction in neonatal mortality, it still identi-fied high perinatal mortality (36/1000 pregnancies) inrural areas including the mountains, and persistent geo-graphic differentials in neonatal death rates, with themountains reporting the highest rates [11, 12]. Cur-rently, the neonatal mortality rate in Nepal’s mountainregion is 35 per thousand live births [11], which is morethan the neonatal mortality rates of the Sub-Saharan Af-rica (28/1000) livebirths [13]. Very similar patterns arealso reported in perinatal mortality, both nationally andin the mountainous region, despite ambiguities in defin-ition and omissions in reporting of stillbirths in theseregions.Analysis of health policies is crucial for understanding their
influence on health systems, and their focus and impact onpopulation health [14, 15]. Hafner and Shiffman [16], whilediscussing the influence of global health policy changes in
strengthening health systems, argue that population healthand equity are affected by the limitations of a vertical medicalapproach (disease oriented initiatives), adverse effects of glo-bal health initiatives on local health systems, and bottlenecksin weak health systems. In this context, other researchers[17–19] recommend that an increasing focus is required toexamine the policy strategies, the policy process and the useof evidence in policy formulation. Therefore, the focus of thecurrent paper on policy review is crucial to examine theunderpinning values and strategies and in order to derive in-sights into potential to improving healthcare delivery, in thiscase, to understand the potential to reduce in-country in-equities in improving poor perinatal survival in Nepal.Up until the year 2000, Nepal did not have specific
policy strategies focusing on maternal and newbornhealth. After 2000, Nepal experienced several keychanges in policies related to perinatal survival. Examin-ing the policy documents is therefore one way to provideinsights into why poor perinatal survival rates continueboth at national, ecological and sub-national levels.This paper commences with an overview of the histor-
ical development of policy relevant to maternal and peri-natal health in general, before explaining how the focusin Nepal after 2000 began to move more towards im-proving newborn survival. Each document is then separ-ately reviewed, providing details of the document,strategies and intended outcomes, and values and princi-ples ingrained in the document.
MethodThis paper is extracted from the first phase of a muchlarger, qualitative research project entitled ‘Socio-cul-tural and healthcare context of perinatal survival in ruralmountain villages of Nepal’ [20]. As its first phase, thelarger research project comprised a review of policy re-lated documents in, and a qualitative research fieldworkconducted in a mountain district of Nepal in its secondphase. Research ethics approval for the project was ob-tained from the Social and Behavioral Research EthicsCommittee of Flinders University in South Australia andfrom the Nepal Health Research Council.
Document identification and selectionPrevious employment in Nepal for nearly 6 years in the pub-lic health sector enabled the first author (a Nepali national)to access professional networks to know and identify the keypolicy related documents currently effective in Nepal. Fig-ure 1 describes the process of document identification andselection. This stage helped to further reflect on the objectiveof this paper and consult experts working in newborn andmaternal health in government and non-governmental sec-tors in Nepal. Drawing on this knowledge base, the decisionwas made to individually review six key documents recom-mended as the most appropriate and most effective in
Paudel et al. BMC Health Services Research (2019) 19:166 Page 2 of 16

shaping Nepal’s policy level response to improve perinatalsurvival at primary healthcare level. These 6 were selectedfrom a pool of 21 documents which focused broadly onhealth service delivery, where the 6 focused particularly onmaternal and newborn health and were also the more recentdocuments in use.
Review processThis review utilized a qualitative content analysis (di-rected approach) as suggested by Hsieh and Shannon(2005), guided by an adapted framework (Table 1) as aninitial framework to code contents in the Nepalese docu-ments. The framework and policy review process were
Strategies for identification of policy related documents
Web search + face-to-face and Email contacts with professionals working in the Nepalese Ministry of Health and Population, the Nepal Department of Health Services, and Non-governmental organisations in maternal and newborn health in Nepal
Documents available
Six Annual Reports (2009 to 2014); Two Program Assessment Reports (related to birth preparedness and newborn care; Six National policy, plan and strategies; Six Implementation Guidelines (6); One training/program management guide (1)
Policy selection
Six documents which were (i) in current use (ii) relevant to perinatal survival that describes the key country policy intent/strategies in primary health care settings, recommended by the experts involved in maternal and newborn health activities of government and non-governmental sector and (iii) published in English or Nepali language
Fig. 1 Document review flow diagram. Source: Author created based on document search
Table 1 Document Review Framework
Key areas Review questions
1. The document • Purpose (what is the main purpose of the document?)• Type of document (is it a policy/strategy/planning document? Progress/assessment report? Training/guideline?• Focus on newborn or stillbirth or both (does it mention newborn, perinatal care explicitly?)• Geographic focus (what type of geographic area is the key focus of the document--National? Topography specific?Development region?)
2. Document development • Process (what led to the formulation of this document? Why was the need felt to formulate this document?)• Developers (which department, section formulated it?)• Stakeholders (who were the stakeholders involved?)
3. Values, definitions andlanguage
• Social or Medical focus (what is the key focus of the policy?)• Key perspective/approach in deciding to reach perinatal care (right based, woman-centered, gender, etc.)• Equity groups (have they targeted vulnerable groups or disadvantaged groups e.g. teenage mothers, scheduledcastes/indigenous and ethnic minorities?)
4. Health outcomes and healthaccess
• Prevention of stillbirths• Prevention of neonatal deaths• Access to care during pre-pregnancy, pregnancy, delivery, postpartum period
5. Strategies for action • The strategies in providing perinatal and neonatal care such as at home, in community, and in health facility• Care across the continuum from pre-pregnancy to postpartum• Integration of perinatal and neonatal care with maternity and child survival and other interventions• Inter-sectoral collaboration, collaboration across departments• Other government departments and agencies involved such as UN, bi-lateral agencies, INGOs• Specific target groups
Source: Adapted from Newman [53], Newman [54] Walt and Gilson [15]
Paudel et al. BMC Health Services Research (2019) 19:166 Page 3 of 16

developed by drawing on insights from Walt and Gilson(1994) and Newman et al. (2006a, 2006b). The first andsecond rows in Table 1 provide context and process, andthe third, fourth and fifth rows provide values and con-tent identified by the policies in Nepal. While reviewingeach document, the five categories of the framework be-came nodes in the NVivo (Version 10.00) software, andthe bullet points under each category became the areasof interests and constant questions to code into eachparticular category. To describe the context of how pol-icy making evolved in Nepal, background papers relatedto the policy documents and the previous versions of thedocuments were also utilized.
ResultsPerinatal survival—Low focus before 2000The document review showed that prior to 2000, perinatalsurvival was not a focused strategic outcome anywhere inpolicy documents in Nepal’s healthcare system. Nepal’s re-sponse to address the health of women and children ingeneral dates back to 1989 with the introduction of a vol-untary network of Female Community Health Volunteersas a foundation of community health [21]. Currently, thereare over 50,000 female volunteers which the nationalhealth policy [22] considered a major pillar in improvinghealthcare for women and children, but their intentionwas mainly to address ongoing high maternal andunder-five mortality. However, the first ever programmaticresponse to high maternal and child mortality rates can betraced back to the Family Planning and Maternal andChild Health initiative of 1968 [23]. Later, in 1998, Nepalformulated the National Reproductive Health Strategywhich included child health and safe motherhood as itscomponents, and endorsed a basic standard of reproduct-ive care from different levels of health facilities [24]. Yet,nowhere did this strategy specifically talk about perinatal sur-vival as such. Its concern was only around whether a mothercould be saved, because a large number of women weredying during pregnancy, childbirth and the postnatal period.Before 2000, the maternal and under-five death tolls in Nepalwere among the highest in the world [8, 25, 26]. Safemotherhood became the government’s priority program, andNepal developed its first Safe Motherhood Policy in 1993[27] with the main and urgent focus to save women’s livesduring childbirth and within the postnatal period. Early in-fant deaths did not come into policy documents when Nepalwas grappling with one of the highest maternal andunder-five mortality rates in the world.
Policies after 2000— ‘Newborn focused’ but low priorityin addressing stillbirthSurvival of newborns did not become a major strategicpriority until Nepal developed the 2004 National Neo-natal Health Strategy [28]. Still, in all policies, prevention
of stillbirths received less priority than in preventingneonatal deaths after birth. The driving force behindNepal’s policy response to prevent neonatal deaths is theinternational initiative- Millennium Development GoalFour - when Nepal realized that reaching under-five andinfant mortality targets was not possible without first ad-dressing its high prevalence of neonatal mortality. Of thesix key documents considered effective in impactingperinatal survival in Nepal, the National Neonatal HealthStrategy 2004 is considered the most specific in address-ing newborn healthcare [28]. The other policies are:
� National Policy on Skilled Birth Attendants, 2006(Supplementary to Safe Motherhood Policy, 1998,[29];
� National Safe Motherhood and Newborn HealthLong Term Plan (2006–2017) [27];
� Mother’s Protection Program-ImplementationGuideline, 2013 (revision on Safe Delivery IncentiveGuideline, 2007 and 2009, [30];
� Maternal and Perinatal Death Surveillance andResponse (MPDSR) Guideline, 2014 [31] and;
� Community Based Integrated Management ofNeonatal and Childhood Illness (ProgramManagement Module, 2015) [32].
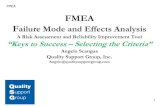
It can be seen that Nepal has been focusing on updatingthese policy documents since 2000. Figure 2 illustrates thepolicies and their subsequent revisions.Guided by the adapted framework (as per Table 1), the
paper now proceeds to provide a detailed analysis of in-dividual documents. The analysis consists of descriptionsof the content and focus of each of these six documents,their development process, their key values and motiva-tions, and their health outcomes and strategies consid-ered to influence perinatal survival in the country.
National Neonatal Health Strategy, 2004Nepal’s National Neonatal Health Strategy [28] is consid-ered as the first strategic response focusing specifically onthe newborn at the country level. This strategy was formu-lated with the aim to prevent neonatal deaths when morethan 30,000 newborns were dying every year in Nepal (p.2)1 which translates into approximately three to four neo-natal deaths an hour, half of which were in the mountains.This document was formulated when the situation wasmarked by a high proportion of home births, poor postna-tal care, a poorly functioning referral system, and un-attended obstetric and neonatal complications (pp. 2–3).Regarding the underpinning values of this policy, it is
stated in the front of the policy document that the thensecretary of the Nepalese Ministry of Health and Popula-tion acknowledges access to care and survival as thegreatest right of every vulnerable newborn:
Paudel et al. BMC Health Services Research (2019) 19:166 Page 4 of 16

Every vulnerable Nepali newborn has the greatestright to be taken care of and therefore we have toimmediately invest resources to improve their healthand survival (p. ii) (Secretary, Ministry of Health andPopulation [Nepal])
The policy recognized the strength of addressingproblems in mothers and babies’ health in a con-tinuum:
The mother and her baby should be treated asone entity and to be successful; any range ofinterventions that seek to prevent perinatal andneonatal deaths must address both maternal andneonatal factors. (p.1)
Although it mentioned that priority should be givento remote and disadvantaged areas, it did not expli-citly identify regional variation in neonatal deathrates and did not provide any regional/ecologicalspecific priorities. Hence, the significantly higherneonatal death rates in the mountain areas are notspecifically highlighted, nor are mountain-specificstrategies outlined to address them, except generallystating that priority should be given to remote andrural areas.The policy considered a set of evidence based and
proven interventions such as immediate newborn carewith drying, delayed bathing, skin to skin contact,breastfeeding and treatment of infections. This policysets its immediate focus on addressing complications ofmothers and babies for immediate impact:
… proven interventions addressing causes of maternaland neonatal complications at family and communitylevels will be the primary focus for immediate impact.These interventions will require the establishment ofa chain of care linking families and communities withthe health system. (p. 2)
The main policy intention remained focused on promot-ing institutional births and prevention of neonatal deathsduring childbirth or shortly after birth. This policy also de-vised strategies to institutionalize provision of newborncare from Nepal’s healthcare system. To do this, the policyset neonatal care at four different levels: (1) home/com-munity level, (2) primary healthcare level, (3) district hos-pital level and zonal, (4) regional and central hospital level(p. 12). It sets forth five key intervention areas related tobirth registration; behaviour change engaging mothers,husbands and mothers-in-law; healthcare delivery bySkilled Birth Attendants (SBAs); ensuring supplies and lo-gistics; and research in areas of quality of care includingverbal autopsy studies (pp. 4–7).This national strategy also discussed the establishment
of a well-functioning referral mechanism for sick new-borns, care for non-sick low birth weight babies, andmanagement of newborn infections with appropriate an-tibiotics from village health institutions. At the hospitallevel, it included additional activities such as manage-ment of obstetric and newborn complications, intraven-ous drug administration, perinatal death audits andtraining and supervisory activities of staff working atperipheral health institutions.
National Policy on skilled birth attendant, 2006Nepal introduced a Skilled Birth Attendant (SBA) policyin 2006 [29] to specifically address high maternal and neo-natal mortality. This policy is supplementary to the NepalSafe Motherhood Policy, 1998. The Ministry of Healthand Population formed a policy advisory group in May2006 which then developed the SBA policy in 2006. Nepalconsidered formulation of this policy imperative in thecontext that only 13% of birthing women were attendedby health workers. Compared with SBAs, Maternal andChild Health Workers (MCHW) and Auxiliary NurseMidwives (ANMs) were identified as being ineffective inreducing the number of maternal and neonatal deaths (p.
199720032014
National Neonatal Health Strategy
National Policy on Skilled Birth Attendant
National Safe Motherhood and Newborn Health Long Term Plan
Mother’s Protection Program-Implementation Guideline
Maternal and Perinatal Death Surveillance and Response (MPDSR) Guideline
Integrated Management of Newborn and Childhood Illness; Programme Management Module (Training Package)
2004
2006
20022006
2005200720092013
199720072015
Fig. 2 The selected documents and the update versions according to timeline. Source: Author created based on the document review
Paudel et al. BMC Health Services Research (2019) 19:166 Page 5 of 16

2). One of the main gaps noted in relation to MCHWsand ANMs concerned lack of professional competency,particularly to manage obstetric complications. This policytherefore set out to address the lack of access tolife-saving emergency obstetric care to women in villagesacross the country.The policy valued woman-friendly care during preg-
nancy and birthing, defined as culturally sensitive and af-fordable care. Although it did not specifically mentionthe mountain areas, it highlighted the priority to begiven to the poor and under-served areas.
… it is important to encourage women to deliver infacilities with skilled attendants with access toEmergency Obstetric Care (EmOC). This will require24 hours a day and 7 days a week, women-friendlyservices that are culturally sensitive and affordable toall families, especially those in poor and underservedareas. (p.1)
The policy stood on the research evidence that improv-ing access to skilled attendants at birth prevents a largeproportion of maternal and neonatal deaths. Citing theNepali context where the majority of women were stillgiving birth at home, the policy explicitly conflatedskilled attendance with institutional births and treatmentof obstetric complications.The strategies focused mainly on recruitment of SBAs
and their deployment. The policy highlighted the needfor creating an enabling environment for SBAs workingin the periphery by ensuring regular supportive clinicalsupervision and medical supplies, effective partnershipin the work environment with other health workers, andliving accommodation and support from the local facilitymanagement committee.
The SBA will work in close partnership with otheressential health care providers at community level andbe supported and guided by a strong District HealthTeam that has the capacity to deal effectively withemergency obstetric complications … . Secretary ofMinistry of Health and Population (p. i)
The policy also outlined the expansion of birthing unitsin health institutions, and encouraged NGOs and com-munities to establish community based birthing units atthe local level (pp. 8–9).
National Safe Motherhood and newborn health long termplan (2006–2017)The purpose of the National Safe Motherhood & New-born Health Long Term Plan (2006–2017) [27] was to in-crease healthy practices and to improve the quality ofprofessional care for both mothers and their newborn
babies. The document was prepared in consultation withboth government and non-governmental stakeholders atthe central level. The formulation of the documentevolved through three stages: (i) first preparatory meetingin November 2005; (ii) first workshop in January 2006after consultants’ review of existing policies, gaps and de-velopment of a background paper for revision; and (iii)second workshop in March 2006 which set the detail ofoutputs and activities across various thematic groups.This plan is the second version of Nepal’s National
Safe Motherhood Long Term Plan (2002–2017) [33].This version incorporated a response to some of the ur-gent changes at the time such as the MDGs and theNepal government’s focus on neonatal health, increasingthe numbers of SBAs at births, and the Health SectorStrategy: An Agenda for Reform [34]. This reform strat-egy was to ensure a system that provides access to es-sential health services to poor and vulnerablepopulation; to develop capacity of local bodies for par-ticipatory and accountable management of health insti-tutions, and to build partnership and mobilize NGOsand the private sector in maternity service delivery. Thissecond version was produced to also incorporate thefirst ever MDG country progress report 2005 [35] whichcame after the first long-term plan introduced in 2002[36]. Compared with the first version, this plan stronglyprioritized SBA mobilization to reduce both maternaland neonatal mortality.The National Safe Motherhood and Newborn Health
Long Term Plan (2006–2017; NSMNH-LTP) was thefirst national plan to introduce a strongly stated focuson equity and social inclusion:
Equity issues in access and utilization of safemotherhood and neonatal health (SMNH) services arenot mentioned in the original NSMLTP and are ofcritical importance if the most needy members of societyare to be targeted and the MDGs achieved. (p. 2)
Another difference of this document from previousdocuments is that this document acknowledged therole of multiple sectors to ensure equity and accessto care in maternal and newborn health:
Since safe motherhood and newborn health arenot purely health issues, they warrant a multi-sectoral approach and the role of other sectors isparticularly important in enhancing access andpromoting equity. (p.1)
The plan also duly recognized the needs of women to beunderstood in complex social contexts:The needs of
women are treated as paramount throughout theNSMNH-LTP, not simply as individuals, but as mem-bers of families and communities.
Paudel et al. BMC Health Services Research (2019) 19:166 Page 6 of 16

The plan set eight strategic outputs to ensure progressin the health of mother and babies. These were: equityand access; delivery of quality maternal and newborncare; public private partnership; decentralization; andhuman resource development, mainly focusing on train-ing of SBAs; information management; physical assetmanagement and procurement; and finance such as fi-nancial safety nets. The plan also emphasized the needto understand local knowledge about the context of ma-ternity and newborn care:
Activities will advantageously use local knowledge,perceptions and values, relevant traditional practices,preferences and beliefs to enhance knowledge andawareness and will be sensitive to conflict issues. (p. 7)
The plan identified access in a broad sense that wouldconsider not only physical and financial access but alsothe cultural and behavioural aspects of service providers:
Access embraces financial, institutional and infra-structural factors including, but not limited to, fund-ing, transportation and education. It also relies uponpositive and welcoming service provider attitudes,trust, honesty, responsiveness, accountability andquality service delivery both at established facilitiesand through outreach programmes. (pp. 7-8)
The service delivery output of the plan emphasizedreaching socially excluded groups, and encouraged the24-h availability of skilled staff and district-specific strat-egies to increase service access:
At service level, efforts to improve the effectiveness ofthe system will focus on ensuring 24-hour availabilityof skilled staff with essential drugs and equipment,good community and inter-facility linkages and feed-back systems to promote further improvements. Re-mote areas present an even greater challenge andrequire additional focused efforts, which will be cov-ered by district specific strategies. (p.10).
With regards to public-private partnerships, the plansought increasing involvement of NGOs, private sectorhospitals and academic institutions. In decentralization,the plan sought to ensure planning and supervising cap-acity with local government, ie the District Health Officeand health institutions. Likewise, as a financial strategy,it sought to implement equity through creating financialsafety nets for the poor and socially excluded. Regardingthe information system, the plan highlighted collectionand use of data according to ethnicity, caste and wealth.
Mother’s protection program, implementation guideline,2013The Mother’s Protection Program, Implementation Guide-line, 2013 [30] is a successive revision of the previous
guidelines of the Safe Delivery Incentive Programme (SDIP).The SDIP was first introduced in 2005, revised in 2007 andsubsequently evolved as the Mother’s Protection Program,Implementation Guideline, 2009. This latest 2013 guidelinewas formulated by a working committee involving both dis-trict and central level experts within the Department ofHealth Services. The amendment to the previous versionof 2009 was felt necessary to set criteria for types of healthinstitutions to be provided with financial incentives, andto highlight that women should be given the first priorityto have financial incentives before institutions and pro-viders. The institutional incentive was to encourage healthinstitutions to cover basic expenses including drugs andlogistics, while the aim of monetary incentives to pro-viders was to encourage them to ensure their 24-h avail-ability for birthing services.Advancing further on the Safe Delivery Incentive
Programme (SDIP), the Mothers Protection Program en-sured free maternity care from government health insti-tutions and hospitals, and community and teachinghospitals throughout the country, not just limiting it tothe 25 low Human Development Index (HDI) mountaindistricts. The SDIP 2005 and 2007 provided incentivesfor women to encourage them to attend institutionalbirths in the 25 low HDI districts. This 2013 guidelineensured free maternity care throughout the country: (i)to reach the MDG maternal and child health targets;and (ii) to ensure the right to health as a fundamentalconstitutional right of every citizen in accordance withthe provision of Nepal’s interim constitution 2006 (p. 4).The document also talked about the partnership ap-proach in providing maternity and newborn care withprivate, teaching and community hospitals (p. 4).The Safe Delivery Incentive Programme guideline
2005 and the first amended version of it (SDIP 2007)provisioned financial safety nets for improving access tomaternity care. The amended 2007 version provisioned freematernity care in the all 25 low HDI remote mountainousdistricts. This also set a slightly higher travel incentive, aboutUSD 15 (NRs 1500) to cover travel expenses from home tothe institutional birth for women from the mountainous dis-tricts [37]. It set about USD 5 (NRs 500) for women in theplains areas, and about USD 10 (NRs 1000) to women in thehills districts. This is reasonable considering that women inthe mountainous areas have considerably further to walk/travel to attend formal healthcare institutions. As alsostated above, this Mother’s Protection Program Im-plementation Guideline continued the monetarytravel incentive for giving birth in health institutions,and also expanded this to encourage pregnantwomen to attend health visits in the health institu-tions. However, this made the intention of the policyexplicit on promoting institutional birth. It provi-sioned that women would receive the additional
Paudel et al. BMC Health Services Research (2019) 19:166 Page 7 of 16

incentive for antenatal check-ups only when theycontinued attending for all the recommended fourantenatal visits and institutional birth.
Mothers who came for four focused antenatal visitsand also gave birth in health institution, will beprovided rupees 400 [about 4 USD] from pregnancyand delivery incentive during discharge from healthinstitution. (p. 6)
This guideline expanded the concept of birthing units (pp.23–25) by setting specific criteria. These criteria includedphysical infrastructure and space with one separate birth-ing room; equipment; living quarters (accommodation)for the SBA; 24-h presence of a SBA including supportstaff; good referral network; friendly behaviour towardsthe woman and her visitors and the respect of a woman’sprivacy while giving birth. In addition, the guideline madeit necessary to report monthly on the number of obstetriccomplications managed (p. 20). The new obstetric report-ing form included reporting to the district and central de-partment of neonatal deaths, stillbirths and babiesresuscitated for asphyxia management by each health in-stitution. To encourage registration of birth and deaths,the guideline made a provision for a provider incentive forhome births only upon submission of the report of the ei-ther birth or the death registration of a baby.
Maternal and perinatal death Surveillance and response(MPDSR), guideline 2014The Maternal and Perinatal Death Surveillance and Re-sponse (MPDSR) [31] evolved from the Maternal andPerinatal Death Review (MPDR) which was initiatedafter first implementing Maternal Death Review (MDR)in selected hospitals in Nepal. The Maternal Death Re-view dates back to 1990 when Nepal’s Family HealthDivision (FHD) first implemented it in a national hos-pital in Kathmandu; this was implemented in technicalsupport of the WHO. However, the Perinatal Death Re-view (PDR) component was introduced only in 2003,and then implemented for the first time in six Nepalesehospitals. By the year 2012, the MPDR had expanded to21 hospitals across the country. In 2013, after revision ofthe PDR tool, this expanded to 42 hospitals that coverabout half of the total hospitals throughout the country.After revision of the PDR tool, it evolved into theMPDSR form. Internationally, Nepal’s MPDSR is in ac-cordance with the UN Global Strategy for Women’s andChildren’s Health and the Commission on Informationand Accountability (CoIA) (p. 4). This document isproof of the search by Nepal’s Ministry of Health andPopulation for a locally appropriate and viable mechan-ism to continuously strive to reduce maternal and peri-natal deaths. The two key objectives of the document
(pp. 4–5) were: (i) “To provide information that effect-ively guides immediate as well as long-term actions toreduce maternal mortality at health facilities and com-munity and perinatal mortality at health facilities”; and(ii) “To count every maternal and perinatal death, per-mitting an assessment of the true magnitude of maternaland perinatal mortality and the impact of actions to re-duce it”.This guideline acknowledged the value of the life of
every mother and every baby:
“MPDSR underlines the critical need to respond toevery maternal and perinatal death, so that theinformation obtained from that death might be actedupon to prevent future deaths” (p. 3) … every deathcan provide information that can result in actions toprevent future maternal and perinatal deaths (p. 25).
Strategically, this document aimed at linking the infor-mation system with the quality improvement process ata health institution level. The purpose was to enablereal-time monitoring of deaths and assessment of the in-terventions employed.:
The notification of every maternal and perinatal deathalso permits the measurement of maternal mortalityratios and perinatal mortality and the real-time moni-toring of trends that provide countries with evidenceabout the effectiveness of interventions. (p. 3)
The above statement identified notification of everydeath, but so far it prioritized notification and review ofevery maternal death occurring both at institutions andin communities; whereas, for perinatal deaths this ap-plied only at institution level. Hence, it is likely to miss aconsiderable number of deaths occurring in communi-ties, and more so in the remote mountainous areaswhich still have high perinatal deaths.This guideline recommended that the MPDSR
cycle comprise five key elements: case identification,information collection, analysis, recommendation foraction, and evaluation. The case identification in-volved notifying any maternal deaths in the institu-tion and community, and perinatal deaths in aninstitution. Likewise, the guideline proposed a com-mittee for the review of maternal and perinatal deathat each health institution level. The committee didnot explicitly include any parent/family representa-tive/s. The review tool comprised structured ques-tions focusing predominantly on clinical details ofthe deceased baby, possible causes of deaths, and thehealthcare procedures followed for treatment. It doesnot include parental views on causes for delayedcare-seeking, nor does it focus on identifyingsocio-cultural aspects of perinatal deaths.
Paudel et al. BMC Health Services Research (2019) 19:166 Page 8 of 16

Community based integrated Management of Neonatal andChildhood Illness (program management module), 2015Community Based Integrated Management of Neonataland Childhood Illness (Program Management Module,2015) [32] describes the most recently revised packageof key interventions to address newborn survival inNepal. This program package is considered the most re-cent update of Nepal’s continuous efforts to increasenewborn survival, including children under-5 years. Itfocuses on the provision of improved care by health ser-vice providers including trained health volunteers inlocal communities.This packaged ‘CB-IMNCI’ programme is the result of
lessons learned over the last three decades from a range ofprevious programmatic interventions related to verticallyimplemented programmes on diarrhoeal disease control,acute respiratory infection (ARI), and integrated manage-ment of childhood illness (IMCI) which aimed to managefive major killer diseases of under-five children: malaria,malnutrition, measles, pneumonia and diarrhoea. TheIMNCI was brought to community level as CommunityBased Integrated Management of Childhood Illness(CBIMCI) where female health volunteers became a keycadre for treating and referring children under-five, in-cluding newborns. The Community Based Newborn CareProgram (CBNCP) from 2007 gave special focus to new-born care at home, community and peripheral healthinstitutions.The CBNCP comprised a package of key interventions to
be delivered from health institutions and female communityhealth volunteers (FCHVs). It included promotion of institu-tional births, social mobilization for health-related behaviourchange mainly through FCHVs and mothers group; postnatalcheck-up visits for mothers and newborns; management ofpossible bacterial infections such as diarrhoea and pneumo-nia; management of low birth weight babies mainly by keep-ing them warm (e.g. via kangaroo care); prevention ofhypothermia; and management of asphyxiated babies. This‘CBNCP’ package was further revised, and is now its mostrecent form as ‘CB-IMNCI’.The CB-IMNCI still emphasizes the newborn compo-
nent, including the interventions of CBNCP, and add-itionally integrating the IMCI for effective managementof problems for all under-5 s in one single package. Thedocument’s key objectives (p. 12) are: (i) to reduce new-born morbidity and mortality by the promotion of im-mediate care of newborn babies; (ii) to reduce newbornmorbidity and mortality by managing health problems ofnewborn babies; and (iii) to reduce under-five morbidityand mortality by managing their health problems.Generally, the document discusses improving the qual-
ity of newborn care; extending care to communities;reaching marginalized and disadvantaged women/babies;strengthening the supply system; continuing research
and investigations for programme improvement andpositive behaviour change at home and community; andcommunity participation in newborn care (p.12). How-ever, the document does not specifically discuss how itwill reach marginalized populations. In addition, despitebeing a recent document, it does not have any focus onstillbirths, though this is an equally serious concern [38].Despite the intention of being community based as per
its title, this document still focuses mainly on promotionof institutional births and strengthening of quality of carefrom health institutions to prevent neonatal deaths. Thefocus has been on strengthening the capacity of institu-tions to manage and treat newborn babies’ complications.The package has also envisioned expanding birthing cen-tres to ensure quality childbirth and referral care for new-borns with complications. Institutionalization has been akey focus, and for the near future it also envisions a newprogramme entitled Facility Based Integrated Manage-ment of Neonatal and Childhood Illness (p. 11). It hasadded a component which describes treatment of baby’scord infections by using an antiseptic ointment, chlorhexi-dine. The package does not consider management of as-phyxia as the local health volunteers’ job responsibility.However, asphyxia management was considered a majorskill in CBNCP package.Overall, a brief summary of key policy values and
strategies of each of the documents described above ispresented in Table 2.
DiscussionNepal’s policies to address perinatal survival since 2000have been formulated only at the national level. The pol-icies are medically focused, have minimal attention topreventing stillbirths, with a priority on saving newbornbabies after birth. The underpinning policy values ac-knowledge the rhetoric of addressing social determinantsof health/health equity and also audit structural determi-nants such as education, income, ethnicity and geog-raphy/ecological differentials in mortality outcomes. Allpolicies have emphasized rural, marginalized and disad-vantaged women, but they are not explicit about whothese groups are and how they are to be prioritized inactions. Drifting from the core policy values, the strat-egies focus on accessing and delivering health/medicalinterventions and health behaviour changes, guided pri-marily by the intention to promote institutional births.The community based and primary healthcare ideology [39,40] can therefore be seen to have turned more to beingsupply-focused, and intended to “correct” communities ra-ther than to engage, sensitize and empower women, familiesand communities. A brief reflective summary of the policycontext is presented in Table 3 that provides take-home mes-sages about what is going on in policy and what could be
Paudel et al. BMC Health Services Research (2019) 19:166 Page 9 of 16

Table 2 Summary of key values and strategies within the six main documents
Key values (approach, underpinning principles) Strategies (strategic interventions)
National Neonatal Health Strategy 2004
• Access to care and survival as the greatest right ofevery vulnerable newborn
• Mothers and babies’ health in a continuum frompre-pregnancy to postnatal
• A linkage of care across home, community andhealth institution
• Gender equality in newborn care
• Focusing on proven interventions addressing causes of maternal and neonatal complications• Promoting institutional births and preventing newborn deaths during theprocess of childbirth or shortly after birth
• Institutionalising provision of newborn care from Nepal’s healthcare system:(i) home/community; (ii) primary healthcare; (iii) district hospital; (iv) above thedistrict hospital at zonal, regional and central hospital level
• Setting forth five key interventions: (i) registration of all births and deaths;(ii) targeted behaviour change of women, their husbands and mothers-in-law;(iii) strengthening health service delivery—focus on SBAs, focus on postnatalcare of mother and baby; (iv) service management--mainly about ensuring suppliesand logistics; (v) and research focussing on quality of care, and verbal autopsy
National Policy on Skilled Birth Attendant, 2006
• Women-friendly services that are culturally sensitiveand affordable to all families, especially those inpoor and underserved areas
• Pregnancy and birthing care by an Skilled Birth Attendant[An accredited health professional such as a midwife, doctor or nurse]
• Focus on (i) production of SBAs by in-service training and incorporating SBA skills inpre-service curricula of ANM, SN and Doctor training; and (ii) deployment ofSBAs to health institutions
• Availability of 24 h a day, 7 days a week emergency obstetric care in a close partnership withhealth workers other than SBAs
• Encouraged NGOs and communities to establish community based birthing units• SBA to be supported by: strong referral back-up by a district health team, includingsupportive supervision; effective partnerships with other health workers, volunteersand TBAs, safety and security
National Safe Motherhood and Newborn Health Long Term Plan (2006–2017)
• Equity and women centred care• Equity in access and utilisation of health servicesfor newborn babies including safe motherhoodservices among the needy
• Access embracing financial, institutional and infra-structural factors including, but not limited to,funding, transportation and education; and positiveand welcoming service provider attitudes, trust, hon-esty, responsiveness, accountability
• Multi-sectoral approach as underlying value toaddress Safe Motherhood and Maternal andNewborn Health (SMNH) issues; the role of othersectors is particularly important in enhancingaccess and promoting equity
• Women understood not simply as individuals, but asmembers of families and communities functioningwithin complex relationships and socialexpectations
• Eight strategic outputs to ensure progress in the health of mother and babies:(i) Equity and access: empowerment of individuals, groups and networks withthe maternal and newborn care related Behaviour Change Communication(BCC) messages and promotion of birth preparedness and non-discriminatoryinterpersonal communication between providers and clients;(ii) Delivery of quality maternal and newborn care: 24-h availability ofskilled staff with essential drugs and equipment, good community andinter-facility linkages and feedback systems;(iii) Public-private partnership;(iv) Decentralisation: planning and supervising capacity of District Health Office;(v) SBA training;(vi) Information management: collection and use of data according to ethnicity,caste and wealth; and supplement quantitative with qualitative information from;(vii) Physical asset management and procurement; and(viii) Finance such as safety nets for poor and socially excluded
Mother’s Protection Program, Implementation Guideline, 2013
• Ensure the right to health as a fundamentalconstitutional right of every citizen in accordancewith the provision of Nepal’s interim constitution2006
• Financial incentives to improve health outcomes,providing incentives to encourage women tocome to institution to have their babies as well aspregnancy check-ups
• The intention of the policy is clear on promoting institutional birth byallocating incentives to women to come to institutions for pregnancycheck-ups and birthing; to service providers to motivate them to providebirthing care at institutions; and to health institutions to encourage themto strengthen birthing and emergency obstetric care
• Expands the concept of birthing units by setting specific criteria such asseparate birthing room, living apartment for SBA, equipment, 24-h presenceof a SBA including a support staff, good referral network, friendly behaviourto woman and her visitors, and the respect of a woman’s privacy
• Obstetric reporting to the district and central department of neonatal deaths,stillbirths and babies resuscitated for asphyxia management by each health institution.
• Birth or the death registration of a baby, providers receive incentive of home birthsonly if births or deaths are registered by parents
Maternal and Perinatal Death Surveillance and Response (MPDSR), Guideline 2014
• Value of a life of every mother and every baby;every death can provide information that canresult in actions to prevent future maternal andperinatal deaths
• Linking the information system with quality improvement processat a health institution level; real-time monitoring of deaths andassessment of interventions employed. Two main focuses are on:(i) Notification of every death, and (ii) review for further actions to prevent future deaths
Paudel et al. BMC Health Services Research (2019) 19:166 Page 10 of 16

future considerations (questions) for policy makers as well asresearchers.
Policy formulation process: Stakeholders mainly fromcentral level, from only within health sectorRegarding the policy development process, from thepresent review, first, it is evident that participation in pol-icy formulation was intended primarily within the healthsector, within departments such as child and family health,and among government and non-governmental agenciesworking in the field of maternal and child health. Second,this review notes that the policy documents were devel-oped with consultation among the central level experts.Pradhan and colleagues [41] discuss wider stakeholder in-volvement in policy making process in formulating Nepal’sNational Neonatal Health Strategy. Still, the participatorynature of policy formulation process in the Nepalese pol-icy documents involved are health/medical experts work-ing at government department and non-governmentalsector at the central level. Only medical evidence and
views of health sector experts are likely to be predomin-ant, as is also evident in the current policies reviewed inthis study. It is therefore likely that the experiences of staffworking at primary healthcare level and other sectorscould be missed. Along with other sectors, the role of im-plementers (service providers at district and primaryhealthcare systems) is crucial, as they influence implemen-tation decisions and uptake of care by the clients, alsostated as ‘street level bureaucrats’ by Sabatier [42]. It is notjust the participation within the health sector which influ-ences population health, but the health system also hasstewardship responsibility to work with the wider partici-pation of the sectors beyond it [43]. Only then could pol-icies be helpful in redefining the health systems’ roleincreasingly towards health promotion and disease pre-vention, rather than narrowly focused on medicalized ser-vices. Otherwise, the focus of the health sector is likely toremain on attending to sick mothers and babies, ratherthan preventing the occurrence of infections and prob-lems early on.
Table 3 A reflective summary of policy context in perinatal survival
Agenda setting What is going on in policydiscourse
Policy considerations (questions) to ask during future policymaking
Prevention of stillbirths
Still not an agenda in policy making, lowcompeting priority
Intention to begin to reportstillbirths (occasional statements),but not yet focussed
• Is the technical/epidemiologic separation of stillbirths andnewborn death having any social implications? Has thisinfluenced realization of seeing mother and baby as a singleunit in any way? Has it affected district/primary healthcarelevel, how?
• Has perinatal survival been considered as an agenda of healthpromotion, and if so, what could that mean?
• Have the policy approach/strategies been community based,empowering individuals and communities, or merely focussedon attempting to correct health behaviours?
• Does policy community and implementing units need furtherrealization that perinatal survival is not just a medical issue?
• Have health systems (primary health care) been considered toleverage delivery of perinatal healthcare in developingcountries? Or are the programmes being implemented just asvertically based technical packages?
Neonatal Survival
An agenda in policy, healthcare system, butpre-dominantly viewed as a vertical technical/medical initiative
Intention to integrate newborn inchild and maternal health withinhealth sector
Source: Authors’ analysis based on document review
Table 2 Summary of key values and strategies within the six main documents (Continued)
Key values (approach, underpinning principles) Strategies (strategic interventions)
• Self-reliant and sustainable approach to the improve-ment of healthcare for women and their babies
Community Based Integrated Management of Neonatal and Childhood Illness (Program Management Module, 2015)
• Reaching care to disadvantaged and marginalisedgroups
• Provision of quality care through a singleintegrated package of interventions for newbornand under-five children
• Community based care
• Takes into it the lessons from CBNCP, and merges the package with IMCI--thus making asingle package for managing newborn and all under-5 years old children’s health problems
• Despite the community based in its title, still focuses mainly on promotion of institutional birthsand strengthening of quality of care from health institutions to prevent neonatal deaths
• Focus on strengthening the capacity of institutions to manage and treat newborn babies’complications such as infection, asphyxia and low birth weight
• Added a component which describes treatment of baby’s cord infections by using anantiseptic ointment, chlorhexidine
• Does not consider management of asphyxia as local health volunteers’ job, which howeverwas considered in previous version—the Community Based Newborn Care
• Envisioned developing one to two birthing centres per district to ensure quality referral carefor newborns with complications
Paudel et al. BMC Health Services Research (2019) 19:166 Page 11 of 16

Medically focused evidence base: Addressing immediatemedical conditionsAt the strategy level, Nepal developed a range of policies,plans and guidelines from around the millennium whichmade as their focus the survival of infants and newborns.Prior to this date, the policies’ key focus was on maternalsurvival and although some policies mentioned aspects ofperinatal survival, the strategic activities predominantly fo-cused on mothers. The change of priority focus to includenewborn survival occurred from 2004 onwards withNepal’s first ever National Neonatal Health Strategy. Indescribing the intended strategies, the policy documentscite both national and international evidence, with the keyfocus to prevent immediate medical conditions such asobstetric emergencies, to provide immediate neonatal careand to provide health behaviour change interventions incommunities. Nepal’s policies have been up to date interms of adopting best medical evidence internationallyfrom WHO, UNICEF, USAID and drawing on Nepal’s na-tional demographic and health surveys. The MDG mater-nal and child survival goals, and the compellinginternational evidence on introducing SBAs, managingobstetric emergencies, and care and treatment of new-borns with infection, complications of low birth weight,and hypothermia have been powerful forces shaping stra-tegic interventions in all of the documents.
Health service delivery: From community towards healthfacility focusPolicies outlined strategies in the health system andattempted to address social health behaviours. By settingstrategies to mobilize FCHVs for counselling, behaviourchange and supportive care during pregnancy, birthingand the postnatal period, policies have prioritized homeand community interventions to address lack of prepared-ness during birth, preventing harmful practices duringbirthing and newborn care, preventing hypothermia andcommon infections such as pneumonia and diarrhoea.Policies have prioritized delivery of quality care duringpregnancy, delivery and newborn care from health institu-tions, with quality defined primarily in terms of birthingin institutions, and having birth and postnatal careattended by SBAs. They have also focused significantly onidentifying and reviewing the causes of neonatal deathsoccurring at institutional level, but not in the community/home- where most of the mountain births take place.Lately, policies have explicitly discouraged home birthsand incentivized institutional antenatal check-ups andbirths. Policies have acknowledged the need to address in-equitable outcomes in neonatal deaths. Yet, the policy in-terventions have been informed by medical evidence inreducing neonatal mortality and show little focus on un-derstanding of the sociocultural or geographic contexts ofthe women and communities on whom they focus, even
when documents acknowledge these as important factors.Despite policies outlining home/community, institutionsand hospital all as care delivery platforms, the focus re-mains mainly on changing health related behaviours andattendance at formal institutional care. In this regard,there are inherent contradictions within policy values andstrategies. Besides the rhetoric of language in policy values(of “culture, community-based and woman-friendly”), pol-icy strategies remain predominantly within the window ofinstitutionalized and medical care.The strategies though titled or intended as “commu-
nity based” do not show any acknowledgement of con-sidering poor perinatal survival in conjunction withComprehensive Primary Health Care. The authors arguethat the health sector has a stewardship role to advocatefor consideration of social, cultural and contextual deter-minants [43] to better address in-country persistent in-equities in perinatal survival in Nepal. Only then will thecurrent policy values and the aim of international initia-tives such as the Every Newborn Action Plan [44] be re-alized. The Every Newborn Action Plan aims to end allpreventable deaths and has set global targets to reducestillbirth (per thousand births) and neonatal deaths (perthousand livebirths) to 7 by the end of 2035.The strategic priority to prevent neonatal mortality at
national level has been shaped primarily by the highproportion of homebirths attended by non-skilled at-tendants. The focus has been on the system: improve-ment in provision of birthing facilities such as birthingunits; the staff: SBAs as birth attendants; and some as-pects of the consumers: providing incentives for womento attend formal institutions for pregnancy checks anddelivery. The key interventions during pregnancy com-prise distribution of iron and anti-worm tablets, Tet-anus Toxoid immunisation and introduction ofantenatal check-ups. In newborn care, the main focushas been on medical care immediately after birth andpostnatally. It is implicit that the policy approach in ad-dressing poor perinatal survival has been viewed mainlyas the job of health service providers and health volun-teers; the strategies fail to have even an implicit motiveto empower women and families and to increase theircontrol or participation over the care and survival path-way. Within the health system itself, besides viewingchildbirth and perinatal survival as a medical emer-gency, to prevent persistent occurrence of perinataldeaths it should be acknowledged first as an agenda ofhealth promotion, as enshrined in the Ottawa Charterfor Health Promotion [45]. Genuine actions are neededin policy communities to reorient health services andthe role of health service providers, and engage individ-uals and communities as true partners to preventdeaths which continue to occur due to socio-culturalfactors [38, 46, 47].
Paudel et al. BMC Health Services Research (2019) 19:166 Page 12 of 16

Policy target: Only newborn survival, very low focus onpreventing stillbirthSmith and Neupane [48] point out that the issue of new-born survival in Nepal received priority attention due tothe country’s commitment to the child health MDGs,leadership, and the policy recognition of newborn healthas a problem. However, this priority seemed only tofocus on preventing deaths of newborns, while stillbirthshave received little focus in the shadow of the competinginterest and priority of newborn survival. Within healthsystems, stillbirths have been considered as a technicallyseparate agenda; stillbirth has also lost social significanceas an agenda within the health system itself. Policiessimply use the word ‘perinatal’ occasionally, without anyintention to focus on the actual issue of perinatal sur-vival. The focus of all policies remains on newborns,with the exception of the MPDSR which does focus onthe review of perinatal and maternal deaths. Neverthe-less, this is limited mainly to identifying medical causesand avoidable factors to prevent perinatal deaths at insti-tution level. The large number of deaths occurring athome and in communities are not still subjects of suchreview. The focus has been on preventing death afterbirth, but paying equal attention to preventing stillbirthswould ensure additional care for pregnant women. Inaddition, it could more strongly help realize the policies’underpinning values of ‘mother and baby as a singleunit’ [49] and ‘continuum of care from pre-pregnancy toup until postnatal period’ [50]. Otherwise, there is thepotential to “underplay” stillbirths, making them a lowpriority in reporting within the health systems, and oflow concern in the communities.
Policy values: Acknowledge rights, socio-cultural contextsAt the value level, one policy – the Maternal and New-born Health Long Term Plan, 2006 to 2017 [27] - doesspecifically acknowledge the inequities in neonatal/infantmortalities in terms of geographical location and familyincome. The National Neonatal Health Strategy identi-fied gender equality and a rights-based approach to en-sure newborn survival, while the Mothers’ ProtectionProgramme identifies the right to health and financialsafety nets as key policy values to ensure healthcare ac-cess. Likewise, MPDSR says it values every mother andevery newborn by aiming for a self-reliant and account-able approach of reviewing every perinatal death at hos-pital level. All policies have intended to addressdisadvantaged and marginalized populations, but arerarely explicit about who the disadvantaged and specifictarget groups are. Despite recording obvious differentialsin mortality/morbidity rates by region, the policies donot explicitly talk about developing approaches to ad-dress these inequitable outcomes on the basis of eco-logical regions. The exception is providing a slightly
higher amount of travel incentive for women from themountainous regions compared with their hills andplains (Terai) counterparts, presumably because theyhave greater distances to travel to attend healthinstitutions.A few policies identified woman-friendly care, respect
and privacy in health institutions, an equity focus, andfocus on socially excluded and under-served regions.The policies have discouraged home births and haveshifted their focus significantly to strengthening and de-livering quality care from health institutions, and makeno mention of how feasible institutional attendance isfor the women involved. Although immediate medical/health behaviour change strategies are reasonable at theoutset of high prevalence of newborn deaths, this doesnot empower women, families and communities towardsa health promoting approach for care of a mother andbaby in a continuum.The ongoing large numbers of perinatal deaths require
immediate priority to identify preventive measureswhich work. However, since the MDG formulation in2000, the strategic actions in Nepal have been predomin-antly medically focussed. If it is to support the survivalof every mother and every newborn as aimed for by theWHO in the Every Newborn Action Plan [44], Nepalneeds to pay equally serious attention to leveraging thesepolicy values, not just by acknowledging them but byputting actions into workable strategies to address theinequities. The maternal factors, low birth weight andpre-maturity as the causes for large number of perinataldeaths can be prevented only when women and babiesare considered as a single unit, when a focus is put onpromoting health in a continuum, and when due care isgiven to the social and cultural contexts in which thesedeaths continue to occur.The cultural acceptance and invisibility of neonatal
deaths, and largely invisible stillbirths, both within thehealth system and in communities, also suggest the needfor planning strategies to address the relatedsocio-cultural factors. The current government strategiespredominantly center on calling women to have institu-tional births and providing healthcare after birth, butthese can prevent babies’ deaths after birth only ifwomen can reach healthcare. These are not sufficientstrategies alone to reach out to promote and sensitizewomen and families at home and in communities wherethe vulnerabilities to poor health and poor survival ori-ginate. The key international calls to improve health, suchas the Ottawa Charter for Health Promotion [45], AlmaAta [51] and the WHO Commission on Social Determi-nants of Health [52], identify strategies which are commu-nity led, engaging and empowering women and families,and inter-sectoral-- going beyond the health sector to pro-mote health and to address health inequities. Smith and
Paudel et al. BMC Health Services Research (2019) 19:166 Page 13 of 16

Neupane [48] discuss the need for priority to be given tonewborn survival as a specific agenda within the healthsector, which they describe mainly as receiving a technicalhealth/medical priority within a country’s health system.However, we would like to go beyond this, and argue thatit is already high time that perinatal death (stillbirth andnewborn death) are integrated as a single unit and allo-cated not just a technical health/medical priority withinthe health system but also simultaneously consider wideropportunities to sustainably address poor perinatal sur-vival. One approach could be to materialize the underpin-ning policy values such as ‘women to be understood incomplex social context’, ‘women centered care’, ‘socially in-clusion’ and ‘rights based care’, as identified in this review.These values should not be treated merely as rhetoric;they should be realized by treating the care and survival ofa woman and her baby as a single social whole, not just asa fragmented concept (mother-baby dichotomy) for med-ical/healthcare. Having this intention within the healthsystem is important because it shapes the behaviours ofindividuals and communities, and only then can the healthsystem play an effective stewardship role.
Limitations of this reviewOne main limitation of this review is that it could not cap-ture how these policy documents have been implemented inpractice, and it was also not aimed at capturing the detailedprocess of policy formulation. Future studies which can illus-trate the actual policy process could yield greater insights asto whether the targeted groups, the disadvantaged and mar-ginalized groups, or the key implementing units at districtlevel have been involved, and whether participation in thepolicy process could become inter-sectoral - as intendedwithin comprehensive primary healthcare - to address socialdeterminants of health/health inequity in relation to peri-natal survival. Likewise, a study that can examine how thepolicy intentions (the values and strategies) have shaped thehealthcare system at the district level, as well as the impactson the women, families and communities in the villages,would provide insights into the effects of these policies onextending healthcare to women, and empowering womenand communities, so as to be prepared for more sustainablehealth promotive and preventive measures in the care andsurvival of babies.
ConclusionThis paper has identified the historic timing changeswhich brought neonatal survival into policy focus inNepal between 2000 and 2015. Even though the policieshave evolved over time to incorporate new evidence andan appropriate shift of focus from maternal survival tomaternal and newborn survival, they have still not takenaccount of the many religio-cultural dimensions of ma-ternal survival which are documented in the research
literature, or how these factors shape successful preg-nancy outcomes and newborn survival. The main con-tent focus has been institutionalized medical care andattempts to correct health behaviour in the communi-ties. The focus of the policies remained on ensuring sur-vival of babies at and after birth; stillbirths still receivevery little attention. In terms of a regional focus to ad-dress the ongoing high mortality rates, there is no ac-knowledgement that social context may vary, yet there isvery little specific focus on improving neonatal outcomesin the remote mountain areas which record the highestneonatal death rates. Policies also exhibit subtle tensionsbetween institutional versus community focus, and showa mismatch between the underpinning policy valueswhich acknowledge community based, rights-based, in-clusion, and social determinants of health/health equity,and yet a strategic orientation focusing predominantlyon healthcare/medical interventions confined withinhealth facility premises. This review suggests that futurepolicies in Nepal should integrate stillbirth with neonatalsurvival, should aim for a separate women and children’shealth policy, and develop a policy specific to key eco-logical/geographic regions. As a further study, it wouldbe imperative to assess whether policy values are notmerely stated (acknowledged) in a written document,but rather how these are implemented and impact inpractice. Such a study could explain the effect of the pol-icy tension in values and strategic focus in improvingperinatal survival in the more disadvantaged regions ofthe country.
Endnotes1The page refers to the page number of the corre-
sponding document. This also applies to the forthcom-ing documents in this review.
AbbreviationsANM: Auxiliary Nurse Midwife; CB-IMCI: Community Based-Integrated Mage-ment of Childhood Illness; CB-IMNCI: Community Based-Integrated Manage-ment of Neonatal and Childhood Illness; CBNCP: Community Based NewbornCare; CoIA: Commission on Information and Accountability;EmOC: Emergency Obstetric and Newborn Care; FCHV: Female CommunityHealth Volunteer; FHD: Family Health Division; M/PDR: Maternal/PerinatalDeath Review; MCHW: Maternal and Child Health Worker; MPDSR: Maternaland Perintal Death Surveillance and Response; NRs: Nepalese Rupees;NSMLTP: National Safe Motherhood Long Term Plan; NSMNH-LTP: NationalSafe Motherhood and Newborn Health-Long Term Plan; RHCC: ReproductiveHealth Coordination Committee; SBA: Skilled Birth Attendant; SDIP: SafeDelivery Incentive Programme
AcknowledgmentsWe are thankful to experts and key contacts in Nepal who helped inidentifying relevant policy documents.
Availability data and materialsThe datasets used and/or analyzed during the current study are availablefrom the corresponding author on reasonable request. No separatepermissions were required to use direct quotes from the policy documentsused in this study.
Paudel et al. BMC Health Services Research (2019) 19:166 Page 14 of 16

FundingThe work was supported by Flinders University, Adelaide. The principalauthor received postgraduate scholarship and research student maintenancesupport, which was used to manage the principal researcher’s living cost inAustralia and to cover overseas travel and living cost during his researchfieldwork in Nepal.
Authors’ contributionsMohan Paudel (MP) designed and analyzed the study in consultation withSara Javanparast (SJ), Gouranga Dasvarma (GD) and Lareen Newman (LN).MP wrote the original draft of the manuscript. SJ, GD and LN reviewed andrevised the manuscript. All authors have approved the final manuscript.
Ethics approval and consent to participateThis policy review is a part of a larger PhD project that was approved by theresearch ethics committees of Flinders University South Australia and NepalHealth Research Council.
Consent for publicationNot applicable.
Competing interestsThe authors declare that they have no competing interests.
Publisher’s NoteSpringer Nature remains neutral with regard to jurisdictional claims inpublished maps and institutional affiliations.
Author details1Initiative for Research, Education and Community Health-Nepal, Kathmandu,Nepal. 2Southgate Institute of Health, Society & Equity, Flinders University,Adelaide, Australia. 3College of Humanities, Arts and Social Sciences, FlindersUniversity, Adelaide, Australia. 4Education Arts and Social Sciences DivisionalOffice, University of South Australia , Adelaide, Australia.
Received: 7 February 2018 Accepted: 27 February 2019
References1. WHO. Definitions and indicators in family planning maternal & child health
and reproductive health used in the WHO regional office for Europe. 2000.2. WHO. Fact Sheet: Maternal, newborn, child and adolescent Health 2015
[cited 2015 12 July]. Available from: http://www.who.int/maternal_child_adolescent/epidemiology/stillbirth/en/.
3. WHO. Global Health Observatory (GHO) Data, neonatal mortality: situationand trends 2015 [cited 2016 12 July]. Available from: http://www.who.int/gho/child_health/mortality/neonatal_text/en/.
4. Lawn JE, Blencowe H, Oza S, You D, Lee AC, Waiswa P, et al. Progress,priorities, and potential beyond survival. The Lancet. 2014;384:189–205.
5. Mason E, McDougall L, Lawn JE, Gupta A, Claeson M, Pillay Y, et al. Fromevidence to action to deliver a healthy start for the next generation. TheLancet. 2014;384:438–54.
6. NPC. The Millennium Development Goals, Final Status Report, 2000–2015.Kathmandu: Nepal Government of Nepal NPC; 2016.
7. UNICEF and WHO. Countdown to 2015 Maternal, newborn and childsurvival: a decade of tracking Progress for maternal, newborn and childsurvival, the 2015 report. Geneva, Switzerland: 2015.
8. MOHP, New ERA, ICF International Inc. Nepal demographic and healthsurvey 2011. Kathmandu, Nepal: Ministry of Health and Population, NewERA, and ICF International, Calverton, Maryland, 2012.
9. Paudel D, Thapa A, Shedain PR, Paudel B. Trends and Determinants ofNeonatal Mortality in Nepal: Further Analysis of the Nepal Demographicand Health Surveys, 2001-2011. Kathmandu, Nepal: 2013 2013. Report No.
10. MOHP, New ERA, ICF International Inc. Nepal demographic and healthsurvey 2006. Kathmandu, Nepal: Ministry of Health and Population, NewERA, and ICF International, Calverton, Maryland, 2007.
11. MOHP, New ERA, ICF International Inc. Nepal demographic and healthsurvey 2016. Kathmandu, Nepal: Ministry of Health and Population, NewERA, and ICF International, Calverton, Maryland, 2017.
12. MOHP, New ERA, ICF International Inc. Nepal demographic and healthsurvey 2016: key indicators report. Kathmandu, Nepal: Ministry of Health
and Population, New ERA, and ICF International, Calverton, Maryland,2017.
13. UNICEF. Levels and trends in child mortality: report 2017, estimatesdeveloped by the UN inter-agency Group for Child Mortality Estimation.New York: UN IGME; 2017.
14. Van Olmen J, Marchal B, Van Damme W, Kegels G, Hill PS. Health systemsframeworks in their political context: framing divergent agendas. BMCPublic Health. 2012;12(1):774.
15. Walt G, Gilson L. Reforming the health sector in developing countries: thecentral role of policy analysis. Health Policy Plan. 1994;9(4):353–70.
16. Hafner T, Shiffman J. The emergence of global attention to health systemsstrengthening. Health policy and planning. 2012:czs023.
17. Black N, Donald A. Evidence based policy: proceed with careCommentary:research must be taken seriously. Bmj. 2001;323(7307):275–9.
18. Fisher M, Baum FE, Macdougall C, Newman L, Mcdermott D. To what Extentdo Australian Health Policy Documents address Social Determinants ofHealth and Health Equity? Journal of Social Policy. 2016:1–20.
19. Murray C, Frenk J. World health report 2000: a step towards evidence-basedhealth policy. Lancet. 2001;357(9269):1698–700.
20. Paudel M. Socio-cultural and health care contexts of perinatal survival inRural Mountain villages of Nepal: Flinders University 2017.
21. Glenton C, Scheel IB, Pradhan S, Lewin S, Hodgins S, Shrestha V. The femalecommunity health volunteer programme in Nepal: decision makers’perceptions of volunteerism, payment and other incentives. Soc Sci Med.2010;70(12):1920–7.
22. Government of Nepal. National health policy. Kathmandu (Nepal): Ministryof Health and Population, 1991.
23. Dixit H. Nepal’s quest for health: (health Services of Nepal): educationalpublishing house; 2005.
24. Ministry of Health and Population [Nepal]. National Reproductive HealthStrategy. Kathmandu (Nepal): Deparment of Health Services (Family HealthDivision), 1998.
25. Pradhan A, Aryal RH, Regmi G, Ban B, Govindasamy P. Nepal family healthsurvey 1996; 1997.
26. Garenne M, Ronsmans C, Campbell H. The magnitude of mortality fromacute respiratory infections in children under 5 years in developingcountries. World health statistics quarterly. 1992;45:180.
27. MOHP. National Safe Motherhood and Newborn Health Long-Term Plan,2006–2017, MOHP, Kathmandu (2006). Kathmandu (Nepal): family healthdivision, Department of Health Services, Nepal, 2006.
28. MOHP. National Neonatal Health Strategy. Kathmandu (Nepal): Departmentof Health Services (Child Health Division), Ministry of Health and Population(MOHP) Nepal, 2004.
29. MOHP. National Policy on skilled birth attendants (Supplementatry to safemotherhood policy 1998). Kathmandu (Nepal): Family Health Division,Department of Health Services, Nepal, 2006.
30. MOHP. Mother’s Protection Program-Implementation Guideline, 2008(Second Amendment 2013). Kathmandu, Nepal: Department of HealthServices (Family Health Division), 2013.
31. MOHP. Maternal and Perinatal Death Surveillance and Response (MPDSR)Guideline, 2014. Kathmandu, Nepal: Department of Health Services (FamilyHelath Division), 2014.
32. DoHS. Community Based Integrated Management of Neonatal andChildhood Illness (Program Management Module). Kathmandu (Nepal):Child Health Division [Department of Health Services], 2015.
33. MOHP. National Safe Motherhood and Newborn Health Long-Term Plan,2002–2017, MOHP, Kathmandu (2002). In: family health division DoHS,Nepal, editor. Kathmandu, Nepal: Department of Health Services, Ministry ofHealth and population (MOHP), Nepal; 2002.
34. MOHP. Health Sector Strategy: An Agenda for Reform. Kathmandu (Nepal):Ministry of Health (MOH), Nepal; 2004.
35. Government of Nepal. Nepal Millennium Development Goals ProgressReport 2005. In: National Planning Commission N, editor. Kathmandu[Nepal]: National Planning Commission, Nepal; 2005.
36. MOHP. National Safe Motherhood and Newborn Health Long-Term Plan,2002–2017, MOHP, Kathmandu (2002). Kathmandu (Nepal): Department ofHealth Services (family health division), Ministry of Health and population(MOHP), Nepal, 2002.
37. MOHP. Safe Delivery Incentive Programme, Implementation Guideline 2005(First amended version 2007). In: Servcies DoH, editor. Kathmandu, Nepal:family health division, Deapartment of Health Services, Nepal; 2007.
Paudel et al. BMC Health Services Research (2019) 19:166 Page 15 of 16

38. Paudel M, Javanparast S, Dasvarma G, Newman L. Religio-cultural factorscontributing to perinatal mortality and morbidity in mountain villages of Nepal:Implications for future healthcare provision. PloS one. 2018;13(3):e0194328-e.
39. Walley J, Lawn JE, Tinker A, De Francisco A, Chopra M, Rudan I, et al. Primaryhealth care: making Alma-Ata a reality. Lancet. 2008;372(9642):1001–7.
40. WHO. Primary Health Care: Report of the international conference onprimary health care. Alma Atta: USSR: World Health Organization; 1978.
41. Pradhan Y, Upreti SR, K C, N P, Ashish K, Khadka N, Syed U, et al. Newbornsurvival in Nepal: a decade of change and future implications. Health policyand planning. 2012;27(suppl 3):iii57–71.
42. Sabatier PA. Toward better theories of the policy process. PS: PoliticalScience & Politics. 1991;24(02):147–56.
43. CSDH. Closing the gap in a generation: health equity through action on thesocial determinants of health. Final Report of the Commission on SocialDeterminants of Health. Geneva: World Health Organization; 2008.
44. WHO. Every newborn: an action plan to end preventable deaths. Geneva,Switzerland: World Health Organization, 2014.
45. WHO. The Ottawa Charter for Health Promotion: First InternationalConference on Health Promotion, Ottawa, 21 November 1986 2016 [cited2016 2 August]. Available from: http://www.who.int/healthpromotion/conferences/previous/ottawa/en/.
46. Paudel M, Javanparast S, Dasvarma G, Newman L. A qualitative study aboutthe gendered experiences of motherhood and perinatal mortality inmountain villages of Nepal: implications for improving perinatal survival.BMC Pregnancy and Childbirth. 2018;18(1):163.
47. Paudel M, Javanparast S, Newman L, Dasvarma G. Health system barriersinfluencing perinatal survival in mountain villages of Nepal: implications forfuture policies and practices. Journal of Health, Population and Nutrition.2018;37(1):16.
48. Smith SL, Neupane S. Factors in health initiative success: learning fromNepal’s newborn survival initiative. Soc Sci Med. 2011;72(4):568–75.
49. MOHP. National Safe Motherhood and newborn health long-term plan,2006–2017. In: family health division DoHS, Nepal, editor. Kathmandu, Nepal:Family Health Division, Department of Health Services, Nepal; 2006.
50. MOHP. National Neonatal Health Strategy. In: Child Health Division DoHS,Nepal, editor. Kathmandu, Nepal: Department of Health Services (ChildHealth Division), Ministry of Health and Population (MOHP) Nepal; 2004.
51. WHO. Declaration of alma ata: Report of the international conference onprimary health care. Alma Atta: USSR: World Health Organization; 1978.
52. Solar O, Irwin A. A conceptual framework for action on the socialdeterminants of health. Social Determinants of Health Discussion Paper 2.Geneva: World Health Organization: World Health Organization; 2010.
53. Newman L, Baum F, Harris E. ‘Review Framework’, Australian Governments & HealthInequities Project2006 October 07, 2014 [cited 2014 October 07]. Available from:http://som.flinders.edu.au/FUSA/PublicHealth/AHIP/projects_list.htm.
54. Newman L, Baum F, Harris E. Federal, state and territory governmentresponses to health inequities and the social determinants of health inAustralia. Health Promotion Journal of Australia. 2006;17(3):217.
Paudel et al. BMC Health Services Research (2019) 19:166 Page 16 of 16