
A comparative evaluation of cardioprotective activity of...
10
Indian Journal of Natural Products and Resources Vol. 2(3), September 2011, pp. 335-344 A comparative evaluation of cardioprotective activity of two Makandi (Coleus forskohlii Willd.) formulations against isoproterenol induced myocardial infarction in hyperlipidaemic rats Madhavi Jagtap 1 , B K Ashok 2 , Sulakshan S Chavan 3 , H M Chandola 1 and B Ravishankar 4 * 1 Department of Kayachikitsa, 2 Pharmacology Laboratory, 3 CCRAS, Pharmacological Research Unit, Institute for Post Graduate Teaching & Research in Ayurveda, Gujarat Ayurved University, Jamnagar - 361 008, Gujarat, India 4 SDM Research Centre for Ayurveda and Allied Sciences, Kuthpady, Udupi - 574 118, Karnataka, India Received 21 July 2010; Accepted 29 March 2011 The present study was undertaken to evaluate cardioprotective activity of Makandi (Coleus forskohli Willd.) Churna and Ghanavati on the basis of electrocardiographic, biochemical, cardiac output and histopathological parameters against isoproterenol (ISO) induced myocardial infarction in diet induced hyperlipidaemic rats. The drug treatment and hyperlipidaemic diets were administered for 20 consecutive days. Myocardial injury was induced by injecting ISO (85 mg/kg) to rats at an interval of 24 h for two days. Forty eight hours after the first dose of ISO injection, parameters like ECG, cardiac output, biochemical and histological observations of the heart tissues were performed. Hyperlipidaemic diet followed by ISO significantly increased heart weight, altered serum lipid profiles, SGPT and ALP activity, caused ST segment elevation, prolonged QT interval and QTc in ECG, increased blood pressure and decreased cardiac output. Histopathologically also, heart showed severe cytoarchitectural disturbances like myonecrosis, fatty changes and endocardial oedema. When administered orally, both the formulations of Makandi decreased atherogenic index, almost normalized ST segment elevation, QT interval prolongation and cardiac output. Histopathologically also remarkable protection was observed. Analysis of the results showed that Makandi in Churna form has both anti-atherogenic potential and cardioprotective activity, while Ghanavti has only weak cardioprotective activity. Keywords: Cardioprotective, Coleus forskohlii, Hyperlipidaemia, Makandi, Makandi churna, Makandi ghanavati, Myocardial infarction. IPC code; Int. cl. (2011.01) A61K 36/53, A61K 125/00, A61P 9/00 Introduction Coleus forskohlii Willd. is popularly known as Makandi in Ayurveda belonging to the family Lamiaceae, has been used in traditional medicine since ancient times for treatment of heart diseases, abdominal colic and respiratory disorders 1,2 . The plant is a rich source of a diterpene, forskolin which is virtually responsible for all reported pharmacological activities. It is an activator of adenylate cyclase 3,4 and also has positive ionotropic, anti-glaucoma, anti-inflammatory, anti-platelet aggregation, bronchospasmolytic actions 5 and reduce body weight by increasing lean body mass 6 . However, almost all activities have been carried out on active principle forskolin i.e., on the isolated fraction of the drug. Till date no work has been reported on conventional Ayurvedic preparations of this drug. The majority of the studies show that hyperlipidaemia, independently from the development of coronary atherosclerosis, worsens the outcome of ischaemic injury 7 . These findings emphasize the necessity of lipid lowering therapy and promote the development of new cardioprotective drugs that are capable to reverse the increased susceptibility of hearts to ischaemic stress and to recapture cardiac stress adaptation in hyperlipidaemia. Thus, the present study was undertaken to evaluate comparative cardioprotective effect of two formulations prepared from Makandi, viz. Makandi churna (powder of roots) and Makandi ghanavati (concentrated form of aqueous extract from roots) against isoproterenol induced cardiac injury in hyperlipidaemic diet induced hyperlipidaemic rats. __________ *Correspondent author: E-mail: [email protected]; Phone: 09483929319 (Mob.)
Transcript of A comparative evaluation of cardioprotective activity of...

Indian Journal of Natural Products and Resources
Vol. 2(3), September 2011, pp. 335-344
A comparative evaluation of cardioprotective activity of two Makandi
(Coleus forskohlii Willd.) formulations against isoproterenol induced
myocardial infarction in hyperlipidaemic rats
Madhavi Jagtap1, B K Ashok
2, Sulakshan S Chavan
3, H M Chandola
1 and B Ravishankar
4*
1Department of Kayachikitsa, 2Pharmacology Laboratory, 3CCRAS, Pharmacological Research Unit, Institute for
Post Graduate Teaching & Research in Ayurveda, Gujarat Ayurved University, Jamnagar - 361 008, Gujarat, India 4SDM Research Centre for Ayurveda and Allied Sciences, Kuthpady, Udupi - 574 118, Karnataka, India
Received 21 July 2010; Accepted 29 March 2011
The present study was undertaken to evaluate cardioprotective activity of Makandi (Coleus forskohli Willd.) Churna and
Ghanavati on the basis of electrocardiographic, biochemical, cardiac output and histopathological parameters against
isoproterenol (ISO) induced myocardial infarction in diet induced hyperlipidaemic rats. The drug treatment and
hyperlipidaemic diets were administered for 20 consecutive days. Myocardial injury was induced by injecting ISO
(85 mg/kg) to rats at an interval of 24 h for two days. Forty eight hours after the first dose of ISO injection, parameters like
ECG, cardiac output, biochemical and histological observations of the heart tissues were performed. Hyperlipidaemic diet
followed by ISO significantly increased heart weight, altered serum lipid profiles, SGPT and ALP activity, caused ST
segment elevation, prolonged QT interval and QTc in ECG, increased blood pressure and decreased cardiac output.
Histopathologically also, heart showed severe cytoarchitectural disturbances like myonecrosis, fatty changes and
endocardial oedema. When administered orally, both the formulations of Makandi decreased atherogenic index, almost
normalized ST segment elevation, QT interval prolongation and cardiac output. Histopathologically also remarkable
protection was observed. Analysis of the results showed that Makandi in Churna form has both anti-atherogenic potential
and cardioprotective activity, while Ghanavti has only weak cardioprotective activity.
Keywords: Cardioprotective, Coleus forskohlii, Hyperlipidaemia, Makandi, Makandi churna, Makandi ghanavati,
Myocardial infarction.
IPC code; Int. cl. (2011.01) A61K 36/53, A61K 125/00, A61P 9/00
Introduction
Coleus forskohlii Willd. is popularly known as
Makandi in Ayurveda belonging to the family
Lamiaceae, has been used in traditional medicine
since ancient times for treatment of heart diseases,
abdominal colic and respiratory disorders1,2
. The plant
is a rich source of a diterpene, forskolin which is
virtually responsible for all reported pharmacological
activities. It is an activator of adenylate cyclase3,4
and also has positive ionotropic, anti-glaucoma,
anti-inflammatory, anti-platelet aggregation,
bronchospasmolytic actions5 and reduce body weight
by increasing lean body mass6. However, almost all
activities have been carried out on active principle
forskolin i.e., on the isolated fraction of the drug. Till
date no work has been reported on conventional
Ayurvedic preparations of this drug.
The majority of the studies show that
hyperlipidaemia, independently from the development
of coronary atherosclerosis, worsens the outcome of
ischaemic injury7. These findings emphasize the
necessity of lipid lowering therapy and promote the
development of new cardioprotective drugs that are
capable to reverse the increased susceptibility of
hearts to ischaemic stress and to recapture cardiac
stress adaptation in hyperlipidaemia. Thus, the present
study was undertaken to evaluate comparative
cardioprotective effect of two formulations prepared
from Makandi, viz. Makandi churna (powder of
roots) and Makandi ghanavati (concentrated form of
aqueous extract from roots) against isoproterenol
induced cardiac injury in hyperlipidaemic diet
induced hyperlipidaemic rats.
__________
*Correspondent author: E-mail: [email protected];
Phone: 09483929319 (Mob.)

INDIAN J NAT PROD RESOUR, SEPTEMBER 2011
336
Materials and Methods
Test formulations
The fresh tuberous roots of Makandi (C. forskohli,
Plate 1) were procured from local market and
authenticated by qualified pharmacognosist of our
institute through macroscopical and microscopical
characters. The tuberous roots were washed with
water, cut into pieces and dried under shade. The
Churna (MC) and Ghanavati of Makandi (MG) were
prepared from dried roots as per classical procedure8,9
.
Prelimnary phytochemical studies
Both Churna and Ghanavati of Makandi were
subjected to preliminary phytochemical studies
including quantitative phytochemical investigation
through HPLC analysis for important chemical
moiety as forskolin10
. The separation was carried out
on a C-18 column (Inertsil C18 250 mm × 4.6 mm i.d.
with a 5 µm particle size) using Acetonitrile : Water
(90:10 v/v) as mobile phase. The eluent was
monitored using a UV-Visible detector at 210 nm.
Standard Forskolin (87.00 %) was used as marker
compound.
Animals
Wistar strain albino rats of either sex weighing
200 ± 30 g were selected from the animal house
attached to the institute. They were housed at
25 ± 03°C with constant humidity of 50-70% on a
12 hour natural day and night cycles. They were fed
with diet Amrut brand rat pellet food supplied by
Pranav Agro Industries, Baroda and tap water was
given ad libitum. Institutional Animal Ethics
Committee had approved the experimental protocol
(Approval number IAEC/09-10/05MD 04) and the
care of animals was taken as per the CPCSEA
guidelines.
Dose selection and schedule
The clinical dose of Makandi ghanavati and
Makandi churna are 3 and 4.2 g, respectively10
. The
dose for experimental animals was calculated by
extrapolating the human dose to animals (270 mg
rounded to 300 mg/kg and 378 mg rounded to
400 mg/kg, respectively) based on the body surface
area ratio by referring to the standard table of Paget
and Barnes (1969)11
. The human doses of the
formulations were decided on the basis of the clinical
experiences, palatability, since the majority of clinical
studies have used injected forskolin, it is unclear if
oral ingestion of these formulations will provide
similar benefits in the amounts recommended by
various authors [About 80 g of dried course powder of
Makandi gives 14 g of Ghana (aqueous extract)]. The
drug solutions were made with distilled water and
administered to animals (0.5 ml/100 g body weight)
with the help of gastric catheter sleeved to syringe.
The drugs were administered to over night fasted
animals.
Statistical analysis
The results were presented as Mean ± SEM for six
rats in each group. Statistical comparisons were
performed by both unpaired student’s t test and one
way ANOVA with Dunnets’ multiple t test as post-hoc
test by using Sigma stat software (version 3.1) for
all the treated groups with the level of significance
set at P<0.05.
Plate 1 Coleus forskohlii: a-Plant, b-Tuberous roots
JAGTAP et al.: EVALUATION OF CARDIOPROTECTIVE ACTIVITY OF MAKANDI FORMULATIONS
337
Experimental protocol
The experimental rats were divided into six groups
of 6 animals each and treated as follows:
Group I: Normal control rats received distilled
water (NC)
Group II: Cholesterol control rats treated with
hyperlipidaemic diet (CC)
Group III: Isoproterenol control rats treated with
Isoproterenol (ISO) (85 mg/kg body weight,
s.c. in saline).
Group IV: Cholesterol plus Isoproterenol
(CCISO) control group
Group V: Makandi ghanavati (MG) +
cholesterol + Isoproterenol (MG + CCISO)
Group VI: Makandi churna (MC) + cholesterol
+ Isoproterenol (MC + CCISO)
Test drugs and vehicles were administered to
respective groups at morning hours and continued for
20 days. The hyperlipidaemic diet was administered
to different groups to induce hyperlipidaemia based
on previous studies12,13
. The hyperlipidaemic diet
includes hydrogenated vegetable oil (Vanaspati Ghee-
'Raag' brand, Batch No. BA 55, Adani Wilmar Ltd.,
Gujarat) and cholesterol extra pure powder (Batch
No. 14022 Suvidhnath Laboratories, Baroda) made in
to 20% suspension in coconut oil (Parachute coconut
oil, Batch No. PSO73, Goa). The suspension was
administered (0.5 ml/100 g) to the rats daily for
20 days (at evening hours) to all the groups except
normal control (Group I) and isoproterenol control
(Group II) group. On 20th day, 1 hour after the
administration of test drug and vehicle, ISO was
administered subcutaneously. Two doses of ISO
(85 mg/kg) were administered at 24 hours interval14
.
Measurement of ECG
At the end of experimental period (after 24 h of
second ISO injection) the rats were anaesthetized with
ether and ECGs were recorded using a portable
electrocardiogram machine (Cardiofax-Medicaid
systems). ECG was recorded by using only the four
standard (limb) leads attached to four extremities of
the animals, the chest leads were not used. In all cases
of myocardial infarction, Lead II show the clear,
distinct individual waves than Lead I and III.
Therefore, ECG was monitored on Lead II only.
Measurement of blood pressure and cardiac output
Systolic blood pressure, diastolic blood pressure,
mean blood pressure, pulse rate, cardiac output (CO),
left cardiac work (LCW), left ventricular ejection time
(LVET), pre-ejection period (PEP) and stroke index
(SI) were recorded using impedance cardiographic
analysis (ICG) provided with BIOPAC student
lab system using Sramek/VEPT method in
anaesthetized rats. Biochemical analysis
After recording the BP and cardiac output, blood
was collected from retro-orbital plexus, serum was
separated and used for estimation of different serum
biochemical parameters. The procedure followed for
this was a requisite quantity of serum fed to the auto
analyzer (Fully automated Biochemical Random
Access Analyzer, BS-200; Lilac medicare Pvt. Ltd.,
Mumbai) which was automatically drawn in to the
instrument for estimating different biochemical
parameters like serum total cholesterol (CHOD–PAP,
end point)15
, serum HDL cholesterol (Trinder
reaction)16
, serum triglyceride (GOP–PAP method,
end point)17
, serum alkaline phosphatase (IFCC
Method, Kinetic method)18
, SGOT (IFCC method
without Pyridoxal Phosphate)19
and SGPT activity
(IFCC method, kinetic without Pyridoxal
Phosphate)20
, VLDL was calculated by using formula
VLDL=TG/5, LDL by LDL={TC-(HDL-VLDL)}21
and atherogenic index by=TC/HDL22
. Histopathological studies
At the end of the study, all the rats were sacrificed
by overdose of ether anaesthesia and the heart was
dissected out, washed in ice cold saline. The weight of
heart was noted and the tissues were immediately
fixed in 10% buffered neutral formalin solution. After
fixation, tissues were embedded in paraffin and serial
sections were cut and each section was stained with
hematoxylin and eosin23
. The slides were viewed
under Trinocular Research Microscope (Germany) at
various magnifications to note down the changes in
the microscopic features of the tissues studied.
Results and Discussion
Effect on heart weight
The heart weight of rats treated with isoprotrenol
significantly increased when compared with the
normal control rats (Table 1). Nirmala and
Puvanakrishnan (1996)24
have reported that this
increase in heart weight might be due to increased
oedema within intramuscular space, massive vascular
hemorrhage and/or extensive necrosis of cardiac
muscle fibres followed by the invasion of damaged
tissues with inflammatory cells. These observations

INDIAN J NAT PROD RESOUR, SEPTEMBER 2011
338
are in line with the histopathological findings of our
study. Both the test drugs did not attenuate the
observed cardiac weight gain. This may be due to
persistent oedematous condition in the heart in spite
of drug treatment.
Effect on serum lipid profiles
High cholesterol diet is regarded as an important
factor in the development of cardiac diseases
since it leads to development of hyperlipidemia,
atherosclerosis and ischemic heart disease25
. In the
present study feeding of hyperlipidemic diet not only
elevated serum cholesterol level but also elevated BP.
Injection of isoprenaline in hyperlipidemic diet given
rats produced higher degree of cardiac injury. Though
the injury profile was similar to isoprenaline treated
but the severity of the injurious lesions were
remarkably high (Plate 2d).
Administration of cholesterol and hyperlipidemic
diet lead to significant elevation of serum total
cholesterol, LDL cholesterol and atherogenic index.
The increase in total cholesterol was maintained even
after injection of the isoprenaline, in addition
significant decrease in serum triglyceride, HDL-
cholesterol and VLDL-cholesterol was observed.
Both MG and MC failed to attenuate serum lipids
elevations. However, CCISO induced atherogenic
index which is the ratio of total cholesterol to
HDL-cholesterol, was remarkably reversed by both
MG and MC treatment (Table 2).
The serum triglyceride levels were found
moderately lowered in CC and ISO given groups.
When both of them were combined as in case of
CCISO group, significant lowering of triglyceride
level was observed. This lowering can be attributed to
isoprenaline induced modulation of triglyceride
metabolism possibly through increased utilization.
Since similar decrease was observed in case of VLDL
cholesterol also. It implies that metabolism of VLDL
may also be modulated. The probable mechanisms of
the observed triglyceride lowering can be due to
increase in β-oxidative degradation of fatty acids, and
lipoprotein lipase activity leading to increased
metabolism of triglycerides in VLDL particles and
chylomicrons and diversion of fatty acids to muscles
for utilization in their activity along with reduction in
Table 1 Effect of Makandi ghanavati and Makandi churna on heart weight
Parameter NC CC ISO CCISO MG + CCISO MC + CCISO
Heart weight
(g/100g)
0.325 ± 0.0169 0.312 ± 0.0098 0.453 ±
0.0144***®
0.436 ±
0.0152***®
0.423 ± 0.0114 0.454 ± 0.0267
The data were expressed as Mean ± SEM; significant differences in each group vs the control is ***P< 0.001.
(® ONE WAY ANOVA-F value 27.133; P<0.001 DMTT- P<0.05 for ISO and CCISO vs Control).
Table 2 Effect of Makandi ghanavati and Makandi churna on serum lipid profiles
Parameter NC CC ISO CCISO MG + CCISO MC + CCISO
Serum
Cholesterol
64.00 ± 2.37 73.50 ± 3.09* 82.50 ± 8.61* 81.00 ± 4.76** 98.33 ± 7.81 86.50 ± 8.01
Serum HDL
cholesterol
36.33 ± 3.04 30.00 ± 1.84 25.17 ± 2.01* 26.83 ± 1.70* 34.33 ± 2.20 36.50 ± 3.27#®®
Serum VLDL
cholesterol
20.57 ± 2.75 17.30 ± 1.21 12.87 ± 3.02 11.60 ± 1.12* 10.00 ± 1.37 14.10 ± 2.76
Serum LDL
cholesterol
48.23 ± 2.53 65.40 ± 6.26* 70.20 ± 7.60* 67.77 ± 5.06** 74.00 ± 7.99 64.10 ± 6.60
Atherogenic
index
1.82 ± 0.15 2.68 ± 0.19**® 3.43 ± 0.50**® 3.42 ± 0.32*** ®
2.28 ± 0.29#¥ 2.42 ± 0.31#
Serum
triglyceride
102.83 ± 13.75 86.50 ± 6.07 64.33 ± 15.09 58.00 ± 5.59* 50.00 ± 6.85 70.50 ± 13.82
The data were expressed as Mean ± SEM and unit of each parameter is (mg/dL).
Significant differences in each group vs. the normal control are *P< 0.05, **P< 0.01 and ***P< 0.001; vs CCISO are #P <0.05
(® ONE WAY ANOVA-F value 5.726; P=0.005 DMTT- P<0.05 for ISO and CCISO vs Control)
(®®ONE WAY ANOVA-F value 4.982; P=0.025 DMTT- P<0.05 for MC + CCISO vs CCISO)
(¥ONE WAY ANOVA-F value 4.240; P=0.038 DMTT- P<0.05 for MG + CCISO vs CCISO)
JAGTAP et al.: EVALUATION OF CARDIOPROTECTIVE ACTIVITY OF MAKANDI FORMULATIONS
339
hepatic production of VLDL26
. CCISO induced
lowering was not antagonized by the test preparations.
Instead, further lowering was observed. The reason
for this lowering of VLDL was not known.
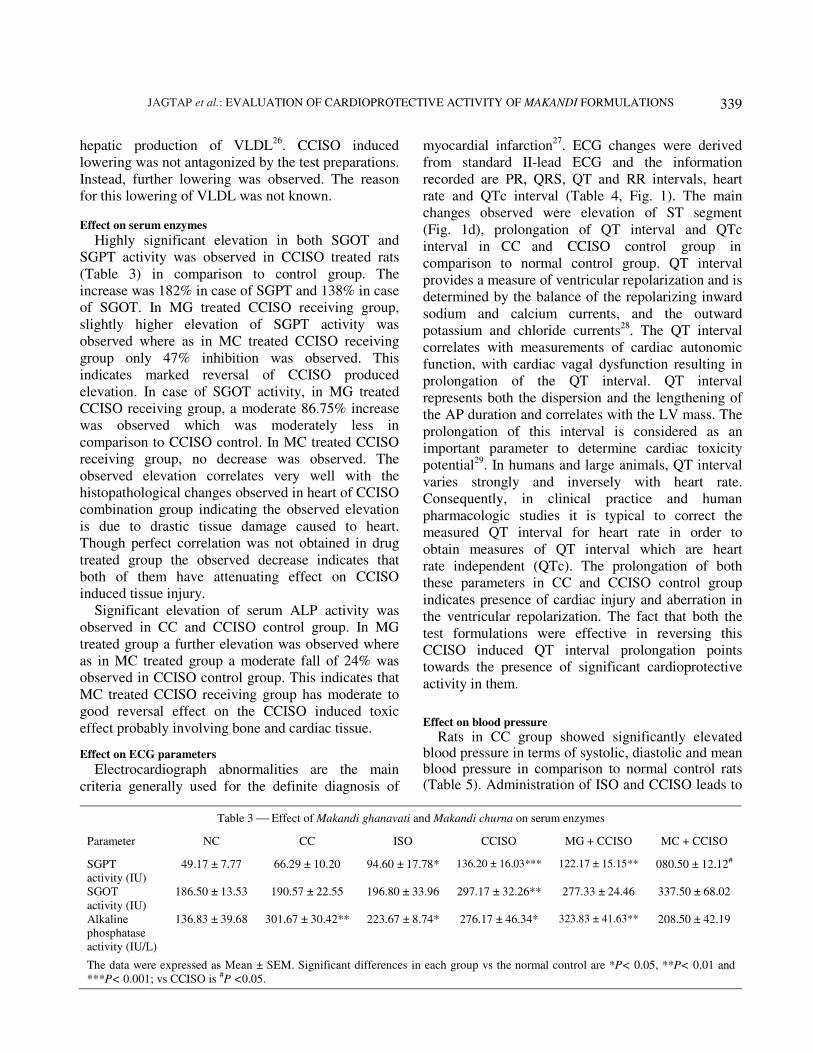
Effect on serum enzymes
Highly significant elevation in both SGOT and
SGPT activity was observed in CCISO treated rats
(Table 3) in comparison to control group. The
increase was 182% in case of SGPT and 138% in case
of SGOT. In MG treated CCISO receiving group,
slightly higher elevation of SGPT activity was
observed where as in MC treated CCISO receiving
group only 47% inhibition was observed. This
indicates marked reversal of CCISO produced
elevation. In case of SGOT activity, in MG treated
CCISO receiving group, a moderate 86.75% increase
was observed which was moderately less in
comparison to CCISO control. In MC treated CCISO
receiving group, no decrease was observed. The
observed elevation correlates very well with the
histopathological changes observed in heart of CCISO
combination group indicating the observed elevation
is due to drastic tissue damage caused to heart.
Though perfect correlation was not obtained in drug
treated group the observed decrease indicates that
both of them have attenuating effect on CCISO
induced tissue injury.
Significant elevation of serum ALP activity was
observed in CC and CCISO control group. In MG
treated group a further elevation was observed where
as in MC treated group a moderate fall of 24% was
observed in CCISO control group. This indicates that
MC treated CCISO receiving group has moderate to
good reversal effect on the CCISO induced toxic
effect probably involving bone and cardiac tissue.
Effect on ECG parameters
Electrocardiograph abnormalities are the main
criteria generally used for the definite diagnosis of
myocardial infarction27
. ECG changes were derived
from standard II-lead ECG and the information
recorded are PR, QRS, QT and RR intervals, heart
rate and QTc interval (Table 4, Fig. 1). The main
changes observed were elevation of ST segment
(Fig. 1d), prolongation of QT interval and QTc
interval in CC and CCISO control group in
comparison to normal control group. QT interval
provides a measure of ventricular repolarization and is
determined by the balance of the repolarizing inward
sodium and calcium currents, and the outward
potassium and chloride currents28
. The QT interval
correlates with measurements of cardiac autonomic
function, with cardiac vagal dysfunction resulting in
prolongation of the QT interval. QT interval
represents both the dispersion and the lengthening of
the AP duration and correlates with the LV mass. The
prolongation of this interval is considered as an
important parameter to determine cardiac toxicity
potential29
. In humans and large animals, QT interval
varies strongly and inversely with heart rate.
Consequently, in clinical practice and human
pharmacologic studies it is typical to correct the
measured QT interval for heart rate in order to
obtain measures of QT interval which are heart
rate independent (QTc). The prolongation of both
these parameters in CC and CCISO control group
indicates presence of cardiac injury and aberration in
the ventricular repolarization. The fact that both the
test formulations were effective in reversing this
CCISO induced QT interval prolongation points
towards the presence of significant cardioprotective
activity in them.
Effect on blood pressure
Rats in CC group showed significantly elevated blood pressure in terms of systolic, diastolic and mean blood pressure in comparison to normal control rats (Table 5). Administration of ISO and CCISO leads to
Table 3 Effect of Makandi ghanavati and Makandi churna on serum enzymes
Parameter NC CC ISO CCISO MG + CCISO MC + CCISO
SGPT
activity (IU)
49.17 ± 7.77 66.29 ± 10.20 94.60 ± 17.78* 136.20 ± 16.03*** 122.17 ± 15.15** 080.50 ± 12.12#
SGOT
activity (IU)
186.50 ± 13.53 190.57 ± 22.55 196.80 ± 33.96 297.17 ± 32.26** 277.33 ± 24.46 337.50 ± 68.02
Alkaline
phosphatase
activity (IU/L)
136.83 ± 39.68 301.67 ± 30.42** 223.67 ± 8.74* 276.17 ± 46.34* 323.83 ± 41.63** 208.50 ± 42.19
The data were expressed as Mean ± SEM. Significant differences in each group vs the normal control are *P< 0.05, **P< 0.01 and
***P< 0.001; vs CCISO is #P <0.05.

INDIAN J NAT PROD RESOUR, SEPTEMBER 2011
340
moderate non-significant fall in BP in comparison to normal control. This shows that ISO instead of elevating BP has the tendency of lowering it in CC given groups. Both MG and MC failed to antagonize the hyperlipidaemic diet induced BP elevation.
Effect on cardiac output parameters
The main and significant change that was observed
after feeding rats with cholesterol rich diet and
CCISO combination was decrease in cardiac output
(Table 6). This decrease was found completely
reversed in MC treated group. MG did not reverse this
decrease, however a slight further decrease was
observed. The left cardiac work was also found to be
decreased in CCISO group in comparison to normal
control rats. This decrease was also reversed by MC
while MG did not produce the reversal. Left
ventricular ejection time was found to be moderately
prolonged by CCISO combination this moderate
prolongation was not influenced by either of the test
drugs. Stroke index was found moderately decreased
in CCISO group in comparison to normal control. The
stroke index was found doubled in MC administered
group in comparison to CCISO control whereas in
MG treated group, a marginal decrease was observed.
Thus, the overall profile indicates that administration
of CCISO combination leads to significant reduction
in the working capacity of the heart. This
incapacitation was completely reversed by MC while
MG was not effective. Histopathological findings
No inflammatory cells infiltration was seen in the
heart of normal control rats (Plate 2a & b).
Isoprenaline injection to rats leads to significant
myonecrosis, infiltration of inflammatory cells, fatty
changes and endocardial oedema compared to normal
control (Plate 2c). In CCISO control group these
Table 4 Effect of Makandi ghanavati and Makandi churna on ECG parameters
Parameter NC CC ISO CCISO MG + CCISO MC + CCISO
PR interval 0.035 ±
0.0034
0.040 ±
0.0022
0.041 ±
0.0051
0.038 ±
0.0016
0.036 ±
0.0036
0.037 ±
0.0019
QRS interval 0.043 ±
0.0021
0.046 ±
0.0015
0.040 ±
0.0039
0.046 ±
0.0029
0.035 ±
0.0056
0.046 ±
0.001
QT interval 0.082 ±
0.0030
0.102 ±
0.0031***
0.109 ±
0.0179
0.113 ±
0.0078***
0.0872 ±
0.0042##
0.0908 ±
0.0025#
Heart rate 339.111 ±
11.08
354.667 ±
39.95
362.200 ±
44.52
384.200 ±
22.24
418.833 ±
12.19
463.750 ±
27.29
RR interval 0.177 ±
0.0062
0.181 ±
0.0206
0.178 ±
0.0258
0.158 ±
0.0086
0.144 ±
0.0043
0.131 ±
0.0075
QTc 0.193 ±
0.0056
0.245 ±
0.0093***®
0.255 ±
0.0183**®
0.285 ±
0.0109***®
0.231 ±
0.0110#β
0.252 ±
0.0068#
The data were expressed as Mean ± SEM.
Significant differences in each group vs. the control are *P< 0.05, **P< 0.01 and ***P< 0.001; vs CCISO are #P<0.05 and ##P<0.01.
(® ONE WAY ANOVA-F value 10.030; P<0.001 DMTT-P<0.05 for CC, ISO and CCISO vs Control).
(β ONE WAY ANOVA-F value 7.408; P=0.006 DMTT-P<0.05 for MG + CCISO vs CCISO).
Table 5 Effect of Makandi ghanavati and Makandi churna on blood pressure
Parameter NC CC ISO CCISO MG + CCISO MC + CCISO
Systolic BP
(mm of Hg)
127.00 ± 09.29 157.0 ± 04.69* 113.400 ± 11.59 130.667 ± 06.87 132.00 ± 06.25 148.75 ± 03.54
Diastolic BP
(mm of Hg)
83.000 ± 05.71 102.16 ± 04.54* 073.800 ± 06.95 093.667 ± 05.51 95.600 ± 04.55 110.250 ± 07.37
Mean blood
pressure
(mm of Hg)
101.167 ± 09.55 128.667 ± 04.08* 93.800 ± 08.89 112.333 ± 06.02 114.800 ± 04.15 128.500 ± 04.94
The data were expressed as Mean ± SEM.
Significant differences in each group vs the control is *P< 0.05.

JAGTAP et al.: EVALUATION OF CARDIOPROTECTIVE ACTIVITY OF MAKANDI FORMULATIONS
341
Fig.1 Photographs of ECG leads showing: a-normal ECG pattern of control (NC) group; b-slight elevation of ST segment in CC
group; c-elevation of ST segment in ISO group; d-marked elevation of ST segment in CCISO group; e-slight elevation of ST segment in
MG treated group; f-elevation of ST segment in MC treated group

INDIAN J NAT PROD RESOUR, SEPTEMBER 2011
342
pathological features were found further increased
involving vast area of the myocardium (Plate 2d).
This shows injection of ISO to hyperlipidemic
diet given rats further enhances myocardial injury.
Administration of MG moderately stemmed these
CCISO combination induced myocardiopathy
(Plate 2e). MC provided marked protection against
CCISO induced myocardiopathy (Plate 2f). Thus,
Plate 2 Photomicrographs of heart sections (1× 400 magnification): a-control group (NC) showing normal cytoarchitecture; b-CC
group showing mild fatty changes and myocarditis; c-ISO group showing multiple focal necrosis with infiltration of leukocytes (arrow);
d-CCISO group showing multiple focal necrosis with infiltration of leukocytes (arrow) and proliferating fibroblasts; e-MG treated group
showing very less degree of focal necrosis and infiltration of leukocytes; f-MC treated group showing almost normal cytoarchitecture.

JAGTAP et al.: EVALUATION OF CARDIOPROTECTIVE ACTIVITY OF MAKANDI FORMULATIONS
343
Makandi in the form of Churna may be of therapeutic
and prophylactic value in the treatment of myocardial
infarction.
Myocardial infarction is the rapid development of
myocardial necrosis caused by critical imbalance
between the oxygen supply and the demand of the
myocardium. A better understanding of the processes
involved in myocardial infarction has stimulated the
search for new drugs which could limit the
myocardial injury30
. The major abnormalities noticed
in myocardial infarction are lipidaemia, peroxidation
and loss of plasma membrane integrity31
. Further,
studies indicate that South Asians have elevated levels
of LDL cholesterol and triglycerides, while also
suffering from a deficiency in HDL cholesterol32,33
.
The mechanism by which hyperlipidaemia may
influence the severity of myocardial ischaemia is not
exactly known, however, accumulation and
redistribution of tissue/membrane cholesterol and the
resulting changes in sarcolemmal and mitochondrial
membrane micro-viscosity rather than the direct effect
of high serum lipoprotein levels and coronary
atherosclerosis may account for this34
. A decrease in
cardiac NO bioavailability35
and ecto-5'-nucleotidase
activity, an inhibition of the mevalonate pathway36
,
as well as enhanced apoptotic cell death have been
also shown to contribute to increased
ischaemia/reperfusion injury and loss of
preconditioning in hyperlipidaemic animal models37
.
Conclusion
Based on activity profile obtained, it can be
concluded that both the formulations of Makandi have
good anti-atherogenic potential and the Churna
formulation has remarkable cardioprotective activity,
while Ghanavati has weak cardioprotective activity. It
is more interesting to note the observed differences in
the activity profiles of the formulations, despite the
fact that both possess the same active ingredient. The
HPLC analysis of these formulations showed
4.812 mg of forskolin in 1 g of Makandi ghanavati
and 3.51 mg of forskolin in 1 g of Makandi churna.
As already stated forskolin is responsible for many
pharmacological actions related to cardio vascular
system. It was hypothesized that the forskolin present
in these two formulations may be responsible for the
anti-atherogenic and cardioprotective effects.
However, the results obtained did not correlate with
the forskolin content. Makandi churna with lower
forskolin content showed better cardioprotective
activity in comparison to Makandi ghanavati which
had higher forskolin content. This indicates that other
constituents may also play a major role. Elucidation
of the full chemical profile may throw light on the
nature of other constituents.
Acknowledgement
Authors are thankful to Prof. M.S. Baghel,
Director, IPGT & RA, Gujarat Ayurved University,
Jamnagar for the constant encouragement and for
providing facilities to carry out this study.
References 1 Bhushnam, Lala Shaligramji Vaishya Virachita Shaligram
nighantu, Khemaraj Shrikrushnadasa Prakashana, Mumbai,
Parishishta Bhaga, Sanskaran, 1993, p. 931.
2 Nighantu Ratnakara, A compendium of system of Hindu
medicine, edited by Bhishagvarya Late Krishna Shastri R.
Navre collated with spacious notes by Vasudev Laxman
Shastri Pansikar & Krishnaji Vitthal Soman, Part I,
Gunadosha Prakarana, 1993, p. 152.
3 Metzer H and Linder E, FORSKOLIN: Its chemical,
biological and medical potential, IRCH Med Sci, 1981, 9, 99.
Table-6 Effect of Makandi ghanavati and Makandi churna on cardiac output
Parameter NC CC ISO CCISO MG + CCISO MC + CCISO
Cardiac output
(ml/min)
20.90 ± 03.40 10.10 ± 01.40* 11.60 ± 04.90 09.70 ± 03.50* 07.60 ± 02.30 23.20 ± 08.10
LCW
(Kg.min/m2)
0.0269 ± 0.0074 0.0162 ± 0.0024 0.0115 ± 0.0052 0.0141 ± 0.0057 0.0108 ± 0.0033 0.0371 ± 0.0134
LVET (sec.) 0.160 ± 0.0202 0.161 ± 0.0163 0.202 ± 0.0116 0.198 ± 0.0359 0.161 ± 0.0201 0.211 ± 0.0197
PEP (sec.) 0.310 ± 0.0452 0.263 ± 0.0242 0.319 ± 0.0658 0.315 ± 0.0436 0.0436 ± 0.0425 0.294 ± 0.0587
Stroke index 4.366 ± 1.052 2.327 ± 0.308 2.913 ± 1.050 3.168 ± 1.072 1.954 ± 0.703 6.021 ± 1.954
The data were expressed as Mean ± SEM. Significant differences in each group vs. the control is *P< 0.05.

INDIAN J NAT PROD RESOUR, SEPTEMBER 2011
344
4 Seamon KB and Daly JW, Activation of adenylate cyclase by
the diterpene Forskolin does not require the guanine
nucleotide regulatory protein, J Biol Chem, 1981, 256,
9799-9801,
5 Ammon HP and Muller AB, Forskolin: From an Ayurvedic
remedy to modern agent, Plant Med, 1985, 51 (6), 473-477.
6 Badmaev V, Majeed M, Conte AA and Parker JE, Diterpene
Forskolin (Coleus forskohlii Benth): A possible new
compound for reduction of body weight by increasing lean
body mass, Nutra COS, 2002, 1 (2), 6-7.
7 Jensen G, Nyboe J, Appleyard M and Schnohr P, Risk
factors for acute myocardial infarction in Copenhagen, II:
Smoking, alcohol intake, physical activity, obesity, oral
contraception, diabetes, lipids, and blood pressure, Eur Heart
J, 1991, 12 (3), 298-308.
8 Sharangadhara, Sharangadhara Samhita, commentaries by
Aadhamalla ‘Dipika’ and Kashiram ‘Gudartha- Dipika’, 6th
Edn, Choukhambha Orientalia, Varanasi, Prathama Khanda,
2005, Chapter 2/1.
9 The Indian Pharmacopoeia, Vol I, 3rd Edn, The Controller of
Publication, Delhi, 1985, p. 501.
10 Madhavi Jagtap, A survey of hypertension in geriatric
population and its management with Makandi (Coleus
forskohlii Wild., MD (Ayu.) Thesis, Gujarat Ayurved
University, Jamnagar, 2010.
11 Paget GE and Barnes JM, Evaluation of drug activities, In:
Pharmacometrics, Vol. I, by DR Lawrence and AL
Bacharach (Eds), Academic Press, New York, 1969, p. 161.
12 Sangram Mishra, Fundamental and applied study of Snigdha
and Ruksha gunas with special reference to Rasa Raktagata
Sneha (Hyperlipidaemia), Ph D (Ayu.) Thesis, Gujarat
Ayurved University, Jamnagar, 2008.
13 Manjiri Nadkarni, Clinico experimental study of
hyperlipidaemia and its management with Mustadi
ghanavati, MD (Ayu.) Thesis, Gujarat Ayurved University,
Jamnagar, 2009.
14 Rona G, Chappel CI and BaLaza T, An infarct like
myocardial lesion and other toxic manifestations produced
by isoproterenol in the rat, Arch Path, 1959, 67, 443-455.
15 Roschlau P, Bernt E and Gruber W, Enzymatishe
Bestimmung des Cesamt-Cholesterins in Serum, Z Clin
Chem Clin Biochem, 1974, 12, 226.
16 Nauk M, Wiebe D and Warnick G, Measurement of High-
Density-Lipoprotein Cholesterol, In: Handbook of
Lipoprotein testing, 2nd Edn, by N Rifai, GR Warnick and
MH Dominiczak (Eds), AACC Press, Washington, 2000,
pp. 161-187.
17 McGowan MW, Artiss JD, Strandbergh DR and Zak B, A
peroxidase coupled method for the colorimetric
determination of serum triglycerides, Clin Chem, 1983, 29,
538-542.
18 Bowers GN and McComb RB, A continuous
spectrophotometric method for measuring the activity of
serum alkaline phosphatase activity, Clin Chem, 1966, 12,
70.
19 Clinical guide to laboratory tests, by NW Tietz (Ed), 3rd Edn,
Philadelphia PA: WB Saunders, 1995, p. 76.
20 Tietz textbook of Clinical Chemistry, by CA Burtis and ER
Ashwood (Eds), 3rd Edn, Philadelphia, 1999, p. 652.
21 Friedewald WT, Levy RI and Fredrickson DS, Estimation of
the concentration of low density lipoprotein cholesterol in
plasma, without the use of preparative centrifuge, Clin Chem,
1972, 18, 499-502.
22 Balogun EA and Adebayo JO, Effect of ethanolic extract of
Daniella Oliveri leaves on some cardiovascular indices in
rats, Pharmacogn Mag, 2007, pp. 16-20.
23 A Manual of Laboratory Techniques, by N Raghuramulu,
KM Nair and S Kalyanasundaram (Eds), National Institute of
Nutrition (NIN), Hyderabad, 1983, pp. 246-253.
24 Nirmala C and Puvanakrishnan R, Effect of curcumin on
certain lysosomal hydrolases in isoproterenol induced
myocardial infarction in rats, Biochem Pharmacol, 1996, 51,
47-51.
25 Roberts WC, Preventing and arresting coronary
atherosclerosis, Am Heart J, 1995, 130, 580-600.
26 Rader Daniel J, Novel approaches to the treatment of
dyslipidemia, Arterioscler Thromb Vasc Biol, 2005, 25,
480-481.
27 Kela AK, Reddy LP and Thrombe DP, ECG findings in
normal rats and after administration of isoproterenol, Indian
J Physiol Pharmacol, 1980, 24, 84-90.
28 Mazzoleni A, Curtin ME, Wolff R, Reiner L and Somes G,
On the relationship between heart weights, fibrosis, and QRS
duration, J Electrocardiol, 1975, 8, 233-236.
29 Oikarinen L, Nieminen MS, Viitasalo M, Toivonen L, Jern S,
Dahlof B, Devereux RB and Okin PM, Life study
investigators: QRS duration and QT interval predict
mortality in hypertensive patients with left ventricular
hypertrophy: Losartan intervention for endpoint reduction in
hypertension study, Hypertension, 2004, 43, 1029-1034.
30 Whellan DJ, Heart failure disease management:
Implementation and outcomes, Cardiol Rev, 2005, 13,
231-239.
31 Krishnamoorthy Gayathri, Shabi Mohamed M, Ravindhran
Dhevi, Uthrapathy Subasini, Rajamanickam Victor G and
Dubey Govindha P, Nardostachys jatamansi:
cardioprotective and hypolipidemic herb, J Pharm Res, 2009,
2(4), 574-578.
32 Reddy KS, Cardiovascular diseases in India, WHO Stat Q,
1993, 46, 101-107.
33 Walsh B, Asia's War with Heart Disease. In: Time,
November 22, 2004, 164 (21).
34 Hexeberg S, Willumsen N, Rotevatn S, Hexeberg E and
Berge RK, Cholesterol induced lipid accumulation in
myocardial cells of rats, Cardiovasc Res, 1993, 27, 442-446.
35 Hoshida S, Yamashita N, Igarashi J, Nishida M, Hori M,
Kuzuya T and Tada M, A nitric oxide donor reverses
myocardial injury in rabbits with acute hypercholesterolemia,
J Pharmacol Exp Ther, 1996, 278, 741-746.
36 Wang TD, Chen WJ, Mau TJ, Lin JW, Lin WW and Lee YT,
Attenuation of increased myocardial ischemia-reperfusion
injury conferred by hypercholesterolemia through
pharmacological inhibition in the caspase-1 cascade, Br J
Pharmacol, 2002, 138, 291-300.
37 Peter Ferdinandy, Myocardial ischaemia/reperfusion
injury and preconditioning: effects of
hypercholesterolaemia/hyperlipidaemia, Br J Pharmacol,
2003, 138, 283-285.


















