
A Cognitive-Behavioral Approach To Temporomandibular
5
A Cognitive-Behavioral Approach To Temporomandibular Dysfunction Treatment Failures: A Controlled Comparison Mark E. Oakley, PhD Research Associate Department of Psychiatry and BiobehavJorsI Sciences School of Medicine Charles P, McCreaty. PhD Professor Department of Psychiatry and BiobehavJorsI Sciences School of Medicine Glenn T, Clark, DDS, MS Professor School of Dentistry Steve Holston, PhD Research Associate Department of Psychiatry and Biobehaviorai Sciences School of Medicine Dorothy Glover, MA Research Associate Department of Psychology Kathleen Kashima, PhD Research Associate Department of Psychiatry and Biobehaviorai Sciences School of Medicine University of California, Los Angeles Los Angeles, California Correspondence to: Dr Charles McCreary UCLA Dentsf Research Institute, 73-017 Center For The Health Sciences 10833 Le Conte Avenue Los Angeles, California 90024-1762 The effects of cagnitive-bebavtoral treatment for patients with tem- poromandibular disorders were studied by comparing active treat- ment to a watt-list control condition. Patients were predominantly women and had been referred to the study after havÍ7ig poor response to dental/physical medicine care. Patients' conditions were evaluated pretreatment and posttreatment based on self-report measures of pain, distress, and ¡aw function problems. They were examined by a dentist who assessed pain-free opening, muscle pal- pation pain, and tenderness of the temporomandibular joints. The 5-week cognitive-behavioral treatment included relaxation training, self-monitoring of Stressors, and cognitive coping strategies. Treatment had its greatest impact on improving mood, especially anxiety; however, there were some effects on the patients' experi- ences of pain. J OROFACiAL PAUS 1994;8:397^01, T emporomandibular disorders (TMD) involve a number of clinicai problems ofthe masticatory musculature and/or temporomandibuiar joint. Common symptoms are pain on palpation of tbe masticatory muscles, earache, headache, and/or facial pain. Patients with these disorders often complain of limited jaw movement and sometimes of joint sounds, described as click- ing, popping, grating, or crepitus. The disorder is common; conser- vative estimates suggest that 5% of the population has relatively chronic TMD.'- The most accepted first line of treatment ti'pically involves a den- tal/physical medicine approach that includes occlusal appliance therapy, physical tberapy, and anti-inflammatory medications. While this approach appears to be successful with the majority of TMD patients, a sizahle percentage (23%) do not respond,^ Therefore, it appears that another form of treatment is needed for these nonresponders. There is evidence suggesting that relaxation training and biofeedback may be useful approaches for certain TMD problems.''' Gale and Funch'° reported on a comparison between electromyograpbic (EMG) biofeedhack and relaxation training for TMD patients wbo had failed a variety of previous dental/physical medicine treatments. The results of their study showed that both methods are effective at teducmg pain but nei- ther is superior to the orher. Dahlstrom and Garlsson^" have com- pared EMG hiofeedback to occlusal appliance therapy and have shown that both treatments produce similar outcomes. Although relaxation and hiofeedback approaches appear to be useful in tbe treatment of TMD, the conspicuous lack of wait-list control groups in previous research leaves open, the possibility that these patients may have improved without treatment, A wait-list Joumal of Orofacial Pain 397
Transcript of A Cognitive-Behavioral Approach To Temporomandibular

A Cognitive-Behavioral Approach To TemporomandibularDysfunction Treatment Failures: A Controlled Comparison
Mark E. Oakley, PhDResearch AssociateDepartment of Psychiatry and
BiobehavJorsI SciencesSchool of Medicine
Charles P, McCreaty. PhDProfessorDepartment of Psychiatry and
BiobehavJorsI SciencesSchool of Medicine
Glenn T, Clark, DDS, MSProfessorSchool of Dentistry
Steve Holston, PhDResearch AssociateDepartment of Psychiatry and
Biobehaviorai SciencesSchool of Medicine
Dorothy Glover, MAResearch AssociateDepartment of Psychology
Kathleen Kashima, PhDResearch AssociateDepartment of Psychiatry and
Biobehaviorai SciencesSchool of Medicine
University of California, Los AngelesLos Angeles, California
Correspondence to:Dr Charles McCrearyUCLA Dentsf Research Institute, 73-017Center For The Health Sciences10833 Le Conte AvenueLos Angeles, California 90024-1762
The effects of cagnitive-bebavtoral treatment for patients with tem-poromandibular disorders were studied by comparing active treat-ment to a watt-list control condition. Patients were predominantlywomen and had been referred to the study after havÍ7ig poorresponse to dental/physical medicine care. Patients' conditions wereevaluated pretreatment and posttreatment based on self-reportmeasures of pain, distress, and ¡aw function problems. They wereexamined by a dentist who assessed pain-free opening, muscle pal-pation pain, and tenderness of the temporomandibular joints. The5-week cognitive-behavioral treatment included relaxation training,self-monitoring of Stressors, and cognitive coping strategies.Treatment had its greatest impact on improving mood, especiallyanxiety; however, there were some effects on the patients' experi-ences of pain.J OROFACiAL PAUS 1994;8:397^01,
Temporomandibular disorders (TMD) involve a number ofclinicai problems ofthe masticatory musculature and/ortemporomandibuiar joint. Common symptoms are pain on
palpation of tbe masticatory muscles, earache, headache, and/orfacial pain. Patients with these disorders often complain of limitedjaw movement and sometimes of joint sounds, described as click-ing, popping, grating, or crepitus. The disorder is common; conser-vative estimates suggest that 5% of the population has relativelychronic TMD.'-
The most accepted first line of treatment ti'pically involves a den-tal/physical medicine approach that includes occlusal appliancetherapy, physical tberapy, and anti-inflammatory medications.While this approach appears to be successful with the majority ofTMD patients, a sizahle percentage (23%) do not respond,^Therefore, it appears that another form of treatment is needed forthese nonresponders. There is evidence suggesting that relaxationtraining and biofeedback may be useful approaches for certainTMD problems.''' Gale and Funch'° reported on a comparisonbetween electromyograpbic (EMG) biofeedhack and relaxationtraining for TMD patients wbo had failed a variety of previousdental/physical medicine treatments. The results of their studyshowed that both methods are effective at teducmg pain but nei-ther is superior to the orher. Dahlstrom and Garlsson^" have com-pared EMG hiofeedback to occlusal appliance therapy and haveshown that both treatments produce similar outcomes.
Although relaxation and hiofeedback approaches appear to beuseful in tbe treatment of TMD, the conspicuous lack of wait-listcontrol groups in previous research leaves open, the possibility thatthese patients may have improved without treatment, A wait-list
Joumal of Orofacial Pain 397
Oakley
control is especially important for an evaluation ofTMD treatment because TMD is an intermittentproblem that can remit spontaneously.'-Furthermore, several other issues have not yet beenadequately explored. Stress-management proce-dures (including relaxation training, time manage-ment, and cognitive therapy) without biofeedbackhave not been adequately investigated with TMDpatients." This approach has potential advantagesover biofeedback because it does not requirelnstrumentarion and can be administered in agroup format. The current study uses a wair-lisrcontrol group to exatnine the effectiveness of cog-nitive-behavioral, stress-management group treat-ment on TMD patients who had recently failed adental/physical medicine treatment approach.
Materials and Methods
Temporomandibuiar disorder patients were selectedaccording to inclusion criteria that involved aware-ness of jaw region pain or subsrantial jaw dysfunc-tion and the presence of an acrive TMD on clinicalexamination. An active TMD was defined by thepresence of one or more of the following signs: tem-poromandibuiar joint (TMJ) noises, recent onset oflimited jaw opening, and pain in the masticatorysystem replicated by palpation of the TMJ or themasticatory muscles. Exclusion criteria involvedthe presence of sinus problems, dental infection, ora current or recurrent ear disorder. The selectedTMD patients who reported less than 50%improvement following a dental/physical medicinecourse of treatment (occlusal appliance therapy,physical therapy, and anti-inflammatory medica-tions) were recommended to enroll in a 6-weekcognitive-behavioral, stress-management/pain-controi class. Of those treatment failures recom-mended to the class, 83 agreed to enroll. An exclu-sion criterion for data analyses was that patientscould not receive additional concurrent treatmentoutside the study conditions. Nme patients wereexcluded from final analyses because they receivedconcomitant treatment during the study. Theauthors helieved this criterion to be a méthodolog-ie strength of the present study because theabsence of concurrent treatment has typically beenassunied but not directly assessed m previousresearch.
In addition to the 9 patients who received con-comitant treatment, 18 patients who did not com-plete the pain class treatment (defined as atten-dance at fewer than 80% of the scheduledsessions) were excluded from analyses. Therefore,
56 patients completed the pain class without con-comitant treatment. Twenty-four of the patientswho completed treatment also served as wait-listcontrol subjects. There was a fee for treatment:discounts were given to patients who agreed toenroll in the wait-list condition, and smaller dis-counts were given to those who participated in thepretreatment and posttreatment assessments.
Study patients were predominantly female(85%) and white (85%). The mean age was 35years. Patients were relatively well educated (44%college graduates). Most were employed eitherfull-time (57%) or part-time (11%) outside thehome. Others were homemakers (15%), retired(7%), or students (7%). Most patients were mar-ried (54%) or single (35%). Some (11%) weredivorced, separated, or widowed. The mean dura-tion of TMD symptoms was 51 months.
Ali patients completed a comprehensive pre-treatment psychosocial evaluation that includedSpielberger's" State-Trait Anxiety Inventory(STAI), the Beck'- Depression Inventory (BDI), andthe McGill Pain Questionnaire (MPQ). The STAIcontains two subtests of 20 items each assessingstate or trait anxiety. The BDI is a 21-item self-rating of depression.'* The MPQ has patientsdescribe their pain by selecting adjective descrip-tors from 20 categories; three scores are obtainedby adding scale values for the sensory, affective,and evaluative categories.
Visual analog scale (VAS) ratings of averagepain during the last week and of pain experiencedduring testing were obtained by asking eachpatient to place a mark on a 100-mm horizontalline that had anchor points on the left for no painand on the right for the most intense pain imagin-able. Ratings of jaw^ function problems wereobtained by asking patients to indicate their diffi-culties in using their jaws (chewing, talking, etc)on an 11-point scale from 0 (no problem) to 10(extensive problems). Pretreatment and posttreat-ment dental exams were done by a dentist whowas not aware of the experimental condition. Thedentist measured pain-free mouth opening, musclepalpation pain, and tendernes.s of the TMJs.
Because recruiting subjects for the study tookseveral months, all subjects were assigned to thefirst two pain classes. After the first nine patients(two groups) went directly into the treatment con-dition, the remaining 47 patients were randomlyassigned to a 6-week wait-hst condition. Twenty-six of the 47 patients agreed to he wait-list sub-jects, and they underwent identical psychosocialassessment and dental evaluation procedures with-out intervening treatment within or outside the
398 Volume 8, Number 4, 1994
Oakley
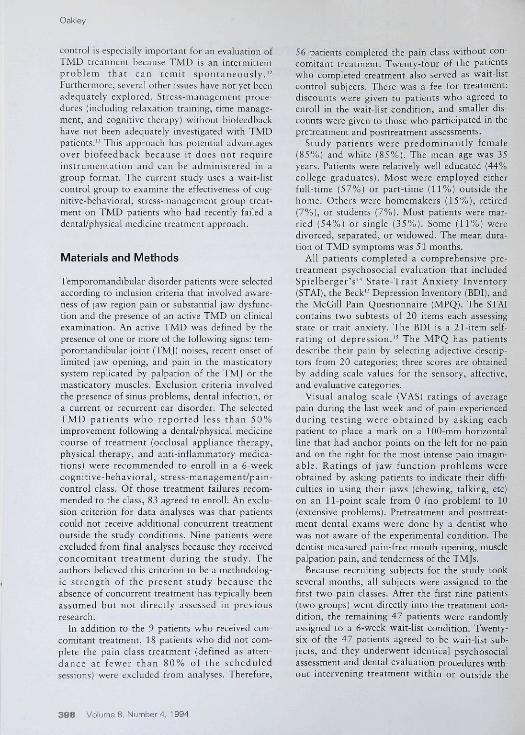
Table 1 Repeated-Measures ANOVA for Wait-List and Pain-Class Subjects
Variable
BDI
STAI stateSTAI trailPain at test limePain last weekMPQ sensoryMPQ affectiveMPQ evaluatiueJaw problemPain-free opening
Wait-list
Pre
9.061.871.620 927 4
7 71.61.41.9
44 B
Post
8.863.067.524.325 2
6 5
1 81.12.1
47.1
Pre
9 869 770 033 340.3
9.42.1
1.53.2
42.5
Post
6.050.356.532.631.3
7.5
2.01.02.5
44 5
(A)
0 290.110.632 802 600 800 560 051.081.02
F tests
Repeat(Bl
9.59"7 8 2 "
0 06
3.640.015.33*1.473 5?
AxB
0 100 472.660.02
-P< .01— P< 001BDt = Beck Depressiori Inuentory.STAI ^ State-Trait Arniety InventoryWPQ ^ McGill Pain Questionnaire.Pre = pietieatmeni. Post = posttreatn
Study. Twenty-four of tbe 26 wait-list patients sub-sequently completed tbe treatment condition withno other concurrent treatment.
The pain class consisted of five 1.5-hour weeklysessiotis and was conducted uith groups averaging threepatients. The class emphasized a broad-spectrumapproach to stress management that involved self-monitoring pain/stress to increase awareness, pro-gressive muscle relaxation training, imagery, cue-controlled rapid relaxation, cognitive therapy,self-hypnosis, and time management. All patientswere given a series of three tapes on gtiided-relaxationand self-hypnotic procedures for home use as well asa manual that covered the content of class material.
During tbe sixth week of the pain-control class,patients were given a 20-minute explanation ofmaintenance issues targeting relapse preventionand what to do in the event of a relapse. Followingthis discussion, all patients completed a posttreat-ment evaluation that was similar to the pretreat-ment evaluation package.
Results
The results were first analyzed using a repeated-measures analysis of variance. Table 1 presents tbepretreatment and posrtreatment scores and f testsof patients assigned either to the wait-list or pain-class condition. Although tbere were no significantdifferences between tbe groups on tbe pretreat-
ment measures, tbere was a trend for the wait-hstpatients to have lower scores on pain and syrnp-tom scores m the direction of less severe difficul-ties. The significant interactions for depression,state, and trait anxiety reflected-Lmproi Êment aftertreatment on these factors in the pain-class condi-tion. On the MPQ evaluative score, there was asignificant pretreatment-posttreatment differenceacross groups.
Because of the trend toward differences amongpatients assigned to the wait-list condition, t testswere done on these patients before and after theireventual participation in the pain-class treatment.Tbese results are summarized in Table 2. Similarto the pattern found above, there was a significantdrop in state and trait aiEíiety following treatment.The reduction in depression did not reach signifi-cance. These previously wait-listed patientsshowed a significant lowering of their ratings ofpain over the past week even though their pretreat-ment levels were not very high.
Table 2 also lists the correlations between tbepretreatment and posttreatment pain-class seoresof tbe patients who had been on tbe wait list. Thecorrelations for mood levels, symptoms, and aver-age pain for the prior week were quite high whilethe correlations between current pain scores werelow. This same pattern appeared for the pain-classonly patients. It was similar for the wait-listpatients during the wait-list period, except the val-ues were generally higher. Current pain valuesseem to be less stable tban the other factors.
Joumal of Orotacial Pain 399

Oakley
Table 2 Pretreatmenr and Posttreatment Datafor Pain-Class Pai:ients Who Were Wajt-ListedPnor to Treatment
Variable
BDISTAI stateSTAI trait
Pain at test timePain last week
MPQ sensoryMPQ affectiveMPQ evaluativeJaw problem
Pam-free open m
*P Í ,05"Pi,01*"P<,001BDI = Beck DepreSTAI = State-TraitMPQ = t^cGill Pail
Pretreatment
Mean
8,7062 20
67 6053 7026,10
6,601,801 102,10
g 47,30
ssion InventoAnïiety Invenn Question nal
SE
0,91
5 203,804,803,501 400,820,21
0,391 40
ry.itory.re.
Ptisttreatment
Meati
6 849 057 419215,45,91,20 81 6
49 4
r
85678402
,70,14,14,446576
t
2,082,56*2,70"0,953,08"0,480,831,451,21
-1,55
Discussion
The results of this study provide evidence for theeffectiveness of a cognitive-behavioral treatment forTMD pain. These results are particularly notewor-thy since the patients selected for treatment werethose who reported less than 50% improvementfrom a dental/physical medicine treatment protocol.Therefore, the cognitive-behavioral treatment wastested with a recalcitrant population. This study isalso the first to employ a wait-list comparison inevaluating a cognitive-behavioral approach to treat-ing TMD. A waic-list control is especially importantfor an evaluation of TMD treatment because TMDis an intermittent problem that can remit sponta-neonsly." In the present study, random assignmentwas difficult to achieve. The trend toward lesssevere pain in the wait-list patients seems to reflectthat patients who accepted random assignment lothe wait-list condition were more willmg to post-pone seeking another active intervention.
Current results indicate that the cognitive-behavioral treatment had its greatest impact onmood, especially anxiety. Although there weresome reductions in current pain levels and a ttendtoward improvement in symptoms, these changesdid not appear to be specifically related to thetreatment. The reduction of mouth opening limita-tions and the decrease iti MPQ evaluative scoresseemed to be related to the passage of time. Whenthe pain level did seem to be reduced, it took theform of lower ratings of the prior week's pain.
This could be explained as a shift in the personalimportance of the pain rather than the currentlevel of actual nociception. Overall, the resultsindicate that the treatment condition producedimprovements in the patient's mood and percep-tion of pain, reflecting a hetter quality of life.Fordyce" has made the distinction between suffer-ing, defined as the negative emotional states thatoccur in response to or in anticipation of nocicep-tion, and pain, defined as perceived nociception.The cognitive-hehavioral treatment appears tohave affected suffering rather than pain. This treat-ment approach has advantages over biofeedbackbecause it can be administered to groups and ohvi-ously does not require instrumentation.
Future research will explore whether the notedimprovements persist over extended time periods.One- to two-year follow-up data are being collectedon the pain-class patients. Follow-up should showwhether other quality-of-life variables, such asimpact of the problem on the person's work orsocial life, change over time.
Finally, the results of this study highlight animportant contribution to cognitive-behavioraltreatment for patients who fail to significantlyimprove with conventional dental/physicalmedicine approaches. Although patients did notreport significant improvements in their pain rat-ings at a specific moment, they still reported signif-icant improvements in their "suffering,"Therefore, improvements were made in the qualityof life in spite of the continued experience of pain.It is recommended that further research be con-ducted with other types of pain patients using thiscurrent methodology.
Acknowledgment
Tbis rescarcb was supported by grant DEO7él8 from tbeNational Institute ot Dental Research, Bethesda, Maryland.
References
1, Hclkimo M, lipidtmiologica! surveys of dysfunction of themasticacory system. Oral Sei Rev l976;7:54-69,
2, Solberg WK. Epidemiology, incidence, and prevalence oftemporotnandibular disorders: A review. In: Laskin DM,Greenfield W, Gale EN, et al (eds}. The President'sConference on tbe Examinarion, Diagnosis, andManagement of Temporomandibular Disorders. Chicago;American Dental Association, 1982:30-39,
3, Clark GT, Lanham F, Flack VF, Treatment: outcomeresults for consecutive TMJ patients, J CraniomandibDiqord Facial Oral Pain I988;Z:87-9S,
400 Volume 8, Number 4, 1994

Oakley
4. Greene CS, Laskin DM. Long-term evaluation of treat-ment for myofastial pa in-dysfunction syndrome: A com-paranve analysis. J Am Dent Assoc 198j;iO7:235-238.
5. Moss RA, Wedding D, Sanders SH. The comparative effi-cacy of relaxation training and masseter EMG feedback inthe rrearment of TMJ dysfunciion. J Oral Rehabil1983ilO:9-17.
6. Dohrmann RJ, Laskin DM. An evaluation of electromyo.graphic biofeedback in the trearment of myofascial pain-dysfunction syndrome. J Am Dent Assoc 197S;96-656-662.
7. Gale EN. Biofeedback for TMJ Pain. In: Ingersoll BD,McCutcheon WD (eds). Clinical Research in BehavioralDentistry. Morgantown, WV: West Virginia University,1979:83-93.
8. Gessel AH, Alderman MM. Management of myofascialpain dysfunction syndrome of the temporomandibularjoint by tension control t raining. Psychosom1971;12:302-309.
9. Dahlstrom L, Carlsson SGP. Comparison of effects ofelectromyographic biofeedback and occlusal splint therapyon mandibular dysfunction. Scand J Dent Res1982;92:151-156,
10. Gale EN, Funch DP. Factors associated with successfuloutcome from behavioral therapy for chronic temporo-matidibulat ioint (TMJ) pain. J Psychosom Res1984;2S:44H48,
11. Dahlsirom L, Carlsson SG. Treatment of mandibular dys-function: The clinical usefulness of biofeedback in relationto splint therapy. J Oral Rehabil 1984^1 1 Í 2 7 7 - 2 8 4 .
12. Rugh JD. Psychological factors in the etiology of mastica-tory pain and dysfunction. Ini Laskin DM, Greenfield W,Gale EN, et al (eds¡. The President's Conference on theExamination., Diagnosis, and Management ofTemporomandibular Disorders. Chicago: AmericanDental Association, 1982:85-94.
13. Gale EN. Behavioral approaches to temporomandibulardisorders. Ann Behav Med 1986;8(4):11-16.
14. Spielberger C, Corsuch R, Tushene R. State-Trait AnxieiyInventory Manual. Palo Alto, CA: Consulting PsychologyPress, 1970.
15. Beck A. Depression: Clinical, Experimental, andTheoretical Aspects. New York: Harper and Row, 1967.
16. Fordyce WE. Pain and Suffering, a reappraisal. AmPsychol 198S;43:276-283.
Resumen
Comportamiento cognoscitivo para el tratamiento decasos de disfunción temporomandibulsr que han fracasa,do: Comparación controlada
Se estudiaron los efectos del tratamiento basado en el compor-tamiento cognoscitivo de pacientes con desórdenes tempciro-mandibulafes. comparando el tratamiento activo a otro de con-trol en lista de espera. La mayoría de los pacientes fueronmujeres que había sido remitidas al estudio después de iiabertenido una respuesta pobre al cuidado dentai/médico-fisrco. Seevaluaron las condiciones de los pacientes antes y después deitratamiento, basados en los auloreportes de doior. afiícción, yproblemas de función mandibular. Los pacientes fueron exami.nados por un odontólogo quien evaluó ia apertura iibre de dolor,el doior a la palpación muscular, y la sensibilidad de ias articula-ciones temporomandibulares. El tratamiento de comportamientocognoscitivo duró 5 semanas e incluyó instnjcoión de relajación,auto-monitoreo del estrés, y el uso de estrategias de manejocognoscitivo. El tratamiento tuvo su mayor impacto ai mejorar elánimo de los pacientes especialmente en lo reiativo a laansiedad; sin embargo, se presentaron algunos efectos sobrelas experiencias de dolor de ios pacientes.
Zusammenfassung
Kognitiv-behaviorsle Therapie bei Myoarthropathie-Patienten nicht ansprechbar auf koventionelle Therapie:Eine Kontrollstudre
Die Auswirkungen einer kognitiv-beiiavicrale Tiierapfe beiPatienten mit Myoarthropathien wurden untersucht. AisKontroligruppe wurden Patienten einer Wartelisle genommenDie Patienten waren verwiegend Frauen und wurden der Studiezugewiesen, nachdem eine zahrärztiich/physiotherapeutischeBehandlung einen schiechten Behandlungserfoig erbrachte. Vorund nach der Behandlung wurde der Zustand der Patienten auf-grund von Seibstreporlen über Schmerz, Distress undKieferfunktionsprobiemer ermitteit. Sie wurden durch einenZahnarzt untersucht, welcher der Grad der schmerzfreienMundöffnung sowie die Muskel und Kiefergelenifdrucii-schmerzhaftigkeit untersuchte. Die fünf Wochen dauemde i<og-nitiv.be h avio rale Behandiung beinhaitete Entspannungsübungen.Selbsterkennung vor Stressoren und Erlernen vonBewalligungsstrategien. Das Haupresuitat lag in einerStimmungsverbessemng, insbesondere bezüglich Angst, EinigeAuswirkungen auf die Schmerzcrfahnjng der Patienten wurdenauch festgestelit.
Journal of Orofacial Pain 4 0 1

















![Behavioral/Systems/Cognitive ... · Behavioral/Systems/Cognitive AcuteCocaineInducesFastActivationofD1Receptorand ProgressiveDeactivationofD2ReceptorStriatalNeurons: InVivoOpticalMicroprobe[Ca2]](https://static.fdocuments.us/doc/165x107/6013f75e26e57852b94803cb/behavioralsystemscognitive-behavioralsystemscognitive-acutecocaineinducesfastactivationofd1receptorand.jpg)
