A 51-year-old woman with shortness of breath and edema
7
A 51-Year-Old Woman With Shortness of Breath and Edema SONALI DESAI, 1 JESSICA CLEMENT, 2 AND STEPHEN LANDAW 2 CASE PRESENTATION A 51-year-old woman was in her usual state of good health until she presented to a local emergency department re- porting dyspnea of 2 days’ duration. Her dyspnea was worse with exertion and with lying flat, but was not asso- ciated with chest pain, cough, or fever. Bilateral lower extremity edema had developed over the few weeks pre- ceding her presentation. Two to three weeks prior to the emergency department visit, she noticed a blister on her left third toe. She was diagnosed with cellulitis and was started on cephalexin. After initiating antibiotic therapy, she developed a diffuse, pruritic, maculopapular rash, and her treatment was switched to doxycycline. The patient stopped taking doxy- cycline after 2 days because of nausea, and the blister resolved without further therapy. In the emergency department, the patient was hyperten- sive and tachycardic, with blood pressure (BP) of 210/110 mm Hg and a heart rate of 105 beats/minute. Her temper- ature was 98.2°F and her oxygen saturation was 100% on room air. Physical examination revealed bibasilar crackles, pitting edema of both lower extremities, and a dusky area on her left third toe. Her laboratory studies showed a hematocrit of 25.2%, blood urea nitrogen level of 90 mg/dl (normal range 6 –20), and serum creatinine level of 9.7 mg/dl (normal range 0.4 –1.1). A chest radiograph showed mild pulmonary vascular congestion with small bilateral pleural effusions. There were no pulmonary infiltrates or nodules. Her hyperten- sion was treated with metoprolol (5 mg intravenously) and her pulmonary edema was treated with furosemide (40 mg via intravenous push). However, she remained hyperten- sive and was transferred to our institution. Past medical history The patient had an unremarkable medical history. She denied any significant previous illnesses and had never undergone surgery. She had had 3 pregnancies and deliv- ered 3 healthy children. The patient denied recent fever, chest pain, jaw pain, diaphoresis, mental status changes, or asymmetric leg swelling. She also denied the use of nonsteroidal antiinflammatory drugs. Medications/allergies The patient was not taking any medications. She noted the cephalosporin skin reaction, but denied any other drug allergies. Social and family history The patient worked as a nurse, was married, and had 3 children ages 18, 21, and 24 years. She denied ever using tobacco and had never used illicit drugs. She rarely drank alcoholic beverages. Her father had died of pancreatic cancer at the age of 68 years, and her mother was still alive at age 74 years. Her family history was negative for any cardiac, renal, or hematologic disorders. Physical examination The initial examination upon transfer to our institution revealed a comfortable-appearing woman with a tempera- ture of 98.6°F and BP of 189/110 mm Hg. Her heart rate was 94 beats/minute, respiratory rate 14 breaths/minute, and she had an oxygen saturation of 98% on room air. She was again noted to have bilateral pitting edema in her lower extremities, but her bibasilar crackles had resolved. Her neurologic examination was unremarkable. Laboratory A complete blood cell count disclosed anemia and throm- bocytopenia (Table 1). The peripheral smear revealed 5 schistocytes/hpf; spherocytes were absent (Figure 1). Ad- ditional laboratory results showed lactate dehydrogenase of 1,146 IU/liter (normal range 94 –250), haptoglobin of 20 mg/dl (normal range 30 –200), and a platelet count of 85,000/l (normal range 150,000 – 440,000). A direct anti- globulin test was negative and her prothrombin and acti- vated partial thromboplastin times were normal. 1 Sonali Desai, MD: Brigham and Women’s Hospital, Bos- ton, Massachusetts; 2 Jessica Clement, MD, Stephen Landaw, MD, PhD, FACP: Beth Israel Deaconess Medical Center, Boston, Massachusetts. Drs. Desai and Clement contributed equally to this work. Address correspondence to Sonali Desai, MD, 75 Francis Street, PBB-B3, Boston, MA 02115. E-mail: sdesai5@ partners.org. Submitted for publication December 21, 2007; accepted in revised form April 10, 2008. Arthritis & Rheumatism (Arthritis Care & Research) Vol. 59, No. 8, August 15, 2008, pp 1184 –1190 DOI 10.1002/art.23934 © 2008, American College of Rheumatology CLINICOPATHOLOGIC CONFERENCE 1184
-
Upload
sonali-desai -
Category
Documents
-
view
215 -
download
0
Transcript of A 51-year-old woman with shortness of breath and edema

A 51-Year-Old Woman With Shortness ofBreath and EdemaSONALI DESAI,1 JESSICA CLEMENT,2 AND STEPHEN LANDAW2
CASE PRESENTATION
A 51-year-old woman was in her usual state of good healthuntil she presented to a local emergency department re-porting dyspnea of 2 days’ duration. Her dyspnea wasworse with exertion and with lying flat, but was not asso-ciated with chest pain, cough, or fever. Bilateral lowerextremity edema had developed over the few weeks pre-ceding her presentation.
Two to three weeks prior to the emergency departmentvisit, she noticed a blister on her left third toe. She wasdiagnosed with cellulitis and was started on cephalexin.After initiating antibiotic therapy, she developed a diffuse,pruritic, maculopapular rash, and her treatment wasswitched to doxycycline. The patient stopped taking doxy-cycline after 2 days because of nausea, and the blisterresolved without further therapy.
In the emergency department, the patient was hyperten-sive and tachycardic, with blood pressure (BP) of 210/110mm Hg and a heart rate of 105 beats/minute. Her temper-ature was 98.2°F and her oxygen saturation was 100% onroom air. Physical examination revealed bibasilar crackles,pitting edema of both lower extremities, and a dusky areaon her left third toe. Her laboratory studies showed ahematocrit of 25.2%, blood urea nitrogen level of 90 mg/dl(normal range 6–20), and serum creatinine level of 9.7mg/dl (normal range 0.4–1.1).
A chest radiograph showed mild pulmonary vascularcongestion with small bilateral pleural effusions. Therewere no pulmonary infiltrates or nodules. Her hyperten-sion was treated with metoprolol (5 mg intravenously) andher pulmonary edema was treated with furosemide (40 mgvia intravenous push). However, she remained hyperten-sive and was transferred to our institution.
Past medical historyThe patient had an unremarkable medical history. Shedenied any significant previous illnesses and had neverundergone surgery. She had had 3 pregnancies and deliv-ered 3 healthy children. The patient denied recent fever,chest pain, jaw pain, diaphoresis, mental status changes,or asymmetric leg swelling. She also denied the use ofnonsteroidal antiinflammatory drugs.
Medications/allergiesThe patient was not taking any medications. She noted thecephalosporin skin reaction, but denied any other drugallergies.
Social and family historyThe patient worked as a nurse, was married, and had 3children ages 18, 21, and 24 years. She denied ever usingtobacco and had never used illicit drugs. She rarely drankalcoholic beverages. Her father had died of pancreaticcancer at the age of 68 years, and her mother was still aliveat age 74 years. Her family history was negative for anycardiac, renal, or hematologic disorders.
Physical examinationThe initial examination upon transfer to our institutionrevealed a comfortable-appearing woman with a tempera-ture of 98.6°F and BP of 189/110 mm Hg. Her heart ratewas 94 beats/minute, respiratory rate 14 breaths/minute,and she had an oxygen saturation of 98% on room air. Shewas again noted to have bilateral pitting edema in herlower extremities, but her bibasilar crackles had resolved.Her neurologic examination was unremarkable.
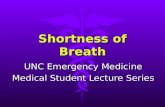
LaboratoryA complete blood cell count disclosed anemia and throm-bocytopenia (Table 1). The peripheral smear revealed �5schistocytes/hpf; spherocytes were absent (Figure 1). Ad-ditional laboratory results showed lactate dehydrogenaseof 1,146 IU/liter (normal range 94–250), haptoglobin of�20 mg/dl (normal range 30–200), and a platelet count of85,000/�l (normal range 150,000–440,000). A direct anti-globulin test was negative and her prothrombin and acti-vated partial thromboplastin times were normal.
1Sonali Desai, MD: Brigham and Women’s Hospital, Bos-ton, Massachusetts; 2Jessica Clement, MD, Stephen Landaw,MD, PhD, FACP: Beth Israel Deaconess Medical Center,Boston, Massachusetts.
Drs. Desai and Clement contributed equally to this work.Address correspondence to Sonali Desai, MD, 75 Francis
Street, PBB-B3, Boston, MA 02115. E-mail: [email protected].
Submitted for publication December 21, 2007; accepted inrevised form April 10, 2008.
Arthritis & Rheumatism (Arthritis Care & Research)Vol. 59, No. 8, August 15, 2008, pp 1184–1190DOI 10.1002/art.23934© 2008, American College of Rheumatology
CLINICOPATHOLOGIC CONFERENCE
1184

The urine dipstick showed “3�” blood and 500 mg/dl ofprotein. Microscopic examination of the urine revealed0–2 white blood cells/hpf, 20–30 red blood cells/hpf, and1 dysmorphic red blood cell. The protein:creatinine ratiowas 4:1. A renal ultrasound showed 11.9 cm kidneys bi-laterally without evidence of hydronephrosis. The patientwas in frank renal failure with a creatinine level of 9.7mg/dl.
A serologic evaluation was sent. This included testingfor antinuclear antibodies, antibodies to double-strandedDNA and extractable nuclear antigens (Ro, La, Sm, andRNP), tests for hepatitis B and hepatitis C, serum comple-ment and cryoglobulin levels, antineutrophil cytoplasmicantibodies, antistreptolysin O titers, anti–glomerular base-ment membrane antibodies, serum and urine electrophore-sis, and measurement of ADAMTS-13 levels.
INTERIM CASE SUMMARY ANDFORMULATION
An otherwise healthy woman developed cellulitis severalweeks prior to evaluation in the emergency department for
shortness of breath and lower extremity edema. Her pre-sentation was remarkable for marked hypertension andvolume overload. She was in acute renal failure (creatinine9.7 mg/dl) and her peripheral blood smear showed schis-tocytes and thrombocytopenia.
Therefore, our patient presented with microangiopathichemolytic anemia (MAHA) and several other issues, in-cluding thrombocytopenia, severe hypertension, and se-vere renal failure. None of these is a diagnosis in itself;each needs to be evaluated within its clinical context.
Microangiopathic hemolytic anemiaMAHA is a form of hemolysis characterized by the intra-vascular deposition of fibrin. The syndrome results inschistocyte (red cell fragment) formation, along with thelaboratory findings typical of hemolysis (e.g., elevated con-centrations of indirect bilirubin and lactate dehydrogenaseand a low haptoglobin concentration). Although up to50% of normal subjects have an occasional schistocyte onthe peripheral blood smear, the presence of �2 schisto-cytes/hpf suggests the existence of a microangiopathic pro-cess (1). The polyspecific direct antiglobulin test is nega-
Table 1. Initial and subsequent laboratory results
Variable Normal rangeHospital
day 1Hospital
day 2Hospital
day 4Hospital
day 6
Hematocrit, % 36–48 25.7 19.0 23.4 23.5White blood cell count, per �l 4,000–11,000 11,400Differential count, %
Neutrophils 50–70 88Lymphocytes 18–42 9
Platelet count, per �l 150,000–440,000 85,000 66,000 129,000 134,000Mean corpuscular volume, fl 82–98 88Red blood cell distribution width index, % 10.5–15.5 17.7Prothrombin time, seconds 10.4–13.1 12.6Partial thromboplastin time, seconds 22–35 27.6Glucose, mg/dl 70–105 115Sodium, mEq/liter 133–145 125Potassium, mEq/liter 3.3–5.1 4.2Chloride, mEq/liter 96–108 87Bicarbonate, mEq/liter 22–32 18Urea nitrogen, mg/dl 6–20 83 80 100 58Creatinine, mg/dl 0.4–1.1 10 10 12.6 9Total bilirubin, mg/dl 0–1.5 1.1Albumin, gm/dl 3.4–4.8 4.1Phosphorus, mg/dl 2.7–4.5 8.6Calcium, mg/dl 8.4–10.2 8.9Lactate dehydrogenase, IU/liter 94–250 1,146 392 440 395Haptoglobin, mg/dl 30–200 �20Alkaline phosphatase, IU/liter 39–117 64Aspartate aminotransferase, IU/liter 0–40 38Alanine aminotransferase, IU/liter 0–40 21Creatinine kinase, IU/liter 26–140 83Troponin T, ng/ml 0–0.01 0.24Urine
Specific gravity 1.001–1.035 1.012Blood 3�Protein, mg/dl 500Red blood cells, per high-power field 0–2 20–30White blood cells, per high-power field 0–5 0–2Bacteria ModerateDysmorphic red blood cells 1
Clinicopathologic Conference 1185

tive in MAHA because the process of red cell destructionin MAHA is not associated with deposition of an autoan-tibody or complement on the surface of the red blood cell.
Renal failureCareful examination of the urine sediment is critical in thesetting of renal dysfunction. Active urinary sediment ischaracterized by the presence of white blood cell casts, redblood cell casts, and/or dysmorphic red blood cells. Thesefeatures generally indicate glomerular disease. Red bloodcell casts were not present in the urine of our patient,pointing away from a glomerular process, although in rarecases red blood cell casts can be seen in acute interstitialnephritis.
DIFFERENTIAL DIAGNOSIS
The finding of renal failure in this patient is consistentwith a working diagnosis of thrombotic microangiopathy(TM), which can be operationally defined as a combinationof MAHA, thrombocytopenia, and microvascular throm-bosis, here involving the kidney. The underlying causes ofTM are multiple and a partial list is shown in Table 2.
Distinguishing among the causes of TM is often chal-lenging because of overlap in the disorder’s presentingsymptoms. However, correct identification of the underly-ing diagnosis is essential, because the treatment of TMvaries substantially according to its cause. For example,high-dose glucocorticoids and cyclophosphamide may berequired to treat systemic vasculitis, whereas high-doseglucocorticoids are suspected of contributing to somecases of scleroderma renal crisis (SRC) and are contrain-dicated in that disorder (2). The mainstay of treatment forantiphospholipid syndrome (APS) is anticoagulation, notimmunosuppression (3). As discussed below, of all of thecauses of TM, only idiopathic thrombotic thrombocytope-nic purpura (TTP) responds to plasma exchange.
Malignant hypertensionOne etiology of TM in a patient with renal dysfunction ismalignant hypertension. It is postulated that severe hyper-tension fosters an inflammatory milieu in the vasculaturethat disrupts the endothelium, leading to activation of thecoagulation cascade and the development of fibrinoid ne-crosis, edema, and local platelet aggregation. Red cells aredamaged or fragmented as they try to pass through thefibrin deposits within narrowed, edematous arterioles (4).Most cases of malignant hypertension are preceded bylengthy periods of moderate hypertension that requiremedical therapy. Our patient had no history of hyperten-sion prior to her presentation, but malignant hypertensionremained a possibility as the inciting event.
Idiopathic TTPThe combination of otherwise unexplained renal dysfunc-tion, MAHA, and thrombocytopenia should trigger theimmediate working diagnosis of TTP. The renal dysfunc-tion in idiopathic TTP is usually characterized by protein-uria, hematuria, and/or active urinary sediment, althoughfrank renal failure as seen in this patient is distinctlyuncommon. Early suspicion of this condition is essentialbecause the mortality of untreated TTP is high and plasmaexchange can be life-saving (5).
The classic pentad of idiopathic TTP includes MAHA,thrombocytopenia, renal abnormalities, fluctuating neuro-logic abnormalities, and fever. The full pentad of features,which was classically seen in the era before plasma ex-change, is not required for the diagnosis of TTP. Therefore,it is critical to consider this diagnosis and to initiateplasma exchange in the presence of only otherwise unex-plained MAHA and thrombocytopenia. Glucocorticoidsmay be added to plasma exchange if the initial response totreatment is poor, although there are no randomized con-trolled studies that demonstrate an improvement in pa-tient outcomes with this strategy (1).
The finding of extremely low levels (i.e., �5% of normalactivity) of the von Willebrand factor–cleaving protease
Figure 1. Peripheral blood smear. This smear from the patient attime of admission shows multiple red blood cell fragments (schis-tocytes) and few platelets at high power. This is consistent with amicroangiopathic hemolytic anemia.
Table 2. Differential diagnosis ofthrombotic microangiopathy
Malignant hypertensionDisseminated intravascular coagulation secondary to
infection or malignancyIdiopathic thrombotic thrombocytopenic purpuraHemolytic uremic syndrome secondary to Shiga
toxin–producing E coliSevere pregnancy complications
(preeclampsia/eclampsia/hemolysis, elevated liverenzymes, and low platelets syndrome)
Posttransplant microangiopathy (e.g., renal, hematopoieticcell transplantation)
GlomerulonephritisSystemic lupus erythematosusSystemic vasculitisAntiphospholipid syndromeScleroderma renal crisisDrugs (cyclosporine, mitomycin C, quinine, ticlopidine)Human immunodeficiency virus infection
1186 Desai et al

(ADAMTS-13) and the demonstration of inhibitors toADAMTS-13 are both highly specific tests for idiopathicTTP. However, the results of such testing are not usuallyavailable for several days, during which time the patientmay die if plasma exchange is not initiated. Moreover, in astudy of 48 patients with idiopathic TTP/hemolytic ure-mic syndrome (HUS), clinical responses to plasma ex-change appeared to occur across a broad range ofADAMTS-13 levels, including some patients whose levelswere �25% of normal (6). The clinical value ofADAMTS-13 appears to be in identifying patients whowill likely relapse; namely those with an activity level�5% in the presence of an inhibitor.
Hemolytic uremic syndromeWhen adult patients present with MAHA, thrombocytope-nia, and prominent renal failure, with or without a pro-dromal diarrheal illness, they are often diagnosed as hav-ing adult HUS. In contrast, those patients with the samehematologic presentation, less renal involvement, andprominent neurologic abnormalities are more likely to bediagnosed as having TTP. Because there is great heteroge-neity of presentations, some clinicians prefer to groupthese patients under the umbrella term of TTP/HUS. How-ever, in general, patients with more classic HUS, such asthose seen after a diarrheal illness associated with Shigatoxin–producing E coli, do not have low levels ofADAMTS-13 and do not respond to treatment with plasmaexchange.
GlomerulonephritisSevere glomerulonephritis (GN) can sometimes lead toMAHA-like changes on the peripheral blood smear. Forexample, in a review of patients with anti–glomerularbasement membrane disease, 50% had peripheral bloodsmear changes consistent with MAHA, accompanied bythe laboratory findings of hemolysis (7). Other potentialetiologies of such renal dysfunction include membranousGN and pauci-immune rapidly progressive GN, althoughMAHA-like changes are less common in those conditions.
Systemic vasculitisSystemic vasculitis can also be associated with MAHA andTM. Such patients typically have severe GN (8). Polyar-teritis nodosa, a vasculitis of medium-sized muscular ar-terioles, can also cause severe malignant hypertension andlead to the abnormal urinalysis changes similar to thoseseen in our patient.
Systemic lupus erythematosusTTP occurs in a subset of patients with systemic lupuserythematosus (SLE) (9). The 2 disorders have been esti-mated to occur together in �0.5% of SLE patients. In�75% of such cases, TTP presents in a patient with anestablished diagnosis of SLE (10). The finding of immunecomplex–mediated GN on renal biopsy is helpful in dis-tinguishing SLE-associated TTP from idiopathic TTP.However, the features of TM on light microscopy alone donot differentiate lupus nephritis from either TTP or the
APS that can be associated with SLE. Immunofluorescenceand electron microscopy studies are essential for the dem-onstration of IgG, IgM, C3, and other immunoreactant dep-ositions that characterize lupus nephritis.
Antiphospholipid syndromeAPS is associated with thrombosis and/or pregnancy-related morbidity occurring in the setting of antiphospho-lipid antibodies. TM, thrombocytopenia, and renal diseasecaused by intraglomerular thrombi can all occur in thespectrum of APS. Catastrophic APS is a rare variant asso-ciated with high mortality due to widespread thrombosis(11). Due to the many clinical variations of APS, patientswith antiphospholipid antibodies and TM are frequentlymisdiagnosed as having TTP/HUS, catastrophic APS,acute renal failure, and/or malignant hypertension (12).
Scleroderma renal crisisSRC is a complication of systemic sclerosis (SSc) associ-ated with malignant hypertension, rapidly progressive re-nal insufficiency, and MAHA (13). Although it is morecommon in patients with diffuse SSc, it can also be seen inthose with limited SSc as well. Before the availability ofangiotensin-converting enzyme (ACE) inhibitors, SRC wasthe most common cause of death among patients with SSc.
Other causesOther disorders associated with TM include disseminatedintravascular coagulation secondary to sepsis or malig-nancy, various drugs, certain pregnancy complications,and posttransplant status. None of these conditions is thelikely cause of TM in our patient.
INITIAL TREATMENT
On hospital day 1, the patient began hemodialysis withplasma exchange for a presumptive diagnosis of idiopathicTTP. Renal biopsy was debated seriously by the RenalConsultative team, but was not performed. Immunosup-pressive and cytotoxic agents were not administered.
Over hospital days 2 through 6, the patient underwentdaily plasma exchange and hemodialysis. Her BP im-proved slightly and there was some decrease in her pe-ripheral edema. However, her anemia, thrombocytopenia,and renal failure persisted, with only a slight decrease inher lactate dehydrogenase (Table 1).
After discussion with the Hematology, Renal, and Trans-fusion Medicine teams, a decision was made to discon-tinue plasma exchange due to the lack of significant initialclinical improvement with therapy, and more importantly,due to additional data that pointed to an alternative diag-nosis to explain the MAHA, thrombocytopenia, and renalfailure.
Additional informationFurther history was obtained. The patient reported 6months of joint pain and stiffness in the metacarpophalan-geal joints of both hands, inability to make a fist, andsymptoms consistent with Raynaud’s phenomenon. A
Clinicopathologic Conference 1187

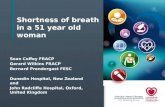
more detailed skin examination revealed thickening of theskin of her hands bilaterally, erythema in her periungualregions, and dilatation of the nailbed capillaries (Figure 2).
The results of her immunologic evaluation are shown inTable 3. The antinuclear antibodies were positive at a titerof 1:1,280 (speckled pattern). The ADAMTS-13 activitywas low (41%), but well above the range characteristic ofidiopathic TTP (i.e., �5% of the normal value) (14). Aninhibitor screen was not indicated for this level of activity.The ADAMTS-13 result was returned the day after plas-mapheresis was discontinued. This result supported theclinical suspicion that the patient did not have idiopathicTTP and that an alternative diagnosis was likely.
A procedure was performed.
ProcedureThe procedure consisted of a skin biopsy of the dorsum ofher left hand (Figure 3). The biopsy sample revealed scle-
rosis of the cutaneous tissues in the mid to deep dermis.There was a slight increase in dense collagen within thisregion, but no inflammation and no basement membraneabnormalities. These findings were consistent with eitherscleroderma or morphea.
Subsequent courseThe patient began treatment with captopril. The dosagewas titrated quickly to the maximum amount (25 mg3 times daily), with some improvement in her BP. How-ever, management of the patient’s BP remained challeng-ing, requiring the addition of an angiotensin receptorblocker and a calcium-channel blocker to the ACE inhibi-tor. Over the next few days, her hematocrit value andplatelet count began to improve, but she remained dialysisdependent.
Pulmonary function testing demonstrated a mild restric-tive process, and a computed tomography scan of the chest
Figure 2. The patient’s hands. Note the prominent periungualcapillary loops of most of the fingers, and the tight, thickened skinmore prominent over the bilateral metacarpophalangeal joints.This is consistent with sclerodactyly. There is no evidence ofsynovitis.
Table 3. Immunologic evaluation
Test Result Reference range
Anticardiolipin antibodyIgM, MPL units 9.2 0–12.5IgG, GPL units 8.0 0–15
Antineutrophil cytoplasmic antibody Negative NegativeAntinuclear antibody Positive NegativeAntinuclear antibody titer 1:1,280 speckledAnti–glomerular basement membrane antibody, U/ml �3 �3Sm Negative NegativeRNP Negative NegativeScl-70 antibody 0.03 �1 index valueAnticentromere antibody Negative NegativeSerum protein electrophoresis Negative NegativeUrine protein electrophoresis Negative NegativeC3, mg/dl 89 90–180C4, mg/dl 22 10–40Human immunodeficiency virus antibody Negative NegativeADAMTS-13 activity, % 41 (low) �67
Figure 3. Skin biopsy sample reveals mid to deep dermal sclero-sis manifested by a slight increase in dense collagen. There is mildto no inflammation and no basement membrane abnormalities.This is consistent with scleroderma or morphea.
1188 Desai et al

revealed possible mild early interstitial lung disease. Anechocardiogram showed a normal left ventricular ejectionfraction of �55% and no evidence of pulmonary arteryhypertension.
After discharge, the patient opted to switch to peritonealdialysis. Eight months after her admission for shortness ofbreath, she underwent the successful implantation of aliving-related renal allograft.
DISCUSSION
The assessment of this patient with MAHA, thrombocyto-penia, severe hypertension, and severe renal dysfunctionposed a clinical challenge that traversed multiple medicalsubspecialties. In the evaluation of such patients, it isessential to think beyond subspecialty boundaries and tocomplete a broad initial evaluation quickly because of thepotentially dire consequences to the patient with this con-stellation of findings who does not receive appropriatetherapy.
A number of findings in our patient eventually pointedaway from the initial working diagnosis of idiopathic TTP.At the time of her admission, the patient had severe hy-pertension and severe renal failure, which are unusualfeatures for TTP (15). In addition, there were subtle his-toric features and physical findings not appreciated by thephysicians who initially evaluated her; specifically, the6-month history of Raynaud’s phenomenon and musculo-skeletal reports, the mild sclerodactyly, and the dilatationof the nailbed capillaries. Later in her hospital course,information from the testing of her ADAMTS-13 status, theonly slightly diminished ADAMTS-13 level without evi-dence of an ADAMTS-13 inhibitor, did not support thediagnosis of idiopathic TTP.
In the endothelium, von Willebrand factor (vWF) ispresent as ultra-large multimers of �20,000 kd. However,vWF circulates in plasma as a series of multimers, gener-ally on the order of 500–20,000 kd. ADAMTS-13 (an ac-ronym for a disintegrin and metalloprotease with throm-bospondin type 1 motif, member 13) is the enzymeresponsible for cleaving vWF after vWF is formed andsecreted into the circulation by the endothelium andmegakaryocytes/platelets (16).
A lack of ADAMTS-13 activity can result from either aninherited gene mutation or autoantibody formation. Thisleads to an increase in the plasma concentration of ultra-large vWF multimers, and it is postulated that an addi-tional insult may then take place, resulting in the patho-logic process seen in congenital or idiopathic TTP.
Since the discovery of ADAMTS-13 and its role in pa-tients with TTP (17), assays for ADAMTS-13 activity anddetection of inhibitors and autoantibodies have been de-veloped. Results of these assays are not usually availablefor �2 days. Accordingly, the diagnosis and treatment ofTTP must be initiated based on the presence of otherwiseunexplained MAHA and thrombocytopenia alone withoutan alternative diagnosis. Because delayed treatment ofTTP can be life-threatening, plasma exchange is recom-mended as the initial management strategy.
Plasma exchange has a dual effect in this condition: it
functions to remove antibodies to ADAMTS-13 if presentand to increase circulating levels of this protease by infus-ing plasma that contains normal levels. Given that plasmaexchange in idiopathic TTP has been demonstrated to bemore effective than plasma infusion alone, it has beensurmised that both effects are required for clinical im-provement (18).
SRC is estimated to occur in 4–6% of patients with SSc(scleroderma) (19). SRC is a catastrophic illness usuallyassociated with the diffuse form of scleroderma. It usuallypresents within 3 years of the first scleroderma manifesta-tion. SRC classically presents with malignant hyperten-sion, MAHA, and diffuse skin thickening. Although in thiscase a skin biopsy was obtained, a careful physical exam-ination of the skin and joints is often sufficient to make thediagnosis of scleroderma. Bland urine sediment with mildproteinuria and dysmorphic red blood cells, precisely themanner in which our patient presented, is characteristic ofSRC.
Scleroderma kidney involvement was initially de-scribed in the mid-1800s, but the term SRC was not coineduntil 1952 (20). The underlying etiology of this conditionis not well understood, but renal vascular intimal prolif-eration, vascular hyperreactivity, decreased cortical bloodflow, and activation of the renin–angiotensin–aldosteroneaxis have all been implicated (21). The systemic manifes-tations of SRC are propagated through renin-aldosterone–mediated malignant hypertension. Therefore, primarytreatment for SRC is aggressive ACE inhibition, even in thepresence of renal failure. The role of angiotensin receptorblockers in the management of renal crisis is less clear(22).
Glucocorticoid use in patients with scleroderma hasbeen postulated to trigger the onset of SRC, although thispoint is contentious. A case–control study showed that theuse of high-dose steroids (�15 mg/day) was associatedwith SRC when used in the 6 months prior to diagnosis(23). Although there is still considerable morbidity asso-ciated with SRC, mostly related to the effects of malignanthypertension, the introduction of ACE inhibitor therapyreduced the 1-year mortality in this disorder from 76% to�15% (24). Some patients who require dialysis are able todiscontinue this intervention if ACE inhibition is main-tained (13).
The diagnosis of SRC can be challenging for severalreasons. SRC may be part of the initial clinical presenta-tion of SSc, as was the case in our patient. Among patientswho have established scleroderma, the differential diagno-sis of renal failure must include hypovolemia and renalartery stenosis, as well as the adverse effects of medica-tions. SRC can also have atypical presentations. For exam-ple, although hypertension is a hallmark of SRC, normalBPs have been described in some patients (21). It is essen-tial for all patients with SSc to have routine BP monitoringto watch for the development of renal crisis.
After the patient was discharged from the hospital, as-says for anti–RNA polymerase I/III antibodies were ob-tained and returned positive on 2 occasions at 312 and 254units (normal value �20 units). In a Canadian cohort ofpatients with SSc, these antibodies were positive by en-zyme-linked immunosorbent assay in 19.4% of patients
Clinicopathologic Conference 1189

and were associated with diffuse disease and the develop-ment of kidney and joint/tendon involvement (25). There-fore, anti–RNA polymerase antibodies may serve as anadjunctive diagnostic tool in patients with SSc and may bea more informative prognostic tool in portending SRC.
FINAL DIAGNOSIS
Scleroderma renal crisis.
REFERENCES
1. George JN. How I treat patients with thrombotic thrombocy-topenic purpura-hemolytic uremic syndrome. Blood 2000;96:1223–9.
2. Steen VD, Medsger TA Jr, Osial TA Jr, Ziegler GL, Shapiro AP,Rodnan GP. Factors predicting development of renal involve-ment in progressive systemic sclerosis. Am J Med 1984;76:779–86.
3. Petri M. Pathogenesis and treatment of the antiphospholipidantibody syndrome. Med Clin North Am 1997;81:151–77.
4. Brain MC. Microangiopathic hemolytic anemia. N Engl J Med1969;281:833–5.
5. Nesher G, Hanna VE, Moore TL, Hersh M, Osborn TG. Throm-botic microangiographic hemolytic anemia in systemic lupuserythematosus. Semin Arthritis Rheum 1994;24:165–72.
6. Vesely SK, George JN, Lammle B, Studt JD, Alberio L, El-Harake MA, et al. ADAMTS13 activity in thrombotic throm-bocytopenic purpura-hemolytic uremic syndrome: relation topresenting features and clinical outcomes in a prospectivecohort of 142 patients. Blood 2003;102:60–8.
7. Stave GM, Croker BP. Thrombotic microangiopathy in anti-glomerular basement membrane glomerulonephritis. ArchPathol Lab Med 1984;108:747–51.
8. Ross CN, Reuter H, Scott D, Hamilton DV. Microangiopathichaemolytic anaemia and systemic vasculitis. Br J Rheumatol1996;35:377–9.
9. Hamasaki K, Mimura T, Kanda H, Kubo K, Setoguchi K, SatohT, et al. Systemic lupus erythematosus and thrombotic throm-bocytopenic purpura: a case report and literature review. ClinRheumatol 2003;22:355–8.
10. Musio F, Bohen EM, Yuan CM, Welch PG. Review of throm-botic thrombocytopenic purpura in the setting of systemiclupus erythematosus. Semin Arthritis Rheum 1998;28:1–19.
11. Asherson RA, Cervera R, Piette JC, Font J, Lie JT, Burcoglu A,et al. Catastrophic antiphospholipid syndrome: clinical and
laboratory features of 50 patients. Medicine (Baltimore) 1998;77:195–207.
12. Espinosa G, Bucciarelli S, Cervera R, Lozano M, Reverter JC,de la Red G, et al. Thrombotic microangiopathic haemolyticanaemia and antiphospholipid antibodies. Ann Rheum Dis2004;63:730–6.
13. Steen VD. Scleroderma renal crisis. Rheum Dis Clin NorthAm 2003;29:315–33.
14. Lammle B, Kremer Hovinga JA, Alberio L. Thrombotic throm-bocytopenic purpura. J Thromb Haemost 2005;3:1663–75.
15. Manadan AM, Harris C, Block JA. Thrombotic thrombocyto-penic purpura in the setting of systemic sclerosis. SeminArthritis Rheum 2005;34:683–8.
16. Liu L, Choi H, Bernardo A, Bergeron AL, Nolasco L, Ruan C,et al. Platelet-derived VWF-cleaving metalloprotease AD-AMTS-13. J Thromb Haemost 2005;3:2536 – 44.
17. Levy GG, Nichols WC, Lian EC, Foroud T, McClintick JN,McGee BM, et al. Mutations in a member of the ADAMTSgene family cause thrombotic thrombocytopenic purpura. Na-ture 2001;413:488–94.
18. Rock GA, Shumak KH, Buskard NA, Blanchette VS, Kelton JG,Nair RC, et al, and the Canadian Apheresis Study Group.Comparison of plasma exchange with plasma infusion in thetreatment of thrombotic thrombocytopenic purpura. N EnglJ Med 1991;325:393–7.
19. Walker UA, Tyndall A, Czirjak L, Denton C, Farge-Bancel D,Kowal-Bielecka O, et al. Clinical risk assessment of organmanifestations in systemic sclerosis: a report from the EULARScleroderma Trials and Research group database. Ann RheumDis 2007;66:754–63.
20. Moore HC, Sheehan HL. The kidney of scleroderma. Lancet1952;1:68–70.
21. Teixeira L, Mahr A, Berezne A, Noel LH, Guillevin L, Mou-thon L. Scleroderma renal crisis, still a life-threatening com-plication. Ann N Y Acad Sci 2007;1108:249–58.
22. Pham PT, Pham PC, Danovitch GM, Gritsch HA, Singer J,Wallace WD, et al. Predictors and risk factors for recurrentscleroderma renal crisis in the kidney allograft: case reportand review of the literature. Am J Transplant 2005;5:2565–9.
23. Steen VD, Medsger TA Jr. Case–control study of corticoste-roids and other drugs that either precipitate or protect fromthe development of scleroderma renal crisis. Arthritis Rheum1998;41:1613–9.
24. Steen VD, Costantino JP, Shapiro AP, Medsger TA Jr. Out-come of renal crisis in systemic sclerosis: relation to avail-ability of angiotensin converting enzyme (ACE) inhibitors.Ann Intern Med 1990;113:352–7.
25. Santiago M, Baron M, Hudson M, Burlingame RW, FritzlerMJ. Antibodies to RNA polymerase III in systemic sclerosisdetected by ELISA. J Rheumatol 2007;34:1528–34.
1190 Desai et al