
955_MonicaKRAFT_SevereasthmaALAT2012Kraft
42
New Insights in the Treatment of Severe Asthma: Focus Upon Phenotypes Monica Kraft, M.D. Professor of Medicine Director, Duke Asthma, Allergy and Airway Center Division of Pulmonary, Allergy and Critical Care Medicine Duke University Medical Center Durham, North Carolina USA
-
Upload
congresos-alat -
Category
Documents
-
view
214 -
download
1
description
http://www.congresosalat.org/images/stories/3_pdf/04_congreso2012/presentaciones/jueves5ago2012_pdf/ballroom_A/am/955_MonicaKRAFT_SevereasthmaALAT2012Kraft.pdf
Transcript of 955_MonicaKRAFT_SevereasthmaALAT2012Kraft

New Insights in the Treatment of Severe Asthma: Focus Upon Phenotypes
Monica Kraft, M.D. Professor of Medicine
Director, Duke Asthma, Allergy and Airway Center Division of Pulmonary, Allergy and Critical Care
Medicine Duke University Medical Center
Durham, North Carolina USA

Disclosures
Speakers bureau: n/a Advisory Board/consultant: n/a Other income: Royalties: Elsevier Research (funds provided to institution):
National Institutes of Health, Genentech GSK, Novartis, Merck, Boston Scientific

Severe Asthma
• Definition
• Phenotypes - Pathologic/Clinical
• Therapeutic Options/Personalized Medicine

Good Poor
Mild
Severe
Ast
hma
seve
rity
good control
poor control
Asthma control
Severity is a property of the disease
Control reflects the adequacy of treatment
We have little influence ! In which we play a
significant role !
Emphasizing Control Rather Than Severity

Approach to Management/Contributing Factors/Co-Morbid Conditions
•Examine for concomitant medical disorders, i.e. sinusitis, OSA, VCD •GERD - acid and non-acid reflux •Environmental control •Alternative diagnoses •Review medication technique •Adherence

We have now moved to defining phenotypes of this heterogeneous disease
Clinical: Pathologic: Fixed obstruction Eosinophilic Obese Non-eosinophilic Adult onset Pauci-granulocytic Exacerbation prone Treatment resistant Triggers Occupational Aspirin Exercise Menses

Severe Asthma Clusters
Moore et al. AJRCCM 2010;181:315-323

Asthma Clusters • Cluster 1: early onset, atopic, nl lung fxn < 2
controllers, minimal healthcare utilization • Cluster 2: early onset, atopic, > 2 controllers, nl lung
fxn, significant health care utilization • Cluster 3: adult onset, obese woman with low lung
fxn, high medication requirement and healthcare utilization
• Cluster 4: early onset, atopic, severe obstruction with some reversibility (FEV1: 57% to 76% pred), high healthcare utilization
• Cluster 5: early onset, severe obstruction, 66% atopic; less reversibility ( FEV1: 43% to 58%), high health care utilization Moore et al. AJRCCM 2010;181:315-323

Association of an IL-6 polymorphism with severe asthma and reduced lung function
(clusters 4 and 5)
Hawkins et al. JACI 2012; in press.
Pathological Phenotypes: Can they determine therapeutic choices?
•Eosinophilic/TH2 (IL-4, IL-5 and IL-13) •Non-eosinophilic •Pauci-granulocytic •Relevance of location of inflammation/remodeling

Variability in IL-13 Responsive Genes
Woodruff, et al. AJRCCM 2009; 180:388-395

Clinical Features of Asthmatics with “High” and “Low” IL-13 Gene
Signatures
Woodruff, et al. AJRCCM 2009; 180:388-395

Interleukin-13 and Non–Interleukin-13 Inflammatory Pathways in Asthma.
Kraft M. N Engl J Med 2011.

Biomarkers that identify the Th2 phenotype
• Sputum eosinophils • Exhaled nitric oxide • Circulating eosinophils • periostin
What Are Treatment Options for the Eosinophilic Phenotype?

Omalizumab Significantly Reduces Submucosal Eosinophils
Eosinophils (cells/mm2)
Baseline Posttreatment 0
20
60
80 80
60
20
0
40 40
Baseline Posttreatment
8.0 1.5
6.3 6.4
Placebo (n=14) Omalizumab (n=14)
P<0.001
P=0.81 P=0.033
Djukanovic et al. AJRCCM 2004

Inhibition of IL-13 and Lung Function
Corren et al. NEJM 2011; in press

Mepolizumab for Severe Eosinophilic Asthma
Nair et al. NEJM 2009;360:985

Other therapies (some under development) for eosinophilic
asthma Anti-CRTH2 Anti-IL-9 Anti-TSLP Zileuton – aspirin sensitive asthma; 25%
of severe asthma and eosinophilic
Non-eosinophilic asthma
Neutrophils in Asthma • Associated with more severe limitation
(Woodruff et al. JACI 2001;108:753 Shaw et al. Chest 2007;132:1871)
• Not associated with greater AHR as compared to eosinophils predominant inflammation (Woodruff)
• Observed in fatal asthma, but primary in small airways (Simoes et al. Clin Exp Allergy 2005;35:602)
• Increased during exacerbations (Lamblin et al. AJRCCM 1998;157:394; Fahy et al. JACI 1995;95:843)

Sputum Differential and Clinical Characteristics – SARP experience
Hastie et al. for SARP. J All Clin Immunol 2010;125:1028

Sputum Differential and Clinical Characteristics
Hastie et al. for SARP. J All Clin Immunol 2010;125:1028
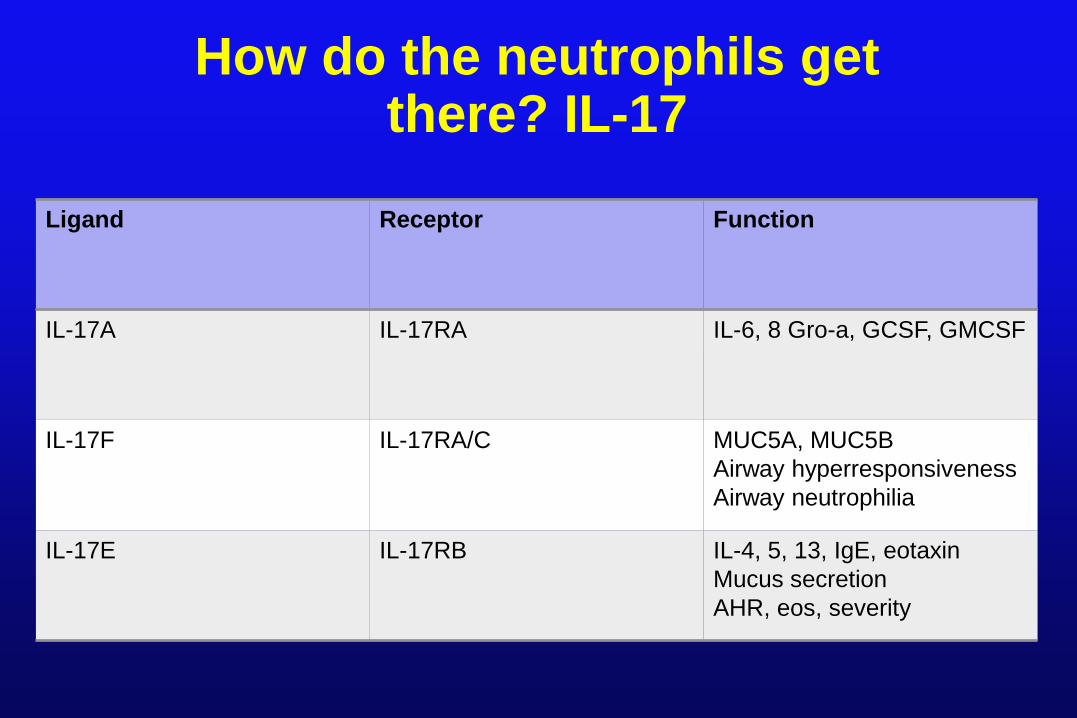
How do the neutrophils get there? IL-17
Ligand Receptor Function
IL-17A IL-17RA IL-6, 8 Gro-a, GCSF, GMCSF
IL-17F IL-17RA/C MUC5A, MUC5B Airway hyperresponsiveness Airway neutrophilia
IL-17E IL-17RB IL-4, 5, 13, IgE, eotaxin Mucus secretion AHR, eos, severity

Question: Is neutrophilic asthma a stable phenotype?

Sputum neutrophils and ICS – Cowen et al.
• Subjects with mild to moderate asthma underwent steroid withdrawal over 28 days; induced sputum with differential performed
• Fluticasone introduced and repeat sputum performed
• Exclusions: respiratory infection within 4 weeks, OCS within 3 months

Sputum differential after fluticasone withdrawal
Cowan et al. Thorax 2010;65:384

Sputum differentials before and after fluticasone
Cowan et al. Thorax 2010;65:384

What other mediators are prominent in non-eosinophilic
asthma?
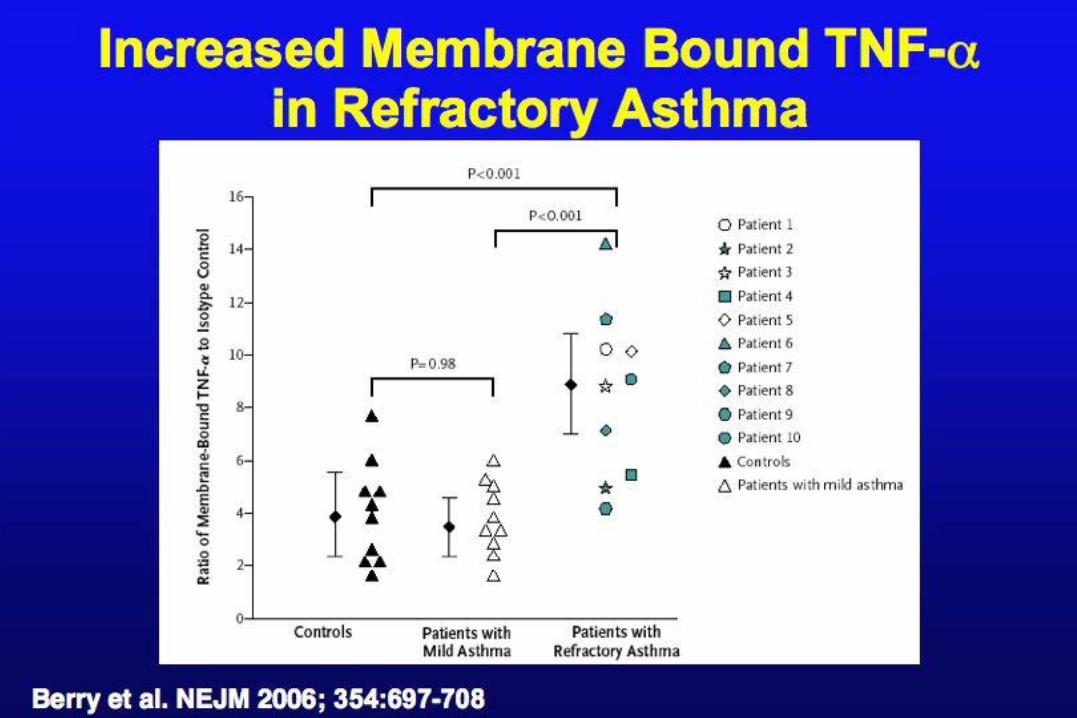

BAL TNF-α Levels are Increased in the lungs of obese asthmatics
**p<0.001, *p<0.01, #p<0.05 Lugogo et al. JACI 2012; in revision

What are the treatment options for the non-eosinophilic phenotype?

Treatment options for the non-eosinophilic phenotype – available
now and under developement • Anti-TNF • zileuton • macrolides • Anti-IL-17 • Anti-IL-22

Pauci-Granulocytic
•No definitive cell type noted in examination of endobronchial biopsies
•May be treated with oral corticosteroids.
•Inflammation may be located distally, but not proven.

Therapies for the pauci-granulocytic phenotype
• Small particle size ICS • Bronchial thermoplasty • tiotropium

Airway & Alveolar Tissue Eosinophils
Alveolar Tissue Airway
40
30
20
10
0 (0.0,1.8) (0.0,0.0)
(17.7,75.0)
(3.0,26.5) *
4 am * †
4 pm
Nv eos x103/mm3
NNA NA
Alveolar Tissue Airway
40
30
20
10
0 (0.0,13.3)
(1.9,18.6) (2.7,16.8) (29.1,18.2) †
Kraft AJRCCM; 1996

HFA BDP 40 µg CFC-BDP 42 µg
31% 94%
Oral
Lung
51% 4%
18% 1% Exhaled
Deposition of BDP in healthy volunteers
Leach CL et al. Eur Respir J 1998; 12(6): 1346-53

Central and Peripheral Airway Eosinophils Before and After Flunisolide HFA
Eosinophils (MBP+) before and after HFA-flunisolide in peripheral and central airways. Mean±SEM. *† p < .001 vs pre treatment.
before after after before peripheral airways central airways
70 60 50 40 30 20 10 0
Eosi
noph
ils/m
m2
Hauber P et al. JACI 2003
*
*
†
†

Airway Smooth Muscle
Airway Smooth Muscle
Normal Airway
Asthmatic Airway

Bronchial Thermoplasty
0.14
0.430.36
0.7
0.07
0.28
0.48
0.04
0.0
0.2
0.4
0.6
0.8
1.0
SevereExacerbations
Unsched. OfficeVisits
ER Visits Hospitalizations
Eve
nts/
Sub
ject
/ Yea
r
Sham Alair
**
*
0.04
*PPS = 95.6%, ** PPS= 95.6%
32%
73%
84% 23%
0.13 7
64
57
3
18
7976
29
0
10
20
30
40
50
60
70
80
90
² - 0.5 > -0.5 to <0.5 ³ 0.5 Net Benefit
Perc
ent o
f Sub
ject
s
Sham Alair
AIR2 TrialNet Benefit = 19%PPS (Alair - Sham) = 100.0%
Castro M et al. Am J Respir Crit Care Med. 2010;181(2):116-24

Tiotropium as Add-On Therapy for Asthma Uncontrolled with ICS
Peters SP and the Asthma Clinical Research Network NEJM 2010;363:1715
Conclusions •Severe asthma is a spectrum of disease, with
different pathologic and clinical phenotypes.
• Importance of contributing factors and adherence cannot be overestimated.
•Defining phenotypes is in its infancy.
•Tailoring treatment to phenotypes is the ultimate goal.


















