9/11 “The Malaria epidemic is like loading up seven Boeing 747 airplanes each day then...
21
9/11 “The Malaria epidemic is like loading up seven Boeing 747 airplanes each day then deliberately crashing them into Mt Kilamanjaro” Chairman Malaria Foundation International
-
Upload
isabel-white -
Category
Documents
-
view
217 -
download
0
Transcript of 9/11 “The Malaria epidemic is like loading up seven Boeing 747 airplanes each day then...

9/11“The Malaria epidemic is like loading up seven Boeing 747 airplanes each day then deliberately crashing theminto Mt Kilamanjaro”
Chairman Malaria Foundation International

• An African dies every 30 seconds from malaria.
• That means that by the end of this conference about 9000 people will have died from this disease.
• By the end of the year just under 1 million will have died.
Please don’t forget
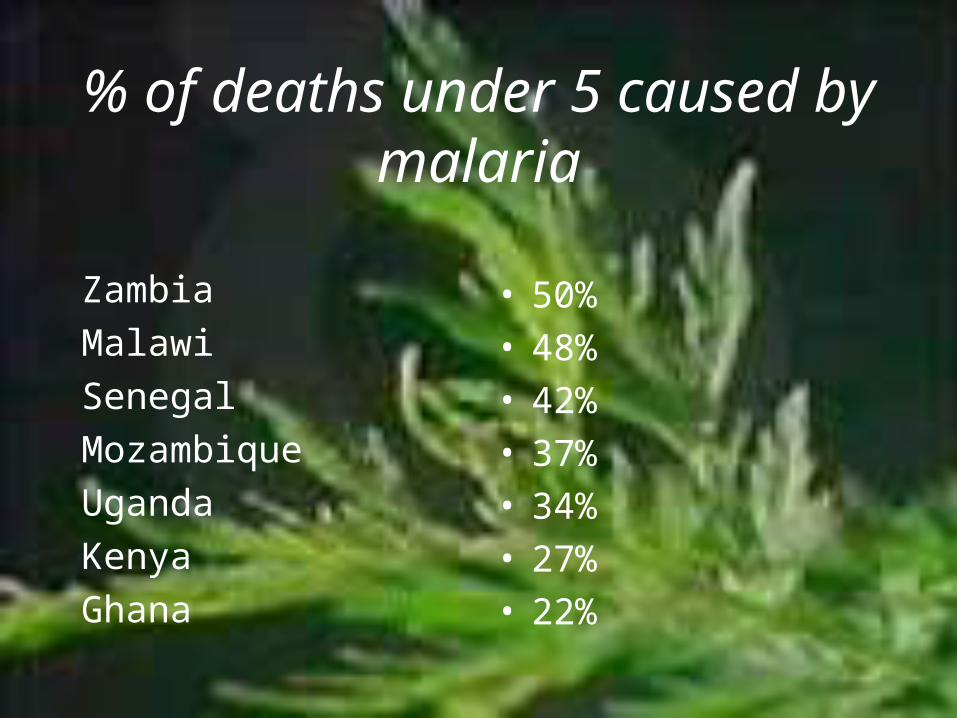
% of deaths under 5 caused by malaria
ZambiaMalawiSenegalMozambiqueUgandaKenyaGhana
• 50%• 48%• 42%• 37%• 34%• 27%• 22%

Counting the cost• Poor families spend 25% of their
annual income on malaria prevention and treatment
• In Malawi Malaria accounts for 40% of the total public health spending
• Malaria costs Africa $12 billion per year
Roll Back Malaria Program report

Where are the products?
“We have a ridiculous situation in that governments together with individuals like Bill Gates and George Soros are providing funds to treat malaria and people are still dying every day from malaria when a treatment approved by WHO exists but is not available to them”
CEO Essential Nutrition August 2005

Access
“the weapons to fight malaria exist: medications, insecticide treatments, spray equipment, tests to diagnose the disease…. But these weapons are useless if they do not reach those who need them.”
RBM report 2004

Fond hopesThe Roll Back Malaria (RBM) programme launched in 1998 by
WHO, UNICEF , UNDP and World Bank has as its stated goal to halve Malaria by 2010
“By the end of 2005 in Africa at least 60% of those suffering malaria should be able to access and use correct,affordable and appropriate Treatment within 24 hours of the onset of treatment ”
Abuja Declaration 2003
Malaria and Malnutrition
• The major cause of malnutition in Africa is not lack of food but malaria and war
• CILSS-IAI report 1982

Cost“Of the currently available
antimalarials only three cost < $1 per treatment which is the threshold set by WHO for affordable treatment. These include chloroquine, sulfadoxine-pyrimethamine and amodiaqunene all of which are fast becoming useless. ACTs are expected to cost circa $3 per treatment. “
White 2003
Some Key Issues 1
• Elite planting material, does it exist?
• Is growing artemisia profitable?• High tech cultivation or
smallholder crop?• Artemisinin yields per hectare?• Shortage or surplus – who knows?• Where should we grow? Asia,
Africa, both?
Some Key Issues 2
• Why focus just on Artemisia?• What alternative herbal
antimalarials exist?• Is sufficient funds going into this?• What about their safety and
efficacy?• Can they be sustainably sourced?• Can they be used in combination?• If so with what else?

Some Key Issues 3
• Combination therapy – dogma or must?
• What combinations are possible?• Who makes the rules?• When is monotherapy appropriate?• What is the risk reward ratio?

Some Key Issues 4
• Finding cost effective products?• ACTs are too expensive for Africa?• Village Artemisia teas are
dangerous?• Novel extraction methods Co2, CFT• Suppositories, sub lingual sprays
Some Key Issues 5
• Drug approvals – why so few?• Who gets fast tracked and why?• Detailed international & national
registration guidelines don’t exist• Is safety testing used as a barrier
to entry?

Some Key Issues 6MARKETING• Antimalarials are not a profitable
business in the first place – compare anticancer drugs
• The suffers cannot afford to pay• It is the travellers market that
makes the money for malaria drug producers
• But artemisia is NOT recommended for prophylaxis
• So who will buy the ACTs, Bill Gates?
Objectives
• Sharing information between research, development, healer, policy and regulatory organizations involved in malaria treatment and control,

Objectives
• Identifying issues affecting the conservation, cultivation and production of potent medicinal plant species relevant to malaria treatment,

Objectives
• Encouraging new products and novel delivery systems that offer cost effective and safe remedies for malaria sufferers, and identifying investors and entrepreneurs will to develop such products,
Objectives
• Encouraging appropriate investment in the growing, processing and distribution of herbal antimalarials,
Objectives
• Forwarding to government and international agencies clear recommendations concerning rationalization and streamlining of safe manufacturing practices and marketing regulations for antimalarials,

Objectives
• Developing appropriate Africa-wide quality control and quality assurance standards for cultivation, production and distribution of herbal antimalarials and methods to implement and police such standards.