9 Viral Hepatitis Dentistry School 2012 2013
46
Viral Viral Hepatitis Hepatitis Khaled Jadallah, MD Assistant Professor of Medicine Gastroenterology, Hepatology, & Nutrition
-
Upload
shanfiza92 -
Category
Documents
-
view
118 -
download
2
description
lect9 pt2
Transcript of 9 Viral Hepatitis Dentistry School 2012 2013
Viral HepatitisViral Hepatitis
Khaled Jadallah, MD
Assistant Professor of Medicine
Gastroenterology, Hepatology, & Nutrition
“Knowing is not enough; we must apply.
Willing is not enough; we must do.” (Goethe)
Educational ObjectivesEducational ObjectivesOutline the epidemiology of viral hepatitisList causative agents for viral hepatitisRecognize the clinical features of acute and
chronic viral hepatitis and their complications
Interpret serologic tests to accurately diagnose the specific cause of viral hepatitis
Identify appropriate candidates for vaccination against HAV and HBV
Why Bother With Viral Why Bother With Viral Hepatitis for a Dentist?Hepatitis for a Dentist?
Dentists can get it…if not properly protected
Dentists can involuntarily transmit it to patients (improper sterilization techniques of tools)
Dental patients with chronic hepatitis complicated by coagulopathy can have uncontrollable bleeding
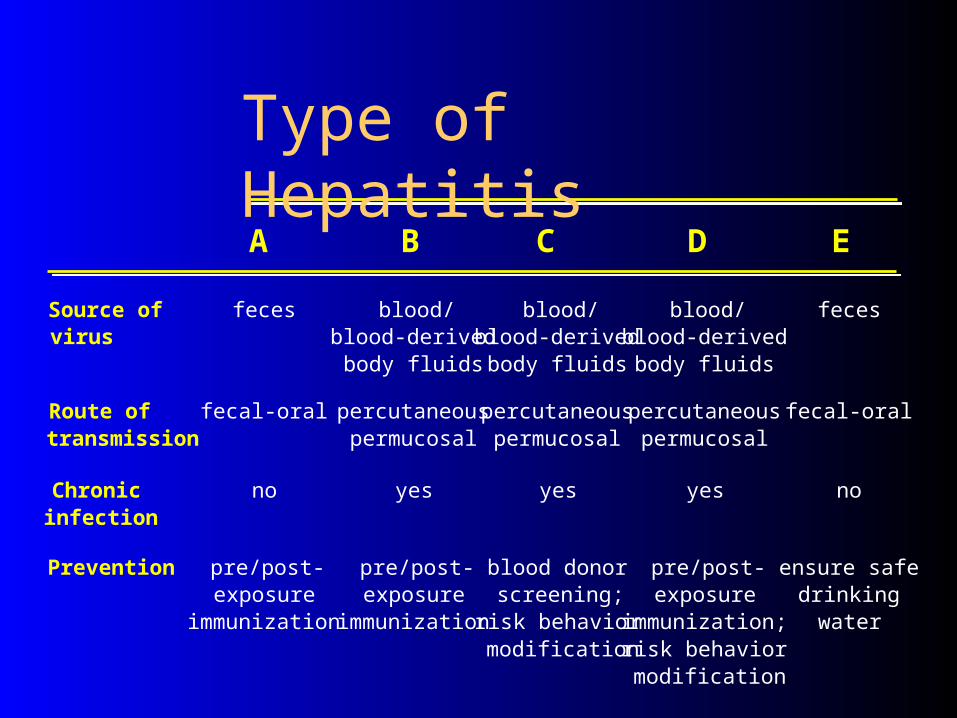
Source ofvirus
feces blood/blood-derived
body fluids
blood/blood-derived
body fluids
blood/blood-derived
body fluids
feces
Route oftransmission
fecal-oral percutaneouspermucosal
percutaneouspermucosal
percutaneouspermucosal
fecal-oral
Chronicinfection
no yes yes yes no
Prevention pre/post-exposure
immunization
pre/post-exposure
immunization
blood donorscreening;
risk behaviormodification
pre/post-exposure
immunization;risk behaviormodification
ensure safedrinking
water
Type of HepatitisA B C D E

Clinical Manifestations of Acute Clinical Manifestations of Acute HepatitisHepatitis
Acute HAV mostly symptomatic, especially in adults Acute HEV is most symptomatic and severe in
pregnant women Acute HCV is least symptomatic Acute HBV can present with a serum sickness-like
picture (fever, arthritis, urticaria, angioedema) Generally, symptoms improve after jaundice appears Symptoms are non specific-the viral syndrome
(fever, malaise, anorexia, RUQ pain, diarrhea, pruritis)
Acute Hepatitis-LABAcute Hepatitis-LAB Markedly elevated levels of AST/ALT (more than
500 U/L) typically occurs in acute hepatocellular injury (viral, drug-induced, ischemic)
Modest elevations (less than 300 U/L) may be seen in a variety of conditions– chronic hepatitis– infiltrative diseases– biliary obstruction– acute alcoholic hepatitis
Bilirubin and AP may or may not be elevated WBC count may show leucopenia

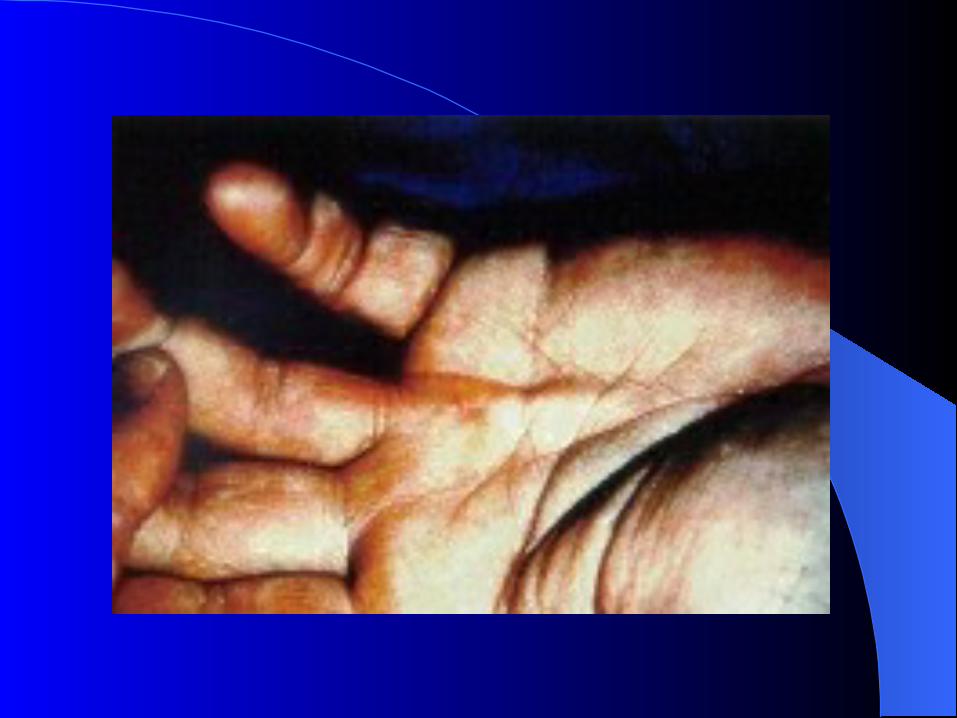
Stigmata of Chronic Liver Stigmata of Chronic Liver DiseaseDisease
Spider AgiomatasPalmar erythemaClubbing of fingersDupuytren contracturesGynecomasita (male) or breast atrophy
(female)Testicular atrophy




Incubation period: Average 25 daysRange 15-50 days
Jaundice by <6 yrs, <10%age group: 6-14 yrs, 40%-50%
>14 yrs, 70%-80% Complications: Fulminant hepatitis (0.1 %)
Prolonged Cholestasis? Autoimmune hepatitis
Chronic sequelae: None
Hepatitis A
Clinical Features
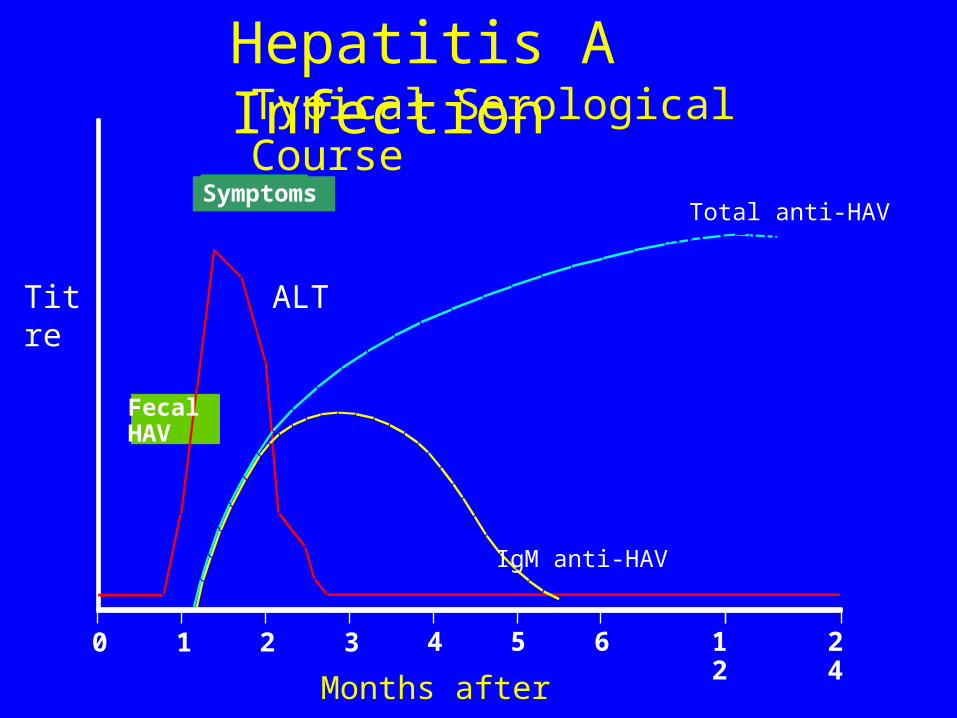
FecalHAV
Symptoms
0 1 2 3 4 5 6 12
24
Hepatitis A Infection
Total anti-HAV
Titre ALT
IgM anti-HAV
Months after exposure
Typical Serological Course
Total anti-HAV
IgM anti-HAV


Many cases occur in community-wide outbreaks– No risk factor identified for most cases– Highest attack rates in 5-14 year olds– Children serve as reservoir of infection
Persons at increased risk of infection– Travelers– Homosexual men– Injecting drug users
Hepatitis A
Vaccination StrategiesEpidemiologic Considerations
Incubation period: Average 60-90 daysRange 45-180 days
Clinical illness (jaundice): <5 yrs: <10%> 5 yrs: 30%-50%
Acute case-fatality rate: 0.5%-1% Chronic infection: <5 yrs: 30%-90%
5 yrs: 2%-10% Premature mortality from
chronic liver disease: 15%-25%
Hepatitis B
Clinical Features

Extrahepatic Manifestations of Extrahepatic Manifestations of Hepatitis BHepatitis B
Acute infection– Arthralgias– Papular acrodrmatitis (Gianotti-Crosti
syndrome)
Chronic infection– Glomerulonephritis– Arthrlalgias– Polyarteritis nodosa (PAN)

Papular acrodermatitis

PAN
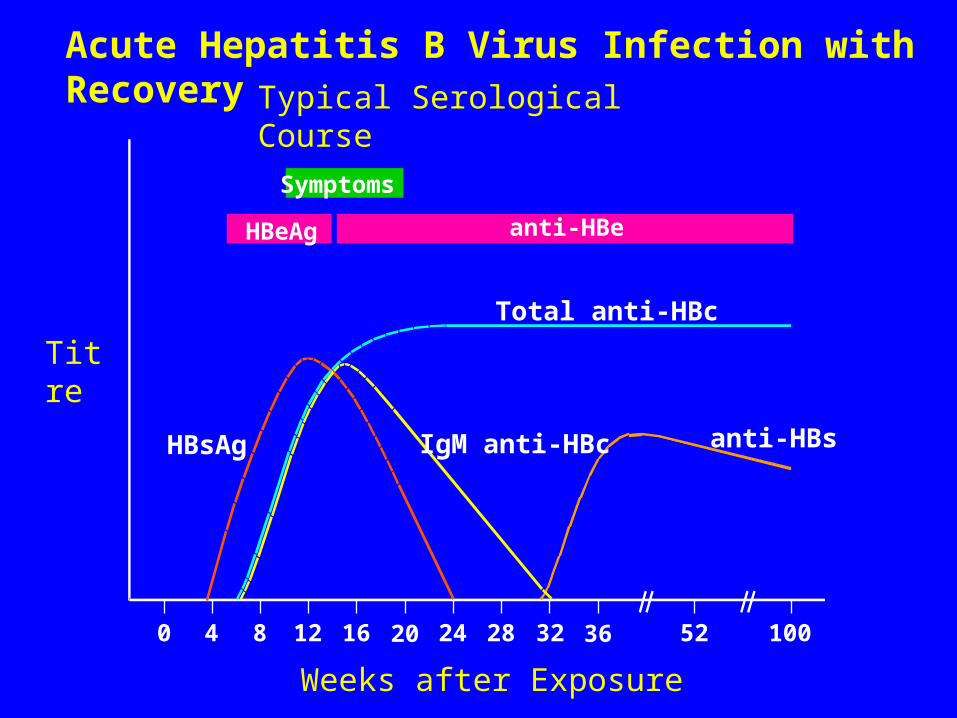
Symptoms
HBeAg anti-HBe
Total anti-HBc
IgM anti-HBc anti-HBsHBsAg
0 4 8 12 16 20 24 28 32 36 52 100
Acute Hepatitis B Virus Infection with RecoveryTypical Serological Course
Weeks after Exposure
Titre

Total anti-HBc
HBsAg
Acute(6 months)
HBeAg
Chronic(Years)
anti-HBe
0 4 8 12 16 20 24 28 32 36 52 Years
Weeks after Exposure
Titre
Progression to Chronic Hepatitis B Virus Infection Typical Serologic Course
Total anti-HBc
IgM anti-HBc
HBsAg

Symptomatic Infection
Chronic Infection
Age at Infection
Chronic Infection (%)
Sym
pto
matic In
fection
(%)
Birth 1-6 months 7-12 months 1-4 years Older Childrenand Adults
0
20
40
60
80
100100
80
60
40
20
0
Outcome of Hepatitis B Virus Infection
by Age at Infection
Ch
ron
ic In
fect
ion
(%
)


High ModerateLow/Not
Detectable
blood semen urineserum vaginal fluid feces
wound exudates saliva sweat
tearsbreastmilk
Concentration of Hepatitis B Virus in Various Body Fluids
Sexual – promiscous heterosexuals and homosexuals are particular at risk
Parenteral - IVDA, Health Workers are at increased risk
Perinatal - Mothers who are HBeAg positive are much more likely to transmit to their offspring than those who are not. Perinatal transmission is the main means of transmission in high prevalence populations
Hepatitis B Virus
Modes of Transmission
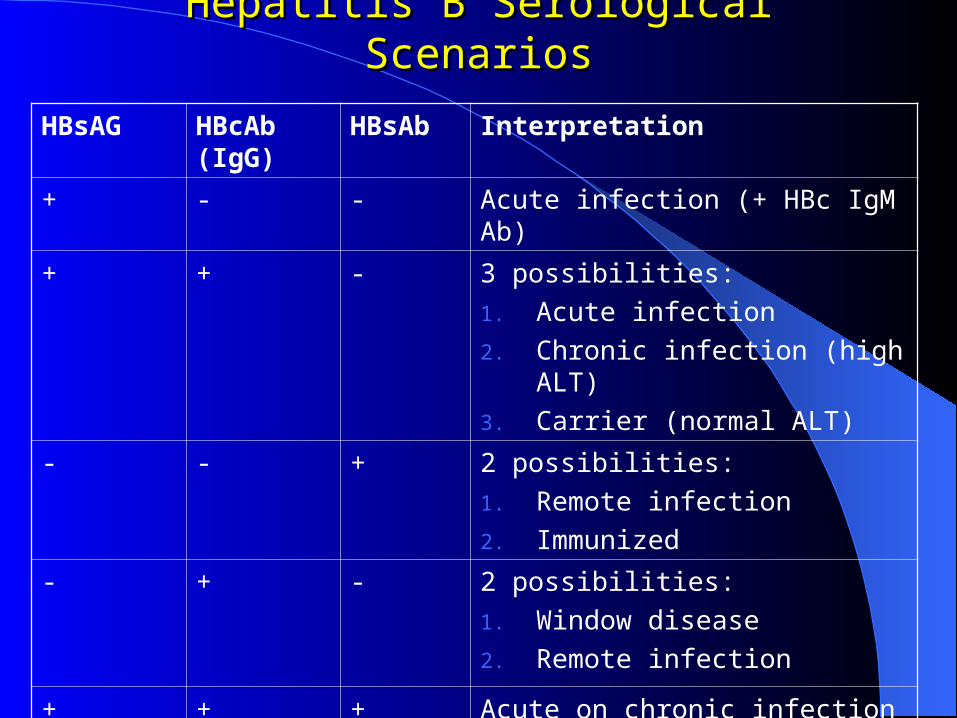
Hepatitis B Serological ScenariosHepatitis B Serological Scenarios
HBsAG HBcAb (IgG)
HBsAb Interpretation
+ - - Acute infection (+ HBc IgM Ab)
+ + - 3 possibilities:
1. Acute infection
2. Chronic infection (high ALT)
3. Carrier (normal ALT)
- - + 2 possibilities:
1. Remote infection
2. Immunized
- + - 2 possibilities:
1. Window disease
2. Remote infection
+ + + Acute on chronic infection
PreventionPrevention
Vaccination - Vaccine can be given to those who are at increased risk of HBV infection such as
– health care workers
– neonates as universal vaccination in many countries. 3 doses are given (at 0,1,and 6 months)
Hepatitis B Immunoglobulin - efficacious within 48 hours of the incident. It may also be given to neonates who are at increased risk of contracting hepatitis B i.e. whose mothers are HBsAg and HBeAg positive
Other measures - screening of blood donors, blood and body fluid precautions
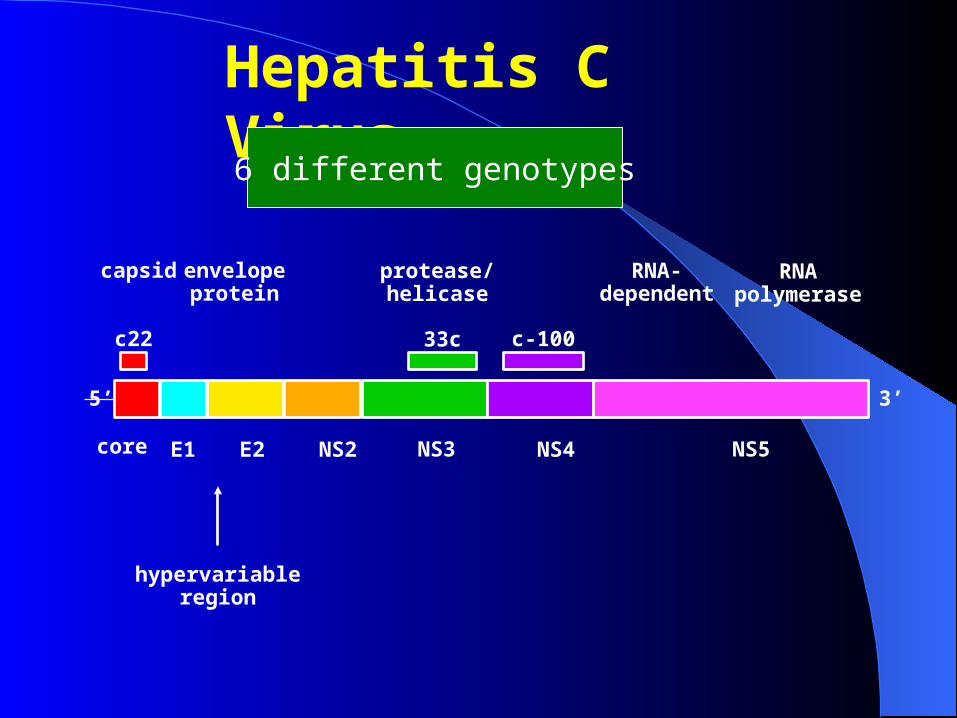
hypervariableregion
capsid envelope
protein
protease/helicase
RNA-dependent
RNA polymerase
c22
5’
core E1 E2 NS2 NS3
33c
NS4
c-100
NS5
3’
Hepatitis C Virus
6 different genotypes
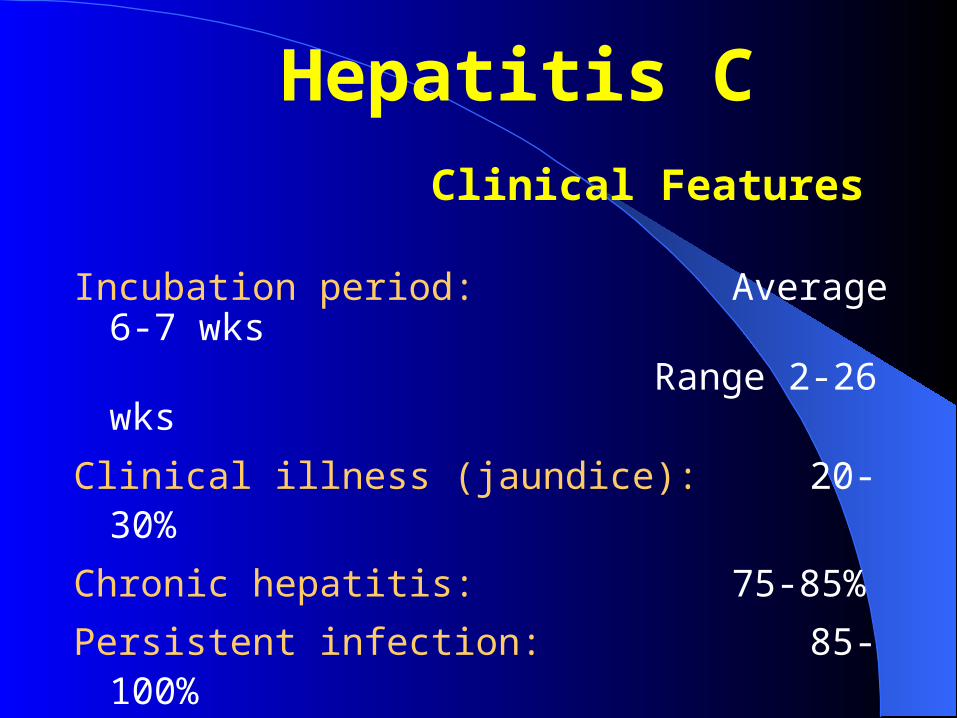
Incubation period: Average 6-7 wks
Range 2-26 wks
Clinical illness (jaundice): 20-30%
Chronic hepatitis: 75-85%
Persistent infection: 85-100%
Immunity: No protective antibody
response identified
Hepatitis C Clinical Features
Extrahepatic Manifestations of Extrahepatic Manifestations of Hepatitis CHepatitis C
Mixed cryoglobulinemia– Vasculitis– non-deforming arthritis– membranous glomerulonepgritis
Porphyria cutanea Sjogren-like syndrome

Porphyria cutanea tarda
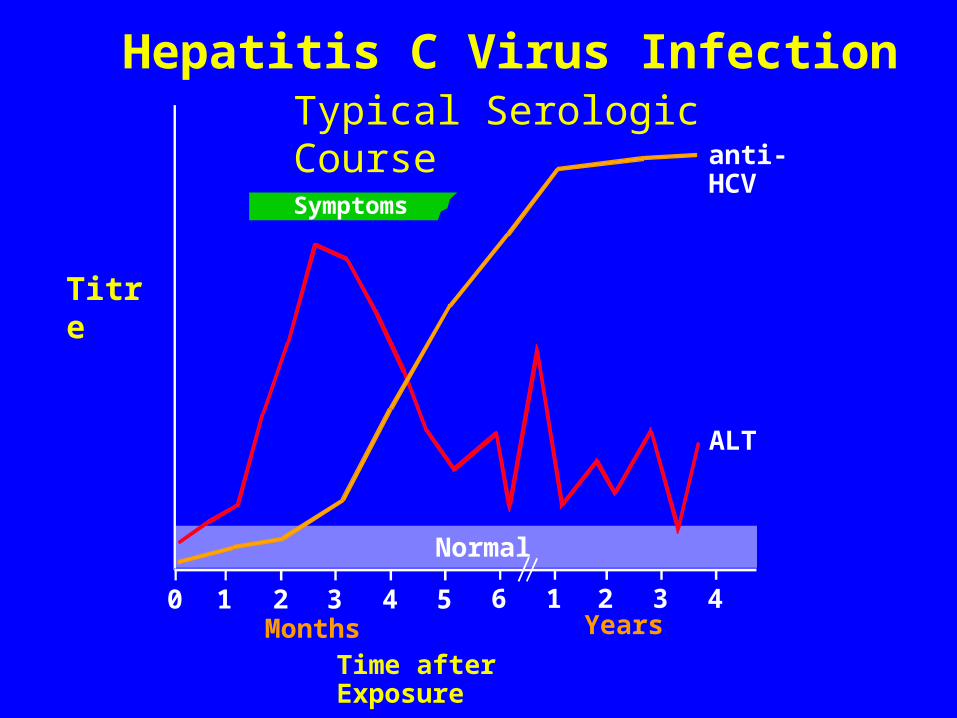
Symptoms
anti-HCV
ALT
Normal
0 1 2 3 4 5 6 1 2 3 4
Hepatitis C Virus InfectionTypical Serologic Course
Titre
Months Years
Time after Exposure
Transfusion or transplant from infected donor
Injecting drug use
Hemodialysis (yrs on treatment)
Accidental injuries with needles/sharps
Sexual/household exposure to anti-HCV-positive contact
Multiple sex partners
Birth to HCV-infected mother
Risk Factors Associated with Transmission of HCV
Laboratory DiagnosisLaboratory Diagnosis
HCV antibody - generally used to diagnose hepatitis C infection. Not useful in the acute phase as it takes at least 4 weeks after infection before antibody appears.
HCV-RNA - various techniques are available e.g. PCR and branched DNA. May be used to diagnose HCV infection in the acute phase. However, its main use is in monitoring the response to antiviral therapy.
HCV-antigen - an EIA for HCV antigen is available. It is used in the same capacity as HCV-RNA tests but is much easier to carry out.

Screening of blood, organ, tissue donors
High-risk behavior modification
Blood and body fluid precautions
Prevention of Hepatitis C
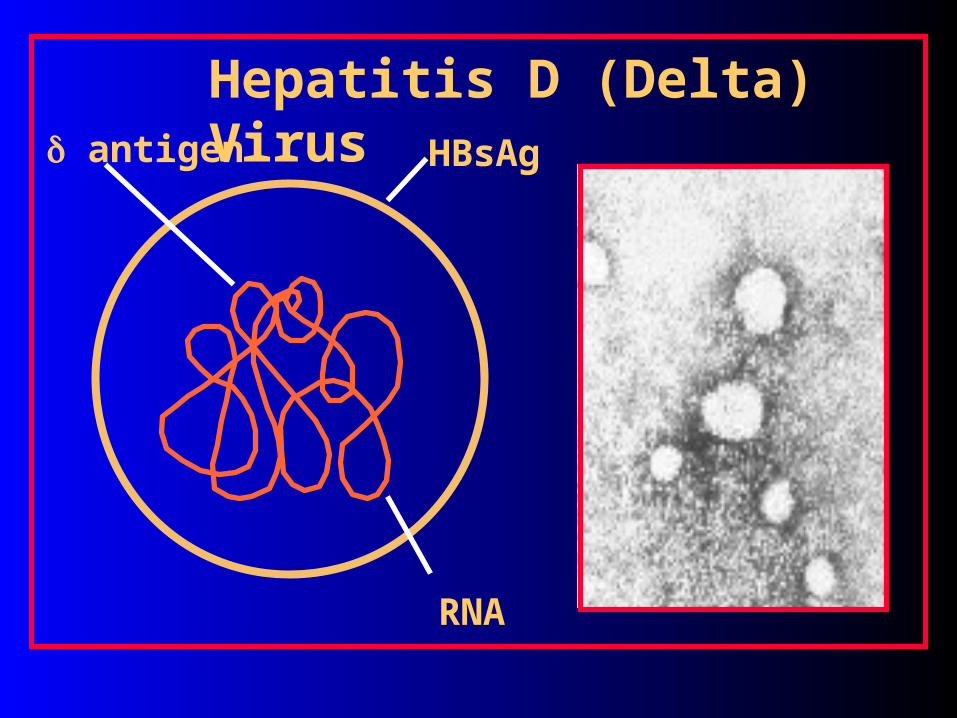
HBsAg
RNA
antigen
Hepatitis D (Delta) Virus

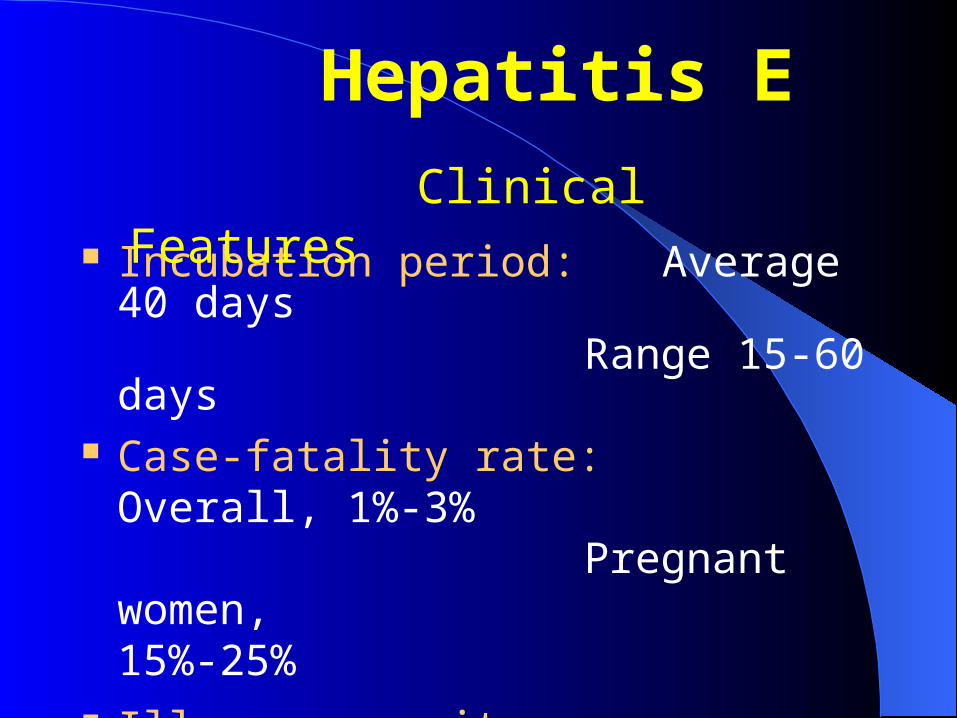
Incubation period: Average 40 days
Range 15-60 days Case-fatality rate: Overall, 1%-3%
Pregnant women, 15%-25%
Illness severity: Increased with age
Chronic sequelae: None identified
Hepatitis E
Clinical Features
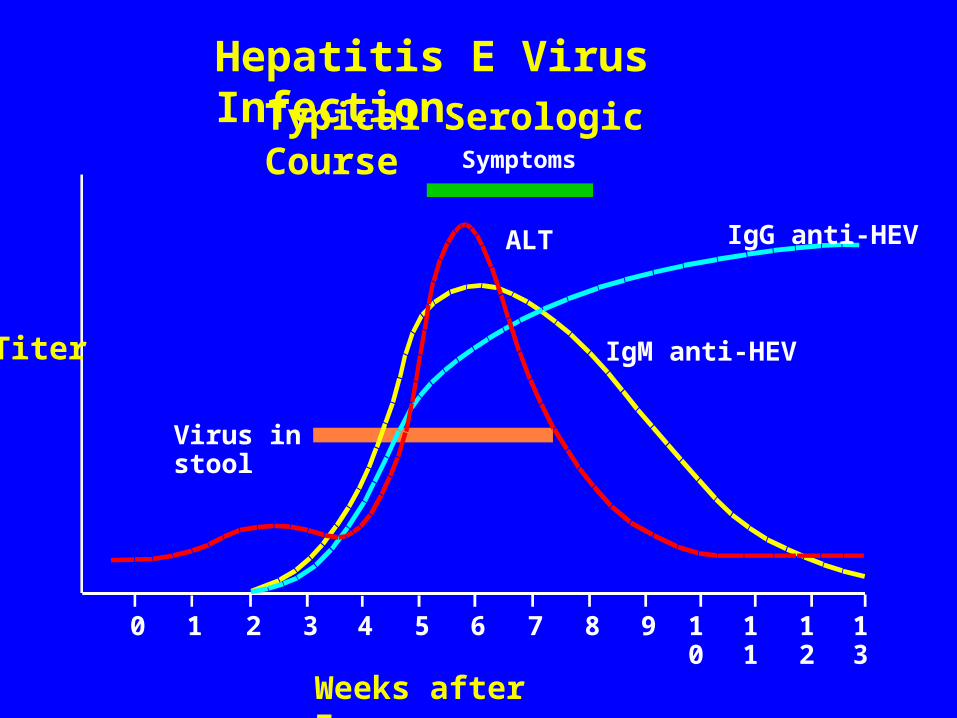
Symptoms
ALT IgG anti-HEV
IgM anti-HEV
Virus in stool
0 1 2 3 4 5 6 7 8 9 10
11
12
13
Hepatitis E Virus InfectionTypical Serologic
Course
Titer
Weeks after Exposure
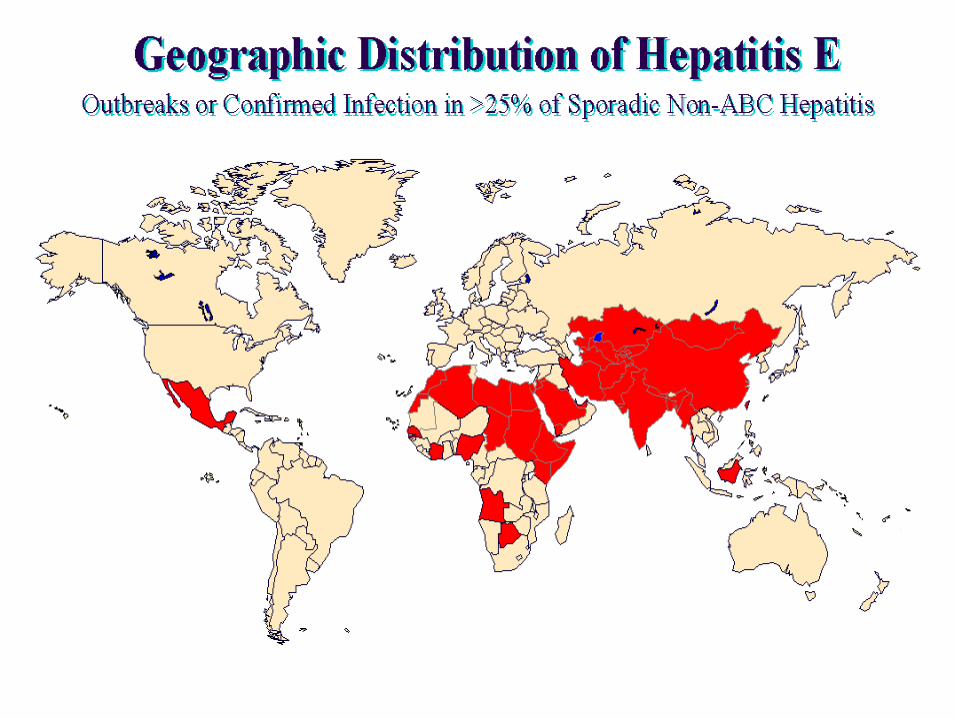
Most outbreaks associated with faecally contaminated drinking water
Several other large epidemics have occurred since in the Indian subcontinent and the USSR, China, Africa and Mexico
Minimal person-to-person transmission
Hepatitis E
Epidemiologic Features
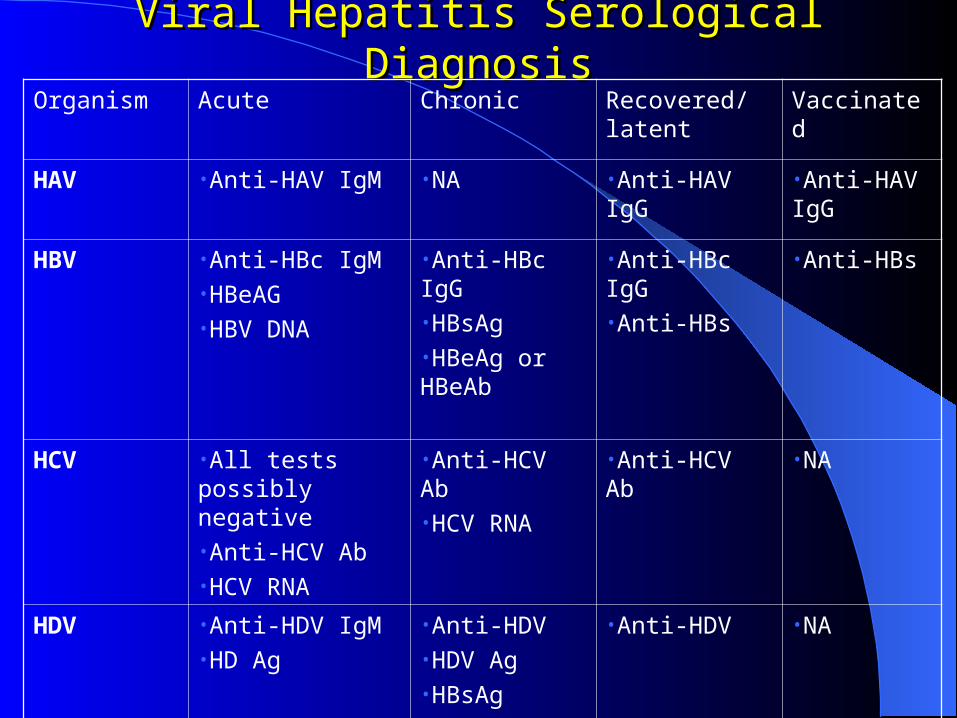
Viral Hepatitis Serological DiagnosisViral Hepatitis Serological DiagnosisOrganism Acute Chronic Recovered/latent Vaccinated
HAV •Anti-HAV IgM •NA •Anti-HAV IgG •Anti-HAV IgG
HBV •Anti-HBc IgM•HBeAG•HBV DNA
•Anti-HBc IgG•HBsAg•HBeAg or HBeAb
•Anti-HBc IgG•Anti-HBs
•Anti-HBs
HCV •All tests possibly negative•Anti-HCV Ab•HCV RNA
•Anti-HCV Ab•HCV RNA
•Anti-HCV Ab •NA
HDV •Anti-HDV IgM•HD Ag
•Anti-HDV•HDV Ag•HBsAg
•Anti-HDV •NA
Thank You !and……get vaccinated!!