8. the Anatomy and Histolog..
8
Ski p to content Ski p to search - Accesskey = s DOTE Anatomy topics 8. The anatomy and histology of the tr achea and lung. The d evelopment of the respiratory tract. Posted in Thorax by Sahaja on December 8, 2008 8. The anatomy and histology of the trachea and lung. The development of the respiratory tract. Lung - Parts, surfaces, function, a/v Lung - Part s, Impressi ons 8. The anatom y and histology of the trach ea and lung. The de velopme nt of t... ht tp://anatom yt opics.wordpress.com/2008/12/08/8-the-an atom y-an d-histo... 1 of 11 1/31/2010 10:12 AM
Transcript of 8. the Anatomy and Histolog..

8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 1/8
Skip to content
Skip to search - Accesskey = s
DOTE Anatomy topics
8. The anatomy and histology of the trachea and lung. The development of therespiratory tract.
Posted in Thorax by Sahaja on December 8, 2008
8. The anatomy and histology of the trachea and lung. The development of the respiratory tract.
Lung - Parts, surfaces, function, a/v
Lung - Parts, Impressions
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a
1 1/31/2010 1
8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 2/8
Lung - lymph, nerves, development
Lung 2 - development, action
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a
1 1/31/2010 1

8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 3/8
Anatomy of the trachea and lung
Trachea:
fibrocartilaginous tube supported by incomplete hyaline cartilage rings
back of ring is completed by trachealis m
Location: from lower end of larynx @ C6 –> Sternal angle @ border b/w T4-5, in superior mediastinum
Topography:
lat to trachea = common carotid a, lobes of thyroid glands,
below the thyroid isthmus = jugular arch, inf thyroid v
R to trachea = brachicephalic thrunk
Trachea bifurcates @ level of sternal angle
R bronchus – wider, shorter and runs more vertically than L
L bronchus – passes inf to arch of aorta and ant to esophagus and thoracic aorta
Lung
Location:
Surface Projection:
R lung:
Apex @ parasternal line , 2 fingers above clavicle
descends till body of 5th rib, then runs lat to make inf border
L lung:
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a
1 1/31/2010 1

8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 4/8
Apex @ parasternal line , 2 fingers above clavicle (Instead of parasternal line, some would prefer that you say,1/3 of
the way b/w midline and mid clavicular line)
@ 4th rib, goes a littl lateral , and then comes back towards midline @ 6th rib = cardiac impressions
Inf border of both lungs:
parasternal line = top of 6th rib
@ midinguinal line = bottom of 6th rib
@ant axillary line = body of 7th rib
@ mid axillary line = body of 8th rib
@post axillary line = body of 9th rib@ para vertebral line = 11th rib
Function: major organs of respiration
Inspiration
Musc = Diaphragm, Ext/Int/Innermost IC m, SCM, Levator scapulae, Serratus Ant, Scalenus m, Pectoral Major & Minor,
Levator costarum, Serratus Post sup m
Action
1. Diaphragm contracts (inc vert diameter of thorax)
2. Pleural cavity & lung expands – dec intrapulmonary pressure (neg) –> air rushes into lungs passively as result of
atmospheric pressure3. Forced inspiration – involves contraction of IC m & elevation of ribs (superiolat movement) w/ sternum moving ant
(bucket handle movement), Ribs move up and ant –> results in inc transverse and antero-post diameteres of thoracic cavity
Ab volume is decreased as ab pressure is increased
Expiration
Musc = m of ant ab wall, int IC m, serratus post inf m
Action
1. Overall process – involves relaxation of diaphragm, int IC m, and other m
dec in thoracic volume, inc in intrathoracic pressure, Ab pressure decreased & ribs depressed
2. Elastic recoil of Lungs – produces subatmospheric pressure in pleural cavities –> much of air is expelled
3. Forced Expiration – contraction of ant ab m and int IC m
* Quiet inspiration results from movement of diaphram mainly,
* Quiet expiration is passive process caused by elastic recoil of lungs
Parts:
Apex – projects into scalenus tent , 1-2cm above clavicle, poorly ventilated
Base – rest on diaphragm, lowers in inspiration, rises in expiration
Root – place where a/v/n, main bronchi enter lung, one place NOT covered by pleura
= main bronchus, pul a/v, bronchial a/v,lymph vessles, Hilus lymph nodes, Pulmonary plexus
root of lung w/in sleeve of pleura = mesopneumonium (mesentary of lung),
unites around root to form pulmonary ligament , that runs inferiorly and attaches to the diaphragm
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a
1 1/31/2010 1
8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 5/8
Topography
Surfaces:
1. Costal surfaces - faces the ribs, sternum, costal cartilages, intercostal m
has costal pleura b/w it and ant thoracic wall,
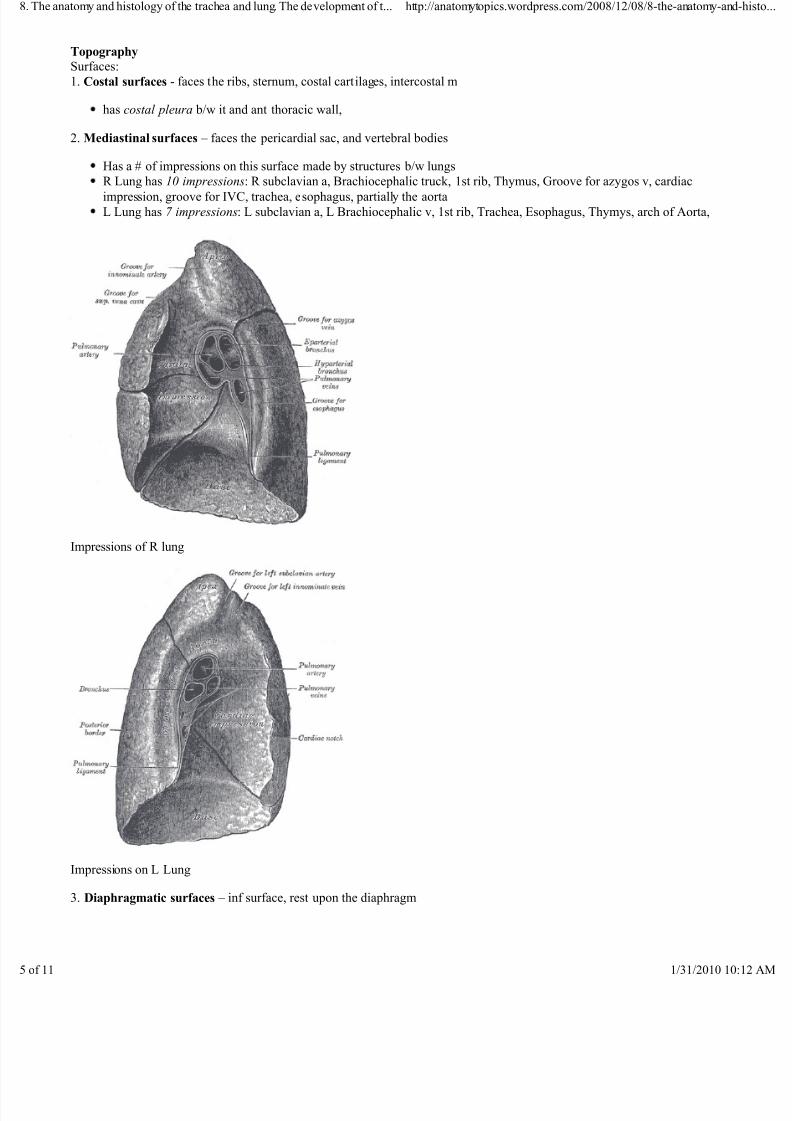
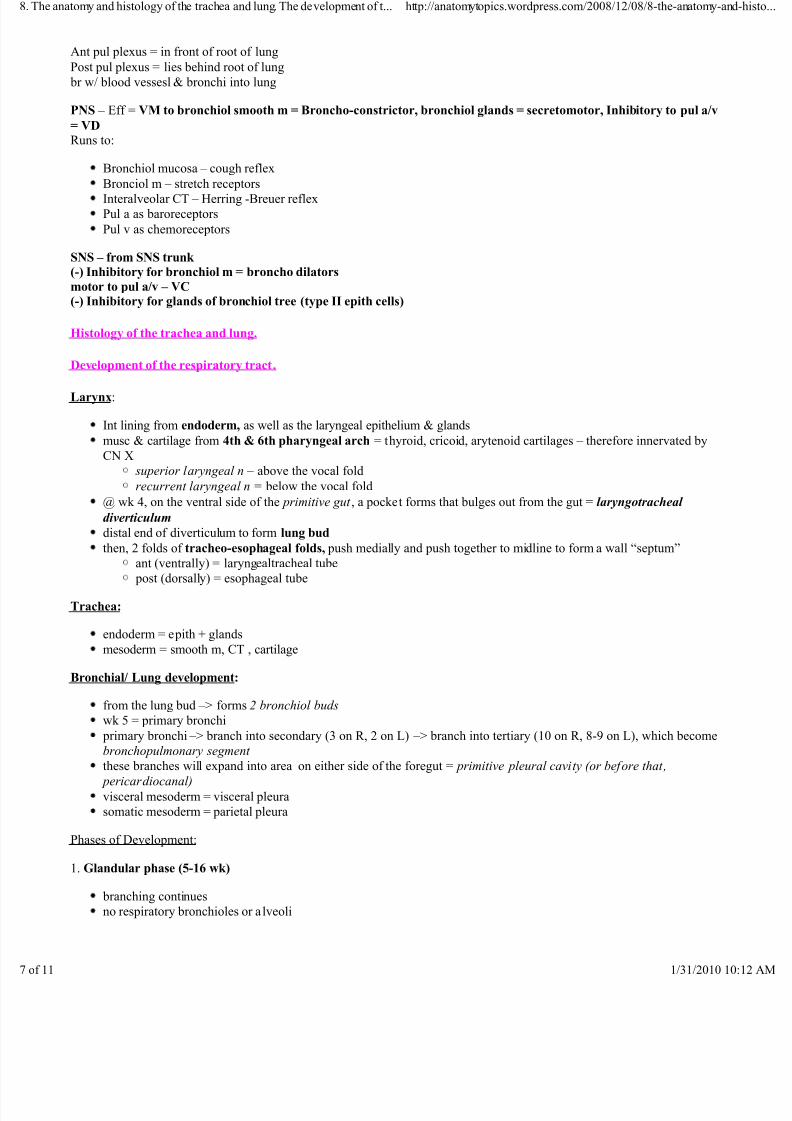
2. Mediastinal surfaces – faces the pericardial sac, and vertebral bodies
Has a # of impressions on this surface made by structures b/w lungs
R Lung has 10 impressions: R subclavian a, Brachiocephalic truck, 1st rib, Thymus, Groove for azygos v, cardiac
impression, groove for IVC, trachea, esophagus, partially the aorta
L Lung has 7 impressions: L subclavian a, L Brachiocephalic v, 1st rib, Trachea, Esophagus, Thymys, arch of Aorta,
Impressions of R lung
Impressions on L Lung
3. Diaphragmatic surfaces – inf surface, rest upon the diaphragm
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a
1 1/31/2010 1

8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 6/8
The R lung has deeper impression, due to the dome of diaphragm on R side being higher w/ liver underneath it.
Structure:R Lung has 3 lobes, and L lung has 2 lobes
The 3 lobes of R are made of the horizontal and oblique fissure, and the L has just the oblique fissure
The anatomical, functional and structural unit of the Lung = BronchoPulmonary Segment
each BP segment has:
a tertiary bronchus,
segmental br of pul a/v,
bronchiol a
pyramid structure w/ apex facing root, and base facing external surface
surgically removable w/o disrupting surrounding tissue
Pul acinus – structural unit w/ alveolar sac of 1 terminal bronchiole
Blood Supply of Lung:
Vasa Publica – pul a/v, called the respiratory circuit = CO2/O2 exchange
Pul Trunk = BP < aorta, covered by pericardium, extends from infundibulum of R ventricle = conus arteriosus
R pul a - behind asc aorta & SVC and ant to R bronchus
L pul a – connected to aorta via ligamentum arteriosum, remnant of ductus arteriosus, & shorter, narrower than R pul a
Pul v - intersegmental in drainage, leave lung as 5 pul v (1 for each lobe), but R upper & middle join so only 4 –> heart
Vasa Privata – bronchiol a/v, called the systemic circuit = supply viscera of lung itself
Bronchiol a – O2 –> visceral lungs & pleura,
connects to pul a that arises from aorta,
L bronchiol a from thoracic aorta
R bronchiol a from sup/post IC a, thoracic aorta, or L bronchiol a
Bronchiol v – rec blood from larger subdivisions of bronchi
drains to azygos v on R side, and acc hemiazygos, and hemiazygos on L side.
Acc hemiazygos –> hemiazygos v
The azygos system drains into SVC
Lymph Drainage:
Drains in 2 directions:
1. Superficial (Subserosal) lymph vessels = Superficial lymph plexus
drain surface and regions close to surface
runs on surface, deep to visceral pleura
–> bronchopul lymph nodes
2. Deep (Pericanalicular) lymph vessels = Deep lymph plexus
drain lymph from deep parts of lung
run along bronchiol treedrain –> (Intra)pulmonary l.n. –> bronchopul lymph nodes
1. Pulmonary nodes –> 2 Bronchopulmonary –> 3. Sup/Inf tracheobronchiol nodes –> 4. Paratracheal nodes –>
5. Bronchomediastinal nodes & trunks @ birfucation of trachea
On R side –> R lymph duct
On L side –> Thoracic duct
Both empty in respective angulus venosus
erve Supply:Pulmonary plexus - aff/eff fibers (PS pre ggl) from C X br, SS post ggl fibers from SS trunk, & cardiac plexus
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a
1 1/31/2010 1
8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 7/8
Ant pul plexus = in front of root of lung
Post pul plexus = lies behind root of lung
br w/ blood vessesl & bronchi into lung
PS – Eff = VM to bronchiol smooth m = Broncho-constrictor, bronchiol glands = secretomotor, Inhibitory to pul a/v
= VDRuns to:
Bronchiol mucosa – cough reflex
Bronciol m – stretch receptorsInteralveolar CT – Herring -Breuer reflex
Pul a as baroreceptors
Pul v as chemoreceptors
SS – from SS trunk (-) Inhibitory for bronchiol m = broncho dilators
motor to pul a/v – VC(-) Inhibitory for glands of bronchiol tree (type II epith cells)
Histology of the trachea and lung.
Development of the respiratory tract.
Larynx:
Int lining from endoderm, as well as the laryngeal epithelium & glands
musc & cartilage from 4th & 6th pharyngeal arch = thyroid, cricoid, arytenoid cartilages – therefore innervated by
CN X
superior laryngeal n – above the vocal fold
recurrent laryngeal n = below the vocal fold
@ wk 4, on the ventral side of the primitive gut , a pocket forms that bulges out from the gut = laryngotracheal
diverticulum
distal end of diverticulum to form lung bud
then, 2 folds of tracheo-esophageal folds, push medially and push together to midline to form a wall “septum”
ant (ventrally) = laryngealtracheal tube post (dorsally) = esophageal tube
Trachea:
endoderm = epith + glands
mesoderm = smooth m, CT , cartilage
Bronchial/ Lung development:
from the lung bud –> forms 2 bronchiol buds
wk 5 = primary bronchi
primary bronchi –> branch into secondary (3 on R, 2 on L) –> branch into tertiary (10 on R, 8-9 on L), which become
bronchopulmonary segment these branches will expand into area on either side of the foregut = primitive pleural cavity (or before that,
pericardiocanal)
visceral mesoderm = visceral pleura
somatic mesoderm = parietal pleura
Phases of Development:
1. Glandular phase (5-16 wk)
branching continues
no respiratory bronchioles or a lveoli
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a
1 1/31/2010 1

8/13/2019 8. the Anatomy and Histolog..
http://slidepdf.com/reader/full/8-the-anatomy-and-histolog 8/8
future airways are narrow with little lumens and a pseudostratified squamous epithelium.
embedded within a rapidly proliferating mesenchyme.
The structure has a glandular appearance.
NO SURVIVAL
2. Canalicular phase (13/16 – 26 wk)
beginning of respiratory bronchiole formation
primitive alveoli begin to form (terminal sacs)
Increased # a/v & capillaries start forming =extensive angiogenisis within the mesenchyme to form a dense capillarynetwork.
Diameter of the airways increases with a consequent decrease in epithelial thickness to a more cuboidal structure.
Terminal bronchioles branch to form several orders of respiratory bronchioles.
Differentiation of the mesenchyme progresses down the developing respiratory tree, giving rise to chondrocytes,
fibroblasts and myoblasts.
RARE SURVIVAL
3. Terminal Sac phase (wk 24/26 – birth)
terminal sacs form
capillaries branching forming around terminal sac
# sacs and a/v increased enormously
Continued thinning of the stroma brings the capillaries right next to alveoliFunctional type-II pneumonocytes differentiate via several intermediate stages from pluripotent epithelial cells in the
prospective alveoli.
Type I pneumonocytes differentiate from cells with a type-II like phenotype.
These cells then flatten, increasing the epithelial surface area by dilation of the saccules, giving rise to immature
alveoli.
Type I & II pneumocytes seen – beginning of Blood brain barrier
CAN SURVIVE
4. Alveolar phase (wk 28/29 – 8 yrs)
mature alveoli continue to form till well developed
continue into childhood
Mature Blood Air Barrier forms
leave a comment
« 7. The anatomy, histology and development of the pharynx, larynx and thyroid gland.
9. The valves of the heart. The histology and development of the heart. »
Leave a Reply
e anatomy and histology of the trachea and lung. The development of t... http://anatomytopics.wordpress.com/2008/12/08/8-the-anatomy-a