7TH ANNUAL CHAIR SUMMIT - neurosciencecme.comneurosciencecme.com/chairsummit/PDF/CH007-day2... ·...
40
#CHAIR2014 Sponsored by September 11 – 13, 2014 | Westin Tampa Harbour Island CHAIR SUMMIT 7TH ANNUAL Master Class for Neuroscience Professional Development
Transcript of 7TH ANNUAL CHAIR SUMMIT - neurosciencecme.comneurosciencecme.com/chairsummit/PDF/CH007-day2... ·...

#CHAIR2014
Sponsored by
September 11 – 13, 2014 | Westin Tampa Harbour Island
CHAIR SUMMIT7TH ANNUAL
Master Class for Neuroscience Professional Development

#CHAIR2014
Improving Quality of Life and Functioning in Patients with Narcolepsy
W. Vaughn McCall, MD, MS The Medical College of Georgia Georgia Regents University Augusta, GA

W. Vaughn McCall, MD, MS
● Research/Grants: National Institutes of Health, Merck & Co.
● Consultant: Merck & Co.; Otsuka America Pharmaceutical, Inc.
● Other Financial Interest: Honoraria from Wolters Kluwer Publishing
Disclosures

#CHAIR2014
Implement the appropriate objective and subjective tools to make an accurate diagnosis of narcolepsy
Learning Objective 1

#CHAIR2014
Establish a treatment plan for patients with narcolepsy that addresses all aspects of the disorder, including excessive daytime sleepiness, cataplexy, and disturbed nighttime sleep
Learning Objective 2

Prevalence of Narcolepsy
Sleepiness or fatigue, a common symptom of narcolepsy, is also a common complaint for which
patients seek care from many types of care providers.
1. Silber MH, et al. Sleep. 2002;25(2):197-202. PMID: 11902429. 2. Longstreth WT Jr, et al. Sleep. 2007;30(1):13-26. PMID:17310860.
General Population 1 in 10,000
prevalence rate1
Sleep Center Population
1 in 20 5%2
No significant gender differences

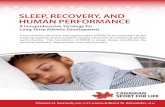
Age of Onset of Symptoms vs. Age of Diagnosis
0
50
100
150
200
250
300
350
400
Symptom onset (n = 992)
Narcolepsy diagnosis (n = 1,029)
Adapted from Thorpy M, Krieger A. Sleep Med. 2014:15(5):502-507.PMID: 24780133.
Num
ber o
f res
pond
ents
Age

Gaps in Understanding and Diagnosing Narcolepsy
● Awareness and Knowledge in Narcolepsy (AWAKEN) survey ! Surveyed 100 sleep specialists and 300 primary care
physicians (PCPs) ! Only 9% of PCPs and 42% of sleep specialists
reported that they are comfortable diagnosing narcolepsy
! Nearly one quarter (22%) of sleep specialists reported they are “not very or not at all comfortable” diagnosing the disorder
Rosenberg R, Kim A. Postgrad Med. 2014;126(1)78-86. PMID: 24393754.

Narcolepsy Misdiagnosis and Delayed Diagnosis
● Patients’ Journeys to a Narcolepsy Diagnosis survey ● 75 expert neurologists, pulmonologists, and psychiatrists
completed a survey using data from the charts of 252 patients with narcolepsy
● Results were that: ! 60% of patients had been misdiagnosed with other
disorders such as depression, insomnia, and/or obstructive sleep apnea before receiving the appropriate narcolepsy diagnosis
! 67% of patients saw multiple providers before receiving a narcolepsy diagnosis
Carter LP, et al. Postgrad Med. 2014;126(3):216-224. PMID: 24918805.

Delayed Diagnosis = Delayed Treatment
● Substantial economic burden ● Decreased productivity ! Mislabeled as lazy or work shy
● Decreased academic performance ● Social and relationship difficulties ● Increased motor vehicle and workplace
accidents ● Decreased functioning and quality of life Thorpy M, Krieger A. Sleep Med. 2014:15(5):502-507.PMID: 24780133.

Burden of Narcolepsy Disease (BOND) Study
● Data from ~9,000 patients with narcolepsy, each with at least five consecutive years of health care data and 46,000 matched control patients
● Key findings: Patients with narcolepsy with or without cataplexy ! Are more likely to experience medical comorbidities ! Are more likely to experience psychiatric
comorbidities, such as anxiety and mood disorders ! Have more than twice the mean annual medical costs
than the general population
Black J, et al. Sleep Med. 2014;15(5):522-529. PMID: 24768358.

Individuals with Narcolepsy Have a Complex Medical History ● Narcolepsy is associated with an approximately
1.5-fold excess mortality compared to the general population1
● Most of the participants (n = 320) with narcolepsy had at least one medical condition or a psychiatric disorder that required treatment2
● High incidence of obesity and sleep apnea put individuals at a greater risk for developing cardiovascular disease
● Significant medical risk if narcolepsy individuals remain undiagnosed or misdiagnosed
1. Ohayon MM, et al. Sleep. 2014;37:439-444. PMID: 24587565. 2. Ohayon MM. Sleep Med. 2013;14(6):488-492. PMID: 23643648.

The Narcolepsy “Tetrad”
● Excessive daytime sleepiness (EDS) ● Cataplexy: Sudden-onset bilateral, axial
muscle weakness, often triggered by strong emotions
● Hypnagogic auditory or visual hallucinations (i.e., at the beginning or end of sleep)
● Sleep paralysis: Inability to move shortly after awakening
Kumar S, Sagili H. J Clin Diagn Res. 2014;8(2):190-195.

Narcolepsy Symptoms
● EDS and cataplexy are the primary symptoms—EDS often most disabling ● Cataplexy onset occurs within 5 years of
EDS in 2/3 of cases ! Cataplexy may occur many years later ! Cataplexy is pathognomonic of narcolepsy
● Mean onset of sleep paralysis and hypnagogic hallucinations 2 – 7 years after onset of EDS
Nishino S. Sleep Med. 2007;8(4):373-399. PMID: 17470414.

Symptoms That Impact Daily Functioning
● 2013 Unite Narcolepsy survey (N = 1,330) found that the three symptoms that had the greatest impact on patients’ lives were: ! Excessive sleepiness: 77% ! Cognitive symptoms—difficulty thinking,
remembering, concentrating or paying attention: 50%
! General fatigue/never feeling rested: 45%
Unite Narcolepsy: Patient Focused Narcolepsy Survey. http://www.unitenarcolepsy.org/wp-content/uploads/Interim-Survey-Analysis-v1.pdf. Accessed September 2, 2014.

Wakefulness/Sleep Neurophysiology
Saper CB, et al. Nature. 2005;437:1257-1263. PMID: 16251950.

Narcolepsy Orexin Neurons
Thannickal TC, et al. Neuron. 2000;27(3):469-474. PMID: 11055430.

Differential Diagnosis of Excessive Daytime Sleepiness (EDS) ● Sleep deprivation, insufficient time in bed ● Another sleep disorder
! Obstructive sleep apnea (OSA) ! Periodic limb movement disorder (PLMD)
● Poor sleep quality due to illness (CHF) ● Medications, drugs, toxins ● Depression ● Delayed sleep-phase syndrome ● Idiopathic hypersomnia

ICSD-3 Diagnostic Criteria for Narcolepsy
Criteria A and B must be met A. The patient has daily periods of irrepressible need to
sleep or daytime lapses into sleep which occur for at least 3 months
B. The presence of 1 or both of the following 1. Cataplexy and a mean sleep latency < 8 min and 2 or more
SOREMPs on an MSLT performed according to standard techniques. A SOREMP (within 15 min of sleep onset) on the preceding nocturnal polysomnography may replace 1 of the SOREMPS on the MSLT
2. CSF hypocretin 1 concentrations measured by immunoreactivity either less than 110 pg/mL or less than one third of mean values obtained in normal individuals with the same assay
Type 1 Narcolepsy
International Classification of Sleep Disorders, 3rd ed, American Academy of Sleep Medicine, Darien, IL 2014.

ICSD-3 Diagnostic Criteria for Narcolepsy
● All of the following criteria must be met: ! The patient has daily periods of irrepressible need to sleep or
daytime lapses into sleep occurring for at least 3 months ! Mean sleep latency < 8 min and 2 or more SOREMPs on an
MSLT performed according to standard techniques. A SOREMP (within 15 min of sleep onset) on the preceding nocturnal polysomnography may replace 1 of the SOREMPS on the MSLT
! Cataplexy is absent ! Either CSF hypocretin 1 concentrations measured by
immunoreactivity either less than 110 pg/mL or less than one third of mean values obtained in normal individuals with the same assay
! Hypersomnia and/or MSLT findings are not better explained by another sleep disorder, medical or neurologic disorder, mental disorder, medication use or substance withdrawal
Type 2 Narcolepsy
International Classification of Sleep Disorders, 3rd ed, American Academy of Sleep Medicine, Darien, IL 2014.

DSM-5 Diagnostic Criteria for Narcolepsy 1. Recurrent periods of an irrepressible need to sleep, lapsing into
sleep, or napping occurring within the same day. These must have been occurring at least 3 times per week during the last 3 months.
2. The presence of at least 1 of the following A. Episodes of cataplexy, defined as either of the following occurring at
least a few times per month: ! In individuals with long-standing disease, brief (seconds to minutes)
episodes of sudden bilateral loss of muscle tone with maintained consciousness that are precipitated by laughter or joking
! In children or in individuals within 6 month of onset, spontaneous grimaces or jaw-opening episodes with tongue thrusting or a global hypotonia, without any obvious emotional triggers
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.) Arlington, VA: American Psychiatric Publishing.

DSM-5 Diagnostic Criteria for Narcolepsy
2. The presence of at least 1 of the following B. Hypocretin deficiency, as measured using CSF
hypocretin 1 immunoreactivity values (less than one third of values obtained in health individuals tested using the same assay, or 110pg/mL or less; low CSF levels of hypocretin 1 must not be observed in the context of acute brain injury, inflammation or infection)
C. Nocturnal sleep polysomnography showing REM sleep latency of 15 minutes or less, or a MSLT showing a mean sleep latency of 8 minutes or less and 2 or more SOREMPs
American Psychiatric Association. (2013). Diagnostic and Statistical Manual of Mental Disorders (5th ed.) Arlington, VA: American Psychiatric Publishing.

Making the Diagnosis: Assessing Sleepiness
● Sleep history ● Sleep diary ● CSF orexin levels ● Subjective scales ! Epworth Sleepiness Scale (ESS)
● Objective testing ! Multiple sleep latency testing (MSLT) ! Maintenance of wakefulness test (MWT)
Roth T, et al. Curr Med Res Opin. 2010;26(suppl 2): S3-S24.

Narcolepsy Goals of Treatment
● Reduce daytime sleepiness ● Control ancillary symptoms ! Cataplexy ! Hallucinations ! Sleep paralysis ! Disturbed nocturnal sleep
● Improve cognitive and daily functioning ! Patient safety (e.g. motor vehicle accidents)

Management of Narcolepsy
Behavioral ● Patient and family
education ! Disease education ! Therapeutic
expectations ● Sleep hygiene ● Planned naps
! Duration and frequency
● Avoid sleep loss/circadian challenges
Pharmacologic ● Stimulants to counter
patients’ excessive daytime sleepiness
● REM suppressants to target cataplexy, hypnagogic hallucinations and sleep paralysis
● Sedatives to consolidate sleep

AASM Recommendations for the Treatment of Narcolepsy
Agent Level Recommendation Modafinil*, Armodafinil* Standard Effective for daytime sleepiness
Sodium oxybate* Standard Effective for cataplexy, daytime sleepiness, and disrupted sleep
Amphetamine*, methamphetamine*, dextroamphetamine*, methylphenidate*
Guideline Effective for daytime sleepiness
Selegiline Option May be effective for cataplexy and daytime sleepiness
Ritanserin Option May be effective for daytime sleepiness
Tricyclic antidepressants, SSRIs, and venlafaxine Guideline
May be effective treatment for sleep paralysis and hypnagogic hallucinations
*Agent is FDA approved for the treatment of symptoms associated with narcolepsy Morganthaler TI, et al. Sleep. 2007;30(12):1705-1711.

Improvement in Treatment of Narcolepsy With Stimulants
* Not FDA approved for treatment of narcolepsy Mitler MM, et al. J Clin Neurophysiol. 1990;7(1):93-118. PMID: 1968069.
0 2 4 6 8
10 12 14 16
Methylphenidate* D-Amphetamine*
MW
T (M
inut
es)
Baseline Low Dose Medium Dose High Dose
p < .05 10-30-60 mg 10-30-60 mg

Mean Change From Baseline in MWT for Morning, Afternoon, and Evening Sessions for Each Modafinil Regimen
Schwartz JR, et al. J Neuropsychiatry Clin Neurosci. 2005;17(3):405-412. PMID: 16179665.
0 2 4 6 8
10 12 14 16 18 20
0900-1100 1300-1500 1700-1900
200 mg QD 400 mg QD 400 mg Split Dose 600 mg Split Dose
Morning Afternoon Evening
*
*
* *
* * *
*
* *
*
Ŧ
Hours (Time of Day)
Ŧ
Cha
nge
in M
WT
from
Bas
elin
e (M
in)
N = 56 *p < .01; Ŧp < .05

Long-Term ESS Improvement with Modafinil in Narcolepsy
0 2 4 6 8
10 12 14 16 18 20
BL 3 6 9
ESS Score
Study Week
Double-Blind PBO MOD 200mg MOD 400mg
BL 2 8 24 40 64 88 112 136
Open-Label MOD 200-400mg
ESS = Epworth Sleepiness Scale Schwartz JR. Expert Opin Pharmacother. 2005;6:115-129.

Armodafinil for the Management of Late-Day Sleepiness (MWT)
-3
-2
-1
0
1
2
3
-1.2
1.5* 1.6 Placebo (n = 58)
Armo 150 mg (n = 58)
Armo 250 mg (n = 59)
*p < .05 vs. placebo; MWT = Maintenance of Wakefulness Harsh JR, et al. Curr Med Res Opin. 2006;22:761-774. PMID: 16684437.
Mean (SEM) Change
From Baseline in Sleep
Latency at Final Visit (min)
3 PM to 7 PM

Sodium Oxybate: Excessive Daytime Sleepiness in Narcolepsy
Xyrem International Study Group. J Clin Sleep Med. 2005(4):391-397. PMID: 17564408.
Compared to baseline, the nightly administration of sodium oxybate was associated with dose-related improvements in Epworth Sleepiness Scale scores at the end of the 8-week trial; *p < .001 compared to placebo; B = Baseline, E = End point
24 22 20 18 16 14 12 10
8 6
Epw
orth
Sle
epin
ess
Sca
le
(Med
ians
1st
/3rd
Qua
rter)
Narcolepsy Range
Normal Range
Placebo B E
4.5 g B E 4.5 g B E
6.0 g B E
9.0 g B E
* *

Sodium Oxybate: Effects on Wakefulness
-40%
-30%
-20%
-10%
0%
10%
20%
30%
Mea
n M
WT
% C
hang
e f
rom
Bas
elin
e
Sodium oxybate
Modafinil withdrawn
n = 50
Sodium oxybate
+ Modafinil
n = 54
Incr
ease
d W
akef
ulne
ss
-28%
5%
26%
ESS = 12 min*
BL = 11.3 min BL = 10.4 min
ESS = 13.2 min*
BL = 10.5 min
ESS = 9.9 min -5%
Modafinil n = 63 Placebo
Modafinil withdrawn
n = 55
BL = 9.7 min
ESS = 6.9 min
*p < .001 MWT = Maintenance of Wakefulness; BL = Baseline; ESS = Epworth Sleepiness Scale Black J, Houghton WC. Sleep. 2006;29(7):939-946. PMID: 16895262.

6 7 8 9
10 11 12 13 14
Day
time
Sle
ep L
aten
cy
(Min
utes
)
Visit 3 Visit 5 Visit 2 Visit 4
Sodium Oxybate + Modafinil Placebo Sodium Oxybate
Modafinil
Daytime Sleep Latency: Maintenance of Wakefulness
Black J, Houghton WC. Sleep. 2006;29(7):939-946. PMID: 16895262.

Side Effect and Safety Profiles
Agent Most Frequent Side Effects
Modafinil, armodafinil Headache, nausea, eosinophilia, diarrhea, dry mouth, anorexia
Sodium oxybate Headache, nausea, dizziness, nasopharyngitis, somnolence, vomiting and urinary incontinence
Dextroamphetamine, methylphenidate, amphetamine*, methamphetamine*
Insomnia, restlessness, tachycardia, psychotic episodes (rare), dizziness, diarrhea, constipation, hypertension, impotence, anorexia, nausea, hypotension, hypersensitivity reactions, headache
Tricyclic antidepressants*, SSRIs*, and venlafaxine*
Asthenia, sweating, nausea, constipation, anorexia, vomiting, somnolence, dry mouth, dizziness, nervousness, anxiety, tremor, blurred vision, abnormal ejaculation/orgasm and impotence in men, confusion, orthostatic hypotension, diet-induced hypertension
*Agent is not FDA approved for the treatment of symptoms associated with narcolepsy Littner M, et al. Sleep. 24(4):451-466. PMID: 11403530.

Future Directions in Narcolepsy
● Non-hypocretin-based therapies ! Histaminergic H3 antagonists/inverse agonists ! Antigen-specific immunopharmacology ! Melanin-concentration hormone antagonist
● Hypocretin-based therapy ! Hypocretin-1 ! Nonpeptide hypocretin agonist ! Hypocretin cell tranplantation ! Gene therapy
De la Herrán-Arita AK, Garcia-Garcia F. Drugs. 2013;73(16):1771-1781. PMID: 24122734.

Clinical Connections
● Narcolepsy is associated with significant social and economic burden
● Misdiagnosis and delayed diagnosis add to burden of narcolepsy
● Psychiatric and medical comorbidities are common ● Symptoms of narcolepsy are chronic and disabling, requiring
long-term treatment ● Sodium oxybate and modafinil/armodanifil are effective in
treating narcolepsy ● Patient education and regular follow-up to monitor treatment
response are vital to the successful management of narcolepsy

#CHAIR2014
Questions & Answers

#CHAIR2014
Reference Slides

Most Common Medical Comorbidities of Narcolepsy
ICD-10 Classification
Narcolepsy (n = 320)
Matched General Population (n = 1464)
Adjusted Odds Ratio
[95% CI]
Hypercholesterolemia 10.3% 6.8% 1.51 [1.02-2.19]***
Diseases of the digestive system 16.3% 5.0% 3.27 [2.34-4.56]*
Upper respiratory tract diseases 27.5% 10.9% 2.52 [2.00-3.17]*
Hypertension 19.2% 14.7% 1.32 [1.02-1.70]***
Heart diseases 5.9% 2.9% 2.07 [1.22-3.51]**
Ohayon MM. Sleep Med. 2013 Jun;14(6):488-492. PMID: 23643648. *p < .001, **p < .01, ***p < .05

Most Common Psychiatric Comorbidities of Narcolepsy
DSM-IV-TR Classification
Narcolepsy (n = 320)
Matched General Population (n = 1464)
Adjusted Odds Ratio
[95% CI] Major depressive
disorder 17.1% 6.4% 2.67 [1.96-3.64]*
Social anxiety disorder 21.1% 8.7% 2.43 [1.86-3.18]*
Panic disorder 12.5% 3.9% 3.23 [2.20-4.73]*
PTSD 11.3% 5.3% 2.11 [1.45-3.07]*
Bipolar disorder 8.5% 1.9% 4.56 [2.72-7.62]*
Ohayon MM. Sleep Med. 2013 Jun;14(6):488-492. PMID: 23643648. *p < .001, **p < .01, ***p < .05