7 Asthma Patho

of 50
-
Upload
sarah-zoraya-mirza -
Category
Documents
-
view
217 -
download
0
Transcript of 7 Asthma Patho
-
7/31/2019 7 Asthma Patho
1/50
Asthma
Asthma
2contacthours:$18
Authors:JoAnnO'Toole,BSNLaurenRobertson,BA,MPT
CourseSummary:Clinicalcharacteristicsofasthmaandrelatedairwayinflammation,plushostandenvironmentalfactorsthatcontributetoasthmaandtheeffectsofinterventiononthenaturalhistoryofasthmainchildrenandadults.
COI/CommercialSupport:Theplannersandauthorsofthiscoursehavedeclarednoconflictofinterestandallinformationisprovidedfairlyandwithoutbias.Wereceivednocommercialsupportforthisactivityanddonotapproveorendorseanycommercialproductsdisplayed.
Off-LabelUse:Nooff-labeluseswerediscussedorrecommendedinthiscourse.
CriteriaforSuccessfulCompletion:80%orhigherontheposttest,acompletedevaluationform,andpaymentwhererequired.Nopartialcreditwillbeawarded.
Thiscoursewasderivedfromthe2007ExpertPanelReport3(EPR3)GuidelinesonAsthma.
Thiscoursewillbereviewedeverytwoyears.ItwillbeupdatedordiscontinuedonJune1,2011.
AccreditationInformation
Nursing:ATrainEducationisanapprovedproviderofcontinuingnursingeducatio
nbytheArizonaStateNursesAssociation*(AzNA),anaccreditedapproverbytheAmericanNursesCredentialingCenter'sCommissiononAccreditation(ANCC).
*AzNAandANCCCommissiononAccreditationdonotapproveorendorseanycommercialproductsdisplayed.
PhysicalTherapy:ATrainEducationisanapprovedreviewerandproviderbythePhysicalTherapyBoardofCaliforniaandanapprovedproviderbytheNewYorkStateBoardforPhysicalTherapy.
OccupationalTherapy:ATrainEducationisanapprovedproviderbytheAmericanOccupationalTherapyAssociation.Ifyouareanoccupationaltherapistoroccupationaltherapyassistantpleasenotethefollowing:
TargetAudience:OccupationalTherapists,OTAsInstructionalLevel:IntermediateContentFocus:Category1DomainofOT,Clientfactors
-
7/31/2019 7 Asthma Patho
2/50
Otherprofessionsandaccreditations:SeetheATrainCEUAccreditationpageathttp://www.ATrainCeu.com/accreditation.php.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
3/50
Asthma
Instructions
1.Readthecoursematerialandthencompletethefollowingforms:A.PostTestB.EvaluationLearningActivityC.RegistrationForm2.Ifyouarenotpayingbycreditcard,prepareacheckfortheamountofthecoursemadeoutto:ATrainEducation,Inc.3.Mailthecompletedformsandyourpaymentto:ATrainEducation,Inc5171RidgewoodRdWillits,CA95490
Whenwereceiveyourformsandpayment,wewillmail(oremail,atyourrequest)yourcompletioncertificate.Ifyouhaveanyquestions,[email protected].
CourseObjectives
Whenyoufinishthiscourse,youwillbeableto:
Describetheclinicalcharacteristicsandpathophysiologyofasthma.OutlinethepathophysiologicmechanismsinthedevelopmentofairwayinflammationDiscussthehostandenvironmentalfactorsthatcontributetothedevelopmentofasthma.Discussthenaturalhistoryofasthmainchildrenandadults.
Summarizetheeffectofinterventionsonnaturalhistoryofasthma.ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
4/50
Asthma
Introduction
Asthmaisachronicinflammatorydiseaseoftheairways.IntheUnitedStates,asthmaaffectsmorethan22millionpersons.Itisoneofthemostcommonchronicdiseasesofchildhood,affectingmorethan6millionchildren.TherehavebeenimportantgainssincethereleaseofthefirstNationalAsthmaEducationandPreventionProgram(NAEPP)clinicalpracticeguidelinesin1991.Forexample,thenumberofdeathsduetoasthmahasdeclined,eveninthefaceofanincreasingprevalenceofthedisease;fewerpatientswhohaveasthmareportlimitationstoactivities;andanincreasingproportionofpeoplewhohaveasthmareceiveformalpatienteducation.
Hospitalizationrateshaveremainedrelativelystableoverthelastdecade,withlowerratesinsomeagegroupsbuthigherratesamongyoungchildren04yearsofage.Thereissome
indicationthatimprovedrecognitionofasthmaamongyoungchildrencontributestotheserates.However,theburdenofavoidablehospitalizationsremains.Collectively,peoplewhohaveasthmahavemorethan497,000hospitalizationsannually.Furthermore,ethnicandracialdisparitiesinasthmaburdenpersist,withsignificantimpactonAfricanAmericanandPuertoRicanpopulations.Thechallengeremainstohelpallpeoplewhohaveasthma,particularlythoseathighrisk,receivequalityasthmacare.Thiscoursepresentsadefinitionofasthma,adescriptionoftheprocessesonwhichthatdefinitionisbasedthepathophysiologyandpathogenesiso
fasthma,andthenaturalhistoryofasthma.
DefinitionofAsthma
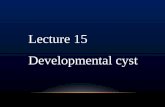
Asthmaisacommonchronicdisorderoftheairwaysthatiscomplexandcharacterizedbyvariableandrecurringsymptoms,airflowobstruction,bronchialhyper-responsiveness,andanunderlyinginflammation(Box1).Theinteractionofthesefeaturesofasthmadeterminestheclinicalmanifestationsandseverityofasthma(Figure1)andtheresponsetotreatment.This
interactioncanbehighlyvariableamongpatientsandwithinpatientsovertime.
Box1.CharacteristicsofClinicalAsthma-Symptoms
AirwayobstructionInflammation
-
7/31/2019 7 Asthma Patho
5/50
Hyper-responsivenessATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
6/50
Asthma
Figure1.TheInterplayandinteractionbetweenairwayinflammationandtheclinicalsymptomsandpathophysiologyofasthma.Adaptedfrom:http://www.nhlbi.nih.gov/guidelines/asthma/03_sec2_def.pdf
Theconceptsunderlyingasthmapathogenesishaveevolveddramaticallyinthepast25yearsandarestillundergoingevaluationasvariousphenotypesofthisdiseasearedefinedandgreaterinsightlinksclinicalfeaturesofasthmawithgeneticpatterns.Centraltothevariousphenotypicpatternsofasthmaisthepresenceofunderlyingairwayinflammation,whichisvariableandhasdistinctbutoverlappingpatternsthatreflectdifferentaspectsofthedisease,suchasintermittentversuspersistentoracuteversuschronicmanifestations.Acutesymptomsofasthmausuallyarisefrombronchospasmandrequireandrespondtobronchodilatortherapy.
Acuteandchronicinflammationcanaffectnotonlytheairwaycaliberandairflowbutalsounderlyingbronchialhyper-responsiveness,whichenhancessusceptibilitytobronchospasm.Treatmentwithanti-inflammatorydrugscan,toalargeextent,reversesomeoftheseprocesses;however,thesuccessfulresponsetotherapyoftenrequiresweekstoachieveand,insomesituations,maybeincomplete.
Forsomepatients,thedevelopmentofchronicinflammationmaybeassociatedwithpermanentalterationsintheairwaystructurereferredtoasairwayremodelingthatarenotpr
eventedbyorfullyresponsivetocurrentlyavailabletreatments.Therefore,theparadigmofasthmahasbeenexpandedoverthelast10yearsfrombronchospasmandairwayinflammationtoincludeairwayremodelinginsomepersons.
Theconceptthatasthmamaybeacontinuumoftheseprocessesthatcanleadtomoderateandseverepersistentdiseaseisofcriticalimportancetounderstandingthepathogenesis,pathophysiology,andnaturalhistoryofthisdisease.AlthoughresearchsincethefirstNAEPP
guidelinesin1991hasconfirmedtheimportantroleofinflammationinasthma,thespecificprocessesrelatedtothetransmissionofairwayinflammationtospecificpathophysiologicconsequencesofairwaydysfunctionandtheclinicalmanifestationsofasthmahaveyettobefullydefined.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
7/50
-
7/31/2019 7 Asthma Patho
8/50
Asthma
Similarly,muchhasbeenlearnedaboutthehost-environmentfactorsthatdeterminethesusceptibilityoftheairwaytotheseprocesses,buttherelativecontributionsofeither(andthepreciseinteractionsbetweenthem)thatleadstotheinitiationorpersistenceofdiseasehaveyettobefullyestablished.Nonetheless,currentscienceregardingthemechanismsofasthmaandfindingsfromclinicaltrialshasledtotherapeuticapproachesthatallowmostpeoplewhohaveasthmatoparticipatefullyinactivitiestheychoose.Aswelearnmoreaboutthepathophysiology,phenotypes,andgeneticsofasthma,treatmentswillbecomeavailabletoensureadequateasthmacontrolforallpersonsand,ideally,toreverseandevenpreventtheasthmaprocesses.
Asaguidetodescribingasthmaandidentifyingtreatmentdirections,aworkingdefinitionofasthmaputforthinthepreviousExpertPanelReportremainsvalid.Asthmaisachronic
inflammatorydisorderoftheairwaysinwhichmanycellsandcellularelementsplayarole:inparticular,mastcells,eosinophils,Tlymphocytes,macrophages,neutrophils,andepithelialcells.Insusceptibleindividuals,thisinflammationcausesrecurrentepisodesofwheezing,breathlessness,chesttightness,andcoughing,particularlyatnightorintheearlymorning.Theseepisodesareusuallyassociatedwithwidespreadbutvariableairflowobstructionthatisoftenreversibleeitherspontaneouslyorwithtreatment.Theinflammationalsocausesanassociatedincreaseintheexistingbronchialhyper-responsivenesstoavarietyofstimuli.Reversibilityo
fairflowlimitationmaybeincompleteinsomepatientswithasthma.
Thisworkingdefinitionanditsrecognitionofkeyfeaturesofasthmahavebeenderivedfromstudyinghowairwaychangesinasthmarelatetothevariousfactorsassociatedwiththedevelopmentofairwayinflammation(e.g.,allergens,respiratoryviruses,andsomeoccupationalexposures)andrecognitionofgeneticregulationoftheseprocesses.Fromthesedescriptiveapproacheshasevolvedamorecomprehensiveunderstandingofasthmapathogenesis,the
processesinvolvedinthedevelopmentofpersistentairwayinflammation,andthesignificantimplicationsthattheseimmunologicaleventshaveforthedevelopment,diagnosis,treatment,andpossiblepreventionofasthma.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
9/50
Asthma
PathophysiologyandPathogenesisofAsthma
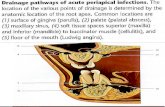
Airflowlimitationinasthmaisrecurrentandcausedbyavarietyofchangesintheairwayincludingbronchoconstriction,airwayedema,airwayhyper-responsiveness,andairwayremodeling.
Figure2.Normalversusasthmaticairway.From:http://www.nhlbi.nih.gov/health/dci/images/asthma.gif
BronchoconstrictionInasthma,thedominantphysiologicaleventleadingtoclinicalsymptomsisairwaynarrowingandasubsequentinterferencewithairflow.Inacuteexacerbationsofasthma,bronchialsmoothmusclecontraction(bronchoconstriction)occursquicklytonarrowtheairwaysinresponsetoexposuretoavarietyofstimuliincludingallergensorirritants.
Allergen-inducedacutebronchoconstrictionresultsfromanIgE-dependentreleaseofmediatorsfrommastcellsthatincludeshistamine,tryptase,leukotrienes,andprostaglandinsthatdirectlycontractairwaysmoothmuscle.Aspirinandothernonsteroidalanti-inflammatorydrugscanalsocauseacuteairflowobstructioninsomepatients,andevidenceindicatesthatthisnon-IgEdependentresponsealsoinvolvesmediatorreleasefromairwaycells.
Inaddition,otherstimuli(includingexercise,coldair,andirritants)cancauseacuteairflow
obstruction.Themechanismsregulatingtheairwayresponsetothesefactorsarelesswelldefined,buttheintensityoftheresponseappearsrelatedtounderlyingairwayinflammation.Stressmayalsoplayaroleinprecipitatingasthmaexacerbations.Themechanismsinvolvedhaveyettobeestablishedandmayincludeenhancedgenerationofpro-inflammatorycytokines.
AirwayEdema
Asthediseasebecomesmorepersistentandinflammationmoreprogressiveotherfactorslimitairflow.Theseincludeedema,inflammation,mucushypersecretionandtheformati
onofinspissatedmucousplugs,aswellasstructuralchangesincludinghypertrophyandhyperplasiaoftheairwaysmoothmuscle.Theselatterchangesmaynotrespondtousualtreatment.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
10/50
Asthma
AirwayHyper-responsiveness
Airwayhyper-responsivenessanexaggeratedbronchoconstrictorresponsetoawidevarietyofstimuliisamajor,butnotnecessarilyunique,featureofasthma.Thedegreetowhichairwayhyper-responsivenesscanbedefinedbycontractileresponsestochallengeswithmethacholine(Provocholine)correlateswiththeclinicalseverityofasthma.Themechanismsinfluencingairwayhyper-responsivenessaremultipleandinclude:
InflammationDysfunctionalneuroregulationStructuralchangesInflammationappearstobeamajorfactorindeterminingthedegreeofairwayhyper-responsiveness.Treatmentdirectedtowardreducinginflammationcanreduceairwa
yhyper-responsivenessandimproveasthmacontrol.
AirwayRemodeling
Insomepersonswhohaveasthma,airflowlimitationmaybeonlypartiallyreversible.Permanentstructuralchangescanoccurintheairway,whichareassociatedwithaprogressivelossoflungfunctionthatisnotpreventedbyorfullyreversiblebycurrenttherapy.
Airwayremodelinginvolvesanactivationofmanyofthestructuralcells,withconsequent
permanentchangesintheairwaythatincreaseairflowobstructionandairwayresponsivenessandrenderthepatientlessresponsivetotherapy.Thesestructuralchangescanincludethickeningofthesub-basementmembrane,subepithelialfibrosis,airwaysmoothmusclehypertrophyandhyperplasia,bloodvesselproliferationanddilation,andmucousglandhyperplasiaandhypersecretion(Box2).Regulationoftherepairandremodelingprocessisnotwellestablished,butboththeprocessofrepairanditsregulationarelikelytobekeyeventsinexplainingthepersistentnatureofthediseaseandlimitationstoatherapeuticresponse.
Box2.FeaturesofAirwayRemodeling
InflammationMucoushypersecretionSubepithelialfibrosus
-
7/31/2019 7 Asthma Patho
11/50
AirwaysmoothmusclehypertrophyAngiogenesis(bloodvesselproliferationanddilation)ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
12/50
Asthma
PathophysiologicMechanismsintheDevelopmentofAirwayInflammation
Inflammationhasacentralroleinthepathophysiologyofasthma.Asnotedinthedefinitionofasthma,airwayinflammationinvolvesaninteractionofmanycelltypesandmultiplemediatorswiththeairwaysthateventuallyresultsinthecharacteristicpathophysiologicalfeaturesofthedisease:bronchialinflammationandairflowlimitationthatresultinrecurrentepisodesofcough,wheeze,andshortnessofbreath.
Theprocessesbywhichtheseinteractiveeventsoccurandleadtoclinicalasthmaarestillunderinvestigation.Moreover,althoughdistinctphenotypesofasthmaexist(e.g.,intermittent,persistent,exercise-associated,aspirin-sensitive,orsevereasthma),airwayinflammationremainsaconsistentpattern.Thepatternofairwayinflammationinasthma,however,doesnotnecessarilyvary
dependingupondiseaseseverity,persistence,anddurationofdisease.Thecellularprofileandtheresponseofthestructuralcellsinasthmaarequiteconsistent.
InflammatoryCells
Lymphocytes
Anincreasedunderstandingofthedevelopmentandregulationofairwayinflammationinasthmafollowedthediscoveryanddescriptionofsubpopulationsoflymphocytes,Thelper1cellsandThelper2cells(Th1andTh2),withdistinctinflammatorymediatorprofilesande
ffectsonairwayfunction.Afterthediscoveryofthesedistinctlymphocytesubpopulationsinanimalmodelsofallergicinflammation,evidenceemergedthat,inhumanasthma,ashift,orpredilection,towardtheTh2-cytokineprofileresultedintheeosinophilicinflammationcharacteristicofasthma.
Inaddition,generationofTh2cytokines(e.g.,interleukin-4(IL-4),IL-5,andIL-13)couldalsoexplaintheoverproductionofIgE,presenceofeosinophils,anddevelopmentofairwayhyper-responsiveness.Therealsomaybeareductioninasubgroupoflymphocytesregulat
oryTcellswhichnormallyinhibitTh2cells,aswellasanincreaseinnaturalkiller(NK)cellsthatreleaselargeamountsofTh1andTh2cytokines.
Tlymphocytes,alongwithotherairwayresidentcells,alsocandeterminethedevelopmentanddegreeofairwayremodeling.AlthoughitisanoversimplificationofacomplexprocesstodescribeasthmaasaTh2disease,recognizingtheimportanceofnfamiliesofcy
-
7/31/2019 7 Asthma Patho
13/50
tokinesandchemokineshasadvancedourunderstandingofthedevelopmentofairwayinflammation.
Mastcells
Activationofmucosalmastcellsreleasesbronchoconstrictormediators(histamine,cysteinylleukotrienes,prostaglandinD2).Althoughallergenactivationoccursthroughhigh-affinityIgEreceptorsandislikelythemostrelevantreaction,sensitizedmastcellsalsomaybeactivatedbyosmoticstimulitoaccountforexercise-inducedbronchospasm(EIB).Increasednumbersofmastcellsinairwaysmoothmusclemaybelinkedtoairwayhyper-responsiveness.Mastcellsalsocanreleasealargenumberofcytokinestochangetheairwayenvironmentandpromoteinflammationeventhoughexposuretoallergensislimited.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
14/50
Asthma
Eosinophils
Increasednumbersofeosinophilsexistintheairwaysofmost,butnotall,personswhohaveasthma.Thesecellscontaininflammatoryenzymes,generateleukotrienes,andexpressawidevarietyofpro-inflammatorycytokines.Increasesineosinophilsoftencorrelatewithgreaterasthmaseverity.Inaddition,numerousstudiesshowthattreatingasthmawithcorticosteroidsreducescirculatingandairwayeosinophilsinparallelwithclinicalimprovement.
However,theroleandcontributionofeosinophilstoasthmaisundergoingareevaluationbasedonstudieswithananti-IL-5treatmentthathassignificantlyreducedeosinophilsbutdidnotaffectasthmacontrol.Therefore,althoughtheeosinophilmaynotbetheonlyprimaryeffectorcellinasthma,itlikelyhasadistinctroleindifferentphasesofthedisease.
Neutrophils
Neutrophilsareincreasedintheairwaysandsputumofpersonswhohavesevereasthma,duringacuteexacerbations,andinthepresenceofsmoking.Theirpathophysiologicalroleremainsuncertain;theymaybeadeterminantofalackofresponsetocorticosteroidtreatment.Theregulationofneutrophilrecruitment,activation,andalterationinlungfunctionisstillunderstudy,butleukotrieneB4maycontributetotheseprocesses.
DendriticCells
Thesecellsfunctionaskeyantigen-presentingcellsthatinteractwithallergensfromtheairwaysurfaceandthenmigratetoregionallymphnodestointeractwithregulatorycellsandultimatelytostimulateTh2cellproductionfromnaveTcells.
Macrophages
Macrophagesarethemostnumerouscellsintheairwaysandalsocanbeactivatedbyallergensthroughlow-affinityIgEreceptorstoreleaseinflammatorymediatorsandcytokinesthatamplifytheinflammatoryresponse.
ResidentCellsoftheAirway
Airwaysmoothmuscleisnotonlyatargetoftheasthmaresponsebyundergoingcontractiontoproduceairflowobstructionbutalsocontributestoit(viatheproductionofitsownfamilyofpro-inflammatorymediators).Asaconsequenceofairwayinflammationandthegenerationofgrowthfactors,theairwaysmoothmusclecellcanundergoproliferation,activat
-
7/31/2019 7 Asthma Patho
15/50
ion,contraction,andhypertrophyeventsthatcaninfluenceairwaydysfunctionofasthma.
EpithelialCells
Airwayepitheliumisanotherairwayliningcellcriticallyinvolvedinasthma.Thegenerationofinflammatorymediators,recruitmentandactivationofinflammatorycells,andinfectionbyrespiratoryvirusescancauseepithelialcellstoproducemoreinflammatorymediatorsortoinjuretheepitheliumitself.Therepairprocess,followinginjurytotheepithelium,maybeabnormalinasthma,thusfurtheringtheobstructivelesionsthatoccurinasthma.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
16/50
Asthma
InflammatoryMediators
Chemokinesareimportantinrecruitmentofinflammatorycellsintotheairwaysandaremainlyexpressedinairwayepithelialcells.Eotaxinisrelativelyselectiveforeosinophils,whereasthymusandactivation-regulatedchemokines(TARCs)andmacrophage-derivedchemokines(MDCs)recruitTh2cells.Thereisanincreasingappreciationfortherolethisfamilyofmediatorshasinorchestratinginjury,repair,andmanyaspectsofasthma.
Cytokinesdirectandmodifytheinflammatoryresponseinasthmaandlikelydetermineitsseverity.Th2-derivedcytokinesincludeIL-5,whichisneededforeosinophildifferentiationandsurvival,andIL-4whichisimportantforTh2celldifferentiationandwithIL-13isimportantforIgEformation.KeycytokinesincludeIL-1andtumornecrosisfactor-(TNF-),whichamplifytheinflammatoryresponse,andgranulocyte-macrophagecolony-stimulatingfactor(GM-
CSF),whichprolongseosinophilsurvivalinairways.Recentstudiesoftreatmentsdirectedtowardsinglecytokines(e.g.,monoclonalantibodiesagainstIL-5orsolubleIL-4receptor)havenotshownbenefitsinimprovingasthmaoutcomes.
Cysteinyl-leukotrienesarepotentbronchoconstrictorsderivedmainlyfrommastcells.Theyaretheonlymediatorwhoseinhibitionhasbeenspecificallyassociatedwithanimprovementinlungfunctionandasthmasymptoms.RecentstudieshavealsoshownleukotrieneB4cancontributeto
theinflammatoryprocessbyrecruitmentofneutrophils.
Nitricoxide(NO)isproducedpredominantlyfromtheactionofinduciblenitricoxidesynthaseinairwayepithelialcells;itisapotentvasodilator.MeasurementsoffractionalexhaledNO(FeNO)maybeusefulformonitoringresponsetoasthmatreatmentbecauseofthepurportedassociationbetweenFeNOandthepresenceofinflammationinasthma.
ImmunoglobulinE(IgE)
IgEistheantibodyresponsibleforactivationofallergicreactionsandisimpo
rtanttothepathogenesisofallergicdiseasesandthedevelopmentandpersistenceofinflammation.IgEattachestocellsurfacesviaaspecifichigh-affinityreceptor.ThemastcellhaslargenumbersofIgEreceptors;these,whenactivatedbyinteractionwithantigen,releaseawidevarietyofmediatorstoinitiateacutebronchospasmandalsotoreleasepro-inflammatorycytokinestoperpetuateunderlyingairwayinflammation.Othercells,basophils,dendriticcel
-
7/31/2019 7 Asthma Patho
17/50
ls,andlymphocytesalsohavehigh-affinityIgEreceptors.
ThedevelopmentofmonoclonalantibodiesagainstIgEhasshownthatthereductionofIgEiseffectiveinasthmatreatment.TheseclinicalobservationsfurthersupporttheimportanceofIgEtoasthma.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
18/50
Asthma
ImplicationsofInflammationforTherapy
Recentscientificinvestigationshavefocusedontranslatingtheincreasedunderstandingoftheinflammatoryprocessesinasthmaintotherapiestargetedatinterruptingtheseprocesses.Someinvestigationshaveyieldedpromisingresults,suchasthedevelopmentleukotrienemodifiersandanti-IgEmonoclonalantibodytherapy.
Otherstudies,suchasthosedirectedatIL-4orIL-5cytokines,underscoretherelevanceofmultiplefactorsregulatinginflammationinasthmaandtheredundancyoftheseprocesses.Alloftheseclinicalstudiesalsoindicatethatphenotypesofasthmaexist,andthesephenotypesmayhaveveryspecificpatternsofinflammationthatrequiredifferenttreatmentapproaches.
Currentstudiesareinvestigatingnoveltherapiestargetedatthecytokines,chemokines,andinflammatorycellsfartherupstreamintheinflammatoryprocess.Forexample,dr
ugsdesignedtoinhibittheTh2inflammatorypathwaymaycauseabroadspectrumofeffectssuchasairwayhyper-responsivenessandmucushypersecretion.Furtherresearchintothemechanismsresponsibleforthevaryingasthmaphenotypesandappropriatelytargetedtherapymayenableimprovedcontrolforallmanifestationsofasthma,and,perhaps,preventionofdiseaseprogression.
Pathogenesis
Whatinitiatestheinflammatoryprocessinthefirstplaceandmakessomeperson
ssusceptibletoitseffectsisanareaofactiveinvestigation.Thereisnotyetadefinitiveanswertothisquestion,butnewobservationssuggestthattheoriginsofasthmaprimarilyoccurearlyinlife.
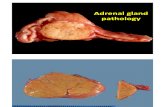
Theexpressionofasthmaisacomplex,interactiveprocessthatdependsontheinterplaybetweentwomajorfactorshostfactors(particularlygenetics)andenvironmentalexposuresthatoccuratacrucialtimeinthedevelopmentoftheimmunesystem.
Figure3.Effectsofgeneticpredispositionandenvironmentalfactorsonasthma.Adaptedfrom:http://www.niehs.nih.gov/research/atniehs/labs/lrb/enviro-cardio/images/asthma.gif.NationalInstituteofEnvironmentalHealthStudies,NIH.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
19/50
-
7/31/2019 7 Asthma Patho
20/50
Asthma
HostFactors
InnateImmunity
Thereisconsiderableinterestintheroleofinnateandadaptiveimmuneresponsesassociatedwithboththedevelopmentandregulationofinflammation.Inparticular,researchhasfocusedonanimbalancebetweenTh1andTh2cytokineprofilesandevidencethatallergicdiseases,andpossiblyasthma,arecharacterizedbyashifttowardaTh2cytokine-likedisease,eitherasoverexpressionofTh2orunder-expressionofTh1.
Airwayinflammationinasthmamayrepresentalossofnormalbalancebetweentwoopposing
populationsofThlymphocytes.TwotypesofThlymphocyteshavebeencharacterized:Th1andTh2.Th1cellsproduceIL-2andinterferon-.(IFN-.),whicharecriticalincellulardefense
mechanismsinresponsetoinfection.Th2,incontrast,generatesafamilyofcytokines(IL-4,-5,-6,9,and-13)thatcanmediateallergicinflammation.
Thecurrenthygienehypothesisofasthmaillustrateshowthiscytokineimbalancemayexplainsomeofthedramaticincreasesinasthmaprevalenceinwesternizedcountries.ThishypothesisisbasedontheassumptionthattheimmunesystemofthenewlybornisskewedtowardTh2cytokinegeneration.Followingbirth,environmentalstimulisuchasinfectionswillactivateTh1responsesandbringtheTh1/Th2relationshiptoanappropriatebalance.
Evidenceindicatesthattheincidenceofasthmaisreducedinassociationwithcertaininfections(M.tuberculosis,measles,orhepatitisA),exposuretootherchildren(e.g.,presenceofoldersiblingsandearlyenrollmentinchildcare),andlessfrequentuseofantibiotics.Furthermore,theabsenceoftheselifestyleeventsisassociatedwiththepersistenceofaTh2cytokinepattern.Undertheseconditions,thegeneticbackgroundofthechildwhohasacytokineimbalancetowardTh2willsetthestagetopromotetheproductionofIgEantibodiestokeyenvironmentalantigens,suchas
house-dustmite,cockroach,Alternaria,andpossiblycat.Therefore,agene-by-environmentinteractionoccursinwhichthesusceptiblehostisexposedtoenvironmentalfactorsthatarecapableofgeneratingIgE,andsensitizationoccurs.Preciselywhytheairwaysofsomeindividualsaresusceptibletotheseallergiceventshasnotbeenestablished.
Therealsoappearstobeareciprocalinteractionbetweenthetwosub-populationsinwhichTh1
-
7/31/2019 7 Asthma Patho
21/50
cytokinescaninhibitTh2generationandviceversa.AllergicinflammationmaybetheresultofanexcessiveexpressionofTh2cytokines.Alternatively,recentstudieshavesuggestedthepossibilitythatthelossofnormalimmunebalancearisesfromacytokinedysregulationinwhichTh1activityinasthmaisdiminished.Thefocusonactionsofcytokinesandchemokinestoregulateandactivatetheinflammatoryprofileinasthmahasprovidedongoingandnewinsightintothepatternofairwayinjurythatmayleadtonewtherapeutictargets.
Genetics
Itiswellrecognizedthatasthmahasaninheritablecomponenttoitsexpression,butthegeneticsinvolvedintheeventualdevelopmentofasthmaremainacomplexandincompletepicture.Todate,manygeneshavebeenfoundthateitherareinvolvedinorlinkedtothepresenceofasthmaandcertainofitsfeatures.Thecomplexityoftheirinvolvementinclinicalasthmaisnotedbylinkagestocertainphenotypiccharacteristics,butnotnecessarilythepathophysiologicdisease
processorclinicalpictureitself.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
22/50
Asthma
TheroleofgeneticsinIgEproduction,airwayhyper-responsiveness,anddysfunctionalregulationofthegenerationofinflammatorymediators(suchascytokines,chemokines,andgrowthfactors)hasappropriatelycapturedmuchattention.Inaddition,studiesareinvestigatinggeneticvariationsthatmaydeterminetheresponsetotherapy.Therelevanceofpolymorphismsinthebeta-adrenergicandcorticosteroidreceptorsindeterminingresponsivenesstotherapiesisofincreasinginterest,butthewidespreadapplicationofthesegeneticfactorsremainstobefullyestablished.
Sex
Inearlylife,theprevalenceofasthmaishigherinboys.Atpuberty,however,thesexratioshifts,andasthmaappearspredominantlyinwomen.Howspecificallysexandsexhormones,orrelatedhormonegeneration,arelinkedtoasthmahasnotbeenestablished,buttheymay
contributetotheonsetandpersistenceofthedisease.
EnvironmentalFactors
Twomajorenvironmentalfactorshaveemergedasthemostimportantinthedevelopment,persistence,andpossiblyseverityofasthma:
AirborneallergensViralrespiratoryinfections
Inthesusceptiblehost,andatacriticaltimeofdevelopment,bothrespiratoryinfectionsandallergenshaveamajorinfluenceonasthmadevelopmentanditslikelypersistence.Itisalsoapparentthatallergenexposure,allergicsensitization,andrespiratoryinfectionsarenotseparateentitiesbutfunctioninteractivelyintheeventualdevelopmentofasthma.
Allergens
Theroleofallergensinthedevelopmentofasthmahasyettobefullydefinedorresolved,butit
isobviouslyimportant.Sensitizationandexposuretohouse-dustmiteandAlternariaareimportantfactorsinthedevelopmentofasthmainchildren.Earlystudiesshowedthatanimaldandersparticularlydogandcatwereassociatedwiththedevelopmentofasthma.
Recentdatasuggestthat,undersomecircumstances,dogandcatexposureinearlylifemayactuallyprotectagainstthedevelopmentofasthma.Thedeterminantofthesediverseoutcomes
-
7/31/2019 7 Asthma Patho
23/50
hasnotbeenestablished.Studiestoevaluatehouse-dustmiteandcockroachexposurehaveshownthattheprevalenceofsensitizationandsubsequentdevelopmentofasthmaarelinked.Exposuretocockroachallergen,forexample,amajorallergenininner-citydwellings,isanimportantcauseofallergensensitization,ariskfactorforthedevelopmentofasthma.Inaddition,allergenexposurecanpromotethepersistenceofairwayinflammationandlikelihoodofanexacerbation.
RespiratoryInfections
Duringinfancy,anumberofrespiratoryviruseshavebeenassociatedwiththeinceptionordevelopmentoftheasthma.Inearlylife,respiratorysyncytialvirus(RSV)andpara-influenzavirusinparticular,causebronchiolitisthatparallelsmanyfeaturesofchildhoodasthma.Anumberoflong-termprospectivestudiesofchildrenadmittedtohospitalwithdocumentedRSVhaveshownthatapproximately40%oftheseinfantswillcontinuetowheezeorhaveasthmainlater
childhood.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
24/50
Asthma
Symptomaticrhinovirusinfectionsinearlylifealsoareemergingasriskfactorsforrecurrentwheezing.Ontheotherhand,evidencealsoindicatesthatcertainrespiratoryinfectionsearlyinlifeincludingmeaslesandevenRSVorrepeatedviralinfections(otherthanlowerrespiratorytractinfections)canprotectagainstthedevelopmentofasthma.Thehygienehypothesisofasthmasuggeststhatexposuretoinfectionsearlyinlifeinfluencesthedevelopmentofachildsimmunesystemalonganon-allergicpathway,leadingtoareducedriskofasthmaandotherallergicdiseases.Althoughthehygienehypothesiscontinuestobeinvestigated,thisassociationmayexplainobservedassociationsbetweenlargefamilysize,laterbirthorder,daycareattendance,andareducedriskofasthma.
Theinfluenceofviralrespiratoryinfectionsonthedevelopmentofasthmamaydependonaninteractionwithatopy.Theatopicstatecaninfluencethelowerairwayresponse
toviralinfections,andviralinfectionsmaytheninfluencethedevelopmentofallergicsensitization.Theairwayinteractionsthatmayoccurwhenindividualsareexposedsimultaneouslytobothallergensandvirusesareofinterestbutarenotdefinedatpresent.
OtherEnvironmentalExposures
Tobaccosmoke,airpollution,occupations,anddiethavealsobeenassociatedwithanincreasedriskfortheonsetofasthma,althoughtheassociationhasnotbeenasclearlyestablishedaswith
allergensandrespiratoryinfections.Inuteroexposuretoenvironmentaltobaccosmokeincreasesthelikelihoodforwheezingintheinfant,althoughthesubsequentdevelopmentofasthmahasnotbeenwelldefined.Inadultswhohaveasthma,cigarettesmokinghasbeenassociatedwithanincreaseinasthmaseverityanddecreasedresponsivenesstoinhaledcorticosteroids(ICSs).
Theroleofairpollutioninthedevelopmentofasthmaremainscontroversialandmayberelatedtoallergicsensitization.Onerecentepidemiologicstudyshowedthatheavyexercise(threeor
moreteamsports)outdoorsincommunitieswithhighconcentrationofozonewasassociatedwithahigherriskofasthmaamongschool-agechildren.Therelationshipbetweenincreasedlevelsofpollutionandincreasesinasthmaexacerbationsandemergencycarevisitshasbeenwelldocumented.
Anassociationoflowintakeofantioxidantsandomega-3fattyacidshasbeennotedin
-
7/31/2019 7 Asthma Patho
25/50
observationalstudies,butadirectlinkasacausativefactorhasnotbeenestablished.Increasingratesofobesityhaveparalleledincreasingratesinasthmaprevalence,buttheinterrelationisuncertain.Obesitymaybeariskfactorforasthmaduetothegenerationofuniqueinflammatorymediatorsthatleadtoairwaydysfunction.
Insummary,ourunderstandingofasthmapathogenesisandunderlyingmechanismsnowincludestheconceptthatgene-by-environmentalinteractionsarecriticalfactorsinthedevelopmentofairwayinflammationandeventualalterationinthepulmonaryphysiologythatischaracteristicofclinicalasthma.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
26/50
Asthma
NaturalHistoryofAsthma
Ifthepersistenceandseverityofasthmainvolvesaprogressionofairwayinflammationtoairwayremodelingandsomeeventualirreversibleairwayobstruction,thenanimportantquestioniswhetheranti-inflammatorymedicationsuchasinhaledcorticosteroids(ICS),givenearlyinthecourseofdiseasemightinterruptthisprocessandpreventpermanentdeclinesinlungfunction.Forearlyinitiationofinhaledcorticosteroidstobemorebeneficialthandelayedinitiation,twoassumptionsmustbevalid:
(1)Asagroup,peoplewhohavemildormoderatepersistentasthmaexperienceaprogressivedeclineinlungfunctionthatismeasurableandclinicallysignificant,and(2)Treatmentwithinhaledcorticosteroidspreventsorslowsthisdecline,inadditiontoprovidinglong-termcontrolofasthma.Reviewsoftheliteraturewereconductedin2002andforthiscurrentreportto
evaluatetheeffectofinterventionwithinhaledcorticosteroidsinalteringtheprogressionofdisease.
NaturalHistoryofPersistentAsthma
Children
Itiswellestablishedthatasthmaisavariabledisease.Asthmacanvaryamongindividuals,anditsprogressionandsymptomscanvarywithinanindividualsexperienceovertime.Thecourseofasthmaovertime,eitherremissionorincreasingseverity,iscommonlyreferred
toasthenaturalhistoryofthedisease.Ithasbeenpostulatedthatthepersistenceorincreaseofasthmasymptomsovertimeisaccompaniedbyaprogressivedeclineinlungfunction.Recentresearchsuggeststhatthismaynotbethecase.Rather,thecourseofasthmamayvarymarkedlybetweenyoungchildren,olderchildrenandadolescents,andadults,andthisvariationisprobablymoredependentonagethanonsymptoms.
Aprospectivecohortstudyinwhichfollowupbeganatbirthrevealedthat,inchildrenwhose
asthma-likesymptomsbeganbefore3yearsofage,deficitsinlunggrowthassociatedwiththeasthmaoccurredby6yearsofage.Continuedfollowuponlungfunctionmeasurestakenat1116yearsofagefoundthat,comparedtothegroupofchildrenwhoexperiencednoasthmasymptomsforthefirst6yearsoflife,thegroupofchildrenwhoseasthmasymptomsbeganbefore3yearsofageexperiencedsignificantdeficitsinlungfunctionat1116yearsofage;
-
7/31/2019 7 Asthma Patho
27/50
however,nofurtherlossinforcedexpiratoryvolumein1second(FEV1)occurredcomparedtochildrenwhodidnothaveasthma.Thegroupwhoseasthmasymptomsbeganafter3yearsofagedidnotexperiencedeficitsinlungfunction.
Alongitudinalstudyofchildren810yearsofagefoundthatbronchialhyper-responsivenesswasassociatedwithdeclinesinlungfunctiongrowthinbothchildrenwhohaveactivesymptomsofasthmaandchildrenwhodidnothavesuchsymptoms.Thus,symptomsneitherpredictednordeterminedlungfunctiondeficitsinthisagegroup.
AstudybySearsandcolleaguesin2003assessedlungfunctionrepeatedlyfromages9to26inalmost1,000childrenfromabirthcohortinDunedin,NewZealand.TheyfoundthatchildrenwhohadasthmahadpersistentlylowerlevelsofFEV1/forcedvitalcapacity(FVC)ratioduringthefollowup.Regardlessoftheseverityoftheirsymptoms,however,theirlevelsoflungfunctionparalleledthoseofchildrenwhodidnothaveasthma,andnofurtherlossesoflungfunctionwere
observedafterage9.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
28/50
Asthma
BaselinedatafromtheChildhoodAsthmaManagementProgram(CAMP)studysupportthefindingthattheindividualsageatthetimeofasthmaonsetinfluencesdeclinesinlungfunctiongrowth.Atthetimeofenrollmentofchildrenwhohadmildormoderatepersistentasthmaat512yearsofage,aninverseassociationbetweenlungfunctionanddurationofasthmawasnoted.Althoughtheanalysisdidnotdistinguishbetweenageofonsetanddurationofasthma,itcanbeinferredthat,becausetheaveragedurationofasthmawas5yearsandtheaverageageofthechildrenwas9years,mostchildrenwhohadthelongerdurationofasthmastartedexperiencingsymptomsbefore3yearsofage.
Thedatasuggestthatthesechildrenhadthelowestlungfunctionlevels.After46yearsoffollowup,thechildrenintheCAMPstudy,onaverage,didnotexperiencedeficitsinlunggrowth(asdefinedbypost-bronchodilatorFEV1),regardlessoftheirsymptomlevelsor
thetreatmenttheyreceived.However,afollowupanalysisoftheCAMPdatashowedthatasubgroupofthechildrenexperiencedprogressive(atleast1%ayear)reductionsinlunggrowth,regardlessoftreatmentgroup.Predictorsofthisprogressivereduction,atbaselineofthestudy,weremalesexandyoungerage.
TheCAMPstudynotedthatwhenmeasuresotherthanFEV1areusedtoassesslungfunctionmeasuresovertimeinchildhoodasthma,progressivedeclinesareobserved:theFEV1/FVCratio
beforebronchodilatorusewassmallerattheendofthetreatmentperiodthanatthestartinallthreetreatmentgroups;thedeclineintheICSgroupwaslessthanthatoftheplacebogroup(0.2%versus1.8%).
InacomparisonoflungfunctionmeasuresofCAMPstudyparticipantswithlungfunctionmeasuresofchildrenwhodidnothaveasthma,byyearfromages5through18,theFEV1/FVCratiowassignificantlylowerforthechildrenwhohadasthmacomparedtothosewhodidnothaveasthmaatage5(meandifference7.3percentforboysand7.1percentforgirls),andt
hedifferenceincreasedwithage(9.8%forboysand9.9%forgirls).
Cumulatively,thesestudiessuggestthatmostofthedeficitsinlungfunctiongrowthobservedinchildrenwhohaveasthmaoccurinchildrenwhosesymptomsbeginduringthefirst3yearsoflife,andtheonsetofsymptomsafter3yearsofageusuallyisnotassociatedwithsignificantdeficitsinlungfunctiongrowth.Thus,apromisingtargetforinterventionsdesignedto
-
7/31/2019 7 Asthma Patho
29/50
preventdeficitsinlungfunction,andperhapsthedevelopmentofmoreseveresymptomslaterinlife,wouldbechildrenwhohavesymptomsbefore3yearsofageandseemdestinedtodeveloppersistentasthma.However,itisimportanttodistinguishthisgroupfromthemajorityofchildrenwhowheezebefore3yearsofageanddonotexperienceanymoresymptomsafter6yearsofage.
Untilrecently,novalidatedalgorithmswereavailabletopredictwhichchildrenamongthosewhohadasthma-likesymptomsearlyinlifewouldgoontohavepersistentasthma.Dataobtainedfromlong-termlongitudinalstudiesofchildrenwhowereenrolledatbirthhavegeneratedsuchapredictiveindex.Thestudiesfirstidentifiedanindexofriskfactorsfordevelopingpersistentasthmasymptomsamongchildrenyoungerthan3yearsofagewhohadmorethanthreeepisodesofwheezingduringthepreviousyear.Theindexwasthenappliedtoabirthcohortthatwasfollowedthrough13yearsofage.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
30/50
Asthma
Seventy-sixpercentofthechildrenwhowerediagnosedwithasthmaafter6yearsofagehadapositiveasthmapredictiveindexbefore3yearsofage;97%ofthechildrenwhodidnothaveasthmaafter6yearsofagehadanegativeasthmapredictiveindexbefore3yearsofage.Theindexwassubsequentlyrefinedandtestedinaclinicaltrialtoexamineiftreatingchildrenwhohadapositiveasthmapredictiveindexwouldpreventdevelopmentofpersistentwheezing.
Theasthmapredictiveindexgeneratedbythesestudiesidentifiesthefollowingriskfactorsfordevelopingpersistentasthmaamongchildrenyoungerthan3yearsofagewhohadfourormoreepisodesofwheezingduringthepreviousyear:
Either(1)oneofthefollowing:oparentalhistoryofasthma,
oaphysiciandiagnosisofatopicdermatitis,oroevidenceofsensitizationtoaeroallergens.Or(2)twoofthefollowing:oevidenceofsensitizationtofoods,o=4percentperipheralbloodeosinophilia,orowheezingapartfromcolds.Adults
Acceleratedlossoflungfunctionappearstooccurinadultswhohaveasthma.Inastudyofadultswhohaveasthmaandwhoreceived2weeksofhigh-doseprednisoneifairflowobstructionpersistedafter2weeksofbronchodilatortherapy,thedegreeofpersistentairflowobstructioncorrelatedwithboththeseverityandthedurationoftheirasthma.
Twolarge,prospectiveepidemiologicalstudiesevaluatedtherateofdeclineinpulmonaryfunctioninadultswhohadasthma.Inan18-yearprospectivestudyof66nonsmokerswhohad
asthma,26smokerswhohadasthma,and186controlparticipantswhohadnoasthma,spirometrywasperformedat3-yearintervals.Seventy-threepercentofthestudygroupunderwentatleastsixspirometricevaluations.
Theslopefordeclineinlungfunction(FEV1)wasapproximately40%greaterfortheparticipantswhohadasthmathanforthosewhohadnoasthma.Thisdidnotappeartoresultfromextreme
-
7/31/2019 7 Asthma Patho
31/50
measurementproducedbyafewparticipants,becausefewerthan25%oftheparticipantswhohadasthmaweremeasuredwithaslopelesssteepthanthemeanforthosewhodidnothaveasthma.Inanotherstudy,threespirometryevaluationswereperformedin13,689adults(778hadasthma,and12,911didnothaveasthma)overa15-yearperiod.
TheaveragedeclineinFEV1wassignificantlygreater(38mLperyear)inthosewhohadasthmathaninthosewhodidnothaveasthma(22mLperyear).Although,inthisstudy,asthmawasdefinedsimplybypatientreport,theresearchersnotedthat,becausethe6percentprevalencerateforasthmadidnotincreaseinthiscohortastheyincreasedinage,itislikelythatthesubjectswhoreportedhavingasthmadidindeedhaveasthmaratherthanchronicobstructivepulmonarydisease(COPD).Itisnotpossibletodeterminefromthesestudieswhetherthelossofpulmonaryfunctionoccurredinthosewhohadmildormoderateasthmaoronlyinthosewhohadsevereasthma.Nevertheless,thedatasupportthelikelihoodofpotentialacceleratedlossofpulmonary
functioninadultswhohaveasthma.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
32/50
Asthma
NewstudieshaveaddressedthisissuesincetheExpertPanelReviewUpdate2002.JamesandcolleaguesreanalyzedthedatafromthestudyofdeclineinlungfunctionfromBusselton,Australia,afteraddinganewsurveyin19941995.Subjects(N=9,317)hadparticipatedasadults(19yearsorolder)inoneormoreofthecross-sectionalBusseltonHealthSurveysbetween1966and1981orinthefollowupstudyof19941995.
Usingthewholedatasample,Jamesandcolleaguesfoundthatsubjectswhohadasthmashowedsignificantlylowerlungfunctionduringthewholefollowupperiod,butmostofthedifferenceswereduetodeficitsinlungfunctionpresentatthebeginningoffollowup(whensubjectswereage19).Oncetheeffectofsmokingwastakenintoaccount,theexcessdeclineinFEV1attributabletoasthmawas3.78mLperyearforwomenand3.69mLperyearformen.Althoughtheseresultswerestatisticallysignificant,theirclinicalrelevanceisdebatable.
In2003,Sherrillandcoworkersre-analyzedthedatafromtheTucsonEpidemiologicStudyofAirwayObstructiveDisease.Atotalof2,926subjects,withlongitudinaldataforlungfunctionassessedinupto12surveysspanningaperiodofupto20years,wereincluded.Theyfoundthat,unlikesubjectswhohadadiagnosisofCOPD,inthosewhohaddiagnosisoflongstandingasthma,FEV1didnotdeclineatamorerapidratethannormal.ThiswasalsotrueforsubjectswhohadasthmaandCOPD.In2001,Griffithandcolleaguesstudieddeclineinlungfunctionin
5,242participantsintheCardiovascularHealthStudywhowereoverage65atenrollment.Eachparticipanthaduptothreelungfunctionmeasurementsovera7-yearinterval.
SubjectswhohadasthmahadlowerlevelsofFEV1thanthosewhoreportednoasthma.However,afteradjustmentforemphysemaandchronicbronchitis,therewerenosignificantincreasesintherateofdeclineinFEV1inparticipantswhohadasthma.
Summary
Takentogether,theselongitudinalepidemiologicalstudiesandclinicaltrialsi
ndicatethattheprogressionofasthma,asmeasuredbydeclinesinlungfunction,variesindifferentagegroups.Declinesinlungfunctiongrowthobservedinchildrenappeartooccurby6yearsofageandoccurpredominantlyinthosechildrenwhoseasthmasymptomsstartedbefore3yearsofage.
Children512yearsofagewhohavemildormoderatepersistentasthma,onaverage,donot
-
7/31/2019 7 Asthma Patho
33/50
appeartoexperiencedeclinesinlungfunctionthrough1117yearsofage,althoughasubsetofthesechildrenexperienceprogressivereductionsinlunggrowthasmeasuredbyFEV1.
Furthermore,thereisemergingevidenceofreductionsintheFEV1/FVCratio,apparentinyoungchildrenwhohavemildormoderateasthmacomparedtochildrenwhodonothaveasthma,thatincreasewithage.Thereisalsoevidenceofprogressivelydeclininglungfunctioninadultswhohaveasthma,buttheclinicalsignificanceandtheextenttowhichthesedeclinescontributetothedevelopmentoffixedairflowobstructionareunknown.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
34/50
Asthma
EffectofInterventionsonNaturalHistoryofAsthma
Dataontheeffectofinterventionsontheprogressionofasthma,asmeasuredbydeclinesinlungfunction,airwayhyper-responsiveness,ortheseverityofsymptoms,wereevaluatedforEPRUpdate2002andthecurrentupdate.TheExpertPaneldoesnotrecommendusinginhaledcorticosteroidsforthepurposeofmodifyingtheunderlyingdiseaseprocess(e.g.,preventingpersistentasthma).Evidencetodateindicatesthatdailylong-termcontrolmedicationdoesnotaltertheunderlyingseverityofthedisease.
Althoughapreliminarystudysuggeststhatappropriatecontrolofchildhoodasthmamaypreventmoreseriousasthmaorirreversibleobstructioninlateryears,theseobservationswerenotverifiedinarecentlong-termrandomizedcontroltrial(RCT)in1,041children512yearsofage.Thisstudydoesnotsupporttheassumptionthat,onaverage,children512yearsofage
whohavemildormoderatepersistentasthmahaveaprogressivedeclineinlungfunction.ChildrenintheplacebogroupdidnotexperienceadeclineinpostbronchodilatorFEV1overthe5-yeartreatmentperiod,andtheyhadpostbronchodilatorFEV1levelssimilartochildrenintheICSandnedocromiltreatmentgroupsattheendofthestudy.
ObservationalprospectivedatafromotherstudiesoflargegroupsofchildrensuggestthatthetimingoftheCAMPinterventionwastoolate,asmostlossoflungfunctioninchildhoodasthma
appearstooccurinthefirst35yearsoflife.However,inarecentrandomized,controlledprospectivestudy,children23yearsofagewhowereathighriskofdevelopingpersistentasthmaweretreatedfor2yearswithinhaledcorticosteroidsandobservedfor1additionalyearaftertreatmentwasdiscontinued.Thatstudydemonstratedthattheinterventiongrouphadlungfunctionandasthmasymptomlevelssimilartotheplacebogroupattheendofthestudy.
Tworecentstudiesaddressedthepossibilitythatinhaledcorticosteroidsmaypreventtheputative
declinesinlungfunctionbelievedtooccurshortlyafterthebeginningofthediseaseinadultswhohavelate-onsetasthma.Aretrospectivestudyreportedtheresultsofanobservationalstudyofadultswhohadmild-to-moderateasthmaandweretreatedfor5yearswithaninhaledcorticosteroid.Onegroup,treatedearlyinthedisease(lessthan2yearsafterdiagnosis),hadbetteroutcomesintermsoflungfunctionthanthosewhostartedtreatmentmorethan2years
-
7/31/2019 7 Asthma Patho
35/50
afterdiagnosis.Thegroupinwhichtreatmentwasstartedmorethan2yearsafterdiagnosis,however,hadlowerlevelsoflungfunctionatthebeginningofthetrial.Therefore,itisnotpossibletodeterminefromthesedatawhattheresultswouldhavebeeninarandomizedtrial.
Tworecentlong-termobservationalstudiesreportanassociationbetweeninhaledcorticosteroidtherapyandreduceddeclineinFEV1inadultswhohaveasthma.However,long-termRCTswillbenecessarytoconfirmacausalrelationship.
TheSTARTstudyenrolled7,241subjects,566yearsofage,whohadmildasthmaoflessthan2yearsduration,accordingtoeachsubjectsreport.Participantswererandomizedtoalow-doseinhaledcorticosteroidorplaceboandwerefollowedprospectivelyfor3years.Thestudyfoundaslightlybetterlevelofpostbronchodilatorlungfunctioninparticipantsintheactivearmthanintheplaceboarm,butthedifferencewasmoreprominentafter1yearoftreatment(+1.48percentpredictedFEV1)thanattheendofthetreatmentperiod(+0.88percentpredicted
FEV1),suggestingnoeffectintheputativeprogressivelossinlungfunctioninthesesubjects.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
36/50
Asthma
Withrespecttothepotentialroleofinhaledcorticosteroidsinchangingthenaturalcourseofasthma,therelevantclinicalquestionis:Aretheyassociatedwithlessdiseaseburdenafterdiscontinuationoftherapy?Thebestavailableevidenceinchildren512yearsofageand23yearsofagedemonstratedthat,althoughinhaledcorticosteroidsprovidesuperiorcontrolandpreventionofsymptomsandexacerbationsduringtreatment,symptomsandairwayhyper-responsivenessworsenwhentreatmentiswithdrawn.Thisevidencesuggeststhatcurrentlyavailabletherapycontrolsbutdoesnotmodifytheunderlyingdiseaseprocess.
ImplicationsofCurrentInformation
Airwayinflammationisamajorfactorinthepathogenesisandpathophysiologyofasthma.Theimportanceofinflammationtocentralfeaturesofasthmacontinuestoexpandandunderscorethischaracteristicasaprimarytargetoftreatment.Ithasalsobecomeapparent,ho
wever,thatairwayinflammationisvariableinmanyaspectsincludingintensity,cellular/mediatorpattern,andresponsetotherapy.Asknowledgeofthevariousphenotypesofinflammationbecomeapparent,itislikelythattreatmentalsowillalsohavegreaterspecificityand,presumably,effectiveness.
Itisalsoapparentthatasthma,anditspersistence,beginsearlyinlife.Althoughthefactorsthatdeterminepersistentversusintermittentasthmahaveyettobeascertained,thisinformationwill
becomeimportantindeterminingthetypeoftreatment,itsduration,anditseffectonvariousoutcomesofasthma.Earlystudieshaveindicatedthatalthoughcurrenttreatmentiseffectiveincontrollingsymptoms,reducingairflowlimitations,andpreventingexacerbations,presenttreatmentdoesnotappeartopreventtheunderlyingseverityofasthma.
Despitetheseunknowns,thecurrentunderstandingofbasicmechanismsinasthmahasgreatlyimprovedappreciationoftheroleoftreatment.TheExpertPanelsrecommendationsforasthmatreatment,whicharedirectedbyknowledgeofbasicmechanisms,shouldresultin
improvedcontrolofasthmaandagreaterunderstandingoftherapeuticeffectiveness.
Reference
NationalHeart,Lung,andBloodInstitute(2007).ExpertPanelReport3(EPR3):GuidelinesfortheDiagnosisandManagementofAsthma.Section2:Definition,Pathophysiology,andPathogenesisofAsthmaandNaturalHistoryofAsthma.Accessed8-1-08from:
-
7/31/2019 7 Asthma Patho
37/50
http://www.nhlbi.nih.gov/guidelines/asthma/asthgdln.htm.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
38/50
Asthma
Glossary
Alternaria
Awidespreadtypeofmoldfoundbothindoorsandoutdoorsthatcantriggerallergicreactionsandasthma.
Antigen
Substancesforeigntothebodysuchasviruses,disease-causingbacteria,andotherinfectiousagents.
Atopy
Thegenetictendencytodevelopcertainallergicresponsessuchasasthma,allergicrhinitis,anddermatitis.
Chemokine
Atypeofsmallcytokine.
Cysteinyl-leukotrienes
Potentbronchoconstrictorsderivedmainlyfrommastcells.
Cytokine
Smallproteinsthatactovershortdistancesandarecriticaltothefunctioningoftheimmunesystem.Cytokinesdirectandmodifytheinflammatoryresponseinasthmaandlikelydetermineits
severity.
Eotaxin
Atypeofchemokinethatisimplicatedinthenarrowingoftheairwaysinasthma.
Hyperplasia
Anabnormalorincreasedgrowthofcellsinnormaltissuesororgans.
IgE
ImmunoglobulinE,atypeofantibodyreleasedinresponsetothepresenceofanallergen.Itisresponsibleforactivationofallergicreactionsandisimportanttothepathogenesisofallergicdiseasesandthedevelopmentandpersistenceofinflammation.
Inspissated
Driedorthickenedinconsistencyduetoevaporationoffluids.
-
7/31/2019 7 Asthma Patho
39/50
Leukotrienes
Ahormonethatcausesvasodilation,mucosalswelling,andotherinflammatoryresponsesseeninhayfeverandasthma.
Mastcells
Cellsthatsynthesizeandstorehistamines,whicharereleasedduringanallergicreaction.Thereleaseofhistaminefrommastcellscausesanimmediatereddeningoftheskin.
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
40/50
Asthma
Methacholine
Adruggiveninincreaseddosestotestairwaysensitivity,whichisusedtotestforthepresenceandseverityofasthma.
Monoclonalantibodies
Proteinsproducedinthelabdesignedtoseekoutanddestroyspecificantigens.
NAEPP
NationalAsthmaEducationandPreventionProgram
Nave
AmatureTcellthatisnotyetactivatedbyanantigen.Naturalhistory:Thecourseofadiseaseovertime,eitherremissionorincreasingseverity,iscommonlyreferredtoasthenaturalhistoryofthedisease.
Nitricoxide(NO)
Apotentvasodilator.
Phenotype
Theobservabletraitsorcharacteristicsofanorganism,forexamplehaircolor,weight,orthepresenceorabsenceofadisease.Phenotypictraitsarenotnecessarilygenetic.
Pro-inflammatorycytokines
Cellsinvolvedwiththeamplificationoftheinflammatoryprocess.
Subepithelialfibrosis
Thedevelopmentofexcessiveconnectivetissueandscarringinthelungsoftenseeninsevereasthma.
(continuedonnextpage)
ATrainEducation,Inc.707459-1315
22
-
7/31/2019 7 Asthma Patho
41/50
Asthma
PostTest
UsetheAnswerSheetfollowingthetesttorecordyouranswers.
1.Airwayinflammation:a.Isusuallytemporaryanddoesnotleadtobronchospasm.b.Isonlyseeninchronicasthmac.Canaffectairwaycaliberandairflow.d.Doesnotaffectbronchialhyper-responsiveness.2.Airwayremodeling:a.Candecreaseairflowobstructionandmakethepatientmoreresponsivetotherapy.b.Isamajorfactorindeterminingthedegreeofairwayhyper-responsiveness.c.Causespermanentstructuralchangesandlossoflungfunction.d.Isanexaggeratedbronchoconstrictorresponse.3.Smoothmusclecontractionoftheairwayscausedbyallergensorirritantsiscalled:a.Inflammation.b.Airwayhyper-responsiveness.c.Inspissation.d.Bronchospasm.
4.Factorsthatlimitairflowasairwaydiseaseprogressesare:a.Edemaandinflammationb.Methacholineandmucusplugs.c.Phenotypetraitsandinspissation.d.Innateimmunityandinflammatorycytokines.5.Airwayhyper-responsivenessincludesallofthefollowingexcept:a.Inflammation.b.Decreasedreleaseofhistamine.c.Dysfunctionalneuroregulation.d.Structuralchanges.6.Airwayremodelingis:a.Atemporaryalterationinairwaystructure.b.Anobservabletraitorcharacteristicofanorganism.
c.Anacutesymptomofasthma.d.Notpreventedbyorfullyresponsivetocurrenttreatments.7.Airwayremodelingcausespermanentchangesintheairwaythatincreaseobstructionandrenderthepatientlessresponsivetotherapy.a.Trueb.FalseATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
42/50
Asthma
8.Angiogenesisisafeatureof:a.Dysfunctionalneuroregulation.b.Airwayremodeling.c.Mucusplugs.d.Releaseofhistaminefrommastcells.9.Airwayinflammationinasthmaisonlyseeninexercise-associatedandaspirin-sensitivephenotypes.Falsea.Trueb.False10.Whenactivatedbyallergensmucosalmastcellsrelease:a.Cytokinesandchemokines.b.RegulatorT-cells.c.Lymphocytes.d.Bronchoconstrictormediators.11.Exercise-inducedbronchospasmiscausedby:a.Decreasedsensitivitytousualtreatments.b.Sensitizedmastcellsactivatedbyosmoticstimuli.c.T-lymphocytesandotherairwayresidentcells.d.Allergenactivationofmastcells.12.Airwayinflammationisseenonlyinexercise-inducedandaspirin-inducedast
hma.a.Trueb.False13.Treatmentwithcorticosteroids:a.Reducescirculatingandairwayeosinophilsthatcontaininflammatoryenzymes.b.Causesanincreaseincirculatingeosinophilsinparallelwithclinicalimprovement.c.Increasestheriskoflungremodeling.d.Cancauseincreasedmucushypersecretion.14.Allergenexposure:a.Isnotassociatedwiththedevelopmentofasthmainchildren.b.Isakeyfactorinthepersistenceofairwayinflammation.
c.Decreasesthelikelihoodofanexacerbation.d.Hasbeenproventoprotectagainstthedevelopmentofasthma.15.Infectionsassociatedwiththedevelopmentofasthmaare:a.Respiratorysyncytialvirusandparainfluenza.b.MeaslesandE-coli.c.Respiratorysyncytialvirusandmeasles.d.Yeastinfectionsandparainfluenza.ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
43/50
Asthma
16.Thehygienehypothesissuggeststhat:a.Peoplewholiveindevelopedcountriesarelesslikelytodevelopasthma.b.Earlyexposuretoallergensleadstoareducedriskofasthma.c.Peoplefromlargefamiliesareatincreasedriskofasthma.d.Frequentbathingcaninfluencethedevelopmentoftheimmunesystemalonganon-allergicpathway.17.Riskfactorsfordevelopmentofpersistentasthmainclude:a.Oneepisodeofwheezingbeforeage3.b.Developmentofwheezingafterage3.c.Wheezingapartfromcoldsandfoodsensitivities.d.Useofbronchodilators.18.Inhaledcorticosteroids:a.Changetheunderlyingdiseaseprocessofasthma.b.Donotprovidecontrolandpreventionofsymptomsduringuse.c.Increaseasthmasymptomsandhyper-responsivenesswhenwithdrawn.d.Helptoslowprogressivelossoflungfunctioninpatients.(answersheetonnextpage)
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
44/50
Asthma
AnswerSheet
Asthma
Name(Pleaseprintyourname):_____________________________________________Date:__________________
Passingscoreis80%
1._____2._____3._____4._____5._____6._____7._____8._____9._____10._____11._____12._____
13._____14._____15._____16._____17._____18._____(continuedonnextpage)
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
45/50
Asthma
CourseEvaluation
Pleaseusethisscaleforyourcourseevaluation.Itemswithasterisks(*)arerequired.
5=Stronglyagree4=Agree3=Neutral2=Disagree1=Stronglydisagree*1.Uponcompletionofthecourse,Iwasableto:
a.Describetheclinicalcharacteristicsandpathophysiologyofasthma...5..4..3..2..1b.Outlinethepathophysiologicmechanismsinthedevelopmentofairwayinflammation
..5..4..3..2..1c.Discussthehostandenvironmentalfactorsthatcontributetothedevelopmentofasthma...5..4..3..2..1d.Discussthenaturalhistoryofasthmainchildrenandadults...5..4..3..2..1e.Summarizetheeffectofinterventionsonnaturalhistoryofasthma...5..4..3..2..1*2.Thecoursewaswritteninawaythatfacilitatedmylearning.
..5..4..3..2..1*3.Thiscoursewasfreefromcommercialbias.
..5..4..3..2..1(continuedonnextpage)
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
46/50
Asthma
*4.Thecoursemetmycontinuingeducationneeds.
..5..4..3..2..1*5.Thematerialpresentedwassupportedbyevidence...5..4..3..2..1*6.Theauthoravoidedtheuseofanecdotalinformationasthemainsourceofmaterial...5..4..3..2..1*7.Thecoursewasfreeofproductpromotion...Yes..No****Ifyouansweredno,pleaseanswer#8.8.Wasproductpromotionthesolepurposeofthepresentation?..Yes..No*9.Ittookme60minutespercontacthourtocompletethecourse,test,andevaluation...Yes..No****Ifyouranswerwasno,howlongdidittake?_____________________________
(continuedonnextpage)
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
47/50
Asthma
10.Myprofessionaleducationallevelis(checkone):Nursing
..NurseAide..LVN/LPN..RN(diploma)..RN(AD)
..BSN..MSN..NursePractitioner/AdvancedPracticeNurse
..PhD/DNScTherapy
..OTAide..COTA..OT..MOT..OTD
..PTAide..PTA..PT..MPT..MSPT..DPT..PhDOther(pleasespecify):_________________________________________11.IheardaboutATrainEducationfrom:..Searchengine..Advertisement..GovernmentorBoardwebsite..ReturningcustomerFriend..Publication(Magazine,etc.)
..Other__________________________12.IfoundtheATrainCEU.comwebsiteeasytouse:..Yes..No13.Commentsorsuggestions(optional):
(Registrationinformationonnextpage)
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
48/50
Asthma
RegistrationInformation
Pleaseanswerallofthefollowingquestions(*required).
*Name:_________________________________________________________________*Address:_________________________________________________________________*City:______________________________________________State:______Zip:_________*Phone:_____________________________________________________________________*ProfessionalDesignation:___________________________________________________*LicenseNumberandState:_________________________________________________Pleaseemailmycertificate:..Yes..NoEmail(requiredifyouwantyourcertificatesentbyemail):_____________________(IfyourequestanemailcertificatewewillnotsendacopyofthecertificatebyUSMail.)
PaymentOptions
Youmaypaybycreditcardorbycheck.
Filloutthissectiononlyifyouarepayingbycreditcard.2contacthours:$18
Creditcardinformation:
Name_______________________________________________________________________
Address(ifdifferentfromabove):____________________________________________
City:__________________________________________________State:____Zip:________
Cardtype:..Visa..MC..AmericanExpress..Discover
Cardnumber_________________________________________CVS#________________
Expirationdate______________________________________________________________
TestCompletionandMailingInstructions
1.Completeallforms:..AnswerSheet..EvaluationLearningActivity..RegistrationForm(thispage)2.Ifyouarepayingbycheck,prepareacheckfor$18madeouttoATrainEducat
ion,Inc.3.Mailthecompletedformsandyourpaymentto:ATrainEducation,Inc5171RidgewoodRdWillits,CA95490Whenwereceiveyourformsandpayment,wewillmail(oremail,ifyourequestit)yourcertificateofcompletion.Ifyouhaveanyquestionsorconcerns,pleasecallorcontactusatSharon@ATrainCEU.com.AndthanksfortakingtheATrain!
-
7/31/2019 7 Asthma Patho
49/50
ATrainEducation,Inc.707459-1315
-
7/31/2019 7 Asthma Patho
50/50