6.pndfs april 14 2010- Dr. Marife Yap
56
Dr Marife C Yap Associate Dean Ateneo School of Medicine and Public Health MECYap 14 April 2010 Health Financing Summit
-
Upload
psecp -
Category
Health & Medicine
-
view
1.662 -
download
4
description
Dr. Maria Eufemia C. Yap, M.D., M.Sc.Serving as Associate Dean Dr. Yap finished with a Bachelor of Science degree in Biology from the Ateneo in 1983. She pursued her medical studies at the Far Eastern University - Nicanor Reyes Medical Foundation in 1987. She attended the University of Heidelberg, where she graduated Master of Science in Community Health and Health Management in 1997. She has held positions in the Ateneo’s health-related projects such the Center for Community Services (CCS) and Health Alternatives for Total Human Development Institute (HEALTHDEV), before she joined the AGSB as a faculty member and then as Associate Director and Assistant to the Vice President for the Professional Schools. Since 2003, she has been Director of the AGSB's Health Unit.[1]
Transcript of 6.pndfs april 14 2010- Dr. Marife Yap
Dr Marife C YapAssociate Dean
Ateneo School of Medicine and Public Health
MECYap 14 April 2010Health Financing Summit

Brief Review: Historical Context Rationale PNDFS and its Mechanisms Pre-requisites and Implications: Implementing the
PNDFS
MECYap 14 April 2010Health Financing Summit

ASSESSMENT OF THE HEALTH TARGETS OF THE MEDIUM TERM PHILIPPINE DEVELOPMENT PLANRamon Pedro Paterno M.D. Paolo Victor N. Medina M.D.

Reduce the cost of medicines commonly bought by the poor to half of their 2004 prices and make these available nationwide through a distribution network as determined by DOH, in coordination with the PITC
Reduce the Cost of Medications by Half

Achievements Generics Act of 1988 Enactment into law of Republic Act 9502 –
“Universally Accessible Cheaper and Quality Medicines Act of 2008” Maximum Drug Retail Price Executive Order
22 Selected drugs reduced to half of their prices as mandated by law
Augment and Strengthen Generics Act, Pharmacy Act and Intellectual Property Act
Signing into law of Republic Act 9711 – “Food and Drug Administration Act” to ensure quality of drugs
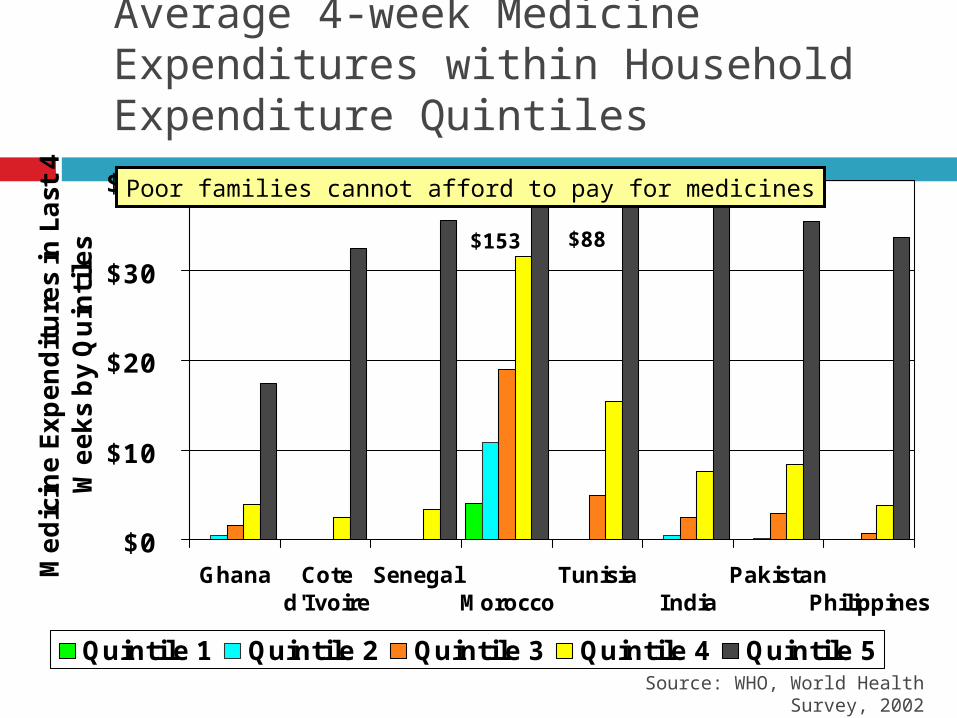
Source: WHO, World Health Survey, 2002
Average 4-week Medicine Expenditures within Household Expenditure Quintiles
$0
$10
$20
$30
$40
Ghana Coted'Ivoire
Senegal Morocco
Tunisia India
Pakistan Philippines
Medic
ine E
xpendit
ure
s in
Last
4
Weeks
by
Quin
tile
s
Quintile 1 Quintile 2 Quintile 3 Quintile 4 Quintile 5
$88$153
Poor families cannot afford to pay for medicines

Recommendations
We have to go BEYOND: Cheaper and Quality Medicines Law Maximum Drug Retail Price EO Food and Drug Authority Law Generics Act of 1988
Expand coverage of MDRP to include ALL essential medications
Increase and sustain awareness and support of using generics not only among consumers, but among health professionals as well
To many Filipinos, good health has always been associated with the availability of medicines and the capacity to purchase these medicines and complete the prescribed dosage;
It is not any wonder therefore that many lay persons (non-health professionals) premise their clamor for cheaper quality medicines on the assumption and definition that
MECYap 14 April 2010Health Financing Summit
Bengzon et al, 2007
April 1987: Promulgation of the PNDP◦ Quality Assurance◦ Rational Drug Use◦ Self Reliance◦ Tailored Procurement
The Philippine National Drug Formulary (PNDF) or the EDL which was based on the WHO World Drug Situation Report and the UNIDO-sponsored Pharmaceutical Industry Development Study was the MAIN INSTRUMENT for promoting access to essential drugs
MECYap 14 April 2010Health Financing Summit
Bengzon et al, 2007

The Generics Act of 1988 is the legal instrument for the promotion of rational drug use (RA 6675, passed Sept 1988)
“While the PNDP and the Generics Act were conceived independently, they evolved into synergistic efforts because of a congruency of objectives with respect to rational drug use.”
MECYap 14 April 2010Health Financing Summit
Bengzon et al, 2007

MECYap 14 April 2010Health Financing Summit
“Government, because of the immense powers at its disposal, can readily institute measures to respondto the problems raised to its attention. In doing so,
however, approaches may be over simplistic,indicating a failure to appreciate the immensity and
complexity of the proposed area of reform. Suchquick fixes, at best, provide temporary relief from the
symptoms of the ills; in the worst case, long-termcomplications could arise. Without the benefit of
thorough diagnosis and management, a cure cannotbe effected.”
Bengzon et al, 2007

“The Philippine National Drug Policy provides a framework that weaves together the various elements necessary to effect successful reform in the area of pharmaceuticals.”
E.O. 49, Jan 21, 1993: “Directing the Mandatory Use of the Phil National Formulary Vol 1 as the Basis for Procurement of Drug Products by the Government”
A.O. 163 s. 2002: “Implementing Guidelines and Procedures in the Procurement and Requisition of Drugs and Medicines by the DOH pursuant to E.O. 49” – procedural bases
22 January 2009Health Financing Summit
Bengzon et al, 2007

Impetus and Drivers of Change:◦ Globalization and its impact on the procurement and
utilization of drugs and medicines◦ Economic and Financial Challenges◦ Drivers of Technology and Information that allow greater
access of knowledge by people potentially moving towards greater empowerment and participation
MECYap 14 April 2010Health Financing Summit

Drug Formulary - a continually updated list of medications and related information, representing the
clinical judgement of physicians, pharmacists and other experts in the diagnosis and/or treatment of
disease and promotion of health.
Drug Formulary System - an ongoing process whereby a health care organization, through its physicians, pharmacists, and other health care
professionals, establishes policies on the use of drug products and therapies, and identifies drug products
and therapies that are the most medically appropriate and cost-effective to best serve the health interests of
a given patient population.
MECYap 14 April 2010Health Financing Summit
Principles of a Drug Formulary System, October 2000

A.O. 2006-0018: Implementing Guidelines of the Philippine National Drug Formulary System
“After reviewing the implementing policies and procedures that ensure the use of the PNDF and the instruments used for the drug inclusion in and deletion from the formulary, the DOH finds it necessary to revise the inputs, processes, and outputs of the PNDF, collectively referred to, thereafter as the Philippine National Drug Formulary System (PNDFS)
MECYap 14 April 2010 Health Financing Summit

To revise the inputs, processes, and outputs of the PNDF
The PNDF SYSTEM◦ Scope
Drug Procurement Guidelines for all government health facilities, units and offices
Guidelines on PhilHealth claims and reimbursements for the entire health sector (public and private)
MECYap 14 April 2010Health Financing Summit

MECYap 14 April 2010Health Financing Summit
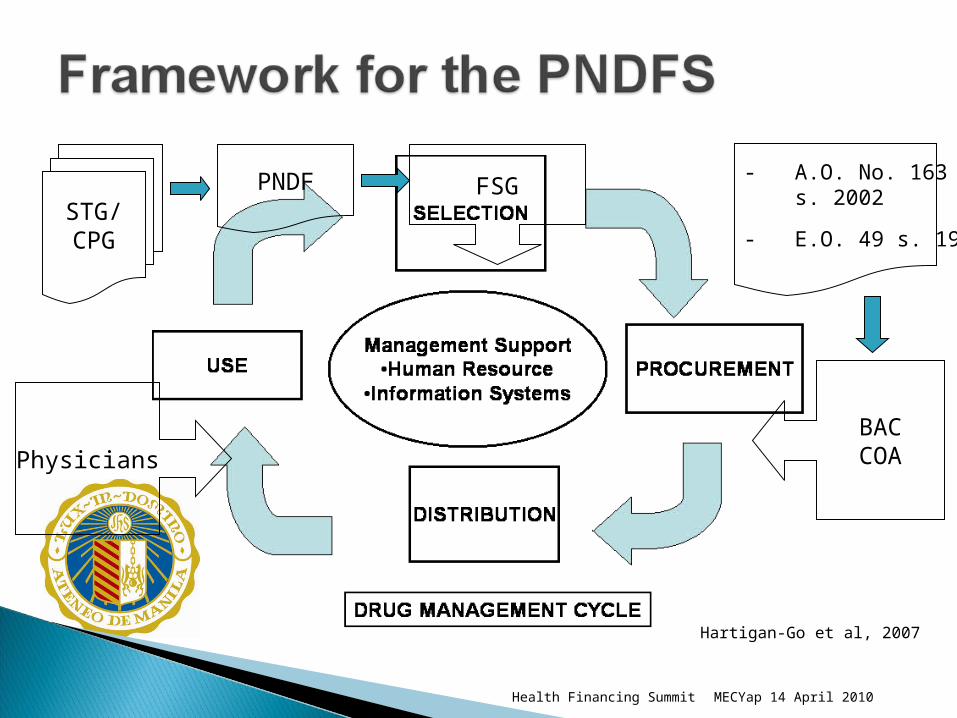
USE
SELECTION
DISTRIBUTION
PROCUREMENT
DRUG MANAGEMENT CYCLE
Management Support•Human Resource
•Information Systems
Hartigan-Go et al, 2007

Formulary list◦ A drug selection tool
Formulary manual◦ A source of drug information
Formulary system◦ A drug management process◦ The whole system for developing, updating, and
promoting the formulary list or EDL
MECYap 14 April 2010Health Financing Summit
Hartigan-Go et al, 2007
MECYap 14 April 2010Health Financing Summit
Physicians
FSGPNDFSTG/CPG
BACCOA
- A.O. No. 163 s. 2002
- E.O. 49 s. 1993
Hartigan-Go et al, 2007

MECYap 14 April 2010Health Financing Summit
FORMULARY
LGU -COBAC
For Procurement
PRIVATE AND PUBLIC PHYSICIANS in prescribing
medicines
PHILHEALTH
3RD PARTY PAYORS
To determine reimbursements
BENEFICIARIES
To obtain information on
the drugs, including prices
Hartigan-Go et al, 2007

A structure◦ The Formulary Study Group (FSG)
A process◦ The Formulary Selection Algorithm (FSA)
An output◦ The Formulary Manual (or the PNDF)
MECYap 14 April 2010Health Financing Summit
Components of the PNDF System (PNDFS)

The Formulary Executive Council (FEC) The Epidemiology Committees (EC)
◦ The Clinical Epidemiology Sub-committee (CES)◦ The Public Health Epidemiology Sub-committee (PHES)
The Pharmacology Committee (PC)
22 January 20092nd MeTA National Forum

Identify common health problems Select clinical practice guidelines (CPG) Assess cost-effectiveness of CPG drugs
MECYap 14 April 2010Health Financing Summit

Assess pharmacokinetic and –dynamic properties Approval or disapproval If disapproved, appeal to the USEC Health
Regulations
MECYap 14 April 2010Health Financing Summit

Clinical Practice Guidelines Public Health Practice Guidelines Essential Drug List Formulary Cross-reference Index
MECYap 14 April 2010Health Financing Summit

PNDF Manual to be published by DOH with assistance from PHIC
USEC for Health Regulations will supervise and guide the FSG
PHIC will provide administrative and secretariat functions for the EC and the PC
MECYap 14 April 2010Health Financing Summit

NDPP will provide administrative and secretariat functions for the FEC
BFAD will provide technical inputs and essential data requirements
PNDF will be basis of government procurement (EO 49)
MECYap 14 April 2010Health Financing Summit

Philhealth will only reimburse drugs in PNDF PNDF will be regularly updated (RA 6675)
MECYap 14 April 2010Health Financing Summit

DOH Secretary may authorize procurement of drugs not listed in the PNDF
All drug establishments must have a copy of the PNDF
BFAD-withdrawn drugs will be automatically delisted from the PNDF
MECYap 14 April 2010Health Financing Summit

MECYap 14 April 2010Health Financing Summit

Structure Process Outcome
MECYap 14 April 2010Health Financing Summit

The Formulary Study Group◦ The Formulary Executive Council (FEC)◦ The Epidemiology Committees (EC)
The Clinical Epidemiology Sub-committee (CES) The Public Health Epidemiology Sub-committee (PHES)
◦ The Pharmacology Committee (PC)
MECYap 14 April 2010Health Financing Summit

Identify common health problems Select clinical practice guidelines (CPG) Assess cost-effectiveness of CPG drugs
MECYap 14 April 2010Health Financing Summit

Frequency Severity
MECYap 14 April 2010Health Financing Summit

Burden of disease (BOD) ◦ A measurement of the gap between current health status
and an ideal situation where everyone lives into old age free of disease and disability
MECYap 14 April 2010Health Financing Summit

Sources of CPGs◦ DOH or PHIC◦ Professional medical societies in the Philippines◦ CPGs in Philippines-similar countries (ASEAN or
Latin American countries)◦ WHO◦ Cochrane Registry◦ CPGs from any country
MECYap 14 April 2010Health Financing Summit
Identify and enumerate drugs recommended in CPG for each of the priority diseases
MECYap 14 April 2010Health Financing Summit

Search databases◦ MEDLINE◦ EMBASE◦ SCISEARCH ◦ Google Scholar
MECYap 14 April 2010Health Financing Summit

Critical appraisal of CPG◦ Study validity◦ Incremental costs and outcomes◦ Generalizability
Hayward RSA et al. How to Use a Clinical Practice Guideline. JAMA (1995;274(7):570-4) and (1995;274(20):1630-2).
MECYap 14 April 2010Health Financing Summit

Conduct periodic drug utilization review of priority drugs
Rationale◦ Evaluates capability of the health workers to use the
drug◦ Basis for continued inclusion or deletion of drug from
PNDF
MECYap 14 April 2010Health Financing Summit
PHIC claims Special surveys of
◦ DOH and private hospitals◦ RHUs
MECYap 14 April 2010Health Financing Summit

Establish responsibility Develop scope of activities Establish criteria Perform DUR and collect data Analyze data Develop recommendations and plan of action Perform follow-up
MECYap 14 April 2010Health Financing Summit

MECYap 14 April 2010Health Financing Summit

Pharmacology Committee is part of the Formulary Study Group
The Committee will do drug evaluations (2 or 3 doctors with pharmacology background, 2 or 3 pharmacists)
Supported by a team of researchers within the secretariat (3 full time researchers with pharmacology or pharmaceutical science qualifications)
All willing to honestly declare conflict/vested interest and to sign confidentiality disclosure
MECYap 14 April 2010Health Financing Summit

Receives drug sets from Epidemiology Committee
Evaluates drugs on the basis of safety
Submits evaluation back to Epidemiology Committee for cost-effectiveness analysis
Have joint deliberations with Epidemiology Committee
Have specific EDL medicines listed in the PNDF only if there is evidence that the generic drug has bio-availability or bio-equivalence data, when required and comes from a drug industry with certified full compliance to cGMP.
MECYap 14 April 2010Health Financing Summit

Support the Pharmacology Committee in matters of organizing literature research for evaluation
Scan the horizon for unsafe drugs that are in the formulary or proposed to be entered into the formulary and send Flags to the sub-committee
Following the joint deliberations of the Pharmacology & Epidemiology Committees, to prepare the write ups of the formulary using a standard framework.
MECYap 14 April 2010Health Financing Summit

The Epidemiology Committee – priority medical conditions and sets of drugs identified for further evaluation
Knowledge of unsafe drugs (for deletions)
Output: a list of less risky drugs.
MECYap 14 April 2010Health Financing Summit

Withdrawn from other countries Evidence of causing deaths or major organ
system damage (Signals) Estimates of risk: 1:10,000 vs 1:1000 If drug is deleted or removed, will it cause great
harm to sick population who needs this medicine?
MECYap 14 April 2010Health Financing Summit

The current anatomic organ-systems of medical conditions can be maintained
Redefine Core and Complementary listing in sync with WHO usage
Set of public health outpatient drug use (in primary care setting) and a set of hospital drugs. One or two prototype drugs per drug category
will be offered Clinical usage information for doctors and other
health professionals
MECYap 14 April 2010Health Financing Summit

MECYap 14 April 2010Health Financing Summit

To provide the framework on which the PNDFS is based;
To provide guideposts on the functions, roles and interactions of the key members and implementers of the PNDFS;
To define and articulate the relationships among the sub-committees and the secretariat for smooth functioning of the PNDFS;
To begin thinking through a transition plan for a seamless shift from the current system to the PNDFS.
MECYap 14 April 2010Health Financing Summit

Secretary of Health
Undersecretary of Health for Regulations
Formulary Executive Council (FEC)
Epidemiology Committees
Clinical Epi Subcomm Public Health Epi Subcomm
Pharmacology Committee
FSG / NFC SecretariatF
S
G
F
S
G
MECYap 14 April 2010Health Financing Summit
Accountability Alignment Transparency Strategic and critical alliances and partnership
MECYap 14 April 2010Health Financing Summit

MECYap 14 April 2010Health Financing Summit

Building on the gains from the past Parallel efforts
◦ Arrive at an alignment of where the PNDFS is to be brought (the envisioned state)
Information as tool◦ The very nature of the PNDFS as a SYSTEM requires
that all service users and stakeholders are informed and updated.
Staying the course
MECYap 14 April 2010Health Financing Summit

Implementation of the PNDFS should be in context with the components of HSRA and FOURmula ONE.
Implementation should be done in small, manageable and systematic phases.
PNDFS is just one of the tools to address drug access.
PNDFS provides more stakeholders an opportunity to improve on the gains, deal with issues in a more rigorous, multi-faceted approach.
MECYap 14 April 2010Health Financing Summit