6Bones and Joints - Mrs. Pillar's A & P Website
40
Skeletal System: Bones and Joints 6 E R 110 Module 5 Skeletal System LEARN TO PREDICT Dr. Thomas Moore and Dr. Roberta Rutledge had worked together for almost two decades, and Roberta knew something was bothering Thomas. She noticed him wincing in pain whenever he bent down to retrieve something from a bottom shelf, and he was short- tempered rather than his usual happy self. Roberta knew Thomas would never admit to being injured if it meant he couldn’t care for his patients, even if only for a few days. Finally, Roberta convinced him to let her x-ray his lower back. Right away, when Roberta showed Thomas the x-ray, he pointed to the cause of the pain he’d been suffering. Using knowledge of the vertebral column, predict the source of Thomas’s pain, based on his x-ray shown in this photo. Also, using your knowledge of vertebral anatomy, predict the region of the injury and explain why this region of the vertebral column is more prone to this type of injury than other regions. limited movement; others allow no apparent movement. The struc- ture of a given joint is directly correlated to its degree of movement. Although the skeleton is usually thought of as the framework of the body, the skeletal system has many other functions in addi- tion to support. The major functions of the skeletal system include: 1. Support. Rigid, strong bone is well suited for bearing weight and is the major supporting tissue of the body. Cartilage provides firm yet flexible support within certain structures, such as the nose, external ear, thoracic cage, and trachea. Ligaments are strong bands of fibrous connective tissue that attach to bones and hold them together. 2. Protection. Bone is hard and protects the organs it surrounds. For example, the skull encloses and protects the brain, and the vertebrae surround the spinal cord. The rib cage protects the heart, lungs, and other organs of the thorax. 6.1 FUNCTIONS OF THE SKELETAL SYSTEM Learning Outcome After reading this section, you should be able to A. Explain the functions of the skeletal system. Sitting, standing, walking, picking up a pencil, and taking a breath all involve the skeletal system. Without the skeletal system, there would be no rigid framework to support the soft tissues of the body and no system of joints and levers to allow the body to move. The skeletal system consists of bones, such as those shown in figure 6.1, as well as their associated connective tissues, which include cartilage, tendons, and ligaments. The term skeleton is derived from a Greek word meaning dried. But the skeleton is far from being dry and nonliving. Rather, the skeletal system consists of dynamic, living tissues that are able to grow, detect pain stimuli, adapt to stress, and undergo repair after injury. A joint, or an articulation, is a place where two bones come together. Many joints are movable, although some of them allow only
Transcript of 6Bones and Joints - Mrs. Pillar's A & P Website

Skeletal System: Bones and Joints6
c H a P t E rc H a P t E r
110
Module 5 SkeletalSystem
lEarnToPrEDictDr.thomasMooreandDr.robertarutledgehadworkedtogether for almost two decades, and roberta knewsomething was bothering thomas. She noticed himwincing in pain whenever he bent down to retrievesomething from a bottom shelf, and he was short-temperedratherthanhisusualhappyself.robertaknewthomaswouldneveradmittobeinginjuredif itmeanthe couldn’t care for his patients, even if only for a fewdays.Finally,robertaconvincedhimtoletherx-rayhislowerback.rightaway,whenrobertashowedthomasthex-ray,hepointedtothecauseofthepainhe’dbeensuffering.
using knowledge of the vertebral column, predictthesourceofthomas’spain,basedonhisx-rayshowninthis photo. also, using your knowledge of vertebralanatomy, predict the region of the injury and explainwhythisregionofthevertebralcolumnismorepronetothistypeofinjurythanotherregions.
limitedmovement;othersallownoapparentmovement.Thestruc-tureofagivenjointisdirectlycorrelatedtoitsdegreeofmovement. Althoughtheskeletonisusuallythoughtofastheframeworkofthebody,theskeletalsystemhasmanyotherfunctionsinaddi-tiontosupport.Themajorfunctionsoftheskeletalsysteminclude:
1. Support.Rigid,strongboneiswellsuitedforbearingweightandisthemajorsupportingtissueofthebody.Cartilageprovidesfirmyetflexiblesupportwithincertainstructures,suchasthenose,externalear,thoraciccage,andtrachea.Ligamentsarestrongbandsoffibrousconnectivetissuethatattachtobonesandholdthemtogether.
2. Protection.Boneishardandprotectstheorgansitsurrounds.Forexample,theskullenclosesandprotectsthebrain,andthevertebraesurroundthespinalcord.Theribcageprotectstheheart,lungs,andotherorgansofthethorax.
6.1 FunctionSoFtHESKElEtalSYStEM
Learning Outcome After reading this section, you should be able to
A. Explainthefunctionsoftheskeletalsystem.
Sitting,standing,walking,pickingupapencil,andtakingabreathall involvetheskeletalsystem.Withouttheskeletalsystem,therewould be no rigid framework to support the soft tissues of thebody and no system of joints and levers to allow the body tomove.Theskeletalsystemconsistsofbones,suchasthoseshowninfigure6.1,aswellastheirassociatedconnectivetissues,whichinclude cartilage, tendons, and ligaments. The term skeleton isderivedfromaGreekwordmeaningdried.Buttheskeletonisfarfrombeingdryandnonliving.Rather,theskeletalsystemconsistsofdynamic,livingtissuesthatareabletogrow,detectpainstimuli,adapttostress,andundergorepairafterinjury. A joint,oranarticulation, isaplacewheretwobonescometogether.Manyjointsaremovable,althoughsomeofthemallowonly
see78267-Chapter06.indd 110 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 111Skeletal
3. Movement.Skeletalmusclesattachtobonesbytendons,whicharestrongbandsofconnectivetissue.Contractionoftheskeletalmusclesmovesthebones,producingbodymovements.Joints,wheretwoormorebonescometogether,allowmovementbetweenbones.Smoothcartilagecoverstheendsofboneswithinsomejoints,allowingthebonestomovefreely.Ligamentsallowsomemovementbetweenbonesbutpreventexcessivemovement.
4. Storage.Somemineralsintheblood—principally,calciumandphosphorus—aretakenintoboneandstored.Shouldbloodlevelsofthesemineralsdecrease,themineralsarereleasedfromboneintotheblood.Adiposetissueisalsostoredwithinbonecavities.Ifneeded,thelipidsarereleasedintothebloodandusedbyothertissuesasasourceofenergy.
5. Blood cell production.Manybonescontaincavitiesfilledwithredbonemarrow,whichproducesbloodcellsandplatelets(seechapter11).
6.2 ExtracEllularMatrixLearning Outcome After reading this section, you should be able to
A. Describethecomponentsoftheextracellularmatrix,andexplainthefunctionofeach.
Thebone,cartilage,tendons,andligamentsoftheskeletalsystemare all connective tissues. Their characteristics are largely deter-minedbythecompositionoftheirextracellularmatrix.Thematrixalways contains collagen, ground substance, and other organic
molecules,aswellaswaterandminerals.Butthetypesandquan-titiesofthesesubstancesdifferineachtypeofconnectivetissue. Collagen (kol′lă-jen; koila, glue + -gen, producing) is atough,ropelikeprotein.Proteoglycans(prō′tē-ō-glī′kanz;proteo,protein+glycan,polysaccharide)arelargemoleculesconsistingofpolysaccharidesattachedtocoreproteins,muchastheneedlesofapinetreeareattachedtothetree’sbranches.Theproteoglycansformlargeaggregates,muchaspinebranchescombinetoformawholetree.Proteoglycanscanattractandretainlargeamountsofwaterbetweentheirpolysaccharide“needles.” Theextracellularmatrixof tendons and ligaments containslarge amounts of collagen fibers, making these structures verytough, like ropes or cables. The extracellular matrix of cartilage(kar′ti-lij) contains collagen and proteoglycans. Collagen makescartilage tough, whereas the water-filled proteoglycans make itsmoothandresilient.Asaresult,cartilageisrelativelyrigid,butit springs back to its original shape after being bent or slightlycompressed.Itisanexcellentshockabsorber. Theextracellularmatrixofbonecontainscollagenandminer-als,includingcalciumandphosphate.Theropelikecollagenfibers,likethereinforcingsteelbarsinconcrete,lendflexiblestrengthtothe bone. The mineral component, like the concrete itself, givesthe bone compression (weight-bearing) strength. Most of themineralinboneisintheformofcalciumphosphatecrystalscalledhydroxyapatite(hī-drok′sē-ap-ă-tīt).
Predict 2
What would a bone be like if all of the minerals were removed? What would it be like if all of the collagen were removed?
acaSEinPoint
Brittle Bone Disease
Maytrix isa10-year-old girlwhohasahistory ofnumerous brokenbones.atfirst,physicianssuspectedshewasavictimofchildabuse,but eventually they determined that she has brittle bone disease,or osteogenesis imperfecta, which literally means imperfect boneformation. May is short for her age, and her limbs are short andbowed.Hervertebralcolumnisalsoabnormallycurved.Brittlebonedisease is a rare disorder caused by any one of a number of faultygenes that results in either too little collagen formation or poorqualitycollagen.asaresult,thebonematrixhasdecreasedflexibilityandismoreeasilybrokenthannormalbone.
6.3 GEnEralFEaturESoFBonELearning Outcomes After reading this section, you should be able to
A. Explainthestructuraldifferencesbetweencompactboneandspongybone.
B. outlinetheprocessesofboneossification,growth,remodeling,andrepair.
Therearefourcategoriesofbone,basedontheirshape:long,short,flat,andirregular.Long bonesarelongerthantheyarewide.Mostofthebonesoftheupperandlower limbsare longbones.Short bones areapproximatelyasbroadas theyare long;examplesarethebonesofthewristandankle.Flat boneshavearelativelythin,
Skull
Sternum
RadiusUlna
Vertebralcolumn
Ribs
Clavicle
Humerus
Femur
Tibia
Fibula
Pelvis
Figure 6.1 Major Bones of the Skeletal System
see78267-Chapter06.indd 111 11-12-01 3:25 PM

112 Chapter 6Sk
elet
al
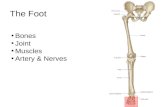
StructureofalongBoneAlongboneservesasausefulmodelforillustratingthepartsofa typical bone (figure 6.2). Each long bone consists of a centralshaft,calledthediaphysis(dī-af′i-sis;growingbetween),andtwo
flattenedshape.Examplesofflatbonesarecertainskullbones,theribs, the scapulae (shoulder blades), and the sternum. Irregular bones include thevertebraeandfacialbones,whichhaveshapesthatdonotfitreadilyintotheotherthreecategories.
Epiphysis
Articular cartilage
Diaphysis
Compact bone
Medullary cavity (containsred marrow in juveniles andyellow marrow in adults)
Periosteum
Endosteum
Epiphyseal linesin adults
Epiphyseal platesin juveniles
Diaphysis
Spongy bone
Adult bone
Young bone
Endosteum
Central canals
Connecting vessels
Osteons(haversian systems)
Inner layer
Outerlayer
Compact bone
Medullarycavity
Periosteum
Spongy bonewith trabeculae
Adult bone
Figure 6.2 Structure of a Long Bone(a)Younglongbone(thefemur)showingtheepiphysis,epiphysealplates,anddiaphysis.(b)adultlongbonewithepiphyseallines.(c)internalfeaturesofaportionofthediaphysisin(a).
(a)
(c)
(b)
see78267-Chapter06.indd 112 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 113Skeletal
HistologyofBoneThe periosteum and endosteum contain osteoblasts (os′tē-ō-blasts; bone-forming cells), which function in the formation ofbone, as well as in the repair and remodeling of bone. Whenosteoblastsbecomesurroundedbymatrix,theyarereferredtoasosteocytes(os′tē-ō-sītz;bonecells). Bone is formed in thin sheets of extracellular matrix calledlamellae (lă-mel′ē; plates), with osteocytes located between thelamellae within spaces called lacunae (lă-koo′nē; a hollows)(figure6.3).Cellprocessesextendfromtheosteocytesacrosstheextracellularmatrixofthelamellaewithintinycanalscalledcana-liculi(kan-ă-lik′ū-lī;sing.canaliculus,littlecanal). Therearetwomajortypesofbone,basedontheirhistologicalstructure.Compact boneismostlysolidmatrixandcells.Spongy bone,orcancellous(kan′sĕ-lŭs)bone,consistsofalacynetworkofbonewithmanysmall,marrow-filledspaces.
Compact BoneCompactbone(figure6.3)formsmostofthediaphysisoflongbonesandthe thinnersurfacesofallotherbones.Mostof the lamellaeofcompactboneareorganizedintosetsofconcentricrings,witheachsetsurroundingacentral canal,orHaversian(ha-ver′shan)canal.Bloodvesselsthatrunparalleltothelongaxisoftheboneare contained within the central canals. Each central canal, withthe lamellae and osteocytes surrounding it, is called an osteon(os′tē-on),orHaversian system.Eachosteon,seenincrosssection,lookslikeamicroscopictarget,withthecentralcanalasthe“bull’s-eye”(figure6.3).Osteocytes,locatedinlacunae,areconnectedtooneanotherbycellprocessesincanaliculi.Thecanaliculigivetheosteontheappearanceofhavingtinycrackswithinthelamellae.
ends,eachcalledanepiphysis(e-pif′i-sis;growingupon).Athinlayerofarticular(ar-tik′ū-lăr;joint)cartilagecoverstheendsoftheepiphyseswherethebonearticulates(joins)withotherbones.A long bone that is still growing has an epiphyseal plate, orgrowth plate, composedof cartilage,betweeneachepiphysis andthediaphysis(figure6.2a).Theepiphysealplateiswherethebonegrows in length. When bone growth stops, the cartilage of eachepiphysealplate is replacedbyboneandbecomesanepiphyseal line(figure6.2b). Bonescontaincavities,suchasthelargemedullary cavityinthediaphysis, aswellas smallercavities in theepiphysesof longbones and in the interior of other bones. These spaces are filledwith soft tissue called marrow. Yellow marrow consists mostlyof adipose tissue. Red marrow consists of blood-forming cellsandistheonlysiteofbloodformationinadults(seechapter11).Children’s bones have proportionately more red marrow thando adult bones because, as a person ages, red marrow is mostlyreplacedbyyellowmarrow.Inadults, redmarrowisconfinedtothebonesinthecentralaxisofthebodyandinthemostproximalepiphysesofthelimbs. Mostoftheoutersurfaceofboneiscoveredbydenseconnec-tive tissue called the periosteum (per-ē-os′tē-ŭm; peri, around+osteon,bone),whichcontainsbloodvesselsandnerves(figure6.2c).Thesurfaceofthemedullarycavityislinedwithathinnerconnec-tivetissuemembrane,theendosteum(en-dos′tē-ŭm;endo,inside).
Lamellae between osteons
Periosteum
Blood vesselconnecting to a central canalbetween osteons
Blood vesselsconnecting to a central canal
Blood vesselswithin a central(Haversian) canal
Lamellae on surface of boneConcentric rings
of lamellae
OsteonOsteon
Blood vessel withinthe periosteum
Canaliculi
Osteocytes inlacunae
Canaliculi
Lacunae
Central canal
LM 400x
(a)(b)
Figure 6.3 Structure of Bone Tissue(a)Photomicrographofcompactbone.(b)Finestructureofcompactbone.
see78267-Chapter06.indd 113 11-12-01 3:25 PM

114 Chapter 6Sk
elet
al
BoneossificationOssification (os′i-fi-kā′shŭn; os, bone+ facio, to make) is theformation of bone by osteoblasts. After an osteoblast becomescompletely surrounded by bone matrix, it becomes a maturebone cell, or osteocyte. In the fetus, bones develop by two pro-cesses,eachinvolvingtheformationofbonematrixonpreexistingconnectivetissue(figure6.5).Boneformationthatoccurswithinconnective tissue membranes is called intramembranous ossifi-cation, and bone formation that occurs inside cartilage is calledendochondralossification.Bothtypesofboneformationresultincompactandspongybone.
Nutrients leave the blood vessels of the central canals anddiffuse to the osteocytes through the canaliculi. Waste productsdiffuseintheoppositedirection.Thebloodvesselsinthecentralcanals, inturn,areconnectedtobloodvessels intheperiosteumandendosteum.
Spongy BoneSpongybone,socalledbecauseofitsappearance,islocatedmainlyin the epiphyses of long bones. It forms the interior of all otherbones. Spongy bone consists of delicate interconnecting rods orplates of bone called trabeculae (tră-bek′ū-lē; beams), whichresemblethebeamsorscaffoldingofabuilding(figure6.4a).Likescaffolding, the trabeculae add strength to a bone without theadded weight that would be present if the bone were solid min-eralizedmatrix.Thespacesbetween the trabeculaeare filledwithmarrow.Eachtrabeculaconsistsofseverallamellaewithosteocytesbetweenthem(figure6.4b).Usually,nobloodvesselspenetratethetrabeculae, and the trabeculae have no central canals. Nutrientsexitvesselsinthemarrowandpassbydiffusionthroughcanaliculitotheosteocytesofthetrabeculae.
Trabeculae
Spaces containingbone marrow andblood vessels
Compact bone
Spongybone
Osteoblast
Osteoclast
Osteocyte
Lamellae Canaliculus
Trabecula
Parietalbone
Ossificationcenter
OssificationcenterSuperior part
of occipitalbone
Inferior partof occipital bone
Temporal bone
Vertebrae
Styloidprocess
Mandible
Maxilla
Zygomatic bone
Frontal bone
Nasal bone
Ethmoid bone
Sphenoid bone
Intramembranousbones forming
Fontanel
Cartilage
Endochondralbones forming
Figure 6.4 Spongy Bone(a)Beamsofbone,thetrabeculae,surroundspacesinthebone.inlife,thespacesarefilledwithredoryellowbonemarrowandwithbloodvessels.(b)transversesectionofatrabecula.
Figure 6.5 Bone Formation in a Fetus(a)intramembranousossificationoccursina12-week-oldfetusatossificationcentersintheflatbonesoftheskull(yellow).Endochondralossificationoccursinthebonesformingtheinferiorpartoftheskull(blue).(b)radiographofan18-week-oldfetus,showingintramembranousandendochondralossification.intramembranousossificationoccursatossificationcentersintheflatbonesoftheskull.Endochondralossificationhasformedbonesinthediaphysesoflongbones.theepiphysesarestillcartilageatthisstageofdevelopment.
(a)
(b)
(a)
(b)
see78267-Chapter06.indd 114 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 115Skeletal
increase in number, enlarge, and die. Then the cartilage matrixbecomescalcified(figure6.6,step2).Asthisprocessisoccurringin thecenterof thecartilagemodel,bloodvesselsaccumulate inthe perichondrium. The presence of blood vessels in the outersurfaceoffuturebonecausessomeoftheunspecifiedconnectivetissuecellsonthesurfacetobecomeosteoblasts.Theseosteoblaststhen produce a collar of bone around part of the outer surfaceof thediaphysis, and theperichondriumbecomesperiosteum inthatarea.Bloodvesselsalsogrowintothecenterofthediaphyses,bringing in osteoblasts and stimulating ossification. The centerpartof thediaphysis,wherebonefirstbeginstoappear, iscalledthe primary ossification center (figure 6.6, step 3). Osteoblastsinvadespacesinthecenteroftheboneleftbythedyingcartilagecells. Some of the calcified cartilage matrix is removed by cellscalled osteoclasts (os′tē-ō-klastz; bone-eating cells), and theosteoblastslineupontheremainingcalcifiedmatrixandbeginto
Intramembranous(in′tră-mem′brā-nŭs)ossificationoccurswhen osteoblasts begin to produce bone in connective tissuemembranes. This occurs primarily in the bones of the skull.Osteoblastslineuponthesurfaceofconnectivetissuefibersandbegin depositing bone matrix to form trabeculae. The processbegins in areas called ossification centers (figure 6.5a), and thetrabeculaeradiateoutfromthecenters.Usually,twoormoreossi-ficationcentersexist ineach flat skullbone,and the skullbonesresultfromfusionofthesecentersastheyenlarge.Thetrabeculaeare constantly remodeled after their initial formation, and theymayenlargeorbereplacedbycompactbone. Thebonesat thebaseoftheskullandmostoftheremainingskeletal system develop through the process of endochondral ossification from cartilage models. The cartilage models havethegeneralshapeofthematurebone(figure6.6,step1).Duringendochondral ossification, cartilage cells, called chondrocytes,
Perichondrium
Cartilage
Perichondrium
Bone collar
Uncalcifiedcartilage
Calcified cartilage
Periosteum
Blood vesselto periosteum
Epiphysis
Epiphysis
Diaphysis
A cartilage model, with the general shape of the mature bone, is produced by chondrocytes. A perichondrium surrounds most of the cartilage model.
2. The chondrocytes enlarge, and cartilage is calcified. A bone collar is produced, and the perichondrium of the diaphysis becomes the periosteum.
3. A primary ossification center forms as blood vessels and osteoblasts invade the calcified cartilage. The osteoblasts lay down bone matrix, forming trabeculae.
4. Secondary ossification centers form in the epiphyses of long bones.
Perichondrium
Bone collar
Cartilage
Calcified cartilage
Periosteum
Blood vessel
Primaryossificationcenter
Trabecula
Medullary cavity
Secondaryossificationcenter
Spongybone
Cartilage
Blood vessel
Calcifiedcartilage
Spongy bone
PeriosteumBone collar
Blood vessel
Medullary cavity
Space inbone
1 2
43
Perichondrium
Cartilage
Perichondrium
Bone collar
Uncalcifiedcartilage
Calcified cartilage
Periosteum
Blood vesselto periosteum
Epiphysis
Epiphysis
Diaphysis
A cartilage model, with the general shape of the mature bone, is produced by chondrocytes. A perichondrium surrounds most of the cartilage model.
2. The chondrocytes enlarge, and cartilage is calcified. A bone collar is produced, and the perichondrium of the diaphysis becomes the periosteum.
3. A primary ossification center forms as blood vessels and osteoblasts invade the calcified cartilage. The osteoblasts lay down bone matrix, forming trabeculae.
4. Secondary ossification centers form in the epiphyses of long bones.
Perichondrium
Bone collar
Cartilage
Calcified cartilage
Periosteum
Blood vessel
Primaryossificationcenter
Trabecula
Medullary cavity
Secondaryossificationcenter
Spongybone
Cartilage
Blood vessel
Calcifiedcartilage
Spongy bone
PeriosteumBone collar
Blood vessel
Medullary cavity
Space inbone
1 2
43
PROCESS Figure 6.6 Endochondral Ossification of a Long Bone
see78267-Chapter06.indd 115 11-12-01 3:25 PM

116 Chapter 6Sk
elet
al
ofthebone,causingthebonetoelongate.Thenthechondrocytesenlargeanddie.Thecartilagematrixbecomescalcified.Muchofthe cartilage that forms around the enlarged cells is removed byosteoclasts, and the dying chondrocytes are replaced by osteo-blasts. The osteoblasts start forming bone by depositing bonelamellae on the surface of the calcified cartilage. This processproducesboneonthediaphysealsideoftheepiphysealplate.
Predict 3
Describe the appearance of an adult if cartilage growth did not occur in the long bones during childhood.
BoneremodelingBone remodelinginvolvestheremovalofexistingbonebyosteoclastsandthedepositionofnewbonebyosteoblasts.Boneremodelingoccursinallbone.Remodelingisresponsibleforchangesinboneshape,theadjustmentofbonetostress,bonerepair,andcalciumionregulationinthebodyfluids.Remodelingisalsoinvolvedin
formbonetrabeculae.Asthebonedevelops,itisconstantlychanging.Amedullarycavityformsinthecenterofthediaphysisasosteo-clastsremoveboneandcalcifiedcartilage,whicharereplacedbybone marrow. Later, secondary ossification centers form in theepiphyses(figure6.6,step4).
BoneGrowthBonegrowthoccursbythedepositionofnewbonelamellaeontoexisting bone or other connective tissue. As osteoblasts depositnewbonematrixonthesurfaceofbonesbetweentheperiosteumand the existing bone matrix, the bone increases in width, ordiameter. This process is called appositional growth. Growth inthelengthofabone,whichisthemajorsourceofincreasedheightinanindividual,occursintheepiphysealplate.Thistypeofbonegrowth occurs through endochondral ossification (figure 6.7).Chondrocytes increase in number on the epiphyseal side of theepiphysealplate.Theylineupincolumnsparalleltothelongaxis
Calcified cartilageis replaced by bone.
Chondrocytesdivide and enlarge.
Length of boneincreases.
Thickness ofepiphysealplate remainsunchanged.
Bone isadded todiaphysis.
Bone of diaphysis
Epiphysealplate
1
2
3
4
Femur
Patella
Epiphysis
Epiphysealplate
Diaphysis
New cartilage isproduced on the epiphyseal sideof the plate as thechondrocytes divideand form stacksof cells.
Chondrocytesmature and enlarge.
Matrix is calcified,and chondrocytesdie.
The cartilage onthe diaphyseal sideof the plate isreplaced by bone.
Epiphyseal side
Diaphyseal side
1
2
3
4LM 400x
1
2
3
4
PROCESS Figure 6.7 Endochondral Bone Growth(a)locationoftheepiphysealplateinalongbone.(b)asthechondrocytesoftheepiphysealplatedivideandalignincolumns,thecartilageexpandstowardtheepiphysis,andtheboneelongates.atthesametime,theoldercartilageiscalcifiedandthenreplacedbybone,whichisremodeled,resultinginexpansionofthemedullarycavityofthediaphysis.thenetresultisanepiphysealplatethatremainsuniforminthicknessthroughtimebutisconstantlymovingtowardtheepiphysis,resultinginelongationofthebone.(c)Photomicrographofanepiphysealplate,demonstratingchondrocytedivisionandenlargementandtheareasofcalcificationandossification.
(c)
(b)
(a)
see78267-Chapter06.indd 116 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 117Skeletal
Compactbone
Periosteum
Medullarycavity
ClotDeadbone
Newbone
Compactbone atbreak site
Spongybone
Deadbone
Cartilage
Fibersand cartilage
Clot formation Callus formation Callus ossification Bone remodeling
1 When a bone is broken, a clot forms in the damaged area.
2 Blood vessels and cells invade the clot and produce a network of fibers and cartilage called a callus.
3 Osteoblasts enter the callus and form spongy bone.
4 Most of the spongy bone is slowly remodeled to form compact bone and the repair is complete.
Callus
PROCESS Figure 6.8 Bone Repair
bonegrowthwhennewly formedspongybone in theepiphysealplate forms compact bone. A long bone increases in length anddiameterasnewboneisdepositedontheoutersurfaceandgrowthoccursattheepiphysealplate.Atthesametime,boneisremovedfromtheinner,medullarysurfaceofthebone.Asthebonediameterincreases,thethicknessofthecompactbonerelativetothemedul-larycavitytendstoremainfairlyconstant.Ifthesizeofthemedullarycavity did not also increase as bone size increased, the compactboneofthediaphysiswouldbecomethickandveryheavy. Becauseboneisthemajorstoragesiteforcalciuminthebody,bone remodeling is important to maintain blood calcium levelswithinnormallimits.Calciumisremovedfromboneswhenbloodcalciumlevelsdecrease,anditisdepositedwhendietarycalciumisadequate.Thisremovalanddepositionisunderhormonalcontrol(see“BoneandCalciumHomeostasis”laterinthischapter). If too much bone is deposited, the bones become thick ordevelopabnormalspursor lumpsthatcan interferewithnormalfunction.Toolittleboneformationortoomuchboneremoval,asoccurs inosteoporosis,weakens thebonesandmakes themsus-ceptibletofracture(seeSystemsPathology,“Osteoporosis”).
BonerepairSometimesaboneisbrokenandneedstoberepaired.Whenthisoccurs, blood vessels in the bone are also damaged. The vesselsbleed, and a clot forms in the damaged area (figure 6.8, step 1).Two to three days after the injury, blood vessels and cells fromsurrounding tissuesbegin to invade theclot.Someof thesecellsproduceafibrousnetworkofconnectivetissuebetweenthebrokenbones,whichholdsthebonefragmentstogetherandfillsthegapbetweenthem.Othercellsproduceisletsofcartilageinthefibrousnetwork.Thenetworkoffibersandisletsofcartilagebetweenthetwobonefragmentsiscalledacallus(figure6.8,step2).
Osteoblastsenter thecallusandbegin formingspongybone(figure6.8,step3).Spongyboneformationinthecallusisusuallycomplete4–6weeksaftertheinjury.Immobilizationoftheboneiscriticaluptothistimebecausemovementcanrefracturethedeli-catenewmatrix.Subsequently,thespongyboneisslowlyremod-eledtoformcompactandspongybone,andtherepairiscomplete(figure6.8,step4).Althoughimmobilizationatafracturepointiscriticalduringtheearlystagesofbonehealing,completeimmobili-zationisnotgoodforthebone,themuscles,orthejoints.Notlongago,itwascommonpracticetoimmobilizeabonecompletelyforaslongas10weeks.Butwenowknowthat,ifaboneisimmobi-lizedforaslittleas2weeks,themusclesassociatedwiththatbonemayloseasmuchashalftheirstrength.Furthermore,ifaboneiscompletelyimmobilized,itisnotsubjectedtothenormalmechanicalstressesthathelpitform.Bonematrixisreabsorbed,andthestrengthofthebonedecreases.Inexperimentalanimals,completeimmobili-zationofthebackfor1monthresultedinuptoathreefolddecreasein vertebral compression strength. Modern therapy attempts tobalancebone immobilizationwithenoughexercise tokeepmuscleandbonefromdecreasinginsizeandstrengthandtomaintainjointmobility.Thesegoals areaccomplishedby limiting theamountoftimeacastisleftonthepatientandbyusing“walkingcasts,”whichallowsomestressontheboneandsomemovement.Totalhealingofthefracturemayrequireseveralmonths.Ifabonehealsproperly,thehealedregioncanbeevenstrongerthantheadjacentbone.
6.4 BonEanDcalciuMHoMEoStaSiSLearning Outcomes After reading this section, you should be able to
A. Explaintheroleofboneincalciumhomeostasis.B. Describehowparathyroidhormoneandcalcitonininfluence
bonehealthandcalciumhomeostasis.
see78267-Chapter06.indd 117 11-12-01 3:25 PM

118 Chapter 6Sk
elet
al Bone fractures can be classi-fied as open (or compound), if the boneprotrudes through the skin, and closed(or simple), if the skin is not perforated.Figure 6a illustrates some of the differenttypes of fractures. if the fracture totallyseparates the two bone fragments, it iscalled complete; if it doesn’t, it is calledincomplete. an incomplete fracture thatoccursontheconvexsideofthecurveofaboneiscalledagreenstick fracture.acom-minuted (kom′i-nū-ted; broken into smallpieces) fracture is one in which the bonebreaks into more than two fragments. animpacted fracture occurs when one of thefragmentsofonepartoftheboneisdrivenintothespongyboneofanotherfragment.
Fracturescanalsobeclassifiedaccord-ing to the direction of the fracture line aslinear(paralleltothelongaxis);transverse
(atrightanglestothelongaxis);orobliqueor spiral (at an angle other than a rightangletothelongaxis).
CLINICALIMPACT Bone Fractures
Complete
Linear
Incomplete
Comminuted
Transverse
Impacted
Oblique
Spiral
Figure 6A typesofbonefractures.
PTH
Osteoclastspromote Ca2+
uptake frombone.
Osteoblasts promoteCa2+ deposition in bone.
Stimulatesosteoclasts
Inhibitsosteoclasts
Bone
Ca2+
Ca2+ Blood
Vitamin D
Kidney
Small intestine
Calcitonin
Decreased blood Ca2+ stimulates PTH secretion from parathyroid glands.
PTH stimulates osteoclasts to break down
bone and release Ca2+ into the blood.
In the kidneys, PTH increases Ca2+ reabsorption from the urine. PTH also stimulates active Vitamin D formation.
Vitamin D promotes Ca2+ absorption from the small intestine into the blood.
Increased blood Ca2+ stimulates calcitonin secretion from the thyroid gland.
Calcitonin inhibits osteoclasts, which allows for enhanced osteoblast uptake of Ca2+ from the blood to deposit into bone.
1
2
3
4
5
6
1
2
3
4
5
6
Posterior aspectof thyroid gland
Parathyroidglands
Thyroid gland
Increasedblood Ca2+
Decreasedblood Ca2+
PROCESS Figure 6.9 Calcium Homeostasis
see78267-Chapter06.indd 118 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 119Skeletal
Calcitonin (kal-si-tō′nin), secreted from the thyroid glandwhenbloodcalciumlevelsaretoohigh,decreasesosteoclastactivityand thus decreases blood calcium levels. Increasing blood cal-ciumlevelsstimulatecalcitoninsecretion.PTHandcalcitoninaredescribedmorefullyinchapter10.
6.5 GEnEralconSiDErationSoFBonEanatoMY
Learning Outcome After reading this section, you should be able to
A. listanddefinethemajorfeaturesofatypicalbone.
It is traditional to list 206 bones in the average adult skeleton(table 6.1), although the actual number varies from person topersonanddecreaseswithageassomebonesfuse. Anatomists use several common terms to describe the fea-turesofbones(table6.2).Forexample,aholeinaboneiscalledaforamen(fō-rā′men;pl.foramina,fō-rā′min-ă;foro,topierce).Aforamenusuallyexistsinabonebecausesomestructure,suchasanerveorbloodvessel,passesthroughtheboneatthatpoint.Iftheholeiselongatedintoatunnel-likepassagethroughthebone,
Boneisthemajorstoragesiteforcalciuminthebody,andmove-ment of calcium into and out of bone helps determine bloodcalcium levels, which is critical for normal muscle and nervoussystem function. Calcium (Ca2+) moves into bone as osteoblastsbuildnewboneandoutofboneasosteoclastsbreakdownbone(figure 6.9). When osteoblast and osteoclast activity is balanced,themovementsofcalciumintoandoutofaboneareequal. When blood calcium levels are too low, osteoclast activityincreases, osteoclasts release calcium from bone into the blood,and blood calcium levels increase. Conversely, if blood cal-ciumlevelsaretoohigh,osteoclastactivitydecreases,osteoblastsremovecalciumfromthebloodtoproducenewbone,andbloodcalciumlevelsdecrease. Calcium homeostasis is maintained by two hormones.Parathyroid hormone (PTH), secreted from the parathyroidglandswhenbloodcalciumlevelsaretoolow,stimulatesincreasedbonebreakdownandincreasedbloodcalciumlevelsbyindirectlystimulatingosteoclastactivity.PTHalsoincreasescalciumuptakefromtheurineinthekidney.Additionally,PTHstimulatesthekid-neystoformactivevitaminD,whichincreasescalciumabsorptionfromthesmallintestine.DecreasingbloodcalciumlevelsstimulatePTHsecretion.
TABle 6.1 Named Bones in the Adult Human Skeleton
Bones NumberThoracic Cage ribs 24 Sternum(3parts,sometimesconsidered3bones) 1
total thoracic cage 25
total axial skeleton 80
Appendicular Skeleton
Pectoral Girdle Scapula 2 clavicle 2
Upper Limb Humerus 2 ulna 2 radius 2 carpalbones 16 Metacarpalbones 10 Phalanges 28
total girdle and upper limb 64
Pelvic Girdle coxalbone 2
Lower Limb Femur 2 tibia 2 Fibula 2 Patella 2 tarsalbones 14 Metatarsalbones 10 Phalanges 28
total girdle and lower limb 62
total appendicular skeleton 126
total bones 206
Bones NumberAxial Skeleton
Skull Braincase Paired Parietal 2 temporal 2 unpaired Frontal 1 occipital 1 Sphenoid 1 Ethmoid 1
Face Paired Maxilla 2 Zygomatic 2 Palatine 2 nasal 2 lacrimal 2 inferiornasalconcha 2
unpaired Mandible 1 Vomer 1
total skull 22
Auditory Ossicles Malleus 2 incus 2 Stapes 2
total 6
Hyoid 1
Vertebral Column cervicalvertebrae 7 thoracicvertebrae 12 lumbarvertebrae 5 Sacrum 1 coccyx 1
total vertebral column 26
see78267-Chapter06.indd 119 11-12-01 3:25 PM

120 Chapter 6Sk
elet
al
TABle 6.2 Anatomical Terms for Features of Bones
Term DescriptionMajor Features
Body,shaft Mainportion
Head Enlarged(oftenrounded)end
neck constrictedareabetweenheadandbody
condyle Smooth,roundedarticularsurface
Facet Small,flattenedarticularsurface
crest Prominentridge
Process Prominentprojection
tubercle,ortuberosity Knoborenlargement
trochanter largetuberosityfoundonlyon proximalfemur
Epicondyle Enlargementnearoraboveacondyle
Openings or Depressions
Foramen Hole
canal,meatus tunnel
Fissure cleft
Sinus cavity
Fossa Depression
itiscalledacanalorameatus(mē-ā′tus;apassage).Adepressionin a bone is called a fossa (fos′ă). A lump on a bone is called atubercle(too′ber-kl;aknob)oratuberosity(too′ber-os′i-tē),andaprojectionfromabone iscalledaprocess.Most tuberclesandprocesses are sites of muscle attachment on the bone. Increasedmuscle pull, as occurs when a person lifts weights to build upmusclemass,canincreasethesizeofsometubercles.Thesmooth,roundedendofabone,whereitformsajointwithanotherbone,iscalledacondyle(kon′dīl;knuckle). Thebonesof the skeletonaredivided intoaxialandappen-dicularportions(figure6.10).
6.6 axialSKElEtonLearning Outcomes After reading this section, you should be able to
A. namethebonesoftheskullanddescribetheirmainfeaturesasseenfromthelateral,frontal,internal,andinferiorviews.
B. listthebonesthatformthemajorityofthenasalseptum.C. Describethelocationsandfunctionsoftheparanasalsinuses.D. listthebonesofthebraincaseandtheface.e. Describetheshapeofthevertebralcolumn,andlistits
divisions.F. Discussthecommonfeaturesofthevertebraeandcontrast
vertebraefromeachregionofthevertebralcolumn.G. listthebonesandcartilageoftheribcage,includingthethree
typesofribs.
Theaxialskeletoniscomposedoftheskull,thevertebralcolumn,andthethoraciccage.
SkullThe22bonesoftheskullaredividedintothoseofthebraincaseandthoseoftheface(seetable6.1).Thebraincase,whichenclosesthecranialcavity,consistsof8bones that immediatelysurroundand protect the brain; 14 facial bones form the structure of theface.Thirteenof the facialbonesare rather solidlyconnected toformthebulkoftheface.Themandible,however,formsafreelymovablejointwiththerestoftheskull.Therearealsothreeaudi-toryossicles(os′i-klz)ineachmiddleear(sixtotal). Manystudentsstudyinganatomyneverseetheindividualbonesoftheskull.Eveniftheydo,itmakesmoresensefromafunctional,or clinical, perspective to study most of the bones as they appeartogetherintheintactskullbecausemanyoftheanatomicalfeaturesof theskullcannotbefullyappreciatedbyexaminingtheseparatebones.Forexample,severalridgesontheskullcrossmorethanonebone,andseveralforaminaare locatedbetweenbonesratherthanwithinasinglebone.Forthesereasons,itismorerelevanttothinkof the skull, excluding themandible, as a singleunit.Themajorfeaturesoftheintactskullarethereforedescribedfromfourviews.
Lateral ViewTheparietal bones(pă-rī′ĕ-tăl;wall)andtemporal(tem′pō-răl)bonesformalargeportionofthesideofthehead(figure6.11).(Theword temporal refers to time,and the temporalbone is sonamedbecausethehairsofthetemplesturnwhite,indicatingthepassageoftime.)Thesetwobonesjoineachotheronthesideoftheheadatthesquamous(skwā′mŭs)suture.Asutureisajointunitingbonesof theskull.Anteriorly, theparietalbone is joinedtothefrontal(forehead)bonebythecoronal(kōr′ō-năl;corona,crown)suture,andposteriorlyitisjoinedtotheoccipital(ok-sip′i-tăl;backofthehead)bonebythelambdoid(lam′doyd)suture.Aprominentfea-tureofthetemporalboneisalargeopening,theexternal auditory canal,acanal thatenablessoundwaves toreachtheeardrum.Themastoid(mas′toyd)processofthetemporalbonecanbeseenandfeltasaprominentlumpjustposteriortotheear.Importantneckmusclesinvolvedinrotationoftheheadattachtothemastoidprocess. Partofthesphenoid(sfē′noyd)bonecanbeseenimmediatelyanteriortothetemporalbone.Althoughitappearstobetwosmall,pairedbonesonthesidesoftheskull,thesphenoidboneisactuallyasinglebonethatextendscompletelyacrosstheskull.Itresemblesabutterfly,with itsbody in thecenterof the skull and itswingsextendingtothesidesoftheskull.Anteriortothesphenoidboneisthezygomatic(zī-gō-mat′ik)bone,orcheekbone,whichcanbeeasilyfelt.Thezygomatic arch,whichconsistsofjoinedprocessesof the temporal and zygomatic bones, forms a bridge across thesideofthefaceandprovidesamajorattachmentsiteforamusclemovingthemandible. The maxilla (mak-sil′ă; jawbone) forms the upper jaw, andthemandible (man′di-bl; jaw) forms the lower jaw.Themaxillaarticulatesbysuturestothetemporalbone.Themaxillacontainsthesuperiorsetofteeth,andthemandiblecontainstheinferiorteeth.
Frontal ViewThemajorstructuresseenfromthefrontalviewarethefrontalbone,thezygomaticbones,themaxillae,andthemandible(figure6.12a).Theteethareveryprominentinthisview.Manybonesofthefacecanbeeasilyfeltthroughtheskin(figure6.12b).
see78267-Chapter06.indd 120 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 121Skeletal
UlnaRadius
Carpal bonesMetacarpalbones
Phalanges
Coxalbone
Femur
Patella
Tibia
Fibula
Tarsal bones
Metatarsal bones
Phalanges
Anterior view Posterior view
Axial Skeleton
Skull
Vertebralcolumn
Mandible
Ribs
Sacrum
Coccyx
Appendicular Skeleton
Clavicle
Scapula
Humerus
Axial Skeleton
Skull
Vertebralcolumn
Mandible
Hyoid bone
Sternum
Ribs
Sacrum
Figure 6.10 Complete SkeletonBonesoftheaxialskeletonarelistedinthefarleft-andright-handcolumns;bonesoftheappendicularskeletonarelistedinthecenter.(theskeletonisnotshownintheanatomicalposition.)
see78267-Chapter06.indd 121 11-12-01 3:25 PM

122 Chapter 6Sk
elet
al
Coronal suture
Parietal bone
Temporal bone
Occipital bone
Squamous suture
Lambdoid suture
External auditory canal
Styloid process
Zygomatic arch
Frontal bone
Sphenoid bone
Nasal bone
Lacrimal bone
Ethmoid bone
Zygomatic bone
Maxilla
Mental foramen
Nasolacrimal canal
Mastoid process
Mandible
Mandibular condyle
Coronoid process
Lateral view
Figure 6.11 Skull as Seen from the Right Side (The names of bones are in bold.)
Fromthisview, themostprominentopenings into the skullaretheorbits(ōr′bitz;eyesockets)andthenasal cavity.Theorbitsarecone-shapedfossae, sonamedbecause theeyesrotatewithinthem.Thebonesoftheorbitsprovidebothprotectionfortheeyesandattachmentpointsforthemusclesthatmovetheeyes.Theorbitisagoodexampleofwhyitisvaluabletostudytheskullasanintactstructure.Nofewerthansevenbonescometogethertoformtheorbit,andforthemostpart,thecontributionofeachbonetotheorbitcannotbeappreciatedwhenthebonesareexaminedindividually. Each orbit has several openings through which structurescommunicate with other cavities (figure 6.12a). The largest ofthesearethesuperiorandinferior orbital fissures.Theyprovideopenings through which nerves and blood vessels communicatewiththeorbitorpasstotheface.Theopticnerve,forthesenseofvision,passesfromtheeyethroughtheoptic foramenandentersthecranialcavity.Thenasolacrimal(nā-zō-lak′ri-măl;nasus,nose+lacrima,tear)canal(seefigure6.11)passesfromtheorbitintothenasalcavity.Itcontainsaductthatcarriestearsfromtheeyestothenasalcavity.Asmalllacrimal(lak′ri-măl)bonecanbeseenintheorbitjustabovetheopeningofthiscanal.
Predict 4
Why does your nose run when you cry?
Thenasalcavityisdividedintorightandlefthalvesbyanasal septum(sep′tŭm;wall)(figure6.12a).Thebonypartofthenasalseptum consists primarily of the vomer (vō′mer) inferiorly andtheperpendicular plateoftheethmoid(eth′moyd;sieve-shaped)bonesuperiorly.Theanteriorpartofthenasalseptumisformedbycartilage. The external part of the nose is formed mostly of cartilage.Thebridgeofthenoseisformedbythenasal bones. Each of the lateral walls of the nasal cavity has three bonyshelves, called the nasal conchae (kon′kē; resembling a conchshell).Theinferiornasalconchaisaseparatebone,andthemiddleandsuperiorconchaeareprojectionsfromtheethmoidbone.Theconchaeincreasethesurfaceareainthenasalcavity.Theincreasedsurfaceareaoftheoverlyingepitheliumfacilitatesmoisteningandwarmingoftheairinhaledthroughthenose(seechapter15). Severalofthebonesassociatedwiththenasalcavityhavelargecavities within them, called the paranasal (par-ă-nā′săl; para,alongside) sinuses (figure6.13),whichopen into thenasal cavity.Thesinusesdecrease theweightof theskullandactasresonatingchambersduringvoiceproduction.Compareanormalvoicewiththevoiceofapersonwhohasacoldandwhosesinusesare“stoppedup.”Thesinusesarenamedfortheboneswheretheyarelocatedandincludethefrontal,maxillary,ethmoidal,andsphenoidalsinuses.
see78267-Chapter06.indd 122 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 123Skeletal
formingthefloorofthecranialcavity,fromanteriortoposterior,arethefrontal,ethmoid,sphenoid,temporal,andoccipitalbones.Several foramina can be seen in the floor of the middle fossa.These allow nerves and blood vessels to pass through the skull.Forexample,theforamenrotundumandforamenovaletransmitimportantnervestotheface.Amajorarterytothemeninges(themembranesaroundthebrain)passesthroughtheforamenspino-sum.Theinternalcarotidarterypassesthroughthecarotidcanal,andtheinternaljugularveinpassesthroughthejugularforamen(see chapter 13). The large foramen magnum, through whichthe spinal cord joins the brain, is located in the posterior fossa.
Theskullhasadditionalsinuses,calledthemastoid air cells,which are located inside the mastoid processes of the temporalbone.Theseaircellsopenintothemiddleearinsteadofintothenasalcavity.Anauditorytubeconnectsthemiddleeartothenaso-pharynx(upperpartofthroat).
Interior of the Cranial CavityWhenthefloorofthecranialcavityisviewedfromabovewiththeroofcutaway(figure6.14),itcanbedividedroughlyintothreecra-nialfossae(anterior,middle,andposterior),whichareformedasthedevelopingskullconformstotheshapeofthebrain.Thebones
Superior orbital fissure
Supraorbital foramen
Optic foramen
Coronal suture
Inferior orbital fissure
Infraorbital foramen
Mental foramen
Nasal cavity
Middle nasal concha
Sphenoid bone
Frontal bone
Parietal bone
Mandible
Orbit
Temporal bone
Nasal bone
Lacrimal bone
Zygomatic bone
Perpendicular plateof ethmoid bone
Vomer
Inferior nasal concha
Maxilla
Nasalseptum
Frontal view
Zygomaticbone
Maxilla
Frontal bone
Mandible
Nasal bone
(b)
(a)
Figure 6.12 Skull and Face (The names of bones are in bold.)(a)Frontalviewoftheskull.(b)Bonylandmarksoftheface.
see78267-Chapter06.indd 123 11-12-01 3:25 PM

124 Chapter 6Sk
elet
al Frontal sinus
Ethmoidal sinus
Sphenoidal sinus
Maxillary sinus
Lateral view Anterior view
Sphenoid bone
Foramen rotundum
Internal auditory canal
Foramen magnum
Frontal sinuses
Crista galli
Cribriform plateEthmoid bone
Frontal bone
Optic foramen
Sella turcica
Foramen ovaleForamen spinosum Carotid canal
Jugular foramen
Parietal bone
Occipital bone
Superior view
Temporal bone
Hypoglossal canal
Anterior cranial fossa
Middle cranial fossa
Posterior cranial fossa
Figure 6.13 Paranasal Sinuses
(a) (b)
Figure 6.14 Floor of the Cranial Cavity (The names of bones are in bold.)theroofoftheskullhasbeenremoved,andthefloorisviewedfromabove.
see78267-Chapter06.indd 124 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 125Skeletal
palatine(pal′ă-tīn)bones.Theconnectivetissueandmusclesthatmakeupthesoft palateextendposteriorlyfromthehard,orbony,palate. The hard and soft palates separate the nasal cavity andnasopharynxfromthemouth,enablingustochewandbreatheatthesametime.
Hyoid BoneThehyoid bone(figure6.16)isanunpaired,U-shapedbone.Itisnotpartoftheskull(seetable6.1)andhasnodirectbonyattach-menttotheskull.Musclesandligamentsattachittotheskull.Thehyoidboneprovidesanattachmentforsometonguemuscles,andit isanattachmentpointforimportantneckmusclesthatelevatethelarynx(voicebox)duringspeechorswallowing.
VertebralcolumnThevertebral column,orbackbone,isthecentralaxisoftheskel-eton,extendingfromthebaseoftheskulltoslightlypasttheendofthepelvis.Inadults, itusuallyconsistsof26individualbones,grouped into five regions (figure 6.17; see table 6.1): 7 cervical(ser′vĭ-kal;neck)vertebrae(ver′tĕ-brē;verto,toturn),12thoracic(thō-ras′ik) vertebrae, 5 lumbar (lŭm′bar) vertebrae, 1 sacral(sā′krăl)bone,and1coccyx (kok′siks)bone.Theadultsacraland
Thecentralregionofthesphenoidboneismodifiedintoastruc-tureresemblingasaddle,thesella turcica(sel′ătŭr′sĭ-kă;Turkishsaddle),whichcontainsthepituitarygland.
Base of Skull Viewed from BelowManyof thesameforaminathatarevisible in the interiorof theskullcanalsobeseeninthebaseoftheskull,whenviewedfrombelow, with the mandible removed (figure 6.15). Other special-izedstructures,suchasprocessesformuscleattachments,canalsobe seen. The foramen magnum is located in the occipital bonenearthecenteroftheskullbase.Occipital condyles(ok-sip′i-tălkon′dīlz),thesmoothpointsofarticulationbetweentheskullandthevertebralcolumn,arelocatedbesidetheforamenmagnum. Two long, pointed styloid (stī′loyd; stylus or pen-shaped)processesprojectfromtheinferiorsurfaceofthetemporalbone.Themusclesinvolvedinmovingthetongue,thehyoidbone,andthepharynx(throat)originatefromthisprocess.Themandibular fossa,where themandiblearticulateswith the temporalbone, isanteriortothemastoidprocess. The hard palate (pal′ăt) forms the floor of the nasal cavityand the roof of the mouth. The anterior two-thirds of the hardpalate is formed by the maxillae, the posterior one-third by the
Figure 6.15 Base of the Skull as Viewed from Below (The names of bones are in bold.)themandiblehasbeenremoved.
Inferior orbital fissure
Foramen ovaleForamen spinosum
External auditory canal
Jugular foramen
Occipital condyle
Incisive fossa
Maxilla
Hard palate
Palatine process of maxillary bone
Horizontal plate of palatine bone
Vomer
Zygomatic bone
Styloid processMandibular fossaCarotid canal
Mastoid process
Temporal bone
Occipital bone
Foramen magnum
Sphenoid bone
Nuchal lines
Inferior view
see78267-Chapter06.indd 125 11-12-01 3:25 PM

126 Chapter 6Sk
elet
al
coccyxbonesfusefrom5and3–4individualbones,respectively.Forconvenience,eachofthefiveregionsisidentifiedbyaletter,andthevertebraewithineachregionarenumbered:C1–C7,T1–T12,L1–L5,S,andCO.Youcanrememberthenumberofvertebraeineachregionbyrememberingmealtimes:7,12,and5. The adult vertebral column has four major curvatures. Thecervical regioncurvesanteriorly, the thoracicregioncurvespos-teriorly, the lumbar region curves anteriorly, and the sacral andcoccygealregionstogethercurveposteriorly. Abnormalvertebralcurvaturesarenotuncommon.Kyphosis(kī-fō′sis)isanabnormalposteriorcurvatureofthespine,mostlyintheupperthoracicregion,resultinginahunchbackcondition.Lordosis (lōr-dō′sis; curving forward) is an abnormal anteriorcurvatureofthespine,mainlyinthelumbarregion,resultinginaswaybackcondition.Scoliosis(skō-lē-ō′sis)isanabnormallateralcurvatureofthespine. Thevertebralcolumnperformsthefollowingfivemajorfunc-tions:(1)supportstheweightoftheheadandtrunk;(2)protectsthespinalcord; (3)allowsspinalnerves toexit thespinalcord;(4)providesasiteformuscleattachment;and(5)permitsmove-mentoftheheadandtrunk.
General Plan of the VertebraeEach vertebra consists of a body, an arch, and various processes(figure6.18).Theweight-bearingportionofeachvertebra is thebody.Thevertebralbodiesareseparatedby intervertebral disks(seefigure6.17),whichareformedbyfibrocartilage.Thevertebral archsurroundsalargeopeningcalledthevertebral foramen.Thevertebral foraminaofall thevertebrae form thevertebral canal,where the spinal cord is located. The vertebral canal protectsthe spinal cord from injury. Each vertebral arch consists of two
Figure 6.16 Hyoid Bone
Figure 6.17 Vertebral Columncompletecolumnviewedfromtheleftside.
Body
Body
Anterior view
Lateral view(from the left side)
Cervicalregion(curvedanteriorly)
Thoracicregion(curvedposteriorly)
Lumbarregion(curvedanteriorly)
Sacral and coccygealregions(curvedposteriorly)
First cervical vertebra(atlas)
Second cervical vertebra(axis)
Seventh cervical vertebra
First thoracic vertebra
Intervertebral disk
Twelfth thoracic vertebra
Intervertebral foramina
First lumbar vertebra
Body
Transverse process
Spinous process
Fifth lumbar vertebra
Sacrum
Coccyx
Lateral view
Sacral promontory
see78267-Chapter06.indd 126 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 127Skeletal
pedicles(ped′ĭ-klz),whichextendfromthebodytothetransverseprocessofeachvertebra,andtwolaminae(lam′i-nē;thinplates),whichextendfromthetransverseprocessestothespinousprocess.Atransverse processextendslaterallyfromeachsideofthearch,between the pedicle and lamina, and a single spinous processprojectsdorsally fromwherethetwolaminaemeet.Thespinousprocessescanbeseenandfeltasaseriesoflumpsdownthemid-line of the back (see figure 6.24b). The transverse and spinousprocessesprovideattachmentsitesforthemusclesthatmovethevertebral column.Spinalnerves exit the spinal cord through theintervertebral foramina, which are formed by notches in thepediclesofadjacentvertebrae(seefigure6.17).Eachvertebrahasasuperiorandinferiorarticular processwherethevertebraearticu-late with each other. Each articular process has a smooth “littleface”calledanarticular facet(fas′et).
Regional Differences in VertebraeThe cervical vertebrae (figure 6.19a–c) have very small bodies,except for the atlas, which has no body. Because the cervicalvertebraearerelativelydelicateandhavesmallbodies,dislocations
Figure 6.18 Vertebra
Superior articular process
Articular facet
Transverse process
Vertebral foramen
Body
Pedicle
Lamina
Vertebral arch
Spinous process
Anterior
Superior view
Posterior
Superiorarticular facet
Spinous process
Transverseprocess
Transverseforamen
Vertebral foramen
Body
Pedicle
Lamina
Posterior arch
Atlas (first cervical vertebra), superior view
Thoracic vertebra, superior view
Lumbar vertebra, superior view
Cervical vertebra, superior view
Superior articularfacet (articulates with occipital condyle)
Facet for dens
Transverseprocess
Transverseforamen
Vertebral foramen
Anterior arch
Body
Spinous process
Transverseprocess
Vertebral foramen
Pedicle
Lamina
Superiorarticular facet
Facets for ribattachment
Superiorarticular facet
Spinous process
Transverseprocess
Vertebral foramenPedicle
Lamina
Body
Dens(articulateswith atlas)
Dens
Body
Axis (second cervical vertebra),superior view
Lateral view
Figure 6.19 Regional Differences in Vertebraetheposteriorportionliesatthetopofeachillustration.
(a)
(d)
(e)
(b)
(c)
see78267-Chapter06.indd 127 11-12-01 3:25 PM

128 Chapter 6Sk
elet
al
Vertebralcanal (sacralcanal)
Posteriorsacralforamina
Median sacralcrest
Sacral hiatus
Articular facet (articulates with fifth lumbar vertebra)
CoccyxCoccyx
Anterior view Posterior view
Anteriorsacralforamina
Sacral promontory
Figure 6.20 Sacrum
(a) (b)
of thebodyof the first sacralvertebrabulges to form thesacral promontory (prom′on-tō-rē) (see figure 6.17), a landmark thatcanbefeltduringavaginalexamination.Itisusedasareferencepointtodetermineifthepelvicopeningsarelargeenoughtoallowfornormalvaginaldeliveryofababy. The coccyx, or tailbone, usually consists of four more-or-lessfusedvertebrae.Thevertebraeofthecoccyxdonothavethetypicalstructureofmostothervertebrae.Theyconsistofextremelyreducedvertebralbodies,without the foraminaorprocesses,usually fusedintoasinglebone.Thecoccyxiseasilybrokenwhenapersonfallsbysittingdownhardonasolidsurfaceorinwomenduringchildbirth.
ribcageTherib cage protectsthevitalorganswithinthethoraxandpre-ventsthecollapseofthethoraxduringrespiration.Itconsistsofthethoracicvertebrae,theribswiththeirassociatedcartilages,andthesternum(figure6.21).
acaSEinPoint
Rib Fractures
Han D. Mann’s ladder fell as he was working on his roof, and helandedontheladderwithhischest.threeribswerefracturedonhisright side. it was difficult for Han to cough, laugh, or even breathewithout severe pain in the right side of his chest.the middle ribsare those most commonly fractured, and the portion of each ribthat forms the lateral wall of the thorax is the weakest and mostcommonly broken.the pain from rib fractures occurs because thebroken ends move during respiration and other chest movements,stimulating pain receptors. Broken rib ends can damage internalorgans, such as the lungs, spleen, liver, and diaphragm. Fracturedribsarenotoftendislocated,butdislocatedribsmayhavetobesetforproperhealingtooccur.Bindingthechesttolimitmovementcanfacilitatehealingandlessenpain.
andfracturesaremorecommoninthisareathaninotherregionsof the vertebral column. Each of the transverse processes has atransverse foramen through which the vertebral arteries passtowardthebrain.Severalofthecervicalvertebraealsohavepartlysplitspinousprocesses.Thefirstcervicalvertebra(figure6.19a)iscalledtheatlasbecauseitholdsupthehead,asAtlasinclassicalmythology held up the world. Movement between the atlas andtheoccipitalboneisresponsiblefora“yes”motionofthehead.Italsoallowsaslighttiltingoftheheadfromsidetoside.Thesecondcervicalvertebra(figure6.19b)iscalledtheaxisbecauseaconsid-erableamountofrotationoccursatthisvertebra,asinshakingthehead“no.”Thisrotationoccursaroundaprocesscalledthedens(denz),whichprotrudessuperiorlyfromtheaxis. Thethoracic vertebrae(figure6.19d)possesslong,thinspinousprocesses thataredirected inferiorly.Thethoracicvertebraealsohaveextraarticular facetsontheir lateral surfaces thatarticulatewiththeribs. Thelumbar vertebrae(figure6.19e)havelarge,thickbodiesandheavy,rectangulartransverseandspinousprocesses.Becausethelumbarvertebraehavemassivebodiesandcarryalargeamountofweight,rupturedintervertebraldisksaremorecommoninthisareathaninotherregionsofthecolumn.Thesuperiorarticularfacetsofthelumbarvertebraefacemedially,whereastheinferiorarticularfacets face laterally. This arrangement tends to “lock” adjacentlumbarvertebraetogether,givingthelumbarpartofthevertebralcolumnmorestrength.Thearticularfacetsinotherregionsofthevertebral column have a more “open” position, allowing for morerotationalmovementbutlessstabilitythaninthelumbarregion. Thefivesacralvertebraearefusedintoasinglebonecalledthesacrum(figure6.20).Thespinousprocessesofthefirstfoursacralvertebraeformthemedian sacral crest.Thespinousprocessofthefifthvertebradoesnot form, leavingasacral hiatus (hī-ā-tŭs)attheinferiorendofthesacrum,whichisoftenthesiteof“caudal”anestheticinjectionsgivenjustbeforechildbirth.Theanterioredge
see78267-Chapter06.indd 128 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 129Skeletal
6.7 aPPEnDicularSKElEtonLearning Outcomes After reading this section, you should be able to
A. identifythebonesthatmakeupthepectoralgirdle,andrelatetheirstructureandarrangementtothefunctionofthegirdle.
B. nameanddescribethemajorbonesoftheupperlimb.C. nameanddescribethebonesofthepelvicgirdleandexplain
whythepelvicgirdleismorestablethanthepectoralgirdle.D. namethebonesthatmakeupthecoxalbone.Distinguish
betweenthemaleandfemalepelvis.e. identifyanddescribethebonesofthelowerlimb.
Theappendicular(ap′en-dik′ū-lăr;appendage)skeletonconsistsofthebonesoftheupperandlowerlimbs,aswellasthegirdles,whichattachthelimbstotheaxialskeleton.
PectoralGirdleThepectoral (pek′tō-răl)girdle,or shoulder girdle (figure6.22),consistsoffourbones,twoscapulaeandtwoclavicles,whichattachtheupper limbtothebody.Thescapula (skap′ū-lă),orshoulder blade, is a flat, triangular bone with three large fossae wheremusclesextendingtothearmareattached(figures6.23and6.24;see figure6.10).A fourth fossa, theglenoid (glen′oyd)cavity, iswheretheheadofthehumerusconnectstothescapula.Aridge,calledthespine,runsacrosstheposteriorsurfaceofthescapula.A projection, called the acromion (ă-krō′mē-on; akron, tip +omos,shoulder)process,extendsfromthescapularspinetoformthe point of the shoulder. The clavicle (klav′i-kl), or collarbone,articulateswiththescapulaattheacromionprocess.Theproximalendoftheclavicleisattachedtothesternum,providingtheonly
Ribs and Costal CartilagesThe 12 pairs of ribs can be divided into true ribs and false ribs.Thetrue ribs,ribs1–7,attachdirectlytothesternumbymeansofcostalcartilages.Thefalse ribs, ribs8–12,donotattachdirectlyto the sternum. Ribs 8–10 attach to the sternum by a commoncartilage;ribs11and12donotattachatalltothesternumandarecalledfloating ribs.
SternumThe sternum (ster′nŭm), or breastbone (figure 6.21), is dividedinto three parts: the manubrium (mă-nū′brē-ŭm; handle), thebody,andthexiphoid(zif′oyd,zī′foyd;sword)process.Thester-numresemblesasword,withthemanubriumformingthehandle,thebodyformingtheblade,andthexiphoidprocessformingthetip. At the superior end of the sternum, a depression called thejugular notch is locatedbetweentheendsof theclavicleswherethey articulate with the sternum. A slight elevation, called thesternal angle, can be felt at the junction of the manubrium andthebodyofthesternum.Thisjunctionisanimportantlandmarkbecauseitidentifiesthelocationofthesecondrib.Thisidentifica-tionallowstheribstobecounted;forexample,itcanhelpahealthprofessionallocatetheapexoftheheart,whichisbetweenthefifthandsixthribs. The xiphoid process is another important landmark of thesternum.Duringcardiopulmonaryresuscitation(CPR), it isveryimportanttoplacethehandsoverthebodyofthesternumratherthan over the xiphoid process. Pressure applied to the xiphoidprocesscandriveitintoanunderlyingabdominalorgan,suchastheliver,causinginternalbleeding.
Clavicle
Jugular notch
Seventh cervical vertebra
First thoracic vertebra
True ribs(1–7)
Costal cartilage
False ribs(8–12)
Manubrium
Body
Xiphoid process
Sternum
Floating ribs
1
2
3
4
5
6
7
8
9
10
11
12
Anterior view
L1
T12
Sternal angle
Figure 6.21 Rib Cage
see78267-Chapter06.indd 129 11-12-01 3:25 PM

130 Chapter 6Sk
elet
al
neck,locatedattheproximalendofthehumeralshaft.Lateraltotheheadaretwotubercles,agreater tubercleandalesser tubercle.Musclesoriginatingonthescapulaattachtothegreaterandlessertubercles and hold the humerus to the scapula. Approximatelyone-thirdofthewaydowntheshaftofthehumerus,onthelateralsurface,isthedeltoid tuberosity,wherethedeltoidmuscleattaches.Thesizeofthedeltoidtuberositycanincreaseastheresultoffre-quentandpowerfulpullsfromthedeltoidmuscle.Forexample,inbodybuilders,thedeltoidmuscleandthedeltoidtuberosityenlargesubstantially.Anthropologists,examiningancienthumanremains,canuse thepresenceofenlargeddeltoid tuberositiesasevidencethatapersonwasengagedinliftingheavyobjectsduringlife.Ifthehumerusofapersonexhibitsanunusuallylargedeltoidtuberosityforherage,itmayindicate,insomesocieties,thatshewasaslaveandwasrequiredtoliftheavyloads.Thedistalendofthehumerusis modified into specialized condyles that connect the humerusto the forearm bones. Epicondyles (ep′i-kon′dīlz; epi, upon) onthedistalendofthehumerus,justlateraltothecondyles,provideattachmentsitesforforearmmuscles.
ForearmTheforearmhastwobones:theulna(ŭl′nă)onthemedial(littlefinger)sideoftheforearmandtheradiusonthelateral(thumb)side(figure6.26).Theproximalendoftheulnaformsatrochlear notchthatfitstightlyovertheendofthehumerus,formingmostoftheelbowjoint.Justproximaltothetrochlearnotchisanextensionof the ulna, called the olecranon (ō-lek′ră-non; elbow) process,whichcanbefeltasthepointoftheelbow(seefigure6.28).Justdistaltothetrochlearnotchisacoronoid(kōr′ŏ-noyd)process,whichhelpscompletethe“grip”oftheulnaonthedistalendofthehumerus.Thedistalendoftheulnaformsahead,whicharticulateswiththebonesofthewrist,andastyloid processislocatedonitsmedialside.Theulnarheadcanbeseenasaprominentlumpontheposteriorulnarsideofthewrist.Theproximalendoftheradiushasaheadbywhichtheradiusarticulateswithboththehumerusandtheulna.Theradiusdoesnotattachasfirmlytothehumerusastheulna does. The radial head rotates against the humerus and ulna.Just distal to the radial head is a radial tuberosity, where one ofthearmmuscles,thebicepsbrachii,attaches.Thedistalendoftheradiusarticulateswiththewristbones.Astyloidprocessislocatedonthelateralsideofthedistalendoftheradius.Theradialandulnarstyloidprocessesprovideattachmentsitesforligamentsofthewrist.
WristThe wrist is a relatively short region between the forearm andthe hand; it is composed of eight carpal (kar′păl; wrist) bones(figure6.27).Theseeightbonesarethescaphoid(skaf′oyd),lunate(lū′nāt), triquetrum(trī-kwē′trŭm),pisiform(pis′i-fōrm), trape-zium(tra-pē′zē-ŭm),trapezoid(trap′ĕ-zoyd),capitate(kap′i-tāt),andhamate(ha′māt).Thecarpalbonesarearrangedintworowsof four bones each and form a slight curvature that is concaveanteriorlyandconvexposteriorly.Anumberofmnemonicshavebeendevelopedtohelpstudentsrememberthecarpalbones.Thefollowing one allows students to remember them in order fromlateral to medial for the proximal row (top) and from medial tolateral(bythethumb)forthedistalrow:SoLongTopPart,HereComes The Thumb—that is, Scaphoid, Lunate, Triquetrum,Pisiform,Hamate,Capitate,Trapezoid,andTrapezium.
bonyattachmentofthescapulatotheremainderoftheskeleton.Theclavicleisthefirstbonetobeginossificationinthefetus.Thisrelatively brittle bone may be fractured in the newborn duringdelivery.Theboneremainsslenderinchildrenandmaybebrokenasachildattemptstotaketheimpactofafallonanoutstretchedhand.Theclavicleisthickerinadultsandislessvulnerabletofrac-ture.Eventhoughitisthefirstbonetobeginossification,itisthelast to complete ossification. The coracoid (kōr′ă-koyd) processcurvesbelowtheclavicleandprovidesfortheattachmentofarmandchestmuscles.
upperlimbTheupper limbconsistsof thebonesof thearm, forearm,wrist,andhand(seefigure6.22).
ArmThe arm is the region between the shoulder and the elbow; itcontains the humerus (hū′mer-ŭs; shoulder) (figure 6.25). Theproximalendofthehumerushasasmooth,roundedhead,whichattachesthehumerustothescapulaattheglenoidcavity.Aroundthe edge of the humeral head is the anatomical neck. When thejointneedstobesurgicallyreplaced,thisneckisnoteasilyacces-sible.Amoreaccessiblesiteforsurgicalremovalisatthesurgical
Upper limb
Pectoral girdle
Phalanges
Anterior view
Metacarpal bones
Clavicle
Scapula
Humerus
Radius
Ulna
Carpal bones
Figure 6.22 Bones of the Pectoral Girdle and Right Upper Limb
see78267-Chapter06.indd 130 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 131Skeletal
Spine of scapula
Supraspinous fossa of scapula
Acromion processof scapula
Distal end of clavicle
Coracoid processof scapula
Body of clavicle
Posterior
Anterior
Distal end
Proximal end
Posterior view
Acromion process
Glenoid cavity
Lateral border
Coracoid process
Subscapularfossa
Medial border
Viewin (d)
Inferior angle
Spine
Supraspinousfossa
Coracoid processAcromion process
Glenoid cavity
Infraspinous fossa
Lateral border
Anterior view
Superior viewSuperior view
Body of clavicle
Figure 6.23 Right Scapula and Clavicle(a)rightscapula,anteriorview.(b)rightscapula,posteriorview.(c)rightclavicle,superiorview.(d)Photographoftherightscapulaandclaviclefromasuperiorview,showingtherelationshipbetweenthedistalendoftheclavicleandtheacromionprocessofthescapula.
(a)
(c) (d)
(b)
Skeletal
the bones and ligaments ontheanteriorsideofthewristformacarpal tunnel, which does not have much“give.”tendonsandnervespassfromtheforearmthroughthecarpaltunneltothehand.Fluidand connective tissue can accumulate inthe carpal tunnel as a result of inflamma-tionassociatedwithoveruseortrauma.theinflammationcanalsocausethetendonsin
the carpal tunnel to enlarge.the accumu-latedfluidandenlargedtendonscanapplypressuretoamajornervepassingthroughthe tunnel. the pressure on this nervecausescarpal tunnel syndrome,character-izedbytingling,burning,andnumbnessinthehand. treatments for carpal tunnel syndromevary, depending on the severity of the
syndrome. Mild cases can be treated non-surgically with either anti-inflammatorymedicationsorstretchingexercises.However,if symptoms have lasted for more than6months, surgery is recommended.Surgicaltechniques involve cutting the carpal liga-menttoenlargethecarpaltunnelandeasepressureonthenerve.
CLINICALIMPACT Carpal Tunnel Syndrome
see78267-Chapter06.indd 131 11-12-01 3:25 PM

132 Chapter 6Sk
elet
al
Sternum
Clavicle
Distal end of clavicle
Acromionprocess
Jugular notch
Head
Anatomical neckLesser tubercle
Surgical neck
Olecranon fossa
Greater tubercle
Deltoid tuberosity
Lateral epicondyle
CondylesCapitulum
Trochlea
Medial epicondyle
Anterior view Posterior view
Trochlea
Lateral epicondyle
Greater tubercle
Spinous process ofseventh cervical vertebra
Lumbar spinousprocesses
Superior borderof scapula
Scapula
Medial borderof scapula
Inferior angleof scapula
Spine of scapula
Figure 6.24 Surface Anatomy of the Pectoral Girdle and Thoracic Cage(a)Bonesofthepectoralgirdleandtheanteriorthorax.(b)Bonesofthescapulaandtheposteriorvertebralcolumn.
Figure 6.25 Right Humerus
(a)
(a)
(b)
(b)
see78267-Chapter06.indd 132 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 133Skeletal
Carpal bones(distalrow)
Radius
TrapezoidTrapezium
Proximalphalanx of thumb
Proximal phalanx of finger
Middle phalanx of finger
Distal phalanx of finger
Posterior view
Ulna
CapitateHamate
1
2345
Digits
Metacarpalbones
Distalphalanxof thumb
Carpalbones(proximalrow)
LunateScaphoid
TriquetrumPisiform
Heads ofmetacarpal
bones(knuckles)
Olecranonprocess
Headof ulna
Acromionprocess
Medial border of scapula
Olecranonprocess
HandFivemetacarpal(met′ă-kar′păl)bonesareattachedtothecarpalbonesandformthebonyframeworkofthehand(figure6.27).Themetacarpalbonesarealignedwiththefivedigits:thethumbandfingers. They are numbered 1 to 5, from the thumb to the littlefinger.Theends,orheads,ofthefivemetacarpalbonesassociatedwiththethumbandfingersformtheknuckles(figure6.28).Eachfinger consistsof three smallbones called phalanges (fă-lan′jēz;sing.phalanx,fā′langks),namedaftertheGreekphalanx,awedgeof soldiers holding their spears, tips outward, in front of them.The phalanges of each finger are called proximal, middle, anddistal,accordingtotheirpositioninthedigit.Thethumbhastwophalanges,proximalanddistal.Thedigitsarealsonumbered1to5,startingfromthethumb.
PelvicGirdleThepelvic girdleistheplacewherethelowerlimbsattachtothebody(figure6.29).Therightandleftcoxal(kok′sul)bones,orhipbones, join each other anteriorly and the sacrum posteriorly toformaringofbonecalled thepelvic girdle.Thepelvis (pel′vis;
Olecranon process
Head
Radial tuberosity
Radius(shaft)
Styloid process
Anterior view
Trochlear notchCoronoid process
Ulna(shaft)
Head
Styloid process
Superior view
Head of radius
Olecranonprocess
Coronoid process
Trochlearnotch
Figure 6.26 Right Ulna and Radius(a)anteriorviewoftherightulnaandradius.(b)Proximalendsoftherightulnaandradius.
(a)
(b)
Figure 6.27 Bones of the Right Wrist and Hand
Figure 6.28 Surface Anatomy Showing Bones of the Pectoral Girdle and Upper Limb
see78267-Chapter06.indd 133 11-12-01 3:25 PM

134 Chapter 6Sk
elet
al
crest can be seen along the superior margin of each ilium, andan anterior superior iliac spine, an important hip landmark, islocatedattheanteriorendoftheiliaccrest.Thecoxalbonesjoineachotheranteriorlyatthepubic(pū′bik)symphysisandjointhesacrum posteriorly at the sacroiliac (sā-krō-il′ē-ak) joints (seefigure6.30).Theacetabulum(as-ĕ-tab′ū-lŭm;vinegarcup)isthesocketofthehipjoint.Theobturator(ob′too-rā-tŏr)foramenisthelargeholeineachcoxalbonethatisclosedoffbymusclesandotherstructures. Themalepelviscanbedistinguishedfromthefemalepelvisbecauseitisusuallylargerandmoremassive,butthefemalepelvistendstobebroader(figure6.32;table6.3).Boththeinletandtheoutletofthefemalepelvisarelargerthanthoseofthemalepelvis,and the subpubic angle is greater in the female (figure 6.32a,b).Theincreasedsizeoftheseopeningshelpsaccommodatethefetus
basin)includesthepelvicgirdleandthecoccyx(figure6.30).Thesacrumandcoccyxformpartofthepelvisbutarealsopartoftheaxialskeleton.Eachcoxalboneisformedbythreebonesfusedtooneanotherto formasinglebone(figure6.31).The ilium (il′ē-ŭm) is themostsuperior, the ischium (is′kē-ŭm) is inferiorandposterior,andthepubis(pū′bis)isinferiorandanterior.Aniliac
Coxal boneSacrum
Femur
Patella
Lower limb
Pelvic girdle
Tibia
Fibula
Tarsal bonesMetatarsalbonesPhalanges
Anterior view
Sacroiliac joint
Anterior superioriliac spine
Acetabulum
Coccyx
Iliac crest
Obturatorforamen
Subpubic angle
Anterosuperior view
Ischium
Pubis
Ilium
Sacrum
Coxalbone
Pubic symphysis
Sacral promontory
Figure 6.29 Bones of the Pelvic Girdle and Right Lower Limb
Figure 6.30 Pelvis
TABle 6.3 Differences Between Male and Female Pelvic Girdles
Area Description of DifferenceGeneral Femalepelvissomewhatlighterinweightand
widerlaterallybutshortersuperiorlyto inferiorlyandlessfunnel-shaped;lessobvious muscleattachmentpointsinfemalethaninmale
Sacrum Broaderinfemale,withtheinferiorportion directedmoreposteriorly;thesacralpromontory projectslessanteriorlyinfemale
Pelvicinlet Heart-shapedinmale;ovalinfemale
Pelvicoutlet Broaderandmoreshallowinfemale
Subpubicangle lessthan90degreesinmale;90degreesormore infemale
ilium Moreshallowandflaredlaterallyinfemale
ischialspines Fartherapartinfemale
ischialtuberosities turnedlaterallyinfemaleandmediallyinmale (notshowninfigure6.32)
see78267-Chapter06.indd 134 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 135Skeletal
Iliac crest
Greatersciatic notch
Ischial spine
Ischial tuberosityLateral view Medial view
Obturator foramen
Pubic symphysis
Acetabulum
Ilium
Pubis
Pelvic brim
Articular surface(area ofarticulationwith sacrum)
Greater sciatic notch
Ischium
Ischial spine
Ischium
Iliac fossa
Coccyx
Pubicsymphysis
Ischialspine
Sacral promontory
Subpubic angle
Pelvicbrim
Pelvicinlet(reddashedline)
Pubicsymphysis
Pelvicoutlet(bluedashedline)
Male Female
(a) Anterosuperior view (b) Anterosuperior view
Pelvic inlet
Pelvicbrim
Coccyx
Sacral promontory
Pelvic outlet
(c) Medial view
Figure 6.31 Right Coxal Bone
Figure 6.32 Comparison of the Male Pelvis to the Female Pelvis(a)inamale,thepelvicinlet(red dashed line)andoutlet(blue dashed line)aresmall,andthesubpubicangleislessthan90degrees.(b)inafemale,thepelvicinlet(red dashed line)andoutlet(blue dashed line)arelarger,andthesubpubicangleis90degreesorgreater.(c)amidsagittalsectionthroughthepelvisshowsthepelvicinlet(red arrowandred dashed line)andthepelvicoutlet(blue arrowandblue dashed line).
(a) (b)
see78267-Chapter06.indd 135 11-12-01 3:25 PM

136 Chapter 6Sk
elet
al
aredamaged.Ifthisoccurs,thefemoralheadmaydegeneratefromlackofnourishment.Thetrochantersarepointsofmuscleattach-ment.Thepatella(pa-tel′ă),orkneecap(figure6.33b), is locatedwithinthemajortendonoftheanteriorthighmusclesandenablesthetendontobendovertheknee.
LegThelegistheregionbetweenthekneeandtheankle(figure6.34).Itcontainstwobones,calledthetibia(tib′ē-ă;shinbone)andthefibula(fib′ū-lă).Thetibiaisthelargerofthetwoandisthemajorweight-bearingboneoftheleg.Theroundedcondylesofthefemurrestontheflatcondylesontheproximalendofthetibia.Justdis-taltothecondylesofthetibia,onitsanteriorsurface,isthetibial tuberosity, where the muscles of the anterior thigh attach. Thefibuladoesnotarticulatewiththefemur,butitsheadisattachedtotheproximalendofthetibia.Thedistalendsofthetibiaandfibula form a partial socket that articulates with a bone of theankle(thetalus).Aprominencecanbeseenoneachsideoftheankle(figure6.34).Thesearethemedial malleolus(mal-ē′ō-lŭs)ofthetibiaandthelateral malleolusofthefibula.
during childbirth. The pelvic inlet is formed by the pelvic brimand the sacralpromontory.The pelvic outlet isboundedby theischialspines,thepubicsymphysis,andthecoccyx(figure6.32c).
lowerlimbThelowerlimbconsistsofthebonesofthethigh,leg,ankle,andfoot(seefigure6.29).
ThighThethighistheregionbetweenthehipandtheknee(figure6.33a).Itcontainsasinglebonecalledthefemur.Theheadofthefemurarticulateswiththeacetabulumofthecoxalbone.Atthedistalendofthefemur,thecondylesarticulatewiththetibia.Epicondyles,locatedmedialandlateraltothecondyles,arepointsofligamentattachment. The femur can be distinguished from the humerusby its long neck, located between the head and the trochanters(trō′kan-terz). A “broken hip” is usually a break of the femoralneck.Abrokenhipisdifficulttorepairandoftenrequirespinningtoholdthefemoralheadtotheshaft.Amajorcomplicationcanoccurifthebloodvesselsbetweenthefemoralheadandtheacetabulum
Head
Neck
Greater trochanter
Lateral epicondyleLateral condyle
Body (shaft) of femur
Head
Neck
Medialepicondyle
Greater trochanter
Lateral epicondyle
Medialcondyle
Patellar groove
Linea aspera
Intercondylar fossa
Lesser trochanter
Anteriorsurface
Anterior view
Anterior view
Posterior view
Figure 6.33 Bones of the Thigh(a)rightfemur.(b)Patella.
(a)
(b)
see78267-Chapter06.indd 136 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 137Skeletal
AnkleThe ankle consists of seven tarsal (tar′săl; the sole of the foot)bones (figure 6.35). The tarsal bones are the talus (tā′lŭs; anklebone), calcaneus (kal-kā′nē-ŭs; heel), cuboid (kū′boyd), andnavicular(nă-vik′yū-lăr),andthemedial,intermediate,andlateralcuneiforms (kū′nē-i-fōrmz). The talus articulates with the tibiaand fibula to form the ankle joint, and the calcaneus forms theheel(figure6.36).AmnemonicforthedistalrowisMILC—thatis,Medial,Intermediate,andLateralcuneiformsandtheCuboid.AmnemonicfortheproximalthreebonesisNoThanksCow—thatis,Navicular,Talus,andCalcaneus.
FootThe metatarsal (met′ă-tar′săl) bones and phalanges of the footarearrangedandnumberedinamannerverysimilartothemeta-carpal bones and phalanges of the hand (see figure 6.35). Themetatarsalbonesaresomewhatlongerthanthemetacarpalbones,whereas the phalanges of the foot are considerably shorter thanthoseofthehand. There are three primary arches in the foot, formed by thepositions of the tarsal bones and metatarsal bones, and held inplacebyligaments.Twolongitudinalarchesextendfromtheheeltotheballofthefoot,andatransversearchextendsacrossthefoot.Thearchesfunctionsimilarlytothespringsofacar,allowingthefoottogiveandspringback.
Lateral condyle
Head
Medial condyle
Tibial tuberosity
TibiaFibula
Lateral malleolus
Anterior view
Medial malleolus
Cuboid
Lateral cuneiform
Metatarsalbones
Proximal phalanx
Middle phalanxDistal phalanx
Calcaneus
Talus
Navicular
Intermediate cuneiform
Medial cuneiform
Proximal phalanxof great toe
1234
5
Tarsal bones
Digits
Navicular
Cuboid
Fibula
Talus
Calcaneus
Tarsal bones
Tibia
Metatarsal bonesDistal phalanxof great toe
Superior view Medial view
Phalanges
Figure 6.34 Bones of the Legtherighttibiaandfibulaareshown.
Figure 6.35 Bones of the Right Foot
(a) (b)
see78267-Chapter06.indd 137 11-12-01 3:25 PM

138 Chapter 6Sk
elet
al
(fon′tă-nelz′),orsoftspots(figure6.37).Theyallowflexibilityinthe skullduring thebirthprocess, aswell asgrowthof theheadafter birth. Syndesmoses (sin′dez-mō′sēz) are fibrous joints inwhichthebonesareseparatedbysomedistanceandheldtogetherby ligaments. An example is the fibrous membrane connectingmostofthedistalpartsoftheradiusandulna.Gomphoses(gom-fō′sēz)consistofpegsfittedintosocketsandheldinplacebyliga-ments.Thejointbetweenatoothanditssocketisagomphosis.
cartilaginousJointsCartilaginous joints unite two bones by means of cartilage. Onlyslightmovementcanoccuratthesejoints.Examplesarethecartilageintheepiphysealplatesofgrowinglongbonesandthecartilages
6.8 JointSLearning Outcomes After reading this section, you should be able to
A. Describethetwosystemsforclassifyingjoints.B. Explainthestructureofafibrousjoint,listthethreetypes,and
giveexamplesofeachtype.C. Giveexamplesofcartilaginousjoints.D. illustratethestructureofasynovialjointandexplaintheroles
ofthecomponentsofasynovialjoint.e. classifysynovialjointsbasedontheshapeofthebonesinthe
jointandgiveanexampleofeachtype.F. Demonstratethedifferencebetweenthefollowingpairs
ofmovements:flexionandextension;plantarflexionanddorsiflexion;abductionandadduction;supinationandpronation;elevationanddepression;protractionandretraction;oppositionandreposition;inversionandeversion.
A joint, or an articulation, is a place where two bones cometogether. A joint is usually considered movable, but that is notalwaysthecase.Manyjointsexhibitlimitedmovement,andothersarecompletely,oralmostcompletely,immovable. Onemethodofclassifyingjointsisafunctionalclassification.Basedonthedegreeofmotion,ajointmaybecalledasynarthrosis(sin′ar-thrō′sis;nonmovablejoint),anamphiarthrosis(am′fi-ar-thrō′sis; slightly movable joint), or a diarthrosis (dī-ar-thrō′sis;freelymovable joint).However, functionalclassificationissome-what restrictive and is not used in this text. Instead, we use astructuralclassificationwherebyjointsareclassifiedaccordingtothe type of connective tissue that binds the bones together andwhetherthereisafluid-filledjointcapsule.Thethreemajorstruc-turalclassesofjointsarefibrous,cartilaginous,andsynovial.
FibrousJointsFibrous joints consist of two bones that are united by fibroustissueandthatexhibitlittleornomovement.Jointsinthisgroupare further subdivided on the basis of structure as sutures, syn-desmoses,orgomphoses.Sutures (soo′choorz)arefibrous jointsbetween the bones of the skull (see figure 6.11). In a newborn,somepartsofthesuturesarequitewideandarecalledfontanels
Lateralmalleolus
Patella
Tibial tuberosity
Anterior crestof tibia
Medial malleolus
Head of fibula
Calcaneus
Medial epicondyle of femur
Lateral epicondyleof femur
Parietalbone
Occipitalbone
Mastoid (posterolateral) fontanel
Lateral view
Superior view
Frontalbone
Sphenoidal(anterolateral)fontanel
Temporal bone
Squamoussuture
Lambdoidsuture
Coronalsuture
Frontal bones(not yet fusedinto a single bone)
Frontal(anterior)fontanel
Parietalbone
Occipital(posterior)fontanelOccipital
bone
Sagittalsuture
Figure 6.36 Surface Anatomy Showing Bones of the Lower Limb
Figure 6.37 Fetal Skull Showing Fontanels and Sutures
(a)
(b)
see78267-Chapter06.indd 138 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 139Skeletal
(ber′să; pocket). Bursae are located between structures that rubtogether,suchaswhereatendoncrossesabone;theyreducefric-tion,whichcoulddamagethestructuresinvolved.Inflammationofabursa,oftenresultingfromabrasion,iscalledbursitis.Asynovialmembrane may extend as a tendon sheath along some tendonsassociatedwithjoints(figure6.38).
Types of Synovial JointsSynovialjointsareclassifiedaccordingtotheshapeoftheadjoiningarticularsurfaces(figure6.39).Plane joints,orgliding joints,consistof two opposed flat surfaces that glide over each other. Examplesof these joints are the articular facets between vertebrae. Saddle joints consist of two saddle-shaped articulating surfaces orientedatrightanglestoeachother.Movementinthesejointscanoccurintwoplanes.Thejointbetweenthemetacarpalboneandthecarpalbone(trapezium)ofthethumbisasaddlejoint.Hinge jointspermitmovementinoneplaneonly.Theyconsistofaconvexcylinderofoneboneapplied toacorrespondingconcavityof theotherbone.Examples are the elbow and knee joints (figure 6.40a,b). The flatcondylarsurfaceofthekneejointismodifiedintoaconcavesurfacebyshock-absorbing fibrocartilagepadscalledmenisci (mĕ-nis′sī).Pivot jointsrestrictmovementtorotationaroundasingleaxis.Eachpivotjointconsistsofacylindricalbonyprocessthatrotateswithinaringcomposedpartlyofboneandpartlyofligament.Therotationthatoccursbetweentheaxisandatlaswhenshakingthehead“no”isanexample.Thearticulationbetweentheproximalendsoftheulnaandradiusisalsoapivotjoint.
betweentheribsandthesternum.Thecartilageofsomecartilaginousjoints,wheremuchstrainisplacedonthejoint,maybereinforcedbyadditionalcollagenfibers.Thistypeofcartilage,calledfibrocartilage(seechapter4),formsjointssuchastheintervertebraldisks.
SynovialJointsSynovial(si-nō′vē-ăl)jointsarefreelymovablejointsthatcontainfluidinacavitysurroundingtheendsofarticulatingbones.Mostjointsthatunitethebonesoftheappendicularskeletonaresyno-vialjoints,whereasmanyofthejointsthatunitethebonesoftheaxialskeletonarenot.Thispatternreflectsthegreatermobilityoftheappendicularskeletoncomparedtothatoftheaxialskeleton. Severalfeaturesofsynovialjointsareimportanttotheirfunc-tion(figure6.38).Thearticularsurfacesofboneswithinsynovialjointsarecoveredwitha thin layerofarticular cartilage,whichprovidesasmoothsurfacewherethebonesmeet.Thejoint cavityisfilledwithfluid.Thecavityisenclosedbyajoint capsule,whichhelpsholdthebonestogetherandallowsformovement.Portionsofthefibrouspartofthejointcapsulemaybethickenedtoformligaments. In addition, ligaments and tendons outside the jointcapsulecontributetothestrengthofthejoint. A synovial membrane lines the joint cavity everywhereexcept over the articular cartilage. The membrane producessynovial fluid, which is a complex mixture of polysaccharides,proteins,lipids,andcells.Synovialfluidformsathin,lubricatingfilmcovering the surfaces of the joint. In certain synovial joints, thesynovialmembranemayextendasapocket,orsac,calledabursa
Bursa
Joint cavity (filledwith synovial fluid)
Articularcartilage
Tendonsheath
Tendon
Bone
Bone
Blood vesselNerve
Synovial membrane
Fibrous part of joint capsule
Jointcapsule
Outer layer
Inner layerPeriosteum
Figure 6.38 Structure of a Synovial Joint
see78267-Chapter06.indd 139 11-12-01 3:25 PM

140 Chapter 6Sk
elet
al
Class and Example of JointPlane
SlightAcromion process of scapula and clavicleCarpals and metacarpals 2–5Ribs and vertebraeBetween carpal bonesBetween metatarsal bonesBetween tarsal bonesBetween articular processes of adjacent vertebrae
(complex joint with several planes and synchondroses)
Acromioclavicular
Two axes
SlightSlight
Carpometacarpal
CostovertebralIntercarpalIntermetatarsalIntertarsalIntervertebral
Sacroiliac
Tarsometatarsal
Multiple axes as a groupSlightSlightSlightSlightSlight
Slight
Slight
SaddleCarpometacarpal pollicisIntercarpalSternoclavicular
Carpal and metacarpal of thumbBetween carpal bonesManubrium of sternum and clavicle
HingeCubital (elbow)KneeInterphalangealTalocrural (ankle)
Humerus, ulna, and radiusFemur and tibiaBetween phalangesTalus, tibia, and fibula
One axisOne axisOne axisMultiple axes; one predominates
PivotMedial atlantoaxialProximal radioulnarDistal radioulnar
Atlas and axisRadius and ulnaRadius and ulna
RotationRotationRotation
Ball-and-SocketCoxal (hip)Humeral (shoulder)
Coxal bone and femurScapula and humerus
Multiple axesMultiple axes
EllipsoidAtlantooccipitalMetacarpopha- langeal (knuckles)Metatarsopha- langeal (ball of foot)Radiocarpal (wrist)Temporomandibular
Atlas and occipital boneMetacarpal bones and phalangesMetatarsal bones and phalangesRadius and carpal bonesMandible and temporal bone
Two axesTwo axes
Two axes
Multiple axesMultiple axes; one predominates
Ball-and-socket
Ellipsoid
Plane
Saddle
Hinge
Pivot
Structures Joined Movement
Between sacrum and coxal bone
Tarsal bones and metatarsal bones
Figure 6.39 Types of Synovial Joints
see78267-Chapter06.indd 140 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 141Skeletal
type of movement, whereas others permit movement in severaldirections.All themovementsaredescribedrelative to theana-tomicalposition.Becausemostmovementsareaccompaniedbymovementsintheoppositedirection,theyareoftenillustratedinpairs(figure6.41). Flexion and extension are common opposing movementsthatmaybedefinedinanumberofways,althougheachdefinitionhasanexception.Theliteraldefinitionsaretobend(flex)andtostraighten (extend). But we have chosen to use definitions withmoreutilityandfewerexceptions.Thus,wesaythatflexionmovesapartofthebodyintheanteriordirectionfromthefrontalplane,whereas extension moves a part in the posterior direction fromthefrontalplane(figure6.41a,b).Anexceptionistheknee,whereflexionmovestheleginaposteriordirectionandextensionmovesitinananteriordirection.
Ball-and-socket joints consistofaball (head)at theendofoneboneandasocket inanadjacentbone intowhichaportionof the ball fits. This type of joint allows a wide range of move-mentinalmostanydirection.Examplesaretheshoulderandhipjoints (figure 6.40c,d). Ellipsoid (ē-lip′soyd) joints, orcondyloid(kon′di-loyd) joints, are elongated ball-and-socket joints. Theshapeofthejointlimitsitsrangeofmovementnearlytothatofahingemotion,but intwoplanes.Examplesofellipsoid jointsarethejointbetweentheoccipitalcondylesoftheskullandtheatlasofthevertebralcolumnandthejointsbetweenthemetacarpalbonesandphalanges.
typesofMovementThetypesofmovementoccurringatagiven jointarerelated tothe structure of that joint. Some joints are limited to only one
Elbow
Humerus
Fat pad
Olecranon bursa
Trochlea
Articular cartilage of the trochlear notch
Joint capsule
Joint cavity
Synovial membrane
Articular cartilage
Coronoid process
Ulna
Femur
Articularcartilage
Meniscus
Tibia
Quadricepsfemoristendon
Suprapatellarbursa
Subcutaneousprepatellarbursa
Patella
Fat padPatellarligamentDeepinfrapatellarbursa
Knee
Pelvic bone
Articular cartilage
Joint cavity
Ligamentum teres
Head of femur
Neck of femur
Joint capsule
Greatertrochanter
Lessertrochanter
Femur
Hip
Subacromial bursa
Joint cavity
Acromion process (articular surface)
Articular cartilage over head of humerus
Scapula (cut surface)
Joint capsule
Articular cartilageover glenoid cavity
Shoulder
Tendon sheath on tendon of long head of biceps brachii
Biceps brachiitendon
Humerus
Biceps brachiimuscle
Sagittal sectionSagittal section
Frontal section Frontal section
Figure 6.40 Examples of Synovial Joints(a)Elbow.(b)Knee.(c)Shoulder.(d)Hip.
(a)
(c)
(b)
(d)
see78267-Chapter06.indd 141 11-12-01 3:25 PM

142 Chapter 6Sk
elet
al
Flexion
Extension
Pronation
Supination
Medial rotation Lateral rotation
Circumduction
Anterior tofrontal plane
Posterior tofrontal plane
Flexion Extension
Frontal plane
Abduction
Abduction
Adduction
(a)
(d)
(e) (f)
(b) (c)
Figure 6.41 Types of Movement(a)Flexionandextensionoftheelbow.(b)Flexionandextensionoftheneck.(c)abductionandadductionofthefingers.(d)Pronationandsupinationofthehand.(e)Medialandlateralrotationofthearm.(f )circumductionofthearm.
see78267-Chapter06.indd 142 11-12-01 3:25 PM

SkeletalSystem:BonesandJoints 143Skeletal
• Depressionismovementofastructureinaninferiordirection.Openingthemouthinvolvesdepressionofthemandible.
• Excursionismovementofastructuretooneside,asinmovingthemandiblefromsidetoside.
• Oppositionisamovementuniquetothethumbandlittlefinger.Itoccurswhenthetipsofthethumbandlittlefingerarebroughttowardeachotheracrossthepalmofthehand.Thethumbcanalsoopposetheotherdigits.
• Repositionreturnsthedigitstotheanatomicalposition.
Mostmovementsthatoccurinthecourseofnormalactivitiesare combinations of movements. A complex movement can bedescribedbynamingtheindividualmovementsinvolved. Whenthebonesofajointareforcefullypulledapartandtheligamentsaround the jointarepulledor torn,a sprain results.Aseparation exists when the bones remain apart after injury to ajoint.Adislocationiswhentheendofoneboneispulledoutofthesocketinaball-and-socket,ellipsoid,orpivotjoint. Hyperextension is usually defined as an abnormal, forcedextensionofajointbeyonditsnormalrangeofmotion.Forexample,if a person falls and attempts to break the fall by putting out ahand, the force of the fall directed into the hand and wrist maycause hyperextension of the wrist, which may result in sprainedjointsorbrokenbones.Somehealthprofessionals,however,definehyperextension as the normal movement of a structure into thespaceposteriortotheanatomicalposition.
Predict 5
What combination of movements at the shoulder and elbow joints allows a person to perform a crawl stroke in swimming?
6.9 EFFEctSoFaGinGontHESKElEtalSYStEManDJointS
Learning Outcome After reading this section, you should be able to
A. Describetheeffectsofagingonbonesandjoints.
Themostsignificantage-relatedchangesintheskeletalsystemaffectthe joints as well as the quality and quantity of bone matrix. Thebonematrixinanolderboneismorebrittlethaninayoungerbonebecause decreased collagen production results in relatively moremineralandlesscollagenfibers.Withaging,theamountofmatrixalsodecreasesbecause therateofmatrix formationbyosteoblastsbecomesslowerthantherateofmatrixbreakdownbyosteoclasts. Bonemassisatitshighestaroundage30,andmengenerallyhavedenserbonesthanwomenbecauseoftheeffectsoftestosteroneand greater body weight. Race also affects bone mass. African-AmericansandHispanicshavehigherbonemassesthancaucasiansandAsians.Afterage35,bothmenandwomenexperiencealossofboneof0.3–0.5%ayear.Thislosscanincrease10-foldinwomenaftermenopause,whentheycanlosebonemassatarateof3–5%ayearforapproximately5–7years(seeSystemsPathology,“Osteoporosis”). Significantlossofboneincreasesthelikelihoodofbonefrac-tures.Forexample,lossoftrabeculaegreatlyincreasestheriskoffracturesofthevertebrae.Inaddition,lossofboneandtheresultingfractures can cause deformity, loss of height, pain, and stiffness.Lossofbonefromthejawscanalsoleadtotoothloss.
Movementofthefoottowardtheplantarsurface(soleofthefoot),aswhenstandingon the toes, iscommonlycalledplantar flexion.Movementofthefoottowardtheshin,aswhenwalkingontheheels,iscalleddorsiflexion.
acaSEinPoint
Dislocated Shoulder
theshoulderjointisthemostcommonlydislocatedjointinthebody.loosh Holder dislocated his shoulder joint while playing basketball.asaresultofa“charging”foul,looshwasknockedbackwardandfell.ashebrokehisfallwithhisextendedrightarm,theheadoftherighthumerus was forced out of the glenoid cavity.While being helpedup from the floor, loosh felt severe pain in his shoulder, his rightarm sagged, and he could not move his arm at the shoulder. Mostdislocations result in stretching of the joint capsule and movementofthehumeralheadtotheinferior,anteriorsideoftheglenoidcavity.thedislocatedhumeralheadismovedbacktoitsnormalpositionbycarefullypulling it laterallyover the inferior lipof theglenoidcavityand then superiorly into the glenoid cavity.once the shoulder jointcapsule has been stretched by a shoulder dislocation, the shoulderjoint may be predisposed to future dislocations. Some individualshave hereditary“loose” joints and are more likely to experience adislocatedshoulder.
Abduction (ab-dŭk′shun; to take away) is movement awayfromthemedianormidsagittalplane;adduction(tobringtogether)ismovementtowardthemedianplane(figure6.41c).Movingthelegsawayfromthemidlineofthebody,asintheoutwardmove-mentof“jumpingjacks,”isabduction,andbringingthelegsbacktogetherisadduction. Pronation (prō-nā′shŭn) and supination (soo′pi-nā′shun)arebestdemonstratedwiththeelbowflexedata90-degreeangle.Whentheelbowisflexed,pronationisrotationoftheforearmsothatthepalmisdown,andsupinationisrotationofthefore-armsothatthepalmfacesup(figure6.41d). Eversion(ē-ver′zhŭn)isturningthefootsothattheplantarsurface(bottomofthefoot)faceslaterally;inversion(in-ver′zhŭn)isturningthefootsothattheplantarsurfacefacesmedially. Rotationistheturningofastructurearounditslongaxis,asinshakingthehead“no.”Rotationofthearmcanbestbedemon-stratedwiththeelbowflexed(figure6.41e)sothatrotationisnotconfusedwithsupinationandpronationoftheforearm.Withtheelbowflexed,medialrotationofthearmbringstheforearmagainsttheanteriorsurfaceoftheabdomen,andlateralrotationmovesitawayfromthebody. Circumduction (ser-kŭm-dŭk′shŭn) occurs at freely mov-able joints, such as the shoulder. In circumduction, the armmovesso that itdescribesaconewith theshoulder jointat theapex(figure6.41f ). Inadditiontothemovementspicturedinfigure6.41,severalothermovementtypeshavebeenidentified:
• Protraction(prō-trak′shŭn)isamovementinwhichastructure,suchasthemandible,glidesanteriorly.
• Inretraction(rē-trak′shŭn),thestructureglidesposteriorly.• Elevationismovementofastructureinasuperiordirection.
Closingthemouthinvolveselevationofthemandible.
see78267-Chapter06.indd 143 11-12-01 3:25 PM

144
Skel
etal
SYSTEMS PATHOLOGY
OsteoporosisBackground InformationOsteoporosis, or porous bone, is a loss of bone matrix. This loss of bone mass makes bones so porous and weakened that they become deformed and prone to fracture (figure 6B). The occurrence of osteo-porosis increases with age. In both men and women (although it is 2.5 times more common in women), bone mass starts to decrease at about age 40 and continually decreases thereafter. Women can eventually lose approximately one-half, and men one-quarter, of their spongy bone.
In women, decreased production of the female reproductive hormone estrogen can cause osteoporosis, mostly in spongy bone, especially in the vertebrae of the spine and the bones of the fore-arm. Collapse of the vertebrae can cause a decrease in height or, in more severe cases, kyphosis in the upper back (figure 6D). Estrogen levels decrease after menopause, removal of the ovaries, amenor-rhea (lack of menstrual cycle) due to extreme exercise or anorexia nervosa (self-starvation) and cigarette smoking.
In men, reduction in testosterone levels can cause loss of bone tissue. However, this is less of a problem in men than in women because men have denser bones than women, and testosterone levels generally don’t decrease significantly until after age 65.
Inadequate dietary intake or absorption of calcium, sometimes due to certain medications, can also contribute to osteoporosis. Absorption of calcium from the small intes-tine decreases with age. Finally, too little exercise or disuse
from injury can all cause osteoporosis. Significant amounts of bone are lost after only 8 weeks of immobilization.
Skel
etal Osteoporosis
Background InformationOsteoporosisbone mass makes bones so porous and weakened that they become deformed and prone to fracture (figure 6B). The occurrence of osteo-porosis increases with age. In both men and women (although it is 2.5 times more common in women), bone mass starts to decrease at about age 40 and continually decreases thereafter. Women can eventually lose approximately one-half, and men one-quarter, of their spongy bone.
In women, decreased production of the female reproductive hormone estrogen can cause osteoporosis, mostly in spongy bone, especially in the vertebrae of the spine and the bones of the fore-arm. Collapse of the vertebrae can cause a decrease in height or, in more severe cases, kyphosis in the upper back (figure 6D). Estrogen levels decrease after menopause, removal of the ovaries, amenor-rhea (lack of menstrual cycle) due to extreme exercise or anorexia nervosa (self-starvation) and cigarette smoking.
bone tissue. However, this is less of a problem in men than in women because men have denser bones than women, and testosterone levels generally don’t decrease significantly until after age 65.
from injury can all cause osteoporosis. Significant amounts of bone are lost after only 8 weeks of immobilization.
Name: Betty Williams
Gender: Female
Age: 65
Comments
Betty has smoked
heavily for at least
50 years. She does not
exercise, seldom goes
outdoors, has a poor
diet, and is slightly underweight.
While attending a family picnic, Betty
tripped and fell. She reported severe right hip
pain and was not able to put any weight on
her right leg when she arrived in the ER.
Radiographs revealed signi� cant loss
of bone density and a fractured femur neck
(� gures 6B, 6C).
Name:
Gender:
Age:
Normalbone
Osteoporoticbone
FractureKyphosis
Figure 6BPhotomicrograph of osteoporotic bone and normal bone.
Figure 6CRadiograph
Figure 6D
see78267-Chapter06.indd 144 11-12-02 11:39 AM

145
Skeletal
Early diagnosis of osteoporosis can lead to more preventativetreatments. instrumentsthatmeasuretheabsorptionofphotons(par-ticles of light) by bone are currently used; of these, dual-energy x-rayabsorptiometry (DExa) is considered the best. Supplementation ofdietary calcium and vitamin D and exercise are the best preventativeandrehabilitorymeasurestopreventbonelossorregainmildboneloss.calcitonin (Miacalcin) inhibits osteoclast activity, and alendronate(Fosamax),whichbinds tohydroxyapatite,also inhibitsosteoclasts.although osteoporosis is linked to estrogen loss, estrogen therapyhasbeenassociatedwithmanysideeffects,includingbreastcancer,andisnolongerrecommendedasatreatment.
OsteoporosisSymptoms
• Painandstiffnessespeciallyinspine
• Easilybrokenbones• lossofheight
Treatment• Dietarycalciumand
vitaminD• Exercise• calcitonin• alendronate
DIGESTIVEinadequatecalciumand
vitaminDintakecancauseinsufficientca2+absorptioninsmallintestine.
REPRODUCTIVEDecreasedestrogenfollowing
menopausecontributestoosteoporosis.
RESPIRATORYExcessivesmokinglowersestrogen
levels,whichincreasesboneloss.
ENDOCRINEcalcitoninisusedtotreatosteoporosis.
NERVOUSPainfrominjurymayreducefurtherinjury.
CARDIOVASCULARifbonebreakagehasoccurred,increasedbloodflowtothatsiteremovesdebris.Bloodcarriesnutrientsnecessaryforrepair.
LYMPHATIC AND IMMUNEimmunecellshelppreventinfectionaftersurgery,suchashipreplacement.
MUSCULARMuscleatrophyfromreducedactivity.increasedchanceoffallingandbreakingabone.
INTEGUMENTARYlimitedsunexposurelowersvitaminDproduction,which
reducesca2+absorption.
Predict 6
What advice should Betty give to her granddaughter so that the granddaughter will be less likely to develop osteoporosis when she is Betty’s age?
see78267-Chapter06.indd 145 11-12-01 3:26 PM

146 Chapter 6Sk
elet
al
degenerationofthejoints,withadvancingage.Inaddition,theligamentsandtendonssurroundingajointshortenandbecomeless flexible with age, resulting in decreased range of motion.Furthermore,manyolderpeoplearelessphysicallyactive,whichcauses the joints to become less flexible and decreases theirrangeofmotion. The most effective preventative measure against the effectsof aging on the skeletal system is the combination of increasingphysicalactivityandtakingdietarycalciumandvitaminDsupple-ments.Intensiveexercisecanevenreverselossofbonematrix.
DISEASES AND DISORDERS Skeletal System
CONDITION DESCRIPTIONtumors Maybemalignantorbenignandcausearangeofbonedefects
SkELETAL DISORDERS
Growth and Developmental Disorders
Gigantism abnormallyincreasedbodysizeduetoexcessivegrowthattheepiphysealplates
Dwarfism abnormallysmallbodysizeduetoimpropergrowthattheepiphysealplates
osteogenesisimperfecta Brittlebonesthatfractureeasilyduetoinsufficientorabnormalcollagen
rickets Growthretardationduetonutritionaldeficienciesinminerals(ca2+)orvitaminD;resultsinbonesthataresoft,weak,andeasilybroken
Bacterial Infections
osteomyelitis Boneinflammationoftenduetoabacterialinfectionthatmayleadtocompletedestructionofthebone
tuberculosis typically,alungbacteriumthatcanalsoaffectbone
Decalcification
osteomalacia Softeningofadultbonesduetocalciumdepletion;oftencausedbyvitaminDdeficiency
osteoporosis reductioninoverallquantityofbonetissue;seeSystemsPathology
JOINT DISORDERS
arthritis inflammationofajoint;causesincludeinfectiousagents,metabolicdisorders,trauma,andimmunedisorders
rheumatoidarthritis Generalconnectivetissueautoimmunedisease
Degenerativejointdisease (osteoarthritis)
Gradualdegenerationofajointwithadvancingage;canbedelayedwithexercise
Gout increasedproductionandaccumulationofuricacidcrystalsintissues,includingjointcapsules
Bursitis and bunions
Bursitis inflammationofabursa
Bunion Mostbunionsaredeformationsofthefirstmetatarsal(thegreattoe);bursitismayaccompanythisdeformity;irritatedbytightshoes
Jointreplacement replacementofpainfuljointswithartificialjoints
Gotowww.mhhe.com/seeleyess8foradditionalinformationonthesepathologies.
Anumberofchangesoccurwithinmanyjointsasapersonages.Changesinsynovialjointshavethegreatesteffectandoftenpresent major problems for elderly people. With use, the carti-lagecoveringarticularsurfacescanweardown.Whenapersonis young, production of new, resilient matrix compensates forthewear.Asapersonages,therateofreplacementdeclines,andthematrixbecomesmorerigid, thusadding to its rateofwear.The production rate of lubricating synovial fluid also declineswith age, further contributing to the wear of the articular car-tilage. Many people also experience arthritis, an inflammatory
see78267-Chapter06.indd 146 11-12-01 3:26 PM

SkeletalSystem:BonesandJoints 147Skeletal
section6.6,thelumbarvertebraesupportmoreweightthanotherregions of the vertebral column. thomas’ ruptured disk may berepairedwithprolongedbedrestoritmayrequiresurgery.onesuchtypeofsurgeryinvolvesremovingtheruptureddiskandreplacingit with a piece of hipbone. Eventually, the adjacent vertebrae willbecomefusedbyboneacrossthegap.
Answers to the rest of this chapter’s Predict questions are in Appendix E.
anSWErtolEarn To PrEDictSincethequestiontellsusthatthomassufferspainwhenbendingover, it is most likely that he has a ruptured intervertebral disk inhis lumbarregion.Whenthesedisksrupture,aportionofthediskprotrudesandpushesagainstthespinalcordorthespinalnerves,compromises their function,andproducespain.Herniationof theinferior lumbar disks is most common because, as you learned in
Theskeletalsystemconsistsofbone,cartilage,tendons,andligaments.
6.1 Functions of the Skeletal System (p. 110)
1. Theskeletalsystemprovidesthemajorsupportforthebody. 2. Boneprotectsinternalorgans. 3. Jointsallowmovementbetweenbones. 4. Bonesstoreandreleasemineralsasneededbythebody. 5. Bonemarrowgivesrisetobloodcellsandplatelets.
6.2 Extracellular Matrix (p. 111)
1. Bone,cartilage,tendons,andligamentsareconnectivetissues. 2. Varyingamountsofcollagen,proteoglycan,organicmolecules,
water,andmineralsinthematrixdeterminethecharacteristicsofconnectivetissue.
6.3 General Features of Bone (p. 111)
Therearefourcategoriesofbone:long,short,flat,andirregular.
Structure of a Long BoneLongbonesconsistofadiaphysis(shaft),epiphyses(ends),andepiphyseal(growth)plates.Thediaphysiscontainsamedullarycavity,whichisfilledwithmarrow,andtheendoftheepiphysisiscoveredbyarticularcartilage.
Histology of Bone 1. Osteoblastsarebone-formingcells. 2. Osteocytesarebonecellslocatedbetweenthinsheetsofextracellular
matrixcalledlamellae. 3. Compactbonetissueconsistsofosteons,whicharecomposedof
osteocytesorganizedintolamellaesurroundingcentralcanals. 4. Spongybonetissueconsistsoftrabeculaewithoutcentralcanals.
Bone Ossification 1. Intramembranousossificationoccurswithinconnectivetissue
membranes. 2. Endochondralossificationoccurswithincartilage.
Bone GrowthBoneelongationoccursattheepiphysealplateaschondrocytesproliferate,enlarge,die,andarereplacedbybone.
Bone RemodelingBoneremodelingconsistsofremovalofexistingbonebyosteoclastsanddepositionofnewbonebyosteoblasts.
Bone RepairDuringbonerepair,cellsmoveintothedamagedareaandformacallus,whichisreplacedbybone.
6.4 Bone and Calcium Homeostasis (p. 117)
1. Osteoclastsremovecalciumfrombone,causingbloodcalciumlevelstoincrease.
2. Osteoblastsdepositcalciumintobone,causingbloodcalciumlevelstodecrease.
3. Parathyroidhormoneincreasesbonebreakdown,whereascalcitonindecreasesbonebreakdown.
6.5 General Considerations of Bone Anatomy (p. 119)
Thereare206bonesintheaverageadultskeleton.
6.6 Axial Skeleton (p. 120)
Theaxialskeletonincludestheskull,vertebralcolumn,andthoraciccage.
Skull 1. Theskullconsistsof22bones:8formingthebraincaseand14facial
bones.Thehyoidboneand6auditoryossiclesareassociatedwiththeskull.
2. Fromalateralview,theparietal,temporal,andsphenoidbonescanbeseen.
3. Fromafrontalview,theorbitsandnasalcavitycanbeseen,aswellasassociatedbonesandstructures,suchasthefrontalbone,zygomaticbone,maxilla,andmandible.
4. Theinteriorofthecranialcavitycontainsthreefossaewithseveralforamina.
5. Seenfrombelow,thebaseoftheskullrevealsnumerousforaminaandotherstructures,suchasprocessesformuscleattachment.
Vertebral Column 1. Thevertebralcolumncontains7cervical,12thoracic,and5lumbar
vertebrae,plus1sacralboneand1coccyxbone. 2. Eachvertebraconsistsofabody,anarch,andprocesses. 3. Regional differences in vertebrae are as follows: Cervical vertebrae
have transverse foramina; thoracic vertebrae have long spinousprocesses and attachment sites for the ribs; lumbar vertebrae haverectangular transverse and spinous processes, and the position oftheir facets limits rotation; the sacrum is a single, fused bone; thecoccyxis4orfewerfusedvertebrae.
SuMMarY
see78267-Chapter06.indd 147 11-12-01 3:26 PM

148 Chapter 6Sk
elet
al
6.8 Joints (p. 138)
Ajointisaplacewherebonescometogether.
Fibrous JointsFibrousjointsconsistofbonesunitedbyfibrousconnectivetissue.Theyallowlittleornomovement.
Cartilaginous JointsCartilaginousjointsconsistofbonesunitedbycartilage,andtheyexhibitslightmovement.
Synovial Joints 1. Synovialjointsconsistofarticularcartilageovertheunitingbones,
ajointcavitylinedbyasynovialmembraneandcontainingsynovialfluid,andajointcapsule.Theyarehighlymovablejoints.
2. Synovialjointscanbeclassifiedasplane,saddle,hinge,pivot,ball-and-socket,orellipsoid.
Types of MovementThemajortypesofmovementareflexion/extension,abduction/adduction,pronation/supination,eversion/inversion,rotation,circumduction,protraction/retraction,elevation/depression,excursion,andopposition/reposition.
6.9 Effects of Aging on the Skeletal System and Joints (p. 143)
1. Bonematrixbecomesmorebrittleanddecreasesintotalamountduringaging.
2. Jointslosearticularcartilageandbecomelessflexiblewithage. 3. PreventionmeasuresincludeexerciseandcalciumandvitaminD
supplements.
Rib Cage 1. Theribcageconsistsofthethoracicvertebrae,theribs,andthe
sternum. 2. Thereare12pairsofribs:7trueand5false(2ofthefalseribsare
alsocalledfloatingribs). 3. Thesternumconsistsofthemanubrium,thebody,andthexiphoid
process.
6.7 Appendicular Skeleton (p. 129)
Theappendicularskeletonconsistsofthebonesoftheupperandlowerlimbsandtheirgirdles.
Pectoral GirdleThepectoralgirdleincludesthescapulaeandclavicles.
Upper LimbTheupperlimbconsistsofthearm(humerus),forearm(ulnaandradius),wrist(8carpalbones),andhand(5metacarpalbones,3phalangesineachfinger,and2phalangesinthethumb).
Pelvic GirdleThepelvicgirdleismadeupofthe2coxalbones.Eachcoxalboneconsistsofanilium,anischium,andapubis.Thecoxalbones,sacrum,andcoccyxformthepelvis.
Lower LimbThelowerlimbincludesthethigh(femur),leg(tibiaandfibula),ankle(7tarsalbones),andfoot(metatarsalbonesandphalanges,similartothebonesinthehand).
1. Whataretheprimaryfunctionsoftheskeletalsystem? 2. Namethemajortypesoffibersandmoleculesintheextracellular
matrixoftheskeletalsystem.Howdotheycontributetothefunctionsoftendons,ligaments,cartilage,andbones?
3. Definediaphysis,epiphysis,epiphysealplate,medullarycavity,articularcartilage,periosteum,andendosteum.
4. Describethestructureofcompactbone.Howdonutrientsreachtheosteocytesincompactbone?
5. Describethestructureofspongybone.Whataretrabeculae?Howdonutrientsreachosteocytesintrabeculae?
6. Defineanddescribeintramembranousandendochondralossification.
7. Howdobonesgrowindiameter?Howdolongbonesgrowinlength? 8. Whatisaccomplishedbyboneremodeling?Howdoesbonerepair
occur? 9. Definetheaxialskeletonandtheappendicularskeleton.10. Namethebonesofthebraincaseandtheface.11. Givethelocationsoftheparanasalsinuses.Whataretheir
functions?12. Whatisthefunctionofthehardpalate?13. Throughwhatforamendoesthebrainconnecttothespinalcord?
14. Howdothevertebraeprotectthespinalcord?Wheredospinalnervesexitthevertebralcolumn?
15. Nameandgivethenumberofeachtypeofvertebra.Describethecharacteristicsthatdistinguishthedifferenttypesofvertebraefromoneanother.
16. Whatisthefunctionofthethoraciccage?Namethepartsofthesternum.Distinguishamongtrue,false,andfloatingribs.
17. Namethebonesthatmakeupthepectoralgirdle,arm,forearm,wrist,andhand.Howmanyphalangesareineachfingerandinthethumb?
18. Definethepelvicgirdle.Whatbonesfusetoformeachcoxalbone?Whereandwithwhatbonesdothecoxalbonesarticulate?
19. Namethebonesofthethigh,leg,ankle,andfoot.20. Definejoint,orarticulation.Nameanddescribethedifferences
amongthethreemajorclassesofjoints.21. Describethestructureofasynovialjoint.Howdothedifferentparts
ofthejointpermitjointmovement?22. Onwhatbasisaresynovialjointsclassified?Describethedifferent
typesofsynovialjoints,andgiveexamplesofeach.Whatmovementsdoeseachtypeofjointallow?
23. Describeandgiveexamplesofflexion/extension,abduction/adduction,andsupination/pronation.
rEViEWanDcoMPrEHEnSion
see78267-Chapter06.indd 148 11-12-01 3:26 PM

SkeletalSystem:BonesandJoints 149Skeletal
1. A12-year-oldboyfellwhileplayingbasketball.Thephysicianexplainedthatthehead(epiphysis)ofthefemurwasseparatedfromtheshaft(diaphysis).Althoughthebonewassetproperly,bythetimetheboywas16,itwasapparentthattheinjuredlowerlimbwasshorterthanthenormalone.Explainwhythisdifferenceoccurred.
2. JustinTimeleapedfromhishotelroomtoavoidburningtodeathinafire.Ifhelandedonhisheels,whatbonewaslikelytofracture?UnfortunatelyforJustin,a240-poundfireman,HeftyStomper,ranbyandsteppedheavilyonthedistalpartofJustin’sfoot(notthetoes).Whatbonesnowcouldbebroken?
3. Onedaywhileshopping,Ms.WanttaBargainpickedupher3-year-oldson,Somm,byhisrightwristandliftedhimintoashoppingcart.Sheheardaclickingsound,andSommimmediatelybegantocryandholdhiselbow.Giventhatliftingthechildcausedaseparationattheelbow,whichismorelikely:separationoftheradiusandhumerus,orseparationoftheulnaandhumerus?
4. Whyarewomenknock-kneedmorecommonlythanmen? 5. Askeletonwasdiscoveredinaremotemountainarea.Thecoroner
determinedthatnotonlywastheskeletonhuman,butitwasfemale.Explain.
Answers in Appendix D
criticaltHinKinG
Visitthisbook’swebsiteat www.mhhe.com/seeleyess8 forchapterquizzes,interactivelearningexercises,andotherstudytools.
see78267-Chapter06.indd 149 11-12-01 3:26 PM