67740161 case-study-aml-intro
61
ANGELES UNIVERSITY FOUNDATION GRADUATE SCHOOL Master of Arts in Nursing A Case Study On ACUTE MYELOGENOUS LEUKEMIA PRESENTED TO ANNA LYN M.PAANO, RN, MAN Professor, Concepts I
-
Upload
homework-ping -
Category
Education
-
view
194 -
download
1
Transcript of 67740161 case-study-aml-intro

ANGELES UNIVERSITY FOUNDATION
GRADUATE SCHOOL
Master of Arts in Nursing
A Case Study On
ACUTE MYELOGENOUS LEUKEMIA
PRESENTED TO
ANNA LYN M.PAANO, RN, MAN
Professor, Concepts I
Presented By
EPIFANIA P. GOGOLIN, RN

MAN Student
I. INTRODUCTION
The terms malignant and cancerous describe cells that are growing and
proliferating in a disorderly, chaotic fashion. In adults, cancer usually occurs in the form
of a solid tumor. In children, the most frequent type of cancer is that of an immature cell
overgrowth, or leukemia (McCance & Heuther,2004).
Acute myelogenous leukemia (AML) is results from a defect from a
hematopoeitic stem cells that differentiates into all myeloid cells: monocytes,
granulocytes (neutrophils, basophils, eosinophils), erythrocytes and platelets (Smeltzer,
et al., 2004). AML comprises approximately 11% of the cases or leukemia in childhood
in the United States, with approximately 400 children diagnosed with AML annually.
Unlike ALL, the incidence of AML is constant from birth throughout the first 10
years of life with a slight peak in late adolescence. Internationally, AML is more
commonly diagnosed in developed countries. AML is also more common in men than in
women. There is no known relationship between race and the incidence of AML. It was
observed though, that AML is more common in whites than in other populations. The
difference is even more apparent in older patients. Prevalence increases with age.
However, this disease affects all age groups (Seiter, 2006).
The prognosis is highly variable. Patient age may be a factor; patients who are
younger may survive for 5 years or more after diagnosis of AML. However., patients who
are older or have a more undifferentiated form of AML tend to have worse prognosis.
Patients with supportive care usually survive less than 1 year, with death usually a result
of infection and hemorrhage (American Cancer Society, 2006).
AML can present with relative subtle, nonspecific symptoms such anorexia,
malaise, irritability, and weight loss. As the disease progresses, they present with signs
and symptoms associated with the failure of normal hematopoiesis, which results from
the replacement of normal marrow cells by malignant cells. The child may exhibit fatigue
pallor, and decreased activity due to anemia; easy bruising and bleeding associated with

thrombocytopenia; or fever and infection secondary to neutropenia. Bone pain and
arthralgias are less-common presenting symptoms in children with AML than those with
ALL. Massive hepatosplenomegaly is uncommon except in infants with AML (Seiter,
2006).
Bone marrow aspiration and biopsy are the definitive diagnostic tests.
Approximately 10% of patients with acute leukemia do not have circulating blasts at
diagnosis. One or more of the following lab tests may be used to diagnose AML and/or
to determine the specific subtype of AML. Samples of blood, bone marrow, or CSF are
looked at under a microscope by a pathologist and may be reviewed by the patient's
hematologist/oncologist. Based on the cells' size, shape, and other traits, doctors can
classify them into specific cell types. A key element of this classification is whether the
cells look like normal cells of circulating blood (mature) or lack features of normal blood
cells (immature).
The percentage of cells in the bone marrow or blood that are blasts (immature) is
particularly important. Having at least 20% blasts in the marrow or blood is generally
required for a diagnosis of acute myeloid leukemia. AML can also be diagnosed if the
blasts have a chromosome change that occurs only in a specific type of AML, even
though the blast percentage doesn't reach 20%. In order for a patient to be considered
to be in remission after treatment, the blast percentage must be no higher than 5%.
Additional tests that are used to confirm the diagnosis of AML are as follows.
Cytochemistry tests involve exposing cells to chemical stains (dyes) that react with only
some types of leukemia cells. Flow cytometry on the other hand is a technique which is
often used to look at the cells from bone marrow and blood samples. It is very accurate
in determining the exact type of leukemia. Related tests, called immunohistochemistry
tests, can be used to detect these substances when viewing cells under a microscope.
These tests are used for immunophenotyping--classifying leukemia cells according to
the substances (antigens) on their surfaces. There is also cytogenetics. These tests
examine a cell's chromosomes (long strands of DNA) under a microscope. Fluorescent
in situ hybridization (FISH) is a procedure similar to cytogenetic testing. It can find most
chromosome changes (such as translocations) that are visible under a microscope in
standard cytogenetic tests, as well as some changes too small to be seen with usual
cytogenetic testing. Very sensitive DNA tests such as polymerase chain reaction (PCR)

tests can also find translocations too small to be seen under a microscope, even if very
few leukemia cells are present in a sample. These tests may also be used after
treatment to find small numbers of leukemia cells that may not be visible under a
microscope.
There are also several imaging studies that might be done in people with AML,
but they are done more often to look for infections or other problems, rather than to look
for the leukemia itself. Because leukemia does not usually form visible tumors, imaging
tests are of limited value. In some cases imaging studies may be done to help
determine the extent of the disease, if it is thought it may have spread beyond the bone
marrow and blood. Routine chest x-rays may be done if a lung infection is suspected.
Computed tomography (CT) scan, Magnetic resonance imaging (MRI) scan, ultrasound,
GaLium amd bone scan can also be done. If leukemia is a possibility, a biopsy of the
area may be needed to confirm this.
The French-American-British (FAB) cooperative group has classified AML in to
eight subtypes (M0-M7) based on blast cell morphology and reactivity with histochemical
stains. A newer classification for hematopoietic and lymphoid neoplasms was developed
by the World Health Organization (WHO) that includes not only morphologic findings but
also genetic, immunophenotypic, biologic, and clinical features to define specific disease
entities. In the WHO classification the blast threshold for the diagnosis of AML is
reduced from 30 to 20% in the blood or marrow. In addition, patients with clonal
recurring cytogenetic abnormalities are classified as having AML regardless of blast
percentage.
The older, more traditional, FAB classification is as follows: M0 - Undifferentiated
leukemia;M1 - Myeloblastic without differentiation; M2 - Myeloblastic with differentiation;
M3 – Promyelocytic; M4 – Myelomonocytic; M4eo - Myelomonocytic with
eosinophilia;M5 - Monoblastic leukemia (M5a - Monoblastic without differentiation / M5b
- Monocytic with differentiation); M6 – Erythroleukemia; M7 - Megakaryoblastic leukemia
The newer WHO classification is as follows: 1) AML with recurrent genetic
abnormalities (AML with t(8;21)(q22;q22), (AML1/ETO) ; AML with abnormal bone
marrow eosinophils and inv(16)(p13q22) or t(16;16)(p13)(q22), (CBFB/MYH11) ; APL
with t(15;17)(q22;q12), (PML/RARa) and variants ; AML with 11q23 (MLL)

abnormalities): 2) AML with multilineage dysplasia (Following myelodysplastic syndrome
(MDS) or MDS/myeloproliferative disease (MPD); Without antecedent MDS or
MDS/MPD but with dysplasia in at least 50% of cells in 2 or more lineages): 3) AML and
MDS, therapy related ( Alkylating agent or radiation-related type; Topoisomerase II
inhibitor type; Others): 4) AML, not otherwise classified (AML, minimally differentiated;
AML, without maturation; AML, with maturation; Acute myelomonocytic leukemia; Acute
monoblastic or monocytic leukemia; Acute erythroid leukemia; Acute megakaryoblastic
leukemia; Acute basophilic leukemia; Acute panmyelosis and myelofibrosis; Myeloid
sarcoma).
Although several factors have been implicated in the causation of AML, most
patients who present with AML have no identifiable risk factor. Some congenital
disorders that predispose patients to AML include Bloom syndrome, Down syndrome,
congenital neutropenia, Fanconi anemia, and neurofibromatosis. Usually, these patients
develop AML during childhood; rarely, some may present in young adulthood. More
subtle genetic disorders, including polymorphisms of enzymes that metabolize
carcinogens, also predispose patients to AML. Several studies demonstrate a
relationship between radiation exposure and leukemia. Early radiologists (prior to
appropriate shielding) were found to have an increased likelihood of developing
leukemia. Persons who smoke have a small but statistically significant (odds ratio, 1.5)
increased risk of developing AML. In several studies, the risk of AML was slightly
increased in people who smoked compared with those who did not smoke. Exposure to
benzene is associated with aplastic anemia and pancytopenia. These patients often
develop AML.
Treatment of AML is divided into two stages: induction of remission and post
remission consolidation or intensification. Long-term maintenance treatment is no longer
generally used. All children should be referred to a pediatric oncology center for
treatment. Patients are placed into high-, intermediate- or low-risk groups, and their
chemotherapy protocols are adjusted accordingly. Approximately 50% of children treated
with chemotherapy alone appear to be cured of their leukemia. The outcome is
somewhat better for children who, while their first remission receive bone marrow
transplants from histocompatible sibling donors, with an 8-year survival rate of 60%. The
prognosis for children who do not enter remission or those that suffer from on-therapy
relapse is poor. Intensive reinduction therapies and bone marrow transplant for second

complete remission is associated with significant treatment-related morbidity and
mortality.
For current trends and issues, a number of new drugs are currently in clinical
trials. The two most promising areas are farnesyl transferase inhibitors and drugs that
target FLT3. Farnesyl transferase inhibitors target ras, a molecule that is involved in the
pathophysiology of various hematologic malignancies. Two drugs of this type, tipifarnib
and lonafarnib, are currently undergoing clinical trials. Early results have demonstrated
responses in 15-30% of patients with minimal toxicity. Drugs that target FLT3, such as
MLN518 and PKC412, are also currently being studied.
Newer treatment for AML is Gemtuzumab ozogamicin. Gemtuzumab ozogamicin
is a monoclonal antibody against CD33 (a molecule present on most AML cells but not
on normal stem cells) conjugated to calicheamicin (a potent chemotherapy molecule).
Gemtuzumab ozogamicin is currently approved by the Food and Drug Administration in
the United States for the treatment of patients with CD33-positive AML in first relapse
who are aged 60 years or older and who are not considered candidates for other
cytotoxic chemotherapy. Sievers reported the results of gemtuzumab ozogamicin
administration in 142 patients with AML who were in their first relapse and who had no
history of an antecedent hematologic disorder (AHD). Sixteen percent of patients
obtained a formal complete response. An additional 13% of patients met criteria for
complete response but did not have the required platelet recovery. Toxicity included
infusion reactions, myelosuppression, and hepatic toxicity. Newer studies are
investigating the use of gemtuzumab ozogamicin in combination with other
chemotherapy agents and in patients with newly diagnosed AML. Although gemtuzumab
ozogamicin is an active drug, the response rate is lower than that obtained with standard
"3 and 7" chemotherapy.
This particular case was chosen because it gave opportunity for the MAN student
to further learn and deepen her understanding about the condition and its treatment.
Aside from providing a learning experience, this case also allowed opportunity to
demonstrate the caring role that a nurse has.
OBJECTIVES
Patient-centered

After handling the patient and do proper nursing interventions, the patient with
the help of the significant others will be able to:
Short-term objectives:
1. Recognized the condition that are threatening to his health
2. Appreciate all the health teaching and cooperate with the nursing
interventions done for his comfort
3. Apply measures taught to prevent the worsening of his condition
Long-term objectives:
1. Maintain a healthy lifestyle that is contributory to health maintenance and
personal development
2. In time, sustain lifestyle that best ensure optimum level of functioning
3.Broaden knowledge regarding self-care measures at home
Nurse-centered
After handling patient and do proper nursing interventions, the nurse will
be able to:
Short-term objectives:
1. Establish a good nurse-client relationship with the client
2. Impart appropriate health teachings according to the clients needs
3. Describe illness and in-hospital experiences as they must appear to the child.
4. Established expected outcomes for the child.
5. Implement measures such as orientation, education and therapeutic play to
reduce stress of illness.

Long-term objective:
1. Improve/ deepen the nurses’ understanding, knowledge and skills with the
disease.
2. Promote effective nursing care to all the clients that may be handled in the
future with the same disease condition.
3. Apply/share the learning from the experience to colleagues, students, clients &
demonstrate a caring role as a nurse has.
4. Identify areas related to illness in children that could benefit from additional
nursing research or application of evidence-based practice.
II. Nursing Assessment
A. Personal History
The subject of this case study is given the name Totoy Bibo to protect his
real identity. He is a 3 year old, male, born on the 23rd of July year 2005 in one of
the medical hospital in Manila. A Filipino citizen, baptized as a Roman Catholic,
and a resident of 48 B Rizal St., Lapaz Tarlac. He was admitted in a tertiary
government hospital in Tarlac, last October 3, 2008 with chief complaints of
epistaxis, gum bleeding and low blood and platelet count.
The Bibo family is a nuclear type of family composing of three members;
his mother, father and Totoy Bibo himself. His father and mother are both 31
years of age. His father formerly works as a security guard at a firm in Manila and
is currently self-employed as a “balot & mani” vendor. His mother on the other
hand is a plain housewife. Mr. and Mrs. Bibo are not married and have been
living together for four years. This is Mrs. Bibo’s second family; she have five
children in her first husband. Totoy Bibo on the other hand is the only child with
her second husband.

The three of them are currently living in a compound comprising of
several families. According to Mrs. Bibo, their place is a wooden-concrete type of
building that is in bad condition because of a fire incident long ago. The residents
are also complaining of foul smelling air because of a poultry located infront of
their vicinity. Their toilet is water sealed and they have water pump as the source
of water supply. According to the mother their place is small but clean and well
maintained, with a small living room, one bedroom where the family sleeps
together, a kitchen and a comfort room. Their water is boiled before it is used by
the family. Mrs. Bibo also mentioned that the father of Totoy Bibo occasionally
smokes and drinks with his peers. The mother on the other hand is fond of
sweets and foods rich in carbohydrates, especially during her pregnancy. She
also admits that at an early age, they already offered Totoy Bibo softdrinks or
carbonated drinks for refreshment.
As for the families health belief and practices, the family believe in several
superstitions which affect their judgment and decisions sometimes. The Bibo
family believes in faith healers and “manghihilot” especially when someone get
fractures or sprains. They also make use of herbal medicines to heal several
conditions which they contemplate to be effective and at the same time
inexpensive. They also practice self-medications and more often than not buy
some over the counter drugs for common illnesses like paracetamol for fever.
They go to medical practitioners when they find no relief or the illness persistently
bothers them.
B. OBSTETRICAL HISTORY/ GROWTH & DEVELOPMENT
Mrs. Bibo’s last menstrual period was November 2004 and after nine months,
she delivered a healthy 8.9 lbs baby boy after five hours of labor at Quirino
Memorial Hospital in Manila, July 23, 2005 via normal spontaneous delivery.
During her nine months pregnancy, she recalls that she was fond of eating
watermelon and bananas. She cannot recall any serious illness or medications
taken. She claims that she did not have any problem at all during the pregnancy.
Totoy Bibo had his first bowel movement and urine output the first 24 hours
after delivery. His umbilical stump fell after 4 days. No jaundice, cyanosis, or

congenital anomalies were noted. Totoy Bibo have no known allergies for foods,
drugs, pollen or dust. Like her other children, Totoy Bibo was never breastfed by
his mother. He was first fed by formulated milk known as Bona, then after two
months was changed to rice milk or what is commonly called as “am” derived
from boiled rice. After that Totoy Bibo was fed in combination of Bear Brand, am
and Milo. He was than introduced to eating lugaw, mashed carrot, potato and
squash. It was also mentioned that even before reaching his first birthday, the
parents already give softdrinks for Totoy Bibo to drink. He is completely
immunized at the local health center in Lapaz, and was commonly noted to be
overweight during his monthly check ups.
Totoy Bibo being three years of age is a toddler under the Autonomy VS
shame and Doubt in Erik Erickson’s Psychosocial Development theory, where
the child focuses on self-control and confidence and failure to reinforce these
efforts will lead the child to doubt themselves and trust in them. As for his
cognitive development according to Jean Piaget, Totoy Bibo is under the Pre-
operational Thought where the thought of the child can comprehend simple
abstract and can arrive at answers mentally instead of physical attempts but
basically their thinking is still concrete and literal. Their type of play in this stage
is parallel play. As for Sigmund Freud’s PsychoAnalytical theory, Totoy bibo is in
the Anal Phase, where his interest is in self-discovery and finds pleasure and
sense of control in retention and defecation of feces & urine.
We can see Totoy Bibo’s autonomy by being able to feed himself and
verbalize and choose the food he wants to eat. The child is also clever and
understands the need for the oxygen cannula when he is having difficulty in
breathing. He also shows interest in playing with his room mates and he has a
robot and cars to play with. He has not been able to practice control in urination
and defection over some time because of the treatment and medication regimen
being imposed.
C. FAMILY-HEALTH ILLNES HISTORY

Legend:Red - Hypertension/Heart Disease Yellow – Tuberculosis
Green – Asthma
Figure 1. Genogram
The paternal grandparents of Totoy Bibo are known to have hypertensions and
all of his uncle and aunts including his father have asthma. In his maternal side, Totoy
Bibo’s grandfather have already passed away due to stroke. His grandmother on the
other hand is still living but has a history of tuberculosis. There are no known disease
or illness that have befallen her aunts and uncles in his mother side. All are in good
health as of the present.
D. HISTORY OF PAST ILLNESS
Totoy Bibo has a history of being brought at the emergency department of a
district hospital in Lapaz Tarlac several times at an early age of 1-2 years. The chief
complaints of which are mainly fever with convulsions and upper respiratory infections,
wherein her mother recalled that paracetamol, oxygen and nebulizations to be the
prompt treatment. Aside from this, there were no other illness or reasons for check up or
hospitalizations.
E. HISTORY OF PRESENT ILLNESS
Grandfather Grandmother Grandfather (†) Grandmother
Uncle 3
Uncle 2
Aunt 3Aunt 2Aunt Uncle 11
TOTOY BIBO
Uncle
Uncle
Aunt
Mother
Father
Uncle

March 29, 2008, Totoy Bibo was rushed to a tertiary government hospital in
Tarlac City after being suggested by the doctors in the district hospital in Lapaz when
results of his platelet and blood components were found to be below normal and in need
of immediate blood transfusion. Severe paleness and a marked decreased of
hemoglobin count of 20-25g/L was the chief complaint. He was then treated with packed
red blood cells and other unrecalled medication. After two weeks of treatment, Totoy
Bibo undergone bone marrow aspiration as ordered by his attending physician and was
diagnosed with Acute Myelogenic Leukemia-M1. Totoy Bibo then undergone
chemotherapy as advised, but the treatment was put to a halt after two months (2
cycles) because of financial constraints. For four months, he was in and out of the
hospital because of bleeding, paleness and severe dropped with his hemoglobin,
platelet and other blood components. Blood transfusions and other unrecalled
medications were given when Totoy Bibo was hospitalized. The persistence of epistaxis
and gum bleeding brought the patient back last October 3, 2008 and was then admitted.
F. PHYSICAL EXAMINATION
October 3, 2008, Emergency Room Pediatrics resident-on-duty’s assessment findings, as lifted from the chart
General: irritable & restless
Pale, palpebral conjunctiva, anicteric sclerae
With gum bleeding & epistaxis
With petechiae on both arms
Distended abdomen, no tenderness
Normal extremities
With vital signs of:
Temp : 37oC RR: 54 PR: 143
October 20, 2008 (Nurse-Patient Interaction )

General Survey
Seen patient on bed, with IVF of D5 0.3 NaCl at 250 cc level infusing on his left cephalic
vein. Patient is crying and restless; with body malaise; increased respiratory effort with
minimal movement; needs full assistance to do ADL. He was wearing a shirt and a pair
of pajamas. No appetite but with increased water intake (4-5 cups of water within an
hour). Vital signs taken as follows:
Temp: 37.4°C RR: 60HR: 154
Physical assessment:Head and Face:
a. Hair: with fine short black hairb. Scalp: no evidence of dandruff or flaking; no tenderness of the scalp
noted.c. Skull: normal skull configuration, no abnormal elevation or depression.d. Face: symmetrical in shape, no tenderness upon palpation
Eyes: a. General: eyes are symmetrical, with noted periorbital hematoma (racoon-
like eyes),b. Pupils: dark brown in color, with equal size approximately 2-3 mm,
positive PERRLAc. Eyebrows: equal distribution of hair on both sided. Eyelids and Eyelashes: no nodules and tenderness noted, with minimal
swelling of lower eyelid.e. Lacrimal puncta: no nodules and tenderness noted.f. Sclerae: whitish sclerae with evident capillaries, no jaundice noted.g. Conjunctiva: pale conjunctiva.h. Vision: with good visual acuity
Ears: a. External: symmetrical appearance of pinna, no lesions or abnormal
discharges or swelling.b. Internal: no discharges notedc. Cranial Nerve VIII: no hearing impairment of both ears.
Nose: Symmetrical nares, no discharge, exudates, no bleeding nor swelling
noted. Mouth and Throat:
a. Mouth/Lips: dry & cracked, with swelling & sores on both lips and gums with minimal bleeding noted.
b. Tongue: no lesion and ulceration and able to take tongue out when instructed
c. Soft palate and uvula: no swelling on palate and uvulad. Throat: no sore throat noted
Neck:a. General: no difficulty with neck mobility

b. Blood vessels: slight distension of jugular vein is noted.c. Trachea: no masses noted, and no thyroid gland enlargement.
Integumentary: a. Skin: pale in color, with warm skin, petechial rashes on both palm of the
hands, with minute hematoma noted on joint areas on both upper and lower extremity,
b. Nails: short and clean; with capillary refill of 3 seconds, absence of clubbing and discoloration
c. Hair: with equal distribution of hairLymph Nodes
With slightly enlarged cervical lymph nodesChest/Back:
a. Respiration: with notable increase in respiratory rate, with slight difficulty in breathing
b. Lungs: Rales auscultated from both lung fields.c. Chest: with equal chest expansion, with equal anterioposterior
diameter, no abnormal retraction, circumference measuring 48 cm in width. Visible heart beat noted
d. Back: with minute hematoma at the back & prominent at shoulder blades
Cardiovascular: a. Heart: positive S1 and S2 sounds, no murmurb. Peripheral pulses: negative palpitations with normal rate
Gastrointestinal:a. Abdomen: with rigid abdomen; abdominal girth of 62 cm; no striae or
rashes noted, no protruding mass or discharge on the umbilicus, no ascites, normoactive bowel sounds, no rebound tenderness, no tenderness on kidneys and liver upon palpation.
Musculoskeletal:a. Upper Extremities: equal in size, symmetrical in shape with no evident
distension of veins, and equal pulses, no edema noted. Pale with petechial rashes on both palms of the hands and minute hematoma on joint areas.
b. Lower Extremities: equal in size, symmetrical in shape with no evident distension of veins, and equal pulses. With enlarged bleeding hematoma at the left foot measuring about 4-5cm in circumference with wound dressing.
October 21, 2008 ( during the Nurse-Patient Interaction )
General Survey
Seen patient on bed, with IVF of D5 0.3 NaCl at 500 cc level infusing on his left cephalic
vein. Patient is crying and restless; with body malaise; increased respiratory effort with
minimal movement; needs moderate assistance to do ADL. He was wearing a shirt and
a pair of pajamas. With minimal appetite (Patient observed chewing hotdogs but not

swallowing the food). With increased water intake (4-5 1/2 cups of water within an hour).
Vital signs taken as follows:
Temp: 37.8°C RR: 44HR: 120
Physical assessment:Head and Face:
a. Hair: with fine short black hairb. Scalp: no evidence of dandruff or flaking; no tenderness of the scalp
noted.c. Skull: normal skull configuration, no abnormal elevation or depression.d. Face: symmetrical in shape, no tenderness upon palpation and no
crepitus heard while moving the jawEyes:
a. General: eyes are symmetrical, with noted periorbital hematoma (racoon-like eyes)
b. Pupils: black in color, with equal size approximately 2-3 mm, positive PERRLA
c. Eyebrows: equal distribution of hair on both sided. Eyelids and Eyelashes: no evidence of infection, no nodules and
tenderness noted, with minimal swelling of lower eyelid.e. Lacrimal puncta: no nodules and tenderness noted.f. Sclerae: whitish sclerae with evident capillaries, no jaundice noted.g. Conjunctiva: pale conjunctiva.h. Vision: with good visual acuity
Ears: a. External: symmetrical appearance of pinna, no lesions or
abnormal discharges or swelling.b. Internal: no discharges notedc. Cranial Nerve VIII: no hearing impairment of both ears
Nose: Symmetrical nares, no discharge, exudates, no bleeding nor swelling
noted. Mouth and Throat:
a. Mouth/Lips: dry & cracked, with swelling & sores on both lips and gums with minimal bleeding noted.
b. Tongue: no lesion and ulceration and able to take tongue out when instructed
c. Soft palate and uvula: no swelling on palate and uvulad. Throat: no sore throat noted
Neck:a. General: no difficulty with neck mobilityb. Blood vessels: slight distension of jugular vein is noted.c. Trachea: no masses noted, and no thyroid gland enlargement.
Integumentary: a. Skin: pale in color, with warm skin, petechial rashes on both palm of
the hands, with minute hematoma noted on joint areas on both upper and lower extremity,

b. Nails: short and clean; with capillary refill of 3 seconds, absence of clubbing and discoloration
c. Hair: with equal distribution of hairLymph Nodes
With slightly enlarged cervical lymph nodesChest/Back:
a. Respiration: with notable increase in respiratory rate, with slight difficulty in breathing
b. Lungs: Rales auscultated from both lung fields.c. Chest: with equal chest expansion, with equal anterioposterior
diameter, no abnormal retraction, circumference measuring 48 cm in width. Visible heart beat noted
d. Back: with minute hematoma at the back & prominent at shoulder blades
Cardiovascular: a. Heart: positive S1 and S2 sounds, no murmurb. Peripheral pulses: negative palpitations with normal rate
Gastrointestinal:a. Abdomen: with rigid abdomen; abdominal girth of 63 cm; no striae or
rashes noted, no protruding mass or discharge on the umbilicus, no ascites, normoactive bowel sounds, no rebound tenderness, no tenderness on kidneys and liver upon palpation.
Musculoskeletal:a. Upper Extremities: equal in size, symmetrical in shape with no evident
distension of veins, and equal pulses, no edema noted. Pale with petechial rashes on both palms of the hands and minute hematoma on joint areas.
b. Lower Extremities: equal in size, symmetrical in shape with no evident distension of veins, and equal pulses. With enlarged bleeding hematoma at the left foot measuring about 5-6cm in circumference with wound dressing.
October 22, 2008 ( during the Nurse-Patient Interaction )
General Survey
Seen patient sitting on bed, with IVF of D5 0.3 NaCl at 500 cc level infusing on his left
cephalic vein, interacts with other patient; with slight body malaise; increased respiratory
effort with minimal movement; needs minimal assistance to do ADL. He was wearing a
shirt and a pair of pajamas. With increased appetite (Patient observed drinking
chocolate drink, eating hotdogs biscuits, and sandwiches , swallowing them). Still with
increased water intake (4-5 1/2 cups of water within an hour). Vital signs taken as
follows:
Temp: 37.4°C RR: 44HR: 126

Physical assessment:Head and Face:
a. Hair: with fine short black hairb. Scalp: no evidence of dandruff or flaking; no tenderness of the scalp
noted.c. Skull: normal skull configuration, no abnormal elevation or depression.d. Face: symmetrical in shape, no tenderness upon palpation and no
crepitus heard while moving the jawEyes:
a. General: eyes are symmetrical, with noted hematoma periorbital edema (racoon-like eyes)
b. Pupils: black in color, with equal size approximately 2-3 mm, positive PERRLA
c. Eyebrows: equal distribution of hair on both sided. Eyelids and Eyelashes: no evidence of infection, no nodules and
tenderness noted, with minimal swelling of lower eyelid.e. Lacrimal puncta: no nodules and tenderness noted.f. Sclerae: whitish sclerae with evident capillaries, no jaundice noted.g. Conjunctiva: pale conjunctiva.h. Vision: with good visual acuity
Ears: a. External: symmetrical appearance of pinna, no lesions or abnormal
discharges or swelling.b. Internal: no discharges notedc. Cranial Nerve VIII: no hearing impairment of both ears
Nose: Symmetrical nares, no discharge, exudates, no bleeding nor swelling
noted. Mouth and Throat:
a. Mouth/Lips: dry & cracked, with swelling & sores on both lips and gums with no bleeding noted.
b. Tongue: no lesion and ulceration and able to take tongue out when instructed
c. Soft palate and uvula: no swelling on palate and uvulad. Throat: no sore throat noted
Neck:a. General: no difficulty with neck mobilityb. Blood vessels: slight distension of jugular vein is noted.c. Trachea: no masses noted, and no thyroid gland enlargement.
Integumentary: a. Skin: pale in color, with warm skin, petechial rashes on both palm of
the hands, with minute hematoma noted on joint areas on both upper and lower extremity
b. Nails: short and clean; with capillary refill of 3 seconds, absence of clubbing and discoloration
c. Hair: with equal distribution of hairLymph Nodes
With slightly enlarged cervical lymph nodesChest/Back:

a. Respiration: with notable increase in respiratory rate, with slight difficulty in breathing
b. Lungs: Rales auscultated from both lung fieldsc. Chest: with equal chest expansion, with equal anterioposterior
diameter, no abnormal retraction, circumference measuring 48 cm in width. Visible heart beat noted
d. Back: with minute hematoma at the back & prominent at shoulder blades
Cardiovascular: a. Heart: positive S1 and S2 sounds, no murmurb. Peripheral pulses: negative palpitations with normal rate
Gastrointestinal:a. Abdomen: with abdominal distention, abdominal girth of 64 cm; no
striae or rashes noted, no protruding mass or discharge on the umbilicus, no ascites, normoactive bowel sounds, no rebound tenderness, no tenderness on kidneys and liver upon palpation.
Musculoskeletal:a. Upper Extremities: equal in size, symmetrical in shape with no evident
distension of veins, and equal pulses, no edema noted. Pale with petechial rashes on both palms of the hands and minute hematoma on joint areas.
b. Lower Extremities: equal in size, symmetrical in shape with no evident distension of veins, and equal pulses. With enlarged bleeding hematoma at the left foot measuring about 6-7cm in circumference with wound dressing.
October 25, 2008 ( during the Nurse-Patient Interaction )
General Survey
Seen on bed, with Oxygen inhalation at 5-6Lpm, with IVF of Plain NSS 1 liter at 900 cc
level infusing on his left cephalic vein, with ongoing 1 unit of PRBC S#5914 as side drip,
(+) pallor, restless and irritable, barely know the people handling him including his
parents, generalized body weakness; with exertional breathing.
Physical assessment:Head and Face:
a. Hair: with fine short black hairb. Scalp: no evidence of dandruff or flaking; no tenderness of the scalp
noted.c. Skull: normal skull configuration, no abnormal elevation or depression.d. Face: symmetrical in shape, no tenderness upon palpation and no
crepitus heard while moving the jawEyes:
a. General: eyes are symmetrical, with noted hematoma periorbital edema (racoon-like eyes)
b. Pupils: black in color, PERRLA (not assessed)c. Eyebrows: equal distribution of hair on both side

d. Eyelids and Eyelashes: no evidence of infection, no nodules and tenderness noted, with minimal swelling of lower eyelid.
e. Lacrimal puncta: no nodules and tenderness noted.f. Sclerae: whitish sclerae with evident capillaries, no jaundice noted.g. Conjunctiva: pale conjunctiva.h. Vision: with good visual acuity
Ears: a. External: symmetrical appearance of pinna, no lesions or abnormal
discharges or swelling.b. Internal: no discharges notedc. Cranial Nerve VIII: no hearing impairment of both ears
Nose: Symmetrical nares, no discharge, exudates, no bleeding nor swelling
noted. Mouth and Throat:
a. Mouth/Lips: dry & cracked, with dried wound on both lips, with mild sores on oral cavity, with no bleeding noted.
b. Tongue: not assessedc. Soft palate and uvula: not assessedd. Throat: not assessed
Neck:a. General: no difficulty with neck mobilityb. Blood vessels: distended jugular vein.c. Trachea: no masses noted, and no thyroid gland enlargement.
Integumentary: a. Skin: pale in color, with warm skin, petechial rashes on both palm of
the hands, with minute hematoma noted on joint areas on both upper and lower extremity
b. Nails: short and clean; with capillary refill of 5-6 secondsc. Hair: with equal distribution of hair
Lymph NodesWith slightly enlarged cervical lymph nodes
Chest/Back:a. Respiration: with notable increase in respiratory rate, with slight
difficulty in breathingb. Lungs: Rales auscultated from both lung fields.c. Chest: with equal chest expansion, with equal anterioposterior
diameter, with labored breathing, circumference measuring 48 cm in width. Visible heart beat noted
d. Back: with minute hematoma at the back & prominent at shoulder blades
Cardiovascular: a. Heart: positive S1 and S2 sounds, no murmurb. Peripheral pulses: negative palpitations with normal rate
Gastrointestinal:a. Abdomen: with abdominal distention, abdominal girth of 72 cm
Musculoskeletal:

a. Upper Extremities: equal in size, symmetrical in shape with no evident distension of veins, and equal pulses, no edema noted. Pale with petechial rashes on both palms of the hands and minute hematoma on joint areas.
b. Lower Extremities: equal in size, symmetrical in shape with no evident distension of veins, and equal pulses. With enlarged bleeding hematoma at the left foot measuring about 6-7cm in circumference with wound dressing & elastic bandage.
III. ANATOMY & PHYSIOLOGY
The Bone Marrow
The Bone marrow is the soft, flexible, vascular tissue found in the hollow interior
cavities and cancellous bone spaces in the center of many bones and which is the
source of erythrocytes (red blood cells) and leukocytes (white blood cells).
There are two main types of bone marrow. Red bone marrow is the center of production
of all blood cells except one type of lymphocyte, which matures in the thymus. Yellow
bone marrow stores fats.
As the source of blood cells, the bone marrow is critical to the health of people. The
disruption of the intricate harmony, such as the production of too many, too few, or
abnormal blood cells, results in diseases, such as leukemia, that can be life-threatening.

Medical procedures have been developed to examine the bone marrow (bone marrow
aspiration and biopsy) of patients and also to transfer normal stem cells from a donor
into a recipient (bone marrow transplantation).
STRUCTURE
Red marrow consists primarily of a loose, soft network of blood vessels and protein
fibers interspersed with developing blood cells. The blood vessels are termed the
vascular component, and the protein fibers and developing blood cells collectively are
referred to as the stroma, or the extravascular component. The protein fibers crisscross
the marrow, forming a meshwork that supports the developing blood cells clustered in
the spaces between the fibers.
Red marrow contains a rich blood supply. Arteries transport blood containing oxygen
and nutrients into the marrow, and veins remove blood containing carbon dioxide and
other wastes. The arteries and veins are connected by capillaries, blood vessels that
branch throughout the marrow. In various places, the capillaries balloon out, forming
numerous thin, blood-filled cavities. These cavities are called sinusoids, and they assist
in blood-cell production.
Yellow marrow is so named because it is composed of yellow fat cells interspersed in a
rich mesh of connective tissue that also supports many blood vessels. While not usually
actively involved in blood formation, in an emergency yellow marrow is replaced by
blood-forming red marrow when the body needs more blood.

Gray's Anatomy illustration of cells in bone marrow. (From New World Encyclopedia)
FUNCTIONS
Red marrow produces all of the body’s blood cells—red blood cells, white blood cells,
and platelets. Red blood cells in the circulatory system transport oxygen to body tissues
and carbon dioxide away from tissues. White blood cells are critical for fighting bacteria
and other foreign invaders of the body. Platelets are essential for the formation of blood
clots to heal wounds.
Within red bone marrow, all blood cells originate from a single type of cell, called a
hematopoietic stem cell. Stimulated by hormones and growth factors, these stem cells
divide to produce immature, or progenitor blood cells. Most of these progenitor cells
remain in the stroma and rapidly undergo a series of cell divisions, producing either red
blood cells or white blood cells. At any one time, the stroma consists largely of
progenitor cells in various stages of development. At the appropriate developmental
stage, the fresh, new cells squeeze through the walls of the capillaries. From there, the
cells leave the bone and enter the body’s circulatory system. Some progenitor cells

migrate to the sinusoids, where they produce platelets, which also travel to the
circulatory system via the capillaries.
Although stem cells are relatively rare—about 1 in every 10,000 marrow cells is a stem
cell—they typically produce the forerunners of an estimated 2 million red cells per
second and 2 billion platelets per day. However, if significant amounts of blood are lost
or other conditions reduce the supply of oxygen to tissues, the kidneys secrete the
hormone erythropoietin. This hormone stimulates stem cells to produce more red blood
cells. To fight off infection, hormones collectively termed colony stimulating growth
factors are released by the immune system. These hormones stimulate the stem cells to
produce more infection-fighting white blood cells. And in severe cases, the body
converts yellow marrow into red marrow to help produce needed blood cells.
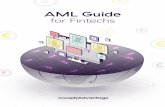
THE HEMATOPOIETIC SYSTEM
Hematology is the science of blood and blood forming tissues. It includes both
cellular and non-cellular blood components. Hematologic activities occur in many organs
of the body and have the potential for multiple forms of pathology. Blood itself is
composed of two elements – the liquid component, plasma, and the solid components,
which are mainly erythrocytes, leukocytes, and thrombocytes. These elements are
formed by hematopoiesis.
Hematopoiesis is the continuous, regulated formation of blood cells. There are
three primary functions of hematopoiesis.
1. Oxygen delivery
2. Hemostasis
3. Host defense

Note that some complexity is omitted from the diagram. Lymphocytes come from
"Lymphoid" line, whereas granulocytes, monocytes, megakaryocytes, and erythrocytes
come from "Myeloid" line. Among myeloid cells, granulocytes and monocytes have a
common precursor, "CFU-GM".
Hematopoiesis occurs in the bone marrow. The degree and location of bone
marrow activity varies depending on the age and health status of your patient. Within the
bone marrow there is a pluripotent stem cell. This stem cell is the “Mother Cell” or the
originator of all blood cells. It has the ability to self-renew and create progenitor stem cell
lines. They are naturally limited in number. By reviewing the chart above, you can see
that all cells come from the stem cell. An attack on the stem cell can theoretically affect
all of them similarly. A disease or agent that impacts erythroblasts could impact all the
cell type in that “line,” but not those in a different “line.”
The Blood

Blood is a liquid tissue. Suspended in the watery plasma are seven types of cells
and cell fragments. The Red Blood Cells (RBCs) or erythrocytes , Platelets or
thrombocytes, and five kinds of white blood cells (WBCs) or leukocytes. Three kinds of
granulocytes are as follows: Neutrophils, Eosinophils, Basophils. Two kinds of
leukocytes without granules in their cytoplasm are: Lymphocytes and Monocytes,
Functions of the BloodBlood performs two major functions: transport through the body of : oxygen and
carbon dioxide, food molecules (glucose, lipids, amino acids), ions (e.g., Na+, Ca2+,
HCO3−), wastes (e.g., urea), hormones, heat and defense of the body against infections
and other foreign materials. All the WBCs participate in these defenses.
Red Blood Cells (erythrocytes)
The most numerous type in the blood. Women average about 4.8 million of these
cells per cubic millimeter (mm3; which is the same as a microliter [µl]) of blood. Men
average about 5.4 x 106 per µl. These values can vary over quite a range depending on
such factors as health and altitude. (Peruvians living at 18,000 feet may have as many
as 8.3 x 106 RBCs per µl.) RBC precursors mature in the bone marrow closely attached
to a macrophage. They manufacture hemoglobin until it accounts for some 90% of the
dry weight of the cell. The nucleus is squeezed out of the cell and is ingested by the
macrophage. No-longer-needed proteins are expelled from the cell in vesicles called
exosomes. Thus RBCs are terminally differentiated; that is, they can never divide. They
live about 120 days and then are ingested by phagocytic cells in the liver and spleen.

Most of the iron in their hemoglobin is reclaimed for reuse. The remainder of the heme
portion of the molecule is degraded into bile pigments and excreted by the liver. Some 3
million RBCs die and are scavenged by the liver each second. Red blood cells are
responsible for the transport of oxygen and carbon dioxide.
Hemoglobin
Hemoglobin is a protein that is carried by red cells. It picks up oxygen in the lungs
and delivers it to the peripheral tissues to maintain the viability of cells. Hemoglobin is
made from two similar proteins that "stick together". Both proteins must be present for
the hemoglobin to pick up and release oxygen normally. One of the component proteins
is called alpha, the other is beta. Before birth, the beta protein is not expressed. A
hemoglobin protein found only during fetal development, called gamma, substitutes up
until birth.
In adult humans the hemoglobin (Hb) molecule consists of four polypeptides: two
alpha (α) chains of 141 amino acids and two beta (β) chains of 146 amino acid. Each of
these is attached the prosthetic group heme. There is one atom of iron at the center of
each heme. One molecule of oxygen can bind to each heme.
Like all proteins, the "blueprint" for hemoglobin exists in DNA (the material that
makes up genes). Normally, an individual has four genes that code for the alpha protein,
or alpha chain. Two other genes code for the beta chain. (Two additional genes code for
the gamma chain in the fetus). The alpha chain and the beta chain are made in precisely
equal amounts, despite the differing number of genes. The protein chains join in
developing red blood cells, and remain together for the life of the red cell.
Hemoglobin synthesis requires the coordinated production of heme and globin.
Heme is the prosthetic group that mediates reversible binding of oxygen by hemoglobin.
Globin is the protein that surrounds and protects the heme molecule.
Erythrocytes and Related Values
Red Blood Cell (RBC)Normal Range: 4.6-6.3 X106/mm3 (males)4.2 -5.4 X106/mm3 (females)

Erythrocytes, or red blood cells, originate from a stem cell. Vitamin B12, folic acid, iron,
and copper are essential in the formation of erythrocytes. Erythropoietin is released by
kidneys in response to hypoxemia which stimulates the bone marrow to produce red
blood cells. Typically, red blood cells live approximately 120 days. When the red blood
cells become old and damaged, the liver, spleen, and bone marrow cleanse them from
the blood.
Reticulocyte CountNormal Range: 0.5-2.5% of RBCsWhen released from the bone marrow red blood cells are slightly immature and are
known as reticulocytes. Reticulocytes mature into red blood cells within a few days.
HemoglobinNormal Range: 14-18 g/dL (males)12-16 g/dl (females)Hemoglobin is a protein-iron compound in red blood cell that carries oxygen. This
laboratory value is used to evaluate the oxygen-carrying capacity of the blood. Red
blood cells and hemoglobin go hand in hand. One unit of packed red blood cells
generally equals one whole number increase in your hemoglobin value. For example:
If your patient’s hemoglobin is 7.0 g/dl, and you give him one unit of packed red blood
cells, your patient’s hemoglobin should come up to 8.0 g/dl.
HematocritNormal Range: 42-52% (males)37-57% (females)Hematocrit is an expression of the total percentage of blood volume that is composed of
red blood cells. It is also known as the packed cell volume of your blood (Sherwood,
1997).
IronNormal Range: 50-150 mcg/dLAs mentioned earlier, iron is necessary for the formation of hemoglobin, an essential part
of the red blood cell. Iron is absorbed from the small intestine into the blood and binds

with transferrin. Transferrin transports iron tothe bone marrow where it is used to make
hemoglobin.
Total Iron Binding CapacityNormal Range: 250-410 mcg/dlThe amount of iron that can still bind with transferrin (to be transported to bone marrow
to make hemoglobin) is known as the total iron binding capacity or TIBC. Think of your
TIBC as the total amount of people that can get on a bus. The iron is the people and the
bus is transferrin. When your serum iron levels increase, your TIBC decreases. When
you serum iron levels decrease, then your TIBC increases.
FerritinNormal Range: 20 - 300 ng/mL (males)20 - 120 ng/mL (females)Ferritin is a protein that binds to iron. Most of the iron stored in the body is attached to
ferritin. Ferritin is found in the liver, spleen, and bone marrow. Only a small amount is
found in the blood. Like the TIBC, the amount of ferritin in the blood may help indicate
the amount of iron stored in your body.
White Blood Cell Count (WBC) and Differential
White blood cells, or leukocytes, are classified into two main groups:
granulocytes and nongranulocytes (also known as agranulocytes). The granulocytes,
which include neutrophils, eosinophils, and basophils, have granules in their cell
cytoplasm. Neutrophils, eosinophils, and basophils also have a multilobed nucleus. As a

result they are also called polymorphonuclear leukocytes or "polys." The nuclei of
neutrophils also appear to be segmented, so they may also be called segmented
neutrophils or "segs." The nongranuloctye white blood cells, lymphocytes and
monocytes, do not have granules and have nonlobular nuclei. They are sometimes
referred to as mononuclear leukocytes.
The lifespan of white blood cells ranges from 13 to 20 days, after which time they
are destroyed in the lymphatic system. When immature WBCs are first released from the
bone marrow into the peripheral blood, they are called "bands" or "stabs." Leukocytes
fight infection through a process known as phagocytosis. During phagocytosis, the
leukocytes surround and destroy foreign organisms. White blood cells also produce,
transport, and distribute antibodies as part of the body's immune response.
LeukocytesTotal WBCNormal Range: 5,000 -10,000/microliter
Leukocytes, or white blood cells, protect the body from bacteria and infection.
The white blood cell count is expressedas the number of leukocytes per microliter of
blood. The total WBC count increases in response to infection or trauma.
LymphocytesNormal Range: 16-46%
There are several kinds of lymphocytes (although they all look alike under the
microscope), each with different functions to perform . The most common types of
lymphocytes are B Lymphocytes ("B cells"). These are responsible for making
antibodies. T lymphocytes ("T cells"). There are several subsets of these: Inflammatory
T-cells that recruit macrophages and neutrophils to the site of infection or other tissue
damage. Cytotoxic T-Lymphocytes (CTLs) that kill virus-infected and, perhaps, tumor
cells. Helper T-cells that enhance the production of antibodies by B cells.
Although bone marrow is the ultimate source of lymphocytes, the lymphocytes
that will become T cells migrate from the bone marrow to the thymus where they mature.
Both B cells and T cells also take up residence in lymph nodes, the spleen and other
tissues where they encounter antigens; continue to divide by mitosis; mature into fully
functional cells. Lymphocytes mature in the lymph nodes. They live approximately 100-
300 days. The total lymphocyte count represents total T and B lymphocytes. T

lymphocytes are killer cells. They tell B lymphocytes to make antibodies. Lymphocytes
increase in viral illnesses, such as measles, mumps, chicken pox, influenza, viral
hepatitis, mononucleosis, and in acute transplant rejection.
MonocytesNormal Range: 0-12%
Monocytes leave the blood and become macrophages. Macrophages are large,
phagocytic cells that engulf foreign material (antigens) that enter the body dead and
dying cells of the body. They ingest cellular debris at the area of infection or
inflammation. They increase after several days of active infection or inflammation. They
are like your body’s garbage truck: they are a little slow, but they pick up all the
“garbage” or cellular debris and take it away.
NeutrophilsNormal Range: 40-70%
The most abundant of the WBCs. This photomicrograph shows a single
neutrophil surrounded by red blood cells. Neutrophils squeeze through the capillary walls
and into infected tissue where they kill the invaders (e.g., bacteria) and then engulf the
remnants by phagocytosis. This is a never-ending task, even in healthy people: Our
throat, nasal passages, and colon harbor vast numbers of bacteria. Most of these are
commensals, and do us no harm. But that is because neutrophils keep them in check.
However, heavy doses of radiation, chemotherapy, and many other forms of stress can
reduce the numbers of neutrophils so that formerly harmless bacteria begin to
proliferate. The resulting opportunistic infection can be life-threatening. Leukocyte types
are counted and expressed as a percentage. Neutrophils are the predominant type of
granulocytes. Neutrophils are special soldiers in your body’s immunity army. Their main
responsibility is to kill bacteria, destroy bacteria’s ability to reproduce, and destroy
bacteria’s ability to produce endotoxins.
BandsNormal Range: 0-8%
Neutrophil’s primal cell type is bands. Bands are adolescent neutrophils. It is
abnormal to have elevated bands in your blood stream. When the percent of bands is
increased you have a “shift to the left.” Historically, the diagram of the hematopoietic

system was read from left to right, not top to bottom as it does today. Thus, if you had an
increase in a cell type, moving left to the progenitor cell – you would have a shift to the
left.
EosinophilsNormal Range: 0-7%
The number of eosinophils in the blood is normally quite low (0–450/µl).
However, their numbers increase sharply in certain diseases, especially infections by
parasitic worms. Eosinophils are cytotoxic, releasing the contents of their granules on
the invader. Eosinophils are responsible for fighting parasites, and are increased in
allergic or autoimmune disorders. For example, eosinophils increase when a patient has
hives due to allergic reaction.
BasophilsNormal Range: 0-1%
The number of basophils also increases during infection. Basophils leave the
blood and accumulate at the site of infection or other inflammation. There they discharge
the contents of their granules, releasing a variety of mediators such as: histamine,
serotonin, prostaglandina and leukotrienes which increase the blood flow to the area and
in other ways add to the inflammatory process. The mediators released by basophils
also play an important part in some allergic responses such as hay fever and an
anaphylactic response to insect stings. Histamine and heparin and increase only in the
healing process.
Leukocytosis, a WBC above 10,000, is usually due to an increase in one of the
five types of white blood cells and is given the name of the cell that shows the primary
increase. Neutrophilic leukocytosis = neutrophilia, Lymphocytic leukocytosis =
lymphocytosis, Eosinophilic leukocytosis = eosinophilia, Monocytic leukocytosis =
monocytosis, Basophilic leukocytosis = basophilia.
PhysiologyIn response to an acute infection, trauma, or inflammation, white blood cells
release a substance called colony-stimulating factor (CSF). CSF stimulates the bone
marrow to increase white blood cell production. In a person with normally functioning
bone marrow, the numbers of white blood cells can double within hours if needed. An

increase in the number of circulating leukocytes is rarely due to an increase in all five
types of leukocytes. When this occurs, it is most often due to dehydration and
hemoconcentration. In some diseases, such as measles, pertussis and sepsis, the
increase in white blood cells is so dramatic that the picture resembles leukemia.
Leukemoid reaction, leukocytosis of a temporary nature, must be differentiated from
leukemia, where the leukocytosis is both permanent and progressive.
Therapy with steroids modifies the leukocytosis response. When corticosteroids
are given to healthy persons, the WBC count rises. However, when corticosteroids are
given to a person with a severe infection, the infection can spread significantly without
producing an expected WBC rise. An important concept to remember is that,
leukocytosis as a sign of infection can be masked in a patient taking corticosteroids.
Leukopenia occurs when the WBC falls below 4,000. Viral infections,
overwhelming bacterial infections, and bone marrow disorders can all cause leukopenia.
Patients with severe leukopenia should be protected from anything that interrupts skin
integrity, placing them at risk for an infection that they do not have enough white blood
cells to fight. For example, leukopenic patients should not have intramuscular injections,
rectal temperatures or enemas.
Leukocytes: critical low and high values
A WBC of less than 500 places the patient at risk for a fatal infection. A WBC
over 30,000 indicates massive infection or a serious disease such as leukemia. When a
patient is receiving chemotherapy that suppresses bone marrow production of
leukocytes, the point at which the count is lowest is referred to as the nadir.
Blood ClottingPlateletsNormal Range: 150,000 – 400,000/microliter
Platelets are cell fragments produced from megakaryocytes. Blood normally
contains 150,000–350,000 per microliter (µl) or cubic millimeter (mm3). This number is
normally maintained by a homeostatic (negative-feedback) mechanism. If this value
should drop much below 50,000/µl, there is a danger of uncontrolled bleeding because

of the essential role that platelets have in blood clotting. Some causes: certain drugs and
herbal remedies; autoimmunity.
When blood vessels are cut or damaged, the loss of blood from the system must
be stopped before shock and possible death occur. This is accomplished by solidification
of the blood, a process called coagulation or clotting. A blood clot consists of a plug of
platelets enmeshed in a network of insoluble fibrin molecules. Platelets are small,
colorless cells that have a lifespan of seven to ten days. They perform three major roles:
1) decreasing the luminal size of damaged vessels to decrease blood loss, 2) forming
blockages in injured vessels to decrease blood loss, and 3) with plasma providing the
correct ingredients needed to accelerate blood coagulation.
THE CLOTTING CASCADEThe end result of the clotting cascade is fibrin clots, fibrin, and thrombin. When
the clotting cascade is activated, usually due to vessel injury or damage, platelets are
one of the first responders. They stick to the damaged vessel and recruit more platelets
to the site. This aggregation of platelets forms a temporary plug that safeguards the
vessel wall from further bleeding. Simultaneously, additional proteins from the clotting
cascade are activated in a specific order that lead to the formation of fibrin. Fibrin is a
very sticky substance and acts as glue at the site, securing the platelet plug. Finally, the
clot must be dissolved in order for normal blood flow to resume following tissue repair.
The dissolution of the clot occurs through the action of plasmin. Plasmin is a protein that
is responsible for digesting fibrin. Eventually, scar tissue forms completing the healing of
the injured vessel (Sherwood, 1997).
PlasmaPlasma is a straw-colored, clear liquid that is ninety percent water. It is essential
for the transport of our blood components. Besides water, plasma also contains
dissolved electrolytes responsible for membrane excitability, plasma proteins that
maintain the osmotic distribution of fluid and substances capable of buffering pH

changes (Sherwood, 1997). Plasma transports materials needed by cells and materials
that must be removed from cells: various ions (Na+, Ca2+, HCO3−, etc.; glucose and
traces of other sugars; amino acids; other organic acids; cholesterol and other lipids;
hormones; urea and other wastes. Most of these materials are in transit from a place
where they are added to the blood (a "source") exchange organs like the intestine and
depots of materials like the liver to places ("sinks") where they will be removed from the
blood, every cell and exchange organs like the kidney, and skin.

IV. THE PATIENT AND HIS ILLNESS
A.PATHOPHYSIOLOGY (BOOK CENTERED)
Predisposing Factors: Race ( White race )Gender (Male)Age (increases with age)Heredity/Familial Tendency
Affectations in different committed cells
Mutant leukemia cells proliferate and fill the bone marrow
Compete and infiltrate hematopoeisis &
Precipitating Factors:Antecedent HematologicDisordersCongenital DisorderEnvironmental Exposures (high doses of radiation, chemicals like benzene, tobacco Smoke)Prior Exposure To Chemotherapeutic Agents For Another Malignancy
Disruption of pluripotent stem cells
Disruption of specific genes
Bone Pain

PetechiaeEcchymosis
Gingival bleedingepistaxis
Bleeding Tendencies
pallorAnemia
Wt. loss Malaise
Easy fatigability
Erythroblasts
Proliferation of immature
phagocytes
Decreased production of normal RBC
Megakaryoid Committed Cells
Megakaryoblast
Proliferation of immature
megakaryocytes
Myeloid Committed Cells
Myeloblasts
Proliferation of immature
myelocytes
Lymphoblasts
Proliferation of immature
lymphocytes
Affectations of B lymphocytes
& T-lymphocytes
Erythroid Committed Cells
Risk for infection
Affectations in different committed cells
Monoblasts
Proliferation of immature
monocytes
Lymphoid Committed Cells
Affectations in WBC cells components
NeutrophilsBasophils
Eosinophils
Inability to protect body against
invasion
Leukoblast

a. SYNTHESIS OF THE DISEASE
GENERAL DESCRIPTION
The underlying pathophysiology consists of a maturational arrest of bone marrow
cells in the earliest stages of development. The mechanism of this arrest is under study,
but in many cases, it involves the activation of abnormal genes through chromosomal
translocations and other genetic abnormalities. This developmental arrest results in 2
disease processes. First, the production of normal blood cells markedly decreases,
which results in varying degrees of anemia, thrombocytopenia, and neutropenia.
Second, the rapid proliferation of these cells, along with a reduction in their ability to
undergo programmed cell death (apoptosis), results in their accumulation in the bone
marrow, blood, and, frequently, the spleen and liver.
b. RISK FACTORS
PRE-DISPOSING FACTORS:
RACE - AML is more common in whites than in other populations.
SEX - AML is more common in men than in women. The difference is even more
apparent in older patients. Some have proposed that the increased prevalence of AML in
men may be related to occupational exposures.
AGE - Prevalence increases with age. The median age of onset is 65 years. However, this disease affects all age groups.
FAMILIAL TENDENCY - Germ-line mutations in the gene AML1 (RUNX1, CBFA2) occur
in the familial platelet disorder with predisposition for AML, an autosomal-dominant
disorder characterized by moderate thrombocytopenia, a defect in platelet function, and
propensity to develop AML. Some hereditary cancer syndromes, such as Li-Fraumeni
syndrome, can manifest as leukemia.
PRECIPITATING FACTORS:

ANTECEDENT HEMATOLOGIC DISORDERS - Unknown etiology that occurs most
often in older patients and manifests as progressive cytopenias that occur over months
to years. Other that predispose patients to AML include aplastic anemia, myelofibrosis,
paroxysmal nocturnal hemoglobinuria, and polycythemia vera.
CONGENITAL DISORDERS - Some congenital disorders that predispose patients to
AML include Bloom syndrome, Down syndrome, congenital neutropenia, Fanconi
anemia, and neurofibromatosis. More subtle genetic disorders, including polymorphisms
of enzymes that metabolize carcinogens, also predispose patients to AML.
ENVIRONMENTAL EXPOSURES -Several studies demonstrate a relationship between
radiation exposure and leukemia. Early radiologists (prior to appropriate shielding) were
found to have an increased likelihood of developing leukemia. Patients receiving
therapeutic irradiation for ankylosing spondylitis were at increased risk of leukemia.
Survivors of the atomic bomb explosions in Japan were at a markedly increased risk for
the development of leukemia. Persons who smoke have a small but statistically
significant (odds ratio, 1.5) increased risk of developing AML. In several studies, the risk
of AML was slightly increased in people who smoked compared with those who did not
smoke. Exposure to benzene is associated with aplastic anemia and pancytopenia.
These patients often develop AML. Many of these patients demonstrate M6 morphology.
PRIOR EXPOSURE TO CHEMOTHERAPEUTIC AGENTS FOR ANOTHER
MALIGNANCY - As more patients with cancer survive their primary malignancy and
more patients receive intensive chemotherapy (including bone marrow transplantation
[BMT]), the number of patients with AML increases because of exposure to
chemotherapeutic agents. Patients with a prior exposure to alkylating agents, with or
without radiation, often have a myelodysplastic phase prior to the development of AML.
The typical latency period between drug exposure and acute leukemia is approximately
3-5 years for alkylating agents/radiation exposure but only 9-12 months for
topoisomerase inhibitors.
C. SIGNS AND SYMPTOMS WITH RATIONALE
1. Anemia, Neutropenia, and Thrombocytopenia – These are due to bone marrow
failure. It results from the fact that as leukemic clone of cells grows, it tends to displace

development of normal blood cells in the bone marrow. There is also decreased
neutrophil levels despite an increased total WBC count.
2. Physical signs of anemia, including pallor and a cardiac flow murmur, are frequently
present – These are due to the increased number of white blood cells displacing or
otherwise interfering with the production of normal blood cells in the bone marrow. The
most common symptom of anemia is fatigue. Patients often retrospectively note a
decreased energy level over past weeks. Other symptoms of anemia include dyspnea
upon exertion, dizziness, and, in patients with coronary artery disease, anginal chest
pain. Myocardial infarction may be the first presenting symptom of acute leukemia in an
older patient.
3.Fever and other signs of infection can occur, including lung findings of pneumonia –
These are due to the lack of normal white blood cell production that makes the patient
susceptible to infections, while the leukemic cells are derived from white blood cell
precursors, they have no infection-fighting capacity. Patients present with fever, which
may occur with or without specific documentation of an infection. Patients with the lowest
absolute neutrophil counts (ie, <500 cells/µL and especially <100 cells/µL) have the
highest risk of infection. Patients also often have a history of upper respiratory infection
symptoms that have not improved despite empiric treatment with oral antibiotics.
4. Abnormal Bleeding ( nosebleeds, gingival bleeding, purpura, ecchymosis, petechiae
–These are due to thrombocytopenia. Patients usually demonstrate petechiae,
particularly on the lower extremities. Petechiae are small, often punctate, hemorrhagic
rashes that are not palpable. Areas of dermal bleeding or bruises (ie, ecchymoses) that
are large or present in several areas may indicate a coexistent coagulation disorder such
as DIC. Purpura is characterized by flat bruises that are larger than petechiae but
smaller than ecchymoses. Potentially life-threatening sites of bleeding include the lungs,
gastrointestinal tract, and the central nervous system.
5. Signs relating to organ infiltration with leukemic cells – The most common sites
of infiltration include the spleen, liver, and gums. These include hepatosplenomegaly
and, to a lesser degree, lymphadenopathy Patients with splenomegaly note fullness in
the left upper quadrant and early satiety. . Occasionally, patients have skin rashes due

to infiltration of the skin with leukemic cells (leukemia cutis). Chloromata are
extramedullary deposits of leukemia. Rarely, a bony or soft-tissue chloroma (solid
leukenic mass or tumor outside of the bone marrow) may precede the development of
marrow infiltration by AML (granulocytic sarcoma).
6. Bone Pain - Patients with a high leukemic cell burden may present this symptom
which is caused by increased pressure in the bone marrow.
7. Signs relating to leukostasis - Patients with markedly elevated WBC counts
(>100,000 cells/µL) can present with symptoms of leukostasis (ie, respiratory distress
and altered mental status). Leukostasis is a medical emergency that requires immediate
intervention.

B. PATHOPHYSIOLOGY (CLIENT-CENTERED)
Predisposing Factors:
Gender (Male)Age (3 years old)
Mutant leukemia cells proliferate and fill the bone marrow
Compete and infiltrate hematopoeisis &
Disruption of pluripotent stem cells
Disruption of specific genes
Precipitating Factors:
Environmental Exposures- Cigarette Smoke- Exposure to certain chemicals (carbonated drinks even before reaching 1-yr of age/ foul-smelling env’t cause by nearby poultry)

• Petechiae* (both palms of the hand)
• Ecchymosis*
• Gingival bleeding*
• Epistaxis (upon admission)
• Hematoma* -Periorbital -in the sole of left foot measuring 6-7 cm diameter
Bleeding Tendencies
Affectations in different committed cells
Erythroblasts
Proliferation of immature
phagocytes
Decreased production of normal RBC
Megakaryoid Committed Cells
Megakaryoblast
Proliferation of immature
megakaryocytes
Myeloid Committed Cells
Myeloblasts
Proliferation of immature
myelocytes
Erythroid Committed Cells
Affectations in different committed cells
Monoblasts
Proliferation of immature
monocytes
Affectations in WBC cells
components
Neutrophils
Lymphocytes
Presence of Blast Cells
Inability to protect body
against invasion
(10-/7/8/14-19-08)
(10-7/8/12/14-19-08)
(10-7/8/12/14-19-08)
10- 3/7/8/12/14/15/17/18/19-08
INFECTION
Signs of infection
• On & off Fever
(10-3/12/13/17/18/19/25- 08)
• Acute
• Organ
Infiltration(distend- ed abdo-
men)
• Leuko-Stasis
• Altered Mental Status
• R

a. SYNTHESIS OF THE DISEASE (CLIENT BASED)
GENERAL DESCRIPTION
The underlying pathophysiology consists of a maturational arrest of bone marrow
cells in the earliest stages of development. This developmental arrest results in 2
disease processes. First, the production of normal blood cells markedly decreases,
which results in varying degrees of anemia, thrombocytopenia, and neutropenia.
Second, the rapid proliferation of these cells, along with a reduction in their ability to
undergo programmed cell death (apoptosis), results in their accumulation in the bone
marrow, blood, and, frequently, the spleen and liver. In AML, the bone
b. RISK FACTORS
PRE-DISPOSING FACTORS:
SEX - AML is more common in men than in women. The difference is even more
apparent in older patients.
AGE- Prevalence increases with age. The median age of onset is 65 years. However,
this disease affects all age groups.
PRECIPITATING FACTORS:
ENVIRONMENTAL EXPOSURES - In several studies, the risk of AML was slightly
increased in people who smoked compared with those who did not smoke.
C. SIGNS AND SYMPTOMS WITH RATIONALE
Pallor*
Malaise/ Fatigue*
(10-7/8/12/14-19-08)
Dyspnea ( RR, PR)(10-3/4/5/6/16/18/25-08)
Anemia*
DEATH

1. Anemia, Neutropenia, and Thrombocytopenia – These are due to bone marrow
failure. It results from the fact that as leukemic clone of cells grows, it tends to displace
development of normal blood cells in the bone marrow. There is also decreased
neutrophil levels despite an increased total WBC count.
2. Physical signs of anemia- including pallor and dyspnea upon exertion.These are
due to the increased number of white blood cells displacing or otherwise interfering with
the production of normal blood cells in the bone marrow. The most common symptom of
anemia is fatigue.
3. Fever and other signs of infection Patients present with fever, which may occur
with or without specific documentation of an infection. These are due to the lack of
normal white blood cell production that makes the patient susceptible to infections, while
the leukemic cells are derived from white blood cell precursors, they have no infection-
fighting capacity.
4. Abnormal Bleeding ( nosebleeds, gingival bleeding, purpura, ecchymosis, petechiae
–These are due to thrombocytopenia.
5. Signs relating to organ infiltration with leukemic cells – The most common sites
of infiltration include the spleen, liver, and gums. These include hepatosplenomegaly
and, to a lesser degree, lymphadenopathy.
6. Bone Pain - Patients with a high leukemic cell burden may present this symptom
which is caused by increased pressure in the bone marrow.
7. Signs relating to leukostasis - Patients with markedly elevated WBC counts
(>100,000 cells/µL) can present with symptoms of leukostasis (ie, respiratory distress
and altered mental status). Leukostasis is a medical emergency that requires immediate
intervention.