6.2Exclusion Criteria - TransCelerate - Pharmaceutical ... · Web viewFor studies of...
31
Common Protocol Template Patient Library v2.0 Common Protocol Template Patient Library v2.0 Section in Common Protocol Template (CPT) V1.0 Library Content 6.2. Exclusion Criteria Exclusion Criteria 8.1 Discontinuation of Study Treatment Error: Reference source not found QTc Stopping Criteria Appendix 7: Liver Safety: Suggested Actions and Follow-up Assessments [and Study Treatment Rechallenge Guidelines] Liver Safety: Suggested Actions and Follow-up Assessments [and Study Treatment Rechallenge Guidelines] 6.2 Exclusion Criteria MEDICAL CONDITIONS 1. Symptomatic herpes zoster within 3 months prior to screening 2. Evidence of active or latent tuberculosis (TB) as documented by medical history and examination, chest x-rays (posterior anterior and lateral), and TB testing: either a positive tuberculin skin test (TST; defined as a skin induration <5 mm at 48 to 72 hours, regardless of Bacillus Calmette-Guerin (BCG) or other vaccination history) or a positive (not indeterminate) QuantiFERON®-TB Gold test. NOTE: The choice to perform a TST or a QuantiFERON- TB Gold test will be made by the investigator according to local licensing and standard of care. The QuantiFERON-TB Gold test can only be used in countries where it is licensed, and the use of this test is dependent on previous treatment(s). This test may not be suitable if previous treatment(s) © 2015 TransCelerate BioPharma 1
Transcript of 6.2Exclusion Criteria - TransCelerate - Pharmaceutical ... · Web viewFor studies of...

Common Protocol Template Patient Library v2.0
Common Protocol Template Patient Library v2.0
Section in Common Protocol Template (CPT) V1.0 Library Content
6.2. Exclusion Criteria Exclusion Criteria
8.1 Discontinuation of Study Treatment Error: Reference source not found
QTc Stopping Criteria
Appendix 7: Liver Safety: Suggested Actions and Follow-up Assessments [and Study Treatment Rechallenge Guidelines]
Liver Safety: Suggested Actions and Follow-up Assessments [and Study Treatment Rechallenge Guidelines]
6.2 Exclusion CriteriaMEDICAL CONDITIONS
1. Symptomatic herpes zoster within 3 months prior to screening
2. Evidence of active or latent tuberculosis (TB) as documented by medical history and examination, chest x-rays (posterior anterior and lateral), and TB testing: either a positive tuberculin skin test (TST; defined as a skin induration <5 mm at 48 to 72 hours, regardless of Bacillus Calmette-Guerin (BCG) or other vaccination history) or a positive (not indeterminate) QuantiFERON®-TB Gold test.
NOTE: The choice to perform a TST or a QuantiFERON-TB Gold test will be made by the investigator according to local licensing and standard of care. The QuantiFERON-TB Gold test can only be used in countries where it is licensed, and the use of this test is dependent on previous treatment(s). This test may not be suitable if previous treatment(s) produced significant immunosuppression.
3. Significant allergies to humanized monoclonal antibodies
4. Clinically significant multiple or severe drug allergies, intolerance to topical corticosteroids, or severe post-treatment hypersensitivity reactions (including, but not limited to, erythema multiforme major, linear immunoglobulin A (IgA) dermatosis, toxic epidermal necrolysis, and exfoliative dermatitis)
5. Lymphoma, leukemia, or any malignancy within the past 5 years except for basal cell or squamous epithelial carcinomas of the skin that have been resected with no evidence of metastatic disease for 3 years
6. Breast cancer within the past 10 years
7. Abnormalities in lumbar spine previously known or determined by a screening
© 2015 TransCelerate BioPharma 1

Common Protocol Template Patient Library v2.0
lumbar x-ray (if conducted)
8. History of clinically significant back pain, back pathology, and/or back injury (eg, degenerative disease, spinal deformity or spinal surgery) that may predispose participant to complications or technical difficulty with lumbar puncture
9. Evidence or history of significant active bleeding or coagulation disorder or use of non-steroidal anti-inflammatory drugs or other drugs that affect coagulation or platelet function within 14 days prior to lumbar catheter insertion
10. Allergy to lidocaine (Xylocaine®) or its derivatives
11. Medical or surgical conditions for which lumbar puncture is contraindicated
<Start of common text for Phase I studies>
12. ALT and bilirubin >1.5xULN (isolated bilirubin >1.5xULN is acceptable if bilirubin is fractionated and direct bilirubin <35%)
13. Current or chronic history of liver disease or known hepatic or biliary abnormalities (with the exception of Gilbert's syndrome or asymptomatic gallstones)
<End of common text for Phase I studies>
<Start of common text for Phase II studies>
12. ALT >2xULN and bilirubin >1.5xULN (isolated bilirubin >1.5xULN is acceptable if bilirubin is fractionated and direct bilirubin <35%)
13. Current or chronic history of liver disease, or known hepatic or biliary abnormalities (with the exception of Gilbert's syndrome or asymptomatic gallstones)
<End of common text for Phase II studies>
<Start of common text for Phase III studies>
12. ALT >2xULN and bilirubin >1.5xULN (isolated bilirubin >1.5xULN is acceptable if bilirubin is fractionated and direct bilirubin <35%)
13. Current active liver or biliary disease (with the exception of Gilbert’s syndrome or asymptomatic gallstones or otherwise stable chronic liver disease per investigator assessment).
NOTES:
Stable chronic liver disease should be defined by the absence of ascites, encephalopathy, coagulopathy, hypoalbuminemia, esophageal or gastric varices, persistent jaundice, and cirrhosis.
Chronic stable hepatitis B or C (eg, presence of hepatitis B surface antigen [HBsAg] or positive hepatitis C antibody test result at screening or within 3 months prior to starting study treatment) is acceptable if the participant otherwise meets entry criteria
© 2015 TransCelerate BioPharma 2

Common Protocol Template Patient Library v2.0
<End of common text for Phase III studies>
<Start of common text>
14. [QTc >450 msec for male participants] [or QTc >470 for female participants] or QTc > 480 msec in participants with bundle branch block
NOTES:
The QTc is the QT interval corrected for heart rate according to Bazett’s formula (QTcB), Fridericia’s formula (QTcF), and/or another method, machine-read or manually over-read.
The specific formula that will be used to determine eligibility and discontinuation for an individual participant should be determined prior to initiation of the study. In other words, several different formulas cannot be used to calculate the QTc for an individual participant and then the lowest QTc value used to include or discontinue the participant from the trial.
<End of common text>
PRIOR/CONCOMITANT THERAPY
15. [Past or] intended use of over-the-counter or prescription medication [including herbal medications] within [X] days prior to dosing. [Specific medications listed in Section 7.7 may be allowed.]
16. Live vaccine(s) within 1 month prior to screening, or plans to receive such vaccines during the study.
17. Treatment with biologic agents (such as monoclonal antibodies including marketed drugs) within 3 months or 5 half-lives (whichever is longer) prior to dosing.
PRIOR/CONCURRENT CLINICAL TRIAL EXPERIENCE
18. Participation in the study would result in donation of blood or blood products in excess of [X] mL within [X].
19. Exposure to more than 4 new chemical entities within 12 months prior to the first dosing day
20. Current enrollment or past participation within the last [X] days before [signing of consent] in [this or] any other clinical study involving an investigational study treatment or any other type of medical research
© 2015 TransCelerate BioPharma 3

Common Protocol Template Patient Library v2.0
DIAGNOSTIC ASSESSMENTS
21. Positive HIV antibody test
<Start of common text for Phase I or II studies>
22. Presence of hepatitis B surface antigen (HBsAg) or positive hepatitis C antibody test result at screening or within 3 months prior to starting study treatment. For potent immunosuppressive agents, presence of the hepatitis B core antibody (HBcAb) should also lead to exclusion from the study.
<End of common text for Phase I or II studies>
OTHER EXCLUSIONS
29. Regular alcohol consumption within [X] months prior to the study defined as:
For UK sites: An average weekly intake of >21 units for males or >14 units for females. One unit is equivalent to 8 g of alcohol: a half-pint (~240 mL) of beer, 1 glass (125 mL) of wine, or 1 measure (25 mL) of spirits.
For US sites: An average weekly intake of >14 drinks for males or >7 drinks for females. One drink is equivalent to 12 g of alcohol: 12 ounces (360 mL) of beer, 5 ounces (150 mL) of wine, or 1.5 ounces (45 mL) of 80 proof distilled spirits.
30. Sensitivity to heparin or heparin-induced thrombocytopenia
31. Sensitivity to any of the study treatments, or components thereof, or drug or other allergy that, in the opinion of the investigator [or Medical Monitor], contraindicates participation in the study.
© 2015 TransCelerate BioPharma 4

Continue Study Treatment
Discontinue Study Treatment
*INR value not applicable to participants on anticoagulants
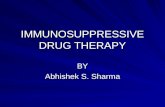
ALT ≥ 3xULN
No
Yes
Must refer to
Liver Safety Required Actions and Follow up Assessments section in the Appendix
Report as an SAE if possible Hy’s Law case: ALT≥3xULN and Bilirubin ≥2xULN (>35% direct) Or INR>1.5, if measured*
Common Protocol Template Patient Library v2.0
8.1 Discontinuation of Study Treatment Liver Function Stopping Criteria<Start of common text>
Study treatment will be discontinued for a participant if liver function stopping criteria are met.
Phase I Liver Function Stopping Algorithm
Liver Safety: Suggested Actions and Follow-up Assessments can be found in Appendix [X].
<End of common text>
© 2015 TransCelerate BioPharma 5

Common Protocol Template Patient Library v2.0
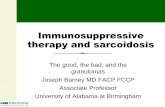
<Start of common text for Phase II studies>
Phase II Liver Function Stopping Criteria and Increased Monitoring Algorithm
Continue Study Treatment
Discontinue Study Treatment
PlusBilirubin≥2xULN (>35%
direct) or plus
INR>1.5, if measured*PossibleHy’s Law
ALT≥3xULN ALT≥5xULN
ALT≥3xULNPlus
Symptoms of liver injury
or hypersensitivity
ALT≥3xULNbut able to monitor
weekly for 4 weeks
No
Yes
YesYes Yes
No No No
No
Yes
ALT≥3xULNpersist for4 weeks or stopping criteria
met
Yes
No
*INR value not applicable to subjects on anticoagulants
Yes
If subject to be monitored weekly must refer to Liver Safety Required Actions and Follow up Assessments section in the Appendix
Must refer to Liver Safety Required Actions and Follow up Assessments section in the Appendix
Report as an SAE if possible Hy’s Law case: ALT≥3xULN and Bilirubin≥2xULN (>35% direct) or INR>1.5, if measured*
Liver Safety: Suggested Actions and Follow-up Assessments can be found in Appendix [X].
<End of common text for Phase II studies>
© 2015 TransCelerate BioPharma 6

Common Protocol Template Patient Library v2.0
<Start of common text for Phase III-IV studies>
Phase III-IV Liver Function Stopping Criteria and Increased Monitoring Algorithm
Continue Study Treatment
Discontinue Study Treatment
Plus Bilirubin≥2xULN (>35%
direct) or plusINR>1.5, if measured*Possible Hy’s Law
ALT≥3xULNALT
≥8xULN
PlusSymptoms of
liver injuryor
hypersensitivity
No
Yes
YesYes
No No No
See algorithm for continued therapy with
increased liver chemistry monitoring
Yes
*INR value not applicable to subjects on anticoagulants
ALT ≥3xULN
but <8xULN
Yes
Must refer to Liver Safety Required Actions and Follow up Assessments section in the Appendix
Report as an SAE if possible Hy’s Law case: ALT≥3xULN and Bilirubin≥2xULN (>35% direct) or INR>1.5, if measured*
Liver Safety: Suggested Actions and Follow-up Assessments can be found in Appendix [X].
© 2015 TransCelerate BioPharma 7

Common Protocol Template Patient Library v2.0
Phase III-IV Liver Function Increased Monitoring Algorithm with Continued Therapy for Participants with ALT 3xULN but <8xULN
Continue Study Treatment and Monitor Liver Chemistry
Discontinue Study Treatment
ALT≥5xULN but <8xULN
+ bili <2xULN +no symptoms
No
Must refer to Liver Safety Required Actions and Follow up Assessments section in the Appendix
Yes
ALT ≥3xULN but <5xULN
+ bili <2xULN +no symptoms
Able to monitor weekly for ≥2 weeks
Persists for ≥2 weeks or other stopping criteria
met
No
YesYes
Yes
NoNo
Able to monitor weekly for ≥4 weeks
Persists for ≥4 weeks or other stopping criteria
met
NoYes Yes Yes Yes
ALT ≥5xULN ALT <5xULN Yes Yes
*INR value not applicable to subjects on anticoagulants
Must refer to Liver Safety Required Actions and Follow up Assessments section in the Appendix
Report as an SAE if possible Hy’s Law case: ALT≥3xULN and Bilirubin≥2xULN (>35% direct) or INR>1.5, if measured*
Liver Safety: Suggested Actions and Follow-up Assessments can be found in Appendix [X].
<End of common text for Phase III-IV studies>
© 2015 TransCelerate BioPharma 8

Common Protocol Template Patient Library v2.0
QTc Stopping Criteria<Start of common text for Phase 1-IV studies iin patients>
A participant who meets [the OR either] bulleted criterion based on the average of triplicate ECG readings will be withdrawn from the study.
QTc >500 msec OR Uncorrected QT >600 msec
[Change from baseline of QTc >60 msec]
Baseline QTc with Bundle Branch Block Discontinuation QTc Threshold with Bundle Branch Block
< 450 msec > 500 msec
450 to 480 msec ≥ 530 msec
<End of common text for Phase I-IV studies in patients>
© 2015 TransCelerate BioPharma 9

Common Protocol Template Patient Library v2.0
Appendix 7: Liver Safety: Suggested Actions and Follow-up Assessments [and Study Treatment Rechallenge Guidelines]
<Start of common text for Phase I studies >
Phase I liver function stopping criteria are designed to assure participant safety and to evaluate liver event etiology.
Phase I Liver Function Stopping Criteria and Follow-Up Assessments
Liver Chemistry Stopping Criteria – Liver Stopping Event
ALT-absoluteALT≥3xULNIf ALT≥3xULN AND bilirubin 2xULN (>35% direct bilirubin) or INR >1.5, Report as an SAE.1,2
See additional Actions and Follow Up Assessments listed below
Suggested Actions and Follow up Assessments following Liver Stopping Event
Actions Follow Up Assessments
Immediately discontinue study treatment. Report the event to the [sponsor] within 24
hours Complete the liver event CRF, and complete an
SAE data collection tool if the event also met the criteria for an SAE.2
Perform liver function follow-up assessments. Monitor the participant until liver function test
abnormalities resolve, stabilize, or return to baseline (see MONITORING).
Do not restart/rechallenge participant with study treatment unless allowed per protocol and [sponsor] approval is granted.
If restart/rechallenge is either not allowed per protocol or not granted, permanently discontinue study treatment. The participant may continue in the study for any protocol-specified follow-up assessments
MONITORING: Repeat liver function tests (include ALT, AST,
alkaline phosphatase, bilirubin) and perform liver function follow-up assessments within 24 hrs.
Monitor participant twice weekly until liver
Blood sample for pharmacokinetic (PK) analysis obtained [insert time interval recommended by clinical pharmacokinetics representative] after the most recent dose4
Serum creatine phosphokinase (CPK) and lactate dehydrogenase (LDH)
Fractionate bilirubin, if total bilirubin 2xULN
Complete blood count with differential to assess eosinophilia
Record the appearance or worsening of clinical symptoms of liver injury, or hypersensitivity, on the AE report form
Record use of concomitant medications (including acetaminophen, herbal remedies, and other over-the-counter medications) on the concomitant medications report form.
Record alcohol use on the liver event alcohol intake CRF
© 2015 TransCelerate BioPharma 10

Common Protocol Template Patient Library v2.0
function test abnormalities resolve, stabilize or return to baseline.
A specialist or hepatology consultation is recommended.
If ALT ≥3xULN AND bilirubin <2xULN and INR ≤1.5: Repeat liver function tests (include ALT, AST,
alkaline phosphatase, bilirubin) and perform liver function follow-up assessments within 24 to 72 hours.
Monitor participants weekly until liver function abnormalities resolve, stabilize, or return to baseline.
If ALT≥3xULN AND bilirubin 2xULN or INR >1.5: Anti-nuclear antibody, anti-smooth
muscle antibody, Type 1 anti-liver kidney microsomal antibodies, and quantitative total immunoglobulin G (IgG) or gamma globulins.
Serum acetaminophen adduct HPLC assay (quantifies potential acetaminophen contribution to liver injury in participants with definite or likely acetaminophen use in the preceding week [James, 2009].) NOTE: Not required in China.
Liver imaging (ultrasound, magnetic resonance, or computerizsed tomography) andor liver biopsy to evaluate liver disease; complete Liver Imaging and/or Liver Biopsy CRFs.
1. Serum bilirubin fractionation should be performed if testing is available. If serum bilirubin fractionation is not immediately available, discontinue study treatment if ALT 3xULN and bilirubin 2xULN. Additionally, if serum bilirubin fractionation testing is unavailable, record the absence/presence of detectable urinary bilirubin on dipstick which is indicative of direct bilirubin elevations suggesting liver injury.
2. All events of ALT 3xULN and bilirubin 2xULN (>35% direct bilirubin) or ALT 3xULN and INR >1.5 may indicate severe liver injury (possible ‘Hy’s Law’) and must be reported as an SAE (excluding studies of hepatic impairment or cirrhosis). The INR measurement is not required and the stated threshold value will not apply to participants receiving anticoagulants.
3. Hepatitis A IgM antibody; hepatitis B surface antigen and hepatitis B Core Antibody (HBcAb); hepatitis C RNA; cytomegalovirus IgM antibody; Epstein-Barr viral capsid antigen IgM antibody (or if unavailable, heterophile antibody or monospot testing); and hepatitis E IgM antibody.
4. PK sample may not be required for participants known to be receiving placebo or non-comparator treatments. Record the date/time of the PK blood sample draw and the date/time of the last dose of study treatment prior to the blood sample draw on the CRF. If the date or time of the last dose is unclear, provide the participant’s best approximation. If the date/time of the last dose cannot be approximated OR a PK sample cannot be collected in the time period indicated above, do not obtain a PK sample. Instructions for sample handling and shipping are in the [Study Reference Manual].
References: James LP, Letzig L, Simpson PM, Capparelli E, Roberts DW, Hinson JA, Davern TJ, Lee WM. Pharmacokinetics of Acetaminophen-Adduct in Adults with Acetaminophen Overdose and Acute Liver Failure. Drug Metab Dispos 2009; 37:1779-1784.
<End of common text for Phase I studies >
© 2015 TransCelerate BioPharma 11

Common Protocol Template Patient Library v2.0
<Start of common wording for
Phase II liver function stopping criteria are designed to assure participant safety and to evaluate liver event etiology.
Phase II Liver Function Stopping Criteria and Follow-Up Assessments
Liver Function Stopping Criteria
ALT-absolute ALT 5xULN
ALT Increase ALT 3xULN persists for 4 weeks
Bilirubin1, 2 ALT 3xULN and bilirubin 2xULN (>35% direct bilirubin)
INR2 ALT 3xULN and INR >1.5, if INR measured
Cannot Monitor
ALT 3xULN and cannot be monitored weekly for 4 weeks
Symptomatic3 ALT 3xULN associated with symptoms (new or worsening) believed to be related to liver injury or hypersensitivity
Suggested Actions and Follow-up Assessments following ANY Liver Function Event that Requires Study Treatment Discontinuation
Actions Follow-Up Assessments
Immediately discontinue study treatment. Report the event to the [sponsor] within 24
hours. Complete the liver event CRF, and complete
an SAE data collection tool if the event also met the criteria for an SAE.2
Perform liver function follow-up assessments. Monitor the participant until liver function test
abnormalities resolve, stabilize, or return to baseline (see MONITORING).
Do not restart/rechallenge participant with study treatment unless allowed per protocol and [sponsor] Medical Governance approval is granted)
If restart/rechallenge not allowed per protocol or not granted, permanently discontinue study treatment and may continue participant in the study for any protocol specified follow up assessments
Viral hepatitis serology4
Blood sample for pharmacokinetic (PK) analysis obtained [insert time interval recommended by clinical pharmacokinetics representative] after the most recent dose5.
Serum creatine phosphokinase (CPK) and lactate dehydrogenase (LDH)
Fractionate bilirubin, if total bilirubin 2xULN
Complete blood count with differential to assess eosinophilia
Record the appearance or worsening of clinical symptoms of liver injury, or hypersensitivity, on the AE report form
Record use of concomitant medications (including acetaminophen, herbal remedies, and other over-the-counter medications) on the concomitant medications report
© 2015 TransCelerate BioPharma 12

Common Protocol Template Patient Library v2.0
MONITORING:For bilirubin or INR criteria: Repeat liver function tests (include ALT,
AST, alkaline phosphatase, bilirubin) and perform liver function follow-up assessments within 24 hrs.
Monitor participant twice weekly until liver function test abnormalities resolve, stabilize or return to baseline.
A specialist or hepatology consultation is recommended.
For All other criteria: Repeat liver function tests (include ALT,
AST, alkaline phosphatase, bilirubin) and perform liver function follow-up assessments within 24 to 72 hours.
Monitor participants weekly until liver function abnormalities resolve, stabilize, or return to baseline.
form. Record alcohol use on the liver event
alcohol intake CRF
For bilirubin or INR criteria: Anti-nuclear antibody, anti-smooth
muscle antibody, Type 1 anti-liver kidney microsomal antibodies, and quantitative total immunoglobulin G (IgG) or gamma globulins.
Serum acetaminophen adduct HPLC assay (quantifies potential acetaminophen contribution to liver injury in participants with definite or likely acetaminophen use in the preceding week [James, 2009].)NOTE: Not required in China.
Liver imaging (ultrasound, magnetic resonance, or computerized tomography) and/or liver biopsy to evaluate liver disease; complete Liver Imaging and/or Liver Biopsy CRFs.
1. Serum bilirubin fractionation should be performed if testing is available. If serum bilirubin fractionation is not immediately available, discontinue study treatment if ALT 3xULN and bilirubin 2xULN. Additionally, if serum bilirubin fractionation testing is unavailable, record the absence/presence of detectable urinary bilirubin on dipstick which is indicative of direct bilirubin elevations suggesting liver injury.
2. All events of ALT 3xULN and bilirubin 2xULN (>35% direct bilirubin) or ALT 3xULN and INR >1.5 may indicate severe liver injury (possible ‘Hy’s Law’) and must be reported as an SAE (excluding studies of hepatic impairment or cirrhosis). The INR measurement is not required and the stated threshold value will not apply to participants receiving anticoagulants.
3. New or worsening symptoms believed to be related to liver injury (such as fatigue, nausea, vomiting, right upper quadrant pain or tenderness, or jaundice) or hypersensitivity (such as fever, rash or eosinophilia).
4. Includes:Hepatitis A IgM antibody; hepatitis B surface antigen and hepatitis B Core Antibody (HBcAb); hepatitis C RNA; cytomegalovirus IgM antibody; Epstein-Barr viral capsid antigen IgM antibody (or if unavailable, heterophile antibody or monospot testing); and hepatitis E IgM antibody.
5. PK sample may not be required for participants known to be receiving placebo or non-comparator treatments. Record the date/time of the PK blood sample draw and the date/time of the last dose of study treatment prior to the blood sample draw on the CRF. If the date or time of the last dose is unclear, provide the participant’s best approximation. If the date/time of the last dose cannot be approximated OR a PK sample cannot be collected in the time period indicated above, do not obtain a PK sample. Instructions for sample handling and shipping are in the [Study Reference Manual].
© 2015 TransCelerate BioPharma 13

Common Protocol Template Patient Library v2.0
Phase II Liver Function Increased Monitoring Criteria with Continued Therapy
Liver Function Increased Monitoring Criterion and Follow-Up
Criteria Actions
ALT 3xULN and <5xULN and bilirubin <2xULN, without symptoms believed to be related to liver injury or hypersensitivity, and who can be monitored weekly for 4 weeks
Notify the [sponsor] medical monitor within 24 hours of learning of the abnormality to discuss participant safety.
Participant can continue study treatment Participant must return weekly for repeat liver
function tests (ALT, AST, alkaline phosphatase, bilirubin) until the abnormalities resolve, stabilize or return to baseline.
If at any time, the participant meets liver function stopping criteria, proceed as described [location].
If, after 4 weeks of monitoring, ALT <3xULN and bilirubin <2xULN, monitor participants twice monthly until liver function tests normalize or return to baseline.
ReferencesJames LP, Letzig L, Simpson PM, Capparelli E, Roberts DW, Hinson JA, Davern TJ, Lee WM. Pharmacokinetics of Acetaminophen-Adduct in Adults with Acetaminophen Overdose and Acute Liver Failure. Drug Metab Dispos 2009; 37:1779-1784.
<End of common wording
© 2015 TransCelerate BioPharma 14

Common Protocol Template Patient Library v2.0
<Start of common wording for Phase III studies>
Phase III-IV liver function stopping criteria are designed to assure participant safety and to evaluate liver event etiology.
Phase III-IV liver function stopping criteria and Follow-Up assessments
Liver Function Stopping Criteria
ALT-absolute ALT 8xULN
ALT Increase ALT 5xULN but <8xULN persists for 2 weeksALT 3xULN but <5xULN persists for 4 weeks
Bilirubin1, 2 ALT 3xULN and bilirubin 2xULN (>35% direct bilirubin)
INR2 ALT 3xULN and INR >1.5, if INR measured
Cannot Monitor
ALT 5xULN but <8xULN and cannot be monitored weekly for 2 weeksALT 3xULN but <5xULN and cannot be monitored weekly for 4 weeks
Symptomatic3 ALT 3xULN associated with symptoms (new or worsening) believed to be related to liver injury or hypersensitivity
Suggested Actions and Follow up Assessments following ANY Liver Stopping Event
Actions Follow Up Assessments
Immediately discontinue study treatment. Report the event to the [sponsor] within 24
hours. Complete the liver event CRF, and
complete an SAE data collection tool if the event also met the criteria for an SAE.2
Perform liver function follow-up assessments.
Monitor the participant until liver function test abnormalities resolve, stabilize, or return to baseline (see MONITORING).
Do not restart/rechallenge participant with study treatment unless allowed per protocol and [sponsor] Medical Governance approval is granted (refer to Appendix [X] )
If restart/rechallenge not allowed per protocol or not granted, permanently discontinue study treatment and may continue participant in the study for any protocol specified follow up assessments
Viral hepatitis serology4
Only in those with underlying chronic hepatitis B at study entry (identified by positive hepatitis B surface antigen) quantitative hepatitis B DNA and hepatitis delta antibody5
Blood sample for pharmacokinetic (PK) analysis obtained [insert time interval recommended by clinical pharmacokinetics representative] after the most recent dose6
Serum creatine phosphokinase (CPK) and lactate dehydrogenase (LDH)
Fractionate bilirubin, if total bilirubin 2xULN
Complete blood count with differential to assess eosinophilia
Record the appearance or worsening of clinical symptoms of liver injury, or
© 2015 TransCelerate BioPharma 15

Common Protocol Template Patient Library v2.0
MONITORING:For bilirubin or INR criteria: Repeat liver function tests (include ALT,
AST, alkaline phosphatase, bilirubin) and perform liver function follow-up assessments within 24 hrs.
Monitor participant twice weekly until liver function test abnormalities resolve, stabilize or return to baseline.
A specialist or hepatology consultation is recommended.
For All other criteria: Repeat liver function tests (include ALT,
AST, alkaline phosphatase, bilirubin) and perform liver function follow-up assessments within 24 to 72 hours.
Monitor participants weekly until liver function abnormalities resolve, stabilize, or return to baseline.
hypersensitivity, on the AE report form Record use of concomitant medications
(including acetaminophen, herbal remedies, and other over-the-counter medications) on the concomitant medications report form.
Record alcohol use on the liver event alcohol intake CRF
For bilirubin or INR criteria: Anti-nuclear antibody, anti-smooth
muscle antibody, Type 1 anti-liver kidney microsomal antibodies, and quantitative total immunoglobulin G (IgG) or gamma globulins.
Serum acetaminophen adduct HPLC assay (quantifies potential acetaminophen contribution to liver injury in participants with definite or likely acetaminophen use in the preceding week [James, 2009]. NOTE: Not required in China.
Liver imaging (ultrasound, magnetic resonance, or computerizsed tomography) andor liver biopsy to evaluate liver disease; complete Liver Imaging and/or Liver Biopsy CRFs.
1. Serum bilirubin fractionation should be performed if testing is available. If serum bilirubin fractionation is not immediately available, discontinue study treatment if ALT 3xULN and bilirubin 2xULN. Additionally, if serum bilirubin fractionation testing is unavailable, record the absence/presence of detectable urinary bilirubin on dipstick which is indicative of direct bilirubin elevations suggesting liver injury.
2. All events of ALT 3xULN and bilirubin 2xULN (>35% direct bilirubin) or ALT 3xULN and INR >1.5 may indicate severe liver injury (possible ‘Hy’s Law’) and must be reported as an SAE (excluding studies of hepatic impairment or cirrhosis). The INR measurement is not required and the stated threshold value will not apply to participants receiving anticoagulants.
3. New or worsening symptoms believed to be related to liver injury (such as fatigue, nausea, vomiting, right upper quadrant pain or tenderness, or jaundice) or hypersensitivity (such as fever, rash or eosinophilia).
4. Includes:Hepatitis A IgM antibody; hepatitis B surface antigen and hepatitis B Core Antibody (HBcAb); hepatitis C RNA; cytomegalovirus IgM antibody; Epstein-Barr viral capsid antigen IgM antibody (or if unavailable, heterophile antibody or monospot testing); and hepatitis E IgM antibody.
5. If hepatitis delta antibody assay cannot be performed,, it can be replaced with a PCR of hepatitis D RNA virus (where needed) [Le Gal, 2005].
6. PK sample may not be required for participants known to be receiving placebo or non-comparator treatments. Record the date/time of the PK blood sample draw and the date/time of the last dose of study treatment prior to the blood sample draw on the CRF. If the date or time of the last dose is unclear, provide the participant’s best
© 2015 TransCelerate BioPharma 16

Common Protocol Template Patient Library v2.0
approximation. If the date/time of the last dose cannot be approximated OR a PK sample cannot be collected in the time period indicated above, do not obtain a PK sample. Instructions for sample handling and shipping are in the [Study Reference Manual].
© 2015 TransCelerate BioPharma 17

Common Protocol Template Patient Library v2.0
Phase III-IV Liver Function Increased Monitoring Criteria with Continued Therapy
Liver Function Increased Monitoring Criteria
Criteria Actions
ALT 5xULN and <8xULN and bilirubin <2xULN without symptoms believed to be related to liver injury or hypersensitivity, and who can be monitored weekly for 2 weeks.ORALT 3xULN and <5xULN and bilirubin <2xULN without symptoms believed to be related to liver injury or hypersensitivity, and who can be monitored weekly for 4 weeks.
Notify the [sponsor] medical monitor within 24 hours of learning of the abnormality to discuss participant safety.
Participant can continue study treatment Participant must return weekly for repeat
liver function tests (ALT, AST, alkaline phosphatase, bilirubin) until the abnormalities resolve, stabilize or return to baseline.
If at any time, the participant meets liver function stopping criteria, proceed as described [location].
If ALT decreases from ALT 5xULN and <8xULN to ≥3xULN but <5xULN, continue to monitor liver chemistries weekly.
If, after 4 weeks of monitoring, ALT <3xULN and bilirubin <2xULN, monitor particpants twice monthly until liver function tests normalize or return to baseline.
ReferencesJames LP, Letzig L, Simpson PM, Capparelli E, Roberts DW, Hinson JA, Davern TJ, Lee WM. Pharmacokinetics of Acetaminophen-Adduct in Adults with Acetaminophen Overdose and Acute Liver Failure. Drug Metab Dispos 2009; 37:1779-1784.
Le Gal F, Gordien E, Affolabi D, Hanslik T, Alloui C, Dény P, Gault E. Quantification of Hepatitis Delta Virus RNA in Serum by Consensus Real-Time PCR Indicates Different Patterns of Virological Response to Interferon Therapy in Chronically Infected Patients. J Clin Microbiol. 2005;43(5):2363–2369.
<End of common text for Phase III studies>
© 2015 TransCelerate BioPharma 18

Common Protocol Template Patient Library v2.0
Liver Safety: Study Treatment Rechallenge Guidelines
A participant who met liver function stopping criteria cannot restart study treatment unless all of the following conditions are met:
[sponsor] approval is granted (as described below) IRB/IEC approval is obtained Separate ICF for treatment restart/rechallenge is signed by the participant
If [sponsor] approval to restart/rechallenge the participant with study treatment is not granted, then the participant must permanently discontinue study treatment and may continue in the study for protocol-specified follow-up assessments
Rechallenge Following Liver Function Events that are Possibly Related to Study Treatment
Following study treatment-induced liver injury, rechallenge is associated with 13% mortality across all study treatments in prospective studies.1 Clinical outcomes vary with nearly 50% fatality with halothane readministered within one month of the initial injury. However, some treatments seldom result in recurrent liver injury or fatality.
Risk factors for a fatal rechallenge outcome include:
o Hypersensitivity with initial liver injury (e.g., fever, rash, eosinophilia) 1
o Jaundice or bilirubin >2xULN with initial liver injury (direct bilirubin >35% of total)
o Ongoing severe liver injury defined by ALT 3xULN AND bilirubin 2xULN (direct bilirubin >35% of total), OR INR1.5
o Serious adverse event or fatality previously observed with rechallenges2,3
o Evidence of treatment-related preclinical liability (e.g., reactive metabolites, mitochondrial impairment)3
Rechallenge refers to resuming study treatment following drug-induced liver injury (DILI). Because of the risks associated with rechallenge after DILI, this should only be considered if there is compelling evidence of benefit from a critical or life-saving medicine, there is no alternative approved medicine available, and a benefit/risk assessment of rechallenge is considered to be favorable.
Approval by the [sponsor] for rechallenge with study treatment can be considered when:
o The Principal Investigator (PI) requests consideration of rechallenge with study treatment for a participant who is receiving compelling benefit with study treatment that exceeds risk and for whom no effective alternative therapy is available.
o IRB/IEC approval for rechallenge with study treatment has been obtained.
© 2015 TransCelerate BioPharma 19

Common Protocol Template Patient Library v2.0
If the rechallenge is approved by the [sponsor] in writing:
The participant must be provided with a clear description of the possible benefits and risks of study treatment administration including the possibility of recurrent, more severe liver injury or death.
The participant must also provide signed informed consent specifically for the rechallenge with study treatment. Documentation of informed consent must be recorded in the study file.
Study treatment must be administered at the dose specified by the [sponsor].
Participants approved by the [sponsor] for rechallenge with study treatment must return to the clinic twice a week for liver function tests until stable liver function tests have been demonstrated and then standard laboratory monitoring may resume as per protocol.
If the participant meets protocol-defined liver function stopping criteria after study treatment rechallenge, study treatment should be permanently discontinued.
The [sponsor] Medical Monitor, and the IRB/IEC, must be informed of the outcome for the participant following study treatment rechallenge.
The [sponsor] must be notified of any adverse events, as per Appendix 4.
Restart Following Transient Resolving Liver Function Events Not Related to Study Treatment
Restart refers to resuming study treatment following liver function events for which there are clear underlying causes (other than DILI) (e.g. biliary obstruction, pancreatic events, hypotension, acute viral hepatitis). Furthermore, there should be no evidence of alcoholic hepatitis or hypersensitivity, and the study treatment should not be associated with Human Leucocyte antigen (HLA) markers of liver injury.
Approval by the [sponsor] for study treatment restart can be considered when:o The investigator requests consideration for study treatment restart if liver function
events have a clear underlying cause (e.g., biliary obstruction, hypotension) and liver function tests have improved to normal or are within 1.5 x baseline and ALT <3xULN.
o Restart risk factors (e.g., fever, rash, eosinophilia, hypersensitivity, alcoholic hepatitis, possible study treatment-induced liver injury or study treatment has an HLA genetic marker associated with liver injury [e.g. lapatinib, abacavir, amoxicillin/clavulanate]) are reviewed and excluded.
o IRB/IEC approval of study treatment restart has been obtained.
If restart of study treatment is approved by the [sponsor] in writing:
The participant must be provided with a clear description of the possible benefits and risks of study treatment administration including the possibility of recurrent, more severe liver injury or death.
© 2015 TransCelerate BioPharma 20

Common Protocol Template Patient Library v2.0
The participant must also provide signed informed consent specifically for the restart of study treatment. Documentation of informed consent must be recorded in the study file.
Study treatment must be administered at the dose specified by the [sponsor].
Participants approved by the [sponsor] for restart of study treatment must return to the clinic twice a week for liver function tests until stable liver function tests have been demonstrated and then standard laboratory monitoring may resume as per protocol.
If the participant meets protocol-defined liver function stopping criteria after study treatment restart, study treatment should be permanently discontinued.
The [sponsor] Medical Monitor, and the IRB/IEC, must be informed of the outcome for the participant following study treatment restart.
The [sponsor] must be notified of any adverse events, as per Appendix 4.
References:Andrade RJ, Robles M, Lucena MI. Rechallenge in drug-induced liver injury: the attractive hazard. Expert Opin Drug Saf. 2009;8:709-714.
Papay JI, Clines D, Rafi R, Yuen N, Britt SD, Walsh JS, Hunt CM. Drug-induced liver injury following positive drug rechallenge. Regul Tox Pharm. 2009;54:84-90.
Hunt, CM. Mitochondrial and immunoallergic injury increase risk of positive drug rechallenge after drug-induced liver injury: A systematic review. Hepatol. 2010;52:2216-2222.
© 2015 TransCelerate BioPharma 21