
Pat Mastors President | Co-Founder PatientVoiceInstitute.org [email protected] [email protected].
Optimizing Patients for SurgeryOptimizing Patients for Surgery
R l f th PAT i iR l f th PAT i iRole of the PAT nurse in assessing Role of the PAT nurse in assessing patient riskpatient risk
Tanya Cowder, RN, CNSSue Burns, RN
Avis Hayden, PhDy ,
PAT: Pre‐Anesthesia
Teaching
Southwestern Vermont Medical C tCenter
•3,100 surgeries per year•35 surgeons 2 PAT nurses•35 surgeons, 2 PAT nurses•80% ambulatory care; 20% inpatient•Physician affiliation DHMC
Objectives for Today:Objectives for Today:
•Factors leading to change•Factors leading to change•Key elements of new processy p•Expanded role of PAT nurse•Outcomes, data•Next steps•Next steps
Frank’s StoryFrank s Story
InterviewsInterviews•Chief Medical Officer•Patient Safety Specialist•Anesthesiologists•Anesthesiologists•Internists & PCP’s•Surgeons•Nurses•Nurses•Support Staffpp


Challenge #1:Challenge #1:
RISK IDENTIFICATION NOT RELIABLE
••Not well definedNot well defined
••No double checkNo double checkNo double checkNo double check
80% cases identified(too low)
Sample of 128 elective cases Mar, Apr 2011
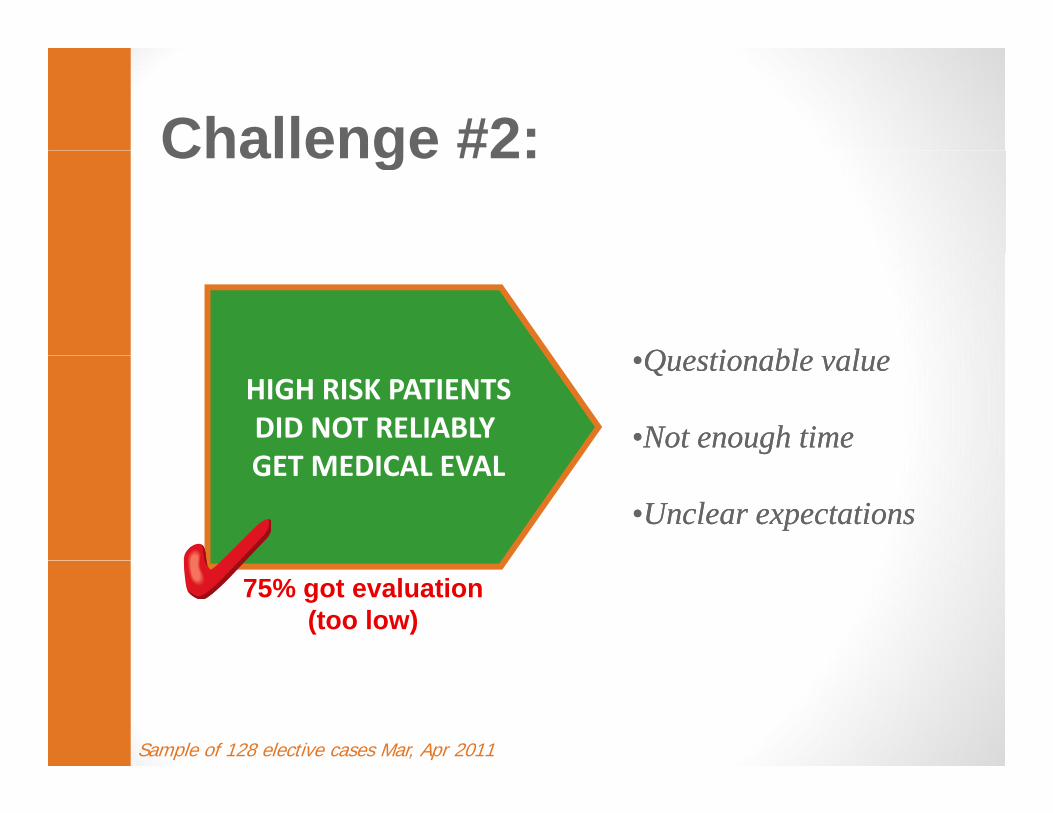
Challenge #2:Challenge #2:
Q ti bl lQ ti bl lHIGH RISK PATIENTSDID NOT RELIABLY GET MEDICAL EVAL
••Questionable valueQuestionable value
••Not enough timeNot enough timeGET MEDICAL EVAL
••Unclear expectationsUnclear expectations
75% got evaluation(too low)
Sample of 128 elective cases Mar, Apr 2011
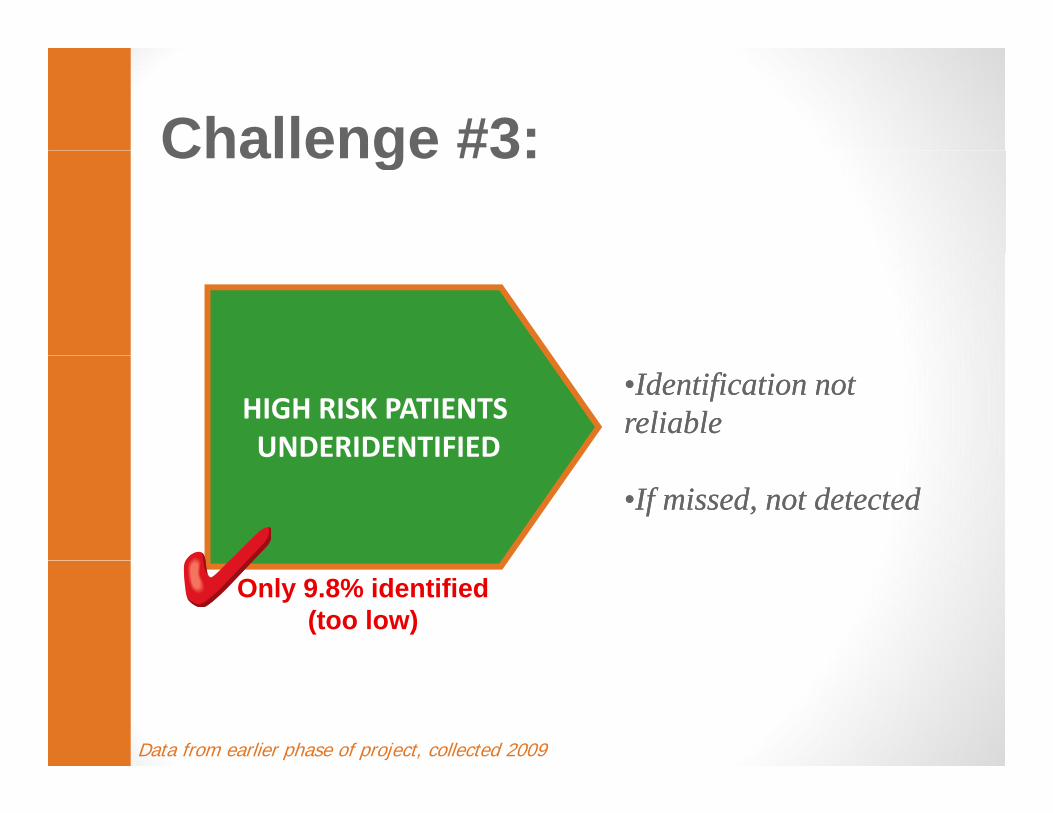
Challenge #3:Challenge #3:
HIGH RISK PATIENTS UNDERIDENTIFIED
••Identification not Identification not reliablereliable
••If missed, not detectedIf missed, not detected
Only 9.8% identified (too low)
Data from earlier phase of project, collected 2009
Summary:Summary: Develop reliable process for:Develop reliable process for:
Ri k id tifi ti•Risk identification
•Medical evaluation
•FOCUS: Timely flow of i f tiinformation

Change #1: Define High RiskChange #1: Define High Risk
• Polypharmacy (7 +)• Polypharmacy (7 +) • Active cardiac disease • Poorly controlled hypertension• Diabetes requiring medication• Diabetes requiring medication• Sleep apnea• Anticoagulation• If clinical intuition raises the• If clinical intuition raises the
question
Change #2: Booking ReportChange #2: Booking Report
DATE OF DATE OF SURGERYREPORT
BOOKINGREPORT
RN VERIFY risk category
RN & Anesthesia UPGRADERN & Anesthesia UPGRADErisk category based on assessment
of patient history
Change #3: Medical EvalChange #3: Medical Eval
•HIGH RISK
•NORMAL RISK•NORMAL RISK
Change #4: Clinical InformationChange #4: Clinical Information
Orders, Consent, H&P
Assemble chart
Change #5: Medical EvalChange #5: Medical Eval
M di l bl• Medical problems• Medication list• Would delaying the procedure allow to better control any of theallow to better control any of the following:
H A1C 7• HgA1C over 7• Poorly controlled hypertension or heart disease• Active infections• Sleep apnea• Anticoagulant therapy
Change #6: Booking ScriptChange #6: Booking Script
•Urgent?•Urgent? Elective?
•High Risk? Normal Risk?Normal Risk?
•If High Risk, gname of PCP
Change # 7: Booking Window•High Risk PatientsHigh Risk Patients
Optimal interval 14 days
All Oth P ti t•All Other Patients Minimal interval -- 7 days

Change #8: FeedbackC a ge #8 eedbac
Risk Factors
AnesthesiaSignatures
Methods & ToolsMethods & Tools
•Process maps•Algorithms•Data
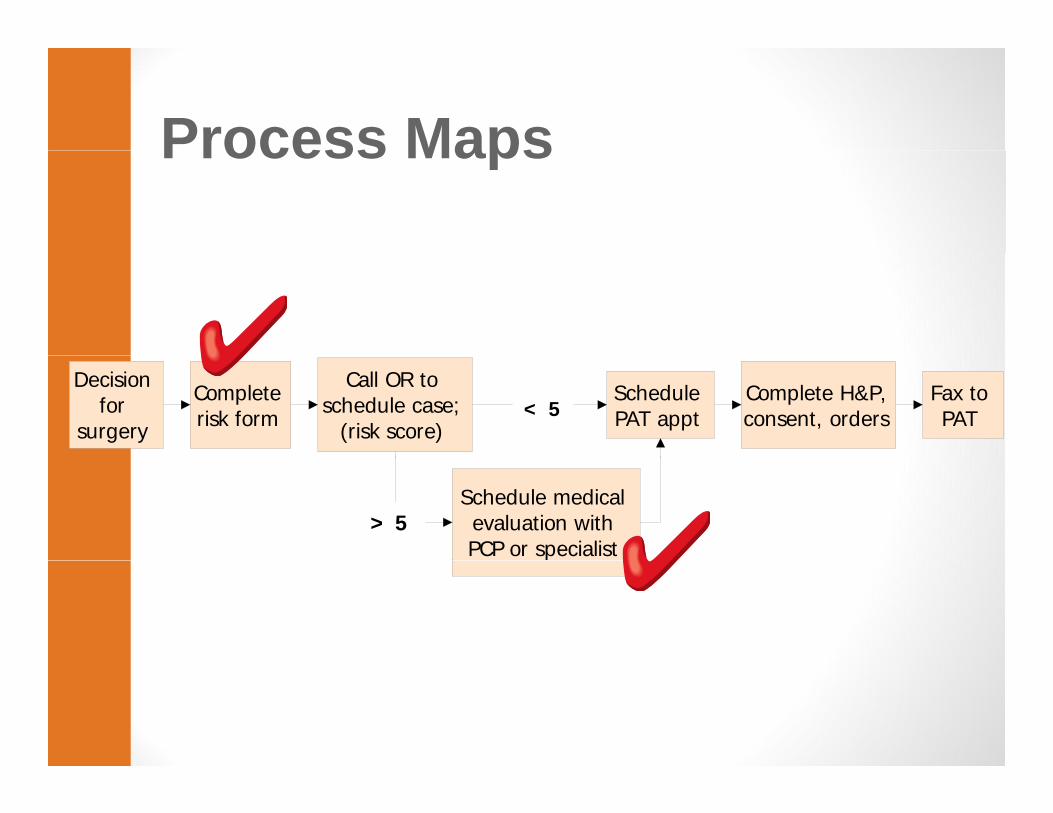
Process MapsProcess Maps
Decision for
surgery
Complete risk form
Call OR to schedule case;
(risk score)
Complete H&P, consent, orders
Fax to PAT
Schedule PAT appt< 5
Schedule medical evaluation with PCP or specialist
> 5
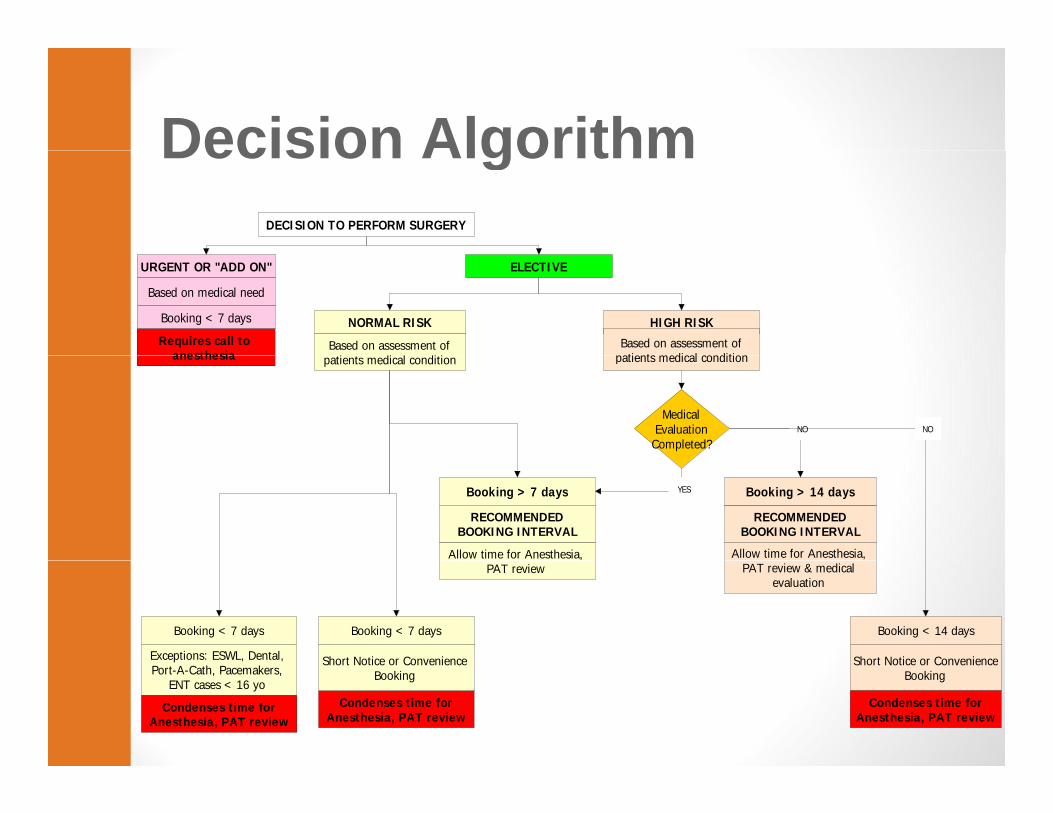
Decision AlgorithmDecision AlgorithmDECISION TO PERFORM SURGERY
URGENT OR "ADD ON" ELECTIVE
Based on medical need
Booking < 7 days
Requires call to anesthesia
NORMAL RISK HIGH RISK
Based on assessment of i di l di i
Based on assessment of patients medical conditionanesthesia patients medical condition patients medical condition
Medical Evaluation Completed?
NO NO
Booking > 7 days
Allow time for Anesthesia,
RECOMMENDED BOOKING INTERVAL
Booking > 14 daysYES
Allow time for Anesthesia,
RECOMMENDED BOOKING INTERVAL
,PAT review PAT review & medical
evaluation
Booking < 14 days
Short Notice or Convenience
Booking < 7 days
Short Notice or Convenience
Booking < 7 days
Exceptions: ESWL, Dental, Short Notice or ConvenienceBooking
Condenses time for Anesthesia, PAT review
Condenses time for Anesthesia, PAT review
Short Notice or Convenience BookingPort-A-Cath, Pacemakers,
ENT cases < 16 yo
Condenses time for Anesthesia, PAT review

Challenge #1Challenge #1
RISK IDENTIFICATION NOT RELIABLE
SIMPLIFYDEFINITIONS, GIVE FEEDBACK
100% cases identified(88% surgeon, 12% PAT nurse)
80% cases identified(too low)
Sample of 128 elective cases Mar, Apr 2011; project data 2012.
)
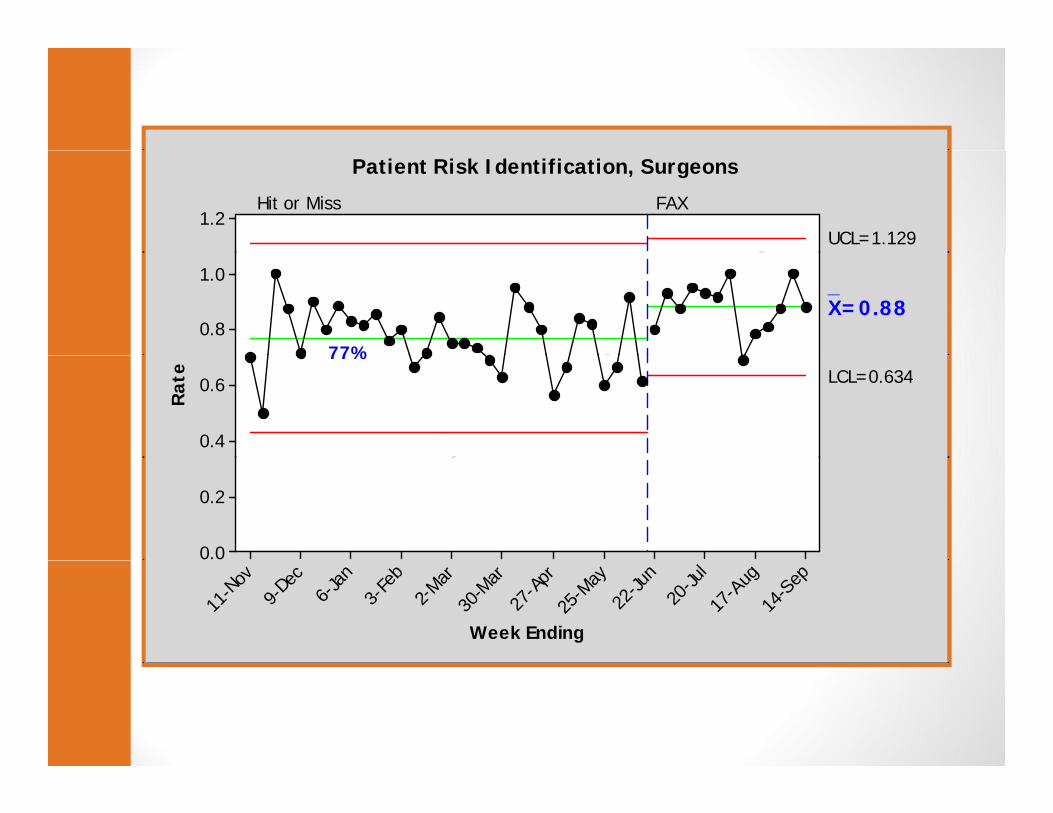
1.2UCL=1.129
Hit or Miss FAX
Patient Risk Identification, Surgeons
1.0
0.8
_X=0.88
77%
0.6
0.4
Rat
e LCL=0.63477%
0.2
0.0
14-S
ep
17-A
ug20
-Jul
22-Ju
n
25-M
ay
27-A
pr
30-M
ar2-M
ar3-
Feb
6-Jan
9-De
c
11-N
ov
Week Ending
Challenge #2:Challenge #2:
HIGH RISK PATIENTSDID NOT RELIABLY GET MEDICAL EVAL
WORKFLOW CHANGE“HARD STOP”
GET MEDICAL EVAL
100% got evaluation75% got evaluation(too low)
Sample of 128 elective cases Mar, Apr 2011; project data 2012

Challenge #3Challenge #3
HIGH RISK PATIENTS UNDERIDENTIFIED
RELIABLE PROCESS CLEAR EXPECTATIONS
Now 26% identifiedOnly 9.8% identified (too low)
Data from earlier project collected 2009; new project data 2012
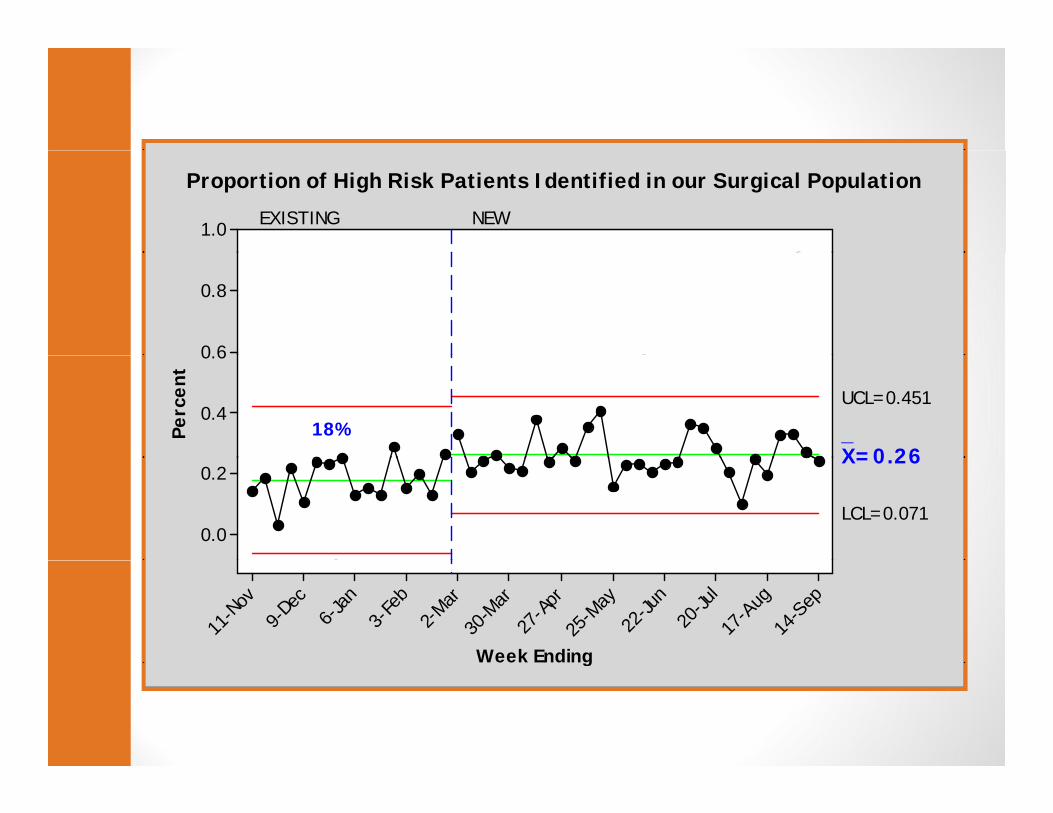
1.0 EXISTING NEW
Proportion of High Risk Patients Identified in our Surgical Population
0.8
0 60.6
0.4
Perc
ent
_X=0 26
UCL=0.451
18%
0.2
0.0
X=0.26
LCL=0.071
14-S
ep
17-A
ug20
-Jul
22-Ju
n
25-M
ay
27-A
pr
30-M
ar2-M
ar3-
Feb
6-Jan
9-De
c
11-N
ov
Week Endingg
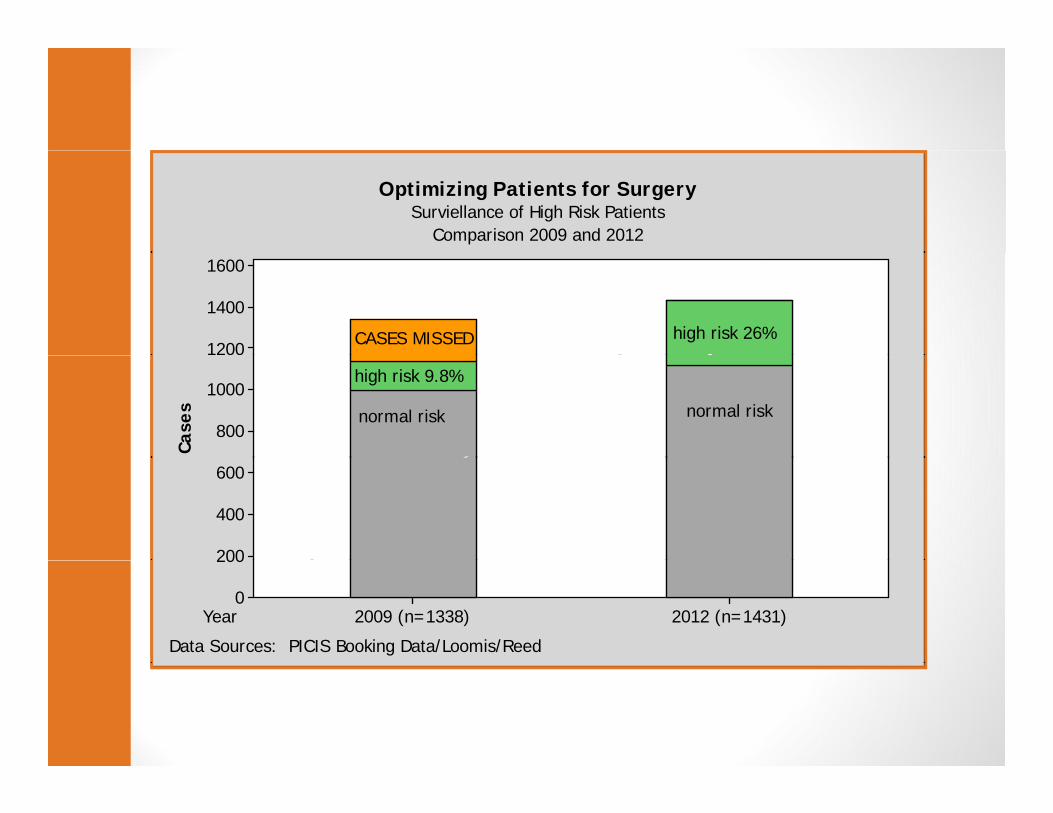
Optimizing Patients for SurgerySurviellance of High Risk Patients
Comparison 2009 and 2012
1600
1400
1200 CASES MISSED high risk 26%
1000
800
Case
s normal risk
high risk 9.8%
normal risk
600
400
200
Year 2012 (n=1431)2009 (n=1338)
200
0
Data Sources: PICIS Booking Data/Loomis/Reed
Issues Still to be Addressed:Issues Still to be Addressed:
• ClinicalClinical• Anticoagulation **• Beta blockersBeta blockers• Poorly controlled diabetes• Sleep apnea **• Obesity
• Process• Post op co-management• Short notice booking
SummarySummary
• Identified a problem•Identified a problem•Interviewed key stakeholders•Reviewed literature•Developed a new process•Developed a new process•Used data to keep the process on track
•After 1 yr – reliable processAfter 1 yr reliable process
Questions Contact emails:[email protected]@phin.orgy @p g


















