
6 - Integrating Therapeutic Advances and Stakeholder ...2017+Slides/Integrating... · God Only...
54
Transcript of 6 - Integrating Therapeutic Advances and Stakeholder ...2017+Slides/Integrating... · God Only...


Integrating Therapeutic Advances and Stakeholder Perspectives to NSCLS Clinical Pathways Discussions and Implementation
This educational activity is supported by an educational grant from
Genentech, and Novartis Pharmaceuticals Corporation

Faculty
David Jackman, MDMedical Director of Clinical PathwaysSenior Physician Dana-Farber Cancer InstituteAssistant Professor Harvard Medical School

Disclosures
Dr Jackman: Consultant – AstraZeneca, Celgene, CVS, Eli Lilly

Learning Objectives
• Describe the current state of NSCLC care and the impact of recent advances in precision medicine on the diagnostic-treatment paradigm
• Outline the factors that contribute to variations in evidence-based practice, patient outcomes, and health-related costs in NSCLC diagnosis and management
• Evaluate the impact of NSCLC pathways on utilization, costs, outcomes, guideline adherence, personalized therapeutic selection, and inclusion of recent advances
• Apply strategies to improve adherence and mitigate barriers to NSCLC pathways within your institution
• Integrate the patient perspective into pathway development and discussions

Stakes & Stakeholders
Stakes
• What is the best care we can provide?– Best care for the many and the individual– Guidance for the present, flexibility for the
future• Considerations: Efficacy, toxicity, cost• Qualities: Comprehensive, granular, dynamic• Off pathway ≠ wrong

Stakeholders

Transparency and Consistency
• Getting to the table– Who is involved– Setting the agenda– Data for consideration
• Making the meal– Level of evidence– Tools for considering value– Quantifying the unquantifiable
• Who eats?– Disseminating decisions– Who is the intended target?
First-line Therapy in Stage IV NSCLC:Turn, Turn, Turn

First-line Therapy in Stage IV NSCLC:Changes

First-line Therapy in Stage IV NSCLC:God Only Knows

March of the Doublets
Schiller JH, et al. N Engl J Med. 2002;346:92.
Perc
ent
Months
Paclitaxel/Cisplatin 7.8 10Gemcitabine/Cisplatin 8.1 13Docetaxel/Cisplatin 7.4 11Paclitaxel/Carboplatin 8.1 11
Median Survival (mo)100
80
60
40
20
00 5 10 15 20 25 30
2-y Survival (%)
Metastatic NSCLC: First-line Therapy2002
NSCLC
Platinum Doublet

Metastatic NSCLC: First-line Therapy Today
NSCLC
SquamousNon-squamous
Platinum Doublet
Targetable Genomic Change
No Targetable Genomic Change
gefitinib
afatinib
ceritinib
alectinib
EGFR
erlotinib
ALK
crizotinib
ROS1
crizotinib
BRAF
dabrafenib+
trametinib
platinum doublet +
bevacizumab
platinum + pemetrexed
platinum doublet +
necitumumab
platinum doublet + necitumumab
PD-L1 > 50%
pembrolizumab
ALK = anaplastic lymphoma kinase gene; EGFR = epidermal growth factor receptor gene.

Metastatic NSCLC: First-line Therapy Today
NSCLC
SquamousNon-squamous
Platinum Doublet
Targetable Genomic Change
No Targetable Genomic Change
gefitinib
afatinib
ceritinib
alectinib
EGFR
erlotinib
ALK
crizotinib
ROS1
crizotinib
BRAF
dabrafenib+
trametinib
platinum + pemetrexed +
PD-L1 > 50%
pembrolizumab
pembrolizumab
ALK = anaplastic lymphoma kinase gene; EGFR = epidermal growth factor receptor gene.

What were you thinking?Pembrolizumab in first-line
NSCLC with PD-L1>50%

Keynote 024: Study Objectives and Design
DOR = duration of response; PD = progressive disease; ORR = objective response rate; OS = overall survival; PFS = progression-free survival; TPS = tumor proportion score.Reck M, et al. New Engl J Med. 2016;375:1823-1833.

Keynote 024: Response in ITT Population
Objective response was considered to be a confirmed complete or partial response, assessed by blinded, independent central radiologic review.Time to response and duration of response were evalueated in the patients who had an objective response.Duration of response was calculated by the Kaplan-Meier method for censored data.ITT = intent to treat; NR = Not Reached.Reck M, et al. New Engl J Med. 2016;375:1823-1833.

Keynote 024: PFS in ITT Population
Reck M, et al. New Engl J Med. 2016;375:1823-1833.

Keynote 024: PFS in ITT Population
Reck M, et al. New Engl J Med. 2016;375:1823-1833.

Keynote 024: OS in ITT Population
Reck M, et al. New Engl J Med. 2016;375:1823-1833.

Keynote 024: Exposure and Safety in ITT Population
Pembrolizumab(n=154)
Chemotherapy(n=150)
Exposure, months median (range) 7.0(1d – 18.8 mo)
3.5(1d – 16.8 mo)
Treatment-related AEs, n (%)Grade 3-4SeriousLed to discontinuationLed to death
113 (73)40 (26)33 (21)11 (7)1 (< 1)
135 (90)77 (51)31 (21)16 (11)3 (2)
AE = adverse event.Reck M, et al. New Engl J Med. 2016;375:1823-1833.
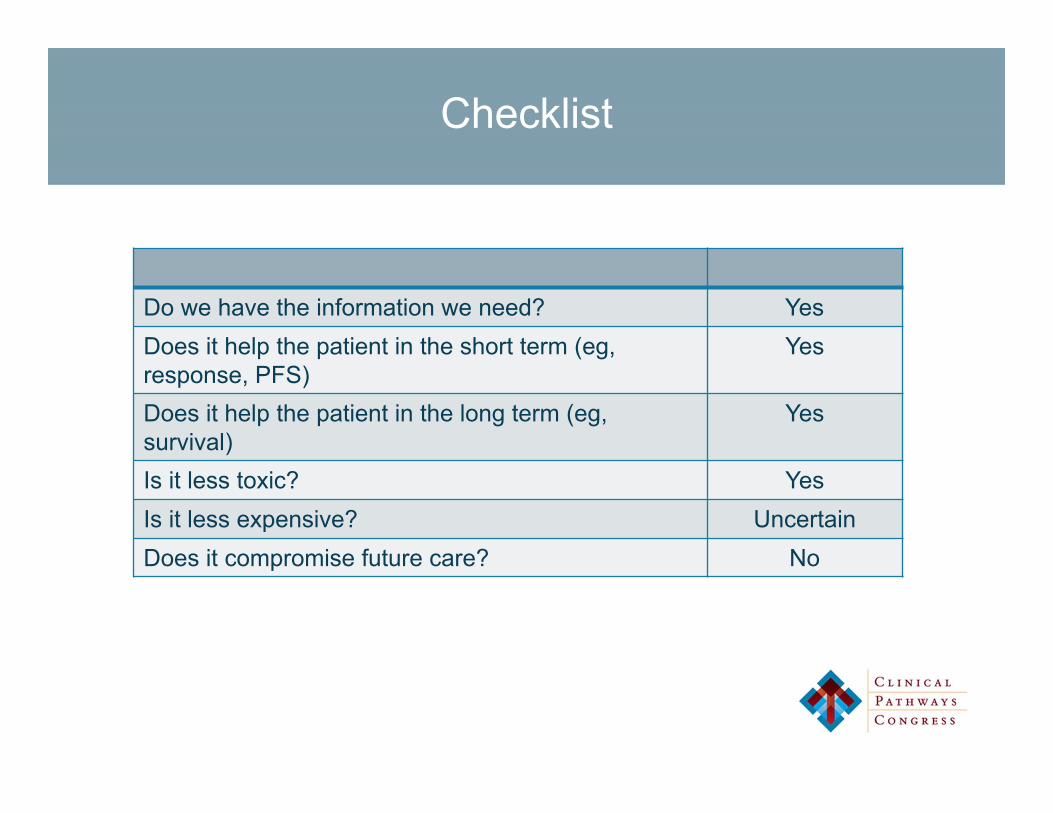
Checklist
Do we have the information we need? YesDoes it help the patient in the short term (eg, response, PFS)
Yes
Does it help the patient in the long term (eg, survival)
Yes
Is it less toxic? YesIs it less expensive? UncertainDoes it compromise future care? No
What were you thinking?nab-paclitaxel for first-line therapy
of stage IV squamous-cell carcinoma

nab-Paclitaxel with First-line Therapy
• CONSORT: randomized 1:1 phase 3 trial of carboplatin with either paclitaxel or nab-paclitaxel
• Primary endpoint: objective response rate• Overall efficacy
Carbo + nab-paclitaxel
Carbo + paclitaxel P-value
N 521 531
ORR 33% (170/521) 25% (132/531)0.005
Response Rate Ratio 1.313(1.082 – 1.593)
PFS 6.3 months 5.8 months 0.214HR 0.902 (0.767 – 1.060)
OS 12.1 11.2 .271HR 0.922 (0.797 – 1.066)
HR = hazard ratio.Socinski MA, et al. J Clin Oncol. 2012;30(17):2055-2062.

Is This Clinically Significant?Is This Cost-effective?
Carbo + nab-paclitaxel
Carbo + paclitaxel P-value
Squamous41%
(94/229)24%
(54/221)
.001Response Rate Ratio
1.680 (1.271 – 2.221)
Non-squamous26%
(76/292)25%
(78/310)
0.808Response Rate Ratio
1.034 (0.788 – 1.358)
Socinski MA, et al. J Clin Oncol. 2012;30(17):2055-2062.

Comparing Costs
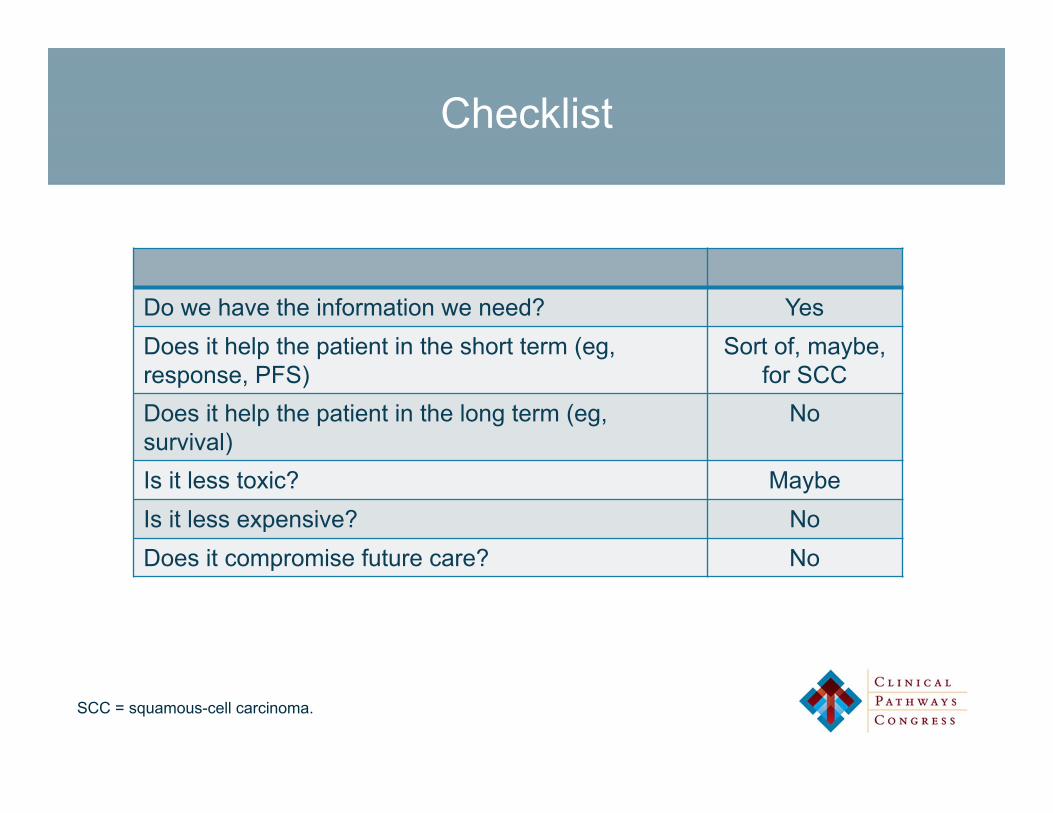
Checklist
Do we have the information we need? YesDoes it help the patient in the short term (eg, response, PFS)
Sort of, maybe,for SCC
Does it help the patient in the long term (eg, survival)
No
Is it less toxic? MaybeIs it less expensive? NoDoes it compromise future care? No
SCC = squamous-cell carcinoma.
What were you thinking?First-line therapy in ALK-
rearranged NSCLC

ALK-rearranged NSCLC: Background
• 2007: Soda et al publish discovery of ALKrearrangements in non-small cell lung cancer1
• 2010: Kwak et al. publish results of phase I trial of crizotinib in ALK rearranged lung cancer2
1. Soda M, et al. Nature. 2007;448(7153):561-566; 2. Kwak EL, et al. N Engl J Med. 2010;363(18):1693-1703.

J-ALEX: Progression-free Survival
J-ALEX = _________.Hida T, et al. Lancet. 2017;390(10089):29-39.

J-ALEX: Secondary Endpoints
Crizotinib AlectinibResponse 79% 92%Overall survival Immature, not publishedGrade 3-4 toxicity 52% 26%Drug-related dose interruption 74% 29%Drug-related discontinuation 20% 9%
Hida T, et al. Lancet. 2017;390(10089):29-39.

ALEX: Progression-free Survival
Mok TS, et al. N Engl J Med. 2017;376(7):629-640.
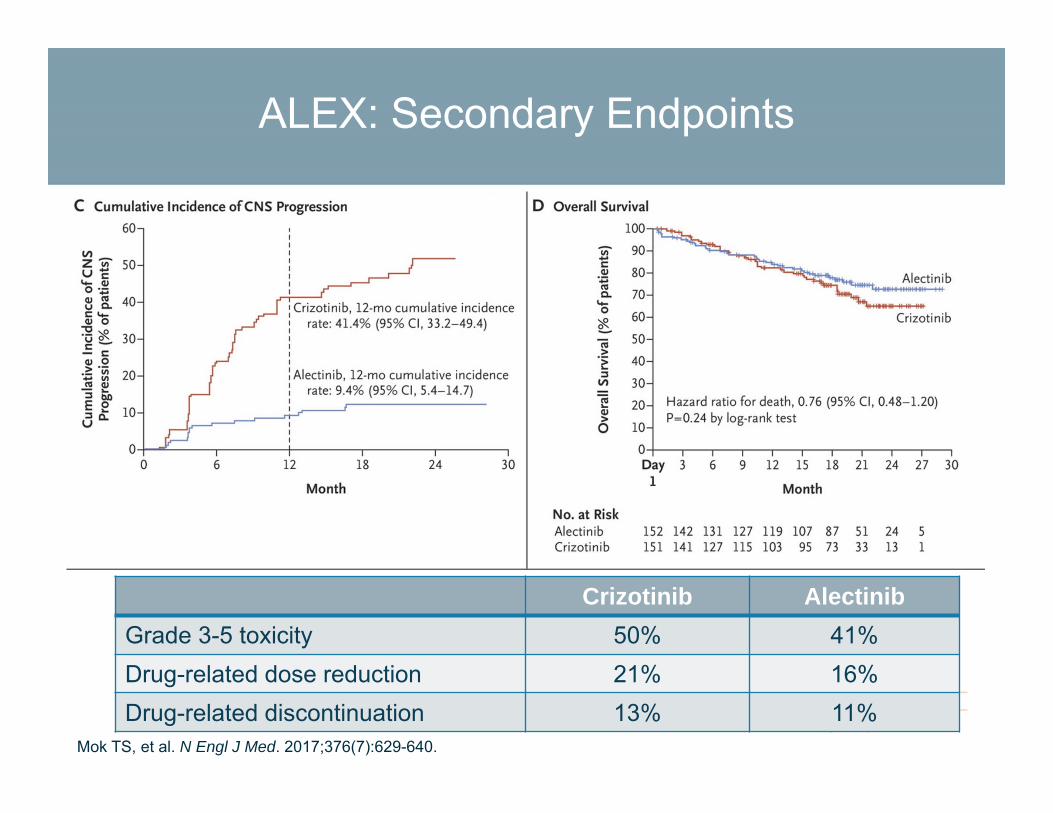
ALEX: Secondary Endpoints
Crizotinib AlectinibGrade 3-5 toxicity 50% 41%Drug-related dose reduction 21% 16%Drug-related discontinuation 13% 11%
Mok TS, et al. N Engl J Med. 2017;376(7):629-640.

ALK Inhibitors: Costs

Checklist
Do we have the information we need? Yes, mostlyDoes it help the patient in the short term (eg, response, PFS)
Yes
Does it help the patient in the long term (eg, survival)
No
Is it less toxic? YesIs it less expensive? YesDoes it compromise future care? No

What were you thinking?Chemo + pembrolizumab in
first-line non-squamous NSCLC
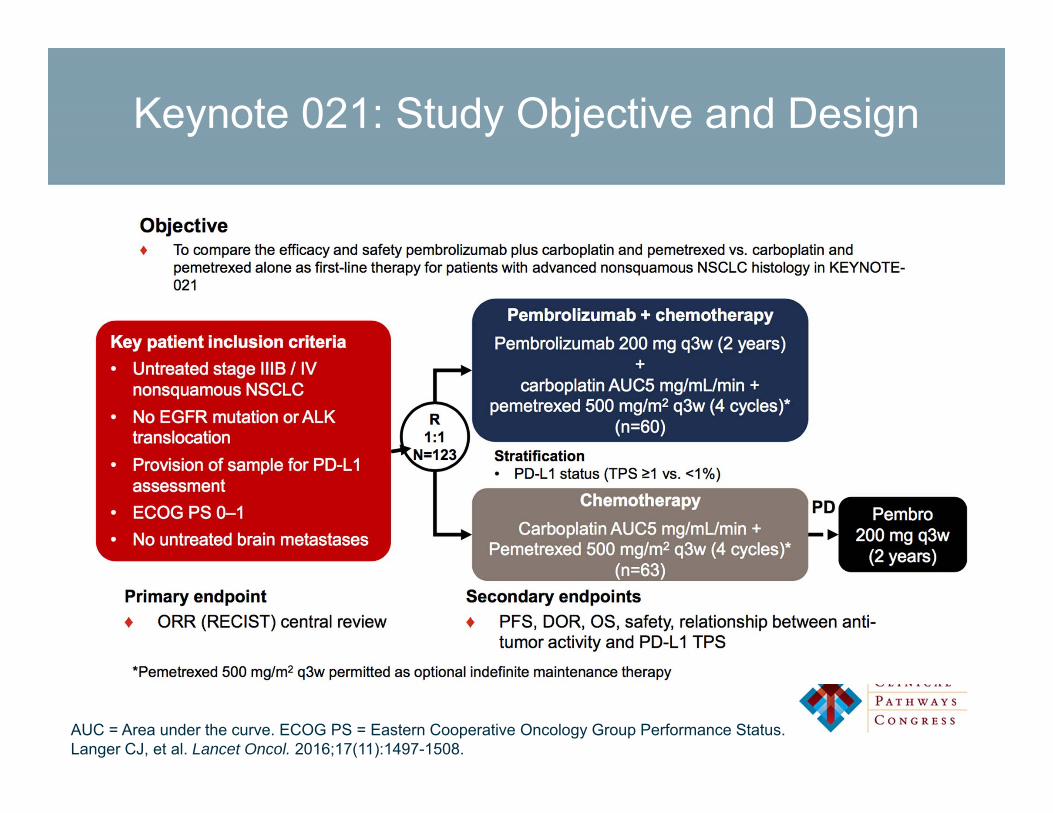
Keynote 021: Study Objective and Design
AUC = Area under the curve. ECOG PS = Eastern Cooperative Oncology Group Performance Status.Langer CJ, et al. Lancet Oncol. 2016;17(11):1497-1508.

Keynote 021: Response and toxicity
Chemo Chemo + pembro
P-value
Response Rate 29% 55% 0.0016
Langer CJ, et al. Lancet Oncol. 2016;17(11):1497-1508.

Keynote 021: Progression-free Survival
Langer CJ, et al. Lancet Oncol. 2016;17(11):1497-1508.

Keynote 021: Overall Survival
Langer CJ, et al. Lancet Oncol. 2016;17(11):1497-1508.

Keynote 021: Toxicity
Pembrolizumab + chemotherapy
(n=59)
Chemotherapy alone (n=62)
Exposure, months median (IQR)
8.0(4.7 to 11.2 mo)
4.9(2.1 to 7.4 mo)
Treatment-related AEs, n (%)Grade 3–4SeriousLed to discontinuation Led to death
55 (93) 22 (37) 16 (27) 6 (10) 1 (2)
56 (90) 14 (23) 6 (10) 8 (13) 2 (3)
Exposure and AE summary
IQR = interquartile range.Langer CJ, et al. Lancet Oncol. 2016;17(11):1497-1508.

Checklist
Do we have the information we need? NoDoes it help the patient in the short term (eg, response, PFS)
Yes
Does it help the patient in the long term (eg, survival)
No
Is it less toxic? NoIs it less expensive? NoDoes it compromise future care? ???

What’s next?
Sorting through Immunotherapy

Targeted Testing Landscape
• Testing has largely been based on drug approvals:– EGFR - BRAF– ALK - NTRK– ROS
• Moving to next-generation sequencing

Data

Complexity of Decision-Making
Abernathy J Clin Oncol. 2010.

Factors in Decision-making
1st Line NSCLC:• Histology• Stage• Brain mets?• ECOG PS• EGFR• ALK• ROS1• PD-L1
• CrCl• LFTs• CBC• Patient concerns• Symptomatic• Trial available• Trial interest• Distance
Whom to Start at Quarterback, Fantasy Football
• Availability/byes• Opponent pass rush• Offensive line
protection• Opponent secondary• Receive matchups• Opponent offense
(high-scoring/low scoring)
• Opponent rushing defense vs offense rushing attack
• Team injuries• Opponent injuries• Past performance
against this team• Recent performance
• Home/away• Crowd noise• Distance the visiting
team has to travel• Time of game• Wind• Precipitation• Done• Confidence in the
place kicker• Coaching factors• What’s at stake
CrCL = creatinine clearance; LFTs = liver function tests; CBC = complete blood count.
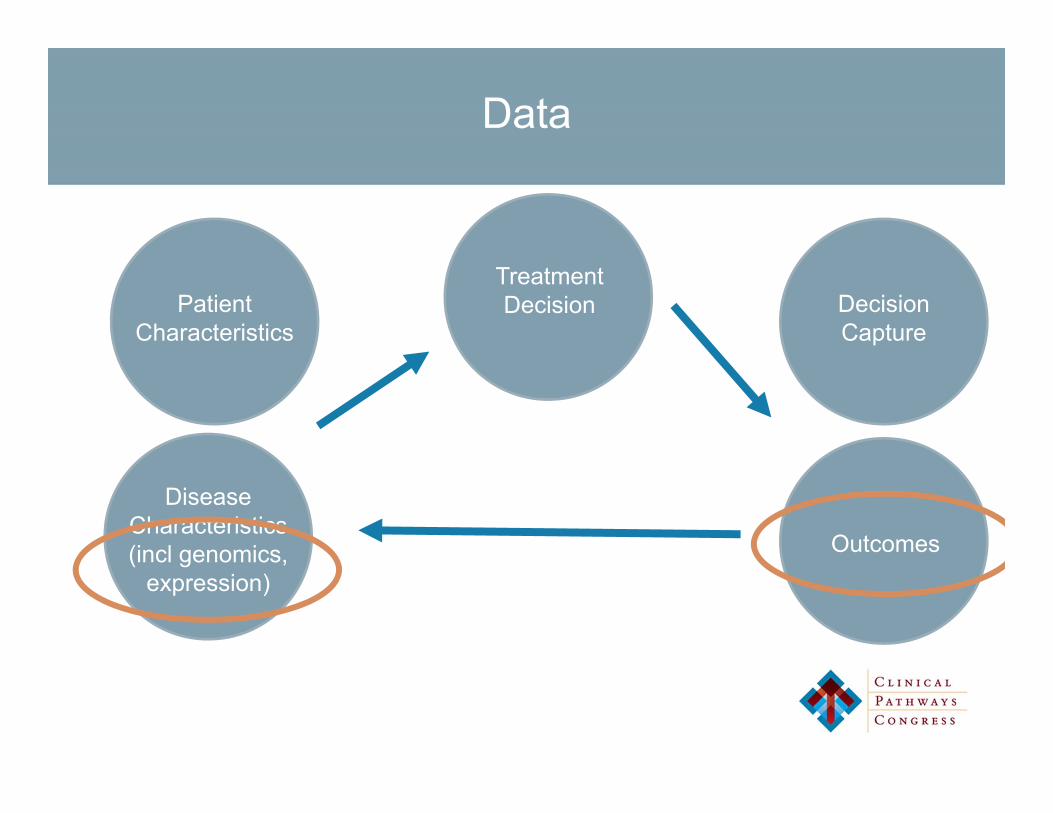
Data
Patient Characteristics
DiseaseCharacteristics(incl genomics,
expression)
TreatmentDecision Decision
Capture
Outcomes

Conclusions
• Pathways in NSCLC continue to evolve as science and drug development advance
• Challenges remain regarding making meaningful comparisons, especially around value
• Pathways should play an integral part in guiding future care

Acknowledgements
Pathways TeamJoseph JacobsonCarole DalbyTeresa GreenbergJulia HallJoanna HamiltonVicky HayneLeah SteinLinda Moroni
Via OncologyKathy LokayEd RodgersStephanie SimonsLauren Bradford
DFCI Leadership SupportDorothy PuhyEric WinerCraig BunnellElizabeth LiebowPasi Jänne
Pathways ArchitectsCaroline BlockSusanna CamposMatt DavidsPeter EnzingerDavid FisherArnold FreemanEric JacobsenCaron JacobsonKerry KilbridgeAnn LaCasceEudocia LeeUrsula Matulonis
Priscilla MerriamJeff MeyerhardtOreofe OdehideClaudia Paba-PradaGuilherme RabinowitsDoug RubinsonDavid SteensmaChristopher SweeneyKatherine ThorntonMartha WadleighBrian WolpinMatt Yurgulan
PharmacyAmal ArnaoutHillary PrescottMarina KaymakcalanHoury LeblebjianAndrew SkirvinJanine NazarroChristy Harris
FinanceBelen FraileYichen Zhang

Questions?


















