
6 December 1969 - bmj.com
3
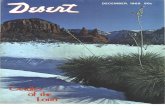
6 December 1969 G. P. T. BARCLAY ET AL.: ABNORMAL HAEMOGLOBINS IN ZAMBIA J. N. FERGUS ET' AL.: KIDNEY FUNCTION AFTER RENAL ARTERIAL EMBOLISM Hb A2 Line of origin H b Bart's Hb H -h FIG. l.-IHaemoglobin H disease (left) in an adult, and an infant's haemolysate with Haemoglobin Bares (right) in members of the Bemba tribe, Zambia. (Paper electrophoresis at PH 8 9.) FIG. 1.-Case 1. Note underfilling of small peripheral branches supply- ing middle and upper pole of right kidney. Main renal artery appears normal. Hb A1 Line of origin Hb A Hb Zambia FIG. Zy-ase 1. lThere is a translucent band in subcapsular region ox middle and upper pole of right kidney. FiG. 2.-Haemoglobin Zambia. Left: control. Right: note that Hb A2 is decreased. The abnormal a2 (Zambia) 82 runs by this method with Hb A. (Paper electrophoresis at pH 8 9.) FIG. 3.-" Fingerprint" (peptide chromatogram) of Haemoglobin Zambia. The abnormal peptlde stains yellow-brown with ninhydrin, indicating N-terminal glycine. For other details see text, FIG. 3.-Case 7. There is adherent thrombus in proxi- mal part of left main renal artery with more recent non-adherent thrombus more distally. Arteries supply- ing mid-portion of kidney distal to thrombus are dimin- ished and of small size. Ventral branch of main renal artery, though containing some fresh thrombus, is patent. A dorsal branch to upper pole is also patent. BRITISH MEDICAL JOURNAL + on 25 April 2022 by guest. Protected by copyright. http://www.bmj.com/ Br Med J: first published as 10.1136/bmj.4.5683.586 on 6 December 1969. Downloaded from
Transcript of 6 December 1969 - bmj.com

6 December 1969
G. P. T. BARCLAY ET AL.: ABNORMAL HAEMOGLOBINSIN ZAMBIA
J. N. FERGUS ET' AL.: KIDNEY FUNCTION AFTERRENAL ARTERIAL EMBOLISM
Hb A2
Line of origin
Hb Bart's
Hb H
-hFIG. l.-IHaemoglobin H disease (left) in an adult, and an infant'shaemolysate with Haemoglobin Bares (right) in members of the
Bemba tribe, Zambia. (Paper electrophoresis at PH 8 9.)
FIG. 1.-Case 1. Note underfilling of small peripheral branches supply-ing middle and upper pole of right kidney. Main renal artery appears
normal.
Hb A1
Line of origin
Hb A
Hb Zambia
FIG. Zy-ase 1. lThere is a translucent band in subcapsular region oxmiddle and upper pole of right kidney.
FiG. 2.-Haemoglobin Zambia. Left: control. Right: note thatHb A2 is decreased. The abnormal a2 (Zambia) 82 runs by this
method with Hb A. (Paper electrophoresis at pH 8 9.)
FIG. 3.-" Fingerprint" (peptide chromatogram) of Haemoglobin Zambia. Theabnormal peptlde stains yellow-brown with ninhydrin, indicating N-terminal
glycine. For other details see text,
FIG. 3.-Case 7. There is adherent thrombus in proxi-mal part of left main renal artery with more recentnon-adherent thrombus more distally. Arteries supply-ing mid-portion of kidney distal to thrombus are dimin-ished and of small size. Ventral branch of main renalartery, though containing some fresh thrombus, ispatent. A dorsal branch to upper pole is also patent.
BRITISHMEDICAL JOURNAL
+
on 25 April 2022 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.4.5683.586 on 6 Decem
ber 1969. Dow
nloaded from

December 1969 Faecal Escherichia coli-Cooke et al. BRITmI 595
soon enough after admission of the patients to hospital to beable to compare inpatient and outpatient strains of E. cOli.
In our work with Pseudomonas aeruginosa we have beenunable to trace the route by which individual strains spreadfrom one patient to another in the same ward. We have,however, found that some patients acquire intestinal strainsfrom food or medicines (Shooter et al., 1969). Preliminarywork suggests that food may also be one way in which ourward patients acquire new types of E. coli.The possible sources of the E. coli strains we have found in
food are of interest. It has been suggested that "animal"strains of E. coli are not so easily established in the bowel as"human" strains (Williams Smith, 1969). In a hospital inwhich selection of antibiotic resistant strains may operate, how-ever, it is possible that a route is provided by which antibiotic-resistant strains of E. coli from animals may reach the humanpopulation.
We are particularly indebted to Dr. Joan Taylor, in whoselaboratory the antisera were tested and the absorbed antisera pre-
pared. We wish to thank the nursing staff of the wards concernedfor their most helpful collaboration, and Dr. K. 0. Black and Dr.A. M. Dawson for permission to work on their wards. We shouldalso like to thank Mrs. N. Patel for technical assistance.The expenses for this investigation were met in part by a grant
from the St. Mark's Foundation.
REFERENCES
Bettelheim, K., and Taylor, Joan (1969). Yournal of Medical Microbio-logy. In press.
Kennedy, R. P., Plorde, J. J., and Petersdorf, R. G. (1965). Yournal ofClinical Investigation, 44, 193.
Roschka, R. (1950). Klinische Medizin, 5, 88.Sears, H. J., Brownlee, J., and Uchiyama, J. M. (1950). lournal of
Bacteriology, 59, 293.Sears, H. J., Janes, H., Saloum', R., Brownlee, J., and Lamoreaux, L. F.
(1956). Yournal of Bacteriology, 71, 370.Shooter, R. A., et al. (1969). Lancet, 1, 1227.Vosti, K. L., Monto, A. S., and Rantz, L. A. (1962). Proceedings of the
Society of Experimental Biology and Medicine, 111, 201.Winterbauer, R. H., Turck, M., and Petersdorf, R. G. (1967). Yournal
of Clinical Investigation, 46, 21.Williams Smith, H. (1969). Lancet, 1, 1174.
Abnormal Haemoglobins in Zambia. A New Haemoglobin Zambiac6O (E9) Lysine -e Asparagine
G. P. T. BARCLAY,* M.D., M.R.C.PATH.; DEBORAH CHARLESWORTHt PH.D.
H. LEHMANN,4 M.D., D.SC., F.R.C.P.
[WITH SPECIAL PLATE]
* Abnormal Haemoglobin Research Unit of Anglo-American Corporation(Central Africa) Ltd., Kitwe, Zambia.
t Research Assistant.* Honorary Director. -
Medical Research Council Abnormal Haemoglobin Unit, University De-partment of Bicchemistry, Cambridge.
British Medical Journal, 1969, 4, 595-596
Summary: A survey for abnormal haemoglobins inZambia has demonstrated Haemoglobin S-including
187 cases of sickle-cell anaemia, Haemoglobin J Oxfordon one occasion, and a new Haemoglobin Zambia in fourunrelated families. No evidence for 8-thalassaemia wasfound, but Haemoglobin H disease and other evidencefor a-thalassaemia were found.
Introduction
The results of a survey of some 10,000 blood samples inZambia differ in several respects from those that have beenreported from East and West Africa. Sickle-cell anaemia wasdiagnosed in 187 cases, most of them in infants, but in contrastto West Africa no Haemoglobin C and no /3-thalassaemia werefound. On the other hand, again in contrast to both East andWest Africa, evidence of Haemoglobin H disease was discovered(Special Plate, Fig. 1), and the presence of the gene fora-thalassaemia was also suggested by the observation of sickle-cell trait carriers with Haemoglobin S proportions of below20 % ; in one case the unusual combination of Haemoglobin Hdisease with sickling was noted-that is, the red cells bothsickled and contained typical Haemoglobin H inclusion bodiesand on electrophoresis Haemoglobin H and Haemoglobin Swere found. The presence of a-thalassaemia in Zambia wasalso confirmed by the observation of Haemoglobin Bart's in
cord blood. As some cord bloods contain " fast " haemoglobinfractions which are derivatives of Haemoglobin F, we isolatedthe " Bart's" fraction on two occasions and confirmed bypreparing peptide chromatograms that the haemoglobins wereindeed consisting of y-chains only-that is, were HaemoglobinBart's or 74.A new observation was that in five families an a-chain
abnormal haemoglobin was discovered. In one case it wasHaemoglobin Ja Oxford (a15 Gly -> Asp), previously foundoccasionally in families of European stock. Our familybelonged to the Manyika tribe of Southern Tanzania. A com-pletely new variant was discovered in four other familiesunrelated to each other (Special Plate, Fig. 2). Three of thefamilies were of the Bemba tribe and the fourth was Tabwa.It was therefore considered appropriate to denote the newhaemoglobin as Zambia rather than Bemba.
Identification of Haemoglobin Zambia
The globin from the abnormal haemoglobin was digestedwith trypsin, and fingerprints were made in the usual way(Sick et al., 1967). The electrophoresis was done at pH. 64.Fig. 3 (Special Plate) is a photograph of the fingerprint. Thereis a new peptide near the position of a and /3TpVII. Thispeptide stains yellow-brown with ninhydrin, and it stains forhistidine. No peptide is seen to be missing.The abnormal peptide gives the following amino-acid
analysis:Amin o-acido 1 Moles Molar Ratio
Asp ... ... .. 00106 ... ... ... 1.04Gly ... ... .. 0-205 ... ... ... 2-02His. ... ... o-985 ... 0.97Lys ... ... ... O O995 ... 0-97
on 25 April 2022 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.4.5683.586 on 6 Decem
ber 1969. Dow
nloaded from

596 6 December 1969 New Haemoglobin Zambia-Barclay et al. MEDICTJISOHRNALThis analysis shows that the abnormal haemoglobin is not
Haemoglobin Norfolk, which is a57 Gly -> Asp and wouldgive a similar fingerprint, though with another new peptidein addition to the one near a and 8TpVII (Baglioni, 1962),and where in contrast to the peptide found here the abnormalpeptide would contain only one glycine residue. The analysisdoes, however, suggest that the abnormal peptide is derivedfrom aTpVII. This is consistent with the fingerprint, whichdoes not show any peptide to be absent; since a and 83TpVIIlie in the same position on fingerprints the absence of aTpVIIwould not be visible. In noxmal haemoglobin aTpVII consistsof a57-60 Gly-His-Gly-Lys. The C-terminal a60 lysyl isfollowed by another lysine residue in position 61.
In order to determine the abnormal amino-acid, the newpeptide was sequenced by the Edman-Dansyl technique (Gray,1967). This showed that in the first and third residues of thepeptide were both glycine and the fourth was aspartic acid(or, because of the electrophoretic mobility of the peptide,
asparagine). The second residue was not detected, and canbe assumed to be histidine, which does not dansylate easily.This sequence is consistent with the mutation a60 Lysine ->Asparagine. The abnormal peptide seen on the fingerprintswould be a57-61.
a 57 58 59 60 61Hb A Gly His Gly Lys t Lys4Hb Zambia.Gly His Gly Asn Lys tThe arrows indicate points of cleavage on tryptic digestion.
This new Haemoglobin Zambia (a60 Lysine -> Asparagine)may well become an important genetic marker in parts ofCentral Africa.
REFERENCES
Baglioni, C. (1962). Yournal of Biological Chemistry, 237, 69.Gray, W. R. (1967). Methods in Enzymology, 11, 469.Sick, K., et al. (1967). Biochemica et Biophysica Acta, 140, 231.
Remission Induction with Cytosine Arabinoside and L-Asparaginasein Acute Lymphoblastic Leukaemia
T. J. McELWAIN,* M.B., M.R.C.P.; R. M. HARDISTYt M.D., M.R.C.P., F.R.C.PATH.
British MedicalJournal, 1969 4, 596-598
* Leukaemia Research Fellow.t Profesor of Waemnatology.Institute of Child Health, the Hospital for Sick Children, Great Ormond
S'treet, London W.C.1.
Summary: Nine patients with acute lymphoblasticleukaemia in relapse were treated with a course of
cytosine arabinoside followed immediately by a course ofL-asparaginase. Eight patients achieved complete remis-sion of their disease. This combination of drugs issufficiently effective to suggest that further trial is needed.It is possible that the combination has a synergistic effect.
IntroductionL-Asparaginase is now established as an effective agent forinduction of remission in acute lymphoblastic leukaemia. Of67 patients treated with L-asparaginase at the Memorial Hos-pital, New York, 63% achieved complete remission. Severaldifferent treatment regimens were used, with doses of 10, 200,1,000, and 5,000 i.u./kg./day for 28 days. There was nosignificant difference between remission rates for dosagesbetween 200 and 5,000 i.u./kg./day, but unmaintained remis-sions were longer in patients who had received 1,000 and 5,000i.u./kg./day than in those who were given the lower dosages(F. L. Horsfall, personal communication, 1969). Tallal andOettgen (1968) also reported remissions in six out of eightchildren with acute lymphoblastic leukaemia, who receivedL-asparaginase in doses of 10 to 200 i.u./kg. intravenously daily,given over three to six weeks.
Experience with the use of cytosine arabinoside (Ara-C) inacute lymphoblastic leukaemia suggests that a remission rateof 20-30% is to be expected (Ellison et al., 1968; Howardet a., 1968). On the basis of experience with other drug com-bhnations in acute lymphoblastic leukaemia it might be hopedthat higher remission rates could be obtained with a combina-tion of Ara-C and L-asparaginase. This is similar to the experi-ence of Burchenal (1969) in mice with leukaemia EARAD, ; he
found that remission rates were higher with Ara-C andL-asparaginase together than when either drug was used alone.We have treated a small series of patients with a course of
Ara-C followed immediately by a course of L-asparaginase, andthough the number of patients is too small to draw any definiteconclusions, preliminary results suggests that this is a highlyeffective combination for remission induction.
Patients and Methods
Nine patients aged 2 to 11 years with acute lymphoblasticleukaemia were treated. All had previously received other anti-leukaemic drugs and were in a second or subsequent relapseexcept Case 1, who had relapsed for the first time (see Table I).At the time of relapse seven patients had between 12 5 and94 5% of leukaemic cells in the bone marrow; of the othertwo, whose marrow was not examined at this stage, one had60,000 and the other 13,000 leukaemic cells/cu. mm of peri-pheral blood.Treatment was started with Ara-C 3 mg./kg. intravenously
daily. The course ranged from 5 to 14 injections given over5 to 24 days. Bone marrow was examined at the end of thecourse of Ara-C, and treatment with L-asparaginase 1,000 i.u./kg. intravenously daily was then started. In none of thepatients did the bone marrow show less than 10% leukaemiccells at the end of the course of Ara-C.Two types of L-asparaginase were used: Escherichia coli
material supplied by Farbenfabriken Bayer A.G. (Cases 1 to 7)and Erwinia carotovorurn material from the MicrobiologicalResearch Establishment, Porton Down, Salisbury (Cases 8and 9). L-Asparaginase was given for 9 to 28 days, treatmentbeing continued until there was a sustained rise in the patients'neutrophil and platelet counts. The bone marrow was thenre-examined and if it showed remission L-asparaginase was dis-continued. Full supportive therapy with packed red cells,platelet-rich plasma, and antibiotics was given whenever indi-cated during the course of treatment with Ara-C andCL-asparaginase.
on 25 April 2022 by guest. P
rotected by copyright.http://w
ww
.bmj.com
/B
r Med J: first published as 10.1136/bm
j.4.5683.586 on 6 Decem
ber 1969. Dow
nloaded from











![THE ASSAM REORGANISATION (MEGHALAYA) ACT, 1969 … · THE ASSAM REORGANISATION (MEGHALAYA) ACT, 1969 ACT NO. 55 OF 1969 [29th December, 1969.] An Act to provide for the formation](https://static.fdocuments.us/doc/165x107/5eba9879e5f87e2dcb5aad91/the-assam-reorganisation-meghalaya-act-1969-the-assam-reorganisation-meghalaya.jpg)





