58654960 case-study-acute-mi
70
I. INTRODUCTION A.) OVERVIEW OF THE STUDY Acute myocardial infarction (MI) is defined as death or necrosis of myocardial cells. It is a diagnosis at the end of the spectrum of myocardial ischemia or acute coronary syndromes. Myocardial infarction occurs when myocardial ischemia exceeds a critical threshold and overwhelms myocardial cellular repair mechanisms that are designed to maintain normal operating function and hemostasis. Ischemia at this critical threshold level for an extended time period results in irreversible myocardial cell damage or death. Critical myocardial ischemia may occur as a result of increased myocardial metabolic demand and/or decreased delivery of oxygen and nutrients to the myocardium via the coronary circulation. An interruption in the supply of myocardial oxygen and nutrients occurs when a thrombus is superimposed on an ulcerated or unstable atherosclerotic plaque and results in coronary occlusion. A high-grade (> 75%) fixed coronary artery stenosis due to atherosclerosis or a dynamic stenosis associated with coronary vasospasm can also limit the supply of oxygen and nutrients and precipitate an MI. Conditions associated with increased myocardial metabolic demand include extremes of physical exertion, severe hypertension 1
-
Upload
homeworkping3 -
Category
Education
-
view
518 -
download
0
Transcript of 58654960 case-study-acute-mi

I. INTRODUCTION
A.) OVERVIEW OF THE STUDY
Acute myocardial infarction (MI) is defined as death or necrosis of
myocardial cells. It is a diagnosis at the end of the spectrum of myocardial
ischemia or acute coronary syndromes. Myocardial infarction occurs when
myocardial ischemia exceeds a critical threshold and overwhelms myocardial
cellular repair mechanisms that are designed to maintain normal operating
function and hemostasis. Ischemia at this critical threshold level for an extended
time period results in irreversible myocardial cell damage or death.
Critical myocardial ischemia may occur as a result of increased myocardial metabolic demand and/or decreased delivery of oxygen and nutrients to the myocardium via the coronary circulation. An interruption in the
supply of myocardial oxygen and nutrients occurs when a thrombus is
superimposed on an ulcerated or unstable atherosclerotic plaque and results in
coronary occlusion. A high-grade (> 75%) fixed coronary artery stenosis due to
atherosclerosis or a dynamic stenosis associated with coronary vasospasm can
also limit the supply of oxygen and nutrients and precipitate an MI. Conditions
associated with increased myocardial metabolic demand include extremes of
physical exertion, severe hypertension (including forms of hypertrophic
obstructive cardiomyopathy), and severe aortic valve stenosis. Other cardiac valvular pathologies and low cardiac output states associated with a
decreased aortic diastolic pressure, which is the prime component of coronary
perfusion pressure, can also precipitate MI
Myocardial infarction can be subcategorized on the basis of anatomic,
morphologic, and diagnostic clinical information. From an anatomic or
morphologic standpoint, the two types of MI are transmural and nontransmural. A
transmural MI is characterized by ischemic necrosis of the full thickness of the
1
affected muscle segment(s), extending from the endocardium through the
myocardium to the epicardium. A nontransmural MI is defined as an area of
ischemic necrosis that does not extend through the full thickness of myocardial
wall segment(s). In a nontransmural MI, the area of ischemic necrosis is limited
to either the endocardium or the endocardium and myocardium. It is the
endocardial and subendocardial zones of the myocardial wall segment that are
the least perfused regions of the heart and are most vulnerable to conditions of
ischemia. An older subclassification of MI, based on clinical diagnostic criteria, is
determined by the presence or absence of Q waves on an electrocardiogram
(ECG). However, the presence or absence of Q waves does not distinguish a
transmural from a non-transmural MI as determined by pathology
A more common clinical diagnostic classification scheme is also based on
ECG findings as a means of distinguishing between two types of MI—one that is
marked by ST elevation and one that is not. The distinction between an ST-
elevation MI and a non-ST-elevation MI also does not distinguish a transmural
from a non-transmural MI. The presence of Q waves or ST segment elevation is
associated with higher early mortality and morbidity; however, the absence of
these two findings does not confer better long-term mortality and morbidity.
The most common etiology of MI is a thrombus superimposed on a
ruptured or unstable atherosclerotic plaque.
.
Myocardial infarction is the leading cause of death in the United States
(US) as well as in most industrialized nations throughout the world.
Approximately 800,000 people in the US are affected and in spite of a better
awareness of presenting symptoms, 250,000 die prior to presentation to a
hospital.4 The survival rate for US patients hospitalized with MI is approximately
90% to 95%. This represents a significant improvement in survival and is related
to improvements in emergency medical response and treatment strategies.
2
In general, MI can occur at any age, but its incidence rises with age. The
actual incidence is dependent upon predisposing risk factors for atherosclerosis,
which are discussed below. Approximately 50% of all MI's in the US occur in
people younger than 65 years of age. However, in the future, as demographics
shift and the mean age of the population increases, a larger percentage of
patients presenting with MI will be older than 65 years
B.) OBJECTIVES OF THE STUDY
The main reason and purpose student nurses conduct care study and
exposure in the clinical area is for them to identify problems encountered by the
clients; this is one of their tools of learning knowledgeably and skillfully.
We, as health care providers, it is indeed our vocation to adjoined hands
w/ the health team for the promotion of wellness of our clients. Our main
objectives for this study are the following:
To identify the chief complaints and admitting diagnosis of our patient so
that we can give specific nursing interventions.
To determine the family and personal health history of our patient that
may affect present health condition
To identify the cause and effect of the main problem through a correct
analysis of the pathophysiology of the case.
To determine the medical management given through identifying the
significant implication of the laboratory and diagnostic examinations
ordered as well as the medical orders and its rationale.
To make a nursing care plan for the different health problems
encountered by the client.
To establish an ideal plan of care for a specific diagnosis or problem of
the client.
3

To evaluate the effectiveness of the actual nursing care plan that was
established.
To impart health teachings to the client giving emphasis on his
medications, exercises, treatment, out- patient follow- up and diet
To give referrals and follow-up for the health promotion of the client.
In general, this study aims to enhance the skills and knowledge of the
students in providing holistic care to the patient. Students logically search further
knowledge in order to attain the desired goal and intervention for the wellness of
the patient.
C.) SCOPE AND LIMITATION
Prior to the day of duty, the group has already chosen a patient for care
study. They performed a physical assessment to the patient to properly identify
the nursing problems, which require necessary and direct interventions and
medical regimen. The study on medications and doctor’s order were limited to
our chosen patient
The preventive care and anticipatory guidance are integral to nursing
practice. Thus, this care study focuses on the particular case of the patient. Since
the patient’s diagnosis is more on cardiovascular disease, the group has focused
on acute myocardial infarction as one of his admitting diagnosis. However, the
group did not just limit the interventions on monitoring cardiac activity of the
patient. Any symptoms and unusualties were kept watch and monitored. Any
Referrals and follow-up, so as with the nursing management were fully granted
and analyzed for the said case.
Supposedly, this case study should be focused on Gynecology concept
but due to the unavailability and presence of gyne patient in Cagayan de Oro
Polymeric General Hospital, the concept is focused on medical from Station 7.
4
The care for our chosen patient is only limited for 2 days of duty excluding the
physical assessment done prior to the day of duty.
II. HEALTH HISTORY
A.) PATIENT’S PROFILE
Name of Patient: ?
Sex: Male
Age: 64 years old
Religion: Roman Catholic
Civil Status: Married
Occupation: ?
Income: P 6,000/ month
Nationality: Filipino
Date Admission: June 29, 2007
Time: 09:40 pm
BASELINE VITAL SIGNSTemperature: 36.6 C
Pulse Rate: 54 bpm
Respiratory rate: 18 cpm Blood Pressure: 130/100 mmHg
Height: 5’3’’
Weight: 55.5 kgs
Chief complaints: epigastric pain
Admitting Diagnosis: Acute myocardial infarction;
Hypertensive cardiovascular disease;
ruled out PUD; diabetic neprhopathy
Attending Physician: Dr. Alenton
5
B.) FAMILY AND PERSONAL HEALTH HISTORY
?, 64-year-old, male, a resident of ? has a critical health problem. He said
that he was an alcohol drinker during his adolescence and late adulthood and
confessed that he only drinks 2-6 glasses even more on occasional basis;
however, he has no history of cigarette smoking. At fist, he experienced
hypertension in the year 1998 when he was still 55 years old. On the year 2006,
because of over workload and emotional stress, Mr. Agustin has experienced
severe chest pain and that same year he was diagnosed of having Diabetes
Nephropathy and Chronic Renal Insufficiency and was admitted at Northern
Mindanao Medical Center. During his admission last 2006, Mr. Sarmiento has
been transfused with 5 bags of Packed Red Blood Cell and there were no reports
of allergic reaction. At that time, he was advised by the doctor to have his
monthly check-up for his health problems.
According to the patient’s wife, there is no history of health problems from
their family. Nobody aside from Mr. Agustin Sarmiento has been admitted for
chronic illness. His children were neither non-smoker nor alcoholic but they do
drink alcohol occasionally Although there were presence of minor illnesses
before like cough, colds, LBM but they were able to catch on the treatment
regimen as a home care management.
6
C.) CHIEF COMPLAINT AND HISTORY OF PRESENT ILLNESS
On the 29th of June, Mr. ? has experienced chest pain with complaints of
acute epigastric pain, growing in character and on and off. The patient was
anorexic and hypertensive (180/ 60 mm Hg). With the help of his family he went
to the hospital for check-up, they thought that it was just an ulcer, but the doctor
came out to have a diagnosis of Acute myocardial infarction; Hypertensive
cardiovascular disease; ruled out PUD; diabetic neprhopathy, and due to the
severity of pain he was prompted for admission in the Polymedic General
Hospital.
III. DEVELOPMENTAL STATUS
ROBERT HAVIGHURST’S DEVELOPMENTAL TASK THEORY
Later Maturity (60 y.o- )
The fact that man learns his way through life is made radically clear by
consideration of the learning tasks of older people. They still have new
experiences ahead of them, and new situations to meet. At age sixty-five when a
man often retires from his occupation, his changes are better than even of living
another ten years. During this time the man or his wife very likely will experience
several of the following things: decreased income, moving to a smaller house,
loss of spouse by death, a crippling illness or accident, a turn in the business
cycle with a consequent change of the cost of living. After any of these events
the situation may be so changed that the old person must learn new ways of
living.
The developmental tasks of later maturity differ in only one fundamental respect
from those of other ages. They involve more of a defensive strategy--of holding
on the life rather than of seizing more of it. In the physical, mental and economic
7

spheres the limitations become especially evident; the older person must work
hard to hold onto what he already has. In the social sphere there is a fair chance
of offsetting the narrowing of certain social contacts and interests by the
broadening of others. In the spiritual sphere there is perhaps no necessary
shrinking of the boundaries, and perhaps there is even a widening of them.
Our patient Agustin Sarmiento is already at the later maturity stage. At
his age he will be adjusting in decreasing physical strength and health, adjusting
to retirement and reduced income, adjusting to death of spouse, establishing an
explicit affiliation with one's age group, meeting social and civic obligations,
establishing satisfactory physical living arrangements: The principal values that
older people look for in housing, according to studies of this matter, are: quiet,
privacy, independence of action, nearness to relatives and friends, residence
among own cultural group, closeness to transportation lines and communal
institutions like libraries, shops, movies, churches, etc.
ERIK ERICKSON’S PSYCHOSOCIAL STAGES OF DEVELOPMENT
Ego Integrity vs Despair (65-)Erik Erikson adapted and expanded Freud’s theory of development to
include the entire life span, believing that people continue to develop throughout
life. He describes eight stages of development. Erikson envisions life as a
sequence of levels of achievement. Each stage signals a task that must be
achieve. The resolution of the task can be complete, partial or unsuccessful.
Erikson believes that the greater the task achievement, the healthier the
personality of the person; failure to achieve the task influences the person’s
ability to achieve the new task. This developmental task can be viewed as a
series of crisis and successful resolution of this crisis and successful resolution of
these crisis is supportive to the person’s ego failure to resole the crisis is
damaging to the ego.
8
Our patient Agustin Sarmiento belongs to the older adult stage. His
central task is Ego Integrity versus Despair. Ego integrity is the ego's
accumulated assurance of its capacity for order and meaning. Despair is signified
by a fear of one's own death, as well as the loss of self-sufficiency, and of loved
partners and friends. He must learn to accept the life that he has led (good and
bad) to have a life in facing death. As he learns to live with his choices and the
certainty of death, he fined a inner-strength to go on with integrity. Some despair
is inevitable, a he mourn his own deaths. When he recognizes all that he have
been, are and will be, then we show his wisdom.
KOHLBERG’S STAGES OF MORAL DEVELOPMENT
Post conventional (Universal Ethical and Principle Orientation
Lawrence Kohlberg’s theory specifically addresses moral development in
children and adults. The morality of an individual’s decision was not Kohlberg’s
concern; rather he focused on the reasons of an individual makes a decision.
According to Kohlberg, moral development progress to three levels and six
stages. At Kohlberg first level, called the premolar or preconventional level,
children are responsive to cultural rules and labels of good and bad, right and
wrong. However, children interpret these terms of the physical consequence of
their action, that is, punishments or reward. At the second level, the conventional
level, the individual is concerned about maintaining the expectation of the family,
group or nation and sees this is right. The emphasis at third level is conformity
and loyalty to one’s own expectation as well as society’s. level three is called the
post conventional, autonomous or principal level. At this level people make an
effort to define valid values and principles without regard to outside authority or to
the expectation of others.
Our patient Agustin Sarmiento belongs to the Post Conventional level
and on the Universal Ethical principle orientation stage. His decisions and
behaviors re based on internalized rules, on conscience rather than social laws,
9

and on self- chosen ethical and abstract principles that are universal,
comprehensive and consistent.
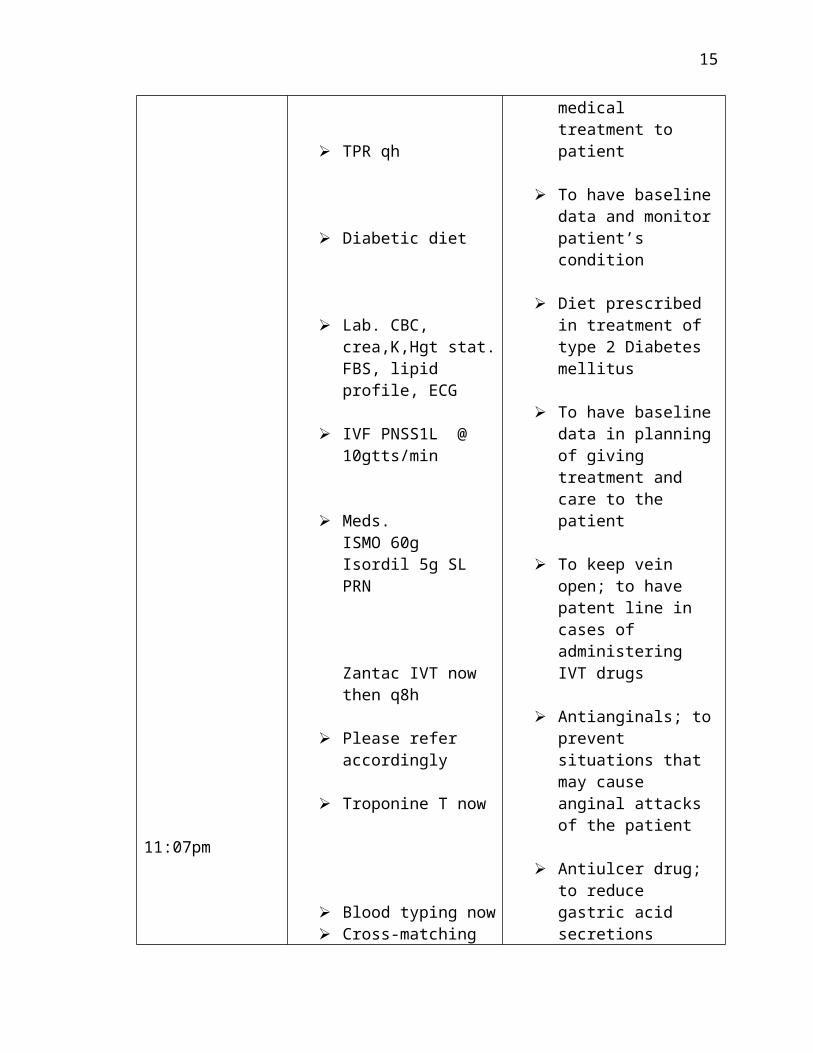
IV. MEDICAL MANAGEMENTA.) DOCTOR’S ORDER
DATE DOCTOR’S ORDER RATIONALE
June 29, 20079:50pm
Hgt:188mgs/dL
BP: 180/60mmHg
HR:92bpm
Please admit under the serviceof Dr. Alenton
Secure consent to care
TPR qh
Diabetic diet
Lab. CBC, crea,K,Hgt stat.FBS, lipid profile, ECG
IVF PNSS1L @ 10gtts/min
Meds. ISMO 60gIsordil 5g SL PRN
Zantac IVT now then q8h
For proper monitoring of the patient’s condition
To have consent in rendering medical treatment to patient
To have baseline data and monitor patient’s condition
Diet prescribed in treatment of type 2 Diabetes mellitus
To have baseline data in planning of giving treatment and care to the patient
To keep vein open; to have patent line in cases of administering IVT drugs
Antianginals; to prevent situations that may cause anginal attacks of the patient
Antiulcer drug; to reduce gastric acid secretions
10
11:07pm
June 30,200711:00am
2:55pmBP:180/100mmHg
8:00pm
Please refer accordingly
Troponine T now
Blood typing now Cross-matching now
Transfuse 2’U’ PRBC
Repeat ECG in AM
Tramadol 50mg IVT now
Pantoprazole (Ulcepraz) 40g IVT OD,start now
Please give captopril 25mg tab SL now
Get BP & HR after 15 minutes
Tramadol 50mg IV now then PRN
Arixtra 25mg SC now then OD
Plavix 75mg 4 tabs now then 1tab OD
To measure levels of cardiac troponins
To determine blood type of the patient & the presence of ABO and Rh factor
For blood replacement
For continued surveillance of the heart’s electrical activity
Relieve of moderate to severe pain
Inhibits proton pump activity thus suppresses gastric acid secretion
To lower down BP of the patient
To determine the effectivity of the medication (captopril)
Relieve of moderate to severe pain
Anticoagulant drug; to maintain arterial patency
To reduce the thrombotic events in patient with
11
July 1. 2007
July 2, 200712:20am BP: 190/90mmHg
10:25amBP: 160/80mmHg
HR: 88bpm
BP: 200/80mmHg
O2 inhalation 2L/min
Repeat ECG in AM
VS qh & record
Lipitor 1 tab OD start tonight
CBC after 2’U’ PRBC
Give captopril 25mg tab SL now, T.O. Dr. Taboclaon
Give captopril 25mg SL now, T.O.
Dr. Espina
IVF PNSS1L @ 10gtts/min
Give captopril 25mg
atherosclerosis
Increases myocardial oxygen supply & relieves pain
For continued surveillance of the heart’s electrical activity
To monitor the health status of the patient & have baseline data in giving medications
Adjunct to diet to reduce LDL cholesterol, total cholesterol, and to increase HDL cholesterol of the patient
To determine the level of the blood components of the patient after transfusion
Antihypertensive drug; to lower the BP of the patient
Antihypertensive drug; to lower the BP of the patient
To keep vein open; to have patent line in cases of administering IVT drugs
Antihypertensive drug;
12
HR: 94bpm
July 3, 2007BP: 200/110mmHg
12:50pm
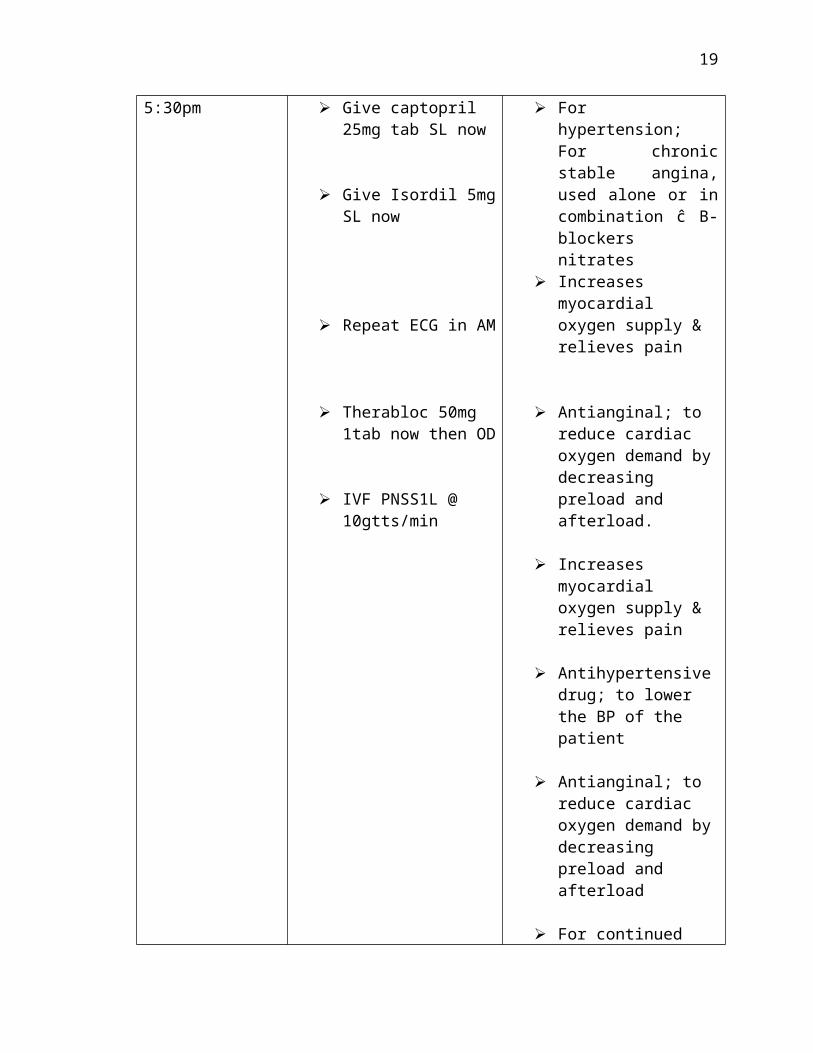
5:30pm
tab SL now
Bepridil (Vascor) 10 mg. 1 tab now then OD P.O.
O2 inhalation 2l/min
Give Isordil 5mg tab SL for 3 doses q 5 minutes if chest pain is not relieved
Increase O2 inhalation to 4L/min
Give captopril 25mg tab SL now
Give Isordil 5mg SL now
Repeat ECG in AM
Therabloc 50mg 1tab now then OD
IVF PNSS1L @ 10gtts/min
to lower the BP of the patient
For hypertension; For chronic stable angina, used alone or in combination ĉ B-blockers nitrates
Increases myocardial oxygen supply & relieves pain
Antianginal; to reduce cardiac oxygen demand by decreasing preload and afterload.
Increases myocardial oxygen supply & relieves pain
Antihypertensive drug; to lower the BP of the patient
Antianginal; to reduce cardiac oxygen demand by decreasing preload and afterload
For continued surveillance of the heart’s electrical activity
Antihypertensive drug; to lower the BP of the patient
To keep vein open; to have patent line in cases of administering IVT drugs
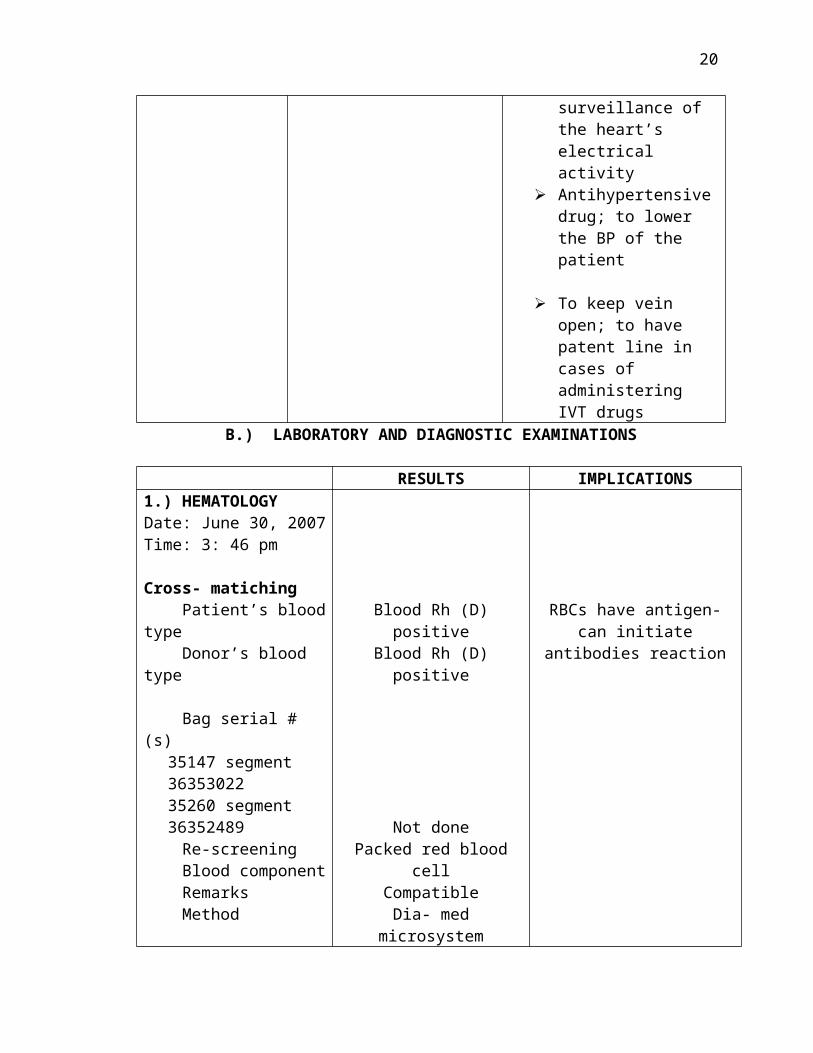
B.) LABORATORY AND DIAGNOSTIC EXAMINATIONS
13

RESULTS IMPLICATIONS1.) HEMATOLOGYDate: June 30, 2007Time: 3: 46 pm
Cross- matiching Patient’s blood type Donor’s blood type
Bag serial # (s)35147 segment 3635302235260 segment36352489
Re-screening Blood component Remarks Method
Blood Rh (D) positiveBlood Rh (D) positive
Not donePacked red blood cell
CompatibleDia- med microsystem
RBCs have antigen- can initiate antibodies reaction
RESULTS REFERENCE VALUES
IMPLICATIONS
1.) BLOOD CHEMISTRYDate: June 30, 2007Time: 5:00 am
Lipid Profile Triglycerides
HDL
LDL
221.64 mgs/dl
28.39 mgs/dl
166.01 mgs/dl
44.33 mgs/dl
<200.00
30.00 – 85.00
<150.00
0.00- 40.00
Increased- Risk of atherosclerotic occlusive coronary diseases and peripheral vascular diseaseDecreased- HDL cholesterol is lower in patients with increased risk for coronary heart disease Increased- higher in patients with increased risk for coronary heart disease
14
VLDL
Fasting blood sugar
106.18 mgs/dl
.
70.00- 99.00
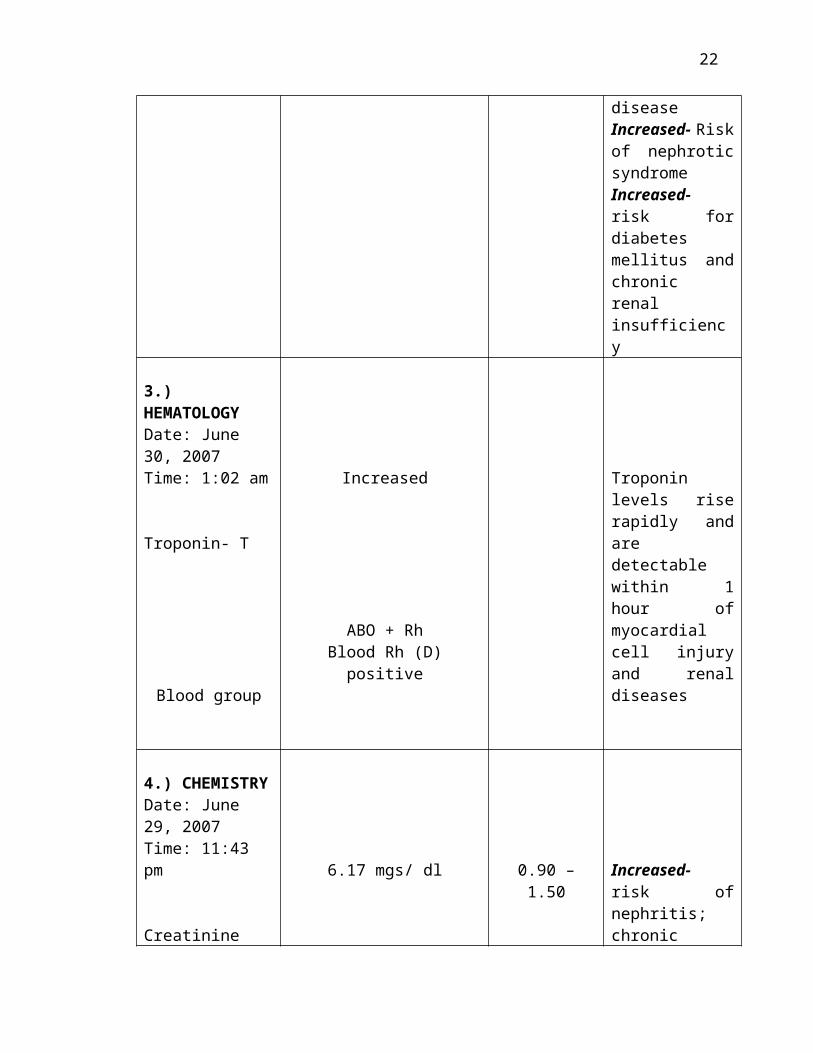
Increased- Risk of nephrotic syndromeIncreased- risk for diabetes mellitus and chronic renal insufficiency
3.) HEMATOLOGYDate: June 30, 2007Time: 1:02 am
Troponin- T
Blood group
Increased
ABO + RhBlood Rh (D) positive
Troponin levels rise rapidly and are detectable within 1 hour of myocardial cell injury and renal diseases
4.) CHEMISTRYDate: June 29, 2007Time: 11:43 pm
Creatinine6.17 mgs/ dl 0.90 – 1.50 Increased- risk
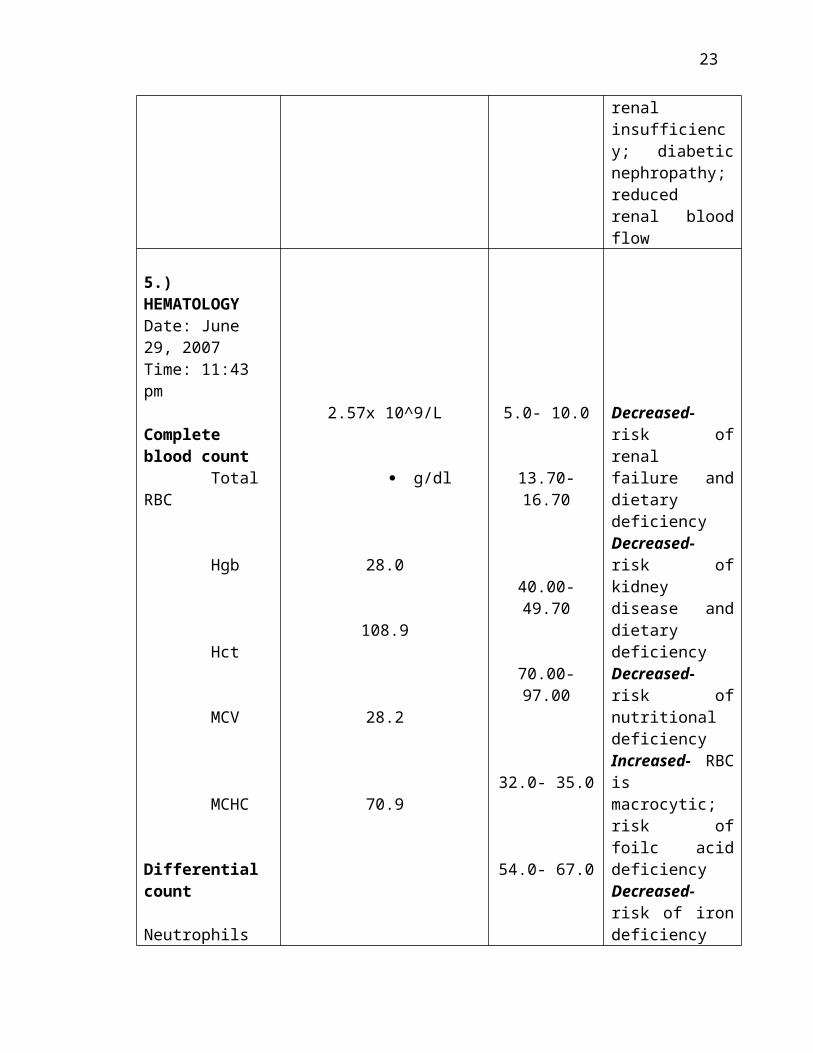
of nephritis; chronic renal insufficiency; diabetic nephropathy; reduced renal blood flow
5.) HEMATOLOGYDate: June 29, 2007Time: 11:43 pm
Complete blood count Total RBC
2.57x 10^9/L 5.0- 10.0 Decreased- risk of renal failure and dietary
15

Hgb
Hct
MCV
MCHC
Differential count Neutrophils
g/dl
28.0
108.9
28.2
70.9
13.70- 16.70
40.00- 49.70
70.00- 97.00
32.0- 35.0
54.0- 67.0
deficiencyDecreased- risk of kidney disease and dietary deficiencyDecreased- risk of nutritional deficiencyIncreased- RBC is macrocytic; risk of foilc acid deficiencyDecreased- risk of iron deficiency anemia
Increased- acute bacterial infection, physical or emotional stress
6.) HEMATOLOGYDate: July 1, 2007Time: 6: 36 pm
Complete Blood Count Total RBC
Hgb
Hct
Differential count Neutrophils
3.49 x10^ 9/L
11.1 g/dl
32.5
66.0
15.4
3.69- 5.90
13.70- 16.70
40.0- 49.70
54.0- 62.0
20.0- 40.0
Decreased- risk of renal failure; dietary deficiencyDecreased- risk of dietary deficiency and kidney diseaseDecreased- risk of nutritional deficiency
Increased- acute bacterial infection; physical or emotional stress
16

Lymphocytes
Monocytes
13.1 4.0- 10.0 Increased- viral infectionIncreased- viral infection; other chronic disease
17

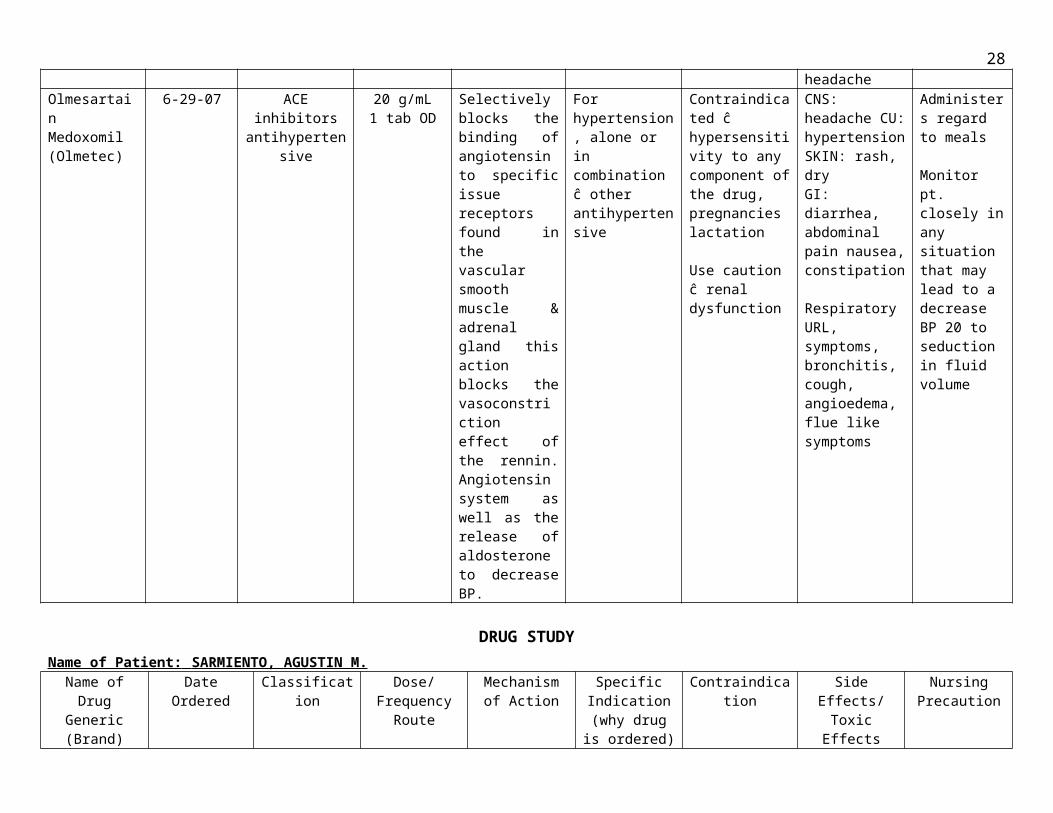
C.) DRUG STUDYName of Patient: SARMIENTO, AGUSTIN M.Name of Drug
Generic (Brand)
DateOrdered
Classification Dose/Frequency
Route
Mechanism of Action
Specific Indication
(why drug is ordered)
Contraindication Side Effects/Toxic Effects
Nursing Precaution
Isosorbide dinitrale (Isordil)
7-2-07 Antianginals 5 mg tabSL for 3
doses every 5minutes if
chest pain is not relieved
Thought to reduce cardiac oxygen demand by decreasing preload & afterload: also, may increase blood flow through the collateral coronary vessels
Acute anginal attacks
Contraindicated potentials ĉ hypersensitivity or idiosyncrasy to nitrates & in those ĉ severe hypolension
Flushing, vascular headache, cerebral ischemia associated ĉ postural hypotension, N/V weakness, restless, pallor, persipiration & collapse
To prevent tolerance a nitrate-free interval of 8 to 12 hours per day is recommended.
Bepridil(Vascor)
7-2-07 Calcium Channel Blocker
Antianginal Antihypertensive
10 mg. 1 tab now then OD
P.O.
Inhibits calcium ion influx across cell membrane during cardiac depolarization, produces, relaxation of coronary vascular muscle diseases coronary vascular arteries, myocardial 02
delivery in pts ĉ vasospastic angina SA/AV node conduction inhibits fast sodium current.
Hypertension For chronic stable angina, used alone or in combination ĉ B-blockers nitrates
Pts. ĉ history of angineurotic edema & other allergic reactions due to ACE inhibitors: pregnancy lactation
Rarely: fatigue, dizziness, hot-flush, diarrhea, nausea, vomiting Discomfort in the throat, non-productive cough, palpitation headache & rash
CHF, hypotension, hepatic injury, pregnancy C, lactation, renal disease, concomitant B-blocker therapy
18
DRUG STUDY
Name of Patient: SARMIENTO, AGUSTIN M.
Name of DrugGeneric (Brand)
DateOrdered
Classification Dose/Frequency
Route
Mechanism of Action
Specific Indication
(why drug is ordered)
Contraindication Side Effects/Toxic Effects
Nursing Precaution
RanitidineHydrochloride(Zantac)
6-29-079:45 pm
Anti-ulcer drug 50 mg IV q 8H
6-2-10
Completely inhibits action of histamine on the H2 at receptors sites of parietal cells, decreasing gastric acid secretion
NSAID-associated peptic ulceration
Contraindicated in patients hypersensitive to drug and those ĉ acute porphyria acute dosage in pt. ĉ impaired renal function
Occasionally, reversible hepatitis. Rarely agranulocytosis, acute pancreatic, hypersensitivity, reversible mental confusion, skin rash; headache
Assess pt. for abdominal pain. Note presence of blood in emesis, stool or gastric aspirate
Olmesartain Medoxomil (Olmetec)
6-29-07 ACE inhibitors antihypertensive
20 g/mL1 tab OD
Selectively blocks the binding of angiotensin to specific issue receptors found in the vascular smooth muscle & adrenal gland this action blocks the vasoconstriction effect of the rennin. Angiotensin system as well as the release of aldosterone to decrease BP.
For hypertension, alone or in combination ĉ other antihypertensive
Contraindicated ĉ hypersensitivity to any component of the drug, pregnancies lactation
Use caution ĉ renal dysfunction
CNS: headache CU: hypertension SKIN: rash, dry GI: diarrhea, abdominal pain nausea, constipation
Respiratory URL, symptoms, bronchitis, cough, angioedema, flue like symptoms
Administers regard to meals
Monitor pt. closely in any situation that may lead to a decrease BP 20 to seduction in fluid volume
DRUG STUDY
19
Name of Patient: SARMIENTO, AGUSTIN M. Name of Drug
Generic (Brand)
DateOrdered
Classification Dose/Frequency
Route
Mechanism of Action
Specific Indication
(why drug is ordered)
Contraindication Side Effects/Toxic Effects
Nursing Precaution
tramadol HCI(Dolmal)
6-30-07 Opioid Analgesics
50 mg IV now then PRN for moderate to severe pain
A centrally acting synthetic analgesic compound not chemically related to opioid. Thought to bind to opioid receptors & of norepinephrine & serotonin
For moderate to severe pain
Contraindicated in patients hypersensitive to drug or other opioids, in breast feeding women and in those ĉ acute intoxication from alcohol use cautiously in pts. at risk for renal or hepatic impairment
Respiratory depression, palpitations, chills, chest pain, decrease in BP, arrhythmia, vomiting, nausea, GI distention, borborygymi, urticaria, excessive bronchial secretions
Releases pt’s level of pain at least 30 min. after administration. Monitor CV and respiratory status w/hold dose & notify prescribe if RR is below 12 cm. Monitor bowel & bladder function anticipate need for laxative for better analgesic effect give drug before onset of pain.
pantoprazole sodium(ulcepraz)
6-30-07 Antiulcer drugs
40 mg IV OD(-6)
Inhibits proton pump activity by finding to hydrogen potassium oderosine triphosphatase, located at secretory surface of gastric parietal cells, to suppress gastric acid secretion
Doudenal & gastric ulcer in combination ĉ 2 appropriate antibiotics for the reduction of H Pylon in pts. ĉ peptic ulcer of the objective of reducing the recurrence of duodemal are unknown
Contraindicated in pts. hypersensitive to any component of the formulation safety & efficacy of using the IV for mutation to start, therapy for GERD are unknown.
Headache, diarrhea, rarely, nausea, upper abdominal pain, flatulence, skin rash, pruritus or dizziness, edema, fever, onset of depression & disturbance in vision
Stop treatment ĉ IV pantoprazole when P.O. form is warranted drug can’t be given regard to meals symptomatic response to therapy doesn’t preclude the presence of gastric malignancy.
20

DRUG STUDY
Name of Patient: SARMIENTO, AGUSTIN M.
Name of DrugGeneric (Brand)
DateOrdered
Classification Dose/Frequency
Route
Mechanism of Action
Specific Indication
(why drug is ordered)
Contraindication Side Effects/Toxic Effects
Nursing Precaution
captopril(Capoten)
7-2-07 Antihypertensive 1. 25 mg Tab SL now 12:10 pm
2. 25 mg ½ tab SL now
Inhibits ACE, preventing conversion of Angiotensin II, a potent vasoconstrictor less angiotensin II decreasing aldosterone secretion, which reduces sodium & water retention & lowers blood pressure.
Hypertension diabetic nephropathy
Contraindicated in pts. hypersensitive to drug or ACE inhibitors use cautiously in pts. ĉ impaired renal function
CNS: dizziness fatigue; rash, pruritus, flushing, angioedema, loss of taste perception; stomatitis, GI irritation & abdominal pain; leucopenia; cough
Monitor patient’s blood pressure & pulse rate frequently elderly pts may be moiré sensitive to drug’s hypotensive effects in patients ĉ impaired renal function or collagen vascular disease, monitor WBC and differential counts before starting treatment, every 2 wks for the first 3 months of therapy and periodically thereafter.
21
DRUG STUDY
Name of Patient: SARMIENTO, AGUSTIN M.
Name of DrugGeneric (Brand)
DateOrdered
Classification Dose/Frequency
Route
Mechanism of Action
Specific Indication
(why drug is ordered)
Contraindication Side Effects/Toxic Effects
Nursing Precaution
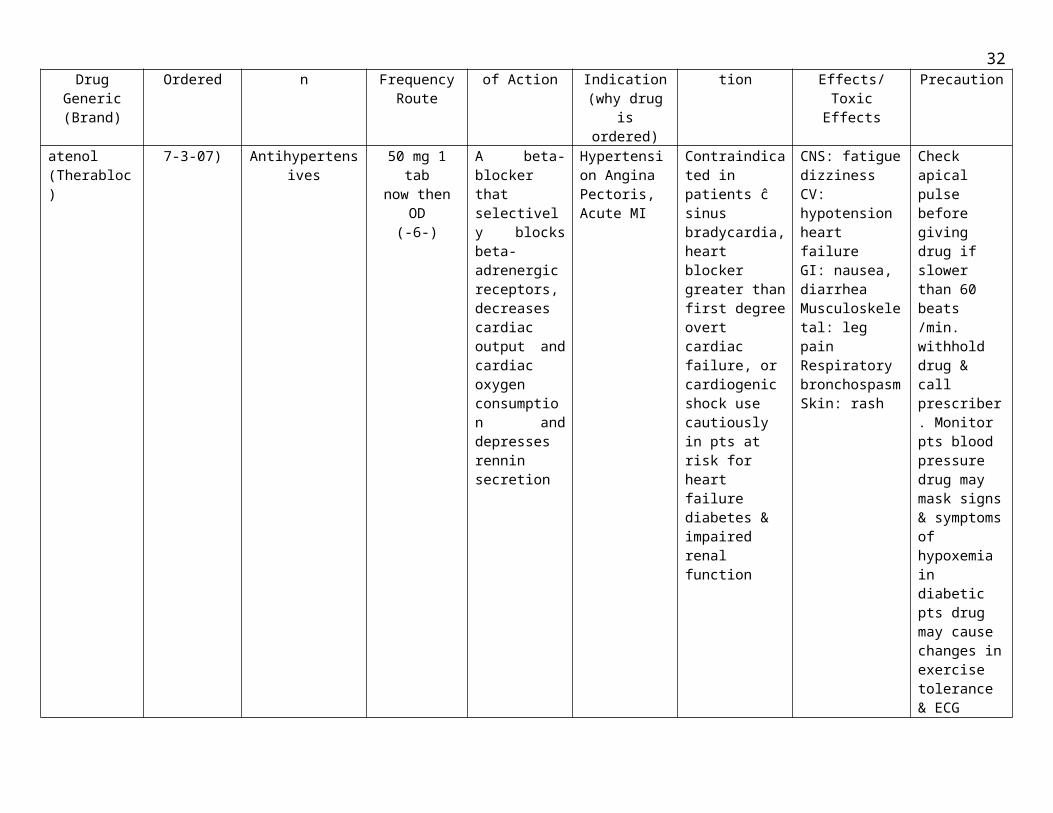
atenol (Therabloc)
7-3-07) Antihypertensives 50 mg 1 tabnow then OD
(-6-)
A beta-blocker that selectively blocks beta-adrenergic receptors, decreases cardiac output and cardiac oxygen consumption and depresses rennin secretion
Hypertension Angina Pectoris, Acute MI
Contraindicated in patients ĉ sinus bradycardia, heart blocker greater than first degree overt cardiac failure, or cardiogenic shock use cautiously in pts at risk for heart failure diabetes & impaired renal function
CNS: fatigue dizziness CV: hypotension heart failure GI: nausea, diarrheaMusculoskeletal: leg pain Respiratory bronchospasm Skin: rash
Check apical pulse before giving drug if slower than 60 beats /min. withhold drug & call prescriber. Monitor pts blood pressure drug may mask signs & symptoms of hypoxemia in diabetic pts drug may cause changes in exercise tolerance & ECG
22
DRUG STUDYName of Patient: SARMIENTO, AGUSTIN M.Generic name
of Ordered Drug
Brand Name
Date Ordered Classification Dose/Frequency/
Route
MechanismOf
Action
Specific Indication
Contra-Indication
SideEffects/Toxic
Effects
NursingPrecaution
Senna Senokot 7-3-07 Laxatives 2 tabstonight -9 pm
Stimulant laxative that increases peristalsis, probably by relaxing the effect on smooth muscle of the intestine. Drug also promotes fluids accumulation in colon and small intestine.
Acute constipation preparation, for bowel elimination
Contraindicated in pts. ĉ ulceration bowel lesions, fecal infaction, S/sx of appendicitis, acute surgical abdomen, N/V abdominal pain
GI: nausea, abdominal crampsGU: red-pink discoloration in alkaline urine, yellow brown discoloration in acid urine
Before giving drug for constipation determine whether pt. has adequate fluid intake exercise & dietLimit diet to clear liquids after X-prep liquid is taken.
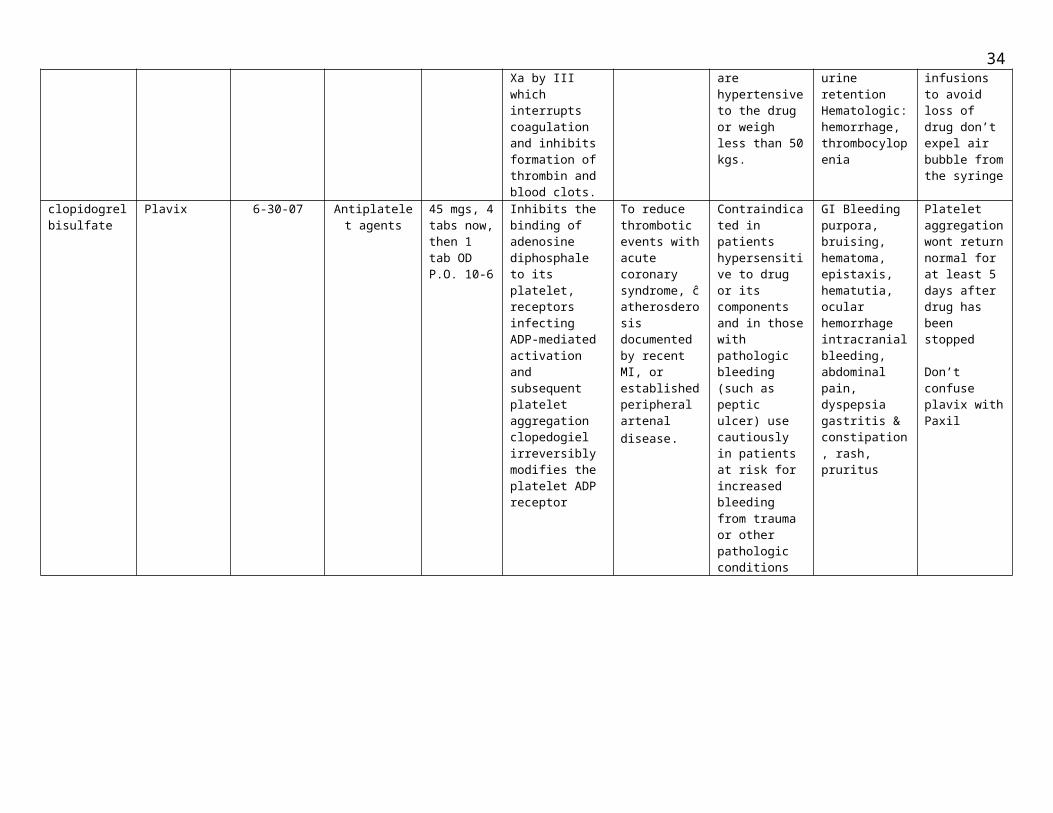
fondaparimuxsodium
Arixtra 6-30-07 Anticoagulants 2.5 mgs SC now then OD 9 pm-8 am
Binds to antithrombin III (at-III) and potentates the neutralization of factor Xa by III which interrupts coagulation and inhibits formation of thrombin and blood clots.
To prevent deep-vein thrombosis (VDT) w/c may lead to acute pulmonary embolism
Contraindicated in pts with creatirine clearance less than 30 mL/min. and in those who are hypertensive to the drug or weigh less than 50 kgs.
CNS: fever, dizziness, confusionCU: hypotension, edemaGI: nauseaGU: UTI, urine retentionHematologic: hemorrhage, thrombocylopenia
Give by S.C. injection only never I.M. Don’t mix ĉ other injections or infusions to avoid loss of drug don’t expel air bubble from the syringe
clopidogrelbisulfate
Plavix 6-30-07 Antiplatelet agents
45 mgs, 4 tabs now, then 1 tab OD P.O. 10-6
Inhibits the binding of adenosine diphosphale to its platelet, receptors infecting ADP-mediated activation and subsequent platelet aggregation clopedogiel irreversibly modifies the platelet ADP receptor
To reduce thrombotic events with acute coronary syndrome, ĉ atherosderosis documented by recent MI, or established peripheral artenal disease.
Contraindicated in patients hypersensitive to drug or its components and in those with pathologic bleeding (such as peptic ulcer) use cautiously in patients at risk for increased bleeding from trauma or other pathologic conditions
GI Bleeding purpora, bruising, hematoma, epistaxis, hematutia, ocular hemorrhage intracranial bleeding, abdominal pain, dyspepsia gastritis & constipation, rash, pruritus
Platelet aggregation wont return normal for at least 5 days after drug has been stopped
Don’t confuse plavix with Paxil
23

DRUG STUDYName of Patient: SARMIENTO, AGUSTIN M.
Generic name of Ordered
Drug
Brand Name
Date Ordered
Classification Dose/Frequency/
Route
MechanismOf
Action
Specific Indication
Contra-Indication
SideEffects/Toxic
Effects
NursingPrecaution
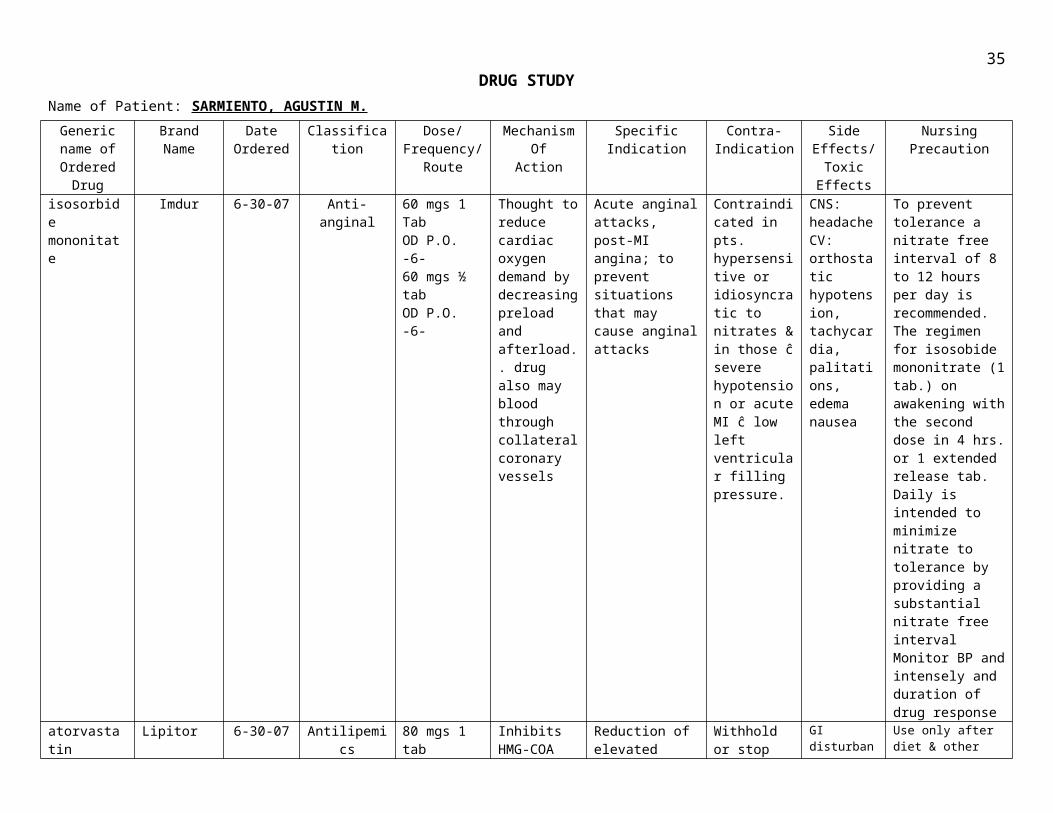
isosorbide mononitate
Imdur 6-30-07 Anti-anginal 60 mgs 1 TabOD P.O.-6-60 mgs ½ tabOD P.O.-6-
Thought to reduce cardiac oxygen demand by decreasing preload and afterload.. drug also may blood through collateral coronary vessels
Acute anginal attacks, post-MI angina; to prevent situations that may cause anginal attacks
Contraindicated in pts. hypersensitive or idiosyncratic to nitrates & in those ĉ severe hypotension or acute MI ĉ low left ventricular filling pressure.
CNS: headache CV: orthostatic hypotension, tachycardia, palitations, edema nausea
To prevent tolerance a nitrate free interval of 8 to 12 hours per day is recommended. The regimen for isosobide mononitrate (1 tab.) on awakening with the second dose in 4 hrs. or 1 extended release tab. Daily is intended to minimize nitrate to tolerance by providing a substantial nitrate free interval Monitor BP and intensely and duration of drug response
atorvastatin Lipitor 6-30-07 Antilipemics 80 mgs 1 tabOD tonight
Inhibits HMG-COA reductase, an early (and rale-limiting) step in cholesterol biosynsthesis
Reduction of elevated total L LDL cholesterol, apolipoprotein B & triglycerides & increase HDL cholesterol in pts. ĉ primary hypercholesterolemia
Withhold or stop drug in pts. at risk for renal failure caused by rhabdomyolysis resulting from trauma, in serious acute conditions like myopathy
GI disturbances, headache, myalgia asthenia, insomnia muscle cramps, bronchitis, rash infection, flu like syndrome allergic reactions
Use only after diet & other condition therapy prove infective Pt should follow a standard low cholesterol diet before & during therapy.Before starting treatment assess pt for underlying causes for hypercholesterolemia.
24

IV. ANATOMY AND PHYSIOLOGY
Human system is also called our cardiovascular system, and is composed of
our heart plus our arteries and veins. In a person’s heart, the atria (plural of atrium)
receive blood from the veins and the ventricles send blood to the arteries. As the
arteries become more finely divided, they are called arterioles. The finest divisions of
our vascular system are called capillaries. As the vessels get larger again, the smallest
are called venules which join and enlarge to form veins. Note that the distinction
between arteries and veins is by direction of blood flow, not oxygen content. Veins
carry blood toward the heart and arteries carry it away from the heart. Because of this,
not all arteries carry oxygenated blood. The two major exceptions, in which arteries
are carrying deoxygenated blood are the pulmonary artery which carries
deoxygenated blood from the heart to the lungs (to pick up oxygen there) and the
umbilical arteries which carry deoxygenated blood away from the baby’s body to the
placenta (to pick up oxygen there). We have double circulation: we have a separate
pulmonary circuit to the lungs and a systemic circuit to the body.
25

The path of blood flow in a human, then, is as follows:
1. The superior (a) and inferior (b) vena cava are the main veins that receive blood from the body. The superior vena cava drains the head and arms, and the inferior vena cava drains the lower body.
2. The right atrium receives blood from the body via the vena cavae. The atria are on the top in the heart.
3. The blood then passes through the right atrioventricular valve, which is forced shut when the ventricles contract, preventing blood from reentering the atrium.
4. The blood goes into the right ventricle (note that it has a thinner wall; it only pumps to lungs). The ventricles are on the bottom of the heart.
5. The right semilunar valve marks the beginning of the artery. Again, it is supposed to close to prevent blood from flowing back into the ventricle.
26

6. The pulmonary artery or pulmonary trunk is the main artery taking deoxygenated blood to the lungs.
7. Blood goes to the right and left lungs, where capillaries are in close contact with the thin-walled alveoli so the blood can release CO2 and pick up O2.
8. From the lungs, the pulmonary vein carries oxygenated blood back into the heart.
9. The left atrium receives oxygenated blood from the lungs.
10.The blood passes through the left atrioventricular valve.
11.The blood enters the left ventricle. Note the thickened wall; the left ventricle must pump blood throughout the whole body.
12.The blood passes through the left semilunar valve at the beginning of the aorta.
13.The aorta is the main artery to the body. One of the first arteries to branch off is the coronary artery, which supplies blood to the heart muscle itself so it can pump. The coronary artery goes around the heart like a crown. A blockage of the coronary artery or one of its branches is very serious because this can cause portions of the heart to die if they don’t get nutrients and oxygen. This is a coronary heart attack. From the capillaries in the heart muscle, the blood flows back through the coronary vein, which lies on top of the artery.
14.The aorta divides into arteries to distribute blood to the body.
27
15.Small arteries are called arterioles.
16.The smallest vessels are the capillaries.
17.These join again to form venules, the smallest of the veins.
These, in turn, join to form the larger veins, which carry the blood back to the superior
and inferior vena cava.
PHYSIOLOGY OF THE HEART
The work of the heart is to pump blood to the lungs through pulmonary
circulation and to the rest of the body through systemic circulation. This is
accomplished by systematic contraction and relaxation of the cardiac muscle in the
myocardium.
Conduction System An effective cycle for productive pumping of blood requires that the heart be
synchronized accurately. Both atria need to contract simultaneously, followed by
contraction of both ventricles. Specialized cardiac muscle cells that make up the
conduction system of the heart coordinate contraction of the chambers.
Cardiac Cycle The cardiac cycle refers to the alternating contraction and relaxation of the
myocardium in the walls of the heart chambers, coordinated by the conduction system,
during one heartbeat. Systole is the contraction phase of the cardiac cycle, and
diastole is the relaxation phase. At a normal heart rate, one cardiac cycle lasts for 0.8
second.
28

Heart Sounds The sounds associated with the heartbeat are due to vibrations in the tissues
and blood caused by closure of the valves. Abnormal heart sounds are called
murmurs.
Heart Rate The sinoatrial node, acting alone, produces a constant rhythmic heart rate.
Regulating factors are reliant on the atrioventricular node to increase or decrease the
heart rate to adjust cardiac output to meet the changing needs of the body. Most
changes in the heart rate are mediated through the cardiac center in the medulla
oblongata of the brain. The center has both sympathetic and parasympathetic
components that adjust the heart rate to meet the changing needs of the body.
Peripheral factors such as emotions, ion concentrations, and body temperature may
affect heart rate. These are usually mediated through the cardiac center.
29

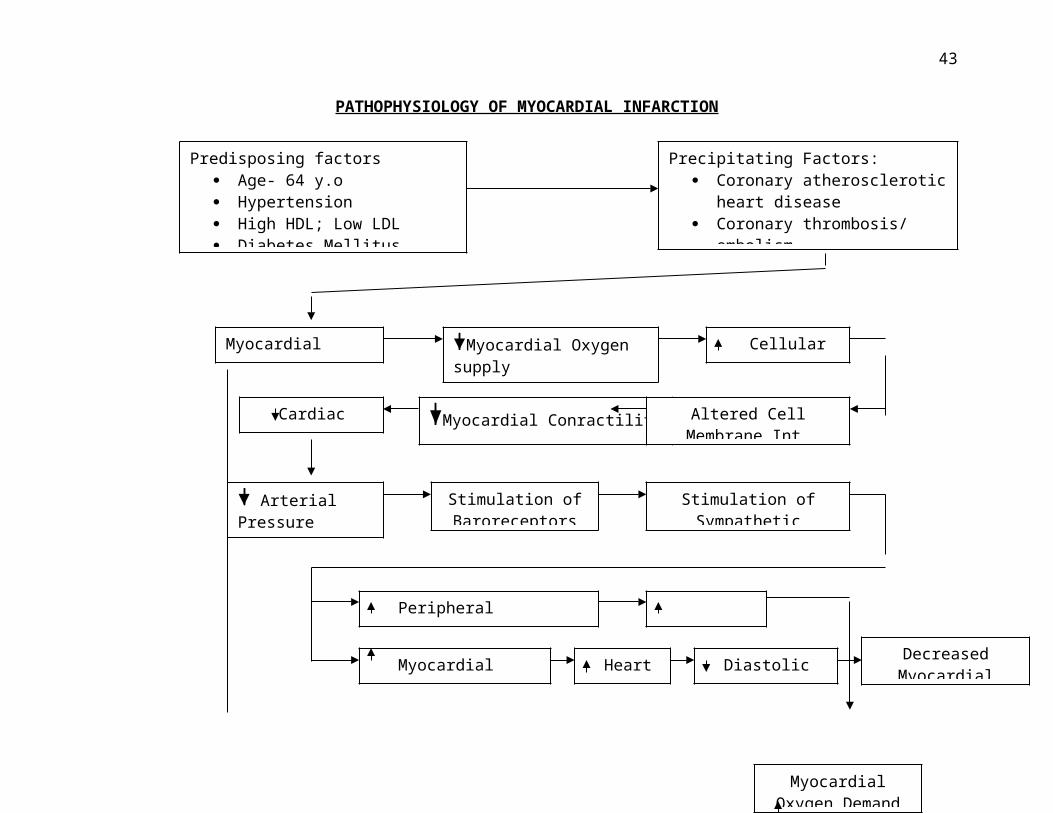
PATHOPHYSIOLOGY OF MYOCARDIAL INFARCTION
Cardiac output
Diastolic Filling
Afterload
Decreased Myocardial Tissue
Per.
Stimulation of Baroreceptors
Myocardial Conractility
Myocardial Oxygen supply
Stimulation of Sympathetic Receptors
Altered Cell Membrane Int.
Cellular HypoxiaMyocardial ischemia
Peripheral vasoconstriction
Arterial Pressure
Heart rate
Myocardial Oxygen Demand
Myocardial Contractility
Predisposing factors Age- 64 y.o Hypertension High HDL; Low LDL Diabetes Mellitus
Precipitating Factors: Coronary atherosclerotic heart
disease Coronary thrombosis/ embolism Decreased blood flow
Increased myocardial oxygen demand
S/Sx:- chest pain, oliguria, ECG changes, Elevated CK-M, Troponin T, LDH, AST
30

Mechanisms of Occlusion
Most MIs are caused by a disruption in the vascular endothelium
associated with an unstable atherosclerotic plaque that stimulates the formation
of an intracoronary thrombus, which results in coronary artery blood flow
occlusion. If such an occlusion persists long enough (20 to 40 min), irreversible
myocardial cell damage and cell death will occur.5
The development of atherosclerotic plaque occurs over a period of years
to decades. The initial vascular lesion leading to the development of
atherosclerotic plaque is not known with certainty. The two primary
characteristics of the clinically symptomatic atherosclerotic plaque are a
fibromuscular cap and an underlying lipid-rich core. Plaque erosion may occur
due to the actions of metalloproteases and the release of other collagenases and
proteases in the plaque, which result in thinning of the overlying fibromuscular
cap. The action of proteases, in addition to hemodynamic forces applied to the
arterial segment, can lead to a disruption of the endothelium and fissuring or
rupture of the fibromuscular cap. The degree of disruption of the overlying
endothelium can range from minor erosion to extensive fissuring that results in
an ulceration of the plaque. The loss of structural stability of a plaque often
occurs at the juncture of the fibromuscular cap and the vessel wall—a site
otherwise known as the plaque's "shoulder region." Any amount of disruption of
the endothelial surface can cause the formation of thrombus via platelet-
mediated activation of the coagulation cascade. If a thrombus is large enough to
completely occlude coronary blood flow for a sufficient time period, MI can result.
Mechanisms of Myocardial Damage
The severity of an MI is dependent on three factors: the level of the
occlusion in the coronary artery, the length of time of the occlusion, and the
presence or absence of collateral circulation. Generally speaking, the more
proximal the coronary occlusion, the more extensive is the amount of
31
myocardium at risk of necrosis. The larger the MI, the greater is the chance of
death due to a mechanical complication or pump failure. The longer the time
period of vessel occlusion, the greater the chances of irreversible myocardial
damage distal to the occlusion.
The death of myocardial cells first occurs in the area of myocardium that
most distal to the arterial blood supply—that is, the endocardium. As the duration
of the occlusion increases, the area of myocardial cell death enlarges, extending
from the endocardium to the myocardium and ultimately to the epicardium. The
area of myocardial cell death then spreads laterally to areas of watershed or
collateral perfusion. Generally, after a 6- to 8-hour period of coronary occlusion,
most of the distal myocardium has died. The extent of myocardial cell death
defines the magnitude of the MI. If blood flow can be restored to at-risk
myocardium, more heart muscle can be saved from irreversible damage or
death.
VII. NURSING MANAGEMENT
A.) IDEAL NURSING CARE PLAN
32

Nursing Diagnosis:
Acute pain may be related to tissue ischemia secondary to coronary artery occlusion
Possibly evidenced by
Reports of pain with our without radiationFacial grimacingRestlessness, changes in level of consciousnessChanges in pulse, BP
Desired outcomes
Patient will verbalize relief control of painDemonstrate use of relaxation techniquesDisplay reduced tension, relaxed manner, ease of movement
INTERVENTIONS RATIONALEIndependent 1. Obtain full description of pain from patient including location, intensity (0-10), duration; quality (dull/crushing); and radiation
2. Instruct patient to report pain immediately
3. Provide quiet environment, calm activities, and comfort measures (e.g., dry/ wrinkle—free linens, backrub). Approach the patient calmly and confidently
4. Assist/ instruct in relaxation techniques, e.g, deep/ slow breathing, distraction behaviors, visualization, guided imagery
Collaborative
Pain is a subjective experience and must be described by the patient. Assist patient to quantify pain by comparing it to other experiences.
Delay in reporting pain hinders pain relief/ may require increased dosage of medication to achieve relief. In addition, severe pain may induce shock by stimulating the sympathetic nervous system, thereby creating further damage and interfering with diagnosis and relief of pain.
Decreases external stimuli, which may aggravate anxiety and cardiac strain and limit coping abilities and adjustment to current situation.
Helpful in decreasing perception of/ response to pain. Provides a sense of having some control over the situation, increase in positive attitude.
33
5. Administer supplemental oxygen by means of nasal cannula
Administer medications as indicated, e.g.:
Antianginals, e.g nitroglycerin (Nitro-Bid, Nitro-stat, Nitro-Dur)
Beta-blockers, e.g., atenolol, pindolol, propanolol
Analgesics, e.g., morphine sulfate (Demerol)
Increases amount of oxygen available for myocardial uptake and thereby may relieve discomfort associated with tissue ischemia
Nitrates are useful for pain control by coronary vasodilating effects, which may increase coronary blood flow and myocardial perfusion. Peripheral vasodilation effects reduce the volume of blood returning to the heart (preload), thereby decreasing myocardial work and oxygen demand.
Important second-lineagents for pain control through effect of blocking sympathetic stimulation, thereby reducing heart rate, systolic BP, and myocardial oxygen demand.
Although IV morphine is the usual drug of choice, other injectable narcotics may be used in acute phase/ recurrent chest pain unrelieved by nitroglycerin to reduce severe pain, provide sedation, and decrease myocardial workload.
Nursing diagnosis
Risk for decreased cardiac output may include changes in rate, rhythm, electrical conduction, reduced preload/ increased SVR, infracted/dyskinetic muscle
Possibly evidenced by
Presence of signs and symptoms establishes actual diagnosis Desired outcomes
Patient will demonstrate hemodynamic instability, e.g., BP, cardiac output within normal range, adequate urinary output, decreased/ absent dysrhythmias,
34
Report decreased episodes of dyspnea,anginaDemonstrate an increase in activity tolerance
INTERVENTIONS RATIONALEIndependent1. Evaluate quality and equality of
pulses, as indicated
2. Auscultate heart sound Note development of S3,S4
3. Monitor heart rate and rhythm. Document dysrhythmias via telemetry
4. Provide small/ easily digested meals. Restrict caffeine intake, e.g., coffee, chocolate, cola
Collaborative5. Administer antidysrhythmics drugs and ACE inhibitors as indicated
Decreased cardiac output results in diminished weak/ thready pulses. Irregularities suggest dysrhythmias, which may require further evaluation. Monitoring.
S3 is usually associated with HF, but it may also be noted with mitral insufficiency (regurgitation) and left ventricular overload that can accompany severe infarction.S4 may be associated with myocardial ischemia, ventricular stiffening and pulmonary or systemic hypertension
Heart rate and rhythm respond to medication and activity, as well as developing complications/ dysrhythmias, which could compromise cardiac function or increase ischemic damage.
Large meals may increase myocardial workload and cause vagal stimulation resulting in bradycardia/ ectopic beats. Caffeine is direct cardiac stimulant that can increase heart rate.
Dysrhythmias are usually treated symptomatically, except for PVCs, which are often treated prophylactically. Early inclusion of ACE inhibitor therapy enhances ventricular output, increases survival and may slow progression of heart failure.
Nursing diagnosis
Tissue perfusion, altered, risk factors may include reduction/ interruption of blood flow, e.g., vasoconstriction, hypovolemia/ shunting and thromboembolic formation
35

Possibly evidence by
Presence of signs and symptoms establishes an actual diagnosis
Desired outcome
Patient will demonstrate adequate tissue perfusion as individually appropriate, e.g. skin warm and dry, peripheral pulses present/strong, vital signs within patient’s normal range, patient alert/ oriented, balanced intake/ output,absence of edema, free of pain/ discomfort.
INTERVENTIONS RATIONALEIndependent1. Inspect for pallor, cyanosis,
mottling, cool/ clammy skin. Note strength of peripheral pulses
2. Encourage active/ passive leg exercises, avoidance of isometric exercises
3. Monitor respirations, note work of breathing
4. Monitor intake, note changes in urine output. Record urine specific gravity
Collaborative5. Administer medications, e.g.:
Ranitidine (Zantac), antacids
Systemic vasoconstriction resulting from diminished cardiac output may be evidenced by decreased skin perfusion and diminished pulses.
Enhances venous return, reduces venous stasis, and decreases risk of thrombophlebitis; however, isometric exercises can adversely affect cardiac output by increasing myocardial work and oxygen consumption.
Cardiac pump failure may precipitate respiratory distress, sudden/ continued dyspnea may indicate thromboembolic pulmonary complications
Decreased intake/ persistent nausea may result in reduced circulating volume, which negatively affects perfusion and organ function. Specific gravity measurements reflect hydration status and renal function.
Reduces or neutralizes gastric acid, preventing comfort or gastric irritation, especially in presence of reduced mucosal circulation
36

Nursing diagnosis
Activity intolerance may be related to imbalance between myocardial oxygen supply and demand; presence of ischemia/necrotic myocardial tissues; cardiac depressant effects of certain drugs (Beta- blockers, antidysrythmics)
Possibly evidenced by
Alterations in heart rate and BP with activityDevelopment of dysrythmiasChanges in skin color/ moistureExertional anginaGeneralized weakness
Desired outcomes
Patient will demonstrate measurable/ progressive increase in tolerance for activity with heart rate/ rhythm and BP within patient’s normal limits and skin warm, pink, dry.Report pain absent/ controlled within time frame for administered medications
INTERVENTIONS RATIONALEIndependent1. Promote rest (bed/ chair) initially.
Limit activity on basis of pain/ hemodynamic response. Provide nonstress diversional activities.
2. Instruct patient to avoid increasing abdominal pressure, e.g., straining during defecation
3. Explain pattern of graded increase of activity level, e.g., getting up in chair when there is no pain, progressive ambulation, and resting for 1 hour after meals
Reduces myocardial workload. Oxygen consumption, reducing risk of complications (e.g., extension of MI)
Activities that require holding the breath and bearing down (Valsalva maneuver) can result in bradycardia, temporarily reduced cardiac output, and rebound tachycardia with elevated BP.
Progressive activity provides a controlled demand on the heart, increasing strength and preventing overexertion
37

4. Limit visitors and or/ visit by patient, initially
Collaborative5. Refer to cardiac rehabilitation program
Lengthy/ involved conversations can be very taxing for the patient; however, periods of quiet visitation can be therapeutic
Provides continued support/ additional supervision and participation in recovery and wellness process
Nursing diagnosis
Anxiety may be related to threat to or change in health and socioeconomic status; threat of loss/ death; unconscious conflict about essential values, beliefs, and goals of life
Possibly evidenced by
Fearful attitudeApprehension, increased tension, restlessness, facial tensionUncertainty, feelings of inadequacySomatic complaints/ sympathetic stimulationFocus on self, expressions of concern about current and future eventsFight or flight behavior
Desired outcomes
Patient will recognize feelings; identify causes, contributing factors; verbalize reduction of anxiety/ fear; demonstrate positive problem- solving skills; identify/ use resources appropriately
INTERVENTIONS RATIONALEIndependent1. Maintain confident manner (without
false reassurance)
2. Accept but do not reinforce use of denial. Avoid confrontations.
Patient and SO can be affected by the anxiety/uneasiness displayed by health team members. Honest explanations can alleviate anxiety.
Denial can be beneficial in decreasing anxiety but can postpone dealing with the reality of the current situation. Confrontation can promote anger and increase use of denial, reducing
38

3. Encourage patient/ SO to communicate with one another, sharing questions and concerns
4. Provide rest periods/ uninterrupted sleep time, quiet surroundings, with patient controlling type, amount of external stimuli
Collaborative5. administer antianxiety/ hypnotics as indicated, e.g., diazepam (Valium), lorazepam (Ativan), flurazepam (Dalmane)
cooperation and possibly impeding recovery.
Sharing information elicits support. Comfort and can relieve tension of unexpressed worries
Conserves energy and enhances coping abilities
Promotes relaxation/ rest and reduces feelings of anxiety
B.) ACTUAL NURSING MANAGEMENT(SOAPIE FORM)
S“Ah! Dili jud makatarong ug tulog. Maka mata-mata man jud labi
na dini sa hospital. Ug tigulang naman “ as verbalized by the
patient
O verbalizations of interrupted sleep complaints of not feeling rested yawning pain/ discomfort
ASleep pattern disturbance related to internal factors such as illness, psychologic stress and external factors such as facility routines
P At the end of 2 days, the patient will be able to report improvement of sleep/ rest pattern and verbalize increased sense of well- being and feeling rested.
At the end of 4 hours, the patient will be able to get enough uninterrupted sleep/ rest.
39

I
1. provided comfortable bedding and some of own possession, e.g., pillows
Rationale: Increases comfort for sleep as well as physiologic and psychologic support
2. Maintained environment conducive to sleep/ rest (e.g. quiet comfortable temperature, ventilation and closed door)
Rationale:This Provides atmosphere conducive to sleep
3. Encouraged position of comfort, assist in turning
Rationale:Repositioning alters areas of pressure and promotes rest
4. Provided nursing aids (e.g. back rub, bedtime care, pain relief, comfortable position [semi- fowler’s], relaxation techniques)
Rationale:To promote rest, relaxation; to induce sleep
5. Attempted to allow for sleep cycles for at least 90 minutes
Rationale:Experimental studies have indicated that 60- 90 minutes are needed to complete one sleep cycle and the completion of an entire cycle is necessary to benefit from sleep.
E
At the end of 4 hours, the patient was able to have sleep and verbalized of feeling rested.
At the end of 2 days, the patient was able to verbalize a fair improvement of his sleep/ rest pattern in between his medication/ treatment regimen.
S “Dili ko palakwon sa doctor kay dili pwede sa ako mangusog kay
sakit akong heart” as verbalized by the patient
40
O patient report chest pain with radiation to epigastrium
pain scale of 6
facial grimaces
changes in vital signs, baseline: HR=54 bpm, BP=140/90
mmHg
A -Acute pain related to tissue ischemia of myocardial tissue
secondary to myocardial infarction.
P At the end of 30 minutes, patient will be able to verbalize relief of
pain, display reduced tension, relaxed manner and ease of
movement
I
1.) Obtained full description of pain from patient including
location, intensity (0-10), duration, quality and radiation.
Rationale:
Pain is a subjective experience and must be described by the pt.
Assist pt. to quantify pain by comparing it to other experiences.
2.) Maintained bed rest at least during periods of pain.
Rationale:
To reduce workload of the heart
3.) Positioned patient comfortably, in moderate high back rest
Rationale:
This allows for lung expansion by lowering the diaphragm
4.) Instructed patient in relaxation techniques, i.e., deep/slow
41

breathing
Rationale:
Helpful in decreasing perception of/ response to pain. Provides a
sense of having some control over the situation, increase in
positive attitude.
COLLABORATIVE
5.) Administered supplemental oxygen by means of nasal
cannula @ 3L/min.
Rationale:
Increases amount of oxygen available for myocardial uptake and
thereby may relieve discomfort associated with tissue ischemia
Administered medications as indicated such as:
Isosorbide dinitrate (Isordil) 5 mg tab SL for 3 doses every
5 minutes if chest pain is not relieved
Isosorbide mononitrate (Imdur) 60 mg ½ tab
OD P.O
Rationale: to reduce cardiac oxygen demand by decreasing
preload and afterload. Increases blood flow through the
collateral coronary vessels.
E At the end of 30 minutes, patient was able to verbalize a slight
relief of chest pain and demonstrated the use of relaxation
techniques.
S “Dili ko pwede mangusog kay magsakit akong heart.” as verbalized by
the patient.
O weakness
42
Patient’s report of pain
Changes in v/s
A Ineffective cardiopulmonary tissue perfusion related to reduced
coronary blood flow.
P At the end of 2 hours, patient will verbalize a relief from pain and
discomfort.
I
1.) Initially assess document and report to the following physician.
Patients description of chest discomfort, including location, intensity,
radiation, duration and factors that affect it. Other symptoms such as
nausea, diaphoresis complains of universal fatigue.
2.) Monitored respiration and note work of breathing.
3.) Assess GI functions and monitor fluid intake and urine output.
4.) Obtained a 12- lead ECG recording during the symptomatic event
as prescribed to determine extension of infarction
COLLABORATIVE:
5.) Administered oxygen @ 3L/min via nasal cannula.
Rationale:
Increases amount of oxygen available for myocardial uptake and
thereby may relieve discomfort associated with tissue ischemia
E At the end 2 hours, patient verbalizes the relief from discomfort around
43

the chest.
S “Hypertensive nako dugay ra kadto pa ning 55 anyos pa ako edad.” as
verbalized by the patient.
O
Elevated BP=140/90 mmHg
Increased creatinine= 6.17 mgs/dl
Urine output of less than 30 ml/hr
A Decreased cardiac output related to diminished blood flow caused by
increased vascular resistance.
P At the end of 1 hour, patient will be able to achieve and maintain BP
within acceptable range.
I
1.) Monitored BP using proper equipment with cuff bladder that is two-
thirds diameter.
Rationale:
To detect changes from baseline that indicate changes in
cardiovascular status
2.) Maintained fluid and dietary sodium restrictions.
Rationale:
To reduce fluid restriction which contributes to hypertension
3.) Discouraged intake of coffee, tea, cola and chocolate which are
44
high in caffeine.
Rationale:
Caffeine stimulates sympathetic nervous system
4.) Maintained physical and emotional rest.
Rationale:
Sedatives can be used to reduce stress and associated
vasoconstriction; to reduce cardiac workload
5.) Administered antihypertensive as prescribed:
atenol (Therabloc) 50 mg 1 tab now then ODRationale: A beta-blocker that selectively blocks beta-adrenergic receptors,
decreases cardiac output and cardiac oxygen consumption and
depresses rennin secretion
E At the end of 1 hour, patient was able to maintain BP within
individually acceptable range.
VIII. REFERRALS AND FOLLOW – UP(Health teaching)
Medication
Advised patient to take prescribed medication at regular basis;
Atenolol( therabloc) 50 mg.tab once a day P.OClopidogiel ( plavix) 75 mg. tab once a day P.OISMN ( Imdur) 60 mg tab once a day P.OAtorvastatin calcium ( lipitor) once a day P.O
Exercise
At the hospital, patient is advised to initiate gradual exercise such as;
a) Lying or sitting exercises ( arms, legs, trunk)b.) Exercise progress to standing and slow walking in
the hall. c.) Exercise must be done twice a day for about 20
45
minutes d.) Exercises (Deep, pursed lip or deep breathing
exercises)
Treatment
In the hospital, patient is provided with the following treatment ;
a.)Supplemental oxygen by nasal cannula @ 2-4 L/min.b.)Cardiac monitoring for continued surveillance of hearts activity.c.)Frequent monitoring of vital signs including temperature , pulse rate ( apical/ radial) and blood pressure and intake and outputd.)Pharmacologic management to stabilize client condition.
Out patient When the patient will be discharge, out patient program consist of supervised , oven ECG monitored , exercised training based on the results of exercised stress test .support and guidance related to the treatment of the disease and education and counseling related to lifestyle modification .
Diet
Client is advised to follow the prescribed recommended diet ;
a) Diabetic diet: eat complex CHO foods with high fiber content avoid added sugar and concentrated sweets and all other CHO foods and eat regularly.
b) Eat foods low in calorie, saturated fats and cholesterol; restriction of sodium; avoidance of spicy foods soft fiber food and take small frequent feedings
Recommendation s Advised the patient for followed up check up from his assigned physician.
Advised patient peer for frequent monitoring of his vital sign to avoid any risk
and possible complication
46

Explain the purpose and preparation for diagnostic test to have clear
understanding of procedures and what is happening increase feeling of
control and lessens anxiety.
Provide positive reinforcement for gains/ improvement and participation in self
care/treatment program. This encourages continuation of healthy behavior.
Advice patient to take his medication at home as prescribed by the physician
for continues medication treatment.
Suggest engaging in relaxing, non strenuous activity to avoid any risk due to
over stress
Teach client on coping mechanisms with recurring pain and other clinical
manifestations
Encourage patient to eat nutritious food like vegetable fruits, foods the high
fiber contain like cereal and foods rich in protein.
IX. EVALUATION & IMPLICATION (PROGNOSIS)
This case study was done successfully although we experienced some
difficulties analyzing the health status of the client and understanding the medical
orders given. Using our critical thinking, we were able to carefully identify the
problem of our patient who needs direct interventions for the wellness of his
health. Moreover, the group was able to discuss some health teachings as stated
above for the improvement of the client’s health and fast recovery.
The patient was able to understand the imparted health teachings and
verbalized to consistently follow his treatment regimen in home care
management. Although patient’s blood pressure did not lower down to his normal
range of blood pressure, other clinical manifestations such as severe chest pain
was not subjectively verbalized by the patient and labored breathing was not
evident. Still, patient has unproductive, dry cough. Mr. Sarmiento is progressing
well in his health condition and is for discharge any soon. Patient may have an
47

uncomplicated episode of myocardial infarction and may return to normal
activities and lifestyle with moderation and modification to some of those.
X. DOCUMENTATION
Upon assessment last July 3, 2007, patient X was received with a diagnosis
of Acute myocardial infarction; Hypertensive cardiovascular disease; ruled out
PUD; diabetic nephropathy. Pt. was sitting on bed and complaint on pain on
chest area upon coughing was noted. Instructed to do deep, breathing exercises
everytime chest pain is recurring. Pertinent data about the patient’s family and
personal health history were gathered.
The next day on the group’s duty, pt. has oxygen inhalation regulated at
3l/min via nasal cannula and vital signs were monitored every 4 hours with
special consideration to the client’s blood pressure. Due medication were
properly given and kept patient in moderate, high back rest and kept comfortably
on bed, keeping back dry. Pt. was observed for any unsualties during the shift.
No further complaints were noted from the patient.
On the 2nd day of duty the doctor ordered that client may go home the next
day if stable. So, the group imparted health teachings important for the client to
follow as his home care management. We helped the client in discharged
planning and reminded them the health teachings that we had discussed.
This study also tests our abilities and skills on how to find answers to the
patient’s problem, what action to be done in order to solve it and how to properly
and correctly use our initiative for the success and for the good outcome of our
care study. This is one of our tasks as a student or future nurses and it serves as
our training ground backed up with strict training in order for us to become
equipped, productive, efficient, and world-class nurses in the future.
48
B I B L I O G R A P H Y
Smeltzer.Bare. Textbook on Medical-Surgical Nursing (10th edition) Lippincott-Raven Publisher.Copyright 1996
Wilson, Billie Ann Nurse’s Drug Guide (vol. 1 & 2) Pearson Education Inc.,Copyright 2000
Mosby’s Pocket Dictionary of Medicine, Nursing and Allied Health (4 th edition) Elsevier(Singapore) PTE LTD> Copyright 2002
Doenges, Marilynn Nursing Care Plans, Guidelines for Individualizing Patient Care(6th edition) F.A Davis Company. Copyright 2000
Kozier. Erb. Blais. Wilkinson. Fundamentals in Nursing (5th Edition). Addison esley Longman Inc. 1998.
MacMahon, S. Blood pressure and the risk of cardiovascular disease. N Engl J Med 2000; 342:50
HTML1Rollins Gina. "With smoking cessation drugs, dosing is key", ACP-
ASIM Observer, 22(4); 1,16-17.
W E B L I O G R A P H Y
http://biology.clc.uc.edu/courses/bio105/circulat.htm
wwwmedlib.med.utah.edu\webpath\TUTORIAL\MYOCARD\MYOCARD
Research Paper help https://www.homeworkping.com/
49