
56 - Göteborgs universitet · whereas children with ADHD and a comorbid bipolar disor-der are...
12
http://jad.sagepub.com/ Journal of Attention Disorders http://jad.sagepub.com/content/15/1/56 The online version of this article can be found at: DOI: 10.1177/1087054709356931 2011 15: 56 originally published online 13 January 2010 Journal of Attention Disorders Lin Sørensen, Kerstin J. Plessen, Jude Nicholas and Astri J. Lundervold Is Behavioral Regulation in Children With ADHD Aggravated by Comorbid Anxiety Disorder? Published by: http://www.sagepublications.com can be found at: Journal of Attention Disorders Additional services and information for http://jad.sagepub.com/cgi/alerts Email Alerts: http://jad.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://jad.sagepub.com/content/15/1/56.refs.html Citations: What is This? - Jan 13, 2010 Proof - Dec 9, 2010 Version of Record >> at Universitetsbiblioteket i Bergen on November 8, 2011 jad.sagepub.com Downloaded from
Transcript of 56 - Göteborgs universitet · whereas children with ADHD and a comorbid bipolar disor-der are...

http://jad.sagepub.com/Journal of Attention Disorders
http://jad.sagepub.com/content/15/1/56The online version of this article can be found at:
DOI: 10.1177/1087054709356931
2011 15: 56 originally published online 13 January 2010Journal of Attention DisordersLin Sørensen, Kerstin J. Plessen, Jude Nicholas and Astri J. Lundervold
Is Behavioral Regulation in Children With ADHD Aggravated by Comorbid Anxiety Disorder?
Published by:
http://www.sagepublications.com
can be found at:Journal of Attention DisordersAdditional services and information for
http://jad.sagepub.com/cgi/alertsEmail Alerts:
http://jad.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://jad.sagepub.com/content/15/1/56.refs.htmlCitations:
What is This?
- Jan 13, 2010Proof
- Dec 9, 2010Version of Record >>
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

Articles
Journal of Attention Disorders15(1) 56 –66© 2011 SAGE PublicationsReprints and permission: sagepub.com/journalsPermissions.navDOI: 10.1177/1087054709356931http://jad.sagepub.com
Is Behavioral Regulation in Children With ADHD Aggravated by Comorbid Anxiety Disorder?
Lin Sørensen,1 Kerstin J. Plessen,1,2
Jude Nicholas,3 and Astri J. Lundervold1
Abstract
Background: The present study investigated the impact of coexisting anxiety disorder in children with ADHD on their ability to regulate behavior. Method: Parent reports on the Behavior Rating Inventory of Executive Function (BRIEF) in a comorbid group of children with ADHD and anxiety (n = 11) were compared to BRIEF reports in a group of children with a “pure” ADHD (n = 23), a “pure” anxiety (n = 24) and a group without any diagnosis (n = 104) in a 2 (ADHD vs. no ADHD) × 2 (anxiety vs. no anxiety) design. Results: The children with ADHD and anxiety disorder scored significantly higher on the Inhibit scale than children within the other three groups. Main effects of diagnosis appeared in ADHD children on the Inhibit, Emotional Control, and Working Memory scales, and on the Shift and Emotional Control scales in anxious children. Conclusion: The results indicate that a behavioral dysregulation in ADHD children is aggravated by comorbid anxiety.
KeywordsADHD, inattention, anxiety, BRIEF, behavioral regulation
Anxiety is one of the most frequent comorbid disorders in children with ADHD, with a frequency of 25% (Tannock, 2000). Several authors have raised the question whether children with both disorders are characterized by a differ-ent symptom cluster than children with “pure” ADHD or anxiety disorder (Schatz & Rostain, 2006). Several studies have suggested that anxiety symptoms protect children with ADHD against the poor inhibitory control normally seen in children with an ADHD diagnosis (Manassis, Tannock, & Barbosa, 2000; Pliszka, 1992; Pliszka, Carlson, & Swanson, 1999; Pliszka, Hatch, Borcherding, & Rogeness, 1993). How-ever, not all studies have confirmed these findings (Abikoff et al., 2002; Newcorn et al., 2001; Oosterlaan, Logan, & Sergeant, 1998).
The notion that symptoms of an anxiety disorder have a positive effect on the behavioral dysregulation in children with ADHD has primarily been explained by referring to the Behavioral Inhibition System (BIS) in Gray’s model of behavioral regulation (Quay, 1988). This model proposes that children with anxiety are high on the temperamental trait of introversion (Gray, 1971, 1972) and hypersensitive for signals of punishment (Quay, 1988). This temperamen-tal trait is associated with a repressed behavior in new and challenging settings (Biederman et al., 1993; Muris, 2006) and an overactive BIS (Quay, 1988). Children with ADHD
are not very sensitive to expectations from the surroundings such as signals of punishment. They are characterized by an impulsive behavior and an underactive BIS (Quay, 1988). The distinction between the two diagnostic groups is sup-ported by the observation that children with ADHD have a primary deficit in inhibiting their impulses (Barkley, 1997), whereas children with anxiety disorder display an enhanced ability to inhibit their impulses (Oosterlaan & Sergeant, 1998). However, other emotional characteristics of a child with an anxiety disorder do not support that their symptoms will have a positive effect on the behavior dysregulation associated with ADHD. Their repressed, inhibited behavior may rather be associated with a distractive and inflexible approach in unfamiliar and stressful situations (Eysenck, Derakshan, Santos, & Calvo, 2007; Muris, 2006; Muris, Meesters, & Rompelberg, 2006). This will influence their attention (Eysenck et al., 2007), leading to an inattentiveness
1University of Bergen, Norway2Haukeland University Hospital, Bergen, Norway3Statped Vest Resource Centre, Bergen, Norway
Corresponding Author:Lin Sørensen, Department of Biological and Medical Psychology, BB-bygget, Jonas Liesv. 91, 5009 Bergen, NorwayEmail: [email protected]
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

Sørensen et al. 57
that probably will have a negative influence on their ability to regulate their behavior.
Studies of behavioral dysregulation in children with ADHD and comorbid anxiety disorder have primarily based their conclusions on psychometric test-data. However, impor-tant aspects of the dysfunctions associated with the two disorders may only be revealed in the child’s natural setting (Stefanatos & Baron, 2007). Studies using ecologically valid and standardized measures hopefully will be able to produce more valid results (Abikoff et al., 2002). The Behavior Rating Inventory of Executive Function (BRIEF; Gioia, Isquith, Guy, & Kenworthy, 2000) is a well validated questionnaire assessing aspects of everyday cognitive control functions. Behavioral regulation is operationalized in the BRIEF by a measure of the child’s ability to inhibit responses (i.e., the Inhibit scale), approaching new settings (i.e., the Shift scale), and controlling the emotional outcomes (i.e., the Emotional Control scale). This instrument seems thus to be well suited in a study of children with ADHD and comor-bid anxiety disorder.
Few studies of children with ADHD have used the BRIEF to investigate the influence of a comorbid diagnosis on the children’s everyday functioning. One study showed that the BRIEF scores were not negatively influenced by a comorbid diagnosis of Tourette syndrome (Mahone et al., 2002a), whereas children with ADHD and a comorbid bipolar disor-der are shown to display an elevated score on the composite scale named the Behavior Regulation Index (BRI; Warner, 2005). Studies reporting BRIEF scores in children with ADHD and a comorbid anxiety disorder are still lacking.
This motivated the present study of BRIEF reports in a population-based group of children with ADHD and a comorbid anxiety disorder. We compared herein the parent reports in this group with parent reports in a group of chil-dren with “pure” ADHD (i.e., no anxiety disorder), a group with a “pure” anxiety disorder (i.e., no ADHD) and a group of children without any disorder diagnosis. We assumed that the use of an ecologically valid measure would reveal that symptoms of behavioral dysregulation in children with ADHD will be aggravated by a comorbid anxiety disorder. The assumption of an attentional control dysfunction in anxious children (Eysenck et al., 2007; Muris, 2006; Muris et al., 2006) led us to expect that the children in the comor-bid group would show less ability to inhibit responses and shift set in their everyday life than children with “pure” disorders. Furthermore, we expected that the increased behavioral dysregulation would give the children in the comorbid group more problems in activities requiring intact working memory function (Barkley, 1997; Eysenck et al., 2007; Gioia et al., 2000). We are aware of the fact that response inhibition problems across the different ADHD subtypes are associated with symptoms of inattention (Chhabildas, Pennington, & Willcutt, 2001; Willcutt, Doyle, Nigg, Faraone, & Pennington, 2005) and that such symptoms
probably also are part of the attentional control deficit shown by children with an anxiety disorder (Muris et al., 2006). A measure of inattention symptoms was therefore included as a covariate in our analyses.
MethodThe Bergen Child Study (BCS) is a prospective study of children’s mental health from primary school age to ado-lescence (Heiervang et al., 2007; Stormark, Heiervang, Heimann, Lundervold, & Gillberg, 2008). The first wave of the study was organized in three stages, where stage 1 comprised screening of symptoms of mental health prob-lems, stage 2 a diagnostic evaluation, and stage 3 a clinical assessment. The present study has drawn data from stage 1 to stage 3.
The target population comprised all 9,430 children who, during October-November 2002, attended 2nd to 4th grade (i.e., 7-9 years old) at any primary school (public or private) in the municipality of Bergen, Norway. In addition, 222 children from the Sund municipality participated in the first wave of the BCS. In stage 1 all parents and teachers in the total sample were asked to complete a questionnaire com-prising the Strengths and Difficulties Questionnaire (SDQ; Goodman, 1999) and the Diagnostic and Statistical Manual of Mental Disorders (4th ed.) (DSM-IV; American Psy-chiatric Association, 1994) diagnostic criteria for ADHD (Swanson et al., 2001). Parents of 6,978 (74%) children in the Bergen municipality and parents of 170 (75.9%) in the Sund municipality returned the questionnaire with informed consent. In stage 2 parents of children defined as screen positive in stage 1 (n = 651) and a random sample of children defined as screen negative (n = 389) were interviewed with the Development and Well-being Assessment (DAWBA). A sample comprising 329 children defined as DAWBA screen “positive” (i.e., children with any DAWBA diagnosis—33%) and screen “negative” was selected to take part in stage 3 when they were 8 to 11 years old. The children came together with their parents to take part in a neuropsychiatric assess-ment including a diagnostic interview of the parent(s) and the child (Schedule for Affective Disorders and Schizophrenia for School-Age Children—Present and Lifetime Version; Kiddie-SADS-PL; Kaufman et al., 1997), the BRIEF ques-tionnaire (Gioia et al., 2000), and the Wechsler’s Intelligence Scale for Children—third version (WISC-III; Wechsler, 1991). The present sample was selected from the 252 chil-dren where the parents completed the BRIEF questionnaire (Figure 1).
Kiddie-SADS-PLThe Kiddie-SADS-PL (Kaufman et al., 1997) is a reliable semistructured diagnostic interview designed to evaluate current and past episodes of psychopathology in children
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

58 Journal of Attention Disorders 15(1)
BiBExcludedStage 3
N = 329 No BRIEF
N = 77
BRIEF + K-SADS N = 252
Excluded
ADHD Definite: N = 37
Probable: N = 19
ANXIETY Definite: N = 43
Probable only: N = 11
No diagnoses N = 104
“Pure” ADHD N = 23
ADHD + ANX. N = 11
“Pure” ANXIETY
N = 24
Comorbid disorders
N = 8
Excluded
Comorbid disorders
N = 10
Excluded
Comorbid disorders
N = 2
Excluded
ADHD + ANX. N = 21
ANXIETY N = 26
ADHD N = 31
Dystymia, OCD, & tourette
Comorbid disorders N = 2 ODD & enuresis
Comorbid disorders N = 8 ODD, enuresis, encopresis, & trans./chronic tic
CD, depression, tourette,psychosis, & FSIQ=<65
CD, tourette, OCD, mania, depression, dystymia, & FSIQ = <65
Other diagnoses than ADHD or anxiety
N = 59
Comorbid disorders N = 4 ODD, enuresis, & encopresis
ANXIETY N = 47
ADHD N = 52
Some children have
bothdisorders
Excluded Excluded
Probable diagnoses of simple phobias and separation anxiety
Probable diagnoses of simple phobias and separation anxiety Anxiety N = 7 ADHD N = 4
N = 3 general anxiety N = 4 general anxiety N = 2 other anxiety N = 7 other anxiety N = 6 simple phobia N = 13 simple phobia
Figure 1. A flowchart showing the selection of children in the present study
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

Sørensen et al. 59
according to the DSM-IV (Ambrosini, 2000; American Psy-chiatric Association, 1994; Kaufman et al., 1997). Diagnoses are scored as either definite, probable, or not present (Kaufman et al., 1997). A probable diagnosis is close to a definite diagnosis in symptom expression, that is, the child’s behavior fulfills all the diagnostic criteria except for one, and the symptoms cause impairment in the everyday life. Children with a probable or definite diagnosis of ADHD or a general anxiety disorder were included in the present study. Children with simple or social phobias, separation anxiety, panic anxiety, or adjustment disorder with anxiety had to obtain a definite diagnosis to be included. Although a probable diagnosis may cause some impairment in the everyday life of children with these anxiety disorders, these are not associated with as severe impairment as a probable diagnosis of ADHD or a general anxiety disorder (American Psychiatric Association, 1994).
The children were allocated to the following diagnostic groups: (a) ADHD with anxiety disorder (n = 11), (b) “pure” ADHD (n = 23), (c) “pure” anxiety disorder (n = 24), (d) no diagnosis (n = 104). Details regarding the selection proce-dure and the inclusion of anxiety disorders are shown in Figure 1; the final sample (n = 162) is thus described in the lower boxes of Figure 1. The mean age of this sample was 9.4 years (SD = 0.9). There were slightly more boys than girls in this sample (61.3%), and gender was unevenly rep-resented across the groups. 58 (55.8%) boys were in the no diagnosis group, 13 (54.2%) boys were in the “pure” anxiety group, 19 (82.6%) in the “pure” ADHD group, and 9 (81.8%) in the ADHD with anxiety disorder group. Children with a comorbid Conduct Disorder (CD) were excluded (Figure 1). Although previous studies have shown that a comorbid ODD and CD in children with ADHD does not influence psychometric measures of response inhibition (Oosterlaan Logan, & Sergeant, 1998; Newcorn et al., 2001), comorbid-ity of ODD and/or CD increases parent reports of impulsivity in anxious children with ADHD (Newcorn et al., 2001). Children with a comorbid ODD were included, due to the fact that a comorbid disorder of only ODD is present in 50% of children with ADHD (Jensen, Martin, & Cantwell, 1997) and is associated with a milder form of delinquent behavior compared to CD. Nine children in the final sample were diagnosed with ODD; six in the group of ADHD with anxi-ety disorder, two children in the group with “pure” ADHD and one child in the “pure” anxiety disorder group.
BRIEF QuestionnaireThe BRIEF (Gioia et al., 2000) comprises 86 items that con-stitute eight theoretically and empirically derived scales, named the Inhibit, Shift, Emotional Control, Initiate, Work-ing Memory, Plan/Organize, Organization of Materials, and Monitor scales. A Behavior Regulation Index (BRI) score can be generated from the Inhibit, Shift, and Emotional Control
scales (Gioia et al., 2000). The BRIEF scales Inhibit, Shift, and Emotional Control were included in the present study as measures of behavioral regulation. The Working Memory scale was also included, because problems in behavioral reg-ulation are associated with problems in acquiring complex information (Gioia et al., 2000). The parents evaluated each item in relation to their child as a behavior that never, some-times, or often occurs. The sum score ranges from 0 to 20 on the Inhibit, Shift, and Working Memory scales, and from 0 to 18 on the Emotional Control scale.
Studies comparing BRIEF and other behavioral rating systems have reported a good convergent and discriminant validity as well as test–retest reliability ranging from .79 to .88 (Gioia et al., 2000). Internal reliability ranged from .80 to .98 using Cronbach’s alpha (Gioia et al., 2000). We used a version of BRIEF that was translated to Norwegian by one of the authors (JN). The Cronbach’s alpha for the dif-ferent BRIEF scales in the whole sample (n = 252) ranged from .81 to .93.
The Inattention SubscaleIn the Kiddie-SADS-PL algorithm the interviewers are instructed to skip the section assessing inattention symp-toms if none of the four ADHD symptoms included in the screening questionnaire are endorsed. Therefore, we included the parents’ ratings on an inattention subscale that was part of stage 1, completed 18 months prior to the in-depth clinical assessment in stage 3. The Inattention subscale contains the nine items used to define the inattention part of the ADHD diagnosis in the DSM-IV (American Psychiatric Association, 1994; Swanson Nolan, and Pelham IV ques-tionnaire; SNAP-IV; Swanson et al., 2001). Each answer was assigned a value 0, 1 or 2, and a sum score ranging from 0 to 18 was computed.
WISC-IIIThe WISC-III (Eilertsen & Johnsen, 2003; Wechsler, 1991) was used to assess intellectual function. The Full Scale IQ (FSIQ) was included with scaled scores derived from Swedish norms (Sonnander, Ramund, & Smedler, 1999).The mean FSIQ was 92.11 (SD = 13.08). The use of the Swedish norms in establishing the IQ of children in the same age group as in the present study has been shown to be too stringent (Sundberg, Egeland, Andreassen, & Stensli, 2006). We therefore included children with a FSIQ > 65. The highest observed FSIQ in the sample was 123. Group means in FSIQ are presented in Table 1.
Statistical AnalysesAll statistical analyses were performed with the SPSS, version 14. We used multivariate analyses of covariance
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from
60 Journal of Attention Disorders 15(1)
(MANCOVA) with a 2 (ADHD vs. no ADHD) × 2 (anxiety vs. no anxiety) design to test for differences between groups. In our model, the dependent vector were the raw scores from the four interrelated BRIEF scales and the between effects were calculated after the dependent variable in both the multivariate and univariate tests was adjusted for the effect of gender, age, FSIQ, and symptoms of inattention. The multivariate F statistic reduces the chances of a Type I error when performing several univariate tests and the alpha levels are adjusted according to the number of comparisons made. Due to an unbalanced design (i.e., different group sizes) the model in all the covariance analyses were custom-ized to run Type III SS.
ResultsThe Effect of Gender, Age, FSIQ, and Inattention Symptoms in the Disorder Groups
Gender was unevenly represented in the diagnostic groups (c2(3) = 8.19, p < .05), with a high percentage of boys in the two ADHD groups. Preliminary multivariate analysis using gender as factor and the BRIEF scales as vector revealed a significant gender effect (Wilks’s Lambda = .86, F(1, 157) = 6.30, p < .001), with univariate effects on all the BRIEF scales (Inhibit scale, F(1, 160) = 17.71, p< .001; Shift scale, F(1, 160) = 5.21, p < .05; Emotional Control scale, F(1, 160) = 8.48, p < .01; Working Memory scale; F(1, 160) = 21.52, p < .001).
Univariate 2 (ADHD, no-ADHD) × 2 (anxiety, no-anxiety) ANOVA including age, FSIQ, and inattention symptoms as dependent variables were computed. A statistically sig-nificant interaction effect was revealed between disorder groups and age, showing that children with ADHD and a comorbid anxiety disorder were significantly older than the children in the other groups (F(3, 158) = 6.29, p < .05; see the mean values in Table 1). In addition, a significant main effect of age was revealed related to an ADHD disorder (F(3, 158) = 5.24, p < .05), showing children with ADHD to be significantly older than the children in the “pure” anxiety
or no diagnosis groups. A statistical significant main effect of FSIQ showed that children with ADHD had a statisti-cally significant lower FSIQ than children in the other groups (F(3, 158) = 20.63, p < .001). On the Inattention symptom subscale, main effects were revealed in relation to the ADHD (F(3, 158) = 69.00, p < .001) and anxiety (F(3, 158) = 4.38, p < .05) factors (see mean scores in Table 1).
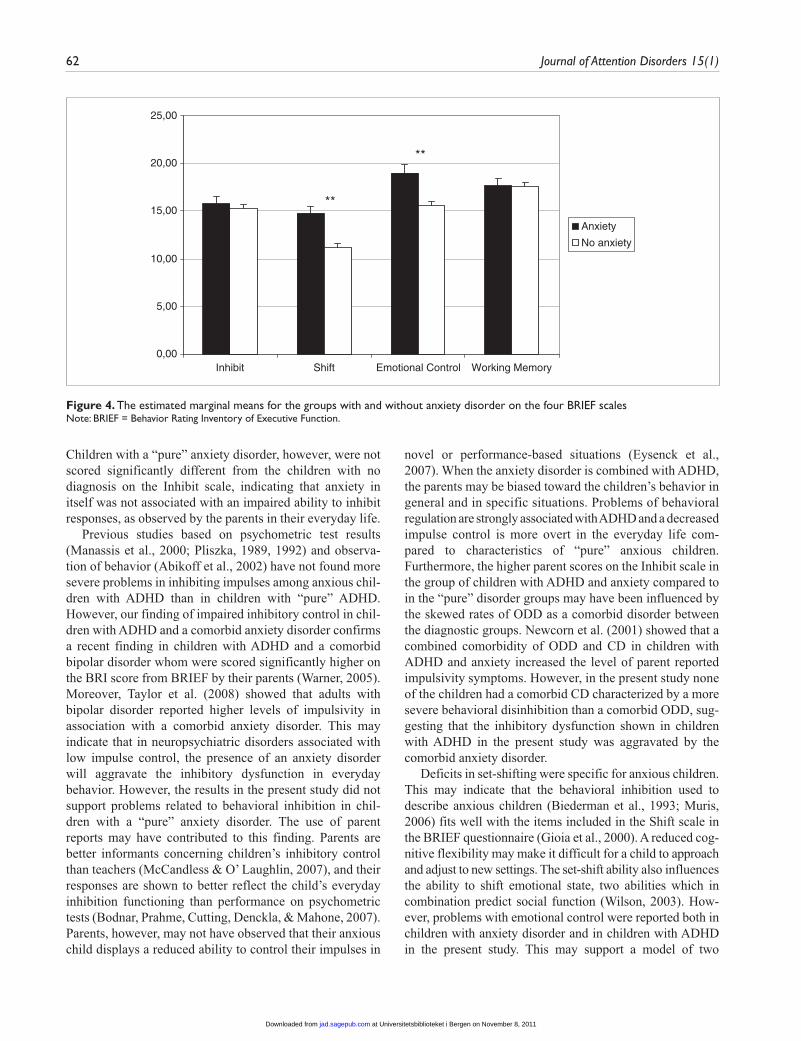
Between Groups Comparison on the BRIEF ScalesA MANCOVA, including gender, age, FSIQ, and inattention symptoms as covariates, showed a statistically significant multivariate main effect on the BRIEF vector both in rela-tion to the ADHD (Wilks’s Lambda = .83, F(1, 151) = 8.01, p < .001) and the anxiety (Wilks’s Lambda = .83, F(1, 151) = 7.91, p < .001) factors. A significant interaction effect was revealed in the univariate analysis for the Inhibit scale (F(1, 154) = 4.09, p < .05). Children with ADHD and a comorbid anxiety disorder had higher mean scores than the children in the other groups (Figure 2). Statistically significant main effects of the ADHD factor were revealed on all the BRIEF scales, except for on the Shift scale (Inhibit, F(1, 154) = 22.64, p < .001; Emotional Control, F(1, 154) = 6.87, p < .05; and Working Memory, F(1, 154) = 15.61, p < .001). Moreover, children with ADHD had higher mean scores on the selected scales than children with a “pure” anxiety dis-order and those with no diagnosis (Figure 3). Significant main effects on the Shift (F(1, 154) = 25.53, p < .001) and the Emotional Control (F(1, 154) = 12.20, p < .01) scales in the BRIEF were revealed concerning the Anxiety factor. Figure 4 shows that anxious children had higher mean scores than children with a “pure” ADHD and no diagnosis.
The multivariate analyses showed that only the Inatten-tion subscale covaried with the BRIEF scores (Wilks’s Lambda = .70, F(1, 151) = 16.03, p < .001), whereas gender, age, and FSIQ did not. The Inattention subscale, gender, and age covaried on the Inhibit scale (the inattention sub-scale, F(1, 154) = 15.39, p < .001; gender, F(1, 154) = 5.40, p < .05; age, F(1, 154) = 6.11, p < .05) in the univariate analyses, whereas the Inattention subscale also covaried on
Table 1. Descriptive Values of the Variables in the Diagnostic Groups
M (SD)
ADHD + Anx ADHD Anxiety No Diagnoses
Age in years 10.00 (0.45) 9.30 (0.82) 9.08 (0.88) 9.35 (0.93)FSIQ 78.00 (11.00) 85.78 (12.62) 92.92 (13.89) 94.82 (11.87)Inattention 10.82 (4.33) 8.78 (4.47) 3.88 (4.00) 2.61 (3.31)Inhibition 21.09 (5.28) 18.70 (5.43) 12.71 (3.00) 13.13 (3.68)Shift 17.36 (4.23) 12.52 (4.85) 13.67 (3.71) 10.55 (2.68)EmoContr 22.36 (5.50) 18.00 (6.11) 17.04 (4.54) 13.97 (4.06)WM 24.55 (4.28) 22.70 (4.19) 15.42 (4.21) 14.71 (4.54)
Note: FSIQ = full scale IQ; Inhibition = inhibit scale; Shift = shift scale; EmoContr = emotional control scale; WM = working memory scale.
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

Sørensen et al. 61
the Working Memory scale (F(1, 154) = 57.14, p < .001) and were marginally significant on the Shift scale (F(1, 154) = 3.77, p = .054). FSIQ appeared not to covary with any BRIEF scale.
DiscussionIn line with the main hypothesis, anxious children with ADHD were scored significantly higher on the Inhibit scale
by their parents than children with a “pure” ADHD or a “pure” anxiety disorder. Thus, the comorbid group showed a distinct symptom pattern of impaired inhibitory control function, whereas the comorbid group’s abilities to shift attention, control emotional processes, and use their work-ing memory capacity were similar to the abilities shown in the “pure” disorder groups. This confirms the assumption of an impaired attentional control in anxious children (Eysenck et al., 2007; Muris, 2006; Muris et al., 2006).
5,00
10,00
15,00
20,00
25,00
Inhibit Shift
ADHD + Anx
ADHD
Anxiety
No diagnoses
*
Emotional Control Working Memory
Figure 2. The estimated marginal means for the four diagnostic groups from the analysis of an interaction effect between an ADHD and anxiety disorder
0,00
5,00
10,00
15,00
20,00
25,00
Inhibit
ADHD
No ADHD
Working MemoryEmotional ControlShift
** * **
Figure 3. The estimated marginal means for the groups with and without ADHD on the four BRIEF scalesNote: BRIEF = Behavior Rating Inventory of Executive Function.
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from
62 Journal of Attention Disorders 15(1)
Children with a “pure” anxiety disorder, however, were not scored significantly different from the children with no diagnosis on the Inhibit scale, indicating that anxiety in itself was not associated with an impaired ability to inhibit responses, as observed by the parents in their everyday life.
Previous studies based on psychometric test results (Manassis et al., 2000; Pliszka, 1989, 1992) and observa-tion of behavior (Abikoff et al., 2002) have not found more severe problems in inhibiting impulses among anxious chil-dren with ADHD than in children with “pure” ADHD. However, our finding of impaired inhibitory control in chil-dren with ADHD and a comorbid anxiety disorder confirms a recent finding in children with ADHD and a comorbid bipolar disorder whom were scored significantly higher on the BRI score from BRIEF by their parents (Warner, 2005). Moreover, Taylor et al. (2008) showed that adults with bipolar disorder reported higher levels of impulsivity in association with a comorbid anxiety disorder. This may indicate that in neuropsychiatric disorders associated with low impulse control, the presence of an anxiety disorder will aggravate the inhibitory dysfunction in everyday behavior. However, the results in the present study did not support problems related to behavioral inhibition in chil-dren with a “pure” anxiety disorder. The use of parent reports may have contributed to this finding. Parents are better informants concerning children’s inhibitory control than teachers (McCandless & O’ Laughlin, 2007), and their responses are shown to better reflect the child’s everyday inhibition functioning than performance on psychometric tests (Bodnar, Prahme, Cutting, Denckla, & Mahone, 2007). Parents, however, may not have observed that their anxious child displays a reduced ability to control their impulses in
novel or performance-based situations (Eysenck et al., 2007). When the anxiety disorder is combined with ADHD, the parents may be biased toward the children’s behavior in general and in specific situations. Problems of behavioral regulation are strongly associated with ADHD and a decreased impulse control is more overt in the everyday life com-pared to characteristics of “pure” anxious children. Furthermore, the higher parent scores on the Inhibit scale in the group of children with ADHD and anxiety compared to in the “pure” disorder groups may have been influenced by the skewed rates of ODD as a comorbid disorder between the diagnostic groups. Newcorn et al. (2001) showed that a combined comorbidity of ODD and CD in children with ADHD and anxiety increased the level of parent reported impulsivity symptoms. However, in the present study none of the children had a comorbid CD characterized by a more severe behavioral disinhibition than a comorbid ODD, sug-gesting that the inhibitory dysfunction shown in children with ADHD in the present study was aggravated by the comorbid anxiety disorder.
Deficits in set-shifting were specific for anxious children. This may indicate that the behavioral inhibition used to describe anxious children (Biederman et al., 1993; Muris, 2006) fits well with the items included in the Shift scale in the BRIEF questionnaire (Gioia et al., 2000). A reduced cog-nitive flexibility may make it difficult for a child to approach and adjust to new settings. The set-shift ability also influences the ability to shift emotional state, two abilities which in combination predict social function (Wilson, 2003). How-ever, problems with emotional control were reported both in children with anxiety disorder and in children with ADHD in the present study. This may support a model of two
0,00
5,00
10,00
15,00
20,00
25,00
Inhibit
Anxiety
No anxiety
Working MemoryEmotional ControlShift
**
**
Figure 4. The estimated marginal means for the groups with and without anxiety disorder on the four BRIEF scalesNote: BRIEF = Behavior Rating Inventory of Executive Function.
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

Sørensen et al. 63
different routes to emotional dysregulation among children with an ADHD and anxiety disorder. Impaired ability to inhibit responses in children with ADHD may lead to a top-down emotional dysregulation (Mullin & Hinshaw, 2007). On the other hand, anxious children may have a primarily emo-tional dysregulation causing a bottom-up control dysfunction leading to problems inhibiting responses and shifting atten-tion focus (Eysenck et al., 2007).
ADHD and anxiety disorder cause a behavioral dysregu-lation which in turn may impair working memory function (Barkley, 1997; Eysenck et al., 2007). Children with comor-bid ADHD and anxiety disorder perform worse on working memory tasks than children with one of the disorders alone (Pliszka, 1989). Furthermore, their working memory func-tion are shown to respond less positively to methylphenidate treatment compare to responses in nonanxious children with ADHD (Bedard & Tannock, 2008; Tannock, Ickowicz, & Schachar, 1995). Despite the finding of the most impaired ability to repress impulses in the comorbid group, we did not find any significant difference in their working memory function when the comorbid group was compared with the “pure” ADHD group. Anxiety may, however, cause working memory problems depending on specific situations charac-terized by novelty or pressure on performance which is not tapped through parent reports. Teachers are shown to be better informants of working memory deficits than parents, probably because they observe the children in settings with high demands on the working memory function (McCandless & O’ Laughlin, 2007). In addition, the work-ing memory scale in the BRIEF comprises items measuring sustained attention (Gioia et al., 2000) and may therefore be more sensitive to deficits in children with ADHD than in children with an anxiety disorder.
Our sample showed significant differences between the groups in relation to age, gender, FSIQ, and inattention symptoms. Those variables were included in the analyses as covariates to control for differences between groups. Some main effects of these covariates should be commented. Gender and age explained a significant proportion of the variance on the Inhibit scale, which can be explained by boys with ADHD to be more impulsive than girls (Gershon, 2002). Moreover, the age-effect is probably caused by the children with ADHD being older than the children in the “pure” anxiety disorder and no diagnosis groups. Gender was also covarying with the Working Memory scale, a find-ing that may be explained by the unbalanced gender representation in the ADHD groups. The dimensional score on the Inattention subscale did also covary on the Inhibit scale, supporting previous findings of inattention symp-toms being associated with response inhibition (Chhabildas et al., 2001; Gioia et al., 2000). However, main effects of inattention symptoms were related both to ADHD and anxi-ety disorder. Failure to control for inattention may therefore explain previous conflicting results in studies of behavioral
regulation in children. Symptoms of inattention showed a statistical tendency to covary on the Shift scale as well, indicating cognitive flexibility to be associated with the core inattention symptoms of an ADHD diagnosis. The finding that FSIQ did not explain the variance on any of the BRIEF scales should be emphasized. This is in contrast to findings in an earlier study of children with ADHD in the BCS using psychometric test measures of attention/execu-tive functions (Adolfsdottir, Sorensen, & Lundervold, 2008), supporting the hypothesis that the BRIEF gives a reliable measure of control function in children on all levels of FSIQ (Mahone et al., 2002b).
Strengths and LimitationsThe main strengths of the present study were our use of an ecologically valid measure of the children’s control func-tioning and further, the control for intelligence level and inattention symptoms. In addition, the cases and controls were selected from a population-based sample of children, and the clinicians providing diagnosis were blind to the results from the other parts of the assessment.
However, some limitations should be noted. The selec-tion of groups in the present study was driven by the aim to make the groups as “pure” as possible to determine the influ-ence of the two disorders on the functions assessed by the BRIEF. This makes the groups different from what clini-cians meet in their clinical practice (Kadesjö & Gillberg, 2001) and in addition reduces the group sizes. This was pri-marily affecting the size of the comorbid group since this group was associated with exceeding comorbid disorder diagnoses than the nonanxious children with ADHD. Fur-thermore, the selection procedure from the first to the third stage of the BCS resulted in different group characteristics with regard to gender, age, and IQ.
Selecting children in risk of mental health problems from a population-based sample such as in the first to the third stage of the BCS, typically results in a lower fre-quency of anxiety disorders compared to selection from clinical samples (Ferdinand, Van Lang, Ormel, & Ver-hulst, 2006). Simple phobia is the most prevalent anxiety disorder in a population (Essau, Conradt, & Petermann, 2000; Silverman & Eisen, 1992), which also was the case in the present study (54.5% in the comorbid group were diagnosed with simple phobia and 54.2% in the “pure” anxiety group). A simple phobia may not cause as severe cognitive control dysfunctions as a general anxiety disor-der, but is still associated with psychosocial impairment (Wittchen, Nelson, & Lachner, 1998) and a chronic course (Wittchen & Essau, 1993). In addition, the theory used in the present study regarding a decrease in attentional con-trol in anxious children is emphasized to be relevant within normal populations (Eysenck et al., 2007). Lastly, parents completed the Inattention subscale about 18 months prior
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

64 Journal of Attention Disorders 15(1)
to the assessment including the BRIEF. Still, we found it important to include this measure of inattention, in that the inattention symptom cluster is shown to influence the Inhibit function (Chhabildas et al., 2001; Gioia et al., 2000).
ConclusionThe findings in the present study imply that a comorbid anx-iety disorder in children with ADHD aggravates problems related to inhibition, adjustment to new settings (i.e., cogni-tive flexibility), and emotional control. These increased difficulties among anxious children with ADHD highlight the importance of including more ecologically valid mea-sures of the everyday life functioning into clinical evaluations and research projects.
Acknowledgments
Thanks to the ADHD organization in Norway for supporting the project. Further, we want to thank C. Gillberg, K. M. Stormark, E. Heiervang, and M. Heimann, the project group of the Bergen Child Study, and K. Hughdal and J. Stevenson for comments on the man-uscript. We are also grateful to the children and parents who participated in the study.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interests with respect to their authorship or the publication of this article.
Funding
This study was financially supported by the Organization of Health and Rehabilitation, the Centre for Child and Adolescent Mental Health, the University of Bergen, the Norwegian Director-ate for Health and Social Affairs, the Western Norway Regional Health Authority, and the Research Council of Norway.
References
Abikoff, H. B., Jensen, P. S., Arnold, L. L., Hoza, B., Hechtman, L., Pollack, S., et al. (2002). Observed classroom behavior of chil-dren with ADHD: Relationship to gender and comorbidity. Journal of Abnormal Child Psychology, 30, 349-359.
Adolfsdottir, S., Sorensen, L., & Lundervold, A. J. (2008). The attention network test: A characteristic pattern of deficits in children with ADHD. Behavioral and Brain Functions, 4, 9.
Ambrosini, P. J. (2000). Historical development and present status of the schedule for affective disorders and schizophrenia for school-age children (K-SADS). Journal of American Academy of Child and Adolescent Psychiatry, 39, 49-58.
American Psychiatric Association. (1994). Diagnostic and statis-tical manual of mental disorders (4th ed.). Washington, DC: Author.
Barkley, R. A. (1997). Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin, 121, 65-94.
Bedard, A.-C., & Tannock, R. (2008). Anxiety, methylphenidate response, and working memory in children with ADHD. Jour-nal of Attention Disorders, 11, 546-557.
Biederman, J., Rosenbaum, J. F., Bolduc-Murphy, E. A., Faraone, S. V., Chaloff, J., Hirshfeld, D. R., et al. (1993). A 3-year follow-up of children with and without behavioral inhi-bition. Journal of American Academy of Child and Adolescent Psychiatry, 32, 814-821.
Bodnar, L. E., Prahme, M. C., Cutting, L. E., Denckla, M. B., & Mahone, E. M. (2007). Construct validity of parent ratings of inhibitory control. Child Neuropsychology, 13, 345-362.
Chhabildas, N., Pennington, B. F., & Willcutt, E. G. (2001). A comparison of the neuropsychological profiles of the DSM-IV subtypes of ADHD. Journal of Abnormal Child Psychol-ogy, 29, 529-540.
Eilertsen, B., & Johnsen, I. M. B. (2003). Manual for Wechsler Intelligence Scale for Children (3rd ed., Norwegian version). Oslo: Assesio.
Essau, C. A., Conradt, J., & Petermann, F. (2000). Frequency, comorbidity, and psychosocial impairment of anxiety disor-ders in German adolescents. Journal of Anxiety Disorders, 14, 263-279.
Eysenck, M. W., Derakshan, N., Santos, R., & Calvo, M. G. (2007). Anxiety and cognitive performance: Attentional con-trol theory. Emotion, 7, 336-353.
Ferdinand, R. F., Van Lang, N. D., Ormel, J., & Verhulst, F. C. (2006). No distinctions between different types of anxiety symptoms in pre-adolescents from the general population. Journal of Anxiety Disorders, 20, 207-221.
Gershon, J. (2002). A meta-analytic review of gender differences in ADHD. Journal of Attention Disorders, 5, 143-154.
Gioia, G. A., Isquith, P. K., Guy, S. C., & Kenworthy, L. (2000). Behavior Rating Inventory of executive function professional manual. Odessa, FL: PAR.
Goodman, R. (1999). The extended version of the Strengths and Difficulties Questionnaire as a guide to child psychiatric case-ness and consequent burden. Journal of Child Psychology and Psychiatry, 40, 791-799.
Gray, J. A. (1971). The psychology of fear and stress. New York: McGraw-Hill.
Gray, J. A. (1972). The psychophysiological nature of introversion-extraversion: A modification of Eysenck’s theory. In V. D. Neblit-sin & J. A. Gray (Eds.), Biological bases of individual behaviour (pp. 182-205). New York, Academic Press.
Heiervang, E., Stormark, K. M., Lundervold, A. J., Heimann, M., Goodman, R., Posserud, M. B., et al. (2007). Psychiatric dis-orders in Norwegian 8- to 10-year-olds: An epidemiological survey of prevalence, risk factors, and service use. Journal of American Academy of Child and Adolescent Psychiatry, 46, 438-447.
Jensen, P. S., Martin, D., & Cantwell, D. P. (1997). Comorbidity in ADHD: Implications for research, practice, and DSM-IV. Journal of American Academy of Child and Adolescent Psy-chiatry, 36, 1065-1079.
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

Sørensen et al. 65
Kadesjö, B., & Gillberg, C. (2001). The comorbidity of ADHD in the general population of Swedish school-age children. Jour-nal of Child and Psychology and Psychiatry, 42, 487-492.
Kaufman, J., Birmaher, B., Brent, D., Rao, U., Flynn, C., Moreci, P., et al. (1997). Schedule for affective disorders and schizo-phrenia for school-age children-present and lifetime version (K-SADS-PL): Initial reliability and validity data. Journal of American Academy of Child and Adolescent Psychiatry, 36, 980-988.
Mahone, E. M., Cirino, P. T., Cutting, L. E., Cerrone, P. M., Hagelthorn, K. M., Hiemenz, J. R., et al. (2002a). Validity of the behavior rating inventory of executive function in children with ADHD and/or Tourette syndrome. Archives of Clinical Neuropsychology, 17, 643-662.
Mahone, E. M., Hagelthorn, K. M., Cutting, L. E., Schuerholz, L. J., Pelletier, S. F., Rawlins, C., et al. (2002b). Effects of IQ on executive function measures in children with ADHD. Child Neuropsychology, 8, 52-65.
Manassis, K., Tannock, R., & Barbosa, J. (2000). Dichotic listen-ing and response inhibition in children with comorbid anxiety disorders and ADHD. Journal of American Academy of Child and Adolescent Psychiatry, 39, 1152-1159.
McCandless, S., & O’ Laughlin, L. (2007). The Clinical Utility of the Behavior Rating Inventory of Executive Function (BRIEF) in the diagnosis of ADHD. Journal of Attention Disorders, 10, 381-389.
Mullin, B. C., & Hinshaw, S. P. (2007). Emotion regulation and externalizing disorders in children and adolescents. In J. J. Gross (Ed.), Handbook of emotional regulation (pp. 523-541). New York: Guilford.
Muris, P. (2006). The pathogenesis of childhood anxiety disor-ders: Considerations from a developmental psychopathology perspective. International Journal of Behavioral Development, 30, 5-11.
Muris, P., Meesters, C., & Rompelberg, L. (2006). Attention control in middle childhood: Relations to psychopathologi-cal symptoms and threat perception distortions. Behaviour Research and Therapy, 45, 997-1010.
Newcorn, J. H., Halperin, J. M., Jensen, P. S., Abikoff, H. B., Arnold, L. E., Cantwell, D. P., et al. (2001). Symptom profiles in children with ADHD: Effects of comorbidity and gender. Journal of American Academy of Child and Adolescent Psy-chiatry, 40, 137-146.
Oosterlaan, J., Logan, G. D., & Sergeant, J. A. (1998). Response inhibition in AD/HD, CD, comorbid AD/HD + CD, anxious, and control children: a meta-analysis of studies with the stop task. Journal of Child Psychology and Psychiatry, 39, 411-425.
Oosterlaan, J., & Sergeant, J. A. (1998). Response inhibition and response re-engagement in attention-deficit/hyperactivity dis-order, disruptive, anxious and normal children. Behavioural Brain Research, 94, 33-43.
Pliszka, S. R. (1989). Effect of anxiety on cognition, behavior, and stimulant response in ADHD. Journal of American Academy of Child and Adolescent Psychiatry, 28, 882-887.
Pliszka, S. R. (1992). Comorbidity of attention-deficit hyperac-tivity disorder and overanxious disorder. Journal of American Academy of Child and Adolescent Psychiatry, 31, 197-203.
Pliszka, S. R., Carlson, C. L., & Swanson, J. M. (1999). ADHD with comorbid disorders. Clinical assessment and manage-ment. New York: Guilford.
Pliszka, S. R., Hatch, J. P., Borcherding, S. H., & Rogeness, G. A. (1993). Classical conditioning in children with attention deficit hyperactivity disorder (ADHD) and anxiety disorders: A test of Quay’s model. Journal of Abnormal Child Psychology, 21, 411-423.
Quay, H. C. (1988). The behavioral reward and inhibition system in childhood behavior disorder. In L. M. Bloomingdale (Ed.), Atten-tion deficit disorder. New research in attention treatment of psy-chopharmacology (Vol. 3, pp. 176-186). Oxford: Pergamon Press.
Schatz, D. B., & Rostain, A. L. (2006). ADHD with comorbid anxiety: A review of the current literature. Journal of Attention Disorders, 10, 141-149.
Silverman, W. K., & Eisen, A. R. (1992). Age differences in the reliability of parent and child reports of child anxious symp-tomatology using a structured interview. Journal of American Academy of Child and Adolescent Psychiatry, 31, 117-124.
Sonnander, K., Ramund, B., & Smedler, A.-C. (1999). Manual for Wechsler Intelligence Scale for Children (3rd ed., Swedish ver-sion). Stockholm: Psykologiforlaget AB.
Stefanatos, G. A., & Baron, I. S. (2007). Attention-deficit/ hyperactivity disorder: A neuropsychological perspective towards DSM-V. Neuropsychology Review, 17, 5-38.
Stormark, K. M., Heiervang, E., Heimann, M., Lundervold, A., & Gillberg, C. (2008). Predicting nonresponse bias from teacher ratings of mental health problems in primary school children. Journal of Abnormal Child Psychology, 36, 411-419.
Sundberg, H., Egeland, J., Andreassen, T. H., & Stensli, O. (2006). Comparison of WISC-R and WISC-III scores in a clinical sample: Are WISC-III flawed, or are WISC-R norms outdated? Journal of the Norwegian Psychological Associa-tion, 43, 476-481.
Swanson, J. M., Kraemer, H. C., Hinshaw, S. P., Arnold, L. E., Conners, C. K., Abikoff, H. B., et al. (2001). Clinical relevance of the primary findings of the MTA: Success rates based on severity of ADHD and ODD symptoms at the end of treatment. Journal of American Academy of Child and Adolescent Psy-chiatry, 40, 168-179.
Tannock, R. (2000). Attention-deficit/hyperacitivty disorder with anxiety disorders. In T. E. Brown (Ed.), Attention-deficit dis-orders and comorbidities in children, adolescents, and adults (pp. 125-170). Washington, DC: American Psyciatric Press.
Tannock, R., Ickowicz, A., & Schachar, R. (1995). Differential effects of methylphenidate on working memory in ADHD
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from

66 Journal of Attention Disorders 15(1)
children with and without comorbid anxiety. Journal of American Academy of Child and Adolescent Psychiatry, 34, 886-896.
Taylor, C. T., Hirshfeld-Becker, D. R., Ostacher, M. J., Chow, C. W., Lebeau, R. T., Pollack, M. H., et al. (2008). Anxiety is associ-ated with impulsivity in bipolar disorder. Journal of Anxiety Disorders, 22, 868-876.
Warner, J. L. (2005). Executive functioning deficits in youth diag-nosed with comorbid bipolar disorder+ADHD. Unpublished doctoral dissertation, The University of Cincinnati—Cincinnati.
Wechsler, D. (1991). Wechsler Intelligence Scale for Children (3rd ed.). San Antonio: Psychological Corp.
Willcutt, E. G., Doyle, A. E., Nigg, J. T., Faraone, S. V., & Pennington, B. F. (2005). Validity of the executive function theory of attention-deficit/hyperactivity disorder: A meta-analytic review. Biological Psychiatry, 57, 1336-1346.
Wilson, B. J. (2003). The role of attentional processes in children’s prosocial behavior with peers: Attention shifting and emotion. Development and Psychopathology, 15, 313-329.
Wittchen, H.-U., & Essau, C. A. (1993). Epidemiology of anxi-ety disorders. In P. J. Wilner (Ed.), Psychiatry (pp. 1-25). Philadelphia, PA: J.B. Lippincott Company.
Wittchen, H.-U., Nelson, C. B., & Lachner, G. (1998). Preva-lence of mental disorders and psychosocial impairments in adolescents and young adults. Psychological Medicine, 28, 109-126.
Bios
Lin Sørensen is a psychologist and in a postdoc position at the University of Bergen and at Division of Psychiatry, Haukeland University Hospital, Norway. Her main research interests are cog-nitive functioning and emotional control in children with symptoms of ADHD.
Kerstin J. Plessen is a specialist in child- and adolescent psychiatry and an associate professor at the University of Bergen. Her main research interest focuses on the brain/behavior correlates during development, such as brain development in children with Tourette syndrome and emotional regulation in children with ADHD.
Jude Nicholas is a specialist in clinical neuropsychology. He specializes in the evaluation and treatment of patients with sen-sory impairment and neuropsychological disorders. His current research investigates the effects of early sensory impairment on the development of neuropsychological functions, especially tac-tile cognitions.
Astri J. Lundervold is a professor in neuropsychology and head of the Neuropsychological Phenotyping Group at the University of Bergen, Norway. Her main research interest is to characterize behavior associated with normal function and neuropsychiatric disorders across the life span.
at Universitetsbiblioteket i Bergen on November 8, 2011jad.sagepub.comDownloaded from






![THE UNIVERSITY OF TEXAS Conflict Of Interests … Assessment & Identification of Comorbid Conditions [OSA, Hypoventilation, Cardiovascular, Difficult airway, DM] Comorbid Conditions](https://static.fdocuments.us/doc/165x107/5b2238847f8b9aac368b4668/the-university-of-texas-conflict-of-interests-assessment-identification-of-comorbid.jpg)











